Review A systematic review of the impact of work environment on smoking cessation, relapse and amount smoked Karen Albertsen a, ⁎ , Vilhelm Borg a , Brian Oldenburg b a National Institute of Occupational Health, Denmark b School of Public Health, Queensland University of Technology, Australia Available online 19 June 2006 Abstract Background. Smoking is an important issue for the majority of the world's working population. It is important to explore in which ways the workplace might contribute to changes in smoking status and smoking behavior. The present article provides a systematic review and quality assessment of studies that have addressed the impact of factors in the work environment on smoking behavior. Methods. An evaluation of the methodological quality of 22 prospective studies was based on 14 explicit criteria, which included features of study design, statistical analysis, sampling issues and measurement. The level of scientific evidence was evaluated for each study. Results. There was strong evidence for an effect of the work environment on the amount smoked, but insufficient or mixed evidence regarding cessation and relapse. Summarizing the results, high job demands were associated with higher amount smoked and with increased likelihood of cessation. Resources at work and social support were positively associated with cessation and negatively associated with relapse and the amount smoked. Conclusions. The results supported the overall hypothesis that the work environment influences aspects of smoking behavior. Recommendations are made for more intervention studies where changes in work environment are carried out in combination with health promotion interventions. © 2006 Elsevier Inc. All rights reserved. Keywords: Work; Workload; Smoking; Smoking cessation; Tobacco use cessation; Lifestyle; Health behavior; Review; Systematic [publication type] Contents Introduction ................................................................ 292 Methods.................................................................. 292 Search methods ............................................................ 292 Methodological quality assessment .................................................. 292 Assessment of evidence........................................................ 292 Results .................................................................. 299 Methodological quality assessment .................................................. 299 The evidence of an association between work environment and changes in smoking ........................ 299 Predictors of cessation ...................................................... 299 Predictors of relapse from cessation ............................................... 299 Predictors of amount smoked ................................................... 300 Discussion ................................................................ 301 Main findings and implications .................................................... 301 Methodological considerations and recommendations for future research .............................. 303 Strength and limitations........................................................ 303 Preventive Medicine 43 (2006) 291 – 305 www.elsevier.com/locate/ypmed ⁎ Corresponding author. National Institute of Occupational Health, Lersø Parkallé 105, DK-2100 Copenhagen Ø, Denmark. Fax: +45 3916 5201. E-mail address: [email protected] (K. Albertsen). 0091-7435/$ - see front matter © 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.ypmed.2006.05.001

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Preventive Medicine 43 (2006) 291–305www.elsevier.com/locate/ypmed
Review
A systematic review of the impact of work environmenton smoking cessation, relapse and amount smoked
Karen Albertsen a,⁎, Vilhelm Borg a, Brian Oldenburg b
a National Institute of Occupational Health, Denmarkb School of Public Health, Queensland University of Technology, Australia
Available online 19 June 2006
Abstract
Background. Smoking is an important issue for the majority of the world's working population. It is important to explore in which ways theworkplace might contribute to changes in smoking status and smoking behavior. The present article provides a systematic review and qualityassessment of studies that have addressed the impact of factors in the work environment on smoking behavior.
Methods. An evaluation of the methodological quality of 22 prospective studies was based on 14 explicit criteria, which included features ofstudy design, statistical analysis, sampling issues and measurement. The level of scientific evidence was evaluated for each study.
Results. Therewas strong evidence for an effect of thework environment on the amount smoked, but insufficient ormixed evidence regarding cessationand relapse. Summarizing the results, high job demandswere associated with higher amount smoked andwith increased likelihood of cessation. Resourcesat work and social support were positively associated with cessation and negatively associated with relapse and the amount smoked.
Conclusions. The results supported the overall hypothesis that the work environment influences aspects of smoking behavior. Recommendationsare made for more intervention studies where changes in work environment are carried out in combination with health promotion interventions.© 2006 Elsevier Inc. All rights reserved.
Keywords: Work; Workload; Smoking; Smoking cessation; Tobacco use cessation; Lifestyle; Health behavior; Review; Systematic [publication type]
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292Methods. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292
Search methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292Methodological quality assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292Assessment of evidence. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Methodological quality assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299The evidence of an association between work environment and changes in smoking . . . . . . . . . . . . . . . . . . . . . . . . 299
Predictors of cessation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Predictors of relapse from cessation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Predictors of amount smoked . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301Main findings and implications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301Methodological considerations and recommendations for future research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303Strength and limitations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303
⁎ Corresponding author. National Institute of Occupational Health, Lersø Parkallé 105, DK-2100 Copenhagen Ø, Denmark. Fax: +45 3916 5201.E-mail address: [email protected] (K. Albertsen).
0091-7435/$ - see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.ypmed.2006.05.001

292 K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
Introduction
Work and smoking are interconnected in many differentways. It is well documented that smoking seriously damageshealth and predicts outcomes such as disability pension(Krokstad et al., 2002), early retirement (Lund et al., 2001)and sickness absence (Wooden and Bush, 1995). Many work-places in developed countries have now almost completely pro-hibited smoking in the workplace or, at least, introduced somesmoking policies, often in association with smoking cessationprograms. Smoking prevalence rates have been reducedsignificantly in many developed countries as a result of thesemeasures and a range of other community-wide initiatives (Osleret al., 2001). However, smoking is still an important issue for amajority of the world's working population. And therefore it isstill important to identify the ways in which the workplace, thework environment and the organization of work might con-tribute – positively or negatively – to changes in smoking statusand smoking behavior. The work environment might behypothesized to influence changes in smoking in the followingways: the work environment might influence (1) the probabilityof smoking cessation; (2) the probability of relapse followinginitial cessation; and (3) the amount of cigarettes smoked. Ofcourse, these three relationships might not necessarily operateindependently of one another, and furthermore, different mecha-nisms might contribute each. Firstly, stressors in the workenvironment might contribute to increased smoking or make itharder to quit (Cohen and Lichtenstein, 1990; Serxner et al.,1991; Steptoe et al., 1996, 1998; Westman et al., 1985). Second-ly, resources in the work environment, e.g. decision latitude orrewards, might strengthen the individual resources and make iteasier to reduce smoking, to quit or to avoid relapse (Pucci andHaglund, 1993). Thirdly, a discrepancy between demands anddecision latitude (job strain) can contribute to increased smo-king, difficulties with cessation and relapse (Cohen et al., 1991).Fourthly, social support can influence changes in smoking.Social support to quit can make cessation easier. Conversely, thepresence of smoking co-workers can contribute to increasedsmoking and counteract cessation (Westman et al., 1985).
Critical analyses of these possible associations and theunderpinning explanations are important for two reasons.Firstly, this might contribute to our understanding of socioeco-nomic health disparities as they are mediated through key healthbehaviors like smoking and, secondly, this might provide afirmer evidence base for integrated health promotion and workenvironment interventions at the worksite. The relationshipshave been investigated in a range of different studies, but so far,there has been no attempt to review and synthesize all therelevant findings.
The present article provides a systematic review and assess-ment of the quality of studies dealing with the impact of factorsin the work environment on the amount smoked, the likelihoodof quitting and the likelihood of relapsing after cessation.
Methods
Search methods
Articles from 1980 to 2004 written in English, German or Scandinavian lan-guages were searched in the bibliographic databases PubMed and PsycINFO. Thesearch terms included in the first screening were: work environment OR workplaceORoccupationOR jobANDsmokingOR tobacco.Abstracts from these articleswerereviewed, and all articles covering the following topics were included in a database:(1) smoking and work environment; (2) smoking and type of job; and (3) healthpromotion programs at the worksite including smoking (i.e. smoking cessationprograms, lifestyle interventions, smoking ban). This database was compiled usingthe Reference Manager software (ISI ResearchSoft, 2000). Articles fulfilling each ofthe following three criteria were selected for this review: prospective study design, atleast two assessments of smoking status and assessment of at least one workenvironment factor. Both interventions and observational studies were included.Studies that only included measures of intentions to quit smoking but not changes insmoking habits were excluded. As the questions being addressed are questions ofcausation, only prospective and longitudinal studies were included. Many cross-sectional studies exist in the field, but from these it is not possible to distinguishselection of smokers into specific work environments from the influence of workenvironment on changes in smoking behavior. Retrospective studies were alsoexcluded because of the difficulty in making causal inferences from such studies.Studies of the effect of smoking policy or smoking bans at the worksite, not includingspecific work environmental factors, were excluded because good reviews of thisissue already exist (Eriksen and Gottlieb, 1998; Heaney and Goetzel, 1997; Pelletier,1993). Individual factors such as self-efficacy and social factors in the family oroutside the workplace might also play a role for changes in smoking (Ockene et al.,2000); but studies of these associations were not included in this review unless thesevariables were examined in combination with work environment factors.
