A Publication of the American Academy of Dermatology | Association FRIDAY. MARCH 1, 2019 © Janssen Biotech, Inc. 2019 01/19 cp-74265v1 VISIT TREMFYA ® AT BOOTH 3801 2019 AMERICAN ACADEMY OF DERMATOLOGY ANNUAL MEETING SEE MORE AAD ANNUAL MEETING NEWS! www.aadmeetingnews.org I f you can, filter out the “noise” of politics for a moment. The truth is, great work can happen in Washington, D.C., exemplified by the quality of education and events that make up this year’s AAD Annual Meeting. With a full schedule of education sessions, live demonstrations, and patient encounter workshops, learning and networking among dermatologists is at its finest. The next five days offer “a whirlwind of educational offerings with updates on the latest advancements from across the specialty,” according to AAD Scientific Assembly Committee Chair Bob Brodell, MD. “We live in a world where a significant percentage of medical students eschew the classroom in favor of digital content. The 2019 AAD Annual Meeting is adjusting to these new realities,” Dr. Brodell said. “However, you will see more ‘hands-on’ coursework, self-assessment sessions, and presentations featuring creative topics and innovative techniques. Still, some things will not change! The Annual Meeting will always have a large number of people getting together under one roof to renew friendships, share knowledge, and learn.” From panel discussions to a look at the latest products and services in the Exhibit Hall, myriad opportunities help dermatologists improve their practice, learn new techniques, hear the latest research, and expand their involvement in the Academy. The AAD Annual Meeting features more than 350 educational sessions and hot topics, as well as opportunities to meet vendors, connect with the Academy, and network with colleagues. The Exhibit Hall is open Friday, Saturday, and Sunday, with more than 350 exhibitors showcasing the latest products and services in dermatology. The Connection, located in Hall D, offers lounges to meet colleagues, check email, charge your phone, vote in the AAD election, claim CME credits, and more. Meet the candidates for president-elect and vice president-elect of the Academy during a live Town Hall on Friday, 12 to 1 p.m. in The Connection. Meet and greet the AAD Board of Directors. Get to know your representatives, tell them what’s on your mind, and learn about current initiatives and programs. The event is Saturday, 12 to 1 p.m. in The Connection. The AAD Resource Center serves as a central resource and features AAD services and new products. This includes CV/resume assistance and free professional headshots. Connect with colleagues and employers at the Career Networking Event, 4:30-6:30 p.m. at the Marriott Marquis, Ballroom Salon 6. “I’ve always seen the Annual Meeting as an opportunity — a chance to get out of my practice setting, learn the latest news and procedures, exchange ideas with fellow dermatologists, and work with my fellow members of the AAD to advance the specialty of dermatology,” said AAD President Suzanne Olbricht, MD. “I go home stimulated and ready to get back prepared to work to do the best job I can for my patients and my practice.” INSIDE EMPOWERING PATIENTS 4 THE TRANSLATIONAL REVOLUTION 6 SHAPING AI FOR DERMATOLOGY 12 EXHIBIT HALL MAP 14 2018 MELANOMA GUIDELINES 20 SLIDING INTO DIGITAL 24 We live in a world where a significant percentage of medical students eschew the classroom in favor of digital content. The 2019 AAD Annual Meeting is adjusting to these new realities. Bob Brodell, MD AAD Scientific Assembly Committee Chair The top concerns and interests of AAD members come to the forefront for the session “Hot Topics,” addressing those top-of-mind subjects established by registrant consensus. The presentations and speakers are: Acne: What’s New? Hilary Baldwin, MD Biologics and Psoriasis: The Beat Goes On Mark Lebwohl, MD Atopic Dermatitis: New Developments Emma Guttman, MD Drug Eruptions: The Good, Bad, and Ugly J. Mark Jackson, MD Melanoma Update 2018 Darrell Rigel, MD Hairy Matters: What’s New in Alopecia? Natasha Mesinkovska, MD Cosmeceuticals: Naturally Absurd? Adam Friedman, MD What’s New in Cosmetic Surgery? Anthony Benedetto, DO WHAT’S HOT? “Hot Topics” (S057) Monday, 1-4 p.m Ballroom C AAD in D.C.: Dermatology at its finest

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A Publication of the American Academy of Dermatology | Association
FRIDAY. MARCH 1, 2019
© Janssen Biotech, Inc. 2019 01/19 cp-74265v1
VISIT TREMFYA® ATBOOTH 3801
2019 AMERICAN ACADEMY OF DERMATOLOGYANNUAL MEETING
cp-74265v1_821516_v2.indd 1 1/31/19 2:13 PM
SEE MORE AAD ANNUAL MEETING NEWS! www.aadmeetingnews.org
I f you can, filter out the “noise” of politics for a moment. The truth is,
great work can happen in Washington, D.C., exemplified by the quality of education and events that make up this year’s AAD Annual Meeting. With a full schedule of education sessions, live demonstrations, and patient encounter workshops, learning and networking among dermatologists is at its finest.
The next five days offer “a whirlwind of educational offerings with updates on the latest advancements from across the specialty,” according to AAD Scientific Assembly Committee Chair Bob Brodell, MD.
“We live in a world where a significant percentage of medical students eschew the classroom
in favor of digital content. The 2019 AAD Annual Meeting is adjusting to these new realities,” Dr. Brodell said. “However, you will see more ‘hands-on’ coursework, self-assessment sessions, and presentations featuring creative topics and innovative techniques. Still, some things will not change! The Annual Meeting will always have a large number of people getting together under one roof to renew friendships, share knowledge, and learn.”
From panel discussions to a look at the latest products and services in the Exhibit Hall, myriad opportunities help dermatologists improve their practice, learn new techniques, hear the latest research, and expand their involvement in the Academy.
The AAD Annual Meeting features more than 350 educational sessions and hot topics, as well as opportunities to meet vendors, connect with the Academy, and network with colleagues.
The Exhibit Hall is open Friday, Saturday, and Sunday, with more than 350 exhibitors showcasing the latest products and services in dermatology.
The Connection, located in Hall D, offers lounges to meet colleagues, check email, charge your phone, vote in the AAD election, claim CME credits, and more.
Meet the candidates for president-elect and vice president-elect of the Academy during a live Town Hall on Friday, 12 to 1 p.m. in The Connection.
Meet and greet the AAD Board of Directors. Get to know your representatives, tell them what’s on your mind, and learn about current initiatives and programs. The event is Saturday, 12 to 1 p.m. in The Connection.
The AAD Resource Center serves as a central resource and features AAD services and new products. This includes CV/resume assistance and free professional headshots.
Connect with colleagues and employers at the Career Networking Event, 4:30-6:30 p.m. at the Marriott Marquis, Ballroom Salon 6.
“I’ve always seen the Annual Meeting as an opportunity — a chance to get out of my practice setting, learn the latest news and procedures, exchange ideas with fellow dermatologists, and work with my fellow members of the AAD to advance the specialty of dermatology,” said AAD President Suzanne Olbricht, MD. “I go home stimulated and ready to get back prepared to work to do the best job I can for my patients and my practice.”
INSIDE EMPOWERING PATIENTS 4 THE TRANSLATIONAL REVOLUTION 6 SHAPING AI FOR DERMATOLOGY 12 EXHIBIT HALL MAP 14 2018 MELANOMA GUIDELINES 20 SLIDING INTO DIGITAL 24
We live in a world where a significant percentage of medical students eschew the classroom in favor of digital content. The 2019 AAD Annual Meeting is adjusting to these new realities.
Bob Brodell, MDAAD Scientific Assembly
Committee Chair
The top concerns and interests of AAD members come to the forefront for the session “Hot Topics,” addressing those top-of-mind subjects established by registrant consensus.
The presentations and speakers are:
Acne: What’s New?Hilary Baldwin, MD
Biologics and Psoriasis: The Beat Goes OnMark Lebwohl, MD
Atopic Dermatitis: New DevelopmentsEmma Guttman, MD
Drug Eruptions: The Good, Bad, and UglyJ. Mark Jackson, MD
Melanoma Update 2018Darrell Rigel, MD
Hairy Matters: What’s New in Alopecia?Natasha Mesinkovska, MD
Cosmeceuticals: Naturally Absurd?Adam Friedman, MD
What’s New in Cosmetic Surgery?Anthony Benedetto, DO
WHAT’S HOT?
“Hot Topics” (S057)Monday, 1-4 p.mBallroom C
AAD in D.C.: Dermatology at its finest

JOB#: 1436851 CLIENT: Sandoz DESC: AAD Daily News Ad FILE NAME: SAN_AML_1436851_JA_D02.indd DATE: 1-28-2019 5:49 PM ROUND: 2PG: Ortiz-Krablin, Helena/Lake, Kathleen AD: Joe Mejia x3943 PM: Renee Roberts x4728 AE: Ron Kearns x5110 CW: Ryan Clark x4859 Last Saved: 1-28-2019 5:41 PMTRIM: 10.375” x 14” BLEED: 10.625” x 14.25” SAFETY: 9.375” x 13” PROD: Mike Haight x4245 INK Spec: 4 Color Process PRINT SCALE: NoneFONTS: Gotham Rounded (Bold, Medium, Light), Helvetica Neue LT Std (47 Light Condensed)
IMAGES: 436851_JA_fn.tif (CMYK; 300 ppi; 100%), 436851_JA_Products_fn.psd (CMYK; 300 ppi; 100%), Amlactin_4C.ai (76.1%), Amlactin_Icon_4C.ai (172%), Derm_Seal_2019_4C.ai (73.8%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: SAN_AML_1436851_JA_D02:Volumes...JA_D02:SAN_AML_1436851_JA_D02.inddNOTES: None
SAN_AML_1436851_JA_D02.indd Galley: 1
S&H PharmaGraphics
Disk
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
THAN A MOISTURIZERAmLactin® gently exfoliatesplus deeply hydrates with beneficial levels of lactic acid
Experience the difference at booth #2925
SUNBURN ALERT: This product contains an alpha-hydroxy acid (AHA) that may increase your skin’s sensitivity to sunburn. Be sun smart: Use sunscreen, wear protective clothing, and limit sun exposure while using this product and for a week afterward.
© 2019 Sandoz Inc., 100 College Road West, Princeton, NJ 08540
S-ALH-1368903 01/2019
S:9.375”S:13”
T:10.375”T:14”
B:10.625”B:14.25”

DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019 3
JOB#: 1436851 CLIENT: Sandoz DESC: AAD Daily News Ad FILE NAME: SAN_AML_1436851_JA_D02.indd DATE: 1-28-2019 5:49 PM ROUND: 2PG: Ortiz-Krablin, Helena/Lake, Kathleen AD: Joe Mejia x3943 PM: Renee Roberts x4728 AE: Ron Kearns x5110 CW: Ryan Clark x4859 Last Saved: 1-28-2019 5:41 PMTRIM: 10.375” x 14” BLEED: 10.625” x 14.25” SAFETY: 9.375” x 13” PROD: Mike Haight x4245 INK Spec: 4 Color Process PRINT SCALE: NoneFONTS: Gotham Rounded (Bold, Medium, Light), Helvetica Neue LT Std (47 Light Condensed)
IMAGES: 436851_JA_fn.tif (CMYK; 300 ppi; 100%), 436851_JA_Products_fn.psd (CMYK; 300 ppi; 100%), Amlactin_4C.ai (76.1%), Amlactin_Icon_4C.ai (172%), Derm_Seal_2019_4C.ai (73.8%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: SAN_AML_1436851_JA_D02:Volumes...JA_D02:SAN_AML_1436851_JA_D02.inddNOTES: None
SAN_AML_1436851_JA_D02.indd Galley: 1
S&H PharmaGraphics
Disk
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
THAN A MOISTURIZERAmLactin® gently exfoliatesplus deeply hydrates with beneficial levels of lactic acid
Experience the difference at booth #2925
SUNBURN ALERT: This product contains an alpha-hydroxy acid (AHA) that may increase your skin’s sensitivity to sunburn. Be sun smart: Use sunscreen, wear protective clothing, and limit sun exposure while using this product and for a week afterward.
© 2019 Sandoz Inc., 100 College Road West, Princeton, NJ 08540
S-ALH-1368903 01/2019
S:9.375”
S:13”
T:10.375”
T:14”
B:10.625”
B:14.25”
Vol. 30, No 1 March 1, 2019
PresidentSuzanne Olbricht, MD
Physician ReviewerMarta Van Beek, MD, MPH
Executive Director & CEOElaine Weiss, JD
Director, CommunicationsKatie Domanowski
Associate Director, PublishingRichard Nelson, MS
Managing Editor, Special Publications
Dean Monti, MFA
Creative ManagerNicole Torling
Senior Graphic DesignerTheresa Oloier
Printed in U.S.A. ©2019American Academy
of Dermatology Association9500 W. Bryn Mawr Ave, Ste 500
Rosemont, IL 60018-5216Phone (847) 330-0230;
Fax (847) 330-0050
Produced for the American Academy of Dermatology
By Ascend Integrated Media
A look at AAD’s Plenary sessionSunday’s speakers offer key insight
This year’s Plenary
speakers cover
a wide range of
topics. Learn more
about these seven
individuals and
what they plan
to share in their
presentations.
Paul Nghiem, MD, PhD“Less Toxic, More Effective: A Win-Win for Merkel Cell Carcinoma”
What does it mean to you to be selected for and speak at this year’s Plenary?Delivering the Van Scott/Frost lectureship is a career-highlight honor for me because I have always hoped my research would have impact in the care of patients. More importantly, I believe this event should help us come together to ensure Merkel cell carcinoma patients get the best possible multi-disciplinary care. Lives will literally be saved and unnecessary toxicities will be avoided due to the awareness that can come from this session.
Diane M. Thiboutot, MD“In Search of the Next Isotretinoin”
What is the key point you hope members will take away from your presentation?Acne remains an important disease that causes distress to millions of individuals and that analysis of large datasets in partnership with industry can accelerate drug discovery.
Robin Farmanfarmaian“Patient Empowerment in the Digital Age”
What does it mean to you to be selected for and speak at this year’s Plenary?I am incredibly honored to be selected for this year’s Plenary! As a chronic disease patient, as well as an entrepreneur working in health care, I have massive respect for physicians and other health care providers, and with good reason — they are the ones on the front lines working to save and improve other people’s lives. For decades, health care providers have helped me, and it is an honor to be able to give back to them in this small way.
Boris D. Lushniak, MD “I Acted and Behold, Service was Joy”
What is one insight you can share about the future of dermatology?
We, as dermatologists, need to be fully engaged in paving the pathway for the future of dermatology as a 21st century specialty. Embrace technology but don’t forget the art, the personal interactions, and the service mission of medicine.
George J. Hruza, MD, MBAPresident-Elect’s Address
How do you plan to address challenges to the profession in your role?Dermatology has the fastest rate of burnout increase in medicine. I will make sure that the Academy is there to support our members through a beefed-up Practice Management Center and reinvigorated advocacy at the federal and state level. A new quality improvement center will help our members improve the care they provide their patients. We will perform an in-depth review of all of our programs to enhance our effectiveness, transparency, and responsiveness to our members and the needs of dermatology.
Crystal L. Mackall, MD“Engineering T Cells for Cancer Therapy”
What is the key point you hope members will take away from your presentation? I am hopeful that I can educate the members regarding recent progress in using engineered T cells for cancer therapy and convey to the members the basis for optimism regarding the potential of this novel class of therapeutics.
Suzanne M. Olbricht, MDPresident’s Address
What has been one of the greatest challenges to the profession in the last year?The future of dermatology is strong. Dermatologists are energetic, passionate, and innovative. Innovating is critical because the practice of medicine will be vastly different in five years due to the digital revolution and advances in augmented intelligence. I encourage AAD members to embrace change and focus on our vision statement: Advancing excellence in dermatology.
Share your photos on Instagram to win big at the Annual Meeting!
The Instagram Challenge is back! Between Friday, Mar. 1, and Monday, Mar. 4, the @AADmember Instagram account will be hosting a photo challenge where attendees can submit pictures of themselves with their friends, colleagues, or mentors at the Annual Meeting. Participants must follow @AADmember and include the hashtag #AAD2019Challenge in the caption of their photo(s) to enter. A winner will be randomly chosen each day to win a $50 gift card, and a grand prize winner will be selected from the total submissions to win free registration to the 2020 Annual Meeting!

