ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes © 2013 Paradigm Medical Communications, LLC except where noted. 1 © 2013 Paradigm Medical Communications, LLC, except where noted. Content may not be reproduced in whole or in part without the express written consent of Paradigm Medical Communications, LLC. Agenda Welcome and Introductions Antibiotic Challenges in the Management of ABSSSIs G. Ralph Corey Presentation and Panel Discussion Community‐Acquired Pneumonia: Continuing Thomas M. File Jr Questions and Controversies Presentation and Panel Discussion The AI Team: Antibiotic Stewardship that Ensures Michael J. Rybak Optimal Outcomes Presentation and Panel Discussion Questions & Answers All Faculty AI, anti‐infection

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.1
© 2013 Paradigm Medical Communications, LLC, except where noted. Content may not be reproduced in whole or in part without the express written consent of Paradigm Medical Communications, LLC.
Agenda
Welcome and Introductions
Antibiotic Challenges in the Management of ABSSSIs G. Ralph CoreyPresentation and Panel Discussion
Community‐Acquired Pneumonia: Continuing Thomas M. File Jr
Questions and ControversiesPresentation and Panel Discussion
The AI Team: Antibiotic Stewardship that Ensures Michael J. Rybak
Optimal Outcomes Presentation and Panel Discussion
Questions & Answers All Faculty
AI, anti‐infection
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.2
Faculty and Disclosures
Thomas M. File Jr, MD, MSc, MACP, FIDSA, FCCP (Chair)Professor, Internal Medicine; Master Teacher
Chair, Infectious Disease SectionNortheast Ohio Medical UniversityRootstown, OHChair, Infectious Disease DivisionSumma Health SystemAkron, OH
G. Ralph Corey, MDGary Hock Distinguished Professor of Global Health
Vice‐Chair of Education and Global HealthDirector, Hubert‐Yeargan Center for Global Health
Professor of Medicine, Pathology, and Infectious Diseases
Duke University Medical CenterDurham, NC
Michael J. Rybak, PharmD, MPH, FCCP, FIDSAProfessor of Pharmacy and MedicineDirector, Anti‐Infective Research Laboratory
Department of Pharmacy PracticeEugene Applebaum College of Pharmacy
Wayne State University Detroit, MI
Consultant: Astellas Pharma US, Inc; Bayer AG; Daiichi Sankyo Co, Ltd; Cubist Pharmaceuticals; Durata Therapeutics, Inc; Forest Laboratories, Inc; GlaxoSmithKline; Merck & Co, Inc; Pfizer, Inc; Tetraphase Pharmaceuticals
Research Support: Boehringer IngelheimGmbH; Gilead Sciences, Inc; Pfizer Inc; Tibotec Pharmaceuticals
Advisory Board: Achaogen, Inc; Cempra; Cerexa, Inc; Forest Laboratories, Inc; Gilead Sciences, Inc; Inimex Pharmaceuticals, Inc; PolyMedix, Inc; Rib‐X Pharma‐ceuticals, Inc; Theravance, Inc; TMC Pharma Services Ltd; Trius Therapeutics
Consultant: Achaeogen, Inc; Cempra; Cerexa, Inc; ContraFect Corporation; Cubist Pharmaceuticals; Dr. Reddy’s Laboratories, Ltd.; Forest Laborato‐ries, Inc; Furiex Pharmaceuticals, Inc; Glaxo‐SmithKline; Inimex Pharmaceuticals, Inc; Innocoll, Inc; Merck & Co, Inc; Pfizer, Inc; Poly‐Medix, Inc; Rib‐X Pharmaceuticals, Inc; Thera‐vance, Inc; TMC Pharma Services Ltd; Trius Therapeutics
Research Support: Cempra; Cerexa, Inc; Dr. Reddy’s Laboratories, Ltd; Forest Laboratories, Inc; GlaxoSmithKline; Innocoll, Inc; Theravance, Inc; TMC Pharma Services Ltd
Research Support: Cerexa, Inc; Cubist Pharmaceuticals; Forest Laboratories, Inc; National Institutes of Health
Speaker: Cubist Pharmaceuticals; Forest Laboratories, Inc; Novartis Corporation
Continuing Medical Education (CME) Information
Educational ObjectivesUpon proper completion of this activity, participants should be better able to:
• Describe the prevalence of causative pathogens in ABSSSIs and the susceptibility of antibiotics approved to treat them.
• Incorporate evidence‐based practices, including 2013 Joint Commission/CMS Core Measures, when managing patients with CABP in the hospital setting.
• Discuss novel, team‐centered approaches for implementing antimicrobial stewardship practices in the hospital setting.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.3
ANTIBIOTIC CHALLENGESIN THE MANAGEMENT OF ABSSSIS:
IS THERE A PLACE FOR NEWER AGENTS?Ralph Corey, MD
Vice‐Chair for Education and Global HealthProfessor of Medicine
Division of Infectious DiseasesDuke University School of Medicine
Durham, NC
5 Steps to Diagnosis and Treatment of Skin and Skin Structure Infections
1. Make sure it is an infection
2. Search for exposures and atypical pathogens
3. Define the severity and depth of infection
4. Define patient’s immune status
5. Treat for Staphylococcus (including MRSA–always!)
and Streptococcus (not including enterococcus)
– Not every antibiotic that kills staph also kills strep
– Be aware of local patterns of resistance
19

