Evidence-based guidelines for the management of abnormally invasive placenta recommendations from the International Society for Abnormally Invasive Placenta Sally L. Collins, MD, PhD; Bahrin Alemdar, MD; Heleen J. van Beekhuizen, MD; Charline Bertholdt, MD; Thorsten Braun, MD; Pavel Calda, MD; Pierre Delorme, MD; Johannes J. Duvekot, MD; Lene Gronbeck, MD; Gilles Kayem, MD; Jens Langhoff-Roos, MD; Louis Marcellin, MD; Pasquale Martinelli, MD; Olivier Morel, MD; Mina Mhallem, MD; Maddalena Morlando, MD; Lone N. Noergaard, MD; Andreas Nonnenmacher, MD; Petra Pateisky, MD; Philippe Petit, MD; Marcus J. Rijken, MD; Mariola Ropacka-Lesiak, MD; Dietmar Schlembach, MD; Loı ¨c Sentilhes, MD; Vedran Stefanovic, MD; Gita Strindfors, MD; Boris Tutschek, MD; Siri Vangen, MD; Alexander Weichert, MD; Katharina Weizsa ¨cker, MD; Frederic Chantraine, MD; on behalf of the International Society for Abnormally Invasive Placenta (IS-AIP) Click Supplemental Materials under article title in Contents at From the Nuffield Department of Women’s and Reproductive Health (Dr Collins), University of Oxford, Oxford, UK; The Fetal Medicine Unit (Dr Collins), John Radcliffe Hospital, Oxford, UK; Department of Obstetrics and Gynecology (Drs Alemdar and Strindfors), South General Hospital, Stockholm, Sweden; Department of Gynaecological Oncology (Dr van Beekhuizen), Erasmus Medical Center, Rotterdam, Netherlands; Centre Hospitalier Régional Universitaire de Nancy (Drs Bertholdt and Morel), Université de Lorraine, France; Departments of Obstetrics and Division of Experimental Obstetrics (Drs Braun, Nonnenmacher, Weichert, and Weizsäcker), Charité Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Campus Virchow-Klinikum and Campus Charité Mitte, Berlin, Germany; Department of Obstetrics and Gynecology (Dr Calda), General Faculty Hospital, Charles University, Prague, Czech Republic; Port-Royal Maternity Unit (Dr Delorme), Cochin Hospital, Paris-Descartes University, DHU Risk and Pregnancy, Assistance Publique-Hôpitaux de Paris, Paris, France; Department of Obstetrics and Gynecology (Dr Duvekot), Erasmus Medical Center Rotterdam, Rotterdam, Netherlands; Department of Obstetrics (Drs Gronbeck, Langhoff-Roos and Noergaard), Rigshospitalet, University of Copenhagen, Denmark; Department of Obstetrics and Gynecology (Dr Kayem), Hôpital Trousseau, Assistance Publique des Hôpitaux de Paris, Sorbonne University, Paris , France; Department of Gynecology Obstetrics II and Reproductive Medicine (Dr Marcellin), Hôpitaux Universitaires Paris Centre, Hôpital Cochin, APHP; Sorbonne Paris Cité, Université Paris Descartes, Faculté de Médecine, Paris, France; Department of Neuroscience (Drs Martinelli and Morlando), Reproductive Sciences and Dentistry, University of Naples Federico II, Naples, Italy; Department of Obstetrics (Dr Mhallem), Cliniques Universitaires Saint-Luc, Brussels, Belgium; Department of Women, Children and of General and Specialized Surgery (Dr Morlando), University “Luigi Vanvitelli”, Naples, Italy; Department of Obstetrics and Gynecology (Dr Pateisky), Division of Obstetrics and Feto-Maternal Medicine, Medical University of Vienna, Vienna, Austria; Department of Obstetrics and Gynecology (Drs Petit and Chantraine), CHR Citadelle, University of Liege, Liege, Belgium; Vrouw & Baby (Dr Rijken), University Medical Centre Utrecht, Utrecht University, Utrecht, Netherlands; Department of Perinatology and Gynecology (Dr Ropacka-Lesiak), University of Medical Sciences, Poznan, Poland; Vivantes Network for Health (Schlembach), Clinicum Neukoelln, Clinic for Obstetric Medicine, Berlin, Germany; Department of Obstetrics and Gynecology (Dr Sentilhes), Hôpital Pellegrin, CHU de Bordeaux, Bordeaux, France; Department of Obstetrics and Gynecology (Dr Stefanovic), Fetomaternal Medical Center, Helsinki University Hospital and University of Helsinki, Finland; Prenatal Zurich (Dr Tutschek), Zürich, Switzerland, and Heinrich Heine University, Düsseldorf, Germany; Division of Obstetrics and Gynaecology (Dr Vangen), Norwegian National Advisory Unit on Women’s Health, Oslo University Hospital, Rikshospitalet and Institute of Clinical Medicine, University of Oslo, Oslo, Norway. Received Nov. 29, 2018; revised Feb. 13, 2019; accepted Feb. 27, 2019. The authors report no conflict of interest. Corresponding author: Sally L. Collins, MD, PhD. [email protected] 0002-9378/$36.00 ª 2019 Elsevier Inc. All rights reserved. https://doi.org/10.1016/j.ajog.2019.02.054 The worldwide incidence of abnormally invasive placenta is rapidly rising, following the trend of increasing cesarean delivery. It is a heterogeneous condition and has a high maternal morbidity and mortality rate, presenting specific intrapartum challenges. Its rarity makes developing individual expertise difficult for the majority of clinicians. The International Society for Abnormally Invasive Placenta aims to improve clinicians’ understanding and skills in managing this difficult condition. By pooling knowledge, experience, and expertise gained within a variety of different healthcare systems, the Society seeks to improve the outcomes for women with abnormally invasive placenta globally. The recommendations presented herewith were reached using a modified Delphi technique and are based on the best available evidence. The evidence base for each is presented using a formal grading system. The topics chosen address the most pertinent questions regarding intrapartum management of abnormally invasive placenta with respect to clinically relevant outcomes, including the following: definition of a center of excellence; requirement for antenatal hospitalization; antenatal optimization of hemoglobin; gestational age for delivery; antenatal corticosteroid administration; use of preoperative cystoscopy, ureteric stents, and prophylactic pelvic arterial balloon catheters; maternal position for surgery; type of skin incision; position of the uterine incision; use of interoperative ultrasound; prophylactic administration of oxytocin; optimal method for intraoperative diagnosis; use of expectant management; adjuvant therapies for expectant management; use of local surgical resection; type of hysterectomy; use of delayed hysterectomy; intraoperative measures to treat life-threatening hemorrhage; and fertility after conservative management. Key words: abnormally invasive placenta, accreta, guideline, increta, morbidly adherent placenta, percreta, placenta, placenta accreta spectrum MONTH 2019 American Journal of Obstetrics & Gynecology 1 Special Report ajog.org

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Special Report ajog.org
Evidence-based guidelines for the managementof abnormally invasive placenta recommendationsfrom the International Society for AbnormallyInvasive Placenta
Sally L. Collins, MD, PhD; Bahrin Alemdar, MD; Heleen J. van Beekhuizen, MD; Charline Bertholdt, MD; Thorsten Braun, MD;PavelCalda,MD; PierreDelorme,MD; Johannes J.Duvekot,MD; LeneGronbeck,MD;GillesKayem,MD; JensLanghoff-Roos,MD;Louis Marcellin, MD; Pasquale Martinelli, MD; Olivier Morel, MD; Mina Mhallem, MD; Maddalena Morlando, MD;Lone N. Noergaard, MD; Andreas Nonnenmacher, MD; Petra Pateisky, MD; Philippe Petit, MD; Marcus J. Rijken, MD;Mariola Ropacka-Lesiak, MD; Dietmar Schlembach, MD; Loıc Sentilhes, MD; Vedran Stefanovic, MD; Gita Strindfors, MD;Boris Tutschek,MD; Siri Vangen,MD;AlexanderWeichert,MD; KatharinaWeizsacker,MD; Frederic Chantraine,MD; on behalf ofthe International Society for Abnormally Invasive Placenta (IS-AIP)Click Supplemental Materials under article title in Contents at
From the Nuffield Department of Women’s and Reproductive Health (Dr Collins), University of Oxford, Oxford, UK; The Fetal Medicine Unit (Dr Collins), John RadcliffeHospital, Oxford, UK; Department of Obstetrics and Gynecology (Drs Alemdar and Strindfors), South General Hospital, Stockholm, Sweden; Department ofGynaecologicalOncology (Dr vanBeekhuizen), ErasmusMedicalCenter,Rotterdam,Netherlands;CentreHospitalierRégionalUniversitairedeNancy (DrsBertholdtandMorel), Université de Lorraine, France; Departments of Obstetrics and Division of Experimental Obstetrics (Drs Braun, Nonnenmacher, Weichert, and Weizsäcker),CharitéUniversitätsmedizinBerlin, corporatemember of FreieUniversität Berlin, Humboldt-Universität zuBerlin, andBerlin Institute ofHealth,CampusVirchow-Klinikumand Campus Charité Mitte, Berlin, Germany; Department of Obstetrics and Gynecology (Dr Calda), General Faculty Hospital, Charles University, Prague, CzechRepublic; Port-RoyalMaternity Unit (Dr Delorme),CochinHospital, Paris-Descartes University, DHURisk andPregnancy, Assistance Publique-Hôpitaux de Paris, Paris,France; Department of Obstetrics and Gynecology (Dr Duvekot), Erasmus Medical Center Rotterdam, Rotterdam, Netherlands; Department of Obstetrics (DrsGronbeck, Langhoff-Roos and Noergaard), Rigshospitalet, University of Copenhagen, Denmark; Department of Obstetrics and Gynecology (Dr Kayem), HôpitalTrousseau, Assistance Publique des Hôpitaux de Paris, Sorbonne University, Paris , France; Department of Gynecology Obstetrics II and Reproductive Medicine (DrMarcellin),HôpitauxUniversitairesParisCentre,HôpitalCochin, APHP;SorbonneParisCité,UniversitéParisDescartes,FacultédeMédecine,Paris, France;Departmentof Neuroscience (Drs Martinelli and Morlando), Reproductive Sciences and Dentistry, University of Naples Federico II, Naples, Italy; Department of Obstetrics (DrMhallem),CliniquesUniversitairesSaint-Luc,Brussels,Belgium;Department ofWomen,ChildrenandofGeneral andSpecializedSurgery (DrMorlando),University “LuigiVanvitelli”, Naples, Italy;Department ofObstetrics andGynecology (DrPateisky),DivisionofObstetrics andFeto-MaternalMedicine,MedicalUniversity ofVienna,Vienna,Austria; Department of Obstetrics and Gynecology (Drs Petit and Chantraine), CHR Citadelle, University of Liege, Liege, Belgium; Vrouw & Baby (Dr Rijken), UniversityMedical Centre Utrecht, Utrecht University, Utrecht, Netherlands; Department of Perinatology and Gynecology (Dr Ropacka-Lesiak), University of Medical Sciences,Poznan, Poland; Vivantes Network for Health (Schlembach), Clinicum Neukoelln, Clinic for Obstetric Medicine, Berlin, Germany; Department of Obstetrics andGynecology (Dr Sentilhes), Hôpital Pellegrin, CHU de Bordeaux, Bordeaux, France; Department of Obstetrics and Gynecology (Dr Stefanovic), Fetomaternal MedicalCenter, Helsinki University Hospital and University of Helsinki, Finland; Prenatal Zurich (Dr Tutschek), Zürich, Switzerland, and Heinrich Heine University, Düsseldorf,Germany; Division of Obstetrics and Gynaecology (Dr Vangen), Norwegian National Advisory Unit on Women’s Health, Oslo University Hospital, Rikshospitalet andInstitute of Clinical Medicine, University of Oslo, Oslo, Norway.
Received Nov. 29, 2018; revised Feb. 13, 2019; accepted Feb. 27, 2019.
The authors report no conflict of interest.
Corresponding author: Sally L. Collins, MD, PhD. [email protected]
0002-9378/$36.00 � ª 2019 Elsevier Inc. All rights reserved. � https://doi.org/10.1016/j.ajog.2019.02.054
The worldwide incidence of abnormally invasive placenta is rapidly rising, following the trend of increasing cesarean delivery. It is a heterogeneous
condition and has a high maternal morbidity and mortality rate, presenting specific intrapartum challenges. Its rarity makes developing individual
expertise difficult for the majority of clinicians. The International Society for Abnormally Invasive Placenta aims to improve clinicians’ understanding
and skills in managing this difficult condition. By pooling knowledge, experience, and expertise gained within a variety of different healthcare
systems, the Society seeks to improve the outcomes for women with abnormally invasive placenta globally.