4 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
Several Th2 cytokines, including IL-13, are key drivers of atopic dermatitis.1
BECOME ANATOPIC DERMATITIS
DETECTIVE
Reference: 1. Gittler JK, Shemer A, Suárez-Fariñas M, et al. J Allergy Clin Immunol. 2012;130(6):1344-1354.
LEO and the LEO Lion Design are registered trademarks of LEO Pharma A/S.©2019 LEO Pharma Inc. All rights reserved. MAT-22212 January 2019 Printed in USA.
FOR MORE INFORMATION CHECK OUT ADdetective.com
Review the case at
LEO Pharma Booth#3227
7 a.m.-5:30 p.m. AAD registration openLocation: Grand Lobby – Street Level The Connection Location: Hall D• View e-posters• Charge your phone in the
Networking Lounge• Utilize e-center to access
voting, claim CME, read emails, and check in for your flight home
8 a.m.-5 p.m.AAD Resource Center openLocation: Hall D
9 a.m.-5 p.m.Gross and Microscopic Symposium (S008) Location: Room 149AB
12-1 p.m.AAD Election 2019• Meet the Candidates • Live Town HallLocation: The Connection, Hall D Unopposed exhibit timeLocation: Exhibit Hall
1-3 p.m.Virtual Dermatopathology Self Assessment: Get Ready for Non-glass Slide Exams (F022) Location: Room 143C
3:30-5:30 p.m.Boards and Beyond (F034) Location: Room 203AB
4-5:30 p.m.Access to Care Learning CollaborativeLocation: Georgetown University Room, Marriott Marquis
4:30-6:30 p.m.AAD Career Networking Event Location: Marquis Ballroom Salon 6, Marriott Marquis, Washington DC
5:30-7 p.m.International Members ReceptionLocation: Marquis Ballroom Salon 5, Marriott Marquis, Washington DC
Early Career ReceptionLocation: Marquis Ballroom Salon 7-10, Marriott Marquis, Washington DC
7 p.m. (6:30 p.m. registration)Industry Non-CME Program: HANDS ON Psoriatic Disease: A Live & Augmented Reality Experience for Advancing Patient Care Despite Modern Time ConstraintsLocation: Renaissance Ballroom West A and B, Renaissance Washington, DC Downtown Hotel
From Novartis
Industry Non-CME Program: PD-1 Targeting Therapy in Advanced Metastatic Cutaneous Squamous Cell Carcinoma (CSCC)Location: Liberty M-P, Marriott Marquis Washington, DC
From Sanofi Genzyme and Regeneron
Industry Non-CME Program: Understanding and Treating Psoriatic Disease in a New Generation of PatientsLocation: Renaissance Ballroom East, Renaissance Washington, DC Downtown Hotel
From UCB Inc.
TODAY’S HIGHLIGHTS
What is one insight you
will share about the future of dermatology?Farmanfarmaian: The use of AI will increase as more and more accurate data is aggregated for AI programs to learn. This is beneficial for the dermatology field, as one of the things AI is best at doing is pattern analysis. AI analysis programs serve as tools that can help physicians and patients catch some problems earlier, when they are easier to treat.
How is technology
impacting health care?Health care is shifting in two major ways. A combination of technology and costs is shifting the point of care to where the patient is located, versus the patient having to physically go to a brick and mortar clinic. Also, patients are becoming more empowered by these same forces — technology and costs — to be in control of their health care: When they want it, where they want it, and how they want it.
If virtual care is the wave of the
future, what are the cons of virtual care?While there are tons of benefits for using virtual care, like most things in life, there are also some cons. Physical human touch is important in the health care relationship, both on an emotional level for the patient and for assessment and diagnostics.
If the physician is relying on data collected by the patient, such as vital signs, there is a risk the equipment is not being used correctly without a physician present. In addition, when the physician is able to see a patient in person, they may notice or catch things that either the patient doesn’t think to mention, or the patient doesn’t know is a symptom or a data point for assessment. Lastly, communication with any subject is always more effective in person, and this can be especially important when dealing with the complexities of health care.
As a non-physician
looking in, what do you believe were the greatest challenges to physicians in the last year?As someone with a high-level viewpoint of health care and technology, not in dermatology specifically, I believe the challenges to the dermatology profession are likely the same as the challenges faced in all other specialties: the high costs of medications and treatments for their patients. No specialty is immune to these rapidly growing costs, combined with reimbursement becoming even more complicated and at times, reduced. This isn’t a dermatology-specific challenge. This is the biggest challenge in health care today.
Q A Empowering patients in the digital age
& :
“Patient Empowerment in the Digital Age.”Sunday, 8-11:30 a.m.Ballroom B
Q
Q
In her session, “Patient Empowerment in the Digital Age,” plenary guest speaker Robin Farmanfarmaian will address a host of current breakthroughs in medical technology that are fundamentally changing the way patients interact with their health care and providers. These include wearable sensors, improved point-of-care diagnostics, augmented intelligence (AI), and virtual care. Farmanfarmaian will discuss methods for integrating these new services and revenue streams into the dermatology practice.
Currently, Farmanfarmaian is working with a few early stage start-ups: as COO for Arc Fusion Programs; as co-founder and former executive director for the Organ Preservation Alliance; as vice president of Business Development for Invicta Medical; and as president of i4j ECO, a summit to disrupt unemployment through innovation to create jobs and meaningful work for everyone.
Learn more about Robin Farmanfarmaian at www.robinff.com.
Pick up your copy of the Onsite Meeting GuideThe 2019 Onsite Meeting Guide, Experience the AAD Annual Meeting, is available in racks throughout the Walter E. Washington Convention Center. It has all of the vital information you need about the meeting, such as:
• Key elements• Daily highlights• AAD honors and awards• Education information• Social media platforms
• Exhibit Hall floor plan and exhibitor lists
• Convention center maps
MEET THE AAD BOARD OF DIRECTORSSATURDAY, MARCH 2 • 12–1 p.m.
In The Connection, located in Hall D
The
THOUGHTLEADER
FORMULAStrategically Leverage
Your Expertise to Drive
Business & Career Goals
R O B I N F A R M A N F A R M A I A N
The ultimate form of career insurance is becoming known as
an expert...Robin’s book lays out a clear, effective strategy...”
— D O R I E C L A R K“
Several Th2 cytokines, including IL-13, are key drivers of atopic dermatitis.1
BECOME ANATOPIC DERMATITIS
DETECTIVE
Reference: 1. Gittler JK, Shemer A, Suárez-Fariñas M, et al. J Allergy Clin Immunol. 2012;130(6):1344-1354.
LEO and the LEO Lion Design are registered trademarks of LEO Pharma A/S.©2019 LEO Pharma Inc. All rights reserved. MAT-22212 January 2019 Printed in USA.
FOR MORE INFORMATION CHECK OUT ADdetective.com
Review the case at
LEO Pharma Booth#3227
Empowering patients in the digital age

6 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
Novartis Pharmaceuticals CorporationEast Hanover, New Jersey 07936-1080 © 2019 Novartis 1/19 T-COS-1362218
Discover theComplete
Cosentyx ApproachBooth #3021
These Industry Expert Sessions are promotional activities and are not approved for continuing education credit. The content of these sessions and opinions expressed by presenters are those of the Presenting Company or presenters and do not represent an endorsement by, nor imply that the products have been evaluated or approved by the
American Academy of Dermatology.
Novartis acts in accordance with the PhRMA Code on Interactions With Health Care Professionals. The PhRMA Code states that inclusion of a health care professional’s spouse or guest at an educational program is not appropriate. Your support of these ethical guidelines will help to ensure a high quality learning environment for all
participating health care professionals. Thank you.
Francisco A. Kerdel, MD, MBBS, BSc
Presented by:
Saturday, March 2, 201911:00 am – 11:45 am Program
Exhibit Hall AWalter E. Washington Convention Center
Washington, DCPlease arrive at 10:45 am to register
Meal will be provided.
Industry Expert Session 2
Ben Lockshin, MD, FAAD
Presented by:
Friday, March 1, 20192:45 pm – 3:30 pm Program
Exhibit Hall AWalter E. Washington Convention Center
Washington, DCPlease arrive at 2:30 pm to register
Meal will be provided.
Industry Expert Session 1
Hear Expert Insights at Two Unique Educational Sessions
Join us for these exciting events at this year’s AAD Annual Meeting!
The first biologic treatment, dupilumab, is producing better or comparable clinical results to any of the pre-biologic era agents. The next step will be other biologics that can perhaps be administered every four to 12 weeks, followed by oral agents.
At least two different agents are in randomized clinical trials, with significant early results. More results may be presented at the AAD Annual Meeting.
Studies are emerging for topical and systemic treatments.
New biologics are emerging.
@AADmemberfacebook.com/AADmemberinstagram.com/aadmember
Get social with AADJoin the thousands of other dermatologists who are already following @aadmember, and be sure to use the official Annual Meeting hashtag #AAD19 in all your meeting-related posts and tweets.
The translational revolution in inflammatory skin diseasesT he scientific revolution
in the understanding of inflammatory skin
diseases as immune-mediated diseases that began in the late 1990s and early 2000s is evolving into a growing stream of new, revolutionary treatments. From initial breakthroughs in psoriasis to improved understanding of the pathogenesis of atopic dermatitis, alopecia areata, vitiligo, hidradenitis suppurativa, acne, and rosacea, the increased body of knowledge
is advancing treatment results that patients and their physicians could only dream about a decade ago.
These advances in the mechanistic understanding of disease translate into the rapid development and testing of targeted treatments that are safer and more effective than traditional agents for long-term disease control.
Dermatologists who want to explore current disease understanding and treatment and future treatments for
inflammatory skin diseases and the rationale for their use can find a comprehensive overview in Friday’s single symposium, “Inflammatory Skin Diseases: The Translational Revolution” that will feature some of the world’s leading experts in these diseases.
While conventional treatments may be effective to improve symptoms, they either harbor significant side effects — such as the risk of permanent kidney damage associated with more than one year of
continuous use of cyclosporine — or are not feasible for many, such as phototherapy. The arrival of new agents that can realistically offer the prospect of long-term disease control is a clinical revolution for treating dermatologists and for their patients.
“I’m excited about “Melanoma: The Future is Now.” It features my melanoma idols such as Dr. Suephy Chen, Dr. Darrell Rigel, and Dr. Susan Swetter. With the latest innovation in melanoma diagnostics and genomic profiling, it is important for us to selectively bring relevant testing/counseling to patient care.”
Shasa Hu, MDMiami
I appreciate the networking. I am able to meet with collaborators for research projects, participate in committee meetings, and catch-up with colleagues. Additionally, the talks on cutaneous oncology, particularly on high-risk squamous cell carcinoma are cutting edge and very apropos to my clinical practice.
David R. Carr, MDColumbus
“I am excited to learn about novel therapies for difficult to treat dermatologic diseases. As a resident, learning new treatment modalities from leading innovators aids me in confidently shaping my own methods of clinical practice. I hope to gain insights and direction from mentors who share my interest in dermatologic oncologic surgery!”
Atieh Jibbe, MDKansas City, Kansas
What are you excited to learn or see at the 2019 AAD Annual Meeting?
WATER COOLER
Biologic treatments are producing amazing results. The next step is targeted small molecule oral agents that are similarly effective in the real world.
Psoriasis Atopic dermatitis Alopecia areata Vitiligo Hidradenitis suppurativa
“Inflammatory Skin Diseases: The Translational Revolution” (S011)Friday, 1-4 p.m.Ballroom B
Novartis Pharmaceuticals CorporationEast Hanover, New Jersey 07936-1080 © 2019 Novartis 1/19 T-COS-1362218
Discover theComplete
Cosentyx ApproachBooth #3021
These Industry Expert Sessions are promotional activities and are not approved for continuing education credit. The content of these sessions and opinions expressed by presenters are those of the Presenting Company or presenters and do not represent an endorsement by, nor imply that the products have been evaluated or approved by the
American Academy of Dermatology.
Novartis acts in accordance with the PhRMA Code on Interactions With Health Care Professionals. The PhRMA Code states that inclusion of a health care professional’s spouse or guest at an educational program is not appropriate. Your support of these ethical guidelines will help to ensure a high quality learning environment for all
participating health care professionals. Thank you.
Francisco A. Kerdel, MD, MBBS, BSc
Presented by:
Saturday, March 2, 201911:00 am – 11:45 am Program
Exhibit Hall AWalter E. Washington Convention Center
Washington, DCPlease arrive at 10:45 am to register
Meal will be provided.
Industry Expert Session 2
Ben Lockshin, MD, FAAD
Presented by:
Friday, March 1, 20192:45 pm – 3:30 pm Program
Exhibit Hall AWalter E. Washington Convention Center
Washington, DCPlease arrive at 2:30 pm to register
Meal will be provided.
Industry Expert Session 1
Hear Expert Insights at Two Unique Educational Sessions
Join us for these exciting events at this year’s AAD Annual Meeting!

8 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
PP-A1D-USA-1788 © 2019 Pfizer Inc. All rights reserved. Printed in USA/January 2019
Friday, March 1, 2019 • 1:30 pm – 2:15 pm • Industry Expert Theater, AAD Exhibit Floor
Please join us for a non-CME program presented by
Refreshments will be provided
This Industry Expert Session is a promotional activity and is not approved for continuing education credit. The content of this session and opinions expressed by presenters are those of the Presenting Company or presenters and do not represent an endorsement by, nor imply that the products have been evaluated or approved by the American Academy of Dermatology.
Notice: This event is conducted in accordance with the PhRMA Code on Interactions with Healthcare Professionals and is limited to healthcare professionals (HCPs). Attendance by guests or spouses is not appropriate. Government employees are subject to state and federal laws and ethics rules that may limit their ability to receive any gifts, including meals, from pharmaceutical companies. If you are a state or federal employee, it is your responsibility to seek guidance and prior approval from your employer or site ethics counselor to attend this or any Pfizer event. Your attendance will be considered confirmation to Pfizer that you have obtained any necessary approvals to attend this event.
State Laws and Pfizer Disclosures: The cost of meals and refreshments provided to US licensed Healthcare Professionals attending this Pfizer-sponsored program will be subject to public disclosure on www.pfizer.com as part of Pfizer’s Healthcare Professional Disclosure policies, and may also be subject to disclosure by state governmental authorities pursuant to your state law and applicable federal law such as the National Physician Payment Transparency Program (otherwise known as “Sunshine”). Pfizer’s disclosure will allocate the cost of meals and refreshments equally across all attendees regardless of actual consumption. If you are licensed to practice in Minnesota or Vermont, we are prohibited from providing you any meals and/or refreshments due to your state limitation on meals, gifts or other items of value to HCPs and ask that you do not partake in the hospitality provided.
Learn About a Topical Option for Mild-to-Moderate Atopic Dermatitis
in Patients 2 Years and Older
Emily M. Becker, MD Sonterra Dermatology Driscoll Children’s Hospital Assistant Clinical Professor in Dermatology at University of Texas Health Science Center San Antonio, Texas
Download the new AAD Meeting Mobile AppFind the most up-to-date information at the AAD Meeting Mobile App. The app’s real-time functionality is easy to navigate and includes countless features, including the following:
Session scheduleList of sessions by day, type, category, and speaker. Bookmark sessions you like, take notes, or access session handouts.
ExhibitorsView the exhibit hall floor plan and search by name or category.Interactive maps. Explore floor plans for session rooms, events, and other areas.
EventsFind details on specific events, such as Council, Committee, or Task Force meetings, Affiliate and Reunion Groups, Industry Expert Sessions, and Industry Non-CME (INC) Programs.
Audience participationAccess Audience Response System sessions and provide feedback via your mobile device.
E-postersAccess e-posters and search by author, title, category, keyword, or poster number.
Vote Cast your ballot for AAD leadership.
NetworkFind and message colleagues to connect or stay in touch. Download the AAD Meeting Mobile App from the App Store or on Google Play. Search “AAD Meetings.” Or, visit www.aad.org/mobile. For platforms other than iOP or Android, there will be a mobile website with limited functionality. Assistance is available at the Walter E. Washington Convention Center in The Connection, Hall D.
Eat, meet, and network at the AAD Food Court
11 a.m.-2:30 p.m. Friday, Saturday, and Sunday.AAD Exhibit Floor located at the back of Hall C
International food stands offering a variety of healthy and delicious options. Ample seating available. Cash or credit accepted.
FAQs
Schedule Exhibitors
Maps
Speakers
CME/Evaluations
Event Listing SearchAudience Response
2019 AAD Annual MeetingWashington, D.C. • March 1–5, 2019
TARGET AUDIENCEThe educational design of this activity addresses the needs of dermatologists, clinical immunologists, and other clinicians involved in the treatment and management of patients with pustular psoriasis.
EDUCATIONAL OBJECTIVESAfter completing this activity, the participant should be better able to:• Describe the genetic and pathophysiologic
mechanisms that contribute to the development of pustular psoriasis including factors that have informed the development of new therapies
• Comprehensively assess patients with suspected pustular psoriasis based on clinical manifestations, diagnostic criteria, and disease severity
• Describe the mechanistic rationales and clinical evidence for current and emerging biologic therapies for the treatment of generalized pustular psoriasis and palmoplantar pustulosis
• Individualize therapeutic regimens for pustular psoriasis, with a focus on generalized disease subtypes and palmoplantar pustulosis
PROGRAM AGENDA7:00–7:10 Preactivity Questionnaire and
Faculty Introductions 7:10–7:30 Introduction to Pustular Psoriasis
Pathophysiology 7:30–7:50 Evaluating Patients With
Generalized Pustular Psoriasis or Palmoplantar Pustulosis
7:50–8:20 Evolving Therapeutic Approaches for Patients With Pustular Psoriasis
8:20–8:40 Case Study Discussion: Prerecorded Patient Examples
8:40–9:00 Postactivity Questionnaire and Q&A Session
AMERICANS WITH DISABILITIES ACT Event staff will be glad to assist you with any special needs (ie, physical, dietary, etc). Please contact Christa Master prior to the live event at [email protected] program is independent and is not part of the official AAD Annual Meeting, as planned by its Scientific Assembly Committee. This program does not qualify for continuing medical education (CME) credit.
PROGRAM OVERVIEWPustular psoriasis is a relatively rare form of psoriasis and has historically been classified into generalized and localized forms of the disease.1 Generalized pustular psoriasis is characterized by widespread sterile pustules on erythematous skin, recurrent fever, and systemic flushing and malaise.1,2 Palmoplantar pustulosis, a localized form, is characterized by erythema, pruritis, burning, and pain on the palms of the hands and soles of the feet. Recent evidence suggests that IL36RN mutations are the most common genetic aberration linked to pustular psoriasis, with the allelic frequency distinguishing generalized pustular psoriasis from palmoplantar pustulosis; the former shows a 4 to 1 increase versus the latter.3 Whether pustular psoriasis presents as localized or generalized, patients are subject to significant health risks and poor quality of life outcomes due to both skin and systemic manifestations. Patients may be subject to delays in diagnosis, in part because the disease states are relatively rare and there are little solid epidemiologic data.4 Dermatologists are faced with limited guidance on selecting therapies for patients with any of the pustular psoriasis subtypes.1 Biologic agents for pustular psoriasis and palmoplantar pustulosis are being examined in clinical trials. These include some biologics approved for psoriasis as well as agents with novel therapeutic targets, such as an anti-interleukin (IL)-36 receptor antibody.5 This Clinical Issues symposium will use both lecture and faculty discussion among leading dermatology experts to explore many of these issues, with an emphasis on evolving diagnostic and management strategies for generalized pustular psoriasis and palmoplantar pustulosis.
REFERENCES1. Robinson A, Van Voorhees AS, Hsu S, et al. Treatment of pustular
psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2012;67(2):279-288.
2. Fujita H, Terui T, Hayama K, et al. Japanese guidelines for the management and treatment of generalized pustular psoriasis: The new pathogenesis and treatment of GPP. J Dermatol. 2018;45(11):1235-1270.
3. Twelves S, Mostafa A, Dand N, et al. Clinical and genetic differences between pustular psoriasis subtypes. J Allergy Clin Immunol. 2018. [Epub ahead of print.]
4. Benjegerdes KE, Hyde K, Kivelevitch D, Mansouri B. Pustular psoriasis: pathophysiology and current treatment perspectives. Psoriasis (Auckl). 2016;6:131-144.
5. Bachelez H, Choon S, Marrakchi S, et al. Efficacy and safety of BI 655130, an anti-interleukin-36 receptor antibody, in patients with acute generalized pustular psoriasis. Abstract D3T01.1E. EADV Congress; September 12-16, 2018; Paris, France.
This activity is jointly provided by Clinical and Patient Educators Association (CPEA) and Integritas Communications.
This activity is supported by an independent educational grant from Boehringer Ingelheim.
There is no registration fee for attending this program; however, seating is limited. Preregistration does not guarantee seating. We recommend arriving at the symposium location early.
Jeffrey J. Crowley, MD, FAADBakersfield Dermatology and Skin Cancer Medical Group
Bakersfield, California
Neil J. Korman, MD, PhDProfessor of Dermatology Department of Dermatology Case Western Reserve University Director, Clinical Trials Unit Clinical DirectorMurdough Family Center for Psoriasis University Hospitals Cleveland Medical Center
Cleveland, Ohio
Abby S. Van Voorhees, MDChair, Department of Dermatology Eastern Virginia Medical School Norfolk, Virginia
Jeffrey J. CrowleyBakersfield Dermatology and Skin Cancer Medical Group
Bakersfield, California
Neil J. KormanProfessor of Dermatology Department of Dermatology Case Western Reserve University
Abby S. Van VoorheesChair, Department of Dermatology Eastern Virginia Medical School Norfolk, Virginia
2019 BI PSORIASIS NewsAd R1.indd 1 1/29/19 3:53 PM

