Shopping for Healthcare: A Retailer's Foray Into Healthcare Service Delivery in the United States Citation Christie, Gillian Pepall. 2020. Shopping for Healthcare: A Retailer's Foray Into Healthcare Service Delivery in the United States. Doctoral dissertation, Harvard T.H. Chan School of Public Health. Permanent link http://nrs.harvard.edu/urn-3:HUL.InstRepos:42676024 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA Share Your Story The Harvard community has made this article openly available. Please share how this access benefits you. Submit a story . Accessibility

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Shopping for Healthcare: A Retailer's Foray Into Healthcare Service Delivery in the United States
CitationChristie, Gillian Pepall. 2020. Shopping for Healthcare: A Retailer's Foray Into Healthcare Service Delivery in the United States. Doctoral dissertation, Harvard T.H. Chan School of Public Health.
Permanent linkhttp://nrs.harvard.edu/urn-3:HUL.InstRepos:42676024
Terms of UseThis article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA
Share Your StoryThe Harvard community has made this article openly available.Please share how this access benefits you. Submit a story .
Accessibility

SHOPPING FOR HEALTHCARE: A RETAILER’S FORAY INTO
HEALTHCARE SERVICE DELIVERY IN THE UNITED STATES
GILLIAN PEPALL CHRISTIE
A Doctoral Thesis Submitted to the Faculty of
The Harvard T.H. Chan School of Public Health
in Partial Fulfillment of the Requirements
for the Degree of Doctor of Public Health
Harvard University
Boston, Massachusetts
May 2020

“To write prescriptions is easy, but to come to an understanding of people is hard.”
– Franz Kafka
The Country Doctor (1919)
ii
Thesis Advisor: Dr. Kimberlyn Leary Gillian Pepall Christie
Shopping for Healthcare: A Retailer’s Foray into Healthcare Service Delivery in the United States
ABSTRACT
The healthcare system in the United States (US) is broken for consumers. It is built on a complex
web of relationships between powerful entities that often exclude the consumer. This can translate into a
poor – and at times disheartening – experience for consumers. Three problems underpin the brokenness of
the healthcare system for consumers: (1) healthcare costs are high and rising; (2) access and convenience to
basic healthcare services are lacking; and (3) the quality of healthcare services is often poor and variable.
Walmart, the major American retailer, is interested in changing the delivery of healthcare in the US.
In September 2019, Walmart opened its first Walmart Health Center in Dallas, Georgia. It offers several basic
healthcare services under one roof – primary care, dental, audiology, vision, behavioral health, and others – at
transparent and affordable prices. The Walmart Health Center accepts insurance and provides reasonable
cash prices for consumers who may be uninsured. It operates with extended hours and is led by a team of
medical professionals from the local community.
With a desire to test, learn, iterate, and eventually expand, Walmart was interested in understanding
the integration and optimization of primary care services at its Walmart Health Center. Integration of basic
healthcare services could allow the company to reduce healthcare costs, provide an accessible and convenient
healthcare experience, and offer high-quality healthcare to consumers. The project had two aims: (1) to
understand existing models of primary care that integrate several services under one roof; and (2) to
determine how Walmart Health could better integrate the healthcare services at its Walmart Health Center.
Based on a series of qualitative interviews, this project established two major conclusions. The first is
that the current landscape of primary care models is influenced by several contextual characteristics that
determine the extent of integration. The second is that the Walmart Health Center has the foundational

iii
structures, operations, and workflows to support the effective integration of primary care services. Given the
early stages of Walmart Health’s operational life, several recommendations are offered to provide a roadmap
for effective integration of basic healthcare services.
iv
TABLE OF CONTENTS
ABSTRACT………………………………………………………………………………………….…… ii
LIST OF FIGURES ……..………………………………………………………………………….…… v
LIST OF TABLES ……………………………………………………………………………………… vi
ACKNOWLEDGMENTS …………………………………………………………………………..…. vii
1.0 INTRODUCTION ……………………………………………………………………………... 1
2.0 ANALYTICAL PLATFORM …………………………………………………………………... 3
2.1 Problem Statement ………………………………………………………………………. 3
2.2 Host Organization ………………………………………………………………….……. 4
2.3 Literature Review ……………………………………………………………………...…. 8
2.4 Theory of Change ………………………………………………………………………. 20
2.5 Methodology …………………………………………………………………………… 24
3.0 RESULTS …………………………………………………………………………………….... 28
3.1 Framing of Results ……………………………………………………………...……..... 28
3.2 The Current Landscape of Integrated Primary Care ……………………………..……… 30
3.3 Integration of Primary Care Services at the Walmart Health Center …………………….. 40
4.0 DISCUSSION & RECOMMENDATIONS …………………………………………………. 50
4.1 Discussion ……………………………………………………………………………… 50
4.2 Recommendations ………………………………………………………………….…... 55
5.0 CONCLUSION …………………………………………………………………………..…… 61
6.0 BIBLIOGRAPHY ……………………………………………………………………………... 63
7.0 APPENDIX ……………………………………………………………………………………. 70
7.1 Important Events in Walmart’s History ……………………………………………….... 70
7.2 Interview Guide …………………………………………………………………...….… 71
7.3 Interview Confidentiality Form ………………………………………………………… 72

v
LIST OF FIGURES
Figure 1: A Comprehensive Theory of Integration (Singer et al., 2018)
vi
LIST OF TABLES
Table 1: Walmart 2019-2020 Select Announcements on Public Health
Table 2: Partner Services at the Walmart Health Center in Dallas, GA
Table 3: Definition and Features of Integrated Care by Select Stakeholders
Table 4: Five Levels of Systemic Collaboration
Table 5: Descriptions of Classifications & Types of Integration (Adapted from Singer et al., 2018)
Table 6: Descriptions of Thought Leaders Interviewed on Integration of Primary Care Services
Table 7: Positions of Associates Interviewed at Walmart Health Center
Table 8: Summary of Research Methodology
Table 9: Thought Leader Criteria for Integration of Primary Care Services
vii
ACKNOWLEDGMENTS
This work would not have been possible without the support and encouragement of several people
who have made my time at Harvard an overwhelming success.
My Committee: My Committee Chair, Dr. Kim Leary, who has truly been a thoughtful mentor, guiding
light, and sounding board throughout my time at Harvard. Drs. Meredith Rosenthal and Robert Huckman,
who completed my outstanding Committee, it has been a tremendous pleasure to work with you. Thank you.
Harvard Faculty: Beyond my Committee, I am immensely grateful to several Harvard professors who
have pushed me to pursue new frontiers in public health. Thank you to Rick Siegrist for his guidance in
helping me navigate the DrPH as well as to Dr. John McDonough, who has expanded my thinking on the
role of business in health. Thank you.
Walmart Team: My team at Walmart Health – Marcus Osborne, Evan Schnur, and Marina Kusserow –
I could not have asked for a better experience. You have indulged my learning, fostered my interests, and
exposed me to the possibilities of the biggest company in America. Thank you.
My Family: Lastly, I would not be where I am without the enduring love of my family and partner.
Mom, Dad, and Fraser, thank you for encouraging me on this journey, and pushing me to become a better
person every day. Andrew, thank you for always helping me see the light through the highs and lows. Thank
you.
1
1.0 INTRODUCTION
The United States (US) healthcare system is broken for consumers. The experience of receiving
multiple basic preventive care services – an annual physical exam and a routine dental cleaning for instance –
can be overly complicated. A person is required to coordinate visits to the doctor and the dentist, each of
whom operate independently and are paid separately. Appointments may be scheduled at inconvenient times
during the workday or take place at different locations. Additional tests (such as laboratory services) may be
in another facility. Finally, the cost of the services may be unknown prior to, or immediately after, the
appointment. For consumers, the US healthcare system can be costly, inconvenient, and variable in the
quality of care received.
Several attempts have been made to improve the consumer experience in healthcare. One recent
example has been Walmart, the major American retailer. Shortly before his death in 1992, Walmart’s founder
and long-time CEO, Sam Walton, presented a vision to change the delivery of healthcare that would “start
saving our customers money and our employees money” (Walton, 1991 cited in Lytle, 2017). Almost thirty
years later in September 2019, Walmart opened the first Walmart Health Center (“the Center”) in Dallas,
Georgia. Dallas is a community of about 13,000 people around 30 miles northwest of Atlanta. Connected to a
Walmart supercenter, the Center offers convenient and accessible healthcare services at affordable prices.
Basic healthcare services such as primary care, dental, audiology, vision, and behavioral health are offered to
all customers – those who are commercially insured, on Medicare, Medicaid, the ACA, or uninsured. Walmart
intends to expand its Centers in the coming years.1
With one Center in operation at the close of 2019 and more planned for 2020 and beyond, Walmart
was interested in testing, learning, and optimizing its operations. This project intended to inform the
company’s strategic agenda as they considered geographic expansion across the US. The project had two
aims: (1) to understand existing models of primary care that integrate several services under one roof; and (2)
1 The ACA refers to the Patient Protection and Affordable Care Act of 2010. It was the signature legislation of President Barack Obama, and is also referred to as “Obamacare.” It had three main goals: (1) make affordable health insurance available to more people; (2) expand Medicaid to cover adults with incomes below 138 percent of the federal poverty level; and (3) support innovative medical care delivery methods that can lower the cost of healthcare.
2
to determine how Walmart Health could better integrate the healthcare services offered at its Walmart Health
Center. Two research questions supported these aims:
RQ 1: What is the current landscape of integrated primary care services in the US?
RQ 2: How can the integration of primary care services be optimized at Walmart Health?
To explore these research questions, I spent eight months as a Doctoral Intern at Walmart Health
during my final year of the Doctor of Public Health (DrPH) program at the Harvard T.H. Chan School of
Public Health. I was not based at Walmart’s headquarters, though I traveled regularly to their offices in
Bentonville, AR and Hoboken, NJ as well as to the Center in Dallas, GA. I reported to Walmart Health’s
Vice President of Health Transformation, who was tasked with leading the development and execution of the
Centers. As a doctoral candidate at Harvard and an associate at Walmart Health, I have attempted to be
objective in my reflections, though am cognizant that my contractual status with the company may introduce
bias. Where I recognize bias in my writing, I have tried to minimize it.
This project examined the integration of primary care services in the US. It focused on the
integration of activities inside a primary care practice (the Walmart Health Center), including services such as
primary care, behavioral health, and oral health. Out of scope was an exploration of how Walmart Health may
integrate with other stakeholders in the healthcare system (such as hospitals, physician practice groups or
specialty referral networks). The dissertation includes three main sections: an analytical platform, results, and
a conclusion. The analytical platform provides a description of the problem, an overview of the host
organization, a review of salient literature, an outline of the theory of change, and an explanation of the
research methodology. Results discuss the findings of the project by demonstrating connections between the
problem statement, literature review, and theory of change. The conclusion presents a discussion and
recommendations for advancing strategy and operations to integrate primary care services.

3
2.0 ANALYTICAL PLATFORM
2.1 Problem Statement
The US healthcare system is broken for consumers. It is built on a complex web of relationships
between powerful entities that often exclude the consumer: health insurers, employers, providers, and the
government. This can translate into a poor – and at times disheartening – experience for consumers
navigating the system. From the consumer’s perspective, three main problems underpin the brokenness of
the healthcare system:
(1) Healthcare costs are high and rising: The US spends approximately 17.7 percent ($3.6 trillion) of gross
domestic product (GDP) on healthcare, the highest among comparable high-income countries (CMS,
2019; Bradley & Taylor, 2013). Annual out-of-pocket costs have increased 54 percent (from $525 to
$806) over the past decade, almost two times faster than wages (Claxton et al., 2018). An estimated
137 million Americans struggle with medical debt, while 64 percent of consumers have delayed
receiving care because of cost (Yabroff et al., 2019; Heath, 2018).
(2) Healthcare access and convenience are lacking: The availability and accessibility of healthcare services
remains uneven across the country. Rural geographies (which include nearly 1,000 Walmart stores) –
often characterized by individuals with lower incomes and poorer health outcomes – are affected by
shortages in healthcare services and longer distances to facilities (Warshaw, 2017). Approximately 30
million people are uninsured with no usual source of care, and consumers often travel between 50
and 100 miles for basic services in rural areas (Tolbert et al., 2019). Rural hospitals are also struggling
to stay afloat, with 168 closing across the country since 2010 (Cecil G. Sheps Center for Health
Services Research, 2020).
(3) Healthcare quality is poor and prices opaque: Healthcare services are often of poor and variable quality.
More than 80 percent of consumers report being unsatisfied with their healthcare experience, while
75 percent of frequent healthcare consumers cite frustration with the system (GE Healthcare, 2017).

4
Younger generations are also more dissatisfied with the status quo of healthcare, while older
generations are becoming more willing to use non-traditional methods for receiving services (Safavi,
Webb & Kalis, 2019). Prices of basic healthcare services are not usually transparent to consumers
prior to receiving them.
Realizing the brokenness of the US healthcare system for consumers, several market participants –
from the smallest of start-ups to the largest of corporations – have entered the healthcare industry. This
project focuses on the delivery of basic healthcare services to all Americans (the commercially insured,
Medicare, Medicaid, ACA, and the uninsured) by a major American retailer, Walmart. Walmart’s initiatives to
expand access to healthcare services is an experiment in delivering more value in healthcare for a lower cost.
2.2 Host Organization
2.2.1 An Introduction to Walmart
Founded in 1962 by Sam Walton, Walmart is a major American retailer that sells general merchandise
at low prices. Walmart operates in 27 countries under 58 banners, along with eCommerce websites in ten
countries. In the US, Walmart has 4,700 stores, and an estimated 90 percent of the population resides within
ten miles of a retail location. Around 150 million Americans – half of the US population – interact with the
company each week, shopping for food, bicycles, garden equipment, and other merchandise. In the US,
Walmart is the largest retailer of food, the largest private employer (with 1.5 million associates and 2.2 million
globally), and generated $514.4 billion in revenue in the last fiscal year. The company remains headquartered
in Bentonville, AR. Appendix A outlines major milestones in the company’s history.
Walmart’s operating philosophy is predicated on delivering the best value at the lowest price to the
customer. Customers vote with their feet and clicks, and have options in the market as to where to spend their
dollars. Decisions made by the company attempt to fulfill the needs, wants, and desires of American consumers.
Sam Walton’s memoir notes the importance of placing the customer at the center of the business:
5
For my whole career in retail, I have stuck by one guiding principle. It’s a simple one, and I have repeated it over and over and over … the secret of successful retailing is to give your customers what they want. Sam Walton (cited in Huey, 1992:173)
This focus on the customer has led Walmart to sell a wide assortment of merchandise at the lowest
possible price.2 Walmart sells more than 60,000 products in their stores, and more than 120,000 products in
their supercenters (Fishman, 2006). The company’s retail experience has been predicated on guaranteed
satisfaction, convenient hours, and free parking, so that customers can “Save Money. Live Better.”
The company’s rapid growth and scale has led to the “Walmart Effect.” This refers to the ways in
which Walmart has changed businesses, work, communities, and everyday life in the US and many countries
around the world (Fishman, 2006). As Fishman (2006: 5) describes: “Walmart shapes where we shop, the
products we buy, the prices we pay – even for those of us who never shop there.” Walmart sets the pace of
retail, and many consider its performance to be a vital indictor of the strength of the US economy (Fishman,
2006).
2.2.2 Walmart and Public Health
Walmart’s foray into public health and healthcare started in 1978, with the opening of its pharmacy
operations. The company has since expanded its health offerings to include several products and services at
its retail locations and online. This includes pharmacies at most Supercenters with a $4 generic drug program;
1,300 vision centers that provide eye examinations, prescription eyewear and contact lenses, and other eye
care services; 19 retail care clinics that provide primary care services in Georgia, South Carolina, and Texas;
health insurance resources during Annual Enrollment Period; Wellness Days that complete basic health
screenings; and a wide array of general health and wellness products sold in-store and online.
In recent months, Walmart has made several strategic decisions that affect public health (Table 1).
Most noteworthy has been changes in Walmart’s firearms policies following two shootings in two stores in
2 Walmart’s focus on providing the lowest price to consumers has led to controversial wage policies for associates. Although starting hourly wages have increased in recent years (to $11/hour in 2018) and the company continues to test different wage models (such as $12/hour for 500 stores), Walmart has come under substantial criticism for these practices from labor unions and activists. In protest, the long-time senator and democratic presidential candidate, Bernie Sanders, attended Walmart’s Shareholders Meeting in June 2019 to encourage the company to raise their wages.