A literature search on the terms used generated 3265 references fromPubMed and700 references from PsycINFO. Abstracts of all articles were read on screen, and 293articles were identified as dealing with both the fields of smoking and the workenvironment. Of these 293 articles, twenty-two separate studies were identified from24 publications using the relevant selection criteria. Two of these studies werestratified by gender (Shields, 1999; Swan et al., 1988; Swan andDenk, 1987), and onepublication covered two different samples (Mermelstein et al., 1986), resulting inthree extra sub-studies (marked with “two samples” in Table 1 and the results with“s1” and “s2” respectively in Table 2). The quality assessment was based oninformation from all the publications.
Methodological quality assessment
In order to decide how much weight should be attributed to the results fromeach of the studies, an assessment of the quality of the studies was performed bytwo reviewers. The criteria used were derived from previous systematic reviews(Hoogendoorn et al., 2000) (see Fig. 1). The criteria differed slightly for studies ofdifferent design types. Each study was rated as positive, negative, unknown orirrelevant on each criterion. In order to keep the evaluation clear and specific, wedid not graduate the allocation of points (for instance from one to ten on each of thecriteria). The ratio of positive points out of possible was calculated. A study wasevaluated as of high quality, if the ratio was 60% or above, and of low quality if itwas below 60%. This limit is of course arbitrary, and therefore sensitivity analyseswere performed where a limit of 75% positive out of possible was imposed.
Any disagreements between the two reviewers were identified and discussed.With eleven to fourteen different criteria, the evaluation becomes rather robust andsingle shortcomings are not decisive for the result.
Assessment of evidence
The outcomes were divided into three broad groups: (1) cessation; (2) relapseafter cessation; and (3) smoking amount. The predictor variables were also
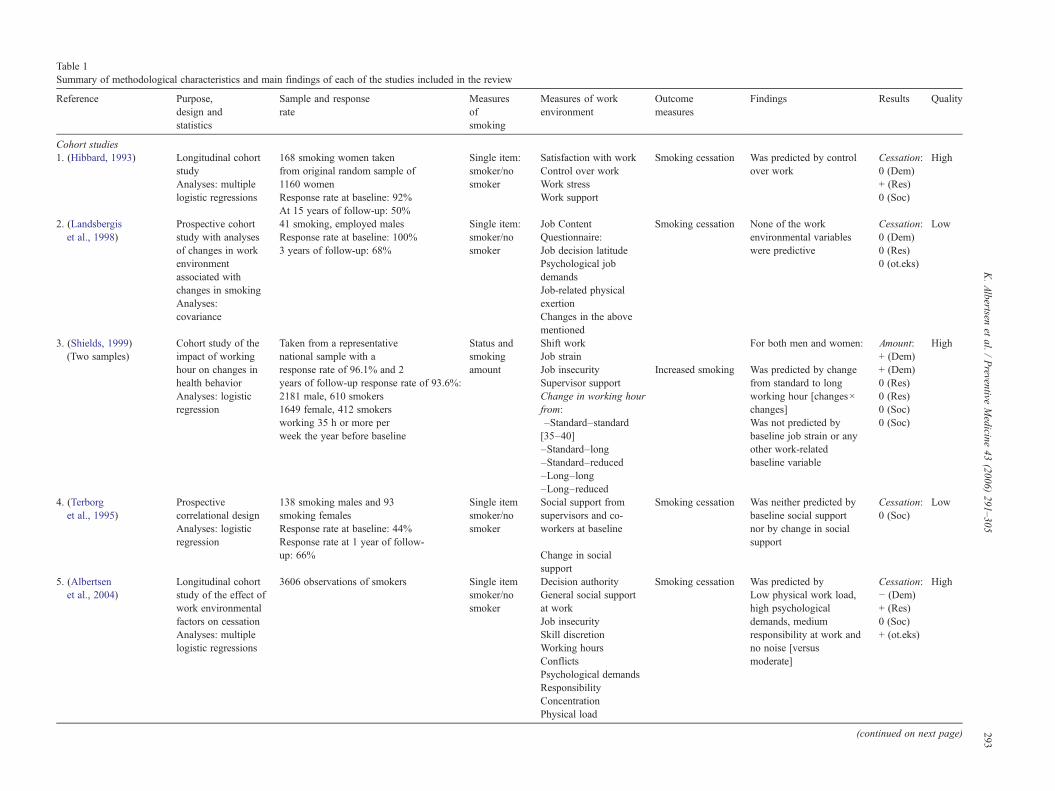
Table 1Summary of methodological characteristics and main findings of each of the studies included in the review
Reference Purpose,design andstatistics
Sample and responserate
Measuresofsmoking
Measures of workenvironment
Outcomemeasures
Findings Results Quality
Cohort studies1. (Hibbard, 1993) Longitudinal cohort
studyAnalyses: multiplelogistic regressions
168 smoking women takenfrom original random sample of1160 womenResponse rate at baseline: 92%At 15 years of follow-up: 50%
Single item:smoker/nosmoker
Satisfaction with workControl over workWork stressWork support
Smoking cessation Was predicted by controlover work
Cessation:0 (Dem)+ (Res)0 (Soc)
High
2. (Landsbergiset al., 1998)
Prospective cohortstudy with analysesof changes in workenvironmentassociated withchanges in smokingAnalyses:covariance
41 smoking, employed malesResponse rate at baseline: 100%3 years of follow-up: 68%
Single item:smoker/nosmoker
Job ContentQuestionnaire:Job decision latitudePsychological jobdemandsJob-related physicalexertionChanges in the abovementioned
Smoking cessation None of the workenvironmental variableswere predictive
Cessation:0 (Dem)0 (Res)0 (ot.eks)
Low
3. (Shields, 1999)(Two samples)
Cohort study of theimpact of workinghour on changes inhealth behaviorAnalyses: logisticregression
Taken from a representativenational sample with aresponse rate of 96.1% and 2years of follow-up response rate of 93.6%:2181 male, 610 smokers1649 female, 412 smokersworking 35 h or more perweek the year before baseline
Status andsmokingamount
Shift workJob strainJob insecuritySupervisor supportChange in working hourfrom:–Standard–standard[35–40]–Standard–long–Standard–reduced–Long–long–Long–reduced
Increased smoking
For both men and women:
Was predicted by changefrom standard to longworking hour [changes×changes]Was not predicted bybaseline job strain or anyother work-relatedbaseline variable
Amount:+ (Dem)+ (Dem)0 (Res)0 (Res)0 (Soc)0 (Soc)
High
4. (Terborget al., 1995)
Prospectivecorrelational designAnalyses: logisticregression
138 smoking males and 93smoking femalesResponse rate at baseline: 44%Response rate at 1 year of follow-up: 66%
Single itemsmoker/nosmoker
Social support fromsupervisors and co-workers at baseline
Change in socialsupport
Smoking cessation Was neither predicted bybaseline social supportnor by change in socialsupport
Cessation:0 (Soc)
Low
5. (Albertsenet al., 2004)
Longitudinal cohortstudy of the effect ofwork environmentalfactors on cessationAnalyses: multiplelogistic regressions
3606 observations of smokers Single itemsmoker/nosmoker
Decision authorityGeneral social supportat workJob insecuritySkill discretionWorking hoursConflictsPsychological demandsResponsibilityConcentrationPhysical load
Smoking cessation Was predicted byLow physical work load,high psychologicaldemands, mediumresponsibility at work andno noise [versusmoderate]
Cessation:− (Dem)+ (Res)0 (Soc)+ (ot.eks)
High
(continued on next page) 293K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305
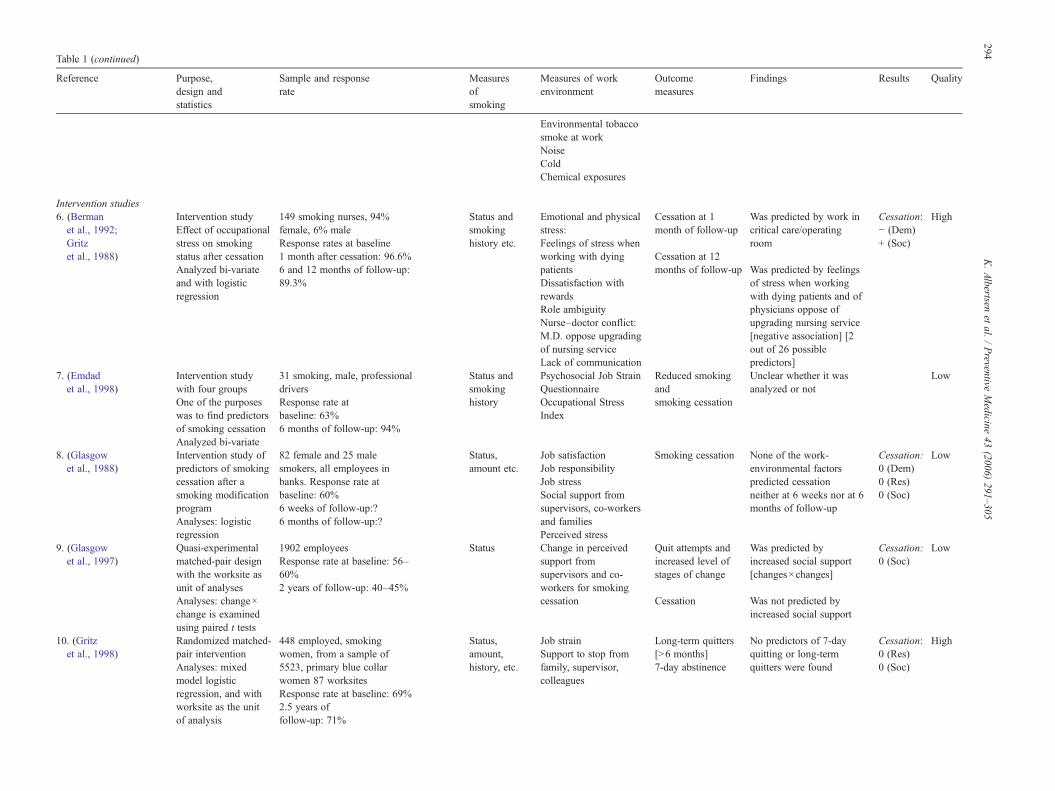
Table 1 (continued)
Reference Purpose,design andstatistics
Sample and responserate
Measuresofsmoking
Measures of workenvironment
Outcomemeasures
Findings Results Quality
Environmental tobaccosmoke at workNoiseColdChemical exposures
Intervention studies6. (Bermanet al., 1992;Gritzet al., 1988)
Intervention studyEffect of occupationalstress on smokingstatus after cessationAnalyzed bi-variateand with logisticregression
149 smoking nurses, 94%female, 6% maleResponse rates at baseline1 month after cessation: 96.6%6 and 12 months of follow-up:89.3%
Status andsmokinghistory etc.
