Pictorial essay Rev. Argent. Radiol. 2017;81(1): 39-49 39 Abstract Even if the diagnosis of abdominal wall hernias is clinical, and the most appropriate test is ultrasound, in a large number of cases hernias are difficult to evaluate, or their presence is notsuspected because of the patient’s biotype, the absence of symptoms, the presence ofcomplications, or the appearance of rare hernias. Additionally, abdominal wall weakness resulting from surgery leads to eventration of sometimes unusual organssuch as the liver, bladder, or appendix. The use ofmultidetector computed tomography (MDCT) is of great advantage when it is difficult to establish a diagnosis by other methods. Hernia may also be an incidental finding that should be considered for potential future complications. In this paper, we describe the main MDCT findings in abdominal wall hernias, including umbilical,epigastric, hypogastric, inguinal, Spigelian, lumbar, obturator, intercostal, and incisional hernias,as well as their content. © 2016 Sociedad Argentina de Radiología. Published by Elsevier.Spain, S.L.U. This is an openaccess article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Keywords: Abdominal wall; Hernia; Multidetector computed tomography Introduction Abdominal wall hernias are the protrusion of the abdominal contents through an area of anatomic weakness, while an eventration is a subcutaneous protrusion of the intraabdomi- nal contents through a weakened area of the abdominal or lumbar wall resulting from a previous surgical procedure, a gap secondary toblunt trauma or to congenital malforma- tion (referred to as incisional hernia in the English-speaking literature) 1 . Predisposition to the development of hernias is often related to any cause of increased intraabdominal pressure1, with the most common causes being obesity, chronic cough and asci- tes. Conditions that favor localized or generalized weaken- ing of the abdominal wall, such asaging, trauma, previous surgery and deficient collagen, should also be considered 2 . Hernias of the abdominal wall are common findings on multi- detector computed tomography (MDCT), ranging from small hernias with fat content to large sacs containing loops or or- gans 3 . MDCT provides an excellent anatomic detail of the ab- dominal wall, allowing accurate identification of wall hernias and their differentiation from other abdominal masses, such as tumors, hematomas or abscesses. In addition, this method allows detection of eventrations in patients who are difficult to evaluate (e.g., obese patients,postsurgical patients or pa- tients with abdominal wall scarring) 3 . Abdominal wall hernias that may be found from the cephalic to the caudal area include: epigastric, ventral, Spigelian, lum- bar, inguinal, femoral and obturator hernias. Incisional her- nias, in turn, may be located at any site, as they do not follow a cephalocaudal direction. Their accurate classification may be established by anatomic repairs 4 . The aim of this paper is to describe MDCT findings of the various types of abdominal wall hernias (inguinal, femoral, obturator, Spigelian, lumbar, intercostal, ventral and incision- al) and their content, evaluating the presence of incarceration and obstruction (table 1). Review Inguinal hernias Inguinal hernias, whether direct or indirect, are the most common abdominal wall hernias. They occur both in chil- dren (most often the indirect type) and adults (both direct and indirect types), and up to 15% of athletes complain of pubalgia 5 . The inguinal canal is a diagonal passage formed by the apo- neuroses of the three abdominal wall muscles. The anterior wall is formed by the aponeuroses of the internal and exter- A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography G. Matzke, G. Espil, J.P. Dos Ramos Alferes, N. Larrañaga, A. Oyarzún and S. Kozima Imaging Department, Hospital General de Agudos Dr. Cosme Argerich, Ciudad Autónoma de Buenos Aires,Argentina

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pictorial essay
Rev. Argent. Radiol. 2017;81(1): 39-49 39
AbstractEven if the diagnosis of abdominal wall hernias is clinical, and the most appropriate test is ultrasound, in a large number of cases hernias are difficult to evaluate, or their presence is notsuspected because of the patient’s biotype, the absence of symptoms, the presence ofcomplications, or the appearance of rare hernias. Additionally, abdominal wall weakness resulting from surgery leads to eventration of sometimes unusual organssuch as the liver, bladder, or appendix. The use ofmultidetector computed tomography (MDCT) is of great advantage when it is difficult to establish a diagnosis by other methods. Hernia may also be an incidental finding that should be considered for potential future complications.In this paper, we describe the main MDCT findings in abdominal wall hernias, including umbilical,epigastric, hypogastric, inguinal, Spigelian, lumbar, obturator, intercostal, and incisional hernias,as well as their content.