6
Southaven, MI and El Paso, TX in July and August 2019. One month thereafter, Walmart announced
modifications to its firearms policy to not sell handguns and select ammunition, and to ban open carry in
stores. Following this announcement, several other retailers – such as CVS, Walgreens, and Kroger –
followed suit. This represents Walmart’s leadership in the market as well as the company’s ability to spur
collective impact among other large retailers (Thomas, 2019).
Table 1: Walmart 2019-2020 Select Announcements on Public Health
Date & Issue Source Headline
Aug 29: Walmart Health CNBC Walmart tests dentistry and mental care as it moves deeper into primary health
Sept 3: Firearm Policy New York Times Walmart to Limit Ammunition Sales and Discourage ‘Open Carry’ of Guns in Stores
Sept 19: Business Roundtable Leadership
Reuters Walmart’s Chief Executive to Chair the Business Roundtable
Sept 20: E-cigarette Ban New York Times Walmart to End Sales of E-Cigarettes as Vaping Concerns Mount
Sept 24: Healthcare Education Offerings
Reuters Walmart expands $1 a day education program to deepen push in healthcare
Oct 3: Associate Healthcare Benefits
Bloomberg Walmart Rolls Out Slew of New Health-Care Benefits for Employees
Jan 23: Gym Benefits for Associates
Fox Business Walmart debuts gym memberships for ‘$9 a paycheck
Jan 26: Wage Increases for Select Associates
Associated Press Walmart is raising starting hourly wage to $12 at 500 stores to lure workers, aid service
Feb 17: Environmental Footprint
Forbes Walmart Challenges Amazon On Sustainable Packaging
Walmart also indirectly impacts public health nationally and internationally through their
environmental and social initiatives. Starting in 2004, the company began changing its approach to society,
and was instrumental in the disaster response to Hurricane Katrina in 2005 (Porter & Ramirez-Vallejo, 2019).
Today, Walmart is frequently among the first relief respondents on the ground delivering food, water, and
other products to support victims of natural disasters. Other initiatives such as Project Gigaton, which aims
to remove 1 billion metric tons of emissions in Walmart’s value chain by 2030, impacts the public health of
associates and communities in the US and around the world.
2.2.3 The Launch of Walmart Health
On September 13, 2019, Walmart announced Walmart Health. Walmart Health aims to provide
customers with access to a simple, convenient, affordable, and integrated healthcare experience. The company
7
opened its first 10,000-square-foot healthcare center in September, while the second site opened in January
2020. Both Walmart Health Centers are at Walmart stores in Dallas and Calhoun, Georgia.3 Walmart intends
to use the Dallas and Calhoun sites to “test and learn,” with the goal of expanding its healthcare footprint to
other communities.
Walmart Health offers several healthcare services under one roof. This includes primary care,
diagnostics, X-ray, behavioral health, dentistry, optometry, audiology, pharmacy, insurance, and home health
services. It also includes a community room to provide physical activity and nutrition classes, as well as
mobile mammography services. As Sean Slovenski, Senior Vice President and President, Health and Wellness,
Walmart US, described at the launch of Walmart Health:
We opened our first-ever Walmart Health center in Dallas, Georgia, working with partners to provide key services such as primary care, labs, X-ray and EKG, counseling, dental, optical, hearing and community health education, all at low, transparent pricing, regardless of customers’ insurance status - the first time all these services are in one facility. Sean Slovenski (2019)
The Center is staffed by primary care physicians (PCPs), nurse practitioners (NPs), medical assistants
(MAs), licensed professional counselors, dentists, and community health workers (CHWs). Walmart had
piloted the services individually at other stores, and several services were still offered by partner organizations
at the Center. The Community Room, for example, is offered by Tivity Health, a provider of nutrition,
physical activity, and social engagement solutions, while the insurance agent is employed by MarketPoint, a
subsidiary of Humana, the large health insurer. The CHWs live within the community and are intended to
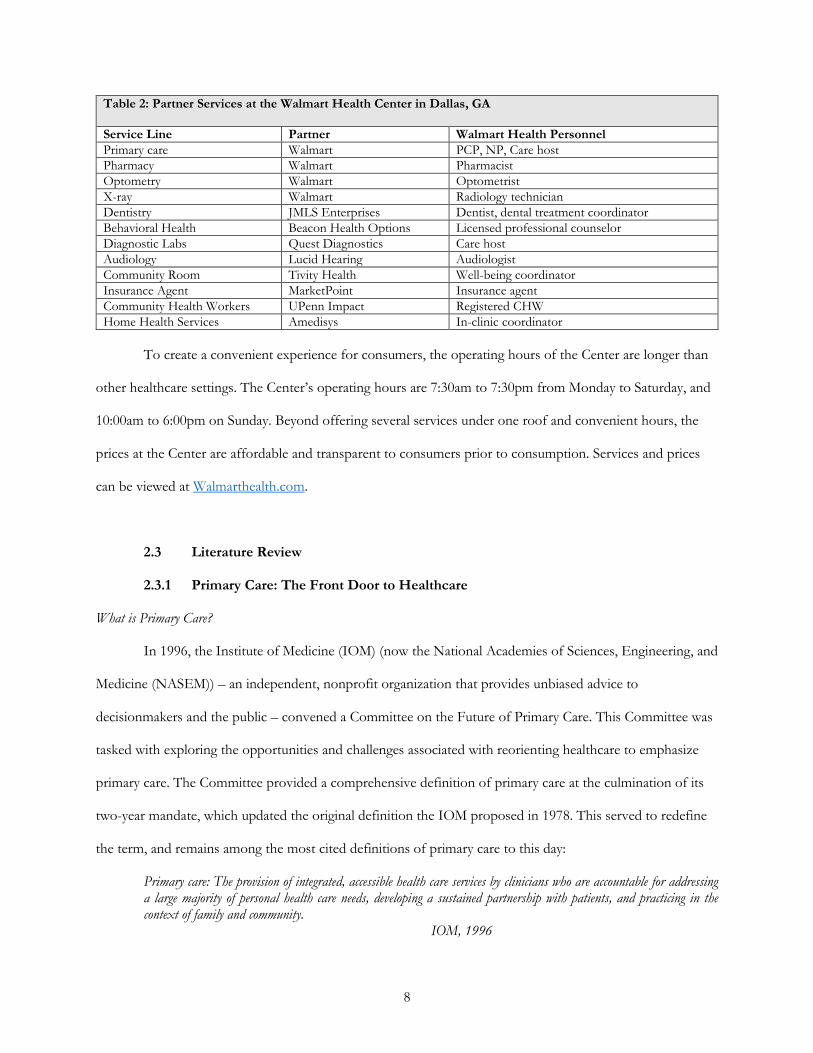
direct patients to local community-based organizations when needed. Table 2 demonstrates the partners
providing services as well as personnel at the Center.
3 Dallas is about 30 miles from Atlanta, while Calhoun is another 45 miles north of Dallas. Georgia was selected as the pilot site for Walmart Health because of its poor access to services and health outcomes. The state has commonly been referred to as a “medical desert” – a term describing geographic areas with inadequate access to affordable yet high-quality healthcare (Nelson, 2016). Of Georgia’s 159 counties, eight fail to have a physician; 63 do not have a pediatrician; 75 do not have an OB/GYN; and 95 do not have a psychiatrist (Harker, 2019). The lack of access to medical care has contributed to among the poorest health outcomes in the country. America’s Health Rankings, which ranks states based on indicators of health behaviors, community and environment, policies, and clinical care, places Georgia number 40 of all states on overall health, and 43 out of 50 states on clinical quality (United Health Foundation, 2019). Overall, the health status of the population and access to healthcare services in Georgia remains poor relative to other states, with entrenched geographic and racial disparities.
8
Table 2: Partner Services at the Walmart Health Center in Dallas, GA
Service Line Partner Walmart Health Personnel
Primary care Walmart PCP, NP, Care host
Pharmacy Walmart Pharmacist
Optometry Walmart Optometrist
X-ray Walmart Radiology technician
Dentistry JMLS Enterprises Dentist, dental treatment coordinator
Behavioral Health Beacon Health Options Licensed professional counselor
Diagnostic Labs Quest Diagnostics Care host
Audiology Lucid Hearing Audiologist
Community Room Tivity Health Well-being coordinator
Insurance Agent MarketPoint Insurance agent
Community Health Workers UPenn Impact Registered CHW
Home Health Services Amedisys In-clinic coordinator
To create a convenient experience for consumers, the operating hours of the Center are longer than
other healthcare settings. The Center’s operating hours are 7:30am to 7:30pm from Monday to Saturday, and
10:00am to 6:00pm on Sunday. Beyond offering several services under one roof and convenient hours, the
prices at the Center are affordable and transparent to consumers prior to consumption. Services and prices
can be viewed at Walmarthealth.com.
2.3 Literature Review
2.3.1 Primary Care: The Front Door to Healthcare
What is Primary Care?
In 1996, the Institute of Medicine (IOM) (now the National Academies of Sciences, Engineering, and
Medicine (NASEM)) – an independent, nonprofit organization that provides unbiased advice to
decisionmakers and the public – convened a Committee on the Future of Primary Care. This Committee was
tasked with exploring the opportunities and challenges associated with reorienting healthcare to emphasize
primary care. The Committee provided a comprehensive definition of primary care at the culmination of its
two-year mandate, which updated the original definition the IOM proposed in 1978. This served to redefine
the term, and remains among the most cited definitions of primary care to this day:
Primary care: The provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community.
IOM, 1996

9
The Committee recommended this definition be adopted by all stakeholders engaged in delivering
and financing primary care as well as by institutions responsible for educating and training primary care
providers. Beyond offering a definition, the Committee further outlined the value of primary care to the
healthcare system and the health of populations. They suggested that: (1) primary care is the logical
foundation of a well-functioning healthcare system; and (2) primary care is pivotal to attaining the objectives
of high-quality care, patient satisfaction, and efficient use of resources, commonly considered the objectives
of any healthcare system (IOM, 1996). Primary care has been associated with improvements in the quality of
care, patient experiences, and outcomes such as lower mortality as well as lower levels of spending (Song &
Gondi, 2019). The gains provided to a population’s health from access to primary care are substantial, as
suggested by the 1996 IOM report. The report proposed five areas in which primary care delivers value to
individuals:
1. It provides a place to which patients can bring a wide range of health problems for appropriate attention—a place in which patients can expect, in most instances, that their problems will be resolved without referral.
2. It guides patients through the health system, including appropriate referrals for services from other health professionals.
3. It facilitates an ongoing relationship between patients and clinicians and fosters participation by patients in decisionmaking about their health and their own care.
4. It provides opportunities for disease prevention and health promotion as well as early detection of problems. 5. It helps build bridges between personal health care services and patients' families and communities that can assist
in meeting the health needs of the patient. IOM, 1996
Access to primary care services has been shown to help fulfill the “quadruple aim” of healthcare:
high-quality care that is lower cost, delivers better health, and an improved experience for clinicians (Pham &
Greiner, 2019). A higher concentration of primary care providers has generated better health outcomes and
care quality, lower medical expenditures, and more equitable health outcomes (Ellner & Phillips, 2017). In
one such study, an increase of ten PCPs per 100,000 people was associated with increased life expectancy of
more than 2.5 times than that associated with similar increases in the density of non-PCPs (Basu et al., 2019).
Similarly, as the concentration of PCPs decreases, there is a relative increase in the number of deaths
attributed to preventable causes, and an average loss of life expectancy of 51.5 days (Zabar, Wallach & Kalet,
2019). While the value of primary care is compelling, its functions are commonly underutilized.
10
(Under) Utilization of Primary Care
Although an estimated 80 to 90 percent of a population’s health needs throughout life can be
provided by primary care – ranging from maternity care and disease prevention to vaccinations and palliative
care – the percentage of Americans with access to a primary care provider has largely not changed in 20 years
(76 percent in 2015 versus 77 percent in 1996) (The Lancet, 2019). Primary care also represents a meagre 5 to
7 percent of total healthcare spending in the US (Pham & Greiner, 2019).
Among the reasons underpinning the underutilization of primary care is the shift into high-
deductible health plans by many Americans. Traditional health plans support primary care visits for a small
co-payment. In contrast, high-deductible health plans charge the patient for utilizing any health service until
an annual deductible has been met. In 2007, 15 percent of the US population was in a high-deductible health
plan, while that increased to 43 percent in 2017 (Cohen & Zammitti, 2018).
Combined with subpar utilization by patients are low revenue streams and high levels of
unreimbursed labor for PCPs. The well-known American surgeon with extensive expertise in healthy policy
and management, Dr. Atul Gawande, suggests that the American healthcare industry is divided by
incremental and interventionist medicine (Gawande, 2017). Primary care professionals provide incremental
medicine, meaning the value provided is based on improving people’s lives over extended periods of time. In
contrast, interventionist medicine includes specialty doctors who generate revenue simply based on
procedures. Gawande goes so far as to note the “100% difference” in incomes between these types of
physicians – PCPs take home half as much as specialists. The poor incomes and revenue provided to primary
care practices has led many to struggle to maintain financial sustainability (Basu et al., 2015).
Shortages of Primary Care Physicians
The current and impending shortages of PCPs are well-established. By 2030, it is estimated there will
be a shortage of up to 49,300 PCPs in the US (Dall et al., 2018). In most other high-income countries, the
ratio of specialists to PCPs is 30:70. In the US, only 35 percent of all physicians (including NPs and physician
assistants (PAs)) deliver primary care (Lazris, Roth & Brownlee, 2018).
11
Shortages of PCPs are further affected by the steady decline in medical school graduates entering
primary care (Zabar, Wallach & Kalet, 2019). Even fewer PCPs are attracted to practice in rural areas. Today,
only 20 percent of all medical students enter primary care fields such as family medicine, general internal
medicine, and pediatrics. Furthermore, many of these recent graduates end up in urgent care facilities rather
than practicing primary care in the community (Lazris, Roth, Brownlee, 2018). A combination of lower
incomes, desired level of debt, type of patients cared for, and perceived work hours, have contributed to
fewer medical students pursuing primary care (Schwartz et al., 2011). Residency placements for primary care
are fewer than specialist care, with selected medical schools not even placing a single student into a primary
care residency (Bodenheimer, 2006). While early training programs and loan forgiveness have encouraged
recently graduated PCPs to practice in rural areas, low levels of reimbursement and high administrative tasks
and reporting burdens that often monopolize patient interactions have led to careers that are difficult to
sustain with low satisfaction (Raymond & Vinson, 2017). Symptoms of burnout are reported by more than 50
percent of PCPs (Peckham, 2015).
2.3.2 Primary Care Delivered Outside the Hospital’s Four Walls
Growing Consumerism in Healthcare
A small yet growing cadre of consumers are demanding choice, convenience, and fair and transparent
prices in healthcare. These early adopters are attempting to use new tools and technologies to better control
their health behaviors and make more informed healthcare choices (Shrank, 2017). Challenges with these
solutions can often emerge, as many do not integrate into the broader healthcare ecosystem (West et al.,
2016). Given these barriers and the interest in consumerism in healthcare, several organizations have
attempted to identify characteristics of the future of primary care. In one example, the Advisory Board
Company (2015) conducted a survey of 4,000 people, and established the following ten insights on what
consumers want from primary care:
1. Convenience is king. 2. Same-day appointments trump walk-in and wait. 3. Evening or weekends? depends on age. 4. Clinic near errands or work? They’d rather meet you online.
12
5. A one-stop shop is worth the drive. 6. Consumers prioritize convenience over credentials—and continuity. 7. High-tech beats high-quality. 8. Don’t rely on your brand. 9. Talk about money—consumers will trade access for bill info. 10. Know your target population—particularly their age.
The Advisory Board Company: Yakovenko, 2015
These ten features appear to align with a system predicated on consumers. New market entrants may
also fill voids in healthcare if traditional primary care practices do not meet the expectations and needs of
consumers (Ellner & Phillips, 2017). Nonetheless, as Ellner & Phillips (2017) note: “Change is never easy,
and dramatic change to something as personal as healthcare is likely to be accompanied by considerable
distress for all involved.” Nonetheless, the space between aspirations and reality with regards to consumerism
in healthcare is wide, and will take substantial periods of time for any major changes to occur.
Retailers’ Foray into Healthcare with the Retail Care Clinic
In recent years, several major retailers have expanded operations to provide primary care services
through their retail stores. This has often been undertaken by opening retail clinics in pharmacies, grocery
stores, and big-box stores (Ashwood et al., 2016). These clinics have longer hours (such as on weekends and
evenings), walk-in availability, and shorter wait times than traditional primary care offices. Services offered
target a limited range of health conditions, which are delivered by mid-level providers such as a NP, PA or
MA instead of a PCP (Sage, 2007). As is the case with retail, prices are fixed and transparent. The rise in
urgent care facilities in retail pharmacies and standalone chains further represent how new businesses are
providing services in areas of healthcare that traditionally have been the domain of primary care practices
(Shrank, 2017).
Sage’s (2007) article on “The Wal-Martization of Health Care” contends that the new generation of
retail clinics can theoretically promote cost containment. Estimates suggest that 20 percent of emergency
department visits for nonemergency conditions could generate annual cost savings of $4.4 billion for the US
healthcare system (Rand Corporation, 2016). While retail clinics provide an alternative to the emergency
department for nonemergency care, concerns have emerged with the concept. The lack of continuity in care
13
and delegating care to nonphysicians have been raised as issues by the American Medical Association (Cassel,
2019; Martsolf et al., 2017). Evidence published by RAND Corporation indicates that retail clinics lead to
new healthcare utilization and increases in spending (Rand Corporation, 2016). Overall, the evidence remains
mixed on the effectiveness of retail clinics in improving health outcomes and healthcare costs.
Nonetheless, Shrank (2017) notes that the future of the retail primary care clinic may be friendly:
If retail clinics were to challenge the existing model, and did aspire to take over the role of the primary care physician (e.g. provide continuous, comprehensive, coordinated, 24-hour access to primary care), this could represent a major disruption in the existing primary care model. Retail primary care could address a need resulting from primary care physician shortages and enhance access to essential care. At the same time, the emergence of retail primary care would create competition with existing primary care physicians, and would raise important new questions about quality and care coordination.
Shrank, 2017 2.3.3 A Model for the Future of Primary Care: Integration of Services
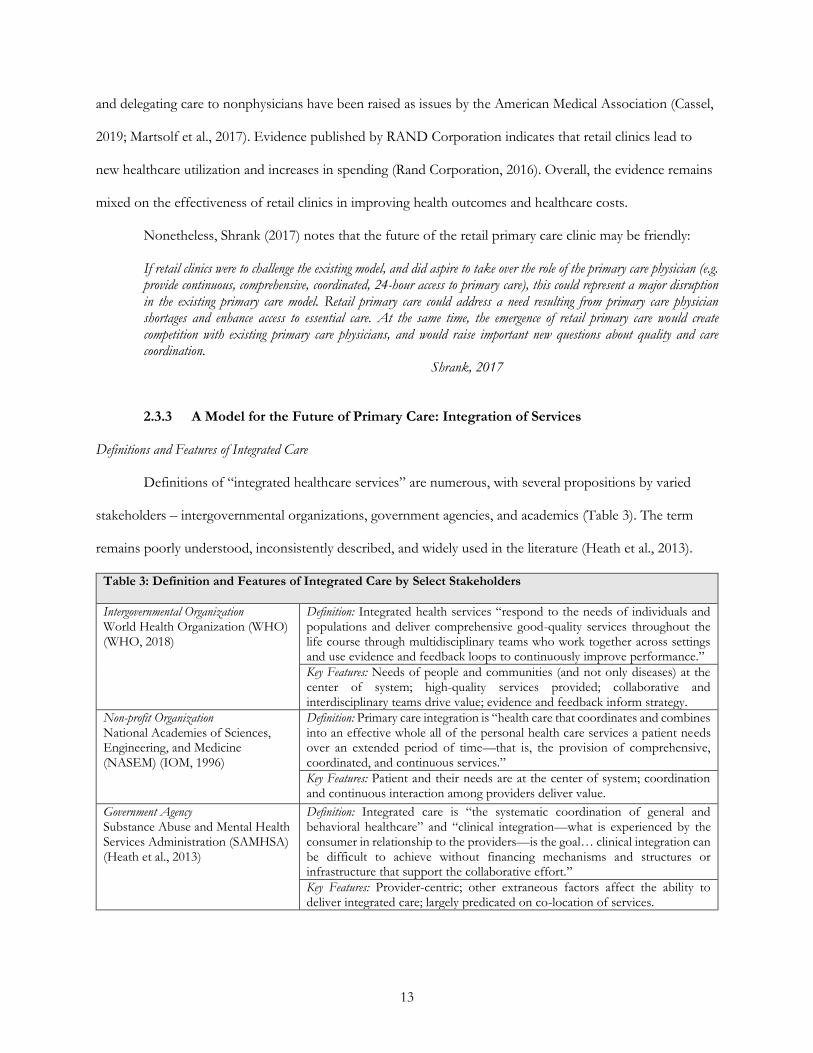
Definitions and Features of Integrated Care
Definitions of “integrated healthcare services” are numerous, with several propositions by varied
stakeholders – intergovernmental organizations, government agencies, and academics (Table 3). The term
remains poorly understood, inconsistently described, and widely used in the literature (Heath et al., 2013).
Table 3: Definition and Features of Integrated Care by Select Stakeholders
Intergovernmental Organization World Health Organization (WHO) (WHO, 2018)
Definition: Integrated health services “respond to the needs of individuals and populations and deliver comprehensive good-quality services throughout the life course through multidisciplinary teams who work together across settings and use evidence and feedback loops to continuously improve performance.”
Key Features: Needs of people and communities (and not only diseases) at the center of system; high-quality services provided; collaborative and interdisciplinary teams drive value; evidence and feedback inform strategy.
Non-profit Organization National Academies of Sciences, Engineering, and Medicine (NASEM) (IOM, 1996)
Definition: Primary care integration is “health care that coordinates and combines into an effective whole all of the personal health care services a patient needs over an extended period of time—that is, the provision of comprehensive, coordinated, and continuous services.”
Key Features: Patient and their needs are at the center of system; coordination and continuous interaction among providers deliver value.
Government Agency Substance Abuse and Mental Health Services Administration (SAMHSA) (Heath et al., 2013)
Definition: Integrated care is “the systematic coordination of general and behavioral healthcare” and “clinical integration—what is experienced by the consumer in relationship to the providers—is the goal… clinical integration can be difficult to achieve without financing mechanisms and structures or infrastructure that support the collaborative effort.”
Key Features: Provider-centric; other extraneous factors affect the ability to deliver integrated care; largely predicated on co-location of services.

