Abdomen Inspect Auscultation Percussion Palpation

Abdomen Inspect Auscultation Percussion Palpation.
Jan 14, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Abdomen
Inspect
Auscultation
Percussion
Palpation
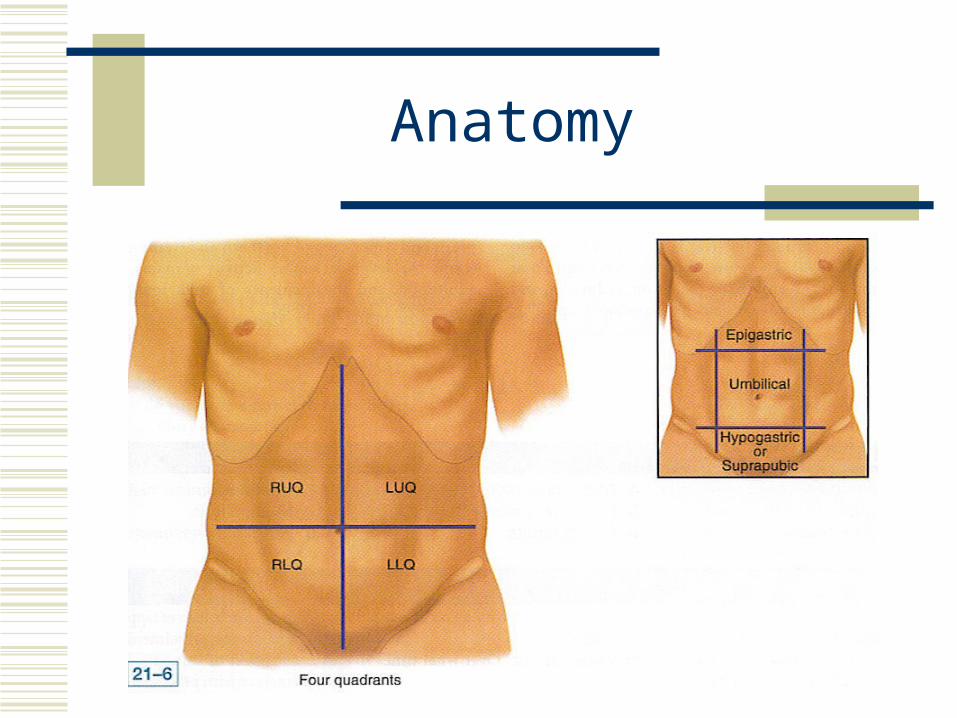
Anatomy
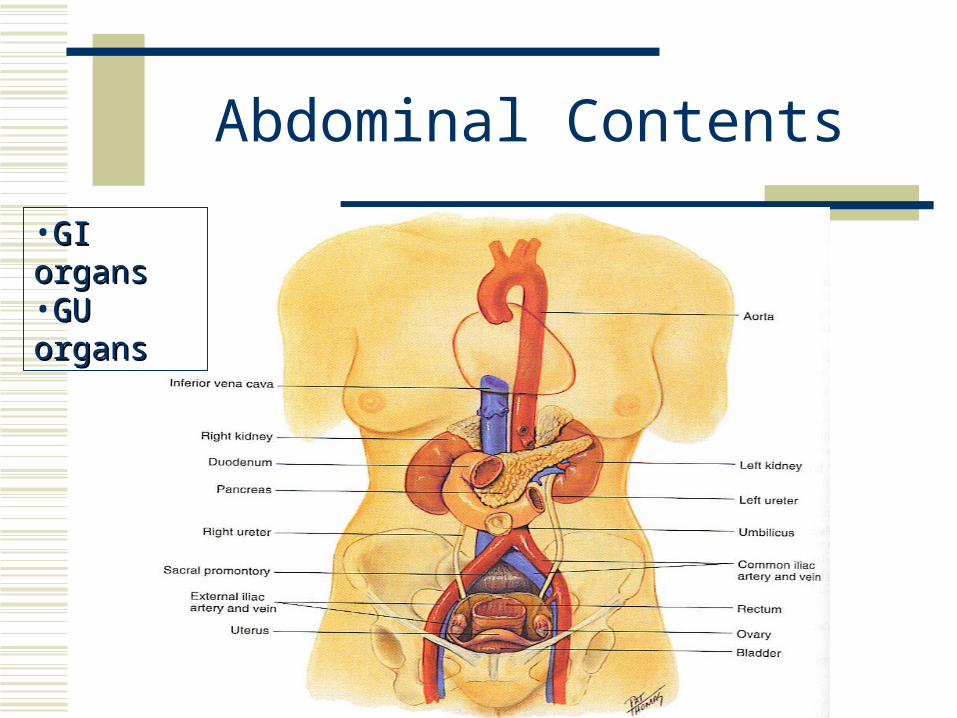
Abdominal Contents
•GI organsGI organs•GU organsGU organs
Health History
Appetite Dysphagia Food intolerance Abd pain N/V/D Bowel & bladder habits Past history (ulcers, gallbladder dx, hepatitis,
appendicitis, colitis, hernia) Medications
Common Symptoms
Indigestion Anorexia Nausea, vomiting, hematemesis Abdominal pain Dysphagia, odynophagia Change in bowel function
Constipation Diarrhea Jaundice/icterus Urinary/renal symptoms Kidney or flank pain Ureteral colic
Equipment
Stethoscope Measuring tape Pen or marker Pillow placed under the knees to relax the
abdominal musculature
Inspection
Contour – normally flat or rounded Scaphoid (sunken) Protuberant (abd distention)
Symmetry (bulging, visible mass) Umbilicus (midline & inverted) Observe for pulsation
A soft pulsation above the umbilicus is normal d/t the aorta
Inspection
Skin - smooth & even, note pigmentation & turgor Red-inflammation Jaundice-best in natural light Glistening & taut, striae –ascities Purple-blue striae –Cushing’s syndrome, may be
normal during pregnancy Petechiae Cutaneous angiomas (spider nevi)- HTN or liver dx
Assess for lesions, draw location, use cm Underlying adhesions and fibrous tissue
Assess for venous patterns, pulsations, hair distribution, demeanor
NOW, go to Ausculation instead of palpation. Palpation can cause motility that may not be there.
