A Systematic Review of Solid-Pseudopapillary Neoplasms Are These Rare Lesions? Joanna K. Law, MD,* Aadil Ahmed, MD,* Vikesh K. Singh, MD,* Venkata S. Akshintala, MD,* Matthew T. Olson, MD,Þ Siva P. Raman, MD,þ Syed Z. Ali, MD,Þ Elliot K. Fishman, MD,þ Ihab Kamel, MD, PhD,þ Marcia I. Canto, MD,* Marco Dal Molin, MD,§ Robert A. Moran, MBBCh,* Mouen A. Khashab, MD,* Nita Ahuja, MD,|| Michael Goggins, MD,*Þ Ralph H. Hruban, MD,§ Christopher L. Wolfgang, MD, PhD,|| and Anne Marie Lennon, MD, PhD* Objective: The aim of the study was to determine if there had been any change in the number of solid-pseudopapillary neoplasm (SPN) cases detected and their evaluation or management over time. Methods: A systematic review of SPN was performed of all articles published in English in PubMed and Scopus. Results: A total of 2744 patients with SPN were identified in 484 studies published between 1961 and 2012; 87.8% of the cases were reported between 2000 and 2012. A total of 2408 (87.8%) were females, and the mean age was 28.5 (SD, 13.7) years. The most common symptom was abdominal pain in 63.6% of the cases and incidentally detected in 38.1% of the cases. There were 2285 patients who underwent pancreatic resection. The mean tumor size was 8.6 (SD, 4.3) cm. Follow-up was reported for 1952 (90.5%) patients, with a mean follow-up of 36.1 (SD, 32.8) months. Disease-free survival was documented in 1866 (95.6%) patients with recurrence in 86 (4.4%) patients; the median time to recur- rence was 50.5 months. Conclusions: The number of SPNs reported in the literature has seen a 7-fold increase in the number of cases reported since 2000 compared with before. Solid-pseudopapillary neoplasms continue to be primarily found in young women and present with nonspecific symptoms. Surgery remains the mainstay of treatment with an excellent long-term prognosis. Key Words: pancreas, solid-pseudopapillary neoplasm, review, systematic review, cyst Abbreviations: CT - computed tomography, EUS - endoscopic ultrasound, EUS-FNA - endoscopic ultrasoundYguided fine-needle aspiration, MRI - magnetic resonance imaging, SPN - solid-pseudopapillary neoplasm, TAUS - transabdominal ultrasound (Pancreas 2014;43: 331Y337) S olid-pseudopapillary neoplasms (SPNs) were first described by Frantz 1 in 1959. Solid-pseudopapillary neoplasms have been referred to using a variety of names including papillary epithelial neoplasm of the pancreas, solid and papillary tumors of the pancreas, and Hamoudi or Frantz tumors. In 1996, the World Health Organization classified them as a borderline tumor of the exocrine pancreas and named them SPN. 2 Solid- pseudopapillary neoplasms occur most frequently in young women. They classically present as a large, solitary, well- circumscribed lesion, which can have a completely cystic, mixed cystic and solid, or a purely solid appearance on ab- dominal imaging (Fig. 1). Most patients have localized dis- ease, with only 9% to 15% of the patients presenting with metastasis or local invasion. The mainstay of treatment is surgical resection, and unlike pancreatic adenocarcinoma, the reported 5-year survival rate is as high as 94% to 97%. 3,4 Solid-pseudopapillary neoplasms are rare pancreatic cystic neoplasms, with the largest single-institution series to date in- cluding only 37 patients who underwent resection of SPN. 3 Papavramidis and Papavramidis 4 performed a review of SPN publications reported in the English language and identified 718 cases of SPN, which were the sum of all the studies re- ported up to 2003. Over the last decade, there has been a marked increase in the number of incidentally detected pan- creatic cysts, with 2.6% of the asymptomatic patients under- going multidetector computed tomographic (CT) scans found to have pancreatic cysts. 5 We hypothesized that there was likely to have been a similar increase in the number of SPN detected. The aims of this study were to perform a systematic review of all studies on SPN published in the English literature since 1959 and to determine if there have been any changes in the number of cases detected and their evaluation or management over time. METHODS Literature Search PubMed and Scopus were queried from the inception of each database to September 19, 2012, using predeter- mined search strings that included the terms pancreas and pseu- dopapillary (see Appendix 1, Supplemental Digital Content 1, http://links.lww.com/MPA/A273 for full search terms). Because of the various names associated with this lesion, historic names ORIGINAL ARTICLE Pancreas & Volume 43, Number 3, April 2014 www.pancreasjournal.com 331 From the *Division of Gastroenterology, †Department of Pathology, ‡Department of Radiology, Johns Hopkins University School of Medicine, §Department of Pathology, Sol Goldman Pancreatic Cancer Research Center, and ||Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD. Received for publication July 24, 2013; accepted September 26, 2013. Reprints: Anne Marie Lennon, MD, PhD, Johns Hopkins Hospital, Division of Gastroenterology, Sheikh ZayedTower, Suite 7125J, Baltimore, MD 21287 (e<mail: [email protected]). This work was supported by Cancer Center (grant number P30 CA006973). Dr Khashab is a consultant for Boston Scientific and Olympus America and has received research support from Cook Medical. Dr Singh is a consultant for AbbVie, Santarus, D-Pharm, and Boston Scientific. Dr Law is the Volker Dolch Fellow in Gastroenterology at Johns Hopkins Hospital. The remaining authors have no funding or conflicts of interest to declare. Author Contributions: Data acquisition, data analysis, and writing of the article: Drs Law and Ahmed. Data and statistical analysis: Dr Akshintala. Interpretation of data: Drs Khashab, Singh, Moran, Canto, and Goggins. Interpretation of radiology data: Drs Raman, Fishman, and Kamel. Interpretation of surgical data: Drs Dal Molin, Ahuja, and Wolfgang. Interpretation of pathology data: Drs Olson, Ali, and Hruban. Radiology images: Drs Raman, Fishman, and Kamel. Concept development and writing and editing of the article: Dr Lennon. Editing of the article and final approval: Drs Raman, Fishman, Kamel, Olson, Ali, Hruban, Akshintala, Khashab, Singh, Moran, Canto, Goggins, Dal Molin, Ahuja, and Wolfgang. Supplemental digital contents are available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.pancreasjournal.com). Copyright * 2014 by Lippincott Williams & Wilkins Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A Systematic Review of Solid-Pseudopapillary NeoplasmsAre These Rare Lesions?
