____________ ____________ ____________ A PROPOSAL TO IMPLEMENT A QUALITY-BASED HAZARD ANALYSIS CRITICAL CONTROL POINT PROGRAM TO REDUCE THE SPREAD OF HOSPITAL-ACQUIRED INFECTIONS IN HEALTHCARE FACILITIES A Thesis Presented to the Faculty of California State University Dominguez Hills In Partial Fulfillment of the Requirements for the Degree Master of Science in Quality Assurance by Mercedes Miles Spring 2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

____________
____________
____________
A PROPOSAL TO IMPLEMENT A QUALITY-BASED HAZARD ANALYSIS
CRITICAL CONTROL POINT PROGRAM TO REDUCE THE SPREAD OF
HOSPITAL-ACQUIRED INFECTIONS IN HEALTHCARE FACILITIES
A Thesis
Presented
to the Faculty of
California State University Dominguez Hills
In Partial Fulfillment
of the Requirements for the Degree
Master of Science
in
Quality Assurance
by
Mercedes Miles
Spring 2018
___________________________________
___________________________________
___________________________________
THESIS: A PROPOSAL TO IMPLEMENT A QUALITY-BASED HAZARD ANALYSIS CRITICAL CONTRL POINT PROGRAM TO REDUCE THE SPREAD OF HOSPITAL-ACQUIRED INFECTIONS IN HEALTHCARE FACILITIES
AUTHOR: MERCEDES MILES
APPROVED:
James Clauson MSQA Thesis Committee Chair
Robert Spencer MA, MSQA Committee Member
Milton Krivokuca DBA, MSQA Committee Member
TABLE OF CONTENTS
PAGE
TABLE OF CONTENTS ................................................................................................... iii
LIST OF TABLES .............................................................................................................. v
LIST OF FIGURES ............................................................................................................ vi
ABSTRACT ...................................................................................................................... vii
CHAPTER
1. INTRODUCTION ........................................................................................................... 1
Crosby’s DRIFT Theory .......................................................................................... 1 The HACCP System ................................................................................................ 8 Statement of the Problem ...................................................................................... 13 Purpose of the Study .............................................................................................. 17 Theoretical Bases ................................................................................................... 20 Definition of Terms ............................................................................................... 27
2. REVIEW OF THE LITERATURE ............................................................................... 31
Implementing Quality Assurance .......................................................................... 32 Corrective Actions ................................................................................................. 39 Ad Hoc Committee for Zero Defects .................................................................... 46 Zero Defects Day ................................................................................................... 46 Do It Over Again ................................................................................................... 48 Quality Improvement Team .................................................................................. 49 Quality Awareness ................................................................................................. 50 Corrective Actions ................................................................................................. 50 Quality Councils .................................................................................................... 52
iii

CHAPTER PAGE
3. METHODOLOGY ........................................................................................................ 53
Observations .......................................................................................................... 54 Discussions ............................................................................................................ 55 Method ................................................................................................................... 56
4. RESULTS AND DISCUSSIONS ................................................................................. 59
Step 1: Establish a Team ....................................................................................... 59 Step 2: Describe the Product or Service ................................................................ 60 Step 3: Identify Intended Purpose of the Service .................................................. 61 Step 4: Draw a Flow Diagram of the System ........................................................ 64 Step 5: On Site Confirmation of Flow Diagram .................................................... 67 Step 6: Identify and Analyze Hazards (Principle 1) ............................................. 69 Step 7: Determine Critical Control Points (Principle 2) ....................................... 73 Step 8: Establish Critical Limits (Principle 3) ...................................................... 74 Step 9: Establish Monitoring Procedures (Principle 4) ........................................ 76 Step 10: Establish Corrective Actions (Principle 5) ............................................. 76 Step 11: Verify the HACCP Plan (Principle 6) .................................................... 77 Step 2: Keep Records (Principle 7) ..................................................................... 78
5. SUMMARY, CONCLUSIONS, AND RECOMMENDATIONS ................................ 81
6. REFERENCES ............................................................................................................. 84
APPENDIX ...................................................................................................................... 89
iv

LIST OF TABLES
PAGE
1. Hospital Acquired Infections Estimates Occurring in US Acute Care Hospitals
in 2011 .............................................................................................................................. 15
2. Hazard Assessment ........................................................................................................ 71
v

LIST OF FIGURES
PAGE
1. Crosby’s DRIFT Theory .................................................................................................. 3
2. Flow of Patient in Acute Hospital ................................................................................. 65
vi

ABSTRACT
This thesis proposes a design for a quality based hazard analysis critical control
HACCP program, incorporating concepts from Philip Crosby’s doing it right the
first time DRIFT theory to reduce the spread of hospital-acquired infections HAI.
HAI are often preventable by incorporating quality assurance QA programs for
analyzing problems and identifying appropriate solutions. Research shows that
HAI rates can be decreased dramatically when healthcare facilities are aware of
infection rates and proactively institute QA-based control measures. The
implementation of a HACCP program, using concepts from the DRIFT theory,
can shift the culture of patient care by setting the standard to do things right the
first time. A HACCP program based on concepts from the DRIFT theory can help
healthcare facilities reform how care is delivered; applying a prevention program
that involves both clinical and non-clinical personnel. This type of program can
reduce HAI and raise HAI awareness.

1 CHAPTER 1
INTRODUCTION
Each year, thousands of patients in the United States US are admitted to
healthcare facilities for routine inpatient and outpatient services. During these routine
services, patients can potentially contract hospital-acquired infections HAI; HAI are
infections that are not present at admission. According to a study conducted by the Center
of Disease Control CDC, approximately one out of every 25 hospitalized patients in the
US has contracted HAI (Center of Disease Control, 2016). These diseases put patient
safety at risk and are usually preventable. Research shows that HAI rates can decrease
significantly when prevention measures are in place.
For the purpose of this thesis, prevention measures for the HAI methicillin-
resistant staphylococcus aureus MRSA are examined. This thesis proposes a quality
assurance QA program design, based on concepts from Philip Crosby’s doing it right first
the first time DRIFT theory (Crosby, 1979) and the hazard analysis critical control point
HACCP program (United States Food and Drug Administration, 1990). This background
provides the history of both the DRIFT theory and the HACCP program.
Crosby’s DRIFT Theory
Philip Crosby’s doing it right the first time DRIFT theory was first introduced in
1979 in his book, Quality is Free (Crosby, 1979). This concept argued that the cost of
non-conformances was the cost of not doing it right the first time; defects should be
identified and corrected immediately. Crosby believed that the cost of quality was the

2 expense of doing things wrong. Quality management was built into the concept of
making things happen.
Crosby’s DRIFT theory was developed to encourage a system that worked towards
zero defects (Crosby, 1996). This type of process eliminated waste and loss of time
“quality management is deliberately creating an organizational and personal culture
where all transactions are accomplished correctly and on time” (Crosby, 1996, p 2).
When deviations occurred, it made the organization place more time and resources
toward correcting the issue. Wassenberg, Wit, Hout, and Bonten (2010) discussed how
“methicillin resistant staphylococcus aures MRSA, pose a global healthcare problem,
resulting in direct costs associated with increased healthcare consumption an indirect
costs due to morbidity and loss of life years” (Wassenberg et al., 2010, p 2).
With the cost of healthcare, the goal should always be aimed towards doing things
right the first time. When things are not done right the first time, ultimately the patient
suffers, and the facility can be at risk of malpractice law suites. Any discrepancy in the
process can put both the patient and healthcare worker at risk. Crosby’s DRIFT theory,
introduced in 1996, is composed of four concepts, as presented in Figure 1.

3
Figure 1. Crosby's drift theory. Introduced in Quality is Free, By Philip Crosby, 1996.
Quality is Conformance to Requirements
The quality is conformance to requirements concept measures the process or
product’s ability to meet specifications of a design. The design specification is an
exposition of what the customer needs. Management must pay close attention to a
product or service to establish conformance, this allows management to identify any
issues that needs to be corrected or adjusted. The quality is conformance to requirements
also measures the effectiveness of the product or process.
Crosby’s quality concept can measure the commitment to evidence-based
standards of care the hospital provides. Length of stay, readmission, and services
provided can be measured to identify incident rates of HAI. According to the Centers of
Medicare and Medicaid Services Deficient Reduction Act of 2005, is required to identify
conditions that are:
• High cost.

4 • Result in assignment of diagnosis related group (DRG) that result in higher
payment.
• Could be preventable based on evidence and guidelines.
The following are evidence-based practices related to healthcare-associated
infections (Kleinpell, Munro, & Giuliano 2008):
• Hospital-associated pneumonia.
• Hand hygiene.
• Respiratory care.
• Patient positioning.
• Urinary tract infections.
• Catheter-related bloodstream infection.
• Sepsis.
• Antibiotic resistant infections.
• Control on patient-to-patient contact.
• Control of antibiotic use.
• Staff education and compliance.
The prevention of HAI ensures a safe healthcare facility for patients and
healthcare workers. Setting specifications allows the facility to establish a standard. By
conforming to requirements, healthcare facilities can set a standard of care and ensure
these standards are being maintained.

Performance Standard is Zero Defects
5
The performance standard is zero defects concept does not mean defects are not
going to occur; however, the goal is to eliminate defects. In order to achieve zero defects,
policies/procedures must be clear and proper training/education must be provided. This
objective requires motivation from the staff and a behavior shift to doing things
according to the process. To encourage employees to meet quality goals, management
can implement incentive programs. Zero defects can be difficult to achieve and result in
extra inspections and monitoring; however, if implemented properly, the program can
eliminate waste and improve quality.
A zero defects performance standard would force healthcare facilities to address
key components and patient safety. This type of standard could prevent accidental deaths.
Based on the standard, this type of system could ensure a well-designed, preventative
process that would recognize and correct errors. A zero defects performance standard
would help healthcare facilities to develop a system that could correct errors and improve
patient safety rates. With a zero defect standard, hospital personnel could communicate
clearly, provide feedback to management, and be aware of potential accident that might
arise. In order for healthcare facilities to accomplish this type of standard, the facility
would need to:
• Evaluate processes in place to reduce HAI.
• Develop preventative and corrective tasks.
• Ensure that staff members are properly trained.
• Analyze precautions in place to reduce errors.

6 A zero defect standard can improve safety and establish a system in which things
are done correctly the first time. In the healthcare industry, when defects occur, they can
result in harm to the patients, which can worsen their conditions and in certain cases,
result in death.
Management System is Prevention
Management must have a strategic plan in place with the objective of preventing
deviations. Prevention measures must be in place and must be enforced. Management
should place emphasis on prevention. It is up to management to set the tone for quality
initiative. Non-conformances mean management has failed to control the process.
Prevention measures for HAI are (Vaidya, 2013):
• Hand washing.
• Environmental hygiene.
• Screening patients.
• Vaccinations.
• Surveillance.
• Antibiotic Stewardship.
• Safety programs.
• Care coordination.
Although prevention measures are in place to prevent HAI, a quality program
based on concepts from Crosby’s DRIFT theory can enforce prevention measures.

Measurement System Is the Cost of Quality
7
The measurement system is the cost of quality concept measures the price of non-
conformances. This system measures how non-conformances can impact the organization
as a whole. An effective quality improvement program can reduce operation costs and
allow the organization to use those saved resources in other areas. A cost analysis
conducted by management should be done regularly to determine effects, opportunities,
savings, and action priorities. The quality cost system can have a positive impact on the
organizations goals, objectives, mission, and provide management with a breakdown of
goals and achievements.
The DRIFT theory focuses on zero defects. Defects are any discrepancy that can
affect the quality, safety, or efficiency of a product or service. Work should be defined by
clear requirements with activities designed to eliminate defects. According to Crosby, the
purpose of zero defects is to communicate and install a program that aims towards
DRIFT (Crosby, 1979). This program would not be a motivational program; it would be a
program that shifts behaviors (Crosby, 1979). When things are done wrong, it can cost
the organization time, money, and resources. In Quality is Free (1979), Crosby
summarizes 14 points:
• Management Commitment.
• Quality Improvement Team.
• Quality Measurement.
• Cost of Quality Awareness.
• Quality Awareness.

8 • Corrective Actions.
• Establish Ad-hoc Commitment for Zero Defects Program.
• Supervisor Training.
• Zero Defects Data.
• Goal Setting.
• Error Cause Removal.
• Recognize.
• Quality Council.
• Doing It Over Again.
The HACCP System
The Pillsbury Corporation developed the hazard analysis critical control point
HACCP program in the 1960’s when working with the National Aeronautics and Space
Administration to develop a system to ensure food safety for the first manned space
mission. The guidelines for the system were designed by the Codex Alimentarius
Commission; a body that was established in early November 1961 by the Food and
Agriculture Organization FAO of the United Nations. The Alimentarius Commission
applied standards from the FAO and World Health Organization to prioritize and control
potential hazards in food production to ensure that food remained safe. The system was
designed to control microbiological, chemical, and physical contamination. In the early
1990s, HACCP transpired worldwide as the foundation for managing food safety.
Currently, the Food and Drug Administration, United States Department of
Agriculture, and various state agencies are involved with and promote the HACCP

9 system. The goal of HACCP in the food industry is to reduce food-born illness and
improve product quality. The HACCP program has helped the food industry
control/prevent contamination and foodborne illness. If implemented properly, a HACCP
program can help prevent the spread of hospital acquired infections HAI in hospitals and
long-term care facilities. The purpose of this thesis is to examine how the HACCP
program has been beneficial in the food industry and develop a program that can be
implemented in the healthcare industry.
The HACCP system addresses safety through the analysis and control of
biological, chemical, and physical hazards. The goal of the HACCP system is to provide
evidence of the establishments’ ability to manage food safety on a global standard. The
HACCP system assures that food is safe from harvest to consumption. According to
McCoy and Rosenblatt (2015) “The beneficial use of HACCP is not limited to any
specific type of hazard or process; the methodology has proved effective and flexible, and
is increasingly applied to industries other than food, including cosmetics,
pharmaceuticals, and bottle water” (McCoy & Rosendblatt, 2015, p. 5). The system is
designed to prevent problems from occurring and identifying potential risk at each step of
the process or procedure. If discrepancies arise, they are to be documented and corrected
once identified.
The HACCP system is broken down into the following seven principles to
identify, evaluate, and control of hazards (McCoy & Rosenblatt, 2015):
Principle 1: Conduct a hazard analysis.
Principle 2: Determine the critical control points CCPs.

