A specific subtype C of human immunodeficiency virus type 1 circulates in Brazil Marcelo A. Soares a , Tulio de Oliveira b , Rodrigo M. Brindeiro a , Ricardo S. Diaz c , Ester C. Sabino d , Luı ´s Brigido e , Ivone L. Pires f , Mariza G. Morgado g , Maria C. Dantas h , Draurio Barreira h , Paulo R. Teixeira h , Sharon Cassol b , Amilcar Tanuri a and the Brazilian Network for Drug Resistance Surveillance Objective: To characterize the subtype C strains of HIV type 1 that circulate in Brazil, especially those originated from the southern part of the country. Design and methods: One hundred and twelve HIV-1-positive subjects had their plasma viral RNA extracted. Protease (PR) and reverse transcriptase (RT) genomic regions were polymerase chain reaction-amplified and sequenced for subtype deter- mination. Subtype C strains were selected and compared to other strains of this subtype from the database, and specific amino acid signature patterns were searched. Results: Brazilian subtype C viruses form a very strong monophyletic group when compared to subtype C viruses from other countries and presented specific signature amino acids. Recombinants between subtype C and B viruses have been documented in areas of co-circulation. The incidence of primary PR and RT inhibitor resistance mutations in drug-naı ¨ve subjects was observed. An increasing number of secondary resistance mutations was also seen, some of which are characteristic of subtype C- related sequences. Conclusions: Introduction of subtype C of HIV-1 in Brazil was likely a single event of one or a mixture of similarly related strains. Recombination between subtype C and B viruses is an ongoing process in the country. Primary and secondary drug resistance mutations were observed, although some of the secondary mutations could be associated with subtype C molecular signatures. Subtype-specific polymorphisms of PR and RT sequences found in this subtype C Brazilian variant might influence this emergence and have an impact on HIV treatment and on vaccine development in the country. & 2003 Lippincott Williams & Wilkins AIDS 2003, 17:11–21 Keywords: subtype C, drug resistance mutations, subtype polymorphism, HIV in primary infection, signature sequence Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. From the a Laborato ´rio de Virologia Molecular, Departamento de Gene ´tica, Universidade Federal do Rio de Janeiro, CCS – Bloco A – Cidade Universita ´ria – Ilha do Funda ˜o, 21944-970 Rio de Janeiro, RJ, Brazil, the b HIV-1 Molecular Virology and Bionformatics Unit, Africa Centre /Nelson Mandela School of Medicine, University of Natal, Durban, South Africa, the c Laboratorio de Retrovirologia Escola Paulista de Medicina/UNIFESP, Sa ˜o Paulo, the d Fundac ¸a ˜ o Pro-Sangue, Hemocentro de Sa ˜o Paulo, Universidade de Sa ˜o Paulo, Sa ˜o Paulo, the e Laboratorio de Retrovirologia, Instituto Adolfo Lutz, Sa ˜o Paulo, SP, the f Laborato ´ rio de Virologia, Instituto de Biologia do Exe ´ rcito, Rio de Janeiro, the g Departamento de Imunologia, Fundac ¸a ˜o Instituto Oswaldo Cruz, Rio de Janeiro, RJ and the h CN-DST/AIDS, Ministe ´ rio da Sau ´ de, Brası ´lia, DF, Brazil. See Appendix. Correspondence to Amilcar Tanuri, Laborato ´rio de Virologia Molecular, Departamento de Gene ´tica, Universidade Federal do Rio de Janeiro, CCS – Bloco A – Cidade Universita ´ria – Ilha do Funda ˜o, 21944-970 Rio de Janeiro, RJ, Brazil E-mail: [email protected] Received: 10 April 2002; revised: 4 July 2002; accepted: 4 September 2002. DOI: 10.1097/01.aids.0000042595.93174.a4 ISSN 0269-9370 & 2003 Lippincott Williams & Wilkins 11

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A specific subtype C of human immunodeficiency virustype 1 circulates in Brazil
Marcelo A. Soaresa, Tulio de Oliveirab, Rodrigo M. Brindeiroa,
Ricardo S. Diazc, Ester C. Sabinod, Luıs Brigidoe, Ivone L. Piresf,
Mariza G. Morgadog, Maria C. Dantash, Draurio Barreirah,
Paulo R. Teixeirah, Sharon Cassolb, Amilcar Tanuria and the Brazilian
Network for Drug Resistance Surveillance�
Objective: To characterize the subtype C strains of HIV type 1 that circulate in Brazil,especially those originated from the southern part of the country.
Design and methods: One hundred and twelve HIV-1-positive subjects had theirplasma viral RNA extracted. Protease (PR) and reverse transcriptase (RT) genomicregions were polymerase chain reaction-amplified and sequenced for subtype deter-mination. Subtype C strains were selected and compared to other strains of thissubtype from the database, and specific amino acid signature patterns were searched.
Results: Brazilian subtype C viruses form a very strong monophyletic group whencompared to subtype C viruses from other countries and presented specific signatureamino acids. Recombinants between subtype C and B viruses have been documentedin areas of co-circulation. The incidence of primary PR and RT inhibitor resistancemutations in drug-naıve subjects was observed. An increasing number of secondaryresistance mutations was also seen, some of which are characteristic of subtype C-related sequences.
Conclusions: Introduction of subtype C of HIV-1 in Brazil was likely a single event ofone or a mixture of similarly related strains. Recombination between subtype C and Bviruses is an ongoing process in the country. Primary and secondary drug resistancemutations were observed, although some of the secondary mutations could beassociated with subtype C molecular signatures. Subtype-specific polymorphisms ofPR and RT sequences found in this subtype C Brazilian variant might influence thisemergence and have an impact on HIV treatment and on vaccine development in thecountry. & 2003 Lippincott Williams & Wilkins
AIDS 2003, 17:11–21
Keywords: subtype C, drug resistance mutations, subtype polymorphism, HIV inprimary infection, signature sequence
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
From the aLaboratorio de Virologia Molecular, Departamento de Genetica, Universidade Federal do Rio de Janeiro, CCS – BlocoA – Cidade Universitaria – Ilha do Fundao, 21944-970 Rio de Janeiro, RJ, Brazil, the bHIV-1 Molecular Virology andBionformatics Unit, Africa Centre /Nelson Mandela School of Medicine, University of Natal, Durban, South Africa, thecLaboratorio de Retrovirologia Escola Paulista de Medicina/UNIFESP, Sao Paulo, the dFundacao Pro-Sangue, Hemocentro de SaoPaulo, Universidade de Sao Paulo, Sao Paulo, the eLaboratorio de Retrovirologia, Instituto Adolfo Lutz, Sao Paulo, SP, thefLaboratorio de Virologia, Instituto de Biologia do Exercito, Rio de Janeiro, the gDepartamento de Imunologia, FundacaoInstituto Oswaldo Cruz, Rio de Janeiro, RJ and the hCN-DST/AIDS, Ministerio da Saude, Brasılia, DF, Brazil. �See Appendix.
Correspondence to Amilcar Tanuri, Laboratorio de Virologia Molecular, Departamento de Genetica, Universidade Federal doRio de Janeiro, CCS – Bloco A – Cidade Universitaria – Ilha do Fundao, 21944-970 Rio de Janeiro, RJ, Brazil
E-mail: [email protected]
Received: 10 April 2002; revised: 4 July 2002; accepted: 4 September 2002.