© 2016 Sociedad Argentina de Radiología. Published by Elsevier.Spain, S.L.U. This is an openaccess article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Abdominal wall; Hernia; Multidetector computed tomography
IntroductionAbdominal wall hernias are the protrusion of the abdominal contents through an area of anatomic weakness, while an eventration is a subcutaneous protrusion of the intraabdomi-nal contents through a weakened area of the abdominal or lumbar wall resulting from a previous surgical procedure, a gap secondary toblunt trauma or to congenital malforma-tion (referred to as incisional hernia in the English-speaking literature)1.Predisposition to the development of hernias is often related to any cause of increased intraabdominal pressure1, with the most common causes being obesity, chronic cough and asci-tes. Conditions that favor localized or generalized weaken-ing of the abdominal wall, such asaging, trauma, previous surgery and deficient collagen, should also be considered2.Hernias of the abdominal wall are common findings on multi-detector computed tomography (MDCT), ranging from small hernias with fat content to large sacs containing loops or or-gans3. MDCT provides an excellent anatomic detail of the ab-dominal wall, allowing accurate identification of wall hernias and their differentiation from other abdominal masses, such as tumors, hematomas or abscesses. In addition, this method allows detection of eventrations in patients who are difficult to evaluate (e.g., obese patients,postsurgical patients or pa-
tients with abdominal wall scarring)3.Abdominal wall hernias that may be found from the cephalic to the caudal area include: epigastric, ventral, Spigelian, lum-bar, inguinal, femoral and obturator hernias. Incisional her-nias, in turn, may be located at any site, as they do not follow a cephalocaudal direction. Their accurate classification may be established by anatomic repairs4.The aim of this paper is to describe MDCT findings of the various types of abdominal wall hernias (inguinal, femoral, obturator, Spigelian, lumbar, intercostal, ventral and incision-al) and their content, evaluating the presence of incarceration and obstruction (table 1).
Review
Inguinal herniasInguinal hernias, whether direct or indirect, are the most common abdominal wall hernias. They occur both in chil-dren (most often the indirect type) and adults (both direct and indirect types), and up to 15% of athletes complain of pubalgia5.The inguinal canal is a diagonal passage formed by the apo-neuroses of the three abdominal wall muscles. The anterior wall is formed by the aponeuroses of the internal and exter-
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed TomographyG. Matzke, G. Espil, J.P. Dos Ramos Alferes, N. Larrañaga, A. Oyarzún and S. Kozima
Imaging Department, Hospital General de Agudos Dr. Cosme Argerich, Ciudad Autónoma de Buenos Aires,Argentina

Rev. Argent. Radiol. 2017;81(1): 39-49
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography
40
nal oblique muscles, the posterior wall by the transversalis fascia and the conjoint tendon, the superior wall by the apo-neuroses of the internal oblique and transverse muscles, and the inferior wall by Poupart’s inguinal ligament1.The indirect inguinal hernia passes through the internal ingui-nal ring into the inguinal canalto emerge through the exter-nal inguinal ring, arising lateral and superior to the course of the inferior epigastric vessels. It may extend along the sper-matic cord or the round ligament into the scrotum or the
labia majora, respectively. The neck of the hernia sac may be seen at the deep inguinal ring 1 (fig. 1). A finding that helps characterization of this type of hernia is “the hook sign”, which takes its name from the concave shape adopted by the proximal course of the inferior epigastric artery on the axial plane when compressed by an indirect hernia6.Direct hernias emerge above the inguinal ligament medially to the inferior epigastric vessels, and are generally acquired. Their incidence increases with age due to weakening of the
Figure 1 Axial multidetector computed tomography image shows an indirect inguinal hernia (curved arrow) with fat and small bowel loops contents. Note the epigastric vessels (black arrow) and the hernia neck (straight white arrows).
