Abdominal Tuberculosis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Abdominal Tuberculosis

Pathophysiology/ Pathology Intestinal TB
Areas involved
• Most commonly involves distal ileum & caecum
• Less commonly:
• ileum, jejunum, colon, anorectum
• Proximal small bowel rare
• Tracheoesophageal fistula

PathologyIntestinal TB
• Hypertrophic
• Ulcerative
• Ulcero-hypertrophic
• Mesenteric thickening
• Strictures
• Vascular involvement
Makharia G et al.The American Journal of Gastroenterology 105, 642-651 (March 2010) | doi:10.1038/ajg.2009.585
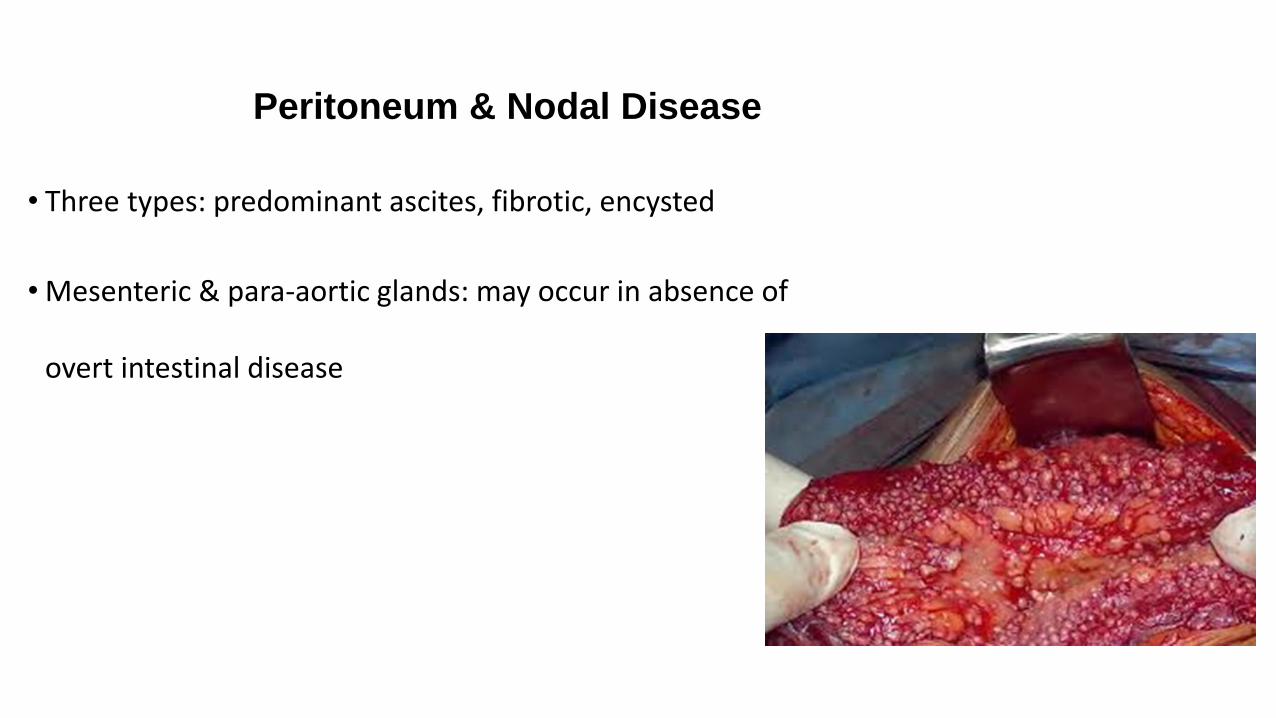
Peritoneum & Nodal Disease
• Three types: predominant ascites, fibrotic, encysted
• Mesenteric & para-aortic glands: may occur in absence of
overt intestinal disease