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.4
1. MAKE SURE IT IS AN INFECTION
Stasis Dermatitis
21Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.5
Fixed Drug Eruption
Cutaneous manifestation of an adverse drug reaction
22Photo courtesy of Ralph Corey, MD. All rights reserved.
Is this ABSSSI?
23
• Yes
• No
Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.6
Intentional Burn
24Photo courtesy of Ralph Corey, MD. All rights reserved.
2. SEARCH FOR EXPOSURES AND
ATYPICAL PATHOGENS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.7
Bites: You Are What You Eat
• Dog: Capnocytophyga
• Cat/lion: Pasteurella
• Bear: Staphylococcus aureus!
• Snake: oral flora = fecal flora of the rat it just ate!
26
Other Causes
• Water contamination
– Fresh water: Aeromonas
– Salt water: Erysipelothrix, Vibrio vulnificus, Mycobacterium marinum
• Trauma
– Clostridia, Pseudomonas
• Many others
27
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.8
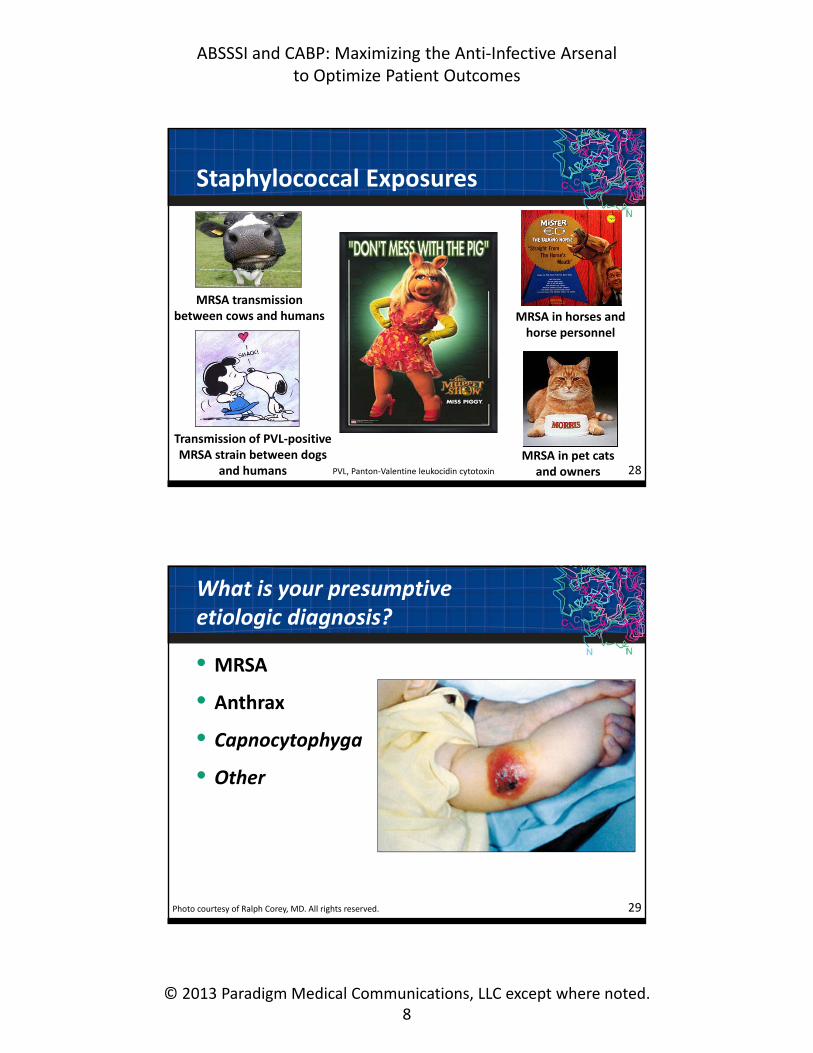
Staphylococcal Exposures
28
MRSA transmission between cows and humans
Transmission of PVL‐positive MRSA strain between dogs
and humans
MRSA in horses and horse personnel
MRSA in pet cats and ownersPVL, Panton‐Valentine leukocidin cytotoxin
What is your presumptive etiologic diagnosis?
• MRSA
• Anthrax
• Capnocytophyga
• Other
29Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.9
Cutaneous Anthrax
30Photo courtesy of Ralph Corey, MD. All rights reserved.
3. DEFINE THE SEVERITY AND
DEPTH OF INFECTION
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.10
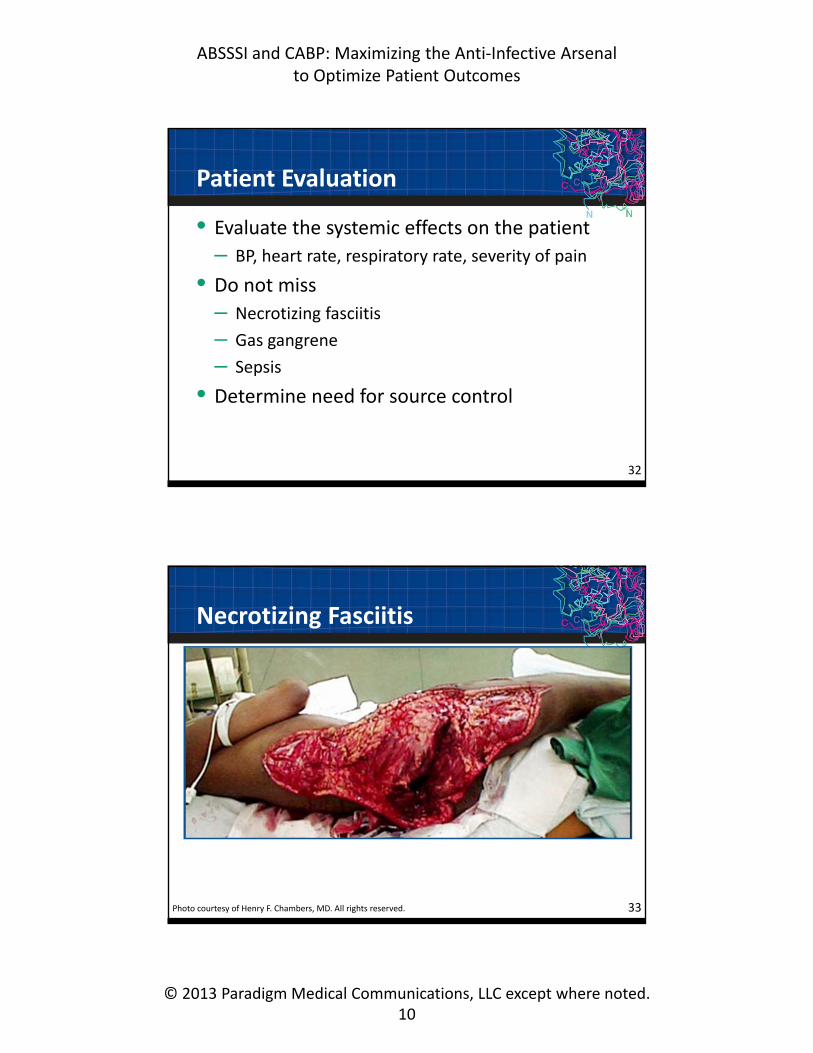
Patient Evaluation
• Evaluate the systemic effects on the patient
– BP, heart rate, respiratory rate, severity of pain
• Do not miss
– Necrotizing fasciitis
– Gas gangrene
– Sepsis
• Determine need for source control
32
Necrotizing Fasciitis
Photo courtesy of Henry F. Chambers, MD. All rights reserved. 33