TARGET AUDIENCEThe educational design of this activity addresses the needs of dermatologists, clinical immunologists, and other clinicians involved in the treatment and management of patients with pustular psoriasis.
EDUCATIONAL OBJECTIVESAfter completing this activity, the participant should be better able to:• Describe the genetic and pathophysiologic
mechanisms that contribute to the development of pustular psoriasis including factors that have informed the development of new therapies
• Comprehensively assess patients with suspected pustular psoriasis based on clinical manifestations, diagnostic criteria, and disease severity
• Describe the mechanistic rationales and clinical evidence for current and emerging biologic therapies for the treatment of generalized pustular psoriasis and palmoplantar pustulosis
• Individualize therapeutic regimens for pustular psoriasis, with a focus on generalized disease subtypes and palmoplantar pustulosis
PROGRAM AGENDA7:00–7:10 Preactivity Questionnaire and
Faculty Introductions 7:10–7:30 Introduction to Pustular Psoriasis
Pathophysiology 7:30–7:50 Evaluating Patients With
Generalized Pustular Psoriasis or Palmoplantar Pustulosis
7:50–8:20 Evolving Therapeutic Approaches for Patients With Pustular Psoriasis
8:20–8:40 Case Study Discussion: Prerecorded Patient Examples
8:40–9:00 Postactivity Questionnaire and Q&A Session
AMERICANS WITH DISABILITIES ACT Event staff will be glad to assist you with any special needs (ie, physical, dietary, etc). Please contact Christa Master prior to the live event at [email protected] program is independent and is not part of the official AAD Annual Meeting, as planned by its Scientific Assembly Committee. This program does not qualify for continuing medical education (CME) credit.
PROGRAM OVERVIEWPustular psoriasis is a relatively rare form of psoriasis and has historically been classified into generalized and localized forms of the disease.1 Generalized pustular psoriasis is characterized by widespread sterile pustules on erythematous skin, recurrent fever, and systemic flushing and malaise.1,2 Palmoplantar pustulosis, a localized form, is characterized by erythema, pruritis, burning, and pain on the palms of the hands and soles of the feet. Recent evidence suggests that IL36RN mutations are the most common genetic aberration linked to pustular psoriasis, with the allelic frequency distinguishing generalized pustular psoriasis from palmoplantar pustulosis; the former shows a 4 to 1 increase versus the latter.3 Whether pustular psoriasis presents as localized or generalized, patients are subject to significant health risks and poor quality of life outcomes due to both skin and systemic manifestations. Patients may be subject to delays in diagnosis, in part because the disease states are relatively rare and there are little solid epidemiologic data.4 Dermatologists are faced with limited guidance on selecting therapies for patients with any of the pustular psoriasis subtypes.1 Biologic agents for pustular psoriasis and palmoplantar pustulosis are being examined in clinical trials. These include some biologics approved for psoriasis as well as agents with novel therapeutic targets, such as an anti-interleukin (IL)-36 receptor antibody.5 This Clinical Issues symposium will use both lecture and faculty discussion among leading dermatology experts to explore many of these issues, with an emphasis on evolving diagnostic and management strategies for generalized pustular psoriasis and palmoplantar pustulosis.
REFERENCES1. Robinson A, Van Voorhees AS, Hsu S, et al. Treatment of pustular
psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2012;67(2):279-288.
2. Fujita H, Terui T, Hayama K, et al. Japanese guidelines for the management and treatment of generalized pustular psoriasis: The new pathogenesis and treatment of GPP. J Dermatol. 2018;45(11):1235-1270.
3. Twelves S, Mostafa A, Dand N, et al. Clinical and genetic differences between pustular psoriasis subtypes. J Allergy Clin Immunol. 2018. [Epub ahead of print.]
4. Benjegerdes KE, Hyde K, Kivelevitch D, Mansouri B. Pustular psoriasis: pathophysiology and current treatment perspectives. Psoriasis (Auckl). 2016;6:131-144.
5. Bachelez H, Choon S, Marrakchi S, et al. Efficacy and safety of BI 655130, an anti-interleukin-36 receptor antibody, in patients with acute generalized pustular psoriasis. Abstract D3T01.1E. EADV Congress; September 12-16, 2018; Paris, France.
This activity is jointly provided by Clinical and Patient Educators Association (CPEA) and Integritas Communications.
This activity is supported by an independent educational grant from Boehringer Ingelheim.
There is no registration fee for attending this program; however, seating is limited. Preregistration does not guarantee seating. We recommend arriving at the symposium location early.
Jeffrey J. Crowley, MD, FAADBakersfield Dermatology and Skin Cancer Medical Group
Bakersfield, California
Neil J. Korman, MD, PhDProfessor of Dermatology Department of Dermatology Case Western Reserve University Director, Clinical Trials Unit Clinical DirectorMurdough Family Center for Psoriasis University Hospitals Cleveland Medical Center
Cleveland, Ohio
Abby S. Van Voorhees, MDChair, Department of Dermatology Eastern Virginia Medical School Norfolk, Virginia
Jeffrey J. CrowleyBakersfield Dermatology and Skin Cancer Medical Group
Bakersfield, California
Neil J. KormanProfessor of Dermatology Department of Dermatology Case Western Reserve University
Abby S. Van VoorheesChair, Department of Dermatology Eastern Virginia Medical School Norfolk, Virginia
2019 BI PSORIASIS NewsAd R1.indd 1 1/29/19 3:53 PM

PREPARED BY FCB
Job #: 11101394Releasing as: PDFx1a Production: Debi Post X2844
Colors: 4C AD: [email protected]
Client: Dermira Bleed: 21" x 14.25" AE: Tyler Byrne
Product: Qbrexza Finished Size: 10.375" x 14" Producer: Hakeem Williams
Client Code: PM-US-QBR-0349 Trim/Final: 20.75" x 14" QC: L.Powell
Date: February 5, 2019 4:08 PM Live/Safety: 20.25" x 13.50"h Digital Artist: tp, VA, tp, VA, tp, VA, lp
Proof: M7 Add’l Info: .25 gutter each sideFR Spellcheck: P. Stoopack
Path: PrePress:Dermira:11101394:11101394_AAD_Ann_Mtg_News_M7
4C AAD Annual Meeting News Daily
For patients aged 9 years and older with primary axillary hyperhidrosis
Once-daily QBREXZA is the first and only FDA-approved, topical anticholinergic cloth towelette1
©2019 Dermira, Inc. All rights reserved. PM-US-QBR-0349 01/2019
Reference: 1. QBREXZA™ (glycopyrronium) cloth prescribing information, Dermira.
QBREXZA.com/HCP
Discover
Visit Booth #415
March 2, 2019 at 2:45 PM | Industry Experts Theater | Booth #002
Come Join Our Industry Expert Session and Raise the Bar for Your Patients With Primary Axillary Hyperhidrosis
INDICATION QBREXZATM (glycopyrronium) cloth is an anticholinergic indicated for topical treatment of primary axillary hyperhidrosis in adult and pediatric patients 9 years of age and older.
IMPORTANT SAFETY INFORMATION Contraindications: QBREXZA is contraindicated in patients with medical conditions that can be exacerbated by the anticholinergic effect of QBREXZA (e.g., glaucoma, paralytic ileus, unstable cardiovascular status in acute hemorrhage, severe ulcerative colitis, toxic megacolon complicating ulcerative colitis, myasthenia gravis, Sjogren’s syndrome).
WARNINGS AND PRECAUTIONSWorsening of Urinary Retention: QBREXZA should be used with caution in patients with a history or presence of documented urinary retention. Prescribers and patients should be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder), especially in patients with prostatic hypertrophy or bladder-neck obstruction. Instruct patients to discontinue use immediately and consult a physician should any of these signs or symptoms develop. Patients with a history of urinary retention were not included in the clinical studies.
Control of Body Temperature: In the presence of high ambient temperature, heat illness (hyperpyrexia and heat stroke due to decreased sweating) can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
Operating Machinery or an Automobile: Transient blurred vision may occur with use of QBREXZA. If blurred vision occurs, the patient should discontinue use until symptoms resolve. Patients should be warned not to engage in activities that require clear vision such as operating a motor vehicle or other machinery, or performing hazardous work until the symptoms have resolved.
ADVERSE REACTIONSThe most common adverse reactions seen in ≥2% of subjects treated with QBREXZA were dry mouth (24.2%), mydriasis (6.8%), oropharyngeal pain (5.7%), headache (5.0%), urinary hesitation (3.5%), vision blurred (3.5%), nasal dryness (2.6%), dry throat
(2.6%), dry eye (2.4%), dry skin (2.2%) and constipation (2.0%). Local skin reactions, including erythema (17.0%), burning/stinging (14.1%) and pruritus (8.1%) were also common.
DRUG INTERACTIONSAnticholinergics: Coadministration of QBREXZA with anticholinergic medications may result in additive interaction leading to an increase in anticholinergic adverse effects. Avoid coadministration of QBREXZA with other anticholinergic-containing drugs.
INSTRUCTIONS FOR ADMINISTERING QBREXZAInstruct patients to use one cloth to apply QBREXZA to both axillae by wiping the cloth across one underarm, ONE TIME. Using the same cloth, apply the medication to the other underarm, ONE TIME. Inform patients that QBREXZA can cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes.
Instruct patients to wash their hands with soap and water immediately after discarding the used cloth.
USE IN SPECIFIC POPULATIONSPregnancy: There are no available data on QBREXZA use in pregnant women to inform a drug-associated risk for adverse developmental outcomes.
Lactation: There are no data on the presence of glycopyrrolate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for QBREXZA and any potential adverse effects on the breastfed infant from QBREXZA or from the underlying maternal condition.
Renal Impairment: The elimination of glycopyrronium is severely impaired in patients with renal failure.
Please see Brief Summary of Full Prescribing Information on adjacent page.
QBREXZATM (glycopyrronium) cloth, 2.4%, for topical useThe following is a Brief Summary; refer to Full Prescribing Information for complete product information.
1 INDICATIONS AND USAGEQBREXZA is indicated for topical treatment of primary axillary hyperhidrosis in adult and pediatric patients 9 years of age and older.
2 DOSAGE AND ADMINISTRATION
For topical use only.
QBREXZA is for topical use in the underarm area only and not for use in other body areas.
QBREXZA is administered by a single-use pre-moistened cloth packaged in individual pouches. QBREXZA should be applied to clean dry skin on the underarm areas only. QBREXZA should not be used more frequently than once every 24 hours.
Tear open the pouch and pull out the cloth, unfold the cloth, and wipe it across one entire underarm once. Using the same cloth, wipe the other underarm once. A single cloth should be used to apply QBREXZA to both underarms.
Wash hands immediately with soap and water after applying and discarding the QBREXZA cloth. QBREXZA may cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes. Avoid transfer of QBREXZA to the periocular area [see Warnings and Precautions (5.3)].
Do not apply QBREXZA to broken skin. Avoid using QBREXZA with occlusive dressings.
4 CONTRAINDICATIONS
QBREXZA is contraindicated in patients with medical conditions that can be exacerbated by the anticholinergic effect of QBREXZA (e.g, glaucoma, paralytic ileus, unstable cardiovascular status in acute hemorrhage, severe ulcerative colitis, toxic megacolon complicating ulcerative colitis, myasthenia gravis, Sjogren’s syndrome).
5 WARNINGS AND PRECAUTIONS5.1 Worsening of Urinary Retention QBREXZA should be used with caution in patients with a history or presence of documented urinary retention. Prescribers and patients should be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder), especially in patients with prostatic hyperplasia or bladder-neck obstruction. Instruct patients to discontinue use immediately and consult a physician should any of these signs or symptoms develop.
Patients with a history of urinary retention were not included in the clinical studies.
5.2 Control of Body Temperature In the presence of high ambient temperature, heat illness (hyperpyrexia and heat stroke due to decreased sweating) can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
5.3 Operating Machinery or an AutomobileTransient blurred vision may occur with use of QBREXZA. If blurred vision occurs, the patient should discontinue use until symptoms resolve. Patients should be warned not to engage in activities that require clear vision such as operating a motor vehicle or other machinery, or performing hazardous work until the symptoms have resolved.
6 ADVERSE REACTIONS
The following adverse reactions are described in greater detail in other sections • Worsening of Urinary Retention [see Warnings and Precautions (5.1)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In two double-blind, vehicle-controlled clinical trials (Trial 1 [NCT02530281] and Trial 2 [NCT02530294]) of 459 subjects treated with QBREXZA once daily and 232 treated with vehicle, subjects were 9 to 76 years of age, 47% male, and the percentages of White, Black (including African Americans), and Asian subjects were 82%, 12%, and 1%, respectively.
Table 1 summarizes the most frequent adverse reactions (≥2%) in subjects with primary axillary hyperhidrosis treated with QBREXZA.
Table 1: Adverse Reactions Occurring in ≥2% of Subjects
Adverse ReactionsQBREXZA (N=459)
n (%)
Vehicle (N=232)
n (%)
Dry mouth 111 (24.2%) 13 (5.6%)
Mydriasis 31 (6.8%) 0
Oropharyngeal pain 26 (5.7%) 3 (1.3%)
Headache 23 (5.0%) 5 (2.2%)
Urinary hesitation 16 (3.5%) 0
Vision blurred 16 (3.5%) 0
Nasal dryness 12 (2.6%) 1 (0.4%)
Dry throat 12 (2.6%) 0
Dry eye 11 (2.4%) 1 (0.4%)
Dry skin 10 (2.2%) 0
Constipation 9 (2.0%) 0
Table 2 shows the most frequently reported local skin reactions, which were relatively common in both the QBREXZA and vehicle groups.
Table 2: Local Skin Reactions
Local Skin ReactionsQBREXZA (N=454)a
n (%)
Vehicle (N=231) a
n (%)
Erythema 77 (17.0%) 39 (16.9%)
Burning/stinging 64 (14.1%) 39 (16.9%)
Pruritus 37 (8.1%) 14 (6.1%)
aPatients with a post-baseline local skin reaction assessment
In an open-label safety trial (NCT02553798), 564 subjects were treated for up to an additional 44 weeks after completing Trial 1 or Trial 2. Adverse reactions occurring at a frequency ≥2.0% were: dry mouth (16.9%), vision blurred (6.7%), nasopharyngitis (5.8%), mydriasis (5.3%), urinary hesitation (4.2%), nasal dryness (3.6%), dry eye (2.9%), pharyngitis (2.2%), and application site reactions (pain [6.4%], dermatitis [3.8%], pruritus [3.8%], rash [3.8%], erythema [2.4%]).
7 DRUG INTERACTIONS7.1 AnticholinergicsCoadministration of QBREXZA with anticholinergic medications may result in additive interaction leading to an increase in anticholinergic adverse effects [see Warnings and Precautions (5) and Adverse Reactions (6)]. Avoid coadministration of QBREXZA with other anticholinergic-containing drugs.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyThere are no available data on QBREXZA use in pregnant women to inform a drug-associated risk for adverse developmental outcomes. In pregnant rats, daily oral administration of glycopyrrolate (glycopyrronium bromide) during organogenesis did not result in an increased incidence of gross external or visceral defects. When glycopyrrolate was administered intravenously to pregnant rabbits during organogenesis, no adverse effects on embryo-fetal development were seen. The available data do not support relevant comparisons of systemic glycopyrronium exposures achieved in the animal studies to exposures observed in humans after topical use of QBREXZA.
The estimated background risks of major birth defects and miscarriage for the indicated population are unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
8.2 LactationThere are no data on the presence of glycopyrrolate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for QBREXZA and any potential adverse effects on the breastfed infant from QBREXZA or from the underlying maternal condition.
8.4 Pediatric UseThe safety, effectiveness and pharmacokinetics of QBREXZA have been established in pediatric patients age 9 years and older for topical treatment of primary axillary hyperhidrosis. Use of QBREXZA in this age group is supported by evidence from two multicenter, randomized, double-blind, parallel-group, vehicle-controlled 4-week trials which included 34 pediatric subjects 9 years and older [see Adverse Reactions (6.1)]. The safety and effectiveness of QBREXZA have not been established in pediatric patients under 9 years of age.
8.5 Geriatric UseClinical trials of QBREXZA did not include sufficient numbers of subjects age 65 years and older to determine whether they respond differently from younger subjects.
8.6 Renal ImpairmentThe elimination of glycopyrronium is severely impaired in patients with renal failure.
10 OVERDOSAGE
Because glycopyrronium is a quaternary amine which does not easily cross the blood-brain barrier, symptoms of glycopyrronium overdosage are generally more peripheral in nature rather than central compared to other anticholinergic agents. Associated signs and symptoms related to excessive anticholinergic activity may include flushing, hyperthermia, tachycardia, ileus, urinary retention, loss of ocular accommodation and light sensitivity due to mydriasis.
In the case of overdose when symptoms are severe or life threatening, therapy may include:
• Managing per standard of care any acute conditions such as hyperthermia, coma, and/or seizures, as applicable, and managing any myoclonic or choreoathetoid movements which may lead to rhabdomyolysis in some cases of anticholinergic overdosage
• Managing severe urinary retention with catheterization if not spontaneously reversed within several hours
• Providing cardiovascular support and/or controlling arrhythmias
• Maintaining an open airway, providing ventilation as necessary
• Administering a quaternary ammonium anticholinesterase such as neostigmine to help alleviate severe and/or life threatening peripheral anticholinergic effects.
Topical overdosing of QBREXZA could result in an increased incidence or severity of local skin reactions. Administration of QBREXZA under occlusive conditions may result in an increase in anticholinergic effects, including dry mouth and urinary hesitation.
16.2 Storage and HandlingStore at room temperature 20° - 25°C (68° - 77°F); excursions permitted to 15° - 30°C (59° - 86°F) [See USP Controlled Room Temperature].
QBREXZA is flammable; keep away from heat or flame.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Worsening of Urinary Retention Instruct patients to be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder). Instruct patients to discontinue use and consult a physician immediately should any of these signs or symptoms develop.
Control of Body Temperature (Risk of Overheating or Heat Illness) In the presence of high ambient temperature, heat illness due to decreased sweating can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
Operating Machinery or an Automobile Transient blurred vision may occur with QBREXZA. If this occurs, instruct patients to contact their healthcare provider, discontinue use of QBREXZA and avoid operating a motor vehicle or other machinery, or performing hazardous work until symptoms resolve.
Instructions for Administering QBREXZA It is important for patients to understand how to correctly apply QBREXZA (see Patient Information).
• Instruct patients to use one cloth to apply QBREXZA to both axillae by wiping the cloth across one underarm, ONE TIME.
• Using the same cloth, apply the medication to the other underarm, ONE TIME.
• Inform patients that QBREXZA can cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes.
• Instruct patients to wash their hands with soap and water immediately after discarding the used cloth.
• Remind patients not to apply QBREXZA to other body areas or to broken skin. Instruct patients to avoid using QBREXZA with occlusive dressings.
• QBREXZA is flammable; avoid use near heat or flame.
Manufactured for:
Dermira, Inc. Menlo Park, CA 94025
Version 1, June 2018
PM-US-QBR-0029
S:20.25”
S:13.5”
T:20.75”
T:14”
B:21”
B:14.25”
F:10.375”
FS:9.875”
F:10.375”
FS:9.875”
11101394_AAD_Ann_Mtg_News_M7.indd 1 2/5/19 4:08 PM