DOI: 10.1097/01.aids.0000042595.93174.a4
ISSN 0269-9370 & 2003 Lippincott Williams & Wilkins 11

Introduction
The subtype B of HIV-1 was initially characterized indeveloped countries, such as the US and in theWestern Europe, and was considered the major variantoutside Africa and in the rest of the world. As thepandemic extended over the globe, other subtypesshowed occurrences in distinct regions. The moreefficient control and treatment of HIV infection in thedeveloped world, together with the explosion of AIDSepidemics in developing countries, has shifted majorincidences to other subtypes in these areas. In thebeginning of this new millennium, subtype C is themost prevalent in the globe, accounting for 56% of theinfections world-wide [1]. Subtype C was first detectedin South Africa and Ethiopia in retrospectively analyzedsamples of 1984 and 1986, respectively [2,3], and it hasbeen found in the majority of South African countries,such as South Africa, Botswana, Tanzania and Kenya[4–9]. Recombinant strains between subtype C andprevious subtypes prevalent in these countries were alsodocumented in Zambia [10] and Tanzania [11]. Out-side Africa, India is the largest population infected bysubtype C viruses [12], and despite its recent introduc-tion in the country [13], it is estimated that India willhave the highest number of HIV-1 infections in theworld by 2010 [14]. Finally, China also has a highprevalence of subtype C, notoriously by B/C recombi-nant genomes [15].
Brazil is the biggest South American country and it isthe most affected by the HIV/AIDS epidemics. A largenumber of individuals have already been infected, andprevalence rates are around 0.6% of the population(Brazilian Ministry of Health, http://www.aids.gov.br).Brazil has shown a constant change in its HIV-1epidemic regarding gender infection ratio and riskbehavior. Since the beginning of the epidemics, HIVinfection patterns have shifted towards women andheterosexuals.
The HIV-1 subtype distribution in Brazil is complexwhen compared with other South American countries.The major circulating subtype of HIV-1 in the countryis B, but other subtypes such as F, C and B/C and B/Frecombinants have been documented [16–20]. SubtypeC was first detected in Brazil by Csillag et al. in thecities of Porto Alegre and Sao Paulo [21]. Retro-spective samples from 1991 and 1992 were sequencedby the World Health Organization HIV Network, andthe first complete genome of a subtype C Brazilianvirus, 92BR025, was generated [22], showing that by1992 this subtype was already present in the country.More recently, another Brazilian full length C virus hasbeen sequenced [15]. Recent HIV-1 genetic diversitysurveillance studies in Brazil have shown a smallincidence of subtype C, around 3% [16,23]. Theseviruses were found in the southern and south-eastern
regions of Brazil, mostly in the states of Rio Grande doSul, Sao Paulo and Rio de Janeiro.
In Brazil, we have recently started a national networkfor drug resistance surveillance in the drug-naive popu-lation sponsored by the Brazilian Ministry of Health(BMoH), and we had the opportunity of surveying agreat number of asymptomatic, drug-naive HIV-1-infected individuals in the southern and south-easternregions of the country in 2001. Since these geographicareas are the most frequently described areas of subtypeC incidence in Brazil, we were interested in assessingthe contribution of this subtype to the overall infec-tions in the area, as well as comparing the subtype Ccirculating strains with other world-wide subtype Cisolates.
Materials and methods
SamplesPlasma from 112 HIV-1-positive individuals confirmedby serology was isolated at different voluntary counsel-ing and testing (VCT) centers of the BMoH. Thesecenters spanned five different Brazilian central-southernstates, Rio Grande do Sul, Parana, Sao Paulo, Rio deJaneiro and Mato Grosso do Sul. Table 1 summarizesall relevant epidemiological data of the individualsanalyzed, such as age, sex, state and risk behavior. Sincethe study was originally focused on maximizing inclu-sion of recently seroconverted individuals, all but twoindividuals had no symptomatic manifestations of anykind. None of these subjects has ever been exposed toany antiretroviral treatment, according to their writtenstatement. The study was approved by the BrazilianIRB (project no. 526 – CONEP) as an anonymousunlinked study.
RNA isolation, polymerase chain reaction andsequencingVirus RNA was isolated as previously described [24].Following cDNA generation with random primers,nested polymerase chain reaction (PCR) was con-ducted for individual amplification of protease (PR,whole region) and reverse transcriptase (RT, nt 105 to651). Primers used and PCR conditions used were asdescribed elsewhere [24]. PCR fragments were se-quenced in an ABI 310 automated sequencer (AppliedBiosystems, Foster City, California, USA), with thesame primers used in the second round of the amplifi-cations. All sequences obtained were subjected toquality control assessments to ensure there were nosample mix-ups or contamination from other sources[25]. Sequences were reported to the GenBank data-base (accession numbers pending). BLAST searches ofsequences from each subject identified best matches inthe HIV sequence database [26] that were always other
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
AIDS 2003, Vol 17 No 112

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Table 1. Epidemiological data of the HIV-1-infected individuals surveyed in this study.
Patient State Sex Age Risk behaviour Subtype in pol
BRBS462 SP M 32 bisexual BBRBS465 SP F 41 heterosexual BBRBS467 SP M 35 homosexual BBRBS469 SP M 48 bisexual BBRBS470 SP F 28 heterosexual BBRBS530 SP M 32 heterosexual B/UBRBS531 SP F 39 bisexual BBRBS532 SP F 22 heterosexual n/dBRBS533 SP M 30 heterosexual CBRBS534 SP F 36 heterosexual BBRBS535 SP M 39 homosexual BBRC1468 PR M 25 bisexual BBRC1472 PR M 19 bisexual BBRP2017 RS M 37 bisexual BBRP2018 RS F 27 multiple BBRP2020 RS F 20 heterosexual BBRP2022 RS F 36 heterosexual CBRP2024 RS M 23 multiple CBRP2025 RS F 23 heterosexual BBRP2026 RS M 40 multiple CBRP2027 RS F 36 heterosexual CBRP2028 RS M 22 IDU BBRP2029 RS F 24 heterosexual CBRP2030 RS M 35 heterosexual CBRP2032 RS F 47 heterosexual BBRP2033 RS M 34 IDU CBRP2034 RS F 27 multiple n/dBRP2035 RS M 23 heterosexual B/CBRP2037 RS F 21 heterosexual CBRP2038 RS M 47 homosexual BBRP2039 RS F 25 heterosexual CBRP2040 RS F 25 heterosexual C/BBRP2041 RS M 28 heterosexual B/CBRP2042 RS M 29 homosexual BBRP2043 RS M 23 heterosexual FBRP2044 RS M 38 IDU CBRP2045 RS F 15 heterosexual CBRP2046 RS F 23 heterosexual BBRP2047 RS M 31 heterosexual CBRP2049 RS F 31 heterosexual CBRP2050 RS M 39 homosexual BBRP2052 RS M 37 bisexual FBRP2053 RS F 37 heterosexual CBRP2054 RS M 45 heterosexual BBRP2055 RS M 33 heterosexual BBRP2056 RS F 34 heterosexual BBRP2057 RS M 18 homosexual CBRP2058 RS F 60 heterosexual CBRP2059 RS M 38 heterosexual BBRP2060 RS M 37 heterosexual BBRP2061 RS M 23 IDU CBRP2062 RS M 49 heterosexual BBRP2066 RS F 24 heterosexual CBRP2069 RS M 30 bisexual CBRP2070 RS F 15 heterosexual BBRP2071 RS F 22 heterosexual BBRP2072 RS F 40 heterosexual B/C/FBRP2073 RS F 39 heterosexual CBRP2076 RS F 27 heterosexual CBRP2079 RS F 31 heterosexual BBRP2080 RS F 51 heterosexual BBRP2081 RS F 35 heterosexual CBRP2083 RS M 23 IDU CBRP2084 RS M 25 IDU C/BBRP2085 RS F 33 heterosexual CBRP2086 RS F 38 heterosexual C/BBRP2087 RS M 22 heterosexual BBRP2088 RS M 25 homosexual B
(continued overleaf )
A specific subtype C Brazilian HIV-1 Soares et al. 13

sequences from Brazil. However, each sequence wasdivergent from those in the database, and amongthemselves, by more than 3%, suggesting an absence ofsample mix-ups with previously characterized se-quences.