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.11
Necrotizing Fasciitis
34Photo courtesy of Ralph Corey, MD. All rights reserved.
An unresponsive 61‐y‐old female with a history of diabetes presented with shock, serum glucose >1000 mg/dL…
Flea Bites
35Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.12
Intraoperative Infection
36Photos courtesy of Ralph Corey, MD. All rights reserved.
Abscess
37Photo courtesy of Ralph Corey, MD. All rights reserved.
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.13
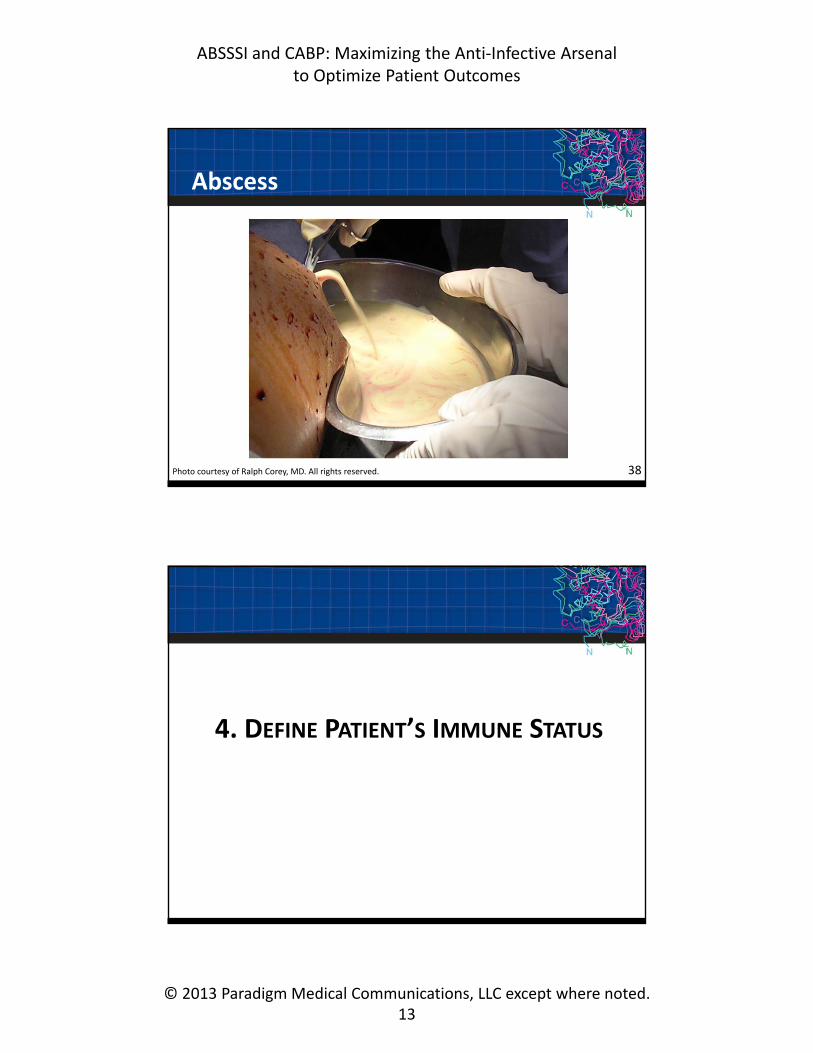
Abscess
38Photo courtesy of Ralph Corey, MD. All rights reserved.
4. DEFINE PATIENT’S IMMUNE STATUS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.14
Immune Status
• Leukopenia– Fungus (Aspergillus, mucor): black fungus
– Bacteremia: ecthyma (Pseudomonas, MRSA)
• Diabetes– Mixed gram‐negative/anaerobic (foot)
– Group B streptococcus
– Fungal coverage (mucor)
40
Ecthyma Gangrenosum
41Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.15
MRSA Ecthyma
Photo courtesy of Noah Craft, MD. 42Photo courtesy of Ralph Corey, MD. All rights reserved.
5. TREAT FOR STAPHYLOCOCCUSAND STREPTOCOCCUS
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.16
Empiric Coverage
• Treat for Staphylococcus (including MRSA–always!) and Streptococcus (not including Enterococcus)
– Remember: not every antibiotic that kills staph also kills strep
– Consider local patterns of antibiotic resistance
44
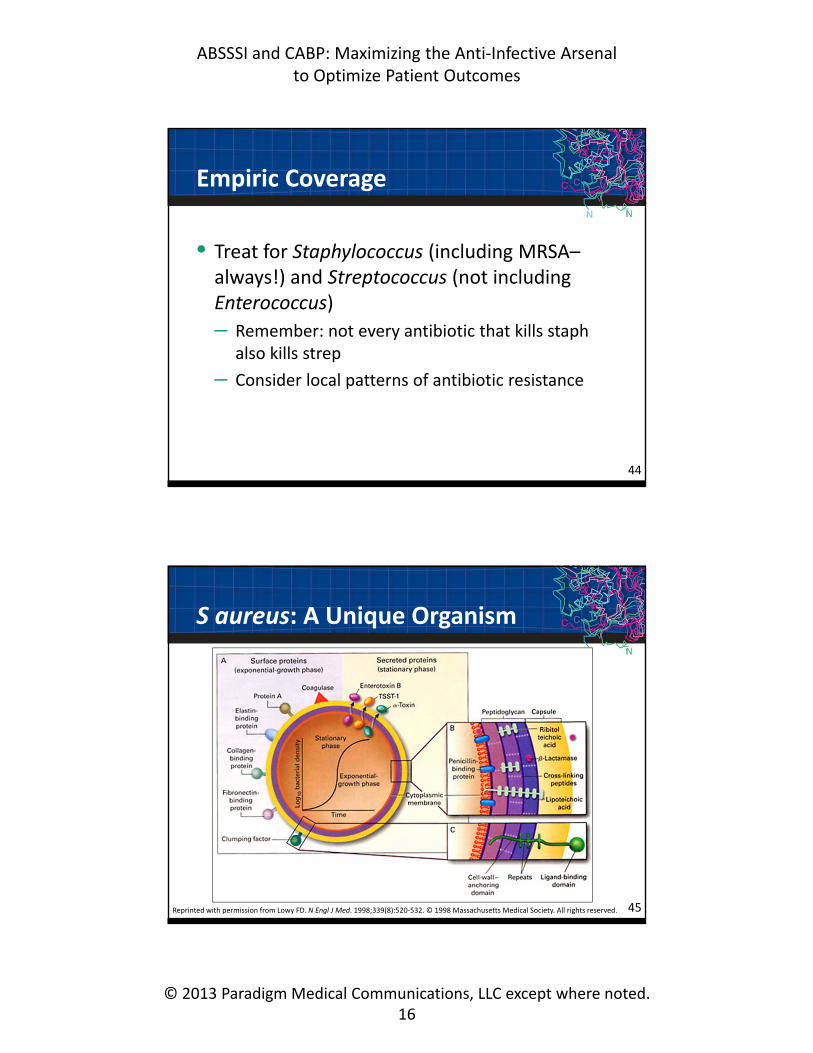
Reprinted with permission from Lowy FD. N Engl J Med. 1998;339(8):520‐532. © 1998 Massachusetts Medical Society. All rights reserved.
S aureus: A Unique Organism
45
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.17
Slide courtesy of Dr. Michael Rybak.1. Rybak MJ et al. Pharmacother. 2004;25:74‐85. 2. Sola C et al. J Clin Microbiol. 2002;40(4):1427‐1435.
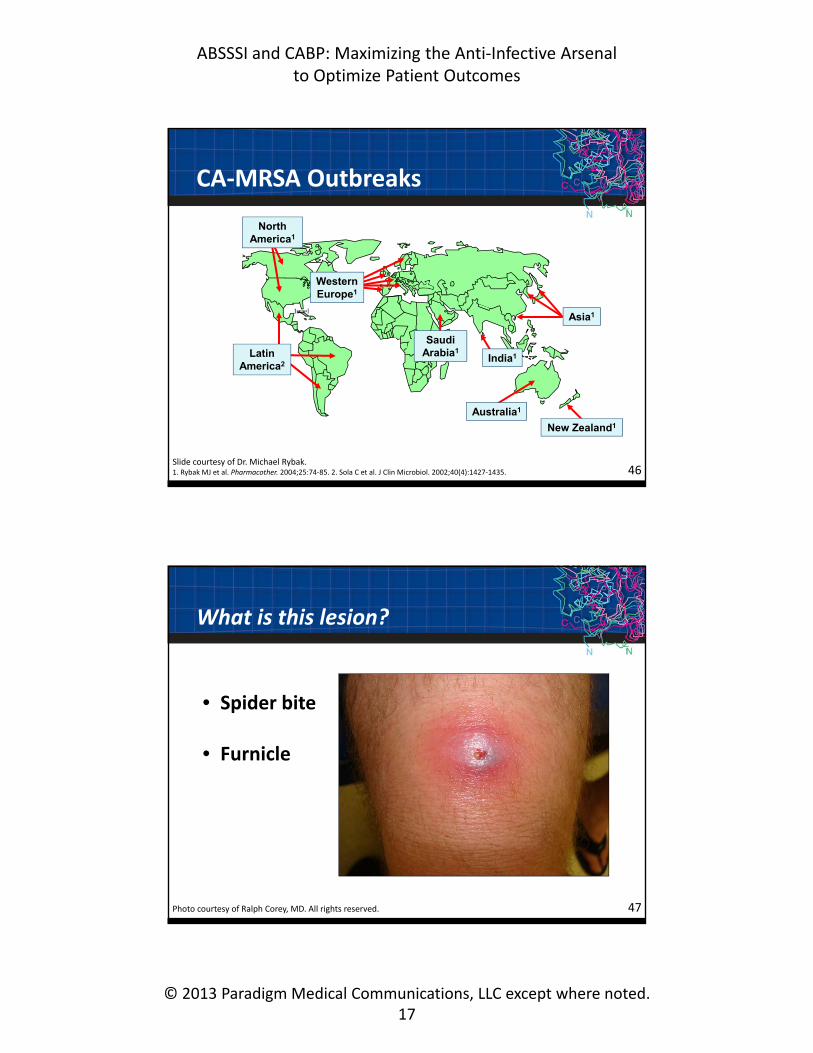
CA‐MRSA Outbreaks
46
IsraelAsia1
Australia1
India1Latin America2
North America1
Western Europe1
New Zealand1
Saudi Arabia1
What is this lesion?
47
• Spider bite
• Furnicle
Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.18
ABSSSIs: “Spider Bites”to Furuncles
48Photos courtesy of Ralph Corey, MD. All rights reserved.
Cellulitis
49Photo courtesy of Ralph Corey, MD. All rights reserved.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.19
Cellulitis
50Photo courtesy of Ralph Corey, MD. All rights reserved.
Cellulitis
51Photo courtesy of Ralph Corey, MD. All rights reserved.
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.20
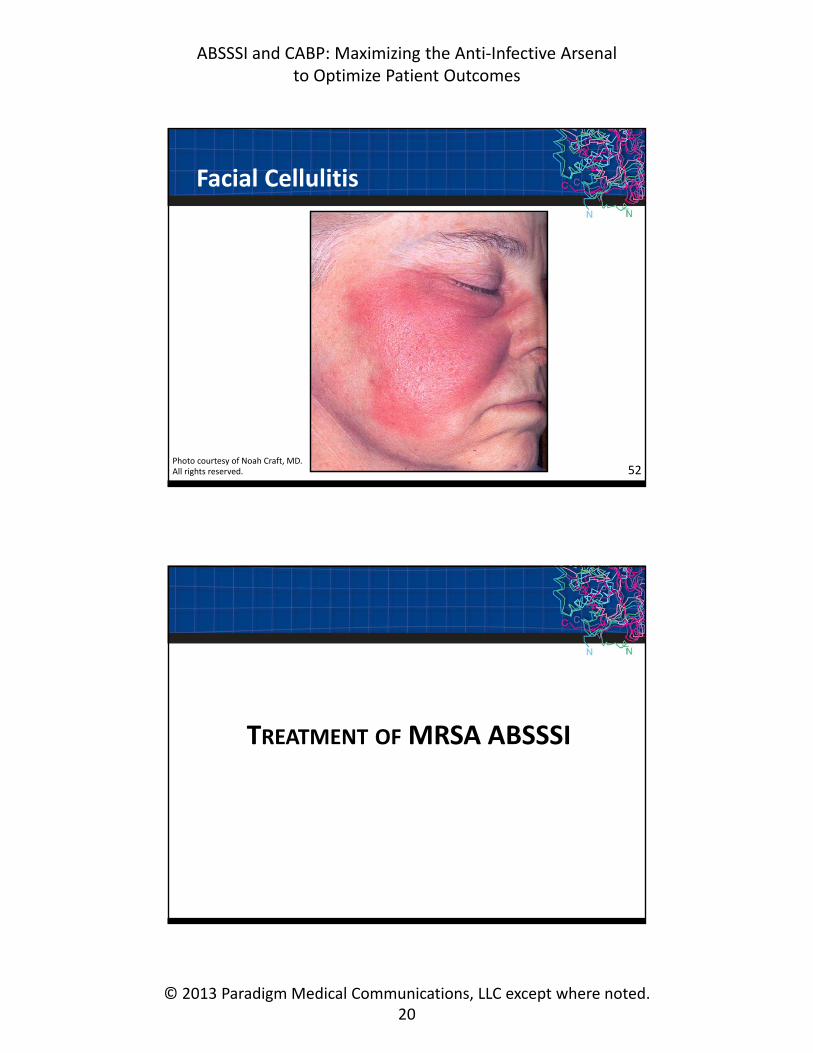
Facial Cellulitis
Photo courtesy of Noah Craft, MD. All rights reserved. 52
TREATMENT OF MRSA ABSSSI

