A needs assessment for orthodontic care in Thames Valley (Buckinghamshire, Oxfordshire, Berkshire)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
A needs assessment for orthodontic care in Thames Valley (Buckinghamshire, Oxfordshire, Berkshire)
OFFICIAL
Final version 2
A needs assessment for orthodontic care in Thames Valley Version number: Final version First published: March 2017 Updated: (only if this is applicable) Prepared by: Anna Ireland, Consultant in Dental Public Health Classification: For local use only
The National Health Service Commissioning Board was established on 1 October 2012 as an
executive non-departmental public body. Since 1 April 2013, the National Health Service
Commissioning Board has used the name NHS England for operational purposes.
OFFICIAL
Final version 3
Acknowledgements NHS England would like to thank all of the individuals, groups and organisations that supported this review in some way. We are particularly grateful to those who contributed data to the review and those who attended stakeholder meetings. NHS England would particularly like to thank the following people:
Alison Marshman, Primary Care Commissioning Assistant
Hugh O’Keeffe, Primary Care Contracts Manager (Thames Valley)
Business Services Authority
Public Health England Knowledge and Information Team
Anna Ireland, Consultant in Dental Public Health
Jenny Oliver, Consultant in Dental Public Health
Devika Vadher, Dental Public Health Clinical Fellow
Members of the Thames Valley Orthodontic Managed Clinical Network
OFFICIAL
Final version 4
1 Contents 1 Contents .............................................................................................................. 4
1 Executive summary ............................................................................................. 6
1.1 Key issues ..................................................................................................... 8 1.2 Recommendations....................................................................................... 10
2 Introduction ........................................................................................................ 12
2.1 What is Orthodontics? ................................................................................. 13
2.2 Who gets orthodontics under the NHS? ...................................................... 13 2.3 Aim of the needs assessment ..................................................................... 13 2.4 Objectives .................................................................................................... 15 2.5 Exclusions ................................................................................................... 15
3 What is meant by ‘need’ in relation to orthodontic treatment ............................. 16
3.1 Types of ‘need’ for orthodontic treatment .................................................... 16 3.2 How do the interactions between types of need impact on service usage? . 17
4 Who needs orthodontic treatment? ................................................................... 17
5 How many 12 year olds are there in TV and how does this vary by lower tier
local authority? ......................................................................................................... 18
5.1 Number of 12 year olds in TV as a whole .................................................... 18
6 How much orthodontic need is in the population of the TV? .............................. 20
6.1 Normative need ........................................................................................... 21
1.1 Survey method to estimate normative need ............................................. 21 2.1 Stephen’s method to estimate normative need ........................................ 23
3.1 The rule of ‘a third’ to estimate normative need ....................................... 24 4.1 Comparison between methods of estimating normative need .................. 25
6.2 Perceived need and demand ....................................................................... 27
7 How much Orthodontics is being commissioned for Thames Valley residents in
primary care? ............................................................................................................ 29
7.1 How much Orthodontics is being delivered for TV residents in secondary care 29
7.2 How much Orthodontics is being delivered in Community Dental Services . 31 7.3 What are the differences between the levels of primary care orthodontic commissioned activity and estimated orthodontic need? ...................................... 31 7.4 Commissioned activity and future need ....................................................... 36
8 Primary care ...................................................................................................... 37
8.1 Location of orthodontic practices ................................................................. 37 8.2 Where are patients coming from?................................................................ 38
9 How does uptake of Orthodontic care vary in TV? ............................................ 39
9.1 Uptake of NHS orthodontic care is variable ................................................. 39 9.2 Variation in uptake by age ........................................................................... 40 9.3 Variation in uptake by socioeconomic status ............................................... 40
9.4 Variation in uptake of orthodontic treatment by gender ............................... 41
10 What orthodontic care is being provided in primary care? .............................. 42
OFFICIAL
Final version 5
10.1 Assessment and acceptance for treatment .............................................. 42 10.2 Severity of cases being treated in primary care ....................................... 44
11 Secondary care ............................................................................................... 44
12 How long are patients waiting for orthodontic treatment? ............................... 45
13 What is the NHS currently spending on Orthodontics in Thames Valley? ...... 46
13.1 Types of orthodontics services in Thames Valley .................................... 46 13.2 Total spend on orthodontics services in TV .............................................. 46 13.3 Secondary care ........................................................................................ 47
14 What are the workforce pressures on the Orthodontic system? ..................... 48
14.1 Orthodontic consultant numbers and consultant training ......................... 48 14.2 Impact of skill mix ..................................................................................... 48
15 Orthodontic services in the community dental service? .................................. 48
15.1 Orthodontic support to the wider system .................................................. 48 15.2 Knowledge gaps ....................................................................................... 51
16 Public views on orthodontics........................................................................... 51
16.1 Stakeholder feedback - national commissioning guide for orthodontics ... 52
17 Conclusions .................................................................................................... 54
17.1 Summary of findings ................................................................................ 54
17.2 Key issues ................................................................................................ 56 17.3 Recommendations ................................................................................... 58
18 Appendices ..................................................................................................... 61
A. Postponed public engagement survey on Orthodontics in South Central (BGSW and Thames Valley) ................................................................................. 61 B. Recommendations from 2012 Thames Valley orthodontic needs assessment – update on progress ............................................................................................ 63 C. Explanation of the Index or Orthodontic Treatment Need ............................ 66 D. The Essex Youth Forum discussion on orthodontics 2014 .......................... 68
19 References ..................................................................................................... 70
OFFICIAL
Final version 6
1 Executive summary
Objective
Findings
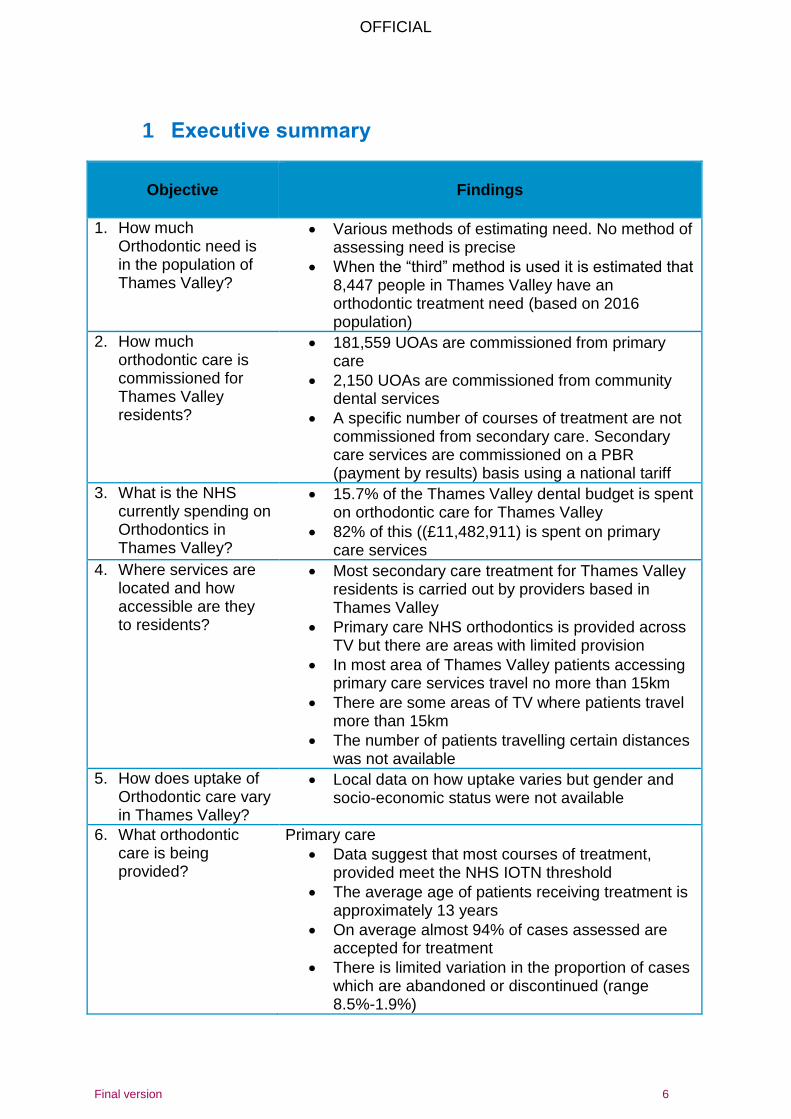
1. How much Orthodontic need is in the population of Thames Valley?
Various methods of estimating need. No method of assessing need is precise
When the “third” method is used it is estimated that 8,447 people in Thames Valley have an orthodontic treatment need (based on 2016 population)
2. How much orthodontic care is commissioned for Thames Valley residents?
181,559 UOAs are commissioned from primary care
2,150 UOAs are commissioned from community dental services
A specific number of courses of treatment are not commissioned from secondary care. Secondary care services are commissioned on a PBR (payment by results) basis using a national tariff
3. What is the NHS currently spending on Orthodontics in Thames Valley?
15.7% of the Thames Valley dental budget is spent on orthodontic care for Thames Valley
82% of this ((£11,482,911) is spent on primary care services
4. Where services are located and how accessible are they to residents?
Most secondary care treatment for Thames Valley residents is carried out by providers based in Thames Valley
Primary care NHS orthodontics is provided across TV but there are areas with limited provision
In most area of Thames Valley patients accessing primary care services travel no more than 15km
There are some areas of TV where patients travel more than 15km
The number of patients travelling certain distances was not available
5. How does uptake of Orthodontic care vary in Thames Valley?
Local data on how uptake varies but gender and socio-economic status were not available
6. What orthodontic care is being provided?
Primary care
Data suggest that most courses of treatment, provided meet the NHS IOTN threshold
The average age of patients receiving treatment is approximately 13 years
On average almost 94% of cases assessed are accepted for treatment
There is limited variation in the proportion of cases which are abandoned or discontinued (range 8.5%-1.9%)
OFFICIAL
Final version 7
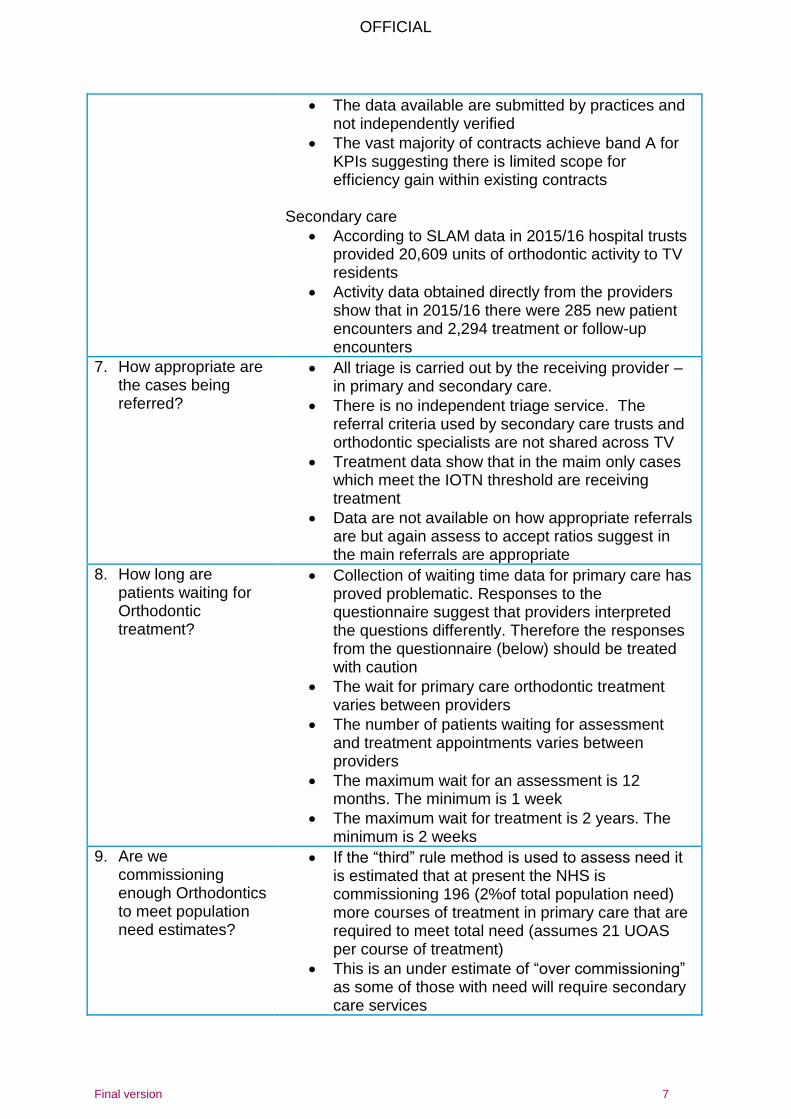
The data available are submitted by practices and not independently verified
The vast majority of contracts achieve band A for KPIs suggesting there is limited scope for efficiency gain within existing contracts
Secondary care
According to SLAM data in 2015/16 hospital trusts provided 20,609 units of orthodontic activity to TV residents
Activity data obtained directly from the providers show that in 2015/16 there were 285 new patient encounters and 2,294 treatment or follow-up encounters
7. How appropriate are the cases being referred?
All triage is carried out by the receiving provider – in primary and secondary care.
There is no independent triage service. The referral criteria used by secondary care trusts and orthodontic specialists are not shared across TV
Treatment data show that in the maim only cases which meet the IOTN threshold are receiving treatment
Data are not available on how appropriate referrals are but again assess to accept ratios suggest in the main referrals are appropriate
8. How long are patients waiting for Orthodontic treatment?
Collection of waiting time data for primary care has proved problematic. Responses to the questionnaire suggest that providers interpreted the questions differently. Therefore the responses from the questionnaire (below) should be treated with caution
The wait for primary care orthodontic treatment varies between providers
The number of patients waiting for assessment and treatment appointments varies between providers
The maximum wait for an assessment is 12 months. The minimum is 1 week
The maximum wait for treatment is 2 years. The minimum is 2 weeks
9. Are we commissioning enough Orthodontics to meet population need estimates?
If the “third” rule method is used to assess need it is estimated that at present the NHS is commissioning 196 (2%of total population need) more courses of treatment in primary care that are required to meet total need (assumes 21 UOAS per course of treatment)
This is an under estimate of “over commissioning” as some of those with need will require secondary care services
OFFICIAL
Final version 8
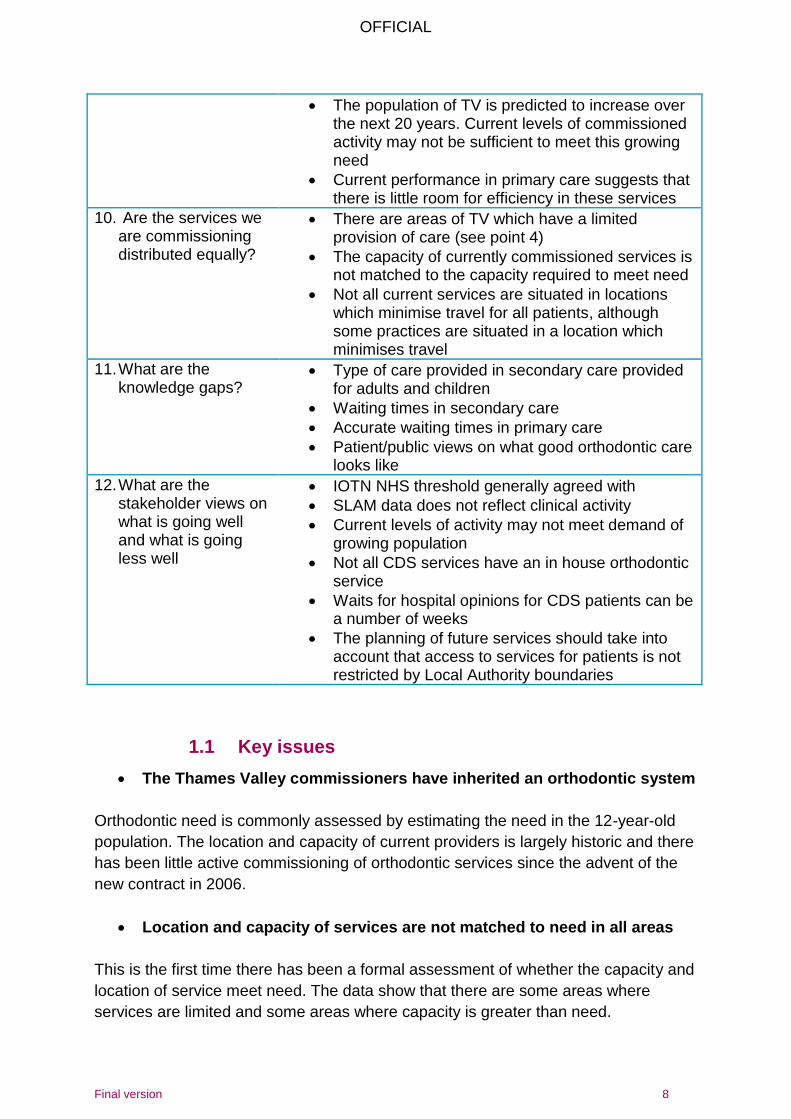
The population of TV is predicted to increase over the next 20 years. Current levels of commissioned activity may not be sufficient to meet this growing need
Current performance in primary care suggests that there is little room for efficiency in these services
10. Are the services we are commissioning distributed equally?
There are areas of TV which have a limited provision of care (see point 4)
The capacity of currently commissioned services is not matched to the capacity required to meet need
Not all current services are situated in locations which minimise travel for all patients, although some practices are situated in a location which minimises travel
11. What are the knowledge gaps?
Type of care provided in secondary care provided for adults and children
Waiting times in secondary care
Accurate waiting times in primary care
Patient/public views on what good orthodontic care looks like
12. What are the stakeholder views on what is going well and what is going less well
IOTN NHS threshold generally agreed with
SLAM data does not reflect clinical activity
Current levels of activity may not meet demand of growing population
Not all CDS services have an in house orthodontic service
Waits for hospital opinions for CDS patients can be a number of weeks
The planning of future services should take into account that access to services for patients is not restricted by Local Authority boundaries
1.1 Key issues
The Thames Valley commissioners have inherited an orthodontic system
Orthodontic need is commonly assessed by estimating the need in the 12-year-old
population. The location and capacity of current providers is largely historic and there
has been little active commissioning of orthodontic services since the advent of the
new contract in 2006.
Location and capacity of services are not matched to need in all areas
This is the first time there has been a formal assessment of whether the capacity and
location of service meet need. The data show that there are some areas where
services are limited and some areas where capacity is greater than need.
OFFICIAL
Final version 9
Inequalities in access to orthodontic services
Whilst most patients are able to access primary care orthodontic services within15km
of their home some have to travel further than this. Travelling large distances may be
particularly difficult for more deprived families and so will increase inequalities in
access.
Waiting times in primary care of variable. Lack of waiting time information, available
to GDPs and patients, means that they may not be able to make choices which take
into account waiting times.
Lack of detailed data
The secondary care data available to support this needs assessment was limited. It
was not possible to obtain information on the ages of patients treated or the
treatment provided.
In primary care there is a lack of accurate information on referral sources, waiting
times and numbers of patients waiting for treatment.
Triage
Triage is carried out by providers on the referrals they receive. There are no agreed
referral criteria, referral forms or independent assessment of referrals. There is also
no routine collection of referral data e.g. referral source. Referrals are not submitted
electronically, as recommended in national guidance.
Pathway
There is no agreed orthodontic pathway, with a single entry point, in TV, as per
national guidance.
OFFICIAL
Final version 10
1.2 Recommendations
Match capacity to need
Ensure capacity meets future population growth
Work in partnership with orthodontic clinical network to:
o Identify a reasonable waiting time standard across TV
o Validate waiting list information
Ensure the location and capacity of service commissioned meets the local
need and takes into account natural patient flows
It is important to note that the number of UOAs needed is used as a proxy for
need across the system. UOAs are not the currency used in secondary care
and this must be taken into account when planning services otherwise there is
a risk that the budget is spent on primary care UOAs only and orthodontic
services may be over-commissioned.
Improve monitoring and data collection across the system
Agree definitions of waits for assessment and waits for treatment so that
commissioners can compare waits between practices
Routinely collect waiting time data from primary care providers
Routinely collect waiting time data form secondary care providers
Consider commissioning an electronic referral management service for
orthodontic referrals. This will enable collection of data on source of referrals,
appropriateness and outcome of referrals and the proportion of referrals meet
NHS criteria.
Contract management and improving quality
Quality based KPIs should continue and be improved
Aim to align KPIs and targets across South Central over medium term
Work with the clinical network to agree how to support orthodontists struggling
to meet DAF standards and how to share best practise
Agree, with the clinical network, appropriate and meaningful PROMs and
PREMs for monitoring quality
Link all Orthodontic providers to clinical network which can lead and support
them to improve quality, such as through peer review and audit
Consider implementing PREMS that look at communication with young people
in a caring, respectful and comprehensible way, including providing
explanations throughout the course of treatment and answering questions.
Pathway redesign
OFFICIAL
Final version 11
Work with clinical network to agree referral criteria and referral form to ensure
consistent processes, and good quality referrals, across TV
Implement an electronic referral service to give single entry point to the
pathway and provide the following benefits: avoidance of duplicate referrals,
ongoing measurement of uptake of services, routine data collection, e.g. on
source of referral, numbers waiting, waiting times, required level of provider.
Work with HEE and the clinical network to support dentists to routinely include
the IOTN score when referring patients for orthodontic treatment.
Implement consistent referral management for secondary and primary care
according to national commissioning guidance, ideally with electronic RMS so
that data can be gathered and monitored.
Work towards agreeing service specifications for secondary care services
including minimum data set
Reach consistent agreement on under what circumstances over 18s receive
orthodontic treatment in secondary care
Involve patients and public in the Orthodontic commissioning cycle, such as
pathway redesign and evaluation
Tackling inequalities
Make use of opportunities in the future to distribute resources/capacity more
according to need/population density. Prioritise areas where high numbers of
patients are travelling long distances, particularly where patients are from lower
deprivation quartile.
Prioritise delivery of prevention activities in GDS contracts, e.g. application of
fluoride varnish. This will help to improve oral health and therefore enable more
people to be suitable for orthodontic care
Involve patients and public in the commissioning cycle, such as pathway
redesign and evaluation and in work regarding addressing inequalities in
access to dental services.
Actively monitor access to GDS
Work with the LPN to explore how to encourage referral of more deprived
patients
Gather information on the local public view on Orthodontic services and apply
findings to action plan.
Review opening hours across the Orthodontic system and expand beyond
school hours where necessary.
Orthodontic support to the wider system
Ensure commissioning of orthodontic treatment planning support to services treating:
special care patients
extractions under GA
OFFICIAL
Final version 12
2 Introduction This needs assessment gives an overview of the current position of orthodontic
commissioning in Thames Valley (TV). It outlines population need and orthodontic
services currently commissioned before identifying gaps in services and knowledge.
It also includes the views of local clinicians on the current orthodontic pathway in TV.
Drivers for this needs assessment include:
1. National commissioning guide for orthodontics’ published by NHS England in
20151
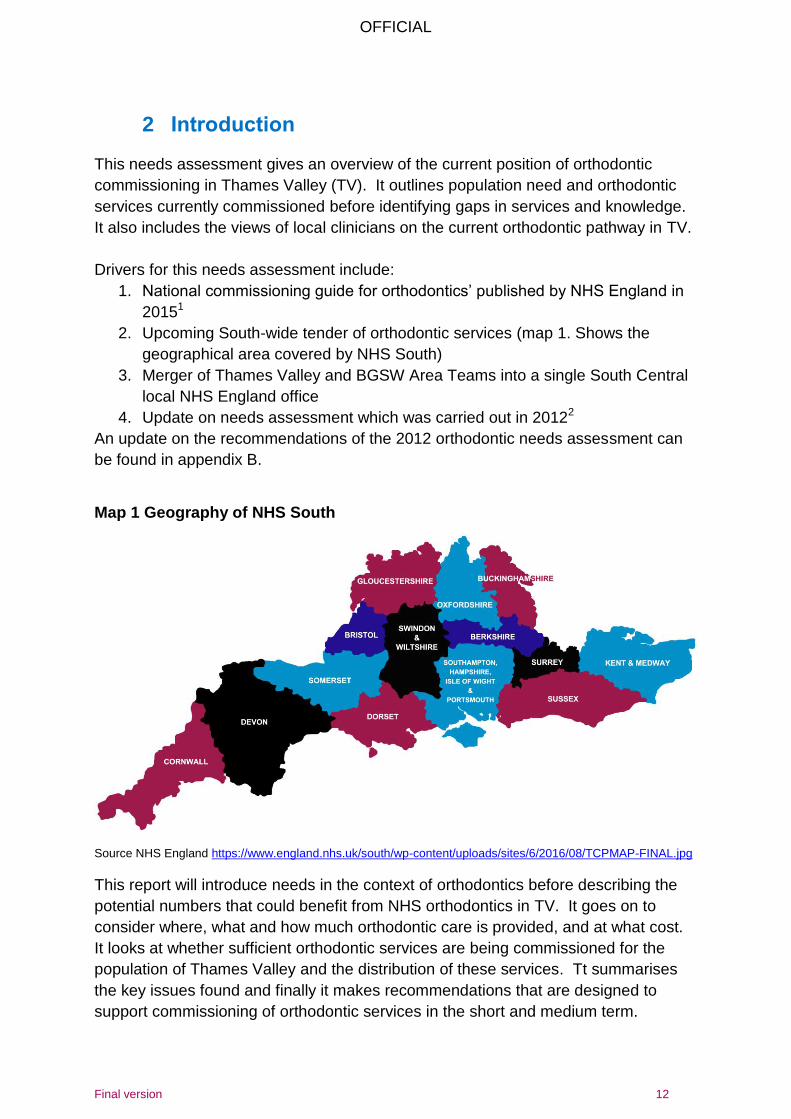
2. Upcoming South-wide tender of orthodontic services (map 1. Shows the
geographical area covered by NHS South)
3. Merger of Thames Valley and BGSW Area Teams into a single South Central
local NHS England office
4. Update on needs assessment which was carried out in 20122
An update on the recommendations of the 2012 orthodontic needs assessment can
be found in appendix B.
Map 1 Geography of NHS South
Source NHS England https://www.england.nhs.uk/south/wp-content/uploads/sites/6/2016/08/TCPMAP-FINAL.jpg
This report will introduce needs in the context of orthodontics before describing the
potential numbers that could benefit from NHS orthodontics in TV. It goes on to
consider where, what and how much orthodontic care is provided, and at what cost.