Joanna K. Law, MD,* Aadil Ahmed, MD,* Vikesh K. Singh, MD,* Venkata S. Akshintala, MD,*Matthew T. Olson, MD,Þ Siva P. Raman, MD,þ Syed Z. Ali, MD,Þ Elliot K. Fishman, MD,þ
Ihab Kamel, MD, PhD,þ Marcia I. Canto, MD,* Marco Dal Molin, MD,§ Robert A. Moran, MBBCh,*Mouen A. Khashab, MD,* Nita Ahuja, MD,|| Michael Goggins, MD,*Þ Ralph H. Hruban, MD,§
Christopher L. Wolfgang, MD, PhD,|| and Anne Marie Lennon, MD, PhD*
Objective: The aim of the study was to determine if there had beenany change in the number of solid-pseudopapillary neoplasm (SPN)cases detected and their evaluation or management over time.Methods: A systematic review of SPN was performed of all articlespublished in English in PubMed and Scopus.Results: A total of 2744 patients with SPN were identified in 484studies published between 1961 and 2012; 87.8% of the cases werereported between 2000 and 2012. A total of 2408 (87.8%) were females,and the mean age was 28.5 (SD, 13.7) years. The most common symptomwas abdominal pain in 63.6% of the cases and incidentally detected in38.1% of the cases. There were 2285 patients who underwent pancreaticresection. The mean tumor size was 8.6 (SD, 4.3) cm. Follow-up wasreported for 1952 (90.5%) patients, with a mean follow-up of 36.1 (SD,32.8) months. Disease-free survival was documented in 1866 (95.6%)patients with recurrence in 86 (4.4%) patients; the median time to recur-rence was 50.5 months.Conclusions: The number of SPNs reported in the literature has seena 7-fold increase in the number of cases reported since 2000 comparedwith before. Solid-pseudopapillary neoplasms continue to be primarilyfound in young women and present with nonspecific symptoms. Surgeryremains the mainstay of treatment with an excellent long-term prognosis.
Key Words: pancreas, solid-pseudopapillary neoplasm, review,systematic review, cyst
Abbreviations: CT - computed tomography, EUS - endoscopicultrasound, EUS-FNA - endoscopic ultrasoundYguided fine-needleaspiration, MRI - magnetic resonance imaging,SPN - solid-pseudopapillary neoplasm, TAUS - transabdominal ultrasound
(Pancreas 2014;43: 331Y337)
Solid-pseudopapillary neoplasms (SPNs) were first describedby Frantz1 in 1959. Solid-pseudopapillary neoplasms have
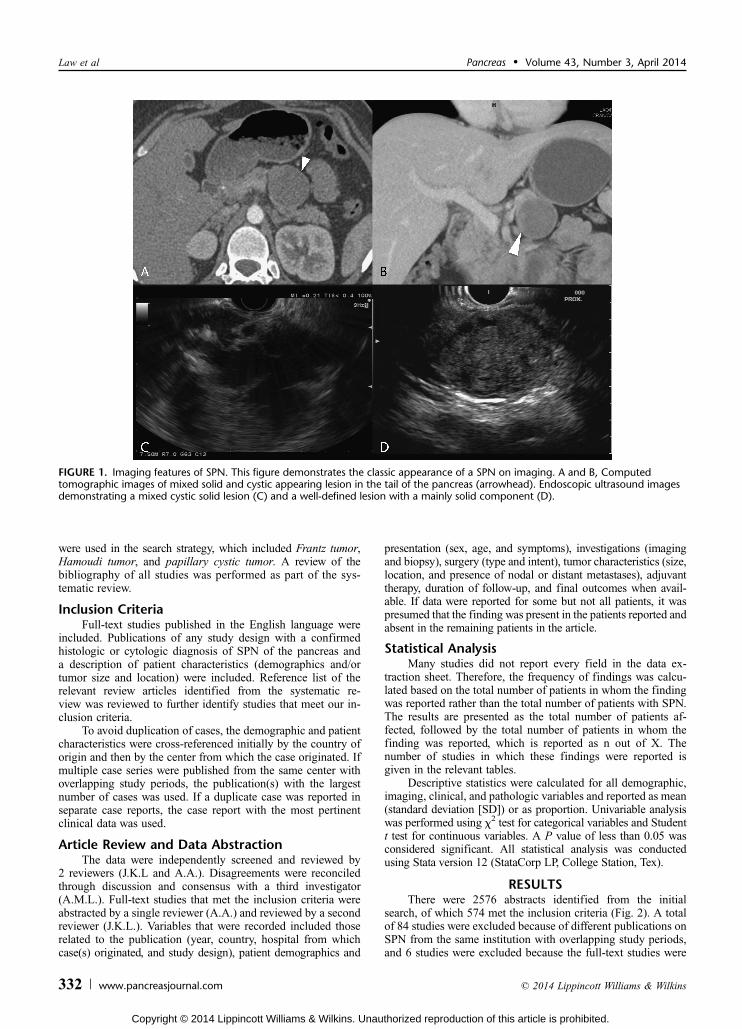
been referred to using a variety of names including papillaryepithelial neoplasm of the pancreas, solid and papillary tumorsof the pancreas, and Hamoudi or Frantz tumors. In 1996, theWorld Health Organization classified them as a borderlinetumor of the exocrine pancreas and named them SPN.2 Solid-pseudopapillary neoplasms occur most frequently in youngwomen. They classically present as a large, solitary, well-circumscribed lesion, which can have a completely cystic,mixed cystic and solid, or a purely solid appearance on ab-dominal imaging (Fig. 1). Most patients have localized dis-ease, with only 9% to 15% of the patients presenting withmetastasis or local invasion. The mainstay of treatment issurgical resection, and unlike pancreatic adenocarcinoma, thereported 5-year survival rate is as high as 94% to 97%.3,4
Solid-pseudopapillary neoplasms are rare pancreatic cysticneoplasms, with the largest single-institution series to date in-cluding only 37 patients who underwent resection of SPN.3