10 Principle 3: Establish critical limits.
Principle 4: Establish monitoring procedures.
Principle 5: Establish corrective actions.
Principle 6: Establish verification procedures.
Principle 7: Establish record keeping and document procedures.
There are 12 steps for implementing the seven principles of HACCP (McCoy &
Rosenblatt, 2015):
1. Establish a team.
2. Describe the system.
3. Identify intended use(s).
4. Construct process flow diagrams.
5. Confirm the accuracy of the process flow diagrams.
6. List all potential hazards associated with each step; conduct a hazard analysis.
7. Determine critical control points CCP.
8. Determine critical limits for each CCP.
9. Establish monitoring procedures.
10. Establish corrective actions.
11. Establish procedures to confirm the plan is being implemented.
12. Establish documentation and record keeping procedures.
In order for the HACCP system to be beneficial for an organization, the program
must have a solid foundation. Procedures must be developed to address operational
conditions. These procedures are known as the prerequisite program. These procedures

11 can be considered in the HACCP plan, but they are established and managed separately.
The prerequisites PRPs are to be established before designing the HACCP plan and must
be documented and audited regularly. The HACCP program operates simultaneously
with the prerequisite program. The HACCP system “is a specific risk management
system designed to reduce identified hazards and risk associated with a particular product
or process, while prerequisite PRPs are general risk reduction practices and procedures”
(Griffith, 2006, p. 2). The PRPs procedures include design/layout, equipment, pest
control, cleaning, sanitation, traceability, personal hygiene, and training. The PRP
programs that are beneficial to the HACCP plan are standard operating procedures SOPs.
The SOPs should be completed, signed, and reviewed daily. [See Appendix for a
SOP example] The SOPs should include the following (Center of Disease Control, 2016):
• The purpose.
• The scope.
• Key words.
• Instructions.
• Monitoring.
• Corrective Actions.
• Verification and record keeping.
To maintain a successful HACCP program, education and training must be
developed; these are important tools for the success of the program. The Food and Drug
Administration Guidance Regulations (2006) suggest, training activities be included with
an outline of instructions and procedures for monitoring CCPs. The education and
12 training should provide information on the hazards and steps to be taken to
control/monitor them. Examples of potential hazards in the healthcare industry can
include bodily fluids, airborne virus, and the cleaning of patient rooms. Griffith (2006)
suggests “Some level of HAI are unavoidable, however, the aim of infection control
should be to keep this to a minimum” (p. 2). In order to fully identify all hazards in the
facility, the HACCP team must analyze the current procedures in place.
It is vital that employees first understand the HACCP plan before it can be
applied. Once employees have a clear understanding, they can learn and develop the
skills necessary to support the HACCP plan. Griffith (2006) argues that, “HACCP could
provide a risk management approach, however, it should be emphasized that individual
human behavior, in the context of the prevailing organizational infection control culture,
is an important determinant of success” (p. 2). The necessary skills needed must be
specific to the facility’s process. Training and education on proper cleaning, sanitation,
and patient contact should be conducted.
An assembled HACCP team must consist of individuals who have specific
knowledge of the process because these members are going to be responsible for
developing the HACCP plan. Team members who have knowledge in organizations
operations must be able to conduct a hazard analysis, identify potential hazards,
determine controls, recommend critical limit, and determine monitoring/validation
procedures. The team should consist of individuals from each department who are
involved in different areas of the process. The Federal Drug Administration FDA suggest
the team include local personal who are involved in operation as they are more familiar

13 with the operation (Food and Drug Administration, 2014). Having a representative from
each department in the organization can be beneficial for the team because it allows
different perspectives to come from various services in the process. Once the HACCP
team is developed, the team must describe the process/product and intended
use/consumer.
Statement of the Problem
Healthcare associated infections are among the top ten leading causes of death in
the United States US. Some of the leading causes for hospital acquired infections HAI
are: the use of medical devices, complications following surgery, overuse of antibiotics,
transmission between patients and healthcare workers, and patients not completing
antibiotic prescriptions. Methicillin-resistant Staphylococcus aureus MRSA is a HAI that
has become resistant to many commonly used antibiotics including methicillin,
amoxicillin, penicillin, and oxacillin. Due to this resistance, it is extremely difficult to
treat the infection. The bacteria can spread from person to person through skin-to-skin
contact. The bacteria can survive for long periods of time on surfaces or objects including
door handles, floors’, sinks, taps, cleaning equipment, and fabric. The MRSA infections
cause illness in people with weak immune systems, open wounds, with skin conditions,
and patients who use invasive medical equipment such as catheters (“Healthline Media”,
2017). The bacteria can spread to others through animate and inanimate environments.
HAI are infections that are developed within 24 hours of hospital stay that were
not present at hospital admission (Hensley & Monson, 2015). Despite the increasing
attention to HAI and current monitoring tools in place, HAI have continued to be an issue

14 for healthcare facilities. Not only does HAI impact the quality of care provided to
patients, it also increases the cost of healthcare. Hensley & Monson (2015) suggest, “HAI
have been associated with increasing medical costs, length of stay, complication rates,
and worsening overall morbidity and mortality” (p. 1). Over the years, there have been
several initiatives implemented for infection control. One of the initiatives that have been
considered most notable is the change in the payment system for Medicare and Medicaid,
which no longer will pay hospitals for HAI.
Although there are processes and procedures in place, HAI continue to be an issue
and concern for healthcare facilities. Carriers or persons/organisms with MRSA
infections can spread the bacteria even when they are not sick. Both colonized and
infected patients can be the source of spreading MRSA. Not only has the bacteria
increased the amount of healthcare-associated deaths, but it also has increased healthcare
costs by forcing healthcare facilities to treat unnecessary illness. Medicare penalizes
hospitals with patients who suffer from avoidable complications (Rau, 2015). These
avoidable complications can result in claims being denied and being left unpaid.
Leading sources of HAI are the hands of healthcare workers (“Newswire”, 2007).
There are five moments when hygiene compliance is required according to the World
Health Organization. These moments occur before patient contact, before performing
aseptic tasks, after exposure to body fluids, after patient contact, and after contact with
patients’ surroundings. There were an estimated 722,000 HAIs in 2011 and
approximately 75,000 patients with HAIs died during their hospitalizations (“Healthcare

15 Prevalence Survey,” 2014). Table 1 provides a breakdown of HAI infections acquired in
acute care hospitals in 2011.
Table 1
HAI Estimates Occurring in US Acute Care Hospitals in 2011 HAI Estimates Occurring in US Acute Care Hospitals, 2011
Major Site of Infection Estimated No. Pneumonia 157,500 Gastrointestinal Illness 123,100 Urinary Tract Infections 93,300 Primary Bloodstream Infections 71,900 Surgical site infections from any inpatient surgery 157,500 Other types of infections 118,500 Estimated total number of infections in hospitals 721,800
Note. Taken from the “Healthcare Prevalence Survey,” 2014.
Federal Steering Committee
The Federal Steering Committee for the Prevention of Health Care-Associated
Infections was developed by the United States Department of Health and Human Services
in January 2009 to identify HAI as an important public health and patient safety issue.
The purpose of this committee was to develop and coordinate prevention efforts across
the federal government. Members of the committee included clinicians, scientists, and
public health leaders. The committee developed the National Action Plan to Prevent
Health Care-Associated Infections in 2017. This plan was broken down into three phases:
acute care hospitals, outpatient settings, influenza vaccination of healthcare personnel,
and long term care facilities (Office of Disease Prevention and Health Promotion, 2017).
Phase one consist of a five year action plan to reduce the spread of hospital
acquired infection HAI in acute care hospitals. The following provides a breakdown of
this five-year plan:

16 • Reduce central line associated bloodstream infections in intensive care unit
ICU and ward-located patients.
• Reduce catheter-associated Urinary Track Infection catheter-associated urinary tracts infections in ICU and ward-located patients.
• Reduce the incidence of invasive healthcare-associated Methicillin-resistant Staphylococcus Aureus infections.
• Reduce facility-onset MRSA in facility-wide healthcare.
• Reduce facility-onset and rate of clostridium difficile infections in facility-wide healthcare.
• Reduce surgical site infections surgical site admission and readmission.
Phase two focuses on outpatient settings and addresses health and safety concerns
for health care workers; consisting of three chapters: Ambulatory Surgical Centers, End-
Stage Renal Disease Facilities, and Influenza Vaccination of Health Care Personnel.
These three chapters provide a breakdown of outpatient environments and safety
concerns of health care works. These three chapters, also discusses the risks of
transmission of influenza from health care personnel to patients and prevention measures
in place (Office of Disease Prevention and Health Promotion, 2017)
Phase three is centered on long-term care facilities. Over the years, there has been
an escalation in patients receiving services in long-term care facilities. As a result, there
have been, an increased risk of HAIs, which can worsen health status and increase health
care costs. Patients in these facilities require complex medical care. The need for long-
term care can be due to a terminal condition, disability, illness, injury, or old age.
According to the Center of Disease Control CDC, one to three million infections occur
every year in long-term care facilities (Center of Disease control, 2016). Long-term care

17 facilities can include nursing homes, skilled nursing facilities, and assistant living
facilities. These facilities provide medical and personal care to patients who are unable to
care for themselves.
Purpose of the Study
The purpose of this study was to propose a HACCP program that implemented
Philip Crosby’s DRIFT theory to help healthcare facilities control the spread of HAI. By
implementing this type of quality assurance QA program, healthcare facilities could
prevent the spread of HAI. According to Hensley & Monson (2015), HAI have been
associated with:
• Increasing medical costs.
• Increasing length of stay.
• Increasing complication rates.
• Increasing overall morbidity and mortality rates.
In order to implement Crosby’s DRIFT theory, this thesis recommended that
healthcare facilities develop a quality-based HACCP program. According to Huebak and
Schlosser (2012), “the major health concerns of the time were the potential for
transmission of diseases from sick animals to humans and the lack of sanitary conditions
for animal slaughter and production of processed products” (p. 2). The purpose of the
program was to prevent meat from diseased animals to enter into commerce. Federal
inspectors inspected every animal for signs of disease. They also inspected unsanitary
practices to eliminate risk of contamination. The goal of the HACCP system was to
reduce the risk of foodborne illness associated with contamination.

18 This new system caused difficult scientific and policy questions. Huebak and
Shlosser (2012) stated, “the setting of specific quantitative limits for each significant
pathogen was precluded because of an inadequate scientific understanding of the link
between specific levels and many pathogens and the risk of foodborne illness that would
be needed to set standards on public health grounds” (p. 4). A primary goal of the
HACCP system was to set standards and regulations for the food and meat industry. A
secondary goal of the system was to help improve the quality and practices of production
and manufacturing. If conducted properly, the system could reduce potential biological,
chemical, and physical foodborne hazards. These targets and standards were to be met on
a consistent basis.
In order to implement a successful HACCP program, healthcare facilities must
identify and evaluate hazards associated with hospital-acquired infections HAI. This can
help identify significant hazards that should be evaluated in the HACCP program. Once
hazards have been identified, critical control points CCP must be established. After CCPs
have been established, monitoring techniques must be developed in order for the HACCP
program to be beneficial to the facility. The critical control points for HAI can be patient-
employee contact, isolating infected or colonized patients into single rooms or cohorts,
and screening patients for infection. In a successful HACCP program for HAI, audits
should be conducted, Adenosine Triphoshate testing on employees hands/equipment
should conducted, and quarterly micro testing on patients’ rooms and healthcare
equipment should be done. This thesis provides a breakdown of a proposed HACCP plan
that will promote Crosby’s DRIFT theory.

19 A HACCP program can be beneficial in the healthcare industry for reducing
unnecessary cost and improving the quality of care provided. When conducted properly,
the HACCP system saves money in day-to-day costs, ensuring that resources are used
effectively. The HACCP system demonstrates high standards and commitment to
compliance for regulatory requirements. This type of quality program applies safe,
effective, and efficient processes to ensure the organization remains compliant with
current laws and regulations. The HACCP system enhances safety and increases
consumer confidence in the service provided. This system also is specific to a particular
product or service and is designed specifically for that product or service. This type of
program provides a timely response to safety problems and is capable of accommodating
change such as:
• Advances in technology.
• Processing procedures.
• Technological development.
In order for the HACCP system to be effective, full commitment from
management and the workforce is required. The HACCP system is a scientific risk
analysis that requires a team approach. Effective staff training ensures:
• A clear understanding of safety.
• Hazard analysis are conducted properly.
• Risk assessment.
• Teamwork.

20 Theoretical B ases
A HACCP system with concepts from Crosby’s DRIFT theory allows healthcare
facilities to develop a quality program that aims towards preventing HAI. This thesis
covers the application of Crosby’s DRIFT theory by implementing a HACCP system to
help control the contamination of HAI in healthcare facilities. Philip Crosby’s DRIFT
theory promotes prevention management in every area. The goal is to train staff and give
them the tools needed for quality management.
The DRIFT theory can allow healthcare facilities to focus on making patients
better rather than focusing on curing them from HAI. One error in the process can
impact the quality of care provided to the patient. The DRIFT theory’s goal is to have
zero defects by ensuring that things are done correctly the first time. It takes time and
resources to implement this a quality-based prevention program: however, in the long
run, it can cut the cost of healthcare and improve the quality of care provided. The
DRIFT theory can encourage healthcare facilities to continuously improve and aim
toward zero defects and errors.
The HACCP system is a systematic quality program that aims towards prevention.
Although there are differences, the HACCP program can be compared to the corrective
and prevention actions corrective and prevention actions CAPA quality program. The
CAPA system focuses on root causes and attempts to prevent reoccurrence. The purpose
of the CAPA program is to collect information, analyze information, investigate and
identify quality concerns, and take appropriate action. The CAPA system can be broken
down into the following 10 steps (United States Food and Drug Administration, 2014):

21 1. Verify CAPA system and procedures.
• Correct and prevent reoccurrence.
• Gain a working knowledge of the organization’s corrective and preventive measures.
• Include procedures on how to meet requirements.
2. Determine if the appropriate sources of quality problems have been identified.
• Develop methods and procedures to input product/quality problems in the CAPA subsystem.
• Routinely analyze quality data.
• Review raw data used by the organization when conducting quality audits and management reviews.
3. Determine if sources of the product/quality information are unfavorable and identify trends.
• Identify product/quality problems that may require preventive measures.
• Review record.
• Review if corrective measures have been taken.
• Determine if the organization is capturing and analyzing data regarding non-conformances.
• Determine if the firm is using statistical control techniques for process controls.
4. Challenge the quality data information system.
• Verify data is complete and accurate.
• Review records.
5. Verify appropriate statistical methods are employed to detect recurring quality problems.