Emotional and physicalstress:Feelings of stress whenworking with dyingpatientsDissatisfaction withrewardsRole ambiguityNurse–doctor conflict:M.D. oppose upgradingof nursing serviceLack of communication
Cessation at 1month of follow-up
Cessation at 12months of follow-up
Was predicted by work incritical care/operatingroom
Was predicted by feelingsof stress when workingwith dying patients and ofphysicians oppose ofupgrading nursing service[negative association] [2out of 26 possiblepredictors]
Cessation:− (Dem)+ (Soc)
High
7. (Emdadet al., 1998)
Intervention studywith four groupsOne of the purposeswas to find predictorsof smoking cessationAnalyzed bi-variate
31 smoking, male, professionaldriversResponse rate atbaseline: 63%6 months of follow-up: 94%
Status andsmokinghistory
Psychosocial Job StrainQuestionnaireOccupational StressIndex
Reduced smokingandsmoking cessation
Unclear whether it wasanalyzed or not
Low
8. (Glasgowet al., 1988)
Intervention study ofpredictors of smokingcessation after asmoking modificationprogramAnalyses: logisticregression
82 female and 25 malesmokers, all employees inbanks. Response rate atbaseline: 60%6 weeks of follow-up:?6 months of follow-up:?
Status,amount etc.
Job satisfactionJob responsibilityJob stressSocial support fromsupervisors, co-workersand familiesPerceived stress
Smoking cessation None of the work-environmental factorspredicted cessationneither at 6 weeks nor at 6months of follow-up
Cessation:0 (Dem)0 (Res)0 (Soc)
Low
9. (Glasgowet al., 1997)
Quasi-experimentalmatched-pair designwith the worksite asunit of analysesAnalyses: change×change is examinedusing paired t tests
1902 employeesResponse rate at baseline: 56–60%2 years of follow-up: 40–45%
Status Change in perceivedsupport fromsupervisors and co-workers for smokingcessation
Quit attempts andincreased level ofstages of change
Cessation
Was predicted byincreased social support[changes×changes]
Was not predicted byincreased social support
Cessation:0 (Soc)
Low
10. (Gritzet al., 1998)
Randomized matched-pair interventionAnalyses: mixedmodel logisticregression, and withworksite as the unitof analysis
448 employed, smokingwomen, from a sample of5523, primary blue collarwomen 87 worksitesResponse rate at baseline: 69%2.5 years offollow-up: 71%
Status,amount,history, etc.
Job strainSupport to stop fromfamily, supervisor,colleagues
Long-term quitters[N6 months]7-day abstinence
No predictors of 7-dayquitting or long-termquitters were found
Cessation:0 (Res)0 (Soc)
High
294K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305
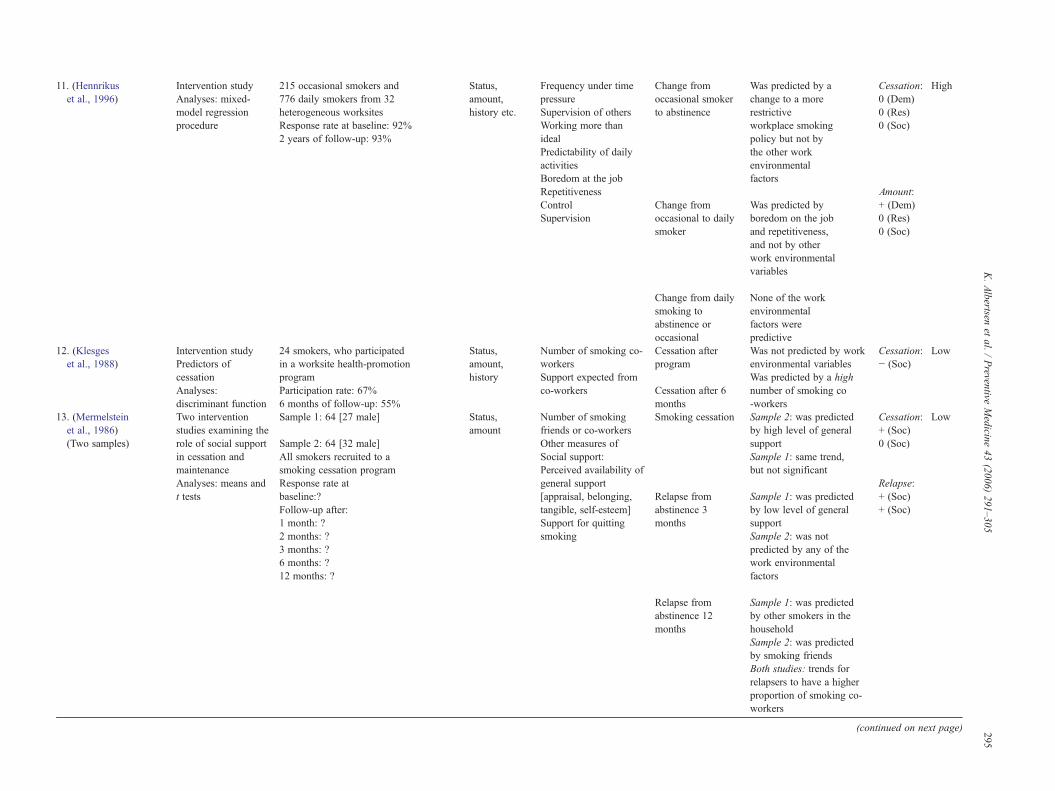
11. (Hennrikuset al., 1996)
Intervention studyAnalyses: mixed-model regressionprocedure
215 occasional smokers and776 daily smokers from 32heterogeneous worksitesResponse rate at baseline: 92%2 years of follow-up: 93%
Status,amount,history etc.
Frequency under timepressureSupervision of othersWorking more thanidealPredictability of dailyactivitiesBoredom at the jobRepetitivenessControlSupervision
Change fromoccasional smokerto abstinence
Change fromoccasional to dailysmoker
Was predicted by achange to a morerestrictiveworkplace smokingpolicy but not bythe other workenvironmentalfactors
Was predicted byboredom on the joband repetitiveness,and not by otherwork environmentalvariables
Cessation:0 (Dem)0 (Res)0 (Soc)
Amount:+ (Dem)0 (Res)0 (Soc)
High
Change from dailysmoking toabstinence oroccasional
None of the workenvironmentalfactors werepredictive
. (Klesgeset al., 1988)
Intervention studyPredictors ofcessationAnalyses:discriminant function
24 smokers, who participatedin a worksite health-promotionprogramParticipation rate: 67%6 months of follow-up: 55%
Status,amount,history
Number of smoking co-workersSupport expected fromco-workers
Cessation afterprogram
Cessation after 6months
Was not predicted by workenvironmental variablesWas predicted by a highnumber of smoking co-workers
Cessation:− (Soc)
Low
. (Mermelsteinet al., 1986)(Two samples)
Two interventionstudies examining therole of social supportin cessation andmaintenanceAnalyses: means andt tests
Sample 1: 64 [27 male]
Sample 2: 64 [32 male]All smokers recruited to asmoking cessation programResponse rate atbaseline:?Follow-up after:1 month: ?2 months: ?3 months: ?6 months: ?12 months: ?