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.21
Key Issues
In addition to efficacy/safety
• Oral therapy: bioavailability
• Abbreviated courses of Rx
• Once daily or weekly dosing: compliance
• Rapid onset of action
– FDA‐mandated early outcomes
54
Antibiotics Commonly Used Off‐Label for MRSA ABSSSI
• TMP/SMX
• Clindamycin
• Tetracyclines
55TMP/SMX, trimethoprim/sulfamethoxazole
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.22
FDA‐Approved MRSA ABSSSI Antibiotics
• Vancomycin
• Linezolid
• Daptomycin
• Telavancin
• Tigecycline
• Ceftaroline
56
ARS
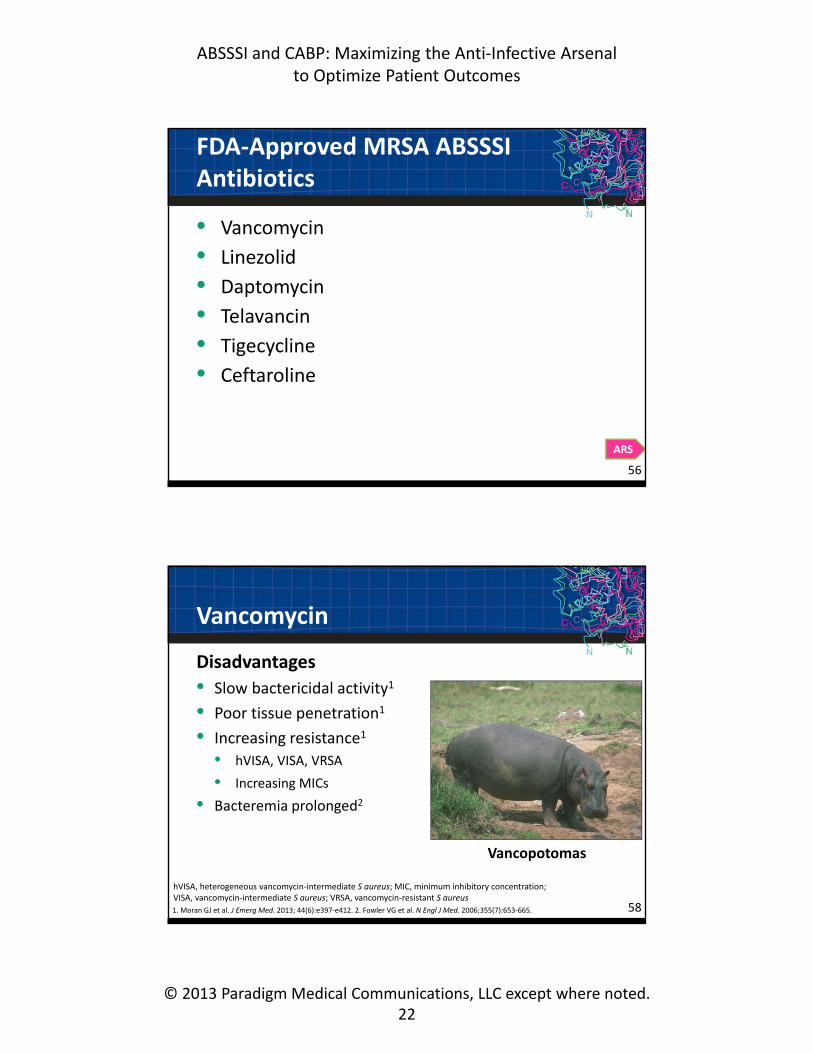
Vancomycin
Disadvantages
• Slow bactericidal activity1
• Poor tissue penetration1
• Increasing resistance1
• hVISA, VISA, VRSA
• Increasing MICs
• Bacteremia prolonged2
581. Moran GJ et al. J Emerg Med. 2013; 44(6):e397‐e412. 2. Fowler VG et al. N Engl J Med. 2006;355(7):653‐665.
Vancopotomas
hVISA, heterogeneous vancomycin‐intermediate S aureus; MIC, minimum inhibitory concentration; VISA, vancomycin‐intermediate S aureus; VRSA, vancomycin‐resistant S aureus

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.23
Linezolid
Advantages• Excellent tissue penetration; protein binding ≈31%1
• Oral and IV formulations2
Disadvantages• Bacteriostatic against gram‐positive pathogens2
• FDA warning on increased risk of death when used to treat CR‐BSI3
• Newly described resistance (Cfr methyltransferase, others)
• Toxicity2
– Bone marrow suppression– Peripheral neuropathy/optic neuritis (after prolonged course)– Lactic acidosis, serotonin syndrome
59
1. Zyvox [package insert]. New York, NY: Pharmacia & Upjohn Company; 2013. 2. Moran GJ et al. J Emerg Med. 2013;44(6):e397‐e412. 3. FDA Drug Safety Alert. 3/16/07. Available at: www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm085249.htm.
CR‐BSI, catheter‐related blood stream infection
Daptomycin
Advantages• Rapidly bactericidal, concentration dependent killing1,2
• Kills without lysis3
• Effective in BSI
Disadvantages• Potential for myotoxicity1 and eosinophilic pneumonia
• Development of treatment‐emergent resistance3
601. Moran GJ et al. J Emerg Med. 2013;44(6):e397‐e412. 2. Stryjewski ME et al. ClinInfect Dis. 2008;46:S368‐S377.3. Bayer AS et al. Ann NY Acad Sci. 2013;1277:139‐158.
BSI, blood‐stream infection

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.24
Telavancin
Advantages• Rapidly bactericidal, concentration‐dependent killing1,2
• Effective in both ABSSSIs and HAP/VAP3
Disadvantages• Renal toxicity with increased mortality (HAP/VAP)1,3
• Risk of fetal toxicity3
611. Moran GJ et al. J Emerg Med. 2013;44(6):e397‐e412. 2. Stryjewski ME et al. Clin Infect Dis. 2008;46:S368‐S377. 3. Vibativ [package insert]. South San Francisco, CA: Theravance, Inc; 2013.
HAP, hospital‐acquired pneumonia; VAP, ventilator‐associated pneumonia
Tigecycline
Advantages• Broad spectrum, active against MRSA, ß‐lactamase
producing gram‐negative (eg, Acinetobacter)1
• Noninferior efficacy in ABSSI2,3
Disadvantages• Bacteriostatic4
• Low serum concentrations5
• Failed HAP/VAP trial6
• Significant incidence of nausea, vomiting2,3,7
• FDA warning of increased risk of death8
62
1. Dryden MS. J Antimicrob Chemother. 2010;65(suppl 3):iii35‐iii44. 2. Sacchidanand S et al. Int J Infect Dis. 2005;9:251‐261. 3. Breedt J et al. Antimicrob Agent Chemother. 2005;49:4658‐4666. 4. Tygacil [package insert]. Philadelphia, PA: Wyeth Pharmaceutical Inc; 2012. 5. SloverCM et al. Ann Pharmacother. 2007;41(6):965‐972. 6. Freire AT et al. Diagn Microbiol Infect Dis. 2010;68(2):140‐151. 7. Mathews P et al. BMC Infect Dis. 2012;12:297. 8. FDA Drug safety Alert. 9/1/10. Available at: www.fda.gov/drugs/drugsafety/ucm224370.htm.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.25
Ceftaroline
Advantages• Broad‐spectrum 5th generation cephalosporin1
• Bactericidal against gram‐positive pathogens, including:
– S aureus MRSA (MIC90 1.0 µg/mL)2
Disadvantages
• Q 12 h dosing
• Eosinophilic pneumonia3
631. Corey GR et al. Clin Infect Dis. 2010;51(6):641‐650. 2. Lodise TP et al. Drugs. 2012;72(1):1473‐1493. 3. Desai KR et al. Pharmacotherapy. 2013;33(7):e166‐e169.
ARS
MRSA ABSSSI Antibiotics in Development
• Oritavancin• Dalbavancin• Tedizolid
• Radezolid• Delafloxacin• 322 GSK• Pleuromutilin BC‐3781• Avarofloxacin
65

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.26
Oritavancin
Advantages
• Rapidly bactericidal against gram positive cocci, including MRSA1
• SOLO I and II in ABSSSI met efficacy endpoints2
– MRSA cure in severe ABSSSI with single IV infusion
– Noninferior to multiple doses of vancomycin IV Q 12 h
• Long half‐life3
Disadvantages
• Long half‐life3
66
1. Stryjewski ME et al. Clin Infect Dis. 2008;46:S368‐S377. 2. The Medicines Company. Press Release. 9/10/13. Available at: http://ir.themedicinescompany.com/phoenix.zhtml?c=122204&p=irol‐newsArticle_pf&id=1853562. 3. Zhanel GG et al. Drugs. 2010;70(7):859‐886.
Dalbavancin
Advantages• Long half‐life supports weekly dosing1
• Bactericidal against gram‐positive cocci, including MRSA1
• In ABSSSI studies noninferior to linezolid1,2
• Long half‐life3
Disadvantages
• Long half‐life3
• Requires 2 doses, results in mandatory follow‐up3
1. Stryjewski ME et al. Clin Infect Dis. 2008;46:S368‐S377. 2. Jauergui LE et al. Clin Infect Dis. 2005;41(10):1407‐1415. 3. Zhanel GG et al. Drugs. 2010;70(7):859‐886. 67

