A review of computer and Internet-based interventions for smoking behavior Scott T. Walters a, T , Jo Anne Wright b , Ross Shegog c a University of Texas School of Public Health, 5323 Harry Hines Blvd, V8.112, Dallas, TX 75390-9128, United States b University of Michigan, United States c Center for Health Promotion and Prevention Research, University of Texas School of Public Health, Texas Medical Center, Houston, United States Abstract This article reviews studies of computer and Internet-based interventions for smoking behavior, published between 1995 and August 2004. Following electronic and manual searches of the literature, 19 studies were identified that used automated systems for smoking prevention or cessation, and measured outcomes related to smoking behavior. Studies varied widely in methodology, intervention delivery, participant characteristics, follow-up period, and measurement of cessation. Of eligible studies, nine (47%) reported statistically significant or improved outcomes at the longest follow-up, relative to a comparison group. Few patterns emerged in terms of subject, design or intervention characteristics that led to positive outcomes. The bfirst generationQ format, where participants were mailed computer-generated feedback reports, was the modal intervention format and the one most consistently associated with improved outcomes. Future studies will need to identify whether certain patients are more likely to benefit from such interventions, and which pharmacological and behavioral adjuncts can best promote cessation. D 2005 Elsevier Ltd. All rights reserved. Keywords: Smoking; Cessation; Computer; Internet; Intervention 1. Introduction The recent Institute of Medicine (2001) report paints a picture of an outdated healthcare system in need of innovative and cost-saving methods for improving health outcomes. In this process, smoking 0306-4603/$ - see front matter D 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.addbeh.2005.05.002 T Corresponding author. Tel.: +1 214 648 1519; fax: +1 214 648 1081. E-mail address: [email protected] (S.T. Walters). Addictive Behaviors 31 (2006) 264 – 277

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Addictive Behaviors 31 (2006) 264–277
A review of computer and Internet-based interventions for
smoking behavior
Scott T. Waltersa,T, Jo Anne Wrightb, Ross Shegogc
aUniversity of Texas School of Public Health, 5323 Harry Hines Blvd, V8.112, Dallas, TX 75390-9128, United StatesbUniversity of Michigan, United States
cCenter for Health Promotion and Prevention Research, University of Texas School of Public Health,
Texas Medical Center, Houston, United States
Abstract
This article reviews studies of computer and Internet-based interventions for smoking behavior, published
between 1995 and August 2004. Following electronic and manual searches of the literature, 19 studies were
identified that used automated systems for smoking prevention or cessation, and measured outcomes related to
smoking behavior. Studies varied widely in methodology, intervention delivery, participant characteristics, follow-up
period, and measurement of cessation. Of eligible studies, nine (47%) reported statistically significant or improved
outcomes at the longest follow-up, relative to a comparison group. Few patterns emerged in terms of subject, design
or intervention characteristics that led to positive outcomes. The bfirst generationQ format, where participants were
mailed computer-generated feedback reports, was the modal intervention format and the one most consistently
associated with improved outcomes. Future studies will need to identify whether certain patients are more likely to
benefit from such interventions, and which pharmacological and behavioral adjuncts can best promote cessation.
D 2005 Elsevier Ltd. All rights reserved.
Keywords: Smoking; Cessation; Computer; Internet; Intervention
1. Introduction
The recent Institute of Medicine (2001) report paints a picture of an outdated healthcare system in
need of innovative and cost-saving methods for improving health outcomes. In this process, smoking
0306-4603/$ -
doi:10.1016/j.a
T Correspond
E-mail add
see front matter D 2005 Elsevier Ltd. All rights reserved.
ddbeh.2005.05.002
ing author. Tel.: +1 214 648 1519; fax: +1 214 648 1081.
ress: [email protected] (S.T. Walters).
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 265
cessation programs will undoubtedly play a large role. Cigarette smoking is the leading cause of
premature morbidity and mortality in the United States, and is responsible for nearly half a million
deaths each year (Centers for Disease Control and Prevention, 2002, 2003). Unfortunately, the U.S.
Preventive Services Task Force has described tobacco cessation as one of the highest priority services
with the lowest delivery rate (Coffield et al., 2001). Indeed, taking into account the number of current
smokers and the number of people who start smoking each year, public health efforts are currently
making very little headway in reducing the total number of smokers.
Among current smokers, an estimated 41% reported that they had stopped smoking for at least one
day in the previous year because they were trying to quit (Centers for Disease Control and Prevention,
2004). However, rates of long-term cessation are significantly lower (U.S. Department of Health and
Human Services, 2000b). Smoking cessation interventions, particularly those that combine behavioral
and pharmacological methods, can produce rates well above the rates of smokers choosing to quit on
their own (U.S. Department of Health and Human Services, 2000b), but these intensive programs also
have the lowest rates of participation. For instance, free clinical interventions offered by health
maintenance organizations (HMOs) may only enroll only about 1% of eligible persons (Lichtenstein &
Hollis, 1992). Less intensive interventions, such as physician advice and self-help materials, may reach
more eligible persons, but they typically result in lower cessation rates (Lancaster & Stead, 2004; Silagy
& Stead, 2004).
Healthy People 2010 established a goal of reducing the rates of adult smoking from 23.3% to 12%
by the year 2010 (U.S. Department of Health and Human Services, 2000a). If this is to be
accomplished, there will be an increased need for interventions that can be disseminated to larger
numbers of smokers at a relatively low cost. In moving toward this goal, one trend is toward
interventions that can be delivered via mail, computer and the Internet. These new modes of delivery
may be well suited for tailoring self-help materials to the individual, a strategy that is generally more
effective than no intervention (Lancaster & Stead, 2004). In a typical format, smokers are surveyed via
a computerized or paper assessment, and the results are tailored to some characteristic of the individual,
such as gender, dependence level, perceived barriers to quitting, or stage of change. Based on a
theoretical model of motivation and change (e.g., Transtheoretical Model; Prochaska, Norcross, &
DiClemente, 1994), the algorithm library generates instructions for each possible survey response. The
resultant feedback, information or advice is then presented on a computer screen or through printed
materials. Indeed, this format has been widely utilized in health behavior areas such as nutrition
education, weight loss, diabetes management, alcohol consumption, HIV risk reduction, and cancer
support and counseling (e.g., Bessell et al., 2002; Brug, Steenhuis, van Assema, & de Vries, 1996;
Cloud, & Peacock, 2001; Firby, Luker, & Caress, 1991; Green & Fost, 1997; Hester, & Delaney, 1997;
Kumar, Bostow, Schapira, & Kritch, 1993; Paperny, 1997; Tate, Jackvony, & Wing 2003; Tate, Wing,
& Winett, 2001).