Status,amount
Number of smokingfriends or co-workersOther measures ofSocial support:Perceived availability ofgeneral support[appraisal, belonging,tangible, self-esteem]Support for quittingsmoking
Smoking cessation
Relapse fromabstinence 3months
Sample 2: was predictedby high level of generalsupportSample 1: same trend,but not significant
Sample 1: was predictedby low level of generalsupportSample 2: was notpredicted by any of thework environmentalfactors
Cessation:+ (Soc)0 (Soc)
Relapse:+ (Soc)+ (Soc)
Low
Relapse fromabstinence 12months
Sample 1: was predictedby other smokers in thehouseholdSample 2: was predictedby smoking friendsBoth studies: trends forrelapsers to have a higherproportion of smoking co-workers
(continued on next page) 295K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305
12
13
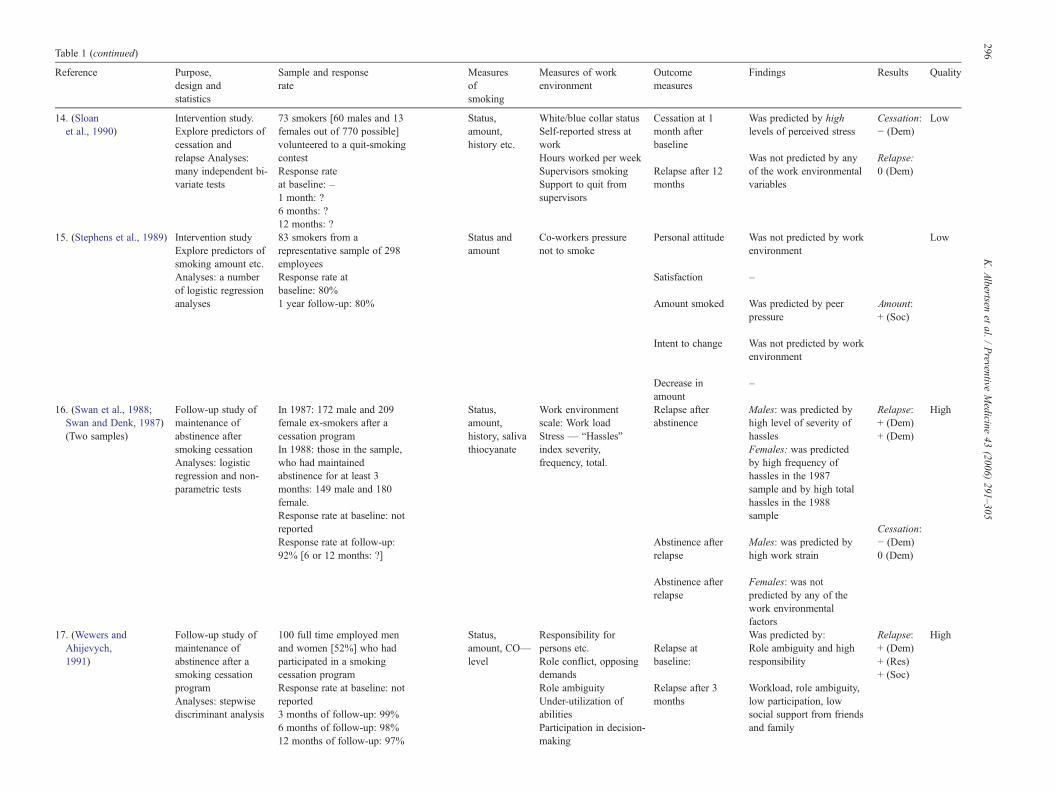
Table 1 (continued)
Reference Purpose,design andstatistics
Sample and responserate
Measuresofsmoking
Measures of workenvironment
Outcomemeasures
Findings Results Quality
14. (Sloanet al., 1990)
Intervention study.Explore predictors ofcessation andrelapse Analyses:many independent bi-variate tests
73 smokers [60 males and 13females out of 770 possible]volunteered to a quit-smokingcontestResponse rateat baseline: –1 month: ?6 months: ?12 months: ?
Status,amount,history etc.
White/blue collar statusSelf-reported stress atworkHours worked per weekSupervisors smokingSupport to quit fromsupervisors
Cessation at 1month afterbaseline
Relapse after 12months
Was predicted by highlevels of perceived stress
Was not predicted by anyof the work environmentalvariables
Cessation:− (Dem)
Relapse:0 (Dem)
Low
15. (Stephens et al., 1989) Intervention studyExplore predictors ofsmoking amount etc.Analyses: a numberof logistic regressionanalyses
83 smokers from arepresentative sample of 298employeesResponse rate atbaseline: 80%1 year follow-up: 80%
Status andamount
Co-workers pressurenot to smoke
Personal attitude
Satisfaction
Amount smoked
Was not predicted by workenvironment
–
Was predicted by peerpressure
Amount:+ (Soc)
Low
Intent to change Was not predicted by workenvironment
Decrease inamount
–
16. (Swan et al., 1988;Swan and Denk, 1987)(Two samples)
Follow-up study ofmaintenance ofabstinence aftersmoking cessationAnalyses: logisticregression and non-parametric tests
In 1987: 172 male and 209female ex-smokers after acessation programIn 1988: those in the sample,who had maintainedabstinence for at least 3months: 149 male and 180female.Response rate at baseline: notreportedResponse rate at follow-up:92% [6 or 12 months: ?]
Status,amount,history, salivathiocyanate
Work environmentscale: Work loadStress — “Hassles”index severity,frequency, total.
Relapse afterabstinence
Abstinence afterrelapse
Males: was predicted byhigh level of severity ofhasslesFemales: was predictedby high frequency ofhassles in the 1987sample and by high totalhassles in the 1988sample
Males: was predicted byhigh work strain
Relapse:+ (Dem)+ (Dem)
Cessation:− (Dem)0 (Dem)
High
Abstinence afterrelapse
Females: was notpredicted by any of thework environmentalfactors
17. (Wewers andAhijevych,1991)
Follow-up study ofmaintenance ofabstinence after asmoking cessationprogramAnalyses: stepwisediscriminant analysis
100 full time employed menand women [52%] who hadparticipated in a smokingcessation programResponse rate at baseline: notreported3 months of follow-up: 99%6 months of follow-up: 98%12 months of follow-up: 97%
Status,amount, CO—level
Responsibility forpersons etc.Role conflict, opposingdemandsRole ambiguityUnder-utilization ofabilitiesParticipation in decision-making
Relapse atbaseline:
Relapse after 3months
Was predicted by:Role ambiguity and highresponsibility
Workload, role ambiguity,low participation, lowsocial support from friendsand family
Relapse:+ (Dem)+ (Res)+ (Soc)
High
296K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305
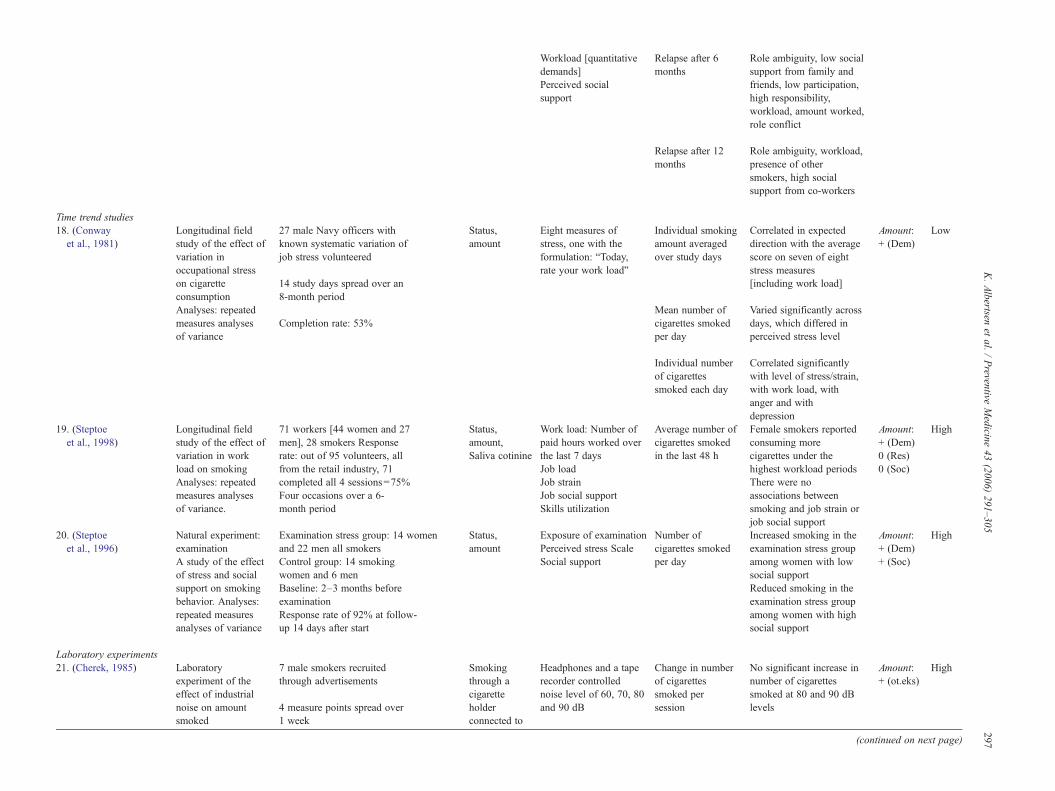
Workload [quantitativedemands]Perceived socialsupport
Relapse after 6months
Role ambiguity, low socialsupport from family andfriends, low participation,high responsibility,workload, amount worked,role conflict
Relapse after 12months
Role ambiguity, workload,presence of othersmokers, high socialsupport from co-workers
Time trend studies18. (Conwayet al., 1981)
Longitudinal fieldstudy of the effect ofvariation inoccupational stresson cigaretteconsumptionAnalyses: repeatedmeasures analysesof variance
27 male Navy officers withknown systematic variation ofjob stress volunteered
14 study days spread over an8-month period
Completion rate: 53%
Status,amount
Eight measures ofstress, one with theformulation: “Today,rate your work load”
Individual smokingamount averagedover study days
Mean number ofcigarettes smokedper day
Correlated in expecteddirection with the averagescore on seven of eightstress measures[including work load]
Varied significantly acrossdays, which differed inperceived stress level
Amount:+ (Dem)
Low
Individual numberof cigarettessmoked each day
Correlated significantlywith level of stress/strain,with work load, withanger and withdepression
19. (Steptoeet al., 1998)
Longitudinal fieldstudy of the effect ofvariation in workload on smokingAnalyses: repeatedmeasures analysesof variance.
