http://aes.sagepub.com/ Aesthetic Surgery Journal http://aes.sagepub.com/content/32/1/46 The online version of this article can be found at: DOI: 10.1177/1090820X11430829 2012 32: 46 Aesthetic Surgery Journal Forster-Perlini, Catherine Hwang, Raymond Douglas and Robert A. Goldberg Konstantinos I. Papageorgiou, Ronald Mancini, Helene Chokron Garneau, Shu-Hong Chang, Imran Jarullazada, Adam King, Erin A Three-Dimensional Construct of the Aging Eyebrow: The Illusion of Volume Loss Published by: http://www.sagepublications.com On behalf of: American Society for Aesthetic Plastic Surgery can be found at: Aesthetic Surgery Journal Additional services and information for http://aes.sagepub.com/cgi/alerts Email Alerts: http://aes.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Jan 9, 2012 Version of Record >> by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from by guest on October 11, 2013 aes.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://aes.sagepub.com/Aesthetic Surgery Journal
http://aes.sagepub.com/content/32/1/46The online version of this article can be found at:
DOI: 10.1177/1090820X11430829
2012 32: 46Aesthetic Surgery JournalForster-Perlini, Catherine Hwang, Raymond Douglas and Robert A. Goldberg
Konstantinos I. Papageorgiou, Ronald Mancini, Helene Chokron Garneau, Shu-Hong Chang, Imran Jarullazada, Adam King, ErinA Three-Dimensional Construct of the Aging Eyebrow: The Illusion of Volume Loss
Published by:
http://www.sagepublications.com
On behalf of:
American Society for Aesthetic Plastic Surgery
can be found at:Aesthetic Surgery JournalAdditional services and information for
http://aes.sagepub.com/cgi/alertsEmail Alerts:
http://aes.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Jan 9, 2012Version of Record >>
by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from by guest on October 11, 2013aes.sagepub.comDownloaded from

Oculoplastics
Aesthetic Surgery Journal32(1) 46 –57© 2012 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X11430829www.aestheticsurgeryjournal.com
The eyebrows and eyebrow fat pads are key landmarks in the aesthetic configuration of the upper face. They are important for conveying emotive expressions and, acting in continuum with the upper eyelid, they significantly affect the three-dimensional (3D) contours of the upper face.1-3 An understanding of the mechanisms underlying the aging process in this area is of paramount importance in allowing the surgeon to appropriately address age-related changes.
Gravity has long been considered the major source of facial aging, and lifting surgeries have been designed to address this issue with inconsistent results.4,5 More recently, surgeons have begun to recognize the complex
A Three-Dimensional Construct of the Aging Eyebrow: The Illusion of Volume Loss
Konstantinos I. Papageorgiou, MD; Ronald Mancini, MD; Helene Chokron Garneau, MPH; Shu-Hong Chang, MD; Imran Jarullazada, MD; Adam King; Erin Forster-Perlini, MD; Catherine Hwang, MD; Raymond Douglas, MD; and Robert A. Goldberg, MD
AbstractBackground: The eyebrows and eyebrow fat pads, key structures in upper facial aesthetics, are particularly vulnerable to age-related changes.Objectives: In this study, the authors compare the impact of aging on the eyebrows and eyebrow fat pad volume in men and women through three-dimensional (3D) volumetric analysis.Methods: Electronic medical records of patients seen at the Jules Stein Eye Institute in the Division of Orbital and Ophthalmic Plastic Surgery between 2005 and 2010 were reviewed. Patients were included if they had undergone investigative imaging of the orbit for unilateral pathology. Computed tomography (CT) scans of patients with Graves disease diagnosis, extensive orbital trauma, and/or previous eyebrow surgery were excluded. A total of 52 CT scans (24 men and 28 women) were retained for analysis. A 3D reconstruction software was used to analyze the scans and calculate volumes of the retroorbicularis oculi fat (ROOF), galeal fat (ROOF and subcutaneous fat), and soft tissue muscles.Results: Galeal and brow fat volumes showed a significant positive trend toward enlargement in women (P values of .01 and .05, respectively). Although men showed a tendency toward fat enlargement with age, this was not statistically significant. Soft tissue–muscle volume decreased significantly in aging women (9.32 mm3/y) (P = .02). Data indicated that soft tissue volume in men tended to increase with age (3.92 mm3/y) but not significantly (P = .36). Neither total volume nor brow thickness appeared to change significantly in women (P = .56, P = .73). In men, total volume and brow thickness showed weak evidence of increasing with age (P = .12, P = .22). Linear regressions of Hertel measurements with and without sex interaction showed no statistically significant trend between the amount of proptosis and the galeal or brow fat.Conclusions: Although overall eyebrow volume does not change with age, the relative contribution of fat and soft tissue to the total volume does seem to change. This pattern also differs between men and women. As women age, the fat volume increases and the soft tissue volume decreases. In men, the shift from soft tissue volume to fat volume is less pronounced. Although many clinicians have been drawn to the concept of fat volume deflation as a key element of facial aging, this study does not support this perspective in the eyebrow fat pad. An increasingly refined understanding of the dynamics of facial aging is mandatory for clinical diagnosis and will likely provide the framework from which to develop more innovative treatment options.
Keywords
aging, eyebrow, facial rejuvenation, fat
Accepted for publication June 9, 2011.
Dr. Papageorgiou is a Fellow, Ms. Chokron Garneau is a Research Coordinator, Dr. Shu-Hong Chang is a Fellow, Dr. Jarullazada is a Fellow, Mr. King is a Biostatistics assistant, Dr. Hwang is an Associate Physician Diplomat, and Dr. Goldberg is a Professor and Division Chief at the Jules Stein Eye Institute, Division of Orbital and Ophthalmic Plastic Surgery, University of California, Los Angeles, California. Dr. Mancini is an Assistant Professor at the UT Southwestern Medical Center, Dallas, Texas. Dr. Forster-Perlini is a medical student at the Bascom Palmer Eye Institute, University of Miami, Miami, Florida. Dr. Douglas is an Associate Professor, Ophthalmology and Visual Sciences, at the Kellogg Eye Center, University of Michigan, Ann Arbor, Michigan.
Corresponding Author:Dr. Konstantinos I. Papageorgiou, Jules Stein Eye Institute, 100 Stein Plaza 2-267, Los Angeles, CA 90049 USA. E-mail: [email protected]

Papageorgiou et al 47
synergy of laxity, fat dimorphism, soft tissue deflation, muscle readaptation, and bony skeleton remodeling with coarsening of the supraorbital ridge—all of which play a role in the aging of the eyebrow region.6-12 Understanding the specific morphologic effects of aging is critical for suc-cessful facial rejuvenation. To that end, we utilized 3D volumetric analysis of computed tomography (CT) scans in order to characterize volumetric changes of the eyebrow complex across different age groups, in both men and women.
MethOdsPatientsThis study was approved by the Institutional Review Board at the University of California, Los Angeles. Electronic Medical Records of patients seen at the Jules Stein Eye Institute in the Division of Orbital and Ophthalmic Plastic Surgery between 2005 and 2010 were retrospectively reviewed. Patients were included if they had undergone investigative imaging of the orbit for uni-lateral pathology. Patients with Graves disease diagnosis, extensive orbital trauma, and/or previous eyebrow sur-gery were excluded. A total of 52 CT scans (24 men and 28 women) were retained for analysis. The sample popu-lation consisted of 52 patients seen between 2001 and 2009 for unilateral pathology (neoplastic, vascular, mus-cular, neurological, lacrimal, trauma). CT scans (0.5- to 3-mm slice increments), demographic information (age, sex, and ethnicity), ocular pathology at presentation, sur-gical history of the orbit and eyebrow, and Hertel exoph-thalmometry were retrieved from the medical records. Supraorbital volumetric analysis was performed unilater-ally on the unaffected side, or, in cases in which no spe-cific orbital pathology was identified, the analyzed side was randomly selected.