Papavramidis and Papavramidis4 performed a review of SPNpublications reported in the English language and identified718 cases of SPN, which were the sum of all the studies re-ported up to 2003. Over the last decade, there has been amarked increase in the number of incidentally detected pan-creatic cysts, with 2.6% of the asymptomatic patients under-going multidetector computed tomographic (CT) scans found tohave pancreatic cysts.5 We hypothesized that there was likely tohave been a similar increase in the number of SPN detected.The aims of this study were to perform a systematic review ofall studies on SPN published in the English literature since 1959and to determine if there have been any changes in the numberof cases detected and their evaluation or management over time.
METHODS
Literature SearchPubMed and Scopus were queried from the inception
of each database to September 19, 2012, using predeter-mined search strings that included the terms pancreas and pseu-dopapillary (see Appendix 1, Supplemental Digital Content 1,http://links.lww.com/MPA/A273 for full search terms). Becauseof the various names associated with this lesion, historic names
ORIGINAL ARTICLE
Pancreas & Volume 43, Number 3, April 2014 www.pancreasjournal.com 331
From the *Division of Gastroenterology, †Department of Pathology, ‡Departmentof Radiology, Johns Hopkins University School of Medicine, §Department ofPathology, Sol Goldman Pancreatic Cancer Research Center, and ||Department ofSurgery, Johns Hopkins University School of Medicine, Baltimore, MD.Received for publication July 24, 2013; accepted September 26, 2013.Reprints: Anne Marie Lennon, MD, PhD, Johns Hopkins Hospital, Division
of Gastroenterology, Sheikh Zayed Tower, Suite 7125J, Baltimore, MD21287 (e<mail: [email protected]).
This work was supported by Cancer Center (grant number P30 CA006973).Dr Khashab is a consultant for Boston Scientific and Olympus America and
has received research support from CookMedical. Dr Singh is a consultantfor AbbVie, Santarus, D-Pharm, and Boston Scientific. Dr Law is theVolker Dolch Fellow in Gastroenterology at Johns Hopkins Hospital. Theremaining authors have no funding or conflicts of interest to declare.
Author Contributions: Data acquisition, data analysis, and writing of thearticle: Drs Law and Ahmed. Data and statistical analysis: DrAkshintala. Interpretation of data: Drs Khashab, Singh, Moran, Canto,and Goggins. Interpretation of radiology data: Drs Raman, Fishman, andKamel. Interpretation of surgical data: Drs Dal Molin, Ahuja, andWolfgang. Interpretation of pathology data: Drs Olson, Ali, and Hruban.Radiology images: Drs Raman, Fishman, and Kamel. Concept developmentand writing and editing of the article: Dr Lennon. Editing of the article andfinal approval: Drs Raman, Fishman, Kamel, Olson, Ali, Hruban, Akshintala,Khashab, Singh, Moran, Canto, Goggins, Dal Molin, Ahuja, and Wolfgang.
Supplemental digital contents are available for this article. Direct URL citationsappear in the printed text and are provided in theHTMLandPDFversions ofthis article on the journal’s Web site (www.pancreasjournal.com).
Copyright * 2014 by Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
were used in the search strategy, which included Frantz tumor,Hamoudi tumor, and papillary cystic tumor. A review of thebibliography of all studies was performed as part of the sys-tematic review.
Inclusion CriteriaFull-text studies published in the English language were
included. Publications of any study design with a confirmedhistologic or cytologic diagnosis of SPN of the pancreas anda description of patient characteristics (demographics and/ortumor size and location) were included. Reference list of therelevant review articles identified from the systematic re-view was reviewed to further identify studies that meet our in-clusion criteria.