2. Rationale for the present review
In an earlier review of ten randomized trials of computer-tailored smoking materials, Strecher (1999)
found a significant impact in a majority of studies. Though few patterns emerged, the computer-tailored
materials seemed to be more effective for those in the precontemplation stage of change. Studies that
combined tailored materials with other behavioral or pharmacological interventions also showed
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277266
promise. At the time of the Strecher (1999) review, however, computer interventions for smoking were
nearly all limited to using the computer to generate printed feedback, which was then mailed to the
recipient. However, in recent years, a few intervention trials have begun to test more sophisticated
methods. Studies now describe multiple iterations of feedback, specific advice or a tailored plan for
quitting, computer generated e-mail reminders, or other multimedia experiences. Such aspects are
particularly apparent in computer programs targeted at youth, some of which incorporate Flash
technology, interactive responses, chat rooms, or video streaming. As discussed below, these newer
interventions are noteworthy both because of their sophisticated presentation (i.e., they look and feel
different), as well as their ability to customize the intervention ipsitively based on the user’s responses to
the program (i.e., they ask questions and respond to the user). By soliciting information and allowing the
program to respond with visual or audible responses, a computer can better mimic the transactional
qualities of human communication (Cassell, Jackson, & Cheuvront, 1998). Such interventions are also
thought to be more persuasive than static text. That is, if the receiver feels there is a bgive and takeQ inthe transaction, they will be more likely to attend to the message, comprehend the argument, and
consider the position (O’Keefe, 1990). The possibilities for tailoring smoking interventions using
interactive computer programs are vast, but the development costs can be high (Science Panel on
Interactive Communication and Health, 1999). These costs may be justified if the program impacts
populations as effectively as other programs or reaches populations which have typically been resistant
to other kinds of interventions. For these reasons, the present study was undertaken to update the
Strecher (1999) review. We were interested in smoking prevention or intervention programs that used the
computer or Internet to calculate or deliver the intervention. Because our intent was to examine the range
of applications under which the automated systems are being used, we chose to examine both adult
cessation and adolescent prevention studies. Although conceptually different, we hoped that one area
might inform the efforts of the other.
3. Methods
3.1. Search strategy
Medline, CINAHL, and PsycInfo databases were used to locate English-language studies published
between 1995 and August 2004. The bibliographies of retrieved articles were scanned for additional
references. Key search terms included (computer or Internet or web) and (behavior change or
intervention or treatment or therapy) and (smoking or tobacco). The search terms were intentionally
broad to ensure, as much as possible, that all relevant articles would be captured.
3.2. Inclusion criteria
Review criteria included English-language peer-reviewed journal articles published since 1995 that
described intervention trials for smoking prevention or cessation that:
1. Used computers (web-based, server-based, or stand-alone programs) as a significant part of the
intervention.
2. Included at least one comparison or control condition.
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 267
3. Included at least one intervention condition that was achieved without significant human contact. This
eliminated interventions that involved non-automated e-mail, chat rooms, discussion boards, or direct
personal contact as the primary delivery mode.
4. Reported at least one outcome directly related to smoking behavior.
Abstracts of journal articles were examined independently by two reviewers using the above criteria
to determine relevance. In cases where multiple outcomes were reported from a single intervention trial,
we selected the most recent (or longest) follow up available.
3.3. Data synthesis
A qualitative analysis was undertaken due to the significant heterogeneity between studies in terms of
subject characteristics, intervention delivery, and outcome measure. Comparisons between studies were
made on the basis of continuous (i.e., no smoking from baseline to follow-up) or point abstinence (e.g., no
smoking for a period of time prior to follow-up) rates, which wewere able to derive frommost studies. This
provided the most useful basis for comparison as the studies differed markedly on most other attributes.
4. Results
Literature searches yielded 199 unique references that met our search criteria. After reviewing articles
for relevance, 19 were retained for this review. Four studies were focused on adolescent smoking
prevention, while 15 targeted adult smokers. Tables 1 and 2 summarize the resulting studies. The number
of study participants ranged from 65 to 8352. Participants ranged from 11 to 65 years old, and the
percent of female participants varied from 40.5% to 100%. Follow-up periods ranged 1 to 24 months.
Studies included both treatment seeking, as well as non-treatment seeking participants.
4.1. Adolescent studies
Interventions targeting adolescents have the goals of delaying onset of smoking among those who
have never tried cigarettes or have only experimented with use, or encouraging cessation among regular
users. Of the four studies that targeted adolescents, two reported a significant reduction in smoking
initiation and prevalence as the result of computer-tailored material sent to the home of the student.
Ausems, Mesters, van Breukelen, and de Vries (2002) randomized elementary school students to
receive: (1) a seven-session in-school program focused on the social factors that influence people to
smoke, education about the effects of smoking on the body, and training in refusal skills; (2) three mailed
letters, tailored to students based on beliefs, efficacy, and intent to smoke; (3) both in-school and mailed
conditions, or; (4) control. At a 6-month follow-up, the mailed condition reduced smoking initiation
(10.4% vs. 18.1%) and continuation (13.1% vs. 23.5%) relative to control. The effects of the in-school
program did not significantly differ from control, nor was the combined approach superior to the mailed-
only condition. Using a similar intervention design with vocational school students, Ausems, Mesters,
van Breukelen, & De Vries (2004) found that those in the in-school condition who had ever tried a
cigarette were less likely to continue smoking at 12 months relative to control (29.4% vs. 42.2%,
respectively). The mailed condition prevented smoking initiation at 18 months, relative to control

Table 1
Effects of computer interventions on smoking cessation among adolescents
Study Participants Follow-up
(Months)
Intervention conditions Smoking Summary of findings
Initiat Contin
Ausems
et al.
(2002)
3734 students
ages 11–12
6 1. Seven-session teacher-led
program
14.9ab 21.6ab Mailed intervention reduced
smoking initiation and
prevalence at 5 months.
No effect of the in-school
program over control, or
combined program over
mailed intervention.
2. Three tailored letters
mailed to students’ homes
10.4a 13.1a
3. Seven session teacher-led
program+3 tailored letters
mailed to students’ homes
15.2ab 14.2ab
4. No treatment control 18.1b 23.5b
Ausems
et al.
