Lung (1981) 159:275-287 L H A Review of 50 Children with Obstructive Sleep Apnea Syndrome * C. Guilleminault 1.., R. Korobkin ~, and R. Winkle 2 1 Stanford Sleep Disorders Center TD114, and 2 Division of Cardiology, Stanford University School of Medicine, Stanford CA 94305, USA Abstract. Fifty children and adolescents with obstructive sleep apnea syndrome and related breathing disorders during sleep are reviewed. Subjects were subdi- vided according to whether their breathing irregularity was secondary to a medi- cal problem (group I) or was the primary complaint (group II). The most com- mon presenting complaint was excessive daytime somnolence; hyperactivity and antisocial behavior also were cited frequently. In 20% of cases, substantial per- sonality changes were reported. Clinical symptoms included failure to thrive, ab- normal weight for age, acute cardiac or cardiorespiratory failure, hypertension, and frequent upper airway infections. Continuous, heavy snoring was reported in all caseJs; disrupted nocturnal sleep, sleep walking, nightmares, and enuresis were common. All subjects, and 22 control patients, were monitored polygraphi- cally during sleep for at least one night. Nocturnal sleep in the reported popu- lation was severely disrupted. A complete disappearance of stage 3 NREM sleep was noted in 86% of cases; REM sleep was decreased less. The management of these cases is reviewed. Eight patients received permanent tracheostomies. Thir- ty children had tonsillectomy and/or adenoidectomy (three later required tracheostomy). Non-surgical approaches also were used, particularly in group 1. Follow-up on these cases to date is presented. Key words: Sleep apnea syndrome - Sleep - Children - Cardio-vascular change Introduction The report of Gastaut et al. in 1966 [3] that obese Pickwickian type patients present- ed obstructive apnea during sleep opened a new era of research. Sleep researchers and neurologists were the first involved in the deciphering of the sleep apnea syn- dromes but, during the past five years, the scope of research and the medical spe- cialties involved in it have enlarged greatly. * Presented in part at the meeting of the American Thoracic Society in May, 1981 ** To whom requests for offprints should be addressed 0341/2040/81/0159/0275/$ 02.60

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lung (1981) 159:275-287 L H
A Review of 50 Children with Obstructive Sleep Apnea Syndrome *
C. Guilleminault 1.., R. Korobkin ~, and R. Winkle 2
1 Stanford Sleep Disorders Center TD114, and 2 Division of Cardiology, Stanford University School of Medicine, Stanford CA 94305, USA
Abstract. Fifty children and adolescents with obstructive sleep apnea syndrome and related breathing disorders during sleep are reviewed. Subjects were subdi- vided according to whether their breathing irregularity was secondary to a medi- cal problem (group I) or was the primary complaint (group II). The most com- mon presenting complaint was excessive daytime somnolence; hyperactivity and antisocial behavior also were cited frequently. In 20% of cases, substantial per- sonality changes were reported. Clinical symptoms included failure to thrive, ab- normal weight for age, acute cardiac or cardiorespiratory failure, hypertension, and frequent upper airway infections. Continuous, heavy snoring was reported in all caseJs; disrupted nocturnal sleep, sleep walking, nightmares, and enuresis were common. All subjects, and 22 control patients, were monitored polygraphi- cally during sleep for at least one night. Nocturnal sleep in the reported popu- lation was severely disrupted. A complete disappearance of stage 3 NREM sleep was noted in 86% of cases; REM sleep was decreased less. The management of these cases is reviewed. Eight patients received permanent tracheostomies. Thir- ty children had tonsillectomy and/or adenoidectomy (three later required tracheostomy). Non-surgical approaches also were used, particularly in group 1. Follow-up on these cases to date is presented.
Key words: Sleep apnea syndrome - Sleep - Children - Cardio-vascular change
Introduction
The report of Gastaut et al. in 1966 [3] that obese Pickwickian type patients present- ed obstructive apnea during sleep opened a new era of research. Sleep researchers and neurologists were the first involved in the deciphering of the sleep apnea syn- dromes but, during the past five years, the scope of research and the medical spe- cialties involved in it have enlarged greatly.
* Presented in part at the meeting of the American Thoracic Society in May, 1981 ** To whom requests for offprints should be addressed
0341/2040/81/0159/0275/$ 02.60

276 C. Guilleminault et al.
Most of the data published to date involve adult subjects. In 1976 [6], we report- ed the first series of children with obstructive sleep apnea in the pediatric literature. Since that time few reports have been published that focus on the breathing prob- lems of children during sleep.
We have had the opportunity to study a fairly large population of children and adolescents (up to the age of 17 years) with obstructive sleep apnea syndrome and related disorders of breathing during sleep. This report will review the findings ob- tained on our patient population over the years, the therapeutic approaches we have taken, and the long term follow-up data we were able to gather. We shall not ad- dress here the problem of the "near miss for Sudden Infant Death Syndrome (SIDS)" infants, although it is true that some of them present obstructive sleep ap- nea during nocturnal polygraphic recording.
Definitions
The basic abnormal breathing pattern during sleep is an "apnea", defined as a cessation of airflow at the level of the nostrils and mouth lasting at least 10 s. Apnea are divided into three types: obstructive apnea occur when the airway is obstructed but respiratory effort continues; central apnea are due to decreased or absent respi- ratory muscle (diaphragmatic) activity; mixed apnea begin with a central com- ponent (lack of respiratory effort) and then develop an obstructive component (ob- struction of the airway).
Some patients demonstrate sleep-related "hypopnea": these are a reduction, but not a complete cessation, of airflow at the level of the nostrils and mouth. Like ap- nea, hypopnea are subdiyided into "obstructive" and "central" [5].