Phylogenetic, recombination and sequenceanalysesThe PR and RT sequences from all samples weresubmitted to phylogenetic analysis for HIV-1 subtypedetermination. Sequences were aligned using CLUS-TAL W [27] and manually edited by codon alignmentusing the Genetic Data Environment (GDE) package[28]. The alignment was then realigned against thereference set for subtyping analysis from the LosAlamos database (http://hiv-web.lanl.gov/). HIV-1
group O sequences were used as outgroups. Phyloge-netic inferences were performed by the neighbor-join-ing method using the F84 model of substitutionimplemented in PAUP version 4.0b2a [29]. Sequencesfrom which both genomic regions clearly clusteredinside one of the subtype reference groups werecompiled and their respective subtypes assigned. Se-quences suggestive of recombination by the abovephylogenetic inferences that have shown unclear ordiscordant subtype classification in PR and RT weresubjected to recombination analysis. The bootscanningmethod implemented in the SIMPLOT software [30]was used. In order to increase the number of informa-tive sites, PR and RT sequence fragments from querysamples were concatenated into one larger fragmentof approximately 850 bp. The subtype reference
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Table 1. (continued ).
Patient State Sex Age Risk behaviour Subtype in pol
BRP2089 RS M 24 heterosexual CBRP2090 RS M 27 heterosexual BBRM2394 MS M 19 homosexual BBRM2395 MS M 27 heterosexual FBRM2396 MS F 24 heterosexual BBRM2397 MS M 50 heterosexual BBRM2398 MS F 35 heterosexual FBRM2399 MS M 39 heterosexual BBRM2400 MS M 24 heterosexual BBRM2401 MS n/i n/i n/i C/BBRRJ819 RJ M 44 heterosexual BBRRJ820 RJ F 44 heterosexual FBRRJ821 RJ M 27 homosexual BBRRJ822 RJ F 38 heterosexual n/dBRRJ824 RJ F 27 heterosexual FBRRJ829 RJ M 31 bisexual BBRRJ832 RJ M 28 homosexual BBRRJ837 RJ M 30 heterosexual BBRRJ838 RJ F 48 heterosexual BBRRJ839 RJ F 46 heterosexual BBRRJ842 RJ M 34 heterosexual BBRRJ845 RJ M 28 homosexual CBRRJ846 RJ n/i n/i n/i CBRRJ848 RJ M 25 heterosexual CBRRJ849 RJ M 23 homosexual BBRRJ850 RJ M 33 homosexual BBRRJ852 RJ F 35 heterosexual BBRRJ853 RJ M 31 heterosexual n/dBRRJ854 RJ M 27 heterosexual BBRRJ855 RJ M 28 homosexual CBRRJ856 RJ F 24 heterosexual FBRRJ858 RJ M 22 heterosexual n/dBRRJ860 RJ M 26 heterosexual F/UBRRJ866 RJ F 36 heterosexual BBRRJ867 RJ n/i n/i n/i BBRRJ872 RJ n/i n/i n/i BBRRJ877 RJ F 49 heterosexual BBRRJ883 RJ M 31 heterosexual n/dBRRJ884 RJ M 25 heterosexual C/BBRRJ891 RJ F 34 heterosexual n/dBRRJ892 RJ F 34 heterosexual BBRRJ893 RJ M 28 homosexual BBRRJ894 RJ M 33 homosexual B
n/i, not informed in the questionnaire; n/d, not determined; IDU, injection drug user.
AIDS 2003, Vol 17 No 114

sequences used in the analyses were representative ofthe three most prevalent subtypes circulating in Brazil,B (BUS83RF), F (F1BR93BR0201) and C (CBR92BR025). The parameters used were window ¼ 250 bp,step ¼ 20 bp, GapStrip ¼ on, Reps ¼ 100, Kimura, T/t ¼ 2, and neighbor. Based on the bootscanning sug-gested breakpoints, phylogenetic analyses were furtherperformed with fragments of the sequences that repre-sented distinct subtypes, using the same subtype refer-ence strains and methods described above.
Further phylogenetic characterization of subtype Csequences was done using maximum likelihood analy-sis. A subset of subtype C sequences, including 19sequences from our new dataset from which both PRand RT sequences were available, three previouslycharacterized Brazilian subtype C viruses, and multiplesequences from South Africa, Zimbabwe, Tanzania,Zambia, Ethiopia and Eastern India were alignedtogether using CLUSTAL W. An appropriate evolu-tionary model for these sequences was selected usingthe Akaike information criteria [31] as implemented inMODELTEST version 3.0 [32]. Parameters of thechosen method (TVM+I+G) were as follows: freqA¼ 0.3784, freqC ¼ 0.1791, freqG ¼ 0.1925, freqT ¼0.2499; R matrix values, R[A-C] ¼ 3.1987, R[A-G] ¼11.7310, R[A-T] ¼ 0.9773, R[C-G] ¼ 1.4501, R[C-T] ¼ 11.7310, R[G-T] ¼ 1.0000; proportion of invari-able sites ¼ 0.3889, and heterogeneous variable sitesdistribution gamma with alpha shape ¼ 0.6691.
Pairwise distances were calculated for different geo-graphic clusters of subtype C sequences, includingBrazilian, Indian and African groups using the Kimura2-parameter model [33] implemented in the softwareMEGA version 2.0 [34]. Both intra- and interclusterdistances were computed and compared. Amino acidsignature analysis using VESPA [35] was also performedfor each of these groups of sequences, and they werecompared to the subtype C world consensus. For thePR coding region, sequences from Zambia, Tanzaniaand South Africa (n ¼ 53) were pooled together,because they are more closely related to each other,whereas sequences from Botswana (n ¼ 8) were left asa separate group. Sequences from India (n ¼ 8), whichwere also suggested to form a monophyletic group[12], were also analyzed together. The Brazilian clusterwas represented by 22 sequences. The Brazilian subtypeB sequences generated in the study were also subjectedto VESPA analysis. All previously published sequencesand consensi used in the pairwise distance and VESPAanalyses were obtained at the Los Alamos HIV Data-base (http://hiv-web.lanl.gov).