To avoid duplication of cases, the demographic and patientcharacteristics were cross-referenced initially by the country oforigin and then by the center from which the case originated. Ifmultiple case series were published from the same center withoverlapping study periods, the publication(s) with the largestnumber of cases was used. If a duplicate case was reported inseparate case reports, the case report with the most pertinentclinical data was used.
Article Review and Data AbstractionThe data were independently screened and reviewed by
2 reviewers (J.K.L and A.A.). Disagreements were reconciledthrough discussion and consensus with a third investigator(A.M.L.). Full-text studies that met the inclusion criteria wereabstracted by a single reviewer (A.A.) and reviewed by a secondreviewer (J.K.L.). Variables that were recorded included thoserelated to the publication (year, country, hospital from whichcase(s) originated, and study design), patient demographics and
presentation (sex, age, and symptoms), investigations (imagingand biopsy), surgery (type and intent), tumor characteristics (size,location, and presence of nodal or distant metastases), adjuvanttherapy, duration of follow-up, and final outcomes when avail-able. If data were reported for some but not all patients, it waspresumed that the finding was present in the patients reported andabsent in the remaining patients in the article.
Statistical AnalysisMany studies did not report every field in the data ex-
traction sheet. Therefore, the frequency of findings was calcu-lated based on the total number of patients in whom the findingwas reported rather than the total number of patients with SPN.The results are presented as the total number of patients af-fected, followed by the total number of patients in whom thefinding was reported, which is reported as n out of X. Thenumber of studies in which these findings were reported isgiven in the relevant tables.
Descriptive statistics were calculated for all demographic,imaging, clinical, and pathologic variables and reported as mean(standard deviation [SD]) or as proportion. Univariable analysiswas performed using W2 test for categorical variables and Studentt test for continuous variables. A P value of less than 0.05 wasconsidered significant. All statistical analysis was conductedusing Stata version 12 (StataCorp LP, College Station, Tex).
RESULTSThere were 2576 abstracts identified from the initial
search, of which 574 met the inclusion criteria (Fig. 2). A totalof 84 studies were excluded because of different publications onSPN from the same institution with overlapping study periods,and 6 studies were excluded because the full-text studies were
FIGURE 1. Imaging features of SPN. This figure demonstrates the classic appearance of a SPN on imaging. A and B, Computedtomographic images of mixed solid and cystic appearing lesion in the tail of the pancreas (arrowhead). Endoscopic ultrasound imagesdemonstrating a mixed cystic solid lesion (C) and a well-defined lesion with a mainly solid component (D).
Law et al Pancreas & Volume 43, Number 3, April 2014
332 www.pancreasjournal.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

not available in English. There were 484 studies (Appendix 2,Supplemental Digital Content 2, http://links.lww.com/MPA/A273)available for analysis. These included 292 (60.3%) case reportsand 191 (39.5%) case series with a mean of 9.9 cases (range,2Y114) and 1 (0.2%) literature review. One hundred forty-six(30%) of the studies were published between 1961 and 1999,with 338 (70%) studies published between 2000 and 2012.
Two literature reviews of SPN, 1 of English language4 andthe other of Chinese-language studies,6 have previously beenpublished. The English-language review was not included,4
but a hand search of the references was performed, and theoriginal studies in the references were included in the currentstudy. The Chinese article identified 553 patients in 117 studies,which were found by querying 2 large databases of Chinese-language publications.6 None of the original publications wereavailable in English, and therefore, the patients from this studywere included in the systematic review without a review ofthe original studies.
Patient PresentationThere were 2744 patients with SPN identified, of whom
6 had synchronous lesions. There were 334 (12.2%) patientsand 2410 (87.8%) patients reported from 1961 to 1999 and2000 to 2012, respectively. The number of patients reported inthe literature by year is shown in Figure 3. The results from theChinese review study6 were excluded from this figure becauseno data were provided as to the number of patients diagnosed
each year. Women accounted for 2408 (87.8%) of the patients,of whom 301 (90.1%; n = 334) were diagnosed before2000 and 2107 (87.4%; n = 2410) were diagnosed between2000 and 2012 (Table 1). The mean age at presentation was28.5 (SD, 13.7) years. The mean tumor size was 8.6 (SD, 4.3) cm(n = 2750). The size of the SPN detected decreased from amean of 9.8 cm before 2000 to 8.1 cm in the lesions foundbetween 2000 and 2012 (P G 0.05). Most of the SPNs werelocated in the body and tail of the pancreas (59.3%; n = 1626),with 36.0% (n = 988) of the SPNs found in the head or uncinateprocess with no difference in the location of the lesions betweenthe 2 periods.
The most common presenting symptom was abdominalpain or discomfort, which was present in 1389 (63.6%; n = 2183)patients. Patients also presented with a palpable abdominal mass,nausea or vomiting, and weight loss (Appendix 3, SupplementalDigital Content 3, http://links.lww.com/MPA/A274). Pancreatitisand jaundice were relatively rare, occurring in 49 (5.0%; n = 974)and 10 (10.3%; n = 97) patients, respectively. There were 593(38.1%; n = 1557) patients who were asymptomatic (Appendix 3,Supplemental Digital Content 3, http://links.lww.com/MPA/A274).