The definition of each of these abnormal sleep-related breathing patterns has been developed with polygraphic monitoring of respiration using strain gauges, thermistors, endosphageal pressure balloons or transducers, and measurement of blood oxygen saturation. In selected cases, fiberoptic studies and filming have pro- vided visual confirmation of the data obtained by polysomnography.
To allow easy computation of the number of respiratory disturbances during sleep, an "Apnea Index" has been developed [10]. The index, which gives the num- ber of abnormal breathing events per sleep hour consists of:
A + H - A I
TST
where A = total apnea during sleep; H=to ta l hypopnea during sleep: A + H thus = total abnormal respiratory events during sleep; TST= total sleep time in minutes.
We obtained normative data on breathing during sleep in children using several approaches. A systematic longitudinal study was performed on 22 normal volun- teers (11 boys and 11 girls), aged 9 to 13 years [2]. Data for children between the ages of 2 and 7 years were obtained from subjects participating in another study. Respiratory variables were measured during one night, using non-invasive tech- niques such as strain gauges, thermistors, and ear oximeters (n = 8). A similar ap- proach was used to obtain data on 15-16 year old adolescents (n = 5). These studies did not demonstrate any effect of sex on breathing patterns. However, sleep states

Obstructive Sleep Apnea in Children 277
clearly do have an impact. The largest number of respiratory pauses were seen dur- ing stage 1 non rapid eye movement (NREM) sleep and during rapid eye movement (REM) sleep. All respiratory pauses seen, regardless of the age group, were of the central type. The maximum AI for controls was 3 in the 2-7 year age group, 3 in the 9 to 13 year age group, and 4 in the 15-16 year age group. We thus consider an AI of greater than 5 to be abnormal.
Techniques and Patients
Polygraphic Techniques
All normal and control patients were monitored during nocturnal sleep for at least one night. Depending on the patient and the clinical protocol or research project, two or three nights' recording were performed in most cases. All patients who underwent surgical procedures had follow-up post-surgery recordings.
The following variables were monitored for indication of sleep stages and states: electroencephalogram (EEG)C3/A2-C4/A1 of the 10-20 international placement system, electrooculogram (EOG), and chin electromyogram (EMG). Respiration was monitored by means of nasal and buccal thermistors and abdominal and tho- racic strain gauges. Blood oxygen saturation was measured using an ear oximeter. Electrocardiogram (ECG) lead II and a 24 h ambulatory Holter ECG monitor were used. Percent expired COs was measured in two thirds of the patients. When several successive nights were monitored during one testing session, more invasive tech- niques usually were applied. The most common additional device was an en- doesophageal~balloon or a 1 mm diameter pressure transducer; it was used in 60% of the patient population. Intraarterial and Swan-Ganz catheters were used in- frequently; two patients only received continuous monitoring of pulmonary arterial pressure. Arterial lines were placed in 15 patients.
Patient Population
The patient population can be subdivided into two groups. Group I consists of chil- dren who presented an illness which might explain the existence of a sleep apnea syndrome (SAS) -"secondary SAS". Group II includes children who did not present a clear illness easily associated with SAS - "primary SAS". Table 1 outlines the as- sociated diagnoses of Group I, the number of children diagnosed with a given ill- ness, and the age range at which the children were referred to a sleep clinic for sus- picion of SAS or sleep disorder. Also indicated are those patients in which the sleep complaint led to the appropriate "primary" diagnosis.
Clinical Symptoms
The age of the child at the time of referral influenced the complaint presented by the patient or, more frequently, reported by the family. Tables 2 and 3 subdivide symptoms according to whether they were nocturnal or diurnal.
The most common complaint was excessive daytime sleepiness (EDS) (84%). In 70% of cases, this symptom was noted by school teachers, whether in a regular or special education class. Kindergartens, day care centers, and schools also often re-
278 C. Guilleminault et al.
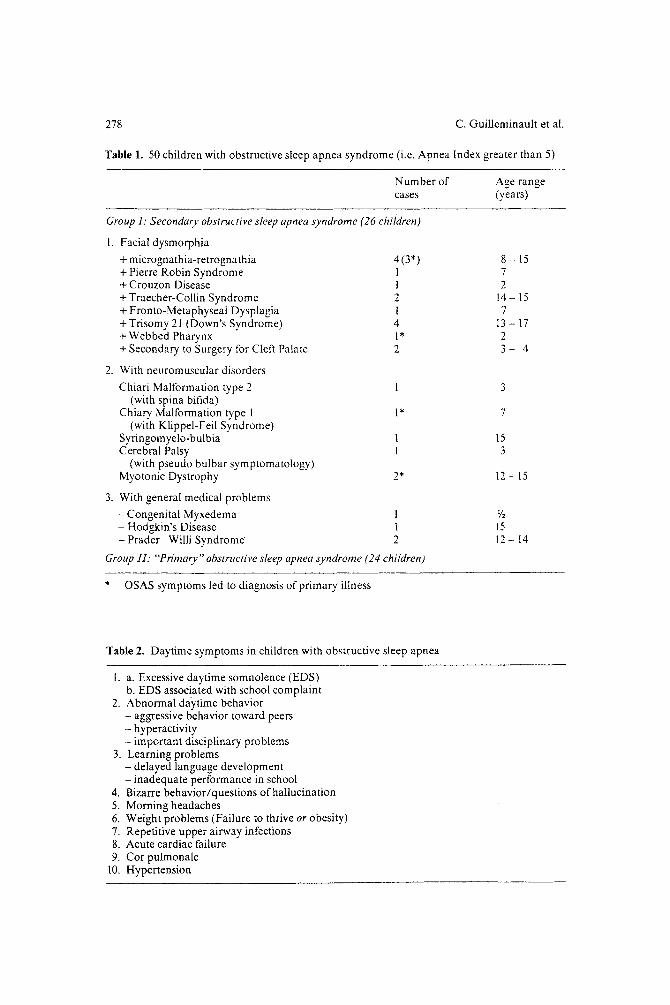
Table 1. 50 children with obstructive sleep apnea syndrome (i.e. Apnea Index greater than 5)
Number of Age range cases (years)
Group t: Secondary obstructive sleep apnea syndrome (26 children)
I. Facial dysmorphia
+ micrognathia-retrognathia 4 (3*) + Pierre Robin Syndrome 1 + Crouzon Disease 1 + Traecher-Collin Syndrome 2 + Fronto-Metaphyseal Dysplagia 1 + Trisomy 21 (Down's Syndrome) 4 + Webbed Pharynx 1" + Secondary to Surgery for Cleft Palate 2
