PII S0360-3016(00)01441-3 CLINICAL INVESTIGATION Head and Neck A PROSPECTIVE STUDY OF SALIVARY FUNCTION SPARING IN PATIENTS WITH HEAD-AND-NECK CANCERS RECEIVING INTENSITY-MODULATED OR THREE-DIMENSIONAL RADIATION THERAPY: INITIAL RESULTS K. S. CLIFFORD CHAO, M.D., JOSEPH O. DEASY,PH.D., JERRY MARKMAN, D.SC., JOYCE HAYNIE, R.N., CARLOS A. PEREZ, M.D., JAMES A. PURDY,PH.D., AND DANIEL A. LOW,PH.D. Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University Medical Center, St. Louis, MO Objectives: In a prospective clinical study, we tested the hypothesis that sparing the parotid glands may result in significant objective and subjective improvement of xerostomia in patients with head-and-neck cancers. The functional outcome 6 months after the completion of radiation therapy is presented. Methods and Materials: From February 1997 to February 1999, 41 patients with head-and-neck cancers were enrolled in a prospective salivary function study. Inverse-planning intensity-modulated radiation therapy (IMRT) was used to treat 27 patients, and forward-planning three-dimensional radiation therapy in 14. To avoid potential bias in data interpretation, only patients whose submandibular glands received greater than 50 Gy were eligible. Attempts were made to spare the superficial lobe of the parotid glands to avoid underdosing tumor targets in the parapharyngeal space; however, the entire parotid volume was used to compute dose–volume histograms (DVHs) for this analysis. DVHs were computed for each gland separately. Parotid function was assessed objectively by measuring stimulated and unstimulated saliva flow before and 6 months after the completion of radiation therapy. Measurements were converted to flow rate (mL/min) and normalized relative to that before treatment. The corresponding quality-of-life (QOL) outcome was assessed by five questions regarding the patient’s oral discomfort and eating/speaking problems. Results: We observed a correlation between parotid mean dose and the fractional reduction of stimulated saliva output at 6 months after the completion of radiation therapy. We further examined whether the functional outcome could be modeled as a function of dose. Two models were found to describe the dose–response data well. The first model assumed that each parotid gland is comprised of multiple independent parallel functional subunits (corresponding to computed tomography voxels) and that each gland contributes equally to overall flow, and that saliva output decreases exponentially as a quadratic function of irradiation dose to each voxel. The second approach uses the equivalent uniform dose (EUD) metrics, which assumes loss of salivary function with increase in EUD for each parotid gland independently. The analysis suggested that the mean dose to each parotid gland is a reasonable indicator for the functional outcome of each gland. The corresponding exponential coefficient was 0.0428/Gy (95% confidence interval: 0.01, 0.09). The QOL questions on eating/speaking function were significantly correlated with stimulated and unstimulated saliva flow at 6 months. In a multivariate analysis, a toxicity score derived from the model based on radiation dose to the parotid gland was found to be the sole significant predictive factor for xerostomia. Neither radiation technique (IMRT vs. non-IMRT) nor chemother- apy (yes or no) independently influenced the functional outcome of the salivary glands. Conclusion: Sparing of the parotid glands translates into objective and subjective improvement of both xerostomia and QOL scores in patients with head-and-neck cancers receiving radiation therapy. Modeling results suggest an exponential relationship between saliva flow reduction and mean parotid dose for each gland. We found that the stimulated saliva flow at 6 months after treatment is reduced exponentially, for each gland independently, at a rate of approximately 4% per Gy of mean parotid dose. © 2001 Elsevier Science Inc. IMRT, Salivary gland, Xerostomia. INTRODUCTION Xerostomia (dry mouth) is a symptom that often occurs as a side effect of many therapeutic interventions, such as radiation therapy for patients with head-and-neck cancer. Xerostomia encompasses a wide range of symptoms, from inconvenience in eating and speaking to a debilitating con- dition. Reduction in salivary flow per se is not life threat- ening, but alteration of eating function and deterioration of dental and oral health has a significant impact on the quality of life (QOL) (1, 2). Saliva also possesses an antibacterial function, and deprivation of saliva flow may lead to frequent Reprint requests to: Dr. K. S. Clifford Chao, Radiation Oncol- ogy Center, Box 8224, Washington University Medical School, 4939 Children’s Place, Suite 5500, St. Louis, MO 63110. E-mail: [email protected] This research was in part supported by NIH grant CA85181 and an industrial grant from NOMOS Corp. Accepted for publication 25 September 2000. Int. J. Radiation Oncology Biol. Phys., Vol. 49, No. 4, pp. 907–916, 2001 Copyright © 2001 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/01/$–see front matter 907

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PII S0360-3016(00)01441-3
CLINICAL INVESTIGATION Head and Neck
A PROSPECTIVE STUDY OF SALIVARY FUNCTION SPARING IN PATIENTSWITH HEAD-AND-NECK CANCERS RECEIVING INTENSITY-MODULATED
OR THREE-DIMENSIONAL RADIATION THERAPY: INITIAL RESULTS
K. S. CLIFFORD CHAO, M.D., JOSEPHO. DEASY, PH.D., JERRY MARKMAN, D.SC., JOYCE HAYNIE, R.N.,CARLOS A. PEREZ, M.D., JAMES A. PURDY, PH.D., AND DANIEL A. LOW, PH.D.
Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University Medical Center, St. Louis, MO
Objectives: In a prospective clinical study, we tested the hypothesis that sparing the parotid glands may resultin significant objective and subjective improvement of xerostomia in patients with head-and-neck cancers. Thefunctional outcome 6 months after the completion of radiation therapy is presented.Methods and Materials: From February 1997 to February 1999, 41 patients with head-and-neck cancers wereenrolled in a prospective salivary function study. Inverse-planning intensity-modulated radiation therapy(IMRT) was used to treat 27 patients, and forward-planning three-dimensional radiation therapy in 14. To avoidpotential bias in data interpretation, only patients whose submandibular glands received greater than 50 Gy wereeligible. Attempts were made to spare the superficial lobe of the parotid glands to avoid underdosing tumortargets in the parapharyngeal space; however, the entire parotid volume was used to compute dose–volumehistograms (DVHs) for this analysis. DVHs were computed for each gland separately. Parotid function wasassessed objectively by measuring stimulated and unstimulated saliva flow before and 6 months after thecompletion of radiation therapy. Measurements were converted to flow rate (mL/min) and normalized relativeto that before treatment. The corresponding quality-of-life (QOL) outcome was assessed by five questionsregarding the patient’s oral discomfort and eating/speaking problems.Results: We observed a correlation between parotid mean dose and the fractional reduction of stimulated salivaoutput at 6 months after the completion of radiation therapy. We further examined whether the functionaloutcome could be modeled as a function of dose. Two models were found to describe the dose–response data well.The first model assumed that each parotid gland is comprised of multiple independent parallel functionalsubunits (corresponding to computed tomography voxels) and that each gland contributes equally to overall flow,and that saliva output decreases exponentially as a quadratic function of irradiation dose to each voxel. Thesecond approach uses theequivalent uniform dose (EUD) metrics, which assumes loss of salivary function withincrease in EUD for each parotid gland independently. The analysis suggested that the mean dose to each parotidgland is a reasonable indicator for the functional outcome of each gland. The corresponding exponentialcoefficient was 0.0428/Gy (95% confidence interval: 0.01, 0.09). The QOL questions on eating/speaking functionwere significantly correlated with stimulated and unstimulated saliva flow at 6 months. In a multivariate analysis,a toxicity score derived from the model based on radiation dose to the parotid gland was found to be the solesignificant predictive factor for xerostomia. Neither radiation technique (IMRT vs. non-IMRT) nor chemother-apy (yes or no) independently influenced the functional outcome of the salivary glands.Conclusion: Sparing of the parotid glands translates into objective and subjective improvement of bothxerostomia and QOL scores in patients with head-and-neck cancers receiving radiation therapy. Modeling resultssuggest an exponential relationship between saliva flow reduction and mean parotid dose for each gland. Wefound that the stimulated saliva flow at 6 months after treatment is reduced exponentially, for each glandindependently, at a rate of approximately 4% per Gy of mean parotid dose. © 2001 Elsevier Science Inc.