Table 1: Type of hernias and their locations.
Type of hernia Location
Inguinal Direct:medial to the epigastric vessels Indirect: within the inguinal canal, lateral to the epigastric vesselsFemoral Protruding through the femoral canal below the inguinal ligament, medially to the femoral vesselsObturator Protruding through the obturator foramen, between the obturator and pectineal musclesLumbar Disruption of thoracolumbar fascia at insertion of aponeurosis of internal oblique and transverse abdominal musclesSpigelian At the junction of the semilunar line and the arcuate lineVentral Umbilical: secondary to weakness in the umbilical canal Epigastric: at midline through linea alba above umbilicus Hypogastric: at midline through linea alba below umbilicusAbdominal intercostal It occurs through a lower intercostal space by various mechanismsIncisional (eventration) It may occur at any site of the abdomen where there is an incision or wall weakness
Figure 2 Axial multidetector computed tomography image shows a direct inguinal hernia (curved arrow), medial to fem-oral vessels (straight arrow), containing bowel loops. Note the epigastric vessels (black arrow).

Rev. Argent. Radiol. 2017;81(1): 39-49
G. Matzke et al.
41
transversalis fascia in the Hesselbach triangle1. They are more common in men and are less oftenassociated with strangula-tion of the loops, possibly because they usually do not tra-verse the entire course of the canal4 (fig.2). The inguinal canal contents are compressed laterally, while the fat of the canal is shaped as a moon crescent, resulting in the crescent sign (a finding that is helpful for characterization of direct inguinal hernias)7.
Femoral herniaLess common than inguinal hernias, femoral hernias occur when the peritoneal content protrudes into the femoral canal with the femoral vein and artery4. This region is simpler than the inguinal canal in its configuration, bordered superiorly by the inguinal ligament, medially by the medial border of the adductor muscle, laterally by the Sartorius muscle with the ilio-psoas, pectineal and long adductor muscles forming its floor8. The main characteristic of the triangle is the femoral sheath,
which is formed by the deep fascia (fascia lata) of the thigh and contains the femoral artery, the femoral vein, and the fem-oral canal, from lateral to medial1.This type of hernia is more common in women and it usually occurs on the right side4.On MDCT the neck of the hernia sac can be seen as a nar-row protrusion through the femoral ring, caudal to the origin of the inferior epigastric vessels and medial to the common femoral vein, which often appears compressed by the hernia sac (fig. 3). Sometimes at clinical examination it is difficult to differentiate between femoral and inguinal hernias; there-fore MDCT plays an important role in differentiation and as-sessment of hernia contents2. The hernia sac most frequently contains small bowel loops; however, the appendix may also be found within this canal, which is rare (1% of cases) and known as De Garengeot hernia9 (table 2). Obturator herniaThe clinical diagnosis of obturator hernia is difficult because its incidence is uncommon, its location is deep and there are few
a b
Figure 3 Coronal (a) and axial (b) multidetector computed tomography images show a femoral hernia (curved arrow in b) with fat content and a loop of small bowel (straight arrow in a), causing closed loop intestinal obstruction. Note the change in loop diameter (curved arrow in a).
Table 2: Location of inguinal and femoral hernias.
Indirect inguinal hernia Direct inguinal hernia Femoral hernia
Hernia neck anterior to the inguinal ligament, Hernia neck anterior to the inguinal ligament, Posterior to thelateral to the inferior epigastric vessels medial to the inferior epigastric vessels inguinal ligament, Search for the hook sign Crescent Sign medial to the femoral vessels

Rev. Argent. Radiol. 2017;81(1): 39-49
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography
42
specific signs and symptoms, as those associated with obtura-tor nerve compression (Howship-Rombeng sign)10. The obtura-tor foramen is formed by the continuity of the pubic and ischial bones, and it is covered by the obturator membrane, except in the anterosuperior aspect, where it is perforated by the obtu-rator artery, vein and nerve, which travel along a 2-3-cm tunnel formed by the internal and external obturator muscles. Perito-neal hernia develops through this defect11.Obturator hernias occur more commonly in elderly multipa-rous women, secondary to weakness of the pelvic floor, but they may also be seen in patients with increased abdominal pressure and in frail elderly patients1.Specific diagnosis can be made if the pelvic MDCT shows
herniation of the small bowel between the external obturator and pectineal muscles, with small bowel obstruction with no apparent cause3 (fig. 4).
