A multicenter randomized, masked comparison trial of natural versus synthetic surfactant for the treatment respiratory distress syndrome of Mark L. Hudak, MD, Elaine E. Farrell, MD, Adam A. Rosenberg, MD, August L, Jung, MD, Richard L. Auten, MD, David J. Durand, MD, Michael J. Horgan, MD, Sharon Buckwald, MD, Marc R. Belcastro, DO, Pamela K. Donohue, CHA, VMen Carrion, MD, William W. Maniscaico, MD, Michael J. Balsan, MD, Benjamin A. Torres, MD, Randy R. Miller, MD, Robert D. Jansen, MD, Janet E. Graeber, MD, Kathleen M. Laskay, MSN, Elizabeth J. Matteson, RNC,NNP, Edmund A. Egan, MD, Alan S. Brody, MD, David J. Martin, MD, Merchline M. Riddlesberger, MD, and Paul Montgomery, MD From the Departments of Pediatrics and Pediatric Radiology, Children's Hospital of Buffalo State University of New York at Buffalo; the Department of Pediatrics, Evanston Hospital, Evanston, Illinois; the Department of Pediatrics, University of Colorado Health Sciences Center and Children's Hospital of Denver; the Department of Pediatrics, University of Utah Medical Center, Salt Lake City; the Department of Pediatrics, Duke University Medical Center, Durham, North Carolina; the Division of Neonatology, Children's Hospital of Oak- land, Oakland, California; the Department of Pediatrics, Alta Bates Hospital, Berkeley, CaF ifornia; the Department of Pediatrics, Albany Medical Center, Albany, New York; the De- partment of Pediatrics, North Shore University Medical Center, Manhasset, New York; the Division of Neonatology, Miami Valley Hospital, Dayton, Ohio; the Department of Pediat- rics, Johns Hopkins University School of Medicine, Baltimore, Maryland; the Department of Pediatrics, Strong Memorial Hospital, Rochester, New York; the Division of Neonatology, Magee Women's Hospital, Pittsburgh, Pennsylvania; the Division of Neonatology, Tampa General Hospital, Tampa, Florida; the Department of Pediatrics, Columbus Children's Hos- pital, Columbus, Ohio; the Department of Pediatrics, Northwestern University Medical School, Chicago, Illinois; the Department of Pediatrics, West Virginia University School of Medicine, Morgantown; and the Department of Pediatrics, University of South Alabama Medical School, Mobile Objective: To compare the efficacy and safety of two surfactant preparations in the treatment of respiratory distress syndrome (RDS). Methods: We conducted a randomized, masked comparison trial at 21 centers. Infants with RDS who were undergoing mechanical ventilation were eligible for treatment with two doses of either a synthetic (Exosurf) or natural (Infasurf) surfac- tant if the ratio of arterial to alveolar partial pressure of oxygen was less than or equal to 0.22. Crossover treatment was allowed within 96 hours of age if severe Supported by a research grant from ONY, Inc., and from Forest Laboratories. Presented in part at the annual meeting of the Society for Pediatric Research, Seattle, Wash., May 1994. Submitted for publication June 20, 1995; accepted Oct. 13, 1995. Reprint requests: Mark L. Hudak, MD, Division of Neonatology, University of Florida at Jacksonville, 653-1 West 8th St., Jackson- ville, FL 32209. Copyright © 1996 by Mosby-Year Book, Inc. 0022-3476/96/$5.00 + 0 9/23/69850 396

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A multicenter randomized, masked comparison trial of natural versus synthetic surfactant for the treatment respiratory distress syndrome
of
Mark L. Hudak, MD, Elaine E. Farrell, MD, Adam A. Rosenberg, MD, August L, Jung, MD, Richard L. Auten, MD, David J. Durand, MD, Michael J. Horgan, MD, Sharon Buckwald, MD, Marc R. Belcastro, DO, Pamela K. Donohue, CHA, VMen Carrion, MD, William W. Maniscaico, MD, Michael J. Balsan, MD, Benjamin A. Torres, MD, Randy R. Miller, MD, Robert D. Jansen, MD, Janet E. Graeber, MD, Kathleen M. Laskay, MSN, Elizabeth J. Matteson, RNC, NNP, Edmund A. Egan, MD, Alan S. Brody, MD, David J. Martin, MD, Merchline M. Riddlesberger, MD, and Paul Montgomery, MD From the Departments of Pediatrics and Pediatric Radiology, Children's Hospital of Buffalo State University of New York at Buffalo; the Department of Pediatrics, Evanston Hospital, Evanston, Illinois; the Department of Pediatrics, University of Colorado Health Sciences Center and Children's Hospital of Denver; the Department of Pediatrics, University of Utah Medical Center, Salt Lake City; the Department of Pediatrics, Duke University