A REPORT ON THE ABORIGINAL POPULATION OF MURRUMBIDGEE LOCAL HEALTH DISTRICT Date: August 2012 Author: Kim Gilchrist, Epidemiologist, Public Health Unit, MLHD [email protected] Input from: Diann Tremain, Manager Aboriginal Health Murrumbidgee Local Health District ABN 71 172 428 618 Locked Bag 10, Wagga Wagga NSW 2650 Tel 02 6933 9100 Fax 02 6933 9188 Website www.health.nsw.gov.au/mlhn/

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A REPORT ON THE ABORIGINAL POPULATION OF
MURRUMBIDGEE LOCAL HEALTH DISTRICT
Date: August 2012
Author: Kim Gilchrist, Epidemiologist, Public Health Unit, MLHD
Input from: Diann Tremain, Manager Aboriginal Health
Sabrina Brown, Coordinator Aboriginal Maternal and Infant Health Service
Copies available: www.gsahs.nsw.gov.au/gsho/refreplink.html
Murrumbidgee Local Health DistrictABN 71 172 428 618
Locked Bag 10, Wagga Wagga NSW 2650Tel 02 6933 9100 Fax 02 6933 9188
Website www.health.nsw.gov.au/mlhn/
CONTENTS
About this Report.........................................................................................................................................................................2
The Population..............................................................................................................................................................................2
Socioeconomic status...............................................................................................................................................................5
Deaths.......................................................................................................................................................................................... 5
Hospitalisations............................................................................................................................................................................6
Potentially Preventable Hospitalisations (PPH).........................................................................................................................9
Health Conditions and Risks........................................................................................................................................................10
Maternal and Child health..........................................................................................................................................................12
Current Staffing in MLHD............................................................................................................................................................14
In Summary.................................................................................................................................................................................15
More Information.......................................................................................................................................................................16
1 | P a g e
Public Health Unit – MLHD (document.docx)

ABOUT THIS REPORT
Data relating to Aboriginal health at LHD level is limited but improving. Small numbers make it difficult to report data for specific conditions and deaths; in addition to this the identification of Aboriginality in some databases is unreliable. This report summarises information available from the NSW Ministry of Health web-site Health Statistics NSW. Where possible, figures for MLHD have been included; however for some health indicators only State level data is available.
Files containing the full data tables and charts are available electronically from www.gsahs.nsw.gov.au/gsho/refreplink.html.
THE POPULATION
Figure 1 - Aboriginal population percentage of total population by LGA and population density by Statistical Area 1*, MLHD, 2011 Census.Note: *Statistical Area 1 (SA1) is a new geographic boundary for the 2011 ABS Census, there may be several SA1’s per LGA.
There were an estimated 10,546 Aboriginal people living in MLHD (including Albury LGA and Lake Cargelligo area) in August 2011 (ABS 2011 Census). In NSW, Aboriginal people made up 2.5 per cent of the total population and in MLHD the percentage of Aboriginal people was 3.8 per cent (Table 1). The shaded areas of the map above () show the distribution of Aboriginal people in MLHD as a percentage of the total population by LGA. The LGAs with the highest proportions of Aboriginal people in MLHD are Lake Cargelligo - part of Lachlan Shire – (14% 247 people), Murrumbidgee Shire (10%, 229 people) and Narrandera Shire (10%, 592). The actual numbers of Aboriginal people are demonstrated by “dot density” on Figure 1 , where one dot represents 20 Aboriginal people with the largest numbers of Aboriginal people in Wagga Wagga (2,732, 4.6%), Albury (1,108, 2.3%) and Griffith (1,003, 4.1%).
2 | P a g e
Public Health Unit – MLHD (document.docx)
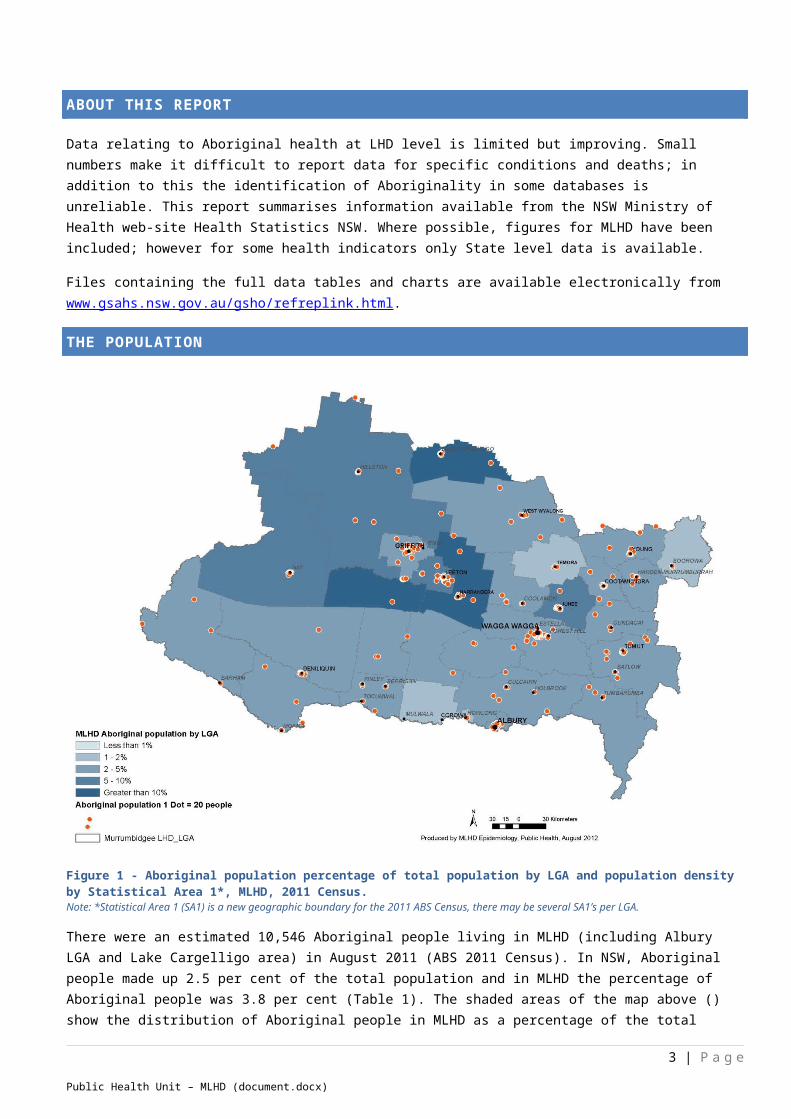
Table 1 – Aboriginal people by Local Government Area, 2011 Census, MLHD
Local Government Area Aboriginal Males
Aboriginal Females
Aboriginal Persons
Total LGA population
Per cent of LGA population Aboriginal
Albury (C) 545 563 1108 47810 2.3%Berrigan (A) 82 84 166 8066 2.1%Bland (A) 120 118 238 5865 4.1%Boorowa (A) 20 25 45 2399 1.9%Carrathool (A) 75 102 177 2587 6.8%Conargo (A) 16 15 31 1540 2.0%Coolamon (A) 47 59 106 4099 2.6%Cootamundra (A) 132 149 281 7334 3.8%Corowa Shire (A) 71 72 143 11000 1.3%Deniliquin (A) 143 115 258 7120 3.6%Greater Hume Shire (A) 91 110 201 9815 2.0%Griffith (C) 498 505 1003 24364 4.1%Gundagai (A) 44 46 90 3662 2.5%Harden (A) 81 80 161 3584 4.5%Hay (A) 93 75 168 2956 5.7%Jerilderie (A) 23 23 46 1496 3.1%Junee (A) 279 112 391 5878 6.7%Leeton (A) 297 356 653 11037 5.9%Lockhart (A) 51 27 78 2998 2.6%Murray (A) 109 121 230 6957 3.3%Murrumbidgee (A) 123 106 229 2261 10.1%Narrandera (A) 290 302 592 5902 10.0%Temora (A) 56 47 103 5776 1.8%Tumbarumba (A) 56 28 84 3358 2.5%Tumut Shire (A) 208 284 492 10934 4.5%Urana (A) 22 16 38 1159 3.3%Wagga Wagga (C) 1333 1399 2732 59458 4.6%Wakool (A) 47 47 94 3962 2.4%Young (A) 175 202 377 12236 3.1%Lake Cargelligo part of Lachlan 119 128 247 1764 14.0%ALL MLHD 5246 5316 10562 277377 3.8%All NSW 85083 87542 172625 6917656 2.5%
Life expectancy for Aboriginal people in NSW born between 2005-2007 was estimated to be 67.2 years for Aboriginal males and 75.0 years for Aboriginal females, this is from 7 to 9 years fewer than the general population. The Aboriginal population is younger, with around 34.7% of the population under 15 years of age, compared with around 19.6% of the non-Aboriginal population in MLHD (Figure 2). The proportion of the Aboriginal population in each 5-year age group decreases with increasing age, whereas in the non-Aboriginal population, there is no decrease until after the age of 49 years. The proportion of the Aboriginal population over the age of 65 years is just 4.5% compared with 17.5% in the non-Aboriginal population. There is also a substantial drop in the size of the Aboriginal population between 10-14 years and 15-19 years, reflecting a relatively high mortality rate among older teenagers as well as migration out of the area for 20-29 year olds. From 1991 to 2011 the proportion of Aboriginal people aged 75 years or over has increased slightly from 1.1 per cent to 1.3 per cent. The proportion of the Aboriginal population aged 0-4 years has decreased from 17.1 per cent to 10 per cent.