Spigelian herniaA Spigelian hernia is a rare acquired ventral hernia4. It occurs through defects in the aponeuroses of the internal oblique and transverse abdominal muscles, with a typical location at the junction of the semilunar line with thesemicircular or ar-cuate line3. It occurs laterally to the rectus abdominis muscle and inferiorly to the umbilicus and it is nearly always found above the level at which the inferior epigastric vessels perfo-rate the posterior wall of the rectus abdominis sheath1.
a b
Figure 4 Axial (a) and coronal (b) multidetector computed tomography images of a left obturator hernia (curved arrows). Straight arrows reveal the obturator foramen.
a b
Figure 5 Axial multidetector computed tomography image of right (a) Spigelian hernia with fat content (curved arrow), lateral to the anterior rectus abdominis muscle (straight arrow), and left (b) Spigelian hernia (curved arrow) with fat and small bowel loops contents (straight arrow).
Rev. Argent. Radiol. 2017;81(1): 39-49
G. Matzke et al.
43
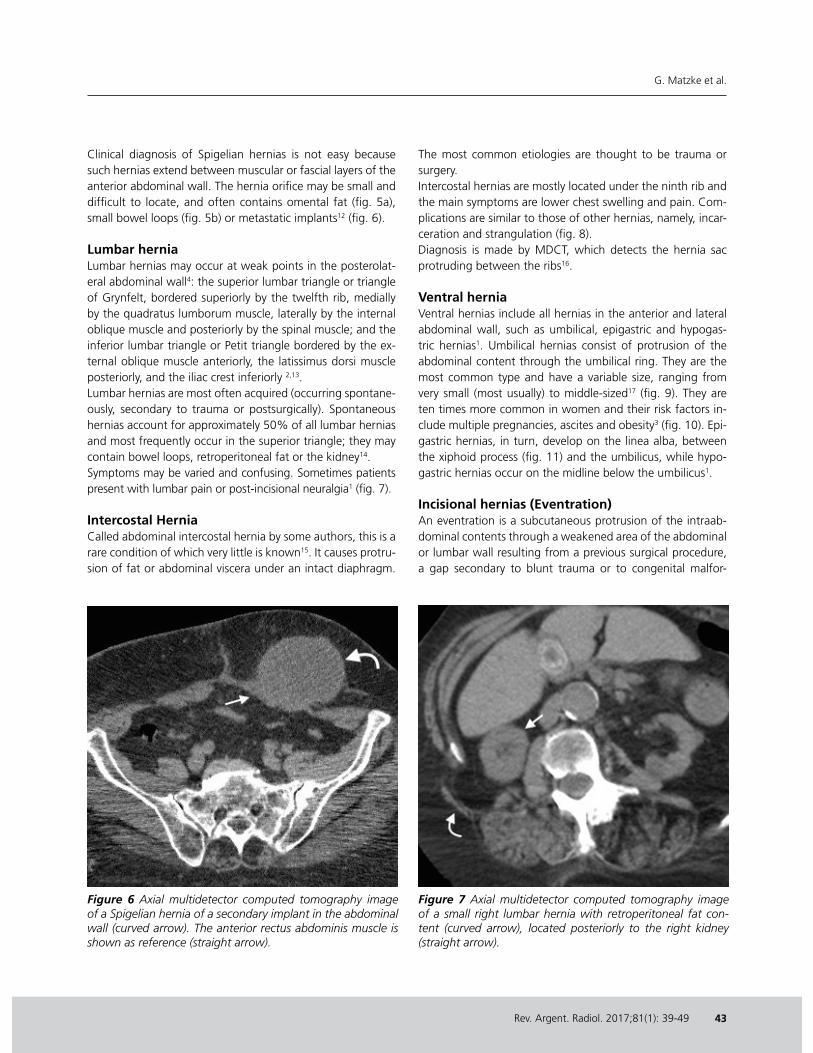
Clinical diagnosis of Spigelian hernias is not easy because such hernias extend between muscular or fascial layers of the anterior abdominal wall. The hernia orifice may be small and difficult to locate, and often contains omental fat (fig. 5a), small bowel loops (fig. 5b) or metastatic implants12 (fig. 6). Lumbar herniaLumbar hernias may occur at weak points in the posterolat-eral abdominal wall4: the superior lumbar triangle or triangle of Grynfelt, bordered superiorly by the twelfth rib, medially by the quadratus lumborum muscle, laterally by the internal oblique muscle and posteriorly by the spinal muscle; and the inferior lumbar triangle or Petit triangle bordered by the ex-ternal oblique muscle anteriorly, the latissimus dorsi muscle posteriorly, and the iliac crest inferiorly 2,13.Lumbar hernias are most often acquired (occurring spontane-ously, secondary to trauma or postsurgically). Spontaneous hernias account for approximately 50% of all lumbar hernias and most frequently occur in the superior triangle; they may