(2004)
36 vocational
schools (students
ages 12–16 years)
6/12 1. Three-session teacher-led
program
28.0a 29.4a In-school intervention reduced
smoking at 12 months, as
compared to control. Mailed
intervention reduced smoking
initiation at 18 months, as
compared to control (in-school
condition not assessed at 18
months). No additional effect
of the combined intervention.
2. Three tailored letters
mailed to students’ homes
25.0a 37.0ab
3. Three-session teacher-led
program+3 tailored letters
mailed to students homes
29.4a 45.0ab
4. No treatment control 40.9a 42.2b
Aveyard
et al.
(2001)
8352 students
ages 13–14
12/24 1. Three class sessions+3
interactive computer sessions
17.7a 83.2ay No benefit of intervention in
terms of initiation or cessation
at 1 or 2 years.2. No treatment control 16.5a 85.0ay
Pallonen
et al.
(1998)
135 adolescent
smokers
6 1. Tailored computer program
focused on smoking cessation
59.4az 30% of participants made at
least one 24-h quit attempt at
6 months, with no differences
between groups.
2. Standard baction orientedQcomputer program
59.4az
Initiat=Percent of baseline never-smokers who initiated smoking during longest follow-up period; Contin=Percent of baseline
ever-smokers who reported smoking at longest follow-up period.
Letters indicate significant ( p b .05) contrasts between intervention conditions: a=a, a=ab, b=ab, apbpc.y Continuation rates: bRegular weekly smokingQ at baseline, bregular weekly smokingQ at follow-up.z No 24 h quit attempts during the last 2 months.
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277268
(27.2% vs. 47.9%, respectively), but the in-school condition was not reassessed at 18 months. There was
no additional effect for the combined condition at any follow-up point.
Conflicting results were reported by Aveyard et al. (2001) who failed to find differences between
groups that received a classroom lecture or computer intervention. At 1- and 2-year follow-ups, the
groups showed similar rates of smoking and stage-of-change movement. Pallonen et al. (1998) compared
a computer intervention with material consistent with the student’s stage of change, to a computer
intervention that emphasized only bactionQ strategies (e.g., suggestions for changing behavior). At a 6-
month follow-up, the authors found no difference between the two groups in terms of cessation.
4.2. Adult studies
All adult interventions targeted cessation in regular smokers. Of the 15 studies targeting adult
smokers, seven reported significantly improved cessation among treatment subjects as compared to
control subjects at the longest follow-up.
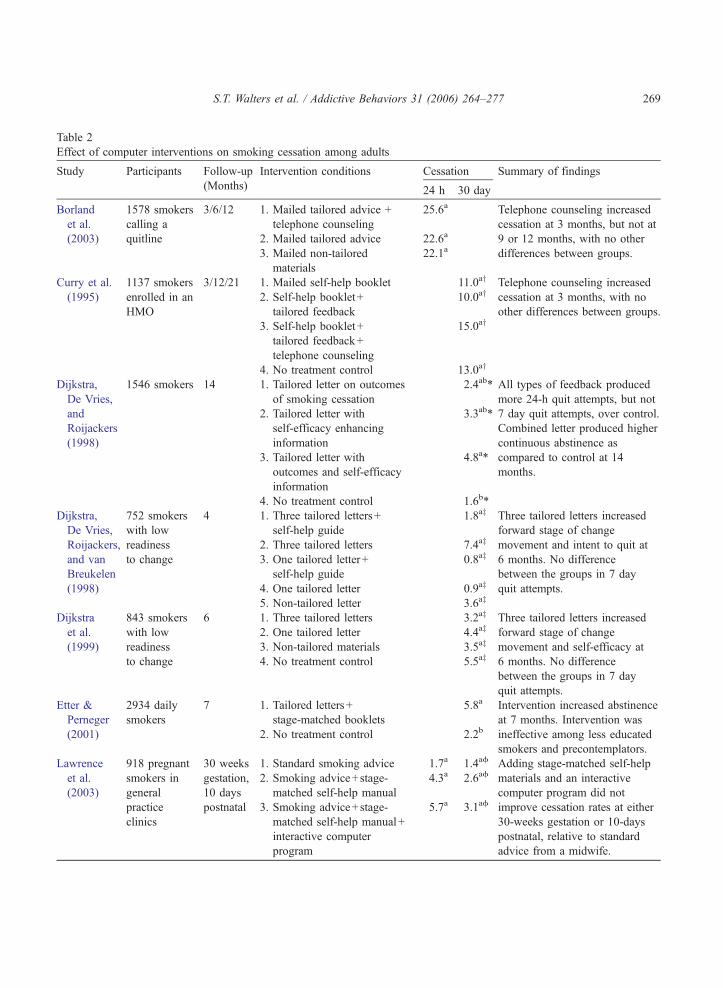
Table 2
Effect of computer interventions on smoking cessation among adults
Study Participants Follow-up
(Months)
Intervention conditions Cessation Summary of findings
24 h 30 day
Borland
et al.
(2003)
1578 smokers
calling a
quitline
3/6/12 1. Mailed tailored advice +
telephone counseling
25.6a Telephone counseling increased
cessation at 3 months, but not at
9 or 12 months, with no other
differences between groups.
2. Mailed tailored advice 22.6a
3. Mailed non-tailored
materials
22.1a
Curry et al.
(1995)
1137 smokers
enrolled in an
HMO
3/12/21 1. Mailed self-help booklet 11.0ay Telephone counseling increased
cessation at 3 months, with no
other differences between groups.
2. Self-help booklet+
tailored feedback
10.0ay
3. Self-help booklet+
tailored feedback+
telephone counseling
15.0ay
4. No treatment control 13.0ay
Dijkstra,
De Vries,
and
Roijackers
(1998)
1546 smokers 14 1. Tailored letter on outcomes
of smoking cessation
2.4ab* All types of feedback produced
more 24-h quit attempts, but not
7 day quit attempts, over control.
Combined letter produced higher
continuous abstinence as
compared to control at 14
months.
2. Tailored letter with
self-efficacy enhancing
information
3.3ab*
3. Tailored letter with
outcomes and self-efficacy
information
4.8a*
4. No treatment control 1.6b*
Dijkstra,
De Vries,
Roijackers,
and van
Breukelen
(1998)
752 smokers
with low
readiness
to change
4 1. Three tailored letters+
self-help guide
1.8az Three tailored letters increased
forward stage of change
movement and intent to quit at
6 months. No difference
between the groups in 7 day
quit attempts.
2. Three tailored letters 7.4az
3. One tailored letter+
self-help guide
0.8az
4. One tailored letter 0.9az
5. Non-tailored letter 3.6az
Dijkstra
et al.
