Review A phase II, single-arm multicenter study of low-dose rituximab for refractory mixed cryoglobulinemia secondary to hepatitis C virus infection Marcella Visentini a, ⁎, Serena Ludovisi b , Antonio Petrarca c , Federica Pulvirenti a , Marco Zaramella b , Monica Monti c , Valentina Conti a , Jessica Ranieri c , Stefania Colantuono a , Elisa Fognani c , Alessia Piluso c , Carmine Tinelli d , Anna Linda Zignego c , Mario U. Mondelli b , Massimo Fiorilli a , Milvia Casato a a Department of Clinical Immunology, Sapienza University of Rome, Rome, Italy b Infectious Diseases Research Laboratories, Policlinico San Matteo, University of Pavia, Pavia, Italy c Research Center for Systemic Manifestations of Hepatitis Viruses, Department of Internal Medicine, University of Firenze, Firenze, Italy d Biometrics Unit, IRCCS Policlinico San Matteo Foundation, Pavia, Italy abstract article info Available online 5 May 2011 Keywords: Mixed cryoglobulinemia HCV Rituximab Eradication of hepatitis C virus (HCV) by antiviral therapy is the treatment of choice for mixed cryoglobulinemia secondary to this infection, but many patients fail to achieve sustained viral responses and need second-line treatments. Several studies have demonstrated that the infusion of the anti-CD20 monoclonal antibody rituximab is highly effective for refractory mixed cryoglobulinemia, with a clinical response in approximately 80% of patients, although the relapse rate is high. Virtually all published studies employed a rituximab dosage of 375 mg/m 2 given four times, a schedule used for treating non-Hodgkin's lymphomas. Based on a prior pilot study, we designed a phase II single-arm two-stage study (EUDRACT n. 2008-000086-38) to evaluate the efficacy of a lower dosage of rituximab, 250 mg/m 2 given twice, for refractory mixed cryoglobulinemia. We present here the preliminary results in the first 27 patients enrolled. The overall response rate in 24 evaluable patients was 79%, and the mean time to relapse was 6.5 months, similar to the 6.7 months reported in studies with high-dose rituximab. Side effects were comparable to those seen in patients treated with high-dose. Increase of HCV viral load, reported in some high-dose studies, was not observed in our patients. Low-dose rituximab may provide a more cost/effective and possibly safer alternative for treating refractory HCV-associated mixed cryoglobulinemia. © 2011 Elsevier B.V. All rights reserved. Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 2. Patients and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 2.1. Patients and study design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 2.2. Laboratory studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 2.3. Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 3.1. Patient population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 3.2. Clinical response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 716 3.3. Laboratory response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 717 3.4. Adverse events and safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 717 4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 717 Take-home messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718 Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718 Autoimmunity Reviews 10 (2011) 714–719 ⁎ Corresponding author at: Department of Clinical Immunology, Sapienza University of Rome, Viale dell'Università 37, 00185 Rome, Italy. Tel.: + 39 3396696011; fax: + 39 6 4463877. E-mail address: [email protected] (M. Visentini). 1568-9972/$ – see front matter © 2011 Elsevier B.V. All rights reserved. doi:10.1016/j.autrev.2011.04.033 Contents lists available at ScienceDirect Autoimmunity Reviews journal homepage: www.elsevier.com/locate/autrev

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Autoimmunity Reviews 10 (2011) 714–719
Contents lists available at ScienceDirect
Autoimmunity Reviews
j ourna l homepage: www.e lsev ie r.com/ locate /aut rev
Review
A phase II, single-arm multicenter study of low-dose rituximab for refractory mixedcryoglobulinemia secondary to hepatitis C virus infection
Marcella Visentini a,⁎, Serena Ludovisi b, Antonio Petrarca c, Federica Pulvirenti a, Marco Zaramella b,Monica Monti c, Valentina Conti a, Jessica Ranieri c, Stefania Colantuono a, Elisa Fognani c, Alessia Piluso c,Carmine Tinelli d, Anna Linda Zignego c, Mario U. Mondelli b, Massimo Fiorilli a, Milvia Casato a
a Department of Clinical Immunology, Sapienza University of Rome, Rome, Italyb Infectious Diseases Research Laboratories, Policlinico San Matteo, University of Pavia, Pavia, Italyc Research Center for Systemic Manifestations of Hepatitis Viruses, Department of Internal Medicine, University of Firenze, Firenze, Italyd Biometrics Unit, IRCCS Policlinico San Matteo Foundation, Pavia, Italy
⁎ Corresponding author at: Department of Clinical Im6 4463877.
E-mail address: [email protected] (M.