The recommendations presented herewith were reached using a modified Delphi technique and are based on the best available evidence. The
evidence base for each is presented using a formal grading system. The topics chosen address the most pertinent questions regarding intrapartum
management of abnormally invasive placenta with respect to clinically relevant outcomes, including the following: definition of a center of excellence;
requirement for antenatal hospitalization; antenatal optimization of hemoglobin; gestational age for delivery; antenatal corticosteroid administration;
use of preoperative cystoscopy, ureteric stents, and prophylactic pelvic arterial balloon catheters; maternal position for surgery; type of skin incision;
position of the uterine incision; use of interoperative ultrasound; prophylactic administration of oxytocin; optimal method for intraoperative diagnosis;
use of expectant management; adjuvant therapies for expectant management; use of local surgical resection; type of hysterectomy; use of delayed
hysterectomy; intraoperative measures to treat life-threatening hemorrhage; and fertility after conservative management.
Key words: abnormally invasive placenta, accreta, guideline, increta, morbidly adherent placenta, percreta, placenta, placenta accreta spectrum
MONTH 2019 American Journal of Obstetrics & Gynecology 1

Special Report ajog.org
IntroductionAbnormally invasive placenta (AIP), alsocalled placenta accreta spectrum disor-der (PAS), describes the clinical situationin which a placenta does not separatespontaneously at delivery and cannot beremoved without causing abnormal andpotentially life-threatening bleeding.1,2
There is increasing epidemiological evi-dence demonstrating that the incidenceof AIP is rising worldwide.3 This is mostlikely due to the rising rates of cesareandelivery, which is the greatest single riskfactor for AIP in subsequent pregnan-cies. Optimal management requires bothaccurate antenatal diagnosis and a robustperinatal management strategy. Howev-er, even with the rising incidence, AIP isstill rare (0.79e3.11 per 1000 births afterprior cesarean),4 and so defining anoptimal management strategy remainsextremely challenging. The literaturecontains a vast number of case reports,case series, and retrospective cohortstudies looking at multiple managementstrategies; however, most studies aresmall, and many are methodologicallyflawed, limiting their utility. The situa-tion is made even more difficult by thespectrum of presentations being pre-sented in most studies as a binaryoutcome (“AIP” or “not AIP”), withvarying diagnostic criteria and noattempted assessment of severity.2
The International Society for Abnor-mally Invasive Placenta (IS-AIP) (www.is-aip.org) evolved from the EuropeanWorking group on AIP (EW-AIP) andcurrently consists of 42 clinicians andbasic science researchers from 13 coun-tries. At the 11th meeting of EW-AIP inNaples (2017), the IS-AIP constitutionwas formally agreed upon and theboard elected. It was registered inBelgium on 12 October 2107 as anon�profit-making association. The So-ciety has strict membership criteria and afull constitution (see www.is-aip.org).
The aim of the IS-AIP is to promoteexcellence in all aspects of healthcarerelating to AIP, including research(clinical, epidemiological, and “wet lab”based), clinical diagnosis and manage-ment, education (including raisingawareness within the general populationand among healthcare providers,
2 American Journal of Obstetrics & Gynecology M
especially with a view to prevention).The group as the EW-AIP has alreadypublished standardized descriptors toaid in the ultrasound diagnosis of AIP.5
This paper aims to generate anevidence-based recommendation for theintrapartum management of AIP usingthe unique, international composition ofthe IS-AIP to provide expert consensusrecommendation where the evidenceidentified is weak, flawed, or absent.
MethodsThe questions to be answered in thisguideline were selected by a modifiedDelphi technique. The IS-AIP member-ship were all invited to suggest issues thatthey believed were pertinent to themanagement of AIP. These questionswere then discussed in detail at an IS-AIPmeeting in Prague (October 2016), withthe final decision on inclusion beingtaken by a vote. All 21 questionsaddressed in this paper were unanimousagreed to be important by the IS-AIPmembership.The search and assessment of the
published evidence was then undertakenby an individual IS-AIP member ac-cording to a predefined pro forma(Supplementary Material). In brief, thisinvolved undertaking a full “systematicreview” process for each topic, includingformulating an appropriate questionspecific to AIP using the PICO frame-work6 and searching all relevant medicaldatabases (PubMed, EMBASE,CINAHL, Cochrane Database, etc) and,where appropriate, some nonmedicaldatabases (eg, Google). All searches forthe 21 different topics were undertakenat various points during 2017. Full-textversions of all potential papers werethen obtained, assessed for relevance,and critically appraised using the levelsof evidence provided by the Centre forEvidence Based Medicine.7
All the completed pro formas detail-ing the formulated question, searchstrategy, results, and critical analysis foreach topic were then sent to the entiremembership for consideration of thesearch strategy used and the resultingliterature retrieved. Where potentialmethodological issues were identified byanother member (eg, problems with
ONTH 2019
search terms, usually relating to languagedifferences; eg, searching only “ureteral”not “ureteric OR ureteral”), a second IS-AIP member repeated the search toensure that no evidence had beenmissed. A few topics that revealed littlehigh-quality evidence during the orig-inal 2017 search were searched again in2018 to ensure that no further evidencehad been published.
Once all the evidence had been iden-tified, the recommendations werereached by a modified Delphi techniqueinvolving the entire membership ofthe IS-AIP. Each topic was discussedface-to-face by themembership, either atan IS-AIP meeting or using Webconferencing. A frank and open discus-sion concerning the available evidenceensured that, to the best of our ability,any personal bias regarding the evidencewas removed and a fair interpretation ofthe data was recorded. Where possible, arecommendation was then drawn upfrom the evidence, taking into accountthe quality (level) of each piece of evi-dence. Where high quality evidence wasscarce and level 5 “expert opinion”required, each topic was then discusseduntil a tentative consensus recommen-dation was reached. Each recommenda-tion was then voted on and ratified onlyif it received support from the group. Oncompletion of the process, all of therecommendations were then circulatedto the entire membership once again toensure that unanimous ratification of allrecommendations remained.
Results1. What constitutes “expertise” in
management of AIP and/or definesa “center of excellence”?
Evidence for what constitutes an“expert” in the management of AIPis missing from the literature, despiteopening the search strategy to non-medical databases such as Google.Therefore, the IS-AIP recommendationis based on a consensus opinion (level 5evidence) and is:
An expert is a person with significantexperience in AIP and a high level ofknowledge and/or skills relating to thecondition (Grade D recommendation).
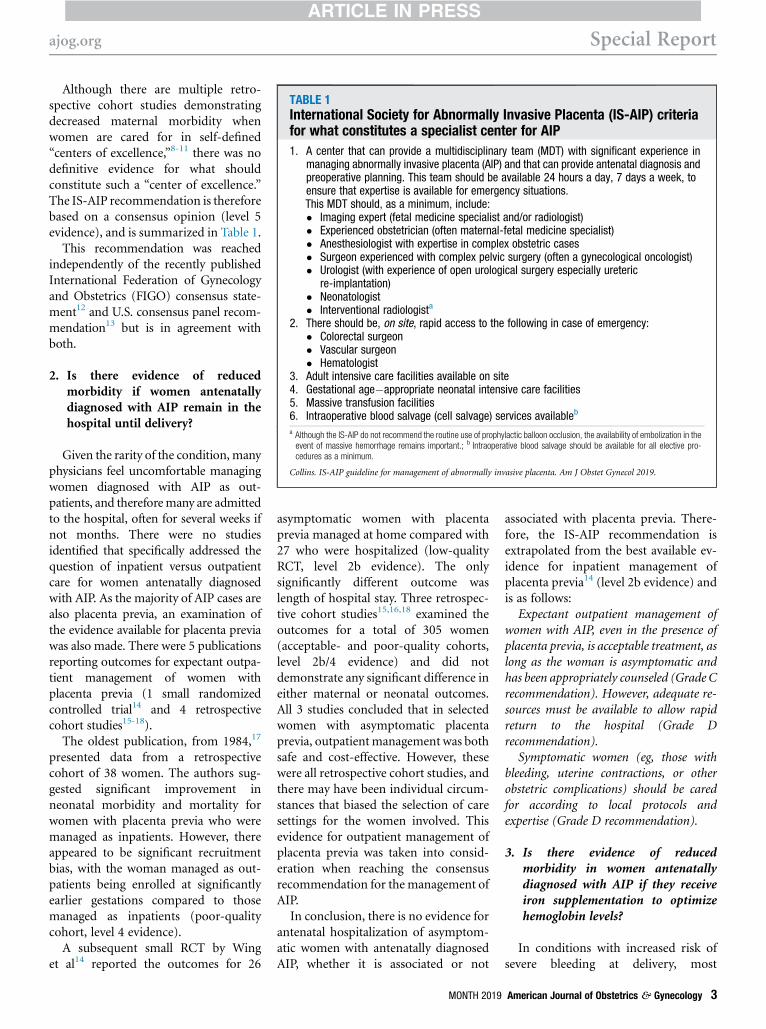
TABLE 1International Society for Abnormally Invasive Placenta (IS-AIP) criteriafor what constitutes a specialist center for AIP
1. A center that can provide a multidisciplinary team (MDT) with significant experience inmanaging abnormally invasive placenta (AIP) and that can provide antenatal diagnosis andpreoperative planning. This team should be available 24 hours a day, 7 days a week, toensure that expertise is available for emergency situations.This MDT should, as a minimum, include:� Imaging expert (fetal medicine specialist and/or radiologist)� Experienced obstetrician (often maternal-fetal medicine specialist)� Anesthesiologist with expertise in complex obstetric cases� Surgeon experienced with complex pelvic surgery (often a gynecological oncologist)� Urologist (with experience of open urological surgery especially ureteric
re-implantation)� Neonatologist� Interventional radiologista
2. There should be, on site, rapid access to the following in case of emergency:� Colorectal surgeon� Vascular surgeon� Hematologist
3. Adult intensive care facilities available on site4. Gestational age�appropriate neonatal intensive care facilities5. Massive transfusion facilities6. Intraoperative blood salvage (cell salvage) services availableb
a Although the IS-AIP do not recommend the routine use of prophylactic balloon occlusion, the availability of embolization in theevent of massive hemorrhage remains important.; b Intraoperative blood salvage should be available for all elective pro-cedures as a minimum.
Collins. IS-AIP guideline for management of abnormally invasive placenta. Am J Obstet Gynecol 2019.
ajog.org Special Report
Although there are multiple retro-spective cohort studies demonstratingdecreased maternal morbidity whenwomen are cared for in self-defined“centers of excellence,”8-11 there was nodefinitive evidence for what shouldconstitute such a “center of excellence.”The IS-AIP recommendation is thereforebased on a consensus opinion (level 5evidence), and is summarized in Table 1.
This recommendation was reachedindependently of the recently publishedInternational Federation of Gynecologyand Obstetrics (FIGO) consensus state-ment12 and U.S. consensus panel recom-mendation13 but is in agreement withboth.
2. Is there evidence of reducedmorbidity if women antenatallydiagnosed with AIP remain in thehospital until delivery?
Given the rarity of the condition, manyphysicians feel uncomfortable managingwomen diagnosed with AIP as out-patients, and thereforemany are admittedto the hospital, often for several weeks ifnot months. There were no studiesidentified that specifically addressed thequestion of inpatient versus outpatientcare for women antenatally diagnosedwith AIP. As the majority of AIP cases arealso placenta previa, an examination ofthe evidence available for placenta previawas also made. There were 5 publicationsreporting outcomes for expectant outpa-tient management of women withplacenta previa (1 small randomizedcontrolled trial14 and 4 retrospectivecohort studies15-18).
The oldest publication, from 1984,17
presented data from a retrospectivecohort of 38 women. The authors sug-gested significant improvement inneonatal morbidity and mortality forwomen with placenta previa who weremanaged as inpatients. However, thereappeared to be significant recruitmentbias, with the woman managed as out-patients being enrolled at significantlyearlier gestations compared to thosemanaged as inpatients (poor-qualitycohort, level 4 evidence).
A subsequent small RCT by Winget al14 reported the outcomes for 26
asymptomatic women with placentaprevia managed at home compared with27 who were hospitalized (low-qualityRCT, level 2b evidence). The onlysignificantly different outcome waslength of hospital stay. Three retrospec-tive cohort studies15,16,18 examined theoutcomes for a total of 305 women(acceptable- and poor-quality cohorts,level 2b/4 evidence) and did notdemonstrate any significant difference ineither maternal or neonatal outcomes.All 3 studies concluded that in selectedwomen with asymptomatic placentaprevia, outpatientmanagement was bothsafe and cost-effective. However, thesewere all retrospective cohort studies, andthere may have been individual circum-stances that biased the selection of caresettings for the women involved. Thisevidence for outpatient management ofplacenta previa was taken into consid-eration when reaching the consensusrecommendation for themanagement ofAIP.In conclusion, there is no evidence for
antenatal hospitalization of asymptom-atic women with antenatally diagnosedAIP, whether it is associated or not
MONTH 2019
associated with placenta previa. There-fore, the IS-AIP recommendation isextrapolated from the best available ev-idence for inpatient management ofplacenta previa14 (level 2b evidence) andis as follows:
Expectant outpatient management ofwomen with AIP, even in the presence ofplacenta previa, is acceptable treatment, aslong as the woman is asymptomatic andhas been appropriately counseled (Grade Crecommendation). However, adequate re-sources must be available to allow rapidreturn to the hospital (Grade Drecommendation).