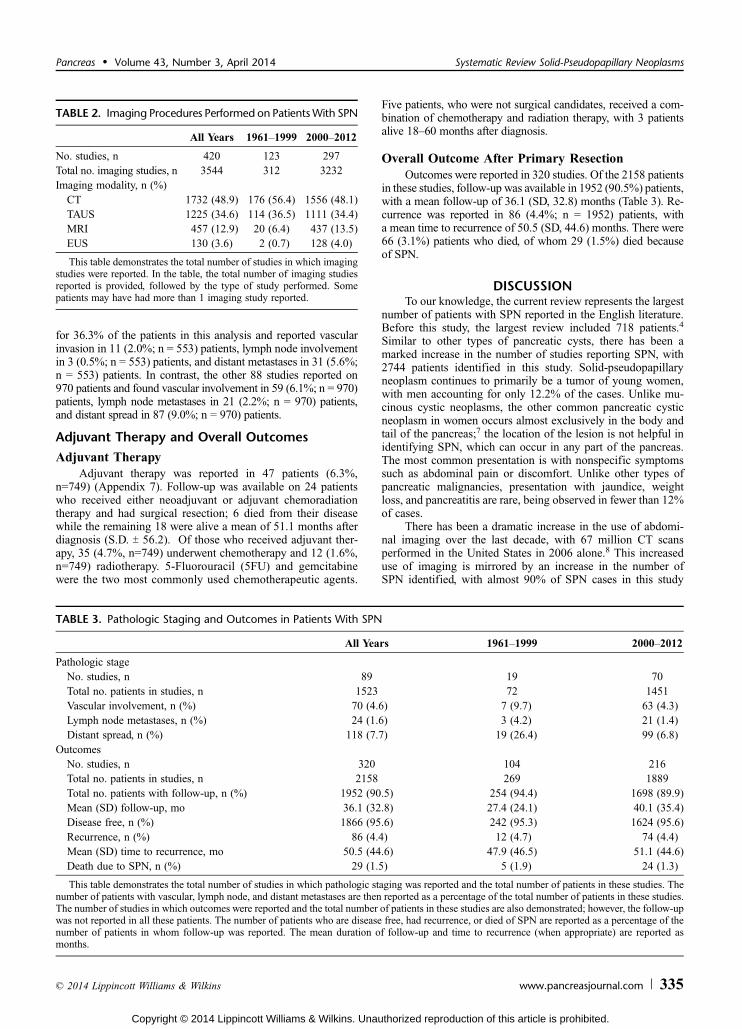
Abdominal ImagingA total of 3544 imaging studies were reported, with 312
studies performed before 2000 and 3232 studies performed be-tween 2000 and 2012 (Table 2). Computed tomography was themost common form of abdominal imaging and accounted for
FIGURE 2. Flow diagram illustrating the search process.
Pancreas & Volume 43, Number 3, April 2014 Systematic Review Solid-Pseudopapillary Neoplasms
* 2014 Lippincott Williams & Wilkins www.pancreasjournal.com 333
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

1732 (48.9%) studies. The secondmost common form of imagingwas transabdominal ultrasound (TAUS), which accounted for1225 (34.6%) studies, followed by magnetic resonance imaging(MRI), accounting for 457 (12.9%) studies. Endoscopic ultra-sound (EUS) accounted for 130 (3.7%) studies.
Preoperative Tissue DiagnosisA total of 253 preoperative biopsies were performed either
percutaneously (58.5%; n = 148) or via EUS-guided fine-needle aspiration (EUS-FNA; 41.5%; n = 105; Appendix 4,Supplemental Digital Content 4, http://links.lww.com/MPA/A275),which correctly identified SPN in 164 (64.8%) of the cases.Percutaneous biopsies correctly identified 91 (61.5%; n = 148;range, 0%Y100%) SPNs. Endoscopic ultrasoundYFNA cor-rectly identified 73 (69.5%; n = 105; range, 0%Y100%) SPNs;all of which were performed after 2000.
Surgical InterventionPancreatic resections were reported in 2285 (85.1%; n = 2685)
patients (Appendix 5, Supplemental Digital Content 5,http://links.lww.com/MPA/A276), of whom 293 (12.8%) wereperformed before 2000 and 1992 (87.2%) were performed
from 2000 to 2012. There were 1111 (48.6%) patients whounderwent a distal pancreatectomy, 552 (24.2%) patientswho underwent pancreaticoduodenectomy, 202 (8.8%) patientswho underwent enucleations, 91 (4.0%) patients who underwentcentral pancreatectomies, and 18 (0.8%) patients who underwenttotal pancreatectomies. The type of pancreatic resection was notspecified in 311 (13.6%) patients. The surgery was performed viaan open procedure in 1903 (83.3%) cases, whereas 39 (1.7%)cases were performed laparoscopically, and in 343 (15.0%) cases,the surgical approach was not indicated. Most laparoscopic pro-cedures (97.4%; n = 38) were performed between January 2000and 2012.
Pathologic StageDetailed pathologic staging was infrequently documented,
with only 89 (18.4%) studies reporting these data (see Appendix 6,Supplemental Digital Content 6, http://links.lww.com/MPA/A277for details), accounting for a total of 1523 (55.5%) patients(Table 3). Vascular involvement was identified in 70 (4.6%;n = 1523) patients, lymph node metastases was reported in 24(1.6%; n = 1523) patients, and distant spread was noted in 118(7.7%; n = 1523) patients. The study by Yu et al6 accounted
FIGURE 3. The number of patients with SPN over time. This figure shows the number of reported cases of SPN reported in the Englishliterature per year.