IMRT, Salivary gland, Xerostomia.
INTRODUCTION
Xerostomia (dry mouth) is a symptom that often occurs asa side effect of many therapeutic interventions, such asradiation therapy for patients with head-and-neck cancer.Xerostomia encompasses a wide range of symptoms, from
inconvenience in eating and speaking to a debilitating con-dition. Reduction in salivary flow per se is not life threat-ening, but alteration of eating function and deterioration ofdental and oral health has a significant impact on the qualityof life (QOL) (1, 2). Saliva also possesses an antibacterialfunction, and deprivation of saliva flow may lead to frequent
Reprint requests to: Dr. K. S. Clifford Chao, Radiation Oncol-ogy Center, Box 8224, Washington University Medical School,4939 Children’s Place, Suite 5500, St. Louis, MO 63110. E-mail:[email protected]
This research was in part supported by NIH grant CA85181 andan industrial grant from NOMOS Corp.
Accepted for publication 25 September 2000.
Int. J. Radiation Oncology Biol. Phys., Vol. 49, No. 4, pp. 907–916, 2001Copyright © 2001 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/01/$–see front matter
907

opportunistic infections in the oral cavity (3, 4). Further-more, xerostomia symptoms are usually permanent, whichillustrates the importance of prevention. Recent advances inconformal radiation therapy enable us to spare the parotidglands while providing adequate dosimetric coverage oftumor targets, and have provided a new avenue to preventxerostomia. Nevertheless, data on dose response of partialvolume irradiation, as encountered in conformal radiationtherapy, are scarce. We describe the results from a prospec-tive clinical study, which suggest that the probability ofsalivary function preservation is an exponential function ofthe mean parotid dose. Most importantly, protecting theparotid glands during radiation therapy improved the QOLin patients with head-and-neck cancer.
METHODS AND MATERIALS
From February 1997 to February 1999, 41 patients withhead-and-neck cancers were enrolled in a prospective sali-vary gland function preservation study at the MallinckrodtInstitute of Radiology, Washington University MedicalCenter. The Institutional Review Board reviewed and ap-proved the protocol. Informed consent was obtained fromeach patient, who acknowledged that the study would in-volve measurement of saliva and answering questions re-garding QOL issues. There were 29 men and 12 women; 32patients were white, and 9 were black or Asian. Age rangedfrom 36 to 75 years. Patient and tumor characteristics areshown in Table 1. Twenty-seven patients were treated withinverse-planning intensity-modulated radiation therapy(IMRT), and 14 patients with forward-planning three-di-mensional (3D) radiation therapy. Twenty-five patients re-ceived postoperative irradiation. Sixteen patients underwentdefinitive radiation therapy, and, among them, 14 receivedconcurrent cisplatin chemotherapy (75–100 mg/m2 every 21days during radiation course). Three patients with nasopha-ryngeal carcinoma received three additional cycles of adju-vant cisplatin and 5-fluorouracil (5-FU) according to Inter-group 0099.
Patient immobilization and imaging acquisitionA noninvasive immobilization method was used. The
patient was placed in the supine position on a custom-madehead support with a reinforced thermoplastic immobiliza-tion mask around the head. A set of volumetric computedtomography (CT) images was acquired from our dedicatedCT simulator (Marconi AcQsim, Marconi Medical System,Inc., Cleveland, OH), with the patient immobilized in thetreatment position. The data were then transferred to aninverse (Peacock treatment-planning system, NOMOSCorp., Sewickley, PA), or forward (Focus treatment-plan-ning system, CMS Corporation., St. Louis, MO) treatment-planning system. The scan slice thickness was 3 mmthroughout the tumor target region. Regions superior andinferior to the tumor target were scanned with a slice thick-ness of 5 mm.
Target definitionThe definition of target volume follows the description in
the International Commission on Radiation Units (ICRU)Report 50 (5). The gross tumor volume (GTV) is defined asall known gross disease determined from CT or magneticresonance imaging (MRI), physical examination, or endo-scopic findings. The clinical target volume (CTV) was de-lineated based on the nature of tumor spread, physicalexamination, radiologic findings, or pathologic features inthe surgical specimen, and includes the areas consideredpotentially containing microscopic disease. Lymph nodegroups or neck levels at risk of microscopic disease wereoutlined as part of the corresponding CTV. The lymph nodegroups at risk were determined according to imaging-basednodal classification (6). Bilateral submandibular (Level Ib)and jugular chain (Level II–IV) lymph nodes were includedin all cases. The submental nodal group (Level Ia) wasincluded only when the adjacent Level Ib nodes were in-volved, either clinically or pathologically. Posterior cervicalnodes (Level V) were treated on the side where there wasevidence of jugular nodal metastases. The planning targetvolume (PTV) provides a margin around each CTV tocompensate for treatment setup and internal organ motionerror. Margins (usually 5 mm) for setup error were incor-
Table 1. Patient and tumor characteristics
AgeMedian 58Range 36–75
GenderMale 29Female 12
RaceWhite 32Nonwhite 9
Tumor histologySquamous cell carcinoma 40Adenosquamous 1
Tumor siteNasopharynx 4Oral cavity 4Oropharynx 19Hypopharynx 2Supraglottic larynx 4Unknown primary 8
Tumor StageI 0II 6III 10IV 24Recurrence 1
Radiation indicationDefinitive 20
Concurrent cisplatin chemotherapy (14)No chemotherapy (6)
Postoperative 21Radiation modality
Inverse-planning IMRT 27Forward-planning 3D therapy 14
Abbreviations:IMRT 5 intensity-modulated radiation therapy;3D 5 three-dimensional.
908 I. J. Radiation Oncology● Biology ● Physics Volume 49, Number 4, 2001

porated in the planning process (5). Because the objectivewas to examine the dose response and functional outcomeof the parotid glands, patients in whom both submandibularglands received greater than 50 Gy were included to avoidambiguity in data analysis. Two patients with Stage I car-cinoma of the true vocal cord served as the control.
Dose specification for targets and normal tissuesIMRT. The beam fluence intensity was determined by
computer optimization to produce the best conformal plan.Based on the tumor burden, target doses were defined infour categories according to our institutional treatmentguidelines. Low-risk regions included primarily the prophy-lactically treated neck. Intermediate-risk regions were thoseadjacent to the gross tumor but not directly involved bytumor. High-risk regions included the surgical bed with softtissue invasion by the tumor or extracapsular extension bymetastatic neck nodes. Table 2 shows the details of doseprescriptions. The hot spot dose within the targets wasdesigned not to exceed the prescribed dose by more than15%. One unique dosimetric characteristic of this form ofIMRT is that different doses to different target structurescan be delivered simultaneously in each daily treatment.Therefore, the concept of biologic equivalent dose (BED)using a linear–quadratic model was implemented to adjustthe dose to targets (7).a:b ratio of 10 Gy was used for BEDconversion for tumor targets. The prescribed fraction sizefor the primary target was set at 1.9 Gy to increase theminimal fraction size in the lower-risk region to greater thanor equal to 1.5 Gy. During the period of this study, weencountered an increasing application of concurrent chem-oirradiation promoted by a positive clinical outcome in amulticenter clinical study and meta-analysis (8, 9). To avoidunexpected late toxicity, which may be associated with ahigh daily fraction size, we elected to constrain the dailyfraction dose to 1.9 Gy. Most of the gross tumors wereeither nasopharyngeal or tonsil primary. The doses to thesubclinical area delivered with IMRT in the upper head-and-neck region were more than 60 Gy in 1.7 Gy dailyfractions. Only small portions of the contralateral posteriorneck received 1.5 Gy daily doses. The majority of low-riskregions was in the lower neck and was treated with aconventional technique at 1.8- to 1.9-Gy daily fractionsprescribed to 3-cm depth. A detailed description of the
IMRT treatment optimization process and the quality assur-ance program has been reported elsewhere (10).
