Abnormal Uterine Bleeding Benjie B. Mills, MD Division Director, Pediatric & Adolescent Gynecology Medical Director of Gynecology, GHS OB/GYN Center Associate Professor of Clinical Obstetrics & Gynecology University of South Carolina School of Medicine Greenville

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Abnormal Uterine Bleeding
Benjie B. Mills, MD
Division Director, Pediatric & Adolescent Gynecology Medical Director of Gynecology, GHS OB/GYN Center
Associate Professor of Clinical Obstetrics & Gynecology
University of South Carolina School of Medicine Greenville

Disclosures
• I have nothing to disclose • This presentation will discuss off-label use of
medications

Objectives
• Describe etiologies, work up, and clinical course of abnormal uterine bleeding
• Formulate a patient-centered and evidence-based treatment plan
• Focus on issues of particular importance to the PCP such as prevention, therapeutic lifestyle changes, health maintenance, and when to refer to a specialist

Etiologies
Abnormal Uterine Bleeding Heavy Menstrual Bleeding (AUB-HMB)
Intermenstrual Menstrual Bleeding (AUB-IMB)
PALM: Structural Polyp (AUB-P)
Adenomyosis (AUB-A) Leiomyoma (AUB-L)
Malignancy & Hyperplasia (AUB-M)
COEIN: Non-Structural Coagulopathy (AUB-C)
Ovulatory Dysfunction (AUB-O) Endometrial (AUB-E)
Iatrogenic (AUB-I) Not Yet Classified (AUB-N)
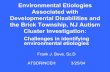
Structural
• Polyps

Structural
• Adenomyosis

Structural
• Leiomyomata

Structural
• Malignancy and Hyperplasia

Coagulopathy
• Inherited and acquired • Occurs in up to 20% of patients with HMB • Indications for evaluation
– Heavy menstrual bleeding since menarche, or – Postpartum hemorrhage, excessive surgical bleeding
or bleeding with dental work, or – Any two of the following
• Bruising 1-2 times per month • Epistaxis 1-2 times per month • Frequent gum bleeding • Family history of bleeding symptoms

Ovulatory Dysfunction
• Encompasses amenorrhea to frequent irregular menses and in between – Hypothalamic hypogonadotropic hypogonadism – Thyroid dysfunction – Hyperprolactinemia – Hyperandrogenemia/PCOS – Premature ovarian insufficiency – Idiopathic anovulation – Chronic illness

Endometrial Abnormalities
• Abnormal endometrial angiogenesis • Prostaglandin production • Vasoconstriction • Increased fibrinolysis

Iatrogenic
• Contraceptives – OCPs, contraceptive patch or ring – DepoProvera (DMPA) – Contraceptive implant (Nexplanon) – Intrauterine device
• Hormonal (levonorgestrel IUD, Mirena, Skyla) • Non-hormonal (Paragard, copper T)
• Other medications – Antipsychotics – Anticoagulants – Other

Evaluation

Evaluation: History
• Age of menarche • Menstrual bleeding pattern • Severity of bleeding (clots or flooding) • Pain • Medical history • Surgical history • Family history of bleeding disorders, PCOS,
diabetes …

Medications
• Anticoagulants • Hormonal medications • NSAIDs • Antipsychotics • Ginkgo • Ginseng • Motherwort

Physical Exam
• Abnormalities of weight • Skin
– Acanthosis nigricans – Hirsutism – Pallor – Petechiae or ecchymoses
• Thyroid • Abdomen • Pelvic

Laboratory Testing
• Pregnancy test • STD testing if indicated • CBC with diff • TSH

Laboratory Testing
• Bleeding disorder – PT/PTT/INR – Platelet function screen – Fibrinogen
• Hyperandrogenism/PCOS – Testosterone, free and total – DHEAS – 17 hydroxyprogesterone – HgbA1C, lipids, CMP

Laboratory Testing
• Amenorrhea/Oligomenorrhea – Prolactin – FSH/LH – Estradiol

• Ultrasound – Transvaginal – Transabdominal
• MRI – Müllerian
anomalies – Fibroid mapping – Adenomyosis
• Saline infusion sonogram – Cavity assessment – Endometrial biopsy
• Hysteroscopy • Endometrial biopsy
Imaging and Tissue Sampling