3 | P a g e
Public Health Unit – MLHD (document.docx)

Figure 2
SIGNIFICANCE:
Proportion of population identifying as Aboriginal in MLHD is higher than the State therefore Aboriginal health issues are even more critical in MLHD.
The Aboriginal population is not evenly spread across all LGAs so areas such as Narrandera and Murrumbidgee Shire need pay particular attention to cultural issues as well as LGAs such as Wagga Wagga, Albury and Griffith where there are higher numbers of Aboriginal people residing.
Life expectancy is much shorter for Aboriginal people as far fewer Aboriginal MLHD residents are living beyond the age of 49 years.
4 | P a g e
Public Health Unit – MLHD (document.docx)

SOCIOECONOMIC STATUS
Figure 3
The relative socioeconomic disadvantage experienced by Aboriginal people in NSW continues to place them at a greater risk of exposure to behavioural and environmental health risk factors. A range of socioeconomic indicators from the 2006 Census demonstrate the relative disadvantage of the Aboriginal population in NSW (Figure 3). In NSW, larger proportions of Aboriginal people are: unemployed; have no post-school qualifications; no household internet connection; a weekly household income less than $500; rent, live in multi-family households; and reside in dwellings with 7 or more people than non-Aboriginal people (Health Statistics NSW).
DEATHS
In NSW the leading causes of death were the same for Aboriginal and non-Aboriginal people in 2003-2007. Cardiovascular diseases were the main cause of death for all people in NSW; accounting for 30.8 per cent of all deaths among Aboriginal people compared to 36.5 per cent of deaths in non-Aboriginal people. Malignant neoplasms (cancers) were the cause of 21.1 per cent of all deaths among Aboriginal people and 28.8 per cent of deaths among non-Aboriginal people. The third most common cause of death for Aboriginal people was injury and poisoning (11.7%) followed by respiratory diseases (8.4%) compared to non-Aboriginal people where respiratory disease made up 8.7 per cent of causes of death and injury and poisoning 5.2 per cent. Among Aboriginal people in NSW, 63.6 per cent of potentially avoidable deaths (death occurring before 75 years of age thought to be able to avoided through prevention or treatment) were classed as preventable compared to 58.8 per cent in the non-Aboriginal population. Data for the MLHD is not reported separately as it varies widely from year to year due to the small number of actual events, making data by Aboriginality unreliable.
5 | P a g e
Public Health Unit – MLHD (document.docx)

SIGNIFICANCE:
Aboriginal people are dying from similar causes as non-Aboriginal people; however they die at a much younger age. Aboriginal people are more likely to die from causes considered to be preventable, than non-Aboriginal people.
HOSPITALISATIONS
In NSW, hospitalisation for the general population occurred at an annual rate (2010-11) of around 35,400 episodes of care per 100,000 people, for Aboriginal people this rate is around 59,000 episodes per 100,000 around 1.7 times the rate of 34,400 per 100,000 for non-Aboriginal people. Hospitalisations for all causes in MLHD occurred at a rate of 39,202 episodes per 100,000 residents; 38,744 per 100,000 non-Aboriginal people with significantly more episodes of hospital care for Aboriginal people at 48,678 per 100,000 Aboriginal residents. When comparing hospitalisation by Aboriginality across Local Health Districts in NSW, MLHD appears to have significantly fewer hospitalisations for the Aboriginal population than NSW and other rural LHDs, however the MLHD non-Aboriginal population has a significantly higher rate of hospitalisation than NSW and other LHDs. This could in part be due to non-identification of Aboriginality for an admission, as 0.4 per cent of hospitalisations in MLHD did not have Aboriginality recorded (if these were for Aboriginal people it would increase the number of admissions by 10%). The rate of hospitalisation for Aboriginal people has increased significantly since the early 1990’s and at a much higher rate than the non-Aboriginal population; this could in part be due to increases in identification and recording of aboriginality at admission and better access to services since the late 1990’s.
CAUSE OF HOSPITALISATION
The major category of cause of hospitalisation for Aboriginal people in Murrumbidgee LHD for 2008-09 to 2010-11 was Injury and Poisoning making up around 16 per cent of all hospitalisations or approximately 600 hospitalisations per year at an age-standardised rate of 6,894 per 100,000 Aboriginal people in 2010-11 significantly higher than the rate of 5,033 per 100,000 non-Aboriginal people. When looking at annual data for MLHD, the number in each category fluctuates due to small numbers, making annual comparisons difficult. Data also has been influenced by the changes in hospital coding, in particular coding for diabetes (Table 2).
In NSW for the 10 years from 2001-02 to 2010-11 the major category for hospitalisation for Aboriginal people was Dialysis followed by Injury and Poisoning. Compared with rates in non-Aboriginal people, hospitalisation rates in Aboriginal people in NSW are (around):
150% higher for conditions for which hospitalisation can be avoided through prevention and early management 170% higher for diabetes 60% higher for cardiovascular diseases 250% higher for chronic respiratory diseases 50% higher for injury and poisoning 200% higher for alcohol-related conditions.