71 workers [44 women and 27men], 28 smokers Responserate: out of 95 volunteers, allfrom the retail industry, 71completed all 4 sessions=75%Four occasions over a 6-month period
Status,amount,Saliva cotinine
Work load: Number ofpaid hours worked overthe last 7 daysJob loadJob strainJob social supportSkills utilization
Average number ofcigarettes smokedin the last 48 h
Female smokers reportedconsuming morecigarettes under thehighest workload periodsThere were noassociations betweensmoking and job strain orjob social support
Amount:+ (Dem)0 (Res)0 (Soc)
High
20. (Steptoeet al., 1996)
Natural experiment:examinationA study of the effectof stress and socialsupport on smokingbehavior. Analyses:repeated measuresanalyses of variance
Examination stress group: 14 womenand 22 men all smokersControl group: 14 smokingwomen and 6 menBaseline: 2–3 months beforeexaminationResponse rate of 92% at follow-up 14 days after start
Status,amount
Exposure of examinationPerceived stress ScaleSocial support
Number ofcigarettes smokedper day
Increased smoking in theexamination stress groupamong women with lowsocial supportReduced smoking in theexamination stress groupamong women with highsocial support
Amount:+ (Dem)+ (Soc)
High
Laboratory experiments21. (Cherek, 1985) Laboratory
experiment of theeffect of industrialnoise on amountsmoked
7 male smokers recruitedthrough advertisements
4 measure points spread over1 week
Smokingthrough acigaretteholderconnected to
Headphones and a taperecorder controllednoise level of 60, 70, 80and 90 dB
Change in numberof cigarettessmoked persession
No significant increase innumber of cigarettessmoked at 80 and 90 dBlevels
Amount:+ (ot.eks)
High
(continued on next page)
297K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305
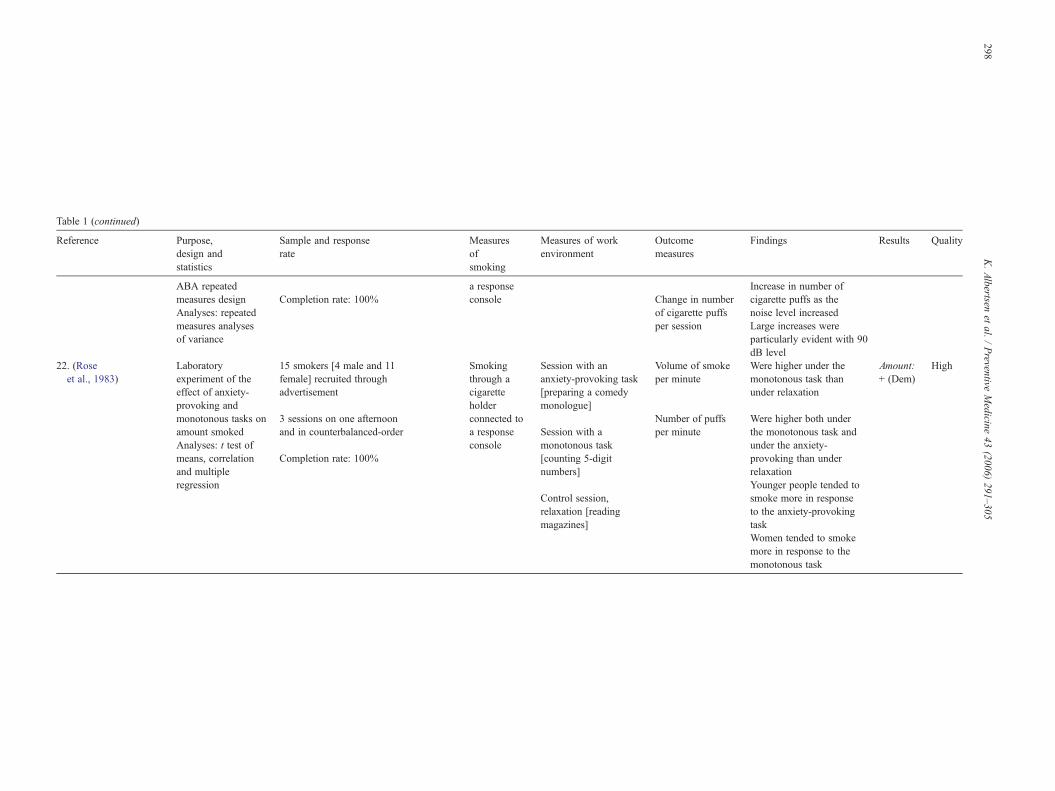
Table 1 (continued)
Reference Purpose,design andstatistics
Sample and responserate
Measuresofsmoking
Measures of workenvironment
Outcomemeasures
Findings Results Quality
ABA repeatedmeasures designAnalyses: repeatedmeasures analysesof variance
Completion rate: 100%a responseconsole Change in number
of cigarette puffsper session
Increase in number ofcigarette puffs as thenoise level increasedLarge increases wereparticularly evident with 90dB level
22. (Roseet al., 1983)
Laboratoryexperiment of theeffect of anxiety-provoking andmonotonous tasks onamount smokedAnalyses: t test ofmeans, correlationand multipleregression
15 smokers [4 male and 11female] recruited throughadvertisement
3 sessions on one afternoonand in counterbalanced-order
Completion rate: 100%
Smokingthrough acigaretteholderconnected toa responseconsole
Session with ananxiety-provoking task[preparing a comedymonologue]
Session with amonotonous task[counting 5-digitnumbers]
Control session,relaxation [readingmagazines]
Volume of smokeper minute
Number of puffsper minute
Were higher under themonotonous task thanunder relaxation
Were higher both underthe monotonous task andunder the anxiety-provoking than underrelaxationYounger people tended tosmoke more in responseto the anxiety-provokingtaskWomen tended to smokemore in response to themonotonous task
Amount:+ (Dem)
High
298K.Albertsen
etal.
/Preventive
Medicine
43(2006)
291–305

299K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
categorized into three broad groups: (1) different kind of demands at work; (2)different kinds of resources at work; and (3) social support. These three groups arebased on the basic dimensions of the Karasek–Theorell Model (Karasek andTheorell, 1990) supplemented by Johnson's measures of social support (Johnson etal., 1989). A list of measures included in each of the groups is presented in Fig. 2.
For each outcome category and each group of predictor variables, the resultswere synthesized according to three levels of scientific evidence, developed byHoogendoorn et al. (2000):
– Strong evidence: provided by generally consistent findings, supporting thehypotheses, in multiple high-quality studies.
– Moderate evidence: provided by generally consistent findings, supportingthe hypotheses, in one high-quality study and one or more low-qualitystudies or in multiple low-quality studies.
– Insufficient evidence: only one study available or inconsistent findings inmultiple studies.
The findings were considered to be insufficient if less than 75% of thestudies in the category supported the hypothesis. In the case of multiple high-quality studies, the low-quality studies were disregarded in the assessment of thelevel of evidence. If different results were reported for different points in time,then an effect was registered if it was present on at least one point. If a studyapplied different measures of work environment within the same main categoryof predictor variables, an effect was registered if it was present for at least one ofthe measures.
Results
Table 1 provides a summary of the methodological charac-teristics and main findings of each of the studies included in thereview.
Methodological quality assessment
With reference to the criteria summarized in Fig. 1, twelve ofthe studies had a positive score for more than 60% of the criteria.
The main methodological problems included:
– Small sample size—six studies had a sample size of less than100.
– Low response rates—five studies reported response ratesunder the limits set.
– Limited measurements of the work environment were foundin six studies.
– Lack of validity analyses or references was found in sixstudies.