Auscultation
Bowel Sounds High-pitched use diaphragm, hold lightly Begin in the RLQ at the ileocecal valve area Bowel sounds are high pitched, gurgling,
cascading sounds, occurring irregularly between 5 to 30 times per minute
Documentation
Normoactive Hyperactive – sounds loud, high pitched,rushing,
tinkling sounds-increased motilitydiarrhea
Hypoactive – sounds decreased motility Partial obstructionconstipation
Absent sounds-no sounds for 5 minutesComplete obstruction from some cause
Vascular Sounds or Bruits
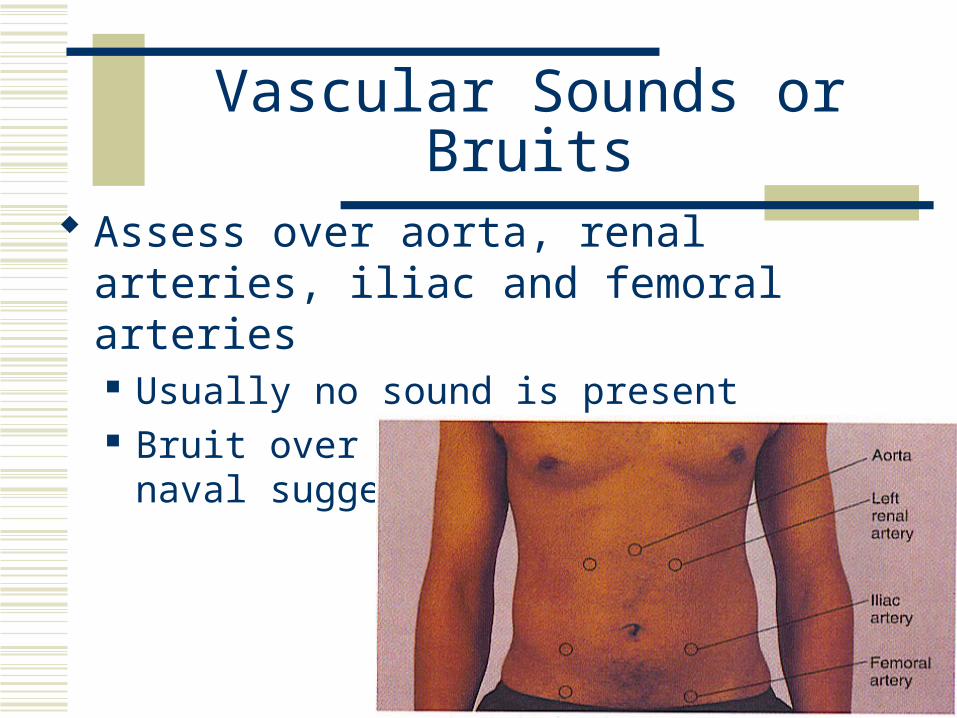
Assess over aorta, renal arteries, iliac and femoral arteries Usually no sound is present Bruit over the aorta or below naval suggests an
aneurysm
Percussion
Percuss 4 quadrants Tympany normally hear due to air in
intestines Dullness over distended bladder, fat, mass Hyperresonance over gaseous distention
Percuss liver span (left for MD) Percuss spleen (left for MD)
Palpation
Light palpation (1 cm, rotary motions) Assess for muscle guarding, rigidity, large
masses, tenderness Deep palpation (5-8 cm, rotary motions)
Use bimanual technique with obesity Tenderness occurs with local inflammation,
enlarged organs. Sigmoid colon is usually mildly tender
Abdominal Masses
For masses note: Location Size Shape Consistency
soft, firm, hard Surface Mobility Pulsality Tenderness
Palpable Structures
Liver Usually not palpable, if palpable more than 1-2 cm
below ribs it is enlarged
Spleen Enlarged 3 times normal size to be palpable Avoid overpalpation of the spleen it will rupture
Kidneys Use 2 hands (duck-bill)
Special Procedures
Rebound tenderness (Blumberg’s sign) Choose a site away from the painful area, push down
slowly, lift up quickly Usually tender if Appendicitis If not tender, GI virus
Inspiratory Arrest (Murphy’s Sign) Palpate liver on inspiration, with pain the test is
positive
Common Laboratory Tests
Esophagogastroduodenoscopy Barium enema (BE) Colonoscopy Computerized tomography scan (CT scan) Magnetic resonance imaging (MRI) Urinalysis, stool, emesis
Question
•Mrs. Jones presents at the emergency departmentcomplaining of severe pain in her abdomen. She has a history of a liver transplant. What would the nurse know NOT to do?
A. Auscultate the abdomen
B. Inspect the abdomen
C. Palpate the abdomen
D. Percuss the abdomen
Answer
•C. Palpate the abdomen
•Rationale: Do not palpate the abdomen of patients who have had an organ transplant or of a child with suspected Wilms’ tumor. Transplanted organs are often located in the anterior portion of the abdomen and not as well protected as the original placed organ.
Related Documents