22 • Include statistical and non-statistical techniques.
• Pareto analysis, spreadsheets, pie charts.
• Non-statistical techniques, quality review boards, quality review meetings.
• Capturing the full extent of problem(s) before the probability of occurrence and corrective measures can be determined.
6. Determine if failure investigation procedures are followed.
• Determine if failure investigations are conducted to determine root causes.
• Review CAPA procedures.
• Determine procedures for failure modes.
• Confirm failure modes.
• Determine depth of the investigation.
7. Determine if corrective and preventive actions are effective, verified, or validated prior to implementation.
• Confirm corrective actions do not adversely affect the finished
product.
• Corrective actions should include: good engineering principles, verification/validation protocols, verification of product requirements/specifications, and ensuring test instruments are maintained.
8. Determine if corrective and preventive measures are effective.
• Review trends.
• Determine if the organization has verified and validated corrective measures.

23 9. Verify that corrective and preventive actions for product/quality problems
were implemented and documented
• Review the most recent corrective and preventive actions.
• Determine if correction/prevention measures and changes have been updated.
10. Determine if information regarding non-conforming product/preventive actions have been properly taken.
• Determine if corrective/prevention information has been submitted to management for review.
• Review raw data submitted to management.
• Review CAPA to confirm mechanisms taken.
The hazard analysis critical control point HACCP program is a systematic system
that identifies where hazard may occur in a production process. Once potential hazards
have been identified, actions to develop preventive measure are developed by monitoring
and controlling each step of the process. The HACCP system controls and prioritizes
potential hazards in the process. By controlling hazards, the organization is able to
provide a safer product or service for the customer. The HACCP system focuses on
prevention and control of hazards that can cause harm to the consumer. The HACCP
system consist of seven principles (United States Food and Drug Administration, 2014):
1. Conduct a hazard analysis.
2. Identify critical control points CCP.
3. Establish critical limits.
4. Establish CCP monitoring requirements.
5. Establish corrective actions.

24 6. Establish record keeping.
7. Establish verification procedures.
The HACCP system demonstrates high standards and commitment to the
customer maintaining regulatory requirements and establishing procedures to ensure the
organization remains compliant with current laws and regulations. If conducted properly,
the HACCP system can save money in day-to-day operation costs. The HACCP applies
safe, effective, and efficient systems. These systems are designed to ensure the
organization remains complaint with current regulations. When conducted properly, the
HACCP system enhances safety, gaining consumer confidence. The HACCP system
provides a timely response to safety issues.
The ultimate goal of the HACCP plan is to prevent problems. If discrepancies
occur, appropriate steps must be taken to reestablish control in a timely manner. The
HACCP programs have been implemented in the food, cosmetics, pharmaceuticals, and
the bottled water industry in order to provide safer products to consumers. The benefits of
a HACCP plan are that it saves the company money in the long run, avoids harming
customers, increases safety, maintains compliance, increases quality standards, organizes
process, promotes teamwork, and provides due diligence. These benefits are provided
through thorough pre-requisite programs, education, training, and ensuring the
organization follows the HACCP plan accordingly. Pre-requisite programs are procedures
that address operation concerns. They are programs and activities needed to ensure the
HACCP program is effective.

25 The building blocks for a HACCP program depend on the design, implementation
and control/management of HACCP systems. In order to conduct a successful HACCP
program, the following must be conducted (United States Food and Drug Administration,
2015):
• A HACCP team must be developed.
• The product and who can be affected must be described.
• A flow diagram must be conducted to determine the flow and describe processes that are to be taken.
• The flow diagram must be verified.
• A hazard analysis must be conducted.
• Critical control points CCPs must be identified.
• Critical limits must be determined.
• Monitoring procedures must be established.
• Corrective actions must be developed.
• Verification procedures are to be developed.
• Record keeping and documentation must be kept.
Shared attitude, shared values, and strong safety culture can determine the
effectiveness of the HACCP program. If there are any flaws in the system, the
organization is at-risk of harming the consumer. The HACCP team must conduct a
hazard analysis to identify threats. Conducting this analysis allows the team to determine
preventative/control measures to eliminate/reduce hazards to safe acceptable levels.
Effective preventive/control measures help avoid hazards and minimize safety and health
risks. Consideration should be given to what control measures should be conducted for

26 each hazard. Hazards can be biological, chemical, or physical. The hazard analysis should
include:
• Likely occurrence of hazard and severity of adverse health effects.
• The qualitative and/or quantitative evaluation of the presence of hazards.
• Survival/multiplication of microorganisms of concern.
• Persistence in toxins, chemicals, or physical agents.
• Limitations of the study.
The HACCP requires the full commitment and involvement of management and
the workforce. In order for the system to be effective, there must be a team approach.
Technical expertise and knowledge of the product or service are essential to develop a
HACCP plan. The HACCP team should include various employees from different
departments to identify potential hazards at different stages of the process. Training must
be specific to operational needs to ensure the understanding of safety, risk assessment,
the hazard analysis, and teamwork.
The DRIFT theory is not going to prevent people from making mistakes, but it
can encourage everyone to continuously work towards improvement. By improving the
attention to detail, the spread of hospital-acquired infection HAI can be controlled,
monitored, and limited. It may be difficult to encourage facilities to fund sufficient
HACCP quality programs because it takes time and resources. However, if conducted
correctly, a HACCP program can save lives and save the facility money by reducing
preventable illnesses. According to Griffin (2006), “taking this type of approach to
manage healthcare associated infections could provide greater transparency, reduce

27 infection rates, and increase consumer confidence” (p. 3). By reducing and eliminating
preventable illnesses, healthcare providers can better care for patients and manage
existing conditions. In the long run, this type of program can cut unnecessary cost and
better serve both patients and healthcare employees.
Definition of Terms
Adenosine Triphosphate (ATP): A measure of residual organic soil. ATP testing is a
process that measures microorganisms through detection of adenosine triphoshphate.
ATP is an organic molecule used to store energy in living things that is found in bacteria,
mold, and yeast. Its presence indicates contamination and can potentially be bio-
hazardous.
Biological Hazards: Also known as biohazards, these are biological substances that pose
a threat to the health of living organisms. Biohazards include medical waste or samples of
microorganisms, viruses or toxins. Exposure to biological hazards can cause skin
irritation, infections, and serve health risk. If biological hazards are not handled properly
they can pose a significant threat the healthcare and communities workers.
Chemical Hazard: Any occupational hazard caused by exposure to chemicals in the
workplace. This type of exposure can have acute and long-term health effects. Chemical
hazards are substances, mixtures, and materials that that can be classified according to
their health and physicochemical risks and dangers. Chemical hazards can include
disinfectants and antiseptics such as detergents, cleaners, and gases. Some drugs that are
administrated to patients can become chemical hazards if not handled properly.

28 Critical Control Point (CCP): A specific point, step, or procedure in the HACCP
program that helps reduce, eliminates, or prevent possible hazards. CCPs ensure
precaution measures are being conducted properly. CCPs are steps in place to prevent the
spread of microorganisms. In the food industry when CCPs are not done correctly can
result in an outbreak of food born illnesses.
Critical Limits: Maximum and/or minimum value, to which a biological, chemical, or
physical parameter must be controlled at the CCP. Each critical control point must have a
critical limit. Critical limits must be monitored and observed to ensure CCPs are within
the HACCP plans guidelines. Critical limits must be scientifically or regulatory based.
Deviation: Failure to meet critical limit. Deviations are occurrences that depart from the
established critical limits. Deviations must be documented, reported, and corrected. If
deviations continue to occur the hazard analysis critical control point HACCP team must
reevaluate their HACCP program.
Hazard Analysis: The process of collection and evaluating information on hazards
associated with the process under consideration. The purpose of the hazard analysis is to
develop a list of hazards that are likely to cause harm if they are not controlled. Once
hazards have been identified the next step is to determine the severity if not controlled.
Hazard Analysis Critical Control Point HACCP: HACCP is a quality assurance program
that demonstrates a systematic prevention approach to prevent biological, chemical, and
physical hazards. HACCP consist of seven principles that were developed by the
National Advisory Committee on microbiological criteria for food. The purpose of the
HACCP program was to prevent and control foodborne illnesses.

29 Hazard: A biological, chemical, or physical agent that is likely to cause illness or injury if
not controlled. If not controlled hazards can cause server health risk. The HACCP team
must identify all potential hazards that can arise and determine the level of risk.
Hospital-acquired Infection HAI: Hospital acquired infections are infections that were not
present prior to admission to the hospital. Hospital acquired infections can be caused by
viral, bacterial, and fungal pathogens. The most common type of HAI are bloodstream
infections.
Methicillin-resistant Staphylococcus Aureus (MRSA): An infection caused by a type of
staph bacteria that is resistant to many of the antibiotics used to treat ordinary staph
infections.
Monitor: A planned sequence of observations. Monitoring is to be done to ensure criteria
for the CCPs is being achieved. Monitoring is to be done regularly and findings are to be
documented. Monitoring should include observation or measurements. If critical limits
are not being met, then actions must be taken to correct the deviation. In the HACCP
program it is important that monitoring be assigned to a specific individual that has been
properly trained.
Physical Hazard: Any type of occupational hazards that involve the environment.
Examples include radiation, heat and cold stress, vibration, and noise hazards. Physical
hazards can cause bodily harm without being touched. Physical hazards can also be
electricity, radiation, pressure, or heights.
Prerequisite Program: Procedures in place to address operational conditions, providing
the foundation for the HACCP system. Prerequisite programs cross all product lines of

30 operations. Prerequisites can include cleaning, pest control, supplier/vendor approval, and
water treatment. Prerequisite programs provide a solid foundation for the HACCP
program.
SSOP: Sanitation standard operating procedure. SSOPs are written procedures that
explain the organizations cleaning program. The program explains sanitary practices and
records used for monitoring. The SSOPs has very specific requirements and procedures.
The SSOP follows regulatory requirements to ensure the facility is following strict
cleaning procedures.
Validation: An element of verification focused on collecting and evaluating scientific and
technical information to determine if the HACCP plan can effectively control the hazard.
Validation ensures the process parameters are being properly controlled. This provides
confidence to consumers.
Verification: Activities, other than monitoring, which determine the validity of the
HACCP plan. Verification ensures the system is operating according to the HACCP plan.
Verification also validates that all hazards have been identified and that the HACCP
program is being implemented properly. Verification allows the facility to make
modifications to the plan is necessary.

31 CHAPTER 2
REVIEW OF THE LITERATURE
Multiple articles and websites were reviewed to research hospital-acquired
infections HAI and the impact they cause in the healthcare industry. These articles
supported the problem statement, providing evidence of the need to intervene with
quality techniques. Many articles and websites were also reviewed to research Philip
Crosby’s doing it right the first time DRIFT theory and the hazard analysis critical
control point HACCP program. The articles reviewed supported the argument of the
benefits of a HACCP program and other quality tools that help control the spread of
infectious disease.
Hospital acquired infections HAI, which are not present at admission, develop
within 48 hours of hospitalization (Hensley & John, 2015). The issue with most infection
control programs is that they target the infection once an outbreak occurs, and cleaning is
generally a control mechanism in response to an outbreak (Dancer, 2009). Research
suggests that areas with hand-touched surfaces often are contaminated by pathogens,
which spread to patients through touch. Many hospitals have disinfection routines in
place as part of their daily routine; however, some infected areas can be missed. Due to
these routinely missed areas, scientists have been researching strategies to improve
previous cleaning methods (Kuehn, 2012).
Methicillin Resistant Staphylococcus MRSA is a strain of staph that is resistant to
beta-lactam antibiotics such as penicillin and cephalosporin, and it is responsible for a

32 wide spectrum of infections (Nour des San, Denis, Gasasira, De Mendonca, Nonhoff, &
Struelens, 2007). This infection can result in pneumonia, surgical site infections, catheter-
related infections, and blood infections.
The MRSA infection accounts for 20%-40% of hospital-acquired pneumonia
(Rubinstein, Kollef, & Nathwani, 2016). Recently, a new strain of MRSA has emerged as
a pulmonary pathogen. The pneumonia is sometimes followed by an influenza-like
illness. This new variant of S aureus that causes pneumonia is community acquired. This
type of MRSA has moved into a healthcare setting, which has made the epidemiologic
differentiation of community acquired CA-MRSA and hospital acquired HA-MRSA
genotypes very difficult. Due to this epidemiologic differentiation, the morbidity and
mortality has dramatically increased (Rubinstein, Kollef, & Nathwani, 2016).
Implementing Quality Assurance
Strict hygiene measures can help reduce the spread of MRSA. According to
Kuehn (2012), regularly bathing patients in the intensive care unit can reduce the spread
of MRSA. All medical staff should be trained and educated on hygiene. It is important
for healthcare staff to practice proper hygiene to avoid spreading or contracting the
infection. It is also important for proper hygiene practices to be in place once MRSA has
been identified. Hand washing is the most effective method for reducing the transmission
of pathogens and hospital acquired infections (Stichler, 2014). One of the number one
sources of HAI, are healthcare workers’ unclean hands.
Implementing quality assurance QA programs in a healthcare setting can help
reduce HAI. In a study conducted in a medical surgical intensive care unit at Royal

33 Melbourne Hospital (Rajah, McBryde, Buising, et al 2010), it was determined that
general quality improvement techniques resulted in a decrease in endemic MRSA. The
study analyzes multiple quality interventions and consumption of antibiotics. Monthly
microbiological data was collected on swab testing and analyzed electronically.
Laboratory identification methods remained the same throughout the study. Monthly
quantities of antibiotics prescribed were reviewed and documented. Infection control
consumables were obtained from purchasing; this included gloves, medicated soap,
gloves, plastic aprons, and disposable gloves. The study analyzed trends based on
statistical data that was collected over the course of the study.
In order to implement a successful QA program, leadership must have a clear
agenda, a clear philosophy of management, and build enduring relationships. This type of
leadership is needed to ensure that corrective actions are not only in place but that
proactive measures are being taken. Crosby (1996) provided supporting evidence of the
importance of individuals taking responsibility for resolving deviations and quality
issues. Management can provide all of the tools, but it is up to every individual to ensure
things are done right. The weakness is that some things don’t get done because there
aren’t clear understandings of what steps are necessary. In healthcare, there are already a
massive amount of standards and requirements. The trouble is that they are not always
understood, communicated, or reinforced (Holpp, 1993). Process improvement requires
an entire quality assurance QA system that sees the hospital as a complex set of
interactions and dependencies.