(Health Statistics NSW)
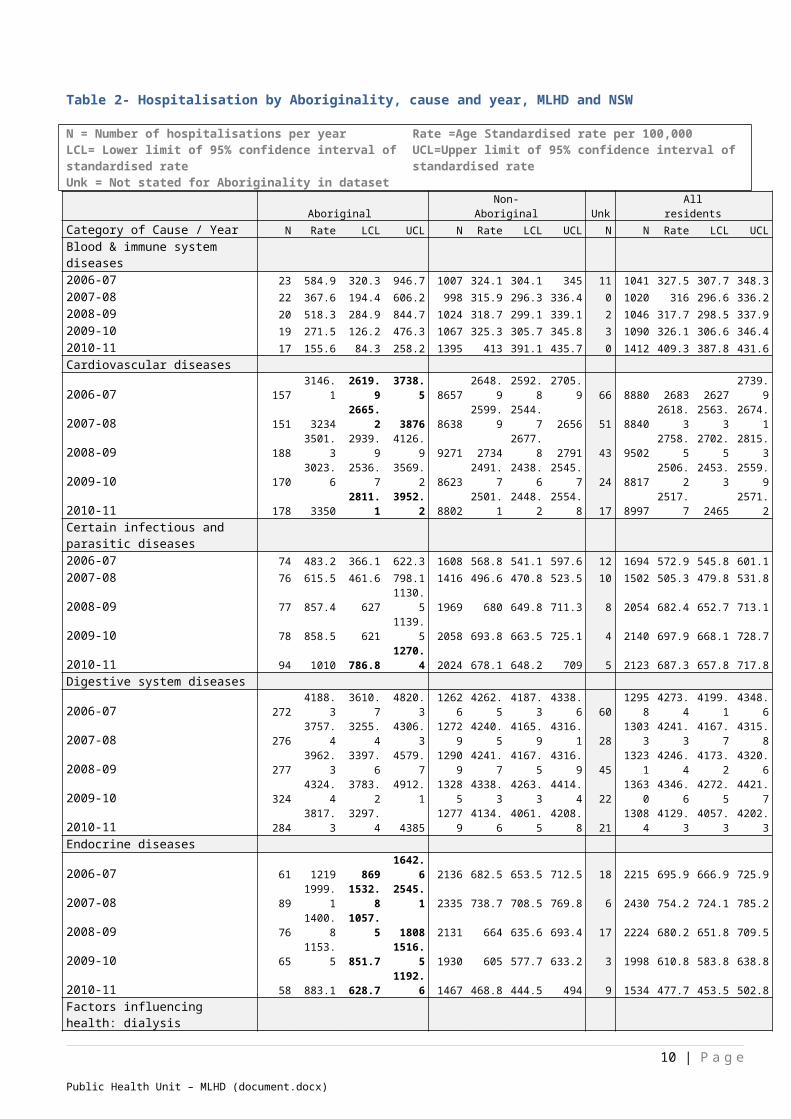
In the MLHD the rates of hospitalisation which were significantly higher in the Aboriginal population compared to the non-Aboriginal population are indicated in the table as bold figures for the 95 per cent confidence interval (Table 2), these include: cardiovascular disease; certain infectious and parasitic diseases; endocrine diseases (includes diabetes); dialysis; injury and poisoning; maternal, neonatal and congenital causes; mental and behavioural disorders; respiratory disease; skin and subcutaneous tissue diseases and ill-defined conditions.
6 | P a g e
Public Health Unit – MLHD (document.docx)

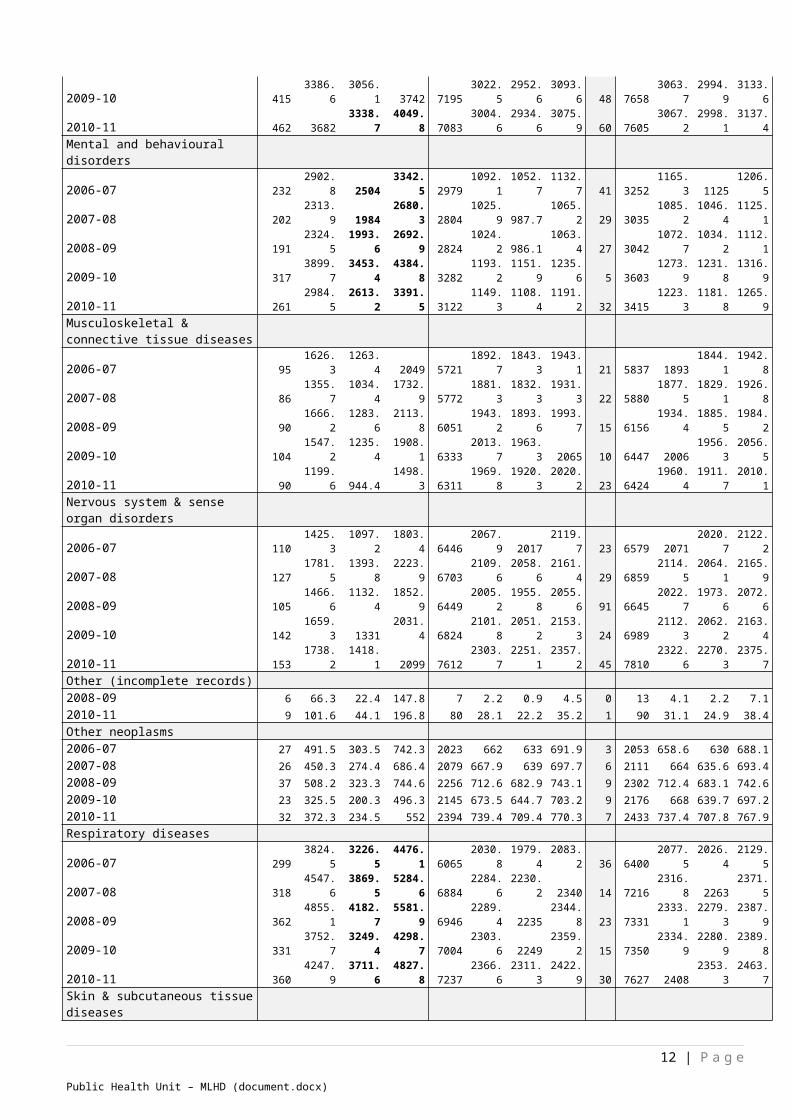
Table 2- Hospitalisation by Aboriginality, cause and year, MLHD and NSW
N = Number of hospitalisations per year Rate =Age Standardised rate per 100,000LCL= Lower limit of 95% confidence interval of standardised rate UCL=Upper limit of 95% confidence interval of standardised rateUnk = Not stated for Aboriginality in dataset
Aboriginal Non-Aboriginal Unk All residentsCategory of Cause / Year N Rate LCL UCL N Rate LCL UCL N N Rate LCL UCLBlood & immune system diseases2006-07 23 584.9 320.3 946.7 1007 324.1 304.1 345 11 1041 327.5 307.7 348.32007-08 22 367.6 194.4 606.2 998 315.9 296.3 336.4 0 1020 316 296.6 336.22008-09 20 518.3 284.9 844.7 1024 318.7 299.1 339.1 2 1046 317.7 298.5 337.92009-10 19 271.5 126.2 476.3 1067 325.3 305.7 345.8 3 1090 326.1 306.6 346.42010-11 17 155.6 84.3 258.2 1395 413 391.1 435.7 0 1412 409.3 387.8 431.6Cardiovascular diseases2006-07 157 3146.1 2619.9 3738.5 8657 2648.9 2592.8 2705.9 66 8880 2683 2627 2739.92007-08 151 3234 2665.2 3876 8638 2599.9 2544.7 2656 51 8840 2618.3 2563.3 2674.12008-09 188 3501.3 2939.9 4126.9 9271 2734 2677.8 2791 43 9502 2758.5 2702.5 2815.32009-10 170 3023.6 2536.7 3569.2 8623 2491.7 2438.6 2545.7 24 8817 2506.2 2453.3 2559.92010-11 178 3350 2811.1 3952.2 8802 2501.1 2448.2 2554.8 17 8997 2517.7 2465 2571.2Certain infectious and parasitic diseases2006-07 74 483.2 366.1 622.3 1608 568.8 541.1 597.6 12 1694 572.9 545.8 601.12007-08 76 615.5 461.6 798.1 1416 496.6 470.8 523.5 10 1502 505.3 479.8 531.82008-09 77 857.4 627 1130.5 1969 680 649.8 711.3 8 2054 682.4 652.7 713.12009-10 78 858.5 621 1139.5 2058 693.8 663.5 725.1 4 2140 697.9 668.1 728.72010-11 94 1010 786.8 1270.4 2024 678.1 648.2 709 5 2123 687.3 657.8 717.8Digestive system diseases2006-07 272 4188.3 3610.7 4820.3 12626 4262.5 4187.3 4338.6 60 12958 4273.4 4199.1 4348.62007-08 276 3757.4 3255.4 4306.3 12729 4240.5 4165.9 4316.1 28 13033 4241.3 4167.7 4315.82008-09 277 3962.3 3397.6 4579.7 12909 4241.7 4167.5 4316.9 45 13231 4246.4 4173.2 4320.62009-10 324 4324.4 3783.2 4912.1 13285 4338.3 4263.3 4414.4 22 13630 4346.6 4272.5 4421.72010-11 284 3817.3 3297.4 4385 12779 4134.6 4061.5 4208.8 21 13084 4129.3 4057.3 4202.3Endocrine diseases2006-07 61 1219 869 1642.6 2136 682.5 653.5 712.5 18 2215 695.9 666.9 725.92007-08 89 1999.1 1532.8 2545.1 2335 738.7 708.5 769.8 6 2430 754.2 724.1 785.22008-09 76 1400.8 1057.5 1808 2131 664 635.6 693.4 17 2224 680.2 651.8 709.52009-10 65 1153.5 851.7 1516.5 1930 605 577.7 633.2 3 1998 610.8 583.8 638.82010-11 58 883.1 628.7 1192.6 1467 468.8 444.5 494 9 1534 477.7 453.5 502.8Factors influencing health: dialysis2006-07 519 12498.1 11412.5 13656.6 7088 2190 2138.7 2242.2 7 7614 2321.3 2269 2374.52007-08 387 8536.1 7682.1 9457 6788 2024.4 1976.1 2073.7 3 7178 2134.9 2085.4 2185.32008-09 223 3786.7 3303.6 4320.3 8397 2462.3 2409.3 2516.1 42 8662 2531.2 2477.6 2585.62009-10 432 7038.6 6389.3 7735.9 7860 2277.5 2226.7 2329 16 8308 2391.2 2339.5 2443.82010-11 267 4193.5 3704.6 4728.8 12463 4398 4318.1 4479 3 12734 4406.7 4328 4486.6Factors influencing health: other2006-07 591 9612.2 8656.8 10627.6 11354 3865.6 3793.9 