2. With neuromuscular disorders
Chiari Malformation type 2 1 (with spina bifida)
Chiary Malformation type 1 1" (with Klippel-Feil Syndrome)
Syringomyelo-bulbia I Cerebral Palsy 1
(with pseudo bulbar symptomatology) Myotonic Dystrophy 2*
3. With general medical problems
- Congenital Myxedema 1 - Hodgkin's Disease t - Prader Willi Syndrome 2
Group II: "Primary'" obstructive sleep apnea syndrome (24 children)
8 - 1 5 7 2
14- 15 7
13 - 17 2 3 - 4
3
7
15 3
12- 15
15 12- 14
* OSAS symptoms led to diagnosis of primary illness
Table 2. Daytime symptoms in children with obstructive sleep apnea
1. a. Excessive daytime somnolence (EDS) b. EDS associated with school complaint
2. Abnormal daytime behavior - aggressive behavior toward peers - hyperactivity - important disciplinary problems
3. Learning problems - delayed language development - inadequate performance in school
4. Bizarre behavior/questions of hallucination 5. Morning headaches 6. Weight problems (Failure to thrive or obesity) 7. Repetitive upper airway infections 8. Acute cardiac failure 9. Cot pulmonale
10. Hypertension

Obstructive Sleep Apnea in Children
Table 3. Nocturnal symptoms in children with obstructive sleep apnea
279
1. Increase in total sleep time during the 24 h (Hypersomnia)
2. Disrupted nocturnal sleep (with or without nightmares and/or night terrors)
3. Continuous, heavy snoring 4. Obstruction during sleep - observed by parents
(associated or not associated with cynanosis) 5. Nocturnal enuresis
(particularly of the 2nd type)
ported abnormal daytime aggressive and bizarre behavior. Educators and teachers frequently were the ones who requested clinical investigation. Hyperactivity was noted in 42% of cases; however, the complaint was more often of children with "asocial" behavior (fighting with peers, aggressiveness, crying easily (particularly in the younger age group), being unable to maintain attention to one subject for an extended period of time, switching very quickly from hyperactivity to excessive som- nolence and withdrawn conduct - 7670 of cases).
A smaller group (20%) had more substantial personality changes, reporting ter- rifying nightmares, hypnagogic hallucinations, or bizarre, withdrawn behavior. Some of the children, such as those with trisomny 21, Crouzon disease, Traecher- Collin Syndrome, etc., already had a severe handicap related to their initial con- genital problem. However, it was noted that these children experienced a further re- gression in their slow development and that their performance in special education classes dropped abruptly without clear explanation. In two cases, appearance of stereotypic bizarre behavior led to psychiatric consultation and a question of psy- chotic episodes.
The older children complained of sleepiness, tiredness, and fatigue. Such com- plaints were not clearly expressed by the younger age groups, but neurophysiologi- cal testing demonstrated delayed language acquisition and decreased school per- formance (16% of cases), leading to medical consultation.
Morning headaches were mentioned as "revealing symptoms" in 16% of cases; careful history elicited the complaint in a further 10%. Failure to thrive was noted in 56% of the children. Massive obesity was present in 10%. Acute cardiac failure or cardio-respiratory failure led tO emergency hospitalization and clinical investigation for sleep apnea syndrome in 20% of the patients. Hypertension was found in 8%. Frequent upper airway infection was reported in 26%.
Nocturnal Symptoms
Noctural symptoms usually were revealed through questioning of parents; occasion- ally, the symptoms were severe enough to have led to the consultation. Continuous heavy snoring, interrupted by pauses and associated with snorts, is the hallmark of obstructive sleep apnea syndrome and was present in 100% of the cases. 84% of the subjects had disrupted nocturnal sleep. This was troublesome for the parents of young children, particularly when it was associated with sleep walking (10%) and/or night terrors and nightmares (2470). Enuresis, most significant when it reappeared
280 C. Guilleminault et al.
after toilet training, was noted in 18% of the cases. Nocturnal profuse sweating was noted in 96% of the children.
Clinical evaluation also revealed clubbing of fingers in 3 children (6%). Depend- ing on the associated clinical diagnosis in "secondary" obstructive apnea syndrome, many different other clinical findings were present. In the "primary" obstructive ap- nea syndrome, limb hypotonia was noted in 18% of children, all of whom were un- der 8 years of age. Oto-laryngological evaluation was performed in all cases. In the "primary" group (group II), 14 of the 24 children were considered to have 2 + mild- ly enlarged tonsils and/or adenoids; only 4 had obvious lymphoid tissue enlarge- ment with adenoidal features. The 12 lead ECG revealed right ventricle hyper- trophy ranging from mild to severe in 28 cases (56%).