The differential incidences of polymorphisms betweensubtypes B and C were statistically evaluated using atwo-tailed Fisher exact test implemented in the soft-ware Analyze-it1 for Microsoft Excel.
Results
Molecular epidemiology of HIV infectionOne hundred and twelve HIV-1-positive samples werecollected and processed. Protease and reverse transcrip-tase (nt 105 to 651) were separately PCR amplifiedfrom plasma through RT-PCR. Seven of the samples(6.2%) did not generate PCR fragments for eithergenomic region (protease or reverse transcriptase) andwere excluded from the analysis. All fragments obtainedwere sequenced and subjected to phylogenetic analysisfor subtype determination. In this manner we identified58 (55.2%) subtype B, 30 (28.6%) subtype C, and seven(6.7%) subtype F viruses. Ten isolates (9.5%) weresubjected to recombination analysis by bootscanningimplemented in the SIMPLOT software [30]. All 10sequences showed evidence of recombination betweentwo or more of these subtypes. A schematic representa-tion of all mosaic viruses found can be seen in Figure1. Of the 10 sequences, five have shown a pattern ofC/B recombination. Despite this large number, each ofthe recombinants showed breakpoints at different sites,and these sequences do not meet the criteria to classifythem as a circulating recombinant form. Two of thesequences showed a B/C recombination pattern, againwith different breakpoints. Interestingly, we found avirus in which three different subtypes were repre-sented in the bootscanning analysis. The B/C/F re-combinant is consistent with the three majorcirculating subtypes of HIV-1 in Brazil. Despite theprevious characterization of individuals infected withmultiple subtypes in Brazil [36,37], this is the first timea triple recombinant has been observed in the country.Finally, we found two viruses, one B and one F, inwhich part of the sequence could not be assigned toany subtype, and they were classified as undetermined(U).
Brazil has its own HIV-1 subtype C virusSince this study has generated the largest collection ofthis subtype yet in Brazil, we wanted to furtherexamine the relationships of all subtype C viruses co-circulating in the country. All Brazilian subtype Cisolates from which both PR and RT sequences wereavailable, three previously characterized Brazilian sub-type C viruses, and multiple sequences from SouthAfrica, Zimbabwe, Tanzania, Zambia, Ethiopia andEastern India were aligned together using CLUSTALW, and subjected to phylogenetic analysis using themaximum likelihood method and parameters as de-scribed in Methods. Two isolates (BRP2024 andBRP2073) were highly indicative of G!A hypermuta-tion, and were excluded from the analysis. All subtypeC sequences from Brazil, including the ones previouslydescribed, form a monophyletic cluster in the tree (Fig.2). This cluster was supported by an 82% bootstrapanalysis value. The cluster of Brazilian sequences stillremained intact when the two hypermutated isolates
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
A specific subtype C Brazilian HIV-1 Soares et al. 15

were included or when trees spanning only RTfragments, for which more subtype C isolates areavailable – see Table 1 (data not shown). Consistentwith the maximum likelihood analysis, all sequencesfrom Brazil also clustered together when analyzed byneighbor-joining analysis (data not shown). Of note,the Brazilian sequences were more tightly clusteredthan any other country’s in the tree. No sequence felloutside the cluster, such as happened for India, whichhas also been recently suggested to comprise an HIV-1subtype C monophyletic group [12].
In order to further analyze the relationships amongHIV-1 isolates of subtype C nucleotide pairwise dis-tances were calculated for each geographic cluster(Brazil, India and Africa). The results of this analysis aredepicted in Table 2. The Indian cluster had the smallestaverage distance (3.7%), followed by the Brazilian(4.5–4.6%) and the African (5.1–5.2%) clusters. Whendistances between each cluster were computed, how-ever, slightly larger values ranging from 5 to 7.5% weredocumented. These values further strengthen the geo-graphic clustering of the clade C sequences analyzed.
We next wanted to more deeply characterize theBrazilian subtype C cluster (CBR) as a distinct group.We therefore looked for specific signature amino acidsin our group of subtype C sequences that were notpresent in other subtype C viruses from around theworld. Signature analyses using VESPA [35] were
performed against the world consensus C individuallyfor PR and RT regions. CBR was represented by the22 sequences included in Figure 2. Figure 3a shows theresults of the VESPA analysis for PR. Only amino aciddifferences that appeared in more than 50% of thesequences from the world consensus C for each setwere computed and shown. None of the consensi fromAfrica had any signature differences from the worldconsensus C. On the other hand, sequences from Indiashowed three differences from the consensus, namelyan arginine at position 14 (a lysine in the consensus;50%), a valine at position 36 (an isoleucine in theconsensus; 62.5%), and a proline at position 63 (aleucine in the consensus, 62.5%). The analysis of CBR
sequences showed four significant amino acid signatureswhich are not present in the world consensus C: athreonine at position 12, a leucine at position 19, alysine at position 37, and an asparagine at position 41.These amino acid changes are highly prevalent amongCBR sequences, with incidences of 95, 85, 90 and100%, respectively, in the sequences analyzed. Ofthose, the first two changes, S12T and I19L, arecommonly observed in subtype B sequences, and infact are present in the world consensus B from LosAlamos. The change I36V, a signature of CIN and alsoprevalent in the Chinese C/B recombinant viruses(Fig. 3c), was not found in any of the CBR sequences.In the RT region analyzed, CBR (n ¼ 28) did not showany signature amino acid changes when compared tothe world consensus C. Sequences from African and
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
B
C
F
U
N/S
BRBS530
BRP2035
BRP2040
BRP2041
BRP2072
BRP2084
BRP2086
BRM2401
BRRJ860
BRRJ884
PR RT
Fig. 1. Schematic drawing showing the breakpoint pattern of the 10 mosaic viruses found in the study. The blank square afterthe protease coding region represents the RT region not sequenced in the study. Each shade represents a subtype. U,undetermined; N/S, not sequenced.