(1999)
843 smokers
with low
readiness
to change
6 1. Three tailored letters 3.2az Three tailored letters increased
forward stage of change
movement and self-efficacy at
6 months. No difference
between the groups in 7 day
quit attempts.
2. One tailored letter 4.4az
3. Non-tailored materials 3.5az
4. No treatment control 5.5az
Etter &
Perneger
(2001)
2934 daily
smokers
7 1. Tailored letters+
stage-matched booklets
5.8a Intervention increased abstinence
at 7 months. Intervention was
ineffective among less educated
smokers and precontemplators.
2. No treatment control 2.2b
Lawrence
et al.
(2003)
918 pregnant
smokers in
general
practice
clinics
30 weeks
gestation,
10 days
postnatal
1. Standard smoking advice 1.7a 1.4af Adding stage-matched self-help
materials and an interactive
computer program did not
improve cessation rates at either
30-weeks gestation or 10-days
postnatal, relative to standard
advice from a midwife.
2. Smoking advice+stage-
matched self-help manual
4.3a 2.6af
3. Smoking advice+stage-
matched self-help manual+
interactive computer
program
5.7a 3.1af
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 269
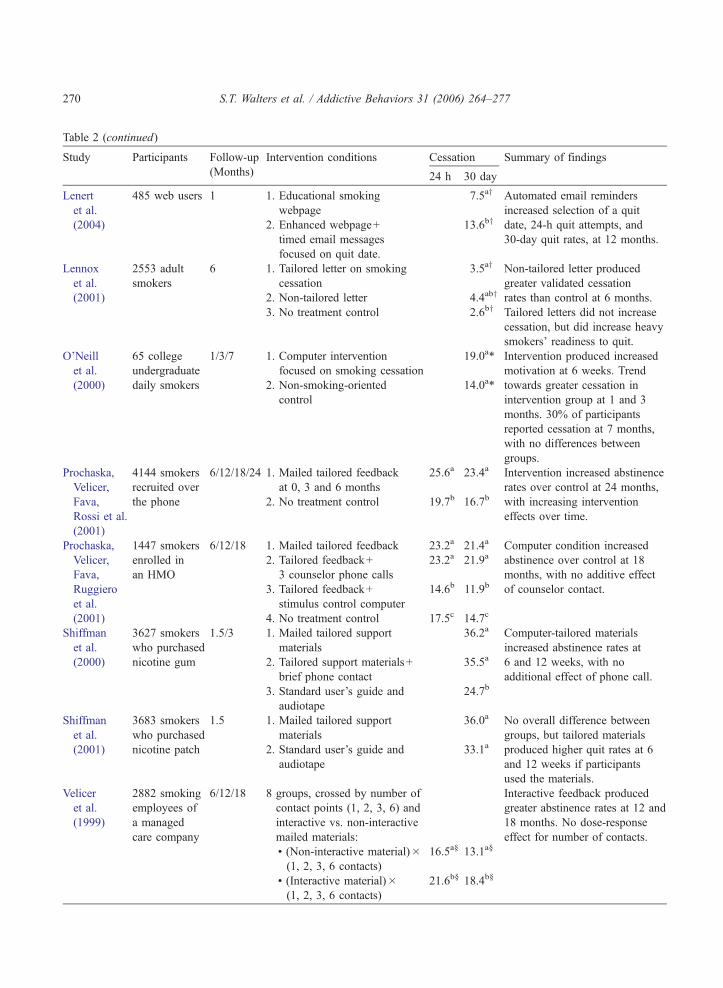
Table 2 (continued)
Study Participants Follow-up
(Months)
Intervention conditions Cessation Summary of findings
24 h 30 day
Lenert
et al.
(2004)
485 web users 1 1. Educational smoking
webpage
7.5ay Automated email reminders
increased selection of a quit
date, 24-h quit attempts, and
30-day quit rates, at 12 months.
2. Enhanced webpage+
timed email messages
focused on quit date.
13.6by
Lennox
et al.
(2001)
2553 adult
smokers
6 1. Tailored letter on smoking
cessation
3.5ay Non-tailored letter produced
greater validated cessation
rates than control at 6 months.
Tailored letters did not increase
cessation, but did increase heavy
smokers’ readiness to quit.
2. Non-tailored letter 4.4aby
3. No treatment control 2.6by
O’Neill
et al.
(2000)
65 college
undergraduate
daily smokers
1/3/7 1. Computer intervention
focused on smoking cessation
19.0a* Intervention produced increased
motivation at 6 weeks. Trend
towards greater cessation in
intervention group at 1 and 3
months. 30% of participants
reported cessation at 7 months,
with no differences between
groups.
2. Non-smoking-oriented
control
14.0a*
Prochaska,
Velicer,
Fava,
Rossi et al.
(2001)
4144 smokers
recruited over
the phone
6/12/18/24 1. Mailed tailored feedback
at 0, 3 and 6 months
25.6a 23.4a Intervention increased abstinence
rates over control at 24 months,
with increasing intervention
effects over time.
2. No treatment control 19.7b 16.7b
Prochaska,
Velicer,
Fava,
Ruggiero
et al.
(2001)
1447 smokers
enrolled in
an HMO
6/12/18 1. Mailed tailored feedback 23.2a 21.4a Computer condition increased
abstinence over control at 18
months, with no additive effect
of counselor contact.
2. Tailored feedback+
3 counselor phone calls
23.2a 21.9a
3. Tailored feedback+
stimulus control computer
14.6b 11.9b
4. No treatment control 17.5c 14.7c
Shiffman
et al.
(2000)
3627 smokers
who purchased
nicotine gum
1.5/3 1. Mailed tailored support
materials
36.2a Computer-tailored materials
increased abstinence rates at
6 and 12 weeks, with no
additional effect of phone call.
2. Tailored support materials+
brief phone contact
35.5a
3. Standard user’s guide and
audiotape
24.7b
Shiffman
et al.
(2001)
3683 smokers
who purchased
nicotine patch
1.5 1. Mailed tailored support
materials
36.0a No overall difference between
groups, but tailored materials
produced higher quit rates at 6
and 12 weeks if participants
used the materials.
2. Standard user’s guide and
audiotape
33.1a
Velicer
et al.
(1999)
2882 smoking
employees of
a managed
care company
6/12/18 8 groups, crossed by number of
contact points (1, 2, 3, 6) and
interactive vs. non-interactive
mailed materials:
Interactive feedback produced
greater abstinence rates at 12 and
18 months. No dose-response
effect for number of contacts.