Monitoring During Sleep
Sleep and Sleep States
In all subjects, sleep was disrupted by the breathing problems [9]. In 86% of the cases, there was a complete disappearance of stage 3 NREM sleep. REM sleep was present, but was decreased in 22% of the cases when compared to age-matched norms. The REM sleep decrease always was moderate; total REM sleep never fell below 16% of total sleep time (TST) (normal = 25% to 20%). Paradoxically, in 7 chil- dren (14%) who presented a mean AI of of 20.5, (i.e. who had intermittent ob- structive apnea and hypopnia during sleep), increased stage 4 NREM sleep was seen (i.e. an increase in total delta sleep). Percent of stage 1 NREM sleep was in- creased. Total movement-time during sleep was at times 100% to 250% higher than noted in control children. The total movement time index gives a good indication of the importance of the sleep disruption noted in severe cases and also in those with intermittent apnea. The combination of an initial disorder such as Trisomy 21 and a secondary sleep apnea syndrome led to very abnormal sleep patterns in some chil- dren.
Breathing Pattern During Sleep
Although the predominent pattern was of obstructive and subobstructive apnea, • there was not a single case where central or mixed apnea was not also observed dur- ing sleep. In some cases, these were minimal; in others, they represented up to 40% of the total respiratory abnormal episodes. In group I ("secondary"), patients w i th myotonic dystrophy, chiari malformation type I, syringomyelo-bulbia, and congeni- tal myxedema presented the highest percentage of central and mixed apnea (range 27% to 42%, mean = 36.7). Group II ("primary") patients also presented with mixed and central apnea (range from 1% to 34%).
The longest apneic and hypopneic pauses were observed during REM sleep. Oxygen saturation varied widely. All patients had oxygen saturation drops to under 60% in association with obstructive apneic events. The most severe oxygen desatu- ration, occurring for the longest period of time during sleep, was noted in the mas- sively obese patients (those with Prader-Willi Syndrome, Down's Syndrome, and
Obstructive Sleep Apnea in Children 281
i . R ° SLEEP APNEA
SECONDS
o . . . . . . . . ! ~,I . . . . . . . . . . . t . . . . . . . . . . . . " t~
6 . . . . . . . I . . . . . . . . . . . . . - . . . . . . . . . . . . . . . . . . . _ . . . . . . . . . . . . . . . . . . - _ _
iI
1 8 . . . . . . - - - . . . . . . . . . . . . . . . . . . - - . . . . . L . - . . . . . . . . . . , , . - . . . .
)I i'l r ,i I 2 4 . . . . - , - • . . . . . . . . " . . . . . . . . . . . . . . . . . . . .
I , ii ' 3 0 - - - - . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . - ...... .......
[r L !!_1200 msec_i, ' • 1~ ]t I~ 36 . . . . . . - . . . . . ~ . . . . . . . . . . . . . . . .
4 2 - - ' " . . . . . . . . . . . , . . . . . . . . . .
i, .... !~ ~ ,, ! ! i I'. ,ll '~ i - I - . ' I f '-,rl "i I'i _ ~,~ _ ~,.' .... ~,m._~,, o~o ~ ......... ,~ ............
r . . . . . . . . . . . . . . , . . . . . . . . , . . . . ; 1 0 0 0 ~
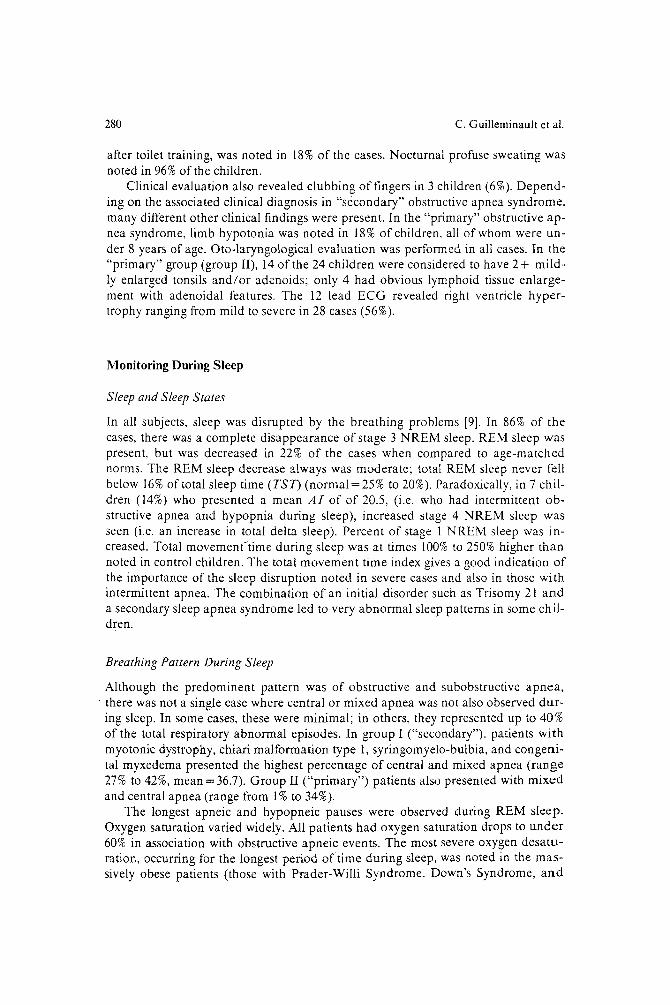
Fig. 1. Example of cardiac arrhythmia monitored in association with obstructive sleep apnea syndrome in a 16-year-old boy, obtained from a Holter ECG recorded simultaneously during polygraphic monitoring. The marked sinus arrhythmia and 2rid degree atrio-ventricular block are seen clearly
cases of prir~ary obstructive sleep apnea) and in patients with severe facial dys- morphia (severe retrognathia, Crouzon Disease, Pierre-Robin Syndrome).
Cardiac Abnormalities
All patients presented marked sinus arrhythmias in association with repetitive ap- nea during sleep (Fig. 1). Sinus arrests lasting from 2.5 to 9 s were noted in 52% of cases. Second degree atrio-ventricular block was noted in 14 children (28%). Parox- ysmal atrial tachycardia was noted in 8 children (16%) and short runs of ventricular tachycardia in 2 children (4%).