1568-9972/$ – see front matter © 2011 Elsevier B.V. Adoi:10.1016/j.autrev.2011.04.033
a b s t r a c t
a r t i c l e i n f oAvailable online 5 May 2011
Keywords:Mixed cryoglobulinemiaHCVRituximab
Eradication of hepatitis C virus (HCV) by antiviral therapy is the treatment of choice for mixedcryoglobulinemia secondary to this infection, but many patients fail to achieve sustained viral responsesand need second-line treatments. Several studies have demonstrated that the infusion of the anti-CD20monoclonal antibody rituximab is highly effective for refractory mixed cryoglobulinemia, with a clinicalresponse in approximately 80% of patients, although the relapse rate is high. Virtually all published studiesemployed a rituximab dosage of 375 mg/m2 given four times, a schedule used for treating non-Hodgkin'slymphomas. Based on a prior pilot study, we designed a phase II single-arm two-stage study (EUDRACT n.2008-000086-38) to evaluate the efficacy of a lower dosage of rituximab, 250 mg/m2 given twice, forrefractory mixed cryoglobulinemia. We present here the preliminary results in the first 27 patients enrolled.The overall response rate in 24 evaluable patients was 79%, and the mean time to relapse was 6.5 months,similar to the 6.7 months reported in studies with high-dose rituximab. Side effects were comparable to thoseseen in patients treated with high-dose. Increase of HCV viral load, reported in some high-dose studies, wasnot observed in our patients. Low-dose rituximab may provide a more cost/effective and possibly saferalternative for treating refractory HCV-associated mixed cryoglobulinemia.
munology, Sapienza University of Rome, Viale dell'Un
Visentini).
ll rights reserved.
© 2011 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7152. Patients and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715
2.1. Patients and study design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7152.2. Laboratory studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7152.3. Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7153.1. Patient population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7153.2. Clinical response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7163.3. Laboratory response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7173.4. Adverse events and safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 717
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 717Take-home messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 718
iversità 37, 00185 Rome, Italy. Tel.: +39 3396696011; fax: +39

715M. Visentini et al. / Autoimmunity Reviews 10 (2011) 714–719
1. Introduction
Hepatitis C virus (HCV)-associated mixed cryoglobulinemia is asystemic vasculitis characterized by the deposition of immunecomplexes formed by IgM rheumatoid factor and endogenous IgG[1]. The clinical manifestations range from a mild form with purpura,arthralgia and fatigue to a more severe form responsible for progres-sive renal disease, skin ulcers and debilitating peripheral neuropathy[2]. As mixed cryoglobulinemia is considered as a benign lympho-prolipherative disorder, characterized in most of the patients by anexpansion of monoclonal IgMk B cells [3], it is not surprising that ~10%of these patients develop over time non-Hodgkin's lymphoma (NHL)[4]. Translocation t(14;18) bcl-2/IgH is suspected to play a role inmixed cryoglobulinemia-associated lymphomagenesis [5,6].
Eradication of HCV with pegylated interferon alpha (PEG-IFN) andribavirin is currently considered the first-choice treatment for mixedcryoglobulinemia [7,8]. Unfortunately, many patients present contra-indications to therapy, fail to respond or relapse after initial response.A number of studies [9–16] have demonstrated that the anti-CD20chimeric monoclonal antibody rituximab is highly effective for re-fractory mixed cryoglobulinemia. Moreover, association of rituximabwith antivirals (PEG-IFN plus ribavirin)may induce a better and fasterclinical remission [17,18]. The rituximab dosage used in nearly allpublished reports was 375 mg/m2 given four times, the treatmentschedule used for B cell NHL.
The number and severity of side effects of rituximab in patientswith cryoglobulinemia appears to be overall moderate, althoughSène et al. [15] reported more frequent adverse events in patientstreated with higher doses. Cacoub et al. [19] recommend caution incryoglobulinemia patients because most data on side effects comefrom small series on short-term follow-up, and data on adverse effectson HCV load and liver enzymes are particularly scarce.
We recently reported [20] 6 patients with HCV-associated mixedcryoglobulinemia that were treated with a low dosage of rituximab,250 mg/m2 given twice, because of associated clinical conditionswarning against a high dosage. A clinical and laboratory response wasnoted in 4 of 5 evaluable patients. Based on this preliminary ob-servation, we designed a phase II, single-arm two-stage multicenterstudy to evaluate the efficacy of low-dose rituximab in patients withrefractory HCV-associated mixed cryoglobulinemia. The clinicalresponse rates, laboratory findings and side effects in our patientpopulation were compared with the available literature data. Ourpresent results in 27 patients support the concept that low-doserituximab is equally effective as high-dose rituximab in this disorder.Thus, low-dose rituximab may provide a less expensive and possiblysafer alternative for treating refractory mixed cryoglobulinemia.