contain bowel loops, retroperitoneal fat or the kidney14.Symptoms may be varied and confusing. Sometimes patients present with lumbar pain or post-incisional neuralgia1 (fig. 7). Intercostal HerniaCalled abdominal intercostal hernia by some authors, this is a rare condition of which very little is known15. It causes protru-sion of fat or abdominal viscera under an intact diaphragm.
The most common etiologies are thought to be trauma or surgery.Intercostal hernias are mostly located under the ninth rib and the main symptoms are lower chest swelling and pain. Com-plications are similar to those of other hernias, namely, incar-ceration and strangulation (fig. 8).Diagnosis is made by MDCT, which detects the hernia sac protruding between the ribs16.
Ventral herniaVentral hernias include all hernias in the anterior and lateral abdominal wall, such as umbilical, epigastric and hypogas-tric hernias1. Umbilical hernias consist of protrusion of the abdominal content through the umbilical ring. They are the most common type and have a variable size, ranging from very small (most usually) to middle-sized17 (fig. 9). They are ten times more common in women and their risk factors in-clude multiple pregnancies, ascites and obesity3 (fig. 10). Epi-gastric hernias, in turn, develop on the linea alba, between the xiphoid process (fig. 11) and the umbilicus, while hypo-gastric hernias occur on the midline below the umbilicus1.
Incisional hernias (Eventration)An eventration is a subcutaneous protrusion of the intraab-dominal contents through a weakened area of the abdominal or lumbar wall resulting from a previous surgical procedure, a gap secondary to blunt trauma or to congenital malfor-
Figure 6 Axial multidetector computed tomography image of a Spigelian hernia of a secondary implant in the abdominal wall (curved arrow). The anterior rectus abdominis muscle is shown as reference (straight arrow).
Figure 7 Axial multidetector computed tomography image of a small right lumbar hernia with retroperitoneal fat con-tent (curved arrow), located posteriorly to the right kidney (straight arrow).