3D irradiation. CT-based treatment planning was used.The beam arrangement in this group of patients was indi-vidualized according to the location and extent of disease(11). Conformality was considered only for target coverage,and no specific effort was made to spare the parotid glands.Three-dimensional dose–volume information was obtainedfor the targets and organ of interest (parotid glands). Thetreatment volume included the primary tumor site and theneck nodes down to the supraclavicular region. Treatmentportals were individualized, but often included two opposedlateral fields. The margin of the field encompassed at least2-cm beyond the tumor boundary visible on CT scan. Aseparate anterior supraclavicular field with spinal cordshield was used for the low neck and supraclavicular fossa.The target volume, which was the entire tumor with a 2-cmmargin in all directions, received at least 90% of the mid-depth central axis dose. Variation within the target volumedid not exceed6 10% of the target dose. The dose to theneck nodes was separately specified, and the dose wasprescribed to at least 3-cm below the skin surface at theappropriate level of anatomic spread. Target doses to dif-ferent risk regions are listed in Table 2. The spinal cord dosedid not exceed 48 Gy in any patient.
Normal tissueThe normal organs/structures, includingbrain, brainstem, retina, optic nerve, optic chiasm, spinalcord, and mandible, were contoured. The dose constraintsused are listed below.
Brainstem 54 GyOptic nerve/chiasm 55 GySpinal cord 45 GyMandible 70 Gy
Saliva flow measurementAll patients underwent saliva collection at two different
time points: within 1 week before radiation treatment and 6months after radiation therapy. QOL questionnaires regard-ing oral discomfort, eating/speaking problems, and distur-bance in social life were obtained at each time point. Allsalivary samples were collected at a standardized time ofday (9:00 am to 3:00 pm) and at least 2 h after a meal. Thecollection technique and treatment of samples are detailedbelow.
Table 2. Target dose specification with biologic equivalent dose (bED) correction
Target volume3D
dose/fraction
Intensity-modulated radiation therapy
Gross (residual) tumor(37 fractions)
High-risk postoperative(35 fractions)
Intermediate-risk postoperative(32 fractions)
Low risk 50.4/1.8 Gy 55.5/1.5 Gy 54.25/1.55 Gy 52.8/1.65 GyIntermediate risk 59.4/1.8 Gy 62.9/1.7 Gy 61.25/1.75 Gy 60.8/1.9 GyHigh risk 66.6/1.8 Gy – 66.5/1.9 Gy –Gross (residual) tumor 70.2/1.8 Gy 70.3/1.9 Gy – –
Abbreviation:3D 5 three-dimensional.
909Parotid gland sparing in head-and-neck cancers● K. S. C. CHAO et al.

Whole unstimulated saliva sampleThe patient was in-structed to sit quietly for 2 min. Then the patient was askedto fill the saliva in his/her mouth and swallow any residualsaliva. After this, the patient leaned forward for 5 min andrefrained from swallowing, and all saliva that collected atthe lips was spit into a preweighed plastic cup. The patientperformed the expectoration of saliva with the nurse orassistant standing behind, checking and providing encour-agement to the patient frequently during the entire proce-dure. At the end of the 5-min period, the cup was weighedagain.
Stimulated whole saliva sampleThe patient was in-structed to chew on a standardized 5-cm3 5-cm squareparaffin strip for 2 min. After 2 min, the patient was in-structed to swallow all saliva in the mouth. A 5-min samplewas then collected with the patient continuing to chew theparaffin strip and expectorating all saliva into a preweighedcup.
Quality-of-life questionnaireFive QOL questions were used to address changes in dry
month, eating, speaking, and swallowing functions. Thepatient marked a visual analog scale (a line with tick marksfrom 0 to10) to assess the change in QOL.
1. During the last 3 days, overall, your mouth or tonguewas: (from very dry to not dry).
2. In general, during the daytime hours of the last 3 days,the feeling of your mouth and tongue was: (from ex-tremely uncomfortable to comfortable).
3. During the last 3 nights, due to the dryness of yourmouth and tongue, how difficult was it to sleep? Con-sider such factors as how difficult it was for you to go tosleep, the duration and quality of your sleep, and howoften you woke up to drink. (from very difficult to easy)
4. During the last 3 days, overall, due to the dryness of yourmouth and tongue, how difficult was it to speak withoutdrinking liquids? (from very difficult to easy)
5. During the last 3 days, overall, due to the dryness of yourmouth and tongue, how difficult was it to chew andswallow food? (from very difficult to easy)
Data analysis and statisticsIn the IMRT planning process, attempts were made to
spare only the superficial lobes of the parotid glands toavoid underdosing tumor targets in the parapharyngealspace; however, the entire parotid volume was used tocompute dose–volume histograms (DVHs) for data analy-sis. DVHs were computed for each gland separately. Meandose to each gland was determined by averaging dose overthe voxel elements in each parotid volume. Saliva measure-ment was converted to flow rate (mL/min) and normalizedrelative to that before treatment.
To elicit the correlation between salivary function andirradiation dose to the parotid glands, we performed thefollowing analysis. Parameter values were derived by re-gression analysis using the parotid dose distributions from
the treatment planning system and the saliva output mea-sure. Two basic models were found to describe the dataadequately. The first assumes that each gland contributes50% of the posttreatment saliva function and neglects anycontribution from the submandibular glands because theycontribute little to saliva output after receiving more than 50Gy of irradiation. In this model, each parotid gland followsa dose-fraction curve separately, and the dose curve isassumed to exponentially decrease as a function of thegland’s equivalent uniform dose (EUD) (defined below)(12). The EUD equation has a single parameter,a, whichcontrols whether EUD is closer to the maximum dose (a 5`), mean dose (a 5 1), or minimum dose (a 5 2 `). In thisstudy, the EUD parameter was found to be near 1, implyingthat EUD is nearly equivalent to the mean dose. This modelis referred to as the EUD-exponential model and is com-puted according to the following equation:
F 5 ~exp@ 2 A 3 EUD @dR,a# 2 B 3 EUD @dR,a#2#
1 exp@ 2 A 3 EUD @dL,a# 2 B 3 EUD @dL,a#2#!/ 2 (1)
whereA and B are fitted parameters,dR(dL) refers to thedose distribution of the right (left) parotid,F is the expectedresulting fractional saliva output, and EUD is the general-ized equivalent uniform dose, as given by the followingequation:
EUD@d,a# 5 S vkOk51
N
dkaD 1/a
(2)
whereN is the number of voxels andvk}is the fractionalvolume of thekth voxel. This is the same mathematicalformula referred to as the “Generalized Mean” inAbramowitz and Stegun (13). In this study, the EUD pa-rameter was found to be small (0.47/Gy), which sug-gested that using the mean dose instead of EUD might besuccessful.
The second model assumes that each CT voxel representsa parallel functional subunit and operates independently(12). Each voxel’s functional saliva output decreases expo-nentially as a function of quadratic polynomial in voxeldose. The contributions of all of the voxels are summed togive the estimate of overall posttreatment saliva function.This model is referred to as the parallel-exponential model.
The parallel-exponential model is computed according to
F 5 S Oi51
NL
vL,iexp@ 2 AdL,i 2 BdL,i2 # 1 O
i51
NR
exp@ 2 AdR,i
2 BdR,i2 #D / 2 (3)
wherev represents the relative volumes of each dose valued, NR, andNL are the number of voxels in the left and right
910 I. J. Radiation Oncology● Biology ● Physics Volume 49, Number 4, 2001
parotid glands, andA and B coefficients are the fittedparameters.
The bootstrap resampling method (14) was used to pro-duce the quoted confidence intervals. Briefly, bootstrapresampling works by refitting many pseudo data sets. Thepseudo data sets are composed of data points (each consistsof patient parotid DVHs and associated saliva measure-ments) that were randomly selected from the original dataset. When a pseudo data set is assembled, any originaldatum point may be randomly included multiple times (i.e.,selection with replacement). Fitting was carried out on eachof these pseudo data sets. In this way, bootstrap resultsprovide a quantitative estimate of how the original data mayhave reasonably varied and, hence, are the basis for confi-dence interval (CI) estimates of the fitted parameters. Aminimum of 1000 bootstrap replications were used, and95% confidence intervals were computed by identifying the25th and 975th largest values for each fitted parameter.
QOL issues were correlated with stimulated and unstimu-lated saliva flow at 6 months using a nonparametric testbased on Spearman’s rank–correlation coefficient (15).Multivariate analysis was performed using log-regressionhazard function in a BMDP program (16) to examine pos-sible influential factors that might have contributed to thechange in salivary output.