2. Patients and methods
2.1. Patients and study design
Three University centers (Sapienza University of Rome, Universityof Florence, and University of Pavia) participated to this study. Thisstudy (EUDRACT n. 2008-000086-38) was approved by the InternalReview Boards of the participating Institutions. A written informedconsent was obtained from each patient, according to the ethicalguidelines of the Declaration of Helsinki.
Twenty-sevenconsecutive, unselectedpatientswithHCV-associatedtype IImixed cryoglobulinemia vasculitiswere enrolled. All patients hadfailed to respond to or had relapsed after standard-of-care (SoC) anti-HCV therapy with Peg-IFNα plus ribavirin, or had contraindication totreatment. Patients previously treated with rituximab were excluded.Rituximab, 250 mg/m2, was given twice at one-week interval afterpremedication with methylprednisolone 1 mg/kg, paracetamol 1 g andchlopheniramine 10 mg.
Clinical and laboratory datawere evaluatedmonthly for 12 monthsafter rituximab infusion; the response rates were analyzed at months3, 6, 9 and 12. Vasculitis activity was evaluated by the BirminghamVasculitis Activity Score (BVAS) [22]. This index provides a total scoreof clinical disease activity in nine separate organs (maximum63pointsfor present symptoms and 32 points for new or worse symptoms). Aclinical response to treatment was defined as complete for BVAS=0,and as partial response for a BVAS b50% of the baseline. Immunologicalresponse was defined as a decrease of cryocrit to less than 50% ofbaseline level. Response to treatment was classified on the basis ofcombined clinical and immunological parameters: a complete re-sponse was defined as BVAS=0 and cryocrit b50% of the baseline; apartial responsewas defined as BVAS b50% of the baseline and cryocritb50% of the baseline. At month 3 the response was evaluated only onthe basis of clinical parameters, since reduction of cryoglobulins oftenoccurs slowly after rituximab [10]. Relapsewas defined as any increasein the BVAS score after response.
2.2. Laboratory studies
All blood samples were drawn with pre-warmed syringes andtubes, allowed to clot and centrifuged at 37 °C for serum separation.Sera were kept at 4 °C for 7 days and cryocrit was expressed as apercentage after centrifugation. The number of circulating B-cells wasmeasured by four-color flow cytometry in fresh blood samples usingantibodies to CD19, CD20, kappa- and lambda-chain fluochrome-conjugated antibodies (Becton Dickinson). B cell depletion wasdefined as a value of circulating B cells ≤5/μl. The presence ofperipheral blood mononuclear cells carrying t(14;18) bcl-2/IgHtranslocation was detected by a “nested” PCR method (MBR bcl-2/JH PCR) on total DNA, as previously described [5]. Serum HCV RNAwas measured by the Amplicor HCV assay (Roche Diagnostics). Bloodsamples were processed at rigorously controlled temperature, aspreviously described [21], to avoid the co-precipitation of virionswith cryoglobulins.
2.3. Statistical analysis
Sample size was estimated by the Simon's optimal two-stagedesign procedure, with 16 patients entering the first stage of thestudy; a minimum of 5/16 responders at week 12 was required forcontinuing enrolment up to the planned final number of 52 patients.All activity and safety variables were summarized using descriptivemethods. Number of cases, mean, standard deviation, median, per-centiles, minimum and maximum were calculated for each quantita-tive variable. Frequency and percentage were used to summarizecategory variables. The relapse free survival was estimated bythe Kaplan–Meier method. Differences were analyzed with non-parametric methods; a P value≤0.05 was considered statisticallysignificant.
3. Results
3.1. Patient population
Patients' demographic and clinical characteristics are summarizedin Table 1. Twenty-seven patients with mixed cryoglobulinemiavasculitis and positive HCV serology were included; in 4 patientsHCV RNA was repeatedly negative both in whole serum and in thecryoprecipitate. Of the 23 viremic patients, 14 had genotype 1 and 9genotype 2. Ten patients (37%) had elevated serum alanine amino-transferase (ALT) levels. Purpura and peripheral neuropathy were themost frequentmanifestations of cryoglobulinemic vasculitis (Table 1).A 64-y old female patient had a low-grade NHL, diagnosed by a bonemarrow biopsy.

Table 1Demographic and clinical characteristics of 27 patients with HCV-associated cryoglo-bulinemia vasculitis before rituximab therapy.