CT Imaging
Mimics (Version 9.12; Materialise, Leuven, Belgium) is an image-processing software with a 3D visualization function. Research conducted by Regensburg et al13,14 showed it to be a reliable tool validated for biomedical research. Reference CT images were imported into the software, processed, ana-lyzed, and reconstructed. Volumetric calculations of the studied tissues (bone, muscle, fat) were then performed.
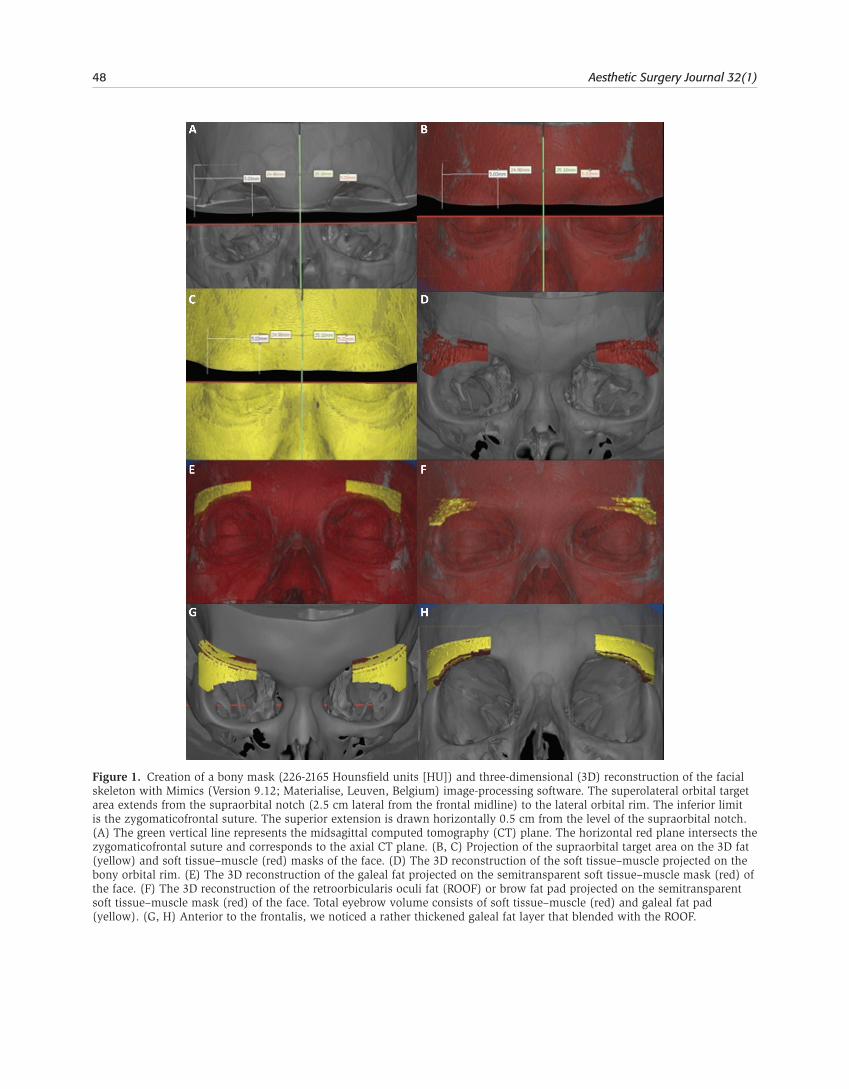
Our methodology of tissue analysis and segmentation was adapted from the approach described by Mourits.14,15 Following the creation of a bony mask (226-2165 Hounsfield units [HU]; Figure 1A-C), the 3D reconstruction of the facial skeleton was performed (Figure 1D-G). On the bony frame-work, the superolateral orbital target area was defined from the supraorbital notch (2.5 cm lateral from the frontal mid-line) to the lateral orbital rim. The inferior limit was defined as the zygomaticofrontal suture, whereas the superior extension was drawn horizontally 0.5 cm from the level of the supraorbital notch (Figure 1A-C).
These specific landmarks were selected based on the anatomic distribution of the eyebrow fat pad or retroor-bicularis oculi fat (ROOF), described as an anatomic and functional unit by Charpy in 1909.16,17 This structure, which contributes significantly to eyebrow volume and definition, extends from the midsupraorbital rim to beyond the lateral orbital rim. It lies over the superolat-eral bone and orbital septum across the upper lateral and middle eyelid region and is considered part of the overall galeal fat pad, which is responsible for the easy motility of the lower 2 cm of the forehead.18-21 The vertical height of the eyebrow fibroadipose tissue is 1 to 1.5 cm superior to the orbital rim—approximately one-third of the verti-cal orbital dimension.22 In our study, we defined the cephalad extension as a horizontal plane 0.5 cm from the supraorbital notch, with its lateral projection at an ade-quately higher level from the rim to contain the entire ROOF structure. This compartment included the orbital component of the orbicularis oculi, frontalis, and the lateral corrugator muscles embedded in the multiple galeal layers.
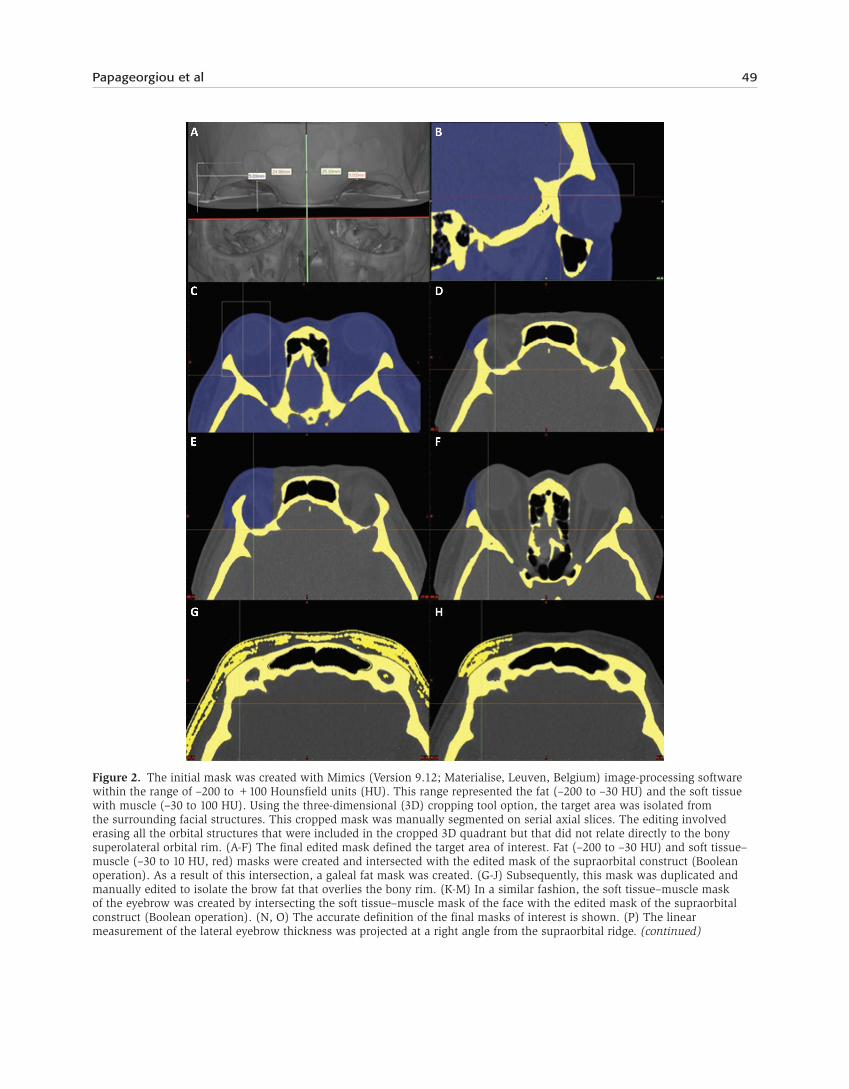
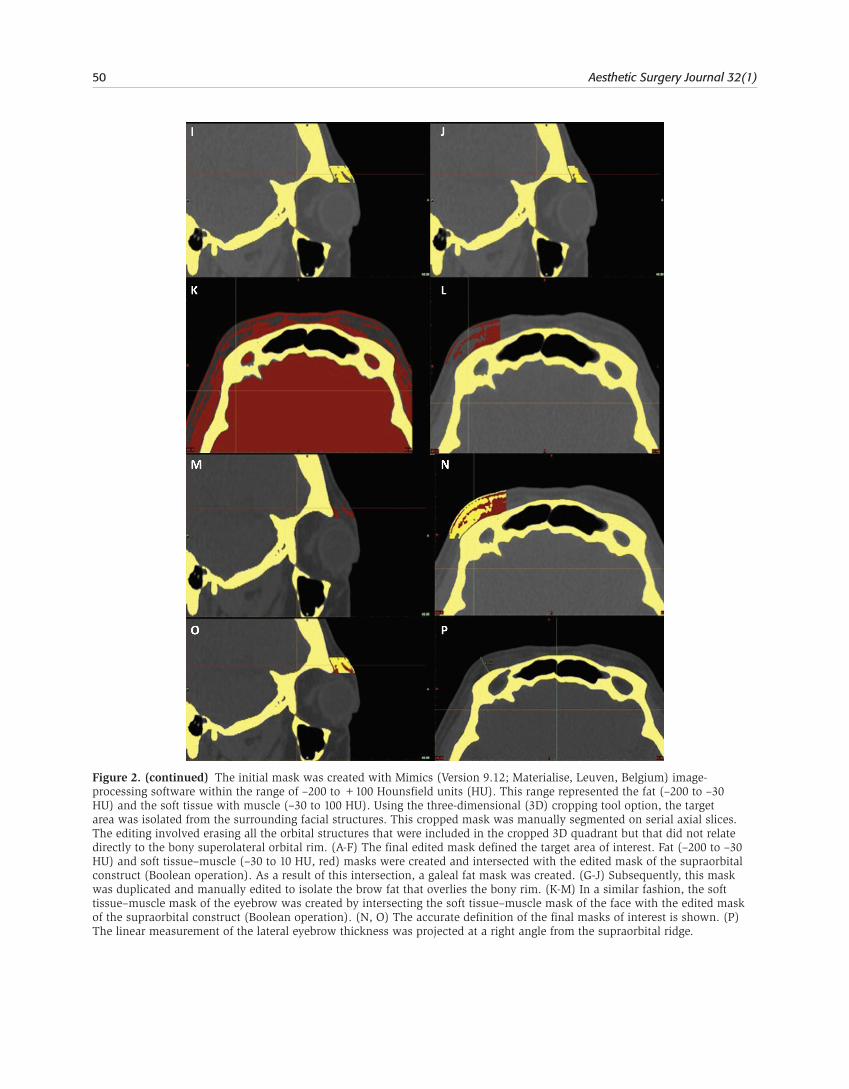
The initial mask was created within the range of –200 to +100 HU. This range included fat (–200 to –30 HU) and soft tissue with muscle (–30 to 100 HU). The 3D software tissue analysis and specific range of Hounsfield units (fat vs soft tissue) allowed for the distinction between fat and soft tissue. Any anatomical structure in the eyebrow and eyebrow fat pad that was not fat (including muscles, nerves, and vessels) was considered soft tissue. Using the 3D cropping tool, the target area was isolated from the surrounding facial structures. This cropped mask was manually segmented on serial axial slices. The editing involved removing orbital structures that were included in the cropped 3D quadrant but that did not relate directly to the bony superolateral orbital rim (Figure 2). The final mask outlines the area of interest.