RESULTS
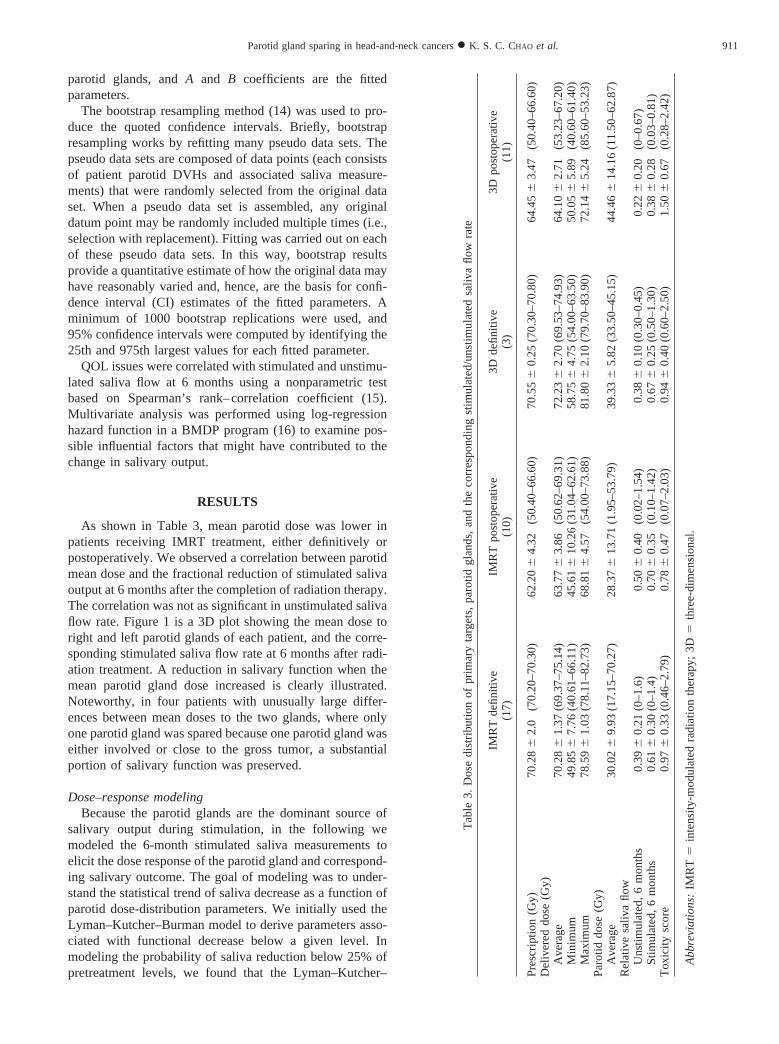
As shown in Table 3, mean parotid dose was lower inpatients receiving IMRT treatment, either definitively orpostoperatively. We observed a correlation between parotidmean dose and the fractional reduction of stimulated salivaoutput at 6 months after the completion of radiation therapy.The correlation was not as significant in unstimulated salivaflow rate. Figure 1 is a 3D plot showing the mean dose toright and left parotid glands of each patient, and the corre-sponding stimulated saliva flow rate at 6 months after radi-ation treatment. A reduction in salivary function when themean parotid gland dose increased is clearly illustrated.Noteworthy, in four patients with unusually large differ-ences between mean doses to the two glands, where onlyone parotid gland was spared because one parotid gland waseither involved or close to the gross tumor, a substantialportion of salivary function was preserved.
Dose–response modelingBecause the parotid glands are the dominant source of
salivary output during stimulation, in the following wemodeled the 6-month stimulated saliva measurements toelicit the dose response of the parotid gland and correspond-ing salivary outcome. The goal of modeling was to under-stand the statistical trend of saliva decrease as a function ofparotid dose-distribution parameters. We initially used theLyman–Kutcher–Burman model to derive parameters asso-ciated with functional decrease below a given level. Inmodeling the probability of saliva reduction below 25% ofpretreatment levels, we found that the Lyman–Kutcher–
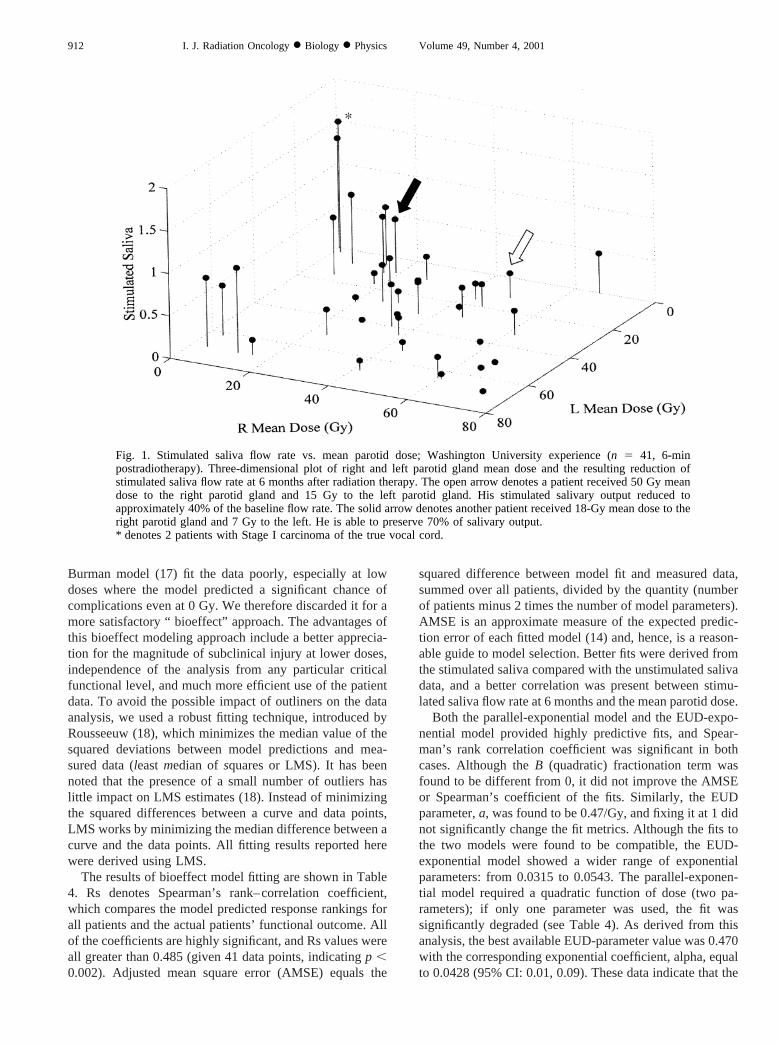
Tab
le3.
Dos
edi
strib
utio
nof
prim
ary
targ
ets,
paro
tidgl
ands
,an
dth
eco
rres
pond
ing
stim
ulat
ed/u
nstim
ulat
edsa
liva
flow
rate
IMR
Tde
finiti
ve(1
7)IM
RT
post
oper
ativ
e(1
0)3D
defin
itive
(3)
3Dpo
stop
erat
ive
(11)
Pre
scrip
tion
(Gy)
70.2
862.
0(7
0.20
–70.
30)
62.2
064.
32(5
0.40
–66.
60)
70.5
560.
25(7
0.30
–70.
80)
64.4
563.
47(5
0.40
–66.
60)
Del
iver
eddo
se(G
y)A
vera
ge70
.286
1.37
(69.
37–7
5.14
)63
.776
3.86
(50.
62–6
9.31
)72
.236
2.70
(69.
53–7
4.93
)64
.106
2.71
(53.
23–6
7.20
)M
inim
um49
.856
7.76
(40.
61–6
6.11
)45
.616
10.2
6(3
1.04
–62.
61)
58.7
564.
75(5
4.00
–63.
50)
50.0
565.
89(4
0.60
–61.
40)
Max
imum
78.5
961.
03(7
8.11
–82.
73)
68.8
164.
57(5
4.00
–73.
88)
81.8
062.
10(7
9.70
–83.
90)
72.1
465.
24(8
5.60
–53.
23)
Par
otid
dose
(Gy)
Ave
rage
30.0
269.
93(1
7.15
–70.
27)
28.3
7613
.71
(1.9
5–53
.79)
39.3
365.
82(3
3.50
–45.