! (Non-interactive material)�(1, 2, 3, 6 contacts)
16.5a§ 13.1a§
! (Interactive material)�(1, 2, 3, 6 contacts)
21.6b§ 18.4b§
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277270

S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 271
The modal intervention format involved computer-generated feedback and advice sent through the
mail. Prochaska and colleagues tested the efficacy of mailed material in two trials. In the first trial
(Prochaska, Velicer, Fava, Rossi, & Tsoh, 2001), smokers were randomized to a mailed intervention or
control. The mailed intervention included information about the pros and cons of quitting, a normative
comparison, and advice commensurate with the smoker’s stage of change. At 24 months, the mailed
information produced 26% point abstinence, as compared to 20% in the control condition. In the second
study (Prochaska, Velicer, Fava, Ruggiero et al., 2001), a series of brief provider phone contacts were
tested as an adjunct to the mailed report. At 24 months, those who received the report again showed
greater point abstinence (21%) as compared to control (15%), with no additional benefit of phone contact.
Using a similar design, Curry, McBride, Grothaus, Loutie, and Wagner (1995) recruited smokers from
a large health maintenance organization (HMO) who were not requesting help with cessation. Using an
incremental design, the authors randomized participants to receive: (1) a self-help manual; (2) a self-help
manual and computer-generated feedback; (3) a self-help manual, computer-generated feedback, and
three telephone calls to reinforce use of the self-help materials; or (4) control. The feedback included
information on stage of change, self-identified reasons for wanting to quit, and cessation advice. The
counseling condition focused on encouraging smokers to use the self-help materials. Telephone
counseling (but not mailed feedback) significantly increased cessation at 3 months (11%, 4%, 5%, and
6% point prevalence for counseling, feedback, booklet, and control conditions, respectively). However,
differences were nonsignificant at 12 and 21 months.
Etter and Perneger (2001) randomized participants to a mailed intervention or control. An average of
1.5 times over a 6-month period, intervention participants received a letter tailored to stage-of-change,
level of dependence, self-efficacy, and other characteristics. Seven months after beginning the program,
intervention participants were more likely to be abstinent than control participants (5.8% vs. 2.2% point
prevalence). In a similar study, Dijkstra, De Vries, and Roijackers (1998) found that tailored information
that emphasized both the benefits of smoking cessation, as well as advice on cessation skills, was more
effective than either presented in isolation.
Three studies compared computer-tailored information to similar, but untailored, information.
Borland, Balmford, Segan, Livingston, and Owen (2003) randomized smokers calling a quitline service
to: (1) mailed untailored self-help materials, (2) computer-generated tailored advice, or (3) computer-
generated tailored advice and brief telephone counseling. At a 3 month follow-up, more individuals in
the tailored advice and counseling condition were abstinent (21% point prevalence) than in the other
conditions (12%), but by 12 months, the effect was nonsignificant when adjusted for multiple
comparisons. Lennox et al. (2001) compared computer-tailored information, non-tailored information, or
control. Interestingly, the authors found that among heavier smokers, the non-tailored letter (but not the
tailored letter) produced greater cessation rates as compared to control. At 6 months, the non-tailored
Notes to Table 2:
Cessation=Rates of cessation at longest follow-up for 24 h point abstinence and 30 day point abstinence. Letters indicate
significant ( p b .05) contrasts between intervention conditions within outcome category: a=a, a=ab, b=ab, apbpc.* Continuous abstinence.y 7 day point abstinence.z 7 day quit attempt.§ Values averaged across number of contacts.f Sustained abstinence of 10 weeks.
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277272
group reported cessation rates of 4.4%, as compared to 3.5% and 2.6% in the tailored and control groups,
respectively.
Three studies tested multiple iterations of feedback. Dijkstra, De Vries, Roijackers, and van
Breukelen (1998) found that multiple tailored letters were more effective than either non-tailored
letters or a single tailored letter. In another study, Dijkstra, De Vries, and Roijackers (1999) found that
multiple tailored letters produced greater stage transition and intent to quit, but not actual quit
attempts. Finally, Velicer, Prochaska, Fava, LaForge, and Rossi (1999) compared interactive vs. non-
interactive computer reports, crossed with number of mailed contacts (i.e., one, two, three, or six). At
an 18-month follow-up, there was an effect of the stage-matched materials (average 30-day cessation
rates of 18.4% and 13.1% for tailored and non-tailored, respectively), but no dose-response effect in
terms of number of mailings.
Two studies tested the efficacy of computer-generated feedback as an adjunct to nicotine replacement
therapy. One study (Shiffman, Paty, Rohay, Di Marino, & Gitchell, 2000) evaluated the effectiveness of
feedback materials as an adjunct to nicotine polycrilex gum. In this study, participants who had
purchased nicotine gum were randomized to receive computer-tailored materials with or without a phone
call, or to receive only the standard information packaged with the gum. At 12 weeks, participants who
had received the tailored information reported significantly higher 30-day abstinence rates (27%) as
compared to control (18%), with no additional effect of the phone call (27%). The intervention in this
study appeared to be effective across gender, level of dependence, and self-efficacy. In contrast,
Shiffman, Paty, Rohay, Di Marino, and Gitchell (2001) did not find an effect when similar tailored
information was compared to standard materials among smokers receiving the nicotine patch. At 12
weeks, abstinence rates did not differ between the two groups. However, among participants who
reported using the materials, cessation rates were generally higher.
Three adult studies tested direct contact with interactive computer programs. Lawrence, Aveyard,
Evans, and Cheng (2003) evaluated a cessation program for expectant mothers. Pregnant smokers
presenting at a general practice clinic were randomized to receive: (1) brief cessation advice delivered by
a midwife, (2) bEnhancedQ cessation advice from a midwife trained in the Transtheoretical Model, plus a
series of self-help manuals, or (3) bEnhancedQ cessation advice from a midwife trained in the
Transtheoretical Model, a series of self-help manuals, and a 20-min computer program that provided
feedback on stage-of-change and other aspects of smoking. At 30-weeks gestation and 10 days postnatal,
there were no significant differences between groups in terms of cessation rates. Lenert, Munoz, Perez,
and Bansod (2004) tested an automated email system that sent timed educational messages to smokers.
