A Practice Pathway for the Identification, Evaluation, and Management of Insomnia in Children and Adolescents With Autism Spectrum Disorders abstract OBJECTIVE: This report describes the development of a practice path- way for the identification, evaluation, and management of insomnia in children and adolescents who have autism spectrum disorders (ASDs). METHODS: The Sleep Committee of the Autism Treatment Network (ATN) developed a practice pathway, based on expert consensus, to capture best practices for an overarching approach to insomnia by a general pediatrician, primary care provider, or autism medical spe- cialist, including identification, evaluation, and management. A field test at 4 ATN sites was used to evaluate the pathway. In addition, a sys- tematic literature review and grading of evidence provided data regarding treatments of insomnia in children who have neurodevelop- mental disabilities. RESULTS: The literature review revealed that current treatments for insomnia in children who have ASD show promise for behavioral/ educational interventions and melatonin trials. However, there is a paucity of evidence, supporting the need for additional research. Consensus among the ATN sleep medicine committee experts included: (1) all children who have ASD should be screened for insomnia; (2) screening should be done for potential contributing factors, including other medical problems; (3) the need for therapeutic intervention should be determined; (4) therapeutic interventions should begin with parent education in the use of behavioral approaches as a first-line approach; (5) pharmacologic therapy may be indicated in certain situations; and (6) there should be follow-up after any intervention to evaluate effectiveness and tolerance of the therapy. Field testing of the practice pathway by autism medical specialists allowed for refinement of the practice pathway. CONCLUSIONS: The insomnia practice pathway may help health care providers to identify and manage insomnia symptoms in children and adolescents who have ASD. It may also provide a framework to evaluate the impact of contributing factors on insomnia and to test the effec- tiveness of nonpharmacologic and pharmacologic treatment strategies for the nighttime symptoms and daytime functioning and quality of life in ASD. Pediatrics 2012;130:S106–S124 AUTHORS: Beth A. Malow, MD, MS, a,b,c Kelly Byars, PsyD, d Kyle Johnson, MD, e Shelly Weiss, MD, f Pilar Bernal, MD, a,c Suzanne E. Goldman, PhD, g Rebecca Panzer, MA, RD, LD, h Daniel L. Coury, MD, i and Dan G. Glaze, MD j Departments of a Neurology and b Pediatrics and c Kennedy Center, Vanderbilt University Medical Center, Nashville, Tennessee; d Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati Hospital Children’ s Medical Center, Cincinnati, Ohio; e Department of Psychiatry, Oregon Health and Science University, Portland, Oregon; f Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada; g Kaiser Permanente Northern, San Jose, California; h MassGeneral Hospital for Children, Boston, Massachusetts; i Department of Pediatrics, Nationwide Children’ s Hospital, Columbus, Ohio; and j Departments of Neurology and Pediatrics, Baylor College of Medicine, Houston, Texas KEY WORDS actigraphy, education, sleep, sleep latency ABBREVIATIONS ASD—autism spectrum disorder ATN—Autism Treatment Network CSHQ—Children’ s Sleep Habits Questionnaire NICHQ—National Initiative for Children’ s Healthcare Quality RCT—randomized controlled trial This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. www.pediatrics.org/cgi/doi/10.1542/peds.2012-0900I doi:10.1542/peds.2012-0900I Accepted for publication Aug 8, 2012 Address correspondence to Beth Malow, MD, MS, Burry Chair in Cognitive Childhood Development, Director, Vanderbilt Sleep Disorders Division, 1161 21st Avenue South, Room A-0116, Nashville, TN 37232. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2012 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. S106 MALOW et al at Vanderbilt Univ on November 13, 2012 pediatrics.aappublications.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
A Practice Pathway for the Identification, Evaluation, andManagement of Insomnia in Children and AdolescentsWith Autism Spectrum Disorders
abstractOBJECTIVE: This report describes the development of a practice path-way for the identification, evaluation, and management of insomnia inchildren and adolescents who have autism spectrum disorders (ASDs).
METHODS: The Sleep Committee of the Autism Treatment Network(ATN) developed a practice pathway, based on expert consensus, tocapture best practices for an overarching approach to insomnia bya general pediatrician, primary care provider, or autism medical spe-cialist, including identification, evaluation, and management. A fieldtest at 4 ATN sites was used to evaluate the pathway. In addition, a sys-tematic literature review and grading of evidence provided dataregarding treatments of insomnia in children who have neurodevelop-mental disabilities.
RESULTS: The literature review revealed that current treatments forinsomnia in children who have ASD show promise for behavioral/educational interventions and melatonin trials. However, there isa paucity of evidence, supporting the need for additional research.Consensus among the ATN sleep medicine committee expertsincluded: (1) all children who have ASD should be screened forinsomnia; (2) screening should be done for potential contributingfactors, including other medical problems; (3) the need fortherapeutic intervention should be determined; (4) therapeuticinterventions should begin with parent education in the use ofbehavioral approaches as a first-line approach; (5) pharmacologictherapy may be indicated in certain situations; and (6) there shouldbe follow-up after any intervention to evaluate effectiveness andtolerance of the therapy. Field testing of the practice pathway byautism medical specialists allowed for refinement of the practicepathway.
CONCLUSIONS: The insomnia practice pathway may help health careproviders to identify and manage insomnia symptoms in children andadolescents who have ASD. It may also provide a framework to evaluatethe impact of contributing factors on insomnia and to test the effec-tiveness of nonpharmacologic and pharmacologic treatment strategiesfor the nighttime symptoms and daytime functioning and quality of lifein ASD. Pediatrics 2012;130:S106–S124
AUTHORS: Beth A. Malow, MD, MS,a,b,c Kelly Byars, PsyD,d
Kyle Johnson, MD,e Shelly Weiss, MD,f Pilar Bernal, MD,a,c
Suzanne E. Goldman, PhD,g Rebecca Panzer, MA, RD, LD,h
Daniel L. Coury, MD,i and Dan G. Glaze, MDj
Departments of aNeurology and bPediatrics and cKennedy Center,Vanderbilt University Medical Center, Nashville, Tennessee;dDepartment of Pediatrics, University of Cincinnati College ofMedicine, Cincinnati Hospital Children’s Medical Center,Cincinnati, Ohio; eDepartment of Psychiatry, Oregon Health andScience University, Portland, Oregon; fHolland Bloorview KidsRehabilitation Hospital, Toronto, Ontario, Canada; gKaiserPermanente Northern, San Jose, California; hMassGeneralHospital for Children, Boston, Massachusetts; iDepartment ofPediatrics, Nationwide Children’s Hospital, Columbus, Ohio; andjDepartments of Neurology and Pediatrics, Baylor College ofMedicine, Houston, Texas
KEY WORDSactigraphy, education, sleep, sleep latency
ABBREVIATIONSASD—autism spectrum disorderATN—Autism Treatment NetworkCSHQ—Children’s Sleep Habits QuestionnaireNICHQ—National Initiative for Children’s Healthcare QualityRCT—randomized controlled trial
This manuscript has been read and approved by all authors.This paper is unique and not under consideration by any otherpublication and has not been published elsewhere.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-0900I
doi:10.1542/peds.2012-0900I
Accepted for publication Aug 8, 2012
Address correspondence to Beth Malow, MD, MS, Burry Chair inCognitive Childhood Development, Director, Vanderbilt SleepDisorders Division, 1161 21st Avenue South, Room A-0116,Nashville, TN 37232. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
S106 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

Approximately 1 in 110 children fulfillsthe Diagnostic and Statistical Manualof Mental Disorders, Fourth Edition,Text Revision, diagnostic criteria forautism spectrum disorders (ASDs)as defined by delayed or abnormalsocial interaction, language as used insocial communication, and/or restrictedrepetitive and stereotyped patternsof behavior, interests, and activities.1
Children who have ASD are at greaterrisk for developing sleep problems thantypically developing children. Researchhas documented that the prevalence ofsleep disturbances ranges from 53% to78% for children who have ASD com-pared with 26% to 32% for typically de-veloping children.2,3
The key components of pediatric in-somnia are repeated episodes of dif-ficulty initiating and/or maintainingsleep, including premature awaken-ings, leading to insufficient or poor-quality sleep. These episodes result infunctional impairment for the child orother family members.4 In typicallydeveloping children, the primary causeof insomnia is behaviorally based.5 Inthe ASD population, however, insomniais multifactorial. It includes not onlybehavioral issues but also medical,neurologic, and psychiatric comorbid-ities; it is also an adverse effect of themedications used to treat symptoms ofautism and these comorbidities.6
Typically developing children who haveinsomnia are at increased risk forneurobehavioral problems such asimpairments in cognition, mood, atten-tion, and behavior.5,7–9 Similar to thebehavioral morbidity associated withpediatric insomnia that is observed inthe general population, children whohave ASD and sleep problems are proneto more severe comorbid behavioraldisturbances compared with childrenwithout sleep disturbances.10 In addition,treating insomnia in children who haveneurodevelopmental disorders may im-prove problematic daytime behaviors.11
Despite theprevalenceof andmorbidityassociated with pediatric insomnia,there is evidence that sleepdisorders inchildren often go undetected and un-treated.12–14 Medical practitioners of-ten do not ask about sleep concerns orparents do not seek assistance.15 Manyparents have poor knowledge aboutsleep development and sleep prob-lems.16 This is particularly relevant tochildren who have ASD, in that parentsmay present to the pediatrician withconcerns regarding aggression, im-pulsivity, inattention/hyperactivity, orother behavioral issues that may besecondary to a sleep disorder. Thecontribution of the sleep disorder maybe undetected due to emphasis ontreating the behavioral issue as op-posed to identifying and treating theunderlying factors. This deemphasis ofunderlying factors may be due to theabsence of a standardized approachfor recognition and treatment of in-somnia in children who have ASD.
Guidelines exist for sleep screeningandintervention in typically developingchildren.17,18 Guidelines and empiricalsupport also exist for the effectivenessof behavioral treatment of bedtimeproblems and night wakings in chil-dren.18–21 Specific behavioral treat-ments supported include the following:unmodified extinction: leaving thechild’s bedroom after putting the childto bed and not returning until morningunless the child is ill or at risk for in-jury; extinction with parent presence:parent is present in the room with thechild but does not interact with himor her; graduated extinction: parentreturns to child’s bedroom to attendto child on request or agitation butincreases the time in between requestsby the child for the parent to return;preventive parent education: providingeducation to parent on sleep habitsand bedtime routine; bedtime fading:delaying bedtime to promote sleep andthen “fading” or advancing bedtime
once child is falling asleep easier; andscheduled awakenings: awakening thechild before a spontaneous awakening.Extinction and parent education havestrong empirical support whereas theother interventions are less confidentlysupported.18 To our knowledge, how-ever, there are no published guidelinesrelated to management of insomniain children who have ASD, includingscreening and treatment. The evidencethat children who have ASD are atgreater risk for insomnia and itsmorbidity suggests that sleep screen-ing in this population of children isextremely important. The ideal evalua-tion of insomnia in children who haveASD involves a comprehensive sleepassessment, as outlined in a recentreview.22
To facilitate the evaluation of childrenwith ASD for insomnia, the Autism Treat-ment Network (ATN) in association withthe National Initiative for Children’sHealthcare Quality (NICHQ) worked col-laboratively to develop the clinicalpractice pathway presented in this arti-cle. The intention of this clinical practicepathway is to emphasize the need forscreening of sleep problems in ASD andto provide a framework for decision-making related to best practices in thecare of children and adolescents withASD in primary care settings, when seenby a general pediatrician, primary careprovider, or autism medical specialist.The pathway is not intended to serve asthe sole source of guidance in the eval-uation of insomnia in children who haveASD or to replace clinical judgment, andit may not provide the only appropriateapproach to this challenge.
METHODS
Guideline Development
The ATN Sleep Committee consists ofpediatric sleep medicine specialists aswell as developmental pediatricians,neurologists, and psychiatrists. The
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S107 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

clinical practice pathway was designedto assist primary care providers andothers working directly with familiesaffected by ASD in addressing the chal-lenge of insomnia with regard to iden-tification,assessment,andmanagement.
Insomnia was defined as “repeateddifficulty with sleep initiation, duration,consolidation, or quality that occursdespite age-appropriate time and op-portunity for sleep that results in day-time functional impairment for thechild and/or family.”18 The responses ofthe parents to selected questions onthe Children’s Sleep Habits Question-naire (CSHQ)23 identified those patientswho have insomnia.