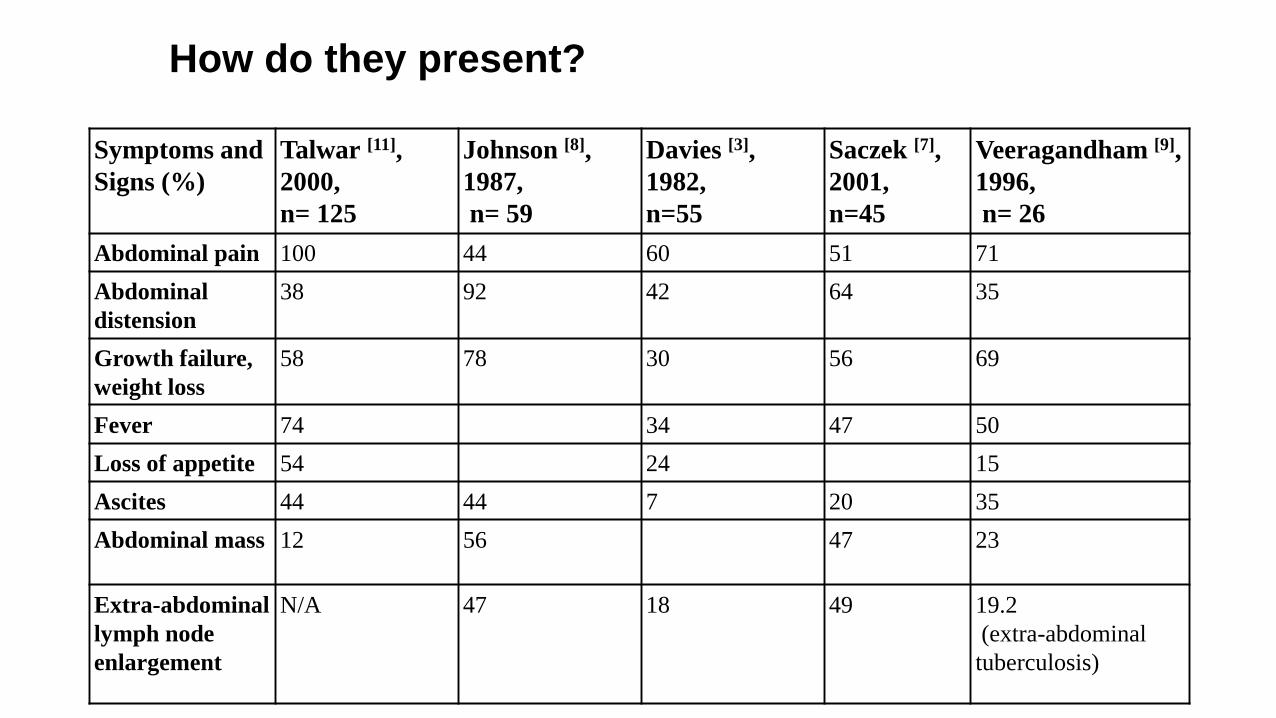
How do they present?
How do they present?
Symptoms and
Signs (%)
Talwar [11],
2000,
n= 125
Johnson [8],
1987,
n= 59
Davies [3],
1982,
n=55
Saczek [7],
2001,
n=45
Veeragandham [9],
1996,
n= 26
Abdominal pain 100 44 60 51 71
Abdominal
distension
38 92 42 64 35
Growth failure,
weight loss
58 78 30 56 69
Fever 74 34 47 50
Loss of appetite 54 24 15
Ascites 44 44 7 20 35
Abdominal mass 12 56 47 23
Extra-abdominal
lymph node
enlargement
N/A 47 18 49 19.2
(extra-abdominal
tuberculosis)