15)
44.4
6614
.16
(11.
50–6
2.87
)R
elat
ive
saliv
aflo
wU
nstim
ulat
ed,
6m
onth
s0.
3960.
21(0
–1.6
)0.
506
0.40
(0.0
2–1.
54)
0.386
0.10
(0.3
0–0.
45)
0.226
0.20
(0–0
.67)
Stim
ulat
ed,
6m
onth
s0.
6160.
30(0
–1.4
)0.
706
0.35
(0.1
0–1.
42)
0.676
0.25
(0.5
0–1.
30)
0.386
0.28
(0.0
3–0.
81)
Tox
icity
scor
e0.
976
0.33
(0.4
6–2.
79)
0.786
0.47
(0.0
7–2.
03)
0.946
0.40
(0.6
0–2.
50)
1.506
0.67
(0.2
8–2.
42)
Ab
bre
via
tion
s:IM
RT
5in
tens
ity-m
odul
ated
radi
atio
nth
erap
y;3D5
thre
e-di
men
sion
al.
911Parotid gland sparing in head-and-neck cancers● K. S. C. CHAO et al.
Burman model (17) fit the data poorly, especially at lowdoses where the model predicted a significant chance ofcomplications even at 0 Gy. We therefore discarded it for amore satisfactory “ bioeffect” approach. The advantages ofthis bioeffect modeling approach include a better apprecia-tion for the magnitude of subclinical injury at lower doses,independence of the analysis from any particular criticalfunctional level, and much more efficient use of the patientdata. To avoid the possible impact of outliners on the dataanalysis, we used a robust fitting technique, introduced byRousseeuw (18), which minimizes the median value of thesquared deviations between model predictions and mea-sured data (leastmedian ofsquares or LMS). It has beennoted that the presence of a small number of outliers haslittle impact on LMS estimates (18). Instead of minimizingthe squared differences between a curve and data points,LMS works by minimizing the median difference between acurve and the data points. All fitting results reported herewere derived using LMS.
The results of bioeffect model fitting are shown in Table4. Rs denotes Spearman’s rank–correlation coefficient,which compares the model predicted response rankings forall patients and the actual patients’ functional outcome. Allof the coefficients are highly significant, and Rs values wereall greater than 0.485 (given 41 data points, indicatingp ,0.002). Adjusted mean square error (AMSE) equals the
squared difference between model fit and measured data,summed over all patients, divided by the quantity (numberof patients minus 2 times the number of model parameters).AMSE is an approximate measure of the expected predic-tion error of each fitted model (14) and, hence, is a reason-able guide to model selection. Better fits were derived fromthe stimulated saliva compared with the unstimulated salivadata, and a better correlation was present between stimu-lated saliva flow rate at 6 months and the mean parotid dose.
Both the parallel-exponential model and the EUD-expo-nential model provided highly predictive fits, and Spear-man’s rank correlation coefficient was significant in bothcases. Although theB (quadratic) fractionation term wasfound to be different from 0, it did not improve the AMSEor Spearman’s coefficient of the fits. Similarly, the EUDparameter,a, was found to be 0.47/Gy, and fixing it at 1 didnot significantly change the fit metrics. Although the fits tothe two models were found to be compatible, the EUD-exponential model showed a wider range of exponentialparameters: from 0.0315 to 0.0543. The parallel-exponen-tial model required a quadratic function of dose (two pa-rameters); if only one parameter was used, the fit wassignificantly degraded (see Table 4). As derived from thisanalysis, the best available EUD-parameter value was 0.470with the corresponding exponential coefficient, alpha, equalto 0.0428 (95% CI: 0.01, 0.09). These data indicate that the
Fig. 1. Stimulated saliva flow rate vs. mean parotid dose; Washington University experience (n 5 41, 6-minpostradiotherapy). Three-dimensional plot of right and left parotid gland mean dose and the resulting reduction ofstimulated saliva flow rate at 6 months after radiation therapy. The open arrow denotes a patient received 50 Gy meandose to the right parotid gland and 15 Gy to the left parotid gland. His stimulated salivary output reduced toapproximately 40% of the baseline flow rate. The solid arrow denotes another patient received 18-Gy mean dose to theright parotid gland and 7 Gy to the left. He is able to preserve 70% of salivary output.* denotes 2 patients with Stage I carcinoma of the true vocal cord.
912 I. J. Radiation Oncology● Biology ● Physics Volume 49, Number 4, 2001
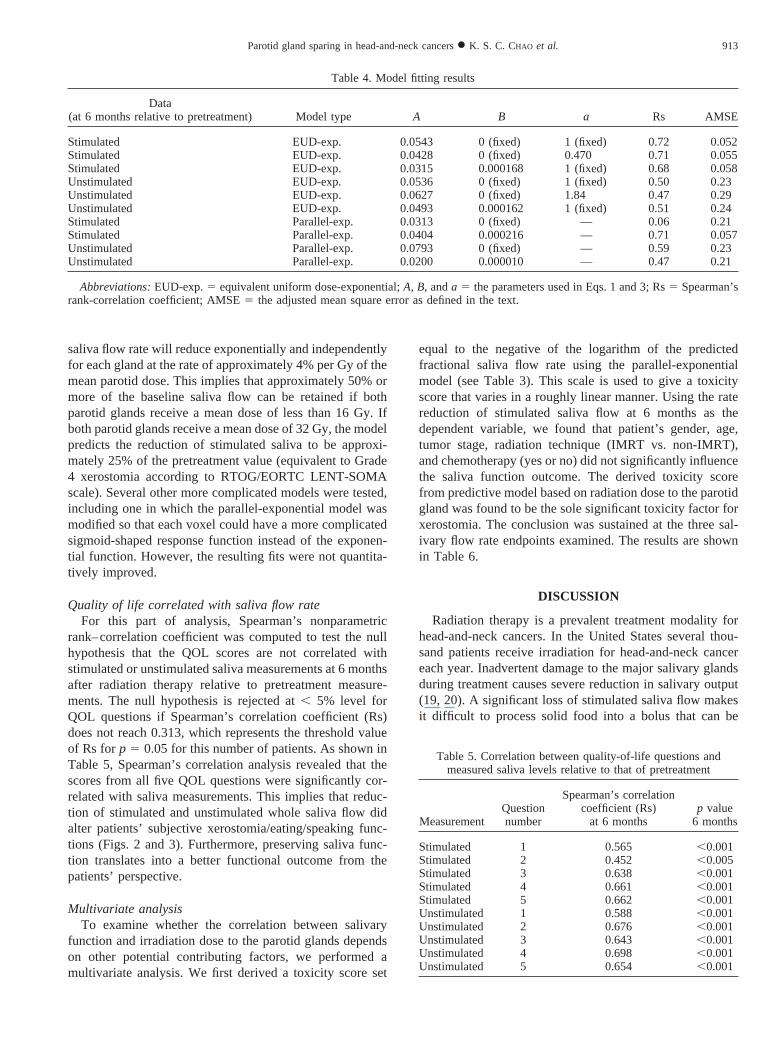
saliva flow rate will reduce exponentially and independentlyfor each gland at the rate of approximately 4% per Gy of themean parotid dose. This implies that approximately 50% ormore of the baseline saliva flow can be retained if bothparotid glands receive a mean dose of less than 16 Gy. Ifboth parotid glands receive a mean dose of 32 Gy, the modelpredicts the reduction of stimulated saliva to be approxi-mately 25% of the pretreatment value (equivalent to Grade4 xerostomia according to RTOG/EORTC LENT-SOMAscale). Several other more complicated models were tested,including one in which the parallel-exponential model wasmodified so that each voxel could have a more complicatedsigmoid-shaped response function instead of the exponen-tial function. However, the resulting fits were not quantita-tively improved.