After performing a systemic review ofthe literature, expert opinion and con-sensuswasused to formthebasisof thepractice pathway (Fig 1). The ATN SleepCommittee’s knowledge of the litera-ture and applicability to clinical prac-tice informed best practices, which inturn created an overarching approachto insomnia within ATN sites by theautism medical specialist.
Systematic Review of the Literature
We conducted a systematic literaturereview to find evidence regardingthe treatment of insomnia in children
diagnosed with ASD (questions andsearch terms available on request fromthe authors). We searched OVID, CINAHL,Embase, Database of Abstracts and Re-view Database of Abstracts of Reviewsand Effects, and the Cochrane Databaseof Systematic reviews databases, withsearches limited to primary and sec-ondary research conducted withhumans, published in the English lan-guage, involving children aged 0 to 18years, and published between January1995 and July 2010. Individual studieswere graded by using an adaptationof the GRADE system24 by 2 primaryreviewers and then reviewed by contentexperts for consensus. Discrepancieswere resolved by a third party.
Pilot Testing of the Pathway
The ATN selected 4 pilot sites (BaylorUniversity, Houston, Texas; OregonHealthandScienceUniversity, Portland,Oregon; Kaiser Permanente Northern,San Jose, California; University of Mis-souri, Columbia, Missouri) to test thefeasibility of the practice pathway andprovide information regarding neededmodifications. The pilot sites collecteddata to document adherence to thepractice pathway and participated inmonthly conference calls to provide
updates, understand variance, and re-commend changes. Working with theNICHQ, members of the ATN SleepCommittee refined and finalized thepractice pathway on the basis of feed-back from the pilot sites. In response torecommendations from the pilot sitesto increase feasibility, the NICHQ alsodeveloped a 1-page checklist designedto guide providers through the practicepathway (Fig 2).
RESULTS
Results of the Literature Review
The search identified 1528 articles. Af-ter removing review articles, com-mentaries, casestudieswith fewer than10 subjects, studies that included chil-dren who did not have ASD, non-intervention trials, and articles thatdid not address our target questions,20 articles remained (Table 1). Wereviewed the literature for studies re-lated to other aspects of the practicepathway (eg, screening for insomnia,identifying comorbidities, importanceof follow-up) in the ASD populationand were unable to identify evidence-based reports for aspects other thantreatment. A comprehensive review25
and consensus statement26 relatedto the pharmacologic management of
FIGURE 1Checklist for carrying out the practice pathway in children who have ASD and insomnia. CSHQ, Children’s Sleep Habits Questionnaire.
S108 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
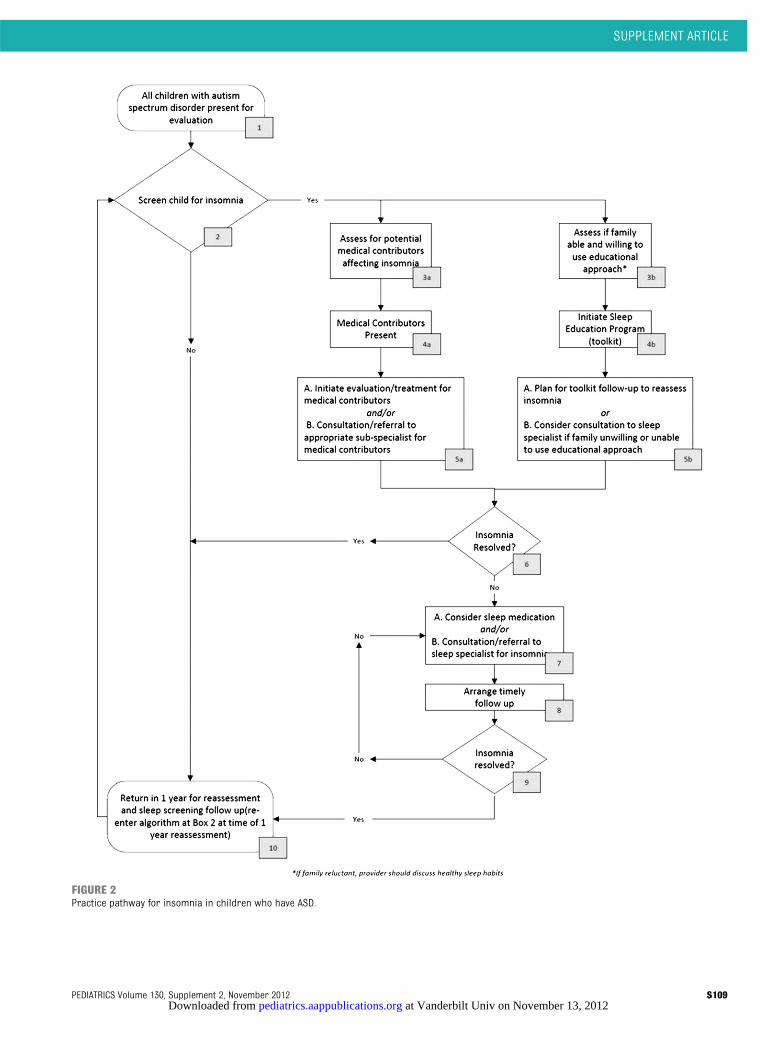
FIGURE 2Practice pathway for insomnia in children who have ASD.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S109 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
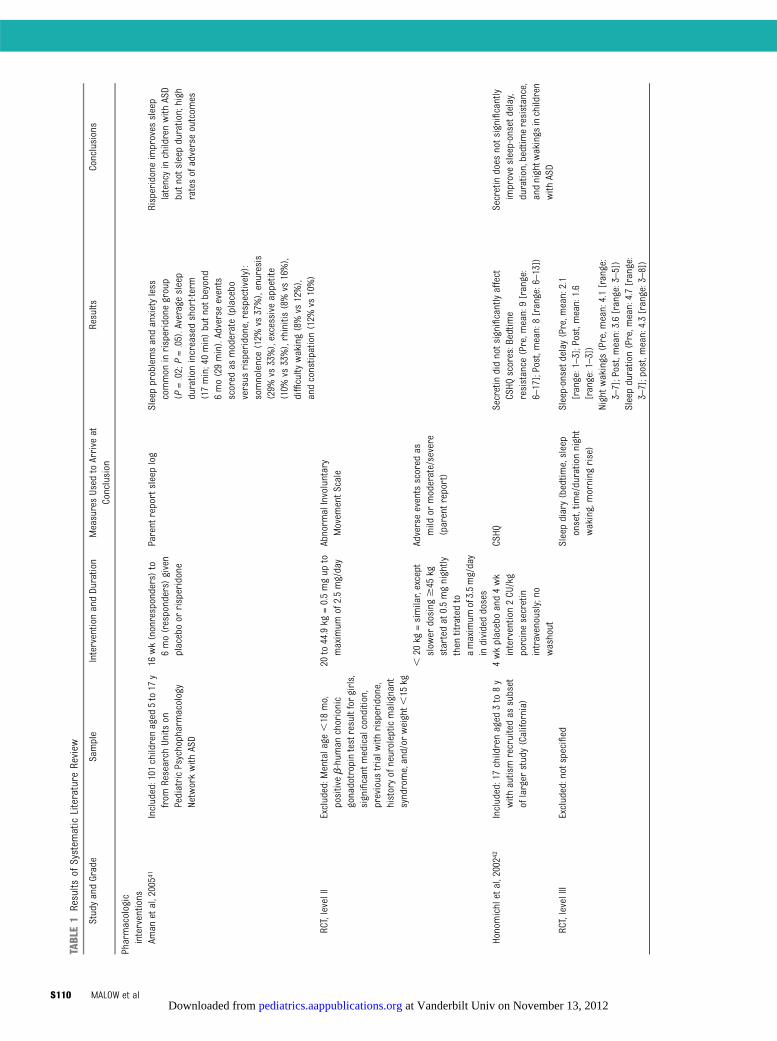
TABLE1
Results
ofSystem
aticLiterature
Review
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Pharmacologic
interventions
Aman
etal,20054
1Included:101
childrenaged
5to17
yfrom
Research
Units
onPediatricPsychopharmacology
Networkwith
ASD
16wk(nonresponders)to
6mo(responders)
given
placeboor
risperidone
Parent
reportsleeplog
Sleepproblemsandanxietyless
common
inrisperidonegroup
(P=.02;P=.05).Average
sleep
durationincreasedshort-term
(17min;40min)butnotb
eyond
6mo(29min).Adverseevents
scored
asmoderate(placebo
versus
risperidone,respectively):
somnolence(12%
vs37%),enuresis
(29%
vs33%),excessiveappetite
(10%
vs33%),rhinitis(8%vs
16%),
difficulty
waking(8%vs
12%),
andconstipation(12%
vs10%)
Risperidoneimproves
sleep
latencyinchildrenwith
ASD
butn
otsleepduration;high
ratesofadverseoutcom
es
RCT,levelII
Excluded:M
entalage
,18
mo,
positiveb-hum
anchorionic
gonadotropintestresultforgirls,
significant
medicalcondition,
previous
trialw
ithrisperidone,
historyofneuroleptic
malignant
syndrome,and/or
weight,
15kg
20to44.9kg
=0.5mgup
tomaximum
of2.5mg/day
Abnorm
alInvoluntary
Movem
entS
cale
,20
kg=similar,except
slow
erdosing
$45
kgstartedat0.5mgnightly
then
titratedto
amaximum
of3.5mg/day
individeddoses
Adverseeventsscored
asmild
ormoderate/severe
(parentreport)
Honomichletal,20024
2Included:17childrenaged
3to8y
with
autismrecruitedas
subset
oflarger
study(California)
4wkplaceboand4wk
intervention2CU/kg
porcinesecretin
intravenously;no
washout
CSHQ
Secretindidnotsignificantlyaffect
CSHQ
scores:Bedtim
eresistance
(Pre,m
ean:9[range:
6–17];Post,m
ean:8[range:6–13])
Secretindoes
notsignificantly
improvesleep-onsetd
elay,
duration,bedtimeresistance,
andnightw
akings
inchildren
with
ASD
RCT,levelIII
Excluded:notspecified
Sleepdiary(bedtim
e,sleep
onset,tim
e/durationnight
waking,morning
rise)
Sleep-onsetd
elay
(Pre,m
ean:2.1
[range:1–3];Post,mean:1.6
[range:1–3])
Nightw
akings
(Pre,m
ean:4.1[range:
3–7];Post,mean:3.6[range:3–5])
Sleepduration(Pre,m
ean:4.7[range:
3–7];post,mean:4.3[range:3–8])
S110 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
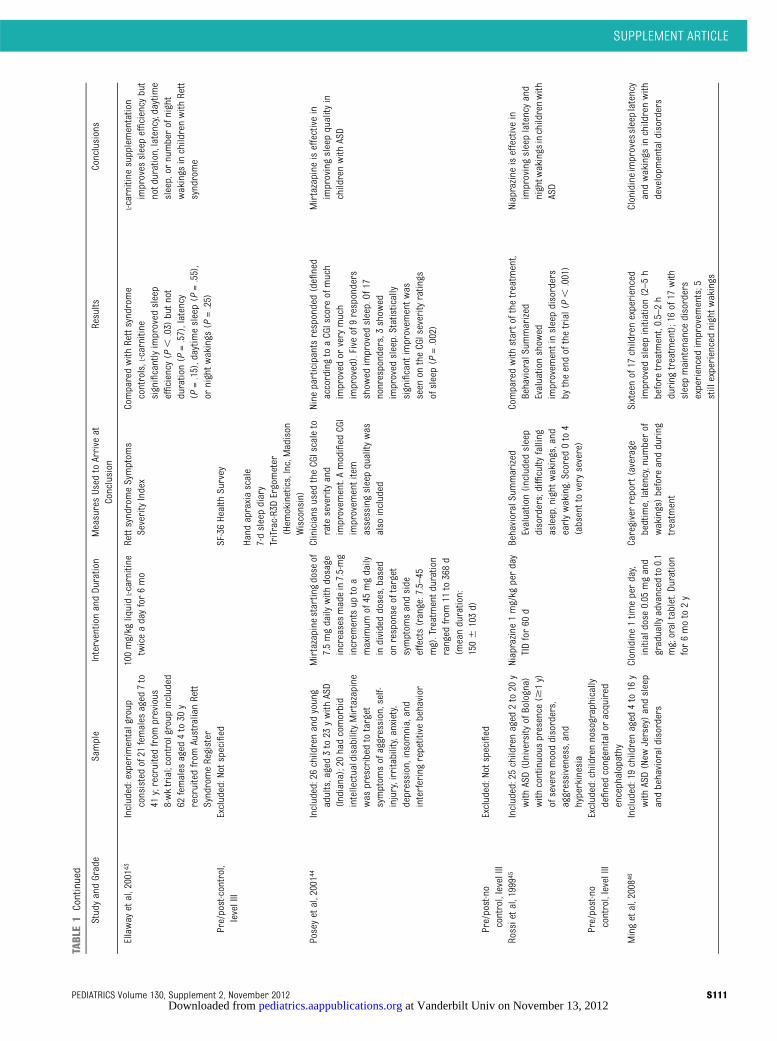
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Ellaway
etal,20014
3Included:experimentalgroup
consistedof21
females
aged
7to
41y;recruitedfrom
previous
8-wktrial;controlgroup
included
62females
aged
4to30