Rev. Argent. Radiol. 2017;81(1): 39-49
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography
44
mation. It may occur in any surgical incision on the abdomi-nal wall, including the laparoscopic trocar insertion sites. It is more commonly encountered in association with vertical than with transverse incisions1.Most incisional hernias develop during the first 4 months af-ter surgery, a critical period for the healing of muscular layers of the abdominal wall18. They may manifest signs and symp-
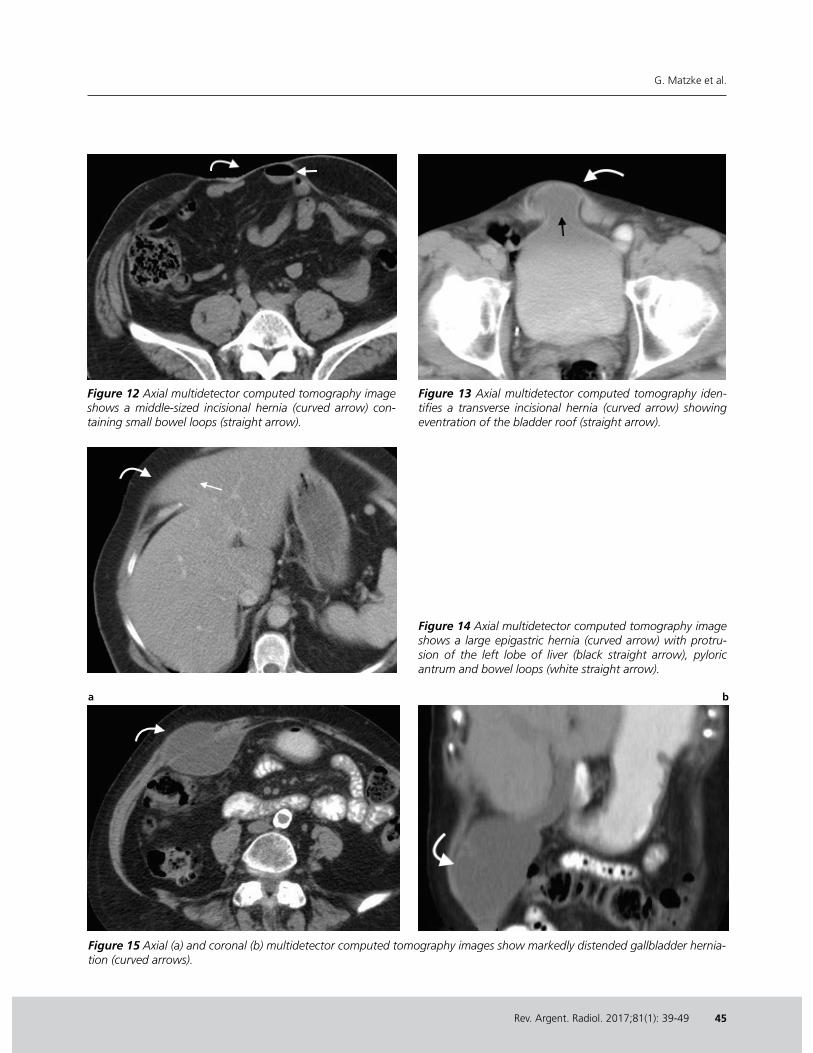
toms within the first year, although 5-10% may remain silent for a long period until their detection2.Radiological studies may be used to visualize the herniated seg-ments and to evaluate associated complications such as intesti-nal obstruction. They are often used in those patients who are difficult to evaluate, such as those with marked obesity, easily reducible hernia content or large scars19 (figs. 12 and 13).
Figure 8 Coronal multidetector computed tomography im-age of a left intercostal hernia with fat and small bowel loops content (straight arrow), showing intercostal spaces involved (curved arrows).
Figure 9 Axial multidetector computed tomography identi-fies a small umbilical hernia (curved arrow) with mesenteric fat content, medially to both anterior rectus abdominis mus-cles (straight arrows).
Figure 10 Axial multidetector computed tomography of an umbilical hernia (curved arrow) with fat and small bowel loops content (straight arrow).
Figure 11 Axial multidetector computed tomography shows a large epigastric hernia (curved arrow) with left lobe of the liver protruding (straight arrows).
Rev. Argent. Radiol. 2017;81(1): 39-49
G. Matzke et al.
45
Figure 12 Axial multidetector computed tomography image shows a middle-sized incisional hernia (curved arrow) con-taining small bowel loops (straight arrow).
Figure 13 Axial multidetector computed tomography iden-tifies a transverse incisional hernia (curved arrow) showing eventration of the bladder roof (straight arrow).