The authors used two consecutive waves of participants visiting a website. The first wave received a
single-point-in-time educational message via a website, and the second wave received an enhanced
website intervention that also sent follow-up emails. Although the two groups were not randomly
assigned, the authors suggest that they did not differ on factors associated with 30-day quit rates. At a
30-day follow-up, the enhanced intervention appeared to increase the rate at which participants set a quit
date (97%) as compared to the standard website (91%). Participants in the enhanced group also reported
greater rates of 24-h quit attempts (83% vs. 54%) and 30-day quit rates (13.6% vs. 7.5%). Finally,
O’Neill, Gillispie, and Slobin (2000) compared a computer intervention targeted to college students to a
non-smoking focused control intervention. The smoking intervention consisted of four computer
sessions that progressed along the lines of the stages of change. Early sessions emphasized
consciousness raising and self-evaluation, whereas later sessions targeted commitment and planning.
At the end of the 6-week study period, 48% of the intervention participants showed forward movement
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 273
in their stage of change as compared to 21% in the control group. Although there was an initial trend
towards greater quitting in the intervention group, by seven months quit rates did not differ between the
groups.
5. Discussion
While computer-based smoking prevention and cessation programs show promise in influencing
tobacco-related behaviors, published studies show mixed results in terms of translating the educational
experience to real-world practice. Of the 19 automated, computer-based interventions that we reviewed,
nine (47%) showed evidence of effectiveness at the longest follow-up.
This review should not be considered an exhaustive analysis. The scope of our investigations was
limited to English-language publications catalogued in three specialist databases. Published studies of
this type are also subject to publication bias-the tendency for studies that show beneficial effects to be
published. As we have noted, study components, subject characteristics (demographics and intention to
treat), length of follow-up, and outcome measures were highly variable. This heterogeneity of methods
makes it difficult to determine consistent predictors of efficacy. Insufficient reporting of the
interventions, subject characteristics, and outcome measures further compounded this difficulty. For
instance, in some studies the outcome measure was simply described as babstinenceQ or bpointabstinenceQ with no further information on how these outcomes were operationalized.
Despite these limitations, three observations are consistent with a previous review (Strecher, 1999).
Studies with smokers who were treatment seeking (e.g., who wanted to quit smoking) typically resulted
in higher abstinence rates than studies that used general population samples of smokers. Second, most
studies that used multiple follow-up points found that the effects of the intervention were lessened with
time. Finally, in all cases, the intervention conditions produced rates of abstinence that were at least
equivalent, if not higher, than non-treatment controls. That is, no intervention condition seemed to make
smokers more likely to smoke relative to control.
Aside from these broad observations, there remains a lack of clarity about what types of computer-
based applications are most effective. The paradox is that while the number of smoking cessation
programs is growing (high dissemination), we have little understanding of how, why, and under what
conditions, such interventions might work (low evaluation). For instance, although Edwards, Elliott,
Conway, and Woodruff (2003) identified 87 Internet programs devoted to teen smoking cessation, our
review found no outcome studies of any of these programs in the peer reviewed literature. To estimate
and improve the effectiveness of computer- and Internet-based interventions, it will be important for
future research efforts to emphasize the importance of (1) theoretical foundations to design and
develop computer-based programs, and (2) rigorous evaluation methods to determine their
effectiveness.
The use of computers for generating tailored interventions has evolved with the capabilities of
computer technology. As with Strecher’s (1999) review, the modal intervention appeared to follow
what Brug, Campbell, and van Assema (1999) call bfirst generationQ formats. In this format,
participants have no direct contact with the computer. Typically, participants complete a paper
screening instrument, which is then entered into the computer and used to derive mailed feedback. Of
the 14 first generation interventions in this review, eight (57%) reduced smoking over control. In a
bsecond generationQ format, participants interact directly with the system. This format provides
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277274
immediate communication between participant and program, but the participant must have access to,
and know how to operate, a computer. Research using second generation tailoring has demonstrated
improved disease management and behavioral determinants of awareness and intentions in other areas
(Bartholomew et al., 2000; Onema, Brug, & Lechner, 2001; Shegog et al., 2005). However, the
effectiveness of second generation tailoring has not been widely tested in the field of smoking
cessation. Only one intervention, a smoking website that generated personalized email messages,
appeared to use this format (Lenert et al., 2004). This intervention increased cessation over control at
12 months. The recently emerging bthird generationQ of computer-based applications employs both
iterative as well as ipsitive feedback, adjusting at multiple time points to the characteristics of the user.
These programs are structured modularly (rather than as a single linear program), so that they can
better adjust to the user’s needs. For instance, whereas a second generation program might tailor a
series of messages, a third generation intervention might add, delete, or rearrange components in
response to the user. None of the third generation interventions in this review (2 for adolescents, 2 for
adults) had a significant impact on smoking over control.
Because the number of computer-based health education programs has increased significantly over
the past ten years, there is a need for smoking prevention and cessation programs that are
theoretically-and empirically-based (Revere & Dunbar, 2001; Rhodes, Fishbein, & Reis, 1997; Skinner
& Kreuter, 1997). Explanatory models of behavior change propose various factors that are thought to
underlie adoption or rejection of a given behavior. Such a theory should be the basis for specifying
program objectives, health behaviors, cognitive determinants of behavior (e.g., knowledge, attitudes,
social perceptions, self-efficacy), change methods, and evaluation and measurement protocols
(Lieberman, 1997; Revere & Dunbar, 2001; Rhodes et al., 1997; Skinner & Kreuter, 1997). Program
design must further impact the array of behavioral determinants by offering an engaging experience
and thereby optimize the chance for translation of computer messages to real-world application
(Shegog et al., 2001). To tailor interventions, programs use a variety of variables, such as gender, level
of problem severity, and motivational readiness (e.g., Stage of Change) for change. However, because
many of these studies did not find a differential effect of the intervention across gender, ethnicity, or
problem severity, future studies will need to determine which types of tailoring are most effective, and
for whom.
Increased rigor in the design of evaluation studies is also necessary to determine which computer-
based smoking programs best affect behavioral outcomes. Adler and Johnson (2000) have noted some
of the shortfalls of existing computer-based research, including demonstration articles over comparison
studies, inexperience of investigators studying computer applications, and studies that compare
interventions that vary in both content and media formats. Future research directions include
investigations of user-media-message interactions to understand effective educational strategies rather
than comparisons of different media approaches, economic analyses regarding the cost and time
benefits of computer-based applications, and diffusion studies that examine how technology might be
best integrated into educational and healthcare settings (Adler & Johnson, 2000; Street & Rimal,
1997).
In the scope of public health interventions, computer-based applications have been available for a
relatively brief time. During this time, however, generations of applications have evolved that have
demonstrated some effectiveness in changing smoking behavior. Increased rigor in design, development,
and evaluation of future programs will provide better insight into how to affect this persistent public
health problem.