yrecruitedfrom
AustralianRett
SyndromeRegister
100mg/kg
liquid
L-carnitine
twiceadayfor6mo
RettsyndromeSymptom
sSeverityIndex
Comparedwith
Rettsyndrome
controls,L-carnitine
significantlyimproved
sleep
efficiency
(P,
.03)
butn
otduration(P
=.57),latency
(P=.15),daytim
esleep(P
=.55),
ornightw
akings
(P=.25)
L-carnitinesupplementation
improves
sleepefficiency
but
notduration,latency,daytime
sleep,or
numberofnight
wakings
inchildrenwith
Rett
syndrome
Pre/post-control,
levelIII
Excluded:Notspecified
SF-36Health
Survey
Hand
apraxiascale
7-dsleepdiary
TriTrac-R3DErgometer
(Hem
okinetics,Inc,Madison
Wisconsin)
Poseyetal,20014
4Included:26childrenandyoung
adults,aged3to23
ywith
ASD
(Indiana);20hadcomorbid
intellectualdisability.M
irtazapine
was
prescribed
totarget
symptom
sofaggression,self-
injury,irritability,anxiety,
depression,insom
nia,and
interferingrepetitivebehavior
Mirtazapine
startingdose
of7.5mgdaily
with
dosage
increasesmadein7.5-mg
increm
entsup
toa
maximum
of45
mgdaily
individeddoses,based
onresponse
oftarget
symptom
sandside
effects(range:7.5–45
mg).Treatmentd
uration
ranged
from
11to368d
(meanduration:
1506
103d)
Clinicians
used
theCGIscaleto
rateseverityand
improvem
ent.Amodified
CGI
improvem
entitem
assessingsleepquality
was
also
included
Nine
participantsresponded(defined
accordingtoaCGIscore
ofmuch
improved
orvery
much
improved).Five
of9responders
show
edimproved
sleep.Of
17nonresponders,3show
edimproved
sleep.Statistically
significant
improvem
entw
asseen
ontheCGIseverity
ratings
ofsleep(P
=.002)
Mirtazapine
iseffectivein
improvingsleepquality
inchildrenwith
ASD
Pre/post-no
control,levelIII
Excluded:Notspecified
Rossietal,1999
45Included:25childrenaged
2to20
ywith
ASD(University
ofBologna)
with
continuous
presence
($1y)
ofsevere
mooddisorders,
aggressiveness,and
hyperkinesia
Niaprazine
1mg/kg
perday
TIDfor60
dBehavioralSummarized
Evaluation(includedsleep
disorders;difficulty
falling
asleep,night
wakings,and
earlywaking.Scored
0to4
(absenttovery
severe)
Comparedwith
startofthe
treatm
ent,
BehavioralSummarized
Evaluationshow
edimprovem
entinsleepdisorders
bytheendofthetrial(P,
.001)
Niaprazine
iseffectivein
improvingsleeplatencyand
nightw
akings
inchildrenwith
ASD
Pre/post-no
control,levelIII
Excluded:childrennosographically
definedcongenitaloracquired
encephalopathy
Mingetal,20084
6Included:19childrenaged
4to16
ywith
ASD(New
Jersey)andsleep
andbehavioraldisorders
Clonidine1tim
eperday,
initialdose
0.05
mgand
gradually
advanced
to0.1
mg;oraltablet.Duration
for6moto2y
Caregiverreport(average
bedtime,latency,numberof
wakings)before
andduring
treatm
ent
Sixteenof17
childrenexperienced
improved
sleepinitiation(2–5h
before
treatm
ent,0.5–2h
during
treatm
ent);16of17
with
sleepmaintenance
disorders
experiencedimprovem
ents;5
stillexperiencednightw
akings
Clonidineimprovessleeplatency
andwakings
inchildrenwith
developm
entaldisorders
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S111 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
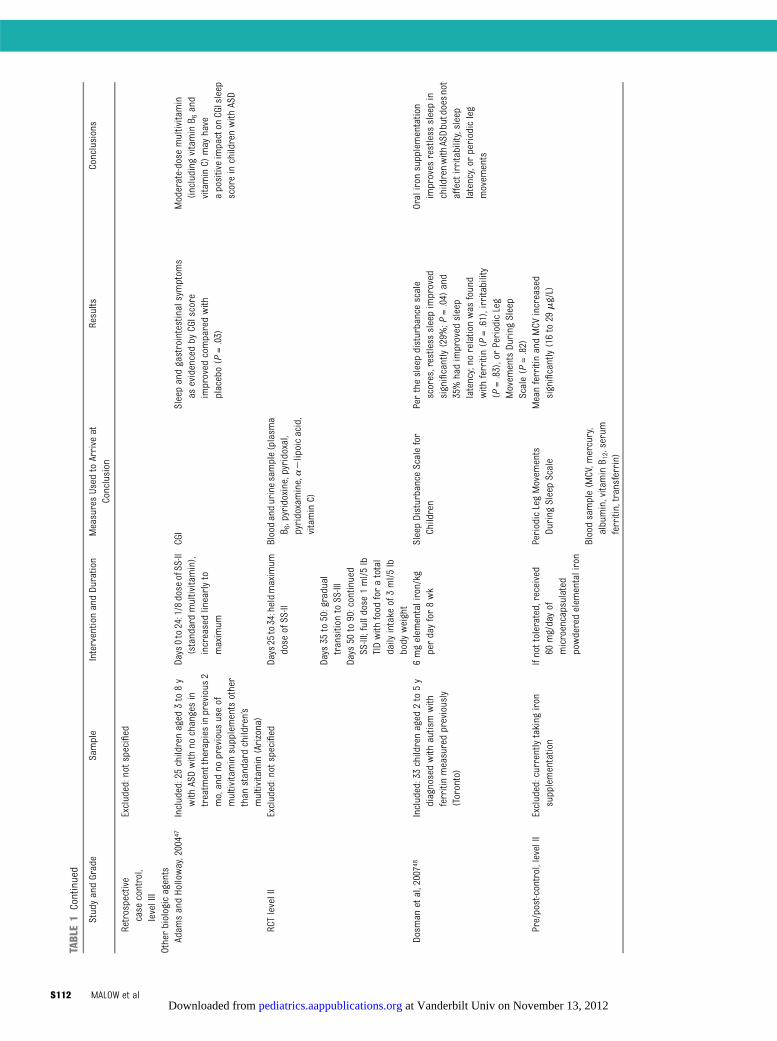
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Retrospective
case
control,
levelIII
Excluded:not
specified
Otherbiologicagents
Adam
sandHolloway,20044
7Included:25childrenaged
3to
8y
with
ASDwith
nochangesin
treatm
enttherapies
inprevious
2mo,andno
previous
useof
multivitaminsupplementsother
than
standard
children’s
multivitamin(Arizona)
Days0to24:1/8dose
ofSS-II
(standardmultivitamin),
increasedlinearlyto
maximum
CGI
Sleepandgastrointestinalsymptom
sas
evidencedby
CGIscore
improved
comparedwith
placebo(P
=.03)
Moderate-dose
multivitamin
(including
vitaminB 6
and
vitaminC)
may
have
apositiveimpacton
CGIsleep
scoreinchildrenwith
ASD
RCTlevelII
Excluded:not
specified
Days25
to34:heldmaximum
dose
ofSS-II
Bloodandurinesample(plasm
aB 6,pyridoxine,pyridoxal,
pyridoxamine,a2lipoicacid,
vitaminC)
Days
35to50:gradual
transitiontoSS-III
Days
50to90:continued
SS-III;fulldose
1ml/5lb
TIDwith
food
foratotal
daily
intake
of3ml/5lb
body
weight
Dosm
anetal,20074
8Included:33childrenaged
2to
5y
diagnosedwith
autismwith
ferritinmeasuredpreviously
(Toronto)
6mgelem
entaliron/kg
perdayfor8wk
SleepDisturbanceScalefor
Children
Perthesleepdisturbancescale
scores,restless
sleepimproved
significantly(29%
;P=.04)
and
35%hadimproved
sleep
latency;no
relationwas
found
with
ferritin(P
=.61),irritability
(P=.83),orPeriodicLeg
Movem
entsDuring
Sleep
Scale(P
=.82)
Oraliron
supplementation
improves
restless
sleepin
childrenwith
ASDbutdoesn
otaffectirritability,sleep
latency,or
periodicleg
movem
ents
Pre/post-control,levelII
Excluded:currentlytaking
iron
supplementation
Ifnottolerated,received
60mg/dayof
microencapsulated
powderedelem
entaliron
PeriodicLegMovem
ents
During
SleepScale
MeanferritinandMCV
increased
significantly(16to29
mg/L)
Bloodsample(M
CV,m
ercury,
albumin,vitaminB 1
2,serum
ferritin,transferrin)
S112 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
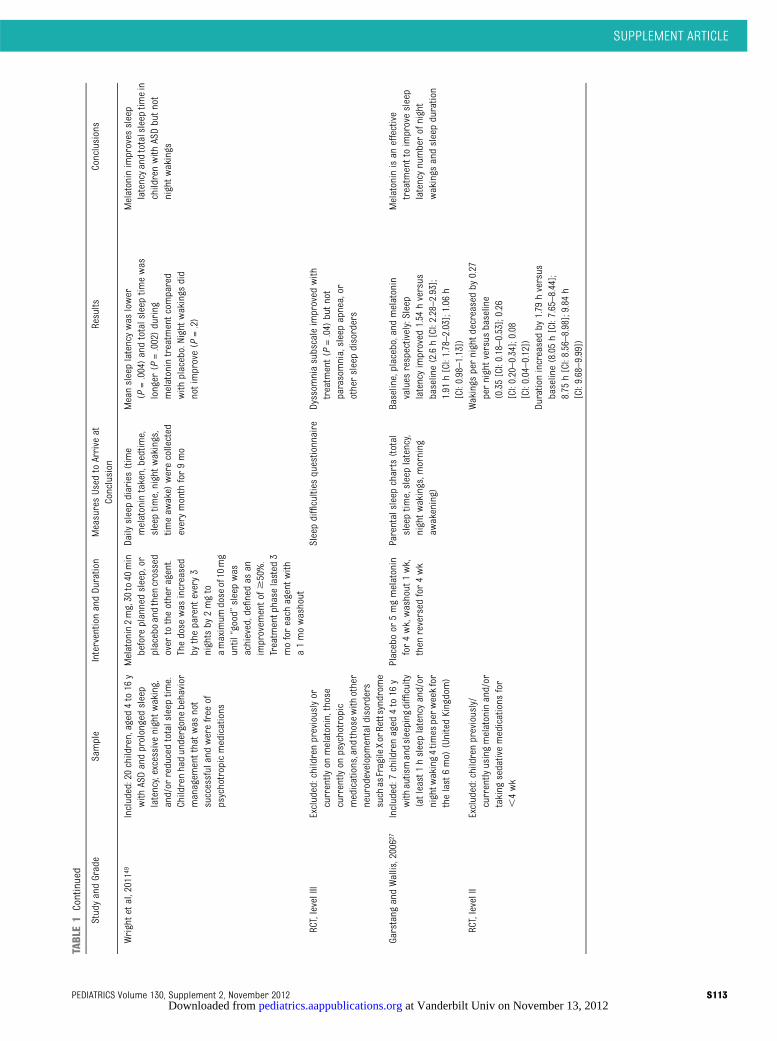
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Wrightetal,20114
9Included:20children,aged
4to16
ywith
ASDandprolongedsleep
latency,excessivenightw
aking,
and/or
reducedtotalsleep
time.
Childrenhadundergonebehavior
managem
entthatwas
not
successfulandwerefree
ofpsychotropicmedications
Melatonin2mg,30
to40
min
before
plannedsleep,or
placeboandthen
crossed
over
totheotheragent.
Thedose
was
increased
bytheparent
every3
nightsby
2mgto
amaximum
doseof10
mg
until“good”
sleepwas
achieved,definedas
animprovem
entof$
50%.