TABLE 1. Patient Demographics and Tumor Characteristics
All Years 1961Y1999 2000Y2012
n 484 146 338Patients with SPN, n 2744 334 2410Female, n (%) 2408 (87.8) 301 (90.1) 2107 (87.4)Mean (SD) age, y 28.5 (13.7) 26.2 (13.1) 29.5 (13.9)Tumor location, n (%)Head 988 (36.0) 125 (37.4) 863 (35.8)Body/tail 1626 (59.3) 202 (60.5) 1424 (59.1)Not documented 99 (3.6) 4 (1.2) 95 (3.9)Extrapancreatic 31 (1.1) 3 (0.9) 28 (1.2)
No. studies reporting on tumor size, n 454 139 315Total no. patients in studies reporting mean tumor size, n (%) 2650 325 (12.3) 2325 (87.7)Mean (SD) tumor size, cm 8.6 (4.3) 9.8 (4.1) 8.1 (4.4)
Sex, age, and tumor location were reported in all studies.
Law et al Pancreas & Volume 43, Number 3, April 2014
334 www.pancreasjournal.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
for 36.3% of the patients in this analysis and reported vascularinvasion in 11 (2.0%; n = 553) patients, lymph node involvementin 3 (0.5%; n = 553) patients, and distant metastases in 31 (5.6%;n = 553) patients. In contrast, the other 88 studies reported on970 patients and found vascular involvement in 59 (6.1%; n = 970)patients, lymph node metastases in 21 (2.2%; n = 970) patients,and distant spread in 87 (9.0%; n = 970) patients.
Adjuvant Therapy and Overall Outcomes
Adjuvant TherapyAdjuvant therapy was reported in 47 patients (6.3%,
n=749) (Appendix 7). Follow-up was available on 24 patientswho received either neoadjuvant or adjuvant chemoradiationtherapy and had surgical resection; 6 died from their diseasewhile the remaining 18 were alive a mean of 51.1 months afterdiagnosis (S.D. T 56.2). Of those who received adjuvant ther-apy, 35 (4.7%, n=749) underwent chemotherapy and 12 (1.6%,n=749) radiotherapy. 5-Fluorouracil (5FU) and gemcitabinewere the two most commonly used chemotherapeutic agents.
Five patients, who were not surgical candidates, received a com-bination of chemotherapy and radiation therapy, with 3 patientsalive 18Y60 months after diagnosis.
Overall Outcome After Primary ResectionOutcomes were reported in 320 studies. Of the 2158 patients
in these studies, follow-up was available in 1952 (90.5%) patients,with a mean follow-up of 36.1 (SD, 32.8) months (Table 3). Re-currence was reported in 86 (4.4%; n = 1952) patients, witha mean time to recurrence of 50.5 (SD, 44.6) months. There were66 (3.1%) patients who died, of whom 29 (1.5%) died becauseof SPN.
DISCUSSIONTo our knowledge, the current review represents the largest
number of patients with SPN reported in the English literature.Before this study, the largest review included 718 patients.4
Similar to other types of pancreatic cysts, there has been amarked increase in the number of studies reporting SPN, with2744 patients identified in this study. Solid-pseudopapillaryneoplasm continues to primarily be a tumor of young women,with men accounting for only 12.2% of the cases. Unlike mu-cinous cystic neoplasms, the other common pancreatic cysticneoplasm in women occurs almost exclusively in the body andtail of the pancreas;7 the location of the lesion is not helpful inidentifying SPN, which can occur in any part of the pancreas.The most common presentation is with nonspecific symptomssuch as abdominal pain or discomfort. Unlike other types ofpancreatic malignancies, presentation with jaundice, weightloss, and pancreatitis are rare, being observed in fewer than 12%of cases.
There has been a dramatic increase in the use of abdomi-nal imaging over the last decade, with 67 million CT scansperformed in the United States in 2006 alone.8 This increaseduse of imaging is mirrored by an increase in the number ofSPN identified, with almost 90% of SPN cases in this study
TABLE 2. Imaging Procedures Performed on PatientsWith SPN
All Years 1961Y1999 2000Y2012
No. studies, n 420 123 297Total no. imaging studies, n 3544 312 3232Imaging modality, n (%)CT 1732 (48.9) 176 (56.4) 1556 (48.1)TAUS 1225 (34.6) 114 (36.5) 1111 (34.4)MRI 457 (12.9) 20 (6.4) 437 (13.5)EUS 130 (3.6) 2 (0.7) 128 (4.0)
This table demonstrates the total number of studies in which imagingstudies were reported. In the table, the total number of imaging studiesreported is provided, followed by the type of study performed. Somepatients may have had more than 1 imaging study reported.