3938.2 226 12171 3996.3 3924.9 4068.72007-08 315 3301.9 2816.4 3829.7 12310 4114.9 4041.5 4189.3 42 12667 4104.1 4032 4177.12008-09 344 4003.4 3488 4561.7 13048 4309.1 4234.2 4384.9 52 13444 4299 4225.6 4373.42009-10 318 3466.6 2981.7 3993.5 13083 4264.9 4190.8 4340 31 13432 4247.4 4174.6 43212010-11 362 3657.8 3211.3 4140.5 12793 4136.2 4063.3 4210 34 13188 4137.5 4065.8 4210.1Genitourinary diseases2006-07 113 1587.3 1259 1964.9 5365 1870 1819.4 1921.6 19 5497 1870.2 1820.4 1921.12007-08 140 2128.6 1722 2589.6 5816 1986.3 1934.6 2039 16 5972 1992.3 1941.2 2044.42008-09 160 2234.7 1854.9 2661.8 6107 2053 2000.7 2106.2 23 6290 2067 2015.2 2119.72009-10 148 2007.2 1634 2428.8 6107 2040.5 1988.3 2093.6 16 6271 2042.2 1990.8 2094.62010-11 160 2199.2 1810.4 2636.4 6294 2071.1 2018.8 2124.3 23 6477 2079.1 2027.5 2131.7
7 | P a g e
Public Health Unit – MLHD (document.docx)
Injury & poisoning2006-07 519 6355.9 5701.3 7054.5 15101 5105 5022.7 5188.4 161 15781 5208.3 5126.2 5291.32007-08 497 5632.1 5059.8 6243.7 15807 5275.4 5192.1 5359.7 105 16409 5333.9 5251.3 5417.52008-09 617 6944.9 6285.9 7644.5 16384 5356.8 5273.5 5441 82 17083 5438.7 5356 5522.42009-10 573 6263.5 5690 6873.6 16560 5369.4 5286.1 5453.6 63 17197 5430.8 5348.3 5514.32010-11 612 6894 6257 7570.2 15729 5033.3 4952.9 5114.6 66 16407 5108.6 5028.8 5189.3Malignant neoplasms= cancers2006-07 53 1306.2 936.9 1759.5 4930 1496.4 1454.5 1539.1 36 5019 1503.2 1461.6 1545.72007-08 46 1079.2 759 1478.2 5003 1492.8 1451.3 1535.2 25 5074 1491.5 1450.4 1533.62008-09 58 1109.4 793 1494.3 5114 1486.3 1445.4 1528.1 22 5194 1489.6 1448.9 1531.12009-10 43 824 568 1145.9 5339 1527.5 1486.2 1569.6 12 5393 1521.5 1480.7 1563.32010-11 75 1601 1216.5 2057.5 5164 1451.1 1411.2 1491.8 12 5251 1455.6 1415.9 1496.1Maternal, neonatal & congenital causes2006-07 419 3648.8 3291.1 4033.3 7355 3097.2 3026.4 3169.2 73 7847 3154.6 3084.7 3225.62007-08 418 3653.1 3296 4037 6942 2908.4 2840 2978 50 7410 2962.9 2895.4 3031.52008-09 460 3973.1 3602.7 4370 7179 2986.6 2917.5 3057 81 7720 3063.1 2994.7 3132.72009-10 415 3386.6 3056.1 3742 7195 3022.5 2952.6 3093.6 48 7658 3063.7 2994.9 3133.62010-11 462 3682 3338.7 4049.8 7083 3004.6 2934.6 3075.9 60 7605 3067.2 2998.1 3137.4Mental and behavioural disorders2006-07 232 2902.8 2504 3342.5 2979 1092.1 1052.7 1132.7 41 3252 1165.3 1125 1206.52007-08 202 2313.9 1984 2680.3 2804 1025.9 987.7 1065.2 29 3035 1085.2 1046.4 1125.12008-09 191 2324.5 1993.6 2692.9 2824 1024.2 986.1 1063.4 27 3042 1072.7 1034.2 1112.12009-10 317 3899.7 3453.4 4384.8 3282 1193.2 1151.9 1235.6 5 3603 1273.9 1231.8 1316.92010-11 261 2984.5 2613.2 3391.5 3122 1149.3 1108.4 1191.2 32 3415 1223.3 1181.8 1265.9Musculoskeletal & connective tissue diseases2006-07 95 1626.3 1263.4 2049 5721 1892.7 1843.3 1943.1 21 5837 1893 1844.1 1942.82007-08 86 1355.7 1034.4 1732.9 5772 1881.3 1832.3 1931.3 22 5880 1877.5 1829.1 1926.82008-09 90 1666.2 1283.6 2113.8 6051 1943.2 1893.6 1993.7 15 6156 1934.4 1885.5 1984.22009-10 104 1547.2 1235.4 1908.1 6333 2013.7 1963.3 2065 10 6447 2006 1956.3 2056.52010-11 90 1199.6 944.4 1498.3 6311 1969.8 1920.3 2020.2 23 6424 1960.4 1911.7 2010.1Nervous system & sense organ disorders2006-07 110 1425.3 1097.2 1803.4 6446 2067.9 2017 2119.7 23 6579 2071 2020.7 2122.22007-08 127 1781.5 1393.8 2223.9 6703 2109.6 2058.6 2161.4 29 6859 2114.5 2064.1 2165.92008-09 105 1466.6 1132.4 1852.9 6449 2005.2 1955.8 2055.6 91 6645 2022.7 1973.6 2072.62009-10 142 1659.3 1331 2031.4 6824 2101.8 2051.2 2153.3 24 6989 2112.3 2062.2 2163.42010-11 153 1738.2 1418.1 2099 7612 2303.7 2251.1 2357.2 45 7810 2322.6 2270.3 2375.7Other (incomplete records)2008-09 6 66.3 22.4 147.8 7 2.2 0.9 4.5 0 13 4.1 2.2 7.12010-11 9 101.6 44.1 196.8 80 28.1 22.2 35.2 1 90 31.1 24.9 38.4Other neoplasms2006-07 27 491.5 303.5 742.3 2023 662 