The evidence of an association between work environment andchanges in smoking
Predictors of cessation
Demands. Seven studies of high and two of low qualityhave examined different measures of demands as predictorsof smoking cessation. Results from three high quality andone low quality study differed from the null hypothesis. Allfound that high levels of demands were predictive ofcessation. Cessation was predicted by high workload amongmen (Swan and Denk, 1987), by high levels of perceivedstress (Sloan et al., 1990), by high demands to concentration
(Albertsen et al., 2004) and, in a study among nurses, bywork in critical care and feelings of stress when workingwith dying patients (Gritz et al., 1988). In summary, therewas strong support that high demands increase theprobability of cessation.
Resources. Three studies of high quality and two of low exa-mined the effect of resources at work on cessation. Two of thehigh-quality studies showed positive associations. In a studywith a 15-year follow-up period, smoking cessation was pre-dicted by control over work (Hibbard, 1993), and, in a studywith a 5-year follow-up period, cessation was predicted by me-dium level of responsibility (Albertsen et al., 2004). Few studiesexplored this problem; two studies of high quality did howeversupport the hypothesis of an effect of resources at work oncessation.
Social support. Five high-quality and six low-quality studiesexamined social support as predictor of cessation. One high andone low quality study reported results supporting a predictivevalue of social support. The high-quality study found thatphysicians' opposing of nurses education decreased theprobability of cessation among the nurses (Gritz et al., 1988).In one out of two samples in a low-quality study, a high level ofgeneral social support was found predictive of cessation(Mermelstein et al., 1986). In one study (Klesges et al.,1988), a high number of smoking co-workers were contrary tothe hypothesis predictive of abstinence after 6 months. Manystudies have analyzed this problem, but most could not rejectthe null hypothesis. Therefore, there is currently insufficientevidence of an effect of social support on smoking cessation inthe workplace.
Other exposures. One study of high quality and one of lowhave examined the effect of other work environmentalexposures on cessation. The study of high quality found thatthe likelihood of cessation was lower when exposed tomoderate levels of noise and to high physical demands(Albertsen et al., 2004). The study of low quality did not findsupport for the hypothesis that physical exertion influencecessation (Landsbergis et al., 1998).
Predictors of relapse from cessation
Demands. Three studies of high quality and one of lowexamined the hypothesis that high demands increase the prob-ability of relapse. All of the high-quality studies supported thehypothesis, while the study of low quality did not. Relapse fromcessation was predicted by workload, role ambiguity, high re-sponsibility for the work of others, long working hours and roleconflict (Wewers and Ahijevych, 1991), by high severity ofhassles among men (Swan et al., 1988; Swan and Denk, 1987),by high frequency of hassles (Swan and Denk, 1987) and byhigh total amount of hassles (Swan et al., 1988) among women.Thus, results from three high-quality studies supply strong evi-dence for the hypothesis that high demands increase the proba-bility of relapse.

300 K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
Resources. One high-quality study examined the effect ofdecision latitude on relapse from cessation. Relapse from ces-sation was, in that study, predicted by low participation indecision-making but not by low skill utilization (Wewers andAhijevych, 1991). This leaves insufficient evidence for an effectof resources on relapse.
Social support. Different measures of lack of social supportwere examined as predictors of relapse after cessation in onehigh-quality and three low-quality studies. Predictive measureswere found in the high-quality study and in two of the low-quality studies, resulting in moderate evidence for an effect.Relapse after 12 months was predicted by the presence ofsmoking co-workers, of high social support from co-workers(Wewers and Ahijevych, 1991) and by the presence of othersmokers in two different samples (Mermelstein et al., 1986).Relapse after 3 and 6 months was predicted by low generalsocial support at work in one of two samples (Mermelstein et
Fig. 1. Criteria list for assessment of the m
al., 1986) and by lack of social support to maintenance fromfriends and family (Wewers and Ahijevych, 1991). Thepresence of other smokers was not predictive of relapse after3 or 6 months Mermelstein et al., 1986).
Predictors of amount smoked
Demands. Six high- and one low-quality study examined thehyothesis that high demands are associated with increasedsmoking among smokers. All high-quality studies supported thehypothesis. Increased smoking was associated with periods withlong working hours and increases in working hours amongwomen (Steptoe et al., 1998), change from standard to longworking hours among both men and women (Shields, 1999),stress level (Conway et al., 1981), boredom and repetitiveness(Hennrikus et al., 1996) and monotonous or anxiety-provokingtasks (Rose et al., 1983). In addition, high stress was associatedwith increased smoking among women with low social support
ethodological quality of the studies.

Fig. 1 (continued ).
301K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
and with reduced smoking among women with high socialsupport (Steptoe et al., 1996). Frequently working under timepressure and working more than ideal failed to predict changesfrom occasional to daily smoker or change from daily to occa-sional smoker over a period of 2 years (Hennrikus et al., 1996).Job–home interference failed to predict variations in smokingamount (Steptoe et al., 1998).
Resources. Three high-quality studies examined the variationin decision latitude on the amount smoked. None of them foundpositive results. One study examined job insecurity and job strain(demands×decision latitude) as predictors of increased smokingin men and women and did not find any effect (Shields, 1999),another study examined skills utilization but failed to predictsmoking amount (Steptoe et al., 1998). In one study, control overwork failed to predict changes from occasional smoker to absti-nence or fromoccasional to daily smoker (Hennrikus et al., 1996).Two studies examined job strain as predictor of increased smo-king in men and women and did not find any effect (Shields,1999).
Thus, insufficient evidence is attained for an effect of deci-sion latitude on amount smoked.
Social support. Five studies of high and one of low qualityexamined different measures of social support as predictors ofamount smoked. Only one study found an effect, and here socialsupport was only predictive in interaction with stress (Steptoe et
al., 1996). Thus, there is insufficient support for an effect of socialsupport on amount smoked.
Other exposures. One experimental study of high qualityexamined the effect of industrial noise (Cherek, 1985) and founda positive association between industrial noise and amountsmoked.
Discussion
Main findings and implications
Taken together, the results support the overall hypothesis thatthe work environment influences smoking. There was strongevidence that high demands increased the amount smoked amongsmokers, that high resources and high demands increased theprobability of cessation and that high demands increased theprobability of relapse. The evidence regarding other associationswas either insufficient or mixed. This pattern of results leads to acouple of discussion points.
How can high demands on the one hand increase the amountsmoked among smokers, and increase the probability of relapse,and on the other hand increase the probability of cessation? A U-shaped relationship between demands and stress has been pro-posed (Warr, 1987). It might be that moderate demands in factare most supportive regarding cessation and that higher demandscause relapse. To have something to be engaged in when trying
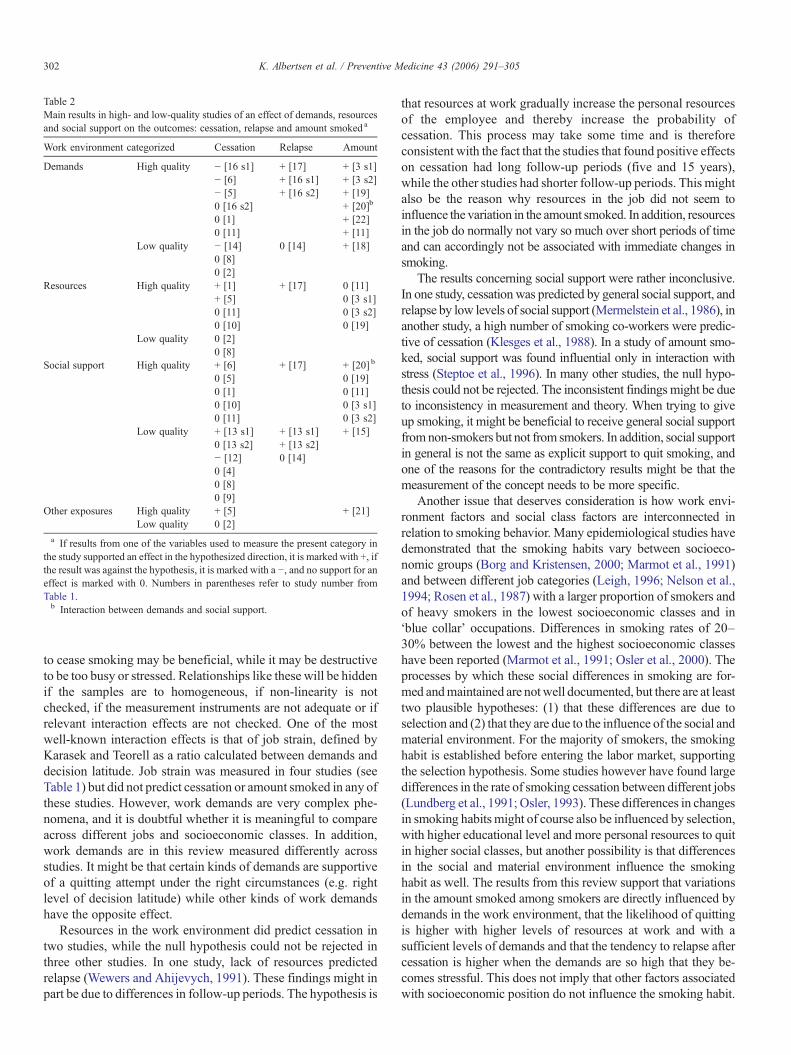
Table 2Main results in high- and low-quality studies of an effect of demands, resourcesand social support on the outcomes: cessation, relapse and amount smoked a
Work environment categorized Cessation Relapse Amount
Demands High quality − [16 s1] + [17] + [3 s1]− [6] + [16 s1] + [3 s2]− [5] + [16 s2] + [19]0 [16 s2] + [20]b
0 [1] + [22]0 [11] + [11]
Low quality − [14] 0 [14] + [18]0 [8]0 [2]
Resources High quality + [1] + [17] 0 [11]+ [5] 0 [3 s1]0 [11] 0 [3 s2]0 [10] 0 [19]
Low quality 0 [2]0 [8]
Social support High quality + [6] + [17] + [20] b
0 [5] 0 [19]0 [1] 0 [11]0 [10] 0 [3 s1]0 [11] 0 [3 s2]
Low quality + [13 s1] + [13 s1] + [15]0 [13 s2] + [13 s2]− [12] 0 [14]0 [4]0 [8]0 [9]
Other exposures High quality + [5] + [21]Low quality 0 [2]
a If results from one of the variables used to measure the present category inthe study supported an effect in the hypothesized direction, it is marked with +, ifthe result was against the hypothesis, it is marked with a −, and no support for aneffect is marked with 0. Numbers in parentheses refer to study number fromTable 1.b Interaction between demands and social support.