14
Table 3 (Continued)
Academic studies and meta-analysis (Baxter et al., 2018; Singer et al., 2018)
Singer et al. (2018:3) describe integration in healthcare as: “The making of a unified whole from distinct and interdependent organizational components.” Baxter et al (2018) did a further systematic review and identified 153 integrated care studies.
Key Features: Features of studies with the most common levels of integration included integrated care pathways or plans, access to a case coordinator or manager, and multi-disciplinary meetings.
Despite the varied definitions of integrated primary care by several stakeholders, calls for integration
have never been stronger (Baxter et al., 2018). Maruthappu, Hasan & Zeltner (2015) suggest that: “A broad
effort should be made to implement integrated care.” Similarly, the Substance Abuse and Mental Health
Services Administration (SAMHSA) contends that: “The solution lies in integrated care, the systematic
coordination of general and behavioral healthcare. Integrating mental health, substance abuse, and primary
care services produces the best outcomes and proves the most effective approach to caring for people with
multiple healthcare needs.”4 Lastly, Heath and colleagues (2013) note that: “Integration is essential to
achieving the triple aim of improved experience of care, improved health of populations, and reduced per
capita healthcare cost.” The literature suggests substantial interest in the concept of integration of healthcare
services, with often unsubstantiated claims on the value or impact of integration on the patient.
Existing and Emerging Models of Integrated Primary Care in the US
President Lyndon B. Johnson’s “War on Poverty” in 1964 largely coincided with the emergence of
primary care in the US (Howell, 2010).5 Embedded within Johnson’s Economic Opportunity Act of 1964 was
funding to start two community health centers – one in South Boston, MA and one in Bolivar County, MS.
These centers provided the foundation for the nearly 1,400 federally qualified health centers (FQHCs) that
4 It must be noted that efforts to integrate healthcare services, and the outcomes generated from the integration of services, are not the same. As an example, the integration of primary care and behavioral health services is substantially different to the additional integration of substance use services. 5 The 1960s were a time of substantial change for healthcare in the US. President Johnson’s “War on Poverty” led to the first funding for community health centers across the country, and the passage of the Social Security Amendments of 1965 that created Medicare and Medicaid. Following these developments, primary care as a term and concept gained traction. Two reports underpinned this development. The first was a 1966 report published by the American Medical Association’s Ad Hoc Committee on Education for Family Practice Report, which recommended that every person have a PCP. The second was the 1966 Council Report on Education for Family Practice, which focused on the need for family medicine to balance the need of medical specialization.

15
exist today as nonprofits providing primary care services in lower income communities (Wells et al., 2019).
FQHCs offer “one stop shopping” – diagnostic labs, dental services, mental health counseling,
immunizations, case management, family planning, domestic violence prevention, substance use treatment,
eye exams, HIV testing and treatment, and several other primary care services are often offered by and for
the community (Wright, 2013). Importantly, FQHCs are mandated by Federal law to include a Board of
Directors, half of which are patients of the FQHC (Wright, 2013). Since FQHC services are coordinated,
convenient, and tailored to the community’s needs, much of the experimentation with integration has
occurred within these settings (Wright, 2013).
The idea of the FQHC model has been replicated across the US by several other private (and often
private equity-backed) companies. These companies generally focus on a targeted insurance type or
population (such as Medicare Advantage or Managed Medicaid). While these primary care practices deliver
several services, they tend to operate in a value-based care (VBC) arrangement. Unlike a fee-for-service (FFS)
approach in which providers are reimbursed based on the number of services provided to patients, VBC
means that providers are allocated a set amount of funding to take care of the full needs of the patient. In this
model, financial incentives are aligned with delivering whole-person, longitudinal care as opposed to acute or
episodic care that is often the case with FFS models. The intent of these healthcare delivery models is a
seamless and integrated experience for the patient. Primary care organizations experimenting with this type of
delivery model include: CareMore Health, ChenMed, CityBlock Health, Iora Health, Landmark Health, and
Oak Street Health.
Typologies of Integrated Primary Care
Several typologies have been proposed to describe integrated care. These typologies broadly span
two areas: (1) the integration of specific services (such as primary care with behavioral or oral health); and (2)
the integration of primary care with specialty care. The literature on both areas is discussed in this section. A
few studies focus on the integration of pharmacies into primary care, though these have been largely
conducted outside of the US (such as in England and Canada). Given the scope, they are not discussed here.
16
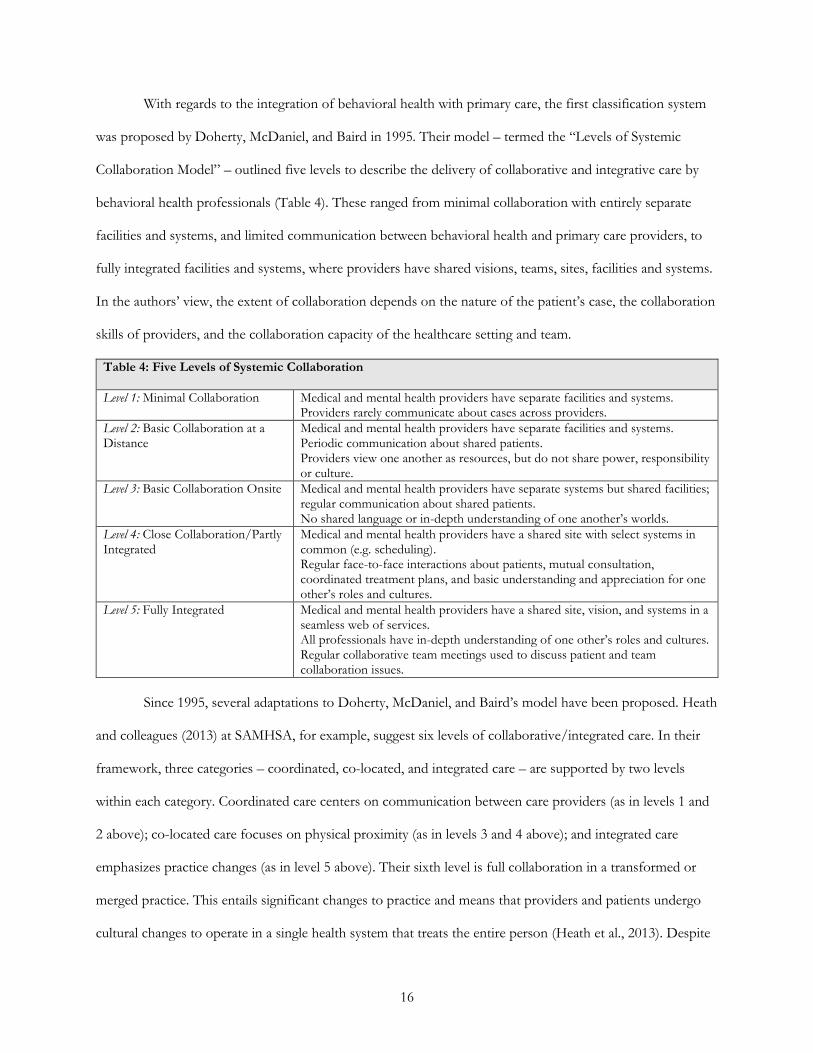
With regards to the integration of behavioral health with primary care, the first classification system
was proposed by Doherty, McDaniel, and Baird in 1995. Their model – termed the “Levels of Systemic
Collaboration Model” – outlined five levels to describe the delivery of collaborative and integrative care by
behavioral health professionals (Table 4). These ranged from minimal collaboration with entirely separate
facilities and systems, and limited communication between behavioral health and primary care providers, to
fully integrated facilities and systems, where providers have shared visions, teams, sites, facilities and systems.
In the authors’ view, the extent of collaboration depends on the nature of the patient’s case, the collaboration
skills of providers, and the collaboration capacity of the healthcare setting and team.
Table 4: Five Levels of Systemic Collaboration
Level 1: Minimal Collaboration Medical and mental health providers have separate facilities and systems. Providers rarely communicate about cases across providers.
Level 2: Basic Collaboration at a Distance
Medical and mental health providers have separate facilities and systems. Periodic communication about shared patients. Providers view one another as resources, but do not share power, responsibility or culture.
Level 3: Basic Collaboration Onsite Medical and mental health providers have separate systems but shared facilities; regular communication about shared patients. No shared language or in-depth understanding of one another’s worlds.
Level 4: Close Collaboration/Partly Integrated
Medical and mental health providers have a shared site with select systems in common (e.g. scheduling). Regular face-to-face interactions about patients, mutual consultation, coordinated treatment plans, and basic understanding and appreciation for one other’s roles and cultures.
Level 5: Fully Integrated Medical and mental health providers have a shared site, vision, and systems in a seamless web of services. All professionals have in-depth understanding of one other’s roles and cultures. Regular collaborative team meetings used to discuss patient and team collaboration issues.
Since 1995, several adaptations to Doherty, McDaniel, and Baird’s model have been proposed. Heath
and colleagues (2013) at SAMHSA, for example, suggest six levels of collaborative/integrated care. In their
framework, three categories – coordinated, co-located, and integrated care – are supported by two levels
within each category. Coordinated care centers on communication between care providers (as in levels 1 and
2 above); co-located care focuses on physical proximity (as in levels 3 and 4 above); and integrated care
emphasizes practice changes (as in level 5 above). Their sixth level is full collaboration in a transformed or
merged practice. This entails significant changes to practice and means that providers and patients undergo
cultural changes to operate in a single health system that treats the entire person (Heath et al., 2013). Despite

17
these nuanced differences among models, the literature broadly supports the notion that integration occurs
along a continuum, with varying levels of collaboration (Miller et al., 2011; Collins et al., 2010; Peek, 2007;
Seaburn et al., 1996).
The literature on the integration of oral health with primary care services is less developed than
behavioral health, though is rapidly emerging. Several calls from US Surgeon Generals, NASEM, and others
have focused on the closer integration of oral health and primary care services (Dwiel et al., 2019; Hostetter
& Klein, 2015; Institute of Medicine, 2011). While primary care providers often ask patients about their
overall health, they rarely inquire about their oral health. Furthermore, there are 108 million Americans who
see a PCP but do not see a dentist each year. This means that primary care providers often miss opportunities
to engage patients in oral health education, prevention strategies, screenings, and/or referrals to a dentist for
treatment (Atchison, Rozier & Weintraub, 2018). Similarly, 27 million Americans visit a dentist but do not
visit a medical professional each year. Dentists and hygienists rarely ask their patients about preventive
behaviors such as vaccinations or screen for diabetes or other chronic diseases (Atchison, Rozier &
Weintraub, 2018). Taken together, advocacy exists for the closer integration of oral health with primary care,
though few examples beyond FQHCs exist with this type of integration.
Lastly, the literature on the integration of primary and specialty care services largely focuses on the
mode of integration – either in-person or through technological solutions such as telemedicine and electronic
consultations (commonly referred to as “e-consults”) (Vimalananda, 2020; Newman et al., 2019; Olayiwola,
2016). Several cases document the integration of specialty and primary care services through physical space
redesigns to support in-person care delivery (Tang et al., 2019). Tang and colleagues (2019), for example,
demonstrate the effectiveness of physically integrating specialty behavioral health services with primary care.
They discuss physically moving a nearby specialty behavioral health facility into their primary care setting
(Tang et al., 2019). Technology tools have also been used to integrate specialty and primary care (Waugh et
al., 2019). While overall uptake of telemedicine remains low, places such as at the Department of Veterans
Affairs (VA) have been using it with effectiveness to treat mental health conditions (such as post-traumatic
stress disorder (PTSD)) for many years (Rubin, 2018). E-consults also provide a mechanism for rapid,
18
documented, asynchronous communication between a primary care clinician and a specialist (Vimalananda,
2020). The research on e-consults is in an early phase, though shows potential for averting the need for face-
to-face visits, reducing avoidable care, and enabling more efficient use of specialty care services (Newman et
al., 2019).
The Value of Integrated Primary Care
The evidence on the benefits of integrated primary care delivery is inconclusive. While intuitively the
notion that several providers interacting in shared facilities with common goals and visions would improve
operations and outcomes, several reviews suggest it is not so simple.
On the one hand and at the most macro-level, the WHO and several systematic reviews highlight the
benefits of integrated care. The WHO (2018) contends that integrated health services contribute to improved
economic, social, and individual benefits. This stems from the better distribution of health outcomes, and
improved well-being and quality of life (WHO, 2018). The WHO also contends that integrated care can lead
to better outcomes, access to services, and adherence to treatments; fewer unnecessary hospitalizations and
readmissions; increased patient satisfaction, health literacy, and self-care; and greater job satisfaction of health
workers (WHO, 2018). Where there is less certainty is on the impact of integrated care on cost-effectiveness,
though the WHO (2018) believes there are efficiency gains from the better allocation and coordination of
resources, less duplication of procedures, and shorter waiting times. The systematic reviews also identify
strong evidence in support of integrated health services in patient satisfaction, perceived quality of care, and
increased and improved patient access (Baxter et al., 2018).
On the other hand, several studies demonstrate limited value of integrated primary care services.
Calls for integrated care are robust, though the literature suggests that integrated care rarely leads to
unequivocally positive effects (Baxter et al., 2018). Beyond improvements in measures of patient satisfaction,
there is minimal impact of integrated care models on experiences and outcomes (Baxter et al., 2018). As an
example, a trial with patients with depression found that patients were more satisfied with collaborative care,
though no difference was noted in their symptoms or rates of readmission (Solberg et al., 2015).
19
Barriers to Integrated Primary Care
Numerous barriers inhibit the effective implementation of integrated care. Many health systems are
also plagued by existing infrastructure and decentralized support structures, making shifts toward integration
of services often more challenging than starting afresh (Maruthappu, Hasan & Zeltner, 2015). According to
Powers, Donoff & Jain (2017), the effective integration of primary care with other services will require
overcoming potential barriers such as cultural and team dynamics; financial alignment; supportive
information technology; interprofessional education and cross training; and legal and regulatory requirements.
Culture and Team Dynamics: The blending of visions, goals, cultures, teams, and other ways of working
have been cited as barriers to facilitating integration of services in primary care. Culture changes and the
building of cultural competence at the clinical and management levels are required to ensure alignment of
vision and goals to support the integration (Maruthappu, Hasan & Zeltner, 2015). An inability to
communicate between providers has also been cited as a challenge to integration, with providers being unable
to find the time necessary to build relationships and communicate with one another (Grazier et al., 2013).
Financial Alignment: Payment models predicated on FFS reimbursement rarely support integrated primary
care. This is because FFS maximizes visits and volume over value, making it difficult for providers to address
patient issues in a holistic way. Although the ACA, Medicaid, and select commercial insurance schemes are
integrating oral health into health insurance plans, the relative separation of medical and dental insurance and
reimbursement structures largely inhibits the integration of care (Powers, Donoff & Jain, 2017).
Technology Systems: Systems that operate independently can stymie the integration of primary care
services. Current electronic medical records (EMRs) are optimized for capturing revenue in FFS
environments and are often not interoperable across service lines (Ellner and Phillips, 2017). Primary care and
behavioral health practices working toward integration have commonly established workarounds because
EMR platforms do not enable the documentation, communication, and information exchange required by
providers (Cifuentes et al., 2015). While it is anticipated that advances in technology will improve diagnoses,
monitoring, and surveillance as well as augment clinical workflows to facilitate rapid and reliable information
20
exchange, enhance task management and care coordination, and improve patient triage and routing,
technology remains a substantial barrier to the integration of primary care services (Ellner and Phillips, 2017).
Education and Training: Siloed professional education and training inhibits the integration of care. PCPs
rarely train in other services (such as oral health) outside their remit, while dentists are rarely educated on the
functions of primary care (Powers, Donoff & Jain, 2017). PCPs frequently cite a lack of knowledge in other
areas such as behavioral or oral health, making it difficult for them to provide such services (Ross et al.,
2015). Oral health risk assessments, specialist referrals, and the delivery of basic preventive measures such as
fluoride therapy, are not covered in training schemes for PCPs (Powers, Donoff & Jain, 2017). Similarly,
select components of annual exams and chronic care management should be covered in the education
received by dental providers (Powers, Donoff & Jain, 2017). This may include screenings and immunizations
as well as medication adherence and blood pressure management (Powers, Donoff & Jain, 2017).
Legal and Regulatory Barriers: At the broadest level are legal and regulatory barriers that can often hamper
the integration of primary care services. In particular, the corporate practice of medicine doctrine and anti-
kickback statues are cited in the literature (Cebul, Rebitzer, Taylor & Votruba cited in Elhauge, 2010). The
corporate practice of medicine doctrine aims to preserve physician autonomy by prohibiting the employment
of physicians by non-physician entities (such as corporations) in certain states (AMA, 2015). Anti-kickback
statutes such as the Stark Law, which prevent physicians from referring patients to entities by which they
have a financial relationship, have been suggested to hinder competition and integration efforts (Porter &
Teisberg, 2006).
2.4 Theory of Change
Several theories, frameworks, and models on integration in healthcare have been proposed to
elucidate the complexity and multidimensionality of the topic as well as to define relationships between
variables that can facilitate integration (Valentijn, 2016; Singer et al., 2018). The theoretical model proposed
by Singer and colleagues (2018) attempts to outline a comprehensive theory of integration that synthesizes,
21
reconciles, and extends these approaches. This model provides the theoretical foundation for exploring the
integration of primary care services to answer the research questions.
2.4.1 Theoretical Model
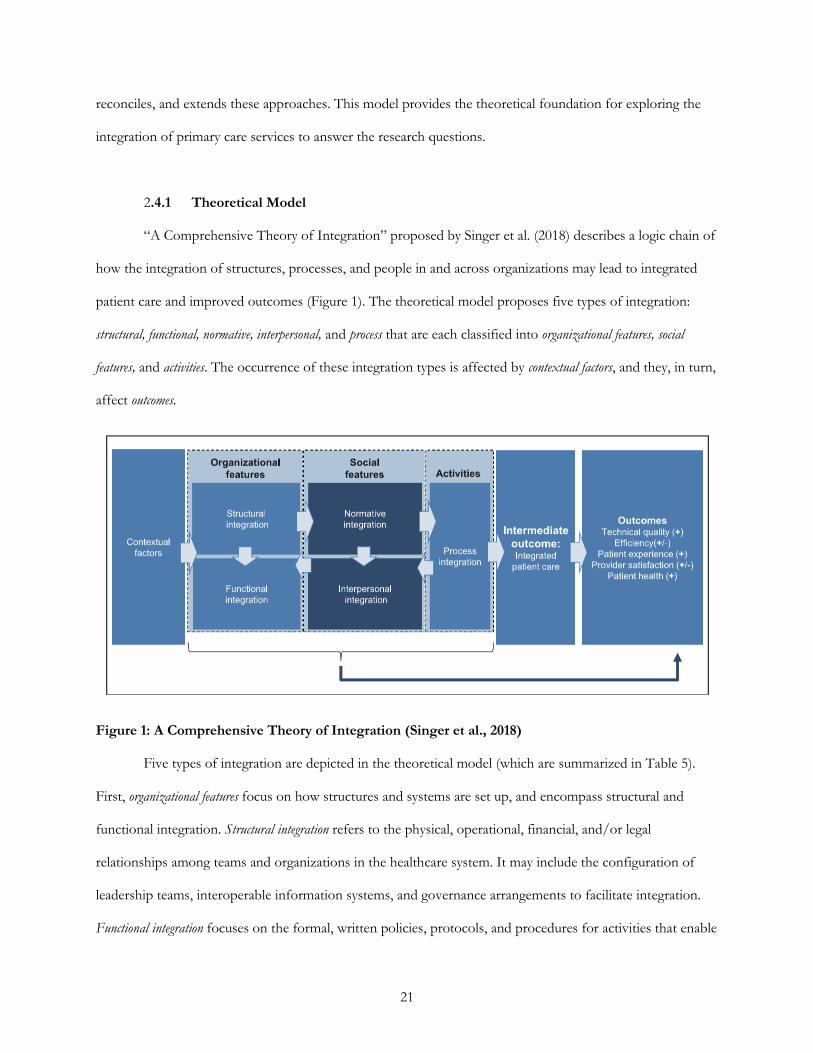
“A Comprehensive Theory of Integration” proposed by Singer et al. (2018) describes a logic chain of
how the integration of structures, processes, and people in and across organizations may lead to integrated
patient care and improved outcomes (Figure 1). The theoretical model proposes five types of integration:
structural, functional, normative, interpersonal, and process that are each classified into organizational features, social
features, and activities. The occurrence of these integration types is affected by contextual factors, and they, in turn,
affect outcomes.
Figure 1: A Comprehensive Theory of Integration (Singer et al., 2018)
Five types of integration are depicted in the theoretical model (which are summarized in Table 5).
First, organizational features focus on how structures and systems are set up, and encompass structural and
functional integration. Structural integration refers to the physical, operational, financial, and/or legal
relationships among teams and organizations in the healthcare system. It may include the configuration of
leadership teams, interoperable information systems, and governance arrangements to facilitate integration.
Functional integration focuses on the formal, written policies, protocols, and procedures for activities that enable

22
accountability and decision-making. It focuses on the protocols for activities, such as the policies for how
personnel share information, as opposed to the structure of the interoperable information system. Both
structural and functional integration are under the direct control of leadership, and can occur horizontally
(across organizations of the same type) and vertically (across organizations of different types within and
outside of the healthcare system).
Second, social features associated with what people believe and how they behave encompass normative
and interpersonal integration. Normative integration focuses on creating a common culture and demonstrating
the prioritization of integrated patient care within this culture. This may entail a shared vision and mission,
and collective attitudes. It may also include the extent to which leadership promotes coordination,
communication, and continuity of care as well as the inclusion of a patient and family’s values, beliefs, and
preferences in decision-making. Interpersonal integration relates to collaboration and teamwork among medical
and non-medical professionals as well as patients, families, and nonprofessional caregivers. Providers may
work collectively as a team, though if the needs and values of the patient are not met, then interpersonal
integration has not been realized. Interpersonal integration requires clarity in roles and responsibilities,
positive attitudes about teamwork, and identification with the team. Normative and interpersonal integration
do not come under the direct control of leadership, though their words and actions may influence the degree
of integration.
Lastly, activities that describe a course of care focus on process integration (or clinical integration).
This refers to actions and activities that integrate patient care services into a coordinated process. It may
include activities such as the use of shared care plans to ensure appointments are kept, referral loops are
closed, and test results are communicated. Process integration can be influenced indirectly by leadership.
Table 5: Descriptions of Classifications & Types of Integration (Adapted from Singer et al., 2018)
Integration Type Description Example(s)
Organizational Features: How structures and systems are set-up and arranged.
Structural Integration
Physical, operational, financial, or legal ties among organizations in a health system and teams within organizations.
Composition of leadership teams; interoperable information systems; governance mechanisms (direct ownership of one entity by another, legal contracts, informal alliances).