Case
• 12 year old boy
• Informal settlement
• 3 month history of• Abdominal pain
• Significant blood loss in stool
• Weight loss
• Initially treated by PHP as dysentery
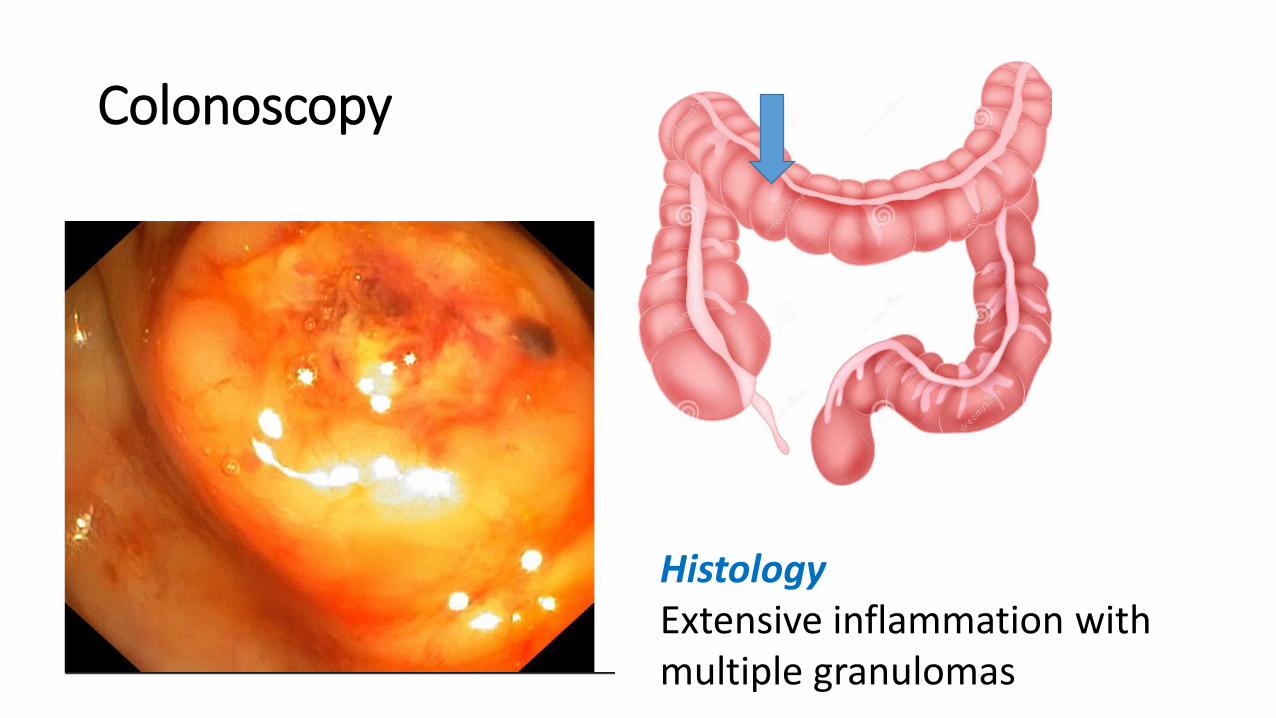
Colonoscopy
HistologyExtensive inflammation with multiple granulomas

Diagnosis

How do we make the diagnosis?
High index of suspicion in an endemic area (is the
child at risk?).
Most children chronically ill
Malnutrition
Signs of systemic disease: ESR, fever, anaemia
BUT
Acute presentations occur

How do we make the diagnosis?
Evidence of contact or infection.
Household contact (36% in Western Cape)
In developed countries often no history of
contact!
TST (44-68%, RSA)
Beware of false negative results
Interpretation differs according to the
population exposure
Case
• No household TBC (but uncle
has PTB)
• TST N/A
• No peripheral
lymphadenopathy