The next step involved the creation of fat (–200 to –30 HU) and soft tissue–muscle (–30 to 10 HU) masks. These were intersected with the edited mask of the supraorbital construct (Boolean operation). The resulting mask defined the total fat tissue in the eyebrow area. This mask was duplicated and manually edited to isolate the brow fat or ROOF overlying the bony rim. In a similar fashion, the soft tissue–muscle mask of the eyebrow was created by intersect-ing the soft tissue–muscle mask of the face with the edited mask of the supraorbital construct (Boolean operation). Following “region growing” (computer-assisted separation of nonconnected tissues), the software three-dimensionally reconstructed the three masks of interest: soft tissue–muscle (or any structure that was not fat) (Figure 1D), total galeal fat (Figure 1E), and brow fat or ROOF (Figure 1F). Volumetric calculations were obtained and expressed in cubic millimeters (mm3).
Imaging analysis was performed by a single investigator who had substantial experience with the software (KIP). Segmentation was performed exclusively on the axial CT cuts. In addition, we evaluated the thickness of the lateral third of the eyebrow on the axial CT, as a linear measurement projected at a right angle from the supraorbital ridge.
48 Aesthetic Surgery Journal 32(1)
Figure 1. Creation of a bony mask (226-2165 Hounsfield units [HU]) and three-dimensional (3D) reconstruction of the facial skeleton with Mimics (Version 9.12; Materialise, Leuven, Belgium) image-processing software. The superolateral orbital target area extends from the supraorbital notch (2.5 cm lateral from the frontal midline) to the lateral orbital rim. The inferior limit is the zygomaticofrontal suture. The superior extension is drawn horizontally 0.5 cm from the level of the supraorbital notch. (A) The green vertical line represents the midsagittal computed tomography (CT) plane. The horizontal red plane intersects the zygomaticofrontal suture and corresponds to the axial CT plane. (B, C) Projection of the supraorbital target area on the 3D fat (yellow) and soft tissue–muscle (red) masks of the face. (D) The 3D reconstruction of the soft tissue–muscle projected on the bony orbital rim. (E) The 3D reconstruction of the galeal fat projected on the semitransparent soft tissue–muscle mask (red) of the face. (F) The 3D reconstruction of the retroorbicularis oculi fat (ROOF) or brow fat pad projected on the semitransparent soft tissue–muscle mask (red) of the face. Total eyebrow volume consists of soft tissue–muscle (red) and galeal fat pad (yellow). (G, H) Anterior to the frontalis, we noticed a rather thickened galeal fat layer that blended with the ROOF.