Treatm
entphase
lasted
3moforeach
agentw
itha1mowashout
Daily
sleepdiaries(time
melatonintaken,bedtime,
sleeptim
e,nightw
akings,
timeaw
ake)
werecollected
everymonth
for9mo
Meansleeplatencywas
lower
(P=.004)andtotalsleep
timewas
longer
(P=.002)during
melatonintreatm
entcom
pared
with
placebo.Nightw
akings
did
notimprove(P
=.2)
Melatoninimproves
sleep
latencyandtotalsleep
timein
childrenwith
ASDbutn
otnightw
akings
RCT,levelIII
Excluded:childrenpreviouslyor
currently
onmelatonin,those
currently
onpsychotropic
medications,and
thosewith
other
neurodevelopmentaldisorders
such
asFragile
XorRettsyndrome
Sleepdifficulties
questionnaire
Dyssom
niasubscaleimproved
with
treatm
ent(P=.04)
butnot
parasomnia,sleepapnea,or
othersleepdisorders
Garstang
andWallis,20062
7Included:7
childrenaged
4to16
ywith
autismandsleeping
difficulty
(atleast1hsleeplatencyand/or
nightw
aking4tim
esperweekfor
thelast6mo)
(UnitedKingdom)
Placeboor
5mgmelatonin
for4wk,washout
1wk,
then
reversed
for4wk
Parentalsleepcharts(total
sleeptim
e,sleeplatency,
nightw
akings,m
orning
awakening)
Baseline,placebo,andmelatonin
values
respectively:Sleep
latencyimproved
1.54
hversus
baseline(2.6h[CI:2.28–2.93];
1.91
h[CI:1.78–2.03];1.06
h[CI:0.98–1.13])
Melatoninisan
effective
treatm
enttoimprovesleep
latencynumberofnight
wakings
andsleepduration
RCT,levelII
Excluded:childrenpreviously/
currently
usingmelatoninand/or
taking
sedativemedications
for
,4wk
Wakings
pernightd
ecreased
by0.27
pernightversusbaseline
(0.35[CI:0.18–0.53];0.26
[CI:0.20–0.34];0.08
[CI:0.04–0.12])
Durationincreasedby
1.79
hversus
baseline(8.05h[CI:7.65–8.44];
8.75
h[CI:8.56–8.98];9.84
h[CI:9.68–9.99])
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S113 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
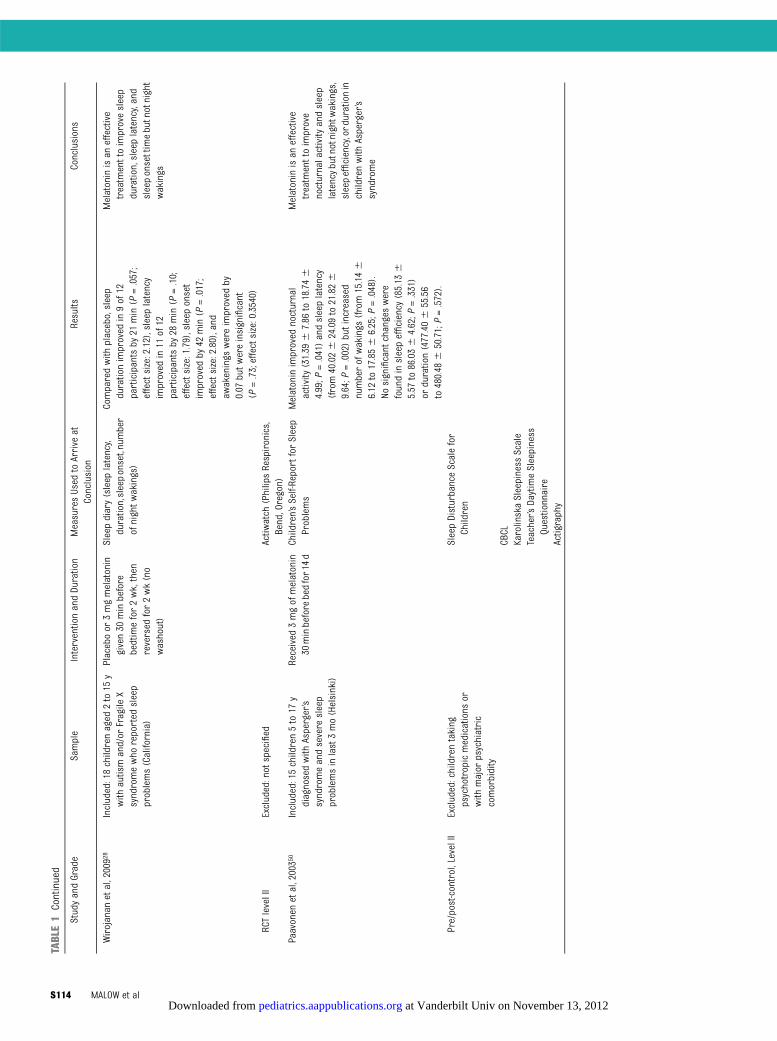
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Wirojanan
etal,20092
8Included:18childrenaged
2to15
ywith
autismand/or
Fragile
Xsyndromewho
reported
sleep
problems(California)
Placeboor
3mgmelatonin
given30
minbefore
bedtimefor2wk,then
reversed
for2wk(no
washout)
Sleepdiary(sleep
latency,
duration,sleeponset,number
ofnightw
akings)
Comparedwith
placebo,sleep
durationimproved
in9of12
participantsby
21min(P
=.057;
effectsize:2.12),sleep
latency
improved
in11
of12
participantsby
28min(P
=.10;
effectsize:1.79),sleep
onset
improved
by42
min(P
=.017;
effectsize:2.80),and
awakenings
wereimproved
by0.07
butwereinsignificant
(P=.73;effectsize:0.3540)
Melatoninisan
effective
treatm
enttoimprovesleep
duration,sleeplatency,and
sleeponsettimebutnotnight
wakings
RCTlevelII
Excluded:not
specified
Actiw
atch
(PhilipsRespironics,
Bend,Oregon)
Paavonen
etal,20035
0Included:15children5to17
ydiagnosedwith
Asperger’s
syndromeandsevere
sleep
problemsinlast3mo(Helsinki)
Received
3mgofmelatonin
30minbeforebedfor14d
Children’sSelf-ReportforSleep
Problems
Melatoninimproved
nocturnal
activity
(31.39
67.86
to18.746
4.99;P
=.041)andsleeplatency
(from40.026
24.09to21.826
9.64;P
=.002)butincreased
numberofwakings
(from15.146
6.12
to17.856
6.25;P
=.048).
Nosignificant
changeswere
foundinsleepefficiency
(85.13
65.57
to86.036
4.62;P
=.331)
orduration(477.406
55.56
to480.48
650.71;P=.572).
Melatoninisan
effective
treatm
enttoimprove
nocturnalactivity
andsleep
latencybutnotnightw
akings,
sleepefficiency,ordurationin
childrenwith
Asperger’s
syndrome
Pre/post-control,LevelII
Excluded:childrentaking
psychotropicmedications
orwith
major
psychiatric
comorbidity
SleepDisturbanceScalefor
Children
CBCL
KarolinskaSleepiness
Scale
Teacher’s
DaytimeSleepiness
Questionnaire
Actigraphy
S114 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
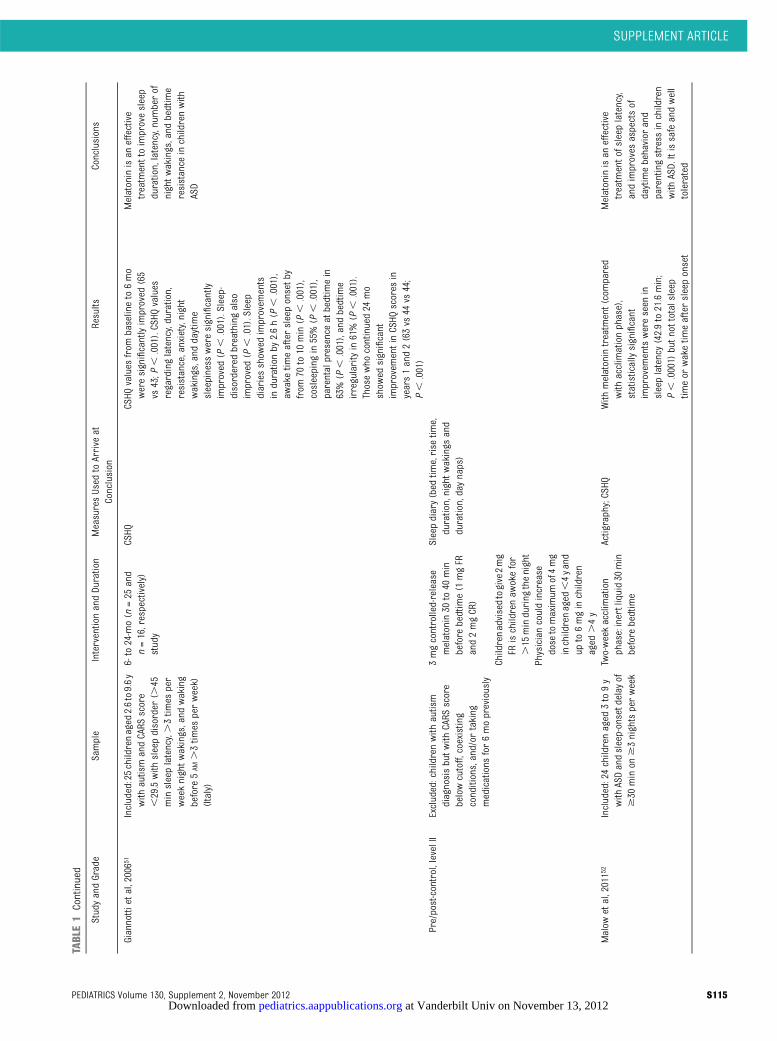
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Giannottietal,20065
1Included:25childrenaged
2.6to9.6y
with
autismandCARS
score
,29.5with
sleepdisorder
(.45
minsleeplatency,.3tim
esper
weeknightwakings,and
waking
before
5AM
.3tim
esperweek)
(Italy)
6-to
24-mo(n
=25
and
n=16,respectively)
study
CSHQ
CSHQ
values
from
baselineto6mo
weresignificantlyimproved
(65
vs43;P
,.001).CSHQ
values
regardinglatency,duration,
resistance,anxiety,night
wakings,and
daytime
sleepiness
weresignificantly
improved
(P,
.001).Sleep-
disordered
breathingalso
improved
(P,
.01).Sleep
diariesshow
edimprovem
ents
indurationby
2.6h(P
,.001),
awaketim
eaftersleeponsetb
yfrom
70to10
min(P
,.001),
cosleeping
in55%(P
,.001),
parentalpresence
atbedtimein
63%(P
,.001),andbedtime
irregularityin61%(P
,.001).