Symptomatic women (eg, those withbleeding, uterine contractions, or otherobstetric complications) should be caredfor according to local protocols andexpertise (Grade D recommendation).
3. Is there evidence of reducedmorbidity in women antenatallydiagnosed with AIP if they receiveiron supplementation to optimizehemoglobin levels?
In conditions with increased risk ofsevere bleeding at delivery, most
American Journal of Obstetrics & Gynecology 3

Special Report ajog.org
physicians will take steps antenatally toensure that the woman’s starting hemo-globin (Hb) level is as high as possible inan attempt to reduce morbidity. Therewas no evidence available for the benefitof antenatal optimization of Hb specif-ically for cases of AIP. A single study wasidentified that looked to identify de-terminants of blood loss at childbirth.This was a “nested cohort study” theparticipants for which had already beenrecruited to a community-based RCToftreatments for severe anemia in womenfrom Zanzibar. This reported thatwomen with Hb of <90 g/L at deliverywere at increased risk for blood loss,both at the time of birth and in the im-mediate postpartum period, irrespectiveof mode of delivery19 (level 1b evidence).This study was taken into consideration,but it does not answer the originalquestion posed; therefore, the IS-AIPrecommendation is based on aconsensus opinion (level 5 evidence) andis:
As soon as women are antenatallydiagnosed with AIP, they should have theirHb level measured. If it is low (<110 g/L[11 g/dL] before 28 weeks’ gestation or<105 g/L [10.5 g/dL] after 28 weeks’gestation), appropriate hematinic in-vestigations should be undertaken and ifindicated, iron supplementation (oral orintravenous) should be given to optimizetheir Hb level before surgery (Grade Drecommendation).
This recommendation was reachedindependently but is in agreement withthe UK Royal College of Obstetriciansand Gynaecologists (RCOG) preventionand management of postpartum hem-orrhage guideline (Green-top Guidelinenumber 52)20 and the recent FIGOconsensus statement.12
4. At what gestation should womenwith antenatally diagnosed AIP bedelivered?
Arranging an elective cesarean de-livery earlier than usual may reduce therisk of an emergency delivery; however,the increased risks to the neonate fromprematurity must also be considered. Sixstudies were found that reportedmaternal and neonatal outcomes for
4 American Journal of Obstetrics & Gynecology M
different gestational ages at delivery inwomen with an antenatal diagnosis ofAIP.9,21-25 All 6 were retrospectiveobservational studies (level 4 evidence).None of the studies provided any robustevidence for the optimal gestational agefor delivery for woman with AIP, toreduce maternal and neonatal morbiditywhile still minimizing the rate of un-planned, emergency delivery.Robinson and Grobman26 published a
decision analysis in 2010 recommendingthat the optimal timing of delivery forwomen with placenta previa andultrasound-based suspicion of AIP was34 weeks. Their aim was to define thegestation that balanced the risks of pre-maturity with the risk of emergency de-livery. The flaw in their elegant model isthat the risk of bleeding used to formu-late the 9 models was based on 400women with placenta previa only andnot previa with AIP.Therefore, although all these studies
were taken into consideration, the IS-AIPrecommendation is based on a consensusopinion (level 5 evidence) and is:The timing of delivery should be tailored
to each unique set of circumstances andbased on the individual woman’s risk ofemergent delivery. To reduce the risk ofneonatal morbidity, it is reasonable tocontinue expectant management until af-ter 36þ0 weeks’ gestation for women withno previous history of preterm delivery(<36þ0 weeks’) and who are stable withno vaginal bleeding, preterm prematurerupture of the membranes (PPROM), oruterine contractions suggestive of pretermlabor (Grade D recommendation).In the case of women with history of
previous preterm birth, multiple episodesof small amounts of vaginal bleeding, asingle episode of a significant amount ofvaginal bleeding or PPROM, planned de-livery at around 34þ0 weeks’ gestationshould be considered given the increasedrisk of emergent delivery (Grade Drecommendation).
5. Is there evidence of reducedmortality ormorbidity in neonates ifwomen with antenatally diagnosedAIP receive corticosteroids fordelivery occurring after 34D0weeks’ gestation?
ONTH 2019
The issue of administration of corti-costeroids for preterm delivery after34þ0 weeks’ gestation is contentious. Itis unclear whether AIP itself makes theneonate more likely to experience res-piratory distress. No prospective RCTexists evaluating the influence of AIP perse on neonatal respiratory morbiditybeside the normal influence of prema-turity when delivered between 34þ0 and37þ0 weeks’ gestation. One retrospec-tive case series (level 4 evidence) ofhistopathologically diagnosed AIPcompared the neonatal outcomes be-tween antenatally diagnosed AIP andAIP cases diagnosed intrapartum.25
Although there was no significant dif-ference between the gestation at delivery(33.9 vs 34.7 weeks; P ¼ .34) for the 2groups, those women who were antena-tally diagnosed were more likely to havereceived antenatal steroids (65% vs 16%;P< .001), yet still demonstrated a higherrate of admission to the neonatal inten-sive care unit (86% vs 60%; P ¼ .005)and longer neonatal hospital stays (11 vs7 days; P ¼ .006). Interpretation of thisdataset is difficult with regard to thespecific question, as there are likely to beconsiderable confounding factors.
There was no evidence available thatthe presence of AIP itself increasesneonatal respiratory morbidity or mor-tality if the scheduled delivery takes placebetween 34þ0 and 37þ0 weeks’ gesta-tion. Therefore, the IS-AIP recommen-dation for antenatal glucocorticoidtreatment to induce fetal lung matura-tion for a scheduled delivery after 34þ0weeks’ gestation is based on consensusopinion (level 5 evidence) and is asfollows:
An individualized approach for ante-natal steroid administration should beemployed, based on the current localguidelines for the specific gestation atdelivery, irrespective of the suspicionor diagnosis of AIP (Grade Drecommendation).
6. Does routine preoperativecystoscopy improve the accuracy ofantenatal diagnosis of AIP and/orreduce maternal morbidity inwomen with antenatally diagnosedAIP?

ajog.org Special Report
Preoperative cystoscopy to assess forbladder wall involvement is recom-mended bymany operators; others arguethat it adds no useful information whileincreasing the time in the operatingroom and the risks of infection andlower urinary tract trauma. No RCTswere found examining the efficacy ofpreoperative cystoscopy for the intra-partum management of AIP. One caseseries presented 12 patients with AIP andgross hematuria (level 4 evidence) whounderwent preoperative cystoscopy.27
The authors reported that the proced-ure did not help to establish a preoper-ative diagnosis in any patient, andconcluded that cystoscopy had minimaldiagnostic value.
The evidence that cystoscopic find-ings, even in the presence of gross he-maturia, do not correlate to the level ofbladder involvement was taken into ac-count; however, given the poor quality ofthe study, the recommendation is sup-ported by consensus opinion (level 5evidence).
The IS-AIP does not recommend un-dertaking routine preoperative cystoscopy.If preoperative cystoscopy is performed forinsertion of ureteric stents, the appearanceof the bladder should not change the (im-aging-based) plan of management (GradeD recommendation).
7. Does routine ureteric stentplacement reduce maternalmorbidity in cases of antenatallydiagnosed AIP?
Ureteric stents may aid identificationof the ureter and prevent inadvertenttransection or ligation at hysterectomy;however, insertion has its own risks,such as urinary tract perforation andinfection. One retrospective cohortstudy28 (level 2b evidence) of 57 cases ofsuspected AIP and 19 undiagnosed casesreported on ureteric stenting and unin-tentional urinary tract injury. Uretericstenting was attempted in 25 of the sus-pected cases. The stent placement wasachieved bilaterally in 17 of 25 cases(68%), on only 1 side in 4 of 25 cases(16%), and on neither side in 4 of 25cases (16%). Women with bilateral ure-teral stents had a lower incidence of early
morbidity compared with womenwithout stents (3/17 [18%] vs 22/40[55%], P ¼ .018). A nonsignificantreduction in ureteric injury wasobserved (0% vs 7%).A systematic review of 49 case series
and case reports (level 3a evidence),including the above cohort study,attempted to examine the efficacy ofapproaches aimed at minimizing urinarytract injuries in AIP.29 Of the 292 womenwith AIP, whether or not ureteric stentswere successfully placed was reported for90 cases only. No details were availableon the number in whom stent placementwas attempted but unsuccessful. The riskof urinary tract injury was significantlylower in the group with ureteric stents insitu (2/35 [6%]) compared to those whowere known not to have stents (18/55[33%]; P ¼ .01).Neither study provided robust evi-
dence regarding the severity of AIP thatmost benefited from stent placement;therefore the recommendation is alsosupported by consensus opinion (level 5evidence) and is:Placement of ureteric stents may be
beneficial in preventing ureteric injury andearly morbidity (Grade B recommenda-tion). However, given the potential risksassociated with stent placement, the evi-dence is not strong enough to recommendroutine placement of ureteric stents for allsuspected cases of AIP. The benefit fromureteric stents is probably limited to casesof percreta with significant invasion wherehysterectomy is likely to be highly complex(Grade D recommendation).
8. Does routine insertion ofprophylactic balloon cathetersinto the pelvic vasculature reducematernal morbidity in cases ofantenatally diagnosed AIP?
Amainmanagement objective for AIPis reduction of blood loss. Endovascularballoon occlusion of the pelvic circula-tion has been proposed as a method ofachieving this. Given the aberrant bloodsupply often seen in AIP as a result of theextensive neovascularization, however,occluding some of the pelvic vesselsmight exacerbate bleeding from thecollateral circulation. Therefore, the
MONTH 2019
benefits of arterial occlusion may notoutweigh the associated risks of vesselrupture and thromboembolism.
A systematic review has recently beenpublished looking at endovascularinterventional modalities for hemor-rhage control in AIP.30 This includedboth prophylactic arterial balloon oc-clusion of different vessels, including theabdominal aorta, and pelvic vasculatureembolization either alone or together.Only 16 of the 69 included studies werecontrolled, with the remaining beinglow-quality cohort, case series, or casestudies. The heterogeneity of the studieswas reported by the authors to be sig-nificant (review level 2a/3a evidence). Allgrades of AIP (accreta/increta/percreta)were grouped together for the meta-analysis with no differentiation inseverity, with some studies includingonly balloon occlusion and others usingvascular embolization as well. The au-thors concluded that “endovascularintervention is effective in controllinghemorrhage in abnormal placentationdeliveries.”
One small RCT (level 1b evidence)31
was found that had been included inthe systematic review.30 This random-ized 27 women with AIP and showed nodifference in the number of packed redblood cell (RBC) units transfused forwomen who underwent placement ofballoon catheters in the iliac arteriescompared to those who did not, orany other reduction in morbidity.This RCT, however, also reported that15% of the women with balloon cathe-ters experienced an interventionalradiology�related complication.
The IS-AIP considered the findings ofboth these 2 studies. The RCT is a muchsmaller data set, but is more methodo-logically rigorous (level 1b evidence).The systematic review, albeit larger, isvery heterogeneous, includes data of verylow quality, and may be open to signifi-cant bias (level 2a/3a evidence). There-fore, taking into account these 2 studies,the IS-AIP recommendation is as follows:
The effect of prophylactic arterialballoon catheters on bleeding andmorbidity among women with a prenataldiagnosis of AIP has yet to be confirmed.Significant adverse events have been
American Journal of Obstetrics & Gynecology 5

Special Report ajog.org
reported from this procedure. Larger, pro-spective, appropriately controlled studies areneeded to demonstrate both the safety andefficacy of prophylactic balloon occlusion.Given this, the IS-AIP cannot recommendroutine use of prophylactic pelvic arterialballoon catheters for all cases of suspectedAIP (Grade B recommendation).
This recommendation was reachedindependently of the recently publishedFIGO consensus statement12 but is inagreement with it.
9. Is there an optimal maternalposition for surgical delivery ofwomen with antenatally diagnosedAIP?
Some operators suggest that womenshould beplaced in the lithotomy positionto aid assessment of vaginal blood loss andto facilitate manipulation of the cervixduring hysterectomy.However, prolongedperiods of time in stirrups may lead tocompartment syndrome and obstetricneuropraxia. There are no publicationsthat specifically address the question ofmaternal position for surgery for womenwith AIP. Therefore, the IS-AIP recom-mendation is based on consensus opinion(level 5 evidence) and is:
When hysterectomy is either planned orlikely, the woman should be placed in aposition in which the vagina is accessible(such as lithotomy or legs straight on theoperating table but parted) to facilitatemanipulation of the cervix, if required toassist the hysterectomy. This will also alloweasier assessment of any blood lost vagi-nally (Grade D recommendation).