34 The HACCP program has been beneficial in reducing foodborne illness and
contamination in the food manufacturing industry. This quality program is a systematic
approach for identifying hazard and implement control measures (Mccay & Rosenblatt,
2015). Griffith (2006) discusses similarities in the food manufacturing and healthcare
industry. In the 1980s, the media focused considerably on concerns over food safety,
cleanliness, and management of food operations. Approximately, 15 years later, the
media began to focus on superbugs, healthcare associated infections, and hospital
cleanliness. In both industries, it was evident that safety was a major concern. The
HACCP program provided a risk management approach, allowing the organization to
identify potential risks, hazards, and to develop preventative measures.
The true success of a HACCP program is determined by individual human
behavior. The HACCP program is only successful if all employees follow the process and
procedures in place. This program is proactive and designed to prevent infections from
happening (Griffin, 2006). The HACCP program is designed to eliminate, reduce, and
identify hazards that can harm the consumer. However, this may not always be possible.
Implementation does not mean the absolute elimination of pathogens, but it does mean
preventing and reducing contamination with pathogenic microorganisms to a degree that
very substantially reduces and minimizes the risk of foodborne illness (Hulebak &
Schlosser, 2002).
The HACCP system’s primary goal is to improve food safety practices by setting
public health oriented standards for manufacturing companies to meet. The program is a
QA program that holds the establishment accountable. However, the HACCP program

35 does not dictate new control measures but how to manage their implementation (Griffin,
2006). The knowledge of control measures lies with the staff; however, the change relates
to the implementation of new management skills.
The HACCP program provides assurances and documentation that processes used
in manufacturing meat and poultry products are under control and produce safe,
wholesome, and unadulterated products (Hulebak & Schlosser, 2002). In order for an
establishment to ensure that critical control points CCPs are controlled,
validation/monitoring must be documented and reviewed; records are to be maintained on
a daily basis. When corrective measures are taken, they must be documented and
evaluated. One of the key HACCP stages is verification, and auditing is a major
component/requirement (Griffin, 2006). Verification and auditing allow the establishment
to properly evaluate their day-to-day operations at each step, allowing them to identify
risk and to assure CCPs are meet. In order for CCPs to remain under control, real time
data is required to ensure appropriate corrective measures are being taken.
A key feature of introducing a HACCP-based approach is that greater consistency
is achieved in the product or the process (Dillon & Griffith, 2001). Although additional
documentation is required, these documents can be used to demonstrate due diligence.
Ensuring reasonable steps are taken to protect consumers, the HACCP approach is
designed to analyze and evaluate every step of the organizations process. The potential
outputs from adapting HACCP to infection control include a reduced risk of infection,
improved bed turnover, less wastage, and improved confidence (Griffin, 2006). These
outputs can result in greater quality care for patients and reduce unnecessary healthcare

36 costs. The HACCP-based approach places the patient first. Making the patient first is a
value-based decision that can drive important changes in the way care is delivered
(Holpp, 1993).
Benefits of a HACCP program are that it forces employees to be consistent,
proactive, and precautious. If conducted properly, validation and monitoring guarantees
critical control points CCPs are within compliance. Each CCP has one or more control
measure to assure that the identified hazards are prevented, eliminated, or reduced to
acceptable levels (Food & Drug Administration, 2016). Documentation of findings
allows management to see trends and potential problems that may occur. The system
enforces employees to be proactive by identifying deviations when they occur and
implementing corrective measures. Corrective actions should include the following
elements: (a) determine and correct the cause of non-compliance; (b) determine and
correct the cause of non-compliance; and (c) record the corrective action that has taken
place (Food and Drug Administration, 2016). Validation and verification activities are
carried out to ensure precaution is taken at each step of the process or procedure. The
National Advisory Committee on Microbiological Criteria for Foods defines verification
as the use of methods, procedures, or tests. In addition, the program is monitored to
determine if the HACCP system is in compliance with the plan or whether the plan needs
modification and revalidation (Hulebak, & Schlosser, 2002). This obligates the
establishment to continuously evaluate the quality of its processes and procedures.
Barriers of the HACCP-based approach are attitudes, behavioral change, and cost.
Getting employees to share the values of the HACCP system also can be difficult, for

37 change can be unfavorable for some employees who have trouble adapting. Attitudes and
behavior change can cause resistance to management requirements. Resource costs can
be divided into initial capital costs and ongoing or recurring costs; ultimately, human
barriers may be the greater problem (Griffin, 2006). Fear of potential legal requirements
may also result in resistance. In the food industry, there is now a legal requirement for a
HACCP-based approach, and this is a powerful driving force (Griffin, 2006). Many
retailers now require their suppliers to be HACCP-certified. These types of requirements
can cause resistance from the healthcare industry. Possible human barriers may be
clinical staff resentment, doing things differently, and closed minds to new approaches
(Griffin, 2006). Resource costs for training, time, and equipment may also result in
opposition.
Hazard Analysis
Once the prerequisites are established, the HACCP team can conduct a hazard
analysis. The team is to develop a list of potential risks and identify the significance of
each. The significance is decided by the severity of each risk. The team determines the
risk of injury or illness if not controlled. Hazards that do not result in injury or illness are
not considered any further ; however, an explanation of why must be documented, and
each step in the process must be analyzed. The team must decide which hazards are
safety concerns and which are quality concerns. If this is not done correctly, the HACCP
program is not going to be effective. (The appendix provides an illustration to further
explain stages of hazard analysis.) The analysis allows the team to determine the CCP.

Critical Control Points
38
The critical control points CCP is a point, step, or procedure to which control can
be applied to prevent, eliminate, or reduce hazards to an acceptable level (Hulebak &
Schlosser, 2002). All risks identified during the hazard analysis must be addressed to
ensure safety. The CCPs can be located at any step of the process where a potential
hazard can occur. CCPs must be developed with precaution and documented. Validation
and correction measures must be in place to ensure CCPs are meet and deviations are
identified/corrected. Once the CCPs are determined, control measures must be developed.
These control measures must be documented and regulated to ensure risk is controlled at
an acceptable level.
Critical Limit
A critical limit is established to determine safe and unsafe operating conditions at
the CCPs. The critical limit is the level at which biological, chemical, or physical levels
must be controlled to eliminate hazards. “A critical limit is defined as a criterion that
must be met for each preventive measure associated with a critical control point”
(Hulebak & Schlosser, 2002, p. 6). There must be at least one control measure per CCP to
ensure hazards are identified, prevented, or reduced to an acceptable level, and critical
limits must be scientifically based. “The approach ultimately choose was to set targets for
pathogen reduction based on what was judged achievable with science and technology,
and to require establishments to meet the limits on a consistent basis” (Hulebak &
Schlosser, 2002, p. 4). This allows a way to achieve control and assess the CCPs’
effectiveness. Critical limits are to be developed to support regulatory standards and

39 guidelines, literature, surveys, experimental results, and experts. Supporting evidence
must be provided to support and provide proof the critical limit can control hazards.
Establish Monitoring Procedures
Monitoring procedures are designed to verify, validate, and report the critical
control points. Observation is important for documenting trends. By overseeing
procedures, deviations can be identified, corrected, and eliminated. If deviations continue
to occur, the process and CCPs need to be reevaluated. “Monitoring consists of
observations or measurements taken to assess whether a CCP is under control” (Hulebak
& Schlosser, 2002, p. 6). Monitoring procedures must be effective to ensure process and
procedures are being conducted. Surveillance should be continuous. Employees in charge
of monitoring must be properly trained and have a full understanding of the process.
Employees should be trained in what procedures to take to ensure that control measures
are maintained. When critical limits are not met, they must be reported immediately so
appropriate corrective measures can be taken.
Corrective Actions
Although the HACCP system is designed to identify health hazards, if any step in
the procedure is done incorrectly, deviations may occur. Corrective actions must be in
place to correct potential hazards. Corrective measures should determine and correct the
non-compliance, determine the disposition of the non-compliance, and document the
correction. The corrective measures should already be in place for each critical control
point CCP. The corrective action should be part of the HACCP plan, specifying what is
to be done and who is responsible for correcting the deviation. A record should be created

40 to document deviations and corrective actions; this allows the establishment to identify
trends. By identifying trends, the HACCP team members are able to determine if they
need to reevaluate their process and procedures.
Verification Procedures
Verification procedures are used to determine the validity of the HACCP plan.
These procedures validate that the system is being followed and help to evaluate the
HACCP plan. “One of the key HACCP stages is verification and auditing is a major
component/requirement. Another key feature is that the HACCP is proactive and
designed to prevent infections from happening” (Griffith, 2006, p. 2). Verification
procedures validate that the HACCP plan is scientifically sound; subsequent validation is
to be performed by the HACCP team as well as an unbiased independent authority.
Verification procedures ensure that the HACCP plan is within compliance and that CCPs
are being controlled.
Record Keeping
The records maintained by the HACCP system should include the following
(Food & Drug Administration, 2006):
1. Summary of Hazard Analysis
2. HACCP Plan:
• CCPs
• Hazards of Concern
• Critical Limits
• Monitoring

41 • Corrective Actions
• Verification Procedures
• Schedule
• Record-keeping Procedures
3. Support Documentations
4. Operating Records
An organization’s quality assurance QA program should be well thought out and
must be followed according to the plan. In order for the QA program to be effective, there
must be a culture change (Crosby, 2005). An effective QA program requires management
to set the standard toward continuous improvement. In order to change the culture, it is
important to have a clear understanding of quality, emphasizing absolute quality. The
organization should understand what quality means (Crosby, 2005):
• Conformance is a must.
• There is no such thing as a quality problem.
• There is no such thing as economics of quality; it is always cheaper to do things right the first time.
• Performance standard is zero defects with no exceptions.
• Performance measurement is the cost of quality.
It is important for the organization to understand that quality is free. In healthcare,
quality patient care should be the facility’s number one concern. Putting the patient first
is a value-based decision, which can result in important changes in the way care is
delivered (Holpp, 1993).

42 Philip Crosby’s 14 points demonstrate how the organization can help employees
understand what quality means. These 14 steps to improvement are as follows (Crosby,
2005):
• Step 1: Management commitment.
• Step 2: Quality improvement team.
• Step 3: Quality measurement.
• Step 4: Cost of quality evaluation.
• Step 5: Quality awareness.
• Step 6: Corrective Action.
• Step 7 Establishment of ad hoc committee.
• Step 8: Supervisor training.
• Step 9: Zero defects day.
• Step 10: Goal setting.
• Step 11: Error cause removal.
• Step 12: Recognition.
• Step 13: Quality councils.
• Step 14: Do it over again.
Management Commitment
Management should develop QA policies that the entire organization is expected
to follow. Management must provide understanding and clear communication (Crosby,
1996). Quality management must develop the tools and procedures for individuals to use
in creating and managing situations that can occur. Participating in a QA program should

43 raise awareness of quality and ensure the cooperation of all individuals (Crosby, 2005).
Management must set the standard and require this standard be meet by all employees in
order for the quality program to be effective.
Quality Improvement Team
The quality improvement team should include individuals from each department
(Crosby, 2005). This allows individuals from each department to commit operations to
action. Developing a quality improvement team with individuals from each department
the organization can develop specific, measurable, and valid requirements based on all
levels of the process. This also allows team members to explain their roles. By having a
clear understanding of team members’ roles, clear action plans can be developed (Crosby,
2005).
Quality Measurement
Quality measurement helps determine the status of quality in the organization.
The status of quality should be documented to show where corrective actions are needed
and improvement is possible (Crosby, 2005). In healthcare, quality measurement can help
measure processes, outcomes, patient care, patient satisfaction, and the facility’s
structure. Quality measurement should identify the effectiveness, efficiency, and safety of
the process currently in place. This allows the quality team to identify potential risks and
develop preventive measures to ensure all process and procedures are effective, efficient,
and safe.

Cost of Quality Evaluation
44
The cost of quality evaluation allows the organization to determine how
implementing a process improvement program can result in potential savings. Quality
evaluation determines where corrective actions are required that can result in more profit
for the organization (Crosby, 2005). Quality evaluation activities can be divided into
preventive costs, appraisal costs, and internal failure costs (Duffy, 2013). Preventive
costs are associated with design, implementation, and maintenance of the quality
program. Preventive costs include (Duffy, 2013):
• Product or service requirements.
• Quality planning.
• Quality assurance.
• Training.
Appraisal costs are affiliated with measuring and monitoring activities. Appraisal
cost can include verification, quality audits, and supplier ratings (Duffy, 2013). Internal
failure cost, are defects that occurred when the product or service was provided for the
customer. Internal failure cost can include (Duffy, 2013):
• Waste.
• Failure analysis.
• Correction of errors.
• Performance of unnecessary.
External failures cost are errors discovered by the customer. External failure costs
occur when the product or service does not meet the quality design standards.

Quality Awareness
45
Quality awareness promotes continuous improvement. All staff members should
be aware of quality standards and understand how quality affects the organization’s
product/service. To ensure employees are aware of quality standards the quality objective
must clear and required of all personnel. Quality awareness also allows staff to provide
management with feedback regarding quality concerns. Quality awareness teaches
fundamental principles and concepts. “For process improvement to be part of your
definition of quality, a significant amount of time must be spent at the upper levels
identifying core processes and communicate them to staff” (Holpp, 1993, p. 6). Quality
awareness helps management and employees to understand their roles in quality
improvement.
Corrective Actions
Opportunities for improvement come to light when employees are encouraged to
discuss problems that occur, involving not only defects found during inspection, audit or
self-evaluation, but also less obvious problems (Crosby, 2005). The less obvious
problems are seen by working people during daily operations and require attention. These
problems should be discussed in supervision meetings at each level. Quality planning and
awareness is driven from within the organization. Efforts from each employee and
initiatives of departments, make an effective quality plan (Holpp, 1993). Corrective
actions target critical goals and behaviors in order improve quality and safety of process
in place. Individuals begin to identify problems and correct them immediately (Crosby,
2005).

46
Ad Hoc Committee for Zero Defects
An ad hoc committee should include three to four members of the team to
investigate the zero defect concept. The quality manager must make it clear to the
organization that this is not a motivational program and communicate with all employees
the meaning of zero defects (Crosby, 2005). All staff members must be required to do
things right the first time. Management must create an organizational and culture where
things are done correctly and on time and where relationships with employees, suppliers,
and customers are successful (Crosby, 1996). It is the ad hoc committee that should
develop a system that matches the company’s personality.
Before implementing all of the steps, a formal orientation should be conducted
with all levels of management. The orientation can ensure each manager knows each step
of the process. It is important for management to know every step in the process in order
to explain them to staff (Crosby, 2005). Management involvement in process
improvement, identifying core processes and communicating to the staff, can define the
importance of quality (Holpp, 1993). In order to build awareness of process
improvement, a significant amount of training and practice must be conducted.
Zero Defects Day
The organization must establish zero defects as the performance standard on day
one (Crosby, 2005). This allows all staff members to have the same understanding of zero
defects. Management should explain the program to staff and do something unique so
staff can recognize the shift in attitude. Management must ensure a standard is set and

47 followed. Zero defect means things are to be done right the first time; eliminating waste
in time and using resources for correcting errors. Zero defects, creates a culture where all
transactions are conducted correctly and on time (Crosby, 1996).
Meetings should be conducted to set goals, and these goals should be measurable.
The goals should be specific and range from 30-, 60-, and 90- days. This type of system
develops an organization that accomplishes specific tasks in a timely manner (Crosby,
2005). Setting goals and accomplishing them allows the organization to work toward
continuous improvement.
Individual staff members should be asked, to document any problem that could
prevent them from conducting error free work (Crosby, 2005). One weakness of
organizations is that things never get done or not done properly because staff members
are not sure what is necessary and who is supposed to do what (Holpp, 1996). This
should not be used as a suggestion system, and appropriate personnel staff should
acknowledge each problem within 24 hours. This type of system displays to staff
members within the organization that their problems are heard and answered. Once
employees know their problems can be heard and answered, they start to trust this form
of communication.
Management should establish reward programs for those who set goals and
accomplish them (Crosby, 2005). Recognizing staff members who meet their goals is
important, for it acknowledges their efforts, and this recognition can gain support for the
program. All problems identified during the error cause removal stage should be treated
the same because they are not suggestions.