Parameter Value
Age (years), median (range) 70 (54–81)Female sex (% of patients) 74Duration of vasculitis (months), median (range) 46 (6–132)BVAS value, median (range) 13 (5–22)Purpura (% of patients) 89Skin ulcers (% of patients) 33Neuropathy (% of patients) 85Nephropathy (% of patients) 48Arthralgia (% of patients) 70Cryocrit (%), median (range) 7 (1–45)Serum C4 (mg/dL), median (range) 7 (0–29)ALT (IU/L), median (range) 32 (10–115)HCV load (copies/mL), median (range) 4.7×105 (56–2.5×107)t(14;18) (% of positive patients) 48
716 M. Visentini et al. / Autoimmunity Reviews 10 (2011) 714–719
All patients were either non-responders (n=7) or relapsers(n=3) or not amenable (n=13) to SoC therapy. Two patients werenot treated because they had persistently negative HCV RNA andnormal ALT levels. Two patients had sustained virological responses(SVR) but continued to have cryoglobulinemia and active vasculitis,and one of them had associated low-grade NHL. Persistence ofcryoglobulinemia in patients with SVR was previously described,particularly in those with underlying B cell lymphoma [23]. Previous
Fig. 1. Clinical and laboratory data at different time points after rituximab infusion. (A) Numdenote, at month 3, the number of non-responders, or, at months 6 and 12, the number of patcryocrit and circulating B cells in responders (complete plus partial). The number of patientsmean values, and lines the standard deviations.
treatments included plasmapheresis (8 patients), low-dose steroids(25 patients) and cyclophosphamide (6 patients).
3.2. Clinical response
Of the 27 patients enrolled in this study, 3 were not evaluable; onepatient was lost to follow-up after completion of rituximab therapy,one patient died of myocardial infarction two months after therapy,while the third could not complete treatment because of a severeadverse reaction that occurred at the beginning of the first infusion ofrituximab. Of 24 evaluable patients 18 did not reach the end of follow-up at month 12, either because they were still on follow-up at themoment of writing this report (5 patients), or because they were non-responders (5 patients) or relapsers (8 patients) and were thereforetreated with additional therapies. All 6 long-term responderscompleted a 12-month follow-up.
Three months after rituximab infusion, 79% (19/24) of the patientswere defined as clinical responders (complete plus partial) (Fig. 1A).Three patients (12%) achieved a complete clinical response(BVAS=0), and 16 patients (67%) a partial clinical response (BVASb50% of baseline). The patient with low-grade NHL had a partialresponse and relapsed at month 7 (purpura and neuropathy). Overall,the BVAS value decreased from 13.9 pre-therapy to 4.2 at month3 (p=0.0001 by Wilcoxon signed rank test) (Fig. 1B).
At month 6 there were 13 responders; 2 partial responders hadnot yet reached this time point, whereas 4 patients had relapsed. At
ber of patients with complete (open bars) or partial (gray bars) responses. Closed barsients who relapsed betweenmonths 3–6 and 6–12, respectively. (B,C,D) Values of BVAS,at each time point is indicated in (B), and is the same as in (C) and (D). Bars denote the
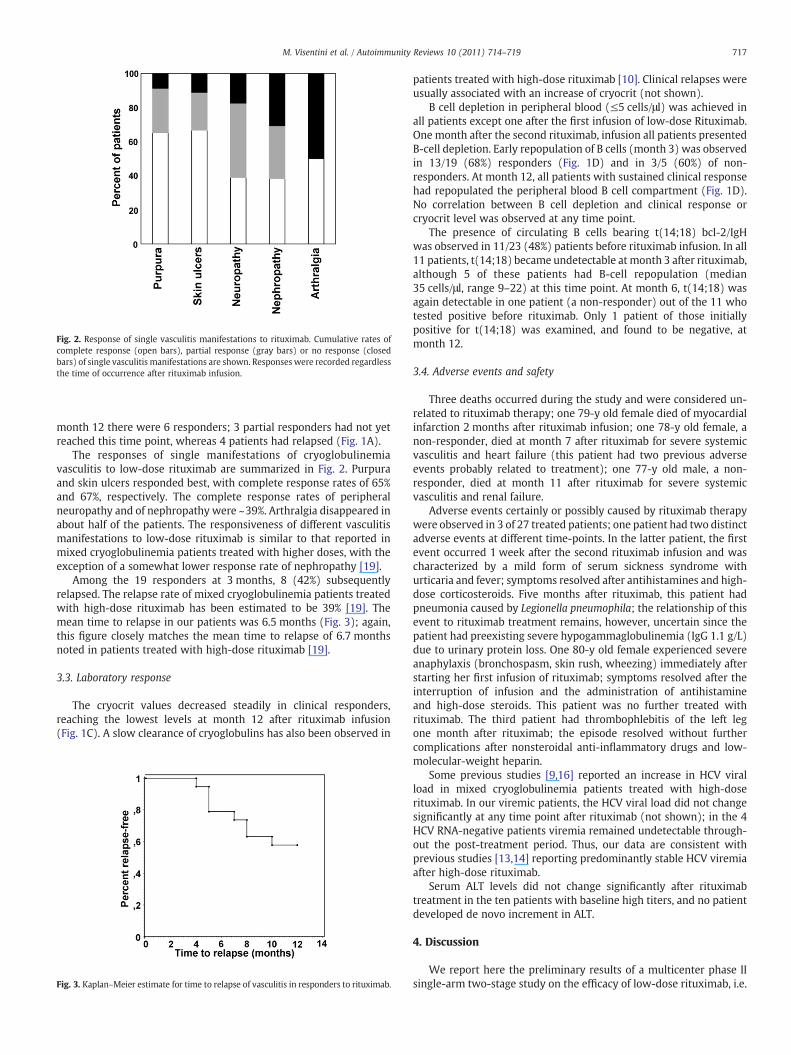
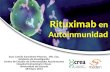
Fig. 2. Response of single vasculitis manifestations to rituximab. Cumulative rates ofcomplete response (open bars), partial response (gray bars) or no response (closedbars) of single vasculitis manifestations are shown. Responses were recorded regardlessthe time of occurrence after rituximab infusion.