It looks at whether sufficient orthodontic services are being commissioned for the
population of Thames Valley and the distribution of these services. Tt summarises
the key issues found and finally it makes recommendations that are designed to
support commissioning of orthodontic services in the short and medium term.
OFFICIAL
Final version 13
The Orthodontic Clinical Network in TV was very helpful in supporting this document.
Their views are presented in speech bubbles throughout the document.
2.1 What is Orthodontics?
Orthodontics is concerned with the development, prevention, and correction of
irregularities of the teeth, bite and jaw,3 known as ‘malocclusions’. This term is given
to mouths that display natural variations from the ‘ideal’ in how the teeth and jaws
relate. The most common feature of malocclusions is dental crowding.4
Orthodontic treatment often involves extraction of teeth (to relieve dental crowding)
and the closing of resultant gaps with appliances. Three main types of appliance are
used: removable appliances (to tip teeth into place), functional appliances (a bulkier
removable appliance that aims to reduce the prominence of upper front teeth) and
fixed appliances (use attachments and wires fixed in the mouth to move multiple
teeth). Most treatment plans use fixed appliances, with or without other appliance
types.
Orthodontic treatment generally takes 18 months – 2 years, and this is followed by
long-term retention to prevent relapse.
2.2 Who gets orthodontics under the NHS?
The Department of Health recommends that NHS orthodontics is commissioned for
children, aged up to 18 years and under at the time of assessment, who are
classified with the Index of Orthodontic Need (IOTN) at IOTN Dental Health
Component (DHC) levels of 4 and 5 or DHC 3 where there is an Aesthetic
Component (AC) of 6 and above. A full explanation of IOTN can be found in
Appendix B.
Primary care delivered NHS orthodontic care is not usually available for adults, but
may be provided on a case-by-case basis if needed for health reasons. Secondary
care services provide care to both adults and children.
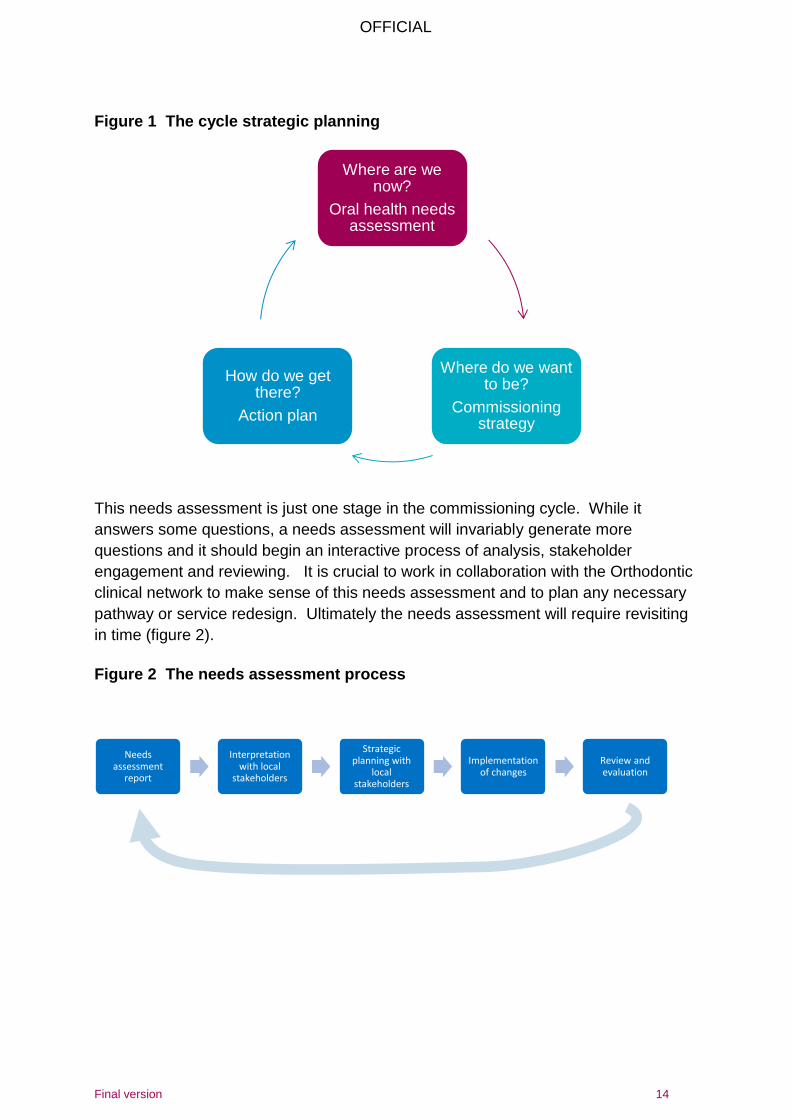
2.3 Aim of the needs assessment
To give an overview of ‘where are we now’ to support commissioning of orthodontic
services in the short and medium term (figure 1).
Most of us, as stakeholders, agree with the IOTN threshold. View expressed by a member of the TV Orthodontic clinical network
OFFICIAL
Final version 14
Figure 1 The cycle strategic planning
This needs assessment is just one stage in the commissioning cycle. While it
answers some questions, a needs assessment will invariably generate more
questions and it should begin an interactive process of analysis, stakeholder
engagement and reviewing. It is crucial to work in collaboration with the Orthodontic
clinical network to make sense of this needs assessment and to plan any necessary
pathway or service redesign. Ultimately the needs assessment will require revisiting
in time (figure 2).
Figure 2 The needs assessment process
Where are we now?
Oral health needs assessment
Where do we want to be?
Commissioning strategy
How do we get there?
Action plan
Needs assessment
report
Interpretation with local
stakeholders
Strategic planning with
local stakeholders
Implementation of changes
Review and evaluation
OFFICIAL
Final version 15
2.4 Objectives
To identify:
1. What is meant by ‘need’ in relation to orthodontic treatment?
2. Who needs orthodontic treatment?
3. How much orthodontic need is in the population of TV?
4. How much orthodontic care is commissioned for TV residents?
5. What is the NHS currently spending on Orthodontics in TV?
6. Where services are located?
7. How does uptake of orthodontic care vary in TV?
8. What orthodontic care is being provided?
9. How appropriate are the cases being referred?
10. How long are patients waiting for orthodontic treatment?
11. Are we commissioning enough orthodontic care in the right location to meet
population need estimates?
12. Are the services being commissioned distributed equally?
13. What are the views of stakeholders in TV?
14. What are the knowledge gaps?
2.5 Exclusions
The following topics are excluded from the scope of this needs assessment:
Private orthodontic activity
Orthodontic need and care for people with a cleft lip or palate
Orthodontic care associated with orthognathic care
Comparison of need for Orthodontics versus other types of dental care
or prevention.
OFFICIAL
Final version 16
3 What is meant by ‘need’ in relation to orthodontic treatment
3.1 Types of ‘need’ for orthodontic treatment
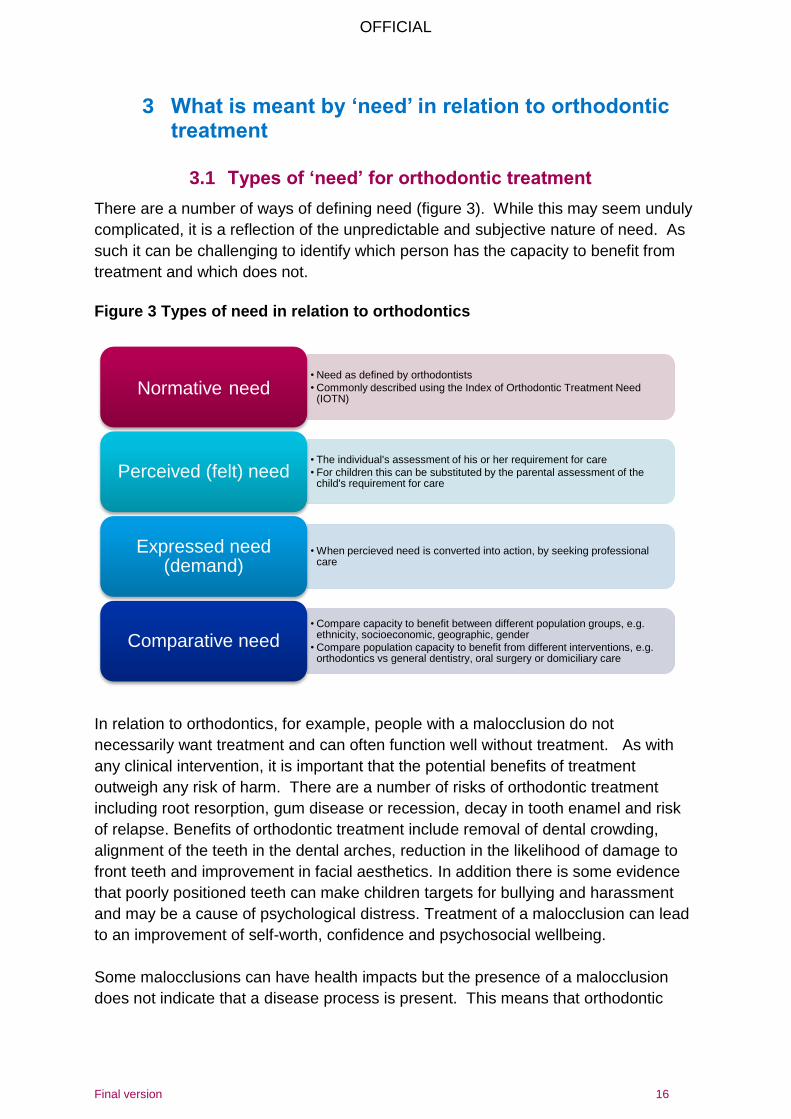
There are a number of ways of defining need (figure 3). While this may seem unduly
complicated, it is a reflection of the unpredictable and subjective nature of need. As
such it can be challenging to identify which person has the capacity to benefit from
treatment and which does not.
Figure 3 Types of need in relation to orthodontics
In relation to orthodontics, for example, people with a malocclusion do not
necessarily want treatment and can often function well without treatment. As with
any clinical intervention, it is important that the potential benefits of treatment
outweigh any risk of harm. There are a number of risks of orthodontic treatment
including root resorption, gum disease or recession, decay in tooth enamel and risk
of relapse. Benefits of orthodontic treatment include removal of dental crowding,
alignment of the teeth in the dental arches, reduction in the likelihood of damage to
front teeth and improvement in facial aesthetics. In addition there is some evidence
that poorly positioned teeth can make children targets for bullying and harassment
and may be a cause of psychological distress. Treatment of a malocclusion can lead
to an improvement of self-worth, confidence and psychosocial wellbeing.
Some malocclusions can have health impacts but the presence of a malocclusion
does not indicate that a disease process is present. This means that orthodontic
• Need as defined by orthodontists
• Commonly described using the Index of Orthodontic Treatment Need (IOTN)
Normative need
• The individual's assessment of his or her requirement for care
• For children this can be substituted by the parental assessment of the child's requirement for care
Perceived (felt) need
• When percieved need is converted into action, by seeking professional care
Expressed need (demand)
• Compare capacity to benefit between different population groups, e.g. ethnicity, socioeconomic, geographic, gender
• Compare population capacity to benefit from different interventions, e.g. orthodontics vs general dentistry, oral surgery or domiciliary care
Comparative need
OFFICIAL
Final version 17
treatment is almost always elective. It can therefore be difficult to decide when and if
orthodontic treatment is required.5
It is important to note however; that population levels of perceived or expressed need
are subjective and therefore changeable. Perceived and expressed need can be
influenced by external factors, such as changes in societal norms on the acceptability
of crowded teeth, awareness of entitlement to treatment (or lack thereof) or
availability of an NHS dentist. As such, they can influence inequalities in uptake of
care.
Finally it is important to consider comparative need: in a context of increasing need
and limited resources it is relevant to look at the added value of different
interventions, e.g. what population needs will be met by spending on orthodontics
versus spending on domiciliary care or prevention programmes. It is also crucial to
look at inequalities in need and attempt to address those through any resulting action
plan or strategy, e.g. inequalities in access to Orthodontic care by deprivation
quartile.
3.2 How do the interactions between types of need impact on service usage?
Where people have a normative need for Orthodontic care, and there are services
available to meet that need, but they do not want treatment they will not present for
treatment or accept referral (termed unwilling recipients). Where, on the other hand,
there is a need and demand but insufficient service capacity to meet that need,
waiting lists will grow. Where there is demand and supply but no normative need,
such as the NHS IOTN threshold is not met, patients may seek private treatment.
4 Who needs orthodontic treatment?
Most orthodontic treatment is carried out in children in the early teenage years (12-13
years old). This is because most treatment requires all permanent teeth to be in the
mouth. It is also thought that treatment is facilitated by pubertal growth. In some
cases, treatment on younger children can be helpful to remove, or reduce, the need
for treatment later (interceptive orthodontics). Orthodontic treatment can also be
carried out in adults.
Where there is a gross difference between the sizes of upper and lower jaws
orthodontics alone is not able to correct the malocclusion. These cases, if treated,
require multidisciplinary care to deliver a treatment plan that includes both surgery to
move the jaws (orthognathic surgery) and orthodontic appliance treatment to move
teeth. In these cases treatment is delayed until the patient has stopped growing
usually at age 18-21 years old.
OFFICIAL
Final version 18
Unlike most oral conditions, malocclusion does not vary between genders or between
socioeconomic groups. To a small extent, racial characteristics mean that there is
some ethnic variation.
In the NHS the majority of orthodontic treatment is carried out in children aged 12-13
years. A small number of younger children receive interceptive orthodontic care, and
a small number of adults receive treatment.
5 How many 12 year olds are there in TV and how does this vary by lower tier local authority?
This chapter details the current population estimates of 12 year old numbers both in
TV as a whole, and in each of the lower tier local authorities therein.
5.1 Number of 12 year olds in TV as a whole
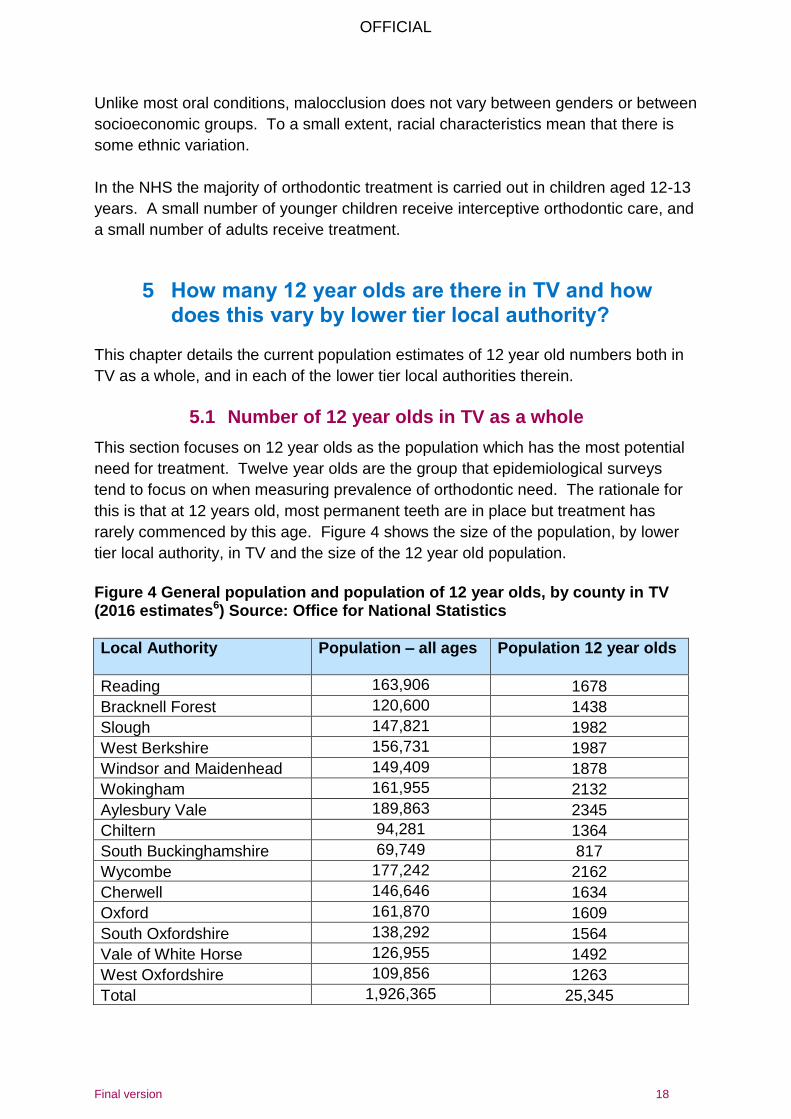
This section focuses on 12 year olds as the population which has the most potential
need for treatment. Twelve year olds are the group that epidemiological surveys
tend to focus on when measuring prevalence of orthodontic need. The rationale for
this is that at 12 years old, most permanent teeth are in place but treatment has
rarely commenced by this age. Figure 4 shows the size of the population, by lower
tier local authority, in TV and the size of the 12 year old population.
Figure 4 General population and population of 12 year olds, by county in TV (2016 estimates6) Source: Office for National Statistics
Local Authority Population – all ages Population 12 year olds
Reading 163,906 1678
Bracknell Forest 120,600 1438
Slough 147,821 1982
West Berkshire 156,731 1987
Windsor and Maidenhead 149,409 1878
Wokingham 161,955 2132
Aylesbury Vale 189,863 2345
Chiltern 94,281 1364
South Buckinghamshire 69,749 817
Wycombe 177,242 2162
Cherwell 146,646 1634
Oxford 161,870 1609
South Oxfordshire 138,292 1564
Vale of White Horse 126,955 1492
West Oxfordshire 109,856 1263
Total 1,926,365 25,345
OFFICIAL
Final version 19
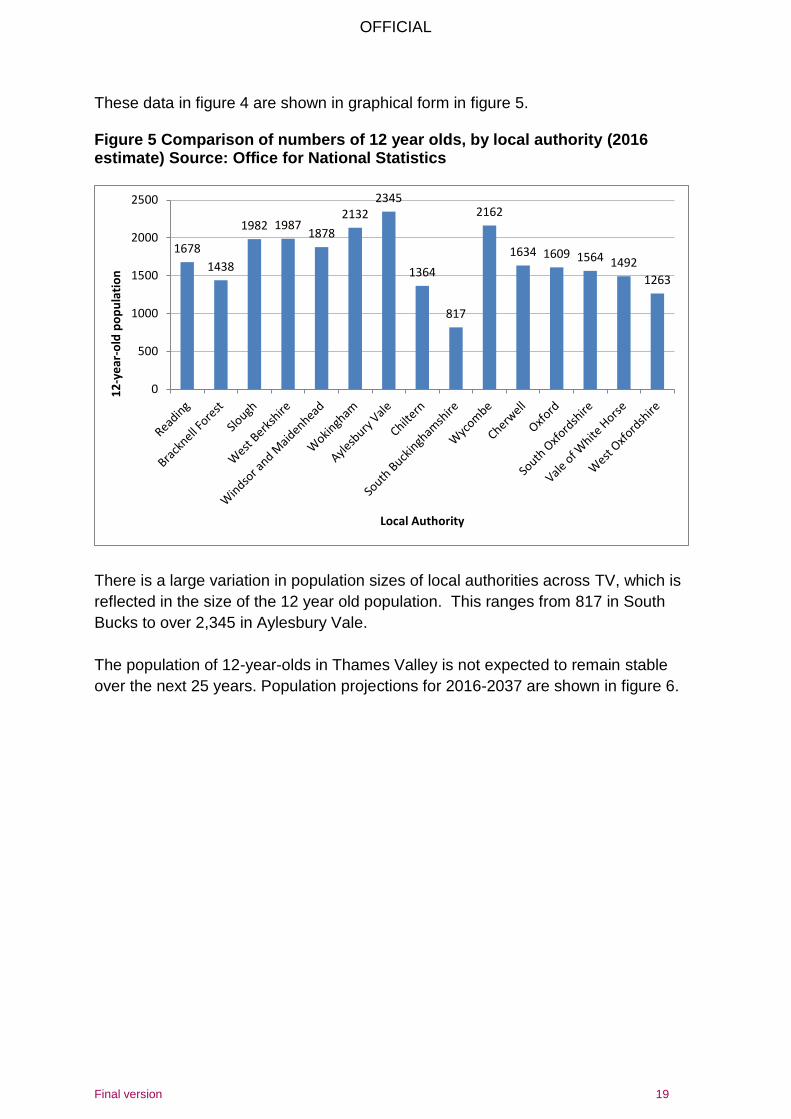
These data in figure 4 are shown in graphical form in figure 5. Figure 5 Comparison of numbers of 12 year olds, by local authority (2016 estimate) Source: Office for National Statistics
There is a large variation in population sizes of local authorities across TV, which is
reflected in the size of the 12 year old population. This ranges from 817 in South
Bucks to over 2,345 in Aylesbury Vale.
The population of 12-year-olds in Thames Valley is not expected to remain stable
over the next 25 years. Population projections for 2016-2037 are shown in figure 6.
1678
1438
1982 1987 1878
2132 2345
1364
817
2162
1634 1609 1564 1492
1263
0
500
1000
1500
2000
2500
12
-ye
ar-o
ld p
op
ula
tio
n
Local Authority
OFFICIAL
Final version 20
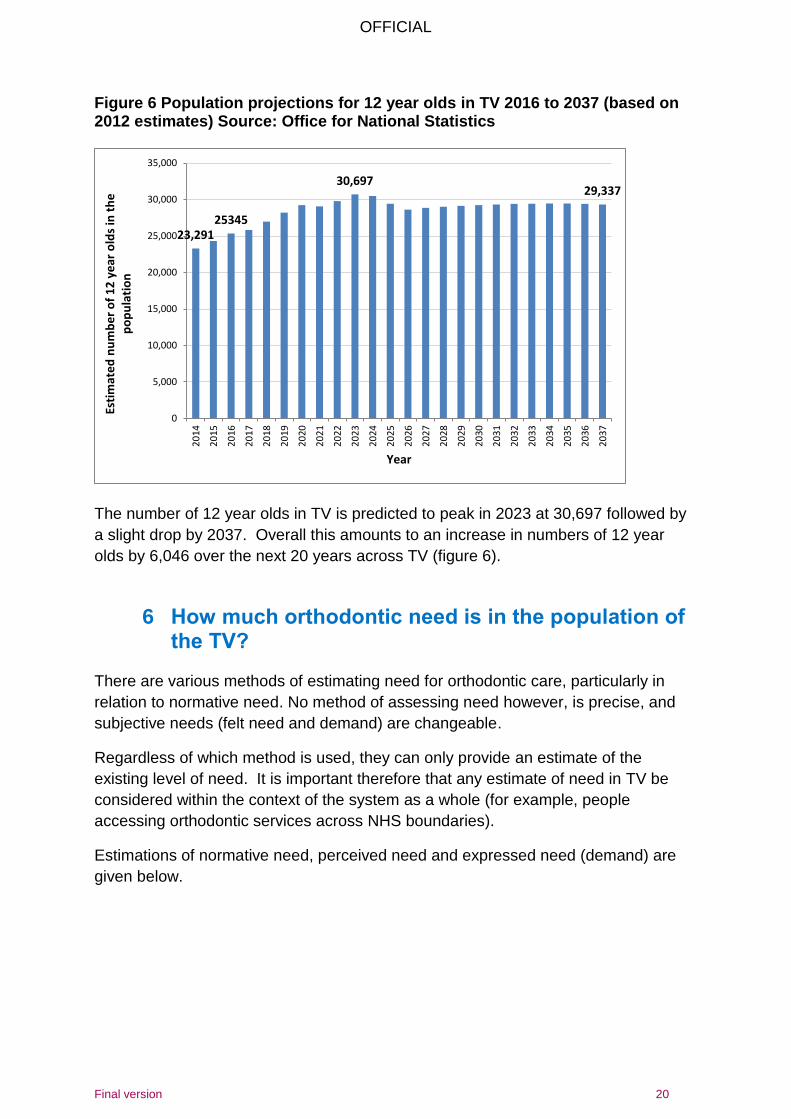
Figure 6 Population projections for 12 year olds in TV 2016 to 2037 (based on 2012 estimates) Source: Office for National Statistics
The number of 12 year olds in TV is predicted to peak in 2023 at 30,697 followed by
a slight drop by 2037. Overall this amounts to an increase in numbers of 12 year
olds by 6,046 over the next 20 years across TV (figure 6).
6 How much orthodontic need is in the population of the TV?
There are various methods of estimating need for orthodontic care, particularly in
relation to normative need. No method of assessing need however, is precise, and
subjective needs (felt need and demand) are changeable.
Regardless of which method is used, they can only provide an estimate of the
existing level of need. It is important therefore that any estimate of need in TV be
considered within the context of the system as a whole (for example, people
accessing orthodontic services across NHS boundaries).
Estimations of normative need, perceived need and expressed need (demand) are
given below.
23,291 25345
30,697 29,337
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
20
14
20
15
20
16
20
17
20
18
20
19
20
20
20
21
20
22
20
23
20
24
20
25
20
26
20
27
20
28
20
29
20
30
20
31
20
32
20
33
20
34
20
35
20
36
20
37
Esti
mat
ed
nu
mb
er
of
12
ye
ar o
lds
in t
he
p
op
ula
tio
n
Year
OFFICIAL
Final version 21
6.1 Normative need
There are various methods of estimating orthodontic normative need. No method
however, is precise. This report describes three methods:
1. Survey method
2. Stephen’s formula method
3. The rule of ‘a third’
The findings of these analyses are discussed below.
1.1 Survey method to estimate normative need
Orthodontic need is not routinely measured through dental epidemiological surveys.
There are two sources of epidemiological data for Orthodontics in England: national
Children’s Dental Health Surveys and Local Dental Epidemiology Programme
surveys (DEP). Both surveys assess need using a modified Index of Orthodontic.
The survey does not recognise a child with an IOTN 3.6-3.7 as having a treatment
need, whereas a child with this IOTN would be eligible for treatment on the NHS.
This means that these figures will slightly underestimate the need for Orthodontic
care according to NHS IOTN threshold.
6.1.1.1 National epidemiological survey Nationally the proportion of children identified as having a need for Orthodontic
treatment in the Children’s Dental Health surveys is around 40% (figure 7).