48 Quality professionals and chairmen should meet regularly to communicate
progress and determine actions when necessary (Crosby, 2005). By conducting regular
meetings, this group can be aware of the status of the program. These meetings allow
staff members to get together on a regular basis to analysis and discuss processes in
place.
Do It Over Again
On average, a program generally takes a year to 18 months to complete. Once the
program has ended, a new team of representatives should be in place. An organization’s
quality program should be well thought out and must be followed according to the plan.
In order for the quality program to be effective, there must be a culture change (Crosby,
2005). An effective quality program requires management to set the standard for
continuous improvement. In order to change the culture, it is important to have a clear
understanding of quality, emphasizing absolute quality. The organization should
understand what quality means as follows (Crosby, 2005):
• Conformance.
• There is no such thing as a quality problem.
• There is no such thing as economics of quality; it is always cheaper to do things right the first time.
• Performance standard is zero defects.
• Performance measurement is the cost of quality.
It is important for the organization to understand that quality is free. In healthcare,
quality patient care should be the facility’s number one concern. Putting the patient first

49 is a value-based decision, which can result in important changes in the way care is
delivered (Holpp, 1993).
Management Commitment
Management should develop quality policies that the entire organization is
expected to follow. Management must provide understanding and clear communication
(Crosby, 1996). Quality management must develop the tools and procedures for
individuals to use in creating and managing situations that can occur. Participating in a
quality program should raise awareness of quality and ensure the cooperation from all
individuals (Crosby, 2005). Management must set the standard and require this standard
be meet by all employees in order for the quality program to be effective.
Quality Improvement T eam
The quality improvement team should include individuals from each department
(Crosby, 2005). This allows individuals from each department to commit operations to
action. Developing a quality improvement team with individuals from each department
the organization can develop specific, measurable, and valid requirements that are based
on all levels of the process. This also allows team members to explain their roles. By
having a clear understanding of team member’s roles, clear action plans can be developed
(Crosby, 2005).
Quality Measurement
Quality measurement helps determine the status of quality within the
organization. The status of quality should be documented to show where corrective
actions are needed and improvement is possible (Crosby, 2005). In healthcare, quality

50 measurement can help measure processes, outcomes, patient care, patient satisfaction,
and the facility’s structure. Quality measurement should identify effectiveness,
efficiency, and safety of the process currently in place. This allows the quality
improvement team to identify potential risks and develop preventive measures to ensure
all process and procedures are effective, efficient, and safe.
Quality Awareness
Quality awareness promotes continuous improvement. All staff members should
be aware of quality standards and understand how quality affects the organization’s
product/service. To ensure employees are aware of quality standards, the quality
objective must clear and required of all personnel. Quality awareness also allows staff to
provide management with feedback regarding quality concerns. Quality awareness
teaches fundamental principles and concepts. “For process improvement to be part of
your definition of quality, a significant amount of time must be spent at the upper levels
identifying core processes and communicate them to staff” (Holpp, 1993, p. 6). Quality
awareness helps management and employees understand their roles in quality
improvement.
Corrective Actions
Opportunities for improvement come to light when employees are encouraged to
discuss problems that occur, involving not only defects found during inspection, audit or
self-evaluation, but less obvious problems as well (Crosby, 2005). The less obvious
problems are seen by working people during daily operations and require attention. These

51 problems should be discussed in supervision meetings at each level. Quality planning and
awareness is driven from within the organization. The efforts of each employee and
initiatives in every department can make an effective quality plan (Holpp, 1993).
Corrective actions target critical goals and behaviors in order to improve the quality and
safety of the process in place. Individuals begin to identify problems and correct them
immediately (Crosby, 2005).
The organization must establish zero defects as the performance standard on day
one (Crosby, 2005). This allows all staff members to have the same understanding of zero
defects. Management should explain the program to staff and do something unique so
staff members can recognize the shift in attitude. Management must ensure a standard is
set and followed. Zero defect means things are to be done right the first time, eliminating
waste in time and resources correcting errors. Zero defects create a culture where all
transactions are conducted correctly and on time (Crosby, 1996).
Individual staff members should be asked to document any problem that prevents
them from conducting error-free work (Crosby, 2005). One weakness of organizations is
that things never get done or not done properly because staff members are not sure of
what is necessary and who is supposed to do what (Holpp, 1996). This should not be used
as a suggestion system. These problems should be acknowledged from the appropriate
personnel staff within 24 hours. This type of system displays to staff that their problems
are heard and answered. Once employees know their problems can be heard and
answered, they are going to trust this form of communication.

52
Quality Councils
Quality professionals and chairmen should meet regularly to communicate
progress and determine action when necessary (Crosby, 2005). By conducting regular
meetings, the council can be aware of the status of the program. These meetings allow
staff members to get together on a regular basis to analyze and discuss processes in place.

53 CHAPTER 3
METHODOLOGY
For the purpose of this study, data was collected on hospital-acquired infections
HAI and methicillin-resistant staphylococcus aureus MRSA to examine risk factors and
current quality assurance QA measures in place. Data was also collected on Crosby’s
doing it right the first time DRIFT theory and the hazard analysis critical control point
HACCP program. This data was evaluated to understand concepts and the history of the
DRIFT theory and HACCP program, which provided a full scope understanding of key
factors, pros, and cons. Based upon the literature reviewed the evaluation, personal
experience, and patient interaction were analyzed to determine barriers. This study took a
qualitative approach, using formal, objective, and systematic processes to develop a
HACCP plan to prevent HAI.
The hypothesis of this study was that implementing a HACCP program with
concepts from Philip Crosby’s DRIFT theory could prevent HAI in healthcare facilities.
A barrier to this study was that it was a proposal. To truly test the hypothesis, this
proposed program would need to be conducted in a healthcare setting and monitored over
time to track improvement rates. This would take time and resources; however,
administering this type of program could be beneficial, both to the hospital and patient
care. This thesis provided a formal written HACCP plan for healthcare facilities to
conduct to prevent HAI.

54 Observations
Low constraint research methods were conducted, using naturalistic observations.
Observations were conducted in a hospital in Orange County California; the name of the
facility was not to be disclosed in this thesis; however, a brief description would be
provided. The hospital observed serves communities throughout the Orange County
California area. The facility is a 400-bed acute care hospital with the following
departments:
• Emergency room
• Intensive care unit
• Neonatal Intensive care unit
• Pediatric intensive care unit
• Pediatric
• Telemetry
• Surgical
• Labor and delivery
• Obstetrics
• Cardiology
• Radiology
• Wound care
• Oncology
Observations were conducted over a period of nine months. The flow of patients
in the hospital was observed. Observations of patients and healthcare staff (clinical and

55 non-clinical) interaction were also observed. Current isolation procedures were
researched and reviewed. This data was applied to the development of the HACCP
program.
During the nine mouths of observation, an infection outbreak occurred in the
facility’s intensive care unit. The outbreak was only disclosed to clinical personnel. The
intensive care unit was shut down, patients were moved, and a deep cleaning of the unit
was conducted. After this outbreak, the quality department conducted a hand washing
demonstration, showing hospital staff how to properly wash their hands after each
interaction with a patient. Based on feedback from hospital staff that had been working
for the hospital over a period of 15 years, this was the first time that this type of hand
washing demonstration had occurred.
Based on these observations, a need for a prevention program that involved all
hospital staff, both clinical and nonclinical, was needed to prevent HAI. A HACCP
program, based on the concept from Crosby’s DRIFT theory, involving the entire
healthcare facility in the prevention of HAI, would be beneficial for acute care hospitals.
This type of prevention program would improve the quality of care provided to patients
and would include all staff in prevention measures.
Discussions
Informal discussions were conducted with hospital staff, both clinical and
nonclinical. Employee names were not disclosed in this study; however, their titles and
direct quotes from the discussions will be used. Various hospital employees were
randomly chosen to conduct brief discussion. These discussions were used to determine

56 the roles of hospital staff and to analyze their roles in preventing HAI. The discussions
were conducted one-on-one individually. Each staff member was asked the same five
survey questions. The following five questions were asked during each discussion:
• What is your title and your role in the hospital?
• On average, how much patient interaction do you have on a daily basis?
• Are you familiar with hospital-acquired infections HAI?
• Do you know the current control measures in place to prevent hospital-acquired infections HAI?
• Do you feel like you have a role in preventing hospital-acquired infection? If so, what do you feel your role is?
The purpose of the discussions was to determine HAI awareness and the role of
various hospital staff in prevention measures. Conducting these discussions provided an
understanding of their job duties, which helped developed a model that accounted for
these roles. This information was used to help develop a HACCP program that accounted
for various patient interactions both clinical and nonclinical. A prevention program that
involved all patient encounters would allow the healthcare facility to provide a higher
quality of service for patients.
Method
The design of this study was a HACCP plan; this was a scientific approach to
preventing potential safety problems. When a HACCP plan was implemented, it placed
control measures in place at each point in a process where safety issues could arise. The
purpose of this study was to design a HACCP plan that could be implemented in
healthcare facilities to prevent HAI. The program was designed, based on the setting and

57 processes in place to help prevent and control HAI. Based on principles from Philip
Crosby’s DRIFT) theory, a HACCP program was developed. The design included:
• Prerequisite program.
• Process description.
• Process flow chart.
• Hazard identifications.
• Critical control point determinations.
This thesis implemented the 12 steps in the HACCP program, which included the
seven principles of HACCP. In order to implement these seven principles, the following
steps were taken:
• Conduct a risk analysis to determine potential risks and preventative measures.
• Determine critical control points critical control point CCP.
• Establish critical measures.
• Establish monitoring procedures.
• Establish corrective actions.
• Establish records and documentation procedures.
• Establish verification procedures.
The flow of a patient in an acute care facility has been observed from admitting to
discharge to determine contact points where HAI can occur. These observations were
used to identify biological, chemical, and physical risks to determine preventive
measures. Current infection control measures, hygiene practices, and the culture of safety
in a healthcare setting were evaluated. Based on these evaluations, a HACCP plan was

58 developed, based on observations, employee interaction and patient contact points: This
model was created, based on concepts from the DRIFT theory, ensuring that protecting
patients from HAI is done right the first time.

59 CHAPTER 4
RESULTS AND DISCUSSION
To ensure that the hazard analysis critical control point HACCP plan’s seven
principles are applied correctly, twelve steps are required. The following is a description
of the 12 steps that are recommended.
Step 1: Establish a T eam
It is valuable for the organization to have a HACCP team made up of
representatives from various departments; this allows the team to identify all potential
hazards at all levels. It is important for a HACCP team in a healthcare setting to include
team members that are both clinical and non-clinical. This is important because it allows
the team to develop a HACCP plan that accounts for all patient interactions. It also allows
team members to have a better understanding of other team members’ roles in the
facility. The team should include:
• A team leader to ensure, concepts are being applied correctly and the group is moving in the right direction.
• A representative from various departments to provide specific insight on patient interaction. Representatives can include: nurses from varies departments, environmental cleaning staff, warehouse staff, epidemiology staff, quality control staff, patient access representative, doctors, surgical technicians, or any other hospital personnel.
• A secretary to document the team’s progress
The HACCP team analyzes the flow of a patient in the hospital and current
hospital-acquired infections HAI control measures and determines the potential risk.

60 The facility can use concepts from the doing it right the first time DRIFT theory by
having the team set a quarterly goal to meet. This goal must be specific, measurable, and
aimed towards improving infection control and awareness. The facility can also change
the team on an 18-month basis, reviewing the HACCP plan currently in place and making
changes where necessary. This can allow the facility to consistently work towards
process improvement. It also can allow new perspectives and feedback to be provided.
Step 2: Describe the Product or service
In order to begin a hazard analysis, a full description of the product or service
must be provided. The service is the prevention of HAI. These are infections contracted
in a hospital setting that were not present at the time of admission known as non-
socomial infections. In order for the infection to be considered a HAI, it must occur
within in 48 hours, up to three days after admission or 30 days after an operation. HAI
can be caused by: bacteria, fungus, or viruses. Common types of HAI are:
• Central line bloodstream infections, which occur when bacteria enters the bloodstream through the central line.
• MRSA infections are resistant to antibiotics and can cause blood stream infections, pneumonia, and surgical site infections.
• Sepsis is caused from bacteria entering the blood stream, typically through the infection of a wound.
All patients can be at risk of contracting HAI; however, patients with the highest
risk are:
• Premature infants
• Young children

61 • Elderly
• Patients with chronic conditions
• The severely ill
Symptoms of HAI:
• Urinary tract infections
• Surgical site infections
• Pneumonia
• Fever
• Headache
• Shortness of breath
• Meningitis
• Gastroenteritis
• Vomiting
Step 3: Identify the Intended Purpose of the Service
The intended goal is to develop a HACCP program to prevent the spread of HAI,
and the purpose of the HAI prevention program is to protect the patient from preventable
illness. By developing a HAI prevention program, the facility is able to provide a better
quality of care for patients and reduce unnecessary healthcare costs. The HACCP plan
uses concepts from Philip Crosby’s DRIFT theory to create a culture change in patient
interaction. This culture change is to set the standard on how patient care is delivered at

62 all levels of patient care. The overall objective of the HACCP program is to prevent,
reduce, and eliminate HAI.
Based on discussions conducted for this study and observations made this type of
quality assurance QA-based program would be beneficial to healthcare facilities. This
type of program would raise awareness to hospital-acquired infections and will account
for, varies roles in the facility. A total of eight hospital employees from various
departments, both clinical and non-clinical, were randomly chosen to conduct a survey.
Out of the eight employees, only three agreed to participate. This caused a barrier
because the purpose of the discussions was to gain an understanding of HAI awareness,
and only a few employees were interested in participating. Responses from the interviews
follow:
Discussion 1:
1) Role in hospital =Sepsis Coordinator
2) 1 to 2 patients per day direct care, review 15 charts per day
3) Very aware of HAI
4) Current measures to prevent HAI:
a) Hand washing/hygiene campaign= Hand Hygiene before and after entering a patient’s room, before and after eating going to restroom and when otherwise soiled
b) ID patient’s with history MRO (multi-drug resistant organisms) prior to bed assignment and isolate and screen until cleared by infection control
c) VAP bundles (oral care q 2 with chlorohexidene mouth wash and suction prn, change suction canister q 24, don’t break inline suction sterile ceil.)