717M. Visentini et al. / Autoimmunity Reviews 10 (2011) 714–719
month 12 there were 6 responders; 3 partial responders had not yetreached this time point, whereas 4 patients had relapsed (Fig. 1A).
The responses of single manifestations of cryoglobulinemiavasculitis to low-dose rituximab are summarized in Fig. 2. Purpuraand skin ulcers responded best, with complete response rates of 65%and 67%, respectively. The complete response rates of peripheralneuropathy and of nephropathy were ~39%. Arthralgia disappeared inabout half of the patients. The responsiveness of different vasculitismanifestations to low-dose rituximab is similar to that reported inmixed cryoglobulinemia patients treated with higher doses, with theexception of a somewhat lower response rate of nephropathy [19].
Among the 19 responders at 3 months, 8 (42%) subsequentlyrelapsed. The relapse rate of mixed cryoglobulinemia patients treatedwith high-dose rituximab has been estimated to be 39% [19]. Themean time to relapse in our patients was 6.5 months (Fig. 3); again,this figure closely matches the mean time to relapse of 6.7 monthsnoted in patients treated with high-dose rituximab [19].
3.3. Laboratory response
The cryocrit values decreased steadily in clinical responders,reaching the lowest levels at month 12 after rituximab infusion(Fig. 1C). A slow clearance of cryoglobulins has also been observed in
Fig. 3. Kaplan–Meier estimate for time to relapse of vasculitis in responders to rituximab.
patients treated with high-dose rituximab [10]. Clinical relapses wereusually associated with an increase of cryocrit (not shown).
B cell depletion in peripheral blood (≤5 cells/μl) was achieved inall patients except one after the first infusion of low-dose Rituximab.One month after the second rituximab, infusion all patients presentedB-cell depletion. Early repopulation of B cells (month 3) was observedin 13/19 (68%) responders (Fig. 1D) and in 3/5 (60%) of non-responders. At month 12, all patients with sustained clinical responsehad repopulated the peripheral blood B cell compartment (Fig. 1D).No correlation between B cell depletion and clinical response orcryocrit level was observed at any time point.
The presence of circulating B cells bearing t(14;18) bcl-2/IgHwas observed in 11/23 (48%) patients before rituximab infusion. In all11 patients, t(14;18) became undetectable at month 3 after rituximab,although 5 of these patients had B-cell repopulation (median35 cells/μl, range 9–22) at this time point. At month 6, t(14;18) wasagain detectable in one patient (a non-responder) out of the 11 whotested positive before rituximab. Only 1 patient of those initiallypositive for t(14;18) was examined, and found to be negative, atmonth 12.
3.4. Adverse events and safety
Three deaths occurred during the study and were considered un-related to rituximab therapy; one 79-y old female died of myocardialinfarction 2 months after rituximab infusion; one 78-y old female, anon-responder, died at month 7 after rituximab for severe systemicvasculitis and heart failure (this patient had two previous adverseevents probably related to treatment); one 77-y old male, a non-responder, died at month 11 after rituximab for severe systemicvasculitis and renal failure.