Figure 14 Axial multidetector computed tomography image shows a large epigastric hernia (curved arrow) with protru-sion of the left lobe of liver (black straight arrow), pyloric antrum and bowel loops (white straight arrow).
a b
Figure 15 Axial (a) and coronal (b) multidetector computed tomography images show markedly distended gallbladder hernia-tion (curved arrows).

Rev. Argent. Radiol. 2017;81(1): 39-49
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography
46
Figure 16 Axial multidetector computed tomography image of an umbilical hernia (curved arrow) with a solid implant (straight arrow) secondary to an ovarian tumor (Sister Mary Joseph’s node).
Figure 17 Axial multidetector computed tomography of the abdomen shows an umbilical hernia (curved arrow) with peri-toneal fat content (white straight arrow) and ascites (black straight arrow).
Figure 18 Axial multidetector computed tomographyimage shows lumbar hernia (curved arrow) containing part of the right lobe of liver (straight arrow).
Figure 19 Axial multidetector computed tomographyimage shows a large bilateral inguinal hernia (curved arrows) with distended small bowel loops (straight arrow).
a b
Figure 20 Axial (a) and sagittal (b) multidetector computed tomography detects an inguinal hernia (curved arrow) with protrud-ing bladder roof (cystocele) (straight arrow).

Rev. Argent. Radiol. 2017;81(1): 39-49
G. Matzke et al.
47
Figure 21 Axial multidetector computed tomography identi-fies a small right inguinal hernia (curved arrow) containing the vermiform appendix (straight arrow), confirmed by sur-gery (Amyand hernia).
a b
Figure 22 Axial (a) and coronal (b) multidetector computed tomography images showvermiform appendix (curved arrow) within the femoral canal, medial to the femoral vessels (straight arrow). This hernia is known as De Garengeot hernia.
Figure 23 Axial multidetector computed tomography shows a transverse incisional hernia (curved arrow) containing a transplanted kidney (black straight arrow) and the bladder roof (white straight arrow).
Figure 24 Sagital multidetector computed tomography of an incisional hernia (curved arrow) with protruding bladder (straight arrow).

Rev. Argent. Radiol. 2017;81(1): 39-49
A Tour of the Abdominal Wall: An Assessment of Hernias by Multidetector Computed Tomography
48
ContentContent is associated with the different sites of abdominal wall weakness. Epigastric hernias may involve herniation of the pyloric antrum, left lobe of the liver (fig. 14) or gallblad-der (fig. 15). Umbilical hernias may contain peritoneal fat, bowel loops, metastatic implants (Sister Mary Joseph’s node) (fig. 16) or ascitic fluid(fig. 17). Spigelian hernias usually con-tain fat and bowel loops, while obturator hernias are often detected because the patient presents with symptoms of mechanical bowel obstruction that help in diagnosis. Lum-bar hernias may involve herniation of fat, the pole of kidney or the right lobe of the liver (fig. 18). Inguinal hernias have highly varied contents, although peritoneal fat and loops are the most common (fig. 19). They may also involve herniation of intrapelvic organs, such as the bladder (cystocele) (fig. 20) or the appendix (Amyandhernia)20 (fig. 21) and, if herniation of the appendix occurs within the crural canal, it is called De Garengeto hernia9 (fig. 22). Finally, incisional hernias contain large and small bowel loops, transplanted kidneys (fig. 23) and bladders (fig. 24)
ConclusionKnowledge of the abdominal wall anatomy and the relation-ship of hernias with vascular structures, fascial and muscu-lar layers is extremely important for determining the type of hernia. MDCT has demonstratedto be very useful for such purpose and can even identify the contents of hernias.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received suf-ficient information and have provided their written informed consent.
Conflicts of interestThe authors declare no conflicts of interest, except for Dr. Kozima, who declares a possible conflict of interest as mem-ber of the Executive Committee of SAR.
References1. Merello Lardies J. Pared abdominal. Hernias y eventraciones. En: Ferraina
P, Oria A, editors. Cirugía de Michans., 35. Buenos Aires: El Ateneo; 2008. p. 417---50.