23
Table 5 (Continued)
Functional Integration
Formal, written policies and protocols for activities that coordinate and support accountability and decision making among organizations and individuals.
Policies for how personnel share information; specified protocols for tracking metrics.
Social Features: What people believe and how they behave.
Normative Integration
A common culture, and a specific culture of integration across units and organizations within a health system.
Shared vision and mission statements; collective attitudes; coordination, communication, and continuity of care.
Interpersonal Integration
Extent of collaboration or teamwork among health care professionals in one or more disciplines and from one or more organizations as well as nonprofessional caregivers and the patients themselves.
Patients, families, and nonprofessional caregivers included in care planning processes; team-based structures; training, mentorship, and feedback on teamwork.
Activities: Processes that determine care delivery actions and activities.
Process Integration
Also termed clinical integration and refers to courses of clinical actions or activities intended to integrate patient care services into a single process across people, functions, activities and operating units over time; specific activities that demonstrate care has been delivered in a coordinated way.
Use of shared care plans to ensure appointments are kept, referral loops are closed, and test results are communicated.
The five integration types can be affected by contextual factors, and in turn affect integrated patient
care and outcomes. Contextual factors are features of the market and organizational context and can be
characterized into internal organizational characteristics and external market characteristics. Internal
organizational characteristics are internal to the organization and may include the size and number of practice
sites in a health system; the specialty-mix; the ratio of non-physician staff to physicians; and the physical
proximity of staff. External market characteristics are external to the organization, and encompass the market
structure, extent, and types of value- and risk-based payments; legal and regulatory factors; and the prevalence
of community-based resources. Organizational actors often perceive contextual factors to be largely
immutable, though they are forms of structural integration if they are modified by organizational leaders.
Integrated patient care is a potential – though not guaranteed – intermediate outcome of the five types
of integration. An organization may be considered integrated across the five types, though integrated patient
care may not be delivered if it is not perceived by the patient. Integrated patient care is only realized when
patients and family members experience it as such, and the extent of it must be evaluated on a patient-by-
patient basis. Improved outcomes are the end goal of integration of the five types and patient care. They include
better technical quality of care, efficiency of care, patient and provider experience of care, and patient health.
24
2.4.2 Alignment of Research Questions with Theoretical Model
The research questions are examined through the lens of Singer et al.’s (2018) theoretical model. The
first research question – “What is the current landscape of integrated primary healthcare services in the US?”
– is investigated through an exploration of contextual factors derived from thought leader interviews. This
attempts to uncover how leaders conceptualize and perceive integration within primary care, as well as the
extent to which internal organizational and external market factors influence integration. The second research
question – “How can the integration of primary care services be optimized at Walmart Health?” – is studied
using the five integration types in Figure 1 using interviews with associates at the Walmart Health Center.
These operational considerations attempt to elucidate the presence of the five integration types at the
Walmart Health Center.
The Singer et al. theory is not used as a direct empirical model for data collection and analysis. The
intent is not to determine whether existing primary care models of integration, including the model used by
Walmart Health, fit into the Singer et al. (2018) model. The theoretical model is rather used as a guide to
inform the methodological approach, including data collection and analysis, though does not limit
investigation into factors solely included in the theoretical model.
2.5 Methodology
2.5.1 Project Methodology
Qualitative research is a form of social inquiry that aims to “understand, describe, and interpret social
phenomena as perceived by individuals, groups, and cultures” (Holloway & Galvin, 2016:3). It entails
listening to participants to gain firsthand knowledge of their lived experiences, which are not reduced to
simple variables (Taylor, Bogdan & DeVault, 2015; Tracy, 2013; Yin, 2011). Qualitative research is a
systematic, though often not standardized, approach to collecting and analyzing data (Marshall & Rossman,
2011). Given the multidimensionality of this project, a qualitative methodology was used to explore the
research questions.
25
Data Collection
The first research question, which focused on better understanding the current landscape of
integration within primary care, included eight site visits to primary care clinics as well as six semi-structured
interviews with thought leaders. The eight site visits included observing primary care operations operated by
several healthcare entities across the US: FQHCs, high-growth start-ups, major retailers, and leading insurers.
These visits were undertaken in my capacity as a Walmart associate, and were used to inform my learning of
existing models of primary care. Notes were taken during the visits, which were supplemented with
reflections following the tours. These notes were not analyzed comprehensively, though were important for
comparing models of primary care.
Exploring the first research question also entailed conducting six semi-structured interviews with
thought leaders. These interviews aimed to better understand contextual factors impacting the extent of
integration in primary care. Interviewees had substantial expertise in primary care (Table 6). These individuals
were identified and recruited through a purposive sampling technique. Outreach was undertaken using email
correspondence, which included details on the aims and objectives of the project. Interviews were conducted
over the phone during November and December 2019. They ranged in length from approximately 20 to 45
minutes and were audio-recorded.
Table 6: Descriptions of Thought Leaders Interviewed on Integration of Primary Care Services
A chief medical officer and practicing PCP at a high-growth healthcare start-up focused on value-based care.
A director of integration and practicing PCP at a FQHC integrating behavioral health and primary care services.
A county health director and practicing PCP delivering frontline care to high-risk individuals.
A professor of healthcare and management with expertise in healthcare integration.
A professor of medicine and public health focused on primary care.
An executive director of a primary care research center and practicing physician.
Answering the second research question, which centered on optimizing the integration of primary
care services at the Walmart Health Center, also entailed conducting site visits and semi-structured interviews.
The site visits and semi-structured interviews aimed to determine the extent of integration of primary care
services at the Center. Prior to conducting the interviews, I visited the Center on several (three) occasions to
understand the perceived and real integration of services as well as workflows, relationships, and culture.
These visits additionally enabled me to build rapport with associates at the Center.

26
The 22 individuals who were interviewed in support of the second research question were associates
at the Center. They spanned many functions and positions (Table 7). Functions included administrative,
primary care service lines, and social support associates. Positions included frontline associates such as care
hosts and dental treatment coordinators, all the way through to the PCP, dentist, optometrist, and audiologist.
They also included interviews with associates who provided social support such as the CHWs and community
room liaison. Interviews were not audio-recorded, though extensive verbatim notes were taken. At the start
of the interviews, I presented myself as a doctoral student in public health, employed by Walmart for a short-
term placement that was a component of my degree. These interviews lasted approximately 15 to 20 minutes
and were conducted in person at the Center in December 2019.
Table 7: Positions of Associates Interviewed at Walmart Health Center
Administrative Associates
Clinic manager Assistant clinic manager Business development manager
Service Line Associates
PCP NP Care host
Dentist Dental treatment coordinator Radiology technician
Pharmacist Audiologist Optometrist
Social Support Associates
CHW Community room liaison Home care coordinator
Two interview guides were prepared, tested, and followed to support the interviews (Appendix B). A
flexible design that started with broad questions and moved into specific ones underpinned the interview
approach (Marshall & Rossman, 2011). As learning evolved, questions became more targeted to better
understand the integration of primary care services in the Center (Taylor, Bogdan & DeVault, 2015).
Interviewees were not provided with an incentive to participate, and interviews were confidential. A
confidentiality agreement was adapted from the Harvard Institutional Review Board (IRB) website and shared
with interviewees (Appendix C). Consent was provided through written or oral communication before the
interview.
Data Analysis
A similar approach to data analysis was used to explore the two research questions. Data from the
semi-structured interviews were transcribed using an online transcribing platform (Happy Scribe). They were
27
edited to ensure alignment with the spoken word, and then imported into NVivo software for coding
analysis. Codes were developed based on an understanding of the primary care field and the literature. Once
the coding was complete, a thematic network analysis was used to identify common themes across the
interviews. Deductive reasoning provided the foundation for the thematic analysis, using the types of
integration in the Singer et al. (2018) theoretical model as a guide. Inductive reasoning was then used to
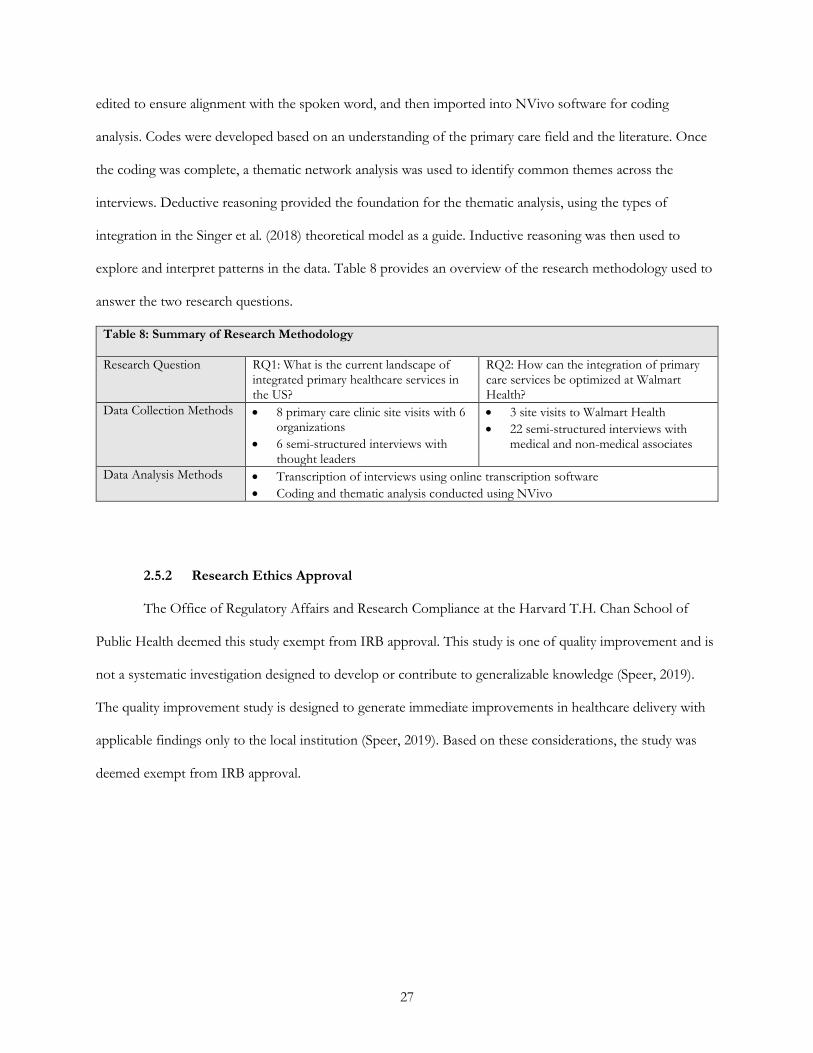
explore and interpret patterns in the data. Table 8 provides an overview of the research methodology used to
answer the two research questions.
Table 8: Summary of Research Methodology
Research Question RQ1: What is the current landscape of integrated primary healthcare services in the US?
RQ2: How can the integration of primary care services be optimized at Walmart Health?
Data Collection Methods • 8 primary care clinic site visits with 6 organizations
• 6 semi-structured interviews with thought leaders
• 3 site visits to Walmart Health
• 22 semi-structured interviews with medical and non-medical associates
Data Analysis Methods • Transcription of interviews using online transcription software
• Coding and thematic analysis conducted using NVivo
2.5.2 Research Ethics Approval
The Office of Regulatory Affairs and Research Compliance at the Harvard T.H. Chan School of
Public Health deemed this study exempt from IRB approval. This study is one of quality improvement and is
not a systematic investigation designed to develop or contribute to generalizable knowledge (Speer, 2019).
The quality improvement study is designed to generate immediate improvements in healthcare delivery with
applicable findings only to the local institution (Speer, 2019). Based on these considerations, the study was
deemed exempt from IRB approval.
28
3.0 RESULTS
3.1 Framing of Results
Healthcare leaders have often advocated for the effective integration of healthcare services (Tang et
al., 2019; Baxter et al., 2018; Maruthappu, Hasan & Zeltner, 2015; Heath, Wise Romero & Reynolds, 2013).
The literature suggests that integration of healthcare services has potential to improve the cost, convenience,
and care of services provided to patients (NIMH, 2017; Olayiwola, 2014). The rationale for Walmart Health
was no different: integration of basic healthcare services meant the cost, convenience, and care of services
delivered to consumers could be optimized. These are each discussed in more detail.
(1) Cost: The Walmart Health Center can generate cost efficiencies from the effective integration of basic
healthcare services. If Walmart Health can operate for less relative to other market competitors, it
can charge lower prices to consumers. This means consumers can save, which allows Walmart Health
to grow sales through volume. This can create a self-reinforcing business model for Walmart Health.
(2) Convenience: The Walmart Health Center can provide a more convenient experience for consumers
through the greater integration of basic healthcare services. The integration of multiple services in a
single location means consumers do not need to visit multiple locations for different appointments.
A visit to a single location for multiple healthcare services can save consumers time and money.
(3) Care: The Walmart Health Center can offer better care to consumers with the effective integration of
basic healthcare services. Rather than one provider viewing the healthcare needs of a patient through
the lens of their expertise and training, proximate collaboration among providers means that the
entire health needs of the patient can be addressed collectively, rather than separately, by providers.
Given the strategic importance of the integration of primary care services at the Center, the Singer et
al. (2018) theoretical model was appropriate for guiding my exploration of the research questions. It provided

29
me with a mental model to identify and isolate variables that could improve the integration of services.6 By
distilling these variables, I could prioritize them to determine where Walmart Health could intervene to
optimize the integration of services. This meant Walmart Health could fulfill their vision of providing cost
effective, convenient, and high-quality care at its Centers.
As I conducted the interviews, it became apparent that the Singer et al. (2018) theoretical model was
bound by several limitations. One example related to the variables included in (or excluded from) the
theoretical model. Features deemed important to Walmart Health, including the cost and convenience of care,
appeared largely absent from the theoretical model. Efficiencies were included as a potential outcome of
integration, though it was unclear what impact this has on cost considerations, while convenience may (or
may not be) a factor embedded in the patient experience variable. The lack of clarity regarding naming of the
variables made it challenging to establish groups or relationships among the variables.
The Singer et al. (2018) theoretical model also did not consider the prioritization of variables. The
model does not consider how an organization in the early stages of its operational life (such as Walmart
Health) can rank activities that are required to integrate basic healthcare services. Other thought leaders I
interviewed were often more familiar with integration activities at healthcare organizations that had been in
operation for many years. This meant there were differences in how interviewees approached and prioritized
integration activities. In using the theoretical model as a foundation for analysis, I found the prioritization of
variables to help facilitate integration for organizations at different stages of operation to be markedly absent.
The frames of reference on the strategic importance of integration to Walmart Health, and the
benefits and limitations of the Singer et al. (2018) theoretical model, shaped my approach to conducting the
research. This section further discusses the results of the project to answer the proposed research questions
using the lens of the theoretical model and motivations of Walmart Health. Outputs from the interviews with
thought leaders were used to understand the current landscape of integration in primary care, while interviews
with Walmart Health associates underpin the examination of integration of healthcare services at the Center.
6 Although I used the theoretical model as a mental representation to explore the research questions, it should be noted that the thought leaders or Walmart Health associates I interviewed were unfamiliar with the model.
30
3.2 The Current Landscape of Integrated Primary Care
The current landscape of integrated primary care models is examined through the lens of the Singer
et al. (2018) theoretical model. It proposes that contextual factors, including external market characteristics
and internal organizational features, influence the extent of integration of basic healthcare services. This
section examines the outputs of the thought leader interviews, using these two contextual characteristics as
the basis for analysis.
External Market Characteristics
Preservation of the Status Quo by Incumbents: The current landscape of integrated primary care services
is influenced by the outlook and operations of incumbents in the healthcare sector. In its current state, the
healthcare system largely aligns with the interests of clinicians. This has meant that traditional healthcare
stakeholders (such as hospitals and physician groups) tend to focus on “just doing things the way they’ve
always done them” to ensure “their own survival.” The result of a system that maintains the status quo by
prioritizing clinicians is that “we can’t even imagine anymore how to put the patients at the middle of their
care.” A professor of medicine and business on the West Coast with expertise in primary care and clinic
culture described to me a patient’s experience in navigating the healthcare system:
These organizations that are organized around the clinicians, what you feel as a patient is you go to a primary care visit and the chief responsibility of that primary care physician is figuring out what specialists they can refer you to, so that you can get your issues addressed, and then you get into this horrible loop of, you know, they start calling you because, you know, they’re feeling like they should follow up, and you’re just feeling like they want to make a revenue generator out of you, and you end up having to spend enormous amounts of time going to different appointments and different providers, and you never get a sense that your doctor actually knows what’s transacted there, and so you become responsible for communicating to the doctors about the other doctors and, you know, it really just doesn’t work.
Even though clinicians are at the center of the healthcare system, it remains challenging for any
stakeholder to innovate within the system. This is particularly the case when an organization does not own or
operate the entire system. Large-scale change from within the system is difficult when a single entity does not
control the actions and activities of others in the system. Given that healthcare incumbents are focused on
maintaining the system, I found integration efforts to be few and far between among these healthcare entities.
31
Emergence of New Competitors: The impatience with the status quo of the healthcare system, and a desire
of “wanting to break through the silos,” has led to the emergence of several new market competitors with
bold and aspirational visions for redefining healthcare. These organizations are largely for-profit entities and
are capitalizing on reimbursement shifts from FFS to VBC. Since VBC models enable providers to innovate
with global payment flows, they are “totally rethinking [primary care] models.” Importantly, these new models
often place the patient at the center of care and are focused on “what’s best for the patient.” The needs of the
patient are prioritized and addressed in a way that is “as seamless for them as possible.” In these models,
primary care is increasingly becoming accessible, convenient, integrated, and affordable for the patient.
For these new market entrants, access to primary care services is top of mind. “It’s access, access,
access,” as a PCP at a private equity-backed primary care start-up shared with me. Access means offering
primary care across several temporal dimensions. Patients can receive care in the clinic, at home, and on-the-
go through digital means. Since “there’s only so much we [the provider] can accomplish for patients when
they’re right in front of us in the office,” the delivery of primary care services should be available “the same
day, next day, 24/7 phone access, [and through provided] transportation.” If the provider is not delivering
indirect patient care (care outside of the clinic setting), providers were “missing the opportunity to really do
what our patients need.” In this regard, patients should be at the center of their care, with access wherever
and whenever they need it.
Several newly formed primary care start-ups also focused on increasing access to services using
telemedicine. While overall utilization of telemedicine remains low (though is increasing), a series of new
organizations are using telemedicine to offer a “telemedicine-first primary care model.” A professor on the
East Coast with expertise in telemedicine who researches these models described them to me:
There are a handful of new startups, for profit primary care delivery models that revolve around telemedicine. They have the primary delivery mechanisms, and there, the primary care integration is really just a part of the primary care model. So it’s really directly integrated and it’s just a different mechanism of having the visit or interaction with your PCP.7
7 This quote additionally demonstrates differences in understanding of the word ‘integration.’ It is clear this interviewee thought of integration as the ability to provide specialty care services in a primary care setting using telemedicine.
32
Nonetheless, it is unclear whether these offerings will remain a “niche phenomenon.” Patient
experience can be suboptimal, and it is challenging for providers to build relationships with patients through a
screen. It was also cautioned to me that telemedicine may further fragment the healthcare system if it is only
used for patients switching between therapists or simply obtaining one-off visits. The same interviewee
continued to question these telemedicine-first models:
Is it just going to be a way that tech savvy, wealthier individuals are going to access care who don’t really have particularly pressing health issues? Is it really just going to be kind of a convenience option? Or will it be, you know, the 50% of healthy adults who take up 5% of medical costs? Or is there a way that it can evolve into a more scalable solution for the health care system? And the larger settings where primary care docs are actually willing to do more complex chronic disease management or more complex coordination of care. At the moment, I think mostly it is a rich person with an iPhone.
The emergence of new competitors operating in VBC arrangements and leveraging technology to
place the patient at the center of care means that the integration of services can be embedded in the operating
model. Since integration efforts are aligned with reimbursement and the needs of patients, these new
organizations appear to be pushing the boundaries of what it means to integrate primary care services.
Intrapreneurship by Community Health Centers: Beyond an array of newly founded start-up entities
attempting to change the primary care experience, community health centers (specifically FQHCs) are a
source of innovation focused on integrating primary care services. These health centers often have several
primary care services offered under one roof, such as behavioral health and oral care, and may refer out for
specialty care services. The usual poor patient experience and lack of follow-up with referrals for specialty
care services has led many of the more innovative FQHCs to test new ideas to bring these services in-house.
The FQHCs serve high-risk populations, making it more imperative for these organizations to develop new
models of care coordination. As one PCP and child psychiatrist at a FQHC described to me:
People have complex needs, they don’t go away with two or three brief CPT sessions. I mean, you know, trauma, parental substance use, psychosis, severe depression, suicide, these do not go away with two or three brief interventions.
Since many of the FQHCs do not have abundant resources, several in a common geographic area
have begun to collaborate in learning networks to share best practices and approaches to delivering high-
quality, integrated care with a high-risk population. Overall, I found there to be innovative models emerging
from FQHCs in pockets across the country focused on the integration of primary care services.