Quality of life correlated with saliva flow rateFor this part of analysis, Spearman’s nonparametric
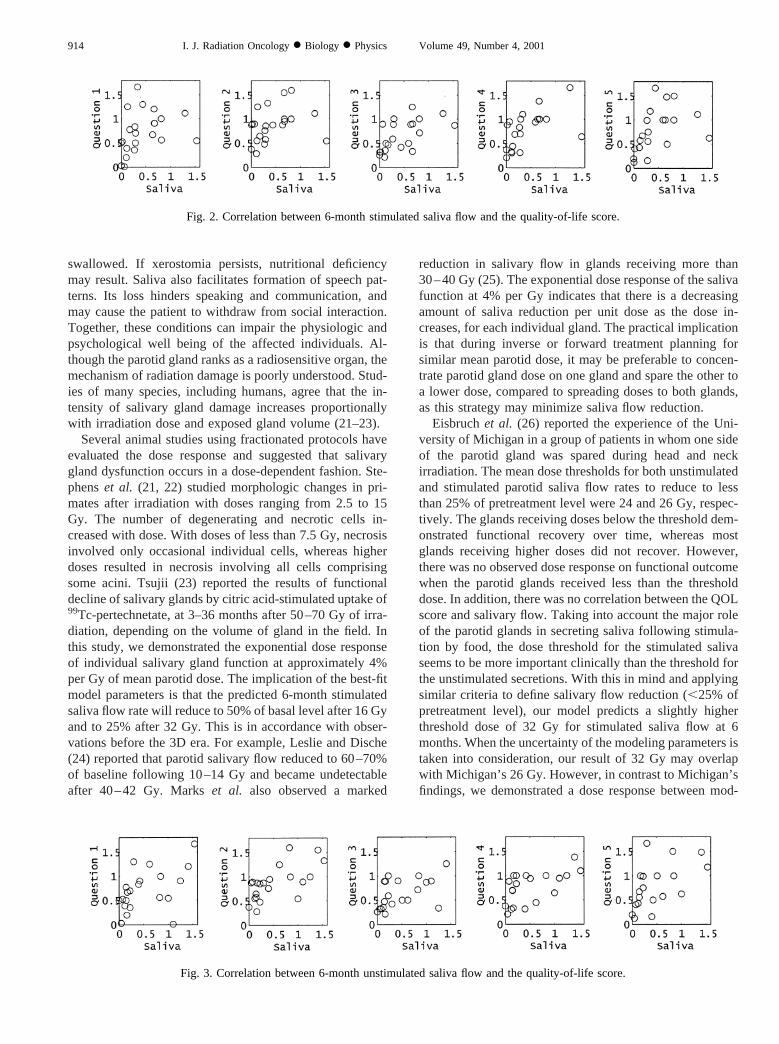
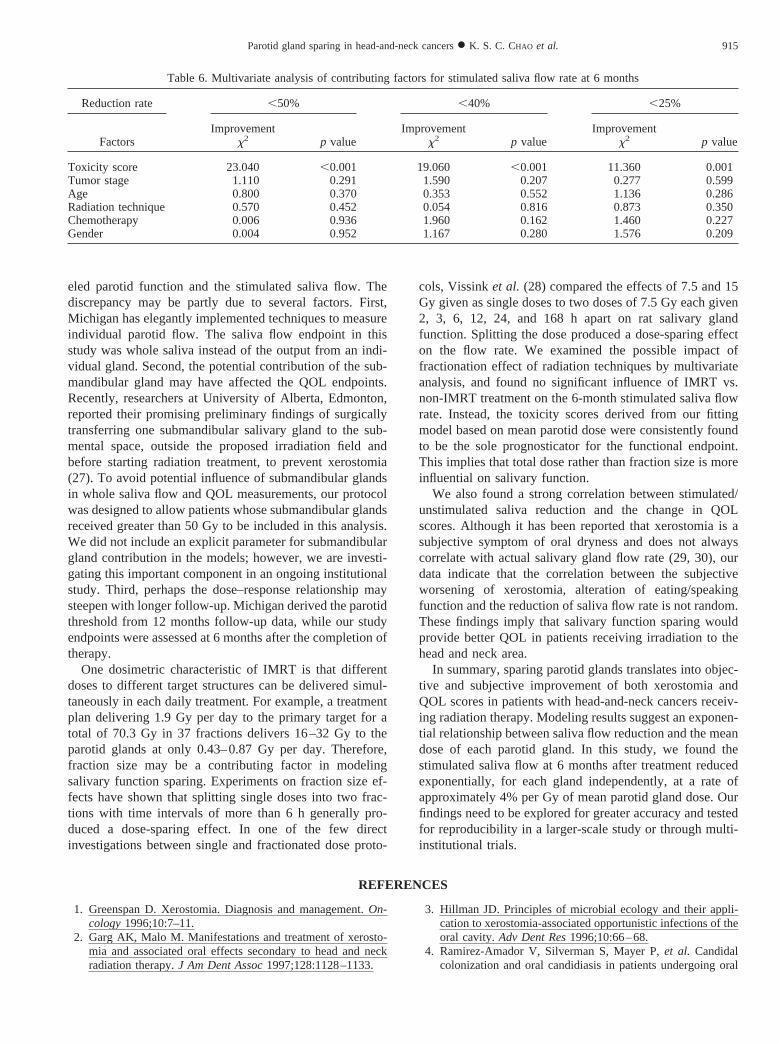
rank–correlation coefficient was computed to test the nullhypothesis that the QOL scores are not correlated withstimulated or unstimulated saliva measurements at 6 monthsafter radiation therapy relative to pretreatment measure-ments. The null hypothesis is rejected at, 5% level forQOL questions if Spearman’s correlation coefficient (Rs)does not reach 0.313, which represents the threshold valueof Rs forp 5 0.05 for this number of patients. As shown inTable 5, Spearman’s correlation analysis revealed that thescores from all five QOL questions were significantly cor-related with saliva measurements. This implies that reduc-tion of stimulated and unstimulated whole saliva flow didalter patients’ subjective xerostomia/eating/speaking func-tions (Figs. 2 and 3). Furthermore, preserving saliva func-tion translates into a better functional outcome from thepatients’ perspective.
Multivariate analysisTo examine whether the correlation between salivary
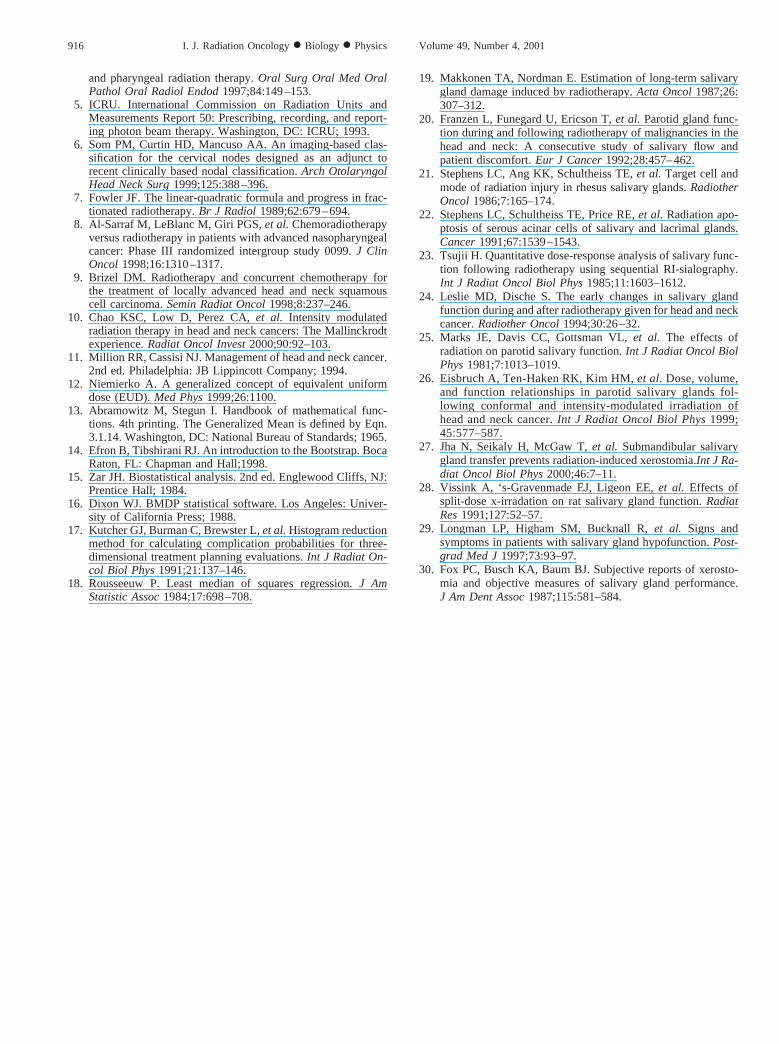
function and irradiation dose to the parotid glands dependson other potential contributing factors, we performed amultivariate analysis. We first derived a toxicity score set
equal to the negative of the logarithm of the predictedfractional saliva flow rate using the parallel-exponentialmodel (see Table 3). This scale is used to give a toxicityscore that varies in a roughly linear manner. Using the ratereduction of stimulated saliva flow at 6 months as thedependent variable, we found that patient’s gender, age,tumor stage, radiation technique (IMRT vs. non-IMRT),and chemotherapy (yes or no) did not significantly influencethe saliva function outcome. The derived toxicity scorefrom predictive model based on radiation dose to the parotidgland was found to be the sole significant toxicity factor forxerostomia. The conclusion was sustained at the three sal-ivary flow rate endpoints examined. The results are shownin Table 6.