Radiography
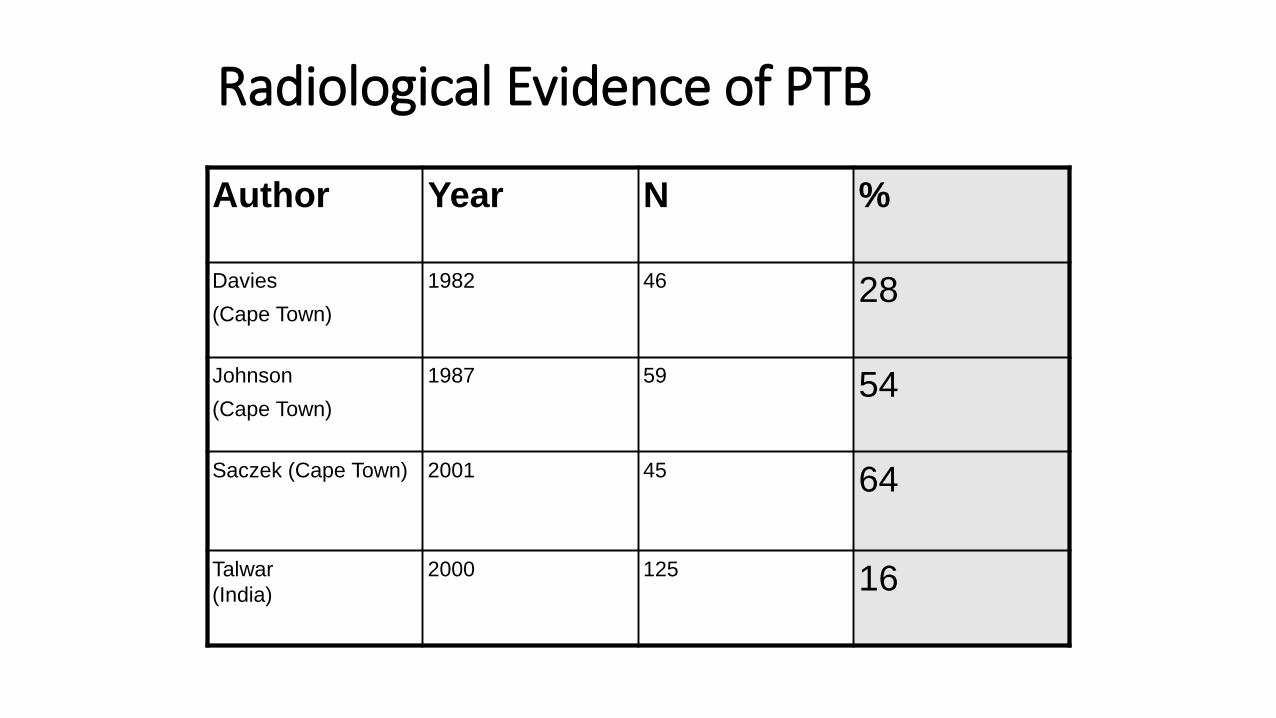
Radiological Evidence of PTB
Author Year N %
Davies
(Cape Town)
1982 46 28
Johnson
(Cape Town)
1987 59 54
Saczek (Cape Town) 2001 45 64
Talwar
(India)
2000 125 16
Abdominal X-Ray
Non-specific
Calcifications

Ultrasound
Lymphadenopathy
Ascites
Inflammatory mass
Thickened omentum
Intestinal involvement
Liver and spleen

Sonar graphic features of Tuberculous Lymph nodes {Bodh, 2016 }
• Hypoechoic, patch anechoic/hypoechoic
• Calcification
• Sharply demarcated borders
• Conglomerate of nodes
• Larger than reactive lymph nodes
• EUS guided FNA {Puri, 2012 } {Chen, 2004}