302 K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
to cease smoking may be beneficial, while it may be destructiveto be too busy or stressed. Relationships like these will be hiddenif the samples are to homogeneous, if non-linearity is notchecked, if the measurement instruments are not adequate or ifrelevant interaction effects are not checked. One of the mostwell-known interaction effects is that of job strain, defined byKarasek and Teorell as a ratio calculated between demands anddecision latitude. Job strain was measured in four studies (seeTable 1) but did not predict cessation or amount smoked in any ofthese studies. However, work demands are very complex phe-nomena, and it is doubtful whether it is meaningful to compareacross different jobs and socioeconomic classes. In addition,work demands are in this review measured differently acrossstudies. It might be that certain kinds of demands are supportiveof a quitting attempt under the right circumstances (e.g. rightlevel of decision latitude) while other kinds of work demandshave the opposite effect.
Resources in the work environment did predict cessation intwo studies, while the null hypothesis could not be rejected inthree other studies. In one study, lack of resources predictedrelapse (Wewers and Ahijevych, 1991). These findings might inpart be due to differences in follow-up periods. The hypothesis is
that resources at work gradually increase the personal resourcesof the employee and thereby increase the probability ofcessation. This process may take some time and is thereforeconsistent with the fact that the studies that found positive effectson cessation had long follow-up periods (five and 15 years),while the other studies had shorter follow-up periods. This mightalso be the reason why resources in the job did not seem toinfluence the variation in the amount smoked. In addition, resourcesin the job do normally not vary so much over short periods of timeand can accordingly not be associated with immediate changes insmoking.
The results concerning social support were rather inconclusive.In one study, cessation was predicted by general social support, andrelapse by low levels of social support (Mermelstein et al., 1986), inanother study, a high number of smoking co-workers were predic-tive of cessation (Klesges et al., 1988). In a study of amount smo-ked, social support was found influential only in interaction withstress (Steptoe et al., 1996). In many other studies, the null hypo-thesis could not be rejected. The inconsistent findings might be dueto inconsistency in measurement and theory. When trying to giveup smoking, it might be beneficial to receive general social supportfromnon-smokers but not from smokers. In addition, social supportin general is not the same as explicit support to quit smoking, andone of the reasons for the contradictory results might be that themeasurement of the concept needs to be more specific.
Another issue that deserves consideration is how work envi-ronment factors and social class factors are interconnected inrelation to smoking behavior. Many epidemiological studies havedemonstrated that the smoking habits vary between socioeco-nomic groups (Borg and Kristensen, 2000; Marmot et al., 1991)and between different job categories (Leigh, 1996; Nelson et al.,1994; Rosen et al., 1987) with a larger proportion of smokers andof heavy smokers in the lowest socioeconomic classes and in‘blue collar’ occupations. Differences in smoking rates of 20–30% between the lowest and the highest socioeconomic classeshave been reported (Marmot et al., 1991; Osler et al., 2000). Theprocesses by which these social differences in smoking are for-med andmaintained are notwell documented, but there are at leasttwo plausible hypotheses: (1) that these differences are due toselection and (2) that they are due to the influence of the social andmaterial environment. For the majority of smokers, the smokinghabit is established before entering the labor market, supportingthe selection hypothesis. Some studies however have found largedifferences in the rate of smoking cessation between different jobs(Lundberg et al., 1991; Osler, 1993). These differences in changesin smoking habits might of course also be influenced by selection,with higher educational level and more personal resources to quitin higher social classes, but another possibility is that differencesin the social and material environment influence the smokinghabit as well. The results from this review support that variationsin the amount smoked among smokers are directly influenced bydemands in the work environment, that the likelihood of quittingis higher with higher levels of resources at work and with asufficient levels of demands and that the tendency to relapse aftercessation is higher when the demands are so high that they be-comes stressful. This does not imply that other factors associatedwith socioeconomic position do not influence the smoking habit.

Fig. 2. Measures of work environment used in the studies.
303K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
For example, interactions might exist between personal factorsand the resources available in the job.
Methodological considerations and recommendations forfuture research
Although there are few prospective studies available in thisfield, a relatively high percentage of these are of high quality. Inmost of the high-quality studies, many predictors are studied andin some of themmore than one outcome or more than one sampleare investigated. The results from the high-quality studies shouldbe given more weight for at least two reasons: firstly, there aregenerally more results from these studies and, secondly, they aremethodologically much stronger than other studies. There aremore studies of low quality in the field of social support aspredictor of cessation and relapse.
With regard to design and statistics, the studies were generallyrated positively. There are, however, room for improvement indirection of larger, more heterogeneously composed samples andbetter response rates. Measurement instruments may further beimproved and better validated, and variables covering, for exam-ple, individual attitudes toward smoking and self-efficacy may bebeneficial to include in future studies.
There is a need for intervention studies where changes in thework environment are carried out alone or in combination withhealth promotion interventions. This kind of studies would beimportant for testing the causal relations between work environ-ment and changes in smoking. In order to test whether the effectof health promotion interventions masks the effect of work
environment on smoking, comparisons should be made of theeffect of work environmental factors in intervention groups andin control groups respectively. Furthermore, the field couldbenefit from coordinated use of well-validated, uni-dimensionalinstruments, with more sub-dimensions, especially of demandsand social support, and with scales covering the whole spectrumfrom low to high levels.
Strength and limitations
Only studies conducted with the workplace as setting wereincluded in this review. Studies of smoking in relation to stress,social support, etc. conducted in other settings may also be relevantfor the understanding of the mechanisms behind smoking andwork environment, but the implications would have been moredifficult to interpret.
The decision about evidence level was based on the pro-portion of studies, which were categorized as high-quality stu-dies. A criterion of 60% was chosen, however, if it had been setat 75%, it would only have changed the status of two of thestudies from high to low quality, and this would not haveinfluenced the levels of evidence.
Due to the large amount of different measures of the workenvironment included in the studies, the results have been reportedclustered in some rather heterogeneous groups. It has not beenpossible to disentangle the relationships and interconnections bet-ween each of the work environmental factors in relation to smo-king, but it is very likely that the effects of the different factors are infact interrelated.

304 K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
Acknowledgments
This research was supported by a grant from The ServiceCentre of the Danish Working Environment Council, grant no.2000-08. The research was initiated by and analyses made bythe investigators. Professor Tage Søndergaard Kristensen andsenior researcher Harald Hannerz, The National Institute ofOccupational Health, Denmark, provided insightful commentson the manuscript.
References
Albertsen, K., Hannerz, H., Borg, V., Burr, H., 2004. Work environment andsmoking cessation over a five-year period. Scand J. Public Health 32,164–171.
Berman, B.A., Read, L.L., Marcus, A.C., Gritz, E.R., 1992. Nurses enrolled in a stopsmoking program: the role of occupational stress. J. Women's Health 1 (1),41–46.
Borg, V., Kristensen, T.S., 2000. Social class and self-rated health: can thegradient be explained by differences in life style or work environment? Soc.Sci. Med. 51 (7), 1019–1030.
Cherek, D.R., 1985. Effects of acute exposure to increased levels of backgroundindustrial noise on cigarette smoking behavior. Int. Arch. Occup. Environ.Health 56 (1), 23–30.
Cohen, S., Lichtenstein, E., 1990. Perceived stress, quitting smoking, and smokingrelapse. Health Psychol. 9 (4), 466–478.
Cohen, S., Schwartz, J.E., Bromet, E.J., Parkinson, D.K., 1991. Mental health, stress,and poor health behaviors in two community samples. Prev. Med. 20 (2),306–315.
Conway, T.L., Vickers, R.R.J., Ward, H.W., Rahe, R.H., 1981. Occupationalstress and variation in cigarette, coffee, and alcohol consumption. J. HealthSoc. Behav. 22 (2), 155–165.