633 691.9 3 2053 658.6 630 688.12007-08 26 450.3 274.4 686.4 2079 667.9 639 697.7 6 2111 664 635.6 693.42008-09 37 508.2 323.3 744.6 2256 712.6 682.9 743.1 9 2302 712.4 683.1 742.62009-10 23 325.5 200.3 496.3 2145 673.5 644.7 703.2 9 2176 668 639.7 697.22010-11 32 372.3 234.5 552 2394 739.4 709.4 770.3 7 2433 737.4 707.8 767.9Respiratory diseases2006-07 299 3824.5 3226.5 4476.1 6065 2030.8 1979.4 2083.2 36 6400 2077.5 2026.4 2129.52007-08 318 4547.6 3869.5 5284.6 6884 2284.6 2230.2 2340 14 7216 2316.8 2263 2371.52008-09 362 4855.1 4182.7 5581.9 6946 2289.4 2235 2344.8 23 7331 2333.1 2279.3 2387.92009-10 331 3752.7 3249.4 4298.7 7004 2303.6 2249 2359.2 15 7350 2334.9 2280.9 2389.82010-11 360 4247.9 3711.6 4827.8 7237 2366.6 2311.3 2422.9 30 7627 2408 2353.3 2463.7Skin & subcutaneous tissue diseases2006-07 68 866 605.4 1178.3 1535 522.6 496.4 549.8 11 1614 536 509.9 563.22007-08 62 604.3 445.4 796.3 1508 504.6 479 531.2 6 1576 515 489.4 541.4
8 | P a g e
Public Health Unit – MLHD (document.docx)
2008-09 60 603.7 444.4 796.9 1569 513.2 487.7 539.8 5 1634 521.9 496.4 548.32009-10 83 861.8 639.3 1123.7 1635 534.6 508.4 561.8 5 1723 549.8 523.6 5772010-11 59 608.3 426.1 829.6 1590 511.4 485.9 537.8 9 1658 519.2 493.9 545.5Symptoms, signs & abnormal findings2006-07 302 4510.5 3926.1 5147 8217 2691.9 2633.2 2751.6 44 8563 2754.7 2695.9 2814.42007-08 313 4444.4 3876.4 5062.1 8796 2841.9 2781.9 2903 35 9144 2894.8 2834.9 2955.72008-09 288 4199.1 3627.3 4823.1 9454 2999.2 2937.9 3061.4 24 9766 3029.5 2968.7 3091.32009-10 355 5249.2 4625.9 5923.5 10149 3175.2 3112.4 3238.9 15 10520 3217 3154.6 3280.42010-11 325 4808.5 4204.9 5463.8 9881 3057.2 2995.8 3119.6 17 10223 3092.6 3031.6 3154.6
POTENTIALLY PREVENTABLE HOSPITALISATIONS (PPH)
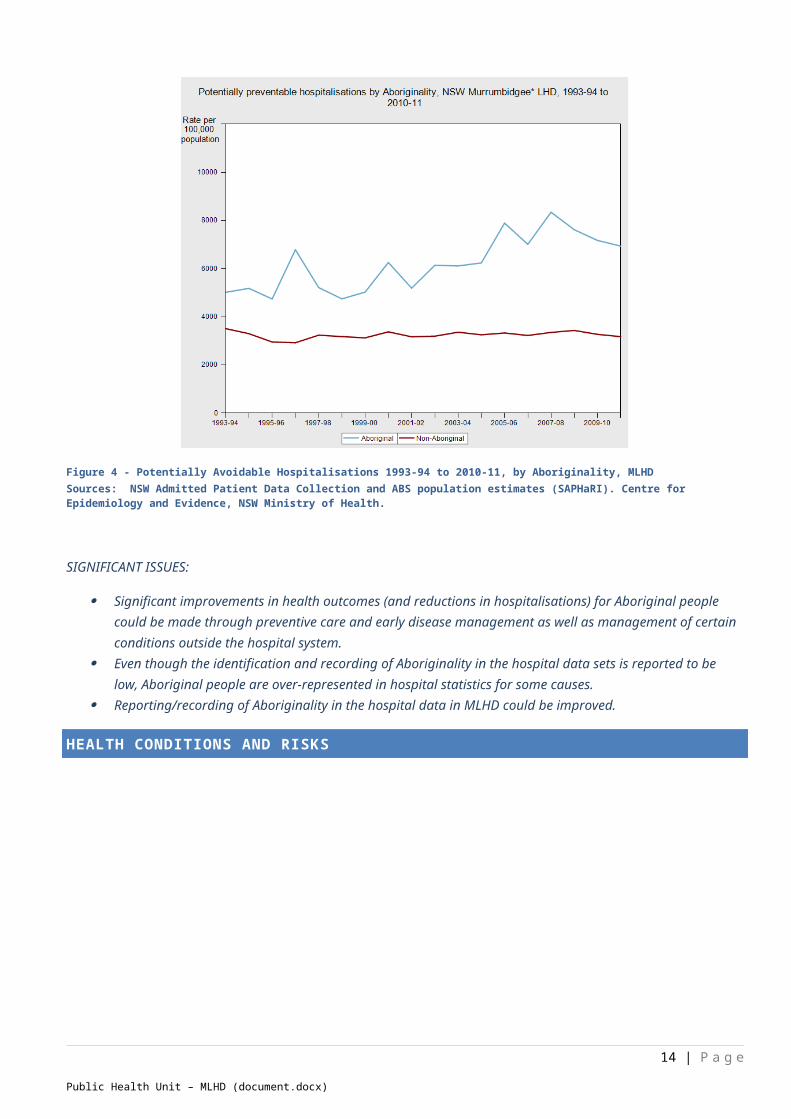
Potentially Preventable Hospitalisations (also known as Ambulatory Care Sensitive Conditions) are those which are considered potentially avoidable through preventive care and early disease management. In NSW over the period 1993-94 to 2010-11, PPH rates in Aboriginal people were consistently more than double those in non-Aboriginal people, both overall and in each of the vaccine-preventable, acute and chronic categories. In 2010-11, in MLHD, the rate of PPH for Aboriginal people was 6,914 per 100,000, more than double the rate for non-Aboriginal people of 3,149 per 100,000. The PPH rate for Aboriginal people in MLHD was also significantly higher than the NSW rate for Aboriginal people of 5,770 per 100,000, but lower than for other rural LHDs. Where the trend in PPH rates for non-Aboriginal people has been gradually decreasing since the early 1990s the rate of PPH for Aboriginal people has been increasing (this is again influenced by increased identification of Aboriginality as well as coding changes for diabetes). After July 2010, numbers and rates were affected by a significant change in coding standards for diabetes, a substantial contributor to total preventable hospitalisations.
Figure 4 - Potentially Avoidable Hospitalisations 1993-94 to 2010-11, by Aboriginality, MLHDSources: NSW Admitted Patient Data Collection and ABS population estimates (SAPHaRI). Centre for Epidemiology and Evidence, NSW Ministry of Health.
SIGNIFICANT ISSUES:
9 | P a g e
Public Health Unit – MLHD (document.docx)
Significant improvements in health outcomes (and reductions in hospitalisations) for Aboriginal people could be made through preventive care and early disease management as well as management of certain conditions outside the hospital system.
Even though the identification and recording of Aboriginality in the hospital data sets is reported to be low, Aboriginal people are over-represented in hospital statistics for some causes.
Reporting/recording of Aboriginality in the hospital data in MLHD could be improved.