PREPARED BY FCB
Job #: 11101394Releasing as: PDFx1a Production: Debi Post X2844
Colors: 4C AD: [email protected]
Client: Dermira Bleed: 21" x 14.25" AE: Tyler Byrne
Product: Qbrexza Finished Size: 10.375" x 14" Producer: Hakeem Williams
Client Code: PM-US-QBR-0349 Trim/Final: 20.75" x 14" QC: L.Powell
Date: February 5, 2019 4:08 PM Live/Safety: 20.25" x 13.50"h Digital Artist: tp, VA, tp, VA, tp, VA, lp
Proof: M7 Add’l Info: .25 gutter each sideFR Spellcheck: P. Stoopack
Path: PrePress:Dermira:11101394:11101394_AAD_Ann_Mtg_News_M7
4C AAD Annual Meeting News Daily
For patients aged 9 years and older with primary axillary hyperhidrosis
Once-daily QBREXZA is the first and only FDA-approved, topical anticholinergic cloth towelette1
©2019 Dermira, Inc. All rights reserved. PM-US-QBR-0349 01/2019
Reference: 1. QBREXZA™ (glycopyrronium) cloth prescribing information, Dermira.
QBREXZA.com/HCP
Discover
Visit Booth #415
March 2, 2019 at 2:45 PM | Industry Experts Theater | Booth #002
Come Join Our Industry Expert Session and Raise the Bar for Your Patients With Primary Axillary Hyperhidrosis
INDICATION QBREXZATM (glycopyrronium) cloth is an anticholinergic indicated for topical treatment of primary axillary hyperhidrosis in adult and pediatric patients 9 years of age and older.
IMPORTANT SAFETY INFORMATION Contraindications: QBREXZA is contraindicated in patients with medical conditions that can be exacerbated by the anticholinergic effect of QBREXZA (e.g., glaucoma, paralytic ileus, unstable cardiovascular status in acute hemorrhage, severe ulcerative colitis, toxic megacolon complicating ulcerative colitis, myasthenia gravis, Sjogren’s syndrome).
WARNINGS AND PRECAUTIONSWorsening of Urinary Retention: QBREXZA should be used with caution in patients with a history or presence of documented urinary retention. Prescribers and patients should be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder), especially in patients with prostatic hypertrophy or bladder-neck obstruction. Instruct patients to discontinue use immediately and consult a physician should any of these signs or symptoms develop. Patients with a history of urinary retention were not included in the clinical studies.
Control of Body Temperature: In the presence of high ambient temperature, heat illness (hyperpyrexia and heat stroke due to decreased sweating) can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
Operating Machinery or an Automobile: Transient blurred vision may occur with use of QBREXZA. If blurred vision occurs, the patient should discontinue use until symptoms resolve. Patients should be warned not to engage in activities that require clear vision such as operating a motor vehicle or other machinery, or performing hazardous work until the symptoms have resolved.
ADVERSE REACTIONSThe most common adverse reactions seen in ≥2% of subjects treated with QBREXZA were dry mouth (24.2%), mydriasis (6.8%), oropharyngeal pain (5.7%), headache (5.0%), urinary hesitation (3.5%), vision blurred (3.5%), nasal dryness (2.6%), dry throat
(2.6%), dry eye (2.4%), dry skin (2.2%) and constipation (2.0%). Local skin reactions, including erythema (17.0%), burning/stinging (14.1%) and pruritus (8.1%) were also common.
DRUG INTERACTIONSAnticholinergics: Coadministration of QBREXZA with anticholinergic medications may result in additive interaction leading to an increase in anticholinergic adverse effects. Avoid coadministration of QBREXZA with other anticholinergic-containing drugs.
INSTRUCTIONS FOR ADMINISTERING QBREXZAInstruct patients to use one cloth to apply QBREXZA to both axillae by wiping the cloth across one underarm, ONE TIME. Using the same cloth, apply the medication to the other underarm, ONE TIME. Inform patients that QBREXZA can cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes.
Instruct patients to wash their hands with soap and water immediately after discarding the used cloth.
USE IN SPECIFIC POPULATIONSPregnancy: There are no available data on QBREXZA use in pregnant women to inform a drug-associated risk for adverse developmental outcomes.
Lactation: There are no data on the presence of glycopyrrolate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for QBREXZA and any potential adverse effects on the breastfed infant from QBREXZA or from the underlying maternal condition.
Renal Impairment: The elimination of glycopyrronium is severely impaired in patients with renal failure.
Please see Brief Summary of Full Prescribing Information on adjacent page.
QBREXZATM (glycopyrronium) cloth, 2.4%, for topical useThe following is a Brief Summary; refer to Full Prescribing Information for complete product information.
1 INDICATIONS AND USAGEQBREXZA is indicated for topical treatment of primary axillary hyperhidrosis in adult and pediatric patients 9 years of age and older.
2 DOSAGE AND ADMINISTRATION
For topical use only.
QBREXZA is for topical use in the underarm area only and not for use in other body areas.
QBREXZA is administered by a single-use pre-moistened cloth packaged in individual pouches. QBREXZA should be applied to clean dry skin on the underarm areas only. QBREXZA should not be used more frequently than once every 24 hours.
Tear open the pouch and pull out the cloth, unfold the cloth, and wipe it across one entire underarm once. Using the same cloth, wipe the other underarm once. A single cloth should be used to apply QBREXZA to both underarms.
Wash hands immediately with soap and water after applying and discarding the QBREXZA cloth. QBREXZA may cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes. Avoid transfer of QBREXZA to the periocular area [see Warnings and Precautions (5.3)].
Do not apply QBREXZA to broken skin. Avoid using QBREXZA with occlusive dressings.
4 CONTRAINDICATIONS
QBREXZA is contraindicated in patients with medical conditions that can be exacerbated by the anticholinergic effect of QBREXZA (e.g, glaucoma, paralytic ileus, unstable cardiovascular status in acute hemorrhage, severe ulcerative colitis, toxic megacolon complicating ulcerative colitis, myasthenia gravis, Sjogren’s syndrome).
5 WARNINGS AND PRECAUTIONS5.1 Worsening of Urinary Retention QBREXZA should be used with caution in patients with a history or presence of documented urinary retention. Prescribers and patients should be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder), especially in patients with prostatic hyperplasia or bladder-neck obstruction. Instruct patients to discontinue use immediately and consult a physician should any of these signs or symptoms develop.
Patients with a history of urinary retention were not included in the clinical studies.
5.2 Control of Body Temperature In the presence of high ambient temperature, heat illness (hyperpyrexia and heat stroke due to decreased sweating) can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
5.3 Operating Machinery or an AutomobileTransient blurred vision may occur with use of QBREXZA. If blurred vision occurs, the patient should discontinue use until symptoms resolve. Patients should be warned not to engage in activities that require clear vision such as operating a motor vehicle or other machinery, or performing hazardous work until the symptoms have resolved.
6 ADVERSE REACTIONS
The following adverse reactions are described in greater detail in other sections • Worsening of Urinary Retention [see Warnings and Precautions (5.1)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In two double-blind, vehicle-controlled clinical trials (Trial 1 [NCT02530281] and Trial 2 [NCT02530294]) of 459 subjects treated with QBREXZA once daily and 232 treated with vehicle, subjects were 9 to 76 years of age, 47% male, and the percentages of White, Black (including African Americans), and Asian subjects were 82%, 12%, and 1%, respectively.
Table 1 summarizes the most frequent adverse reactions (≥2%) in subjects with primary axillary hyperhidrosis treated with QBREXZA.
Table 1: Adverse Reactions Occurring in ≥2% of Subjects
Adverse ReactionsQBREXZA (N=459)
n (%)
Vehicle (N=232)
n (%)
Dry mouth 111 (24.2%) 13 (5.6%)
Mydriasis 31 (6.8%) 0
Oropharyngeal pain 26 (5.7%) 3 (1.3%)
Headache 23 (5.0%) 5 (2.2%)
Urinary hesitation 16 (3.5%) 0
Vision blurred 16 (3.5%) 0
Nasal dryness 12 (2.6%) 1 (0.4%)
Dry throat 12 (2.6%) 0
Dry eye 11 (2.4%) 1 (0.4%)
Dry skin 10 (2.2%) 0
Constipation 9 (2.0%) 0
Table 2 shows the most frequently reported local skin reactions, which were relatively common in both the QBREXZA and vehicle groups.
Table 2: Local Skin Reactions
Local Skin ReactionsQBREXZA (N=454)a
n (%)
Vehicle (N=231) a
n (%)
Erythema 77 (17.0%) 39 (16.9%)
Burning/stinging 64 (14.1%) 39 (16.9%)
Pruritus 37 (8.1%) 14 (6.1%)
aPatients with a post-baseline local skin reaction assessment
In an open-label safety trial (NCT02553798), 564 subjects were treated for up to an additional 44 weeks after completing Trial 1 or Trial 2. Adverse reactions occurring at a frequency ≥2.0% were: dry mouth (16.9%), vision blurred (6.7%), nasopharyngitis (5.8%), mydriasis (5.3%), urinary hesitation (4.2%), nasal dryness (3.6%), dry eye (2.9%), pharyngitis (2.2%), and application site reactions (pain [6.4%], dermatitis [3.8%], pruritus [3.8%], rash [3.8%], erythema [2.4%]).
7 DRUG INTERACTIONS7.1 AnticholinergicsCoadministration of QBREXZA with anticholinergic medications may result in additive interaction leading to an increase in anticholinergic adverse effects [see Warnings and Precautions (5) and Adverse Reactions (6)]. Avoid coadministration of QBREXZA with other anticholinergic-containing drugs.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyThere are no available data on QBREXZA use in pregnant women to inform a drug-associated risk for adverse developmental outcomes. In pregnant rats, daily oral administration of glycopyrrolate (glycopyrronium bromide) during organogenesis did not result in an increased incidence of gross external or visceral defects. When glycopyrrolate was administered intravenously to pregnant rabbits during organogenesis, no adverse effects on embryo-fetal development were seen. The available data do not support relevant comparisons of systemic glycopyrronium exposures achieved in the animal studies to exposures observed in humans after topical use of QBREXZA.
The estimated background risks of major birth defects and miscarriage for the indicated population are unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
8.2 LactationThere are no data on the presence of glycopyrrolate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for QBREXZA and any potential adverse effects on the breastfed infant from QBREXZA or from the underlying maternal condition.
8.4 Pediatric UseThe safety, effectiveness and pharmacokinetics of QBREXZA have been established in pediatric patients age 9 years and older for topical treatment of primary axillary hyperhidrosis. Use of QBREXZA in this age group is supported by evidence from two multicenter, randomized, double-blind, parallel-group, vehicle-controlled 4-week trials which included 34 pediatric subjects 9 years and older [see Adverse Reactions (6.1)]. The safety and effectiveness of QBREXZA have not been established in pediatric patients under 9 years of age.
8.5 Geriatric UseClinical trials of QBREXZA did not include sufficient numbers of subjects age 65 years and older to determine whether they respond differently from younger subjects.
8.6 Renal ImpairmentThe elimination of glycopyrronium is severely impaired in patients with renal failure.
10 OVERDOSAGE
Because glycopyrronium is a quaternary amine which does not easily cross the blood-brain barrier, symptoms of glycopyrronium overdosage are generally more peripheral in nature rather than central compared to other anticholinergic agents. Associated signs and symptoms related to excessive anticholinergic activity may include flushing, hyperthermia, tachycardia, ileus, urinary retention, loss of ocular accommodation and light sensitivity due to mydriasis.
In the case of overdose when symptoms are severe or life threatening, therapy may include:
• Managing per standard of care any acute conditions such as hyperthermia, coma, and/or seizures, as applicable, and managing any myoclonic or choreoathetoid movements which may lead to rhabdomyolysis in some cases of anticholinergic overdosage
• Managing severe urinary retention with catheterization if not spontaneously reversed within several hours
• Providing cardiovascular support and/or controlling arrhythmias
• Maintaining an open airway, providing ventilation as necessary
• Administering a quaternary ammonium anticholinesterase such as neostigmine to help alleviate severe and/or life threatening peripheral anticholinergic effects.
Topical overdosing of QBREXZA could result in an increased incidence or severity of local skin reactions. Administration of QBREXZA under occlusive conditions may result in an increase in anticholinergic effects, including dry mouth and urinary hesitation.
16.2 Storage and HandlingStore at room temperature 20° - 25°C (68° - 77°F); excursions permitted to 15° - 30°C (59° - 86°F) [See USP Controlled Room Temperature].
QBREXZA is flammable; keep away from heat or flame.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Worsening of Urinary Retention Instruct patients to be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, distended bladder). Instruct patients to discontinue use and consult a physician immediately should any of these signs or symptoms develop.
Control of Body Temperature (Risk of Overheating or Heat Illness) In the presence of high ambient temperature, heat illness due to decreased sweating can occur with the use of anticholinergic drugs such as QBREXZA. Advise patients using QBREXZA to watch for generalized lack of sweating when in hot or very warm environmental temperatures and to avoid use if not sweating under these conditions.
Operating Machinery or an Automobile Transient blurred vision may occur with QBREXZA. If this occurs, instruct patients to contact their healthcare provider, discontinue use of QBREXZA and avoid operating a motor vehicle or other machinery, or performing hazardous work until symptoms resolve.
Instructions for Administering QBREXZA It is important for patients to understand how to correctly apply QBREXZA (see Patient Information).
• Instruct patients to use one cloth to apply QBREXZA to both axillae by wiping the cloth across one underarm, ONE TIME.
• Using the same cloth, apply the medication to the other underarm, ONE TIME.
• Inform patients that QBREXZA can cause temporary dilation of the pupils and blurred vision if it comes in contact with the eyes.
• Instruct patients to wash their hands with soap and water immediately after discarding the used cloth.
• Remind patients not to apply QBREXZA to other body areas or to broken skin. Instruct patients to avoid using QBREXZA with occlusive dressings.
• QBREXZA is flammable; avoid use near heat or flame.
Manufactured for:
Dermira, Inc. Menlo Park, CA 94025
Version 1, June 2018
PM-US-QBR-0029
S:20.25”S:13.5”
T:20.75”T:14”
B:21”B:14.25”
F:10.375”
FS:9.875”
F:10.375”
FS:9.875”
11101394_AAD_Ann_Mtg_News_M7.indd 1 2/5/19 4:08 PM