Hemodynamic Studies
Hemodynamic studies were not performed in all cases. Blood pressure recording during sleep was obtained in only 8 patients all of whom were 10 years of age or older. A progressive increase in blood pressure associated with repetitive apnea was noted. This increase, compared to baseline supine awake values, was at least 30 mm Hg (systolic) and 20 mm Hg (diastolic). The most significant increases were noted in patients with repetitive apnea.
Pulmonary arterial pressure was measured in only two patients who presented with myotonic dystrophy and major cardiac problems. An increase in pulmonary arterial pressure associated with obstructive sleep apnea was noted. This increase disappeared with resumption of intermittent bouts of normal air exchange [7].
282 C. Guitleminauk et al.
a . , ~ ^ o NOT C~STRUCTED ~v~ i OBSTRUCTED
E N D O E S O ~ / ~ ~ } ~,, / -*',
0 d~O O O o k ~ o o o o o o o • 4 r ~ O o o 4 o c l o • • • • • •
% CO. EXPRED- - - - - - - - - ' ~P " - -~ ,:~V'L"--~I~ ~ _ ~ J " g ' - ~ ,
b /
0 2 SATURATION J
EIXOOESOPHAGEAL . E~ c~ Hzo PRESSURE ' ' 'v'-',,--.,"~--,."",..~:'~,..~,"-..."
% CO 2 EXPIRED ~ -
PCOz k~m • 2•79nw,~ Hq
O B S T R U C T I V E S L E E P A P N E A • I. SaO 2
• ..% • .
"% i
%~- (".
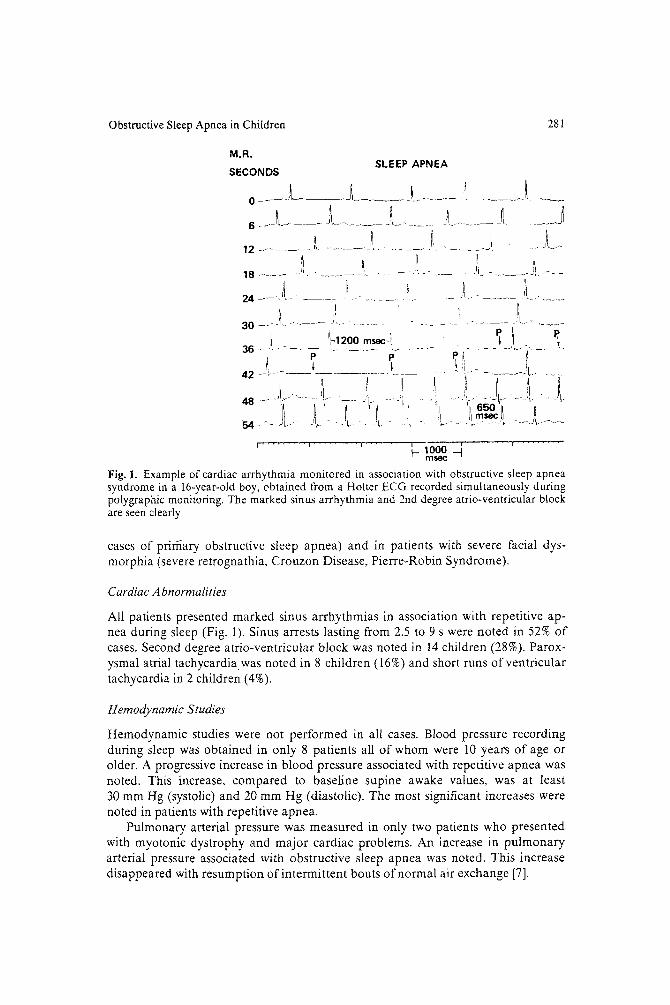
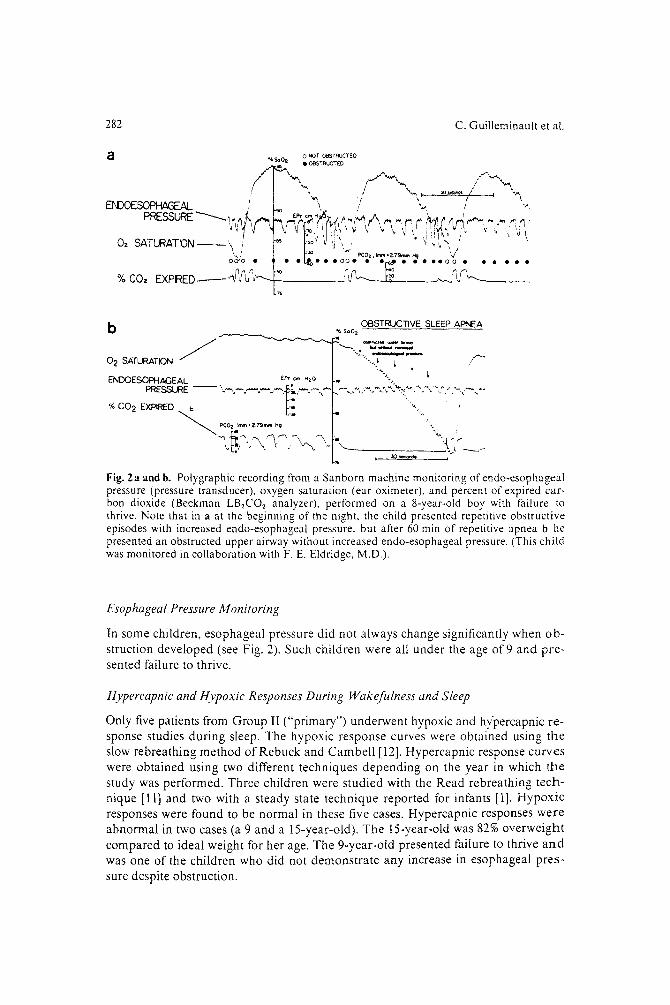
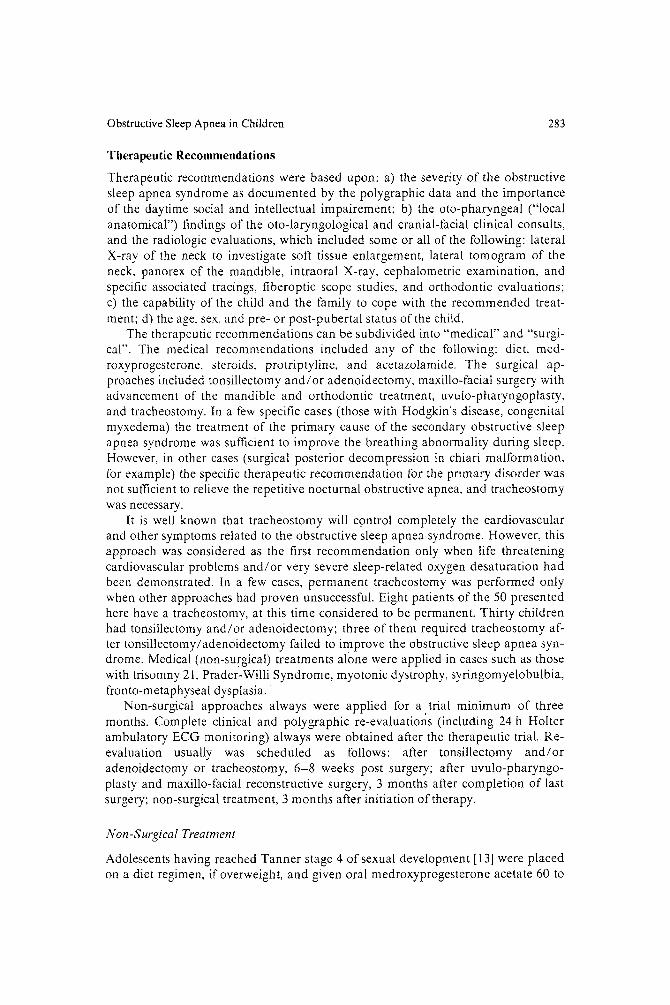
Fig. 2a and b. Polygraphic recording from a Sanborn machine monitoring of endo-esophageal pressure (pressure transducer), oxygen saturation (ear oximeter), and percent of expired car- bon dioxide (Beckman LB2CO2 analyzer), performed on a 8-year-old boy with failure to thrive. Note that in a at the beginning of the night, the child presented repetitive obstructive episodes with increased endo-esophageal pressure, but alter 60 min of repetitive apnea b he presented an obstructed upper airway without increased endo-esophageal pressure. (This child was monitored in collaboration with F. E. Eldridge, M.D.).
Esophageal Pressure Monitoring
In some children, esophageal pressure did not always change significantly when ob- struction developed (see Fig. 2). Such children were all under the age of 9 and pre- sented failure to thrive.
H)~pereapnic and Hypoxic Responses During Wakefulness and Sleep