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.27
Tedizolid
Advantages• Activity against major gram‐positive pathogens1
• Available as IV or PO1
– Oral: qd dosing; 6 d was noninferior to linezolid Q 12 h for 10 d1
– IV: qd dosing for 6 d was noninferior to linezolid Q 12 h for 10 d2
• No cfr resistance reported
Disadvantages• Toxicity for extended therapy unknown
68
1. Prokocimer P et al. JAMA. 2013;309(6):559‐569. 2. Fang E et al. Presented at the European Congress of Clinical Microbiology and Infectious Diseases: Berlin; 4/28/13. Poster LB 2964. Available at: http://triusrx.com/pdfs/LB_2964_Efficacy_and_Safety_Results_from_the_ESTABLISH‐2_ABSSSI_Study_Comparing_IV_and_Oral_Tedizolid_Phosphate_and_Linezolid.pdf
The BIG Question Now
Which serious staphylococcal infections will these new compounds “take on”?
• HAP/VAP
• Prosthetic joint infections
• Bloodstream infections (± IE)
• Less commonly considered problems– Meningitis1
– Endophthalmitis2
– Gastroenteritis3
691. Kim JH et al. Rev Infect Dis. 1989;11(5):698‐706. 2. Durand ML. Clin Microbiol Infect. 2013;19(3):227‐234. 3. Boyce JM et al. J Clin Microbiol. 2005;43(12):5992‐5995.
IE, infectious endocarditis

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.28
Conclusions
• Infections of skin and skin structures can be tricky
1. Make sure you are dealing with infection
2. Search for exposures and atypical pathogens
3. Define severity and depth of infection
4. Define patient’s immune status
5. THEN treat for staph (always include MRSA) and strep
• Use the most effective and safest antibiotic for each patient!
70
COMMUNITY‐ACQUIRED PNEUMONIA:CONTINUING QUESTIONS AND CONTROVERSIES
Thomas M. File Jr, MD, MSc, MACP, FIDSA, FCCP Professor, Internal Medicine; Master Teacher;
Head, Infectious Disease SectionNortheastern Ohio Universities College of Medicine
Rootstown, OHChief, Infectious Disease Service and Director, HIV Research
Summa Health SystemAkron, OH

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.29
The Impact of CAP in the United States
• Leading cause of morbidity and mortality1‐4
– ≈50,000 deaths/y, especially elderly and patients with comorbidities1,5
– #1 cause of mortality due to infection in US6
• Annual incidence7
– General population: 1‐12 cases/1,000
– ≥65 y/o: 25‐44 cases/1,000
• Annual prevalence: >4 million cases3
– ≈1.1 million admissions/y, 40% 1‐y mortality4,5
– ≈80% treated as outpatients8
• Annual cost of treatment >$17 billion3
73
1. File TM Jr. Lancet. 2003;362(9400):1991‐2001. 2. File TM Jr et al. JAMA. 2005;294(21):2760‐2763. 3. File TM Jr et al. Postgrad Med. 2010;122(2):130‐141. 4. Kaplan V et al. Arch Intern Med. 2003;163(3):317‐323. 5. CDC/National Center for Health Statistics. April 5, 2013. http://www.cdc.gov/nchs/fastats/pneumonia.htm. 6. Klevens RM et al. Public Health Rep. 2007 ;122(2):160‐166. 7. Ochoa‐Gondar O et al. BMC Public Health. 2008;8:222. 8. Gaydos CA. Infect Dis Clin North Am. 2013;27(1):46‐69.
ARS
CAP
HCAP
HAP/VAP
1. Yap V et al. Infect Dis Clin North Am. 2013;27(2):1‐18. 2.Craven DE. Curr Opin Infect Dis. 2006;19(2):153‐160.
Are Present CAP and HCAP Definitions the Best Way to Define Risk of MDR Infection?1
75

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.30
2005 Guidelines for Nosocomial Pneumonia: HCAP Etiology
• Risk factors for MDR pathogens causing HCAP1
– Hospitalized ≥2 d in preceding 90 d
– Nursing home/extended care facility residence
– Home infusion therapy (including antibiotics)
– Chronic dialysis within 30 d
– Home wound care
– Family member with MDR pathogen
• Treat for MDR pathogens1
– But this is an overgeneralization; updated guidelines are under development
• Designation of HCAP—poor predictor of resistant pathogens2
• Current definition needs further modification so adequate coverage can consistently be provided while avoiding excessive antibiotic use2
761. ATS/IDSA. Am J Respir Crit Care Med. 2005;171:388‐416. 2. Yap V et al. Infect Dis Clin North Am. 2013;27(2):1‐18.
Which Scoring Tool Best Predicts Clinical Response, Long‐term Outcomes?
• PSI• CURB‐65• CRB‐65• SMART COP• SCAP
“In regards to the best scoring tool to predict clinical response and long term outcomes, Pneumonia Severity Index (PSI) is probably a more accurate score to predict a wide range of clinical outcomes.”
77
PSI, Pneumonia Severity Index; CURB‐65, Confusion, elevation of blood Urea nitrogen, Respiratory rate, low Blood pressure, age ≥65 y; CRB‐65, Confusion, Respiratory rate, low Blood pressure, age ≥65 y; SMART COP, low Systolic blood pressure, Multilobar chest X‐ray involvement, low Albumin, high Respiratory rate, Tachycardia, Confusion, poor Oxygenation, low arterial pH; SCAP, Severe Community‐Acquired Pneumonia
Wiemken T. Infect Dis Clin North Am. 2013;27(1):33‐48.
ARS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.31
Guidelines and Quality Measures: Do They Improve Outcomes of Patients with CAP?1
• “…body of evidence supporting the positive effects of guidelines on outcomes in patients with CAP is extraordinary”1
– Recent meta‐analysis concluded guideline compliance more important than choice of antimicrobials2
• “…no evidence that…pay‐for‐performance program led to a decrease in 30‐d mortality”3
– 30‐d mortality (2003–2009)3
– Pay‐for‐performance hospitals: 11.71%• Non‐pay‐for‐performance hospitals: 11.85% (95% CI, –0.67‐0.38)
791. Johnstone J et al. Infect Dis Clin North Am. 2013;27(1):71‐86. 2. Asadi L et al. Clin Infect Dis. 2012;55(3):371‐380. 3. Jha A et al. N Engl J Med. 2012;366(17):1606‐1615.
CMS 2014 CAP Quality Measures for Inpatients
• Empiric antimicrobials according to guidelines― Exceptions: pathogen-directed therapy,
clinical trials, diagnostic uncertainty
• CAP mortality
• 30-d readmission rate for pneumonia*
*Complements Core Measures as part of the Hospital Readmissions Reduction Program—hospitals with higherthan expected 30-d readmission rates for AMI, heart failure, and pneumonia will incur penalties against their total Medicare payments beginning in FFY 2013.
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html File TM Jr, personal communication, Sept. 2013. CMS community-acquired pneumonia Technical Expert Panel, 9/19/13. 80