Figure 7. Summary of level of treatment need as measured by consecutive Children’s Dental Health Surveys, 2003 and 2013
Year % in treatment % treatment need
% total need
2003 8 35 43
2013 20 Not gathered Not gathered
6.1.1.2 Local epidemiological survey The most recent Dental Epidemiology Programme survey that included an
orthodontic element was in 2008/9. It involved the examination of a sample of
children attending mainstream schools who were aged 12 years at the time of the
survey.7 One of the conditions looked at in this survey was orthodontic need and
demand.
This survey did not produce TV level results as NHS boundaries in 2008/9 did not
match today’s boundaries. The survey did however, give results by local authority
and, from this, weighted estimates can be calculated for TV (figure 8).
OFFICIAL
Final version 22
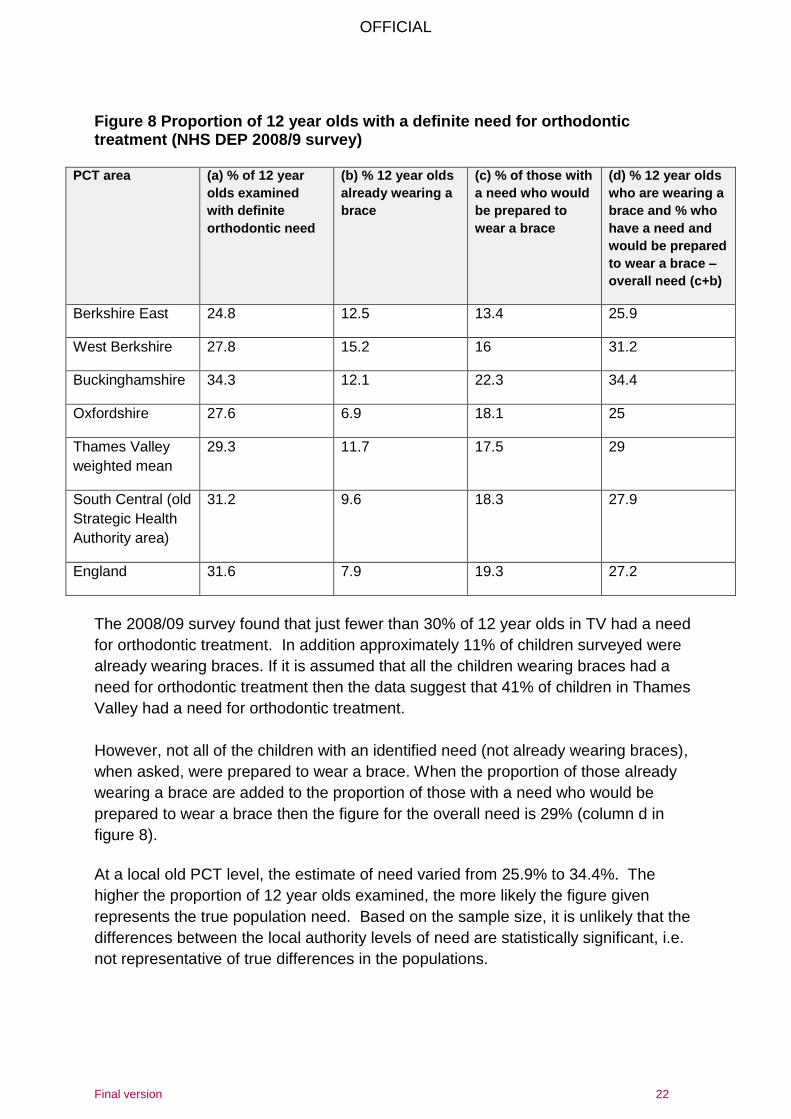
Figure 8 Proportion of 12 year olds with a definite need for orthodontic treatment (NHS DEP 2008/9 survey)
PCT area (a) % of 12 year
olds examined
with definite
orthodontic need
(b) % 12 year olds
already wearing a
brace
(c) % of those with
a need who would
be prepared to
wear a brace
(d) % 12 year olds
who are wearing a
brace and % who
have a need and
would be prepared
to wear a brace –
overall need (c+b)
Berkshire East 24.8 12.5 13.4 25.9
West Berkshire 27.8 15.2 16 31.2
Buckinghamshire 34.3 12.1 22.3 34.4
Oxfordshire 27.6 6.9 18.1 25
Thames Valley
weighted mean
29.3 11.7 17.5 29
South Central (old
Strategic Health
Authority area)
31.2 9.6 18.3 27.9
England 31.6 7.9 19.3 27.2
The 2008/09 survey found that just fewer than 30% of 12 year olds in TV had a need
for orthodontic treatment. In addition approximately 11% of children surveyed were
already wearing braces. If it is assumed that all the children wearing braces had a
need for orthodontic treatment then the data suggest that 41% of children in Thames
Valley had a need for orthodontic treatment.
However, not all of the children with an identified need (not already wearing braces),
when asked, were prepared to wear a brace. When the proportion of those already
wearing a brace are added to the proportion of those with a need who would be
prepared to wear a brace then the figure for the overall need is 29% (column d in
figure 8).
At a local old PCT level, the estimate of need varied from 25.9% to 34.4%. The
higher the proportion of 12 year olds examined, the more likely the figure given
represents the true population need. Based on the sample size, it is unlikely that the
differences between the local authority levels of need are statistically significant, i.e.
not representative of true differences in the populations.
OFFICIAL
Final version 23
By extrapolating the proportion of the population of 12 year old with need and
demand to the current population size it is possible to estimate the numbers of 12
year olds that may benefit from treatment (figure 9).
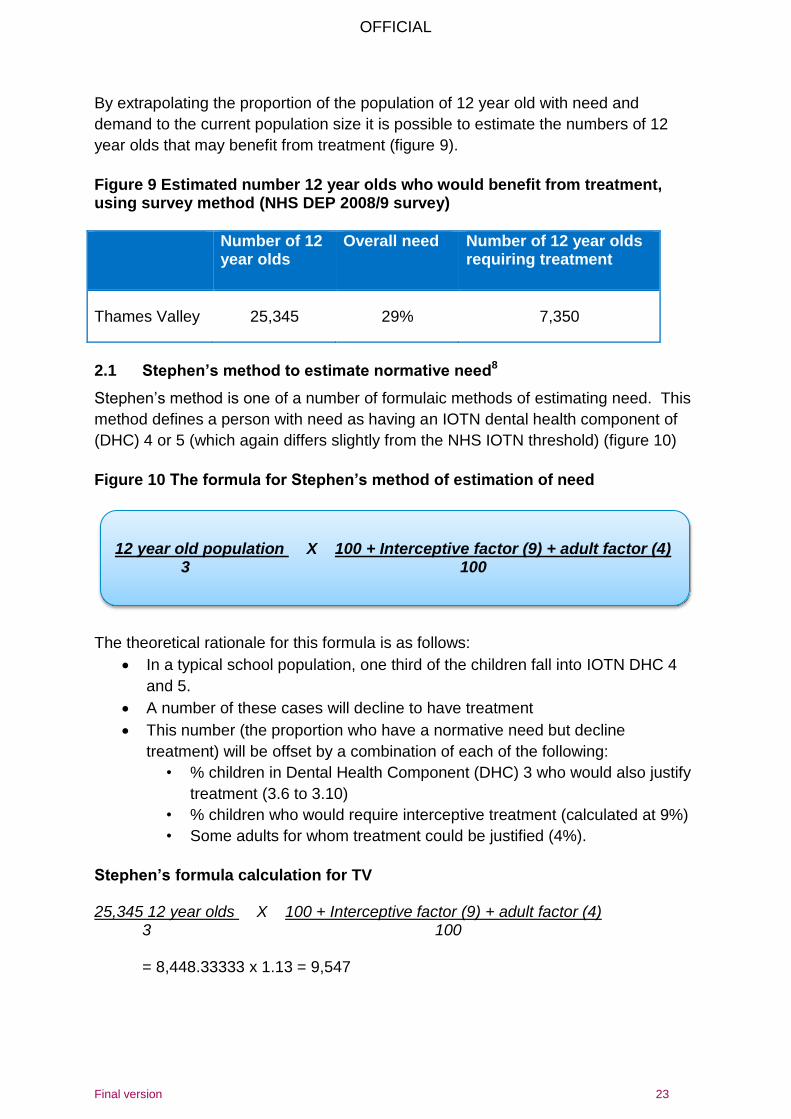
Figure 9 Estimated number 12 year olds who would benefit from treatment, using survey method (NHS DEP 2008/9 survey)
Number of 12 year olds
Overall need Number of 12 year olds requiring treatment
Thames Valley 25,345 29% 7,350
2.1 Stephen’s method to estimate normative need8
Stephen’s method is one of a number of formulaic methods of estimating need. This
method defines a person with need as having an IOTN dental health component of
(DHC) 4 or 5 (which again differs slightly from the NHS IOTN threshold) (figure 10)
Figure 10 The formula for Stephen’s method of estimation of need
The theoretical rationale for this formula is as follows:
In a typical school population, one third of the children fall into IOTN DHC 4
and 5.
A number of these cases will decline to have treatment
This number (the proportion who have a normative need but decline
treatment) will be offset by a combination of each of the following:
• % children in Dental Health Component (DHC) 3 who would also justify
treatment (3.6 to 3.10)
• % children who would require interceptive treatment (calculated at 9%)
• Some adults for whom treatment could be justified (4%).
Stephen’s formula calculation for TV 25,345 12 year olds X 100 + Interceptive factor (9) + adult factor (4) 3 100 = 8,448.33333 x 1.13 = 9,547
12 year old population X 100 + Interceptive factor (9) + adult factor (4)
3 100
OFFICIAL
Final version 24
Therefore the Stephen’s method estimates that 9,547 individuals in TV will have
need for treatment.
3.1 The rule of ‘a third’ to estimate normative need
Evidence from national surveys and literature suggest that around 33% of 12-year-
olds have an objective need for orthodontic treatment (figure 11). In a typical school
population, one third of the children fall into IOTN categories 4 and 5. This method of
estimation is supported by the NHS England commissioning guide for orthodontics.1
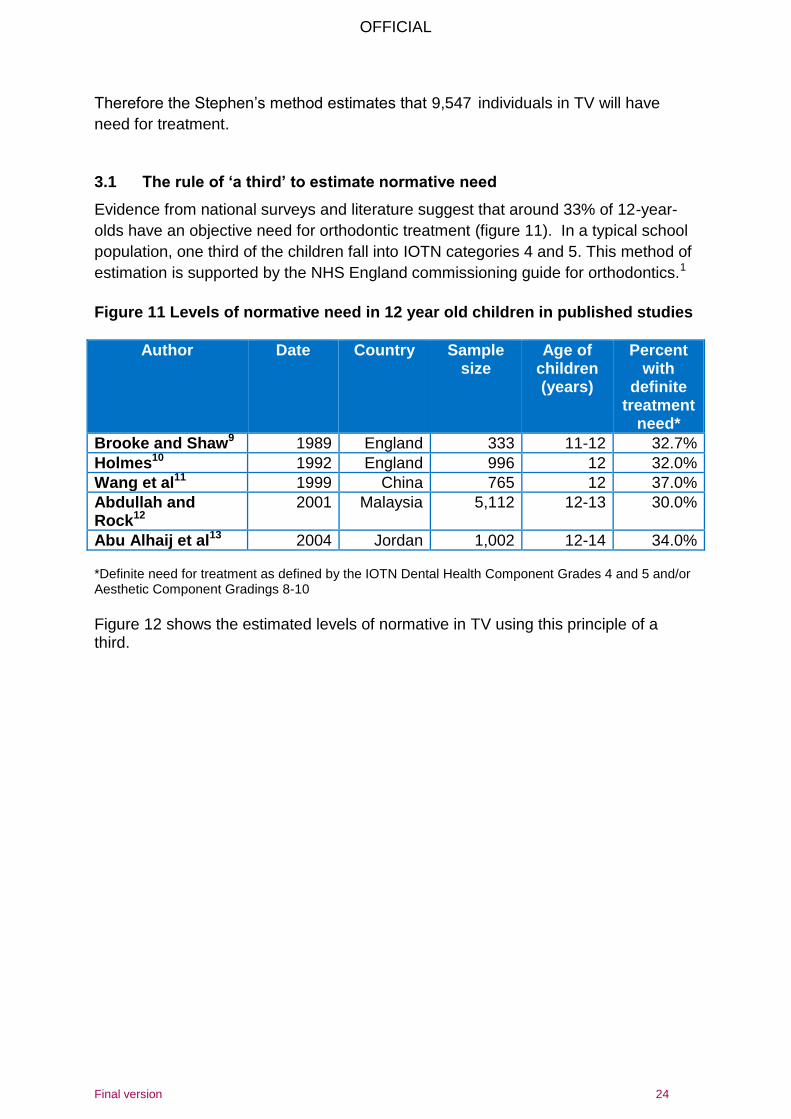
Figure 11 Levels of normative need in 12 year old children in published studies
Author Date Country Sample size
Age of children (years)
Percent with
definite treatment
need*
Brooke and Shaw9 1989 England 333 11-12 32.7%
Holmes10 1992 England 996 12 32.0%
Wang et al11 1999 China 765 12 37.0%
Abdullah and Rock12
2001 Malaysia 5,112 12-13 30.0%
Abu Alhaij et al13 2004 Jordan 1,002 12-14 34.0% *Definite need for treatment as defined by the IOTN Dental Health Component Grades 4 and 5 and/or Aesthetic Component Gradings 8-10
Figure 12 shows the estimated levels of normative in TV using this principle of a third.
OFFICIAL
Final version 25
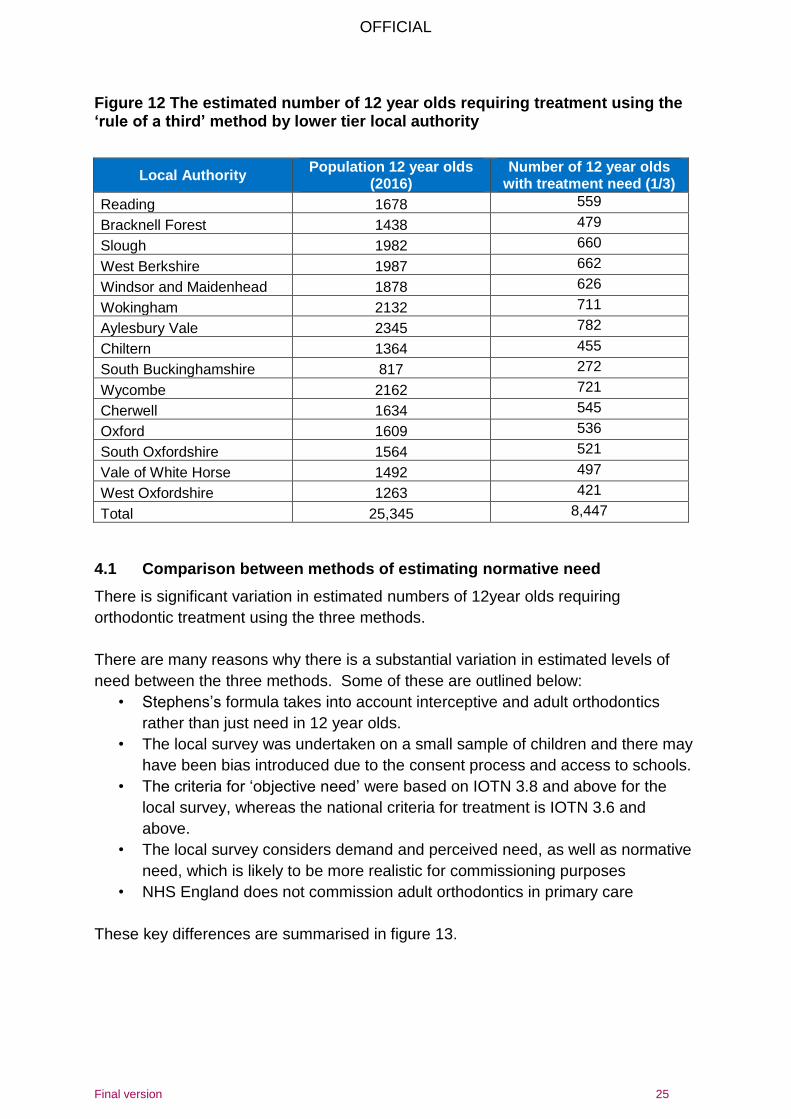
Figure 12 The estimated number of 12 year olds requiring treatment using the ‘rule of a third’ method by lower tier local authority
Local Authority Population 12 year olds
(2016) Number of 12 year olds
with treatment need (1/3)
Reading 1678 559
Bracknell Forest 1438 479
Slough 1982 660
West Berkshire 1987 662
Windsor and Maidenhead 1878 626
Wokingham 2132 711
Aylesbury Vale 2345 782
Chiltern 1364 455
South Buckinghamshire 817 272
Wycombe 2162 721
Cherwell 1634 545
Oxford 1609 536
South Oxfordshire 1564 521
Vale of White Horse 1492 497
West Oxfordshire 1263 421
Total 25,345 8,447
4.1 Comparison between methods of estimating normative need
There is significant variation in estimated numbers of 12year olds requiring
orthodontic treatment using the three methods.
There are many reasons why there is a substantial variation in estimated levels of
need between the three methods. Some of these are outlined below:
• Stephens’s formula takes into account interceptive and adult orthodontics
rather than just need in 12 year olds.
• The local survey was undertaken on a small sample of children and there may
have been bias introduced due to the consent process and access to schools.
• The criteria for ‘objective need’ were based on IOTN 3.8 and above for the
local survey, whereas the national criteria for treatment is IOTN 3.6 and
above.
• The local survey considers demand and perceived need, as well as normative
need, which is likely to be more realistic for commissioning purposes
• NHS England does not commission adult orthodontics in primary care
These key differences are summarised in figure 13.
OFFICIAL
Final version 26
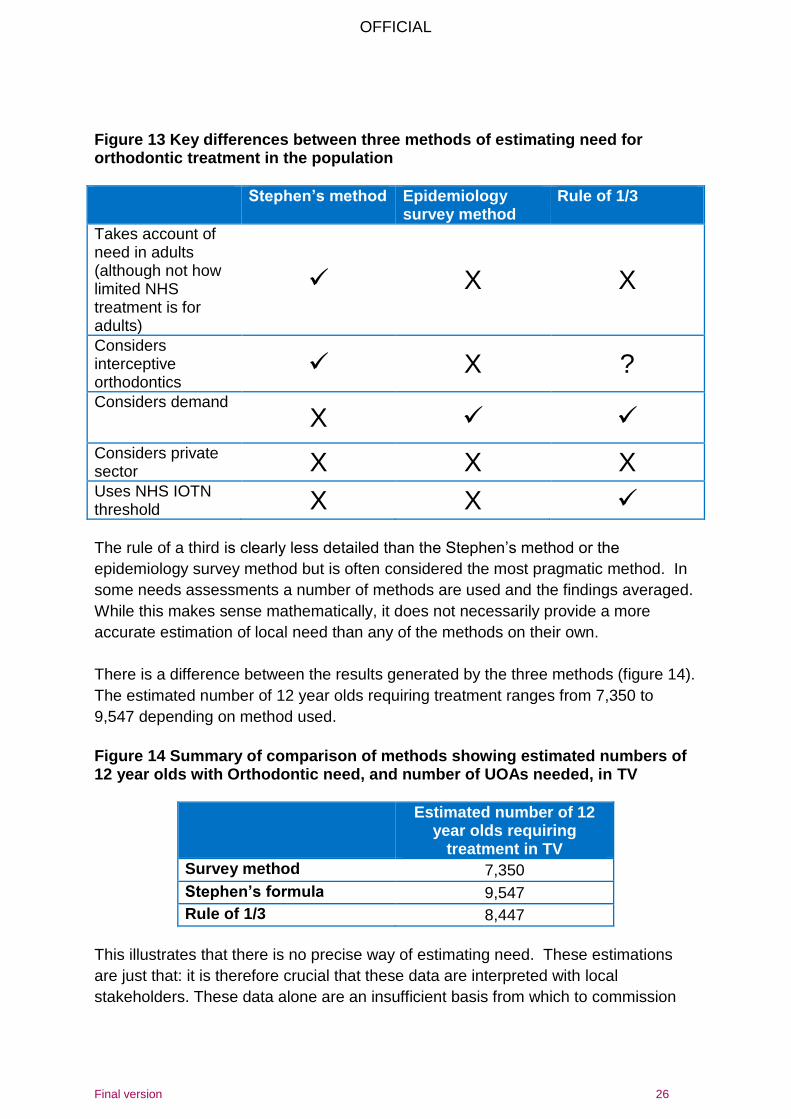
Figure 13 Key differences between three methods of estimating need for orthodontic treatment in the population
Stephen’s method Epidemiology survey method
Rule of 1/3
Takes account of need in adults (although not how limited NHS treatment is for adults)
X X
Considers interceptive orthodontics
X ?
Considers demand
X
Considers private sector X X X Uses NHS IOTN threshold X X The rule of a third is clearly less detailed than the Stephen’s method or the
epidemiology survey method but is often considered the most pragmatic method. In
some needs assessments a number of methods are used and the findings averaged.
While this makes sense mathematically, it does not necessarily provide a more
accurate estimation of local need than any of the methods on their own.
There is a difference between the results generated by the three methods (figure 14).
The estimated number of 12 year olds requiring treatment ranges from 7,350 to
9,547 depending on method used.
Figure 14 Summary of comparison of methods showing estimated numbers of 12 year olds with Orthodontic need, and number of UOAs needed, in TV
Estimated number of 12 year olds requiring
treatment in TV
Survey method 7,350
Stephen’s formula 9,547
Rule of 1/3 8,447
This illustrates that there is no precise way of estimating need. These estimations
are just that: it is therefore crucial that these data are interpreted with local
stakeholders. These data alone are an insufficient basis from which to commission
OFFICIAL
Final version 27
services and must only be used in the context of understanding the strengths and
weaknesses of the wider Orthodontic system.
For the purposes of this needs assessment the figures obtained by using the third
rule are used in calculations in this document. This is to ensure that this document is
consistent with the NHS England orthodontic commissioning guide and the other
needs assessments being completed across the south of England as part of the NHS
south wide orthodontic procurement project. This method also gives and estimation
of need which represents the mid-range of the three methods.
6.2 Perceived need and demand
Perceived need varies between individuals, is inconsistent even at the same IOTN,
and is difficult to predict with accuracy. Demand for orthodontic treatment has
increased substantially and continues to increase.1
Demand is likely to be greater in females and children from higher socio-economic
groups.15
It is therefore not possible to predict demand by looking at levels of normative need
alone. Children with a more extreme malocclusion are more likely to demand
treatment than those without. That said, demand can be absent in children with a
high need and present in others with no objective need. This means that there are
groups in society who do not receive orthodontic care but who may benefit from it.14
The NHSDEP 2008/9 survey provides local data on perceived need and demand. In
the survey, 12 year olds were asked a number of questions7:
1. “Have you got an orthodontic brace or appliance?”
2. “Do you think your teeth need straightening?”
3. “Would you be prepared to have treatment and wear a brace if it were
necessary?”
Question 2 relates to perceived need. Question 3 indicates potential demand. The
findings are summarised in figure 15.
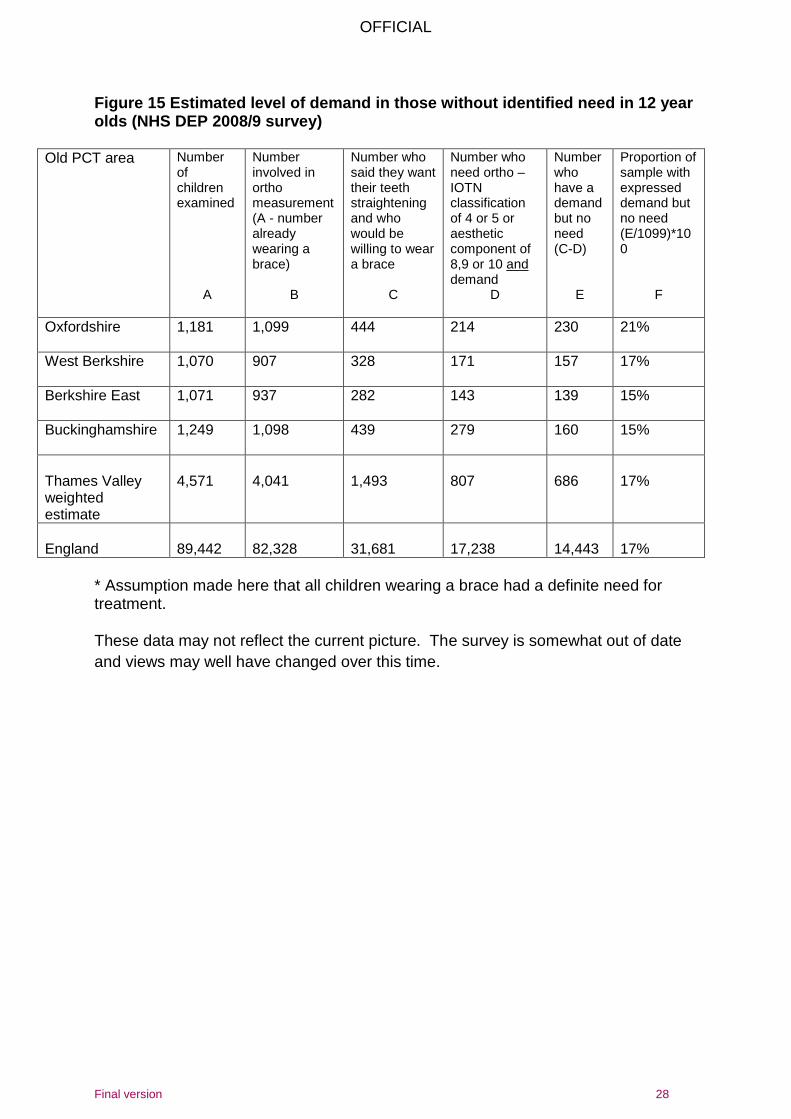
There are no routinely collected data on demand in TV. The only estimate available
is from the 2008/09 survey which suggested that (figure 15):
In all areas of Thames Valley there are more children who want to wear a
brace than actually need it. This finding is most pronounced in Oxfordshire
where 21% of children examined said they would like and prepared to have
orthodontic treatment but did not have an identified need.