10. Does routine use of verticalmidline incision instead of atransverse incision reducematernal morbidity in cases ofantenatally diagnosed AIP?
Many operators advise routine use of avertical skin incision to facilitate access tothe fundus and pelvic walls. However, atransverse incision may heal faster andreduce the risk of incisional hernia, aswell as being more cosmetically pleasingfor the woman. No studies were foundcomparing either maternal or fetal out-comes for different skin incisions. In the
6 American Journal of Obstetrics & Gynecology M
few publications thatmention the type ofskin incision, a vertical midline incisionappears to be usedmost frequently and isoften anecdotally recommended. Othertransverse incisions, such as PfannenstielandMaylard, have been reported and arerecommended based on both estheticconsiderations and the potential for areduction in postsurgical complications.Given the lack of evidence, the IS-AIPrecommendation is based on consensusopinion (level 5 evidence) and is:There is no evidence of benefit for routine
use of a vertical midline incision for all casesof antenatally diagnosed AIP. The decisionregarding which type of skin incision is usedshould be made by the operating team. Thelocation of the placenta, degree of invasionsuspected, likelihood of intraoperativecomplications, maternal body habitus,gestational age, and preference of the oper-ating surgeon/obstetrician should all betaken into consideration (Grade Drecommendation).
11. Does making a uterine incision inthe upper segment to avoidtransecting the placenta reducematernal morbidity in cases ofantenatally diagnosed AIP?
One of the main surgical strategies inAIP is making the uterine incision awayfrom the placental bed, often in thefundus. However, gaining access to thefundus may require a larger skin inci-sion. One retrospective case series (level4 evidence)32 reported blood loss aftertransverse fundal uterine incision toavoid the placenta in 34 women withplacenta previa, 19 of whom had intra-operatively confirmed AIP. The averageblood loss reported was 1370 g. Therewas no control group, and the severity ofAIP was not reported, yet the authorsconclude that this blood loss “comparesfavorably with the volume lost during aroutine transverse lower segment sectionperformed in patients without placentaprevia or accreta.” It is not possible todraw any firm conclusion from thisstudy; therefore the IS-AIP recommen-dation is based on expert consensus(level 5 evidence) and is as follows:Avoiding placental transection when
making the uterine incision is essential if
ONTH 2019
AIP is clearly evident on opening theabdomen, and is reasonable for womenwith antenatally suspected AIP but withno definite evidence seen at laparotomy,even if it means making an upper segmentor fundal incision, as it is likely to reducematernal blood loss from the placental bed(Grade D recommendation).
12. Does routine intraoperativeultrasound (US) to map theplacental edges before uterineincision reducematernalmorbidityin cases of antenatally diagnosedAIP?
Several reports in the literature anec-dotally recommend the use of intra-operative US, usually with the probedirectly placed on the uterus protected bya sterile cover to enable the upper edge ofthe placenta to be identified. This is oftenmapped out with small, superficialdiathermy marks. There is, however, atheoretical risk of introducing infection.No publications were found that addresseither the risks or benefits of intra-operative US scanning for placentallocalization inwomenwith suspected AIP.One study by Al-Khan et al9 retrospec-tively analyzed patients before and after aninstitutional protocol for AIP manage-ment was introduced. In their protocol,intraoperative US for placental localiza-tion is performed, but the improvementin outcomes cannot be directly attributedto any individual measure. Therefore, theIS-AIP recommendation is based on aconsensus of experts (level 5 evidence)and is as follows:
If the US scan is undertaken in anappropriately sterile manner, the smalltheoretical risk of introducing infection isoutweighed by the benefit of ensuring theincision is made away from the placentalbed. Therefore, intraoperative US of theexposed uterus should be used, wherepossible, to locate the placental edge andassist decision making regarding the uterineincision site (Grade D recommendation).
13. Does routine prophylacticadministration of oxytocin afterdelivery of the infant reducematernal morbidity in cases ofantenatally diagnosed AIP?

ajog.org Special Report
There is evidence for the prophylacticadministration of oxytocin after deliveryat routine cesarean delivery to preventPPH.33 However, the use of routineoxytocin at cesarean delivery in cases ofantenatally suspected AIP has not beenaddressed in any study. Therefore, theIS-AIP recommendation is based on aconsensus of experts (level 5 evidence)and is as follows:
Prophylactic administration of oxytocinimmediately after delivery increasescontraction of the uterus, which could behelpful for the assessment of placentalseparation. If the whole placental bed isabnormally invasive, uterine contractionwill not result in any placental separation.If, however, the placenta is only partiallyadherent or invasive, uterine contractionmay cause some separation, leading toincreased blood loss, which could promptthe surgeon to either forcibly remove therest of the placenta or perform a morehurried hysterectomy. In light of this risk,the IS-AIP recommend that when AIP issuspected antenatally, prophylactic utero-tonic agents should not be routinely givenimmediately after delivery of the infant.Instead a full assessment should be madein accordance with the intraoperativediagnosis recommendations (see nexttopic). Only if the placenta is removed,either fully or partially, or if there isalready significant bleeding, should ute-rotonics be given (Grade Drecommendation).
14. Is there an optimal method forintrapartum clinical diagnosis ofAIP?
Although AIP can be suspected ante-natally, ultimate confirmationoccurs onlywhen the placenta fails to separate afterdelivery of the infant. Attempts to forciblyremove an AIP may lead to catastrophichemorrhage; hence reliable diagnosticsigns are highly desirable. No evidencewas found for which clinical diagnosticmethod best correlates with the gold-standard histopathological diagnosis;therefore, the IS-AIP recommendation isbased on a consensus of experts (level 5evidence) and is as follows:
The IS-AIP agree with the ACOGrecommendation (level 5 evidence) that,
given the high risk of false-positive resultswith all methods of antenatal diagnosis,there must be robust intrapartum evidencethat there is actually significant AIP beforesurgical treatment is commenced. Caremust be taken, however, that major hem-orrhage is not caused by inappropriateattempts to manually remove an AIP. TheIS-AIP recommend the following methodsfor clinically diagnosing AIP:Diagnosis of AIP after vaginal
delivery:The diagnosis of AIP should not be
made if the placenta spontaneously sepa-rates and is delivered by maternal effort,controlled cord traction, or simple manualremoval of an already separated placenta,even if there is a subsequent diagnosis ofretained products of conception (RPOC).For the diagnosis of AIP, a manualremoval of the placenta is required and atthe time of manual exploration of theuterine cavity, in the opinion of a senior,experienced obstetrician, no plane ofcleavage can be identified between theplacenta and the myometrium. This can befor the entire placenta bed or just in “focal”areas. Major hemorrhage after piecemealremoval, removal of a “ragged placenta,”or discovery of subsequent RPOC is notsufficient to make the diagnosis of AIP(Grade D recommendation).For diagnosis of AIP after
laparotomy, a stepwise process shouldbe followed:Step 1: On opening the abdomen, the
external surface of the uterus and the pelvisshould be thoroughly inspected for franksigns of AIP, which include the following:
� Uterus over the placental bed appearsabnormal (can have a bluish/purpleappearance) with obvious distension (a“placental bulge”) (Figure 1).
� Placental tissue is seen to have invadedthrough the surface of the uterus. Thismay or may not have penetrated theserosa (Figure 2).
Note that care should be taken not toconfuse this with a “uterine window,”which is a uterine scar dehiscence with theplacenta visible directly underneath it. If itis a “uterine window,” the surroundinguterine tissue will appear normal(Figure 3).
MONTH 2019
� Excessive, abnormal neo-vascularity isobserved in the lower segment (partic-ularly with vessels running cranio-caudally in the peritoneum) (Figure 4).
If these are clearly seen, AIP can bediagnosed confidently without recourse toany further procedures (Grade Drecommendation).
Step 2: If these are not seen, then theuterine incision should be made accordingto the level of suspicion for AIP (see sepa-rate topic above). If the incision has beenplaced such that the placenta is undis-turbed, then gentle cord traction should beattempted. If traction on the umbilicalcord causes the uterine wall to be visiblypulled inward in the direction of tractionwithout any separation of the placenta(the “dimple” sign) and there is apparentcontraction of the uterus separate from theplacental bed, then AIP can be diagnosed(Grade D recommendation).
Step 3: If AIP has not been diagnosed bythe previous 2 steps, then gentle digitalexploration can be attempted to assesswhether there is a plane of cleavage(following method for diagnosis of AIPdescribed for vaginal delivery). Care mustbe taken to avoid causing hemorrhage(Grade D recommendation).
In an attempt to assess severity, the IS-AIP use the clinical grading score inTable 2. A version of this grading scale isalso recommended by the recently pub-lished FIGO guidelines.34
15. Is expectant management ofclinically confirmed AIP effective,and does it reduce maternalmorbidity when compared tosurgical treatment options?
The “leaving the placenta in situ”approach, or expectant management,consists of leaving the entire placentauntouched and waiting for its completeresorption. Attempting forcible removalof the placenta significantly increasesblood loss, hysterectomy rates, infection,and disseminated intravascular coagula-tion35 (level 2b evidence).
Kutuk et al36 recently published aretrospective cohort study comparingwomen undergoing hysterectomywithout placental removal (n ¼ 20),
American Journal of Obstetrics & Gynecology 7

FIGURE 1Uterus over the placental bed appears abnormal (note the bluish/purpleappearance) with obvious distension of the lower segment (a “placentalbulge”)
Collins. IS-AIP guideline for management of abnormally invasive placenta. Am J Obstet Gynecol 2019.
Special Report ajog.org
expectant management (n¼ 15), andplacental removal with uterus-conserving surgery (n ¼ 11) (level 2bevidence). In 2 cases of percreta, treat-ment was planned to be uterus-conserving surgery, but managementwas changed to expectant when thesurgeons found that the placenta hadinfiltrated the parametrium and thecervix. There was significantly lowerblood loss in the expectantly managed
FIGURE 2Placental tissue seen to have invadedthe serosa
Collins. IS-AIP guideline for management of abnormally invasi
8 American Journal of Obstetrics & Gynecology M
group (400 [250e2500] mL) than inboth the hysterectomy (2000[500e3500] mL; P < .001), and uterus-conserving surgery (3000 [1100e4000]mL; P < .001) groups. None of theexpectantly managed women receivedblood products, compared with trans-fusions of 700 (200e2400) mL packedRBC in the hysterectomy group and1200 (400e1800) mL in the uterus-conserving surgery group. Uterine
through to the surface of the uterus. Th
ve placenta. Am J Obstet Gynecol 2019.
ONTH 2019
preservation rates were not significantlydifferent between the expectantlymanaged women and those havinguterus-conserving surgery (14/15 [93%]vs 33/37 [89%]; P > .99).
Most studies use avoidance of hyster-ectomy as the outcome measure of suc-cessful expectant management. Thesingle largest case series of expectantmanagement published to date is amulticenter retrospective study thatincluded 167 cases of AIP in 40 teachinghospitals (level 2b evidence).37 Theoverall success rate of uterine preserva-tion was 78% (95% CI, 71e84%), withsevere maternal morbidity reported in10 cases (6%). An empty uterus wasobtained spontaneously in 75% of cases,with additional hysteroscopic resectionand/or curettage performed in 25%. Onematernal death occurred as a directresult of methotrexate injection into theumbilical cord. As no hysterectomyspecimens were available for histo-pathogical confirmation, a criticism ofthis study is that some women may notactually have had an AIP. However, anexperienced acoucher should be able todiagnose the vast majority of AIP casesclinically at laparotomy (see point 14),and subsequent histopathological find-ings from cases of “failed” expectantmanagement suggest that the risk ofmisdiagnosis is very low. For this caseseries,37 histopathological examination
is may or may not have penetrated
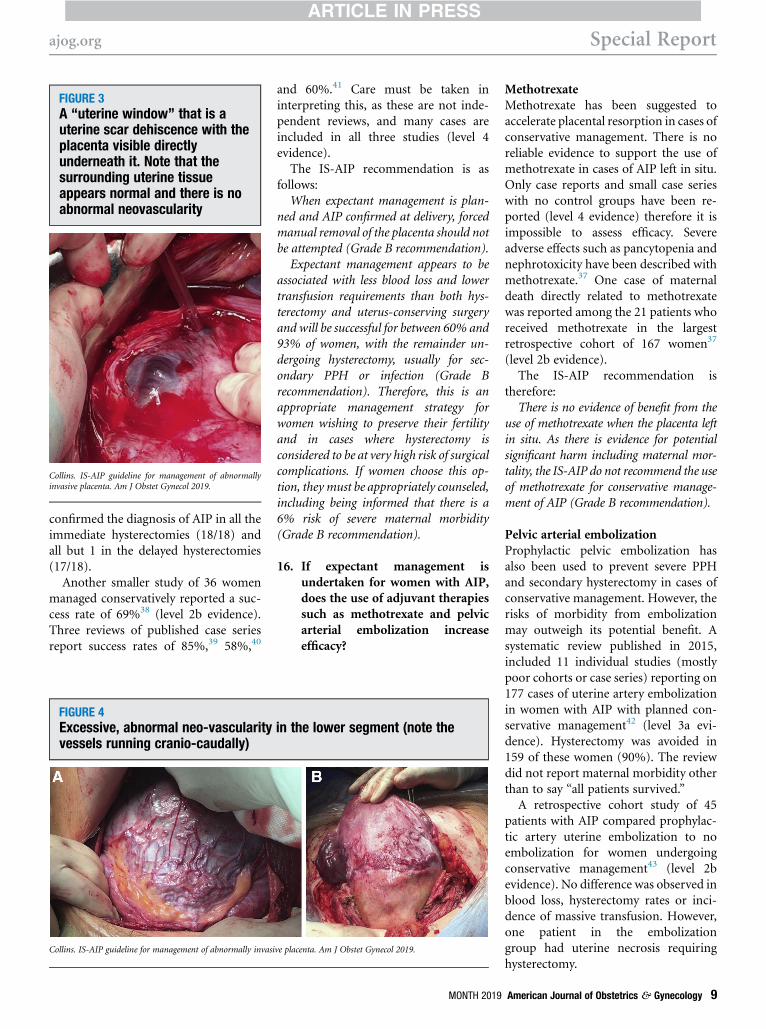
FIGURE 3A “uterine window” that is auterine scar dehiscence with theplacenta visible directlyunderneath it. Note that thesurrounding uterine tissueappears normal and there is noabnormal neovascularity
Collins. IS-AIP guideline for management of abnormallyinvasive placenta. Am J Obstet Gynecol 2019.
ajog.org Special Report
confirmed the diagnosis of AIP in all theimmediate hysterectomies (18/18) andall but 1 in the delayed hysterectomies(17/18).