Papageorgiou et al 49
Figure 2. The initial mask was created with Mimics (Version 9.12; Materialise, Leuven, Belgium) image-processing software within the range of –200 to +100 Hounsfield units (HU). This range represented the fat (–200 to –30 HU) and the soft tissue with muscle (–30 to 100 HU). Using the three-dimensional (3D) cropping tool option, the target area was isolated from the surrounding facial structures. This cropped mask was manually segmented on serial axial slices. The editing involved erasing all the orbital structures that were included in the cropped 3D quadrant but that did not relate directly to the bony superolateral orbital rim. (A-F) The final edited mask defined the target area of interest. Fat (–200 to –30 HU) and soft tissue–muscle (–30 to 10 HU, red) masks were created and intersected with the edited mask of the supraorbital construct (Boolean operation). As a result of this intersection, a galeal fat mask was created. (G-J) Subsequently, this mask was duplicated and manually edited to isolate the brow fat that overlies the bony rim. (K-M) In a similar fashion, the soft tissue–muscle mask of the eyebrow was created by intersecting the soft tissue–muscle mask of the face with the edited mask of the supraorbital construct (Boolean operation). (N, O) The accurate definition of the final masks of interest is shown. (P) The linear measurement of the lateral eyebrow thickness was projected at a right angle from the supraorbital ridge. (continued)
50 Aesthetic Surgery Journal 32(1)
Figure 2. (continued) The initial mask was created with Mimics (Version 9.12; Materialise, Leuven, Belgium) image-processing software within the range of –200 to +100 Hounsfield units (HU). This range represented the fat (–200 to –30 HU) and the soft tissue with muscle (–30 to 100 HU). Using the three-dimensional (3D) cropping tool option, the target area was isolated from the surrounding facial structures. This cropped mask was manually segmented on serial axial slices. The editing involved erasing all the orbital structures that were included in the cropped 3D quadrant but that did not relate directly to the bony superolateral orbital rim. (A-F) The final edited mask defined the target area of interest. Fat (–200 to –30 HU) and soft tissue–muscle (–30 to 10 HU, red) masks were created and intersected with the edited mask of the supraorbital construct (Boolean operation). As a result of this intersection, a galeal fat mask was created. (G-J) Subsequently, this mask was duplicated and manually edited to isolate the brow fat that overlies the bony rim. (K-M) In a similar fashion, the soft tissue–muscle mask of the eyebrow was created by intersecting the soft tissue–muscle mask of the face with the edited mask of the supraorbital construct (Boolean operation). (N, O) The accurate definition of the final masks of interest is shown. (P) The linear measurement of the lateral eyebrow thickness was projected at a right angle from the supraorbital ridge.
Papageorgiou et al 51
Results
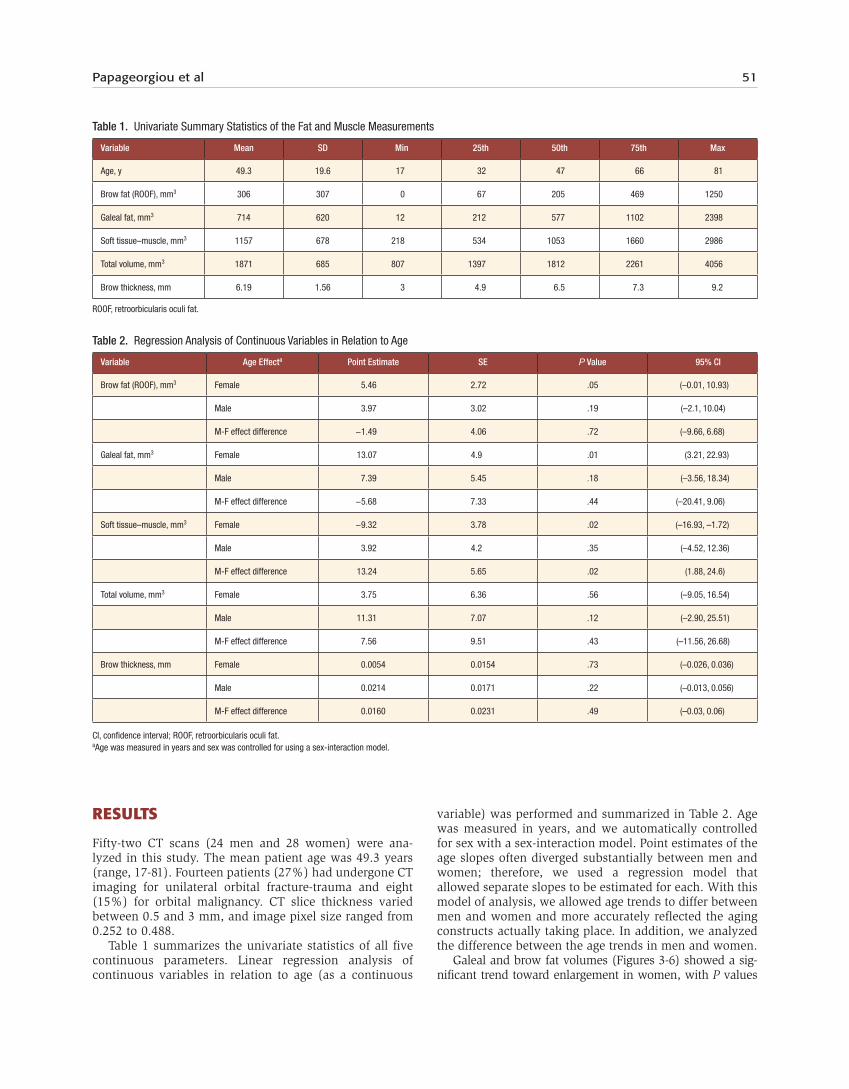
Fifty-two CT scans (24 men and 28 women) were ana-lyzed in this study. The mean patient age was 49.3 years (range, 17-81). Fourteen patients (27%) had undergone CT imaging for unilateral orbital fracture-trauma and eight (15%) for orbital malignancy. CT slice thickness varied between 0.5 and 3 mm, and image pixel size ranged from 0.252 to 0.488.
Table 1 summarizes the univariate statistics of all five continuous parameters. Linear regression analysis of continuous variables in relation to age (as a continuous
variable) was performed and summarized in Table 2. Age was measured in years, and we automatically controlled for sex with a sex-interaction model. Point estimates of the age slopes often diverged substantially between men and women; therefore, we used a regression model that allowed separate slopes to be estimated for each. With this model of analysis, we allowed age trends to differ between men and women and more accurately reflected the aging constructs actually taking place. In addition, we analyzed the difference between the age trends in men and women.
Galeal and brow fat volumes (Figures 3-6) showed a sig-nificant trend toward enlargement in women, with P values
Table 1. Univariate Summary Statistics of the Fat and Muscle Measurements
Variable Mean SD Min 25th 50th 75th Max
Age, y 49.3 19.6 17 32 47 66 81
Brow fat (ROOF), mm3 306 307 0 67 205 469 1250
Galeal fat, mm3 714 620 12 212 577 1102 2398
Soft tissue–muscle, mm3 1157 678 218 534 1053 1660 2986
Total volume, mm3 1871 685 807 1397 1812 2261 4056
Brow thickness, mm 6.19 1.56 3 4.9 6.5 7.3 9.2
ROOF, retroorbicularis oculi fat.
Table 2. Regression Analysis of Continuous Variables in Relation to Age
Variable Age Effecta Point Estimate SE P Value 95% CI
Brow fat (ROOF), mm3 Female 5.46 2.72 .05 (–0.01, 10.93)
Male 3.97 3.02 .19 (–2.1, 10.04)
M-F effect difference −1.49 4.06 .72 (–9.66, 6.68)
Galeal fat, mm3 Female 13.07 4.9 .01 (3.21, 22.93)
Male 7.39 5.45 .18 (–3.56, 18.34)
M-F effect difference −5.68 7.33 .44 (–20.41, 9.06)
Soft tissue–muscle, mm3 Female −9.32 3.78 .02 (–16.93, –1.72)
Male 3.92 4.2 .35 (–4.52, 12.36)
M-F effect difference 13.24 5.65 .02 (1.88, 24.6)
Total volume, mm3 Female 3.75 6.36 .56 (–9.05, 16.54)
Male 11.31 7.07 .12 (–2.90, 25.51)
M-F effect difference 7.56 9.51 .43 (–11.56, 26.68)
Brow thickness, mm Female 0.0054 0.0154 .73 (–0.026, 0.036)
Male 0.0214 0.0171 .22 (–0.013, 0.056)
M-F effect difference 0.0160 0.0231 .49 (–0.03, 0.06)
CI, confidence interval; ROOF, retroorbicularis oculi fat.aAge was measured in years and sex was controlled for using a sex-interaction model.