HEALTH CONDITIONS AND RISKS
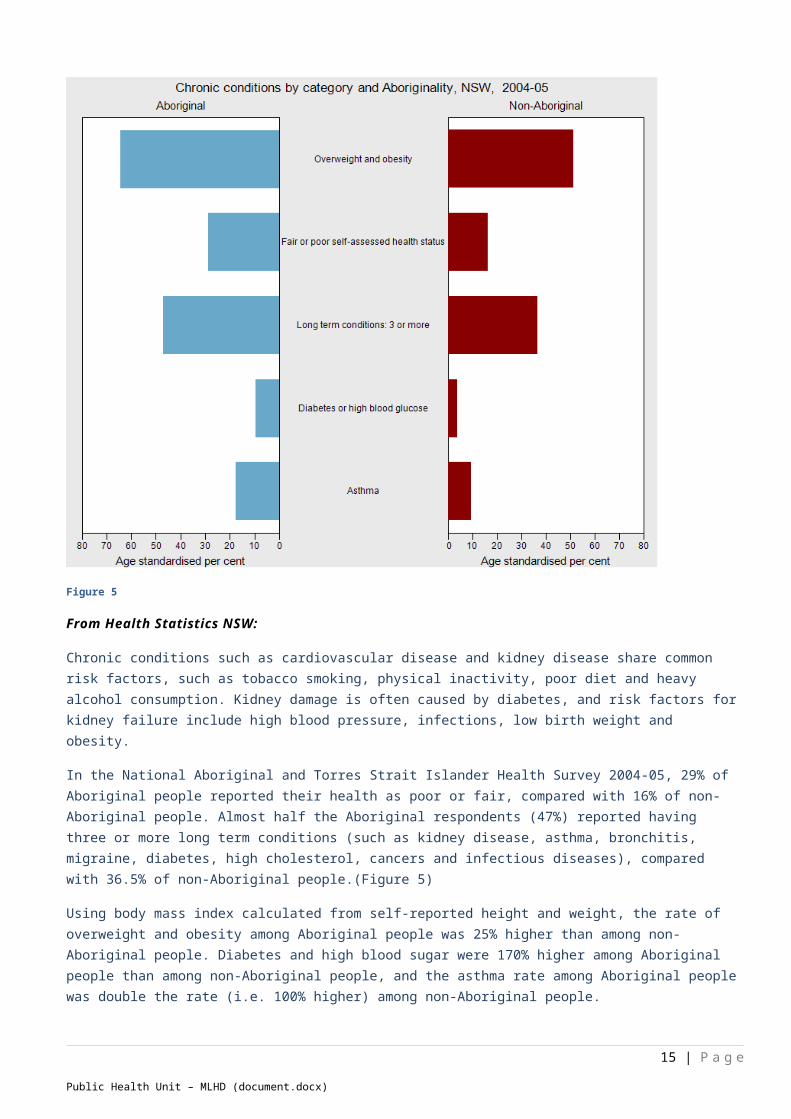
Figure 5
From Health Statistics NSW:
Chronic conditions such as cardiovascular disease and kidney disease share common risk factors, such as tobacco smoking, physical inactivity, poor diet and heavy alcohol consumption. Kidney damage is often caused by diabetes, and risk factors for kidney failure include high blood pressure, infections, low birth weight and obesity.
In the National Aboriginal and Torres Strait Islander Health Survey 2004-05, 29% of Aboriginal people reported their health as poor or fair, compared with 16% of non-Aboriginal people. Almost half the Aboriginal respondents (47%) reported having three or more long term conditions (such as kidney disease, asthma, bronchitis, migraine, diabetes, high cholesterol, cancers and infectious diseases), compared with 36.5% of non-Aboriginal people.(Figure 5)
Using body mass index calculated from self-reported height and weight, the rate of overweight and obesity among Aboriginal people was 25% higher than among non-Aboriginal people. Diabetes and high blood sugar were 170% higher among
10 | P a g e
Public Health Unit – MLHD (document.docx)

Aboriginal people than among non-Aboriginal people, and the asthma rate among Aboriginal people was double the rate (i.e. 100% higher) among non-Aboriginal people.
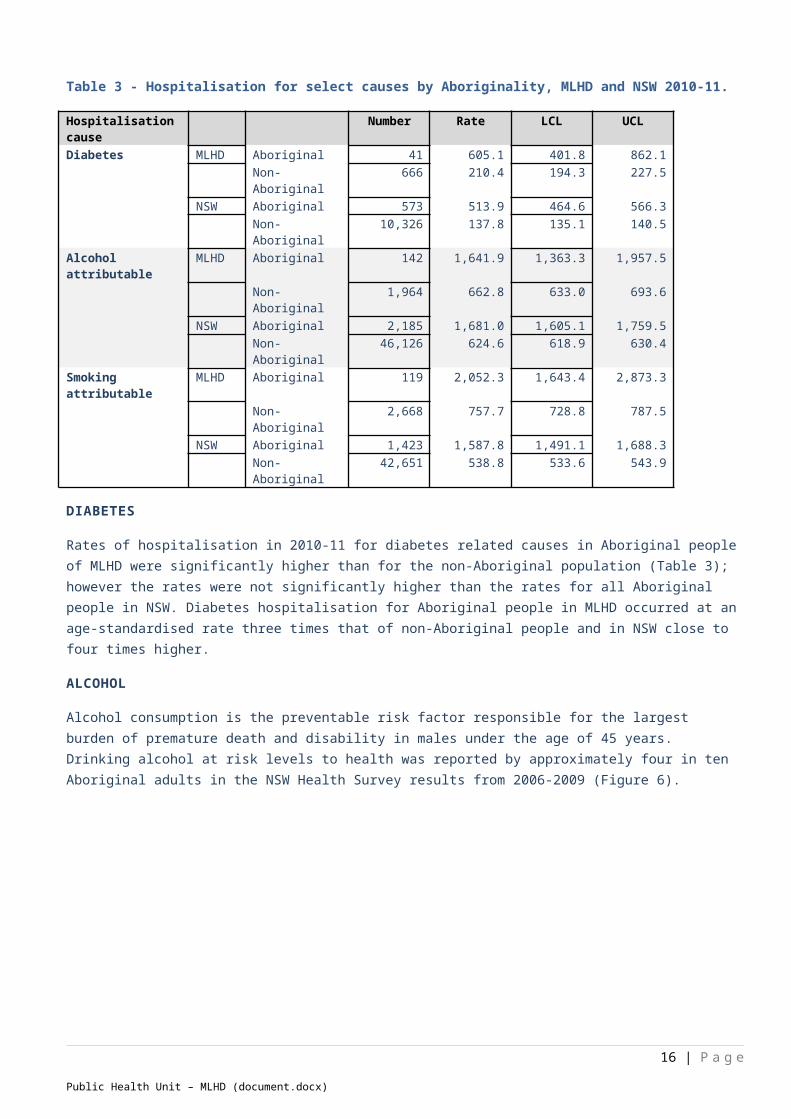
Table 3 - Hospitalisation for select causes by Aboriginality, MLHD and NSW 2010-11.
Hospitalisation cause Number Rate LCL UCLDiabetes MLHD Aboriginal 41 605.1 401.8 862.1
Non-Aboriginal 666 210.4 194.3 227.5NSW Aboriginal 573 513.9 464.6 566.3
Non-Aboriginal 10,326 137.8 135.1 140.5Alcohol attributable MLHD Aboriginal 142 1,641.9 1,363.3 1,957.5
Non-Aboriginal 1,964 662.8 633.0 693.6NSW Aboriginal 2,185 1,681.0 1,605.1 1,759.5
Non-Aboriginal 46,126 624.6 618.9 630.4Smoking attributable MLHD Aboriginal 119 2,052.3 1,643.4 2,873.3
Non-Aboriginal 2,668 757.7 728.8 787.5NSW Aboriginal 1,423 1,587.8 1,491.1 1,688.3
Non-Aboriginal 42,651 538.8 533.6 543.9
DIABETES
Rates of hospitalisation in 2010-11 for diabetes related causes in Aboriginal people of MLHD were significantly higher than for the non-Aboriginal population (Table 3); however the rates were not significantly higher than the rates for all Aboriginal people in NSW. Diabetes hospitalisation for Aboriginal people in MLHD occurred at an age-standardised rate three times that of non-Aboriginal people and in NSW close to four times higher.