Another smaller study of 36 womenmanaged conservatively reported a suc-cess rate of 69%38 (level 2b evidence).Three reviews of published case seriesreport success rates of 85%,39 58%,40
FIGURE 4Excessive, abnormal neo-vascularityvessels running cranio-caudally)
Collins. IS-AIP guideline for management of abnormally invasi
and 60%.41 Care must be taken ininterpreting this, as these are not inde-pendent reviews, and many cases areincluded in all three studies (level 4evidence).The IS-AIP recommendation is as
follows:When expectant management is plan-
ned and AIP confirmed at delivery, forcedmanual removal of the placenta should notbe attempted (Grade B recommendation).Expectant management appears to be
associated with less blood loss and lowertransfusion requirements than both hys-terectomy and uterus-conserving surgeryand will be successful for between 60% and93% of women, with the remainder un-dergoing hysterectomy, usually for sec-ondary PPH or infection (Grade Brecommendation). Therefore, this is anappropriate management strategy forwomen wishing to preserve their fertilityand in cases where hysterectomy isconsidered to be at very high risk of surgicalcomplications. If women choose this op-tion, they must be appropriately counseled,including being informed that there is a6% risk of severe maternal morbidity(Grade B recommendation).
16. If expectant management isundertaken for women with AIP,does the use of adjuvant therapiessuch as methotrexate and pelvicarterial embolization increaseefficacy?
in the lower segment (note the
ve placenta. Am J Obstet Gynecol 2019.
MONTH 2019
MethotrexateMethotrexate has been suggested toaccelerate placental resorption in cases ofconservative management. There is noreliable evidence to support the use ofmethotrexate in cases of AIP left in situ.Only case reports and small case serieswith no control groups have been re-ported (level 4 evidence) therefore it isimpossible to assess efficacy. Severeadverse effects such as pancytopenia andnephrotoxicity have been described withmethotrexate.37 One case of maternaldeath directly related to methotrexatewas reported among the 21 patients whoreceived methotrexate in the largestretrospective cohort of 167 women37
(level 2b evidence).The IS-AIP recommendation is
therefore:There is no evidence of benefit from the
use of methotrexate when the placenta leftin situ. As there is evidence for potentialsignificant harm including maternal mor-tality, the IS-AIP do not recommend the useof methotrexate for conservative manage-ment of AIP (Grade B recommendation).
Pelvic arterial embolizationProphylactic pelvic embolization hasalso been used to prevent severe PPHand secondary hysterectomy in cases ofconservative management. However, therisks of morbidity from embolizationmay outweigh its potential benefit. Asystematic review published in 2015,included 11 individual studies (mostlypoor cohorts or case series) reporting on177 cases of uterine artery embolizationin women with AIP with planned con-servative management42 (level 3a evi-dence). Hysterectomy was avoided in159 of these women (90%). The reviewdid not report maternal morbidity otherthan to say “all patients survived.”
A retrospective cohort study of 45patients with AIP compared prophylac-tic artery uterine embolization to noembolization for women undergoingconservative management43 (level 2bevidence). No difference was observed inblood loss, hysterectomy rates or inci-dence of massive transfusion. However,one patient in the embolizationgroup had uterine necrosis requiringhysterectomy.
American Journal of Obstetrics & Gynecology 9
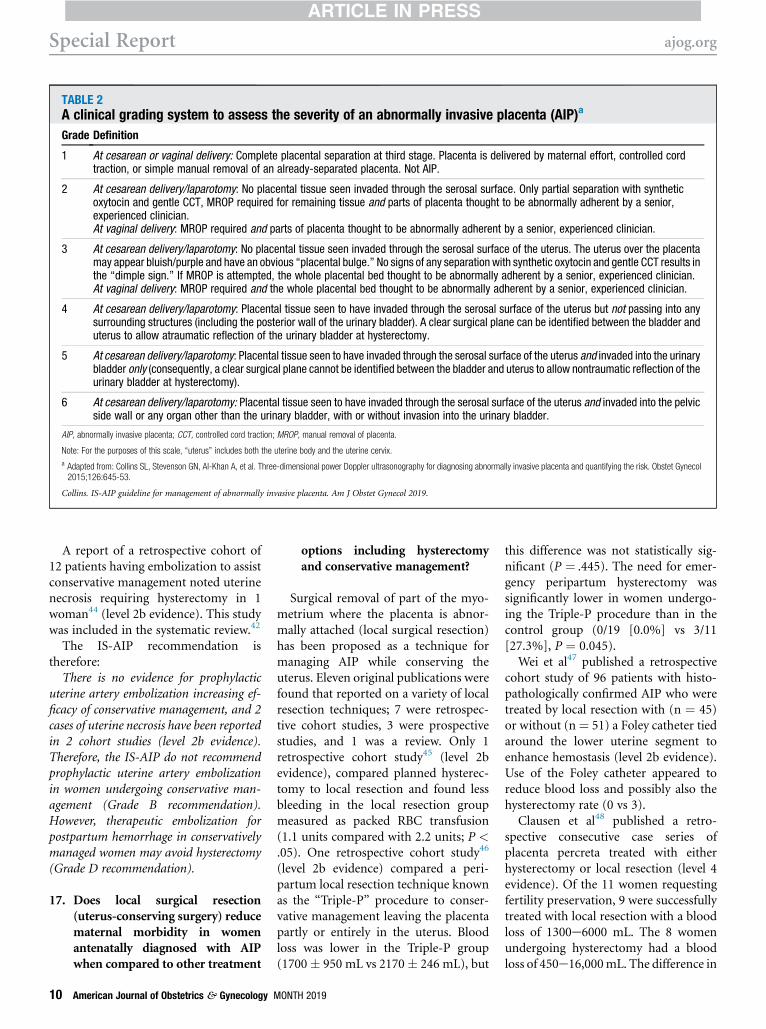
TABLE 2A clinical grading system to assess the severity of an abnormally invasive placenta (AIP)a
Grade Definition
1 At cesarean or vaginal delivery: Complete placental separation at third stage. Placenta is delivered by maternal effort, controlled cordtraction, or simple manual removal of an already-separated placenta. Not AIP.
2 At cesarean delivery/laparotomy: No placental tissue seen invaded through the serosal surface. Only partial separation with syntheticoxytocin and gentle CCT, MROP required for remaining tissue and parts of placenta thought to be abnormally adherent by a senior,experienced clinician.At vaginal delivery: MROP required and parts of placenta thought to be abnormally adherent by a senior, experienced clinician.
3 At cesarean delivery/laparotomy: No placental tissue seen invaded through the serosal surface of the uterus. The uterus over the placentamay appear bluish/purple and have an obvious “placental bulge.” No signs of any separation with synthetic oxytocin and gentle CCT results inthe “dimple sign.” If MROP is attempted, the whole placental bed thought to be abnormally adherent by a senior, experienced clinician.At vaginal delivery: MROP required and the whole placental bed thought to be abnormally adherent by a senior, experienced clinician.
4 At cesarean delivery/laparotomy: Placental tissue seen to have invaded through the serosal surface of the uterus but not passing into anysurrounding structures (including the posterior wall of the urinary bladder). A clear surgical plane can be identified between the bladder anduterus to allow atraumatic reflection of the urinary bladder at hysterectomy.
5 At cesarean delivery/laparotomy: Placental tissue seen to have invaded through the serosal surface of the uterus and invaded into the urinarybladder only (consequently, a clear surgical plane cannot be identified between the bladder and uterus to allow nontraumatic reflection of theurinary bladder at hysterectomy).
6 At cesarean delivery/laparotomy: Placental tissue seen to have invaded through the serosal surface of the uterus and invaded into the pelvicside wall or any organ other than the urinary bladder, with or without invasion into the urinary bladder.
AIP, abnormally invasive placenta; CCT, controlled cord traction; MROP, manual removal of placenta.
Note: For the purposes of this scale, “uterus” includes both the uterine body and the uterine cervix.
a Adapted from: Collins SL, Stevenson GN, Al-Khan A, et al. Three-dimensional power Doppler ultrasonography for diagnosing abnormally invasive placenta and quantifying the risk. Obstet Gynecol2015;126:645-53.
Collins. IS-AIP guideline for management of abnormally invasive placenta. Am J Obstet Gynecol 2019.
Special Report ajog.org
A report of a retrospective cohort of12 patients having embolization to assistconservative management noted uterinenecrosis requiring hysterectomy in 1woman44 (level 2b evidence). This studywas included in the systematic review.42
The IS-AIP recommendation istherefore:
There is no evidence for prophylacticuterine artery embolization increasing ef-ficacy of conservative management, and 2cases of uterine necrosis have been reportedin 2 cohort studies (level 2b evidence).Therefore, the IS-AIP do not recommendprophylactic uterine artery embolizationin women undergoing conservative man-agement (Grade B recommendation).However, therapeutic embolization forpostpartum hemorrhage in conservativelymanaged women may avoid hysterectomy(Grade D recommendation).
17. Does local surgical resection(uterus-conserving surgery) reducematernal morbidity in womenantenatally diagnosed with AIPwhen compared to other treatment
10 American Journal of Obstetrics & Gynecology
options including hysterectomyand conservative management?
Surgical removal of part of the myo-metrium where the placenta is abnor-mally attached (local surgical resection)has been proposed as a technique formanaging AIP while conserving theuterus. Eleven original publications werefound that reported on a variety of localresection techniques; 7 were retrospec-tive cohort studies, 3 were prospectivestudies, and 1 was a review. Only 1retrospective cohort study45 (level 2bevidence), compared planned hysterec-tomy to local resection and found lessbleeding in the local resection groupmeasured as packed RBC transfusion(1.1 units compared with 2.2 units; P <.05). One retrospective cohort study46
(level 2b evidence) compared a peri-partum local resection technique knownas the “Triple-P” procedure to conser-vative management leaving the placentapartly or entirely in the uterus. Bloodloss was lower in the Triple-P group(1700� 950 mL vs 2170� 246 mL), but
MONTH 2019
this difference was not statistically sig-nificant (P ¼ .445). The need for emer-gency peripartum hysterectomy wassignificantly lower in women undergo-ing the Triple-P procedure than in thecontrol group (0/19 [0.0%] vs 3/11[27.3%], P ¼ 0.045).
Wei et al47 published a retrospectivecohort study of 96 patients with histo-pathologically confirmed AIP who weretreated by local resection with (n ¼ 45)or without (n¼ 51) a Foley catheter tiedaround the lower uterine segment toenhance hemostasis (level 2b evidence).Use of the Foley catheter appeared toreduce blood loss and possibly also thehysterectomy rate (0 vs 3).
Clausen et al48 published a retro-spective consecutive case series ofplacenta percreta treated with eitherhysterectomy or local resection (level 4evidence). Of the 11 women requestingfertility preservation, 9 were successfullytreated with local resection with a bloodloss of 1300e6000 mL. The 8 womenundergoing hysterectomy had a bloodloss of 450e16,000mL. The difference in

ajog.org Special Report
blood loss between the 2 treatments,however, does not reflect intention totreat. The 1 woman who had a 16,000-mL blood loss had requested fertilitypreservation, and local resection wasattempted initially followed by a hyster-ectomy, as the placenta had invaded intothe cervix and parametrium.