52 Aesthetic Surgery Journal 32(1)
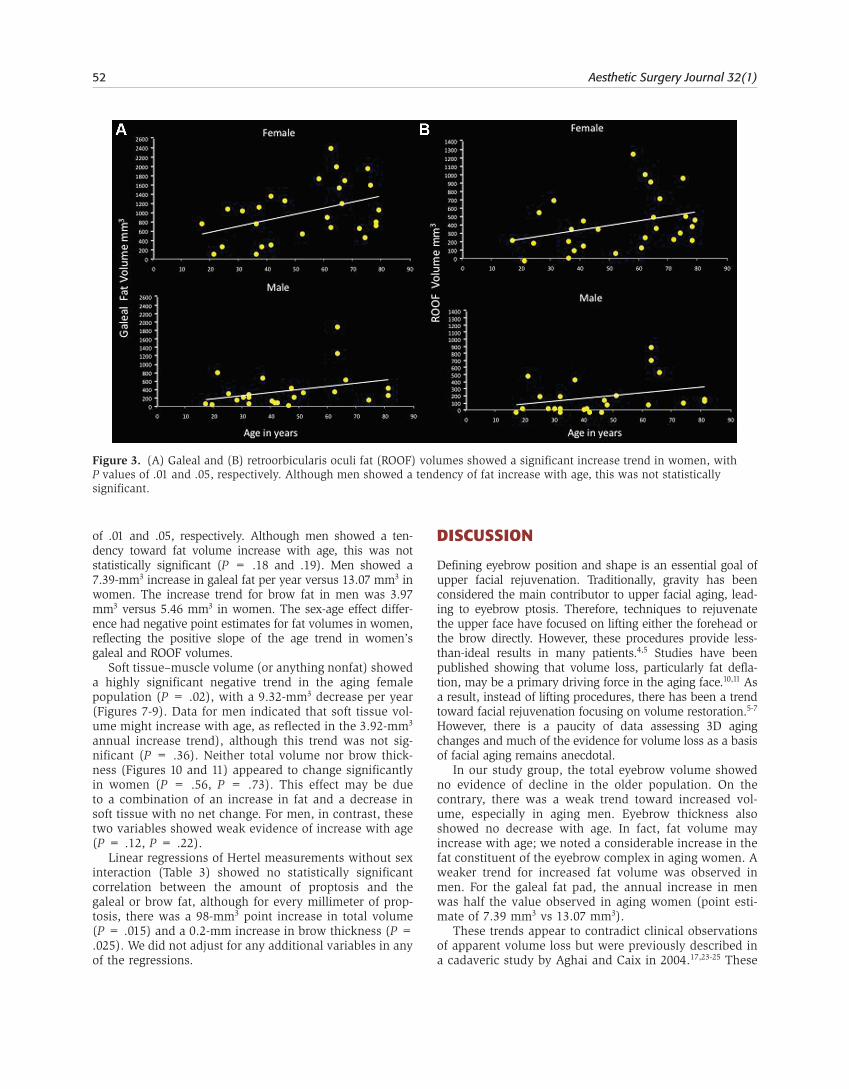
of .01 and .05, respectively. Although men showed a ten-dency toward fat volume increase with age, this was not statistically significant (P = .18 and .19). Men showed a 7.39-mm3 increase in galeal fat per year versus 13.07 mm3 in women. The increase trend for brow fat in men was 3.97 mm3 versus 5.46 mm3 in women. The sex-age effect differ-ence had negative point estimates for fat volumes in women, reflecting the positive slope of the age trend in women’s galeal and ROOF volumes.
Soft tissue–muscle volume (or anything nonfat) showed a highly significant negative trend in the aging female population (P = .02), with a 9.32-mm3 decrease per year (Figures 7-9). Data for men indicated that soft tissue vol-ume might increase with age, as reflected in the 3.92-mm3 annual increase trend), although this trend was not sig-nificant (P = .36). Neither total volume nor brow thick-ness (Figures 10 and 11) appeared to change significantly in women (P = .56, P = .73). This effect may be due to a combination of an increase in fat and a decrease in soft tissue with no net change. For men, in contrast, these two variables showed weak evidence of increase with age (P = .12, P = .22).
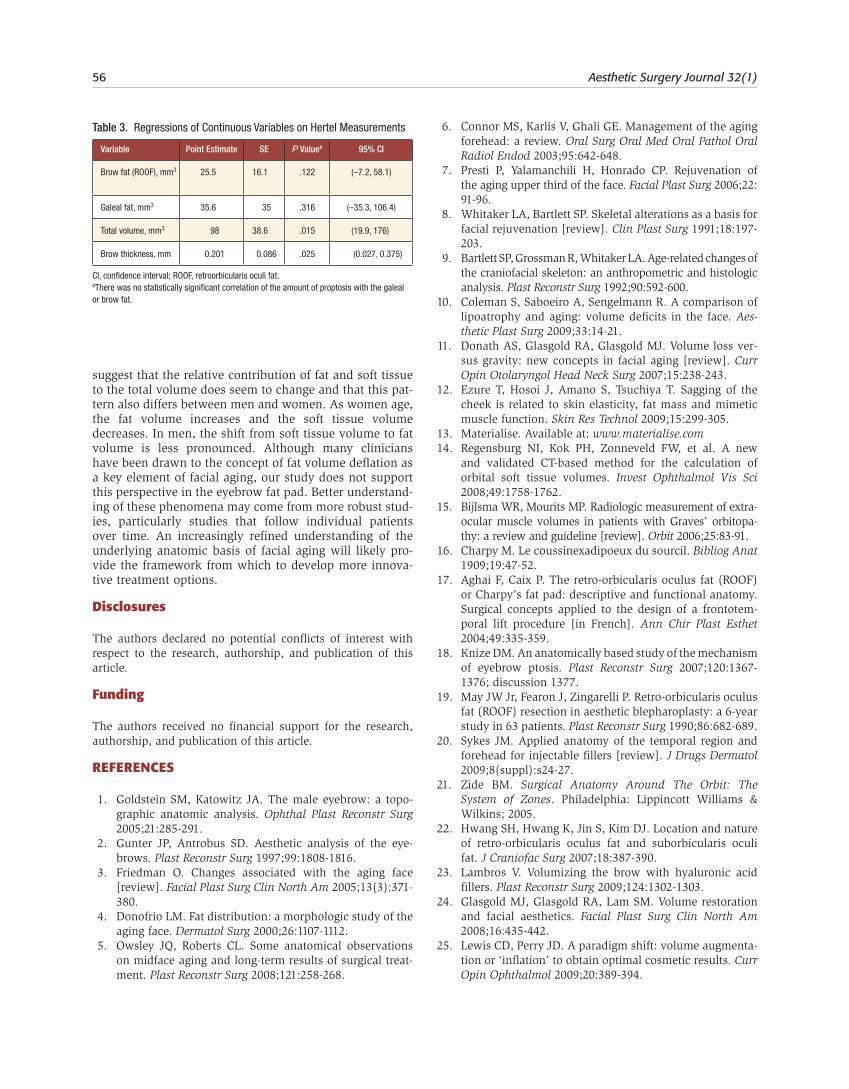
Linear regressions of Hertel measurements without sex interaction (Table 3) showed no statistically significant correlation between the amount of proptosis and the galeal or brow fat, although for every millimeter of prop-tosis, there was a 98-mm3 point increase in total volume (P = .015) and a 0.2-mm increase in brow thickness (P = .025). We did not adjust for any additional variables in any of the regressions.
disCussiOn
Defining eyebrow position and shape is an essential goal of upper facial rejuvenation. Traditionally, gravity has been considered the main contributor to upper facial aging, lead-ing to eyebrow ptosis. Therefore, techniques to rejuvenate the upper face have focused on lifting either the forehead or the brow directly. However, these procedures provide less-than-ideal results in many patients.4,5 Studies have been published showing that volume loss, particularly fat defla-tion, may be a primary driving force in the aging face.10,11 As a result, instead of lifting procedures, there has been a trend toward facial rejuvenation focusing on volume restoration.5-7 However, there is a paucity of data assessing 3D aging changes and much of the evidence for volume loss as a basis of facial aging remains anecdotal.