OFFICIAL
Final version 28
Figure 15 Estimated level of demand in those without identified need in 12 year olds (NHS DEP 2008/9 survey)
Old PCT area Number of children examined
A
Number involved in ortho measurement (A - number already wearing a brace)
B
Number who said they want their teeth straightening and who would be willing to wear a brace
C
Number who need ortho – IOTN classification of 4 or 5 or aesthetic component of 8,9 or 10 and demand
D
Number who have a demand but no need (C-D)
E
Proportion of sample with expressed demand but no need (E/1099)*100
F
Oxfordshire 1,181 1,099 444 214 230 21%
West Berkshire 1,070 907 328 171 157 17%
Berkshire East 1,071 937 282 143 139 15%
Buckinghamshire 1,249 1,098 439 279 160 15%
Thames Valley weighted estimate
4,571
4,041
1,493
807
686
17%
England
89,442
82,328
31,681
17,238
14,443
17%
* Assumption made here that all children wearing a brace had a definite need for treatment. These data may not reflect the current picture. The survey is somewhat out of date
and views may well have changed over this time.
OFFICIAL
Final version 29
7 How much Orthodontics is being commissioned for Thames Valley residents in primary care?
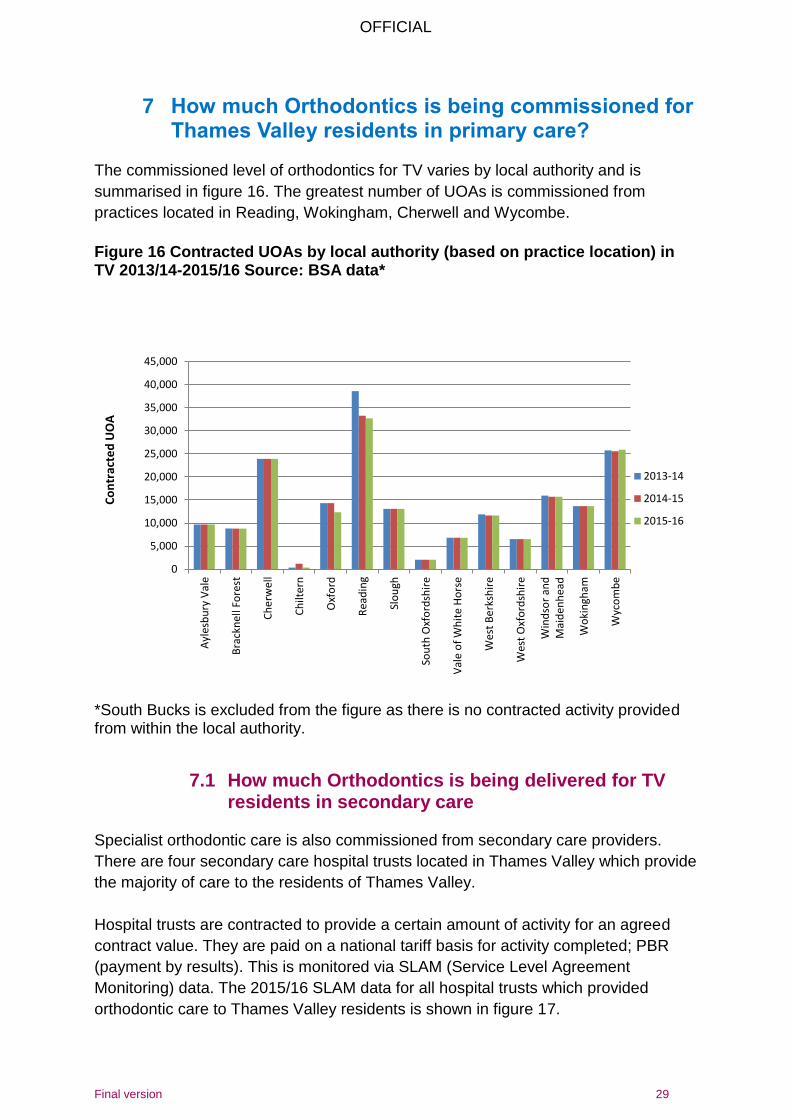
The commissioned level of orthodontics for TV varies by local authority and is
summarised in figure 16. The greatest number of UOAs is commissioned from
practices located in Reading, Wokingham, Cherwell and Wycombe.
Figure 16 Contracted UOAs by local authority (based on practice location) in TV 2013/14-2015/16 Source: BSA data*
*South Bucks is excluded from the figure as there is no contracted activity provided from within the local authority.
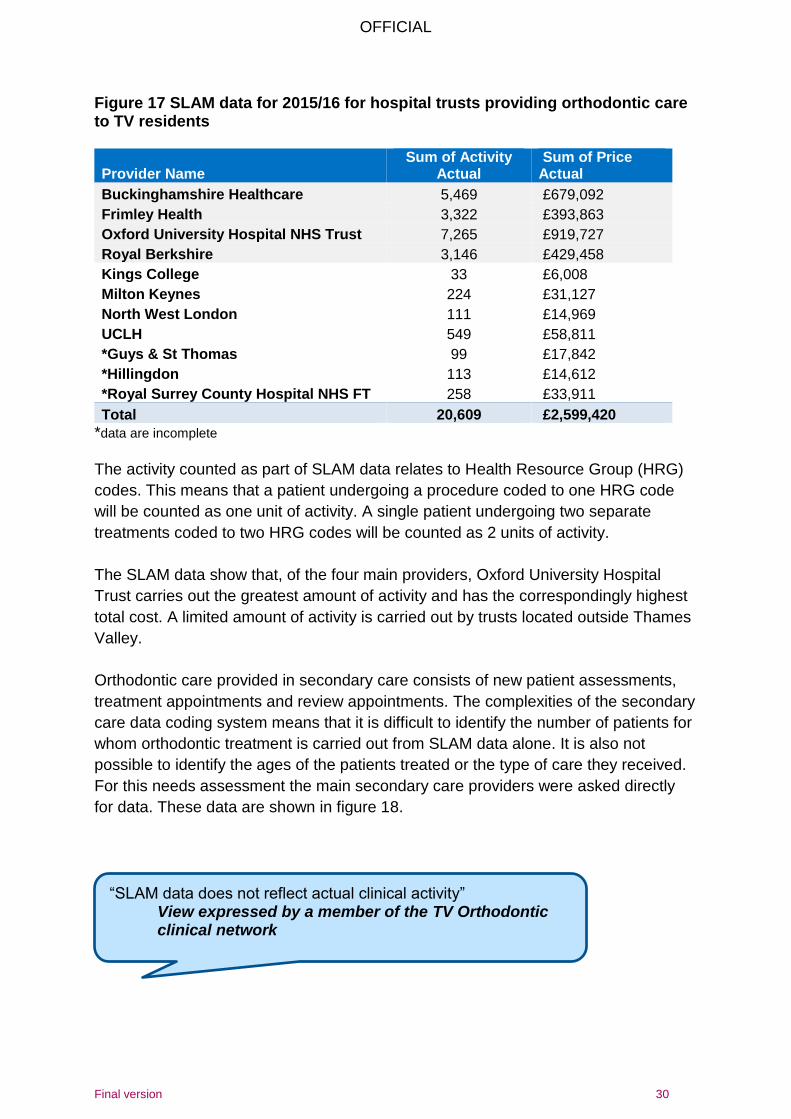
7.1 How much Orthodontics is being delivered for TV residents in secondary care
Specialist orthodontic care is also commissioned from secondary care providers.
There are four secondary care hospital trusts located in Thames Valley which provide
the majority of care to the residents of Thames Valley.
Hospital trusts are contracted to provide a certain amount of activity for an agreed
contract value. They are paid on a national tariff basis for activity completed; PBR
(payment by results). This is monitored via SLAM (Service Level Agreement
Monitoring) data. The 2015/16 SLAM data for all hospital trusts which provided
orthodontic care to Thames Valley residents is shown in figure 17.
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
e H
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
dM
aid
enh
ead
Wo
kin
gham
Wyc
om
be
Co
ntr
acte
d U
OA
2013-14
2014-15
2015-16
OFFICIAL
Final version 30
Figure 17 SLAM data for 2015/16 for hospital trusts providing orthodontic care to TV residents
Provider Name Sum of Activity
Actual Sum of Price Actual
Buckinghamshire Healthcare 5,469 £679,092
Frimley Health 3,322 £393,863
Oxford University Hospital NHS Trust 7,265 £919,727
Royal Berkshire 3,146 £429,458
Kings College 33 £6,008
Milton Keynes 224 £31,127
North West London 111 £14,969
UCLH 549 £58,811
*Guys & St Thomas 99 £17,842
*Hillingdon 113 £14,612
*Royal Surrey County Hospital NHS FT 258 £33,911
Total 20,609 £2,599,420
*data are incomplete
The activity counted as part of SLAM data relates to Health Resource Group (HRG)
codes. This means that a patient undergoing a procedure coded to one HRG code
will be counted as one unit of activity. A single patient undergoing two separate
treatments coded to two HRG codes will be counted as 2 units of activity.
The SLAM data show that, of the four main providers, Oxford University Hospital
Trust carries out the greatest amount of activity and has the correspondingly highest
total cost. A limited amount of activity is carried out by trusts located outside Thames
Valley.
Orthodontic care provided in secondary care consists of new patient assessments,
treatment appointments and review appointments. The complexities of the secondary
care data coding system means that it is difficult to identify the number of patients for
whom orthodontic treatment is carried out from SLAM data alone. It is also not
possible to identify the ages of the patients treated or the type of care they received.
For this needs assessment the main secondary care providers were asked directly
for data. These data are shown in figure 18.
“SLAM data does not reflect actual clinical activity” View expressed by a member of the TV Orthodontic clinical network
OFFICIAL
Final version 31
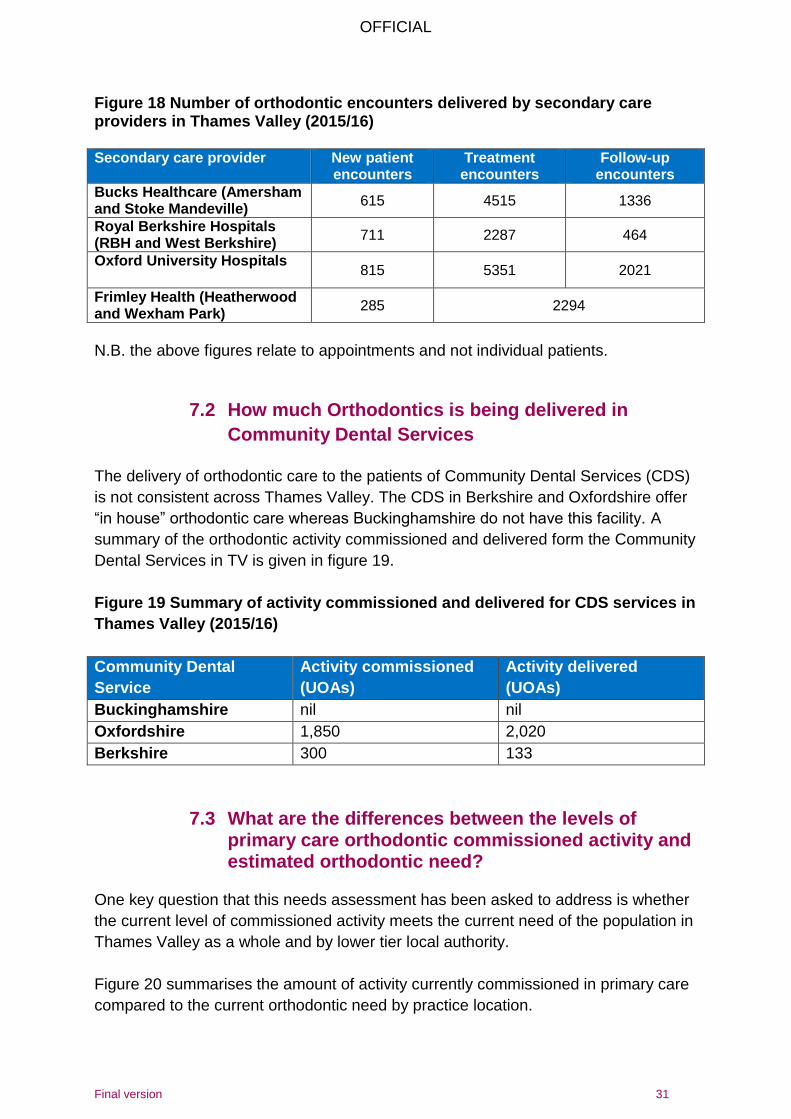
Figure 18 Number of orthodontic encounters delivered by secondary care providers in Thames Valley (2015/16) Secondary care provider New patient
encounters Treatment encounters
Follow-up encounters
Bucks Healthcare (Amersham and Stoke Mandeville)
615 4515 1336
Royal Berkshire Hospitals (RBH and West Berkshire)
711 2287 464
Oxford University Hospitals 815 5351 2021
Frimley Health (Heatherwood and Wexham Park)
285 2294
N.B. the above figures relate to appointments and not individual patients.
7.2 How much Orthodontics is being delivered in
Community Dental Services
The delivery of orthodontic care to the patients of Community Dental Services (CDS)
is not consistent across Thames Valley. The CDS in Berkshire and Oxfordshire offer
“in house” orthodontic care whereas Buckinghamshire do not have this facility. A
summary of the orthodontic activity commissioned and delivered form the Community
Dental Services in TV is given in figure 19.
Figure 19 Summary of activity commissioned and delivered for CDS services in
Thames Valley (2015/16)
Community Dental
Service
Activity commissioned
(UOAs)
Activity delivered
(UOAs)
Buckinghamshire nil nil
Oxfordshire 1,850 2,020
Berkshire 300 133
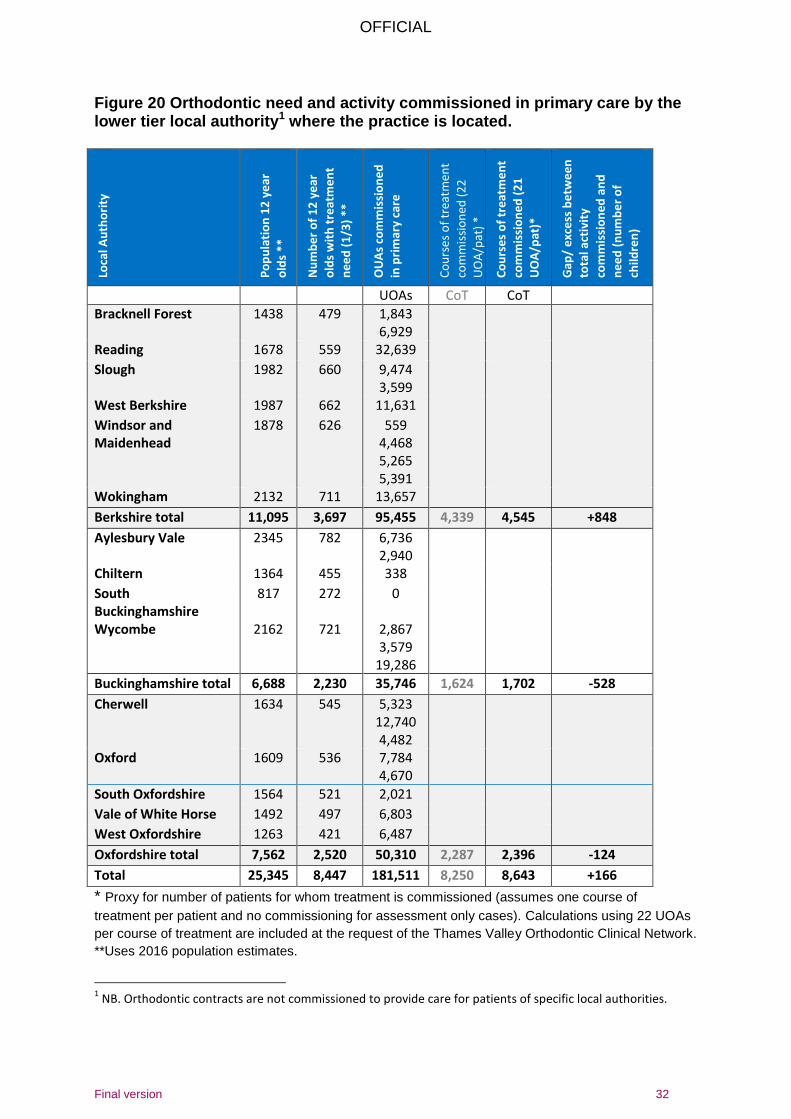
7.3 What are the differences between the levels of primary care orthodontic commissioned activity and estimated orthodontic need?
One key question that this needs assessment has been asked to address is whether
the current level of commissioned activity meets the current need of the population in
Thames Valley as a whole and by lower tier local authority.
Figure 20 summarises the amount of activity currently commissioned in primary care
compared to the current orthodontic need by practice location.
OFFICIAL
Final version 32
Figure 20 Orthodontic need and activity commissioned in primary care by the lower tier local authority1 where the practice is located.
Loca
l Au
tho
rity
Po
pu
lati
on
12
ye
ar
old
s **
Nu
mb
er
of
12
ye
ar
old
s w
ith
tre
atm
en
t
ne
ed
(1
/3)
**
OU
As
com
mis
sio
ne
d
in p
rim
ary
care
Co
urs
es
of
trea
tmen
t
com
mis
sio
ned
(2
2
UO
A/p
at)
*
Co
urs
es
of
tre
atm
en
t
com
mis
sio
ne
d (
21
UO
A/p
at)*
Gap
/ e
xce
ss b
etw
ee
n
tota
l act
ivit
y
com
mis
sio
ne
d a
nd
ne
ed
(n
um
be
r o
f
child
ren
)
UOAs CoT CoT
Bracknell Forest 1438 479 1,843 6,929
Reading 1678 559 32,639
Slough 1982 660 9,474 3,599
West Berkshire 1987 662 11,631
Windsor and Maidenhead
1878 626 559 4,468 5,265 5,391
Wokingham 2132 711 13,657
Berkshire total 11,095 3,697 95,455 4,339 4,545 +848
Aylesbury Vale 2345 782 6,736 2,940
Chiltern 1364 455 338
South Buckinghamshire
817 272 0
Wycombe 2162 721 2,867 3,579
19,286
Buckinghamshire total 6,688 2,230 35,746 1,624 1,702 -528
Cherwell 1634 545 5,323 12,740 4,482
Oxford 1609 536 7,784 4,670
South Oxfordshire 1564 521 2,021
Vale of White Horse 1492 497 6,803
West Oxfordshire 1263 421 6,487
Oxfordshire total 7,562 2,520 50,310 2,287 2,396 -124
Total 25,345 8,447 181,511 8,250 8,643 +166
* Proxy for number of patients for whom treatment is commissioned (assumes one course of
treatment per patient and no commissioning for assessment only cases). Calculations using 22 UOAs
per course of treatment are included at the request of the Thames Valley Orthodontic Clinical Network.
**Uses 2016 population estimates.
1 NB. Orthodontic contracts are not commissioned to provide care for patients of specific local authorities.
OFFICIAL
Final version 33
At the request of the NHS England commissioners the calculations in figure 20 are
based on the assumption that each course of treatment will attract 21 UOAs. The
table does not include activity commissioned from secondary care and community
dental services so underestimates the total orthodontic activity commissioned.
From the data in figure 20 it can be seen that currently across Thames Valley the
estimated orthodontic need of the population is met by the activity commissioned in
primary care. There is an estimated excess of 166 i.e. it is estimated that there are
166 more courses of treatment commissioned in primary care than the estimated
need. This equates to 2% of the total population in need. As activity provided by
secondary care and community dental services are not included in table 20 the figure
of 166 underestimates the excess activity commissioned compared to need.
The data also show that when need and commissioned activity are looked at by
lower tier local authority the picture is variable. The data suggest that in Berkshire
there is more commissioned activity than need whereas in Buckinghamshire and
Oxfordshire there is less commissioned activity than need.
However, the orthodontic contracts in Thames Valley are all PDS (personal Dental
Service) contracts. This means that there are no geographical restrictions placed on
them and they can draw patients from any local authority area. Patients do not
recognise local authority boundaries when seeking care and will travel to the practice
which is the most convenient for them or choose to seek care from a practice
because of reputation or waiting times. Therefore using local authority boundaries for
the planning the future location of services may not be appropriate.
The current geographical distribution of orthodontic practices in Thames Valley is not
due to active commissioning; that is practices were set up, prior to 2006, in locations
determined by providers. These practices have continued with little change since the
advent of the new dental contract in 2006. With the decision to re-commission
services across Thames Valley there is an opportunity to re-visit the geographical
distribution and ensure that practices are located in the most appropriate areas.
When planning future services it is necessary to take into account that patients do
not access care within the confines of the local authority in which they live and that
new contracts will also be PDS contracts and so will not have geographical
boundaries.
“..need to look at population density as patient flows don’t just happen within local authority boundaries.”
View expressed by a member of the TV Orthodontic clinical network
OFFICIAL
Final version 34
An alternative way of determining the need and future location of practices across
Thames Valley is via mapping. The Thames Valley orthodontic clinical network made
the suggestion that future services should be provided from areas with high
population density and close to secondary schools. They asked if it would be
possible to provide a map of the main towns in Thames Valley with a circle drawn
round them (representing the area from which patients are drawn). A radius of 10km
was chosen for this map as it was felt that this was a reasonable distance for patients
to travel. The following towns were chosen:
a. Aylesbury b. High Wycombe c. Buckingham d. Amersham e. Banbury f. Bicester g. Abingdon h. Oxford i. Witney j. Thame k. Kidlington l. Reading m. Newbury n. Slough o. Bracknell PHE were approached to provide the mapping and the resulting map is shown in
figure 21.
“..need to look at acceptable travel distance radius around each practice.”
View expressed by a member of the TV Orthodontic clinical network
OFFICIAL
Final version 35
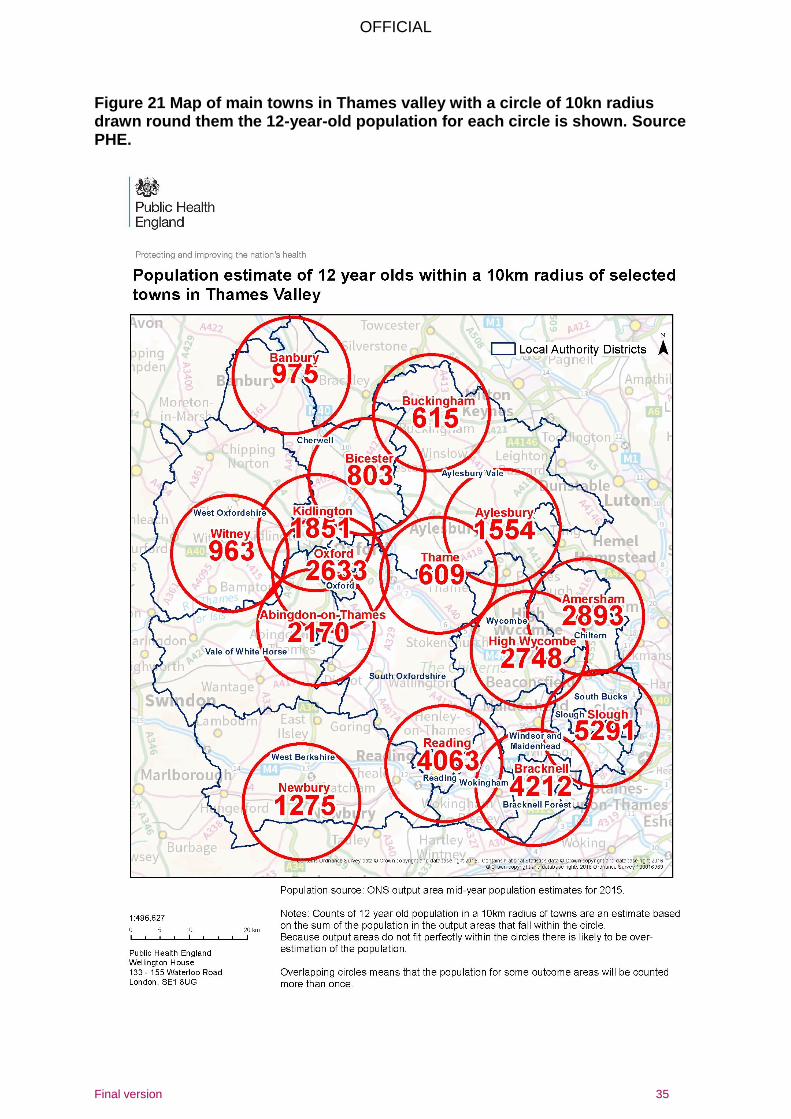
Figure 21 Map of main towns in Thames valley with a circle of 10kn radius drawn round them the 12-year-old population for each circle is shown. Source PHE.
OFFICIAL
Final version 36
The 12-year-old population of each of the circles is shown. It should be noted that
because of overlap the total population within the circles is greater than the actual
total 12-year-old population.
The map in figure 21 shows that there are some areas of Thames Valley which are
not included within the circles. These are largely rural areas. When considering the
location of lots for the future procurement of services the NHS will need to consider
how to address the gaps in these areas. As the population density is relatively low in
most of these areas one option is to accept that patients in these areas may have to
travel more than 10km to access specialist care. Local knowledge about patient flows
will also need to inform the choice of lots.
The findings from the map need to be considered along with the findings in figure 20
when choosing the location and particularly the size of lots. For example if the town
of Reading is looked at, figure 20 suggests that the current services commissioned
are considerably in excess of the need (1,554 courses of treatment commissioned
compared with a need of 559). However, if the need is expanded to a population
within 10km of Reading it increases to 1,354. This is much closer to the current
commissioned activity.
The above map was shared with the south orthodontic procurement working group
and it was considered to be a useful tool to inform the development of lots. It has
been agreed that similar maps will be requested for the whole of NHS south. These
maps will inform the decision on how much activity will be commissioned as part of
the procurement and where services will be commissioned from.
The map for Thames Valley, requested as part of the south procurement, has been
amended slightly from the one in figure 21. The epicentres and radii on the new map
are aimed to reduce overlap and ensure coverage of the whole of Thames Valley.
There will be one single map produced for the NHS South Central area
7.4 Commissioned activity and future need
The population of twelve-year-olds in Thames Valley is predicted in increase over the
next seven years peaking in 2023 at 30,697 (see section 5). This equates to an
increase of 10,232 compared to the population of 2016. Working on the assumption
that a third of this increase will have an orthodontic need there will be an additional
1,785 children in Thames Valley with a need for treatment by 2023.