AIDS 2003, Vol 17 No 116
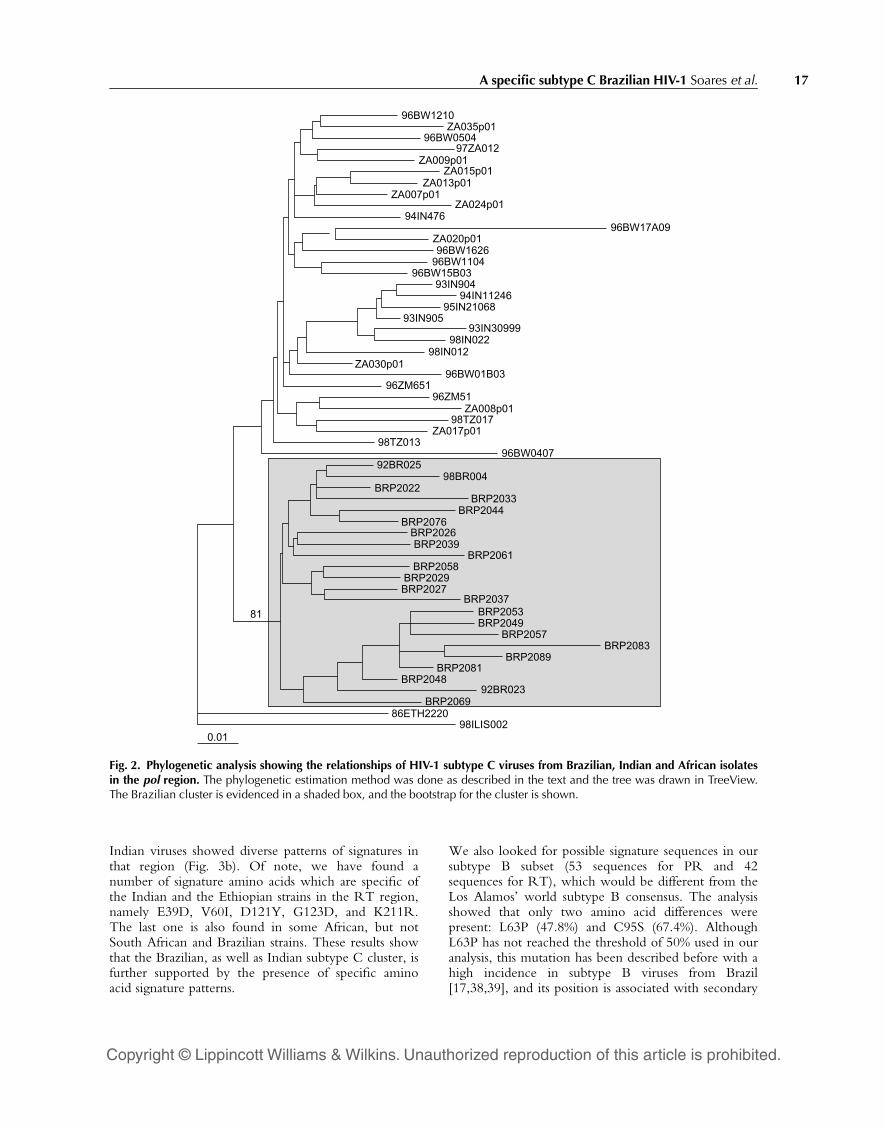
Indian viruses showed diverse patterns of signatures inthat region (Fig. 3b). Of note, we have found anumber of signature amino acids which are specific ofthe Indian and the Ethiopian strains in the RT region,namely E39D, V60I, D121Y, G123D, and K211R.The last one is also found in some African, but notSouth African and Brazilian strains. These results showthat the Brazilian, as well as Indian subtype C cluster, isfurther supported by the presence of specific aminoacid signature patterns.
We also looked for possible signature sequences in oursubtype B subset (53 sequences for PR and 42sequences for RT), which would be different from theLos Alamos’ world subtype B consensus. The analysisshowed that only two amino acid differences werepresent: L63P (47.8%) and C95S (67.4%). AlthoughL63P has not reached the threshold of 50% used in ouranalysis, this mutation has been described before with ahigh incidence in subtype B viruses from Brazil[17,38,39], and its position is associated with secondary
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
96BW1210ZA035p01
96BW050497ZA012
ZA009p01ZA015p01
ZA013p01ZA007p01
ZA024p01
ZA020p01
94IN47696BW17A09
96BW162696BW1104
96BW15B0393IN904
94IN1124695IN21068
93IN90593IN30999
98IN02298IN012
ZA030p0196BW01B03
96ZM65196ZM51
ZA008p0198TZ017
ZA017p0198TZ013
96BW040792BR025
98BR004BRP2022
BRP2033BRP2044
BRP2076BRP2026BRP2039
BRP2061BRP2058
BRP2029BRP2027
BRP2037BRP2053BRP2049
BRP2057BRP2083
BRP2089BRP2081
BRP204892BR023
BRP206986ETH2220
98ILIS0020.01
81
Fig. 2. Phylogenetic analysis showing the relationships of HIV-1 subtype C viruses from Brazilian, Indian and African isolatesin the pol region. The phylogenetic estimation method was done as described in the text and the tree was drawn in TreeView.The Brazilian cluster is evidenced in a shaded box, and the bootstrap for the cluster is shown.
A specific subtype C Brazilian HIV-1 Soares et al. 17

drug resistance. The biological significance of the C95Schange is unknown. As for subtype CBR, no specificsignature patterns of subtype BBR were observed in theRT region (Fig. 3b).
When PR sequences representing these two subtypeswere analyzed separately, we observed differentialfrequencies of mutations in a number of secondaryresidues associated with protease inhibitor resistance.Notably, the mutations M36I and L63P/H/A/T hadsignificant differences. The M36I mutation had inci-dences of 24.5% (13 of 53) and 68.2% (15 of 22) forsubtypes B and C, respectively (P ¼ 0.001). Similarly,L63P/H/A/T had incidences of 52.8% (28 of 53) and13.6% (3 of 22) for subtypes B and C (P ¼ 0.003). Incontrast to that, the mutation L10I/V, which waspresent in 24.5% (13 of 53) of the subtype B sequencesand in 36.4% (8 of 22) of the subtype C sequences, aswell as the mutation K20R, with an incidence of 5.7%(3 of 53) in B sequences, and of 9.1% (2 of 22) in Csequences, had no significant subtype-specific differ-ences (P ¼ 0.445 and 0.921, respectively).
Recombinant viruses are composed of genuineBrazilian subtypesSince we had observed specific signature patters inBrazilian HIV-1 subtype C and B sequences, wewanted to see if the recombinant forms we havedescribed had been generated by truly local parentalviruses. To accomplish that, we looked for the CBR
and BBR signature amino acids in our B/C and C/Brecombinants. The results of this analysis for theprotease region are shown in Figure 3. The reversetranscriptase region was not subjected to analysis sinceno specific Brazilian signatures were found in it (seeabove). Brazilian B/C viruses (labeled BR.BC in theFig. 3c) retain the signature pattern of BBR in theirsubtype B portions, such as L63P and C95S in the PRregion. Similarly, the C/B recombinant viruses showedspecific CBR signatures in their subtype C-derivedsequences, such as N37K and K41N in the PR region.These results strongly suggest that the recombinant
forms observed in our study were generated locally byrecombination events of subtypes B and C parentalstrains, and do not represent introductions by migrationof external recombinant viruses.
Discussion
In this study, a large proportion of HIV-1 subtype C inthe south of Brazil was observed. Previous surveys inBrazil have shown frequencies of around 3% forsubtype C viruses in the country [16,23]. In this newdataset, we have found that almost 30% of the virusescirculating in south and south-eastern Brazil are ofsubtype C. In fact, the local incidence of this subtypein the city of Porto Alegre, RS, where it was firstdetected, reaches remarkable 37% of the viruses, andcan increase to 44% when the recombinant virusescontaining subtype C-related sequences are considered.Although there are no previous reports of subtype Cincidence in the south of Brazil, an analysis of AIDSpatients in Porto Alegre in 2001 using env HMA hasshown a frequency of 22% for HIV-1 subtype C-infected individuals (A.M.B. Martinez, personalcomm.). Despite our analysis has been based on the polregion, we could speculate an increase in the preva-lence of C subtype in that city.