In our study group, the total eyebrow volume showed no evidence of decline in the older population. On the contrary, there was a weak trend toward increased vol-ume, especially in aging men. Eyebrow thickness also showed no decrease with age. In fact, fat volume may increase with age; we noted a considerable increase in the fat constituent of the eyebrow complex in aging women. A weaker trend for increased fat volume was observed in men. For the galeal fat pad, the annual increase in men was half the value observed in aging women (point esti-mate of 7.39 mm3 vs 13.07 mm3).
These trends appear to contradict clinical observations of apparent volume loss but were previously described in a cadaveric study by Aghai and Caix in 2004.17,23-25 These
Figure 3. (A) Galeal and (B) retroorbicularis oculi fat (ROOF) volumes showed a significant increase trend in women, with P values of .01 and .05, respectively. Although men showed a tendency of fat increase with age, this was not statistically significant.

Papageorgiou et al 53
authors demonstrated an age-related increase in the ROOF (or Charpy’s fat pad) and suggested this trend might explain the “masculinization” of the eyebrows in aging women. There is good clinical evidence that individual fat compartments age independently. The eyebrow fat pad may exhibit distinct behavior with age when compared to the rest of the face. Additionally, lower eyelid magnetic resonance imaging (MRI) has shown similar infraorbital fat expansion with age, and others described the orbital fat as resistant to lipolysis.26,27
In our study, there was no statistically significant cor-relation between the amount of proptosis and the galeal or brow fat, although for every millimeter of proptosis, there was a 98-mm3 point increase in total volume. Although galeal facial planes are less discernable with age, galeal compartmentalization could minimize proptotic anterosu-perior redistribution of preseptal fat across the supraorbi-tal rim. Also, although fat volume increased, the soft
tissue–muscle volume decreased with age in women. Menopause might account for the lack of total volume change in the aging female eyebrow, as increasing fat vol-ume balances decreased soft tissue volume. In women, declining estrogen levels are associated with a variety of cutaneous changes, many of which can be improved with estrogen supplementation. Postmenopausal estrogen dep-rivation is related to epidermal atrophy and thinning, as well as declining dermal collagen content.28-31 Hormonal changes in women could explain the difference in observed distributional shifts compared to men, who may have slightly increased total eyebrow volume with age.
In 2007, Le Louarn et al32 introduced the “facial recurve concept,” stating that the increased resting tone and repeated contractions of facial mimetic muscles change the shape and 3D morphology of the overlying and under-lying fat distribution. The lack of frontalis and corrugator muscles at the lateral third of the eyebrow might be an additional factor affecting the volumetric increase of eye-brow fat with aging. These findings may appear counter-intuitive at first. If eyebrow volume does not decrease with age, what accounts for the appearance of the aging eye-brow, and why does adding volume to the lateral eyebrow seem to rejuvenate the periorbital complex? Gunter and Antrobus’s two-part study2 on eyebrow aesthetics showed that most surgeons preferred recontouring of the brow-eyelid continuum rather than frank elevation, and Donath et al11 highlighted lipoaugmentation of the superior orbital rim and conservative upper blepharoplasty as the means to achieve more youthful aesthetics. Perhaps qualitative replacement of soft tissue–muscle with fat lacks the inher-ent colloidal components, proteins, hyaluronan, fluidics, or osmotic aspects essential for the youthful texture and appearance of the eyebrow. Additionally, age-related skin changes play a role in a dynamic aesthetic, leading some authors to suggest that thinning and loss of skin elasticity can create a false impression of soft tissue deflation and brow ptosis.1,11 Therefore, the addition of volume in the aging eyebrow can restore a youthful skin texture.
Figure 4. A 21-year-old woman with eyebrow fat representing 18% of the total estimated volume (264 mm3 over the 1393 mm3 of the total volume) is shown. The major part of the eyebrow fullness is due to the contribution of soft tissue–muscle.
Figure 5. This 76-year-old woman shows age-related increase of the galeal fat pad (including the retroorbicularis oculi fat). Eighty-one percent of the total eyebrow volume is represented by an increased fat constituent.
Figure 6. This 67-year-old woman shows age-related increase of the eyebrow fat constituent. Seventy-five percent of the eyebrow volume is represented by the expanded fat volume (1690 mm3 of galeal volume out of 2269 mm3).
54 Aesthetic Surgery Journal 32(1)
As the supraorbital rim widens and deepens with age, more volume is required to maintain the 3D projection of the eyebrow.8,9 The increased orbital width and superome-dial height of the orbit lead to an accordion-like spreading of overlying tissues. This might explain the relative main-tenance of eyebrow volume on 3D analysis and the clinical appearance of a deflated supraorbital region. This concept
represents a twisting of the “concertina” effect described by Pessa et al33 for the relationship between soft tissue changes and reduced height of the aging maxilla.
There are inherent flaws in our study. Due to its retro-spective nature, it was not possible to obtain longitudinal measurements for our sample. This would have been valu-able to assess changes in volume over time. Furthermore, it is also virtually impossible to select patients at the same point in their aging process because there is a great varia-tion in the aging process between individuals. Therefore, to overcome these obstacles, we analyzed age as a linear rather than as a categorical parameter. Sex was controlled for the whole analysis. It is also possible that the dynamic effect of gravity on brow position was underestimated, as CT imaging was acquired while the patients were supine. Perhaps in the supine position, the relationship between brow ptosis and volume is distorted, resulting in errone-ous calculations. If this were the case, however, the analy-sis would likely show an increase in volume with age. Furthermore, it is not clear whether the eyebrow descends with age.11 Matros et al34 described paradoxical elevation of the eyebrow with age, especially in women, and Lambros35,36 showed that 71% of eyebrows were either stable or visibly elevated with age. Body mass index (BMI) scores were also not available for correlation, since in the clinical setting of an oculoplastic service, the BMI is not routinely assessed. A potential correlation between BMI and eyebrow volume might have been interesting, although it would have been a challenge to define, assess, or grade facial weight and its impact on eyebrow volume. An increased BMI does not necessarily equate to a “heavy” face. In addition, the study group of 52 patients should offer a balanced distribution of anthropometric-biometric indexes in both younger and older patients.