12 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
Brought to you byBe the first to know. Find out more at
www.SkyriziHCP.com
©2019 AbbVie Inc. North Chicago, IL 60064 US-RISN-180097 March 2019 Printed in U.S.A.
SOMETHING NEWIS APPROACHINGIS APPROACHING
Brought to you byBe the first to know. Find out more atBe the first to know. Find out more atBe the first to know. Find out more at
www.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.com
EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111
US-RISN-180097_M03_Map_Premium_Coming Soon Ad.indd 1 1/15/19 12:59 PM
Shaping AI for dermatologyN ew technologies and
techniques are changing melanoma diagnosis and
treatment. Noninvasive biopsies, augmented intelligence (AI), novel detection strategies, and other technologies that sound like clinical dreams are already changing practice. This technological shift is as important as the paradigm shifts that followed the introduction of Mohs surgery and immunohistochemical staining in dermatology and skin cancer.
“Melanoma is the most deadly cancer in the sense that more life years are lost to it than to any other cancer,” said Eric Tkaczyk, MD, PhD, assistant professor of dermatology and of biomedical engineering at Vanderbilt University and director of the Vanderbilt Cutaneous Imaging Clinic. “Anyone can get it at any age. It is the flag that the entire community of dermatology gathers around because early diagnosis saves so many lives.”
Dr. Tkaczyk is among the presenters at Friday’s “Melanoma: The Future Is Now.” On Saturday, the session, “Predicting the Future: AI, Machine Learning, and Dermatology” adds more perspective.
Current data suggests AI is equal or better at diagnosing melanoma than most dermatologists. In 2018,
the third Grand Challenge, sponsored by the International Skin Imaging Collaboration unveiled algorithms that can diagnose melanoma and six other types of skin cancers using skin images more accurately than 97% of expert dermatologist readers.
But don’t worry. More patients will be driven to see dermatologists“The reality is that the more computers can diagnose, the more people will be driven to see dermatologists, not fewer. The role of the dermatologist may change, but rather than being usurped, our role will be augmented,” said Allan C. Halpern, MD, chief of dermatology at Memorial Sloan Kettering Cancer Center. He is president of the ISIC.
Dermatologists who worry they may be replaced by apps should agonize less about the perceived threat and consider the opportunities that AI presents.
“We should embrace AI and help shape the changing environment, mold it in ways that benefit our patients and improve treatment,” said Roger S. Ho, MD, MS, MPH, assistant professor of dermatology at the Ronald O. Perelman Department of Dermatology at New York University School of Medicine.
One of the ways to shape AI is to help train dermatology algorithms so they can diagnose more accurately in more skin types. The problem is limited data sets.
What can the data tell dermatologists?“You use a data set to teach the algorithm what is right and what is wrong, what is melanoma and what is not melanoma. If the data set is biased, say the majority of tumors are in light skin, the algorithm may miss potentially life-threatening tumors when presented with darker skin types,” said Adewole Adamson, MD, MPP, assistant professor of dermatology at Dell Medical School at the University of Texas at Austin.
AI engineers may not know enough about dermatology to recognize or remedy the problem. That’s where dermatologists help, says Clara Curiel-Lewandrowski, MD, professor of medicine and dermatology at the University
of Arizona, director of the University Cutaneous Oncology Program, clinical director of the Skin Cancer Institute, and Alan and Janice Levin endowed chair in Cancer Research.
Responsibility lies with dermatologists“As dermatologists we have the responsibility to lead the development and adoption of AI-based technologies into our field. It is up to us to transform the implementation of AI into an opportunity, not a threat, and to ultimately augment our clinical practice,” Dr. Curiel-Lewandrowski said.
“Melanoma: The Future is Now” (S001)Friday, 9 a.m.-12 p.m.Room 204A
“Predicting the Future: AI, Machine Learning and Dermatology” (D004)Saturday, 3:30-5:30 p.m.Room 101
New imaging technologiesNew technologies and techniques are changing melanoma diagnosis and treatment.
Confocal microscopy: Reflectance confocal microscopy uses laser illumination to visualize cellular details of the superficial dermis and epidermis in real time.
Photoacoustics: A combination of sound and light frequencies.
Raman spectroscopy: Lesion identification based on its molecular makeup.
Molecular assays: Determining which genes are upregulated to predict tumor behavior via DecisionDx-Melanoma assays mRNA within a tumor.
Augmented intelligence: SkinVision is among the early commercial apps to diagnose skin cancer.
We should embrace AI and help shape the changing environment, mold it in ways that benefit our patients and improve treatment.
Roger S. Ho, MD, MS, MPH

Brought to you byBe the first to know. Find out more at
www.SkyriziHCP.com
©2019 AbbVie Inc. North Chicago, IL 60064 US-RISN-180097 March 2019 Printed in U.S.A.
SOMETHING NEWIS APPROACHINGIS APPROACHING
Brought to you byBe the first to know. Find out more atBe the first to know. Find out more atBe the first to know. Find out more at
www.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.comwww.SkyriziHCP.com
EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111EXPERIENCE THE SKY AT BOOTH #2111
US-RISN-180097_M03_Map_Premium_Coming Soon Ad.indd 1 1/15/19 12:59 PM
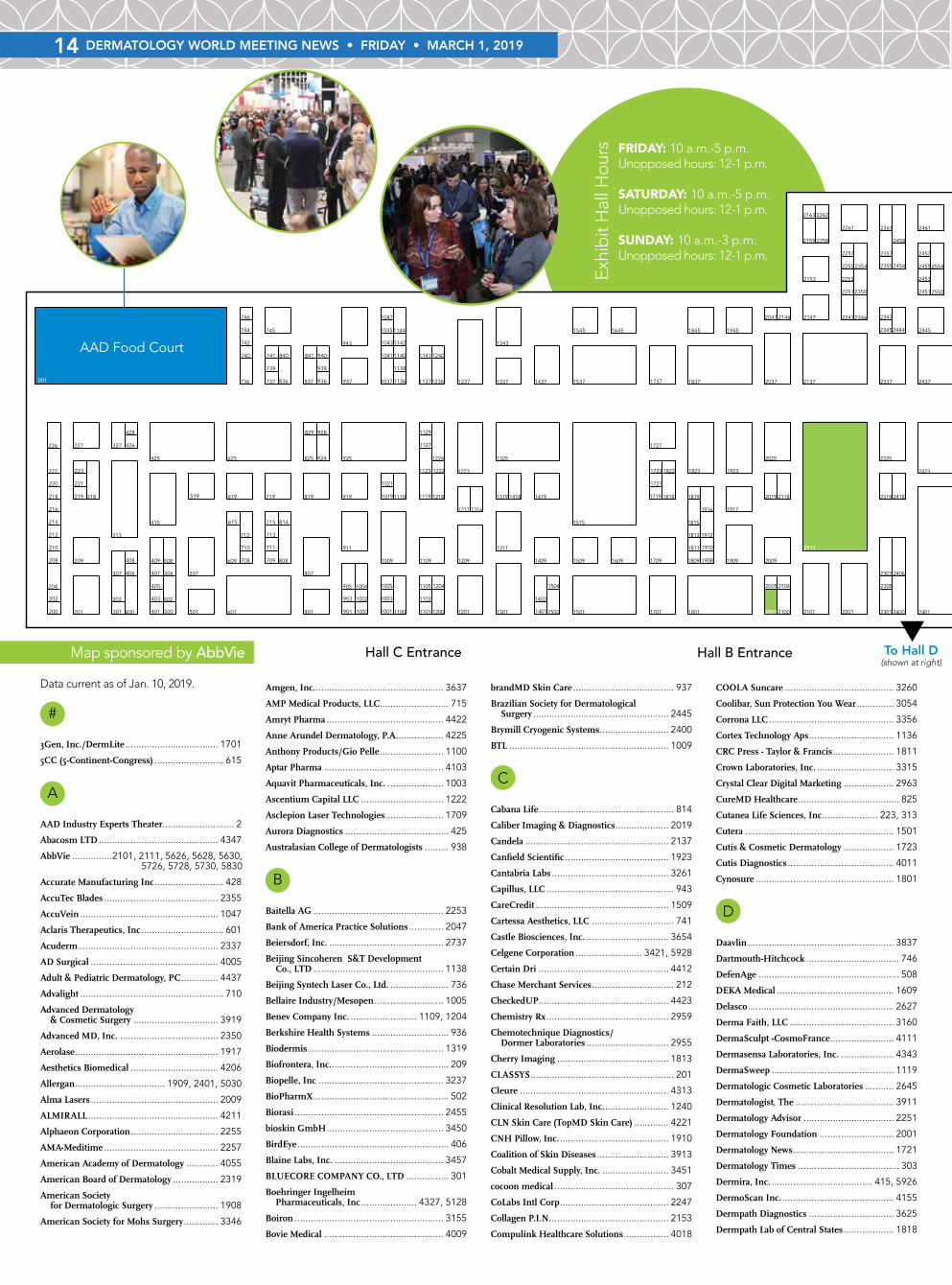
14 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
001
1000 1001
1002 1003
1004 1005
1009
1019
1021
1037
1041
1043
1045
1047
1100 1101
1103
1105
1109
1118 1119
1123
1127
1129
1136 1137
1138
1140 1141
1142
1144
1200 1201
1204
1209
1217
1218
1222 1223
1224
1236 1237
1240
1301
1311
1316
1319
1325
1337
1343
1401
1403
1409
1418 1419
1437
1500 1501
1504
1509
1515
1537
1545
1609
1645
1701
1709
1719
1721
1723
1727
1737
1801
1809
1811
1813
1815
1818 1819
1822 1823
1837
1845
1908 1909
1910
1912
1916 1917
1923
1945
200 2001
2005
2009
201
2019
202
2025
2037
204
2047
208 209
210
2100 2101
2104
2111
2118
212
2137
214
2146 2147
2153
2159
216
2163
218 219
220
2201
221
222 223
2247
2251
2253
2255
2257
2258
226
2261
2262
227
2301
2305
2307
2319
2325
2337
2345
2346 2347
2350
2354 2355
2357
2361
2400 2401
2406
2418
2423
2437
2444 2445
2451
2453
2454 2455
2457
2458
2461
2545
2550
2554 2555
2561
2601
2619
2627
2637
2645
2655
2660
2719
2725
2737
2751
2761
2819
2861
2901
2909
2919
2925
2937
2943
2955
2959
2963
3001301
3015
3021
303
3037
3054 3055
3058
3060 3061
3062
307
313
3154 3155
3157
3159
3160 3161
3163
318 3219
3227
3237
3247
3254 3255
3256 3257
3260 3261
327
3301
3309
3315
3321
3337 3345
3346
3351
3354
3356 3357
3361
3401
3411
3421
3450 3451
3454
3457
3459
3555
3556 3557
3558
3560 3561
3563
3600
3621
3625
3637
3645
3654
3658
3661
3662
3720 3721
3761
3801
3811
3819
3820
3825
3837
3845
3855
3910 3911
3913
3917
3919
3945
3947
3951
3953
3955
3957
3961
400 4001
4005
4009
401
4010 4011
4012 4013
4014
4016 4017
4018
4023
403
4037
4044
4046
405
4050
4052 4053
4054 4055
406
4061
407
408 409
4100 4101
4103
4104 4105
4107
4108
4110 4111
4119
4125
415
4152
4155
4156 4157
4159
4161
4163
4200 4201
4202
4206
4208
4210 4211
4221
4223
4225
4227
4229
425
426
428
4301
4309
4313
4315
4317
4319
4320 4321
4322
4324
4326 4327
4328
4337
4341
4343
4347
4405
4407
4408
4411
4412
4414
4416
4418 4419
4420
4422 4423
4429
4436 4437
4438
4440 4441
4442 4443
4444
4446 4447
4448
500 501
502
502650285030
506 507
508
512651285130
519
522652285230
532653285330
542654285430
552655285530
562656285630
572657285730
582658285830
592659285930
601
602660286030
609
615
619
625
708 709
710 711
712 713
715
719
736 737
739
740 741
742
744 745
746
801
807
808
814
819
825
829
836 837
840 841
901
903
905
911
919
924 925
928
936 937
938
940
943
Hall C Entrance
IndustryExpertsTheater
AAD Food Court
002
Hall B Entrance Hall A Entrance
#
3Gen, Inc./DermLite ................................... 1701
5CC (5-Continent-Congress) .......................... 615
A
AAD Industry Experts Theater........................... 2
Abacosm LTD ............................................. 4347
AbbVie ...............2101, 2111, 5626, 5628, 5630, 5726, 5728, 5730, 5830
Accurate Manufacturing Inc .......................... 428
AccuTec Blades ........................................... 2355
AccuVein .................................................... 1047
Aclaris Therapeutics, Inc ............................... 601
Acuderm..................................................... 2337
AD Surgical ................................................ 4005
Adult & Pediatric Dermatology, PC .............. 4437
Advalight ...................................................... 710
Advanced Dermatology & Cosmetic Surgery ................................ 3919
Advanced MD, Inc. ..................................... 2350
Aerolase ...................................................... 1917
Aesthetics Biomedical ................................. 4206
Allergan .................................. 1909, 2401, 5030
Alma Lasers ................................................ 2009
ALMIRALL ................................................. 4211
Alphaeon Corporation ................................. 2255
AMA-Meditime ........................................... 2257
American Academy of Dermatology ............ 4055
American Board of Dermatology ................. 2319
American Society for Dermatologic Surgery ........................ 1908
American Society for Mohs Surgery ............. 3346
Amgen, Inc. ................................................ 3637
AMP Medical Products, LLC.......................... 715
Amryt Pharma ............................................ 4422
Anne Arundel Dermatology, P.A. ................. 4225
Anthony Products/Gio Pelle ........................ 1100
Aptar Pharma ............................................. 4103
Aquavit Pharmaceuticals, Inc. ..................... 1003
Ascentium Capital LLC ............................... 1222
Asclepion Laser Technologies ...................... 1709
Aurora Diagnostics ....................................... 425
Australasian College of Dermatologists ......... 938
B
Baitella AG ................................................. 2253
Bank of America Practice Solutions ............. 2047
Beiersdorf, Inc. ........................................... 2737
Beijing Sincoheren S&T Development Co., LTD ................................................. 1138
Beijing Syntech Laser Co., Ltd. ...................... 736
Bellaire Industry/Mesopen .......................... 1005
Benev Company Inc. ......................... 1109, 1204
Berkshire Health Systems ............................. 936
Biodermis ................................................... 1319
Biofrontera, Inc. ............................................ 209
Biopelle, Inc ............................................... 3237
BioPharmX ................................................... 502
Biorasi ........................................................ 2455
bioskin GmbH ............................................ 3450
BirdEye ......................................................... 406
Blaine Labs, Inc. ......................................... 3457
BLUECORE COMPANY CO., LTD ................ 301
Boehringer Ingelheim Pharmaceuticals, Inc ..................... 4327, 5128
Boiron ........................................................ 3155
Bovie Medical ............................................. 4009
brandMD Skin Care ...................................... 937
Brazilian Society for Dermatological Surgery ................................................... 2445
Brymill Cryogenic Systems .......................... 2400
BTL ............................................................ 1009
C
Cabana Life ................................................... 814
Caliber Imaging & Diagnostics .................... 2019
Candela ...................................................... 2137
Canfield Scientific ....................................... 1923
Cantabria Labs ............................................ 3261
Capillus, LLC ................................................ 943
CareCredit .................................................. 1509
Cartessa Aesthetics, LLC ............................... 741
Castle Biosciences, Inc. ............................... 3654
Celgene Corporation ......................... 3421, 5928
Certain Dri ................................................. 4412
Chase Merchant Services ............................... 212
CheckedUP................................................. 4423
Chemistry Rx .............................................. 2959
Chemotechnique Diagnostics/ Dormer Laboratories ............................... 2955
Cherry Imaging .......................................... 1813
CLASSYS ...................................................... 201
Cleure ........................................................ 4313
Clinical Resolution Lab, Inc. ........................ 1240
CLN Skin Care (TopMD Skin Care) ............. 4221
CNH Pillow, Inc. ......................................... 1910
Coalition of Skin Diseases ........................... 3913
Cobalt Medical Supply, Inc. ......................... 3451
cocoon medical ............................................. 307
CoLabs Intl Corp ......................................... 2247
Collagen P.I.N. ............................................ 2153
Compulink Healthcare Solutions ................. 4018
COOLA Suncare ......................................... 3260
Coolibar, Sun Protection You Wear .............. 3054
Corrona LLC ............................................... 3356
Cortex Technology Aps ................................ 1136
CRC Press - Taylor & Francis ....................... 1811
Crown Laboratories, Inc. ............................. 3315
Crystal Clear Digital Marketing ................... 2963
CureMD Healthcare ...................................... 825
Cutanea Life Sciences, Inc ..................... 223, 313
Cutera ........................................................ 1501
Cutis & Cosmetic Dermatology ................... 1723
Cutis Diagnostics ........................................ 4011
Cynosure .................................................... 1801
D
Daavlin ....................................................... 3837
Dartmouth-Hitchcock ................................... 746
DefenAge ..................................................... 508
DEKA Medical ............................................ 1609
Delasco ....................................................... 2627
Derma Faith, LLC ....................................... 3160
DermaSculpt -CosmoFrance ........................ 4111
Dermasensa Laboratories, Inc. .................... 4343
DermaSweep .............................................. 1119
Dermatologic Cosmetic Laboratories ........... 2645
Dermatologist, The ..................................... 3911
Dermatology Advisor .................................. 2251
Dermatology Foundation ............................ 2001
Dermatology News ...................................... 1721
Dermatology Times ...................................... 303
Dermira, Inc. ...................................... 415, 5926
DermoScan Inc. .......................................... 4155
Dermpath Diagnostics ................................ 3625
Dermpath Lab of Central States ................... 1818
▼To Hall D
(shown at right)
Exhi
bit
Hal
l Hou
rs FRIDAY: 10 a.m.-5 p.m.Unopposed hours: 12-1 p.m.
SATURDAY: 10 a.m.-5 p.m.Unopposed hours: 12-1 p.m.
SUNDAY: 10 a.m.-3 p.m.Unopposed hours: 12-1 p.m.
Map sponsored by AbbVie
Data current as of Jan. 10, 2019.

DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019 15
001
1000 1001
1002 1003
1004 1005
1009
1019
1021
1037
1041
1043
1045
1047
1100 1101
1103
1105
1109
1118 1119
1123
1127
1129
1136 1137
1138
1140 1141
1142
1144
1200 1201
1204
1209
1217
1218
1222 1223
1224
1236 1237
1240
1301
1311
1316
1319
1325
1337
1343
1401
1403
1409
1418 1419
1437
1500 1501
1504
1509
1515
1537
1545
1609
1645
1701
1709
1719
1721
1723
1727
1737
1801
1809
1811
1813
1815
1818 1819
1822 1823
1837
1845
1908 1909
1910
1912
1916 1917
1923
1945
200 2001
2005
2009
201
2019
202
2025
2037
204
2047
208 209
210
2100 2101
2104
2111
2118
212
2137
214
2146 2147
2153
2159
216
2163
218 219
220
2201
221
222 223
2247
2251
2253
2255
2257
2258
226
2261
2262
227
2301
2305
2307
2319
2325
2337
2345
2346 2347
2350
2354 2355
2357
2361
2400 2401
2406
2418
2423
2437
2444 2445
2451
2453
2454 2455
2457
2458
2461
2545
2550
2554 2555
2561
2601
2619
2627
2637
2645
2655
2660
2719
2725
2737
2751
2761
2819
2861
2901
2909
2919
2925
2937
2943
2955
2959
2963
3001301
3015
3021
303
3037
3054 3055
3058
3060 3061
3062
307
313
3154 3155
3157
3159
3160 3161
3163
318 3219
3227
3237
3247
3254 3255
3256 3257
3260 3261
327
3301
3309
3315
3321
3337 3345
3346
3351
3354
3356 3357
3361
3401
3411
3421
3450 3451
3454
3457
3459
3555
3556 3557
3558
3560 3561
3563
3600
3621
3625
3637
3645
3654
3658
3661
3662
3720 3721
3761
3801
3811
3819
3820
3825
3837
3845
3855
3910 3911
3913
3917
3919
3945
3947
3951
3953
3955
3957
3961
400 4001
4005
4009
401
4010 4011
4012 4013
4014
4016 4017
4018
4023
403
4037
4044
4046
405
4050
4052 4053
4054 4055
406
4061
407
408 409
4100 4101
4103
4104 4105
4107
4108
4110 4111
4119
4125
415
4152
4155
4156 4157
4159
4161
4163
4200 4201
4202
4206
4208
4210 4211
4221
4223
4225
4227
4229
425
426
428
4301
4309
4313
4315
4317
4319
4320 4321
4322
4324
4326 4327
4328
4337
4341
4343
4347
4405
4407
4408
4411
4412
4414
4416
4418 4419
4420
4422 4423
4429
4436 4437
4438
4440 4441
4442 4443
4444
4446 4447
4448
500 501
502
502650285030
506 507
508
512651285130
519
522652285230
532653285330
542654285430
552655285530
562656285630
572657285730
582658285830
592659285930
601
602660286030
609
615
619
625
708 709
710 711
712 713
715
719
736 737
739
740 741
742
744 745
746
801
807
808
814
819
825
829
836 837
840 841
901
903
905
911
919
924 925
928
936 937
938
940
943
Hall C Entrance
IndustryExpertsTheater
AAD Food Court
002
Hall B Entrance Hall A Entrance
INDUSTRY EXPERTS THEATERThese unique sessions provide exhibiting companies the opportunity to present new research findings on products; conduct demonstrations, detail products, and highlight new products. These sessions are solely promotional and are not eligible for continuing medical education credit.
Brought to you by
©2019 AbbVie Inc. North Chicago, IL 60064 US-RISN-180097 March 2019 Printed in U.S.A.
Brought to you by
©2019 AbbVie Inc. North Chicago, IL 60064 US-RISN-180097 March 2019 Printed in U.S.A.©2019 AbbVie Inc. North Chicago, IL 60064 US-RISN-180097 March 2019 Printed in U.S.A.
EXPERIENCE THE SKY AT BOOTH #2111
001
1000 1001
1002 1003
1004 1005
1009
1019
1021
1037
1041
1043
1045
1047
1100 1101
1103
1105
1109
1118 1119
1123
1127
1129
1136 1137
1138
1140 1141
1142
1144
1200 1201
1204
1209
1217
1218
1222 1223
1224
1236 1237
1240
1301
1311
1316
1319
1325
1337
1343
1401
1403
1409
1418 1419
1437
1500 1501
1504
1509
1515
1537
1545
1609
1645
1701
1709
1719
1721
1723
1727
1737
1801
1809
1811
1813
1815
1818 1819
1822 1823
1837
1845
1908 1909
1910
1912
1916 1917
1923
1945
200 2001
2005
2009
201
2019
202
2025
2037
204
2047
208 209
210
2100 2101
2104
2111
2118
212
2137
214
2146 2147
2153
2159
216
2163
218 219
220
2201
221
222 223
2247
2251
2253
2255
2257
2258
226
2261
2262
227
2301
2305
2307
2319
2325
2337
2345
2346 2347
2350
2354 2355
2357
2361
2400 2401
2406
2418
2423
2437
2444 2445
2451
2453
2454 2455
2457
2458
2461
2545
2550
2554 2555
2561
2601
2619
2627
2637
2645
2655
2660
2719
2725
2737
2751
2761
2819
2861
2901
2909
2919
2925
2937
2943
2955
2959
2963
3001301
3015
3021
303
3037
3054 3055
3058
3060 3061
3062
307
313
3154 3155
3157
3159
3160 3161
3163
318 3219
3227
3237
3247
3254 3255
3256 3257
3260 3261
327
3301
3309
3315
3321
3337 3345
3346
3351
3354
3356 3357
3361
3401
3411
3421
3450 3451
3454
3457
3459
3555
3556 3557
3558
3560 3561
3563
3600
3621
3625
3637
3645
3654
3658
3661
3662
3720 3721
3761
3801
3811
3819
3820
3825
3837
3845
3855
3910 3911
3913
3917
3919
3945
3947
3951
3953
3955
3957
3961
400 4001
4005
4009
401
4010 4011
4012 4013
4014
4016 4017
4018
4023
403
4037
4044
4046
405
4050
4052 4053
4054 4055
406
4061
407
408 409
4100 4101
4103
4104 4105
4107
4108
4110 4111
4119
4125
415
4152
4155
4156 4157
4159
4161
4163
4200 4201
4202
4206
4208
4210 4211
4221
4223
4225
4227
4229
425
426
428
4301
4309
4313
4315
4317
4319
4320 4321
4322
4324
4326 4327
4328
4337
4341
4343
4347
4405
4407
4408
4411
4412
4414
4416
4418 4419
4420
4422 4423
4429
4436 4437
4438
4440 4441
4442 4443
4444
4446 4447
4448
500 501
502
502650285030
506 507
508
512651285130
519
522652285230
532653285330
542654285430
552655285530
562656285630
572657285730
582658285830
592659285930
601
602660286030
609
615
619
625
708 709
710 711
712 713
715
719
736 737
739
740 741
742
744 745
746
801
807
808
814
819
825
829
836 837
840 841
901
903
905
911
919
924 925
928
936 937
938
940
943
Hall C Entrance
IndustryExpertsTheater
AAD Food Court
002
Hall B Entrance Hall A Entrance
Hall D
▼TO AAD CONNECTION(Poster Exhibits, Resource Center, Networking Lounge)
DermTec, Inc. ............................................. 2861
Dermwise ................................................... 1142
Designs for Vision, Inc. ................................. 500
Dino-Lite Scopes (BigC) .............................. 3255
Doctor Multimedia ....................................... 200
Doctor.com ................................................. 4405
Dow Development Laboratories ................... 3558
DRE Medical Inc ......................................... 3917
Dubai Business Events .................................. 744
E
eClinicalWorks.............................................. 801
Eclipse .......................................................... 925
Eclipse Loupes and Products ......................... 405
eclipserx ..................................................... 4326
Elite Research Network, LLC ......................... 202
Ellis Instruments ........................................ 2301
ELON Hair, Nails & Skin ............................. 1819
Elsevier ....................................................... 3309
EltaMD SkinCare ........................................ 1325
eMIRAmed USA......................................... 2458
EndyMed Medical Inc ................................. 1209
Envy Medical .............................................. 2943
Epionce ...................................................... 1343
Epiphany Dermatology ................................ 1001
Epocrates, an athenahealth service ............... 4163
eRelevance Corp ......................................... 2357
Espada Dermatology subsidiary of Mission Pharmacal ................................. 1845
EunSung Global Corp ................................... 919
European Academy of Dermatology and Venereology ....................................... 100
Evolus, Inc. ................................................. 2147
Excimer Therapies Inc. ............................... 4319
ExoCoBio Inc. ............................................. 4152
EZDerm, LLC ............................................. 3845
F
FDA Center for Drug Evaluation and Research ............................................ 711
Ferndale Healthcare, Inc. ............................ 3301
FibroTx LLC ................................................ 4108
FineMec Co, Ltd ............................................ 409
Foamix Pharmaceuticals ............................. 4301
Focus Medical ............................................. 1218
Forefront Dermatology .................................. 719
FORMATK Systems Ltd .............................. 2159
Fotofinder Systems, Inc ............................... 2719
Fotona Lasers .............................................. 2545
G
Galderma Laboratories, LP ...... 2601, 5026, 5028
Genentech, a Member of the Roche Group ..................................................... 2725
GliSODin Skin Nutrients ............................ 3357
GluStitch Inc. ............................................... 407
Gold Bond Ultimate ...................................... 519
Grand Aespio Inc. ....................................... 4053
GreenSky Patient Solutions, LLC ................. 4436
Guangzhou Huafei Tongda Technology Co., Ltd ..................................................... 713
H
Haircheck ................................................... 3951
HairMax-Lexington International................. 1815
Hansderma ................................................. 4210
Hayden Medical Instruments ........................ 901
Heine USA Ltd ........................................... 3720
Henkel Consumer Goods ............................ 2637
Henry Schein .............................................. 1103
Hidrex USA ................................................ 4014
Hill Laboratories Co. ................................... 3055
Hill Top Research ....................................... 2451
Hironic Co., LTD .......................................... 507
Huons Global ............................................... 745
HydroPeptide ............................................. 2555
I
Iagnosis Inc./DermatologistOnCall ............. 2457
Ibero Latin American Collage of Dermatology/CILAD ................................. 401
ILOODA Co., Ltd .......................................... 400
To Hall D (shown at right)
Please go to aad.org/meetings or the
AAD Meeting Mobile App for the most
up-to-date exhibitor list.
16 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
11106200_AAD_Daily_News_Full_Pg_M2.indd 1 1/25/19 12:50 PM
Image Skincare ......................................... 2655
INDIBA, S.A. .............................................. 204
Infinity Massage Chairs ............................... 924
Inform Diagnostics ................................... 2819
Inga Ellzey Billing Companies ................... 3957
Innovaderm Research ................................ 2454
Innovative Optics Laser Eye Protection ....... 2104
Integrated Dermatology Group .................. 3015
International Society of Dermatology ......... 4013
Invitrx Therapeutics .................................. 4438
ISDIN ............................................. 1545, 1645
J
JAMA Network, The .................................. 2305
Jan Marini Skin Research .......................... 3819
Janssen Biotech, Inc. ....................... 3801, 5126
Johnson & Johnson Consumer Inc .....................................3401, 5826, 5828
Journal of Clinical and Aesthetic Dermatology ......................................... 4101
Journey Medical Corporation ..................... 4016
K
Kaiser Permanente .................................... 1916
Kamedis ................................................... 4223
Kao USA Inc. (Bio-Oil) .............................. 2660
Kao-Curel ................................................. 2037
Karger Publishers ...................................... 1401
KCD Medical ............................................. 4328
Kernel Medical ............................................ 905
Kyowa Kirin .............................................. 1043
L
L’Oreal ...................................................... 3345
la parfait cosmetics .................................... 4429
Laboratorio Genove ................................... 3561
Laseroptek Co., LTD. ................................. 2461
Laservision ................................................ 4100
LC Cell...................................................... 2354
LearnSkin ................................................... 739
LEO Pharma Inc. 3227, 3825, 5130, 5226, 5230
LIFTLAB Skin Regeneration ...................... 1041
Light Age, Inc. .......................................... 1419
LightStim .................................................... 318
Lilly USA, LLC .......................................... 2751
Lipotec USA, Inc ....................................... 3955
Locks of Love, Inc. ..................................... 2453
Luma Therapeutics, Inc ............................. 2347
Lumenis ................................................... 1837
LUTRONIC ............................................... 1301
M
M.A. Dermaceuticals ................................. 4322
MartiDerm ................................................ 2261
Mastocytosis Society, Inc., The ................... 1141
Mayne Pharma .......................................... 3855
McGraw-Hill Education ............................. 1822
MCV Physicians-VCU Health ....................... 903
MD Charts, Inc. .......................................... 222
MD Cosmetica .......................................... 4161
Med-Aesthetic Solutions Inc. ...................... 3961
MedCo Data ................................................ 837
Medesthetics Magazine................................ 829
Medicol USA ............................................. 3621
Medjet ...................................................... 3945
Medline Industries, Inc. ............................ 3163
Meridian Clinical Research ........................ 4156
Merz ......................................................... 2937
Mesoestetic SL .......................................... 2258
MetaOptima Technology Inc. ..................... 4320
Microsurgery Instruments, Inc. ................. 3820
Midmark Corporation................................ 2901
Millennium Medical Technologies ............... 218
MiraDry, Inc. .............................................. 911
MJ Products Association LLC ....................... 403
Modernizing Medicine, Inc. ....................... 1237
MolluscumRx. ........................................... 3555
MotherToBaby Pregnancy Studies ................ 220
MTI, Inc. .................................................. 2919
MyDermRecruiter/MyMDRecruiter ........... 4315
Myriad Genetic Laboratories, Inc ............... 1002
N
NAOS/Laboratoire Bioderma ........... 3361, 3459
National Biological Corp. ........................... 2025
National Psoriasis Foundation ..................... 408
Nelly De Vuyst Derme & Co ....................... 4119
NeoStrata Company, Inc. ........................... 3411
Neutrogena ............................................... 3600
New Medical Technology, Inc. .................... 1217
NewBeauty ................................................ 4052
NEWPONG CO., LTD ................................ 4407
Nextech..................................................... 1823
NIA24 ...................................................... 1418
NIAMS ..................................................... 1809
NoIR LaserShield ...................................... 1504
NOURITRESS HAIR PRODUCTS ............. 3161
NovaCutis, Inc. ........................................... 708
Novartis Pharmaceuticals Corporation ....... 3021
Novella Clinical ......................................... 1200
Nutrafol .................................................... 4054
O
Obagi Medical Products ............................. 4125
Oculo-Plastik Inc. ...................................... 1000
OCuSOFT Skin Care ................................... 836
Officite ...................................................... 2345
Omni Bioceutical Innovations .................... 2554
Omnilux ................................................... 4104
Ontos, Inc. ................................................ 1004
Ortho Dermatologics ................................. 3001
Otto Trading Inc ............................. 2146, 3254
Oxygenetix Institute Inc. ............................ 3454
P
Palmer’s .................................................... 4309
PCA Skin .................................................. 3661
Peninsula Medical ....................................... 327
PerfAction Technologies ............................ 3761
Perigee ....................................................... 808
Perimed Inc. ............................................. 4105
Perrigo...................................................... 4050
Person & Covey ......................................... 2406
Pfizer Inc. .........1537, 5426, 5428, 5430, 5526, ................................................... 5528, 5530
Pharma Cosmetics, Inc. ............................. 2325
PharmaDerm a division of Fougera Pharmaceuticals .................................... 2925
Philips Respironics.................................... 3256
PhytoCeuticals, Inc. ................................... 1123
Pierre Fabre USA ...................................... 2423
Pinnacle.................................................... 4341
Practical Dermatology ............................... 2346
Practice Flow Solutions ............................. 4317
PracticeLink ................................................ 840
Precision Medical Devices, LLC.................. 4447
ProCell Therapies ...................................... 4012
Procter & Gamble ..................................... 3037
Proinnovera GmbH ................................... 1118
Promius Pharma ....................................... 3351
ProPath Dermatopathology ........................ 1737
Prostemics Co, LTD .................................. 3947
Providence - Provider Solutions + Development ........................................ 210
PSI/Vanicream Skin Care .......................... 1224
Q
Quanta System SPA................................... 1311
Quantificare .............................................. 2550
Quintessence Skin Science ........................ 1137
R
Ra Medical Systems, Inc. ........................... 2307
Red Spot Interactive .................................. 2163
Refine USA ................................................. 841
Regen Lab ................................................... 619
Regeneron/ Sanofi Genzyme .......3645, 5326, 5328, 5330
Restoration Robotics ................................... 625
Revision Skincare ...................................... 3219
Revitalash ................................................. 2444
Robbins Instruments................................. 1500
Rohrer Aesthetics, LLC ................................ 609
Root of Skin MD by AIVITA Biomedical, Inc. ....................................................... 4420
Rose Micro Solutions....................... 1129, 4229
RoyalZ ...................................................... 2262
S
Saalmann medical GmbH & Co, KG .......... 1021
Sanford Health ............................................ 742
SanovaWorks (including JDD) ................... 4010
Sawgio, LLC .............................................. 4227
Scar Heal .................................................. 1127
Schweiger Dermatology Group .................. 4337
SciBase ..................................................... 4110
SCIENTIST SKINLAB LTD. ......................... 426
Sciton ....................................................... 2100
Sebela Pharmaceuticals Inc. ...................... 3257
Sensus Healthcare ..................................... 4201
Sesderma .......................................... 819, 2619
SESHA Skin Therapy ................................ 3058
Shanghai Wonderful Opto-Electrics Tech. Co., Ltd ........................................ 1140
Shantel Medical Supply ............................. 2418
shenb Co., Ltd ............................................. 506
SILAB ....................................................... 3953
Skagit Regional Health ................................ 214
Skin & Cancer Associates/Advanced Dermatology Mgmt ............................... 1236
Skin Cancer Foundation, The .................... 4001
Skin Disease Education Foundation ........... 1719
SkinCeuticals ............................................ 3337
SkinGen International Inc. ........................ 4107
SkinIO ...................................................... 3662
SkylineDX ................................................... 940
SmartPractice ........................................... 2005
SNJ Co., Ltd ................................................ 219
Society of Dermatology Physician Assistants .............................................. 1912
Solumbra by Sun Precautions .................... 1337
Solvital ...................................................... 3159
Speclipse, Inc. ............................................. 208
Springer ................................................... 3910
STRATA Skin Sciences .............................. 1223
Summit Health ......................................... 4044
Sun Pharma .............................................. 4037
Sun Protection Zone ................................. 2118
SurgiTel/General Scientific Corp. ................. 928
Sutter Health .............................................. 740
Symbio LLC .............................................. 3556
Synergy MedSales ....................................... 221
Synteract ................................................... 2909
Syris Scientific .......................................... 1101
T
taberna pro medicum ................................ 3247
Teoxane Laboratories ................................. 2761
Tergus Pharma, LLC .................................. 4208
The HydraFacial Company......................... 4017
Thermi ....................................................... 501
Tiemann-Bernsco ...................................... 3321
Tizo by Fallene, Ltd ................................... 1437
TKL Research ............................................ 1403
Tooti Enterprise Inc. .................................. 3157
Topix Pharmaceuticals, Inc. ....................... 1515
Toskani SL. ............................................... 4061
Total Clinical Trial Management ................ 3061
Tulip Medical Products .............................. 3563
U
U.S. Dermatology Partners ........................ 3557
UCB, Inc. .................................................... 807
Ultra V CO., Ltd .......................................... 216
Under Skin ............................................... 1945
Unilever ................................................... 2437
UV Skinz, Inc. .......................................... 3154
UVBIOTEK ............................................... 1316
V
Vector Surgical .......................................... 1019
Venus Concept USA Inc. ........................... 1201
VERRICA ................................................. 4046
VI Aesthetics ..................................... 737, 5228
Viscot Medical LLC .................................... 1105
VisualDx ................................................... 3721
Vivacare .................................................... 4159
Viviscal Professional .................................. 4321
Vydence Medical ......................................... 712
W
Wallaroo Hat Company ............................. 1037
Water’s Edge Dermatology ......................... 4324
WCD 2019 Milan ........................................ 226
Wells Fargo Practice Finance ..................... 1144
West-TeleVox Solutions .............................. 1727
Wiley ........................................................ 4408
Wolters Kluwer ......................................... 3811
WON TECH Co, Ltd .................................... 227
X
Xstrahl, Inc. .............................................. 2561
Y
Young Pharmaceuticals, Inc. ...................... 4023
Z
Zero Gravity ...................................... 709, 4200
Zhuhai Yasha Bio Technology Company ..... 1045
Zimmer Medizin Systems ......................... 1409
ZO Skin Health, Inc. ................................. 2201
Data current as of Jan. 10, 2019. Please go to aad.org/meetings or the AAD Meeting Mobile App for the most up-to-date exhibitor list.