Thosewho
continued24
mo
show
edsignificant
improvem
entinCSHQ
scores
inyears1and2(63vs
44vs
44;
P,
.001)
Melatoninisan
effective
treatm
enttoimprovesleep
duration,latency,numberof
nightwakings,and
bedtime
resistance
inchildrenwith
ASD
Pre/post-control,levelII
Excluded:childrenwith
autism
diagnosisbutw
ithCARS
score
belowcutoff,coexisting
conditions,and/or
taking
medications
for6mopreviously
3mgcontrolled-release
melatonin30
to40
min
before
bedtime(1
mgFR
and2mgCR)
Sleepdiary(bed
time,rise
time,
duration,nightw
akings
and
duration,daynaps)
Childrenadvisedtogive2mg
FRischildrenaw
okefor
.15
minduring
thenight
Physiciancouldincrease
dose
tomaximum
of4mg
inchildrenaged
,4yand
upto6mginchildren
aged
.4y
Malow
etal,20115
2Included:24childrenaged
3to9y
with
ASDandsleep-onsetdelay
of$30
minon
$3nightsperweek
Two-weekacclimation
phase:inertliquid30
min
before
bedtime
Actigraphy;CSHQ
With
melatonintreatm
ent(compared
with
acclimationphase),
statisticallysignificant
improvem
entswereseen
insleeplatency(42.9to21.6min;
P,
.0001)
butnottotalsleep
timeor
waketim
eaftersleeponset
Melatoninisan
effective
treatm
entofsleeplatency,
andimproves
aspectsof
daytimebehavior
and
parentingstress
inchildren
with
ASD.Itissafeandwell
tolerated
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S115 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
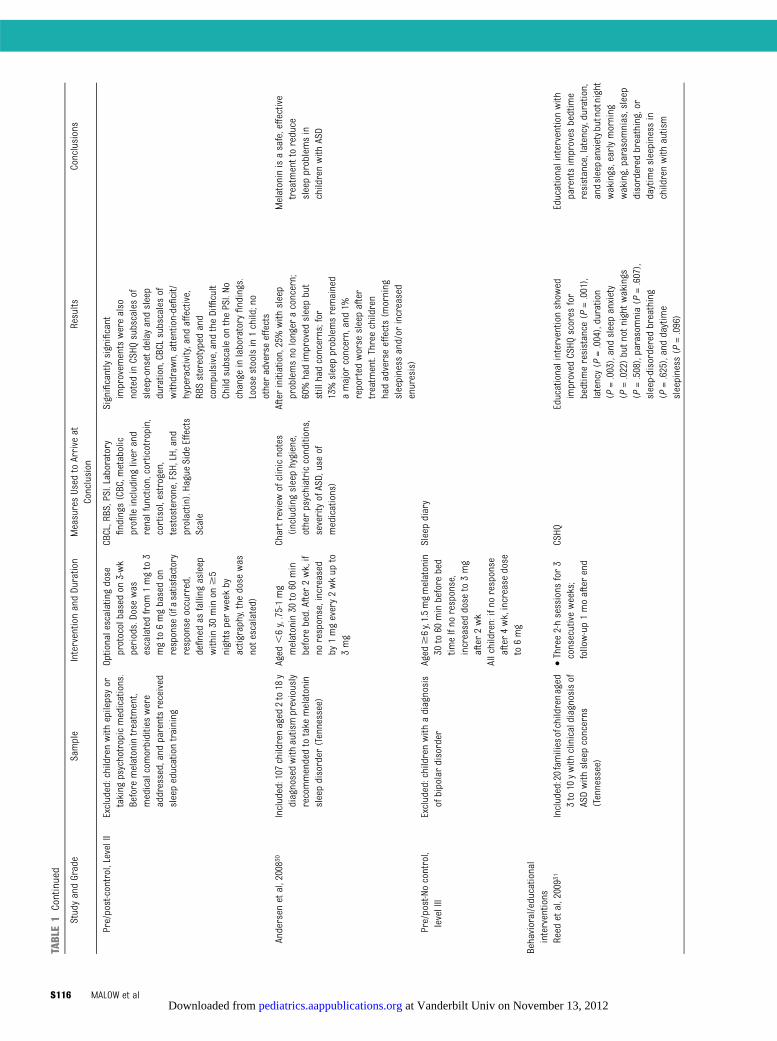
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Pre/post-control,LevelII
Excluded:childrenwith
epilepsyor
taking
psychotropicmedications.
Before
melatonintreatm
ent,
medicalcomorbiditieswere
addressed,andparentsreceived
sleepeducationtraining
Optionalescalatingdose
protocolbasedon
3-wk
periods.Dose
was
escalatedfrom
1mgto3
mgto6mgbasedon
response
(ifasatisfactory
response
occurred,
definedas
falling
asleep
within30
minon
$5
nightsperweekby
actigraphy,thedose
was
notescalated)
CBCL,RBS,PSI.Laboratory
findings
(CBC,m
etabolic
profileincludingliver
and
renalfunction,corticotropin,
cortisol,estrogen,
testosterone,FSH,LH,and
prolactin).HagueSide
Effects
Scale
Significantlysignificant
improvem
entswerealso
notedinCSHQ
subscalesof
sleep-onsetd
elay
andsleep
duration,CBCL
subscalesof
withdraw
n,attention-deficit/
hyperactivity,and
affective,
RBSstereotypedand
compulsive,andtheDifficult
Child
subscaleon
thePSI.No
change
inlaboratory
findings.
Loosestoolsin1child;no
otheradverseeffects
Andersen
etal,20083
0Included:107
childrenaged
2to18
ydiagnosedwith
autismpreviously
recommendedtotake
melatonin
sleepdisorder
(Tennessee)
Aged
,6y,.75-1mg
melatonin30
to60
min
before
bed.After2wk,if
noresponse,increased
by1mgevery2wkup
to3mg
Chartreviewofclinicnotes
(including
sleephygiene,
otherpsychiatricconditions,
severityofASD,useof
medications)
Afterinitiation,25%with
sleep
problemsno
longer
aconcern;
60%hadimproved
sleepbut
stillhadconcerns;for
13%sleepproblemsremained
amajor
concern,and1%
reported
worse
sleepafter
treatm
ent.Threechildren
hadadverseeffects(m
orning
sleepiness
and/or
increased
enuresis)
Melatoninisasafe,effective
treatm
enttoreduce
sleepproblemsin
childrenwith
ASD
Pre/post-Nocontrol,
levelIII
Excluded:childrenwith
adiagnosis
ofbipolardisorder
Aged
$6y,1.5mgmelatonin
30to60
minbefore
bed
timeIfno
response,
increaseddose
to3mg
after2wk
Sleepdiary
Allchildren:ifno
response
after4wk,increase
dose
to6mg
Behavioral/educational
interventions
Reed
etal,20093
1Included:20familiesofchildrenaged
3to10
ywith
clinicaldiagnosisof
ASDwith
sleepconcerns
(Tennessee)
•Three2-hsessions
for3
consecutiveweeks;
follow-up1moafterend
CSHQ
Educationalinterventionshow
edimproved
CSHQ
scores
for
bedtimeresistance
(P=.001),
latency(P
=.004),duration
(P=.003),andsleepanxiety
(P=.022)butn
otnightw
akings
(P=.508),parasomnia(P
=.607),
sleep-disordered
breathing
(P=.625),anddaytime
sleepiness
(P=.096)
Educationalinterventionwith
parentsimproves
bedtime
resistance,latency,duration,
andsleepanxietybutnotnight
wakings,earlymorning
waking,parasomnias,sleep
disordered
breathing,or
daytimesleepiness
inchildrenwith
autism
S116 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
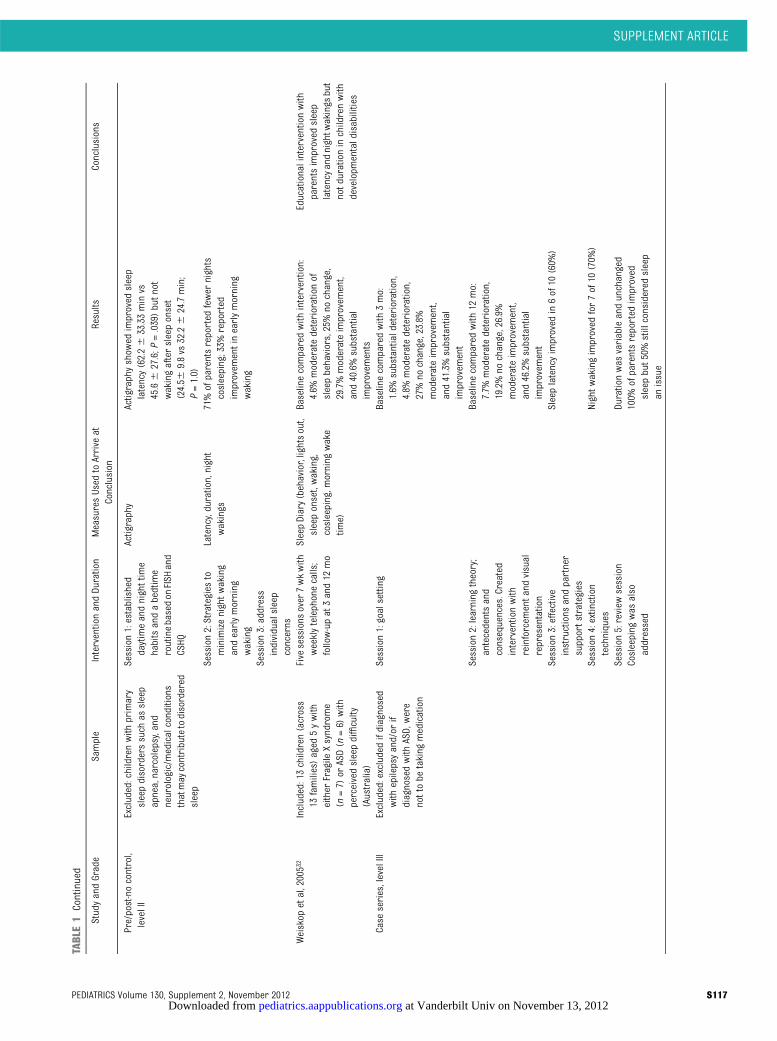
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Pre/post-nocontrol,
levelII
Excluded:childrenwith
primary
sleepdisorderssuch
assleep
apnea,narcolepsy,and
neurologic/m
edicalconditions
thatmaycontributetodisordered
sleep
Session1:established
daytimeandnighttime
habitsandabedtime
routinebasedon
FISH
and
CSHQ
Actigraphy
Actigraphyshow
edimproved
sleep
latency(62.26
33.33minvs
45.66
27.6;P
=.039)butn
otwakingaftersleeponset
(24.56
9.8vs
32.26
24.7min;
P=1.0)
Session2:Strategies
tominimizenightwaking
andearlymorning
waking
Latency,duration,night
wakings
71%ofparentsreported
fewer
nights
cosleeping;33%
reported
improvem
entinearlymorning
waking
Session3:address
individualsleep
concerns
Weiskop
etal,20053
2Included:13children(across
13families)aged
5ywith
either
Fragile
Xsyndrome
(n=7)
orASD(n
=6)
with
perceivedsleepdifficulty
(Australia)
Five
sessions
over
7wkwith
weeklytelephonecalls;
follow-upat3and12
mo
SleepDiary(behavior,lightsout,
sleeponset,waking,
cosleeping,m
orning
wake
time)
Baselinecomparedwith
intervention:
4.6%
moderatedeteriorationof
sleepbehaviors,25%no
change,
29.7%moderateimprovem
ent,
and40.6%substantial
improvem
ents
Educationalinterventionwith
parentsimproved
sleep
latencyandnightw
akings
but
notd
urationinchildrenwith
developm
entaldisabilities
Case
series,levelIII
Excluded:excludedifdiagnosed
with
epilepsyand/or
ifdiagnosedwith
ASD,were
nottobe
taking
medication
Session1:goalsetting
Baselinecomparedwith
3mo:
1.6%
substantialdeterioration,
4.8%
moderatedeterioration,
27%no
change,23.8%
moderateimprovem
ent,
and41.3%substantial
improvem
ent
Session2:learning
theory;
antecedentsand
consequences.Created
interventionwith
reinforcem
entand
visual
representation
Baselinecomparedwith
12mo:
7.7%
moderatedeterioration,
19.2%no
change,26.9%
moderateimprovem
ent,
and46.2%substantial
improvem
ent
Session3:effective
instructions
andpartner
supportstrategies
Sleeplatencyimproved
in6of10
(60%
)
Session4:extinction
techniques
Nightw
akingimproved
for7of10
(70%
)
Session5:review
session
Durationwas
variableandunchanged
Cosleeping
was
also
addressed
100%
ofparentsreported
improved
sleepbut50%
stillconsidered
sleep
anissue
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S117 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
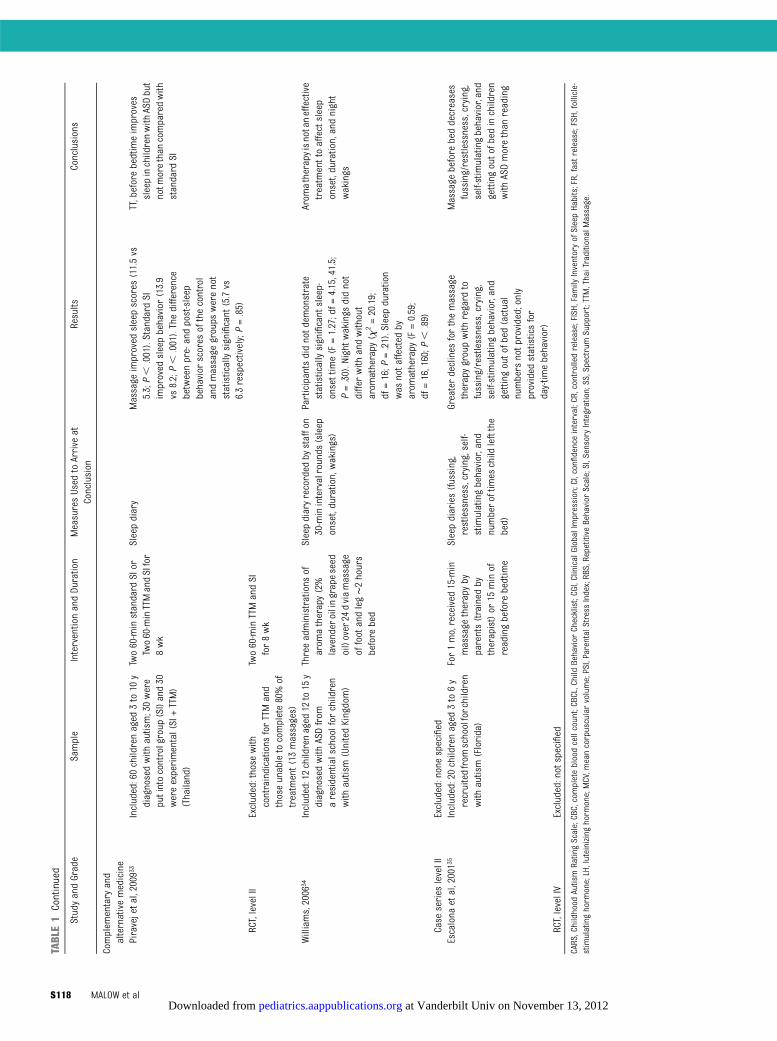
TABLE1
Continued
StudyandGrade
Sample
InterventionandDuration
MeasuresUsed
toArrive
atConclusion
Results
Conclusions
Complem
entary
and
alternativemedicine
Piravejetal,2009
33Included:60childrenaged
3to10
ydiagnosedwith
autism;30were
putintocontrolgroup
(SI)and30
wereexperimental(SI+TTM)
(Thailand)
Two60-minstandard
SIor
Two60-minTTMandSIfor
8wk
Sleepdiary
Massage
improved
sleepscores
(11.5vs
5.3;P,
.001).Standard
SIimproved
sleepbehavior
(13.9
vs8.2;P,
.001).Thedifference
betweenpre-andpost-sleep
behavior
scores
ofthecontrol
andmassage
groups
werenot
statisticallysignificant
(5.7vs
6.3respectively;P=.85)
TT,beforebedtimeimproves
sleepinchildrenwith
ASDbut
notm
orethan
comparedwith
standard
SI
RCT,levelII
Excluded:those
with
contraindications
forTTMand
thoseunabletocomplete80%of
treatm
ent(13
massages)
Two60-minTTMandSI
for8wk
Williams,2006
34Included:12childrenaged
12to15
ydiagnosedwith
ASDfrom
aresidentialschoolfor
children
with
autism(UnitedKingdom)
Threeadministrations
ofarom
atherapy(2%
lavenderoilingrapeseed
oil)over24
dviamassage
offootandleg∼2hours
before
bed
Sleepdiaryrecorded
bystaffon
30-minintervalrounds
(sleep
onset,duration,wakings)
Participantsdidnotdemonstrate
statisticallysignificant
sleep-
onsettime(F=1.27;df=
4.15,41.5;
P=.30).Night
wakings
didnot
differwith
andwithout
arom
atherapy
(x2=20.19;
df=16;P
=.21).Sleep
duration
was
notaffected
byarom
atherapy
(F=0.59;
df=16,160;P
,.89)
Arom
atherapyisnotaneffective
treatm
enttoaffectsleep
onset,duration,andnight
wakings
Case
series
levelII
Excluded:nonespecified
Escalona
etal,20013
5Included:20childrenaged
3to6y
recruitedfrom