Abdominal Ultrasound
• Calcified lesion in the liver• Small amount of ascites• Large necrotic nodes through-
out the abdomen
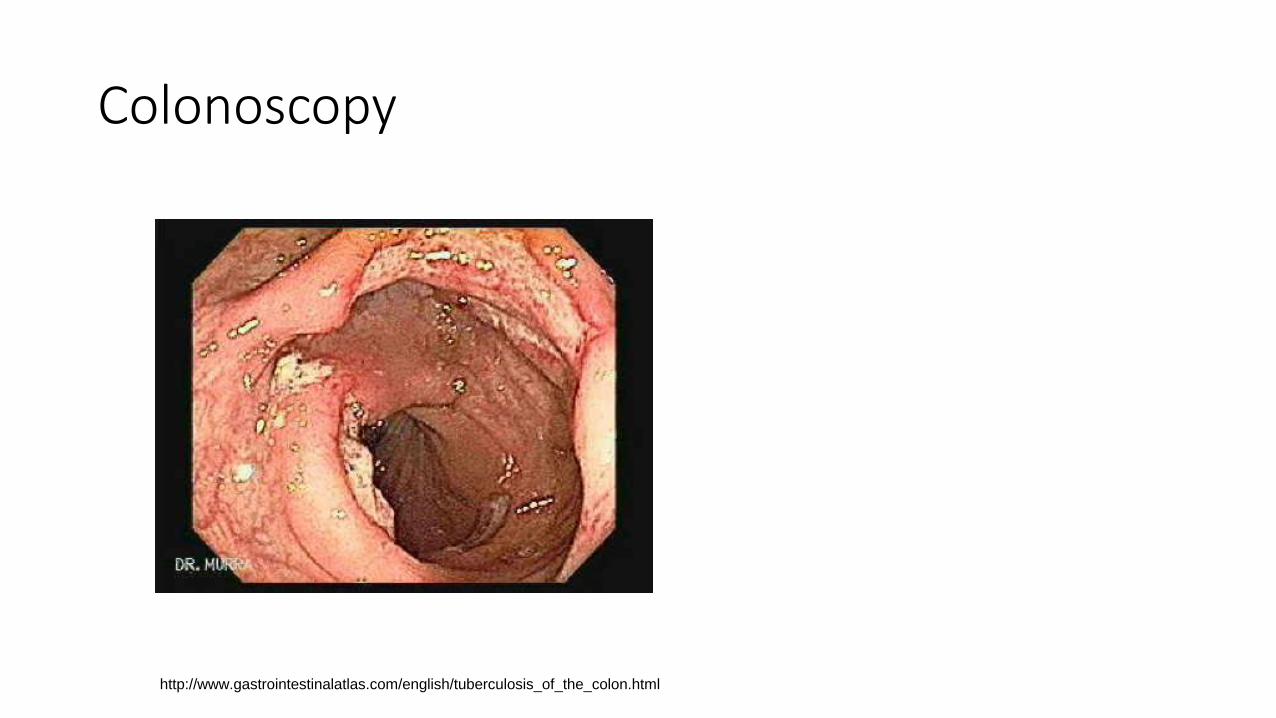
Colonoscopy
http://www.gastrointestinalatlas.com/english/tuberculosis_of_the_colon.html

Colonoscopy{Larsson, 2014 #2274} {Huang, 2015 #2259} {Makharia, 2010 #2270}
CD TBExtensive disease Mucosal nodularity
Multiple segments involved (skip lesions)
Distal disease more common Mostly limited to the right colon & TI
Aphtous or linear ulcers or superficial ulcers
Ring ulcers
Cobble stone appearance Ulcer scars
Erythema
Friability
Perianal disease