If volume loss, particularly fat deflation, does not fully explain aging of the supraorbital complex, what are the clinical implications for designing and implementing
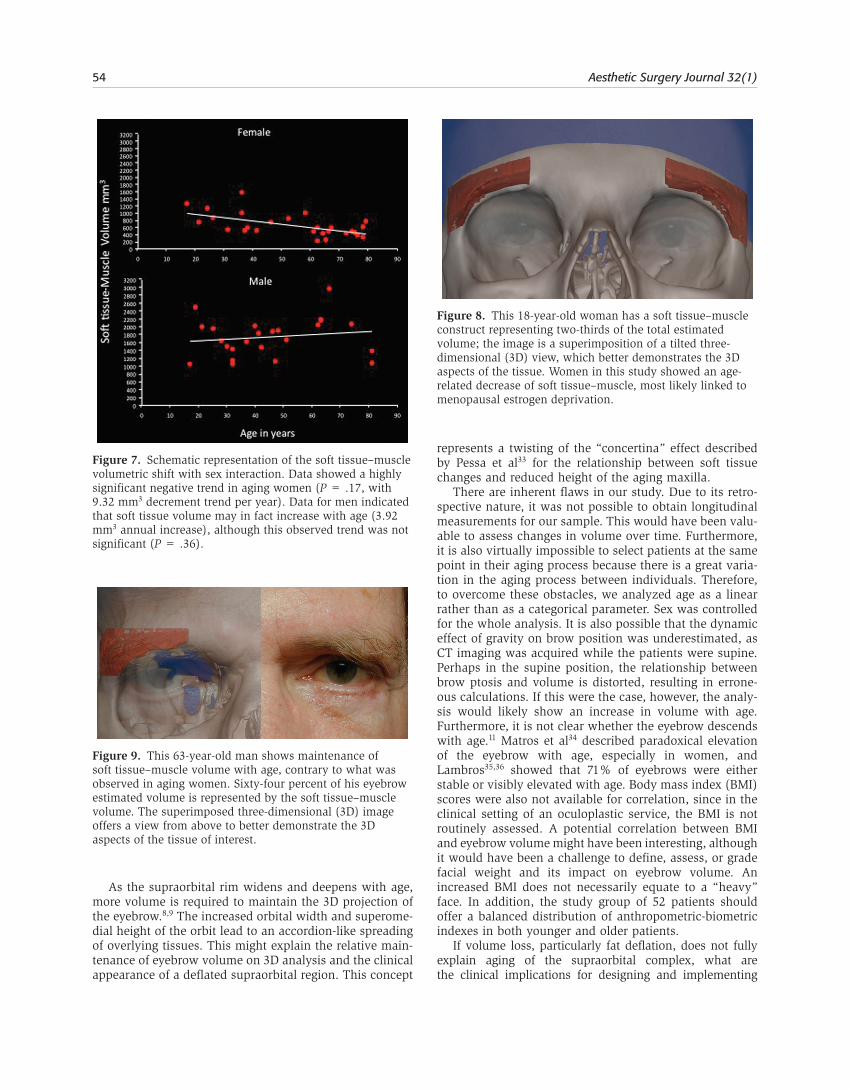
Figure 7. Schematic representation of the soft tissue–muscle volumetric shift with sex interaction. Data showed a highly significant negative trend in aging women (P = .17, with 9.32 mm3 decrement trend per year). Data for men indicated that soft tissue volume may in fact increase with age (3.92 mm3 annual increase), although this observed trend was not significant (P = .36).
Figure 8. This 18-year-old woman has a soft tissue–muscle construct representing two-thirds of the total estimated volume; the image is a superimposition of a tilted three-dimensional (3D) view, which better demonstrates the 3D aspects of the tissue. Women in this study showed an age-related decrease of soft tissue–muscle, most likely linked to menopausal estrogen deprivation.
Figure 9. This 63-year-old man shows maintenance of soft tissue–muscle volume with age, contrary to what was observed in aging women. Sixty-four percent of his eyebrow estimated volume is represented by the soft tissue–muscle volume. The superimposed three-dimensional (3D) image offers a view from above to better demonstrate the 3D aspects of the tissue of interest.
Papageorgiou et al 55
rejuvenating therapeutic approaches? Preservation of eye-brow volume with age, combined with the apparent orbital hollowing, accentuates the impact of light reflections and shadows on the eye and creates a false impression of eye-brow ptosis.24 Adding volume to the orbital sulcus and eyebrow-eyelid continuum can minimize the impact of eyebrow shadowing and camouflage the physiologic orbital hollowing. Rejuvenation should ideally be based on analy-sis of the specific anatomic changes involved in aging. These dynamics are secondary to complex interactions of
endocrine changes,28,29 skin laxity alterations,30,31 bony skel-etal remodeling,37 and fat/soft tissue compartment redistri-bution,38 especially in aging women.
COnClusiOns
Our pilot study suggests that eyebrow volume may not decrease with age and furthermore that the fat component may actually increase with age. Specifically, our results
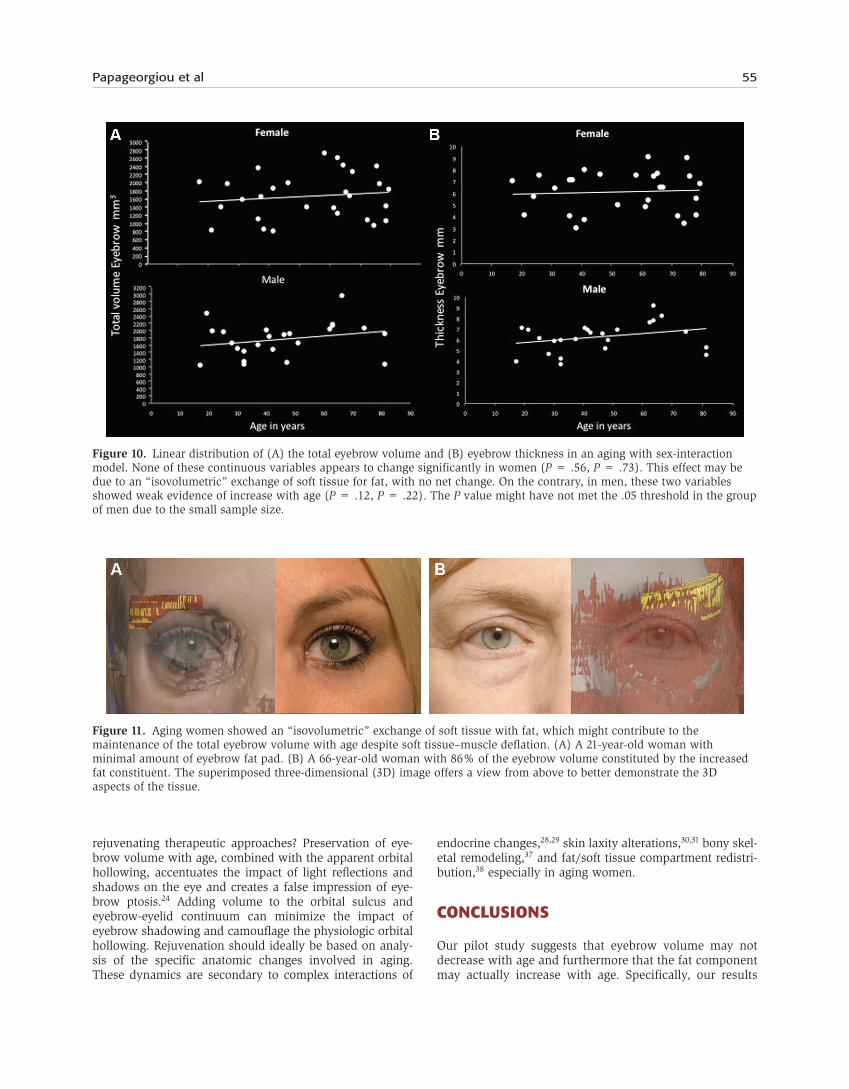
Figure 11. Aging women showed an “isovolumetric” exchange of soft tissue with fat, which might contribute to the maintenance of the total eyebrow volume with age despite soft tissue–muscle deflation. (A) A 21-year-old woman with minimal amount of eyebrow fat pad. (B) A 66-year-old woman with 86% of the eyebrow volume constituted by the increased fat constituent. The superimposed three-dimensional (3D) image offers a view from above to better demonstrate the 3D aspects of the tissue.
Figure 10. Linear distribution of (A) the total eyebrow volume and (B) eyebrow thickness in an aging with sex-interaction model. None of these continuous variables appears to change significantly in women (P = .56, P = .73). This effect may be due to an “isovolumetric” exchange of soft tissue for fat, with no net change. On the contrary, in men, these two variables showed weak evidence of increase with age (P = .12, P = .22). The P value might have not met the .05 threshold in the group of men due to the small sample size.