schoolforchildren
with
autism(Florida)
For1mo,received
15-min
massage
therapyby
parents(trained
bytherapist)or
15minof
readingbefore
bedtime
Sleepdiaries(fussing,
restlessness,crying,self-
stimulatingbehavior,and
numberoftim
eschild
leftthe
bed)
Greaterdeclines
forthemassage
therapygroupwith
regard
tofussing/restlessness,crying,
self-stimulatingbehavior,and
gettingoutofbed(actual
numbers
notp
rovided;only
provided
statisticsfor
day-tim
ebehavior)
Massage
before
beddecreases
fussing/restlessness,crying,
self-stimulatingbehavior,and
gettingoutofbed
inchildren
with
ASDmorethan
reading
RCT,levelIV
Excluded:notspecified
CARS,Childhood
Autism
RatingScale;CBC,completebloodcellcount;CBCL,ChildBehavior
Checklist;CGI,ClinicalGlobalImpression;CI,confidenceinterval;CR,controlledrelease;FISH,Fam
ilyInventoryofSleepHabits;FR,fastrelease;FSH,follicle-
stimulatinghorm
one;LH,luteinizing
horm
one;MCV,m
eancorpuscularvolume;PSI,ParentalStress
Index;RBS,RepetitiveBehavior
Scale;SI,Sensory
Integration;SS,SpectrumSupport;TTM,ThaiTraditionalM
assage.
S118 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

insomnia in children (not specific toASD) were identified.
The results of the systematic literaturereview demonstrate that treatmenttrials are limited in the ASD population.There are 3 categories of treatment:pharmacologic/biologic treatments,behavioral/educational interventions,and complementary and alternativemedicine.
Theevidencebase todateshows limitedevidence for the use of medications totreat insomnia in children who haveASD. The most evidence exists for theuse of supplemental melatonin, anindoleamine with sleep-promoting andchronobiotic (sleep phase shifting)properties considered a nutritionalsupplement by the US Food and DrugAdministration. Several small, ran-domized controlled trials (RCTs) dem-onstrated the efficacy of supplementalmelatonin in treating insomnia inchildren who have ASD,27–29 althoughlarger studies are needed. Melatoninseems to be relatively safe based onthese trials and on other series.30
Other pharmacologic interventionssuch as risperidone, secretin, L-carni-tine, niaprazine, mirtazapine, and clo-nidine, as well as multivitamins andiron, have limited evidence supportingtheir use in treating insomnia in ASD.The research evidence to date does notsupport the efficacy of other supple-ments or vitamins.
Behavioral interventions are clearlybeneficial for typically developing chil-dren experiencing significant insom-nia.21 However, few treatment trialsfound that behavioral treatments pro-vide consistent success rates in chil-dren who have ASD, particularly thoseexperiencing sleep-onset insomnia. Thesystematic review of the literature iden-tified 2 studies examining the efficacyof behavioral treatment of insomniain children who have ASD.31,32 Each ofthese studies demonstrated statisti-cally significant improvements in sleepTA
BLE2
SleepQuestionnaire
Options
Questionnaire
Description
Form
atRespondent
CSHQ
(Owensetal,2000)
36Assesses
sleepbehaviorsacross
arangeofbehavioraland
medicaldimensionsinchildrenaged
4to10
yForty-five
itemsthatrollinto8subscales:bedtimeresistance,
sleeponsetdelay,sleep
duration,sleepanxiety,nightw
akings,
parasomnias,sleep-disorderedbreathing,anddaytime
sleepiness
Parent
Children’sSleepHabitsQuestionnaire
inToddlers
andPreschool
Children(Goodlin-Jones
etal,2008)
23
Assesses
theCSHQ
(see
above)
inchildrenaged
2to5.5ywith
autism,developmentaldelay
withoutautism,and
typically
developing
children
Sameas
theCSHQ
(above)
Parent
SleepDisturbanceScaleforChildren3
7Characterizessleepdisordersoverthepast6moinchildrenaged
5to
15y
Twenty-sixitemsthatroleinto6subscales:sleepinitiationand
maintenance,daytim
esleepiness,sleep
arousal,andsleep-
disordered
breathing
Parent
Family
InventoryofSleepHabits38
Autismspecificquestionnaireassessingsleephygieneinchildren
aged
3to10
yTwelve
items,includingdaytimeandprebedtim
ehabits,bedtim
eroutine,andsleepenvironm
ent
Parent
BehavioralEvaluationofDisordersofSleepScale3
9Assesses
sleepbehaviorsinchildrenaged
5to12
yFive
typesofsleepproblems:expressive
sleepdisturbances;
sensitivitytotheenvironm
ent;disorientedaw
akening;sleep
facilitators;andapnea/bruxism
Parent
BEARS1
7Assesses
5sleepdomains
inchildrenaged
5to18
yFivesleepdomains:bedtim
eproblems(difficulty
goingtobedand
falling
asleep);excessivedaytimesleepiness
(includes
behaviorstypically
associated
with
daytimesomnolencein
children);awakenings
during
thenight;regularityofsleep/
wakecycles
(bedtim
e,waketim
e)andaveragesleepduration;
andsnoring
Parent
Adolescent
SleepWakeScale4
0Assesses
sleepquality
inadolescentsaged
11to21
yTwenty-eight
itemsroleinto5subscales:goingtobed,falling
asleep,awakening,reinitiatingsleep,andwakefulness
Adolescent
BEARS,B=Bedtimeproblems,E=ExcessiveDaytimeSleepiness,A
=Aw
akenings
During
theNight,R=RegularityandDurationofSleep,S=Snoring.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S119 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
posttreatment. Both studies used mul-ticomponent treatments, although theyvaried with respect to the specificcomponents of treatment. However,they were representative of treatmentscommonly used in clinical practice aswell as supported as effective in thegeneral pediatric population. Bothstudies used extinction and positivereinforcement as treatments. Bothstudies provided parent training, asfollows: (1) identifying a treatmentgoal/treatment target for therapy; (2)discussion of how the sleep problem ismaintained by conditioning/learning;and (3) emphasis on establishing a de-velopmentally appropriate bedtimeand a consistent bedtime routine. Othertreatment components addressed in a
single study included sleep hygiene in-structions, use of effective instructions/directions to shape appropriate sleepbehavior, and use of the bedtime passprotocol.23 The studies did not addressrelative efficacy of these individual treat-ment components.
Complementary and alternative medi-cine therapies addressed in the litera-ture review include massage therapyand aromatherapy.33–35 The systematicreview found no evidence to supportthese therapies for insomnia in chil-dren who have ASD. Neither of thegraded studies examining the efficacyof massage therapy or aromatherapyfor insomnia in children who have ASDled to statistically significant improve-ments in sleep posttreatment.33–35
Results of the GuidelineDevelopment
Basedon the feasibility testing, a numberof observations resulted in the devel-opment of resources to assist cliniciansin theapplicationof thepracticepathway.After reviewing the literature and con-ducting pilot testing, the ATN SleepCommittee developed and refined theinsomniapracticepathwayandmade thefollowing consensus recommendations:
A. General pediatricians, family careproviders, and autism medical spe-cialists should screen all childrenwho have ASD for insomnia.
This screening is best done by askinga short series of questions targetinginsomnia, such as those from theCSHQ, and asking if the parent consid-ers these a problem. These questionsare: (1) child falls asleep within 20minutes after going to bed; (2) childfalls asleep in parent’s or sibling’s bed;(3) child sleeps too little; and (4) childawakens once during the night. Thesequestions were selected on the basisof review of the CSHQ and expert con-sensus. The ATN database was alsoreviewed (n = 4887), and we foundthat 81% of parents who reportedthat their child awakening more thanonce during the night was a problemalso answered affirmatively to thequestion “Does your child awaken onceduring the night?” Therefore, to limitthe questions asked, we did not in-clude “Does your child awaken morethan once during the night?” Askingspecific questions is essential becauseparents may not volunteer concernsabout insomnia given their concernswith behavioral issues (although theseissues may be secondary to the in-somnia). Identifying significant insom-nia is paramount given its impact ondaytime functioning, not only for thechild with ASD but also the family. Table2 lists available questionnaires.