33
Legal and Regulatory Guardrails: The legal and regulatory environment at state and federal levels can
promote or inhibit the integration of primary care services. Certain states (such as Massachusetts) were cited
by interviewees for their progressiveness in tackling barriers to integration. “The state has been
acknowledging the fact that people are trying to be innovative and do what’s best for patients, and they’re
chipping away at some of these regulations,” noted one PCP interviewee in Massachusetts.
While some states are removing barriers to integration, others are not moving as swiftly. Selected
states have introduced metrics predicated on incentive payouts to encourage the delivery of high-quality care
by providers. Providers receive a payment for reaching pre-defined targets. While the intent may be right in
facilitating greater integration, the underlying policies can still silo care. As one PCP employed in a county
health department mentioned, it “doesn’t matter how many of these constructs you create” when the policy
prevents integration. Similar frustrations were noted with state-level telemedicine restrictions. Even though
some states are attempting to promote policy innovation, it remains challenging to align the interests of
stakeholders. The same interviewee mentioned that:
We’re always pushing on each other, and trying to use leverage to get people to chip-in to more rationally use those dollars, and at the same time, the policies kind of make us favor different types of approaches.
Despite these barriers, interviewees largely found a way to overcome legal and regulatory challenges
to promote integration efforts: “There are some barriers [to integration], but none of them are
insurmountable.”
New Models of Financial Reimbursement: The healthcare system is increasingly moving from a FFS
reimbursement model toward a VBC one. Instead of providers being reimbursed based on the number of
services given to patients (FFS), payers provide a set amount of funds to providers to manage the complete
care of their patient population (VBC) – an arrangement that promotes value of care over volume of services.
As the healthcare system shifts from “payers hav[ing] historically been responsible, and now see[ing]
providers being responsible,” the integration of primary care services plays an even more important role in
care delivery. One PCP at a VBC primary care start-up described integration with its relationship to VBC:
I think the integration is, in our case, just a sort of a feature of a value-based model … It's hard to distinguish in my mind those benefits of integration from the benefits that you get from value-based models in a financial sense, because

34
they really allow you in a meaning of life way to tie the work you do to your underlying values, which in the case of primary care doctors in so many cases, are evidence-based care and health equity and personal mastery of the field.
The underlying reimbursement model enables providers to more tightly integrate operations,
services, and workflows to deliver high-quality care. This is because the provider is incentivized to take care
of the needs of the patient throughout their healthcare journey. Even though selected interviewees cited the
importance of VBC models, other interviewees believed that the reimbursement model was only marginally
important in enabling providers to effectively integrate primary care services. The interviewee from a county
department of health noted that: “Payment is a necessary condition for a lot of these innovations to happen,
but it’s not sufficient.” Incentives matter, though delivering a more integrated primary care experience is
motivated by a mindset rather than a reimbursement model.
In other settings such as FQHCs, building a sustainable FFS model often provided the foundation to
transition to a VBC arrangement. By “doing fee-for-service really, really well … you’re preparing yourself for
value-based care,” noted a PCP and child psychiatrist at an FQHC. In the case of behavioral health, which is
often viewed as unprofitable, creating and maintaining a profitable FFS operation by blending primary care
and specialty behavioral health into the same operation was essential for moving toward VBC:
So fee-for-service, if you get paid $85.91 for a 45-minute therapy visit [Medicaid billing for a behavioral health visit in a particular state], and you see, you do the equivalent of 23 of these a week, which is 17.5 hours of patient care, which is totally doable in a 40-hour work week, you’ve seen patients 40% of the time, less than half the time, and you worked 45 weeks a year, then 45 times 23 times $85.91 is $89,000. $89,000 covers the cost of a social worker, and your fringe, and a little overhead.
Given the economics of a profitable FFS behavioral health offering, the ability to have a “financially
self-sustaining social worker” was a “game changer.” Having made the behavioral health service profitable,
the organization was able to create the business case to hire additional personnel to build the team for the
transition to VBC. “It is a more incremental process that positions us well for value-based care,” noted the
interviewee.
Even though there were different perspectives on the integration of primary care services within FFS
and VBC reimbursement models, a common sentiment expressed by the interviewees was that integration is
an embedded component of operating in a VBC reimbursement arrangement, though could still be done in a
35
FSS model. The financial payment flows appeared to be a consideration, though not necessarily the
determinant, of effective integration efforts.
Primary Care Educational Training: Training in medical schools to prepare future healthcare leaders could
have a greater emphasis on primary care models that integrate care. A shortage of PCPs graduating from
medical schools each year combined with training programs that often do not teach VBC models has made it
challenging to facilitate the effective integration of primary care services. One interviewee from a VBC
primary care start-up described the challenge to me:
Our health care educational system doesn’t prepare people to come in to run these [VBC] models because nobody’s running them. So they’re not trained, and what it means is you cannot just start this and hire people and have them running, and run high-quality value-based models. You have to train them to do those workflows and to understand how the model works.
An insufficient pool of talent with training on VBC models persists, making it more difficult to hire
talent to operate VBC models that seamlessly integrate primary care services. This was cited as important for
creating sustainable models that effectively integrate primary care services.
Internal Organizational Characteristics
Physical Layout of Clinic: A necessary condition for enabling integration of primary care services that was
cited by several interviewees was the physical structure of the clinic. Although physical space is often
constrained in medical settings, the design of the physical space can promote or prevent integration efforts.
If, for instance, the space was too small to physically allow for the co-location of services or collaboration
among providers, it became challenging to integrate multiple primary care services.
The physical space can also feature or shield specific services. With behavioral health, for example,
co-location with other services destigmatized the service. Patients could be in the waiting area for any type of
service, not only for a behavioral health appointment. As one PCP and child psychiatrist noted:
It’s a better patient experience, it’s destigmatizing because patients are sitting in a waiting room that says pediatric clinic or adult medicine clinic, but it’s not identified as a behavioral health clinic. And that’s really destigmatizing, it’s a regular primary care clinic.
Integrating and co-locating several services under one roof also means that it is more convenient for
patients. Patients no longer needed to visit several medical facilities to receive multiple services. Although the

36
physical structure of clinical settings was described by interviewees as important for integration, others
discussed the evolution of the in-person clinic model to a “decentralized” model of delivering care in the
community. This is a “community centered construct,” whereby medical teams are in the community
providing care. In this model, the “teams are not based in a clinical setting,” meaning that physical space is a
non-issue. Overall, however, my interviews largely confirmed that the design and layout of the physical clinic
can support or hamper activities to integrate primary care services.
Technology and Workflow Design: The design and implementation of technological systems that support
workflows can determine the effectiveness of integration efforts of primary care services. If technology
systems do not interoperate or align with clinical workflows, integration can become challenging for
providers. One VBC start-up noted that an important lesson was to focus on the workflows, and
subsequently design the technology systems to support the workflows:
Because we started small and we didn’t have a whole bunch of capital on day one and, what we did was focus on the workflows, focus on what you’re trying to get done, [we] built a bunch of Google sheets and PowerPoint presentations to train people, and really honed and developed what were the right workflows. And then we could come back and use technology to structure and coordinate those. Once the organization had identified the appropriate clinical workflows, technology was used to
structure direct and indirect patient care. This created accountability among associates because the technology
could be used to delegate tasks to individual clinicians. The technology could also be used to manage clinician
time between appointments. Leaving empty space in provider schedules for unanticipated situations that
arose was deemed important. When schedules could not accommodate patients for follow-up appointments
or if patients were “referred out” to other specialty practices, the chances of successful follow-up and long-
term care were limited.
Lastly, the need and “huge opportunity” to harness the power of data in decisions-making was noted
by interviewees. Triangulating different sources of data can inform decisions for patient care. Data being used
at the point of care and not only retrospectively were cited as necessary considerations for integration of
services.
Organizational Reporting Structure: Interviewees expressed that facilitating the integration of primary care
services is a managerial approach with a supporting organizational structure. With an aligned organizational
37
structure, “the management approach enables the soft pieces.” One example that was shared with me was
from a behavioral health setting. In this case, behavioral health personnel reported to a different leader than
primary care associates. The organizational structure was modified so that behavioral health and primary care
reported to the same person. The Primary Care Director managed the medical and behavioral health
providers as well as social workers, child psychiatrists, and CHWs. The managerial approach and supporting
organizational structure were used to “design a more rational system so that people can focus on what they’re
trained to do…This is a systems approach to making this work.”
Relationship-building and Teamwork: Multidisciplinary teams “teaming together” were deemed to be
central to the integration of primary care services. While care teams often include PCPs, NPs, PAs, MAs, and
in some cases scribes, the extension of the care team to include other non-traditional actors that assisted with
providing care was cited as essential. This included CHWs, medical case workers, family members, and non-
professional caregivers. The medical staff could then focus on the “need to team with everybody around a
given patient.” This meant that the team caring for the patient expanded to include “everybody in the office,”
ranging from the front desk scheduler to staff in the billing department. Each person had a role in the health
journey of the patient. Even though the longest-existing and closest teams “talk to one another as family,” it
was suggested by interviewees that teams be expanded to include non-traditional actors that are also engaged
in patient care and coordination.
The expansion of care teams also meant that providers could specialize in providing care that was
within their medical training. Commenting on the expanded role of primary care doctors, one interviewee
said: “There’s so much pressure now for primary care doctors to become psychiatrists or to be prescribing all
these psych meds.” A care team that allowed for PCPs to engage in a warm handoff to a psychiatrist or other
provider that was co-located in the physical space allowed for teaming and stronger relationships. It enabled
providers to be at ease in deciding whether to deliver more complex care that may be outside their expertise.
Finally, an intimate understanding of the local community – the needs of patients in the community
and resources culturally tailored to the community – were important for building relationships and integrating
care. An interviewee at a county health department described the role of teams in his context:
38
We have teams that essentially catch people when they fall through the cracks of our delivery system. And we use community health workers and other people who have a certain cultural competency to engage them and try to bring them back into the system. And where there are no systems, we try to create them.
Effective integration of primary care services requires teams collaborating with people with whom
they may not routinely work. It was also important for teams to be integrated into the communities where
they operate, and in certain positions, be from the community where they are working.
Leadership Capabilities and Building Organizational Culture: Leaders made integration of primary care
services occur. Payment models only take a clinic’s operations so far, though leaders are central to
organizational changes that promote integration. Leadership can motivate committed associates to make
necessary changes, though discipline is required to see these changes come to fruition. The interviewee with
expertise in telemedicine further commented on leadership:
Technology, telemedicine, payment reform, access to specialty services, all these things, these are all really important individual components, but to actually link them together in an effective way takes a really dedicated leader or set of leaders who are willing to put a lot of time and energy into making things work. Like it doesn’t just happen on its own.
The extent to which leaders can create an organizational culture that promotes integration was cited
as essential by interviewees. The cultures of different medical environments – medical culture, behavioral
health culture, substance use disorder culture – can be very different, so bringing employees together across
different services requires leaders that can create an inclusive culture. “It takes effort to try to merge cultures”
to “bring people on to the same page” to blend organizational cultures.
The complex management skills required by leadership to form and foster organizational cultures
that supported integrated were also mentioned. This required persistent leaders as well as tolerance for
iteration and experimentation to identify models that work and fit the needs of the patient population. Lastly,
building organizational cultures required concerted communication from leaders to team members. This was
found to often occur in town halls with all associates, team meetings that celebrated accomplishments and
reviewed protocols for care delivery, or daily or weekly huddles that could structure indirect patient care.
Language of Primary Care: The language of primary care was cited by several interviewees as a challenge to
integrating primary care services. Definitions of primary care were seen to be too narrow, and the language to
39
describe workflow processes as being antithetical to integration. For example, one PCP and child psychiatrist
noted the nuance in referral language:
The specialty clinic is primary care, we don’t refer anyone out, so that language of refer out is not very meaningful. We refer in, everyone is referred in. Because of that, we have a much higher success rate and so that’s I think a huge piece of trying to understand those subtleties about when people talk about integration.
Similarly, a PCP at a VBC start-up indicated that the definition of primary care should be expanded to include
other features of care delivery:
Those of us who are clinically trained tend to have a pretty narrow definition of what it is to take care of patients. And what we’ve learned is that definition should be far more expansive, and should include things like educating people on the value of primary care, which many people now use the term patient engagement to include, but helping people with affordability, helping them understand their Medicare/Medicaid benefits, engaging them in their community in a way that lowers the bar to participate in a primary care model.
The everyday language used by the healthcare community to describe primary care and its activities
can make integration of services difficult. This is particularly the case when there is nuance in meaning of the
language used in primary care.
Summary
In examining the first research question – “What is the current landscape of integrated primary care
services in the US?” – using the Singer et al. (2018) theoretical model as a foundation, interviews with thought
leaders established that contextual factors influence the extent of integration of primary care services. The
current landscape of integrated primary care services as well as the environment within which primary care
centers operate is shaped by external market and internal organizational characteristics. These characteristics
often shape the boundaries by which primary care facilities can integrate services. The interviews also
identified primary care models that effectively integrate basic healthcare services. These models have been
pioneered by emerging start-ups as well as community health centers. Nonetheless, the extent of integration
of basic healthcare services remains predicated on leaders and teams to promote and maintain these activities.

40
3.3 Integration of Primary Care Services at the Walmart Health Center
With an understanding of the features relevant to the current landscape of integrated primary care
models, this section outlines the results of the second research question: “How can the integration of primary
care services be optimized at Walmart Health?” This research question is explored from the perspective of
the Singer et al. (2018) theoretical model using the Walmart Health Center in Dallas, GA as the setting for
analysis. In order to frame the discussion on how Walmart Health may optimize the integration of primary
care services, it is important to recognize the immediate and substantial impact of the Center on people’s
everyday lives. Given this context, this section commences with a narrative describing the effect of the
Center. It is viewed through the lens of associates employed at the Dallas, GA location. This section follows
with a discussion of integration of primary care services at the Center. This is examined through the lens of
the five types of integration included in the Singer et al. (2018) theoretical model: organizational features
(structural and functional integration), social features (normative and interpersonal integration), and activities
(process integration).
An Early Narrative of the Impact of the Walmart Health Center
The Walmart Health Center in Dallas, GA appears to be meaningfully and substantially changing
people’s lives. People from within the community and further afield are visiting the Center to receive primary
care services many have not gotten for years. It seems that Walmart Health has designed an experience that
meets customers’ needs; is affordable, convenient, and accessible; and delivers high-quality healthcare
services.
The opening of the Center has led to increased access to basic healthcare services for individuals and
families. Anecdotally, many people receiving care at the Center have not visited the doctor or dentist in three
to five years, and some even longer. The cost was simply prohibitive, the system too complex, the distance
too great. Patients have underutilized and delayed care for so long that many do not realize they are in poor
health with undiagnosed health conditions. Consider the type 2 diabetes patient who indicated that he simply
41
injects himself with insulin when he “feels funny,” or the dental patient that “hadn’t been [to the dentist] for
thirty years. He went as a child, and then couldn’t afford it.”8
With the Center opening its doors, patients are now receiving needed care. One of the lead providers
shared with me the direct impact of the Center on health outcomes:
Patients are getting better results faster. We are getting more patients to follow-up with their treatment plans because behavioral health, pharmacy, [community] health workers are following up on needs, affordability because patients are coming back more for follow ups, better communication, we are seeing the results faster in terms of better care in terms of them picking up their medicine.
Beyond receiving an annual physical exam or a dental cleaning, access to healthcare services has led
patients to become overwhelmed with tears of joy. “It is very eye opening to hear that the patients are really
wanting these services and to the point of every week, we have patients who cry because of the access,” noted
a lead dentist.
The multiple healthcare services that are offered under one roof at the Center has also created a
convenient and accessible experience for patients. While Dallas is less than an hour’s drive to Atlanta,
Paulding County (where Dallas is located) is usually considered rural Georgia. This means that the
“professional staff is limited [and that] driving into Atlanta traffic, and the hours of traffic, is an obstacle to
getting to appointments.” The ability for patients to receive several healthcare services at the Center allows
for more time to be spent with family and loved ones.
For the associates employed at the Center, the impact on their lives – and often their families’ and
friends’ lives – has been equally considerable. Almost every associate I interviewed at the Center mentioned
their support of the broader mission to change healthcare in the US. Associates were enthusiastic, excited,
and extremely grateful to be part of the Walmart Health story. A few quotes reflected the satisfaction of the
associates at the Center when I spoke with them:
I am really proud to be part of this movement. I believe in the vision that they have with this, and I am happy to be here.
8 You may wonder whether these are simply anecdotes that have been shared with me by Walmart Health associates, and are unreflective of the US population or the population being seen at the Walmart Health Center. The reality is that Walmart serves America. I do not believe that these stories are one-offs, though rather are reflective of people’s life situations across the country. I could include dozens of other stories that were shared with me on the impact of the Center.
42
I think it’s an amazing concept. For me, I’m just excited about the future of it, the success of it being one of the first clinics. I think it is going to change the industry of healthcare.
We are exploring the new world, we are on the ship of healthcare reform and we are being successful. The associates have been the backbone to creating a caring, friendly, and empathetic culture, not to mention
the source of the Center’s word-of-mouth marketing efforts. One dental associate shared with me her
experience of receiving services at the Center, and subsequently referring others in her network:
I had an [annual] physical here…It cost me $66. Elsewhere this cost me $150. I felt like I had spent $300. I referred my husband, I referred my son. Here you are your name and not a number.
Walmart Health set out to change the delivery of healthcare in the US. From the perspective of cost,
convenience, and care, the model that Walmart Health has deployed appears to be working. Patients are
receiving needed care, volumes are high, and associates are excited.
Optimizing the Integration of Services at the Walmart Health Center
The early narrative on the impact of the Center on the lives of people residing in Dallas and the
surrounding community provides context for exploring the integration of primary care services. Using the
Singer et al. (2018) theoretical model, this section further discusses sentiments from interviewees employed at
the Center on the existing state of play of integration of primary care services. It is organized into five
sections that align with the theoretical model: (1) structural integration; (2) functional integration; (3)
normative integration; (4) interpersonal integration; and (5) process integration.
Structural Integration
Organizational Structure: The organizational structure adopted by Walmart Health has potential to
facilitate integration of primary care services, though associates also proposed several changes. While the
Clinic Manager is responsible for all operations at the Center (“everything is technically under my roof,” he
says), he only has direct responsibility of segments of the medical team. This includes the NPs, MAs, CHWs,
and radiology technicians. The medical providers as well as associates in other service lines (such as dental
and behavioral health) report to others at Walmart’s Home Office. The associates mentioned a more