ALCOHOL
Alcohol consumption is the preventable risk factor responsible for the largest burden of premature death and disability in males under the age of 45 years. Drinking alcohol at risk levels to health was reported by approximately four in ten Aboriginal adults in the NSW Health Survey results from 2006-2009 (Figure 6).
Figure 6
11 | P a g e
Public Health Unit – MLHD (document.docx)
Hospitalisations regarded as being attributable to alcohol consumption occurred at a rate of 1,642 hospitalisation per 100,000 Aboriginal people in MLHD (2010-11) which is 2.5 times the rate for non-Aboriginal people in MLHD and slightly higher than the rate for Aboriginal people in all NSW (Table 3 - Hospitalisation for select causes by Aboriginality, MLHD and NSW 2010-11.Table 3). Alcohol attributable hospitalisations for Aboriginal people have risen steadily since the early 1990’s in MLHD but have remained relatively steady for non-Aboriginal people in MLHD for the same period.
SMOKING
Tobacco smoking is the single most preventable cause of ill-health and death in Australia, contributing to more drug-related hospitalisations and deaths than alcohol and illicit drugs combined. It is a major risk factor for cardiovascular disease and
cancer. In NSW over the period 2006-2009 approximately one in three Aboriginal males and females aged 16 years or over were current smokers, which was double the reported rate for non-Aboriginal people (
). The reported rate of smoking for Aboriginal adults has significantly decreased since 2002-2005. For the former Greater Southern Area (approximately MLHD plus Southern NSW LHD) for 2006-2009, the adult Aboriginal smoking rate was 50 per cent, compared to around 34 per cent of Aboriginal adults (NSW Health Survey results).
Hospitalisations regarded as being attributable to tobacco smoking occurred at a rate of 2,052 hospitalisation per 100,000 Aboriginal people in MLHD (2010-11) which is 2.7 times the rate for non-Aboriginal people in MLHD and slightly higher than the rate for Aboriginal people in all NSW, but not significantly so (Table 3 - Hospitalisation for select causes by Aboriginality, MLHD and NSW 2010-11.). Smoking attributable hospitalisations for Aboriginal people have increased since the early 1990’s to 2010-11 for Aboriginal males and females in NSW, but decreased for non-Aboriginal people, similarly in MLHD the rates of smoking attributable hospitalisations have increased for Aboriginal people and decreased slightly for non-Aboriginal people for the same period.
Smoking during pregnancy can increase the risk of pregnancy complications as well as premature births, low birth weight babies and the risk of stillbirths; as smoking reduces the oxygen supply to the baby in the womb. Smoking at all during pregnancy was reported by approximately 50 per cent of Aboriginal mothers in MLHD (50.5 per cent of Aboriginal mothers in NSW) who had babies in 2009 (NSW Perinatal Data Collection) compared to 10.1 per cent of all mothers in NSW and of 17.3 per cent of all mothers in MLHD.
INJURY
Injury and poisoning hospitalisation for Aboriginal people of MLHD was significantly higher than non-Aboriginal people at around 1.4 times the rate (Table 2). Deaths from injury and poisoning for Aboriginal people in NSW made up 12 per cent of deaths compared to 5 per cent for non-Aboriginal people. Aboriginal people are more likely than non-Aboriginal people to be victims of inter-personal violence. In NSW in the past 20 years the rate of hospitalisation for interpersonal violence was consistently five times higher in Aboriginal people compared to non-Aboriginal people.
SIGNIFICANT ISSUES:
Smoking rates, including smoking during pregnancy Alcohol consumption Injury prevention
MATERNAL AND CHILD HEALTH
INFANT MORTALITY
Aboriginal infant mortality was 6.8 per 100,000 live births in NSW in 2007-2009. The rates of Aboriginal infant mortality are closer to rates of Indigenous communities in other countries than they are to rates in the general population of Australia (4.3
12 | P a g e
Public Health Unit – MLHD (document.docx)

deaths per 1,000 live births in 2007-2009). Infant mortality in the Aboriginal population of NSW has approximately halved since 1998-2000. Infant mortality is the number of deaths in children aged up to one year per 1,000 live births.
PERINATAL DEATH
Perinatal deaths include stillbirths or deaths within 28 days of birth and only include those reported to the Perinatal Data Collection (PDC), deaths occurring after discharge or transfer of the baby may not be included, and Aboriginality is not well reported, such that there is likely to be an under-reporting of true number by around 30%. In NSW, the perinatal death rate in babies born to Aboriginal mothers was higher than to non-Aboriginal mothers from 1991 to 2010, although the rate has decreased from around 20-25 deaths per 1,000 live births to around 15 deaths per 1,000 live births compared to around 9-10 per 1,000 live births to non-Aboriginal mothers. In general, perinatal mortality rates are higher among teenage mothers and Aboriginal teenage mothers make up 5 times the proportion of Aboriginal mothers compared to non-Aboriginal mothers.
LOW BIRTH WEIGHT
Low birth weight babies (birth weight less than 2,500 grams) have a greater risk of poor health and dying, require longer hospitalisation after birth, and are more likely to develop disabilities. Low birth weight is also an indication of the health and care of the mother during pregnancy. In NSW in 2010, the proportion of low birth weight babies among Aboriginal mothers was around double the proportion in non-Aboriginal mothers, this proportion has not changed over the past twenty years (Health Statistics NSW). It is difficult to analyse data for births in the MLHD as only births occurring in NSW facilities or attended by NSW midwives are recorded in the NSW Midwives Data Collection. MLHD has significant patient flows across State borders to Victoria (including all births to mothers of Albury LGA and surrounding areas) and the Australian Capital Territory. Where a birth occurred in NSW for MLHD residents in 2007, around seven per cent of babies of Aboriginal mothers were of low birth weight compared to around five per cent of babies with non-Aboriginal mothers. Another data source is the locally collected data for the Universal Home Visit and Safe Start programs. In this data-base for the period July 2011 to May 2012, there were 3,083 births to MLHD mothers with 228 families identifying as Aboriginal (approximately 7% of births). Six per cent of all babies born in MLHD were low birth weight babies during this period, five per cent of non-Aboriginal babies were low birth weight and nine per cent of Aboriginal babies. Aboriginal babies made up seven per cent of all births in MLHD but twelve per cent of all low birth weight babies.
ANTENATAL CARE
Antenatal care should commence as early as possible in pregnancy to ensure the best outcomes for the mother and baby. In NSW for the period 1996 to 2010, the proportion of Aboriginal mothers who attended their first antenatal visit before 14 weeks gestation increased from 44 per cent to 71 per cent. However the proportion is still below that recorded for non-Aboriginal mothers. For MLHD-based mothers giving birth in NSW, 75 per cent of Aboriginal mothers attended their first antenatal visit before 14 weeks gestation compared to 88 per cent of non-Aboriginal mothers. Antenatal visits prior to 20 weeks gestation were reported by 87 per cent of Aboriginal mothers and 95 per cent of non-Aboriginal mothers in MLHD in 2010 compared to 84 per cent of Aboriginal mothers and 92 per cent of non-Aboriginal mothers in NSW. The proportion of Aboriginal women in MLHD attending antenatal care has been gradually increasing from 1996 to 2010
PREMATURITY
Births for a gestational age less than 37 weeks are classified as premature. In NSW in period 2009-2010, 7.3 per cent of all babies were premature; 11 per cent of Aboriginal babies and 7.2 per cent of non-Aboriginal babies. For the MLHD from the NSW-based births; 7.3 per cent of Aboriginal babies were premature compared to 6.3 per cent of non-Aboriginal babies. The proportion of Aboriginal babies born prematurely has decreased slightly since 2000-01 to 2009-10.