Differential Diagnosis by Age Category

Ages 13-18 Years
• Pregnancy – UCG – TV Ultrasound for positive UCG and bleeding
and/or pain • Pelvic infection
– GC and chlamydia NAATs – Trichomonas or cervicitis – PID
Ages 13-18 Years
• Anovulation – immaturity or dysregulation of the hypothalamic-pituitary-ovarian axis – Irregular cycle length – Within 3 years of menarche (80% in a regular pattern) – Plan:
• R/O pregnancy • Cyclic medroxyprogesterone acetate 10 mg x 10 days per
month or OCPs if desires treatment • TSH in patients with other symptoms of thyroid dysfunction • Coagulopathy workup if heavy since menarche • Assess for anemia if heavy or prolonged bleeding

Ages 13-18 Years
• Coagulopathies – Prolonged, heavy menses – May be irregular due to immature HPO axis – Plan:
• TSH • Bleeding disorder labs • Treat underlying condition • Treatment choices
– OCPs (increases factor secretion) – Anti-fibrinolytics – Menstrual suppression

Ages 13-18 Years
• Hormonal contraceptive use – OCPs
Cycle 1 Cycle 4
Extended Cycle OCP
> 7 days 65% 42% > 20 days 35% 15%
Cycles 1-4 Cycles 10-13
28d Cyclic OCP
> 7 days 38% 39% > 20 days 6% 4%

Ages 13-18 Years
• Hormonal contraceptive use – Etonogestrel implant
Bleeding Patterns Definitions %*
Infrequent Less than three bleeding and/or spotting episodes in 90 days (excluding amenorrhea)
33.6
Amenorrhea No bleeding and/or spotting in 90 days 22.2
Prolonged Any bleeding and/or spotting episode lasting more than 14 days in 90 days
17.7
Frequent More than 5 bleeding and/or spotting episodes in 90 days 6.7

Ages 13-18 Years
• Hormonal contraceptive use – Depo Medroxyprogesterone Acetate (DMPA)
• 54% with AUB at 1 year • 46% with amenorrhea • 25% discontinue because of AUB

Ages 19-39 Years
• Pregnancy • Infection • Hormonal contraception • Structural abnormalities
– Fibroids – Polyps – Adenomyosis

Ages 19-39 Years
• Anovulation – Polycystic ovarian syndrome is the most common
cause – Chronic disease – Idiopathic – Premature ovarian insufficiency
• Endometrial hyperplasia and malignancy (rare) – Endometrial sampling in high risk patients

Ages 40 to Menopause
• Pregnancy • Anovulation
– Physiologic when approaching menopause – PCOS
• Structural abnormalities • Endometrial hyperplasia and malignancy

Imaging & Tissue Sampling

Who gets imaging?
• Abnormal pelvic examination • Unresponsive to initial treatment in a patient
with a normal pelvic exam • Suspicion for structural abnormality

Which imaging is best?
• Transvaginal ultrasound (2D and 3D) – Screening test – Intracavitary pathology
• Sensitivity 56% • Specificity 73%
– Endometrial thickness is not helpful • Saline infusion sonography
– Superior at determining intracavitary pathology – Global changes vs. specific lesions
• MRI is not recommended for evaluation of AUB

Who needs endometrial sampling? • Women > age 45 with AUB • Women < age 45 with AUB and chronic
anovulation (unopposed estrogen) – Obesity – PCOS – Endometrial cancers and hyperplasias can be
diagnosed in young patients at very high risk

Evidence-Based Evaluation and Treatment Plans

Adolescent with AUB (IMB or HMB)
History & Physical Exam
Peripubertal Anovulatory
Bleeding Bleeding Disorder
Labs Refer to Peds Gyn
Expectant Management
Treat with Cyclic MPA or
OCPs

Reproductive Age with HMB
History, Physical Exam & Labs
Abnormal Pelvic Exam Normal Pelvic Exam
Treat: OCPs
LngIUD DMPA
Tranexamic acid
Ultrasound Treat Abnormality
Treatment Success No further workup
Treatment Failure Ultrasound
Refer to OB/Gyn

Reproductive Age with IMB History, Physical Exam, Normal
Pelvic Exam & Labs
Long-standing IMB
Expectant Management or
Treat: OCPs
Cyclic MPA
Treatment Success No further workup
Treatment Failure Needs Cavity Eval Refer to OB/Gyn
Short-term IMB
EMB and Cavity Evaluation
Refer to OB/Gyn
Prevention

Prevention
• Maintain healthy weight • Evaluate for PCOS if patient is 3 years post-
menarche and having IMB – Prevent hirsutism – Prevent long-term morbidity of PCOS via education
and health maintenance – Prevent psychologic sequelae
• Avoid use of DMPA for AUB • Recognize patients at high-risk for hyperplasia or
malignancy

Related Documents