63 d) Foley cath insert training and care=our ER is “Foley free”, d/c Foley
within 24 hours for post op surgical patients, use alternative condom cath or easy-wick female external cath. FV has foley “care bundle” and only nurses that have gone through the BARD training can insert foley’s. CNA’s have been trained to clean once per shift with the “castile soap” per manufacture guidelines and FV policy.
e) Central Line Infection
a. Reduce central line insertions unless medically necessary
b. Weekly and prn dressing change per policy use sterile technique, chloro-prep, bio-patch and clear occlusive dressing, assess site q shift. Use Green “Curo” Caps port protectors.
5) Sepsis early identification of patients in the hospital that develop signs and symptoms of an infection (SIRS/Organ DYSFUNCTION/ Possible Source of Infection) all three criteria met then nurses can enact sepsis bundle protocol to initiate early treatment. Isolation standard: Standard, Contact, Contact – enhanced (for C-diff), Airborne and Droplet
a. Have list of organisms that require isolation in each unit and it includes type of isolation: for example MRSA, (contact) C-diff, (enhanced contact) TB, (Airborne) Influenza, (Droplet)
Discussion 2:
1) Certified Surgical Technologist. My role is to set up/maintain a sterile field and assist the surgeon during surgery.
2) Direct patient care 100% of the time.
3) Yes, I am familiar with hospital-acquired infections
4) Yes. Hand washing/hand sanitizer is key before and after patient contact. Wearing the proper personal protective equipment (PPE) when necessary is critical as well. Environmental services plays an important role when patient rooms and other areas of the hospital need to be properly decontaminated.
5) Yes. Encourage my co-workers to wear PPE and make sure they wash their hands with hand sanitizer before and after patient care. My role is to ensure sterility of the equipment and supplies being used on the patient and to correct and break in sterility. It is also my role to report any unusual occurrences that

64 may have harmed the patient.
Discussion 3:
1) Financial Counselor. My role is to inform and educate patients on their financial liability and responsibility of their in-patient status and outpatient services provided.
2) I would consider having 99% contact with patients. Most of my patient interaction is visiting patients at bedside to discuss financial matters.
3) Yes. I am pretty familiar with hospital-acquired infections.
4) Yes, from previous employer and current. Making sure you always hand wash and use hand sanitizer when coming and walking out a patient's room. Also making sure you wear (gown, mask and gloves) when direct outside a patient's room.
5) Yes, I do. Always be sure to clean your hands walking into a room and specially when walking out of the room. In my position I meet with multiple patients throughout the day and all have a different medical situation. My way of preventing anything spreading is to always hand wash and sanitize.
Step 4: Draw a Flow Diagram of the System
In order to identify the potential risk of a patient contracting HAI, the flow of a
patient in an acute care facility must be analyzed. This allows the facility to identify all
hospital personal interactions patients encounter during their hospital visit. Both clinical
and non-clinical interaction must be identified and included in the infection prevention
program. By identifying all patient and hospital personal interaction, the facility is able to
design a program that involves all hospital personnel. Figure 2 is a flowchart that
provides a break down of a patient in an acute care hospital. Once the HACCP team has
reviewed and evaluated the patients’ condition, they can add this information to the
flowchart, making it more detailed or making necessary changes. The flowchart should

65 constantly be evaluated and adjusted as needed. Once the team has evaluated the
flowchart, the team can add:
• Additional services provided to the patient step-by-step.
• Equipment used.
• Working conditions.
Figure 2. Flow of patient in acute care hospital. Prepared by the author of this thesis.

66
The flowchart in Figure 2 provides an overview of the process of patient care.
Patients come into the facility for a scheduled appointment or for emergency services.
Patients, who have scheduled services, check-in the main entrance of the hospital and
wait in the waiting room to be registered/admitted. Depending on the size of the waiting
room and how many scheduled appointments there are, the waiting room can become
crowded and busy.
Patients are called into the admitting office to be registered by an admitting
representative. During registration, the admitting representative verifies the patients’
identification, demographics information, and insurance information and has patients sign
hospital forms. The registration room is an enclosed cubicle designed to protect personal
patient information. Once the patient has been registered, the patient is taken to the
department for outpatient services. Outpatient services include: outpatient surgery,
cardiology, radiology, catheterization, laboratory, nuclear medicine, labor and delivery,
or observation care.
The patient is taken to the department in a hospital wheel chair unless the patient
requests to walk. Patients, who are being admitted for outpatient surgeries, are taken to
the recovery room once their surgery is done for observation. In order to be discharged,
the patient has to be cleared by the doctor. Patients who are scheduled for same-day
surgeries are generally discharged the same day unless the doctor places an inpatient
order due to a medical concern. For all other outpatient services, the patients are
discharged once services are done.

67 Patients, who come to the facility for emergency services, either walk in or are
transported via ambulance. When the patients come in for emergency services, they are
triaged by a nurse. During triage, the nurse evaluates the patient’s condition in order to
determine the severity of the problem. This allows the nurse to determine the priority of
the patient’s admission into the emergency room and for treatment. Once the patient has
been triaged, he or she is placed in an emergency bed for observation. The patient is then
seen by a physician and diagnosed. Depending on the level of care required, the patient is
either admitted as an inpatient or provided with follow-up instructions and discharged.
Patients transferred from other facilities may also arrive at the hospital for
emergency services via ambulance and are admitted for inpatient services. Once admitted
for inpatient services, the patient can be admitted to the following departments: telemetry,
oncology, intensive care unit ICU, medical acute, surgical, pediatrics, pediatrics intensive
care PICU, or labor and delivery. During the patients’ hospital stay, they experience
various interactions with hospital staff, both clinical and non-clinical. Some patients are
transferred to various departments within the hospital during their hospital stay.
Environmental services are constantly cleaning the hospital throughout the day. Patient
and operating rooms are to be cleaned before and after patient arrivals. Equipment should
also be cleaned and sanitized regularly throughout the day.
Step 5: On Site Confirmation of Flow Diagram
Once the flow diagram is complete, members of the team must conduct a walk
through of the facility to compare the information. This provides a step-by-step practice

68 to ensure that all steps and information on the flowchart are accurate. The flow chart
should also include:
• Shipment and inventory.
• Environmental cleaning process and procedures.
• Surgical technicians’ process for sterilizing equipment and operating room.
It is important to include shipment and inventory in order for the HACCP team to
identify vendors and supply chain management. This allows the team to identify products
that are being used to ensure cleaning and sterilized products that are within
specifications. This also allows the team to ensure that sterilizers are being used within
their shelf life. By including shipment and inventory, the HACCP team is able to monitor
if inventory is being stored properly and being used accordingly.
The environmental cleaning department plays an important role in infection
control. By including the environmental cleaning process, the team is able to analyze:
• The process for cleaning blood, bodily fluids, vomit, urine, and feces. This allows the team to know how to verify if patient rooms are properly clean, what cleaning solution is used. How often are cleaning supplies replaced.
• Process for cleaning and decontaminating patients rooms, bathrooms, and waiting rooms.
• The cleaning levels of different areas of the facility what are considered low-risk, high-risk, and very high-risk areas.
• Decontamination of environment and equipment such as airways, ventilator tubes, ceilings, bed frames, mattresses, pillows, cradles, baby baths, blood pressure cuffs, incubators, dressing trolleys, blood/bodily fluid containers, medical equipment, procedure tables, floors, and walls.
Once the team members have analyzed these processes, they can implement them
in the flow chart. This also allows the team to develop verification procedures to ensure

69 these procedures are done properly. The effectiveness of cleaning plays a significant role
in pathogen control. Verification procedures provide monitor techniques to evaluate the
effectiveness of the cleaning procedures in place. Hospitals rely on visual inspections of
surfaces, only using verification microbiological testing in outbreak investigations
(Griffith, 2006). This type of system is flawed because it addresses the issue once an
outbreak has already occurred. The HACCP team can conduct quarterly microbiological
swab testing of the hospital to continuously monitor the effectiveness of cleaning
procedures in place.
Surgical technicians play a significant role in the operating room. They prepare
the operating rooms by setting up sterile surgical equipment, supplies, gloves, gowns,
drapes, and suction tubing. The surgical technologists check to ensure the equipment is
sterile and working properly. The technician also assists with transporting patients to the
operating room, assists with positioning the patient on the operating table, and prepares
the patient for surgery by shaving and disinfecting incision sites. The HACCP team
should analyze each step taken to sterilize the operating room and prepare the patient for
surgery. This allows the team to determine if verification procedures are needed to verify
and validation procedures in place.
Step 6: Identify and Analyze Hazards (Principle 1)
In order for the HACCP plan to be successful, hazard identification and analysis
must be effective. Hazards can be classified into one of three types: biological, chemical,
and physical. The probability that a hazard can occur determines the risk. After hazards

70 have been identified, a risk analysis must be conducted to identify relative health risks.
The risk can be assessed as low, medium, or high. Table 2 provides a hazard assessment
that can be conducted to identify potential risks. This hazard assessment assists the
HACCP team with identifying risks and assessing the severity of each risk. The
assessment also documents the task, potential non-targets, risk assessment, and
justification and justifies and determines critical control points. Potential hazards in a
hospital can include:
• Blood
• Bodily fluids
• Vomit
• Feces
• Food
• Fungus
• Mold
• Contaminated water
• Cleanliness of healthcare workers’ hands

71 Table 2
Hazard Assessment
1
Tasks
(FromStep 2)
2
Potential Non-targets
(From Step 3)
3
Risk Assessment
Are any non-targets
significant?
Yes or No
4
Justification
Justify your answer in Column 3
5
Control
What control measures can be
applied during this task to reduce the
risk of non-targets?
6
CCP?
Is this task a CCP?
Yes or No
7
Justification
Justify your answer in Column 6
Title: DietaryServices
Title: Condition of the building
Title: Direct patient contact
Food Yes If food provided to patients is not stored,prepared, orhandled properly could cause illness to the patient.
Monitor temperatures ofrefrigerators andcooking. Use first in first out method. Food should be properly cooked.Patient allergyform to be followed. Propercleaning of dishes, refrigerators,kitchens, and healthcare workers hands.
Yes HAI can come from food handlers if food is not handled properly andproper hygieneproceduresfollowed.
Fungus, mold and contaminated drinking water
Yes The condition of the building is significant because if these non-targets arepresent thepatients and employees health can be at risk
Quarterly microswab testing can be conducted and results documented
No Will be monitored throughquarterly swab testing
Healthcare workers hands
Yes Healthcare workers have direct contact with patientsthroughout theday
Healthcare workers are to wash their hands with antibacterial soapbefore and after patient contact
Yes ATP swab testing onhealthcare workers hands done weekly and temperature ofwater taken once a week. If not controlled properlyMRSA and other HAI can spread

72 Table 2 Continued
1 2 3 4 5 6 7
Tasks Potential Non-targets
Risk Assessment
Justification
Justify your
Control
What control
CCP?
Is this
Justification
Justify your (From (From Step 3) Are any non- answer in measures can be task a answer in Step 2) targets
significant?
Yes or No
Column 3 applied during this task to reduce the risk of non-targets?
CCP?
Yes or No
Column 6
Title: Patients rooms Room to be Yes Sanitizer to be Patients Patients Room Yes become properly clean and tested and room contaminated
everyday sanitized prior toadmission, atdischarge andduring patient stay as needed
document. Cleaning to bedocumented. Quarterlyswabs of rooms and equipment.If not done properly HAIcan be spread
Note. Developed by the author of this thesis.
Table 2 is broken into 7 sections.
• Section 1 is the tasks that will be conducted/the area of focus.
• Section 2 describes potential non-targets; identifying potential areas that can
result is risk.
• Section 3 is an assessment of significant risk based on finding from section 2.
• Section 4 justifies the risk assessment.
• Section 5 identifies control measures for potential risk.
• Section 6 determines if the task requires a critical control point CCP
• Section 7 justifies why the task does/or doesn’t require a CCP

73 Step 7: Determine Critical
Control Points (Principle 2)
The HACCP team develops the critical control points CCPs based on results from
the hazard analysis. Determining the CCPs requires the HACCP team to evaluate
processes and procedures from the flowchart and hazard analysis. The CCPs should deal
specifically with safety issues. The CCPs must be realistic and have appropriate critical
limits. If hazards are identified in the hazard analysis, control measures must be
implemented in the system to prevent occurrences. There are some hazards that can be
controlled by prerequisite programs. Prerequisite programs provide basic environmental
and operating conditions required to provide a safe product or service. The HACCP team
needs to develop a prerequisite program that is specific to policies and procedures in their
system. An example of a perquisite program can be found in the Appendix.
A prerequisite program to prevent hospital-acquired infections HAI should
include the sanitation standard operating procedures SSOPs. These SSOPs are written
procedures that explain the organization’s cleaning program and are to be documented
and monitored. The program should explain procedures in place that explain how the
facility maintains a clean working condition. Specific requirements should explain step-
by-step procedures. The SSOPs for the HAI prevention program can include cleaning and
sanitizing patient contact surfaces. These SSOPs also should provide the scope, purpose,
and required procedures to validate and verify that the SSOP program is effective.
The HACCP team has to determine CCPs, based on the hazard analysis
conducted. The CCPs for HAI can include:
• Dietary services.

74 • Patients rooms and surgery areas.
• Employees’ hands.
Step 8: Establish Critical limits (Principle 3)
For each critical control point CCP, critical limits must be established. The critical
limit is the acceptable level to which a biological, chemical, or physical parameter must
be met by a CCP in order to prevent, eliminate, or reduce occurrence. The critical limit
establishes what is safe and unsafe. All CCPs must have least, one control measure in
order to ensure hazards are prevented.
Due to weak immune systems, age, illness, and impaired immune responses, it is
important for the hospital to ensure that the microbiological safety of food is maintained.
The dietary service department is responsible for feeding patients throughout their
hospital stay. Food service workers go from room to room, providing breakfast, lunch,
and dinner to patients. Meals are given to patients on a portable food cart. Food served to
patients should be properly stored, cooked, and handled in order to avoid contamination
and illness. Control measures can include:
• Refrigerator temperatures must be monitored, and temperatures should bedocumented to ensure food is being stored at acceptable, safe levels.
• Food handlers must wash their hands and wear gloves when preparing andserving food.
• First in first out should be used to avoid spoilage and waste.
• Thermometers should be calibrated daily to check the temperature of food and refrigerators.
• An allergy list is to be followed for each patient to ensure patient safety.