2. Murphy KP, O’Connor OJ, Maher MM. Adult abdominal hernias. AJR Am J Roentgenol. 2014;202:W506---11.
3. Balfe D, Gratz B, Peterson C. Anatomía normal del abdomen y la pelvis. En: Lee JK, Sagel SS, Stanley RJ, Heiken JP, editores. Computed body to-mography with MRI correlation. Philadelphia: Lippincott Williams & Wil-liams; 2007. p. 10.
4. Jeffrey B, Federle MP. Hernias externas. En: Federle MP, Jefrey BR, Wood-ward PJ, Borhani A, editores. Diagnostic imaging:. Abdomen. Madrid: Marbán; 2011. p. 2.
5. Koulouris G. Imaging review of groin pain in elite athletes: an anatomic approach to imaging findings. AJR Am J Roentgenol. 2008;191:962---72.
6. Cubero Carralero J, Gonzalez Cabestreros S, Corral Ramos B, Fernandez Jara J, Ferreiro Arguelles C, Martinez-Perez M. Let The Hook Sign get you off the hook: an easy way to diagnose indirect inguinal hernias with axial images in MDCT. Radiological Society of North America, 2013. Scientific As-sembly and Annual Meeting, December 1-6, 2013, Chicago IL. Disponible en: http://archive.rsna.org/2013/13016741.html (Consultado Mar 2016).
7. Burkhardt J, Arshanskiy Y, Munson JL, Scholz FJ. Diagnosis of inguinal re-gion hernias with axial CT: the lateral crescent sign and other key findings. Radiographics. 2011;31:E1---12.
8. Shadbolt CL, Heinze SB, Dietrich RB. Imaging of groin masses: in-guinal anatomy and pathologic conditions revisited. Radiographics. 2001;21:S261---71.
9. Chin CM, Lim KL. Appendicitis: atypical and challenging CT appearances. Radiographics. 2015;35:123---4.
10. Cubillo E. Obturator hernia diagnosed by computed tomography. AJR Am J Roentgenol. 1983;140:735---6.
11. Keogan MT, Paulson EK. Gastrointestinal case of the day. Obturator hernia causing small bowel obstruction. AJR Am J Roentgenol. 1995;165:192---3.
Document downloaded from http://www.elsevier.es, day 21/04/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
12. Harrison LA, Keesling CC, Martin NL, Lee KR, Wetzel LH. Abdominal wall hernias: review of herniography and correlation with cross-sectional imag-ing. Radiographics. 1995;15:315---32.
13. Baker ME, Weinerth JL, Andriani RT, Cohan RH, Dunnick NR. Lumbar her-nia: diagnosis by CT. AJR Am J Roentgenol. 1987;148:565---7.
14. Lassandro F, Iasiello F, Pizza NL, Valente T, Stefano ML, Grassi R, et al. Abdominal hernias: radiological features. World J Gastrointest Endosc. 2011;3:110---7.
15. Erdas E, Licheri S, Caló PG, Pomata M. Acquired abdominal intercos-tal hernia: case report and systematic review of the literature. Hernia. 2014;18:607---15.
16. Carre˜no Sáenz O, Montilla Navarro E, Aguilar Martí M, Bonafé Diana S, Carbonell Tatay F. Hernia intercostal abdominal traumática con preser-vación de diafragma: comunicación de un caso. Rev Hispanoam Hernia. 2013;1:105---7.
17. Aguirre DA, Santosa AC, Casola G, Sirlin CB. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi---detector row CT. Radiographics. 2005;25: 1501---20.
18. Ghahremani GG, Jimenez MA, Rosenfeld M, Rochester D. CT diagnosis of occult incisional hernias. AJR Am J Roentgenol. 1987;148:139---42.
19. Zarvan NP, Lee FT Jr, Yandow DR, Unger JS. Abdominal hernias: CT find-ings. AJR Am J Roentgenol. 1995;164:1391---5.
20. Bhosale PR, Patnana M, Viswanathan C, Szklaruk J. The inguinal canal: anatomy and imaging features of common and uncommon masses. Ra-diographics. 2008;28:819---35.
Related Documents