ACUTE RESPIRATORY INFECTIONS
In 2010-11, hospitalisation rates for acute respiratory infections in Aboriginal children (younger than 5 years) were 7393.1 per 100,000 population for males and 5317.8 per 100,000 for females. The rates have generally been 70-80% higher among Aboriginal children than among non-Aboriginal children. Rates for male Aboriginal children have been 30-40% higher than for females. Across all ages, rates in the Aboriginal population have been twice the rates in the non-Aboriginal population.
13 | P a g e
Public Health Unit – MLHD (document.docx)
Housing has been identified as a major factor affecting the health of Aboriginal people. Inadequate or poorly maintained housing and the absence of functioning infrastructure can pose serious health risks. Overcrowded dwellings and poor quality housing can lead to the spread of infectious diseases. (Health Statistics NSW)
Note: acute respiratory infections include various acute upper and lower respiratory infections, influenza and pneumonia.
IMMUNISATION
At the end of December 2010, 91.8 per cent of Aboriginal children in MLHD (excluding Albury LGA) and 100 per cent of Aboriginal children in Albury LGA aged 12-15 months were fully immunised compared to 93.4 per cent of all children in MLHD and 94.4 per cent in Albury LGA. In NSW for the same period, 88.3 per cent of Aboriginal children aged 12-15 months were fully immunised compared to 91.5 per cent of all children of that age.
SIGNIFICANT ISSUES:
Increasing antenatal care at very early stages of pregnancy to assess risks and improve health outcomes. Educate pregnant women and families about the risk factors associated with perinatal morbidity and mortality i.e.
reducing alcohol and tobacco use in pregnancy and promote breastfeeding. Transport services, whether provided by public system, Aboriginal Community Controlled Organisations or the AMIHS
team, are essential for access to care.
CURRENT STAFFING IN MLHD
Figure 7 - Location of Aboriginal Health Staff and Aboriginal populations in MLHD, 2011
Aboriginal Health Staff in MLHD consists of a Manager in Albury and Aboriginal Health Education and Hospital Liaison Officers (AHEO_LO) in other centres across the District, as well as the Aboriginal Maternal Infant Health Strategy (AMIHS) staff;
14 | P a g e
Public Health Unit – MLHD (document.docx)
Chronic Care; and Home Visiting (Table 4). Murrumbidgee LHD employs many Aboriginal people throughout the District who bring their expertise to areas such as Mental Health and Drug and Alcohol as well as Aboriginal traineeships in mental health, Environmental Health and administration. Most staff are centred where the large populations of Aboriginal people reside, Albury, Wagga Wagga and Griffith and provide outreach to other areas. Some Aboriginal people in MLHD live 100 to 200km from specialist staff requiring long distance travel by either MLHD staff or Aboriginal clients, this is of particular note in West Wyalong, Young, Boorowa and Hay regions (Figure 7).
Other organisations with an Aboriginal health focus within the MLHD - but not funded by MLHD - are the Aboriginal Medical and Dental Health Services in Albury and Wagga Wagga and the Griffith Aboriginal Medical Service as well a as programs run through the Medicare Locals.
Table 4 – MLHD Staff either employed by Aboriginal Health or with an Aboriginal health focus, August 2011
Location Service FTE Position
Albury Area Office Aboriginal Health 1.0 Manager Aboriginal HealthAlbury Area Office Aboriginal Health 1.0 Team Leader Aboriginal Health
Albury Area Office Aboriginal Health 1.0 Coordinator Aboriginal Maternal Infant Health StrategyAlbury Area Office Public Health 1.0 Aboriginal Environmental Health Officer
Albury CHC Aboriginal Health 1.0 Aboriginal Health Education/Hospital Liaison OfficersAlbury CHC Aboriginal Health Vacant Aboriginal Health Education/Hospital Liaison Officers
Deniliquin CHC Aboriginal Health 1.0 Aboriginal Health Education/Hospital Liaison OfficersGriffith Hospital Aboriginal Health Vacant Team Leader Aboriginal Health
Griffith CHC Aboriginal Health Vacant Aboriginal Health Education/Hospital Liaison OfficersGriffith Hospital Aboriginal Health 2 x 0.6 Aboriginal Maternal Infant Health Strategy
Lake Cargelligo Aboriginal Health 2 x 0.2 Aboriginal Maternal Infant Health StrategyLake Cargelligo Aboriginal Health 0.8 Aboriginal Health Education/Hospital Liaison Officers
Leeton CHC Aboriginal Health 0.8 Aboriginal Health Education/Hospital Liaison OfficersNarrandera CHC Aboriginal Health 1.0 Aboriginal Health Education/Hospital Liaison Officers
Narrandera CHC Aboriginal Health 2 x 0.6 Aboriginal Maternal Infant Health StrategyTumut CHC Aboriginal Health 2 x 1.0 Aboriginal Health Education/Hospital Liaison Officers
Wagga Aboriginal Health Unit Aboriginal Health 1.0 Coordinator Chronic CareWagga Aboriginal Health Unit Aboriginal Health 1.0 Administrative assistant
Wagga CHC Aboriginal Health 1.0 Aboriginal Health Chronic CareWagga CHC Aboriginal Health 1.0 Aboriginal Health Education/Hospital Liaison Officers
Wagga CHC Aboriginal Health 2 x 1.0 Aboriginal Home VisitingWagga CHC Aboriginal Health 1.1 Aboriginal Maternal Infant Health Strategy
*Vacant positions are currently being recruited
IN SUMMARY
Socioeconomic disadvantage is a key determinant of health and Aboriginal people in NSW experience significant disadvantage compared to non-Aboriginal people. Aboriginal people have lower household incomes than the general population which is contributed to by lower labour force participation, school retention rates, and lack of post school qualifications.
The higher burden of disease in the Aboriginal population is due largely to preventable disease such as cardiovascular disease; type 2 diabetes; mental disorders; chronic respiratory disease; and cancer, the major risk factors for which are tobacco, overweight, physical inactivity and alcohol (Aboriginal Health Report Card).
The MLHD should continue to work in partnership with the Aboriginal population to improve lifestyles with focus on diet, exercise, tobacco use, and alcohol consumption. In addition the health service should work towards providing culturally appropriate health care services which enable early detection and treatment of conditions to avoid disease progression and hospitalisation and sustain the Aboriginal Maternal Infant Health Service (AMIHS) where partnership between the
15 | P a g e
Public Health Unit – MLHD (document.docx)
AHEO/Midwife is a crucial factor in the provision of culturally appropriate care. The health service needs to ensure that Aboriginal people are correctly identified in data collection systems to improve the quality of our health data and accuracy of health indicator reporting.
MORE INFORMATION
Health Statistics NSW, online www.healthstats.nsw.gov.au Reports complied from Health Statistics NSW for Aboriginal populations available from:
www.gsahs.nsw.gov.au/gsho/refreplink.htmlo Health Statistics reports Burden of disease (deaths and hospitalisations)o Health Statistics reports Maternal and child healtho Health Statistics reports Health Conditions and risk behaviours
2006-2009 Report on Adult Aboriginal Health from the NSW Health Survey (former Area Health Service data) www.health.nsw.gov.au/publichealth/surveys/hsa/0609ab/index.asp
Aboriginal Health in NSW www.health.nsw.gov.au/publichealth/aboriginal/index.asp Aboriginal Health Report Card www.healthstats.nsw.gov.au/ContentText/Display/ReportCards
16 | P a g e
Public Health Unit – MLHD (document.docx)
Related Documents



![[RNIB Report format template] of... · Web viewChronic obstructive pulmonary disease or COPD is the name for a group of lung conditions that cause breathing difficulties. It includes:](https://static.cupdf.com/doc/110x72/5b20b67a7f8b9a2e378b56ee/rnib-report-format-template-of-web-viewchronic-obstructive-pulmonary-disease.jpg)