We have shown evidence that subtype C HIV-1viruses from Brazil form a monophyletic group whencompared with other viruses of the same subtype fromaround the world, suggesting that subtype C hasentered the country as a single introduction, or at leastas a very small group of genetically related viruses.Alternatively, a more rapid spread of this subtypethroughout susceptible individuals, when comparedwith the subtype B counterparts that co-circulate in thecountry, could also explain the tighter relatedness ofsubtype C Brazilian viruses. The intra-clade geneticdiversity of CBR also supported the observed clusteringof the sequences (Table 2). The Brazilian clustershowed an intermediary mean genetic divergence(4.5%) when compared with the Indian and Africansubtype C sequences (3.7 and 5.0%, respectively).Inter-cluster distances were higher, ranging from 5 to7.5%, showing that viruses within each group are moregenetically related to each other than to viruses fromother groups.
The high incidence of subtype C HIV-1 viruses in thesouth and south-eastern part of the country, a regionwith equally high incidences of subtype B viruses, hasenabled a high number of recombination events be-tween viruses from these two subtypes. This is demon-strated by a large number of B/C and C/Brecombinants seen among the mosaic viruses analyzedin our dataset. Eight out of 10 recombinant viruses
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Table 2. Genetic diversity of different geographic clusters of sub-type C HIV-1.
Protease n Brazilian Indian African
Brazilian 22 4.5%.7.5% 6.8%Indian 8 3.7% 5.3%African 26 5.1%
Reverse transcriptase n Brazilian Indian African
Brazilian 22 4.6% 5.7% 6.1%Indian 8 3.7% 5.0%African 26 5.2%
Values represent averages of protease and reverse transcriptase DNApairwise distances inside each group of sequences (intra-group) andamong them (inter-group).
AIDS 2003, Vol 17 No 118

showed subtype B- and C-related sequences in theirgenomes. We cannot completely exclude the possibilitythat PR and RT sequences were amplified from twodifferent viruses co-infecting an individual. However,as the methods we have used amplify the predominantstrain of the individual, strains of different subtypeswould have to be present in approximately equalamounts in order to explain the obtained results. As theraw sequence data obtained were clear and unambig-uous, we believe that the majority of the describedstrains are likely to represent true mosaic viruses. Theabsence of a defined prevailing CRF suggests that these
recombination events are recent and probably an on-going process in Brazil. The recombinant viruses seemto have been generated locally, and not imported fromanother country, as shown by the presence of CBR andBBR signatures in their sequences (Fig. 3c).
We have shown that subtype CBR has its own signaturepatterns which are not seen in any other subtype Cgroup, as we could determine by VESPA analysis. Thoseincluded the changes S12T, I19L, N37K and R41N ofthe protease amino acid sequence. Velazquez-Campoyet al. [40] have recently reported specific amino acid
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
ConsensusCZM_TZ_ZA.CBW.CIN.CBR.C
PQITLWQRPLVSIKVGGQIKEALLDTGADDTVLEEINLPCKWKPKMIGGIGGFIKVRQYDQILIEICGKKAIGTVLVGPTPVNIIGRNMLTQLGCTLNF...................................................................................................................................................................................................................R.....................V..........................P...............................................T......L.................K...N..........................................................
..............................................................P...............................S....
PQITLWQRPLVTIKIGGQLKEALLDTGADDTVLEEMNLPGRWKPKMIGGIGGFIKVRQYDQILIEICGHKAIGTVLVGPTPVNIIGRNLLTQIGCTLNF
PROTEASE
(a)
ConsensusCConsensusCBRBR.BCBR.CBCN.CB
ConsensusBConsensusBBRBR.BCBR.CBCN.CB
PQITLWQRPLVSIKVGGQIKEALLDTGADDTVLEEINLPGKWKPKMIGGIGGFIKVRQYDQILIEICGKKAIGTVLVGPTPVNIIGRNMLTQLGCTLNF...........T......L.................K...N.....................................................................T..I...L................M....R.....................P...............................S...............T......L.................K...N.....................................................................T......L...............DV.......................E..P....................................
PQITLWQRPLVTIKIGGQLKEALLDTGADDTVLEEMNLPGRWKPKMIGGIGGFIKVRQYDQILIEICGHKAIGTVLVGPTPVNIIGRNLLTQIGCTLNF..............................................................P...............................S..................................................................P.....K...................M...L.S..................V....................IK...N...........................K.......................L....................V...................DV....K..................E..P.....K...................M...L......
PROTEASE
(c)
ConsensusBBR.B
ConsensusCZM_TZ_ZA.CZA.CET.CIN.CBR.C
ConsensusBBR.B
PISPIETVPVKLKPGMDGPKVKQWPLTEEKIKALTAICEEMEKEGKITKIGPENPYNTPVFAIKKKDSTKWRKLVDFRELNKRTQDFWEVQLGIPHPAGLKKKKSVTVLDVGDAYF...................R..........................................................................................................................................................................................................................................................D....................I..............................................................................................D....................I........................................................***********************************.................................................................................
SVPLDEGFRKYTAFTIPSINNETPGIRYQYNVLPQGWKGSPAIFQSSMTKILEPFRAQNPEIVIYQYMDDLYVGSDLEIGQHRAKIEELREHLLKWGFTTP..................T.....................................T.....................................R...............................................................................................................Y.D.......................................................................................R..........Y.D.......................................................................................R...........................................................................................................
***********************************.................................................................................PISPIETVPVKLKPGMDGPKVKQWPLTEEKIKALVEICTEMEKEGKISKIGPENPYNTPVFAIKKKDSTKWRKLVDFRELNKRTQDFWEVQLGIPHPAGLKKKKSVTVLDVGDAYF
.....................................................................................................
SVPLDKDFRKYTAFTIPSINNETPGIRYQYNVLPQGWKGSPAIFQSSMTKILEPFRKQNPDIVIYQYMDDLYVGSDLEIGQHRTKIEELRQHLLRWGFTTP
REVERSE TRANSCRIPTASE
(b)
ConsensusCZM_TZ_ZA.CZA.CET.CIN.CBR.C
ConsensusB
BR.B
Fig. 3. VESPA analyses of protease and reverse transcriptase consensus sequences from HIV-1 isolates from Brazil, India andAfrica, showing signature sequences for each of these groups. (a), protease consensus of subtype C sequences for each groupwere compared to the Los Alamos world consensus C sequence. Brazilian viruses of subtype B were also compared to the worldconsensus B. (b), same as in (a), but for the reverse transcriptase sequences. (c), Brazilian recombinant viruses (BR.BC andBR.CB) showed amino acid signatures of Brazilian subtypes in their respective regions. No comparisons were made in the RTregion, since Brazilian viruses of subtypes B and C do not show any specific signature sequence which differ them from theworld consensi. Signatures present in less than 50% of the samples are not shown, with the exception of L63P in the protease ofBR.B (47.5%).