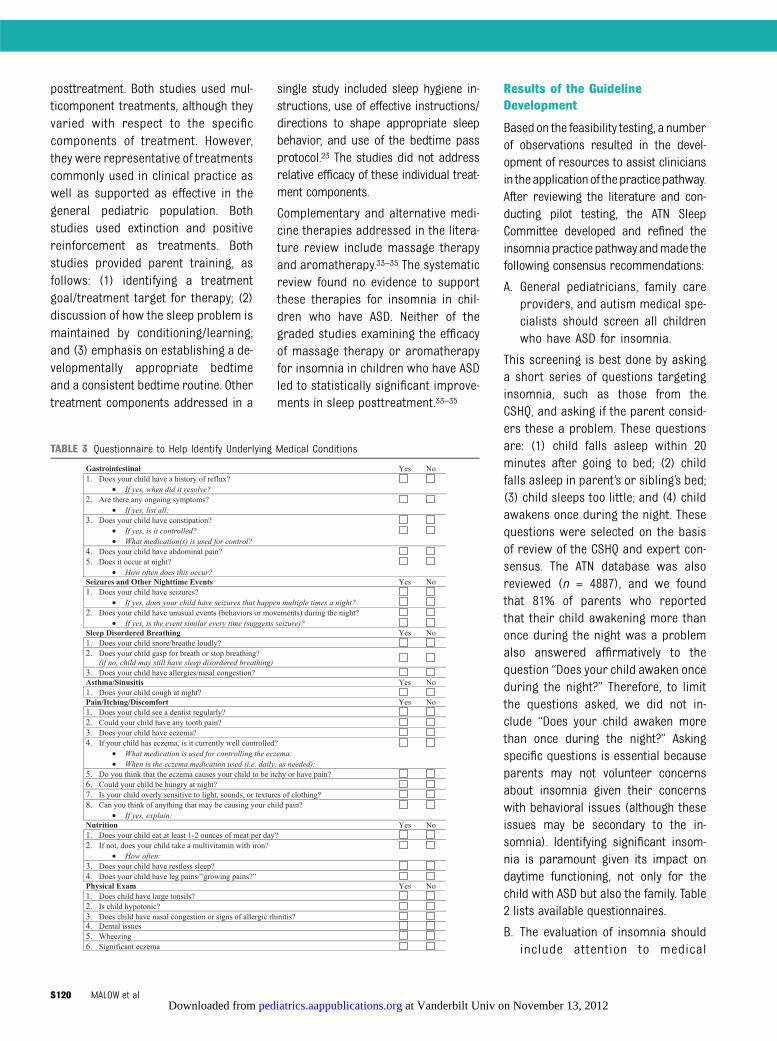
B. The evaluation of insomnia shouldinclude attention to medical
TABLE 3 Questionnaire to Help Identify Underlying Medical Conditions
S120 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

contributors that can affect sleep(including neurologic conditions andother sleep disorders that contrib-ute to insomnia).
These contributors should be ad-dressed because their treatment mayimprove insomnia. Within the ATN, wehave developed a list of questions formedical contributors, including gas-trointestinal disorders, epilepsy, pain,nutritional issues, and other under-lying sleep disorders responsible forinsomnia, including sleep-disoderedbreathing and restless legs symptoms(Table 3) that pediatricians can in-corporate within their review of sys-tems. Psychiatric conditions, such asanxiety, depression, and bipolar disor-der, should be considered becausethese may contribute to insomnia. Fi-nally, because many medications con-tribute to insomnia, a careful review ofmedications should be performed.
C. Educational/behavioral interventionsare the first line of treatment, afterexcluding medical contributors. How-ever, if an educational (behavioral)approach does not seem feasible,or the intensity of symptoms hasreached a crisis point, the use of phar-macologic treatment is considered.
Educational/behavioral approaches tothe treatment of insomnia are advo-cated as a first-line treatment in typi-cally developing children.21 In childrenwho have ASD, educational/behavioralapproaches are also recommended,especially because these children maynot be capable of expressing adverseeffects caused by the medications. Thecore behavioral deficits associatedwith ASD may impede the establish-ment of sound bedtime behaviors androutines. These include: (1) difficultywith emotional regulation (eg, ability tocalm self); (2) difficulty transitioningfrom preferred or stimulating activi-ties to sleep; and (3) deficits in com-munication skills affecting a child’sunderstanding of the expectations of
parents related to going to bed and fall-ing asleep. Conversely, given preferencesfor sameness and routine, children whohave ASD may adapt well to establish-ment of bedtime routines, especially ifvisual schedules are implemented.
The ATN has developed an educationaltoolkit for parents that consists ofpamphlets to promote good sleephabits; a survey to assess for habitsthat may interfere with sleep; samplebedtime routines, including a visualsupports library, tip sheets for imple-menting the bedtime routine, andmanaging night wakings; and a sleepdiary. The toolkit is being tested forfeasibility in an ongoing research pro-ject funded by the Health Resourcesand Services Administration of parentsleep education at 4 ATN sites and isalso being used in clinical practicethroughout the network. As with othereducational/behavioral approaches,the success of this toolkit depends onappropriate implementation by par-ents, with the guidance provided bypractitioners an essential element formany families. Families can often beencouraged to implement educational/behavioral strategies when presentedwith these tools, especially if they re-ceive hands-on instruction in the toolsand are providedwith an explanation ofwhy a behavioral approach is recom-mended. However, some families maybe in a state of crisis or may not bewilling or able to use the behavioraltools. These familiesmay be challengedby difficult daytime behaviors in theirchild or by financial concerns. Thesechildren might require pharmacologictreatment. In addition, practitionersmaynot be able to provide sufficient in-struction in the tools for a family to besuccessful with their implementation.Therefore, there is the option in thepractice pathway (Fig 2, Box 5b) ofmedication or consultation to a sleepspecialist if the family is unwilling orunable to use an educational approach,
depending on the comfort level of thepediatrician.
Behavioral Treatments for Insomnia
The behavioral treatments most com-monly used to treat insomnia in chil-dren who have ASD include behavioralmodification strategies such as extinc-tion (eg, withdrawal of reinforcementfor inappropriate bedtime behaviors)and positive reinforcement of adaptivesleep behavior. Sleep hygiene instruc-tions (eg, appropriate sleep schedulesand routines) often accompany behav-ioral modification protocols. Behavioralinterventions are effective in the treat-ment of insomnia in typically developingchildren.21 However, the evidence basefor effectiveness of such interventions inchildren who have ASD is limited. Thedata from the literature review providepreliminary support for the use of be-havioral modification to treat insomniain children who have ASD. These datawere the basis for the development of aneducational toolkit used to guide behav-ioral management of insomnia in theinsomnia practice pathway.
Alternative Treatments for Insomnia
The most common alternative therapywith a presence in the literature is mas-sage therapy.33,35 However, the results donot demonstrate consistent, statisticallysignificant improvements in sleep.
Pharmacologic Treatments forInsomnia
Although medications and supplementsare often used to treat insomnia experi-enced by children and adolescents whohave ASD, the evidence base for phar-macologic treatment is limited. At thistime, there are nomedications approvedby the US Food and Drug Administrationfor pediatric insomnia. The most evi-dence exists for the use of melatonin.
D. Clinicians should assure timelyfollow-up to monitor progress andresolution of insomnia.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S121 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

Assuring adequate follow-up is crucialwhen treating children who have ASDand significant insomnia. Follow-upshould occur within 2 weeks to 1month after beginning treatment. Theprovider and family should expect tosee some benefits and improvementswithin 4 weeks. Follow-up may be con-ducted by telephone or in person.Timely follow-up allows for fine-tuningof treatment interventions, support ofparents, and provision of referrals ifneeded. In addition to short-termfollow-up (eg, 1–2 months), at long-term follow-up (eg, 1-year visit) thesteps from the beginning of the prac-tice pathway should be repeated.
As outlined in the practice pathway,treatment of insomnia can be initiatedby the general pediatrician, primarycare provider, or autism medical spe-cialist. Many children will improve withthese initial interventions. Consultationwith a sleep specialist is indicated ifinsomnia is not improving with theseinitial interventions or when the in-somnia is particularly severe, causingsignificant daytime impairment orplacing the child at risk for harm whileawake during the night. For thosechildren who have ASD and are takingmultiple medications for sleep wheninitially assessed by the health careprovider, consultation with a sleepspecialist may be indicated, dependingon the comfort level of the provider.Other indications for consultation witha pediatric sleep specialist may includewhen underlying sleep disorders areresponsible for the sleeplessnesssymptoms (including sleep apnea,restless legs syndrome, periodic limbmovements of sleep, and unusual night-time behaviors [parasomnias] such assleepwalking or sleep terrors).
Results of the Field Testing
Results of the pilot phase indicatedchallenges in implementing the practicepathway due to a number of conflicts,
including: (1)competingdemandsonthepediatric provider in a busy clinicalpractice; (2) knowledge level of the pe-diatric provider; and (3) when consul-tation to the sleep specialist occurs,ensuring communication back to thepediatric provider.
In response to these barriers, we de-veloped the following resources: (1)a short set of screening questions forinsomnia as well as a checklist formedical conditions contributing to in-somnia (Table 3); and (2) a sleep edu-cation toolkit, available in hard copy aswell as on the internal ATN Web site(www.autismspeaks.org/atn) that willfacilitate parent teaching.
Additional issues were identified re-lated to provider comfort level in thefollowing areas: (1) assessing formedical or sleep contributors them-selves rather than referring to a spe-cialist, which led us to modify thepractice pathway to allow for bothoptions; (2) providing education tofamilies in use of the toolkit, which af-fected the length at which follow-upoccurred (eg, a second visit witha nurse educator might be needed fortoolkit implementation if the providerwas too busy to educate families at thetime of the initial clinic visit); and (3)treating insomnia with medications ontheir own versus referring to a sleepspecialist. When a child was referred tothe sleep specialist, ensuring that thesleep specialist communicated backto the provider regarding recommen-dations was also an issue related toapplying the practice pathway in ourfield testing, particularly as related tofollow-up care.
We modified the flow of the practicepathway in response to feedback dur-ing the field testing. Initially, the prac-tice pathway prioritized evaluationand treatment of medical contributorsbefore implementing educationalmeasures, such as the toolkit. However,based on the feedback of clinicians, the
evaluation/treatment of medical con-tributors and the implementation ofeducational measures became a paral-lel process as opposed to a sequential“first–then” approach.
DISCUSSION
We report here on the development ofa practice pathway for the evaluationand management of insomnia in chil-dren who have ASD. There are severalkey points of this practice pathway.First, general pediatricians, primarycare providers, and autism medicalspecialists should screen all childrenwho have ASD for insomnia becauseparents may not volunteer sleep con-cerns despite these concerns beingcontributors to medical comorbiditiesand behavioral issues. Second, theevaluation of insomnia should in-clude attention to medical contributorsthat can affect sleep, including othermedical problems that encompassgastrointestinal disorders, epilepsy,psychiatric comorbidities, medications,and sleep disorders including sleep-disordered breathing, restless legssyndrome (unpleasant sensations in thelegs associated with an urge to move),periodic limb movements of sleep(rhythmic leg kicks during sleep), andparasomnias (undesirable move-ments or behaviors during sleep,such as sleepwalking, sleep terrors, orconfusional arousals). In parallel withthis screening, the need for therapeu-tic intervention should be determined.We also determined that educational/behavioral interventions are the firstline of treatment, after excludingmedical contributors. If an educa-tional (behavioral) approach does notseem feasible, or the intensity ofsymptoms has reached a crisis point,the use of pharmacologic treat-ment is considered. Finally, cliniciansshould assure timely follow-up tomonitor progress and resolution ofinsomnia.
S122 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

This practice pathway expands the lit-erature that currently exists for typi-cally developing children related toscreening and management.5,7–9 Therationale for developing a practicepathway that uniquely addresses thispopulation is because children whohave ASD, and their families, haveunique needs. For example, medical,neurologic, and psychiatric comorbid-ities are common in children who haveASD, as is the use of medications thatinfluence sleep. In addition, parents ofchildren who have ASD, struggling withthe stressors related to their child’sdisability and the often accompanyingbehavioral challenges, may not volun-teer sleep to be of concern. In turn,pediatric providers may not ask aboutsleep due to competing medical andbehavioral issues. Furthermore, sleepproblems are more common in chil-dren who have ASD than in childrenof typical development,2,3 and theirtreatment may impact favorably ondaytime behavior and family function-ing. Given these factors, we do recog-nize that children who have otherdisorders of neurodevelopment couldalso benefit from this practice pathway,as they share common features withchildren who have ASD, including
comorbid conditions, parental stres-sors, and prevalent sleep problems.
The systematic review of the availabletreatment literature allowed for therecognition that evidence-based stan-dards for the behavioral, pharmaco-logic, and other treatments of insomniain ASD are not yet available. Thus, muchof these guidelines reflect expertopinion given the absence of data. Ad-ditional studies are needed to establishthe efficacy and safety of supplementalmelatonin, as well as other pharma-cologic agents, in large RCTs. Similarstudies are needed to address the ef-ficacy of parent-based sleep educa-tional programs to address insomnia,as well as the combination of theseeducational programs with pharma-cologic strategies. Finally, the roleof nonpharmacologic methods (apartfrom educational therapies) warrantsstudy as well. As additional researchstudies are performed, the clinicalpathwaywill likely requiremodification.However, it is expected that the over-arching approach to insomnia in thechild who has ASD will not change. Al-though the practice pathway waspiloted at 4 ATN sites, the next stepsinvolve the wide dissemination ofthe practice pathway into pediatric
practices. We would also like to developa practice pathway for nonmedicalhealth professionals who are likely toprovide behavioral interventions, in-cluding psychologists.