Only five patients from Group II ("primary") underwent hypoxic and hfpercapnic re- sponse studies during sleep. The hypoxic response curves were obtained using the slow rebreathing method of Rebuck and Cambell [12]. Hypercapnic response curves were obtained using two different techniques depending on the year in which the study was performed. Three children were studied with the Read rebreathing tech- nique [11] and two with a steady state technique reported for infants [1]. Hypoxic responses were found to be normal in these five cases. Hypercapnic responses were abnormal in two cases (a 9 and a 15-year-old). The t5-year-old was 82% overweight compared to ideal weight for her age. The 9-year-old presented failure to thrive and was one of the children who did not demonstrate any increase in esophageal pres- sure despite obstruction.
Obstructive Sleep Apnea in Children 283
Therapeutic Recommendations
Therapeutic recommendations were based upon: a) the severity of the obstructive sleep apnea syndrome as documented by the polygraphic data and the importance of the daytime social and intellectual impairement; b) the oto-pharyngeal ("local anatomical") findings of the oto-laryngological and cranial-facial clinical consults, and the radiologic evaluations, which included some or all of the following: lateral X-ray of the neck to investigate soft tissue enlargement, lateral tomogram of the neck, panorex of the mandible, intraoral X-ray, cephalometric examination, and specific associated tracings, fiberoptic scope studies, and orthodontic evaluations; c) the capability of the child and the family to cope with the recommended treat- ment; d) the age, sex, and pre- or post-pubertal status of the child.
The therapeutic recommendations can be subdivided into "medical" and "surgi- cal". The medical recommendations included any of the following: diet, med- roxyprogesterone, steroids, protriptyline, and acetazolamide. The surgical ap- proaches included tonsillectomy and/or adenoidectomy, maxillo-facial surgery with advancement of the mandible and orthodontic treatment, uvulo-pharyngoplasty, and tracheostomy. In a few specific cases (those with Hodgkin's disease, congenital myxedema) the treatment of the primary cause of the secondary obstructive sleep apnea syndrome was sufficient to improve the breathing abnormality during sleep. However, in other cases (surgical posterior decompression in chiari malformation, tbr example) the specific therapeutic recommendation for the primary disorder was not sufficient to relieve the repetitive nocturnal obstructive apnea, and tracheostomy was necessary.