A specific subtype C Brazilian HIV-1 Soares et al. 19

differences between HIV-1 proteases of subtypes A, Cand B that account for a higher vitality of the first twoenzymes when compared with the third one in in vitroassays. These changes were M36I, R41K, H69K andL89M in subtype C PR, and I13V, E35D and R57Ktogether with the previous four changes in subtype APR. Moreover, these amino acid changes also makeHIV-1 proteases more resistant to most of the commer-cially available protease inhibitors, such as indinavir,ritonavir, saquinavir and nelfinavir [40]. Our subtypeCBR contains three out the four substitutions reportedfor subtype C PR, but it lacks R41K. It shows insteadan R41N mutation, which is in fact one of the CBR
signatures. Although this change is not as conservativeas R41K, the effect of that mutation in the vitality ofsubtype C protease is not known. In addition, themutation N37K, which is represented in 91% ofBrazilian subtype C sequences and is not associated toany specific phenotype, remains to be determined.When we analyzed our new subtype B sequences, wealso found that positions E35, N37 and R41 aresubjected to a very high degree of amino acid variation(data not shown). Although they did not meet ourthreshold of 50% to be included as subtype B signa-tures, they had percentages of variation ranging from30 to 43%. The position E35 had changed to D andthe position R41 had changed to K both in 94% of theisolates where variation was detected. In interpretingthese data, we could envisage a scenario in whichproteases from viruses circulating in drug-naive sub-jects, independent of their subtype, could incorporateamino acid changes that enable them to evolve into ahigher fitness state, with a higher catalytic efficiency.However, experimental evidence to support this hy-pothesis remains to be demonstrated. Additionally, anumber of secondary residues associated with proteaseinhibitor drug resistance such as M36I and L63P/H/A/T were clearly associated with different subtype, repre-senting signature sequences of subtypes C and B,respectively. Although experimental evidences of theimpact of these substitutions in subtype C viruses onresistance and clinical outcome are largely unknown,we could speculate that these mutations may decreasetheir genetic barrier to resistance acquisition.
The study of HIV-1 genetic variability in distinctregions of the globe is of pivotal importance in thedesign of more efficient, customized HIV vaccineswhich must include locally circulating subtypes. De-spite the recent report pointing out the elevatedincidence of subtypes B and F, and the existence of B/F CRFs in South America [41], a major concernprovided by our study is the high, and perhaps increas-ing, prevalence of subtype C in Brazil. Moreover,differences in vitality and fitness of subtype C viralproteases, and their relative in vitro resistance tocommercially available and widely used PIs when com-pared to subtype B, should be of special concern to
clinicians and epidemiologists. The differential poly-morphisms between PR and RT of clades C and Bassociated with drug resistance justify the setting up ofclinical trials comparing efficiencies of antiretroviraldrug treatment and vaccine intervention in which thesetwo subtypes circulate.
Acknowledgements
We would like to thank all participants of the BrazilianNetwork for Drug Resistance Surveillance (HIV-BResNet) who contributed to this study.
Sponsorship: this work was supported by the AIDS/STDNational Program, Brazilian Ministry of Health, the StateScience Foundation of Rio de Janeiro Grant E-26/151.970/00, the Brazilian Council for Scientific andTechnologic Development Grant 462394/00-0, andWellcome Trust Grant 061238/Z/00/Z.
References
1. Esparza J, Bhamarapravati N. Accelerating the development andfuture availability of HIV-1 vaccines: Why, when, where, andhow? Lancet 2000; 355:2061–2066.
2. Johansson B, Sherefa K, Sonnerborg A. Multiple enhancer motifsin HIV type 1 strains from Ethiopia. AIDS Res Hum Retrovir1995; 11:761–764.
3. Zacharova V, Becker ML, Zachar V, Ebbesen P, Goustin AS. DNAsequence analysis of the long terminal repeat of the C subtypeof human immunodeficiency virus type 1 from Southern Africareveals a dichotomy between B subtype and African subtypes onthe basis of upstream NF-IL6 motif. AIDS Res Hum Retrovir1997; 13:719–724.
4, Novitsky VA, Montano MA, McLane MF, Renjifo B, Vannberg F,Foley BT, et al. Molecular cloning and phylogenetic analysis ofhuman immunodeficiency virus type I subtype C: a set of 23full-length clones from Botswana. J Virol 1999; 73:4427–4432.
5. Renjifo B, Chaplin B, Mwakagile M, Shah P, Vamberg F,Msamanga G, et al. Epidemic expansion of HIV type 1 subtypeC and recombinant genotypes in Tanzania. AIDS Res HumRetrovir 1998; 14:635–638.
6. van Harmelen JH, Wood R, Lambrick M, Rybicki EP, WilliamsonAL, Williamson C. An association between HIV-1 subtypes andmode of transmission in Cape Town, South Africa. AIDS 1997;11:81–87.
7. van Harmelen JH, Van der Ryst E, Loubser AS, York D, MaduraiS, Lyons S, et al. A predominantly HIV-1 subtype C-restrictedepidemic in South African urban populations. AIDS Res HumRetrovir 1999; 15:395–398.
8. Neilson JR, John GC, Carr JK, Lewis P, Kreiss JK, Jackson S, et al.Subtypes of human immunodeficiency virus type 1 and diseasestage among women in Nairobi, Kenya. J Virol 1999; 73:4393–4403.
9. Robbins KE, Kostrikis LG, Brown TM, Anzala O, Shin S, PlummerFA, et al. Genetic analysis of human immunodeficiency virustype 1 strains in Kenya: a comparison using phylogenetic analy-sis and a combinatorial melting assay. AIDS Res Hum Retrovir1999; 15:329–335.
10. Salminen MO, Carr JK, Roberston DL, Hegerich P, Gotte D, KochC, et al. Evolution and probable transmission of intersubtyperecombinant human immunodeficiency virus type 1 in a Zam-bian couple. J Virol 1997; 71:2647–2655.
11. Koulinska IN, Ndung’u T, Mwakagile D, Masamanga G, KagomaC, Fawzi W, et al. A new human immunodeficiency virus type 1circulating recombinant form from Tanzania. AIDS Res HumRetrovir 2001; 17:423–431.
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
AIDS 2003, Vol 17 No 120

12. Shankarappa R, Chatterjee R, Learn GH, Neogi D, Ding M, RoyP, et al. Human immunodeficiency virus type 1 env sequencesfrom Calcutta in Estearn India: identification of features thatdistinguish subtype C sequences in India from other subtype Csequences. J Virol 2001; 75:10479–10487.
13. Delwart EL, Shpaer EG, McCutchan FE, Louwagie J, Grez M,Rubsamen-Waigmann H, et al. Genetic relationships determinedby a DNA heretroduplex mobility assay: analysis of HIV-1 envgenes. Science 1993; 292:1257–1261.
14. Bollinger RC, Tripathy SP, Quinn TC. The human immuno-deficiency virus epidemic in India: current magnitude and futureprojections. Medicine (Baltimore) 1995; 74:97–106.
15. Rodenburg CM, Li Y, Trask SA, Chen Y, Decker J, Robertson DL,et al. Near full-length clones and reference sequences forsubtype C isolates of HIV type 1 from three different continents.AIDS Res Hum Retrovir 2001; 17:161–168.
16. Bongertz V, Bou-Habib DC, Brigido LF, Caseiro M, Chequer PJ,Couto-Fernandez JC, et al. HIV-1 diversity in Brazil: genetic,biologic, and immunologic characterization of HIV-1 strains inthree potential HIV vaccine evaluation sites. J Acquir ImmuneDefic Syndr 2000; 23:184–193.