Histology{Kirsch, 2006 #2273}
• Granulomas in TB• More common• More per biopsy site• Larger (>0.05mm)• Confluent• Caseous necrosis• Submucosal more common (mucosal equal in TB & CD)
• Ulcer• Epithelioid cells more common in TB
• Disproportionate submucosal chronic inflammation
CT/MRI
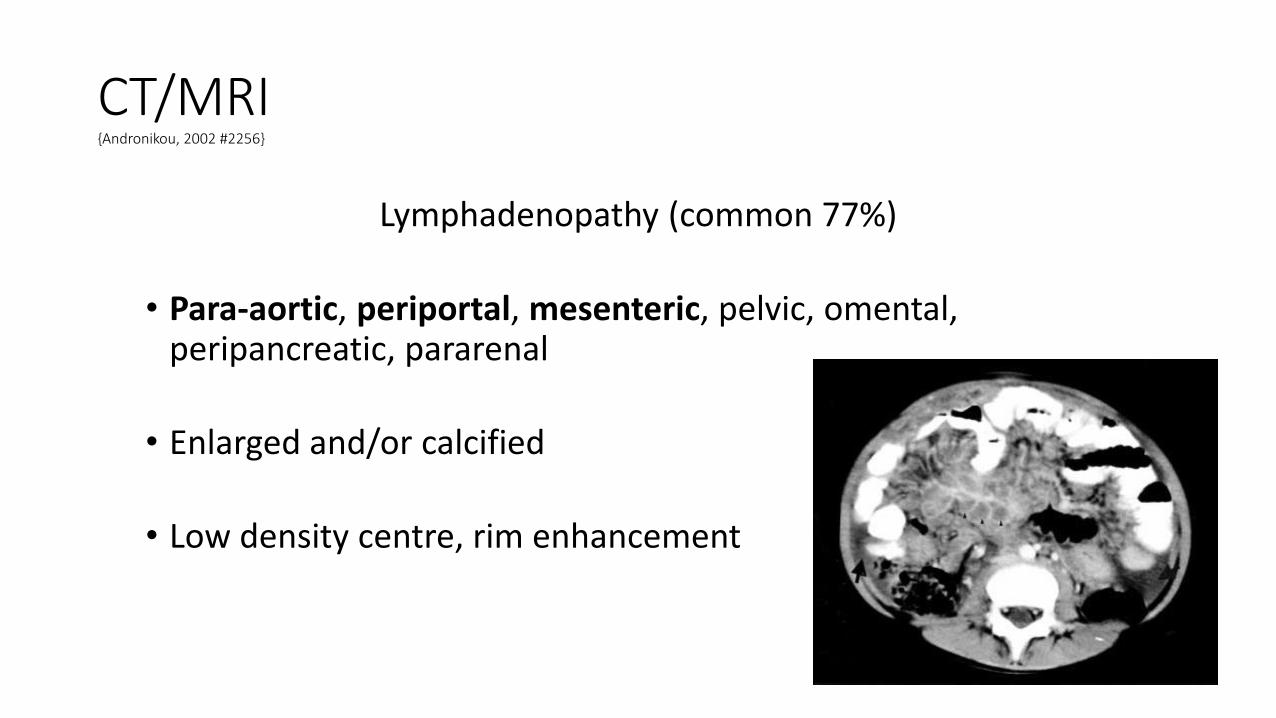
CT/MRI{Andronikou, 2002 #2256}
Lymphadenopathy (common 77%)
• Para-aortic, periportal, mesenteric, pelvic, omental, peripancreatic, pararenal
• Enlarged and/or calcified
• Low density centre, rim enhancement