56 Aesthetic Surgery Journal 32(1)
suggest that the relative contribution of fat and soft tissue to the total volume does seem to change and that this pat-tern also differs between men and women. As women age, the fat volume increases and the soft tissue volume decreases. In men, the shift from soft tissue volume to fat volume is less pronounced. Although many clinicians have been drawn to the concept of fat volume deflation as a key element of facial aging, our study does not support this perspective in the eyebrow fat pad. Better understand-ing of these phenomena may come from more robust stud-ies, particularly studies that follow individual patients over time. An increasingly refined understanding of the underlying anatomic basis of facial aging will likely pro-vide the framework from which to develop more innova-tive treatment options.
disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
ReFeRenCes
1. Goldstein SM, Katowitz JA. The male eyebrow: a topo-graphic anatomic analysis. Ophthal Plast Reconstr Surg 2005;21:285-291.
2. Gunter JP, Antrobus SD. Aesthetic analysis of the eye-brows. Plast Reconstr Surg 1997;99:1808-1816.
3. Friedman O. Changes associated with the aging face [review]. Facial Plast Surg Clin North Am 2005;13(3):371-380.
4. Donofrio LM. Fat distribution: a morphologic study of the aging face. Dermatol Surg 2000;26:1107-1112.
5. Owsley JQ, Roberts CL. Some anatomical observations on midface aging and long-term results of surgical treat-ment. Plast Reconstr Surg 2008;121:258-268.
6. Connor MS, Karlis V, Ghali GE. Management of the aging forehead: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:642-648.
7. Presti P, Yalamanchili H, Honrado CP. Rejuvenation of the aging upper third of the face. Facial Plast Surg 2006;22: 91-96.
8. Whitaker LA, Bartlett SP. Skeletal alterations as a basis for facial rejuvenation [review]. Clin Plast Surg 1991;18:197-203.
9. Bartlett SP, Grossman R, Whitaker LA. Age-related changes of the craniofacial skeleton: an anthropometric and histologic analysis. Plast Reconstr Surg 1992;90:592-600.
10. Coleman S, Saboeiro A, Sengelmann R. A comparison of lipoatrophy and aging: volume deficits in the face. Aes-thetic Plast Surg 2009;33:14-21.
11. Donath AS, Glasgold RA, Glasgold MJ. Volume loss ver-sus gravity: new concepts in facial aging [review]. Curr Opin Otolaryngol Head Neck Surg 2007;15:238-243.
12. Ezure T, Hosoi J, Amano S, Tsuchiya T. Sagging of the cheek is related to skin elasticity, fat mass and mimetic muscle function. Skin Res Technol 2009;15:299-305.
13. Materialise. Available at: www.materialise.com 14. Regensburg NI, Kok PH, Zonneveld FW, et al. A new
and validated CT-based method for the calculation of orbital soft tissue volumes. Invest Ophthalmol Vis Sci 2008;49:1758-1762.
15. Bijlsma WR, Mourits MP. Radiologic measurement of extra-ocular muscle volumes in patients with Graves’ orbitopa-thy: a review and guideline [review]. Orbit 2006;25:83-91.
16. Charpy M. Le coussinexadipoeux du sourcil. Bibliog Anat 1909;19:47-52.
17. Aghai F, Caix P. The retro-orbicularis oculus fat (ROOF) or Charpy’s fat pad: descriptive and functional anatomy. Surgical concepts applied to the design of a frontotem-poral lift procedure [in French]. Ann Chir Plast Esthet 2004;49:335-359.
18. Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg 2007;120:1367-1376; discussion 1377.
19. May JW Jr, Fearon J, Zingarelli P. Retro-orbicularis oculus fat (ROOF) resection in aesthetic blepharoplasty: a 6-year study in 63 patients. Plast Reconstr Surg 1990;86:682-689.
20. Sykes JM. Applied anatomy of the temporal region and forehead for injectable fillers [review]. J Drugs Dermatol 2009;8(suppl):s24-27.
21. Zide BM. Surgical Anatomy Around The Orbit: The System of Zones. Philadelphia: Lippincott Williams & Wilkins; 2005.
22. Hwang SH, Hwang K, Jin S, Kim DJ. Location and nature of retro-orbicularis oculus fat and suborbicularis oculi fat. J Craniofac Surg 2007;18:387-390.
23. Lambros V. Volumizing the brow with hyaluronic acid fillers. Plast Reconstr Surg 2009;124:1302-1303.
24. Glasgold MJ, Glasgold RA, Lam SM. Volume restoration and facial aesthetics. Facial Plast Surg Clin North Am 2008;16:435-442.
25. Lewis CD, Perry JD. A paradigm shift: volume augmenta-tion or ‘inflation’ to obtain optimal cosmetic results. Curr Opin Ophthalmol 2009;20:389-394.
Table 3. Regressions of Continuous Variables on Hertel Measurements
Variable Point Estimate SE P Valuea 95% CI
Brow fat (ROOF), mm3 25.5 16.1 .122 (–7.2, 58.1)
Galeal fat, mm3 35.6 35 .316 (–35.3, 106.4)
Total volume, mm3 98 38.6 .015 (19.9, 176)
Brow thickness, mm 0.201 0.086 .025 (0.027, 0.375)
CI, confidence interval; ROOF, retroorbicularis oculi fat.aThere was no statistically significant correlation of the amount of proptosis with the galeal or brow fat.
Papageorgiou et al 57
26. Darcy SJ, Miller TA, Goldberg RA, Villablanca JP, Demer JL, Rudkin GH. Magnetic resonance imaging character-ization of orbital changes with age and associated contri-butions to lower eyelid prominence. Plast Reconstr Surg 2008;122:921-929; discussion 930-931.
27. Sires BS, Lemke BN, Dortzbach RK, Gonnering RS. Char-acterization of human orbital fat and connective tissue. Ophthal Plast Reconstr Surg 1998;14:403-414.
28. Tchernof A, Poehlman ET, Despres JP. Body fat distribu-tion, the menopause transition and hormone replace-ment therapy. Diabetes Metab 2000;26:12-20.
29. Aloia JF, Vaswani A, Russo L, Sheehan M, Flaster A. The influence of menopause and hormonal replacement ther-apy on body cell mass and body fat mass. Am J Obstet Gynecol 1995;172:896-900.
30. Hall G, Phillips TJ. Estrogen and skin: the effects of estro-gen, menopause and hormone replacement therapy on the skin. J Am Acad Dermatol 2005;53:555-568.
31. Brincat MP, Muscat Baron Y, Galea R. Estrogens and skin. Climacteric 2005;8:110-123.
32. Le Louarn C, Buthiau D, Buis J. Structural aging: the facial recurve concept. Aesthetic Plast Surg 2007;31:213-218.
33. Pessa JE, Zadoo VP, Yuan C, et al. Concertina effect and facial aging: nonlinear aspects of youthfulness and skel-etal remodeling, and why, perhaps, infants have jowls. Plast Reconstr Surg 1999;103:635-644.
34. Matros E, Garcia JA, Yaremchuk MJ. Changes in eye-brow position and shape with aging. Plast Reconstr Surg 2009;124:1296-1301.
35. Lambros V. Observations on periorbital and midface aging. Plast Reconstr Surg 1996;97:1321-1333.
36. Lambros V. Discussion: changes in eyebrow position and shape with aging. Aesthetic Surg J 2009;29:174-179.
37. Sharabi SE, Hatef DA, Koshy JC, Hollier LH Jr, Yaremchuk MJ. Mechanotransduction: the missing link in the facial aging puzzle? Aesthetic Plast Surg 2010;34:603-611.
38. Fitzgerald R, Graivier MH, Kane M, et al. Update on facial aging. Aesthetic Surg J 2010;30(suppl):11S-24S.
Related Documents