It is well known that tracheostomy will control completely the cardiovascular and other symptoms related to the obstructive sleep apnea syndrome. However, this approach was considered as the first recommendation only when life threatening cardiovascular problems and/or very severe sleep-related oxygen desaturation had been demonstrated. In a few cases, permanent tracheostomy was performed only when other approaches had proven unsuccessful. Eight patients of the 50 presented here have a tracheostomy, at this time considered to be permanent. Thirty children had tonsillectomy and/or adenoidectomy; three of them required tracheostomy af- ter tonsillectomy/adenoidectomy failed to imProve the obstructive sleep apnea syn- drome. Medical (non-surgical) treatments alone were applied in cases such as those with trisomny 21, Prader-Willi Syndrome, myotonic dystrophy, syringomyelobulbia, fronto-metaphyseal dysptasia.
Non-surgical approaches always were applied for a trial minimum of three months. Complete clinical and polygraphic re-evaluations (including 24 h Holter ambulatory ECG monitoring) always were obtained after the therapeutic trial. Re- evaluation usually was scheduled as follows: after tonsillectomy and/or adenoidectomy or tracheostomy, 6-8 weeks post surgery; after uvulo-pharyngo- plasty and maxillo-facial reconstructive surgery, 3 months after completion of last surgery; non-surgical treatment, 3 months after initiation of therapy.
Non-Surgical Treatment
Adolescents having reached Tanner stage 4 of sexual development [13] were placed on a diet regimen, if overweight, and given oral medroxyprogesterone acetate 60 to
284 C. Guilleminault et al.
80 mg daily. Acetazolamide or protriptyline were prescribed in addition in some cases, particularly during the initial 3 or 4 weeks of treatment. Such treatment was used, for example, in association with symptomatic medical regimens for acute car- diorespiratory failure. Steroids were tried in some of the younger children. Female adolescents received medroxyprogesterone acetate only after gynecologic consulta- tion and regular gynecologic follow-up had been arranged,
Post-Treatment Follow-Up
The longest follow-up obtained on the reported cases is now for 10 years, the mean follow-up is 2.5 years (range 12 months to 10 years). Very often, parents and chil- dren ceased to respond to follow-up appointment requests within two or three years of treatment, particularly in cases managed surgically.
Tonsillectomy and~or A denoidectomy Follow- Up
As mentioned, 3 children did not experience improvement and required tracheosto- my. Twenty seven children presented significant improvement within two months post-surgery. Some of them demonstrated spectacular increases in weight (up to 20% in young children -4 .5 kg). The mean weight increase was 7.2%. Height in- creases also were noticeable, particularly in children with failure to thrive (range 15 to 50 mm).
Polysomnography confirmed disappearance of apnea and oxygen desaturation. However, intermittent snoring was noted in 8 patients. Later follow-up of these 8 patients has revealed that snoring may worsen in association with upper respiratory allergies, and with physical fatigue or crying spells just before sleep onset. At a 3-year follow-up examination, one child presented intermittent obstructive hy- popnea with characteristic associated sinus arrhythmia.
Maxillo-Facial Surgery Follow-Up
Maxillo-facial surgery rarely has been performed at Stanford. In 4 cases, improve- ment was not sufficient and tracheostomy was necessary before symptoms were re- lieved. In 5 other cases, initial improvement was clear; however, our longest follow- up has been 6 months post-surgery and longer follow-up is not available due to dis- tance or other factors influencing the family.
Tracheostomy Follow- Up
Problems seen in adults also were noted in children [8]. During the first few months, there were local problems with inaccurately fitted tubes, low grade infections caus- ing tissue granulation, etc. Good understanding and cooperation on the part of the parents is critical if these problems are to be avoided. In children and adolescents, the major problems was depression secondary to surgery. Good familial support and, eventually, psychotherapy may be needed after surgery.

Obstructive Sleep Apnea in Children 285
Extended Tracheostomy Follow- Up
Two children who had tracheostomy performed at 12 and 14 years of age were fol- lowed for 9 and 8 years respectively. No long term local or psychological side effects were noted in 1981 at the time of the last evaluation. Both young adults were in- tegrated into their community and pursued active social and professional activities. One of them, who was considered to have intellectual impairment at the time of sur- gery, still presents a borderline IQ.
Non-Surgical Treatment Follow-Up
Three of the 4 children with Down's Syndrome and the myotonic dystrophy patients have had the longest follow-up (myotonic dystrophy, 5 years, trisomy 2l, 2-4 years, fronto-metaphyseal dysplasia, 18 months).
Intermittent snoring is noted in 2 of the 3 Down's Syndrome children, but hy- persomnolence and repetitive upper airway infections have disappeared. Oxygen saturation always was above 89% on follow-up polygraphic monitoring, and marked sinus arrhythmias or other cardiac arrhythmias were not observed during sleep.
Comments
Secondary obstructive sleep apnea syndrome can occur in association with many different abnormalities involving the oro-pharynx. Although not all subjects with such congenital abnormalities present a sleep apnea syndrome, it is necessary to consider the. effect of specific maxillo-facial malformations on breathing during sleep because of the possible impact on growth, intellectual development, and the cardiovascular system.
It is not clear how early in childhood obstructive sleep apnea can be noted. Tonkin et al. [14] have shown that some "near miss for SIDS" infants and some in- fants who have died of SIDS present anatomical abnormalities of the oropharynx. We have followed 5 near miss SIDS infants who progressively developed a clear cut obstructive sleep apnea syndrome with slightly enlarged tonsils and/or adenoids. Thus it appears that obstructive sleep apnea syndromes may have an impact very early in life and may lead to sudden death or to unexplained acute breathing prob- lems during sleep. In our series, none of the children were suspected of having ob- structive apnea during the first year of life; most of them presented significant im- pairment before a correct diagnosis was performed.