Adverse events certainly or possibly caused by rituximab therapywere observed in 3 of 27 treated patients; one patient had two distinctadverse events at different time-points. In the latter patient, the firstevent occurred 1 week after the second rituximab infusion and wascharacterized by a mild form of serum sickness syndrome withurticaria and fever; symptoms resolved after antihistamines and high-dose corticosteroids. Five months after rituximab, this patient hadpneumonia caused by Legionella pneumophila; the relationship of thisevent to rituximab treatment remains, however, uncertain since thepatient had preexisting severe hypogammaglobulinemia (IgG 1.1 g/L)due to urinary protein loss. One 80-y old female experienced severeanaphylaxis (bronchospasm, skin rush, wheezing) immediately afterstarting her first infusion of rituximab; symptoms resolved after theinterruption of infusion and the administration of antihistamineand high-dose steroids. This patient was no further treated withrituximab. The third patient had thrombophlebitis of the left legone month after rituximab; the episode resolved without furthercomplications after nonsteroidal anti-inflammatory drugs and low-molecular-weight heparin.
Some previous studies [9,16] reported an increase in HCV viralload in mixed cryoglobulinemia patients treated with high-doserituximab. In our viremic patients, the HCV viral load did not changesignificantly at any time point after rituximab (not shown); in the 4HCV RNA-negative patients viremia remained undetectable through-out the post-treatment period. Thus, our data are consistent withprevious studies [13,14] reporting predominantly stable HCV viremiaafter high-dose rituximab.
Serum ALT levels did not change significantly after rituximabtreatment in the ten patients with baseline high titers, and no patientdeveloped de novo increment in ALT.
4. Discussion
We report here the preliminary results of a multicenter phase IIsingle-arm two-stage study on the efficacy of low-dose rituximab, i.e.

718 M. Visentini et al. / Autoimmunity Reviews 10 (2011) 714–719
2 weekly doses of 250 mg/m2, for the treatment of refractory HCV-related mixed cryoglobulinemia. This study originated from a smallpilot trial in 6 patients with refractorymixed cryoglobulinemia, whichsuggested a satisfactory efficacy of this regimen [20].
The objective of the present study was to conclusively evaluate thenon-inferiority of a low-dose regimen compared to the high-doseregimen of 4 weekly 375 mg/m2 doses for mixed cryoglobulinemia. Asingle-arm two-stage design was chosen because of the relative rarityof this disorder. Indeed, a randomized, non-inferiority two-arm studywith an expected percentage of positive outcomes of 60% (±15%)would require, for a 0.80 power, 132 patients in each arm. The designof our single-arm study plans to eventually enroll a total of 52patients, a number expected to provide a 0.85 power for a 60%(±15%) response rate.
Recent meta-analyses of the literature data on high-dose ritux-imab for refractory mixed cryoglobulinemia [19,24] provide anexcellent basis to compare the results of our low-dose study. Themost recent review [24] collected data from 8 studies, providing atotal of 111 patients treated with high-dose rituximab; the responserates could be evaluated in 7 of these studies, for a total of 89 patients.The cumulated response rates from these 7 studies were as follows:no response 17% (15/89), partial response 26% (23/89), completeresponse 60% (53/89). Thus, the overall response rate (partial pluscomplete) in these studies was 86%.We achieved a similar 79% overallresponse rate atmonth 3, but the rate of complete responsewas lower(12%). It is important to note that the criteria used to define completeresponse were different in the above reported studies, and this wasreflected by remarkable differences in the complete response ratesthat ranged from none (0/12 patients) [13] to 100% (5/5 patients)[12]. At variance with all previous studies, we adopted a validatedscoring system [22] to uniform the clinical evaluation criteria amongthe centers participating in our trial. The lower complete responserate in our study, compared to previous studies, is seemingly due, atleast in part, to the more stringent definition of complete clinicalresponse (BVAS=0, meaning the complete disappearance of diseasemanifestations).
The meta-analysis by Cacoub et al. [19] collected 57 patients from13 studies, including single- or 2-case reports, treated with rituximabdosages of 375 mg/m2 or higher. Clinical response (complete pluspartial) of skin involvement, artralgia and glomerulonephritis wasreported in approximately 80% of cases,whereas peripheral neuropathyresponded in 93% of cases. These figures are similar to ours except for alower response rate of nephropathy in our study. The overall relapserate (42% at 12 months) and the mean time to relapse (6.5 months) inour study were similar to those reported [19] in patients treated withhigh-dose rituximab (39% and 6.7 months, respectively).
Adverse events were observed in 11% (3/27) of our patients,compared to the 19% (27/142) reported in patients with high-doserituximab [24]. In our series, an anaphylactic reaction occurred in onepatient immediately after starting her first rituximab infusion; thereason for previous sensitization to rituximab in this patient isunclear. The three deaths recorded in our study were apparently notrelated to rituximab treatment, since all patients were elderly, non-responders, and had severe organ involvement by cryoglobulinemiavasculitis.