Emdad, R., Belkic, K., Theorell, T., Cizinsky, S., 1998. What prevents professionaldrivers from following physicians' cardiologic advice. Psychother. Psychosom.67 (4–5), 226–240.
Eriksen, M.P., Gottlieb, N.H., 1998. A review of the health impact of smokingcontrol at the workplace. Am. J. Health Promot. 13 (2), 83–104.
Glasgow, R.E., Klesges, R.C., Klesges, L.M., Somes, G.R., 1988. Variablesassociated with participation and outcome in a worksite smoking control pro-gram. J. Consult. Clin. Psychol. 56 (4), 617–620.
Glasgow, R.E., Cummings, K.M., Hyland, A., 1997. Relationship of worksitesmoking policy to changes in employee tobacco use: findings fromCOMMIT. Community Intervention Trial for Smoking Cessation. Tob.Control 6 (Suppl 2), S44–S48.
Gritz, E.R., Marcus, A.C., Berman, B.A., Read, L.L., Kanim, L.E., Reeder, S.J.,1988. Evaluation of a worksite self-help smoking cessation program forregistered nurses. Am. J. Health Promot. 3 (2), 26–35.
Gritz, E.R., Thompson, B., Emmons, K., Ockene, J.K., McLerran, D.F., Nielsen,I.R., 1998. Gender differences among smokers and quitters in the WorkingWell Trial. Prev. Med. 27 (4), 553–561.
Heaney, C.A., Goetzel, R.Z., 1997. A review of health-related outcomes of multi-component worksite health promotion programs. Am. J. Health Promot. 11 (4),290–307.
Hennrikus, D.J., Jeffery, R.W., Lando, H.A., 1996. Occasional smoking in aMinnesota working population. Am. J. Public Health 86 (9), 1260–1266.
Hibbard, J.H., 1993. Social roles as predictors of cessation in a cohort of womensmokers. Women Health 20 (4), 71–80.
Hoogendoorn, W.E., van Poppel, M.N., Bongers, P.M., Koes, B.W., Bouter,L.M., 2000. Systematic review of psychosocial factors at work and privatelife as risk factors for back pain. Spine 25 (16), 2114–2125.
ISI ResearchSoft. Reference manager professional network. [9.5N]. 2000. ISI;Research Soft. 1984. Ref Type: Computer Program.
Johnson, J.V., Hall, E.M., Theorell, T., 1989. Combined effects of job strain andsocial isolation on cardiovascular disease morbidity and mortality in arandom sample of the Swedish male working population. Scand J. WorkEnviron. Health 15, 271–279.
Karasek, R., Theorell, T., 1990. Healthy Work. Stress, Productivity, and theReconstruction of Working Life. Basic Books.
Klesges, R.C., Brown, K., Pascale, R.W., Murphy, M., 1988. Factors associatedwith participation, attrition, and outcome in a smoking cessation program atthe workplace. Health Psychol. 7 (6), 575–589.
Krokstad, S., Johnsen, R., Westin, S., 2002. Social determinants of disabilitypension: a 10-year follow-up of 62,000 people in a Norwegian county pop-ulation. Int. J. Epidemiol. 31 (6), 1183–1191.
Landsbergis, P.A., Schnall, P.L., Deitz, D.K., Warren, K., Pickering, T.G.,Schwartz, J.E., 1998. Job strain and health behaviors: results of a prospectivestudy. Am. J. Health Promot. 12 (4), 237–245.
Leigh, J.P., 1996. Occupations, cigarette smoking, and lung cancer in theepidemiological follow-up to the NHANES I and the California Occupa-tional Mortality Study. Bull. N. Y. Acad. Med. 73 (2), 370–397.
Lund, T., Iversen, L., Poulsen, K.B., 2001. Work environment factors, health,lifestyle and marital status as predictors of job change and early retirement inphysically heavy occupations. Am. J. Ind. Med. 40, 161–169.
Lundberg, O., Rosen, B., Rosen, M., 1991. Who stopped smoking? Results froma panel survey of living conditions in Sweden. Soc. Sci. Med. 32 (5),619–622.
Marmot, M.G., Smith, G.D., Stansfeld, S., Patel, C., North, F., Head, J., White,I., Brunner, E., Feeney, A., 1991. Health inequalities among British civilservants: the Whitehall II study. Lancet 337 (8754), 1387–1393.
Mermelstein, R., Cohen, S., Lichtenstein, E., Baer, J.S., Kamarck, T., 1986.Social support and smoking cessation and maintenance. J. Consult. Clin.Psychol. 54 (4), 447–453.
Nelson, D.E., Emont, S.L., Brackbill, R.M., Cameron, L.L., Peddicord, J., Fiore,M.C., 1994. Cigarette smoking prevalence by occupation in the UnitedStates. A comparison between 1978 to 1980 and 1987 to 1990. J. Occup.Med. 36 (5), 516–525.
Ockene, J.K., Emmons, K.M., Mermelstein, R.J., Perkins, K.A., Bonollo, D.S.,Voorhees, C.C., Hollis, J.F., 2000. Relapse and maintenance issues forsmoking cessation. Health Psychol. 19 (1), 17–31 (Suppl).
Osler, M., 1993. Social class and health behaviour in Danish adults: a longitudinalstudy. Public Health 107 (4), 251–260.
Osler, M., Gerdes, L.U., Davidsen, M., Bronnum-Hansen, H., Madsen, M.,Jorgensen, T., Schroll, M., 2000. Socioeconomic status and trends inrisk factors for cardiovascular diseases in the Danish MONICApopulation, 1982–1992. J. Epidemiol. Community Health 54 (2),108–113.
Osler, M., Holstein, B., Avlund, K., Damsgaard, M.T., Rasmussen, N.K., 2001.Socioeconomic position and smoking behaviour in Danish adults. Scand J.Public Health 29 (1), 32–39.
Pelletier, K.R., 1993. A review and analysis of the health and cost-effectiveoutcome studies of comprehensive health promotion and disease preventionprograms at the worksite: 1991–1993 update. Am. J. Health Promot. 8 (1),50–62.
Pucci, L.G., Haglund, B.J., 1993. Organizational factors affecting smoking atwork: results from focus group interviews with smokers and ex-smokers.J. Prim. Prev. 14 (2), 115–127.
Rose, J.E., Ananda, S., Jarvik, M.E., 1983. Cigarette smoking during anxiety-provoking and monotonous tasks. Addict. Behav. 8 (4), 353–359.
Rosen, M., Wall, S., Hanning, M., Lindberg, G., Nystrom, L., 1987. Smokinghabits and their confounding effects among occupational groups in Sweden.Scand J. Soc. Med. 15 (4), 233–240.
Serxner, S., Catalano, R., Dooley, D., Mishra, S., 1991. Tobacco use: selection,stress, or culture? J. Occup. Med. 33 (10), 1035–1039.
Shields, M., 1999. Long working hours and health. Health Rep. 11 (2), 33–48.Sloan, R.P., Dimberg, L., Welkowitz, L.A., Kristiansen, M.A., 1990. Cessation
and relapse in a year-long workplace quit-smoking contest. Prev. Med. 19(4), 414–423.
Stephens, T., Jackson, K., Garrison, C., Blair, Steven, 1989. Smokingbehaviors and attitudes in the workplace. Health Educ. Res. 4 (2),245–249.
Steptoe, A., Wardle, J., Pollard, T.M., Canaan, L., Davies, G.J., 1996.Stress, social support and health-related behavior: a study of smoking,alcohol consumption and physical exercise. J. Psychosom. Res. 41 (2),171–180.

305K. Albertsen et al. / Preventive Medicine 43 (2006) 291–305
Steptoe, A., Wardle, J., Lipsey, Z., Mills, R., Oliver, G., Jarvis, M., Kirschbaum, C.,1998. A longitudinal study of work load and variations in psychological well-being, cortisol, smoking, and alcohol consumption. Ann. Behav. Med. 20 (2),84–91.
Swan, G.E., Denk, C.E., 1987. Dynamic models for the maintenance of smokingcessation: event history analysis of late relapse. J Behav. Med. 10 (6),527–554.
Swan, G.E., Denk, C.E., Parker, S.D., Carmelli, D., Furze, C.T., Rosenman, R.H.,1988. Risk factors for late relapse in male and female ex-smokers. Addict.Behav. 13 (3), 253–266.
Terborg, J.R., Hibbard, J., Glasgow, R.E., 1995. Behavior change at the worksite:
does social support make a difference? Am. J. Health Promot. 10 (2),125–131.
Warr, P., 1987. Work, Unemployment, and Mental Health. Oxford University Press,New York.
Westman, M., Eden, D., Shirom, A., 1985. Job stress, cigarette smoking andcessation: the conditioning effects of peer support. Soc. Sci. Med. 20 (6),637–644.
Wewers, M.E., Ahijevych, K.L., 1991. Work stress after smoking cessation.AAOHN J. 39 (12), 547–551.
Wooden, M., Bush, R., 1995. Smoking cessation and absence from work. Prev.Med. 24 (5), 535–540.
Related Documents