Also unexplained is the fact that failure to thrive is seen in the younger age groups, while obesity usually develops at a later age. Frequently, parental reports clearly establish the presence of heavy snoring during sleep before the development of obesity. The question of the long term side effects, particularly on intellect, of the obstructive sleep apnea syndrome is unresolved. There is no doubt that certain chil- dren present low or borderline IQ, but a question may be raised about the relation- ship of the initial event which led to the local problem and the mental deterioration. However, it is clearly recognized that sleep fragmentation, sleep deprivation, exces- sive daytime somnolence, and repetitive, sleep-related oxygen desaturation have an impact on learning and intellectual development. If obstructive sleep apnea syn-
286 C. Guilleminault et al.
drome is not the cause of the initial intellectual impairment in these children, it cer- tainly will worsen the already impaired capabilities. This was clearly demonstrated in our Down's Syndrome cases, where improvement of the obstructive sleep apnea syndrome led to much better social adaptation.
On major issue is what treatment should be recommended. Good objective documentation of the severity of the problem is required; nocturnal poly- somnography is an essential minimum test if tracheostomy is contemplated. Our approach has been conservative. All approaches that we know of. as mentioned above, have disadvantages. No-one has successfully analyzed the psychological im- pact on a child of, lbr example, tracheostomy. Therapeutic approaches must be weighed according to the age of the subject, the familial support available, and the capability of the child to understand the chosen approach. Depression sometimes has been a significant problem in our population. Certain errors can be avoided when tracheostomy is judged to be necessary; for example, a nonfenestrated tube should not be used. particularly when the child is young, because this will prevent others hearing a child who awakens crying in the middle of the night from a night- mare. A young subject may not know or remember how to place a finger in front of the open tracheostomy tube so as to make him/herself audible. A non-fenestrated tube thus can cause the subject to feel isolated and may lead to psychiatric dis- turbances. Further, absence of fenestration may lead to abrupt choking sensations while awake. It is necessary to follow a child with a tracheostomy regularly, to be sure that the tube is the correct size.
Other therapeutic approaches can be tried. In our experience, these may be suc- cessful at least for a few years. Drug treatment may work for only a limited period, and surgery may be required eventually; however, the surgery then will be per- formed on a child who ig~older and has a better understanding of the problem re- quiting surgery.
One other point should be emphasized. In our population, there were chil- dren who very quickly ceased to fight obstruction; i.e. there was no increase in esophageal pressure during an obstructive apneic event after the first 30 to 60 rain of sleep. Is this due to "fatigue" on the part of the diaphragmatic muscles? Such was the finding in adults with long obstructive event [4]. Or are the receptors being "re- set" to a level such that they l~ail to respond to an obstruction and its consequences, and no motor response is triggered? Might there be another mechanism? These questions require an answer. We find it interesting that we have noted this lack of response in children presenting with failure to thrive and/or decreased hypercapnic response while awake.
Although these issues and questions are unresolved, it is important to remember that obstructive sleep apnea syndrome in children is not uncommon. Considering the cardiovascular and intellectual impact of the syndrome, tests for it should be performed as soon as it is suspected.
Acknowledgements. This work was supported in part by a grant from the KROC foundation and by INSERM to CG. We acknowledge the technical help of S. Coons, R. Baldwin, S. Co- burn, D. Zeiger and the editorial assistance ofL. Dupr+.

Obstructive Sleep Apnea in Children 287
References
1. Ariagno R, Nagel L, Guilleminault C (1980) Waking and ventilatory responses during sleep in infants and near-miss for sudden infant death syndrome. Sleep 3:351-361
2. Carskadon MA, Harvey K, Dement WC, Guilleminault C. Simmons FB, Anders TF (1978) Respiration during sleep in children. West J Med 128:477-481
3. Gastaut H, Tassinari CA, Duron B (1966) Polygraphic study of episodic diurnal and noc- turnal (hypic and respiratory) manifestations of the Pickwick Syndrome. Brain Res 1:167-186
4. Guitleminault C (1980) Sleep apnea syndromes: impact of sleep and sleep states. Sleep 3:227-234
5. Guilleminault C, Cummiskey J, Motta J (1980) Chronic obstructive airflow disease and sleep studies. Am Rev Respir Dis 122:397-406
6. Guilleminault C, Eldrige F, Simmons FB, Dement WC (1976) Sleep apnea in eight chil- dren. Pediatrics 58:23-30
7. Guilleminault C, Eldrige F, Simmons FB, Dement WC (1975) Sleep apnea syndrome: can it induce hemodynamic changes? West J Med t23: 7-16
8. Guilleminault C, Simmons B, Motta J, Cummiskey J, Rosekind M, Schroeder JS, Dement WC (1981) Obstructive sleep apnea syndrome and tracheostomy: long term follow-up ex- perience. Arch Intern Med 141:985-988
9. Guilleminault C, Tilkian AG, Dement WC (1976) Sommeil et respiration dans le syn- drome "apnee au cours du sommeil" chez l'enfant. Electroencephalgr Clin Neurophysiol 41 : 367-378
10. Guilleminault C, van den Hoed J, Mitler M (1978) Clinical overview of the sleep apnea syndromes. In: Guilleminault C, Dement W (eds) Sleep apnea syndromes, Alan R. Liss, Inc, New York, pp 1-12
tl. Read DJC (1976) A clinical method for assessing ventilatory response to carbon dioxide. Aust Ann Med 16:20-32
12. Rebuck AS, Cambell EJM (1974) A clinical method for assessing the ventilatory response to hypoxia. Am Rev Respir Dis 109:345-350
13. Tanner JM-(1962) Growth in adolescence (2nd edn). Blackwell, Oxford 14. Tonkin SL, Stewart JH, Withey S (1980) Obstruction of the upper airway as a mechanism
of sudden infant death syndrome: evidence for a restricted nasal airway contributing to pharyngeal obstruction. Sleep 3:375-383
Accepted for publication: 15 June 1981
Related Documents