11106200_AAD_Daily_News_Full_Pg_M2.indd 1 1/25/19 12:50 PM

© 2019 Allergan. All rights reserved. All trademarks are the property of their respective owners.Allergan.com SkinMedica.com 190396 AGE120684 01/19
These SkinMedica® products are intended to meet the FDA’s defi nition of a cosmetic product, an article applied to the human body to cleanse, beautify, promote attractiveness, and alter appearances. These SkinMedica® products are not intended to be drug products that diagnose, treat, cure, or prevent any disease or condition. These products have not been approved by the FDA, and the statements have not been evaluated by the FDA.
BLUE LIGHT EXPOSUREIS HERE TO STAYBUT WITH THE LUMIVIVE™ SYSTEM, SKIN DAMAGE DOESN’T HAVE TO
LUMIVIVE™ System helps your patients
GET THAT GLOWand keeps them coming back for more.
Defend their skin againstblue light damage all day
Support their skinrecovery at nightblue light damage all dayblue light damage all day recovery at night
Visit SkinMedica® at booth 2401 to learn more.
Sponsored by Celgene
Paul Yamauchi, MD, PhDDermatology Institute & Skin Care CenterSanta Monica, CA
Moving Beyond Topicals: Perspectives on Systemic Treatment for Psoriasis
I N D U S T R Y E X P E R T S E S S I O N
Friday, March 1, 2019 / 12:15 PM - 1:00 PM / 12:15 PM - 1:00 PM Walter E. Washington Convention Center / Washington, DC
This Industry Expert Session is a promotional activity and is not approved for continuing education credit. The content of this session and opinions expressed by presenters are those of the Presenting Company or presenters and do not represent an endorsement by, nor imply that the products have been evaluatedor approved by the American Academy of Dermatology.
Pursuant to the PhRMA Code on Interactions with Healthcare Professionals, attendance at this promotional program is restricted to healthcare professionals. Accordingly, spouses and other guests who are not healthcare professionals may not attend this event. Celgene will report transfers of value made to US healthcare professionals to the extent required by federal and state laws, as applicable. To learn about how Celgene Corporation complies with the Physician Payments Sunshine Act visit http://www.celgene.com/about/compliance/sunshine-act/.
© Celgene Corporation 11/18 US-CLG-18-0496
You’re invited to join the discussion!
PROGRAM FACULTY

© 2019 Allergan. All rights reserved. All trademarks are the property of their respective owners.Allergan.com SkinMedica.com 190396 AGE120684 01/19
These SkinMedica® products are intended to meet the FDA’s defi nition of a cosmetic product, an article applied to the human body to cleanse, beautify, promote attractiveness, and alter appearances. These SkinMedica® products are not intended to be drug products that diagnose, treat, cure, or prevent any disease or condition. These products have not been approved by the FDA, and the statements have not been evaluated by the FDA.
BLUE LIGHT EXPOSUREIS HERE TO STAYBUT WITH THE LUMIVIVE™ SYSTEM, SKIN DAMAGE DOESN’T HAVE TO
LUMIVIVE™ System helps your patients
GET THAT GLOWand keeps them coming back for more.
Defend their skin againstblue light damage all day
Support their skinrecovery at nightblue light damage all dayblue light damage all day recovery at night
Visit SkinMedica® at booth 2401 to learn more.
Sponsored by Celgene
Paul Yamauchi, MD, PhDDermatology Institute & Skin Care CenterSanta Monica, CA
Moving Beyond Topicals: Perspectives on Systemic Treatment for Psoriasis
I N D U S T R Y E X P E R T S E S S I O N
Friday, March 1, 2019 / 12:15 PM - 1:00 PM / 12:15 PM - 1:00 PM Walter E. Washington Convention Center / Washington, DC
This Industry Expert Session is a promotional activity and is not approved for continuing education credit. The content of this session and opinions expressed by presenters are those of the Presenting Company or presenters and do not represent an endorsement by, nor imply that the products have been evaluatedor approved by the American Academy of Dermatology.
Pursuant to the PhRMA Code on Interactions with Healthcare Professionals, attendance at this promotional program is restricted to healthcare professionals. Accordingly, spouses and other guests who are not healthcare professionals may not attend this event. Celgene will report transfers of value made to US healthcare professionals to the extent required by federal and state laws, as applicable. To learn about how Celgene Corporation complies with the Physician Payments Sunshine Act visit http://www.celgene.com/about/compliance/sunshine-act/.
© Celgene Corporation 11/18 US-CLG-18-0496
You’re invited to join the discussion!
PROGRAM FACULTY
20 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
Novel Treatment Strategies and the Trial-Based Rationale for
PD-1 TARGETING THERAPY in
ADVANCED and METASTATIC CUTANEOUS SQUAMOUS CELL
CARCINOMA (CSCC)
REGISTER NOW: www.reg-CSCC.com
JOIN US TONIGHT FOR A MILESTONE SATELLITE SYMPOSIUM!World Experts Navigate the Evolving and Complex Landscape of Advanced and Metastatic CSCC
Focus on Real World Cases, High Level Consultation, and Up-to-the-Minute Clinical Trials!
Save the Time and Date: Friday, March 1, 2019Time: 6:30 PM – 9:00 PM | Program Registration and Dinner: 6:30 PM – 7:00 PM
Clinical Program: 7:00 PM – 9:00 PMCity: Washington, DC | Location: Marriott Marquis Washington DC | Address: 901 Massachusetts Avenue NW
Conference Room: Liberty Ballroom M/N/O/P
Supported by an educational grant from Sanofi Genzyme and Regeneron PharmaceuticalsThis program is independent and is not part of the offi cial AAD Annual Meeting, as planned by its Scientifi c Assembly Committee
CMEducation Resources, LLCA Medical Education Company
(CSCC)Focus on the Pathoimmunobiology, Clinical Trials, Translational and Immunotherapeutic
Implications of PD-1 Checkpoint Inhibition in Advanced, Unresectable, and Metastatic Skin Cancers
Program Chairman: TODD E. SCHLESINGER, MD, FAADDirector, Dermatology and Laser Center of Charleston | Clinical Research Center of the Carolinas | Clinical Instructor, University at Bu� alo Department of Dermatology | Assistant Clinical Professor, Medical University of South Carolina Department of Family
Medicine | Clinical Preceptor, Medical University of South Carolina College of Health Professions | Charleston, SC
A YEAR 2019, DERMATOLOGY-FOCUSED, BEST PRACTICE IMMUNO-ONCOLOGY UPDATE FOR THE DERMATOLOGY AND DERMATOLOGIC ONCOLOGY SPECIALIST
T he 2010s have been an inflection point in the diagnosis and treatment
of cutaneous melanoma. FDA-approved checkpoint inhibitors and targeted therapies spurred broad adoption of these new agents across a range of dermatology practices. As the use of these newer systemic agents grew in melanoma and other cancers, dermatologists began to see dermatologic side effects in their own patients, as well as broader populations of cancer patients.
Susan M. Swetter, MD, chaired the interdisciplinary AAD melanoma work group that devoted the last two
years to updating the 2011 AAD guidelines. The current guidelines were published in late 2018 and use the eighth Edition of the American Joint Committee on Cancer melanoma staging system for pathologic diagnosis, as well as
refer to National Comprehensive Cancer Network and other international guidelines for cutaneous melanoma. She will moderate Friday’s “Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines.”
“Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines” (S017)Friday, 1–4 p.m. Room 207B
This is a whole new era for melanoma as we advocate for our patients. A decade ago, we looked at melanoma as a surgically treated disease and hoped to one day find the magic bullet to treat the disease systemically. Now melanoma has become the poster child of cancer for the success of both immunotherapies and targeted therapies.
– Susan M. Swetter, MD
PEARLS FROM MEMBERSPeter Lio, MD Medical Dermatology Associates of Chicago
1234 56AJCC staging changes impact patient selection for sentinel node biopsy in T1 melanoma. The eighth Edition of the staging system is based on a global data set and provides the most accurate long term prognosis available to data. Based on tumor characteristics, patients may or may not be appropriate for adjuvant therapy.
Patients with resected stage III (lymph node) disease, including those detected by sentinel lymph node biopsy, can be treated using anti-PD1 monotherapy with nivolumab, as well as combination BRAF/MEK inhibitors dabrafenib or trametinib. These agents are more effective than previously FDA-approved high-dose interferon or high-dose ipilimumab and far better tolerated.
The new guidelines expand coverage of melanoma and pregnancy. Look for guidance in managing the pregnant woman with melanoma and how a melanoma diagnosis may impact future pregnancies.
The role of genetic testing in melanoma is growing. Single gene and multi-gene testing can help guide treatment in hereditary risk melanoma and for detection and monitoring in cancer syndromes that may include cutaneous melanoma.
Dermatologists should understand the cutaneous toxicity of checkpoint inhibitors and targeted therapies. These agents are now used for melanoma, advanced cutaneous squamous cell carcinoma, and other cancers. The guidelines help clinicians manage these agents more effectively to maintain life-saving and potentially curative therapy.
The latest surveillance data was incorporated into new recommendations for biopsy techniques, pathology evaluation, baseline/surveillance studies, and surgical management, including Mohs micrographic surgery and other staged excision techniques for certain types of melanoma in anatomically challenging locations.
Key updates in new guidelines
Putting patients at ease
C ryotherapy for a wart, administering filler, and
excising an atypical nevus can all bring some pain, discomfort, and anxiety. Using a combination of distraction techniques such as an iPad, topical anesthetics, and excellent local anesthesia (buffered, warmed, and injected slowly along with cooling and vibration to the area) can make an incredible difference. Beyond the patient’s comfort, there is real evidence that the success rate for procedures is actually higher when pain, anxiety, and discomfort are appropriately addressed.”
Learn more at: “Pain-free Dermatology: Minimizing Discomfort in Procedures for Children and Adults” (U001)Friday, 7:30–8:30 a.m.Room 146B
key updates in the 2018 melanoma guidelines