CT AbdomenSolid organ disease
• Hepatic & splenic granuloma/abscess
• Low density
• Ring enhancement
• Calcify
• Pancreatic involvement rare in children
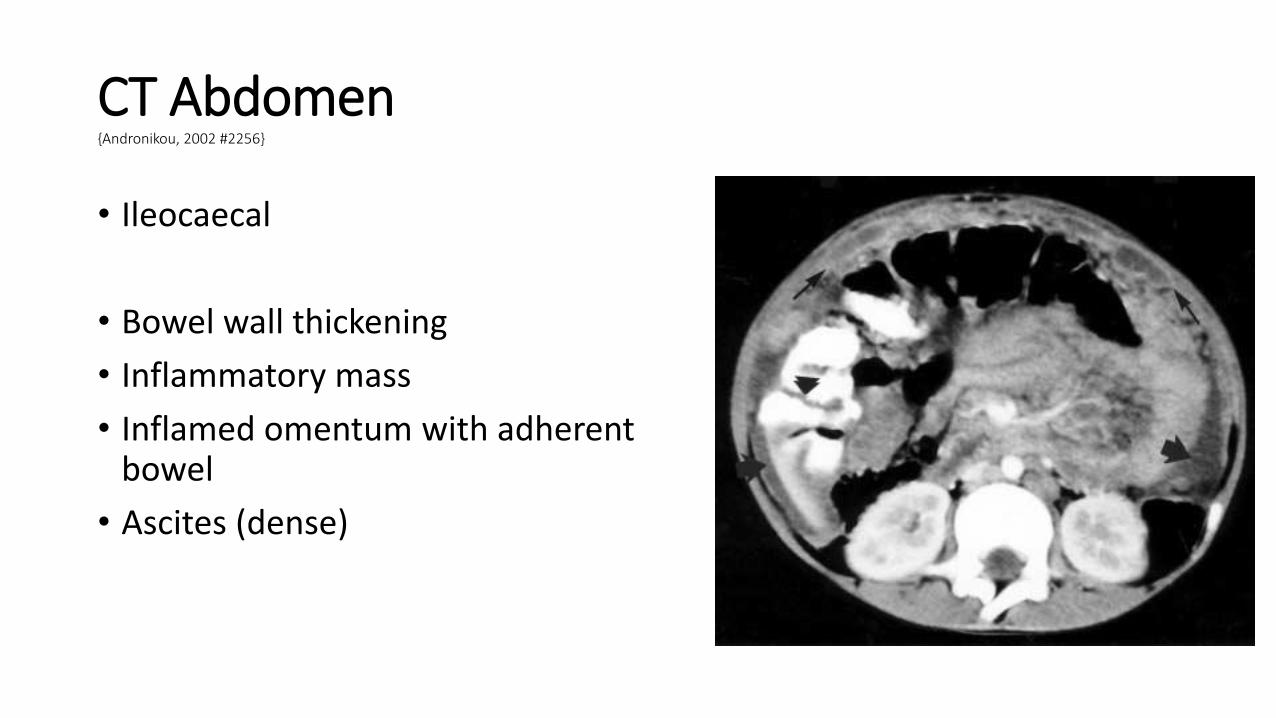
CT Abdomen{Andronikou, 2002 #2256}
• Ileocaecal
• Bowel wall thickening
• Inflammatory mass
• Inflamed omentum with adherent bowel
• Ascites (dense)

Laparoscopy
{Muroni, 2015}
{Islam, 2014} KZN{Malik, 2011} Pakistan
>60% - 80%• histology suggestive or • Typical appearance
BUT
Complications: 2 bowel perforations, 3 intra-operative bleeds, 6 required conversion to laparotomy due to adhesions

What should we do?
Do we have enough information to make a
therapeutic decision?

When can we treat without a bacteriological diagnosis?
Where is this appropriate?High prevalence
Presentation consistent with abdominal tuberculosis (“typical”)
Caveats“atypical” clinical presentation
Monitor response carefullyGeneral condition
Fever
Ascites
Abdominal mass
Lymphnodes
Nutrition
Incorrect diagnosis e.g. lymphoma, CD

Clinical Outcome
• 4 drug treatment for extra-pulmonary TB
• Large intestinal haemorrhage 2 days after the endoscopy
• Continue treatment: weight gain (2 kg), feels better
BUT
• Hb 7,7g/dl
• Rectal bleeding after 6 months

What are the principles of treatment?
Nutritional support
AscitesPoor response to diuretics
Anti-Tb drugs4 drugs intensive phase/ 2 drugs consolidation
6 months
SurgeryDiagnostic
Obstruction not responding to conservative measures
Perforation
Fistula
Haemorrhage

Conclusions
• TB mimics other diseases
• Definitive diagnosis not always possible
• Closely monitor the response to treatment
Related Documents