S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 275
References
Adler, M. D., & Johnson, K. B. (2000). Quantifying the literature of computer-aided instruction in medical education. Academic
Medicine, 75(10), 1025–1028.
Ausems, M., Mesters, I., van Bruekelen, G., & De Vries, H. (2002). Short-term effects of a randomized computer-based out-of-
school smoking prevention trial aimed at elementary schoolchildren. Preventive Medicine, 34, 581–589.
Ausems, M., Mesters, I., van Breukelen, G., & De Vries, H. (2004). Effects of in-school and tailored out-of-school smoking
prevention among Dutch vocational school students. Health Education Research, 19, 51–63.
Aveyard, P., Sherratt, E., Almond, J., Lawrence, T., Lancashire, R., Griffin, C., et al. (2001). The change-in-stage and updated
smoking status results from a cluster-randomized trial of smoking prevention and cessation using the Transtheoretical Model
among British adolescents. Preventive Medicine, 33, 313–324.
Bartholomew, I. K., Gold, R., Parcel, G. S., Czyzewski, D., Sockrider, M., Fernandez, M., et al. (2000). Watch, discover, think
then act: Evaluation of computer-assisted instruction to improve asthma self-management in inner-city children. Journal of
Patient Education and Counseling, 39, 269–280.
Bessell, T. L., McDonald, S., Silagy, C. A., Anderson, J. N., Hiller, J. E., & Sansom, L. N. (2002). Do internet interventions for
consumers cause more harm than good? A systematic review. Health Expectations, 5(1), 28–37.
Borland, R., Balmford, J., Segan, C., Livingston, P., & Owen, N. (2003). The effectiveness of personalized smoking cessation
strategies for callers to a Quitline service. Addiction, 98, 837–846.
Brug, J., Campbell, M., & van Assema, P. (1999). The application and impact of computer-generated personalized nutrition
education: A review of the literature. Patient Education and Counseling, 36(2), 145–156.
Brug, J., Steenhuis, I., van Assema, P., & de Vries, H. (1996). Impact of a computer-tailored nutrition intervention. Preventive
Medicine, 25, 236–242.
Cassell, M. M., Jackson, C., & Cheuvront, B. (1998). Health communication on the internet: An effective channel for health
behavior change? Journal of Health Communication, 3(1), 71–79.
Centers for Disease Control and Prevention (2002). Annual smoking – attributable mortality, years of potential
life lost, and economic costs – United States, 1995–1999. Morbidity and Mortality Weekly Report, 51(14),
300–303.
Centers for Disease Control and Prevention (2003). Tobacco information and prevention source. Retrieved June 25, 2003, from.
http://www.cdc.gov/tobacco/issue.html
Centers for Disease Control and Prevention (2004). Cigarette smoking among adults, United States, 2002. Morbidity and
Mortality Weekly Report, 53, 427–431.
Cloud, R. N., & Peacock, P. L. (2001). Internet screening and interventions for problem drinking: Results from the
www.carebetter.com pilot study. Alcoholism Treatment Quarterly, 19(2), 23–44.
Coffield, A. B., Maciosek, M. V., McGinnis, J. M., Harris, J. R., Caldwell, M. B., Teutsch, S. M., et al. (2001). Priorities among
recommended clinical preventive services. American Journal of Preventive Medicine, 21(1), 1–9.
Curry, S. J., McBride, C., Grothaus, L. C., Loutie, D., & Wagner, E. H. (1995). A randomized trial of self-help materials,
personalized feedback, and telephone counseling with nonvolunteer smokers. Journal of Consulting and Clinical
Psychology, 6, 1005–1014.
Dijkstra, A., De Vries, H., & Roijackers, J. (1998a). Long-term effectiveness of computer-generated tailored feedback in
smoking cessation. Health Education Research, 13, 207–214.
Dijkstra, A., De Vries, H., & Roijackers, J. (1999). Targeting smokers with low readiness to change with tailored and
nontailored self-help materials. Preventive Medicine, 28, 203–211.
Dijkstra, A., De Vries, H., Roijackers, J., & van Breukelen, G. (1998b). Tailoring information to enhance quitting in smokers
with low motivation to quit: Three basic efficacy questions. Health Psychology, 17, 513–519.
Edwards, C. C., Elliott, S. P., Conway, T. L., & Woodruff, S. I. (2003). Teen smoking cessation help via the Internet: A survey
of search engines. Health Promotion Practice, 4(3), 262–265.
Etter, J. -F., & Perneger, T. V. (2001). Effectiveness of a computer-tailored smoking cessation program. Archives of Internal
Medicine, 161, 2596–2601.
Firby, P. A., Luker, K. A., & Caress, A. L. (1991). Nurses’ opinions of the introduction of computer-assisted learning for use in
patient education. Journal of Advanced Nursing, 16, 987–995.
Green, M. J., & Fost, N. (1997). An interactive computer program for educating and counseling patients about genetic
susceptibility to breast cancer. Journal of Cancer Education, 12(4), 204–208.

S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277276
Hester, R. K., & Delaney, H. D. (1997). Behavioral self-control program for Windows: Results of a controlled clinical trial.
Journal of Consulting and Clinical Psychology, 65, 686–693.
Institute of Medicine (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC7 National
Academy Press.
Kumar, N. G., Bostow, D. W., Schapira, D. V., & Kritch, K. M. (1993). Efficacy of interactive automated programmed
instruction in nutrition education for cancer prevention. Journal of Cancer Education, 8, 203–211.
Lancaster, T., & Stead, L. F. (2004). Self help interventions for smoking cessation. Cochraine library. Issue 1. Chechester, UK7
Wiley.
Lawrence, T., Aveyard, P., Evans, O., & Cheng, K. K. (2003). A cluster randomized controlled trial of smoking cessation in
pregnant women comparing interventions based on the transtheoretical (stages of change) model to standard care. Tobacco
Control, 12, 168–177.
Lenert, L., Munoz, R. F., Perez, J. E., & Bansod, A. (2004). Automated e-mail messages as a tool for improving quit rates in an
Internet smoking cessation intervention. Journal of the American Medical Informatics Association, 4, 235–240.
Lennox, A. S., Osman, L. M., Reiter, E., Robertson, R., Fiend, J., McCann, I., et al. (2001). Cost effectiveness of computer
tailored and non-tailored cessation letters in general practice: Randomised controlled trial. British Medical Journal, 322,
1–7.
Lichtenstein, E., & Hollis, J. (1992). Patient referral to a smoking cessation program: Who follows through? Journal of Family
Practice, 34(6), 739–744.