TABLE 3. Pathologic Staging and Outcomes in Patients With SPN
All Years 1961Y1999 2000Y2012
Pathologic stageNo. studies, n 89 19 70Total no. patients in studies, n 1523 72 1451Vascular involvement, n (%) 70 (4.6) 7 (9.7) 63 (4.3)Lymph node metastases, n (%) 24 (1.6) 3 (4.2) 21 (1.4)Distant spread, n (%) 118 (7.7) 19 (26.4) 99 (6.8)
OutcomesNo. studies, n 320 104 216Total no. patients in studies, n 2158 269 1889Total no. patients with follow-up, n (%) 1952 (90.5) 254 (94.4) 1698 (89.9)Mean (SD) follow-up, mo 36.1 (32.8) 27.4 (24.1) 40.1 (35.4)Disease free, n (%) 1866 (95.6) 242 (95.3) 1624 (95.6)Recurrence, n (%) 86 (4.4) 12 (4.7) 74 (4.4)Mean (SD) time to recurrence, mo 50.5 (44.6) 47.9 (46.5) 51.1 (44.6)Death due to SPN, n (%) 29 (1.5) 5 (1.9) 24 (1.3)
This table demonstrates the total number of studies in which pathologic staging was reported and the total number of patients in these studies. Thenumber of patients with vascular, lymph node, and distant metastases are then reported as a percentage of the total number of patients in these studies.The number of studies in which outcomes were reported and the total number of patients in these studies are also demonstrated; however, the follow-upwas not reported in all these patients. The number of patients who are disease free, had recurrence, or died of SPN are reported as a percentage of thenumber of patients in whom follow-up was reported. The mean duration of follow-up and time to recurrence (when appropriate) are reported asmonths.
Pancreas & Volume 43, Number 3, April 2014 Systematic Review Solid-Pseudopapillary Neoplasms
* 2014 Lippincott Williams & Wilkins www.pancreasjournal.com 335
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

reported in the last 12 years. Although more imaging is per-formed, one can hypothesize that the number of incidentallydetected SPN would increase. In this study, the number of in-cidentally detected SPN has grown and now accounts for justover 40% of all SPN cases, with 90% of the incidental casesdetected in the last 12 years. During the same period, the meantumor size has decreased from almost 10 cm to just over 8 cm.
Computed tomography, TAUS, MRI, and EUS have allbeen used to detect SPN. Computed tomography is by far thedominant imaging modality, accounting for almost 50% of theprocedures performed. The use of MRI and EUS has increasedsubstantially in the United States, with 791% and 517% in-crease, respectively, in the number of procedures performedbetween 2000 and 2010.9 This increased use has been mirroredin SPN for MRI but not EUS. Although the number of EUSprocedures increased between the 2 periods, EUS is still infre-quently used, accounting for only 3.6% of imaging proceduresperformed during the last 12 years. In this series, the overallaccuracy of EUS-FNA was 69.5%. This is lower than whatwas routinely reported for EUS-FNA for pancreatic adenocar-cinoma, which is in the range of 86% to 91%.10,11 This could becaused by the presence of on-site evaluation for adequacy ofsamples obtained by EUS-FNA that can affect results. Operatorand/or institutional experience may also play a role in adequacyof tissue sampling by EUS-FNA, with a recent study demon-strating a trend toward increasing diagnostic yield with time.12
Given the wide variation in accuracy reported (0%Y100%) forSPN, it is likely that a number of these factors may have beeninvolved.
Surgery is associated with an improved overall survivaland continues to be the standard of care for localized SPN. Incomparison with pancreatic adenocarcinoma and pancreaticneuroendocrine neoplasms, the survival of resected SPN is ex-cellent. However, it should be noted that SPN is clearly a ma-lignant neoplasm with local and metastatic potential. Thus,there is debate about the optimum extent and type of surgicaloperation for SPN. Laparoscopic pancreas surgery is a relativelynew approach. Although laparoscopic distal pancreatectomiesare performed in most high-volume centers, laparoscopic pan-creaticoduodenectomies or central pancreatectomies are onlyperformed by a very small number of surgeons.13,14 This, inaddition to low experience with SPN, is likely to influence therelatively low number of cases approached laparoscopically.Although still relatively rare, the number of pancreatic parenchymaYsparing operations performed for SPN has doubled over thelast 12 years as compared with previous operations and nowaccount for almost 15% of all pancreatic resections. One ofthe critical questions when considering parenchymal-sparingsurgery in patients with SPN is the risk of lymph node me-tastases. Overall, lymph node involvement was reported to bealmost 2.0% in this study. However, more than a third ofthese patients were from a study by Yu et al6 in which thelymph node involvement was 0.5%, compared with a rate of2.2% in the other 88 studies that reported on lymph node in-volvement. The number of lymph nodes examined at surgeryhas been shown to influence the staging in patients withpancreatic ductal adenocarcinoma, where patients with fewerthan 12 lymph nodes were found to be understaged.15 Nodetails of the total number of lymph nodes evaluated wereprovided in the study of Yu et al,6 and it is possible that therisk of lymph node metastases may have been underestimated.
There are few studies that have addressed the use of ad-juvant therapy for patients with SPN. These include case reportsof successful management of otherwise nonsurgical patientswith SPN managed by radiotherapy alone16 and patients who
underwent initial curative resection with subsequent recurrencemanaged by chemotherapy with subsequent disease-free sur-vival.17 However, the small numbers of cases make it difficult todraw any conclusions on the role of adjuvant therapy or theoptimal type of therapy for SPN.
Overall, SPN has a very good prognosis, with just over95% of patients reported as disease free after surgical resectionand with less than 2% mortality. The mean time to recurrence ofthe tumor in this study was just over 4 years; however, the meanfollow-up reported for patients was only 3 years. These findingssuggest that the recurrence rate may be underestimated in theliterature. The data from this study suggest that all patients withSPN should be followed up for a minimum of 5 years.