If primary care orthodontic activity continues to be commissioned at 2016 levels then
there will not be sufficient orthodontic activity provided in primary care to meet this
additional need. However this gap assumes that all activity is delivered in primary
OFFICIAL
Final version 37
care and as the data in section 7.1 show there is a considerable amount of activity
delivered in secondary care. However, secondary care data has limitations and
ideally there should be further analysis of these data so that it can be determined
whether the current level of commissioned activity is sufficient to meet the need of
the growing population.
8 Primary care
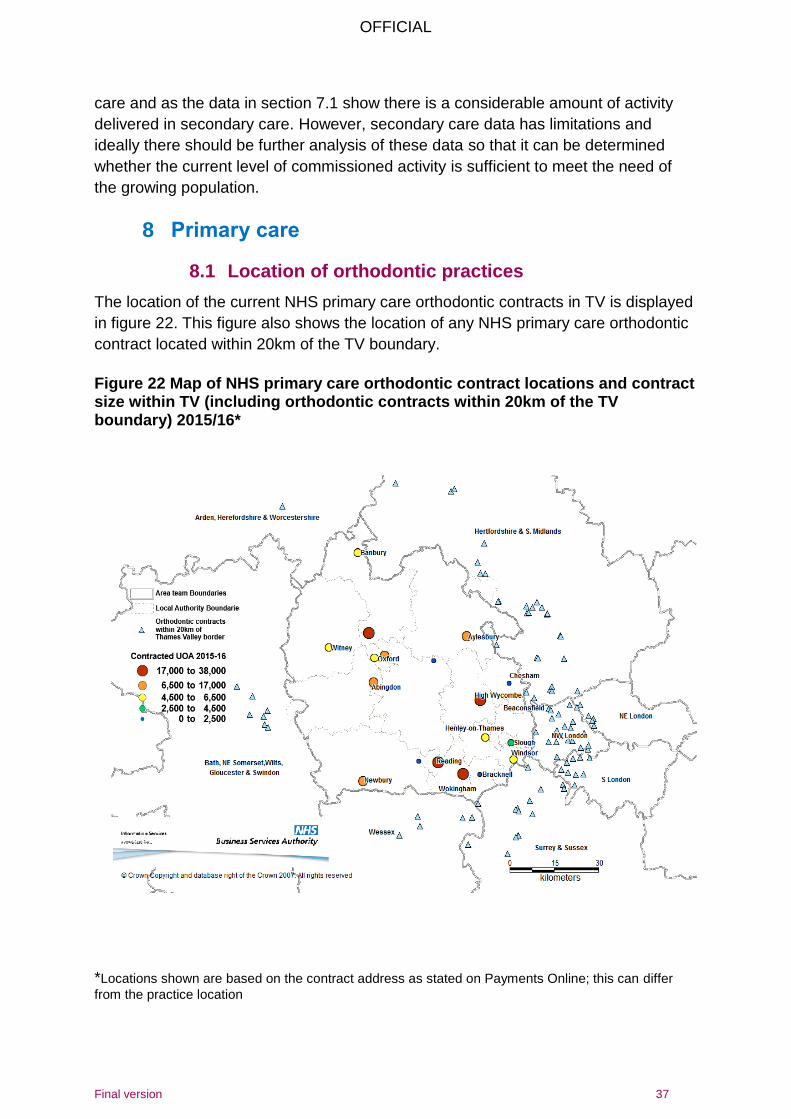
8.1 Location of orthodontic practices
The location of the current NHS primary care orthodontic contracts in TV is displayed
in figure 22. This figure also shows the location of any NHS primary care orthodontic
contract located within 20km of the TV boundary.
Figure 22 Map of NHS primary care orthodontic contract locations and contract size within TV (including orthodontic contracts within 20km of the TV boundary) 2015/16*
*Locations shown are based on the contract address as stated on Payments Online; this can differ
from the practice location
OFFICIAL
Final version 38
The map shows that whilst most areas in Thames Valley have orthodontic contracts
there are some areas which do not. These include South Buckinghamshire, Bicester
area, North Buckinghamshire, North West Oxfordshire and the area between
Abingdon and Newbury.
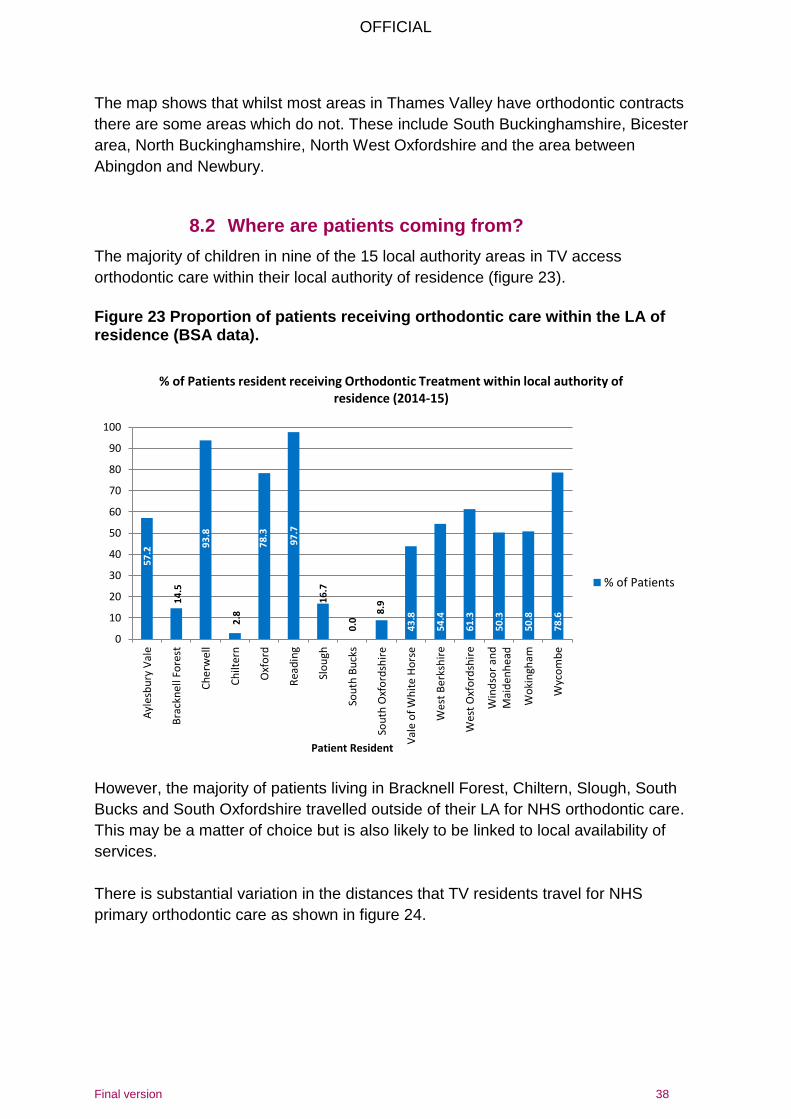
8.2 Where are patients coming from?
The majority of children in nine of the 15 local authority areas in TV access
orthodontic care within their local authority of residence (figure 23).
Figure 23 Proportion of patients receiving orthodontic care within the LA of residence (BSA data).
However, the majority of patients living in Bracknell Forest, Chiltern, Slough, South
Bucks and South Oxfordshire travelled outside of their LA for NHS orthodontic care.
This may be a matter of choice but is also likely to be linked to local availability of
services.
There is substantial variation in the distances that TV residents travel for NHS
primary orthodontic care as shown in figure 24.
57
.2
14
.5
93
.8
2.8
78
.3
97
.7
16
.7
0.0
8.9
43
.8
54
.4
61
.3
50
.3
50
.8
78
.6
0
10
20
30
40
50
60
70
80
90
100
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th B
uck
s
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
e H
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
dM
aid
enh
ead
Wo
kin
gham
Wyc
om
be
Patient Resident
% of Patients resident receiving Orthodontic Treatment within local authority of residence (2014-15)
% of Patients
OFFICIAL
Final version 39
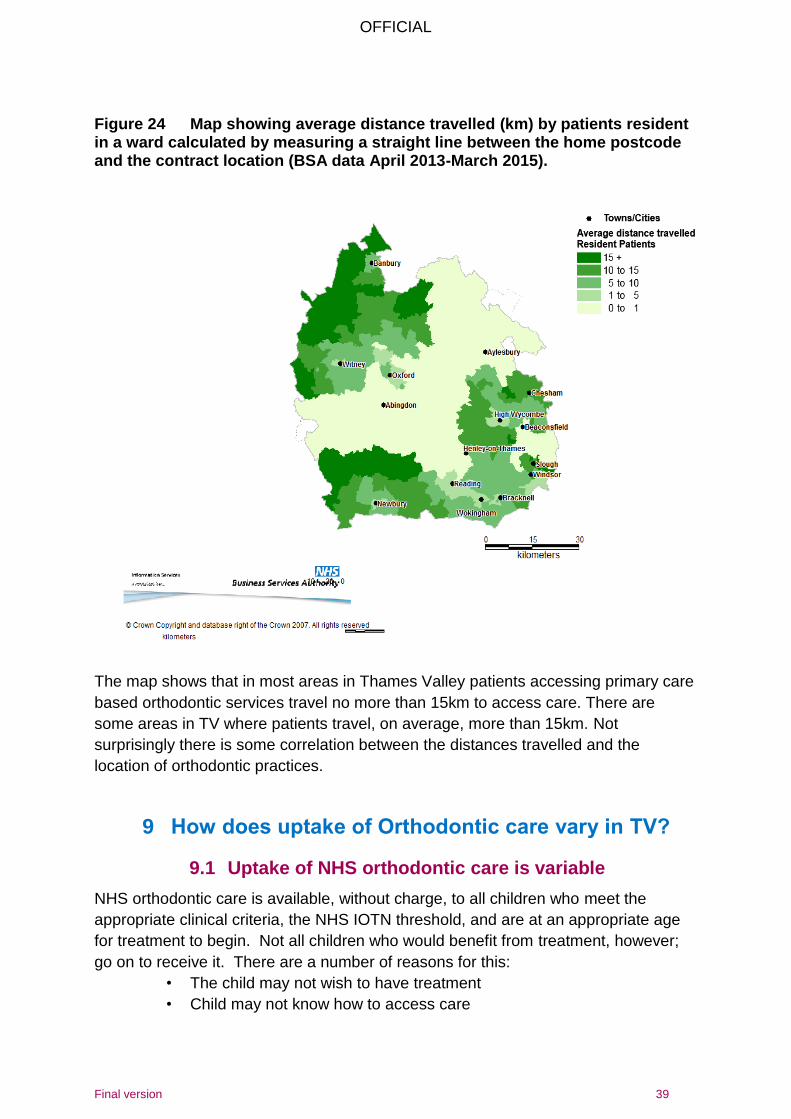
Figure 24 Map showing average distance travelled (km) by patients resident in a ward calculated by measuring a straight line between the home postcode and the contract location (BSA data April 2013-March 2015).
The map shows that in most areas in Thames Valley patients accessing primary care
based orthodontic services travel no more than 15km to access care. There are
some areas in TV where patients travel, on average, more than 15km. Not
surprisingly there is some correlation between the distances travelled and the
location of orthodontic practices.
9 How does uptake of Orthodontic care vary in TV?
9.1 Uptake of NHS orthodontic care is variable
NHS orthodontic care is available, without charge, to all children who meet the
appropriate clinical criteria, the NHS IOTN threshold, and are at an appropriate age
for treatment to begin. Not all children who would benefit from treatment, however;
go on to receive it. There are a number of reasons for this:
• The child may not wish to have treatment
• Child may not know how to access care

OFFICIAL
Final version 40
• Child/parent may not be aware that treatment is available free of charge
• Child may not attend the dentist who is gatekeeper
• Dentist may not suggest treatment if oral health is poor, e.g. poor oral
hygiene, active caries
Variations in uptake of NHS orthodontic care are seen by socio-economic status and gender.
9.2 Variation in uptake by age
BSA data suggests that the average age of children receiving primary care
orthodontic treatment in TV under the NHS is just under 13 years old (figure 25).
Across Thames Valley there is little variation in the average age at which patients
receive treatment.
Figure 25 At what age are patients receiving orthodontic treatment? BSA data 2014-15
9.3 Variation in uptake by socioeconomic status
National survey data show there is a significant difference in uptake of orthodontic
treatment in children who are eligible for free school meals compared with those who
are not. This can be used as a proxy for socioeconomic status. These data suggest
that children from lower socioeconomic groups are less likely to receive orthodontic
treatment by the time they are 15 than others (figure 26).
13
.2
12
.7
13
.2
12
.3
12
.9
12
.9
13
.3
12
.8
13
.0
13
.4
13
.3
13
.2
12
.6
12
.6
12
.3
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th B
uck
s
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
e H
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
dM
aid
enh
ead
Wo
kin
gham
Wyc
om
be
Ave
rage
Age
Patient Resident
Average Age Thames Valley
OFFICIAL
Final version 41
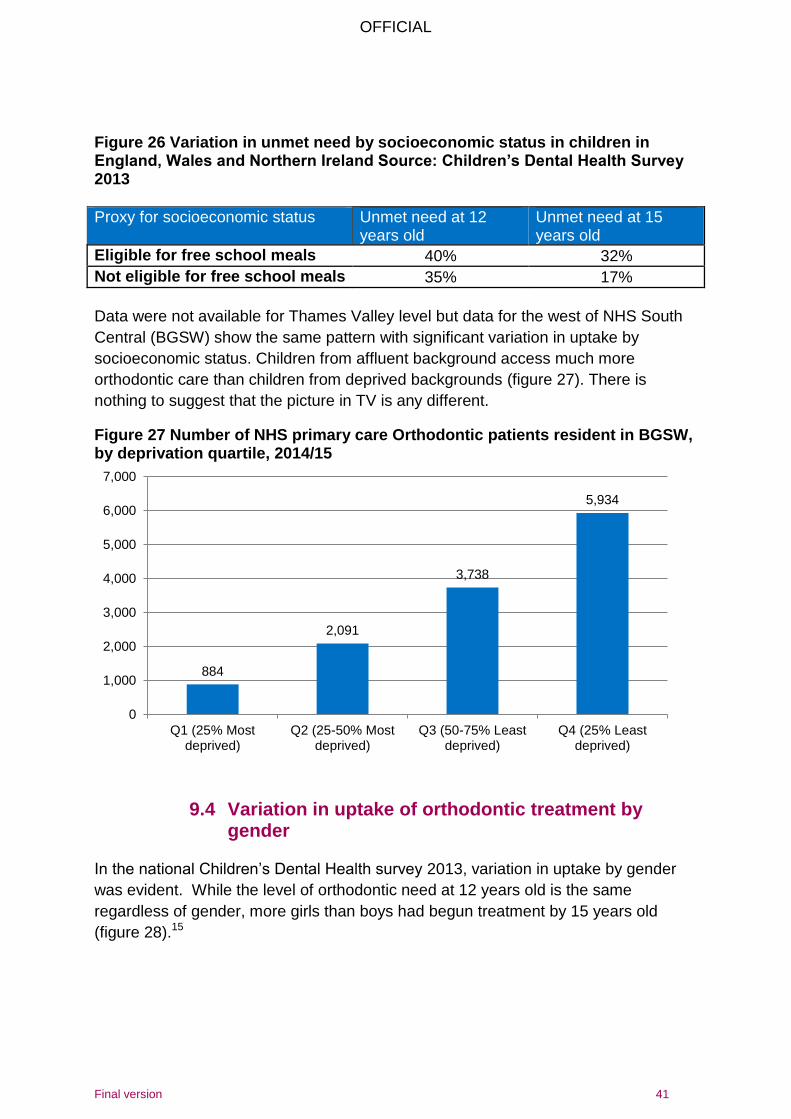
Figure 26 Variation in unmet need by socioeconomic status in children in England, Wales and Northern Ireland Source: Children’s Dental Health Survey 2013
Proxy for socioeconomic status Unmet need at 12 years old
Unmet need at 15 years old
Eligible for free school meals 40% 32%
Not eligible for free school meals 35% 17%
Data were not available for Thames Valley level but data for the west of NHS South
Central (BGSW) show the same pattern with significant variation in uptake by
socioeconomic status. Children from affluent background access much more
orthodontic care than children from deprived backgrounds (figure 27). There is
nothing to suggest that the picture in TV is any different.
Figure 27 Number of NHS primary care Orthodontic patients resident in BGSW, by deprivation quartile, 2014/15
9.4 Variation in uptake of orthodontic treatment by gender
In the national Children’s Dental Health survey 2013, variation in uptake by gender
was evident. While the level of orthodontic need at 12 years old is the same
regardless of gender, more girls than boys had begun treatment by 15 years old
(figure 28).15
884
2,091
3,738
5,934
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
Q1 (25% Mostdeprived)
Q2 (25-50% Mostdeprived)
Q3 (50-75% Leastdeprived)
Q4 (25% Leastdeprived)
OFFICIAL
Final version 42
Figure 28 Variation in unmet need by gender in children in England, Wales and Northern Ireland Source: Children’s Dental Health Survey 2013
Gender of children Unmet need at 12 years old
Unmet need at 15 years old
Male 36% 21%
Female 36% 18%
These data are not available at a local level but it is reasonable to assume that a
similar pattern would be seen.
10 What orthodontic care is being provided in primary care?
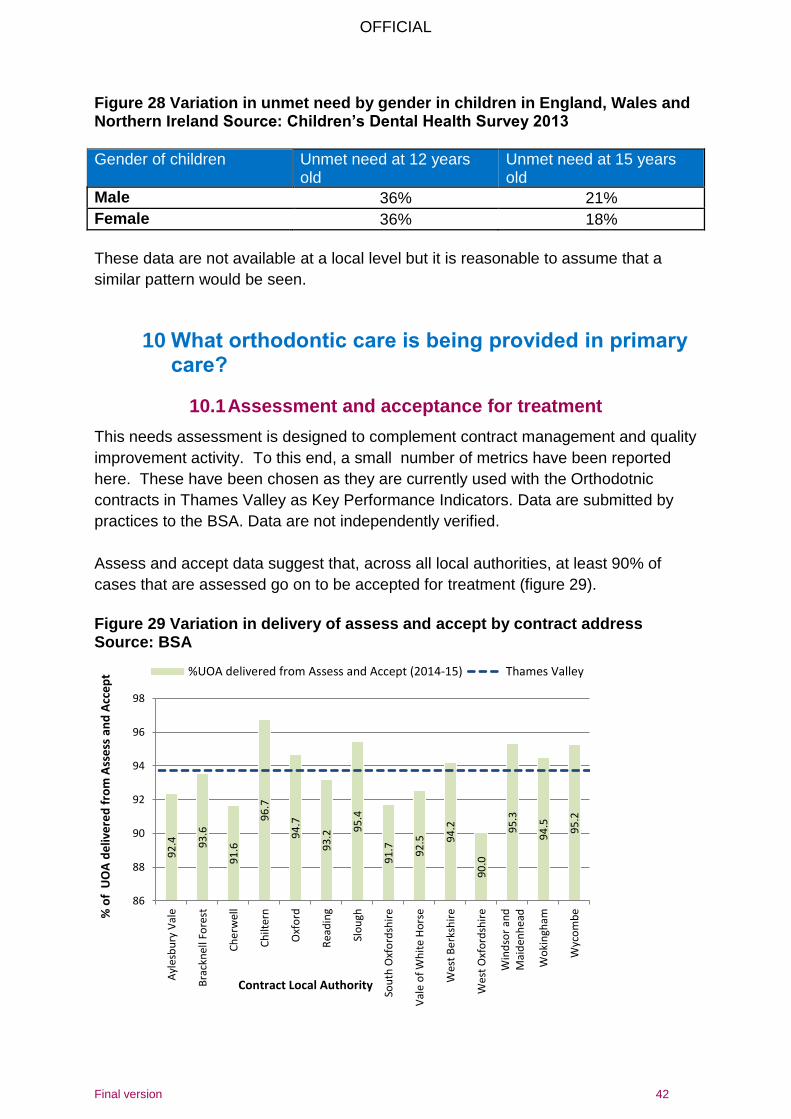
10.1 Assessment and acceptance for treatment
This needs assessment is designed to complement contract management and quality
improvement activity. To this end, a small number of metrics have been reported
here. These have been chosen as they are currently used with the Orthodotnic
contracts in Thames Valley as Key Performance Indicators. Data are submitted by
practices to the BSA. Data are not independently verified.
Assess and accept data suggest that, across all local authorities, at least 90% of
cases that are assessed go on to be accepted for treatment (figure 29).
Figure 29 Variation in delivery of assess and accept by contract address Source: BSA
92
.4
93
.6
91
.6
96
.7
94
.7
93
.2 95
.4
91
.7
92
.5
94
.2
90
.0
95
.3
94
.5
95
.2
86
88
90
92
94
96
98
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
e H
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
dM
aid
enh
ead
Wo
kin
gham
Wyc
om
be%
of
UO
A d
eliv
ere
d f
rom
Ass
ess
an
d A
cce
pt
Contract Local Authority
%UOA delivered from Assess and Accept (2014-15) Thames Valley
OFFICIAL
Final version 43
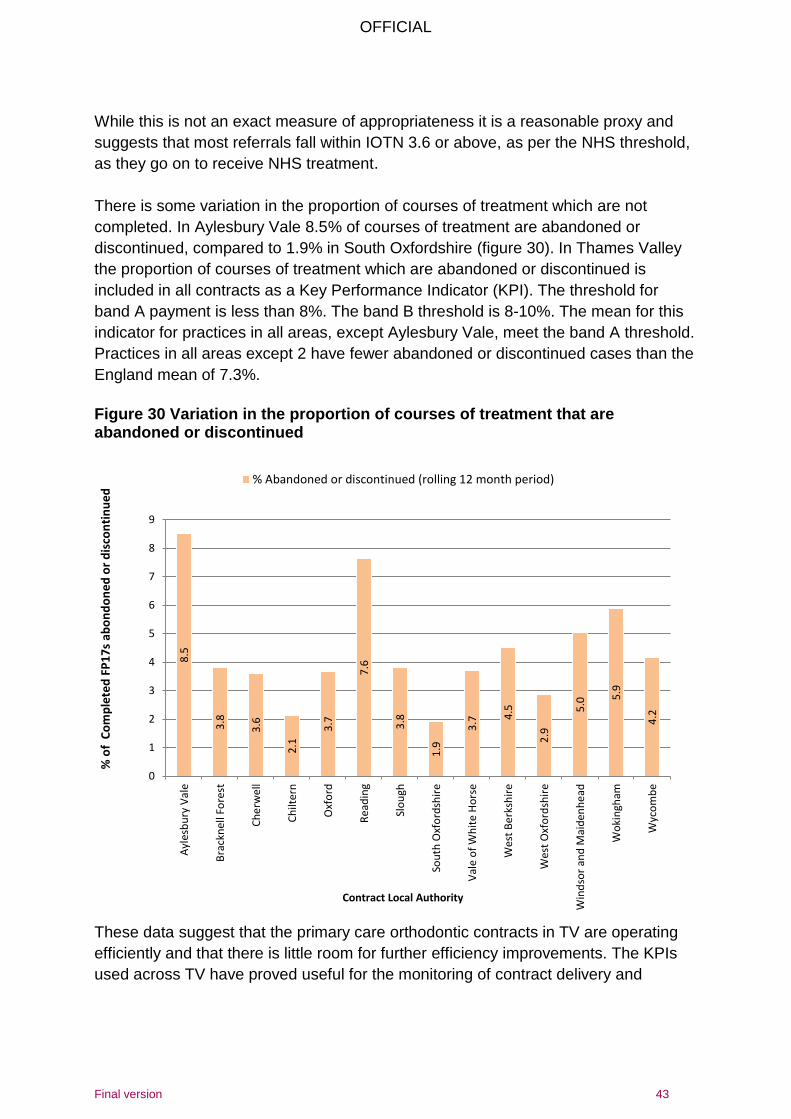
While this is not an exact measure of appropriateness it is a reasonable proxy and
suggests that most referrals fall within IOTN 3.6 or above, as per the NHS threshold,
as they go on to receive NHS treatment.
There is some variation in the proportion of courses of treatment which are not
completed. In Aylesbury Vale 8.5% of courses of treatment are abandoned or
discontinued, compared to 1.9% in South Oxfordshire (figure 30). In Thames Valley
the proportion of courses of treatment which are abandoned or discontinued is
included in all contracts as a Key Performance Indicator (KPI). The threshold for
band A payment is less than 8%. The band B threshold is 8-10%. The mean for this
indicator for practices in all areas, except Aylesbury Vale, meet the band A threshold.
Practices in all areas except 2 have fewer abandoned or discontinued cases than the
England mean of 7.3%.
Figure 30 Variation in the proportion of courses of treatment that are abandoned or discontinued
These data suggest that the primary care orthodontic contracts in TV are operating
efficiently and that there is little room for further efficiency improvements. The KPIs
used across TV have proved useful for the monitoring of contract delivery and
8.5
3.8
3.6
2.1
3.7
7.6
3.8
1.9
3.7
4.5
2.9
5.0
5.9
4.2
0
1
2
3
4
5
6
7
8
9
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
e H
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
d M
aid
enh
ead
Wo
kin
gham
Wyc
om
be
% o
f C
om
ple
ted
FP
17
s ab
on
do
ne
d o
r d
isco
nti
nu
ed
Contract Local Authority
% Abandoned or discontinued (rolling 12 month period)
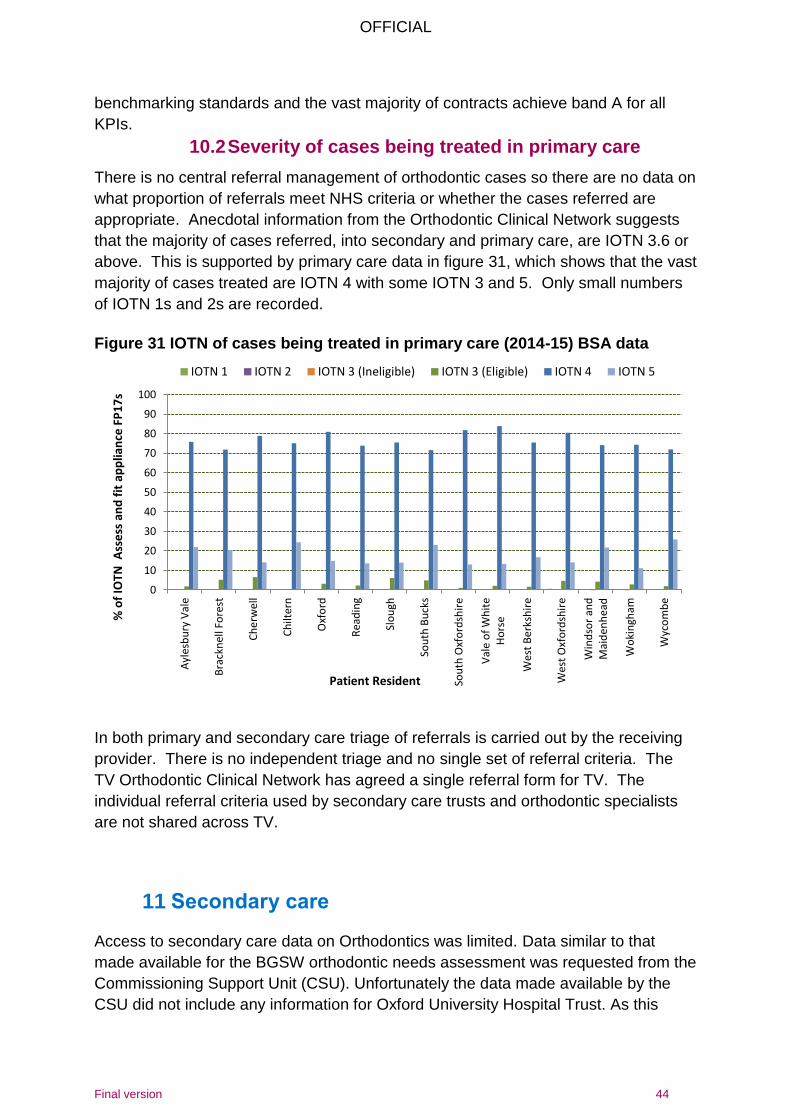
OFFICIAL
Final version 44
benchmarking standards and the vast majority of contracts achieve band A for all
KPIs.