Kutuk et al36 published a retrospectivecohort study comparing women under-going hysterectomy without placentalremoval (n ¼ 20), expectant manage-ment (n ¼ 15), and women who un-derwent placental removal and uterineconserving surgery (n ¼ 11) (level 2bevidence) (see the topic on expectantmanagement for further details).
In all of the other studies, the intendedsurgical procedure was local resection,and there was no comparator group.49-54
The success rates for avoiding hysterec-tomy ranged between 67% and 100%.
In 2014, Clausen et al published a re-view of 119 patients with placenta per-creta stratified by mode ofmanagement40 (level 3a evidence). In all,17 cases reported were local resectionwith no secondary hysterectomies; 36cases were conservatively managed, in 3of which the patients underwent aplanned delayed hysterectomy and 18had emergency hysterectomies; and 66had primary cesarean hysterectomies.Local resection was reported to be asso-ciated with a lower rate of complicationsincluding urinary tract injury, secondaryhemorrhage, and infection. However,there was no information providedregarding how the choice for localresection was made.
The evidence available for the efficacyof local resection is complicated by se-lection bias and poor comparatorgroups, making interpretation of theresults difficult. However, the IS-AIPrecommendation based on the availableevidence and supported by consensusopinion is as follows:
There is no evidence to demonstrate thatroutine local resection in all cases of AIPreduces maternal morbidity or mortalitycompared to other treatment methods.However, in appropriately selected cases,local resection appears to be reasonablysuccessful (level 2b evidence), and mayreduce blood loss and maternal morbidity
compared to hysterectomy (level 2b/4 evi-dence) and requirement for emergencyhysterectomy compared with conservativemanagement (level 3b evidence). There-fore, local resection should be considered inappropriately selected cases (Grade Brecommendation).There is, however, some evidence to
suggest that attempting local resection maybe detrimental in cases involving invasioninto the uterine cervix and/or para-metrium (level 4 evidence). Therefore,local resection should be considered onlywhere there is no invasion into the para-metrium and/or uterine cervix (Grade Crecommendation).The IS-AIP expert consensus of what
constitutes an “appropriate case” for localresection is focal disease with an adherent/invasive area which is <50% of the ante-rior surface of the uterus (Grade Drecommendation). More evidence isrequired to fully identify which womenwillmost benefit from this managementstrategy.
18. Does performing a subtotalhysterectomy reduce maternalmorbidity in women antenatallydiagnosed with AIP whencompared to total hysterectomy?
Subtotal, or supracervical, hysterec-tomy has been reported to be associatedwith lower maternal morbidity than to-tal hysterectomy, particularly in preg-nant women. Although several studieson AIP reported the actual numbers ofsubtotal and total hysterectomy per-formed in their cohorts, no evidence forthe benefit of one type of hysterectomycompared to another was presented.Wright et al55 reported on a retrospec-tively collected cohort of 4967 peri-partum hysterectomies performed in theUnited States (level 2b evidence). AIPwas the stated indication for 1789 (36%)of these hysterectomies. No subgroupanalysis of the AIP cases was presented.For the overall dataset of all peripartumhysterectomies, total hysterectomy wasassociated with more bladder injuries(10.2% vs 7.2%, P < .001), an increasednumber of other operative injuries(10.4% vs 8.3%, P ¼ 0.02), moregastrointestinal complications (7.9% vs.
MONTH 2019 A
6.3%, P¼ .04), and a longer hospital stay(P < .001). Subtotal hysterectomy wasassociated with more secondary opera-tions (5.0% vs 3.6%, P ¼ .02), higherrates of transfusions (52.4% vs 42.7%, P< .001), and a higher perioperativematernal death rate (1.4% vs 0.8%, P ¼.04).
Knight et al, on behalf of the UKObstetric Surveillance System (UKOSS),examined all the peripartum hysterec-tomies occurring in the United Kingdomover a 12-month period56 (level 2b evi-dence). For the 318 hysterectomies per-formed, there were no significantdifferences in outcomes between totaland subtotal hysterectomy. In all, 119 ofthe hysterectomies were performed forAIP; these were more commonly totalhysterectomies, but no subgroup anal-ysis between the 2 methods wasreported.
Another 6 small retrospective studieswere identified (level 3b/4 evidence).Ogunniyi et al reported 32 cases of per-ipartum hysterectomy57 and demon-strated that subtotal hysterectomy wasassociated with higher postoperativemorbidity than total (55.6% vs 71.4%; P< .01). Roopnarinesingh et al. reported52 cases in a single center in Dublin.58
They found that total hysterectomy wasassociated with a significantly highertransfusion rate (12.7 units vs 9.4 units;P < .001). Saeed et al reported on 39cases from a single center in Pakistan59
and found that total hysterectomy hada significantly higher number of post-operative complications than did sub-total hysterectomy.
D’Arpe et al reported on 51 cases froma single center in Italy60; Daskalakis et alreported on 45 cases from a single centerin Athens61; and Olamijulo et al reportedon 34 cases from a single center inNigeria.62 No significant differences inmorbidity were found in these studies(level 4 evidence).
No information was available in anystudy regarding how the decision wasmade regarding the method of hyster-ectomy. Therefore, the evidence avail-able is highly likely to be complicated byconsiderable selection bias, makinginterpretation of these results extremelydifficult. For that reason, the IS-AIP
merican Journal of Obstetrics & Gynecology 11

Special Report ajog.org
recommendation is also supported byconsensus opinion (level 5 evidence):
There is no evidence to demonstrate thatroutine subtotal hysterectomy in all casesof AIP reduces maternal morbidity ormortality compared to total hysterectomy;in fact, the largest study published sug-gested that subtotal might be associatedwith a higher maternal mortality rate(level 2b evidence).
The type of hysterectomy performed,therefore, should be individualized on acase-by-case basis, taking into account thesite and degree of invasion both suspectedantenatally and found at laparotomy,amount of bleeding, stability of thewoman, and the skills, experience andpreference of the operating team (Grade Crecommendation). In cases with cervicalinvasion, total hysterectomy should beperformed (Grade D recommendation).
19. Does performing a planneddelayed hysterectomy reducematernal morbidity in womenantenatally diagnosed with AIPwhen compared to hysterectomyat the time of cesarean delivery?
A planned delayed hysterectomy in-volves leaving the placenta untouched inthe uterus at the time of delivery, withthe intention of performing a hysterec-tomy at a later date (days to weeks) afterthe cesarean delivery. This is performedin an attempt to reduce morbidity fromthe hysterectomy, as the uterine perfu-sion reduces after delivery of the infanteven with the placenta in situ. Only 1retrospective study was identified thatattempted to compare planned delayedhysterectomy with immediate hysterec-tomy.63 However, all the immediatehysterectomy cases presented as emer-gencies without antenatal diagnosis andwith signs of shock from hemorrhage.The delayed cases were all antenatallydiagnosed and the women underwentdelivery in a hemodynamically stablecondition (poor-quality cohort, level 4evidence).
This study was taken into consider-ation, but as it is methodologicallyflawed, the IS-AIP recommendation isbased on a consensus opinion (level 5evidence) and is as follows:
12 American Journal of Obstetrics & Gynecology
Given the evidence for the success ofexpectant management for AIP, the IS-AIPrecommend that the surgical choice shouldbe between immediate surgical manage-ment (hysterectomy or local resection) andexpectant management. There is no evi-dence of benefit of planned delayed hys-terectomy, and the potential complicationsof performing a second intentional surgicalprocedure in a stable patient outweigh thebenefits (Grade D recommendation).
20. What are the most effectiveintraoperative measures totreat life-threatening massivehemorrhage in women with AIP,should it occur at the time ofdelivery?
Strategies for massive bleeding fromAIP vary according to operator experi-ence and resources available. We foundno RCTs providing direct comparison ofdifferent intraoperative strategies toreduce blood loss in the event of life-threatening hemorrhage.
Pharmacological treatmentsThere were no publications that specif-ically addressed the question of theeffectiveness of uterotonics or hemo-static/procoagulant agents as life-savingmeasures to treat massive hemorrhagedirectly attributable to AIP. Therefore,the IS-AIP recommendation is based onconsensus opinion (level 5 evidence) andis as follows:Uterotonics should be considered in
accordance with local protocols whenevermassive uterine bleeding occurs until eitherhemostasis is achieved or the uterus isremoved. Hemostatic/procoagulant agentscan also be used in accordance withlocal protocols where the surgeon believesthey will be of benefit (Grade Drecommendation).The benefit of early administration of
tranexamic acid in reducing maternalmortality has been proven in theWOMAN study. This is a large multi-center, double-blind, placebo-controlledRCT comparing tranexamic acid to pla-cebo to prevent death from all causes ofbleeding, including AIP and other mor-bidities64 (level 1b evidence). Therefore,the IS-AIP recommendation for its use isas follows:
MONTH 2019
Tranexamic acid should be adminis-tered whenever massive hemorrhage oc-curs, preferably as soon as possible afteronset of significant bleeding (Grade Arecommendation).
Surgical treatmentsInternal iliac artery ligationFour retrospective studies were identi-fied reporting a total of 105 cases of in-ternal iliac artery ligation (IIAL)performed to reduce hemorrhage at de-liveries complicated by AIP.65-68 Three ofthese were retrospective cases series ofwomen undergoing IIAL, with nocomparator group (level 4 evi-dence),65,66,68 and 1 was a retrospectivecohort study comparing outcomes forwomenwith AIP treated with or withoutIIAL, at the time of delivery (poor-quality cohort, level 4 evidence).67 Theauthors concluded that IIAL did notcontribute to a reduction in blood loss;however, as the indication for under-taking IIALwas not described, this studyis highly likely to be confounded by se-lection bias. Consequently, it was notpossible to appropriately evaluate theefficacy of IIAL for reducing blood loss.
Uterine devascularizationOne retrospective study, from Verspycket al,69 reported immediate and long-term outcomes in 6 women undergoingsurgical uterine devascularization at thetime of cesarean delivery, followed byconservative management of their AIP(level 4 evidence). No conclusion can bedrawn from this regarding the efficiencyof the technique for hemorrhage control,but the study demonstrated that uterinedevascularization appears to be areasonably safe technique as long as it isnot associated with ovarian arteryligation.
Uterine compression suturesCompression sutures after extirpation ofplacenta were reported in 3 retrospectivestudies70-72 including a total of 47women. Shahin et al reported 26 cases ofwomen who had had bilateral uterineartery ligation followed by insertion of aB-Lynch suture for major hemorrhagefrom AIP (level 4 evidence).70 Two of the26 women died. Shazly et al reported a

ajog.org Special Report
similar case series of 7 women withhemorrhage from AIP who underwentbilateral uterine artery ligation and thenmultiple compression suturing (level 4evidence).71 The authors reported thatthe procedure was successful. For boththese studies, it is impossible to assess theefficacy of compression sutures alone, asthe treatment also involved arterial liga-tion. The absence of a control groupmakes it impossible to assess the effi-ciency of this technique to reduce bloodloss. Hwu et al reported a case series of14 women who had a vertical compres-sion suture involving both the anteriorand posterior uterine walls to controlbleeding from the placental bed (level 4evidence).72 One of these women wasdiagnosed with AIP. Again, there was nocontrol group, making assessment ofefficacy in reducing blood lossimpossible.
Balloon tamponadeOne retrospective study73 comparedfirst-line hysterectomy (17 women) andballoon tamponade (19 women).Women who were assessed to have>50% invasion of the axial plane of theuterus were treated with immediatehysterectomy. The remainder had aballoon tamponade after extirpation ofplacenta, with or without extra squarecompression sutures to the placentalbed. Blood loss and transfusion amountswere significantly lower in the tampo-nade group (P < .05); however, the se-lection criteria used brings into questionthe appropriateness of the 2 groups(poor-quality cohort, level 4 evidence).Also, it was not clear whether the tam-ponade was used to prevent or to treathemorrhage. Three retrospective studieslooking at treatment for PPH have alsoreported that the presence of an AIP isassociated with a higher failure rateof balloon tamponade (level 4evidence).74-76
Pelvic tamponadeA variety of techniques have beendescribed for pelvic tamponade in thecase of persistent bleeding after hyster-ectomy. Ghourab et al77 described 5cases of pelvic packing with 10e12 dryabdominal swabs (level 4 evidence).