The primary limitation of the present systematic review isthat the quality of the included studies is poor because mostpublications are case reports or case series involving fewer than10 patients with no prospective or randomized studies. Manyof the studies failed to report on all of the outcomes evaluated inthe present study. Therefore, we analyzed the results based onthe total number of cases reported in the literature. Additionally,care was taken to avoid duplication of cases based on review ofpatient demographics, presentation, and source of each case.Some cases that were excluded were not duplicates but werenested in small case series of which other patients were pub-lished in another larger case series. Despite these limitations,this is the largest systematic review published to date of thisexceedingly rare tumor.
In conclusion, SPN is a rare pancreatic tumor with just lessthan 2800 cases reported in the English literature over 51 years.There has been a 7-fold increase in the number of cases detectedsince 2000, most likely secondary to improvement in the qual-ity and use of cross-sectional imaging. Solid-pseudopapillaryneoplasm typically occurs in young women with imagingdemonstrating a solitary lesion in the pancreas. Surgery is themainstay of treatment, with an overall excellent prognosis.
REFERENCES
1. Frantz V. Tumor of the pancreas. Atlas of Tumor Pathology.1st series. Washington, DC: US Armed Forces Institute of Pathology;1959:32Y33.
2. Kloppel G, Heitz PU, Capella C, et al. Pathology and nomenclatureof human gastrointestinal neuroendocrine (carcinoid) tumors andrelated lesions. World J Surg. 1996;20(2):132Y141.
3. Reddy S, Cameron JL, Scudiere J, et al. Surgical management ofsolid-pseudopapillary neoplasms of the pancreas (Franz or Hamouditumors): a large single-institutional series. J Am Coll Surg.2009;208(5):950Y957.
4. Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of thepancreas: review of 718 patients reported in English literature.J Am Coll Surg. 2005;200(6):965Y972.
5. Laffan TA, Horton KM, Klein AP, et al. Prevalence of unsuspectedpancreatic cysts on MDCT. AJR Am J Roentgenol.2008;191(3):802Y807.
6. Yu PF, Hu ZH, Wang XB, et al. Solid pseudopapillary tumor of thepancreas: a review of 553 cases in Chinese literature. World JGastroenterol. 2010;16(10):1209Y1214.
7. Yamao K, Yanagisawa A, Takahashi K, et al. Clinicopathologicalfeatures and prognosis of mucinous cystic neoplasm with ovarian-typestroma: a multi-institutional study of the Japan pancreas society.Pancreas. 2011;40(1):67Y71.
8. Mettler FA Jr, Thomadsen BR, Bhargavan M, et al. Medical radiationexposure in the U.S. in 2006: preliminary results. Health Phys.2008;95(5):502Y507.
9. Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease inthe United States: 2012 update. Gastroenterology.2012;143(5):1179Y1187, e1171Ye1173.
Law et al Pancreas & Volume 43, Number 3, April 2014
336 www.pancreasjournal.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
10. Haba S, Yamao K, Bhatia V, et al. Diagnostic ability and factorsaffecting accuracy of endoscopic ultrasound-guided fine needleaspiration for pancreatic solid lesions: Japanese large singlecenter experience. J Gastroenterol. 2013;48:973Y981.
11. Yoshinaga S, Suzuki H, Oda I, et al. Role of endoscopicultrasound-guided fine needle aspiration (EUS-FNA) for diagnosis ofsolid pancreatic masses. Dig Endosc. 2011;23(suppl 1):29Y33.
12. Olson MT, Ali SZ. Cytotechnologist on-site evaluation of pancreas fineneedle aspiration adequacy: comparison with cytopathologists andcorrelation with the final interpretation. Acta Cytol.2012;56(4):340Y346.
13. Gagner M, Palermo M. Laparoscopic Whipple procedure: review of theliterature. J Hepatobiliary Pancreat Surg. 2009;16(6):726Y730.
14. Kendrick ML, Cusati D. Total laparoscopic pancreaticoduodenectomy:feasibility and outcome in an early experience. Arch Surg.2010;145(1):19Y23.
15. Slidell MB, Chang DC, Cameron JL, et al. Impact of total lymph nodecount and lymph node ratio on staging and survival afterpancreatectomy for pancreatic adenocarcinoma: a large,population-based analysis. Ann Surg Oncol. 2008;15(1):165Y174.
16. Zauls JA, Dragun AE, Sharma AK. Intensity-modulated radiationtherapy for unresectable solid pseudopapillary tumor of the pancreas. JClin Oncol. 2006;29:639Y640.
17. Ansari D, Elebro J, Tingstedt B, et al. Single-institution experiencewith solid pseudopapillary neoplasm of the pancreas. Scand JGastroenterol. 2011;46(12):1492Y1497.
Pancreas & Volume 43, Number 3, April 2014 Systematic Review Solid-Pseudopapillary Neoplasms
* 2014 Lippincott Williams & Wilkins www.pancreasjournal.com 337
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Related Documents


![Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report ... · It is a mixed odontogenic ... lesions appear to be true neoplasms [1]. ... The lesions present as well-circumscribed, unilocular](https://static.cupdf.com/doc/110x72/5ed590debb43ae0d0e021b61/cronicon-open-access-ec-dental-science-case-report-it-is-a-mixed-odontogenic.jpg)