Lieberman, D. A. (1997). Interactive video games for health promotion: Effects on knowledge, self-efficacy, social support, and
health. In R. Street, W. Gold, & T. Manning (Eds.), Health promotion and interactive technology: Theoretical applications
and future directions. Mahwah, NJ7 Lawrence Erlbaum Associates.
Oenema, A., Brug, J., & Lechner, L. (2001). Web-based tailored nutrition education: Results of a randomized controlled trial.
Health Education and Research, 16(6), 647–660.
O’Keefe, D. J. (1990). Persuasion. Newbury Park, CA7 Sage.
O’Neill, H. K., Gillispie, M. A., & Slobin, K. (2000). Stages of change and smoking cessation: A computer-administered
intervention for young adults. American Journal of Health Promotion, 15, 93–96.
Pallonen, U. E., Velicer, W. F., Prochaska, J. O., Rossi, J. S., Bellis, J. M., Tsoh, J. Y., et al. (1998). Computer-based cessation
interventions in adolescents: Description, feasibility and six month follow-up findings. Substance Abuse and Misuse, 33,
935–965.
Paperny, D. M. (1997). Computerized health assessment and education for adolescent HIV and STD prevention in health care
settings and schools. Health Education and Behavior, 24(1), 54–70.
Prochaska, J. O., Norcross, J. C., & DiClemente, C. C. (1994). Changing for good: The revolutionary program that explains the
six stages of change and teaches you how to free yourself from bad habits. New York7 W. Morrow.
Prochaska, J. O., Velicer, W. F., Fava, J. L., Rossi, J. S., & Tsoh, J. Y. (2001a). Evaluating a population-based recruitment
approach and a stage-based expert system intervention for smoking cessation. Addictive Behaviors, 26, 583–602.
Prochaska, J. O., Velicer,W. F., Fava, J. L., Ruggiero, L., Laforge, R. G., Rossi, J. S., et al. (2001b). Counselor and stimulus control
enhancements of a stage-matched intervention for smokers in a managed care setting. Preventive Medicine, 32, 23–32.
Revere, D., & Dunbar, P. J. (2001). Review of computer-generated outpatient health behavior interventions. Journal of the
Medical Informatics Association, 8, 62–79.
Rhodes, F., Fishbein, M., & Reis, J. (1997). Using behavioral theory in computer-based health promotion and appraisal. Health
Education and Behavior, 24, 20–34.
Science Panel on Interactive Communication and Health (1999). Wired for health and well-being: The emergence of interactive
health communication. Office of Disease Prevention and Health Promotion. U. S. Dept. of Health and Human Services.
Washington DC: Author.
Shegog, R., Sockrider, M., Bartholomew, L. K., Masse, L., Parcel, G., & Abramson, S. (2001). Impact of a computer-assisted
self-management education program on factors related to asthma self-management behavior. Journal of American Medical
Informatics Association, 8(1), 49–61.
Shegog, R., McAlister, A., Hu, S., Ford, K., Meshak, A., & Peters, R. (2005). Use of interactive health communication to affect
smoking intentions in middle school students: A pilot test of the bHeadbuttQ risk assessment program. American Journal of
Health Promotion, 19(5), 334–338.
Shiffman, S., Paty, J. A., Rohay, J. M., Di Marino, M. E., & Gitchell, J. (2000). The efficacy of computer-tailored smoking
cessation material as a supplement to nicotine polacrilex gum therapy. Archives of Internal Medicine, 160, 1675–1681.

S.T. Walters et al. / Addictive Behaviors 31 (2006) 264–277 277
Shiffman, S., Paty, J. A., Rohay, J. M., Di Marino, M. E., & Gitchell, J. G. (2001). The efficacy of computer-tailored smoking
cessation material as a supplement to nicotine patch therapy. Drug and Alcohol Dependence, 64, 35–46.
Silagy, C., & Stead, L. F. (2004). Physician advice for smoking cessation. Cochraine library. Issue 1. Chechester, UK7 Wiley.
Skinner, C. S., & Kreuter, M. (1997). Using theories in planning interactive computer programs. In R. Street, W. Gold, & T.
Manning (Eds.), Health promotion and interactive technology: Theoretical applications and future directions. Mahwah, NJ7
Lawrence Erlbaum Associates.
Street, R. L., & Rimal, R. N. (1997). Health promotion and interactive technology: A conceptual foundation. In R. Street, W.
Gold, & T. Manning (Eds.), Health promotion and interactive technology: Theoretical applications and future directions.
Mahwah, NJ7 Lawrence Erlbaum Associates.
Strecher, V. J. (1999). Computer-tailored smoking cessation materials: A review and discussion. Patient Education and
Counseling, 36, 107–117.
Tate, D. F., Jackvony, E. H., & Wing, R. R. (2003). Effects of Internet behavioral counseling on weight loss in adults at risk for
type 2 diabetes: A randomized trial. Journal of the American Medical Association, 289(14), 1833–1836.
Tate, D. F., Wing, R. R., & Winett, R. A. (2001). Using Internet technology to deliver a behavioral weight loss program. Journal
of the American Medical Association, 285(9), 1172–1177.
U.S. Department of Health and Human Services (2000a). Healthy people 2010. 2nd ed. Washington, DC7 U.S. Department of
Health and Human Services.
U.S. Department of Health and Human Services (2000b). Treating tobacco use and dependence. Rockville, MD7 U.S.
Department of Health and Human Services, Public Health Service.
Velicer, W. F., Prochaska, J. O., Fava, J. L., Laforge, R. G., & Rossi, J. S. (1999). Interactive versus noninteractive intervention
and dose-response relationships for stage matched smoking cessation programs in a managed care setting. Health
Psychology, 18, 21–28.
Related Documents
![Acupuncture and related interventions for smoking cessation€¦ · [Intervention Review] Acupuncture and related interventions for smoking cessation Adrian R White1, Hagen Rampes2,](https://static.cupdf.com/doc/110x72/5ec0046c1636277aa90423ab/acupuncture-and-related-interventions-for-smoking-cessation-intervention-review.jpg)










![Interventions for promoting smoking cessation during pregnancy · [Intervention Review] Interventions for promoting smoking cessation during pregnancy Judith Lumley2, Catherine Chamberlain1,](https://static.cupdf.com/doc/110x72/5f1557a404f3e23fed68e54d/interventions-for-promoting-smoking-cessation-during-pregnancy-intervention-review.jpg)