75 Refrigerator temperature should be below 40 degrees Fahrenheit (F), and the
freezer should be 0 degrees Celsius (C). Food service workers should monitor and
document temperatures and expiration dates. They should also ensure that dishes, food
storage carts, and the kitchen are cleaned properly. Refrigerators and freezers should be
checked and documented every three hours. The kitchen should be cleaned before
preparing breakfast lunch, and dinner. Deep cleaning should be done at the end of every
day. To ensure that proper cleaning and temperature needs are addresses, a monthly audit
should be conducted.
Patient rooms and operating rooms can be highly contaminated areas if not
properly cleaned and maintained. As a control measure, patient and operating rooms
should be cleaned before admission, after patient discharge, and as needed during a
patient’s stay. Rooms should be cleaned with soap, water, and bleach and disinfected
with a sanitizer before admission and after discharge. The sanitizer should be tested with
a kit before use and prepared exactly as instructed on the label. If the sanitizer’s level is
below standard, it should be re-mixed, and the acceptable area should be sanitized and
documented. Environmental cleaning staff should ensure containers and cleaning
equipment are not contaminated.
Hospital employees have interaction with multiple patients with various illnesses
throughout their day; due to this, it is vital to ensure proper hand washing hygiene is
maintained. All staff should be trained on proper hand washing hygiene. The facility
should ensure that sanitizers and hand wash areas are available for healthcare personnel.
Hands should be washed or sanitized before and after every interaction with a patient. As

76 a control measure, the HACCP team can randomly conduct adenosine triphosphate ATP
testing on hands once a week in various departments throughout the hospital. The
acceptable level for the ATP testing should be <500 Relative Light Units RLU and
unacceptable >500 RLU. If the ATP test is not within range, the employees must re-
wash their hands, and the test must be re-done. The deviation should be documented and
re-done during that week. By testing employees’ hand hygiene, it develops a culture
where hand washing is the standard not the exception, ensuring hands are washed
properly the first time.
Step 9: Establish Monitoring Procedures (Principle 4)
Monitoring must be conducted to ensure CCPs are being conducted properly. The
HACCP team can develop and conduct daily, weekly, and monthly audits to ensure CCPs
are being meet and maintained. The team must also develop documents that are
completed daily to document date, time, signature, and findings for daily procedures.
Monitoring can be conducted by observation or measurement; however, all findings must
be documented.
Step 10: Establish Corrective Actions (Principle 5)
If CCPs are not being meet, corrective actions must be completed. If CCPs are out
of control, corrective measures must be taken immediately. Corrective actions must
ensure that CCPs are brought under control. Training must be provided to personnel on

77 identifying potential hazards and implementing corrective actions when necessary.
Corrective actions should include how to:
• Determine and correct the deviation.
• Determine deposition.
• Record the corrective action taken.
Each CCP should have specific corrective actions that are to be included in the
HACCP plan. The HACCP plan should develop a specific process for what to do when
non-complaints occur, who is responsible for implementing corrective actions, and what
records are to be documented and maintained.
Step 11: Verify the HACCP Plan (Principles 6)
Once the team has developed the HACCP plan and CCPs have been verified, the
complete plan must then be verified. This verification also allows the team to ensure the
HACCP plan identifies all hazards and properly implements preventive measures.
Verification should include:
• Scientific studies.
• Expert advice.
• Observations, measurements, and evaluations.
The HACCP plan should regularly be validated and documented. External and
internal audits should be conducted to ensure the HACCP program is working properly.
The system can be verified by: (1) observing CCPs, (2) collecting samples for analysis,
and (3) questioning staff.

78 Step 12: Keep Records (Principle 7)
An essential part of the HACCP system is record keeping. Keeping records
ensures the HACCP plan procedures are being followed properly. Record keeping
provides a record of compliance. Records should include:
• A summary of hazard analysis.
• The HACCP plan.
• CCPs.
• Hazard analysis.
• Monitoring procedures.
• Audits.
• Corrective actions.
• Verification procedures.
The challenge with implementing a HACCP plan that follows the DRIFT theory
in healthcare is changing behaviors. It can be difficult to get an entire organization on
board with instituting new changes and breaking old habits. No matter how much
training and quality tools are provided, if employees do not follow the program, the
HACCP program is not going to be successful. The first goal must be to change
behavior.
Another obstacle that can cause resistance when implementing a HACCP plan is
potentially requiring that an external audit be conducted to ensure the facility is in
compliance. In the food/beverage manufacturing industry, external audits must be
conducted on products regulated by the United States Department of Agriculture USDA

79 and the Food and Drug Administration FDA to ensure that companies are following
their HACCP programs and are in compliance. Audits are conducted to validate that
food safety standards are being meet and to evaluate the system to ensure the
establishment is meeting regulatory requirements.
First and second party audits allow the establishment to identify and correct issues
before the external audit. Correcting non-conformances gives the establishment the
opportunity to work toward continuous improvement. In order for these types of audits to
be beneficial to the facility, the organization must be committed to conducting an
unbiased audit. This can result in possible resistance from healthcare facilities
implementing a HACCP program.
Once the third party audit is completed, the establishment is notified of non-
conformities. Any non-conformances found during the audit must be corrected before
certification can be rewarded. The audits are conducted on a yearly basis, and without
this certification, the company is at risk of losing business. HACCP certification
demonstrates to customers that the establishment has provided a safe product for their
customers. In addition, HACCP certification means the establishment maintains an
effective HACCP program. This ensures that the facilities program is built around the
seven HACCP principles:
• Conduct Hazard Analysis of biological, chemical, or physical food hazards.
• Determine critical control CCPs.
• Establish critical control limits (or example: minimum cooking temperature and time).
• Establish a system to monitor control of CCPs.

80 • Establish corrective actions.
• Establish procedure for verification to confirm that the HACCP system is working effectively.
• Establish documentation and record keeping.
The benefit of conducting a HACCP program that follows the DRIFT theory in
healthcare is reducing the spread of HAI. By reducing HAI, hospitals can reduce
unnecessary costs. Reducing these cost, can provide healthcare facilities with more
resources to put towards the facility’s budget. A HACCP program can also improve the
quality of care provided. By eliminating and reducing the spread of HAI, the facility can
provide quality care focusing on the patients’ initial illness and reduce preventable
deaths. Improving quality care can allow for greater patient experience.
To encourage a change in behavior, the facility can provide incentives for meeting
requirements. When requirements are not met, non-conformances should be documented,
and educational training should be conducted. Documentation and education can help
make employees accountable, set a standard, and encourage a shift in behavior.

81 CHAPTER 5
CONCLUSION, RECOMMENDATIONS, SUMMARY
Although the food industry and healthcare industry are completely different, they
both serve the same purpose; that is to provide a product or service that does not harm the
public. The hazard analysis critical control point HACCP program has been a beneficial
and essential tool in the food manufacturing industry for reducing contamination and
food-borne illness. The HACCP system can be a useful system to implement in the
healthcare industry to control and/or prevent hospital-acquired infections HAI. To
provide the intended purpose, modifications must be made to the HACCP program;
however, the same principles must be applied. Exposure to HAI places both patients and
healthcare workers at risk; therefore, it is essential that management can take control and
change behaviors.
Applying Crosby’s DRIFT theory can enforce processes aimed toward
conformances and encourage shifts in behavior and expectations. The DRIFT theory does
not eliminate errors, but it can set the standard towards zero defects. Monitoring tools
need to be in place and maintained. Management must provide feedback and correct
errors as soon as they occur. Doing it right the first time can save time, resources, and, in
the case of healthcare, lives.
Further research must be conducted on current HAI prevention programs to
implement a HACCP program. However, with the right team and the right effort, this
could be a great start for a HACCP plan aimed towards preventing HAI. The program

82 would have to be specific to the facility’s process and would take time to develop.
Getting each department involved would provide for a full analysis of patient care.
Preventing hospital-acquired infections HAI would allow healthcare facilities to provide
a higher quality of care and to reduce unnecessary healthcare costs.

REFERENCES

84 REFERENCES
Ananda-Rajah, M. R., McBryde, E. S., Buising, K. L., Redl, L., MacIsaac, C., Cade, J. F.,
& Marshall, C. (2010). The role of general quality improvement measures in
decreasing the burden of endemic MRSA in a medical–surgical intensive care
unit. Intensive care medicine, 36(11), 1890-1898.
BSA Publishers Clearing House. (2010). Methicillin-resistant staphylococcus aureus
(MRSA): Etiology, at risk populations and treatment.
Center of Disease Control (CDC). (2016). General Information about MRSA in the
Community. Retrieved from https://www.cdc.gov/mrsa/community/index.html
Center of Disease Control (CDC). (2016). HAI Data and Statistics. Retrieved from
https://www.cdc.gov/hai/surveillance/index.html
Center of Disease Control Prevention (CDCP). (2012). Healthcare associations
infections (HAI). AT, GA: Author
Crosby, P (1979). Quality is Free. NY, NY: McGraw Hill.
Crosby, P. (1995). Philip Crosby's Reflections on Quality. NY, NY: McGraw-Hill. ISBN
0-07-014525-3.
Crosby, P. B. (1979). Quality is free: The art of making quality certain. New York:
McGraw-Hill.
Crosby, P. (1996). The leadership and quality nexus. The Journal for Quality and
Participation, 19(3). Retrieved from
http://0search.proquest.comtorofind.csudh.edu

85 Crosby, P. (1999). Quality and me: Lessons from an evolving life. Hoboken, NJ: Jossey-
Bass. ISBN 0-7879-4702-4.
Crosby, P. B. (2005). Crosby's 14 steps to improvement. Quality progress, 38(12), 60-64.
Dancer, S. (2009). The Role of Environmental Cleaning in the Control of Hospital
Acquired Infections. Journal of Hospital Infections Volume 73, Issue 4
Duffy, G. (2013). Cost of Quality. The ASQ Quality Improvement Pocket Guide: Basic
History, Concepts, Tools, and Relationships. ASQ Quality Press, P.62-65
Diseases and conditions MRSA infection. (2015). Retrieved from
http://www.mayoclinic.org/disease-conditions.
Good Hygiene is Key to Preventing MRSA. (2007) US. Newswire, n/a
Griffith, C. (2006). HACCP and management of healthcare associated infections.
International Journal of Health Care Quality Assurance,19(4), 351-367.
Holpp, L. (1993). Eight Definitions of Quality in Healthcare. The Journal for Quality and
Participation, 16(3). Retrieved from http://0-search.proquet.com
Klevens, R. M., Edwards, J. R., Richards, C. L., JR., Horan, T. C, Gaynes, R. P., Polluck,
D. A., & Cardio, D. M. (2002). Estimating healthcare associated infections &
death in US hospitals. Public Health Report, 122,160-166.
Kuehn, B. (2012). Scientists Probe Strategies to Curb Hospital-Acquired Infections.
JAMA. 2012;308(20):2069–2070. doi:10.1001/jama.2012.50841
Kurley, B. (2014). ATP Testing: An Anecdotal Look at its use in an Office Based Plastic
Surgery Setting. Plastic Surgical Nursing, 34 (4),167-170

86 Krein, S. L., Kowalski, C. P., Hofer, T. P., & Saint, S. (2012). Preventing Hospital-
Acquired Infections: A National Survey of Practices Reported by U.S. Hospitals
in 2005 and 2009. Journal of General Internal Medicine, 27(7), 773–779.
http://doi.org/10.1007/s11606-011-1935-y
Hensley, B., Monson, J. (2015). Hospital Acquired Infections. Surgery - Oxford
International Edition , Volume 33 , Issue 11 , 528 – 533
Hulebak, K., Schlosser, W. (2002). Hazard Analysis and Critical Control Point (HACCP)
History and Conceptional Overview. Risk Analysis, 22 (3), 547-552
McCoy, W., & Rosenblatt, A. (2015). HACCP-based programs for preventing disease
and injury from premise plumbing: A building consensus. Pathogens, 4(3), 5/3-
528.
Newswire (2007). APIC Releases Prevalence study of MRSA in Healthcare Facilities.
Healthcare Purchasing News. ABI/inform Collection pg. 9
Office of Disease Prevention and Health Promotion (2017). Healthcare Associated
Infections. Retrieved from https://health.gov/hcq/prevent-hai.asp
Rau J. (2015). 758 Hospitals Penalized For Patient Safety in 2016: Data Table. Retrieved
from http://khn.org/news/758-hospitals-penalized-for-patient-safety-in-2016-data-
table/
Rubinstein, E., Kollef, M. H., & Nathwani, D. (2016). Pneumonia caused by Methicillin-
Resistant Staphylococcus Aureus. Retrieved from
http://cid.oxfordjournals.org/content/46/Supplement_5/S378.full

87 Sassmannshausen, R., Deurenberg, R., Kock, R., Hendrix, R. Jurke, A. et al (2016).
MRSA Prevalence and Associated Risk Factors Among Healthcare Workers in
Non-outbreak Situations. The dutch-german eurefio.frontiers in microbiology
Sreeramoju, P. (2012). Preventing healthcare associated infection: Beyond best practice.
AM J Med Sci.
Stichler, F. (2014). Facility design and Healthcare acquired infections: State of the
science. JONA: The Journal of Nursing Administration, 44(3), 129-132.
United States Food and Drug Administratin (2014). HACCP Principles and Application
Guidelines. Retrieved from
https://www.fda.gov/Food/GuidanceRegulation/HACCP/ucm2006801.htm
Vaidya, A (2013). Ten Best Strategies for Infection Prevention and Control. Retrieved
from https://www.beckershospitalreview.com/quality/10-best-strategies-for-
infection-prevention-and-control.html
Wassenberg, M., Wit, G., Hout, B., Bonten, M. (2010). Qualifying Cost-Effectiveness of
Controlling Nosocomial Spread of Antibiotic-Resistant Bacteria: The Case of
MRSA. PLos One 5(7): e11562

APPENDIX

89 APPENDIX
Six Elements in the Cycle of Infection
Element in the cycle of infection
Explanation Common examples
1. Infectious Agent When germs enter the body, they can cause illness
• Bacteria, virus, fungi, protozoa
2. Reservoir Where germs normally live and multiply
• Humans
• Contaminated food, water, toys, sports equipment
• Insects, animals, soil
3. Portal of Exit How germs leave the body
• Respiratory tract
• Intestinal tract
• Urinary/genitourinary tract
• Open wounds
• Blood and body fluids
4. Transmission How germs are spread *
• Direct physical contact
• Respiratory droplet
• Stool (fecal-oral route)
• Contact with blood/body fluids
• Indirect contact
• Needle stick injury
• Ingestion of contaminated food and water
• Contaminated dust particles
• Contaminated objects
• Insects/animals
5. Portal of Entry How germs enter the body
• Respiratory tract
• Intestinal tract
• Urinary/genitourinary tract
• Open wounds
• Mucus membrane, e.g. eye, mouth

90 Table continued
6. Susceptible Host A person who gets an infection because he/she is unable to successfully fight the infection
• Infants, elderly and debilitated.
• Persons who are ill.
• Children who are not fully immunized or have underdeveloped immune systems.
• Persons taking certain drugs that lower their defenses against germs.
• Persons with underlying disease conditions that lower their defense against
other germs.
HACCP Team:
• Epidemiology Director
• Nursing Staff
• Doctors
• Admitting Department
• Environmental Cleaning department
HACCP Based SOPs
Cleaning and Sanitizing Patient Contact Surfaces
Purpose: to prevent spread of hospital acquired infections HAI by ensuring patient
contact surfaces are properly cleaned and sanitized.
Scope: This procedure applies to the environmental cleaning department.
Keywords: Patient contact surfaces, sanitizing, and cleaning
Instructions:
• Train environmental cleaning department.