10.2 Severity of cases being treated in primary care
There is no central referral management of orthodontic cases so there are no data on
what proportion of referrals meet NHS criteria or whether the cases referred are
appropriate. Anecdotal information from the Orthodontic Clinical Network suggests
that the majority of cases referred, into secondary and primary care, are IOTN 3.6 or
above. This is supported by primary care data in figure 31, which shows that the vast
majority of cases treated are IOTN 4 with some IOTN 3 and 5. Only small numbers
of IOTN 1s and 2s are recorded.
Figure 31 IOTN of cases being treated in primary care (2014-15) BSA data
In both primary and secondary care triage of referrals is carried out by the receiving
provider. There is no independent triage and no single set of referral criteria. The
TV Orthodontic Clinical Network has agreed a single referral form for TV. The
individual referral criteria used by secondary care trusts and orthodontic specialists
are not shared across TV.
11 Secondary care Access to secondary care data on Orthodontics was limited. Data similar to that
made available for the BGSW orthodontic needs assessment was requested from the
Commissioning Support Unit (CSU). Unfortunately the data made available by the
CSU did not include any information for Oxford University Hospital Trust. As this
0
10
20
30
40
50
60
70
80
90
100
Ayl
esb
ury
Val
e
Bra
ckn
ell F
ore
st
Ch
erw
ell
Ch
ilter
n
Oxf
ord
Rea
din
g
Slo
ugh
Sou
th B
uck
s
Sou
th O
xfo
rdsh
ire
Val
e o
f W
hit
eH
ors
e
Wes
t B
erk
shir
e
Wes
t O
xfo
rdsh
ire
Win
dso
r an
dM
aid
enh
ead
Wo
kin
gham
Wyc
om
be
% o
f IO
TN A
sse
ss a
nd
fit
ap
plia
nce
FP
17
s
Patient Resident
IOTN 1 IOTN 2 IOTN 3 (Ineligible) IOTN 3 (Eligible) IOTN 4 IOTN 5
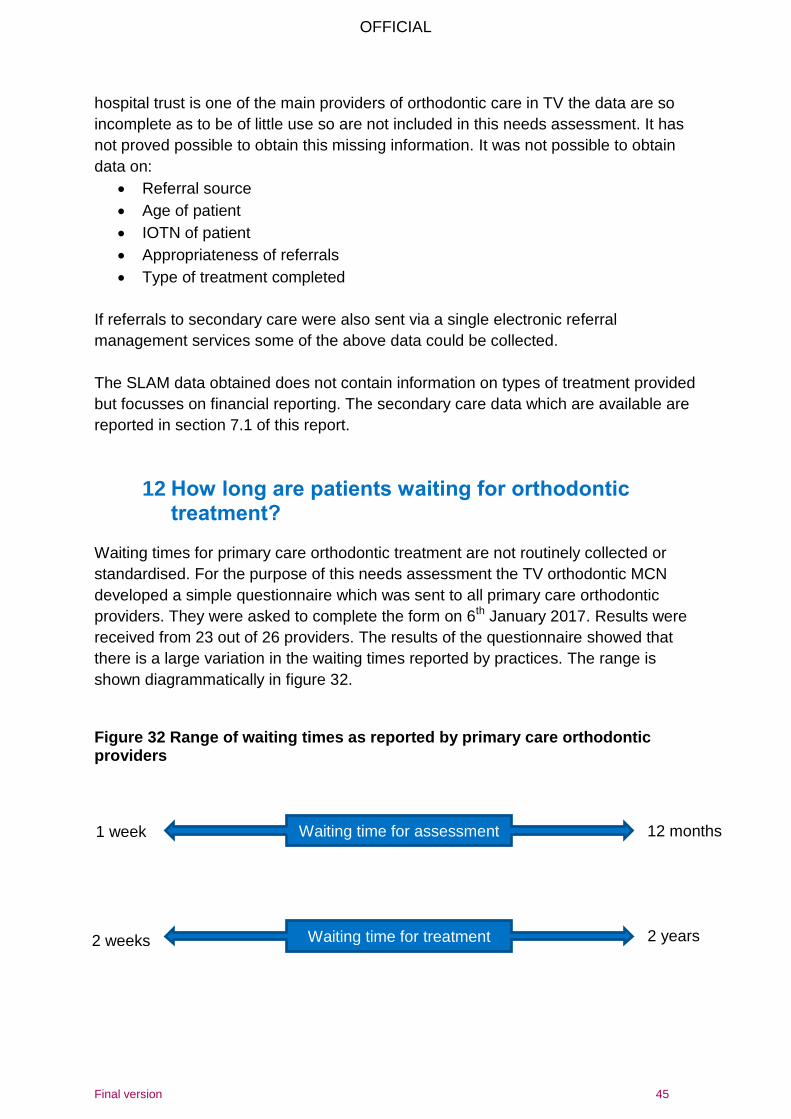
OFFICIAL
Final version 45
hospital trust is one of the main providers of orthodontic care in TV the data are so
incomplete as to be of little use so are not included in this needs assessment. It has
not proved possible to obtain this missing information. It was not possible to obtain
data on:
Referral source
Age of patient
IOTN of patient
Appropriateness of referrals
Type of treatment completed
If referrals to secondary care were also sent via a single electronic referral
management services some of the above data could be collected.
The SLAM data obtained does not contain information on types of treatment provided
but focusses on financial reporting. The secondary care data which are available are
reported in section 7.1 of this report.
12 How long are patients waiting for orthodontic treatment?
Waiting times for primary care orthodontic treatment are not routinely collected or
standardised. For the purpose of this needs assessment the TV orthodontic MCN
developed a simple questionnaire which was sent to all primary care orthodontic
providers. They were asked to complete the form on 6th January 2017. Results were
received from 23 out of 26 providers. The results of the questionnaire showed that
there is a large variation in the waiting times reported by practices. The range is
shown diagrammatically in figure 32.
Figure 32 Range of waiting times as reported by primary care orthodontic providers
Waiting time for assessment
Waiting time for treatment
1 week
2 weeks 2 years
12 months
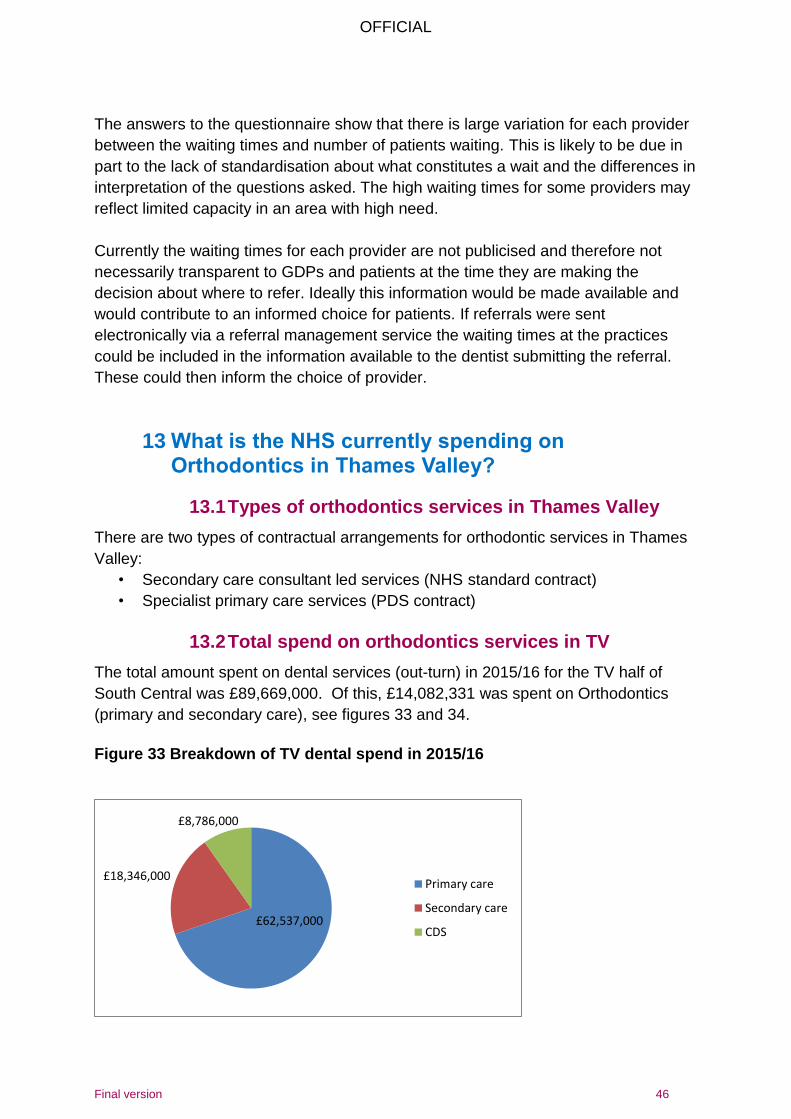
OFFICIAL
Final version 46
The answers to the questionnaire show that there is large variation for each provider
between the waiting times and number of patients waiting. This is likely to be due in
part to the lack of standardisation about what constitutes a wait and the differences in
interpretation of the questions asked. The high waiting times for some providers may
reflect limited capacity in an area with high need.
Currently the waiting times for each provider are not publicised and therefore not
necessarily transparent to GDPs and patients at the time they are making the
decision about where to refer. Ideally this information would be made available and
would contribute to an informed choice for patients. If referrals were sent
electronically via a referral management service the waiting times at the practices
could be included in the information available to the dentist submitting the referral.
These could then inform the choice of provider.
13 What is the NHS currently spending on Orthodontics in Thames Valley?
13.1 Types of orthodontics services in Thames Valley
There are two types of contractual arrangements for orthodontic services in Thames
Valley:
• Secondary care consultant led services (NHS standard contract)
• Specialist primary care services (PDS contract)
13.2 Total spend on orthodontics services in TV
The total amount spent on dental services (out-turn) in 2015/16 for the TV half of
South Central was £89,669,000. Of this, £14,082,331 was spent on Orthodontics
(primary and secondary care), see figures 33 and 34.
Figure 33 Breakdown of TV dental spend in 2015/16
£62,537,000
£18,346,000
£8,786,000
Primary care
Secondary care
CDS
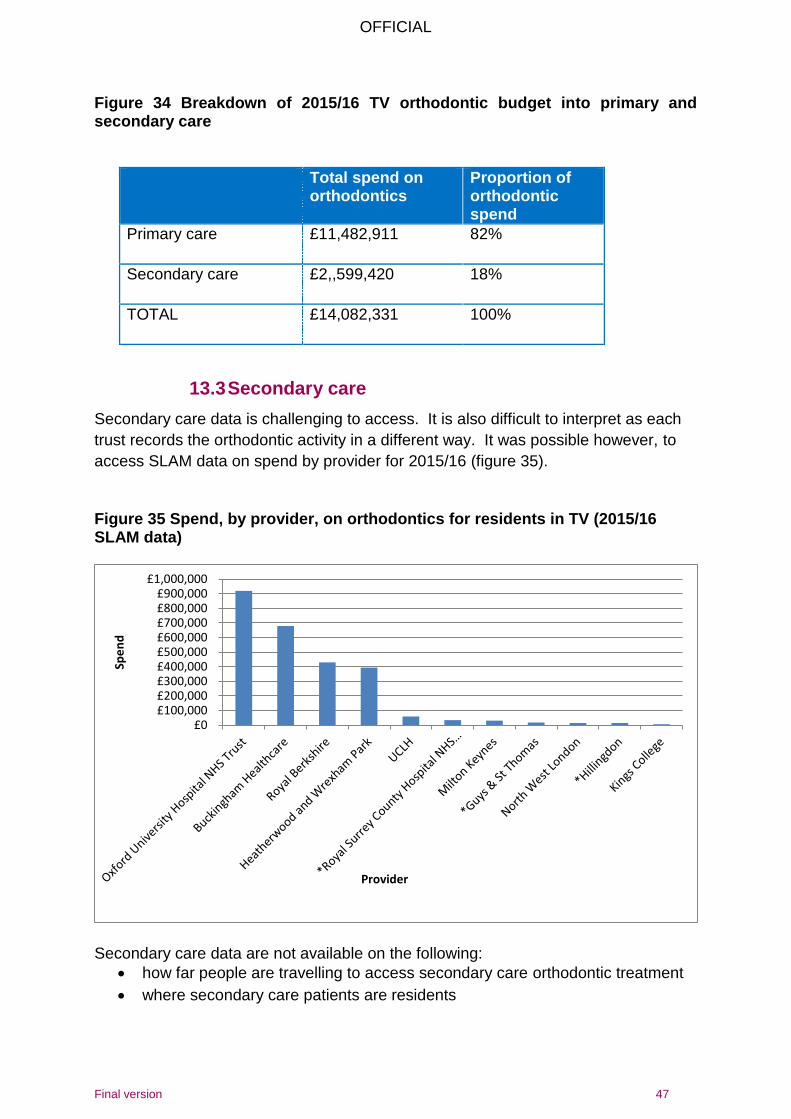
OFFICIAL
Final version 47
Figure 34 Breakdown of 2015/16 TV orthodontic budget into primary and secondary care
Total spend on orthodontics
Proportion of orthodontic spend
Primary care £11,482,911 82%
Secondary care £2,,599,420 18%
TOTAL £14,082,331 100%
13.3 Secondary care
Secondary care data is challenging to access. It is also difficult to interpret as each
trust records the orthodontic activity in a different way. It was possible however, to
access SLAM data on spend by provider for 2015/16 (figure 35).
Figure 35 Spend, by provider, on orthodontics for residents in TV (2015/16 SLAM data)
Secondary care data are not available on the following:
how far people are travelling to access secondary care orthodontic treatment
where secondary care patients are residents
£0£100,000£200,000£300,000£400,000£500,000£600,000£700,000£800,000£900,000
£1,000,000
Spe
nd
Provider
OFFICIAL
Final version 48
deprivation of patients being treated in secondary care
procedure level activity
waiting times
14 What are the workforce pressures on the Orthodontic system?
14.1 Orthodontic consultant numbers and consultant
training Recruitment of consultants is a challenge nationally and has been shown to be a
problem within NHS South Central, e.g. in Swindon and Cheltenham. This poses a
threat to sustainability of current hospital model if this trend continues.
The background to this is that trainees are reluctant to undergo consultant level
training due to the level of debt they emerge from specialist training with. They tend
now to prefer to stop specialist training after CCST (3 years training) when they can
join the specialist list. The additional two years post-CCST training to consultant
level is now less attractive than it was in the past.
14.2 Impact of skill mix
There are relatively high numbers of orthodontic therapists trained nationally. The
impact of this on future service delivery is unclear. Many practices are already using
skill mix as routine.
15 Orthodontic services in the community dental service?
15.1 Orthodontic support to the wider system
Limited orthodontic services are provided by the Community Dental services in
Oxfordshire and Berkshire. The services were asked to summarise their service for
this document. Their responses are given below.
Berkshire response:
Services provided o 0.2wte specialist orthodontist – also works at Guildford Hospital part-
time. o working at West Berkshire Community Hospital and Whitley Dental
Clinic, Reading o Only sees continuing care special care children o Variety of fixed and removable appliances
OFFICIAL
Final version 49
External advice source o Agreed guidance with Berkshire Orthodontic network on orthodontic
opinion prior to extraction of carious 6s o A patient referred by General Dental Practitioner for an orthodontic
opinion only is referred back with request for GDP to get ortho opinion from the orthodontist they would normally use
o Continuing care special care patient resident in the East of Berkshire are frequently referred to Wexham Park Hospital
Oxfordshire response:
Services provided o Full range of orthodontic treatment - simple removable appliances,
functional appliances and fixed appliances o opinions on the growing patient - carious/hypoplastic 6s o Access for complex patients i.e. emotional and physical special needs,
learning difficulties, Child and Adolescent Mental Health Services etc. o Clinic location: Banbury clinic N Oxon; JR (mid Oxon)
External advice source o Reciprocal support between CDS and Oxford University Hospital
Foundation Trust o Multidisciplinary Paediatric/ortho cases for trauma and Hypodontia /cleft o Network including audit and peer support/supervision and governance.
Attendance at Regional Ortho meetings and monthly JR Governance meetings
Buckinghamshire response
Services provided o There is no ortho provision in house. The pts are referred to either the
local hospitals or to a limited number of practices
The need for Orthodontic support to dental services that deliver extractions under
general anaesthetics is supported by the British society for Paediatric Dentistry
(BSPD) Guidelines For The Management Of Children Referred For Dental
Extractions Under General Anaesthesia, which state16
Dental assessment should ideally be performed by a specialist in paediatric dentistry or a dentist who can demonstrate the necessary competencies to carry out comprehensive treatment planning for children who require general anaesthesia. Where the assessing dentist is not a specialist, support from a specialist or consultant should be readily available, if required, through established clinical networks. Access to other specialties, such as orthodontics, oral surgery and maxillofacial surgery should also be available for all children.
OFFICIAL
Final version 50
Currently all the CDS in Thames Valley provide extractions under general anaesthetic. They all receive orthodontic support for this service but the way in which they receive it varies between the services. When the community dental services were asked for their views on current issues they responded with the following comments: Berkshire response:
o Much improved since guidance on 6s has reduced the need to refer for ortho opinion and saves months of waiting for patients before XGA
o No waiting list for orthodontics within CDS Oxfordshire response
o Timely access to opinions In house orthodontist can see patients within 6 to 8 weeks and urgent patients can be seen the week requested. Hospital opinions a few months but if urgent can call for advice to discuss case.
Buckinghamshire response
o The issues are related to the waiting times, however, both hospital and practices can be very accommodating and see patients quickly on request
o Sometimes the treatment plan provided by the orthodontic practice is very unrealistic and as such the clinicians seek further clarification and therefore there is further delay with patient’s treatment
“If the service were specifically dealing with patients within special care dentistry and Paediatric categories and the Consultant orthodontist at the hospital were happy to see them then I don’t think we would need an orthodontist in-house”
View expressed by a member of the CDS
“Ideally the CDS would have access to specialist orthodontist with skills in looking after patients with special needs including learning disabilities and autism as well as competent orthodontic skills.” “Clinics should be are easily accessible to these patients and familiar to them”
View expressed by a member of the CDS
OFFICIAL
Final version 51
15.2 Knowledge gaps
There are a number of areas where it has not been possible to obtain data or information to inform this needs assessment. These include:
Public/patient views (survey suspended)
Professional stakeholder views (LDC meeting plus clinical network meeting)
Opening times of practices
Uptake of NHS primary care by socio-economic status
Secondary care data Trends over time Detail on adults being treated Orthognathic data2 Waiting times Procedural data Patient characteristics, e.g. area of residence, deprivation quartile
16 Public views on orthodontics There are no local data on public views on orthodontics. A survey was prepared for this needs assessment but not used due to competing corporate priorities. The survey design is in appendix A. Whilst local public/patient views are not available other areas of England have carried out engagement events. An example of the results from such an event, carried out in Essex, can be found in appendix D.
2 Orthognathic data
An attempt was made to source data from orthognathic cases for this needs assessment however; it was not possible due to the complexities of how activity is recorded in these cases.
“The ideal would be to have the orthodontic service provided in house.”
View expressed by a member of the CDS
“We need to understand where is most convenient for patients to access care e.g. secondary schools, parent’s work”
View expressed by a member of the TV Orthodontic clinical network
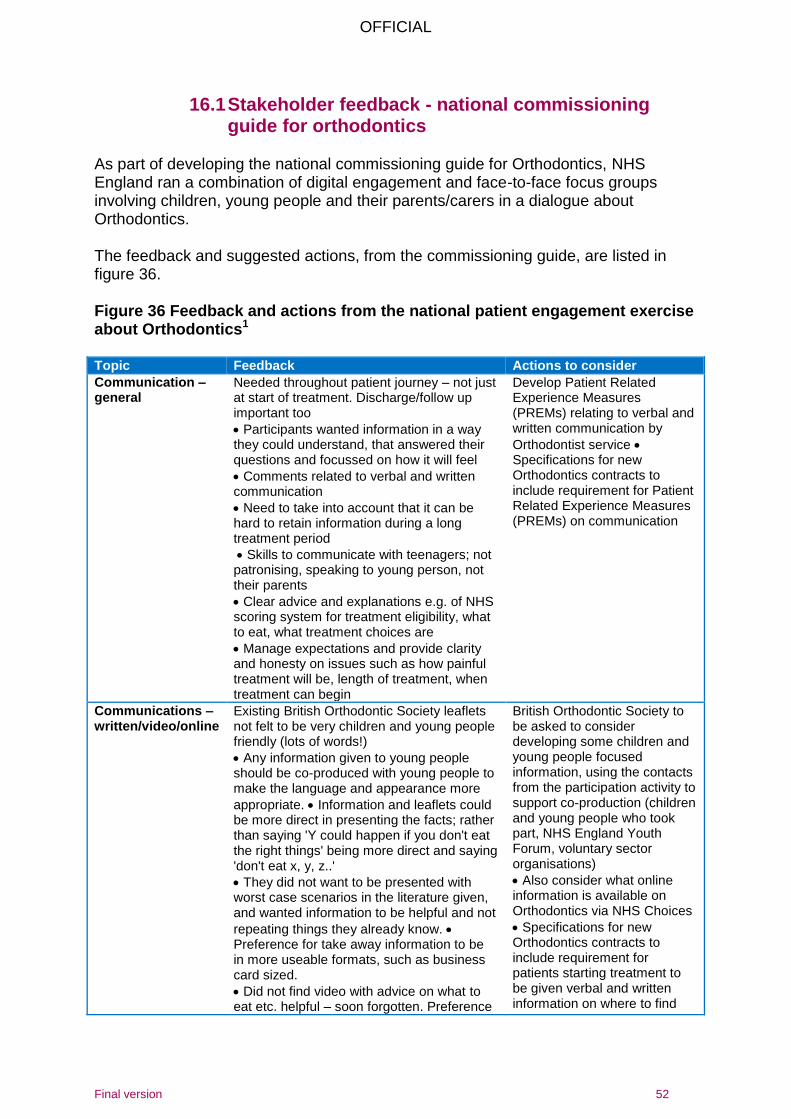
OFFICIAL
Final version 52
16.1 Stakeholder feedback - national commissioning guide for orthodontics
As part of developing the national commissioning guide for Orthodontics, NHS England ran a combination of digital engagement and face-to-face focus groups involving children, young people and their parents/carers in a dialogue about Orthodontics. The feedback and suggested actions, from the commissioning guide, are listed in figure 36. Figure 36 Feedback and actions from the national patient engagement exercise about Orthodontics1
Topic Feedback Actions to consider
Communication – general
Needed throughout patient journey – not just at start of treatment. Discharge/follow up important too
Participants wanted information in a way they could understand, that answered their questions and focussed on how it will feel
Comments related to verbal and written communication
Need to take into account that it can be hard to retain information during a long treatment period
Skills to communicate with teenagers; not patronising, speaking to young person, not their parents
Clear advice and explanations e.g. of NHS scoring system for treatment eligibility, what to eat, what treatment choices are
Manage expectations and provide clarity and honesty on issues such as how painful treatment will be, length of treatment, when treatment can begin
Develop Patient Related Experience Measures (PREMs) relating to verbal and written communication by
Orthodontist service Specifications for new Orthodontics contracts to include requirement for Patient Related Experience Measures (PREMs) on communication
Communications – written/video/online
Existing British Orthodontic Society leaflets not felt to be very children and young people friendly (lots of words!)
Any information given to young people should be co-produced with young people to make the language and appearance more
appropriate. Information and leaflets could be more direct in presenting the facts; rather than saying 'Y could happen if you don't eat the right things' being more direct and saying 'don't eat x, y, z..'
They did not want to be presented with worst case scenarios in the literature given, and wanted information to be helpful and not
repeating things they already know. Preference for take away information to be in more useable formats, such as business card sized.