Dildy et al78 described a case seriesspanning 38 years of pelvic packing usinga variety of materials, including pillowcases, gauze sheets, plastic X-ray cassettedrapes, and orthopedic stockings, filledwith gauze rolls (level 4 evidence).Charoenkwan et al79 reported a case se-ries of 3 woman treated with pelvictamponade using a large-volume Bakriballoon (level 4 evidence). There were nomaternal deaths in any of the 3 reports.No comment can be made on whichtechnique provides the most effectivetamponade.In light of the quality and potentially
conflicting evidence available, the IS-AIPrecommendations for the surgical pro-cedures to be used in case of massivehemorrhage are based mostly on aconsensus of expert opinion (level 5 ev-idence) and are as follows:If the woman is stable, the bleeding is
not imminently life threatening, and aconservative approach was planned (eitherfor maternal request or if hysterectomy isanticipated to be at very high risk ofsurgical complications), surgical uterus-conserving procedures should be attemp-ted before resorting to hysterectomy. Thesimplest techniques with the lowest com-plications should be performed first (GradeD recommendation).If the placenta has been removed, in-
trauterine tamponade (eg, balloon tam-ponade) should be the first-linemanagement. If this fails, or the placentaremains in situ, uterine devascularization,with or without uterine compressive su-tures, should be tried. Internal iliac arteryligation has the highest risk of post-operative complications and thereforeshould be performed only if the previoussteps have failed to control the bleeding(Grade D recommendation).If the woman is unstable or the bleeding is
life threatening, treatment must be focusedon the source of the blood loss; this will mostoften be the placental bed, so emergencyhysterectomy should be performed as rapidlyas possible. Vascular compression (commoniliac arteries or aorta) can be used as atemporary measure to gain time to resusci-tate the woman and to complete definitivetreatment (Grade D recommendation).In case of persistent pelvic bleeding
following hysterectomy, internal iliac
MONTH 2019 A
artery ligation and/or pelvic tamponadeshould be considered. Pelvic tamponadeshould be performed with appropriate,sterile equipment such as large abdominalswabs and broad-spectrum antibioticsgiven while the packing remains in situ(Grade D recommendation).
21. What is the likelihood of a furtherpregnancy for women who havehad an AIP and successful uterineconservation?
Counseling women requesting uterineconserving treatment of AIP requiresknowledge of the evidence regarding thepossibility of subsequent pregnancy andassociated risk of recurrence of AIP.There are case reports80-84 (level 4 evi-dence), case series49,71,85,86 (level 4 evi-dence), case-controlled studies87 (level3b evidence), and cohort studies88-92
(level 2b evidence) that clearly demon-strate preservation of fertility after suc-cessful conservative management of AIP.There are, however, no prospective orrandomized studies.
In the largest cohort study, of 131women who had successful conservativemanagement of AIP, the authors re-ported that 27 women expressed a desirefor a subsequent pregnancy. Of thesewomen, 24 (89%) had 34 spontaneouslyconceived pregnancies (level 2b evi-dence).90 Another retrospective obser-vational study assessed 46 women whohad successful conservativemanagementof AIP91; 12 (86%) of the 14 patientsdesiring another pregnancy achieved atotal of 15 pregnancies (level 2b evi-dence). The only other cohort studypresenting outcomes for womendesiring a subsequent pregnancy re-ported that 5 of 6 women (83%) ach-ieved a successful pregnancy (level 2bevidence).88 These studies includedwomen who had received a multitude ofadditional treatments, includingadministration of methotrexate, embo-lization of uterine arteries, pelvic arterialligation, hysteroscopic resection ofretained tissues, and segmental excisionof the uterus. No study addressed theeffect that these different managementstrategies had on fertility preservation orwhat degree of placental adherence/
merican Journal of Obstetrics & Gynecology 13

Special Report ajog.org
invasion each woman had prior to con-servative management.
Two of the cohort studies also exam-ined the recurrence rates for AIP. In thelargest study,90 AIP recurred in 6 (29%)of the 21 pregnancies that continuedbeyond 34 weeks’ gestation and wasassociated with placenta previa in 4 cases(level 2b evidence). The other study re-ported that of the 9 patients who deliv-ered after 35 weeks’ gestation, 2 (22%)had recurrence of placenta accreta (level2b evidence).91
There is considerable evidencedemonstrating that women who havesuccessful conservative management ofAIPmay go on to have a successful futurepregnancy. What remains unclear iswhat effect different methods used forconservative management, such as arte-rial embolization or uterine resection,have on fertility rates, and what is impactthe original degree of adherence or in-vasion. The IS-AIP recommendation isbased on the available evidence sup-ported by expert consensus (level 5 evi-dence) and is as follows:
Women wishing to preserve their fertilityshould be counseled that this is possible(Grade B recommendation). If conservativemanagement is successful, the subsequentpregnancy rate is between 86% and 89%(Grade B recommendation). There is noevidence regarding the association ofAIP degree (accreta/increta/percreta) ormethods used for conservative manage-ment, and successful preservation of fertility.
Women wishing for fertility preserva-tion should be managed by a team withappropriate resources and experience inconservative management according tothat team’s local protocols (Grade Drecommendation). These women shouldbe counseled that their risk of AIP in asubsequent pregnancy is between 22% and29% (Grade B recommendation).
DiscussionThere were few questions that could beanswered using high-level evidence, andmany of the recommendations are basedon expert opinion. The paucity ofappropriate evidence for the optimalmanagement of this difficult andpotentially life-threatening conditionhighlights the urgent need for large,
14 American Journal of Obstetrics & Gynecology
multicenter collaborations. However,until the international communitycomes to an agreement on robust clinicaldiagnostic criteria and appropriatestratification of severity for AIP, the is-sues with comparing studies and trans-lating research results into clinicalpractice will remain. -
ACKNOWLEDGMENTS
We would like to thank the past and presentmembership of the IS-AIP, formerly the Euro-pean Working group on AIP (EW-AIP), for theirdedication to this international collaborationaimed at improving the outcomes for womenaffected by AIP worldwide. We would like tothank all of the librarians who assisted with morethan 30 searches, especially Ms. Nia Roberts,Librarian at University of Oxford. Pavel Calda issupported by a research grant (RVO-VFN64165) from the Ministry of Health of theCzech Republic.
REFERENCES
1. Chantraine F, Langhoff-Roos J. Abnormallyinvasive placentaeAIP. Awareness and pro-active management is necessary. Acta ObstetGynecol Scand 2013;92:369–71.2. Jauniaux E, Collins S, Burton GJ. Placentaaccreta spectrum: pathophysiology andevidence-based anatomy for prenatal ultra-sound imaging. Am JObstet Gynecol 2018;218:75–87.3. Klar M, Michels KB. Cesarean section andplacental disorders in subsequent preg-nanciesea meta-analysis. J Perinat Med2014;42:571–83.4. Jauniaux E, Chantraine F, Silver RM, Langh-off-Roos J. Diagnosis FPA, Management ExpertConsensus Panel. FIGO consensus guidelineson placenta accreta spectrum disorders:epidemiology. Int J Gynaecol Obstet 2018;140:265–73.5. Collins SL, Ashcroft A, Braun T, et al. Pro-posal for standardized ultrasound descriptors ofabnormally invasive placenta (AIP). UltrasoundObstet Gynecol 2016;47:271–5.6. Schardt C, Adams MB, Owens T, Keitz S,Fontelo P. Utilization of the PICO framework toimprove searching PubMed for clinical ques-tions. BMC Med Inform Decis Mak 2007;7:16.7. Phillips B, Ball C, Sackett D, et al. OxfordCentre for Evidence-based MedicineeLevels of Evidence (March 2009). Available at:https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/. Accessed April 16, 2019.8. Smulian JC, Pascual AL, Hesham H, et al.Invasive placental disease: the impact of a multi-disciplinary team approach to management.J Matern Fetal Neonatal Med 2017;30:1423–7.9. Al-Khan A, Gupta V, Illsley NP, et al. Maternaland fetal outcomes in placenta accreta after
MONTH 2019
institution of team-managed care. Reprod Sci2014;21:761–71.10. Eller AG, Bennett MA, Sharshiner M, et al.Maternal morbidity in cases of placenta accretamanaged by a multidisciplinary care teamcompared with standard obstetric care. ObstetGynecol 2011;117:331–7.11. Shamshirsaz AA, Fox KA, Salmanian B,et al. Maternalmorbidity in patientswithmorbidlyadherent placenta treated with and without astandardized multidisciplinary approach. Am JObstet Gynecol 2015;212:218.e1-9.12. Allen L, Jauniaux E, Hobson S, et al. FIGOconsensus guidelines on placenta accretaspectrum disorders: nonconservative surgicalmanagement. Int J Gynaecol Obstet 2018;140:281–90.13. Silver RM, Fox KA, Barton JR, et al. Centerof excellence for placenta accreta. Am J ObstetGynecol 2015;212:561–8.14. Wing DA, Paul RH, Millar LK. Managementof the symptomatic placenta previa: a random-ized, controlled trial of inpatient versus outpa-tient expectant management. Am J ObstetGynecol 1996;175:806–11.15. Droste S, Keil K. Expectant management ofplacenta previa: cost-benefit analysis of outpa-tient treatment. Am JObstet Gynecol 1994;170:1254–7.16. Mouer JR. Placenta previa: antepartumconservative management, inpatient versusoutpatient. Am J Obstet Gynecol 1994;170:1683–5; discussion 85e6.17. D’Angelo LJ, Irwin LF. Conservative man-agement of placenta previa: a cost-benefitanalysis. Am J Obstet Gynecol 1984;149:320–6.18. Love CD, Fernando KJ, Sargent L,Hughes RG. Major placenta praevia should notpreclude out-patient management. Eur J ObstetGynecol Reprod Biol 2004;117:24–9.19. Kavle JA, Stoltzfus RJ, Witter F, Tielsch JM,Khalfan SS, Caulfield LE. Association betweenanaemia during pregnancy and blood loss atand after delivery among women with vaginalbirths in Pemba Island, Zanzibar, Tanzania.J Health Popul Nutr 2008;26:232–40.20. Prevention andManagement of PostpartumHaemorrhage: Green-top Guideline No. 52.BJOG 2017;124:e106–49.21. Rac MW, Wells CE, Twickler DM,Moschos E, McIntire DD, Dashe JS. Placentaaccreta and vaginal bleeding according togestational age at delivery. Obstet Gynecol2015;125:808–13.22. Bowman ZS, Manuck TA, Eller AG,Simons M, Silver RM. Risk factors for un-scheduled delivery in patients with placentaaccreta. Am J Obstet Gynecol 2014;210:241.23. Fishman SG, Chasen ST. Risk factors foremergent preterm delivery in women withplacenta previa and ultrasound findings suspi-cious for placenta accreta. J Perinat Med2011;39:693–6.24. Pri-Paz S, Fuchs KM, Gaddipati S, Lu YS,Wright JD, Devine PC. Comparison betweenemergent and elective delivery in women with

ajog.org Special Report
placenta accreta. J Matern Fetal Neonatal Med2013;26:1007–11.25. Warshak CR, Ramos GA, Eskander R, et al.Effect of predelivery diagnosis in 99 consecutivecases of placenta accreta. Obstet Gynecol2010;115:65–9.26. Robinson BK, Grobman WA. Effectivenessof timing strategies for delivery of individuals withplacenta previa and accreta. Obstet Gynecol2010;116:835–42.27. Washecka R, Behling A. Urologic compli-cations of placenta percreta invading the urinarybladder: a case report and review of the litera-ture. Hawaii Med J 2002;61:66–9.28. Eller AG, Porter TF, Soisson P, Silver RM.Optimal management strategies for placentaaccreta. Br J Obstet Gynaecol 2009;116:648–54.29. Tam Tam KB, Dozier J, Martin JN Jr. Ap-proaches to reduce urinary tract injury duringmanagement of placenta accreta, increta, andpercreta: a systematic review. J Matern FetalNeonatal Med 2012;25:329–34.30. Shahin Y, Pang CL. Endovascular interven-tional modalities for haemorrhage control inabnormal placental implantation deliveries: asystematic review andmeta-analysis. Eur Radiol2018;28:2713–26.31. Salim R, Chulski A, Romano S, Garmi G,Rudin M, Shalev E. Precesarean prophylacticballoon catheters for suspected placentaaccreta: a randomized controlled trial. ObstetGynecol 2015;126:1022–8.32. Kotsuji F, Nishijima K, Kurokawa T, et al.Transverse uterine fundal incision for placentapraevia with accreta, involving the entire anterioruterine wall: a case series. BJOG 2013;120:1144–9.33. Murphy DJ, MacGregor H, Munishankar B,McLeod G. A randomised controlled trial ofoxytocin 5IU and placebo infusion versusoxytocin 5IU and 30IU infusion for the control ofblood loss at elective caesarean sectionepilotstudy. ISRCTN 40302163. Eur J Obstet Gyne-col Reprod Biol 2009;142:30–3.34. Jauniaux E, Bhide A, Kennedy A, et al. FIGOconsensus guidelines on placenta accretaspectrum disorders: prenatal diagnosis andscreening. Int J Gynaecol Obstet 2018;140:274–80.35. Kayem G, Keita H. [Management ofplacenta previa and accreta]. J Gynecol ObstetBiol Reprod (Paris) 2014;43:1142–60.36. Kutuk MS, Ak M, Ozgun MT. Leaving theplacenta in situ versus conservative and radicalsurgery in the treatment of placenta accretaspectrum disorders. Int J Gynaecol Obstet2018;140:338–44.37. Sentilhes L, Ambroselli C, Kayem G, et al.Maternal outcome after conservative treatmentof placenta accreta. Obstet Gynecol 2010;115:526–34.38. Miyakoshi K, Otani T, Kondoh E, et al.Retrospective multicenter study of leaving theplacenta in situ for patients with placenta previaon a cesarean scar. Int J Gynaecol Obstet2018;140:345–51.