91 • Follow directions when using chemicals and sanitizer for patient contact
surfaces.
• Wash, rinse, and sanitize all patient contact surfaces before use and/or anytime contamination occur.
• Wash surfaces and equipment with detergent solution, rinse surface with clean water, sanitize surfaces.
• Sanitizer to be mixed at a concentration specified my manufacturing label.
• Allow area to air dry.
Monitoring:
• Sanitizer to be tested with appropriate kit.
• Visual and physical inspection to be conducted.
• Visual and physical inspections by all healthcare employees whenever
contamination occurs.
Corrective Action:
• If appropriate sanitizer level is not achieved, sanitizer to be mixed and
retested.
Verification and Record Keeping:
• Environmental cleaning staff will record and monitor activities.
• Environmental cleaning staff will record any corrective actions.
• Environmental cleaning manager will verify records are completed and correction measures are being conducted.
• Cleaning log must be completed daily with reviewing, initialing, and dating.
• Log to be kept on file for one year.
• Environmental manager to complete a cleaning checklist daily.

92
Personal Hygiene
Purpose: To prevent contamination by healthcare employees
Scope: This procedures applies to all healthcare employees and volunteers
Keywords: Personal hygiene, contamination
Instructions:
• Train all healthcare staff and volunteers.
• Report to work in good health and clean.
• Change clothing if soiled.
• Wash hands properly, frequently, and before and after patient contact.
• Keep nails clean.
• Wear single-use gloves when needed.
• Treat and bandage wounds immediately.
• When wounds are present single use gloves are to be warn.
• Lesions with pus are to be covered with clean bandage.
Monitoring and verification procedures will further be discussed in the HACCP plan.

93 HACCP Plan: Step 1 – Activity Description
Management Objective & Contact Information
HACCP Plan Title: Control and Prevention of HAI
Management Objective: To control, monitor, and prevent the spread of HAI in hospitals and long-term care facilities.
Contact Person: Epidemiology Director
Phone:
Email:
Activity Description: The purpose of the HACCP program is to protect patients and staff form contracting HAI by implementing monitor and control measures. All healthcare staff will be properly educated on the bacteria, risk, and precaution measures to be taken.

94
HACCP Step 2: Activity Flow Chart Outline Sequential Tasks of Activity
Task 1
Title: Before patient arrival
Description: Patients room to be cleaned properly and sanitized by environmental cleaning staff.
Task 2
Title: Admitting
Description: Patient admitted into the facility. Admitting representative has direct patient contact to collect patient information and have consent forms signed.
Task 3
Title: Patient admitted to room
Description: Patient transported to room by volunteer, hospital staff, or EMT worker. If patient is in an isolation room signs to be posted and mask, gloves, and gowns must be within reach before entering patients room.
Task 4 Title: Inpatient Services provided/Surgery
Description: Patient receives services direct contact with nurses, doctors, and hospital staff.
Task 5 Title: Outpatient Services/Surgery provided
Description: Patient receives services direct contact with nurses, doctors, and hospital staff.
Task 6 Title: Discharge
Description: Patient discharged from facilities.

95
HACCP Step 3 – Identify Potential Non-Targets
Non-Targets That May Potentially Be Moved/Introduced
Visitors: Visitors entering in and out of the hospital could potential introduce new bacteria/virus. Visitors could be at risk of contracted HAI.
Vendors: Vendors entering in and out of the hospital could introduce new bacterial/virus. Vendors could be at risk of contracting HAI.
Food: Food if not properly stored, prepared, or handled properly can cause illness. Can cause stomach aches, diarrhea, vomiting, or fever. In severe cases can cause kidney failure, blood infection, or paralysis. Babies, elderly, and people with weak immune systems are at a greater risk.
Other Organisms (pathogens, parasites, etc.): Fungus and mold in building. Contaminated drinking water.

96
HACCP Step 3 – Identify Potential Non-Targets
Non-Targets That May Potentially Be Moved/Introduced
Hospital Employees hands: Employees have direct contact with patients throughout the day.
Patients Room: Patients room can be contaminated by • Illness • feces • vomit • soil • blood

97
1
Tasks
(From Step2)
2
Potential Non-
targets
(From Step3)
3
Risk Assessment
Are any non-targets
significant?
Yes or No
4
Justification
Justify your answer in Column 3
5
Control
What control measures can be
applied during thistask to reduce the
risk of non-targets?
6
CCP?
Is this task a CCP?
Yes or No
7
Justification
Justify your answer in Column 6
Title: DietaryServices
Title: Condition of the building
Title: Direct patient contact
Food Yes If food provided to patients is not stored,prepared, orhandled properly could cause illness to the patient.
Monitor temperaturesof refrigerators and cooking. Use first in first out method. Food should be properly cooked. Patient allergy formto be followed.
Yes HAI can come from food handlers if food not handled properly
Fungus, mold and contaminat ed drinking water
Yes The condition of the building is significantbecause if these non-targets arepresent thepatients and employees health can be at risk
Quarterly microswab testing can beconducted and results documented
No Will be monitored throughquarterlyswab testing
Healthcare workers
Yes Healthcare workers have direct contact
Healthcare workers are to wash their hands with
Yes ATP swab testingon healthcare workers hands done weekly and
hands with patients throughout the day
antibacterial soapbefore and after patient contact
temperature ofwater taken once a week. If not controlled properly MRSAand other HAI can spread

98 Table Continued
1 2 3 4 5 6 7
Tasks
(From Step 2)
Potential Non-targets
(From Step3)
Risk Assessment
Are any non-targetssignificant?
Yes or No
Justification
Justify your answer in Column 3
Control
What control measures can be applied during thistask to reduce the risk of non-targets?
CCP?
Is this task a CCP?
Yes or No
Justification
Justify your answer in Column 6
Title: Patients Room to be properly Yes Sanitizer to Patients Patients Yes rooms clean and sanitized be tested and room Room become
contaminated everyday
prior to admission, atdischarge and duringpatient stay asneeded
document. Cleaning to be documented. Quarterlyswabs of rooms and equipment. If not done properly HAIcan be spread

99
HACCP Step 5 – Non-Target Risk Action Plan (NTRAP)
(Use this form for a ny "Yes" from Column 6 of HACCP Step 4 - Non-Target Analysis Worksheet) One page for each Critical Control Point
Mangement Objective To ensure food prepared for patient to handled properly to avoid risk to the patient
Critical Control Title: Dietary Services
Point: Significant Non-Target(s) Food served to patients must be properly stored, cooked, and handled to avoid contaminiation and illness. Control Measure(s) Refrigerators temperatures to be monitored and documented. Food handlers must wash their hands and
wear gloves when preparing and serving food. First in first out should be used to avoid spoilage. Thermometers should be calibrated daily to check the temp of food and refirgerators. Allergy list to be follwed for each patient to ensure patient safety.
Precribed ranges, limits, or Refirigerator temperature should be below 40 degrees F citeria for control measure(s): and the freezer be 0 degrees F Monitoring the Who? Control Dietary staff Measure(s) Monitor tempatures and expireation dates. Ensure dishes
How? and kitchen are cleaned properly. Dietary Kitchen Where? Refrigerators/freezer checked and documented every there hours. Kitchen to be cleaned before preparing breakfast,
How often? lunch, and dinner. Deep cleaning at the end of every day. Findings to be document with finding, time, and signature
Corrective Action(s) If refrigrator/freezor temperature not withing range if Control Measures Fail temperature to be adjusted and check every hour until ( within compliance.
Supporting Documents (For example, Management Plan, Checklist, Decontamination Techniques, SOPs, Scientific Journal Articles, etc.) SOP cleaning log, temperature log, first in first out log, temperature calibration log, patient allery log, Audit conducted once a month Development Team Members Dietary Staff
Date Developed: Feb 2017 Date(s) Reviewed:

100
HACCP Step 5 – Non-Target Risk Action Plan (NTRAP)
(Use this form for a ny "Yes" from Column 6 of HACCP Step 4 - Non-Target Analysis Worksheet) One page for each Critical Control Point
Mangement Objective To ensure patients rooms are properly cleaned before From S tep 1 admission, after patient discharge, and as needed during
patient stay.
Critical Control Title: Patients rooms and surgery areas Point:
Significant Non-Target(s) Patients rooms and surgery areas Control Measure(s) Sanitizer to be tested with a kit before use. Sanitizer to be prepared exactly how intructed by the label. Ensure containers and cleaning equipment is not contaminated.
Precribed ranges, limits, or Cleaning area should be documented with time, sanitizer citeria for control measure(s): level, and signature of person cleaning area. (PRLC) Monitoring the Environmental cleaning staff Who? Control Measure(s)
How? Room to be cleaned with soap and water and disinfected with sanitizer before admission and after patient discharge. Patients rooms and surgeical areas Where? Before patient admission, after surgery or procedure, after
How often? discharge, and as needed during patient stay
Corrective Action(s) If sanitizer level below standard, re mix sanitizer, once if Control Measures Fail acceptable sanitize area and document. (or P RLC cannot be met)
Supporting Documents (For example, Management Plan, Checklist, Decontamination Techniques, SOPs, Scientific Journal Articles, etc.) Cleaning log, SOP, Audit conducted once a month Development Team Members
Date Developed: Date(s) Reviewed: Feb 2017
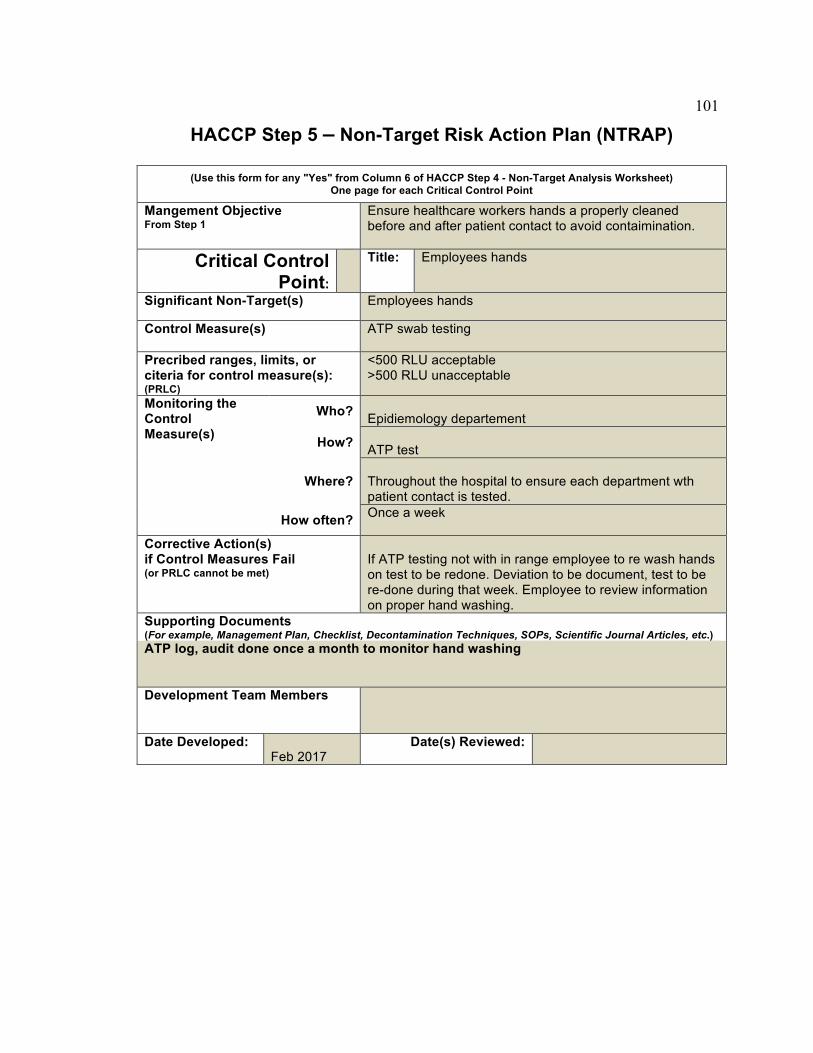
101
HACCP Step 5 – Non-Target Risk Action Plan (NTRAP)
(Use this form for a ny "Yes" from Column 6 of HACCP Step 4 - Non-Target Analysis Worksheet) One page for each Critical Control Point
Mangement Objective Ensure healthcare workers hands a properly cleaned From S tep 1 before and after patient contact to avoid contaimination.
Critical Control Title: Employees hands
Point: Significant Non-Target(s) Employees hands Control Measure(s) ATP swab testing Precribed ranges, limits, or <500 RLU acceptable citeria for c ontrol measure(s): >500 RLU unacceptable (PRLC) Monitoring the Who? Control Epidiemology departement Measure(s) How? ATP test
Where? Throughout the hospital to ensure each department wth
patient contact is tested. Once a week How often?
Corrective Action(s) if Control Measures Fail If ATP testing not with in range employee to re wash hands (or P RLC cannot be met) on test to be redone. Deviation to be document, test to be
re-done during that week. Employee to review information on proper hand washing.
Supporting Documents (For example, Management Plan, Checklist, Decontamination Techniques, SOPs, Scientific Journal Articles, etc.) ATP log, audit done once a month to monitor hand washing Development Team Members
Date Developed: Date(s) Reviewed: Feb 2017
Related Documents