Mixed cryoglobulinemia patients are at risk for developing overtB cell NHL, and the presence of circulating B cells with t(14;18) bcl-2/IgH is suspected to facilitate lymphomagenesis in these patients [5].Sustained virological response is associated with a reduction of B cellsbearing t(14;18), and this might contribute to attenuate the risk ofdeveloping NHL in mixed cryoglobulinemia patients [6]. We observedthat B cells with t(14;18) disappeared in all responders and remainedundetectable for at least 6 months after rituximab infusion despitesignificant B cell repopulation, suggesting that low-dose rituximabmay similarly contribute to attenuate the risk of NHL in mixedcryoglobulinemia patients.
Collectively, our present results support the efficacy of low-doserituximab for refractory HCV-associated mixed cryoglobulinemia,thus providing a more cost/effective treatment for this disorder.Owing to the relatively small number of patients, a reduced rate ofside effects of low-dose compared to high-dose rituximab cannot beconcluded by our present findings; however, the rate of adverseevents in our study was slightly lower than in studies with high-doserituximab [19,24], and one report claimed that higher rituximabdosage was a risk factor for side effects [15]. The completion of ourstill ongoing study is needed to confirm a higher safety of low-doserituximab.
Take-home messages
• Rituximab at the dosage of 250 mg/m2 given twice is efficacious forthe treatment of HCV-associated mixed cryoglobulinemia refractoryto antivirals.
• Low-dose rituximab is as efficacious as the high-dose of 375 mg/m2
given four times commonly used for the treatment of refractoryHCV-associated mixed cryoglobulinemia.
• Additional data are needed to confirm a higher safety of low-dosecompared to high-dose rituximab.
• Low-dose rituximab may provide a more cost/effective alternativefor treating refractory HCV-associated mixed cryoglobulinemia.
Acknowledgements
This study was supported by the Agenzia Italiana per il Farmaco(AIFA), contract FARM6KMZFY.
References
[1] Agnello V. The etiology and pathophysiology of mixed cryoglobulinemiasecondary to hepatitis C virus infection. Springer Semin Immunopathol 1997;19(1):111–29.
[2] Lamprecht P, Gause A, Gross WL. Cryoglobulinemic vasculitis Arthritis Rheum1999;42:2507–16.
[3] Carbonari M, Caprini E, Tedesco T, Mazzetta F, Tocco V, Casato M, et al. Hepatitis Cvirusdrives theunconstrainedmonoclonal expansionof VH1-69-expressingmemoryB cells in type II cryoglobulinemia: a model of infection-driven lymphomagenesis.J Immunol 2005;174:6532–9.
[4] Marcucci F, Mele A. Hepatitis viruses and non-Hodgkin lymphoma: epidemiology,mechanisms of tumorigenesis and therapeutic opportunities. Blood 2011;117(6):1792–8.
[5] Zignego AL, Ferri C, Giannelli F, Giannini C, Caini P, Monti M, et al. Prevalence ofbcl-2 rearrangement in patients with hepatitis C virus-related mixed cryoglobu-linemia with or without B-cell lymphomas. Ann Intern Med 2002;137:571–80.
[6] Giannelli F, Moscarella S, Giannini C, Caini P, Monti M, Gragnani L, et al. Effect ofantiviral treatment in patients with chronic HCV infection and t(14;18)translocation. Blood 2003;102:1196–201.
[7] Casato M, Laganà B, Antonelli G, Dianzani F, Bonomo L. Long-term results oftherapy with interferon-alpha for type II essential mixed cryoglobulinemia. Blood1991;78:3142–7.
[8] Saadoun D, Resche-Rigon M, Thibault V, Piette JC, Cacoub P. Antiviral therapy forhepatitis C virus-associated mixed cryoglobulinemia vasculitis: a long-termfollowup study. Arthritis Rheum 2006;54:3696–706.
[9] Sansonno D, De Re V, Lauletta G, Tucci FA, Boiocchi M, Dammacco F. Monoclonalantibody treatment of mixed cryoglobulinemia resistant to interferon alpha withan anti-CD20. Blood 2003;101:3818–26.
[10] Zaja F, De Vita S, Mazzaro C, Sacco S, Damiani D, De Marchi G, et al. Efficacy andsafety of rituximab in type II mixed cryoglobulinemia. Blood 2003;101:3827–34.
[11] Bryce AH, Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV. Response to rituximabin patients with type II cryoglobulinemia. Clin Lymphoma Myeloma 2006;7(2):140–4.
[12] Quartuccio L, Soardo G, Romano G, Zaja F, Scott CA, De Marchi G, et al. Rituximabtreatment for glomerulonephritis in HCV-associated mixed cryoglobulinaemia:efficacy and safety in the absence of steroid. Rheumatology 2006;45:842–6.
[13] Roccatello D, Baldovino S, Rossi D, Giachino O, Mansouri M. Rituximab as atherapeutic tool in severe mixed cryoglobulinemia. Clin Rev Allergy Immunol2008;34:111–7.