39. Timmermans S, van Hof AC, Duvekot JJ.Conservative management of abnormally inva-sive placentation. Obstet Gynecol Surv2007;62:529–39.40. Clausen C, Lonn L, Langhoff-Roos J. Man-agement of placenta percreta: a review of pub-lished cases. Acta Obstet Gynecol Scand2014;93:138–43.41. Pather S, Strockyj S, Richards A,Campbell N, de Vries B, Ogle R. Maternaloutcome after conservative management ofplacenta percreta at caesarean section: a reportof three cases and a review of the literature. AustN Z J Obstet Gynaecol 2014;54:84–7.42. Mei J, Wang Y, Zou B, et al. Systematicreview of uterus-preserving treatmentmodalitiesfor abnormally invasive placenta. J ObstetGynaecol 2015;35:777–82.43. Pan Y, Zhou X, Yang Z, Cui S, De W, Sun L.Retrospective cohort study of prophylacticintraoperative uterine artery embolization forabnormally invasive placenta. Int J GynaecolObstet 2017;137:45–50.44. Bouvier A, Sentilhes L, Thouveny F, et al.Planned caesarean in the interventional radi-ology cath lab to enable immediate uterine arteryembolization for the conservative treatment ofplacenta accreta. Clin Radiol 2012;67:1089–94.45. Kilicci C, Ozkaya E, Eser A, et al. Plannedcesarean hysterectomy versus modified form ofsegmental resection in patients with placentapercreta. J Matern Fetal Neonatal Med 2017:1–6.46. Teixidor Vinas M, Belli AM, Arulkumaran S,Chandraharan E. Prevention of postpartumhemorrhage and hysterectomy in patients withmorbidly adherent placenta: a cohort studycomparing outcomes before and after intro-duction of the Triple-P procedure. UltrasoundObstet Gynecol 2015;46:350–5.47. Wei Y, Cao Y, Yu Y, Wang Z. Evaluation of amodified "Triple-P" procedure in women withmorbidly adherent placenta after previouscaesarean section. Arch Gynecol Obstet2017;296:737–43.48. Clausen C, Stensballe J, Albrechtsen CK,Hansen MA, Lonn L, Langhoff-Roos J. Balloonocclusion of the internal iliac arteries in themultidisciplinary management of placenta per-creta. Acta Obstet Gynecol Scand 2013;92:386–91.49. Palacios Jaraquemada JM, Pesaresi M,Nassif JC, Hermosid S. Anterior placenta per-creta: surgical approach, hemostasis and uter-ine repair. Acta Obstet Gynecol Scand 2004;83:738–44.50. Chandraharan E, Rao S, Belli AM,Arulkumaran S. The Triple-P procedure as aconservative surgical alternative to peripartumhysterectomy for placenta percreta. Int JGynaecol Obstet 2012;117:191–4.51. Shabana A, Fawzy M, Refaie W. Conser-vative management of placenta percreta: astepwise approach. Arch Gynecol Obstet2015;291:993–8.52. Karaman E, Kolusari A, Cetin O, et al. Localresection may be a strong alternative to
MONTH 2019 A
cesarean hysterectomy in conservative surgicalmanagement of placenta percreta: experiencesfrom a tertiary hospital. J Matern Fetal NeonatalMed 2017;30:947–52.53. Barinov S, Tirskaya Y, Medyannikova I,Shamina I, Shavkun I. A new approach tofertility-preserving surgery in patients withplacenta accreta. J Matern Fetal Neonatal Med2017:1–5.54. Polat I, Yucel B, Gedikbasi A, Aslan H,Fendal A. The effectiveness of double incisiontechnique in uterus preserving surgery forplacenta percreta. BMC Pregnancy Childbirth2017;17:129.55. Wright JD, Herzog TJ, Shah M, et al.Regionalization of care for obstetric hemorrhageand its effect on maternal mortality. ObstetGynecol 2010;115:1194–200.56. Knight M, Ukoss. Peripartum hysterectomyin the UK: management and outcomes of theassociated haemorrhage. BJOG 2007;114:1380–7.57. Ogunniyi SO, Esen UI. Obstetric hysterec-tomy in Ile-Ife, Nigeria. Int J Gynaecol Obstet1990;32:23–7.58. Roopnarinesingh R, Fay L, McKenna P.A 27-year review of obstetric hysterectomy.J Obstet Gynaecol 2003;23:252–4.59. Saeed F, Khalid R, Khan A, Masheer S,Rizvi JH. Peripartum hysterectomy: a ten-yearexperience at a tertiary care hospital in a devel-oping country. Trop Doct 2010;40:18–21.60. D’Arpe S, Franceschetti S, Corosu R, et al.Emergency peripartum hysterectomy in a ter-tiary teaching hospital: a 14-year review. ArchGynecol Obstet 2015;291:841–7.61. Daskalakis G, Anastasakis E,Papantoniou N, Mesogitis S, Theodora M,Antsaklis A. Emergency obstetric hysterectomy.Acta Obstet Gynecol Scand 2007;86:223–7.62. Olamijulo JA, Abiara OE, Olaleye OO,Ogedengbe OK, Giwa-Osagie F, Oluwole OO.Emergency obstetric hysterectomy in a Nigerianteaching hospital: a ten-year review. Nig Q JHosp Med 2013;23:69–74.63. Ansar A, Malik T, Shuja S, Khan S. Hyster-ectomy as a management option for morbidlyadherent placenta. J Coll Physicians Surg Pak2014;24:318–22.64. Collaborators WT. Effect of early tranexamicacid administration on mortality, hysterectomy,and other morbidities in women with post-partum haemorrhage (WOMAN): an interna-tional, randomised, double-blind, placebo-controlled trial. Lancet 2017;389:2105–16.65. Camuzcuoglu H, Toy H, Vural M, Yildiz F,Aydin H. Internal iliac artery ligation for severepostpartum hemorrhage and severe hemor-rhage after postpartum hysterectomy. J ObstetGynaecol Res 2010;36:538–43.66. Camuzcuoglu A, Vural M, Hilali NG, et al.Surgical management of 58 patients withplacenta praevia percreta. Wien KlinWochenschr 2016;128:360–6.67. Iwata A, Murayama Y, Itakura A, Baba K,Seki H, Takeda S. Limitations of internal iliacartery ligation for the reduction of intraoperative
merican Journal of Obstetrics & Gynecology 15
Special Report ajog.org
hemorrhage during cesarean hysterectomy incases of placenta previa accreta. J ObstetGynaecol Res 2010;36:254–9.68. Rauf M, Ebru C, Sevil E, Selim B. Conser-vative management of post-partum hemorrhagesecondary to placenta previa-accreta with hy-pogastric artery ligation and endo-uterine he-mostatic suture. J Obstet Gynaecol Res2017;43:265–71.69. Verspyck E, Resch B, Sergent F,Marpeau L. Surgical uterine devascularizationfor placenta accreta: immediate and long-termfollow-up. Acta Obstet Gynecol Scand2005;84:444–7.70. Shahin AY, Farghaly TA, Mohamed SA,Shokry M, Abd-El-Aal DE, Youssef MA. Bilateraluterine artery ligation plus B-Lynch procedurefor atonic postpartum hemorrhagewith placentaaccreta. Int J Gynaecol Obstet 2010;108:187–90.71. Shazly SA, Badee AY, Ali MK. The use ofmultiple 8 compression suturing as a novelprocedure to preserve fertility in patients withplacenta accreta: case series. Aust N Z J ObstetGynaecol 2012;52:395–9.72. Hwu YM, Chen CP, Chen HS, Su TH. Par-allel vertical compression sutures: a technique tocontrol bleeding from placenta praevia oraccreta during caesarean section. BJOG2005;112:1420–3.73. Pala S, Atilgan R, Baspinar M, et al. Com-parison of results of Bakri balloon tamponadeand caesarean hysterectomy in management ofplacenta accreta and increta: a retrospectivestudy. J Obstet Gynaecol 2018;38:194–9.74. Maher MA, Abdelaziz A. Comparison be-tween two management protocols for post-partum hemorrhage during cesarean section inplacenta previa: balloon protocol versus non-balloon protocol. J Obstet Gynaecol Res2017;43:447–55.
16 American Journal of Obstetrics & Gynecology
75. Mathur M, Ng QJ, Tagore S. Use of Bakriballoon tamponade (BBT) for conservativemanagement of postpartum haemorrhage: atertiary referral centre case series. J ObstetGynaecol 2018;38:66–70.76. ChoHY, Park YW,KimYH, Jung I, Kwon JY.Efficacy of intrauterine Bakri balloon tamponadein cesarean section for placenta previa patients.PLoS One 2015;10:e0134282.77. Ghourab S, Al-Nuaim L, Al-Jabari A, et al.Abdomino-pelvic packing to control severehaemorrhage following caesarean hysterec-tomy. J Obstet Gynaecol 1999;19:155–8.78. Dildy GA, Scott JR, Saffer CS, Belfort MA.An effective pressure pack for severe pelvichemorrhage. Obstet Gynecol 2006;108:1222–6.79. Charoenkwan K. Effective use of the Bakripostpartum balloon for posthysterectomy pelvicfloor hemorrhage. Am J Obstet Gynecol2014;210:586.80. Kayem G, Pannier E, Goffinet F, Grange G,Cabrol D. Fertility after conservative treatment ofplacenta accreta. Fertil Steril 2002;78:637–8.81. Tamate M, Matsuura M, Habata S, et al.Preservation of fertility and subsequent childbirthafter methotrexate treatment of placenta per-creta: a case report. J Med Case Rep 2015;9:232.82. Mahendru R, Taneja BK, Malik S. Preser-vation of fertility following abnormally adherentplacenta treated conservatively: a case report.Cases J 2009;2:9349.83. Endo T, Hayashi T, Shimizu A, et al. Suc-cessful uterus-preserving surgery for treatmentof chemotherapy-resistant placenta increta.Gynecol Obstet Invest 2010;69:112–5.84. Alanis M, Hurst BS, Marshburn PB,Matthews ML. Conservative management ofplacenta increta with selective arterial emboli-zation preserves future fertility and results in a
MONTH 2019
favorable outcome in subsequent pregnancies.Fertil Steril 2006;86:1514.85. Hequet D, Morel O, Soyer P, Gayat E,Malartic C, Barranger E. Delayed hysteroscopicresection of retained tissues and uterine con-servation after conservative treatment forplacenta accreta. Aust N Z J Obstet Gynaecol2013;53:580–3.86. Legendre G, Zoulovits FJ, Kinn J,Senthiles L, Fernandez H. Conservative man-agement of placenta accreta: hysteroscopicresection of retained tissues. J Minim InvasiveGynecol 2014;21:910–3.87. Kabiri D, Hants Y, Shanwetter N, et al.Outcomes of subsequent pregnancies afterconservative treatment for placenta accreta. IntJ Gynaecol Obstet 2014;127:206–10.88. Salomon LJ, deTayrac R, Castaigne-Meary V, et al. Fertility and pregnancy outcomefollowing pelvic arterial embolization for severepost-partum haemorrhage. A cohort study.Hum Reprod 2003;18:849–52.89. Ornan D, White R, Pollak J, Tal M.Pelvic embolization for intractable postpartumhemorrhage: long-term follow-up and implica-tions for fertility. Obstet Gynecol 2003;102:904–10.90. Sentilhes L, Kayem G, Ambroselli C, et al.Fertility and pregnancy outcomes followingconservative treatment for placenta accreta.Hum Reprod 2010;25:2803–10.91. Provansal M, Courbiere B, Agostini A,D’Ercole C, Boubli L, Bretelle F. Fertility andobstetric outcome after conservative manage-ment of placenta accreta. Int J Gynaecol Obstet2010;109:147–50.92. Bai Y, Luo X, Li Q, et al. High-intensityfocused ultrasound treatment of placentaaccreta after vaginal delivery: a preliminarystudy. Ultrasound Obstet Gynecol 2016;47:492–8.
Related Documents



![Nueva Ley Issste 2007 Marzo 13 2007 Nbsp Dip[1]. Nbsp Arizmendi2](https://static.cupdf.com/doc/110x72/5578cfaed8b42ad1598b4781/nueva-ley-issste-2007-marzo-13-2007-nbsp-dip1-nbsp-arizmendi2.jpg)