43
streamlined approach to clinical and operational oversight may facilitate greater integration of services within
the Center.
Physical Space Design: The physical layout of the Center enables co-location of services and collaboration
among associates. This allows providers from various service lines to “have immediate access to a [medical]
physician [by] walk[ing] across the hall.” The medical team also mentioned the benefit of having other
services co-located at the Center by doing warm handoffs to other service lines: “We can hand off services to
the social worker…That personal interview that they have is just enough for the patient to go through with it
[the appointment],” noted one PCP. From a clinical perspective, providers additionally cited the benefit of
obtaining clinical guidance from colleagues. One provider noted that it is: “Easy to turn around and say what
do you think about this?”
One downside raised by associates related to the physical space was the lack of privacy. The
workstations and check-out area of the Center is an open space. Conversations with or about patients –
which may include sensitive information – may be overheard. The CHWs also believed physical space and
privacy were challenges because they do not have a dedicated workspace. A patient is unable to share their
thoughts and feelings if they do not feel comfortable in the space. “I don’t want it to be a ‘me statement’, but
it’s for the patients,” noted one CHW.
Financial Payment and Prices: Services provided at the Center were cited as “so affordable” by associates
who had used the services. The affordable prices have led patients to often pay out-of-pocket because the
direct cash prices are less than the co-payments with their health plan. Since many health plans have high
deductibles, it can often by less expensive for patients not to use their insurance. Even though patients may
pay out-of-pocket for services, challenges were raised with regards to the Center only accepting select
insurance plans. For example, Walmart Health may accept a patient’s medical insurance but not their dental
insurance. It was believed that with time, additional insurance plans would be available.
The way in which providers are paid is also aligned with their ability to integrate primary care
services. Providers are salaried, so they are not as beholden to the volume demands of traditional FFS

44
practices. As one dental provider noted: “We are taking the financial burden off the clinicians. They do not
need to try to upsell patients. We here are salaried and not production driven.”
Technology Capabilities: Each service line offered at the Center uses its own EMR platform. The most
cited challenge by associates was technology. “Technology is really the challenge,” noted a care host.
Associates also believed they would feel more comfortable if technology were improved:
Ultimately [a technology fix] would help everyone feel more at ease, to feel more conducive to the work environment, not to fear what happens if. We have had so many ups and downs that people don’t trust it. It creates tension and apprehension.
Although a single platform may facilitate greater integration of services, it is unclear whether access
to patient information from other service lines would be beneficial to all provider types. One provider
suggested that dataflows from his service to others may be more unidirectional to medical, suggesting that:
“There is potential value for sharing of medical records. It would be more one way…to medical. There isn’t a
whole lot that they are doing over there [in medical] that I’m interested in or need to see.”
Finally, regulations were cited as a barrier to data-sharing. In the case of behavioral health, counselors
can view a patient’s medical record, though medical providers are unable to view behavioral health
information. As one of the behavioral health counselors mentioned: “The stigma attached to mental health,
and we can’t even share the information with the doctor. It does keep it all very hush hush.” The inability for
data-sharing across provider types from a regulatory perspective inhibited addressing the collective needs of
the patient. Interviewees also noted that information sharing is only done with consent from the patient.
Functional Integration
Definition of Roles: Since the Center is still relatively new, establishing exact roles and responsibilities was
an ongoing activity for the associates. Once positions become more solidified, there may be opportunities for
greater integration of primary care services. As an example, the care host position includes several
responsibilities: welcoming and checking in patients (front line care host); bringing patients to the assigned
exam room, completing patient vitals, and supporting the providers (clinical care host); completing
phlebotomy, immunizations, and employment screenings in the lab diagnostic space (phlebotomist care host);
45
and coordinating and managing the flow of patient traffic (charge master). The lack of clarity and
accountability with the care host role has at times led to challenges. As one provider noted: “One MA (care
host) for one provider, it should be like that. People don’t know their jobs. They are trying to learn. One
person is in four different places.” The associates indicated that having one care host assigned to an
individual provider may assist with streamlining patient flow and integration. The potential consequence of
poorly defined roles is patient error. One associate indicated that: “We could be missing stuff and that could
be bad for us. Patients are also confused. They are frustrated too a couple of times.” The integration of
services could be better optimized after solidifying workflows, operations, and roles.
Policies, Procedures, and Protocols: The Center has a dedicated position for ensuring regulatory
compliance. Associates alluded to the Stark Law, which inhibits providers from referring patients to services
operated by entities with a financial relationship. This translates into several comments about providers
offering choice to patients in where they receive services (“I try to let everything be patient choice”). As
another associate noted: “I don’t want my session to be marketing of other services.”
Normative Integration
Creating a Caring Culture: The Center is “a start-up” with “lots of unknowns.” Walmart Health’s focus on
iteration and experimentation – “the test and learn environment” – was reflected in the culture. As one
associate noted: “They [senior leadership] want you to think outside of the box.” While “there’s a lot of stuff
we need to change, we are still working on it,” was a common sentiment among associates. Although the
company continues to “learn what will work and what doesn’t,” its history of listening to customers is
reflected in a patient-centered culture. One associate described the culture as being:
People minded and [having a] heart for the people, regardless if you have insurance or are self-pay, you are treated the same. We treat you the same if you are the janitor or the CEO, rich or poor, you are not treated differently because of your socioeconomic status.
The culture was inclusive, with one provider noting that “you don’t feel like you are by yourself” and
another associate suggesting that she was “here to help one another out.” Associates felt their voices and
opinions were heard and acted upon. “I feel like I’m heard, feel that I am an integral component of the

46
operation,” said one associate. Overall, associates enjoyed employment at the Center, with organizational
values and a culture that is reflective of Walmart more broadly.
Professional Development Goals: While certain associates employed at the Center were hired from other
divisions across Walmart, others came from hospitals and medical practices in the communities surrounding
Dallas, GA. Associates were motivated to advance their careers while working at Walmart, and saw their
employment at the Center as an opportunity to do so. For example, a dental treatment coordinator cited her
previous experience stocking shelves at another Walmart location. She “took a chance” to apply to a dental
position at Walmart Health, and was excited when she received an offer. She said that her current position:
“Doesn’t compare. It’s what I’ve been wanting to do since I finished dental assistant school in 2015.”
Another care host mentioned her desire to participate in Walmart’s Live Better U College $1 a Day Program.
Associates enrolled in this program earn a bachelor’s degree with tuition being $1 per day.
Interpersonal Integration
Communication and Collaboration: Associates most frequently interact with associates within their own
service line. For example, the dental technician coordinators collaborate with other dental associates.
Similarly, care hosts interact most directly with other care hosts and medical providers, so they can “keep the
[patient] flow going.” These interactions were largely predicated on operational issues rather than clinical care.
Most associates indicated consistent communication among the service lines – “daily, multiple times
throughout the day” – and that they “all work hand-in-hand” to deliver care to the patient. Associates further
noted that communication between the service lines becomes most important when conflict arises. “If there
is a conflict, we have to go back to talk with all the different service lines,” indicated one care host. For the
most part, communication appeared to occur, though others expressed issues with communication. An
administrator mentioned the communication challenges in coordinating patient care by the medical team:
Whether that’s the charge care host communicating with providers that there’s a patient in the room, providers communicating with the lab care host that there’s a lab that’s needed, and then bringing them back to the room.
Other providers outside of the medical team were unclear on the extent of communication between
the other service lines. They believed there were opportunities for increased collaboration between the
47
providers as it relates to clinical care and referrals to other services. In this regard, the medical team drives
much of the communication with other service lines, with limited communication between services outside of
medical.
Team Dynamics: Team meetings occurred at the individual service level. The Clinic Manager hosts team
meetings with the medical associates that focus on “a little policy, a little procedure, anything else they want
to discuss.” Achievements and promotions are recognized, and changes to staffing are discussed as additional
Centers open. Care hosts also have team huddles every day to cover operational issues. At the leadership
level, the Clinic Manager, the lead PCP, and the lead NP meet on a weekly basis to discuss operations. The
lead dentist and PCP also meet on occasion to discuss capabilities and referrals between dental and medical
service lines. A dentist indicated that: “We each can be advocates of each specialty to take care of the
patient…I don’t want to only be focused on dental because you just see the tree and not the forest.”
Providers in other service lines such as optometry and audiology expressed interest in more interdisciplinary
meetings with the other providers. One dental treatment coordinator described the team dynamics as:
[We are] working together as a team, not just in our particular location or dental but working in Walmart Health. We refer patients to us, we communicate with them, we refer them.
Employment Training: Walmart Health associates employed at the Center underwent training on Walmart’s
policies and procedures. This included understanding Walmart’s history and culture as well as exercises on
delivering moments of care to patients. Each service line also had their own training. For example, the CHWs
had training provided by the University of Pennsylvania’s Penn Center for Community Health Workers
IMPaCT Training Program. This certified the CHWs to become nationally recognized. Similarly, the dental
team had training provided by dental partners to train associates on procedures, equipment, and technology.
Associates were impressed with the training, with selected associates indicating that the training could be
more adapted for a retail context than a hospital or medical environment.
Process Integration
Warm Handoffs and Clinical Referrals: Integration between service lines often “occurs organically.”
Medical associates interact most commonly with associates from the other service lines. The most common
48
pathways between services were medical to dental, and medical to behavioral health or CHW. In the case of
audiology, several older patients have presented to the Center with blocked ears. This means that audiology
tests cannot be performed. In these cases, the audiologist has coordinated with the care hosts for medical
providers to remove the blockage so the test can be performed. This has led to interaction between the
audiology and medical teams. Similarly, since the behavioral health counselor cannot prescribe medications,
there are often interactions between medical and behavioral health service lines. Lastly, other associates
mentioned interactions between dental and behavioral health, particularly with regards to drug use or
emotional issues. As a dental treatment coordinator described: “They [the patient] share a lot in that chair.”
Upon occasion, a dental patient is referred to behavioral health. There is also interaction between dental and
medical at the clinical level with regards to addressing cardiovascular and periodontal needs. Every dental
patient has their blood pressure tested. When it is high, a referral will be made to the medical team. At the
end of the day, however, warm handoffs, clinical referrals, and integration of services were due to the
“motivation of the physicians.”
Operational Workflows: Scheduling and patients with multiple appointments can cause challenges in
operations. Walk-in patients can delay operations or a patient can present with multiple chronic issues. A 20-
minute appointment can turn into an hour. In addition, approximately every 3 in 10 patients visit the Center
with multiple appointments. This can often cause challenges for associates as a result of the technology
scheduling platform. The technology platform does not alert the care host that the patient has multiple
appointments. Despite the technology challenges, associates said that fitting in a patient who required more
than one appointment varied depending on the service. For example, it was difficult for patients to receive
dental and optometry services, while medical and behavioral health teams were more willing to try to fit
patients in if needed.
Workflows were also “still not solidified,” meaning that associates were at times “doing things off the
cuff.” Even though the workflows are not fully formed, associates mentioned that they do not feel this is a
“production office” or an “assembly line.” As one dental treatment coordinator noted: “We are literally here
to help people in need who can’t afford the high-end prices, real prices, and that’s the difference.”

49
Other associates cited challenges with patient follow-up. The dental team performs well at following
up with patients to schedule their next appointment, though this was not always the case with the medical
service line. The CHWs also indicated they were involved with follow-up with their patients:
Continuation of care is a huge thing. It’s not just, ‘Here is your prescription.’ I can take you to the pharmacy. I’ll call them later to see how they are feeling. I encourage that communication because so many people feel they are alone in their care.
Summary
This section has explored the second research question: “How can the integration of primary care
services be optimized at Walmart Health?” The interviews I conducted with associates at the Walmart Health
Center in Dallas, GA provided me with a baseline understanding of the current operations. It also helped me
to identify the extent of integration of primary care services as well as possible approaches for optimization.
Using the Singer et al. (2018) theoretical model as a guide, the interviews established that the Center has the
foundational components in place – and is already engaged in activities – to support the integration of basic
healthcare services. Across each of the five dimensions presented in the theoretical model, there are efforts to
integrate healthcare services. Given the early operational life of the Center, it is unlikely for the company to
have fully established how to most effectively integrate basic healthcare services. Overall, however, the basic
tenets, structures, and people are in place to optimize the integration of services in the months and years to
come as the company solidifies their operating model. While a discussion on other relevant insights gained
from the interviews follows, the section on recommendations provides specific strategies on how Walmart
Health can optimize the integration of primary care services at the Center.
50
4.0 DISCUSSION & RECOMMENDATIONS
The Singer et al. (2018) theoretical model provided me with a guide to explore the research
questions. It offered me a frame of reference to understand the current landscape of integrated primary care
services as well as the extent of, and opportunities for, effective integration at the Walmart Health Center in
Dallas, GA. The qualitative interviews helped me establish that contextual characteristics influence the extent
of integration of primary care services. They also enabled me to conclude that the existing structures,
operations, and people at the Center are already engaged in preliminary activities that support the effective
integration of basic healthcare services. Integration activities are occurring even with the early operational life
of the Center.
Despite the identification of salient insights from the qualitative interviews, the results are presented
in a way that aligns with the theoretical model. I believe this presentation excludes other observations that are
relevant to the research questions. Given these omissions, this section further discusses the results by placing
them in the broader context of Walmart Health. It also proposes recommendations for primary care
organizations, including Walmart Health, to facilitate greater integration of primary care services.
4.1 Discussion
Setting aside the Singer et al. (2018) theoretical model, this section attempts to organize and interpret
the most meaningful insights I have gained from the qualitative interviews on integration of primary care
services. I have identified five themes that are related to the current landscape of integrated primary care
services as well as the optimization of integration of primary care services at the Walmart Health Center.
1. People have high hopes for Walmart to change healthcare, though others tread with caution.
There are high hopes – and not to mention intrigue – related to Walmart’s foray into healthcare.
With Walmart’s focus on listening to their consumers, many with whom I spoke believe Walmart can bring
the voice of the consumer into healthcare in a meaningful and considerable way. For many interviewees, it
was a sigh of relief that at last people could have their health needs met in an affordable, convenient, and

51
integrated manner. The sentiment was similar among associates with whom I interviewed at the Center. Every
one of them was excited about Walmart’s ability to change healthcare for consumers. They are the company’s
biggest cheerleaders and are organically spreading the word to their family and friends in the community.
Since many of the associates worked in other nearby healthcare settings before joining Walmart Health, they
understand why they do what they do and why Walmart Health is different. They are Walmart Health’s
greatest asset.
Where there was less enthusiasm with Walmart’s entry into healthcare was among interviewees
representing already established healthcare organizations. They often viewed Walmart Health with
apprehension, and at times, dismissal. They are concerned that Walmart Health’s low prices will erode their
margins and dissolve their profits. Others (who were usually based on the East and West Coasts) believed
Walmart Health would not be in their backyard any time soon. For them, there was no need to be concerned.
As Walmart Health considers optimization of the services offered and eventual geographic
expansion, there may also be opportunities to clarify the type of care provided. The “muddled lexicon” of
primary care combined with the rapid growth of urgent care centers has contributed to misperceptions in the
marketplace on the services offered (Miller, Cumming & Lewis, 2018:171). Patients at the Center are
uncertain as to whether primary care, urgent care or both types of care are provided. Given the varying
expectations of patients, this lack of clarity may make it more difficult to integrate services at the Center.
2. Walmart Health could further fragment the healthcare system without continuity-of-care.
Retail care clinics have often been criticized by leading medical associations9 for their poor
integration into the broader healthcare system (AMA, 2016; AAFP, 2014; AAP, 2006). The leaders of these
medical associations contend that retail care clinics simply provide episodic and uncoordinated care by non-
physicians, which is at odds with the longitudinal and directed care offered by established medical homes
(AMA, 2016; AAFP, 2014; AAP, 2006). They further contend that the lack of integration with the medical
9 Most prominently by the American Medical Association (AMA), the American Academy of Family Practice (AAFP), and the American Academy of Pediatrics.
52
home can disrupt the patient-PCP relationship and does not provide referral pathways to more sophisticated
specialty care.
Given the concerns with retail care clinics, Walmart Health risks being perceived as further
fragmenting the healthcare system by not providing continuity-of-care. This may include access to specialty
care services that may be needed for patients presenting at the Center.
There are several ways Walmart Health could ensure continuity-of-care through access to specialty
care services at the Center. As a start, Walmart Health could build on Walmart’s Centers of Excellence (CoE)
program. This program enables Walmart associates needing advanced medical care (such as cardiac treatment
or hip and knee replacements) to receive care at premier institutions across the country (Woods, Slotkin &
Coleman, 2019). Examples include the Cleveland Clinic, Geisinger Medical Center, and Kaiser Permanente
Irvine Medical Center. These (and other) institutions have been identified as delivering high-quality,
affordable specialty care services. Walmart Health could leverage the CoE program in unique and novel ways
to offer access to specialty care services at the Centers.
Walmart Health could also consider leveraging technology to integrate specialty care services.
Telemedicine is one example, which has been most widely used in offering advanced mental health services
(such as telepsychiatry). Telemedicine could expand access to specialty care services in the Center. Lastly, e-
consults could link PCPs with specialists using technology in the Center. E-consults would enable access to
leading specialists across the country for guidance on a variety of conditions.
3. The volume of patients at Walmart Health could lead to associate burnout.
During the interviews I conducted, I learned that PCPs have different values relative to other
physicians. When deciding on a medical field for one’s career, students often have different motivations.
Some may be more focused on pursuing specialty fields that center on technical expertise, while PCPs are
often more inspired by the ability to promote health equity, social justice, and public health outcomes. Once
PCPs begin practicing medicine, they often realize that their visions of primary care are in opposition to the
daily burdens of administrative tasks and cumbersome technology platforms. They may also find that their