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.32
CABP: JC/CMS Antimicrobial Recommendations by Site of Care1,2
Inpatient, Non‐ICU Inpatient, ICU
β‐lactam (IV or IM) + macrolide (IV or po) –OR–
Macrolide (IV) + β‐lactam (IV) –OR–antipneumococcal + antipseudomonal β‐lactam (IV) –OR–
Anti‐pneumococcal quinolone monotherapy (IV or po) –OR–
Antipneumococcal quinolone (IV) –OR–antipseudomonal quinolone (IV) + either β‐lactam (IV) –OR–antipneumococcal/antipseudomonal β‐lactam (IV)–OR–
β‐lactam (IV or IM) + doxycycline (IV or po) –OR–Tigecycline monotherapy (IV) –OR–Macrolide monotherapy (IV or po)a
Antipneumococcal/antipseudomonal β‐lactam (IV)+ aminoglycoside (IV) + either antipneumococcal quinolone (IV) –OR–macrolide (IV)
81
aIf aged <65 y with no risk factors for drug‐resistant Pneumococcus.
1. JC, CMS. http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Good through 12/31/2013. 2. File TM Jr et al. Clin Infect Dis. 2011;53(suppl 1):S15‐S22, by permission of Oxford University Press.
CABP: New Antimicrobials
• Tigecycline IV– Glycylcycline (derivative of minocycline): broad spectrum including
S pneumoniae, atypicals1
– Approved for ABSSSI, CABP, intra‐abdominal infections2
• CABP: comparable to levofloxacin1
• HAP/VAP: comparable to imipenem for HAP; inferior for VAP3,4
– Listed as option for CABP admitted to general ward • 100 mg initially, then 50 mg Q 12h2
• Adverse effects: nausea, vomiting2
• Ceftaroline IV– Prodrug, broad‐spectrum cephalosporin5
– Bactericidal in CABP infections vs S pneumoniae, S aureus (MSSA), H influenzae, K pneumoniae, K oxytoca, E coli6
– Approved for CABP, ABSSSI; 600 mg q 12 h6
82
1. Tanaseanu C et al. Diag Microbiol Infect Dis. 2008;61:329‐38. 2. Tygacil [package insert]. Philadelphia, PA: Wyeth Pharmaceuticals, Inc; 2012. 3. Freire AT et al. Diagn Microbiol Infect Dis. 2010;68:140‐151. 4. Ramirez J et al. Antimicrobial Agents Chemother. 2013;57:1756‐1762. 5. File TM Jr et al. Clin Infect Dis. 2010;51(12):1395‐1405. 6. Teflaro [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2013.
MSSA, methicillin‐susceptible S aureus
ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.33
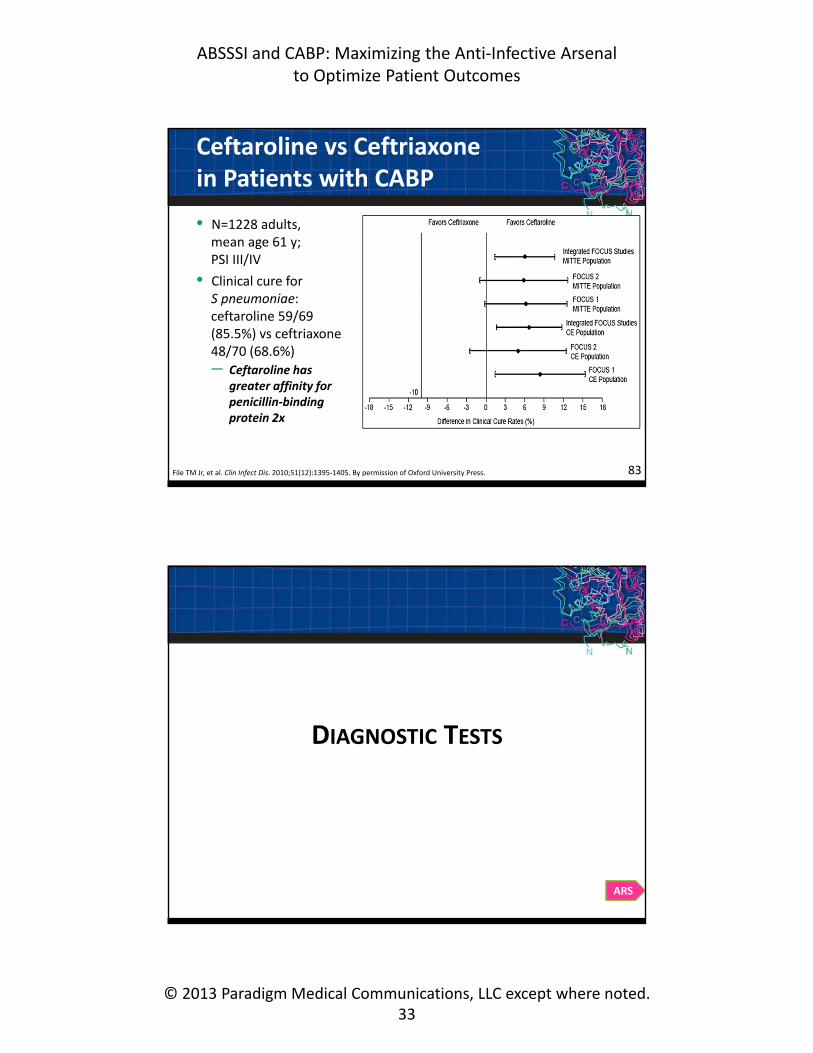
Ceftaroline vs Ceftriaxone in Patients with CABP
• N=1228 adults, mean age 61 y; PSI III/IV
• Clinical cure for S pneumoniae: ceftaroline 59/69 (85.5%) vs ceftriaxone 48/70 (68.6%)
– Ceftaroline has greater affinity for penicillin‐binding protein 2x
83File TM Jr, et al. Clin Infect Dis. 2010;51(12):1395‐1405. By permission of Oxford University Press.
DIAGNOSTIC TESTS
ARS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.34
What is the Benefit of CAPBiomarkers in Patient Management?
861. Upadhyay S, et al. Infect Dis Clin North Am. 2013;27(1):19‐31. 2. Christ‐Crain M et al. Am J Respir Crit Care Med. 2006;174:84‐93. 3. Schuetz P et al. JAMA. 2009;302:1059‐1066. 4. Bouadma L et al. Lancet. 2010;375:463‐474.
Biomarker procalcitonin (PCT) guides reduction in hospital antibiotic treatment of CAP without increasing mortality risk1
Trials of PCT to Guide Therapy Duration in CAP Hospital Patients1
Study LocationDuration PCT, d
Duration Control, d
Mortality PCT
Mortality Control
Christ‐Crain M et al2 1 ED 5 (median) 12 (median) 10% 10%
Schuetz P et al3 6 EDs 7 (median) 10 (median) 5.2% 5.6%
Bouadma L et al4 7 ICUs 5.5 (mean) 10.5 (mean) 16.9% 19%
PCT for Antimicrobial Stewardship When Treating RTIs
PCT value <.01 µg/L <.025 µg/L ≥0.25 µg/L >0.5 µg/L
Bacterial infection?
Very unlikely Unlikely Likely Very likely
Antibiotic recommendation
Strongly discouraged
Discouraged EncouragedStrongly
encouraged
F/UReassess and recheck PCT after 6‐24h if no clinical improvement
Recheck PCT every 2‐3 d to consider early stop antibiotic therapy
When to overrule
Consider antibiotic if patient is clinically unstable or at high risk for adverse outcomes (PSI IV‐V) or has strong evidence for bacterial pathogen
87RTI, respiratory tract infectionSchuetz P et al. Curr Opin Infect Dis. 2013;26:159‐167.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.35
Role of Newer Molecular Tests in CAP Management1
• Standard culture methods (blood, sputum)
– Low yield, time to results2
• Gram stain, urinary antigen testing
– S pneumoniae, Legionella spp3
• Newer molecular tests (PCR, MALDI‐TOF)4‐6
– Potential for more rapid diagnosis, greater sensitivity
– Allows for pathogen‐directed therapy
88
1. Gaydos CA. Infect Dis Clin North Am. 2013;27(1):49‐69. 2. Bartlett JG. Clin Infect Dis. 2011;52(suppl 4):S296‐S304. 3. Falguera M et al. Thorax. 2010;65:101‐106. 4. Christ‐Crain M et al. Crit Care. 2010;14:203. 5. Schuetz P et al. Curr Opin Infect Dis. 2013;26:159‐167. 6. Xiao D et al. Diagn Microbiol Infect Dis. 2012;73(4):301‐307.
PCR, polymerase chain reaction; MALDI‐TOF, matrix‐assisted laser desorption/ionization Time of Flight mass spectrometry
Enriched PCR Detection of CAP Pathogens
89
Among the 38 patients who had complete sampling (conventional + molecular assays), a microbial etiology was determined for 89%
Reprinted from Johansson N et al. Etiology of community‐acquired pneumonia: increased microbiological yield with new diagnostic measures. Clin Infect Dis. 2010;50(2):202‐209 by permission of Oxford University Press.
ARS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.36
Empiric Therapy for Atypical Pathogens: Does it Improve CAP Outcomes?
Issues of controversy regarding significance of atypical pathogens
• Clinical relevance of terminology
• Awareness of such pathogens
• Diagnostic testing
• Debate as to the clinical impact of treating these infections
• Perceived contradictory results of published evidence
91File TM Jr et al. Infect Dis Clin North Am. 2013;27(1):99‐114.
Empiric Therapy for Atypical Pathogens: Early Outcome Assessment
76.6
89.1
57.6
87.9
40
50
60
70
80
90
100
Day 4 Clinical Stabilityand Symptom Improvement
Test of Cure
Response, %
FOCUS 1 (macrolide) FOCUS 2 (no macrolide)
92
“Thus, empiric therapy for atypical pathogens does improve outcomes for patients with CAP.”2
1. File TM Jr et al. Presented at ECCMID, London: 3/3/12‐4/3/12. 2. File TM Jr et al. Infect Dis Clin North Am. 2013;27(1):99‐114.
Early outcome assessment may identify benefit of macrolides