Strengths of the study include the gath-ering of the following groups: experts insleep medicine from a variety of dis-ciplines, including neurology, psychiatry,pulmonary medicine, and psychology;engaged pediatricians specializingin ASD; and parents of children whohave ASD. Weaknesses include limitedevidence-basedstudiesonwhich tobasethe practice pathway, making it neces-sary to rely on expert opinion.
CONCLUSIONS
The practice pathway regarding theidentification of insomnia in childrenwho have ASD requires future fieldtesting in clinical settings but repre-sents a starting point to managing in-somnia in a growing population ofchildren with the most commonneurodevelopmental disability.
ACKNOWLEDGMENTThevaluableassistanceof themembersof the ATN Sleep Committee in re-viewing this document is gratefullyacknowledged.
REFERENCES
1. American Psychiatric Association. Di-agnostic and Statistical Manual of MentalDisorders, Revised. 4th ed. Washington,DC: American Psychiatric Association;2000
2. Couturier JL, Speechley KN, Steele M, NormanR, Stringer B, Nicolson R. Parental perceptionof sleep problems in children of normal intel-ligence with pervasive developmental dis-orders: prevalence, severity, and pattern. J AmAcad Child Adolesc Psychiatry. 2005;44(8):815–822
3. Krakowiak P, Goodlin-Jones B, Hertz-Picciotto I, Croen LA, Hansen RL. Sleepproblems in children with autism spec-trum disorders, developmental delays, andtypical development: a population-basedstudy. J Sleep Res. 2008;17(2):197–206
4. American Academy of Sleep Medicine. In-ternational Classification of Sleep Disorders.Diagnostic and Coding Manual. 2nd ed.Westchester, IL: American Academy of SleepMedicine; 2005
5. Armstrong KL, Quinn RA, Dadds MR. Thesleep patterns of normal children. Med JAust. 1994;161(3):202–206
6. Johnson KP, Malow BA. Assessment andpharmacologic treatment of sleep distur-bance in autism. Child Adolesc PsychiatrClin N Am. 2008;17(4):773–785, viii
7. Kataria S, Swanson MS, Trevathan GE. Per-sistence of sleep disturbances in preschoolchildren. J Pediatr. 1987;110(4):642–646
8. Pollock JI. Night-waking at five years of age:predictors and prognosis. J Child PsycholPsychiatry. 1994;35(4):699–708
9. Zuckerman B, Stevenson J, Bailey V. Sleepproblems in early childhood: continuities,predictive factors, and behavioral corre-lates. Pediatrics. 1987;80(5):664–671
10. Wiggs L, Stores G. Severe sleep disturbanceand daytime challenging behaviour inchildren with severe learning disabilities. JIntellect Disabil Res. 1996;40(pt 6):518–528
11. Wiggs L, Stores G. Behavioural treatment forsleep problems in children with severelearning disabilities and challenging daytimebehaviour: effect on daytime behaviour.J Child Psychol Psychiatry. 1999;40(4):627–635
12. Meltzer LJ, Johnson C, Crosette J, Ramos M,Mindell JA. Prevalence of diagnosed sleepdisorders in pediatric primary care practices.Pediatrics. 2010;125(6). Available at: www.pediatrics.org/cgi/content/full/125/6/e1410
SUPPLEMENT ARTICLE
PEDIATRICS Volume 130, Supplement 2, November 2012 S123 at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

13. Meissner HH, Riemer A, Santiago SM, SteinM, Goldman MD, Williams AJ. Failure ofphysician documentation of sleep com-plaints in hospitalized patients. West J Med.1998;169(3):146–149
14. Owens JA. The practice of pediatric sleepmedicine: results of a community survey.Pediatrics. 2001;108(3). Available at: www.pediatrics.org/cgi/content/full/108/3/E51
15. Blunden S, Lushington K, Lorenzen B, Ooi T,Fung F, Kennedy D. Are sleep problemsunder-recognised in general practice? ArchDis Child. 2004;89(8):708–712
16. Schreck KA, Richdale AL. Knowledge ofchildhood sleep: a possible variable in un-der or misdiagnosis of childhood sleepproblems. J Sleep Res. 2011;20(4):589–597
17. Owens JA, Dalzell V. Use of the ‘BEARS’ sleepscreening tool in a pediatric residents’continuity clinic: a pilot study. Sleep Med.2005;6(1):63–69
18. Mindell JA, Kuhn B, Lewin DS, Meltzer LJ,Sadeh A; American Academy of Sleep Medi-cine. Behavioral treatment of bedtime prob-lems and night wakings in infants and youngchildren. Sleep. 2006;29(10):1263–1276
19. Mindell JA. Empirically supported treat-ments in pediatric psychology: bedtimerefusal and night wakings in young chil-dren. J Pediatr Psychol. 1999;24(6):465–481
20. Kuhn BR, Elliott AJ. Treatment efficacy inbehavioral pediatric sleep medicine. JPsychosom Res. 2003;54(6):587–597
21. Morgenthaler TI, Owens J, Alessi C, et al;American Academy of Sleep Medicine.Practice parameters for behavioral treat-ment of bedtime problems and night wak-ings in infants and young children. Sleep.2006;29(10):1277–1281
22. Reynolds AM, Malow BA. Sleep and autismspectrum disorders. Pediatr Clin North Am.2011;58(3):685–698
23. Goodlin-Jones BL, Sitnick SL, Tang K, Liu J,Anders TF. The Children’s Sleep Habits Ques-tionnaire in toddlers and preschool children.J Dev Behav Pediatr. 2008;29(2):82–88
24. Guyatt GH, Oxman AD, Vist GE, et al; GRADEWorking Group. GRADE: an emerging con-sensus on rating quality of evidence andstrength of recommendations. BMJ. 2008;336(7650):924–926
25. Owens JA, Moturi S. Pharmacologic treat-ment of pediatric insomnia. Child AdolescPsychiatr Clin N Am. 2009;18(4):1001–1016
26. Mindell JA, Emslie G, Blumer J, et al. Phar-macologic management of insomnia in chil-dren and adolescents: consensus statement.Pediatrics. 2006;117(6). Available at: www.pediatrics.org/cgi/content/full/117/6/e1223
27. Garstang J, Wallis M. Randomized con-trolled trial of melatonin for children with
autistic spectrum disorders and sleepproblems. Child Care Health Dev. 2006;32(5):585–589
28. Wirojanan J, Jacquemont S, Diaz R, et al.The efficacy of melatonin for sleep prob-lems in children with autism, fragile Xsyndrome, or autism and fragile X syn-drome. J Clin Sleep Med. 2009;5(2):145–150
29. Wasdell MB, Jan JE, Bomben MM, et al. Arandomized, placebo-controlled trial ofcontrolled release melatonin treatment ofdelayed sleep phase syndrome and im-paired sleep maintenance in children withneurodevelopmental disabilities. J PinealRes. 2008;44(1):57–64
30. Andersen IM, Kaczmarska J, McGrew SG,Malow BA. Melatonin for insomnia in chil-dren with autism spectrum disorders.J Child Neurol. 2008;23(5):482–485
31. Reed HE, McGrew SG, Artibee K, et al. Parent-based sleep education workshops in autism.J Child Neurol. 2009;24(8):936–945
32. Weiskop S, Richdale A, Matthews J. Behav-ioural treatment to reduce sleep problems inchildren with autism or fragile X syndrome.Dev Med Child Neurol. 2005;47(2):94–104
33. Piravej K, Tangtrongchitr P, Chandarasiri P,Paothong L, Sukprasong S. Effects of Thaitraditional massage on autistic children’sbehavior. J Altern Complement Med. 2009;15(12):1355–1361
34. Williams TI. Evaluating effects of aroma-therapy massage on sleep in children withautism: a pilot study. Evid Based Comple-ment Alternat Med. 2006;3(3):373–377
35. Escalona A, Field T, Singer-Strunck R, CullenC, Hartshorn K. Brief report: improvementsin the behavior of children with autismfollowing massage therapy. J Autism DevDisord. 2001;31(5):513–516
36. Owens JA, Spirito A, McGuinn M. TheChildren’s Sleep Habits Questionnaire(CSHQ): psychometric properties of a sur-vey instrument for school-aged children.Sleep. 2000;23(8):1043–1051
37. Bruni O, Ottaviano S, Guidetti V, et al. TheSleep Disturbance Scale for Children(SDSC). Construction and validation of aninstrument to evaluate sleep disturbancesin childhood and adolescence. J Sleep Res.1996;5(4):251–261
38. Malow BA, Crowe C, Henderson L, et al. Asleep habits questionnaire for childrenwith autism spectrum disorders. J ChildNeurol. 2009;24(1):19–24
39. Schreck KA, Mulick JA, Rojahn J. Devel-opment of the behavioral evaluation of dis-orders of sleep scale. J Child Fam Stud. 2003;12(3):349–359 doi:10.1023/A:1023995912428
40. LeBourgeois MK, Giannotti F, Cortesi F,Wolfson AR, Harsh J. The relationship
between reported sleep quality and sleephygiene in Italian and American adolescents.Pediatrics. 2005;115(suppl 1):257–265
41. Aman MG, Arnold LE, McDougle CJ, et al.Acute and long-term safety and tolerabilityof risperidone in children with autism.J Child Adolesc Psychopharmacol. 2005;15(6):869–884
42. Honomichl RD, Goodlin-Jones BL, BurnhamMM, Hansen RL, Anders TF. Secretin andsleep in children with autism. Child Psy-chiatry Hum Dev. 2002;33(2):107–123
43. Ellaway CJ, Peat J, Williams K, Leonard H,Christodoulou J. Medium-term open labeltrial of L-carnitine in Rett syndrome. BrainDev. 2001;23(suppl 1):S85–S89
44. Posey DJ, Guenin KD, Kohn AE, Swiezy NB,McDougle CJ. A naturalistic open-label studyof mirtazapine in autistic and other perva-sive developmental disorders. J Child Ado-lesc Psychopharmacol. 2001;11(3):267–277
45. Rossi PG, Posar A, Parmeggiani A, PipitoneE, D’Agata M. Niaprazine in the treatment ofautistic disorder. J Child Neurol. 1999;14(8):547–550
46. Ming X, Gordon E, Kang N, Wagner GC. Use ofclonidine in children with autism spectrumdisorders. Brain Dev. 2008;30(7):454–460
47. Adams JB, Holloway C. Pilot study ofa moderate dose multivitamin/mineralsupplement for children with autisticspectrum disorder. J Altern ComplementMed. 2004;10(6):1033–1039
48. Dosman CF, Brian JA, Drmic IE, et al. Chil-dren with autism: effect of iron supple-mentation on sleep and ferritin. PediatrNeurol. 2007;36(3):152–158
49. Wright B, Sims D, Smart S, et al. Melatoninversus placebo in children with autismspectrum conditions and severe sleepproblems not amenable to behaviourmanagement strategies: a randomisedcontrolled crossover trial. J Autism DevDisord. 2011;41(2):175–184
50. Paavonen EJ, Nieminen-von Wendt T, VanhalaR, Aronen ET, von Wendt L. Effectiveness ofmelatonin in the treatment of sleep dis-turbances in children with Asperger disor-der. J Child Adolesc Psychopharmacol. 2003;13(1):83–95
51. Giannotti F, Cortesi F, Cerquiglini A,Bernabei P. An open-label study of controlled-release melatonin in treatment of sleepdisorders in children with autism. J AutismDev Disord. 2006;36(6):741–752
52. Malow B, Adkins KW, McGrew SG, et al. Mel-atonin for sleep in children with autism:a controlled trial examining dose, tolerability,and outcomes [published correction appearsin J Autism Dev Disord. 2012;42(8):1738].J Autism Dev Disord. 2012;42(8):1729–1737
S124 MALOW et al at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2012-0900I 2012;130;S106Pediatrics
Goldman, Rebecca Panzer, Daniel L. Coury and Dan G. GlazeBeth A. Malow, Kelly Byars, Kyle Johnson, Shelly Weiss, Pilar Bernal, Suzanne E.
Insomnia in Children and Adolescents With Autism Spectrum DisordersA Practice Pathway for the Identification, Evaluation, and Management of
ServicesUpdated Information &
_2/S106.full.htmlhttp://pediatrics.aappublications.org/content/130/Supplementincluding high resolution figures, can be found at:
References
_2/S106.full.html#ref-list-1http://pediatrics.aappublications.org/content/130/Supplementat:This article cites 49 articles, 11 of which can be accessed free
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Vanderbilt Univ on November 13, 2012pediatrics.aappublications.orgDownloaded from
Related Documents