[14] Cavallo R, Roccatello D, Menegatti E, Naretto C, Napoli F, Baldovino S. Rituximab incryoglobulinemic peripheral neuropathy. J Neurol 2009;256:1076–82.
[15] Sène D, Ghillani-Dalbin P, Amoura Z, Musset L, Cacoub P. Rituximab may form acomplex with IgMkappa mixed cryoglobulin and induce severe systemic reactions

719M. Visentini et al. / Autoimmunity Reviews 10 (2011) 714–719
in patients with hepatitis C virus-induced vasculitis. Arthritis Rheum 2009;60:3848–55.
[16] Petrarca A, Rigacci L, Caini P, Colagrande S, Romagnoli P, Vizzutti F, et al. Safety andefficacy of rituximab in patients with hepatitis C virus-related mixed cryoglobu-linemia and severe liver disease. Blood 2010;116:335–42.
[17] Dammacco F, Tucci FA, Lauletta G, Gatti P, De Re V, Conteduca V, et al.Pegylated interferon-alpha, ribavirin, and rituximab combined therapy ofhepatitis C virus-related mixed cryoglobulinemia: a long-term study. Blood2010;116:343–53.
[18] Saadoun D, Resche Rigon M, Sene D, Terrier B, Karras A, Perard L, et al. Rituximabplus Peg-interferon-alpha/ribavirin comparedwith Peg-interferon-alpha/ribavirinin hepatitis C-related mixed cryoglobulinemia. Blood 2010;116:326–34.
[19] Cacoub P, Delluc A, Saadoun D, Landau DA, Sene D. Anti-CD20 monoclonalantibody (rituximab) treatment for cryoglobulinemic vasculitis: where do westand? Ann Rheum Dis 2008;67:283–7.
Predictors of mortality in diffuse alveolar haemorrhage associated wit
The objective of this studywas the evaluation of clinical, demographic andhaemorrhage (DAH) associated with systemic lupus erythematosus (SLlaboratory test, SLEDAI-2K, predictors of mortality (APACHE II) and differerituximabwere evaluated in SLEpatientswhowerediagnosedwithDAH, toof DAH in 22 SLE patients were included (one patient with four episodes, fowas 25.1 years and 1.5 years of SLE evolutionwith haemoglobin drop 3.4g/episodes were in patients under 18 years of age (2 patients with recurrenpatients, 17 were women and 22/29 had DAH episodes. Dyspnea and nepfever (65.5%); haemoptysis was present only in 44.8%. Through evalurequirement for mechanical ventilation and high APACHE II were associatless mortality (not statistically significant).
[20] Visentini M, Granata M, VenezianoML, Borghese F, CarlesimoM, Pimpinelli F, et al.Efficacy of low-dose rituximab for mixed cryoglobulinemia. Clin Immunol2007;125:30–3.
[21] Bianchettin G, Bonaccini C, Oliva R, Tramontano A, Cividini A, Casato M, et al.Analysis of hepatitis C virus hypervariable region 1 sequence from cryoglobuli-nemic patients and associated controls. J Virol 2007;81:4564–71.
[22] Lamprecht P, Moosig F, Gause A, Herlyn K, Gross WL. Birmingham vasculitisactivity score, disease extent index and complement factor C3c reflect diseaseactivity best in hepatitis C virus-associated cryoglobulinemic vasculitis. Clin ExpRheumatol 2000;18:319–25.
[23] Landau DA, Saadoun D, Halfon P, Martinot-Peignoux M, Marcellin P, Fois E, et al.Relapse of hepatitis C virus-associated mixed cryoglobulinemia vasculitis inpatients with sustained viral response. Arthritis Rheum 2008;58:604–11.
[24] WinkF,HoutmanPM, JansenTL. Rituximab incryoglobulinaemicvasculitis, evidence forits effectivity: a case report and review of literature. Clin Rheumatol 2011;30:293–300.
h systemic lupus erythematosus
treatment-associatedmortality factors in patientswith diffuse alveolarE). Martínez-Martínez M, et al. (Lupus 2011:20:568–74). Clinical,nt treatments including cyclophosphamide, methylprednisolone anddeterminepotential associationwithmortality. Twenty-nineepisodesur patients with two episodes (seven recurrences), 15 died.Mean agedl. In 4 of 22 patients, theDAHdiagnosiswas confirmed by autopsy. Sixce). DAH was the initial manifestation of SLE in 10 patients. Of the 22hritis occurred in all patients, less common were arthritis (75.9%) andation of all included factors, only thrombocytopenia, renal failure,ed with higher mortality. Cyclophosphamide use was associated with
Related Documents