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.37
Fluoroquinolone or ß‐Lactam + Macrolide
Which has better outcomes in non‐ICU CAP?1
• Reviewed evidence– Multiple studies; but different designs– Considered “collateral damage”– Immunomodulatory effects of macrolides– Fluoroquinolone PK and resistance
• Conclusion– Neither of the two first‐line regimens has been proved to have clear‐cut
clinical superiority
• “Therapeutic decision making should be individualized, taking into account additional patient information such as the presence of drug allergies, local resistance patterns, patient comorbidities, and risk factors for the presence of resistant S pneumoniae”
93Ruhe J et al. Infect Dis Clin North Am. 2013;27(1):115‐132.
How Important is MRSA as a Cause of CAP?1
“MRSA clearly is an important pathogen in CAP. While currently causing a relatively low percentage of CAP cases, the disproportionate frequency of otherwise healthy young people with this infection drives concern and therefore empiric antibiotic therapy.”1
• EMERGEncy ID Net study (2006‐2007)2
– N=595 CAP patients, pathogen identified in 17%
– S pneumoniae: 9.6%; MRSA, 2.4%; MSSA: 1.5%;K pneumoniae: 0.7%; H influenzae: 0.3%
• Clinical features suggesting increased risk of CA‐MRSA pneumonia1
– Cavitary pneumonia ‒ Lung necrosis
– Neutropenia ‒ Hemoptysis
941. Wunderink RG. Infect Dis Clin North Am. 2013;27(1):177‐188. 2. Moran G et al. Clin Infect Dis. 2012;54:1126‐1133.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.38
MRSA CAP: What is the Best Antimicrobial Therapy?
• Antimicrobials for MRSA pneumonia1
– Appropriate: vancomycin, linezolid
– Under study: ceftaroline
– Unclear: clindamycin, trimethoprim/sulfa
• “Linezolid consistently demonstrates better clinical response rates than vancomycin in clinical trials of MRSA pneumonia.
Linezolid also suppresses exotoxin production in in vitromodels, which may be important in CA‐MRSA CAP”1
– Zephyr study (HAP/VAP)2
• Clinical response: linezolid, 57.6%; vancomycin, 46.6%; P <.05
• No difference in mortality
951. Wunderink RG. Infect Dis Clin North Am. 2013;27(1):177‐188. 2. Wunderink RG et al. Clin Infect Dis. 2012;54(5):621‐629.
Do Adjunctive Therapies Improve Patient Outcomes in Severe CAP?
• Corticosteroids
• Statins
• Angiotensin‐converting enzyme inhibitors
• Anticoagulant agents– Human activated protein C
– Tissue factor pathway inhibitor
• Surfactant
• Immunoglobulin
• Interferon γ
Sibila O et al. Infect Dis Clin North Am. 2013;27(1):133‐147.
“Adjunctive therapies directed at the host response rather than the pathogens are attractive to improve outcomes.
Corticosteroids, statins, ACE inhibitors, and anticoagulants have been used with some encouraging results, although data are still scarce.
Future research is needed in these areas to decrease mortality due to severe CAP.”
96

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.39
Conclusions
• CAP is very common and serious
• Despite many advances, controversies and questions remain
• New guidelines are under development
97
Recent journal devoted to current issues in the management of inpatient CAP
File TM Jr. Infect Dis Clin North Am. 2013;27(2):253‐500.
98

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.40
ANTIMICROBIAL STEWARDSHIP THAT ENSURES OPTIMAL OUTCOMES
Michael J. Rybak, PharmD, MPH, FCCP, FIDSAProfessor of Pharmacy and Medicine
Director, Anti‐Infective Research LaboratoryDepartment of Pharmacy Practice
Eugene Applebaum College of PharmacyWayne State University, Detroit, MI
Drug Resistance is Rising
With permission from Wenzel RP et al. Infect Control Hosp Epidemiol. 2008;29(11):1012‐1018. © 2008 by The Society for Healthcare Epidemiology of America. Published by the University of Chicago Press. 101

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.41
CDC. 2013. Available at: www.cdc.gov/drugresistance/threat‐report‐2013/pdf/ar‐threats‐2013‐508.pdf#page=13.
Antibiotic Stewardshipin Your Facility Will…
DECREASE•Antibiotic resistance
•C difficileinfections
•Costs
INCREASE
• Good patient outcomes
102
CLINICAL AND ECONOMIC
COSTS OF RESISTANCE

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.42
The Burden of Antimicrobial Resistance
Outcomesa MSSAb
(n=390)MRSAb
(n=335)
6-mo mortalityc 11.5% 23.6%
Hospital chargesd
6-mo median (range)$6,748
($0–$35,089)$26,274
($4,531–$86,974)
104
Greater impact of MRSA on clinical and economic outcomes
Filice GA et al. Infect Control Hosp Epidemiol. 2010;31:365‐373.
aBased on medical records, accounting systems, and interviews between January 1, 2004 and June 30, 2006bPatients with S aureus infection within the Minneapolis Veterans Affairs hospital and associated clinicscWithin 6 mo of onsetdMedian 6‐mo inpatient unadjusted costs in 2006 US dollars
Attributable Costs of Resistance*
Outcomes Patients with ARI (n=188)
Length of stay (LOS) 6.4 ± 12.7 d
Deatha 6.5%
Medical costs (mean ± SE)b,c $18,588–$29,069
Total hospital costsb,d $3.4–$5.4 million
Total societal costsb,e $10.7–$15.0 million
105Roberts RR et al. Clin Infect Dis. 2009;49:1175‐1184.
ARI, antibiotic‐resistant infection*Additional clinical or economic costs of ARI relative to the costs without ARI, based on analysis of medical records for a sample of 1,391 high‐risk adult patients at an urban teaching hospital in 2000 (without ARI, n=1203)aAdjusted attributable mortality. Absolute mortality 18.1% with ARI vs 3.0% without ARI; adjusted OR = 2.16bEconomic costs were reported in 2008 US dollarscVariable costs for a base case patient, including medications and blood productsdIncluding labor, benefits, supplies, equipment used, and allocated administrative and support costs for employees and space occupiedeCosts of mortality, lost productivity

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.43
Cost Savings if Antimicrobial Resistance Reduced
106Roberts RR et al. Clin Infect Dis. 2009;49:1175‐1184. By permission of the Oxford University Press.
ANTIMICROBIAL
STEWARDSHIP PROGRAMS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.44
Issues Related to ASP Implementation
• Restrictions common in academic centers, not community hospitals1,2
• Lack of strong scientific evidence to support improved outcomes1,3
• Lack of a full‐time ID consult service2
– Role of pharmacist, physician, ID fellow unclear and varies1
• Limited use of local guidelines1
• Limited use of CPOE and CDSS1
• Program funding inconsistent1
• Administrative support and data analysis inconsistent1
108
CPOE, computerized provider order entry; CDSS, clinical decision support system
1. Barlam TF et al. Infect Control Hosp Epidemiol. 2006;27:695‐703. 2. Weston A et al. Presented at IDWeek 2012. October 19, 2012; San Diego, CA. Poster 717. Available at: https://idsa.confex.com/idsa/2012/webprogram/Paper34170.html. 3. Chung GW et al.Virulence. 2013;4(2):151‐157.
Antibiotic Use Evaluation = Antimicrobial Stewardship
109
Assess patient Make diagnosis Select treatment plan
• Are antibiotics needed?• What are my options?• Formulary restrictions?• Will it work?
Implement plan Reassess patient Modify plan
• Risk stratification (severity, risk factors for MDROs)• Guidelines (local or national)• Spectrum of activity and local antibiogram• Nonscientific inputs: peer opinion, marketing
• Are antibiotics still needed?• Can I streamline therapy?• Specific microbiology• Convenience and cost
1. MacDougal C et al. Clin Microbiol Rev. 2005;18(4):638‐656. 2. File TM Jr et al. Clin Infect Dis. 2011;53(suppl 1)S15‐S22.
MDROs, multi‐drug resistant organisms

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.45
Stewardship Strategies: Therapeutic Guidelines and Pathways
• Disease‐based treatment guidelines to target– Selection: initial empiric therapy and alternatives
– Dosing: pharmacodynamic optimization
– Route: IV/PO conversions
– Duration of therapy, facilitate discharge from hospital
• Must have multidisciplinary involvement and input from all stakeholders (eg, surgery, pulmonary, nurse managers)
• Should account for local resistance patterns
110Dellit TH et al. Clin Infect Dis. 2007;44(2):159‐177.
Prospective audit with intervention and feedback
Formulary restriction and pre‐
authorization requirements
“Back-End Approach”
“Front-End Approach”
Advantages1,2
- Can be customized to facility- Preserves prescriber autonomy- Circumvents potential for delays in
initiating therapy- Provides educational opportunities
Disadvantages1,2
- Labor intensive- Recommendations optional- Potential for inappropriate exposure
Advantages1,3
- Initial orders funneled through experts- Can be facilitated through computer
surveillance- Immediate educational opportunities- Control of antimicrobial use
Disadvantages1,3
- Delays therapy for critically ill patients- Requires trained personnel- Loss of prescriber autonomy- Potential for prescriber to circumvent- Potential for inappropriate exposure
1. Dellit TH et al. Clin Infect Dis. 2007;44(2):159‐177. 2. Chung GW et al. Virulence. 2013;4(2):151‐157. 3. Reed EE et al. Virulence. 2013;4(2):158‐162. 111