Novel Treatment Strategies and the Trial-Based Rationale for
PD-1 TARGETING THERAPY in
ADVANCED and METASTATIC CUTANEOUS SQUAMOUS CELL
CARCINOMA (CSCC)
REGISTER NOW: www.reg-CSCC.com
JOIN US TONIGHT FOR A MILESTONE SATELLITE SYMPOSIUM!World Experts Navigate the Evolving and Complex Landscape of Advanced and Metastatic CSCC
Focus on Real World Cases, High Level Consultation, and Up-to-the-Minute Clinical Trials!
Save the Time and Date: Friday, March 1, 2019Time: 6:30 PM – 9:00 PM | Program Registration and Dinner: 6:30 PM – 7:00 PM
Clinical Program: 7:00 PM – 9:00 PMCity: Washington, DC | Location: Marriott Marquis Washington DC | Address: 901 Massachusetts Avenue NW
Conference Room: Liberty Ballroom M/N/O/P
Supported by an educational grant from Sanofi Genzyme and Regeneron PharmaceuticalsThis program is independent and is not part of the offi cial AAD Annual Meeting, as planned by its Scientifi c Assembly Committee
CMEducation Resources, LLCA Medical Education Company
(CSCC)Focus on the Pathoimmunobiology, Clinical Trials, Translational and Immunotherapeutic
Implications of PD-1 Checkpoint Inhibition in Advanced, Unresectable, and Metastatic Skin Cancers
Program Chairman: TODD E. SCHLESINGER, MD, FAADDirector, Dermatology and Laser Center of Charleston | Clinical Research Center of the Carolinas | Clinical Instructor, University at Bu� alo Department of Dermatology | Assistant Clinical Professor, Medical University of South Carolina Department of Family
Medicine | Clinical Preceptor, Medical University of South Carolina College of Health Professions | Charleston, SC
A YEAR 2019, DERMATOLOGY-FOCUSED, BEST PRACTICE IMMUNO-ONCOLOGY UPDATE FOR THE DERMATOLOGY AND DERMATOLOGIC ONCOLOGY SPECIALIST

BOOTH38012019 AMERICAN ACADEMY OFDERMATOLOGY ANNUAL MEETING
March 1 to 5, 2019
Washington, DC
© Janssen Biotech, Inc. 2019 02/19 cp-74266v2
cp-74266v2_821512_v1b.indd 1 2/11/19 4:56 PM

BOOTH38012019 AMERICAN ACADEMY OFDERMATOLOGY ANNUAL MEETING
March 1 to 5, 2019
Washington, DC
© Janssen Biotech, Inc. 2019 02/19 cp-74266v2
cp-74266v2_821512_v1b.indd 1 2/11/19 4:56 PM

24 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
Data on file. ©2019 Beiersdorf Inc.
Triple-action formula enriched with urea30 and ceramides to smooth, soften, and intensively hydrate thick, rough skin
For use on dry, cracked skin, minor wounds and burns, and skin in need
VISIT THE BEIERSDORF BOOTH 2737TO EXPERIENCE OUR BRANDS
C
M
Y
CM
MY
CY
CMY
K
PRO_62308_AAD_Annual_Meeting_Daily_News_Ad_M.pdf 1 1/14/19 11:32 AM
For this session, a laptop with Adobe Flash Player is required. The most effective browsers include Internet Explorer 11 and Firefox on Windows; Mozilla Firefox 29 and Safari 7 on Mac. Please practice using the software in advance by logging onto https://vdpmaterial.nivdp.com/dsb/login.php, using activation key 023.
• Simultaneous access to the clinical information with the ability to toggle between clinical photographs and histological slides.
• Cloud storage allows for global use across congresses, courses, and consultations.
• Can also be used on mobile devices and where available, in EMRs.
• Associated software can also be used to accrue CME credit.
• Software allows for 360-degree rotation of images.• By using crosshairs on the thumbnail image, the area to be
inspected can be located before it is magnified.• In addition to tabs and a slider, double clicking on the image
increases magnification.• Arrows in the upper left corner allow users to toggle between
the histological slide and clinical photographs.
• Software-assisted manipulation of high-definition digital images of tissue sections.
• Simulates the experience of examining glass slides under a microscope and magnification up to x40.
• Viewable by computer, over a network or via the internet.
• Can be used in internet-based exams, such as in the American Board of Dermatology Certification and Re-certification Exams beginning in 2020.
A TED-talks approach to improving practice management and
quality improvement (QI) offers dermatologists a glimpse into the hottest topics facing their practices and their professional reputations within their communities. Amanda Fleming Marsch, MD, assistant professor of dermatology at the University of California San Diego, moderates the session, “Derm Rapid Fire: Putting Residents at the Center of QI Initiative,” covering topics of pressing interest, including patient reviews, DataDerm™, QI in the fee-for-service environment, business administration skills
for optimizing health care, and teledermatology.
A dozen speakers who combine physician skills with MBA credentials will provide the foundation for the financial, analytical, crisis management, and leadership skills professionals will need to excel in their careers and optimize patient care.
At the close of the session, resident recipients of the “AAD Excellence in Patient Care Award” will present their QI projects.
“Derm Rapid Fire: Putting Residents at the Center of QI Initiatives” (S046)Sunday, 1-4 p.m.Salon G
Quality does not equal cost. Quality equals cost savings over time. Going into quality care should be the driver and finances should support that mission, not the other way around.
Amanda Fleming Marsch, MD
“Virtual Dermatopathology Self Assessment: Get Ready For Non-glass Slide Exams” (F022)Friday, 1-3 p.m.Room 143C
Some physicians score higher than others in patient reviews. It may be dependent upon the populations served by the physician. There are some things physicians can control and some they cannot when it comes to scoring.
Demonstrating quality of patient care isn’t always easy. Yet, the game is changing with DataDerm, the Academy’s clinical data registry created by dermatologists, for dermatologists. It’s designed to transform a dermatology practice and elevate the specialty.
Don’t overlook the path to the bottom line. The only way to positively impact
financial results is to focus on delivering quality.
Enhanced leadership skills and improved patient care can be achieved through QI projects, buy-in from all staffing levels, clear communication, budgets, cost analysis, and team management skills.
Teledermatology has its pros and cons. While it’s a cost effective method for connecting physicians and patients, convenient for patients, and reduces wait time, it does increase the risk of HIPAA violations, security breaches, and the potential for misdiagnosis when technology and imaging is poor.
“Rapid-fire” practice management
The wave of change is here. Moving from glass to digital slides for self-assessment and exam settings, as well as electronic medical records and consultations, is happening. Dermatologists who haven’t made the transition will need training. Ellen Mooney, MD, director of the Nordic Institute of Virtual Dermatopathology, will provide the latest on what dermatologists need to know during this afternoon’s session, “Virtual Dermatopathology Self Assessment: Get Ready For Non-glass Slide Exams.” The session includes an introduction to digital pathology and the software that is integral to making the switch, a self-assessment exam that incorporates clinical information, clinical photographs, digital histopathological slides, and an exercise in clinical-pathological correlation. Attendees are given access to real-time training on their laptops.
Sliding into digital

Data on file. ©2019 Beiersdorf Inc.
Triple-action formula enriched with urea30 and ceramides to smooth, soften, and intensively hydrate thick, rough skin
For use on dry, cracked skin, minor wounds and burns, and skin in need
VISIT THE BEIERSDORF BOOTH 2737TO EXPERIENCE OUR BRANDS
C
M
Y
CM
MY
CY
CMY
K
PRO_62308_AAD_Annual_Meeting_Daily_News_Ad_M.pdf 1 1/14/19 11:32 AM

26 DERMATOLOGY WORLD MEETING NEWS • FRIDAY • MARCH 1, 2019
So�zone® Syringe TrayCap needles with one hand
Limited show pricing:Booth 1105
www.viscot.com800.221.0658
See demo & save 60%at Booth 1105
E•Z Removable Ink® Skin Marker
Botox® is a registered trademark of Allergan, Inc.
Ink comeso� easily!
1.800.221.0658 • [email protected]
o� easily!Consultations
Botox®
Injectable Fillers
PRO
DU
CT S
POTL
IGH
T
How to beat bureaucracy-induced burnout
T he frustration is real. For many dermatologists, regulatory red tape is
the line in the sand. And an equal number of physicians are unwilling to cross it.
Mark D. Kaufmann, MD, chief medical officer for The Dermatology Group and associate clinical professor of dermatology at Icahn School of Medicine at Mount Sinai, identifies the regulatory, social, and professional forces leading to feelings of frustration, dejection, and hopelessness among dermatologists during Friday’s “Bureaucracy, Compliance, and Burnout: What it Means to Dermatologists.”
Autonomy, authority, and “burdens”“We have two global problems. One is the loss of autonomy and the other is the loss of authority,” Dr. Kaufmann said. “The government is hitting us with regulatory programs, all the acronyms that dermatologists have learned to hate (EHR, HIPAA, etc.). Government has taken the fun out of practicing medicine. That’s a heavy burden on physicians today and explains why some physicians are considering early retirement.”
As part of the audience-focused symposium, experts will join Dr. Kaufmann to discuss a wide range of factors leading to frustration, anxiety, and dissatisfaction for dermatologists, including the impact of government bureaucracy, social media, non-dermatologist encroachment, and false advertising. These “burdens,” as Dr. Kaufmann calls them, take away from patient care.
“The prescription pad has become a suggestion pad. Today, all the regulatory hurdles in front of dermatologists have
stripped away their authority,” Dr. Kaufmann said. “We’re supposed to follow the word of pharmacists and insurance payers. These are people with a fraction of the knowledge we, as physicians, have. Physicians feel frustrated and helpless.”
Creating solutionsIt’s important to formulate strategies for lifelong success and happiness before bureaucracy and burnout take hold, Dr. Kaufmann said. One solution has been to parcel out non-patient care tasks to a third party. That can occur by either selling your practice or maintaining ownership in your practice and outsourcing certain business functions to a management service organization (MSO). Another solution, he says, is to pool your business resources with other practices to share in the day-to-day work of running a practice.
It can be a tough choice for dermatologists, Dr. Kaufmann said. He describes dermatology as the “last hold out for the ‘mom and pop shop’ model.” While some dermatologists may fear selling their practice
to a private equity group or contracting with an MSO, some physicians feel relieved to get back to practicing medicine. And that positively impacts patient care.
“There’s a portion of physicians who are burned out and patients are at risk when physicians feel that way. They may feel as if they are getting the short end of the stick and not getting 110%,” he said. “It’s important to identify if you’re burned out. From my own personal experience, now that I’ve unloaded my burdens of the business portion of my practice life, I feel much less burned out and much better.”
Dr. Kaufmann predicts the “mom and pop” model of dermatology will continue to transform into larger systems.
“Find a system you are comfortable in, minimize your non-clinical duties, and you will become happy again,” he said.
“Bureaucracy, Compliance, and Burnout: What it Means to Dermatologists” (S015)Friday, 1-4 p.m.Room 140A
Career Networking Event The AAD Career Networking EventFriday, from 4:30-6:30 p.m. Marquis Ballroom Salon 6, Marriott Marquis.
Meet with more than 50 employers from around the country who are looking to hire during this high-energy event. You can also get a complimentary CV review, learn about AAD’s Career Center, and explore practice setting opportunities. CeraVe is a registered trademark.
©2019 CeraVe LLC CVE.D.P.0107
REFERENCES: 1. Takikawa M, Inoue S, Horio F, Tsuda T. Dietary anthocyanin-rich bilberry extract ameliorates hyperglycemia and insulin sensitivity via activation of AMP-activated protein kinase in diabetic mice. J Nutr. 2010;140(3):527-533. 2. Morgan N. What you need to know about xerosis in patients with diabetic feet. Wound Care Advisor. https://woundcareadvisor.com/what-you-need-to-know-about-xerosis-in-patients-with-diabetic-feet_vol2-no4/. Accessed June 25, 2018.
Developed with dermatologists for individuals with diabetes to help moisturize and soothe dry skin.
Bilberry• Has antioxidant properties1
• Is a source of lactic and ascorbic acid
Urea• Helps facilitate exfoliation2
• Helps moisturize and promote smoother skin
DRY TO VERY DRY SKIN
AND HELP
RESTORERELIEVE
Formulated with ceramides 1, 3, & 6-ll to help repair and restore the natural skin barrier, CeraVe offers over 70 different skincare products.
VISIT BOOTH #3337 TO SEE MORE.
Mark D. Kaufmann, MD

CeraVe LLC IBCpage 27
CeraVe is a registered trademark. ©2019 CeraVe LLC CVE.D.P.0107
REFERENCES: 1. Takikawa M, Inoue S, Horio F, Tsuda T. Dietary anthocyanin-rich bilberry extract ameliorates hyperglycemia and insulin sensitivity via activation of AMP-activated protein kinase in diabetic mice. J Nutr. 2010;140(3):527-533. 2. Morgan N. What you need to know about xerosis in patients with diabetic feet. Wound Care Advisor. https://woundcareadvisor.com/what-you-need-to-know-about-xerosis-in-patients-with-diabetic-feet_vol2-no4/. Accessed June 25, 2018.
Developed with dermatologists for individuals with diabetes to help moisturize and soothe dry skin.
Bilberry• Has antioxidant properties1
• Is a source of lactic and ascorbic acid
Urea• Helps facilitate exfoliation2
• Helps moisturize and promote smoother skin
DRY TO VERY DRY SKIN
AND HELP
RESTORERELIEVE
Formulated with ceramides 1, 3, & 6-ll to help repair and restore the natural skin barrier, CeraVe offers over 70 different skincare products.
VISIT BOOTH #3337 TO SEE MORE.
COME FOR THE DATA STAY FOR THE RESULTS
80 mg/mL
80 mg/mL
Learn about the Taltz Savings Card Program at taltz.com/hcp
Taltz® is a registered trademark of Eli Lilly and Company. PP-IX-US-2573 01/2019 ©2019, LILLY USA, LLC. ALL RIGHTS RESERVED. PRINTED IN USA ON POST-CONSUMER RECYCLED PAPER
If you are a US medical doctor with an active state license number, the value of the food, beverage, and/or educational item that you receive when attending this program may be disclosed on Eli Lilly and Company’s Physician Payment Registry and/or the National Physician Payment Transparency Program (NPPTP) Open Payments report under the federal Sunshine Act as a transfer of value made to you by Lilly. As a result of enacted state regulations, food and beverages will not be provided to healthcare professionals licensed in the states of Minnesota, Massachusetts, and Vermont. Additionally, educational items will not be provided to healthcare professionals licensed in Minnesota. Federal Veterans Affairs (VA) regulations and several states also prohibit state/government employees from receiving or being provided gift items, which may include educational materials and meals. Please consult your state regulations and ethics laws to see if such prohibition would apply to you. This medical presentation is intended only for invited healthcare professionals for whom the information to be presented is relevant to their practice. We regret that spouses or other guests cannot be accommodated. This is a promotional program and no continuing medical education (CME) credits are offered.
This program is independent and is not part of the official AAD Annual Meeting, as planned by its Scientific Assembly Committee.
EVENT NAME: ONGOING EXPERIENCE WITH TALTZ (IXEKIZUMAB) INJECTION EFFICACY AND SAFETY—AAD UPDATE MARCH 2, 2019 | 7:00 PM – 8:30 PM Renaissance Ballroom East | Renaissance Washington, DC Downtown Hotel
Washington D.C. PRESENTED BYCraig L. Leonardi, MDAdjunct Professor of Dermatology, St. Louis University & Jennifer Cather, MD, FAADMedical Director, Mindful Dermatology
Sponsored by Lilly USA, LLC
MEET TALTZ AT BOOTH 2751
PP-IX-US-2571 HCP - P2P Product Theater Journal Ad-2019.indd 1 31/01/19 10:03 PM
Related Documents