53
ability to influence lifestyle behaviors is limited and takes up precious time with patients (Kim et al., 2018).
The combination of these daily routines often means PCPs become isolated in their practices and suffer
burnout.
Physician burnout10 is high in many medical fields and PCPs usually rank among the highest (around
40 to 50 percent of family medicine physicians indicate they are burned out) (AMA, 2019). Burnout impacts
physicians through declines in interpersonal relationships and increases in substance use and early retirement.
It can also impact patients by creating higher medical errors and poorer overall satisfaction (AMA, 2018).
For Walmart Health, there could be concerns with physician burnout as time progresses and
additional sites open. There is a tremendous amount of excitement associated with the opening of the Center,
though the volume of patients is high. One medical associate I interviewed indicated to me that: “Keeping up
with the demand is the challenge.” The convenient hours contribute to long days for the associates and could
result in burnout among associates. The associates are the greatest supporters of Walmart Health, though
enthusiasm could fade if they feel overwhelmed with patient volume and long hours.
With the integration of primary care services at the Center occurring as a result of motivated
providers, the care provided to patients may be impacted if providers and associates suffer burnout. PCPs
may neglect to provide a warm handoff to a patient or miss required steps in delivering care. If they suffer
burnout, PCPs will only be motivated by moving through their long list of patients.
Establishing appropriate schedules, workflows, and care delivery models are unlikely to be generated
by the associates at the Center. Rather, they will be identified and supported by Walmart Health in
Bentonville, AR. In this regard, identifying ways for associates to avoid burnout will ensure that Walmart
Health remains a great place to work. Early ideas of ways physician burnout could be avoided would be to
encourage CHWs to meet with every patient to offer lifestyle counseling and plan preparation; offer
multidisciplinary team-based care so that providers from multiple service lines interact on care delivered to
patients; and consider hiring scribes to assist with administrative tasks.
10 The American Medical Association (AMA) defines physician burnout as: “a stress reaction marked by depersonalization, emotional exhaustion, a feeling of decreased personal achievement and a lack of empathy for patients” (AMA, 2020).
54
4. Regulations and reimbursement at Walmart Health can in fact support integration.
As the US healthcare system shifts from FFS to VBC reimbursement, a common area of
conversation with interviewees was the trade-offs with operating each type of model. While an interviewee
from a primary care start-up indicated that his organization had decided to operate a VBC model from the
outset, others employed at organizations with more traditional FFS contracts had a different approach to
VBC. What was most compelling from these discussions was that most organizations using FFS constructs
aimed to create a self-sustaining operation prior to moving into VBC arrangements. They also indicated that
VBC models were able to support greater integration of services because integration was viewed as an
inherent component of the operating model. Given Walmart Health’s current path of largely operating a FFS
reimbursement model, the company may consider establishing a sustainable FFS offering while
simultaneously exploring VBC arrangements. This would enable Walmart Health to build a sustainable
business model from the outset, while additionally considering VBC arrangements.
Where a VBC reimbursement model may become more challenging for Walmart Health is in the
context of the legal and regulatory environment. As I conducted the interviews, I learned that the legal and
regulatory environments were often unsupportive of integration efforts. The Physician Self-Referral Law
(commonly called the Stark Law), a federal statute that prevents direct self-referrals between entities operated
by the same company, was commonly cited by interviewees. While the Centers for Medicare & Medicaid
Services (CMS) is undergoing a review of the Stark Law to support the transition to VBC arrangements,
operational challenges may remain (CMS, 2019). At the Center, the Stark Law was framed as an issue of
patient choice. Patients could determine where to receive other services or their medications. Although
policies were often discussed as enabling or inhibiting integration efforts, I learnt that effective integration
efforts were the result of dedicated leaders operating in the existing regulatory environment. If leaders aspire
to integrate services, they can do so under the law.
55
5. Leaders inspire change, managers get things done.
The vision of change among leaders is the final ingredient needed to integrate basic healthcare
services. Leaders set the tone and create a culture that enables or inhibits innovation, experimentation, and
integration. Often the integration of healthcare services requires new structures to be built, teams to adapt,
and a redesign of existing workflows. This can only be undertaken and achieved with the support, dedication,
and discipline of leaders. At the end of the day, the extent and effectiveness of integration efforts were
dependent on leaders prioritizing those activities. Once leaders have set the strategic direction for integration
efforts, managers are required for executing on the vision and getting the job done. They can only do so if
they are empowered.
Effective integration of primary care services at the Centers is unlikely to come from the associates,
but rather from corporate leaders at Walmart Health. They are the ones who will see integration efforts
through and foster them over time. If leaders place value on the integration of healthcare services at Walmart
Health, it becomes a priority. This is the view I was left with having spent considerable time speaking with
interviewees and in understanding the Center’s operations in Dallas, GA.
4.2 Recommendations
In bringing together the results obtained from the interviews and themes explored in the discussion,
this section outlines several recommendations to facilitate the effective integration of primary care services.
These recommendations provide a roadmap for primary care organizations such as Walmart Health to
embark on the journey of integration. The recommendations are separated into activities for the short-,
medium-, and long-term, though all can be achieved in a twelve-month period.
Summary of Recommendations
The interviews with thought leaders facilitated the identification of recommendations that promote
the effective integration of basic healthcare services. Fifteen high-level strategies, which are categorized into
five short-, medium-, and long-term recommendations, are presented in Table 9. Since every primary care

56
organization is at a different stage of operational life, it is not anticipated or expected that any organization
fulfills all strategies.
Table 9: Thought Leader Criteria for Integration of Primary Care Services
Short-term recommendations: 3-6 months
Design the healthcare offering around the consumer.
Create a physical space that provides privacy and anonymity for patients.
Foster warm handoffs of patients between providers.
Form multidisciplinary care teams to address the full needs of the patient.
Host huddles to review patient clinical care and enable communication between providers.
Medium-term recommendations: 6-8 months
Align organizational reporting structures to promote integration.
Provide management skills and training to clinic managers.
Train physicians in providing integrated primary care.
Offer specialty services in-house either in-person or using telemedicine.
Link the clinic to the community as well as to family members and caregivers.
Long-term recommendations: 8-12 months
Use data to make data-informed decisions.
Move to VBC following the creation of a sustainable FFS offering.
Build technology around workflows.
Provide healthcare services across several temporal dimensions.
Promote leaders and foster cultures and mindsets that are supportive of integration efforts.
Short-term Recommendations
Design the healthcare offering around the consumer: By engaging with, and listening to, consumers,
primary care organizations can design the healthcare journey around the needs, preferences, and desires of the
consumer. These insights can be gathered using primary research methods such as interviews, focus groups,
and ethnographies. Designing the healthcare experience around the consumer can support the integration of
primary care services because it can ensure that the most affordable, convenient, and appropriate care is
offered.
Create a physical space that provides privacy and anonymity for patients: The physical design of
primary care facilities can affect the extent to which patients are willing to share their health concerns.
Physical spaces should promote privacy and anonymity for patients. Privacy means that patient information is
not shared openly among providers and associates, while anonymity allows patients to receive services
without others necessarily knowing. Ensuring privacy and anonymity can facilitate integration of services
because patients may be more willing to return for care and receive multiple services.
57
Foster warm handoffs of patients between providers: Warm handoffs are an intuitive way for providers
to ensure patients receive appropriate care by facilitating an introduction between the patient and another
provider. Providers may use warm handoffs to refer patients to other services and are most effectively used in
tandem with multidisciplinary care teams.
Form multidisciplinary care teams to address the full needs of the patient: An integrated approach to
delivering care is the formation of multidisciplinary care teams. Providers from several service lines
collaborate to determine the best care for a patient. This may initially focus on high-risk and older patients,
and in time expand to other populations. This would further enable multidisciplinary care teams to provide
personalized care based on the age, gender, and health characteristics of the patient population.
Hold regular huddles to review patient clinical care and enable communication between providers:
With the formation of multidisciplinary care teams, team meetings such as huddles can be used to review
patient records. Several primary care clinics additionally leverage technology to host huddles and provide
indirect care. Clinical huddles can also encourage collaboration, communication, and integrated care among
providers.
Medium-term Recommendations
Align organizational reporting structures to promote integration: Organizational reporting structures
can promote or inhibit efforts to integrate primary care services. More closely aligning reporting structures so
that Clinic Managers oversee the full operations of primary care clinics can facilitate greater integration of
services.
Provide management skills and training to clinic managers: Clinic Managers are usually responsible for
overseeing the daily operations of the clinic and resolving operational issues. Given the managerial complexity
of overseeing several service lines, Clinic Managers should be provided with management skills and training
to enable them to better perform their jobs and navigate these scenarios.
Train physicians in providing integrated primary care: Training materials for providers and associates on
the delivery of integrated care should be used. Associates should be trained on the specifics of integrated care,
58
including the rationale, impact on patients, and potential modifications to care workflows. In doing so,
providers and associates should understand the benefits and potential drawbacks of service integration.
Offer specialty services in-house either in-person or using technology: Once a patient exits a primary
care facility, they may enter the broader healthcare system to receive additional care. Patients will often need
specialty care, which can be expensive. This can result in patients not receiving care, even when it is needed
and recommended by their PCP. Specialty care services should be integrated into primary care clinics using
telemedicine or e-consults. This would enable patients to receive timely specialty care.
Link the clinic to the community as well as to family members and caregivers: The notion of “who
cares” for a patient is expanding from the provider to include family members, non-professional caregivers,
and others in the community. Linking the provision of care to family members and caregivers should be
considered by primary care organizations. This may be undertaken by ensuring family members and
caregivers attend appointments and are tasked with follow-up activities such as booking future appointments
or filling medications.
Long-term Recommendations
Use data to make data-informed decisions: Data should be used to inform future design, operational, and
other decisions. While the qualitative voice of the consumer should be at the center of decision-making,
quantitative data should be leveraged to understand the consumer from varying perspectives.
Move to VBC following the creation of a sustainable FFS offering: Experimentation should occur with
testing new forms of payment for healthcare services. This may include moving toward VBC arrangements
that align the interests of payers and providers and provide a better consumer experience, following the
creation of a FFS offering.
Build technology around workflows: Technology can be expensive to build, and wasteful if poorly
designed and implemented. Any new technology should be built around existing workflows. These workflows
become apparent over time as processes become more standardized. Simple technology tools can be used in
the interim to understand workflows before new investment in technology.

59
Provide healthcare services across several temporal dimensions: Longitudinal care requires primary care
organizations to provide healthcare services across several temporal dimensions to increase access. Healthcare
services should be available 24/7 through phone, text, and email. This will serve to increase access for
patients during off-hours in the chance of an emergency. It could also lead to patients avoiding the emergency
room.
Promote leaders and foster cultures and mindsets that are supportive of integration efforts: Leaders
must take the lead on promoting efforts to integrate primary care services. They should provide the strategic
vision, culture, motivation, and discipline for integration activities. New ways of working can create
resentment and frustration among associates, though having the backing and support of leadership is required
to facilitate implementation of the strategic vision. Without clear leadership, integration activities are bound
to fail.
Walmart Health Analysis
Despite being early in its operational life, there are areas where the Center is excelling in providing an
integrated primary care experience. The Center was clearly designed around the customer. Consider the care
host greeting patients entering the facility or the extended operating hours or affordable prices. These are all
features of a system that has been designed around the consumer.
The Center is also a physical space that provides anonymity for patients. Patients can receive
healthcare services without having to share with others their reason for visiting Walmart. In the case of
behavioral health, the design of the physical space can also address concerns with stigma. The door to the
behavioral health exam room is the same as any other medical exam room, and patients can sit in the lobby
without others knowing why they are visiting the Center.
Lastly, the Center is supporting integration with providers using warm handoffs of patients to other
providers. These warm handoffs occur between providers, depending on the needs, risk, and complexity of a
patient. If a patient presents in distress, the medical provider may conduct a warm handoff to the CHW, or
the audiologist will do a warm handoff to the medical team if needed. In future iterations of the Centers and

60
as Walmart Health continues to consider how to provide longitudinal primary care, multidisciplinary care
teams can be used to fully address the needs of high-risk, complex patients.
Given the preceding short-, medium-, and long-term recommendations, Walmart Health has the
opportunity to consider a more standardized approach to integrate primary care services at its Centers. In
doing so, Walmart Health has the potential to realize its vision of changing the cost, convenience, and care
delivery of basic healthcare services across the country.

61
5.0 CONCLUSION
This dissertation has proposed that the US healthcare system is broken for consumers. A web of
complex relationships between powerful entities that often exclude the consumer can translate into a poor
experience for consumers navigating the healthcare system. Three primary problems underpin the brokenness
of the healthcare system for consumers: (1) healthcare costs are high and rising; (2) access and convenience to
basic healthcare services are lacking; and (3) the quality of healthcare services is often poor and variable.
In September 2019, Walmart opened their first Walmart Health Center in Dallas, GA. This facility
offers basic healthcare services under one roof, including primary care, dental, audiology, optometry, and
behavioral health. The effective integration of these healthcare services was of strategic importance to
Walmart. It allowed the company to potentially reduce the cost of providing basic healthcare services, offer
an accessible and convenient healthcare experience, and deliver high-quality healthcare services. Given this
objective, two aims guided the exploration of this project: (1) to understand existing models of primary care
that integrate several services under one roof; and (2) to determine how Walmart Health could better
integrate the healthcare services offered at their Walmart Health Center in Dallas, GA.
Based on a series of qualitative interviews, this dissertation established several themes, conclusions,
and recommendations. Using the Singer et al. (2018) theoretical model as a guide, I found that the current
landscape of primary care models is influenced by several contextual characteristics that impact the extent of
integration. External market and internal organizational characteristics affect the integration of primary care
services. They range from financial reimbursement and educational training to the physical layout of the clinic
as well as leadership capabilities to the building of organizational culture. The second major finding was that
the Walmart Health Center has the foundational structures, operations, and workflows to support the
effective integration of primary care services. Several activities such as the physical clinic design and
workflows that include huddles and team meetings are already occurring to support the integration of basic
healthcare services.
The interviews also supported the identification of five themes that relate to the integration of
primary care services at the Walmart Health Center. These arose outside the confines of the Singer et al.
62
(2018) theoretical model. These include that: (1) people have high hopes for Walmart to change healthcare,
though others tread with caution; (2) Walmart Health could further fragment the healthcare system without
continuity-of-care; (3) the volume of patients at Walmart Health could lead to associate dissatisfaction and
burnout; (4) regulations and reimbursement at Walmart Health can in fact support integration; and (5) leaders
inspire change, managers get things done.
Lastly, the findings and themes informed 15 recommendations for primary care centers, including
Walmart Health, to effectively integrate basic healthcare services. These recommendations are separated into
activities for the short-, medium-, and long-term, though can be achieved in a twelve-month timeframe. They
provide a prioritized roadmap of strategies for optimizing the integration of primary care services.
As the former Dean of the Harvard T.H. Chan School of Public Health, Dr. Julio Frenk, has noted:
“Primary health care has moved with time from idea to heterodoxy, mainstream, disappointment, and search
for renewal” (Frenk, 2009:170). Perhaps more than ten years after his writing, the time has come for the
renewal of primary care in the US.

63
6.0 BIBLIOGRAPHY American Academy of Family Practice. “Retail Clinics.” American Academy of Family Practice, 2014. Web. August 2014. American Academy of Pediatrics Committee on Practice and Ambulatory Medicine. “AAP principles concerning retail-based clinics.” Pediatrics. vol. 118, no. 6, 2006, pp. 2561-2. American Medical Association. “Issue brief: Corporate practice of medicine.” American Medical Association, 2015. Web. 2015. American Medical Association. “Report of the Council on Medical Service: Retail Health Clinics.” American Medical Association, 2016. Web. 2016. American Medical Association. “How much physician burnout is costing your organization.” American Medical Association, 2018. Web. 11 October 2018. American Medical Association. “New survey shows decline in physician burnout.” American Medical Association, 2019. Web. 21 February 2019. American Medical Association. “What should be done about the physician burnout epidemic.” American Medical Association, 2020. Web. 2020. Ashwood, J. Scott, Martin Gaynor, Claude M. Setodji, Rachel O. Reid, Ellerie Weber & Ateev Mehrotra. “Retail Clinic Visits for Low-Acuity Conditions Increase Utilization and Spending.” Health Affairs. vol. 35, no. 3, 2016, pp. 449-455. Atchison, Kathryn A., Jane A. Weintraub & R. Gary Rozier. “Bridging the dental-medical divide: Case studies integrating oral health care and primary health care.” J Am Dent Assoc. vol. 149, no. 10, 2018, pp. 850-858. Balu, Nivedita. “Walmart’s Chief Executive to Chair the Business Roundtable.” Reuters, 2019. Web. 19 September 2019. Basu, Sanjay, Seth A. Berkowitz, Robert L. Phillips, Asaf Bitton, Bruce E. Landon & Russell S. Phillips. “Association of Primary Care Physician Supply With Population Mortality in the United States, 2005-2015.” JAMA Intern Med. vol. 179, no. 4, 2019, pp. 506-514. Basu, Sanjay, Russell S. Phillips, Asaf Bitton, Zirui Song & Bruce E. Landon. “Medicare Chronic Care Management Payments and Financial Returns to Primary Care Practices: A Modeling Study.” Ann Intern Med. vol. 163, no. 8, 2015, pp. 580-8. Baxter, Susan, Maxine Johnson, Duncan Chambers, Anthea Sutton, Elizabeth Goyder & Andrew Booth. “The effects of integrated care: a systematic review of UK and international evidence.” BMC Health Serv Res. vol. 18, no. 1, 2018, p. 350. Bodenheimer, Thomas. “Primary Care — Will It Survive?” N Engl J Med. vol. 355, 2006, pp. 861-864. Bose, Nandita. “Walmart expands $1 a day education program to deepen push in healthcare.” Reuters, 2019. Web. 24 September 2019. Boyle, Matthew. “Walmart Rolls Out Slew of New Health-Care Benefits for Employees.” Bloomberg, 2019. Web. 3 October 2019.

64
Bradley, Elizabeth & Lauren Taylor. The American Health Care Paradox: Why Spending More is Getting Us Less. New York: PublicAffairs, 2013. Carter, Shawn M. “Walmart debuts gym memberships for ‘$9 a paycheck.” Fox Business, 2020. Web. 23 January 2020. Cash-Gibson, Lucinda. “Technical Series on Primary Health Care: Integrating health services.” World Health Organization, 2018. Web. 2018. Cassel, Christine K. “Can Retail Clinics Transform Health Care?” JAMA. vol. 319, no. 18, 2018, pp. 1855-1856. Cecil G. Sheps Center for Health Services Research. “168 Rural Hospital Closures: January 2005 – Present (126 since 2010).” The University of North Carolina at Chapel Hill Cecil G. Sheps Center for Health Services Research, 2020. Web. 2014. Centers for Medicare & Medicaid Services. “Modernizing and Clarifying the Physician Self-Referral Regulations Proposed Rule.” Centers for Medicare & Medicaid Services, 2019. Web. 9 October 2019. Centers for Medicare & Medicaid Services. “National Health Expenditure Data.” Centers for Medicare & Medicaid Services, 2019. Web. 17 December 2019. Cifuentes, Maribel, Melinda M. Davis, Douglas Fernald, Rose Gunn, Perry Dickinson & Deborah J. Cohen. “Electronic Health Record Challenges, Workarounds, and Solutions Observed in Practices Integrating Behavioral Health and Primary Care.” J Am Board Fam Med. vol. Sep-Oct, no. 28, 2015, pp. S63-72. Claxton, Gary, Larry Levitt, Matthew Rae, and Bradley Sawyer. “Increases in cost-sharing payments continue to outpace wage growth.” Peterson-KFF, 2018. Web. 15 June 2018. Cohen, Robin A. & Emily P. Zammitti. “High-deductible Health Plan Enrollment Among Adults Aged 18–64 With Employment-based Insurance Coverage.” Centers for Disease Control and Prevention, 2018. Web. 9 August 2018. Collins, Chris, Denise Levis Hewson, Richard Munger & Torlen Wade. “Evolving models of behavioral health Integration in primary care.” Millbank, 2010. Web. 25 May 2010. Committee on an Oral Health Initiative Board on Health Care Services. Advancing Oral Health in America. National Academies Press, Washington (DC), 2010. Corkery, Michael. “Walmart to Limit Ammunition Sales and Discourage ‘Open Carry’ of Guns in Stores.” New York Times, 2019. Web. 3 September 2019. D'Innocenzio, Anne. “Walmart is raising starting hourly wage to $12 at 500 stores to lure workers, aid service.” Associated Press, 2020. Web. 24 January 2020. Dall, Tim, Terry West, Ritashree Chakrabarti, Ryan Reynolds & Will Iacobucci. “The Complexities of Physician Supply and Demand: Projections from 2016 to 2030.” Association of American Medical Colleges, 2018. Web. March 2018. Donaldson, Molla S, Karl D. Yordy, Kathleen N. Lohr, Neal A. Vanselow, editors. Primary Care: America's Health in a New Era. National Academies Press, Washington (DC), 1996.
65
Doherty, William J., Susan H. McDaniel, Macaran A. Baird. “Five levels of primary care/behavioral healthcare collaboration.” Behav Healthc Tomorrow. vol. 5, no. 5, 1996, pp. 25-7. Dwiel, Kathleen, Martell A. Hesketh, Jessica L. Alpert, Jacqueline Cellini, Kristen Goodell, Russell S. Phillips & Erin E. Sullivan. “The Impact of Oral Health Training for Primary Care Clinicians: A Systematic Review.” Fam Med. vol. 51, no. 3, 2019, pp. 251-261. Elhauge, Einer. The fragmentation of US health care: causes and solutions. New York: Oxford University Press, 2010. Ellner, Andrew L. & Russell S. Phillips. “The Coming Primary Care Revolution.” J Gen Intern Med. vol. 32, no. 4, 2017, pp. 380–386. Farr, Christina & Lauren Thomas. “Walmart tests dentistry and mental care as it moves deeper into primary health.” CNBC, 2019. Web. 29 August 2019. Fishman, Charles. The Wal-Mart Effect. New York: Penguin Books, 2006. Frenk, Julio. “Reinventing primary health care: the need for systems integration.” The Lancet. vol. 374, no. 9684, 2009, pp. 170-173. Gawande, Atul. “The Heroism of Incremental Care.” Ann Med, 2017. Web. 23 January 2017. GE Healthcare. “The Current State of the Patient Experience.” GE Healthcare Camden Group, 2017. Web. Date Unknown. Grazier, Kyle L., Mary L. Smiley & Kirsten S. Bondalapati. “Overcoming Barriers to Integrating Behavioral Health and Primary Care Services.” J Prim Care Community Health. vol. 7, no. 4, 2016, pp. 242-248. Harker, Laura. “Efforts Advance to Put More Health Care Providers in Reach of Georgians.” Georgia Budget and Policy Institute, 2019. Web. 8 May 2019. Heath, S. “64% of Patients Avoid Care Due to High Patient Healthcare Costs.” Patient Engagement HIT, 2018. Web. 15 February 2018. Heath B., Pamela Wise Romero, and K. Reynolds. “A Review and Proposed Standard Framework for Levels of Integrated Healthcare.” SAMHSA-HRSA Center for Integrated Health Solutions, 2013. Web. March 2013. Holloway, Immy & Kathleen Galvin. Qualitative Research in Nursing and Healthcare. Oxford: Wiley Blackwell, 2016. Hostetter, Martha & Sarah Klein. “In Focus: Integrating Oral Health into Primary Care.” The Commonwealth Fund, 2015. Web. 26 February 2015. Howell, Joel D. “Reflections on the past and future of primary care.” Health Aff (Millwood). vol. 29, no. 5, 2010, pp. 760-5. Huey, John. Sam Walton: Made in America. New York: Bantam Doubleday Dell Publishing Group, 1992. Kim, Linda Y., Danielle E. Rose, Lynn M. Soban, Susan E. Stockdale, Lisa S. Meredith, Samuel T. Edwards, Christian D. Helfrich & Lisa V. Rubenstein. “Primary Care Tasks Associated with Provider Burnout: Findings from a Veterans Health Administration Survey.” J Gen Intern Med. vol. 33, no. 1, 2018, pp. 50-56.