DISCUSSION
Radiation therapy is a prevalent treatment modality forhead-and-neck cancers. In the United States several thou-sand patients receive irradiation for head-and-neck cancereach year. Inadvertent damage to the major salivary glandsduring treatment causes severe reduction in salivary output(19, 20). A significant loss of stimulated saliva flow makesit difficult to process solid food into a bolus that can be
Table 4. Model fitting results
Data(at 6 months relative to pretreatment) Model type A B a Rs AMSE
Stimulated EUD-exp. 0.0543 0 (fixed) 1 (fixed) 0.72 0.052Stimulated EUD-exp. 0.0428 0 (fixed) 0.470 0.71 0.055Stimulated EUD-exp. 0.0315 0.000168 1 (fixed) 0.68 0.058Unstimulated EUD-exp. 0.0536 0 (fixed) 1 (fixed) 0.50 0.23Unstimulated EUD-exp. 0.0627 0 (fixed) 1.84 0.47 0.29Unstimulated EUD-exp. 0.0493 0.000162 1 (fixed) 0.51 0.24Stimulated Parallel-exp. 0.0313 0 (fixed) — 0.06 0.21Stimulated Parallel-exp. 0.0404 0.000216 — 0.71 0.057Unstimulated Parallel-exp. 0.0793 0 (fixed) — 0.59 0.23Unstimulated Parallel-exp. 0.0200 0.000010 — 0.47 0.21
Abbreviations:EUD-exp.5 equivalent uniform dose-exponential;A, B,anda 5 the parameters used in Eqs. 1 and 3; Rs5 Spearman’srank-correlation coefficient; AMSE5 the adjusted mean square error as defined in the text.
Table 5. Correlation between quality-of-life questions andmeasured saliva levels relative to that of pretreatment
MeasurementQuestionnumber
Spearman’s correlationcoefficient (Rs)
at 6 monthsp value
6 months
Stimulated 1 0.565 ,0.001Stimulated 2 0.452 ,0.005Stimulated 3 0.638 ,0.001Stimulated 4 0.661 ,0.001Stimulated 5 0.662 ,0.001Unstimulated 1 0.588 ,0.001Unstimulated 2 0.676 ,0.001Unstimulated 3 0.643 ,0.001Unstimulated 4 0.698 ,0.001Unstimulated 5 0.654 ,0.001
913Parotid gland sparing in head-and-neck cancers● K. S. C. CHAO et al.
swallowed. If xerostomia persists, nutritional deficiencymay result. Saliva also facilitates formation of speech pat-terns. Its loss hinders speaking and communication, andmay cause the patient to withdraw from social interaction.Together, these conditions can impair the physiologic andpsychological well being of the affected individuals. Al-though the parotid gland ranks as a radiosensitive organ, themechanism of radiation damage is poorly understood. Stud-ies of many species, including humans, agree that the in-tensity of salivary gland damage increases proportionallywith irradiation dose and exposed gland volume (21–23).
Several animal studies using fractionated protocols haveevaluated the dose response and suggested that salivarygland dysfunction occurs in a dose-dependent fashion. Ste-phenset al. (21, 22) studied morphologic changes in pri-mates after irradiation with doses ranging from 2.5 to 15Gy. The number of degenerating and necrotic cells in-creased with dose. With doses of less than 7.5 Gy, necrosisinvolved only occasional individual cells, whereas higherdoses resulted in necrosis involving all cells comprisingsome acini. Tsujii (23) reported the results of functionaldecline of salivary glands by citric acid-stimulated uptake of99Tc-pertechnetate, at 3–36 months after 50–70 Gy of irra-diation, depending on the volume of gland in the field. Inthis study, we demonstrated the exponential dose responseof individual salivary gland function at approximately 4%per Gy of mean parotid dose. The implication of the best-fitmodel parameters is that the predicted 6-month stimulatedsaliva flow rate will reduce to 50% of basal level after 16 Gyand to 25% after 32 Gy. This is in accordance with obser-vations before the 3D era. For example, Leslie and Dische(24) reported that parotid salivary flow reduced to 60–70%of baseline following 10–14 Gy and became undetectableafter 40–42 Gy. Markset al. also observed a marked
reduction in salivary flow in glands receiving more than30–40 Gy (25). The exponential dose response of the salivafunction at 4% per Gy indicates that there is a decreasingamount of saliva reduction per unit dose as the dose in-creases, for each individual gland. The practical implicationis that during inverse or forward treatment planning forsimilar mean parotid dose, it may be preferable to concen-trate parotid gland dose on one gland and spare the other toa lower dose, compared to spreading doses to both glands,as this strategy may minimize saliva flow reduction.
Eisbruchet al. (26) reported the experience of the Uni-versity of Michigan in a group of patients in whom one sideof the parotid gland was spared during head and neckirradiation. The mean dose thresholds for both unstimulatedand stimulated parotid saliva flow rates to reduce to lessthan 25% of pretreatment level were 24 and 26 Gy, respec-tively. The glands receiving doses below the threshold dem-onstrated functional recovery over time, whereas mostglands receiving higher doses did not recover. However,there was no observed dose response on functional outcomewhen the parotid glands received less than the thresholddose. In addition, there was no correlation between the QOLscore and salivary flow. Taking into account the major roleof the parotid glands in secreting saliva following stimula-tion by food, the dose threshold for the stimulated salivaseems to be more important clinically than the threshold forthe unstimulated secretions. With this in mind and applyingsimilar criteria to define salivary flow reduction (,25% ofpretreatment level), our model predicts a slightly higherthreshold dose of 32 Gy for stimulated saliva flow at 6months. When the uncertainty of the modeling parameters istaken into consideration, our result of 32 Gy may overlapwith Michigan’s 26 Gy. However, in contrast to Michigan’sfindings, we demonstrated a dose response between mod-
Fig. 2. Correlation between 6-month stimulated saliva flow and the quality-of-life score.
Fig. 3. Correlation between 6-month unstimulated saliva flow and the quality-of-life score.
914 I. J. Radiation Oncology● Biology ● Physics Volume 49, Number 4, 2001
eled parotid function and the stimulated saliva flow. Thediscrepancy may be partly due to several factors. First,Michigan has elegantly implemented techniques to measureindividual parotid flow. The saliva flow endpoint in thisstudy was whole saliva instead of the output from an indi-vidual gland. Second, the potential contribution of the sub-mandibular gland may have affected the QOL endpoints.Recently, researchers at University of Alberta, Edmonton,reported their promising preliminary findings of surgicallytransferring one submandibular salivary gland to the sub-mental space, outside the proposed irradiation field andbefore starting radiation treatment, to prevent xerostomia(27). To avoid potential influence of submandibular glandsin whole saliva flow and QOL measurements, our protocolwas designed to allow patients whose submandibular glandsreceived greater than 50 Gy to be included in this analysis.We did not include an explicit parameter for submandibulargland contribution in the models; however, we are investi-gating this important component in an ongoing institutionalstudy. Third, perhaps the dose–response relationship maysteepen with longer follow-up. Michigan derived the parotidthreshold from 12 months follow-up data, while our studyendpoints were assessed at 6 months after the completion oftherapy.