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.46
Prospective audit with intervention and feedback
Formulary restriction and pre‐
authorization requirements
“Back-End Approach”
“Front-End Approach”
•Most frequently employed intervention
•Essential element of any ASP Education
•ASP should facilitate development of evidenced‐based guidelines
•Must be tailored to local practice and epidemiologyGuidelines
•Opportunity for screening information as it becomes available
•Can develop alerts, reports, and decision support pathways
Computer Surveillance
OutcomesMeasurement
•Determines the impact of new policies
•Opportunities for research and publication
Dellit TH et al. Clin Infect Dis. 2007;44(2):159‐177. 112
ARS
ASP Improves Clinical Outcomes
1141. Fishman N. Am J Med. 2006;119(suppl 1):S53‐S61. 2. Ohl CA et al. Clin Infect Dis.2011;53(1):S23‐S28. By permission of the Oxford University Press.
University of Pennsylvania Hospital observational study, clinical outcomes with a comprehensive stewardship program compared with usual practice.1,2
90 91
51
32
55
31
9
0
20
40
60
80
100
AppropriateAntimicrobial
ClinicalCure
TreatmentFailure
AntibioticResistance
Patients, %
ASP Usual practice

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.47
ANTIMICROBIAL STEWARDSHIP
INTERVENTION: OUTCOMES WITH ABSSSI
Epidemiology of Skin and Soft Tissue Infections (SSTIs)
63% 8%
7%
15%
5%
2%
SSTI Hospitaliza on by Type of Infec on (2009‐2011; N=471,550)
Cellulits and abscess
Impe go
Other infec ons of the skin
Folliculi s
Carbuncle and furuncle
Other SSTI
Other infections of the skin: folliculitis.
Other SSTI: erysipelas, mastitis, acute lymphadenitis, hydradenitis, and necrotizing fasciitis.
Ray GT et al. BMC Infect Dis. 2013;13:252. 116
ARS

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.48
Antibiotic Resistance and Treatment Outcomes
118
46
CA‐MRSA leads to significantly greater rates of hospitalization, failure of initial therapy, and infection recurrence in patients with cSSSI vs those with CA‐MSSA (2003‒2005)
P <.001
P <.001
P <.015
Davis SL et al. J Clin Microbiol. 2007;45(6):1705‐1711.
46
39
181816
6
0
10
20
30
40
50
Hospitalized Failed Therapy Recurrent Infection
Patients, %
CA‐MRSA (n=102)
CA‐MSSA (n=102)
Antibiotic Use in ABSSSI
0
10
20
30
40
50
60
2000(N=647)
2001(N=1597)
2002(N=1644)
2003(N=1849)
2004(N=1625)
2005(N=2349)
2006(N=3082)
2007(N=3934)
2008(N=4255)
2009(N=1400)
Adult cSSSI Admissions, %
Vancomycin Piperacillin‐tazobactam Clindamycin
Pip‐tazo + vancomycin Cefazolin Ampicillin‐sulbactam
Parenteral antibiotic use in >10% (by 2009) of adult cases within first 24 h of admission to ≈100 US hospitals, based on chart review of 22,382 admissions for cSSSI between 1/1/00 and 6/30/09.
Vancomycin used as initial therapy in 58% of cSSSI cases in 2009
Berger A et al. Infect Dis Clin Pract. 2013;21(3):159‐167.
[p159, 160 Table 2, p161 Table 3]
119

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.49
OPPORTUNITIES FOR ANTIMICROBIAL
STEWARDSHIP PROGRAMS
Opportunity for ASPsSSTIs Requiring Hospitalization
Study Parameters
• Retrospective chart review of adults discharged with diagnosis of SSTI from 1/107 to 12/31/07
– 477‐bed academic hospital in Denver
– SSTI classified as cellulitis, cutaneous abscess, or SSTI with additional complicating factors
• Results (N=322)
– 66 (20%): cellulitis
– 103 (32%): abscess (incision and drainage in 98%)
– 153 (48%): complicating factors
• Common comorbidities in each group: IV drug use, diabetes mellitus, alcohol abuse
121Jenkins TC et al. Clin Infect Dis. 2010;51(8):895‐903.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.50
SSTIs Requiring Hospitalization (continued)
Study Findings• 150 pts had positive cultures from abscess, deep tissue, or blood
– S aureus or streptococci identified in 145 (97%)
• Duration of antibiotic therapy, (median, d)– Cellulitis: 13 (IQR, 10–14 d)– Cutaneous abscess: 13 (IQR, 10–16 d)– SSTI with complications: 14 (IQR, 11–17 d)
• 30‐d treatment failure, recurrence, readmission– Cellulitis: 12.1%– Cutaneous abscess: 4.9%– SSTI with complications: 9.2%
122IQR, interquartile range
Jenkins TC et al. Clin Infect Dis. 2010;51(8):895‐903.
Parenteral AntibioticPatients (N=322)
Vancomycin 73%–79%
Gram positive activity, without MRSA coverage
≤20%
Broad aerobic gram‐negative activity 61%–80%
Anaerobic coverage 73%–83%
SSTIs Requiring Hospitalization: Excess Resource Utilization
• ESR or CRP determined in nearly 70% of patients
• Blood cultures for 47%–58% of patients
• Imaging studies in 94% of patients– SSTI with complicating factors: 86%
– Significant association between cellulitis and use of plain film
(P <.004) and ultrasound (P <.001)
– Advanced imaging (CT, MRI) in 20% of all cases
• Yield of imaging studies: 14 (4%) of 322 cases– Plain film: 4 (1%) – Ultrasound: 1 (0.3%)– CT: 7 (2%)– MRI: 3 (1%)
123
ESR, erythrocyte sedimentation rate; CRP, C‐reactive protein
Jenkins TC et al. Clin Infect Dis. 2010;51(8):895‐903.

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.51
SSTIs Requiring Hospitalization:Study Conclusions
• Additional therapy results– 85% of cellulitis inpatients received MRSA coverage
• ≈50% of 66 cases discharged on TMP/SMX
• Highest rate of failure, 12.1% (8/66)
• 5/8 (63%) cases of cellulitis failure discharged on TMP/SMX
• Conclusions– Substantial healthcare resources used to treat SSTI
– Some diagnostic testing poorly defined, expensive, unnecessary
– Many patients received inappropriate broad antibiotic coverage, including gram‐negative and anaerobic coverage
– Duration of hospitalization for treatment appeared excessive, and many patients could have received part of therapy at home
124Jenkins TC et al. Clin Infect Dis. 2010;51(8):895‐903.
ARS
Impact of ASP on Inpatient Treatment of ABSSSI
• Objective
Observe impact of ASP on ABSSSI treatment and outcomes since ASP implemented 2/2012– Appropriateness of antibiotic therapy
– LOS
– 30‐d readmission rate
• Historic controlTreatment outcomes of ABSSSI (ICD9 codes 681‐682.9) at Summa Health System in 2011– Mean LOS: 6.2 d
– 30‐d readmission rate: 6.2%
126Pasquale TR et al. Presented at: IDWeek 2012. October 19, 2012; San Diego, CA. Poster 744. Available at: https://idsa.confex.com/idsa/2012/webprogram/Session4786.html.
76%
26%
8%3% 2%
ABSSSI Subtypes (N=62)
Cellulitis Major or deep abscess Surgical site infection Diabetic wound Decubitus ulcer

ABSSSI and CABP: Maximizing the Anti‐Infective Arsenal to Optimize Patient Outcomes
© 2013 Paradigm Medical Communications, LLC except where noted.52
Impact of ASP on Inpatient Treatment of ABSSSI (continued)
24%
37%44%
7% 11%
ASP Intervention Types (N=85)
Antibiotic regimen change De‐escalation Dose change ID consult Other
Outcomes2012(N=62)
2011 (N=1149)
LOS, mean (d) 4.4 6.2
30‐d All‐Cause Readmission
6.5% 16.71%
30‐d ABSSSI Readmission
3.33% 6.27%
127Pasquale TR et al. Presented at: IDWeek 2012. October 19, 2012; San Diego, CA. Poster 744. Available at: https://idsa.confex.com/idsa/2012/webprogram/Session4786.html.
Summary: Antimicrobial Stewardship Programs
• Driven by increasing antibiotic resistance
– Limited pipeline
• Needs leaders and training programs
• Requires administration support
• Some components may be forced based on:
– Future Joint Commission and CMS requirements
• Requires evaluation of ASP impact
– To improve and develop effective policies
– Maintain services and resources
128
Related Documents