Did not find video with advice on what to eat etc. helpful – soon forgotten. Preference
British Orthodontic Society to be asked to consider developing some children and young people focused information, using the contacts from the participation activity to support co-production (children and young people who took part, NHS England Youth Forum, voluntary sector organisations)
Also consider what online information is available on Orthodontics via NHS Choices
Specifications for new Orthodontics contracts to include requirement for patients starting treatment to be given verbal and written information on where to find
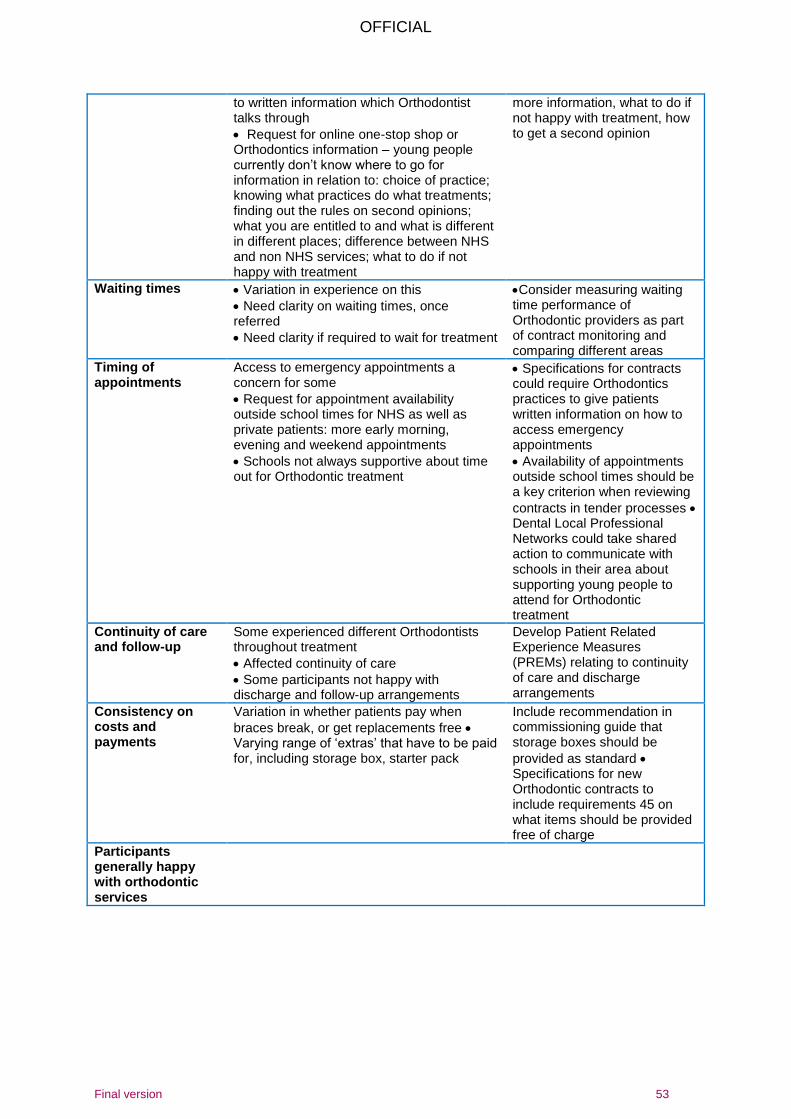
OFFICIAL
Final version 53
to written information which Orthodontist talks through
Request for online one-stop shop or Orthodontics information – young people currently don’t know where to go for information in relation to: choice of practice; knowing what practices do what treatments; finding out the rules on second opinions; what you are entitled to and what is different in different places; difference between NHS and non NHS services; what to do if not happy with treatment
more information, what to do if not happy with treatment, how to get a second opinion
Waiting times Variation in experience on this
Need clarity on waiting times, once referred
Need clarity if required to wait for treatment
Consider measuring waiting time performance of Orthodontic providers as part of contract monitoring and comparing different areas
Timing of appointments
Access to emergency appointments a concern for some
Request for appointment availability outside school times for NHS as well as private patients: more early morning, evening and weekend appointments
Schools not always supportive about time out for Orthodontic treatment
Specifications for contracts could require Orthodontics practices to give patients written information on how to access emergency appointments
Availability of appointments outside school times should be a key criterion when reviewing
contracts in tender processes Dental Local Professional Networks could take shared action to communicate with schools in their area about supporting young people to attend for Orthodontic treatment
Continuity of care and follow-up
Some experienced different Orthodontists throughout treatment
Affected continuity of care
Some participants not happy with discharge and follow-up arrangements
Develop Patient Related Experience Measures (PREMs) relating to continuity of care and discharge arrangements
Consistency on costs and payments
Variation in whether patients pay when
braces break, or get replacements free Varying range of ‘extras’ that have to be paid for, including storage box, starter pack
Include recommendation in commissioning guide that storage boxes should be
provided as standard Specifications for new Orthodontic contracts to include requirements 45 on what items should be provided free of charge
Participants generally happy with orthodontic services
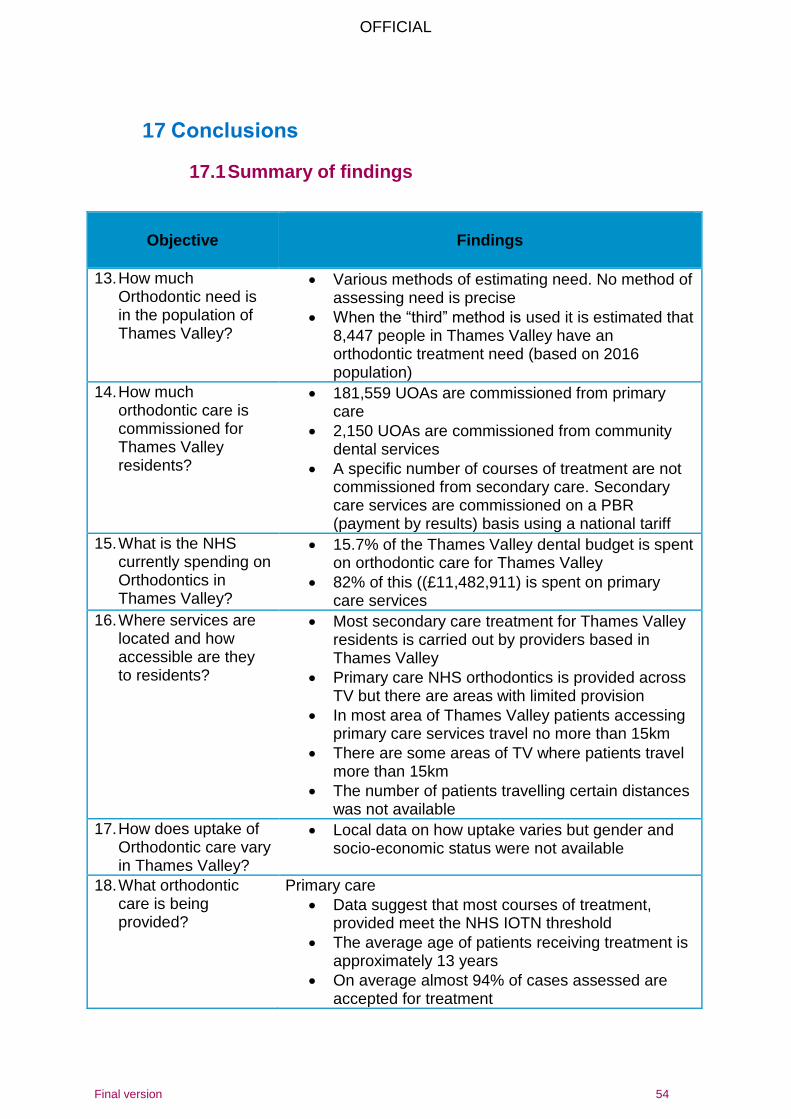
OFFICIAL
Final version 54
17 Conclusions
17.1 Summary of findings
Objective
Findings
13. How much Orthodontic need is in the population of Thames Valley?
Various methods of estimating need. No method of assessing need is precise
When the “third” method is used it is estimated that 8,447 people in Thames Valley have an orthodontic treatment need (based on 2016 population)
14. How much orthodontic care is commissioned for Thames Valley residents?
181,559 UOAs are commissioned from primary care
2,150 UOAs are commissioned from community dental services
A specific number of courses of treatment are not commissioned from secondary care. Secondary care services are commissioned on a PBR (payment by results) basis using a national tariff
15. What is the NHS currently spending on Orthodontics in Thames Valley?
15.7% of the Thames Valley dental budget is spent on orthodontic care for Thames Valley
82% of this ((£11,482,911) is spent on primary care services
16. Where services are located and how accessible are they to residents?
Most secondary care treatment for Thames Valley residents is carried out by providers based in Thames Valley
Primary care NHS orthodontics is provided across TV but there are areas with limited provision
In most area of Thames Valley patients accessing primary care services travel no more than 15km
There are some areas of TV where patients travel more than 15km
The number of patients travelling certain distances was not available
17. How does uptake of Orthodontic care vary in Thames Valley?
Local data on how uptake varies but gender and socio-economic status were not available
18. What orthodontic care is being provided?
Primary care
Data suggest that most courses of treatment, provided meet the NHS IOTN threshold
The average age of patients receiving treatment is approximately 13 years
On average almost 94% of cases assessed are accepted for treatment
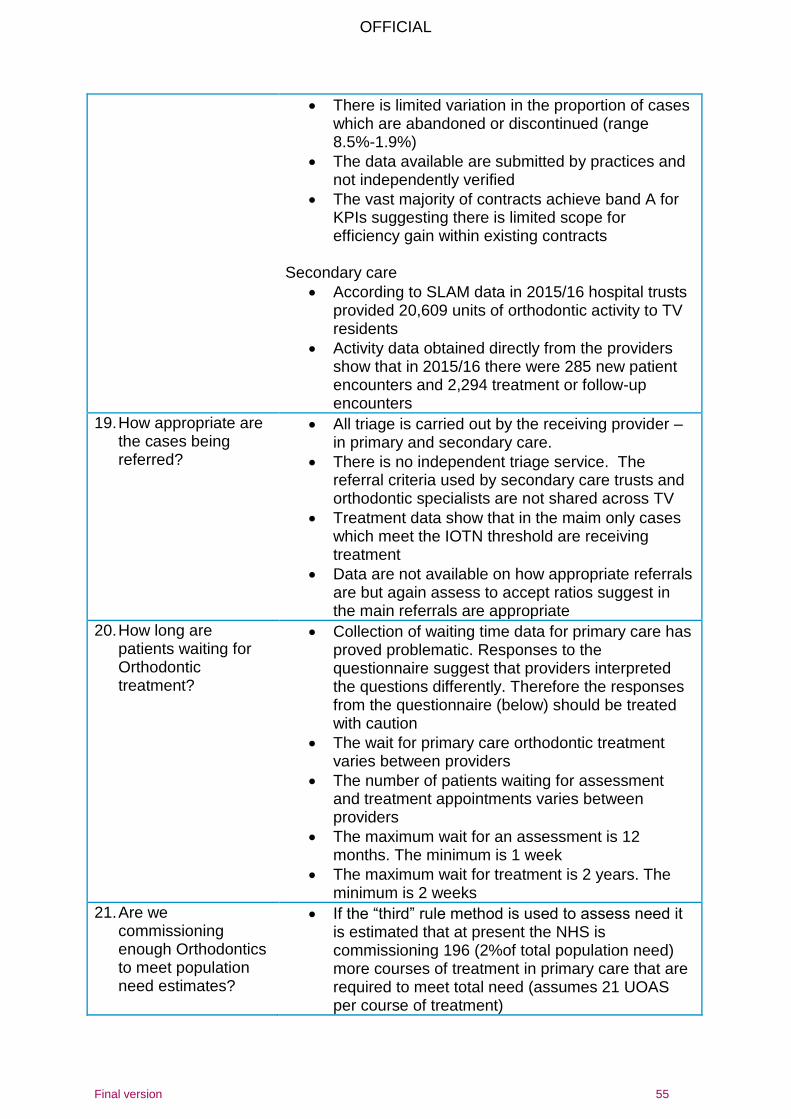
OFFICIAL
Final version 55
There is limited variation in the proportion of cases which are abandoned or discontinued (range 8.5%-1.9%)
The data available are submitted by practices and not independently verified
The vast majority of contracts achieve band A for KPIs suggesting there is limited scope for efficiency gain within existing contracts
Secondary care
According to SLAM data in 2015/16 hospital trusts provided 20,609 units of orthodontic activity to TV residents
Activity data obtained directly from the providers show that in 2015/16 there were 285 new patient encounters and 2,294 treatment or follow-up encounters
19. How appropriate are the cases being referred?
All triage is carried out by the receiving provider – in primary and secondary care.
There is no independent triage service. The referral criteria used by secondary care trusts and orthodontic specialists are not shared across TV
Treatment data show that in the maim only cases which meet the IOTN threshold are receiving treatment
Data are not available on how appropriate referrals are but again assess to accept ratios suggest in the main referrals are appropriate
20. How long are patients waiting for Orthodontic treatment?
Collection of waiting time data for primary care has proved problematic. Responses to the questionnaire suggest that providers interpreted the questions differently. Therefore the responses from the questionnaire (below) should be treated with caution
The wait for primary care orthodontic treatment varies between providers
The number of patients waiting for assessment and treatment appointments varies between providers
The maximum wait for an assessment is 12 months. The minimum is 1 week
The maximum wait for treatment is 2 years. The minimum is 2 weeks
21. Are we commissioning enough Orthodontics to meet population need estimates?
If the “third” rule method is used to assess need it is estimated that at present the NHS is commissioning 196 (2%of total population need) more courses of treatment in primary care that are required to meet total need (assumes 21 UOAS per course of treatment)
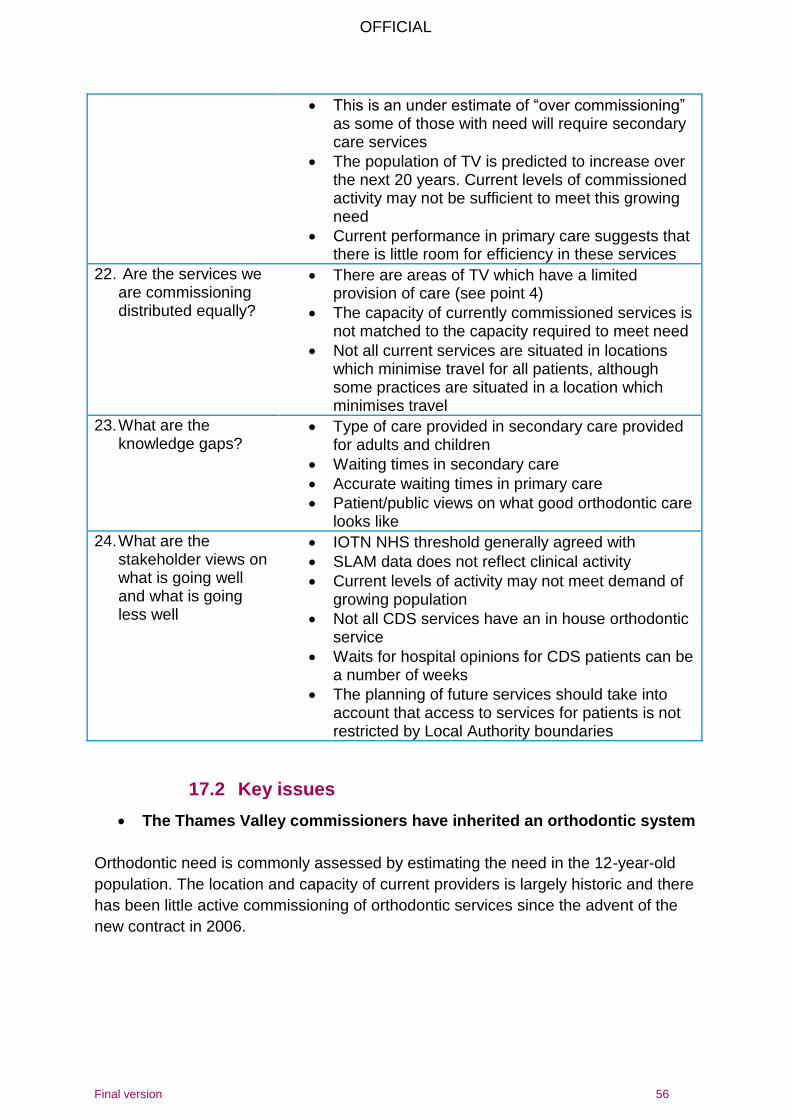
OFFICIAL
Final version 56
This is an under estimate of “over commissioning” as some of those with need will require secondary care services
The population of TV is predicted to increase over the next 20 years. Current levels of commissioned activity may not be sufficient to meet this growing need
Current performance in primary care suggests that there is little room for efficiency in these services
22. Are the services we are commissioning distributed equally?
There are areas of TV which have a limited provision of care (see point 4)
The capacity of currently commissioned services is not matched to the capacity required to meet need
Not all current services are situated in locations which minimise travel for all patients, although some practices are situated in a location which minimises travel
23. What are the knowledge gaps?
Type of care provided in secondary care provided for adults and children
Waiting times in secondary care
Accurate waiting times in primary care
Patient/public views on what good orthodontic care looks like
24. What are the stakeholder views on what is going well and what is going less well
IOTN NHS threshold generally agreed with
SLAM data does not reflect clinical activity
Current levels of activity may not meet demand of growing population
Not all CDS services have an in house orthodontic service
Waits for hospital opinions for CDS patients can be a number of weeks
The planning of future services should take into account that access to services for patients is not restricted by Local Authority boundaries
17.2 Key issues
The Thames Valley commissioners have inherited an orthodontic system
Orthodontic need is commonly assessed by estimating the need in the 12-year-old
population. The location and capacity of current providers is largely historic and there
has been little active commissioning of orthodontic services since the advent of the
new contract in 2006.
OFFICIAL
Final version 57
Location and capacity of services are not matched to need in all areas
This is the first time there has been a formal assessment of whether the capacity and
location of service meet need. The data show that there are some areas where
services are limited and some areas where capacity is greater than need.
Inequalities in access to orthodontic services
Whilst most patients are able to access primary care orthodontic services within15km
of their home some have to travel further than this. Travelling large distances may be
particularly difficult for more deprived families and so will increase inequalities in
access.
Waiting times in primary care of variable. Lack of waiting time information, available
to GDPs and patients, means that they may not be able to make choices which take
into account waiting times.
Lack of detailed data
The secondary care data available to support this needs assessment was limited. It
was not possible to obtain information on the ages of patients treated or the
treatment provided.
In primary care there is a lack of accurate information on referral sources, waiting
times and numbers of patients waiting for treatment.
Triage
Triage is carried out by providers on the referrals they receive. There are no agreed
referral criteria, referral forms or independent assessment of referrals. There is also
no routine collection of referral data e.g. referral source. Referrals are not submitted
electronically, as recommended in national guidance.
Pathway
There is no agreed orthodontic pathway, with a single entry point, in TV, as per
national guidance.
OFFICIAL
Final version 58
17.3 Recommendations
Match capacity to need
Ensure capacity meets future population growth
Work in partnership with orthodontic clinical network to:
o Identify a reasonable waiting time standard across TV
o Validate waiting list information
Ensure the location and capacity of service commissioned meets the local
need and takes into account natural patient flows
It is important to note that the number of UOAs needed is used as a proxy for
need across the system. UOAs are not the currency used in secondary care
and this must be taken into account when planning services otherwise there is
a risk that the budget is spent on primary care UOAs only and orthodontic
services may be over-commissioned.
Improve monitoring and data collection across the system
Agree definitions of waits for assessment and waits for treatment so that
commissioners can compare waits between practices
Routinely collect waiting time data from primary care providers
Routinely collect waiting time data form secondary care providers
Consider commissioning an electronic referral management service for
orthodontic referrals. This will enable collection of data on source of referrals,
appropriateness and outcome of referrals and the proportion of referrals meet
NHS criteria.
Contract management and improving quality
Quality based KPIs should continue and be improved
Aim to align KPIs and targets across South Central over medium term
Work with the clinical network to agree how to support orthodontists struggling
to meet DAF standards and how to share best practise
Agree, with the clinical network, appropriate and meaningful PROMs and
PREMs for monitoring quality
Link all Orthodontic providers to clinical network which can lead and support
them to improve quality, such as through peer review and audit
Consider implementing PREMS that look at communication with young people
in a caring, respectful and comprehensible way, including providing
explanations throughout the course of treatment and answering questions.
OFFICIAL
Final version 59
Pathway redesign
Work with clinical network to agree referral criteria and referral form to ensure
consistent processes, and good quality referrals, across TV
Implement an electronic referral service to give single entry point to the
pathway and provide the following benefits: avoidance of duplicate referrals,
ongoing measurement of uptake of services, routine data collection, e.g. on
source of referral, numbers waiting, waiting times, required level of provider.
Work with HEE and the clinical network to support dentists to routinely include
the IOTN score when referring patients for orthodontic treatment.
Implement consistent referral management for secondary and primary care
according to national commissioning guidance, ideally with electronic RMS so
that data can be gathered and monitored.
Work towards agreeing service specifications for secondary care services
including minimum data set
Reach consistent agreement on under what circumstances over 18s receive
orthodontic treatment in secondary care
Involve patients and public in the Orthodontic commissioning cycle, such as
pathway redesign and evaluation
Tackling inequalities
Make use of opportunities in the future to distribute resources/capacity more
according to need/population density. Prioritise areas where high numbers of
patients are travelling long distances, particularly where patients are from lower
deprivation quartile.
Prioritise delivery of prevention activities in GDS contracts, e.g. application of
fluoride varnish. This will help to improve oral health and therefore enable more
people to be suitable for orthodontic care
Involve patients and public in the commissioning cycle, such as pathway
redesign and evaluation and in work regarding addressing inequalities in
access to dental services.
Actively monitor access to GDS
Work with the LPN to explore how to encourage referral of more deprived
patients
Gather information on the local public view on Orthodontic services and apply
findings to action plan.
Review opening hours across the Orthodontic system and expand beyond
school hours where necessary.

OFFICIAL
Final version 60
Orthodontic support to the wider system
Ensure commissioning of orthodontic treatment planning support to services treating:
special care patients
extractions under GA
OFFICIAL
Final version 61
18 Appendices
A. Postponed public engagement survey on Orthodontics in South Central (BGSW and Thames Valley)
NHS England, South Central – Orthodontic Services review project We would like to ask for your views on orthodontic services to help us develop them for the future. Orthodontic treatment is used to improve the appearance, position and how crooked or abnormally positioned teeth work. Orthodontic treatment can straighten teeth and move them into a better position. Devices such as braces are used to help move teeth although your exact treatment will depend on the problems you have. Orthodontic services in Bath, Gloucestershire, Swindon, Wiltshire and the Thames Valley areas are planned and bought by NHS England, South Central. We need to look at those who are using the service locally to make sure services meet the needs of patients, provide a quality service and identify opportunities to develop these services in the future. We want to hear from those who have used these services in the past two years or may need to use them in future. Confidentiality
Responses from individuals will be made available to the NHS organisations involved in this engagement exercise, to enable them to consider respondents’ views fully, but will otherwise be kept confidential. Your name will be kept confidential and will not be disclosed, except as may be required by law. You don’t have to give your name if you don’t want to, we will still take your views. About you For each question below, please put a in the box/boxes or provide the information required.
1. I am providing a response on behalf of: (please tick one box only)
Myself
My child
My organisation o Please note that responses on behalf of organisations may be made
available for the public to look at
Other (please state)
OFFICIAL
Final version 62
2. Have you or your child been seen by an orthodontist in the past two years? Yes No
3. If you think that you or your child needed braces, what would you do? a. Talk it over with your usual family dentist b. Go directly to an orthodontic specialist c. Ask your Dr to refer you to hospital d. I wouldn’t know what to do e. Other
4. If you felt you or your child needed braces, which of the following would put
you off seeking treatment a. Probably too expensive b. Not aware if available on the NHS c. Appointments only available 9am-5pm Monday to Friday d. Don’t want to wear braces e. I wouldn’t know what to do f. I would wait for the dentist to tell me whether I/my child needed them or
not g. Nothing would stop me h. Fear of the dentist/orthodontist i. Other
5. Thinking about NHS braces (orthodontic treatment) please tick true or false for
each of the points below a. NHS braces are free for all children b. NHS braces are free for all adults c. NHS braces are only free for children with the most crooked teeth d. NHS braces are only free for adults with the most crooked teeth e. You can’t get braces for children on the NHS f. You can’t get braces for adults on the NHS
6. If you or your child is having treatment for crooked teeth (braces) it will
normally involve 18 months to 2 years of monthly appointments. What days and times would suit you best for your appointments
a. Monday to Friday 9am-5pm b. Monday to Friday evenings c. Saturday and Sunday 9am-5pm
7. Please indicate how far you would be prepared to travel for an orthodontic
appointment (for braces) a. 0-5miles b. 6-10miles c. 11-20 miles d. More than 20 miles
8. Do you have any other comments on orthodontic treatment? If so, please
write them in the box below. Please complete the monitoring questions that follow. Thank you for your time.
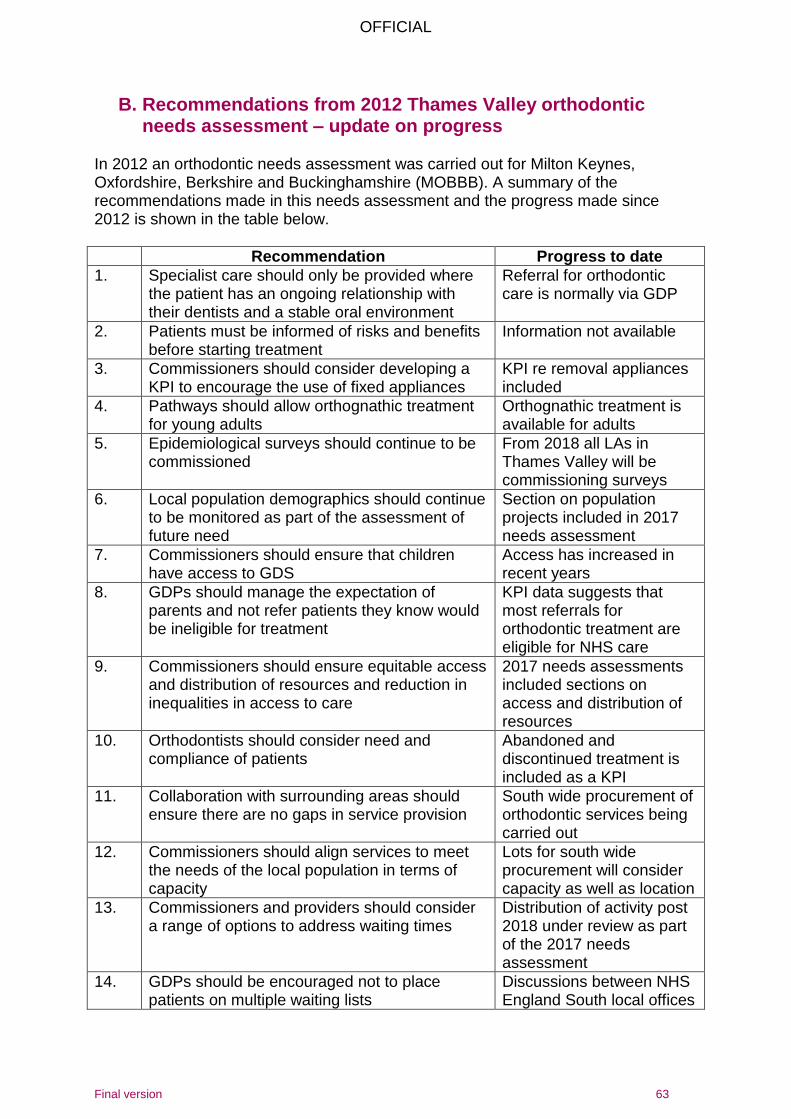
OFFICIAL
Final version 63
B. Recommendations from 2012 Thames Valley orthodontic needs assessment – update on progress
In 2012 an orthodontic needs assessment was carried out for Milton Keynes, Oxfordshire, Berkshire and Buckinghamshire (MOBBB). A summary of the recommendations made in this needs assessment and the progress made since 2012 is shown in the table below.