66
Lazris, Andy, Alan Roth & Shannon Brownlee. “No More Lip Service; It’s Time We Fixed Primary Care (Part One).” Health Affairs Blog, 2018. Web. 20 November 2018. Lytle, Stephen. “Sam Walton's Vision for the Future of Retail Healthcare.” YouTube, 6 March 2017, www.youtube.com/watch?v=iNs6cDUKl7Y. Marshall, Catherine & Gretchen B. Rossman. Designing Qualitative Research. Thousand Oaks: Sage Publications, 2011. Martsolf, Grant R, Kathryn R. Fingar, Rosanna Coffey, Ryan Kandrack, Tom Charland, Christine Eibner, Anne Elixhauser, Claudia Steiner & Ateev Mehrotra. “Association Between the Opening of Retail Clinics and Low-Acuity Emergency Department Visits.” Ann Emerg Med. vol. 69, no. 4, 2017, pp. 397-403.e5. Maruthappu, Mahiben, Ali Hasan & Thomas Zeltner. “Enablers and Barriers in Implementing Integrated Care.” Health Syst Reform. vol. 1, no. 4, 2015, pp. 250-256. Miller, Benjamin F., Rodger Kessler, C.J. Peek & Gene A. Kallenberg. “A national agenda for research in collaborative care: Papers from the Collaborative Care Research Network Research Development Conference.” Agency for Healthcare Research and Quality, 2011. Web. July 2011. Miller, Robin, Jacqueline Cumming & Richard Q. Lewis. “Keeping the faith in integration and primary care.” J Integr Care. vol. 26, no. 3, 2018, pp. 170-174. Nelson, Gary. “The two Georgias: Disparities in rural health and healthcare.” J Ga Public Health Assoc, vol. 5, no. 4, 2016, pp:294-296. Newman, Eric D., Paul F. Simonelli, Shelly M. Vezendy, Chelsea M. Cedeno, and Daniel D. Maeng. “Impact of Primary and Specialty Care Integration via Asynchronous Communication.” Am J Manag Care. vol. 25, no 1, 2019, pp. 26-31. National Institute of Mental Health. “Integrated Care.” National Institute of Mental Health, 2017. Web. February 2017. Olayiwola, J. Nwando, Daren Anderson, Nicole Jepeal, Robert Aseltine, Christopher Pickett, Jun Yan & Ianita Zlateva. “Electronic Consultations to Improve the Primary Care-Specialty Care Interface for Cardiology in the Medically Underserved: A Cluster-Randomized Controlled Trial.” Ann Fam Med. vol. 14, no. 2, 2016, pp. 133-40. Peckham, Carol. “Physician Burnout: It Just Keeps Getting Worse.” Medscape, 2015. Web. 26 January 2015. Peek, C.J. “Integrated Care: Aids to Navigation.” Pennsylvania, Eastern Ohio & West Virginia Summit: Integrating Mental Health and Primary Care, 2007. Web. 2007. Petro, Greg. “Walmart Challenges Amazon On Sustainable Packaging.” Forbes, 2020. Web. 17 February 2020. Pham, Hoangmai and Ann Greiner. “The Importance Of Primary Care—And Of Measuring It.” Health Affairs, 2019. Web. 6 August 2019. Porter, Michael & Elizabeth Olmsted Teisberg. Redefining Health Care: Creating Value-Based Competition on Results. Boston: Harvard Business School Publishing, 2006.

67
Porter, Michael and Jorge Ramirez-Vallejo. Walmart: Navigating a Changing Retail Landscape. Harvard Business Publishing, July 2019. Case Study. Powers, Brian, R. Bruce Donoff & Sachin H. Jain. “Bridging The Dental Divide: Overcoming Barriers To Integrating Oral Health And Primary Care.” Health Affairs Blog, 2017. Web. 19 January 2017. Rand Corporation. “The Evolving Role of Retail Clinics.” Rand Corporation, 2016. Web. 2016. Raymond Guilbault, Ryan William & Vinson, Joseph Alexander. “Clinical medical education in rural and underserved areas and eventual practice outcomes: a systematic review and meta-analysis.” Educ Health (Abingdon). vol. 30, no. 2, 2017, pp. 146-155. Ross, Lori E., Simone Vigod, Jessica Wishart, Myera Waese, Jason Dean Spence, Jason Oliver, Jennifer Chambers, Scott Anderson & Roslyn Shields. “Barriers and facilitators to primary care for people with mental health and/or substance use issues: a qualitative study.” BMC Fam Pract. vol. 16, no. 135, 2015, pp. 1-13. Rubin, Rita. “VA Using Telemedicine to Provide Therapy to Rural Veterans With PTSD.” JAMA. vol. 319, no. 16, 2018, p. 1648. Safavi, Kaveh, Kip Webb & Brian Kalis. “Today’s Consumers Reveal the Future of Healthcare.” Accenture Consulting, 2019. Web. 2019. Sage, William M. “The Wal-Martization of Health Care.” J Leg Med. vol. 28, no. 4, 2007, pp. 503-19. Schwartz, Mark D., Steven Durning, Mark Linzer, Karen E. Hauer. “Changes in Medical Students' Views of Internal Medicine Careers From 1990 to 2007.” Arch Intern Med. vol. 171, no. 8, 2011, pp. 744-749. Seaburn, David B., Alan D. Lorenz, William B. Gunn Jr., Barbara A. Gawinksi & Larry Mauksch. Models of collaboration: A guide for mental health professionals working with health care practitioners. New York: Basic Books, 1996. Shrank, William H. “Primary Care Practice Transformation and the Rise of Consumerism.” J Gen Intern Med. vol. 32, no. 4, 2017, pp. 387-391. Singer, Sara J., Michaela Kerrissey, Mark Friedberg & Russell Phillips. “A Comprehensive Theory of Integration.” Med Care Res Rev. vol. Mar, 2018, pp. 1-23. Slovenski, Sean. “Our Goal of Becoming America’s Neighborhood Health Destination: Introducing the Walmart Health Center.” Walmart, 2019. Web. 13 September 2019. Solberg, Leif I., A. Lauren Crain, Michael V. Maciosek, Jürgen Unützer, Kris A. Ohnsorg, Arne Beck, Lisa Rubenstein, Robin R. Whitebird, Rebecca C. Rossom, Pamela B. Pietruszewski, Benjamin F. Crabtree, Kenneth Joslyn, Andrew Van de Ven, & Russell E. Glasgow. “A Stepped-Wedge Evaluation of an Initiative to Spread the Collaborative Care Model for Depression in Primary Care.” Ann Fam Med. vol. 13, no. 5, 2015, pp. 412-20. Song, Zirui and Gondi, Suhas. “Will Increasing Primary Care Spending Alone Save Money?” JAMA. vol. 322, no. 14, 2019, pp. 1349-1350. Speer, Alyssa. “Blurred Lines: QA/QI vs. Research.” Office of Human Research Administration. Date Unknown. Tang, Michael H, Nandini Sengupta, Stacy Longo & Barry Zuckerman. “Behavioral Health Integration in a Medicaid Accountable Care Organization: Management Lessons from a Health Center.” J Health Care Poor Underserved. vol. 30, no. 4, 2019, pp. 1252-1258.

68
Taylor, Steven J., Robert Bogdan & Marjorie DeVault. Introduction to Qualitative Research Methods: A Guidebook and Resource. Hoboken: John Wiley & Sons, 2015. The Lancet. “Prioritising primary care in the USA.” The Lancet. vol. 394, no. 10195, 2019, p. 273. Thomas, Lauren. “Walgreens, CVS join Walmart, Kroger in asking shoppers not to openly carry guns in stores.” CNBC, 2019. Web. 5 September 2019. Tolbert, Jennifer, Kendal Orgera, Natalie Singer, and Anthony Damico. “Key Facts about the Uninsured Population.” Kaiser Family Foundation, 2019. Web. 13 December 2019. Tracy, Sarah J. Qualitative Research Methods: Collecting Evidence, Crafting Analysis, Communicating Impact. Oxford: John Wiley & Sons, 2013. United Health Foundation. “America’s Health Rankings Annual Report 2019.” United Health Foundation, 2019. Web. 2019. Valentijn, Pim Peter. “Rainbow of Chaos: A study into the Theory and Practice of Integrated Primary Care.” Int J Integr Care. vol. 16, no. 2, 2016, p. 3. Vimalananda, Varsha, Jay Orlander, Melissa Afable, B. Graeme Fincke, Amanda Solch, Seppo Rinne, Eun Ji Kim, Sarah Cutrona, Dylan Thomas, Judith Strymish & Steven Simon. “Electronic consultations (E-consults) and their outcomes: a systematic review.” J Am Med Inform Assoc. vol. 27, no. 3, 2020, pp. 471-479. Warshaw, Robin. “Health Disparities Affect Millions in Rural U.S. Communities.” Association of American Medical Colleges, 2017. Web. 31 October 2017. Waugh, Maryann, Jacqueline Calderone , Shandra Brown Levey, Corey Lyon, Marshall Thomas, Frank DeGruy & Jay Shore. “Using Telepsychiatry to Enrich Existing Integrated Primary Care.” Telemed J E Health. vol. 25, no. 8, 2019, pp. 762-768. Wells, Rebecca, Ellen D. Breckenridge, Sasha Ajaz, Aman Narayan, Daniel Brossart, James H. Zahniser & Jolene Rasmussen. “Integrating Primary Care Into Community Mental Health Centres in Texas, USA: Results of a Case Study Investigation.” Int J Integr Care. vol. 19, no. 4, 2019, pp. 1-11. West, Peter, Richard Giordano, Max Van Kleek & Nigel Shadbolt. “The Quantified Patient in the Doctor's Office: Challenges & Opportunities.” CHI '16: Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, 2016. Web. 2016. Woods, Lisa, Jonathan R. Slotkin & M. Ruth Coleman. “How Employers are Fixing Health Care.” Harvard Business Review, 2019. Web. 19 March 2019. Wright, Brad. “Who Governs Federally Qualified Health Centers?” J Health Polit Policy Law. vol. 38, no. 1, 2013, pp. 27–55. Yabroff, K. Robin, Jingxuan Zhao, Xuesong Han & Zhiyuan Zheng. “Prevalence and Correlates of Medical Financial Hardship in the USA.” J Gen Intern Med. vol. 34, no. 8, 2019, pp. 1494-1502. Yaffe-Bellany, David, Michael Corkery & Sheila Kaplan. “Walmart to End Sales of E-Cigarettes as Vaping Concerns Mount.” New York Times, 2019. Web. 20 September 2019.

69
Yakovenko, Anna, Emily Zuehlke, Alicia Daugherty & Kevin Reardon. “What do consumers Want from Primary care?” The Advisory Board Company, 2014. Web. 6 June 2014. Yin, Robert K. Qualitative research from start to finish. New York: The Guilford Press, 2011. Zabar, Sondra, Andrew Wallach, Adina Kalet. “The Future of Primary Care in the United States Depends on Payment Reform.” JAMA Intern Med. vol. 179, no. 4, 2019, pp. 515-516.
70
7.0 APPENDIX 7.1 Appendix A: Important Events in Walmart’s History
Important Events in Walmart’s History (Adapted from Porter & Jorge Ramirez-Vallejo, 2019)
1962-1971: Growth in Rural Areas 1962: First store opened in Rogers, Arkansas. 1967: 24 Walmart stores, with $12.7 million in sales. 1970: Walmart became publicly traded. 1971: First distribution center and Home Office facility opened in Bentonville, Arkansas.
1972-1990: National Expansion 1982: Walmart Foundation established. 1983: First Sam’s Club opened in Midwest City, Oklahoma. 1987: Largest private satellite communication system in the US established. 1988: First Supercenter opened in Washington, Missouri; David Glass became CEO.
1991-2003: Growth of the Grocery Business and Internationalization 1992: Sam Walton died at age 74. 1994: Expanded into Canada with the purchase of 122 Woolco stores. 1996: Opened its first store in China. 1998: Neighborhood Market format started with 3 stores in Arkansas; Entered UK by acquiring ASDA. 2000: H. Lee Scott, Jr. became CEO; Walmart.com was founded in the US. 2002: Walmart topped Fortune 500 ranking as America’s largest company; Entered the Japanese market.
2014-2017: A New Value Chain and Building an Online Channel 2005: Delivered supplies to survivors of Hurricane Katrina; Made major commitments to sustainability. 2006: Introduced $4 generic-drug prescription program. 2007: Launched Walmart.com Site to Store service to enable purchasing online and pick-up in stores. 2009: Michael Duke became CEO. 2010: Bharti Walmart joint venture opened in India; launched commitment to sustainable agriculture. 2014: Doug McMillon became CEO. 2015: Announced $2.7 billion investment over two years in its US workforce. 2016: Launched Walmart Pay as an in-store payment method. 2016: Opened its first training Academy in South Carolina, with 200 locations planned at stores in the US. 2016: Raised compensation for 1.2 million associates as part of a $2.7 billion human capital investment. 2017: Launched free two-day shipping on more than 2 million items with no membership required. 2017: Launched Store No 8, a tech incubator with a focus on innovation and the future of retail.
71
7.2 Interview Guide 7.2.1 For Key Thought Leaders in Integrated Primary Care
Preamble: Thank you very much for speaking with me today. I am a Doctor of Public Health student at Harvard, and I am completing my dissertation on the integration of primary care services. I am interviewing a handful of key thought leaders who I have identified as having expertise in this area. You should have received a copy of the Confidentiality Agreement outlining your rights as an interviewee, though I am hoping to use this interview in my dissertation. Would you be fine if I recorded our conversation today? If so, turn on recorder. Interview Questions:
1. When you think about the integration of primary care services, what does this mean to you? How do you define integration?
2. How prevalent would you say these models of integrated primary care services are in the US? 3. What have you seen that has or has not worked in integrating primary care? 4. What primary services or programs have you seen included in these models? Are there necessary
components or defining features that facilitate integration in these models? 5. How have you seen medical professionals interact with one another to deliver primary services in these
integrated models? 6. How have you seen payment or reimbursement models facilitate integrated primary care? 7. How do technological systems support the integration of primary care services? 8. What have you seen as challenges or barriers in standing up these integrated primary care models? 9. Who are the leaders in integrating services? Are you familiar with other models that integrate services? 10. Is there anything else you would like to share with me today?
Wrap-up: That’s all I have for today, thank you very much for agreeing to speak with me. Do you have any questions before we close out our conversation? Turn off recorder and save file.
7.2.2 For Medical Personnel at Walmart Health
Preamble: Thank you very much for speaking with me today. I am a Doctor of Public Health student at Harvard, and I am completing my dissertation on the integration of primary care services. Part of my degree entails working at an organization, so I am with Walmart Health, working to develop a case study on the clinic. I am interested in better understanding integration at the clinic, and was interested in speaking with you to learn more. The interview shouldn’t take more than 15 minutes, and you can decline to answer at any time. Interview Questions:
1. Tell me about your position and how you are finding your experience working at Walmart Health. 2. How does this practice differ from other past practices in which you have worked? 3. When you think about the integration of the services in this space, what does that mean to you? 4. Do you work with the other medical professionals in the space? How often do you meet? Where do
you normally meet? 5. What do you like about the integration of the healthcare services? What is working? 6. How would you improve the integration of the healthcare services in the space? What is not working? 7. Are there other unanticipated benefits that you have seen that have arisen because of the integration
of primary care services? 8. Anything else you would like to share with me today?
Wrap-up: That’s all I have for today, thank you very much for agreeing to speak with me. Do you have any questions before we close out our conversation? Turn off recorder and save file.

72
7.3 Interview Confidentiality Form The below is a copy of the Interview Confidentiality Form provided to thought leader participants. For associates at the Walmart Health Center, the information was provided orally.
Please consider this information carefully before deciding whether to participate in this research. Purpose of the research: To understand the landscape of integrated primary care models to inform my dissertation, which focuses on the integration of primary care services by a major American retailer. What you will do in this research: If you decide to volunteer, you will be asked to participate in one interview. You will be asked several questions. With our permission, I will tape record the interviews so I don't have to take so many notes. You will not be asked to state your name on the recording. Time required: The interview will take approximately 30-60 minutes. Benefits: This is a chance for you to tell your story about your experiences related to the integration of primary care services. This data will be used to enhance ways to approach to improve experience for patients and enhance models of care. Confidentiality: Your responses to interview questions will be kept confidential. The recording will be destroyed when my dissertation has been accepted. I won’t use your name or information that would identify you in any publications or presentations. Participation and withdrawal: Your participation in this study is completely voluntary, and you may refuse to participate or withdraw from the study without penalty or loss of benefits to which you may otherwise be entitled. You may withdraw by informing the experimenter that you no longer wish to participate (no questions will be asked). You may skip any question during the interview but continue to participate in the rest of the study. To Contact the Researcher: If you have questions or concerns about this research, please contact: [Gillian Christie, 917-280-5121, [email protected]]. You may also contact the faculty member supervising this work: [Kimberlyn Leary, Associate Professor of Department of Health Policy and Management, 677 Huntington Avenue, Boston, MA 02115, [email protected]]. Agreement: The nature and purpose of this research have been sufficiently explained and I agree to participate in this study. I understand that I am free to withdraw at any time without incurring any penalty. Signature: _____________________________________ Date: __________________ Name (print): _________________________________________________________
Related Documents