17. Caride E, Brindeiro R, Hertogs K, Larder B, Dehertogh P,Machado E, et al. Drug-resistance reverse transcriptase genotyp-ing and phenotyping of B and non-B subtypes (F and A) ofhuman immunodeficiency virus type 1 found in Brazilian pa-tients failing HAART. Virology 2000; 275:107–115.
18. Cornelissen M, Kampinga G, Zorgdrager F, GousmitJ, UnaidsNetwork for HIV Isolation and Characterization. Humanimmunodeficiency virus type 1 subtypes defined by env showhigh frequency of recombinant gag genes. J Virol 1996;70:8209–8212.
19. Couto-Fernandez JC, Morgado MG, Bongertz V, Tanuri A,Andrade T, Brites C, et al. HIV-1 subtyping in Salvador, Bahia,Brazil: a city with African sociodemographic characteristics. JAcquir Immune Defic Syndr 1999; 22:288-293.
20. Sabino EC, Shpaer EG, Morgado MG, Korber BT, Diaz RS,Bongertz V, et al. Identification of human immunodeficiencyvirus type 1 envelope genes recombinant between subtypes Band F in two epidemiologically linked individuals from Brazil. JVirol 1994; 68:6340–6346.
21. Csillag C. HIV-1 subtype C in Brazil. Lancet 1994; 344:1354.22. Gao F, Robertson DL, Carruthers CD, Morrison SG, Jian B, Chen
Y, et al. A comprehensive panel of near full-length clones andreference sequences for non-subtype B isolates of humanimmunodeficiency virus type 1. J Virol 1998; 72:5680–5698.
23. Brindeiro R, Vanderborght B, Caride E, Correa L, Oravec RM,Berro O, et al. Sequence diversity of the reverse transcriptase ofhuman immunodeficiency virus type 1 from Brazilian untreatedindividuals. Antimicrob Agents Chemother 1999; 43:1674–1680.
24. Stuyver L, Wyseur A, Rombout A, Louwagie J, Scarcez T,Verhofstede C, et al. Line probe assay for rapid detection ofdurg-selected mutations in the human immunodeficiency virustype 1 reverse transcriptase gene. Antimicrob Agents Chemother1997; 41:284–291.
25. Korber BT, Learn G, Mullins JI, Hahn BH, Wolinsky S. ProtectingHIV databases. Nature 1995; 378:242–244.
26. Gaschen B, Kuiken C, Korber B, Foley F. Retrieval and on-the-flyalignment of sequence fragments from the HIV database.Bioinformatics 2001; 17:415–418.
27. Thompson JD, Higgins DG, Gibson TJ. CLUSTAL W: improvingthe sensitivity of progressive multiple sequence alignmentthrough sequence weighting, position-specific gap penalties andweight matrix choice. Nucl Acids Res 1994; 22:4673–4680.
28. Smith SW, Overbeek CR, Woese W, Gilbert W, Gillevet PM. TheGenetic Data Environment: An expandable GUI for multiplesequence analysis. Comput Appli Biosci 1994; 10:671–675.
29. Swofford D. PAUP 4.0: Phylogenetic analysis using parsimony(and other methods), 4.0b2a. Sunderland, MA, USA: SinauerAssociates, Inc.; 1999.
30. Salminen MO, Carr JK, Burke DS, McCutchan FE. Identification
of breakpoints in intergenotypic recombinants of HIV type 1 bybootscanning. AIDS Res Hum Retrovir 1995; 11:1423–1425.
31. Akaike H. A new look at statistical model identification. IEEETrans Automatic Control 1974; 19:716–723.37.
32. Posada D, Crandall KA. MODELTEST: testing the model of DNAsubstitution. Bioinformatics 1998; 14:817–818.
33. Kimura M. A simple method for estimating evolutionary rates ofbase substitution through comparative studies of nucleotidesequences. J Mol Evol 1980; 16:111–120.
34. Kumar S, Tamura K, Jakobsen IB, Nei M. MEGA2: MolecularEvolutionary Genetics Analysis software, Bioinformatics 2001;17:1244–1245.
35. Korber B, Myers G. Signature pattern analysis: a method forassessing viral sequence relatedness. AIDS Res Hum Retrovir1992; 8:1549–1560.
36. Janini LM, Pieniazek D, Peralta JM, Schechter M, Tanuri A,Vicente AC, et al. Identification of single and dual infectionswith distinct subtypes of human immunodeficiency virus type 1using restriction fragment length polymorphism analysis. VirusGenes 1996; 13:69–81.
37. Janini LM, Tanuri A, Schechter M, Peralta JM, Vicente AC, De LaTorre N, et al. Horizontal and vertical transmission of humanimmunodeficiency virus type 1 dual infections caused by virusesof subtypes B and C. J Infect Dis 1998; 177:227–231.
38. Dumans AT, Soares MA, Pieniazek D, Kalish M, De Vroey V,Hertogs K, et al. Prevalence of protease and reverse transcriptasedrug resistance mutations over time in drug-naıve HIV-1-positiveindividuals in Rio de Janeiro, Brazil. Antimicrob Agents Che-mother (submitted).
39. Pieniazek D, Rayfield M, Hu DJ, Knengasong J, Wiktor SZ,Downing R, et al. Protease sequences from HIV-1 group Msubtypes A-H reveal distinct amino acid mutation patternsassociated with protease resistance in protease inhibitor-naıveindividuals worldwide. HIV Variant Working Group. AIDS 2000;14:1489–1495.
40. Velazquez-Campoy A, Todd MJ, Vega S, Freire E. Catalyticefficiency and vitality of HIV-1 proteases from African viralsubtypes. Proc Natl Acad Sci 2001; 98:6062–6067.
41. Carr JK, Avila M, Carrillo MG, Salomon H, Hierholzer J,Watanaveeradej V, et al. Diverse BF recombinants have spreadwidely since introduction of HIV-1 into South America. AIDS2001; 15:F41–F47.
Appendix
Participants in the Brazilian Network for DrugResistance SurveillanceA. Tanuri, M. Soares, R. Brindeiro, M. Arruda, and E.Soares (UFRJ, Rio de Janeiro); E. Caride (IOC,FIOCRUZ), C. Lauria (Hospital Pedro Ernesto,UERJ, Rio de Janeiro), F. Esperanza, S. Ishii, F.Oliveira, and I. Pires (IBEX, Rio de Janeiro); M.Morgado, J. Fernandez, S. Fernandez (FIOCRUZ,Rio de Janeiro); R. Diaz, L. Costa and E. Cavalieri(EPM/UNIFESP, Sao Paulo); E. Sabino, N. GaburoJr., and A. Shoko (Fundacao Pro-Sangue, Sao Paulo);R. Rodrigues, L. Brigido, and R. Custodio (InstitutoAdolfo Lutz, Sao Paulo), M. Dantas, D. Barreira andP. Teixeira (CN/DST-AIDS, Brasılia).
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
A specific subtype C Brazilian HIV-1 Soares et al. 21
Related Documents