Recommendation Progress to date
1. Specialist care should only be provided where the patient has an ongoing relationship with their dentists and a stable oral environment
Referral for orthodontic care is normally via GDP
2. Patients must be informed of risks and benefits before starting treatment
Information not available
3. Commissioners should consider developing a KPI to encourage the use of fixed appliances
KPI re removal appliances included
4. Pathways should allow orthognathic treatment for young adults
Orthognathic treatment is available for adults
5. Epidemiological surveys should continue to be commissioned
From 2018 all LAs in Thames Valley will be commissioning surveys
6. Local population demographics should continue to be monitored as part of the assessment of future need
Section on population projects included in 2017 needs assessment
7. Commissioners should ensure that children have access to GDS
Access has increased in recent years
8. GDPs should manage the expectation of parents and not refer patients they know would be ineligible for treatment
KPI data suggests that most referrals for orthodontic treatment are eligible for NHS care
9. Commissioners should ensure equitable access and distribution of resources and reduction in inequalities in access to care
2017 needs assessments included sections on access and distribution of resources
10. Orthodontists should consider need and compliance of patients
Abandoned and discontinued treatment is included as a KPI
11. Collaboration with surrounding areas should ensure there are no gaps in service provision
South wide procurement of orthodontic services being carried out
12. Commissioners should align services to meet the needs of the local population in terms of capacity
Lots for south wide procurement will consider capacity as well as location
13. Commissioners and providers should consider a range of options to address waiting times
Distribution of activity post 2018 under review as part of the 2017 needs assessment
14. GDPs should be encouraged not to place patients on multiple waiting lists
Discussions between NHS England South local offices

OFFICIAL
Final version 64
regarding establishment of Electronic Referral System to capture and track referrals
15. Orthodontic practices should be restricted to treatment children under the age of 18 years
Very few adults are treated in primary care
16. There should be consideration of a referral proforma across the whole of MOBBB
Proforma developed by MCN
17. New performers should be made aware of referral pathways and systems
Information not available
18. Commissioners should consider KPIs which ensure compliance with FP17 data entry
KPI relating to Discontinued and Abandoned treatment introduced in 2013. Incentivises providers to record completion of treatments.
19. Investigation at a practice level of IOTN at start of treatment
IOTN data available via BSA
20. A KPI to measure the ratio of reviews to treatment should be considered
Included as KPI
21. A KPI about discontinued and abandoned courses of treatment should be considered
Included as KPI
22. Further work is needed to assess the role of a service to treat difficult patients and provide a safety net function
Information not available
23. Salaried orthodontists should ensure completion of FP17s
CDS complete FP17s
24. Private orthodontists should consider sharing information about private treatment provided
Information not available
25. Commissioners should include private orthodontists in communications
Information not available
26. A service specification for secondary care should be developed
No progress
27. Activity data for primary and secondary care should be consistent
No progress
28. Performance monitoring of secondary care should be as robust as primary care
Data challenges with secondary care remain
29. There should be agreement about the number of cases commissioned from secondary care for training purposes
Information not available
30. Commissioners should consider the patient pathway in terms of location of provider
Under review as part of the needs assessment for the service post 2018
31. Re-negotiation of UOA values should be considered to reach an average value
UOA values were re-based in 2013 with all providers in the Thames Valley paid at the same UOA rate
32. Commissioners should confirm best value by ensuring patients are treated in the most
Information not available
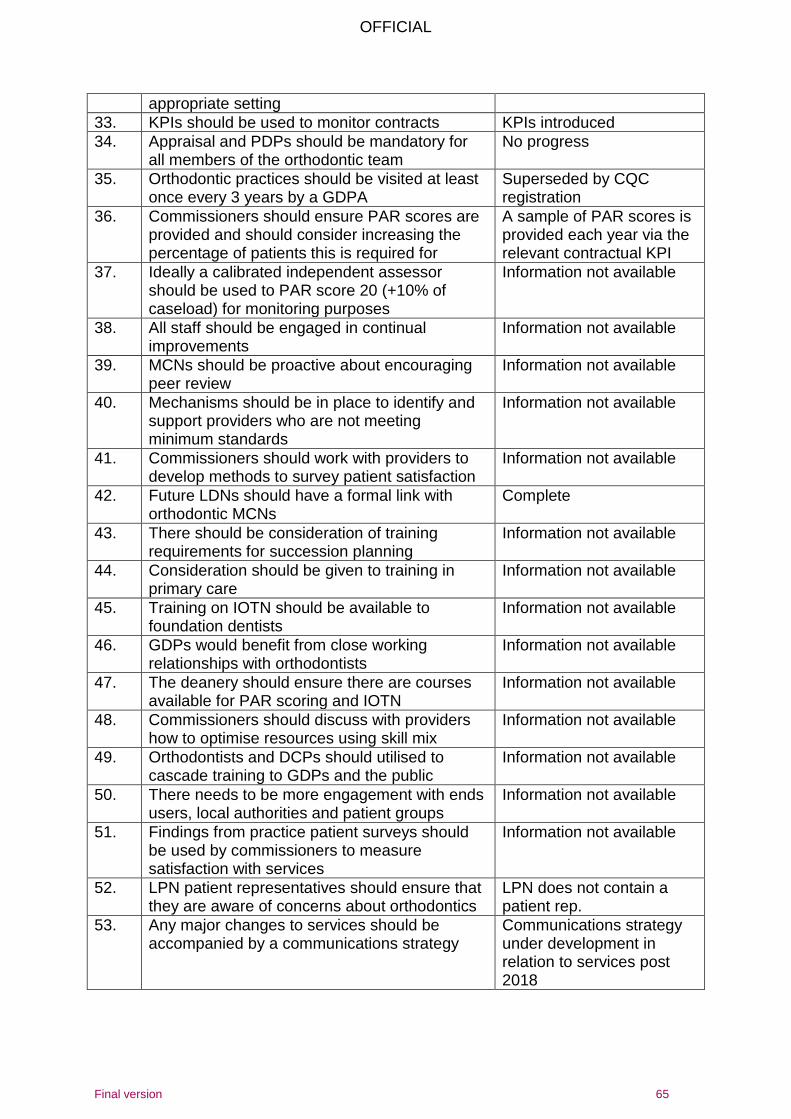
OFFICIAL
Final version 65
appropriate setting
33. KPIs should be used to monitor contracts KPIs introduced
34. Appraisal and PDPs should be mandatory for all members of the orthodontic team
No progress
35. Orthodontic practices should be visited at least once every 3 years by a GDPA
Superseded by CQC registration
36. Commissioners should ensure PAR scores are provided and should consider increasing the percentage of patients this is required for
A sample of PAR scores is provided each year via the relevant contractual KPI
37. Ideally a calibrated independent assessor should be used to PAR score 20 (+10% of caseload) for monitoring purposes
Information not available
38. All staff should be engaged in continual improvements
Information not available
39. MCNs should be proactive about encouraging peer review
Information not available
40. Mechanisms should be in place to identify and support providers who are not meeting minimum standards
Information not available
41. Commissioners should work with providers to develop methods to survey patient satisfaction
Information not available
42. Future LDNs should have a formal link with orthodontic MCNs
Complete
43. There should be consideration of training requirements for succession planning
Information not available
44. Consideration should be given to training in primary care
Information not available
45. Training on IOTN should be available to foundation dentists
Information not available
46. GDPs would benefit from close working relationships with orthodontists
Information not available
47. The deanery should ensure there are courses available for PAR scoring and IOTN
Information not available
48. Commissioners should discuss with providers how to optimise resources using skill mix
Information not available
49. Orthodontists and DCPs should utilised to cascade training to GDPs and the public
Information not available
50. There needs to be more engagement with ends users, local authorities and patient groups
Information not available
51. Findings from practice patient surveys should be used by commissioners to measure satisfaction with services
Information not available
52. LPN patient representatives should ensure that they are aware of concerns about orthodontics
LPN does not contain a patient rep.
53. Any major changes to services should be accompanied by a communications strategy
Communications strategy under development in relation to services post 2018
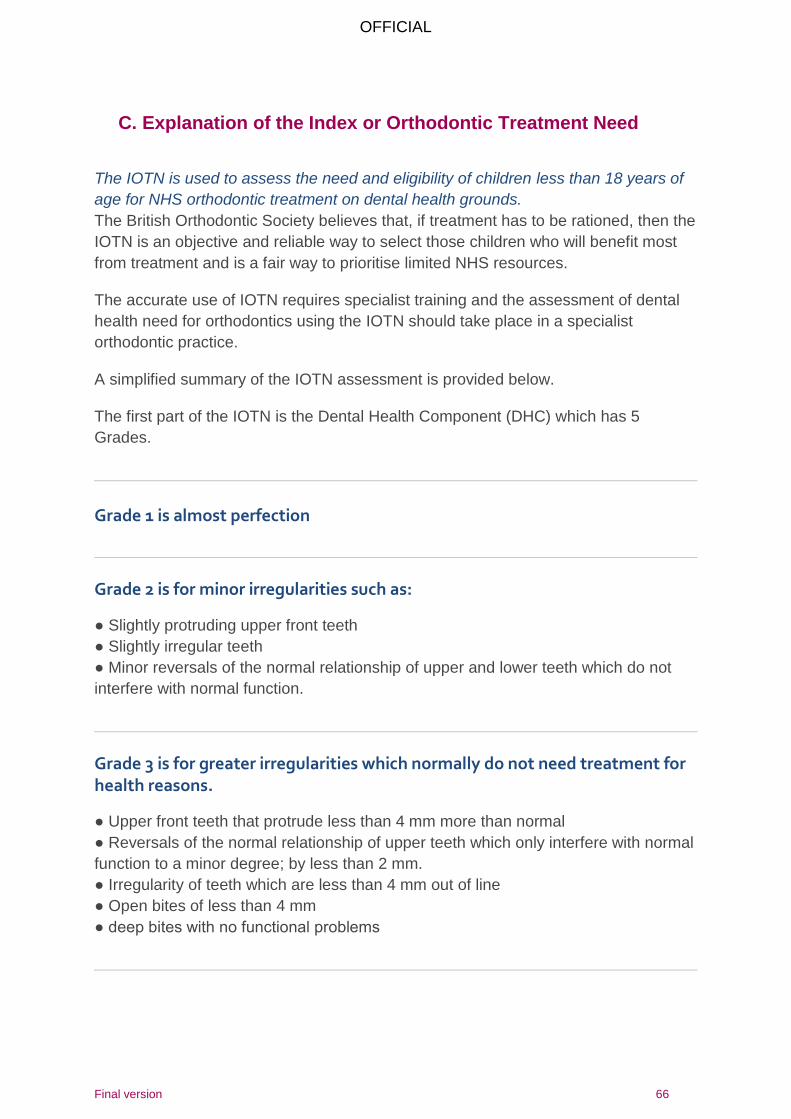
OFFICIAL
Final version 66
C. Explanation of the Index or Orthodontic Treatment Need
The IOTN is used to assess the need and eligibility of children less than 18 years of
age for NHS orthodontic treatment on dental health grounds.
The British Orthodontic Society believes that, if treatment has to be rationed, then the
IOTN is an objective and reliable way to select those children who will benefit most
from treatment and is a fair way to prioritise limited NHS resources.
The accurate use of IOTN requires specialist training and the assessment of dental
health need for orthodontics using the IOTN should take place in a specialist
orthodontic practice.
A simplified summary of the IOTN assessment is provided below.
The first part of the IOTN is the Dental Health Component (DHC) which has 5
Grades.
Grade 1 is almost perfection
Grade 2 is for minor irregularities such as:
● Slightly protruding upper front teeth
● Slightly irregular teeth
● Minor reversals of the normal relationship of upper and lower teeth which do not
interfere with normal function.
Grade 3 is for greater irregularities which normally do not need treatment for health reasons.
● Upper front teeth that protrude less than 4 mm more than normal
● Reversals of the normal relationship of upper teeth which only interfere with normal
function to a minor degree; by less than 2 mm.
● Irregularity of teeth which are less than 4 mm out of line
● Open bites of less than 4 mm
● deep bites with no functional problems
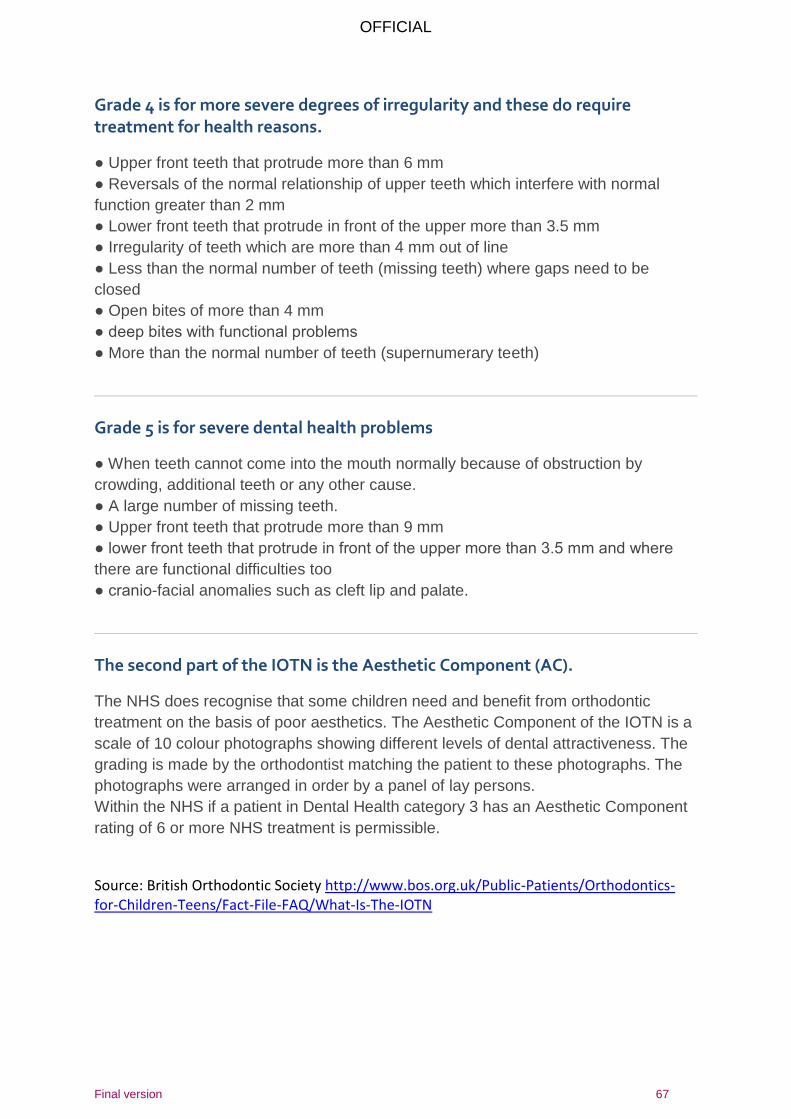
OFFICIAL
Final version 67
Grade 4 is for more severe degrees of irregularity and these do require treatment for health reasons.
● Upper front teeth that protrude more than 6 mm
● Reversals of the normal relationship of upper teeth which interfere with normal
function greater than 2 mm
● Lower front teeth that protrude in front of the upper more than 3.5 mm
● Irregularity of teeth which are more than 4 mm out of line
● Less than the normal number of teeth (missing teeth) where gaps need to be
closed
● Open bites of more than 4 mm
● deep bites with functional problems
● More than the normal number of teeth (supernumerary teeth)
Grade 5 is for severe dental health problems
● When teeth cannot come into the mouth normally because of obstruction by
crowding, additional teeth or any other cause.
● A large number of missing teeth.
● Upper front teeth that protrude more than 9 mm
● lower front teeth that protrude in front of the upper more than 3.5 mm and where
there are functional difficulties too
● cranio-facial anomalies such as cleft lip and palate.
The second part of the IOTN is the Aesthetic Component (AC).
The NHS does recognise that some children need and benefit from orthodontic
treatment on the basis of poor aesthetics. The Aesthetic Component of the IOTN is a
scale of 10 colour photographs showing different levels of dental attractiveness. The
grading is made by the orthodontist matching the patient to these photographs. The
photographs were arranged in order by a panel of lay persons.
Within the NHS if a patient in Dental Health category 3 has an Aesthetic Component
rating of 6 or more NHS treatment is permissible.
Source: British Orthodontic Society http://www.bos.org.uk/Public-Patients/Orthodontics-for-Children-Teens/Fact-File-FAQ/What-Is-The-IOTN
OFFICIAL
Final version 68
D. The Essex Youth Forum discussion on orthodontics 2014 The Essex Youth Forum was asked by Essex County Council to consider Orthodontics as part of a consultation on the Orthodontic needs assessment. The vast majority of orthodontic care is provided to the age group 11 – 18, represented by this Forum. A written briefing was prepared for them, which they used to create a simple questionnaire to take back to their schools to capture views, anonymously, of people who had had orthodontic care. These views were then fed back to representatives of the local dental commissioning team. Views expressed are summarised in figure 33. Some key points are as follows:
Services were considered generally good and accessible although waiting times for first appointments were sometimes long.
Young people wanted their orthodontist to treat them as adults, to converse and explain simply and clearly directly with them (not their parents), throughout the whole course of treatment and after the braces are removed, responding to individual questions in a caring and comprehensible way, ensuring that any pain and problems were anticipated and that patients were clear and confident about what to do if an appliance breaks.
Young people wanted Orthodontic practices to have excellent communication with the referring dental practices and schools and ensure there was good information about their services and who is eligible, and importantly who not.
Young people wanted good parking facilities to be available. They also wanted a range of appointment times, including after school.
Young people wanted information about eligibility for Orthodontic treatment to be available through non-dental health services, such as youth health trainers, height and weight checks and sexual health clinics.
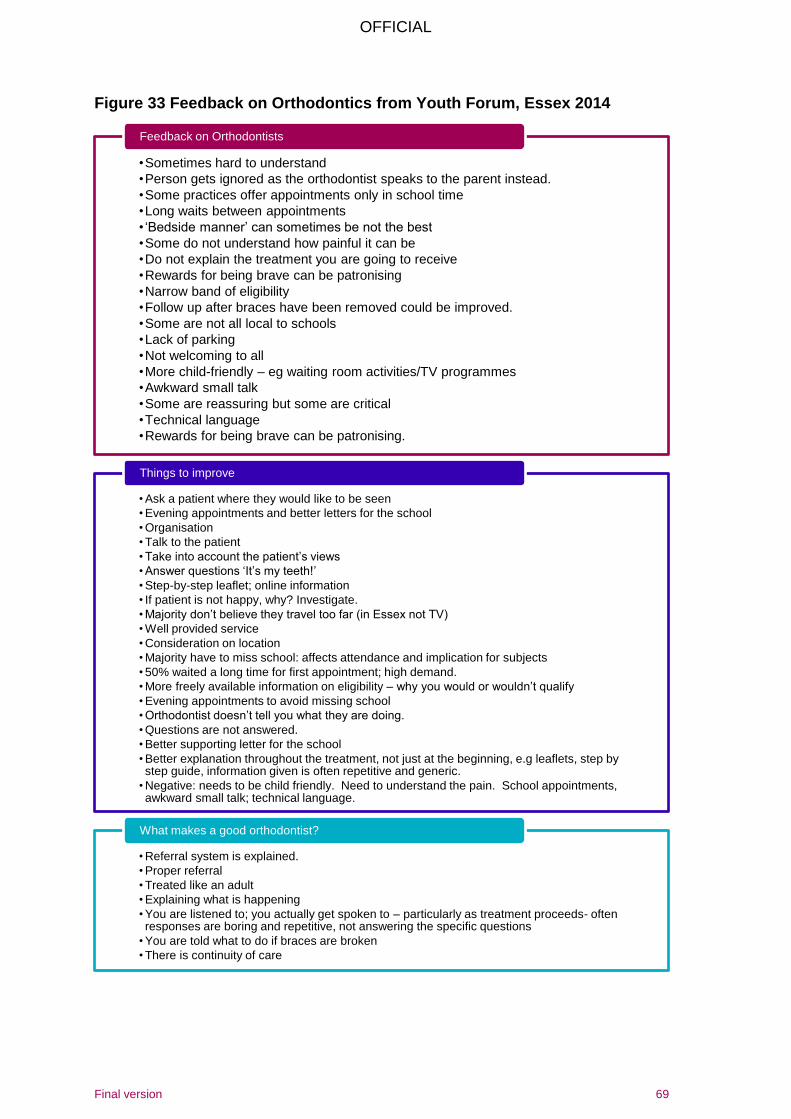
OFFICIAL
Final version 69
Figure 33 Feedback on Orthodontics from Youth Forum, Essex 2014
•Sometimes hard to understand
•Person gets ignored as the orthodontist speaks to the parent instead.
•Some practices offer appointments only in school time
•Long waits between appointments
• ‘Bedside manner’ can sometimes be not the best
•Some do not understand how painful it can be
•Do not explain the treatment you are going to receive
•Rewards for being brave can be patronising
•Narrow band of eligibility
•Follow up after braces have been removed could be improved.
•Some are not all local to schools
•Lack of parking
•Not welcoming to all
•More child-friendly – eg waiting room activities/TV programmes
•Awkward small talk
•Some are reassuring but some are critical
•Technical language
•Rewards for being brave can be patronising.
Feedback on Orthodontists
• Ask a patient where they would like to be seen
• Evening appointments and better letters for the school
• Organisation
• Talk to the patient
• Take into account the patient’s views
• Answer questions ‘It’s my teeth!’
• Step-by-step leaflet; online information
• If patient is not happy, why? Investigate.
• Majority don’t believe they travel too far (in Essex not TV)
• Well provided service
• Consideration on location
• Majority have to miss school: affects attendance and implication for subjects
• 50% waited a long time for first appointment; high demand.
• More freely available information on eligibility – why you would or wouldn’t qualify
• Evening appointments to avoid missing school
• Orthodontist doesn’t tell you what they are doing.
• Questions are not answered.
• Better supporting letter for the school
• Better explanation throughout the treatment, not just at the beginning, e.g leaflets, step by step guide, information given is often repetitive and generic.
• Negative: needs to be child friendly. Need to understand the pain. School appointments, awkward small talk; technical language.
Things to improve
• Referral system is explained.
• Proper referral
• Treated like an adult
• Explaining what is happening
• You are listened to; you actually get spoken to – particularly as treatment proceeds- often responses are boring and repetitive, not answering the specific questions
• You are told what to do if braces are broken
• There is continuity of care
What makes a good orthodontist?
OFFICIAL
Final version 70
19 References 1 NHS England Guides for commissioning dental specialties – Orthodontics 2015
https://www.england.nhs.uk/commissioning/wp-
content/uploads/sites/12/2015/09/guid-comms-orthodontics.pdf
2 Thames Valley Dental Public Health Network. Orthodontic Healthcare Needs Assessment, MOBBB Dental Cluster. June 2012 3 General Dental Council website. Orthodontics. Accessed at: URL: http://www.gdc-
uk.org/Search+our+registers/home/Home.htm
4 Holmes, (1992) The prevalence of orthodontic need. British Journal of Orthodontics
19 177-182
5 Artun J. The role of minimal intervention in orthodontics. Medical Principles and
Practice 2002; 11:7-15.
6 Mid-year estimates: Population Estimates by single year of age and sex for local
authorities in the UK, mid-2014 ONS data http://www.ons.gov.uk/ons/publications/re-
reference-tables.html?edition=tcm%3A77-335242
7 NHS Dental Epidemiology Programme for England Oral Health Survey of 12 year
old Children 2008 / 2009
http://www.nwph.net/dentalhealth/reports/Report_NHS_DEP_for_England_OH_Surv
ey_12yr_2008-09.pdf
8 Stephens C.D. Standing Dental Advisory Committee – Report of an Expert Group
1992 Department of Health – Unpublished
9 Brook PH, Shaw WC. The development of an index of orthodontic treatment
priority. European Journal of Orthodontics 1989; 11 :309-320.
10 Holmes A. The Prevalence of Orthodontic Treatment Need. British Journal of
Orthodontics 1992; 19:177-182.
11 Wang G, Hagg U, Ling J. The orthodontic treatment need and demand of Hong
Kong Chinese children. Chinese Journal of Dental Research 1999; 2(3-4):84-92.
12 Abdullah MS, Rock WP. Assessment of orthodontic treatment need in 5,112
Malaysian children using the IOTN and DAI indices. Community Dental Health 2001;
18(4):242-248.
OFFICIAL
Final version 71
13 Abu Alhaija ES, Al-Nimri KS, Al-Khateeb SN. Orthodontic treatment need and
demand in 12-14-year-old north Jordanian school children. European Journal of
Orthodontics 2004; 26(3):261-263.
14 Health and Social Care Information Centre. 2015 Children’s Dental Health Survey 2013 Report 4: The Burden of Dental Disease in Children England, Wales and Northern Ireland http://www.hscic.gov.uk/catalogue/PUB17137/CDHS2013-Report4-Burden-of-Dental-Disease.pdf 15 Health and Social Care Information Centre. 2015 Children’s Dental Health Survey
2013 Report 5: Contemporary Challenges in Children’s Dental Health England,
Wales and Northern Ireland
http://www.hscic.gov.uk/catalogue/PUB17137/CDHS2013-Report5-Contemporary-
Challenges.pdf
16 British society for Paediatric Dentistry (BSPD) Guidelines For The Management Of Children Referred For Dental Extractions Under General Anaesthesia http://bspd.co.uk/Portals/0/Public/Files/Guidelines/Main%20Dental%20Guidelines.pdf
Related Documents