One dosimetric characteristic of IMRT is that differentdoses to different target structures can be delivered simul-taneously in each daily treatment. For example, a treatmentplan delivering 1.9 Gy per day to the primary target for atotal of 70.3 Gy in 37 fractions delivers 16–32 Gy to theparotid glands at only 0.43–0.87 Gy per day. Therefore,fraction size may be a contributing factor in modelingsalivary function sparing. Experiments on fraction size ef-fects have shown that splitting single doses into two frac-tions with time intervals of more than 6 h generally pro-duced a dose-sparing effect. In one of the few directinvestigations between single and fractionated dose proto-
cols, Vissinket al. (28) compared the effects of 7.5 and 15Gy given as single doses to two doses of 7.5 Gy each given2, 3, 6, 12, 24, and 168 h apart on rat salivary glandfunction. Splitting the dose produced a dose-sparing effecton the flow rate. We examined the possible impact offractionation effect of radiation techniques by multivariateanalysis, and found no significant influence of IMRT vs.non-IMRT treatment on the 6-month stimulated saliva flowrate. Instead, the toxicity scores derived from our fittingmodel based on mean parotid dose were consistently foundto be the sole prognosticator for the functional endpoint.This implies that total dose rather than fraction size is moreinfluential on salivary function.
We also found a strong correlation between stimulated/unstimulated saliva reduction and the change in QOLscores. Although it has been reported that xerostomia is asubjective symptom of oral dryness and does not alwayscorrelate with actual salivary gland flow rate (29, 30), ourdata indicate that the correlation between the subjectiveworsening of xerostomia, alteration of eating/speakingfunction and the reduction of saliva flow rate is not random.These findings imply that salivary function sparing wouldprovide better QOL in patients receiving irradiation to thehead and neck area.
In summary, sparing parotid glands translates into objec-tive and subjective improvement of both xerostomia andQOL scores in patients with head-and-neck cancers receiv-ing radiation therapy. Modeling results suggest an exponen-tial relationship between saliva flow reduction and the meandose of each parotid gland. In this study, we found thestimulated saliva flow at 6 months after treatment reducedexponentially, for each gland independently, at a rate ofapproximately 4% per Gy of mean parotid gland dose. Ourfindings need to be explored for greater accuracy and testedfor reproducibility in a larger-scale study or through multi-institutional trials.
REFERENCES
1. Greenspan D. Xerostomia. Diagnosis and management.On-cology1996;10:7–11.
2. Garg AK, Malo M. Manifestations and treatment of xerosto-mia and associated oral effects secondary to head and neckradiation therapy.J Am Dent Assoc1997;128:1128–1133.
3. Hillman JD. Principles of microbial ecology and their appli-cation to xerostomia-associated opportunistic infections of theoral cavity.Adv Dent Res1996;10:66–68.
4. Ramirez-Amador V, Silverman S, Mayer P,et al. Candidalcolonization and oral candidiasis in patients undergoing oral
Table 6. Multivariate analysis of contributing factors for stimulated saliva flow rate at 6 months
Reduction rate ,50% ,40% ,25%
FactorsImprovement
x2 p valueImprovement
x2 p valueImprovement
x2 p value
Toxicity score 23.040 ,0.001 19.060 ,0.001 11.360 0.001Tumor stage 1.110 0.291 1.590 0.207 0.277 0.599Age 0.800 0.370 0.353 0.552 1.136 0.286Radiation technique 0.570 0.452 0.054 0.816 0.873 0.350Chemotherapy 0.006 0.936 1.960 0.162 1.460 0.227Gender 0.004 0.952 1.167 0.280 1.576 0.209
915Parotid gland sparing in head-and-neck cancers● K. S. C. CHAO et al.
and pharyngeal radiation therapy.Oral Surg Oral Med OralPathol Oral Radiol Endod1997;84:149–153.
5. ICRU. International Commission on Radiation Units andMeasurements Report 50: Prescribing, recording, and report-ing photon beam therapy. Washington, DC: ICRU; 1993.
6. Som PM, Curtin HD, Mancuso AA. An imaging-based clas-sification for the cervical nodes designed as an adjunct torecent clinically based nodal classification.Arch OtolaryngolHead Neck Surg1999;125:388–396.
7. Fowler JF. The linear-quadratic formula and progress in frac-tionated radiotherapy.Br J Radiol1989;62:679–694.
8. Al-Sarraf M, LeBlanc M, Giri PGS,et al.Chemoradiotherapyversus radiotherapy in patients with advanced nasopharyngealcancer: Phase III randomized intergroup study 0099.J ClinOncol 1998;16:1310–1317.
9. Brizel DM. Radiotherapy and concurrent chemotherapy forthe treatment of locally advanced head and neck squamouscell carcinoma.Semin Radiat Oncol1998;8:237–246.
10. Chao KSC, Low D, Perez CA,et al. Intensity modulatedradiation therapy in head and neck cancers: The Mallinckrodtexperience.Radiat Oncol Invest2000;90:92–103.
11. Million RR, Cassisi NJ. Management of head and neck cancer.2nd ed. Philadelphia: JB Lippincott Company; 1994.
12. Niemierko A. A generalized concept of equivalent uniformdose (EUD).Med Phys1999;26:1100.
13. Abramowitz M, Stegun I. Handbook of mathematical func-tions. 4th printing. The Generalized Mean is defined by Eqn.3.1.14. Washington, DC: National Bureau of Standards; 1965.
14. Efron B, Tibshirani RJ. An introduction to the Bootstrap. BocaRaton, FL: Chapman and Hall;1998.
15. Zar JH. Biostatistical analysis. 2nd ed. Englewood Cliffs, NJ:Prentice Hall; 1984.
16. Dixon WJ. BMDP statistical software. Los Angeles: Univer-sity of California Press; 1988.
17. Kutcher GJ, Burman C, Brewster L,et al.Histogram reductionmethod for calculating complication probabilities for three-dimensional treatment planning evaluations.Int J Radiat On-col Biol Phys1991;21:137–146.
18. Rousseeuw P. Least median of squares regression.J AmStatistic Assoc1984;17:698–708.
19. Makkonen TA, Nordman E. Estimation of long-term salivarygland damage induced by radiotherapy.Acta Oncol1987;26:307–312.
20. Franzen L, Funegard U, Ericson T,et al. Parotid gland func-tion during and following radiotherapy of malignancies in thehead and neck: A consecutive study of salivary flow andpatient discomfort.Eur J Cancer1992;28:457–462.
21. Stephens LC, Ang KK, Schultheiss TE,et al. Target cell andmode of radiation injury in rhesus salivary glands.RadiotherOncol 1986;7:165–174.
22. Stephens LC, Schultheiss TE, Price RE,et al. Radiation apo-ptosis of serous acinar cells of salivary and lacrimal glands.Cancer1991;67:1539–1543.
23. Tsujii H. Quantitative dose-response analysis of salivary func-tion following radiotherapy using sequential RI-sialography.Int J Radiat Oncol Biol Phys1985;11:1603–1612.
24. Leslie MD, Dische S. The early changes in salivary glandfunction during and after radiotherapy given for head and neckcancer.Radiother Oncol1994;30:26–32.
25. Marks JE, Davis CC, Gottsman VL,et al. The effects ofradiation on parotid salivary function.Int J Radiat Oncol BiolPhys1981;7:1013–1019.
26. Eisbruch A, Ten-Haken RK, Kim HM,et al. Dose, volume,and function relationships in parotid salivary glands fol-lowing conformal and intensity-modulated irradiation ofhead and neck cancer.Int J Radiat Oncol Biol Phys1999;45:577–587.
27. Jha N, Seikaly H, McGaw T,et al. Submandibular salivarygland transfer prevents radiation-induced xerostomia.Int J Ra-diat Oncol Biol Phys2000;46:7–11.
28. Vissink A, ‘s-Gravenmade EJ, Ligeon EE,et al. Effects ofsplit-dose x-irradation on rat salivary gland function.RadiatRes1991;127:52–57.
29. Longman LP, Higham SM, Bucknall R,et al. Signs andsymptoms in patients with salivary gland hypofunction.Post-grad Med J1997;73:93–97.
30. Fox PC, Busch KA, Baum BJ. Subjective reports of xerosto-mia and objective measures of salivary gland performance.J Am Dent Assoc1987;115:581–584.
916 I. J. Radiation Oncology● Biology ● Physics Volume 49, Number 4, 2001
Related Documents