Medical Center, Durham, North Carolina; the Division of Neonatology, Children's Hospital of Oak- land, Oakland, California; the Department of Pediatrics, Alta Bates Hospital, Berkeley, CaF ifornia; the Department of Pediatrics, Albany Medical Center, Albany, New York; the De- partment of Pediatrics, North Shore University Medical Center, Manhasset, New York; the Division of Neonatology, Miami Valley Hospital, Dayton, Ohio; the Department of Pediat- rics, Johns Hopkins University School of Medicine, Baltimore, Maryland; the Department of Pediatrics, Strong Memorial Hospital, Rochester, New York; the Division of Neonatology, Magee Women's Hospital, Pittsburgh, Pennsylvania; the Division of Neonatology, Tampa General Hospital, Tampa, Florida; the Department of Pediatrics, Columbus Children's Hos- pital, Columbus, Ohio; the Department of Pediatrics, Northwestern University Medical School, Chicago, Illinois; the Department of Pediatrics, West Virginia University School of Medicine, Morgantown; and the Department of Pediatrics, University of South Alabama Medical School, Mobile
Objective: To compare the efficacy and safety of two surfactant preparations in the treatment of respiratory distress syndrome (RDS). Methods: We conducted a randomized, masked comparison trial at 21 centers. Infants with RDS who were undergoing mechanical ventilation were eligible for treatment with two doses of either a synthetic (Exosurf) or natural (Infasurf) surfac- tant if the ratio of arterial to alveolar partial pressure of oxygen was less than or equal to 0.22. Crossover treatment was allowed within 96 hours of age if severe
Supported by a research grant from ONY, Inc., and from Forest Laboratories.
Presented in part at the annual meeting of the Society for Pediatric Research, Seattle, Wash., May 1994.
Submitted for publication June 20, 1995; accepted Oct. 13, 1995.
Reprint requests: Mark L. Hudak, MD, Division of Neonatology, University of Florida at Jacksonville, 653-1 West 8th St., Jackson- ville, FL 32209.
Copyright © 1996 by Mosby-Year Book, Inc.
0022-3476/96/$5.00 + 0 9/23/69850
3 9 6

The Journal of Pediatrics Hudak et al. 3 9 7 Volume 128, Number 3
respiratory failure (defined as two consecutive arterial/alveolar oxygen tension ratios -<0.10) persisted after two doses of the randomly assigned surfactant. Four primary outcome measures of efficacy (the incidence of pulmonary air leak [-<7 days]; the severity of RDS; the incidence of death from RDS; and the incidence of survival without bronchopulmonary dysplasia [BPD] at 28 days after birth) were compared by means of linear regression techniques. Results: The primary analysis of efficacy was performed in 1033 eligible infants and an analysis of safety outcomes in the 1126 infants who received study surfactant. Preentry demographic characteristics and respiratory status were similar for the two treatment groups, except for a small but significant difference in mean ges- tational age (0.5 week) that favored the Infasurf treatment group. Pulmonary air leak (-~7 days) occurred in 21% of Exosurf- and 11% of Infasurf-treated infants (adjusted relative risk, 0.53; 95% confidence interval, 0.40 to 0.7 I; p -<0.000 I). Dur- ing the 72 hours after the initial surfactant treatment, the average fraction of inspired oxygen (±SEM) was 0.47 ± 0.01 for Exosurf- and 0.39 ± 0.01 for Infasurf- treated infants (difference, 0.08; 95% confidence interval, 0.06 to 0.10; p <0.000 I); the average mean airway pressure (±SEM) was 8.6 ± 0. I cm H20 for Exosurf- and 7.2 ± 0.1 cm H20 for Infasurf-treated infants (difference, 1.4 cm H20; 95% con- fidence interval, 1.0 to 1.8 cm H2o; P <0.0001). The incidences of RDS-related death, total respiratory death, death to discharge, and survival without bron- chopulmonary dysplasia at 28 days after birth did not differ. The number of days of more than 30% inspired oxygen and of assisted ventilation, but not the duration of hospitalization, were significantly lower in Infasurf-treated infants. Conclusion: Compared with Exosurf, Infasurf provided more effective therapy for RDS as assessed by significant reductions in the severity of respiratory disease and in the incidence of air leak complications. (J PEDIATR 1996; 128:396-406)
Preclinical comparisons of commercially available and investigational surfactants have shown substantial differ- ences in physical composition as well as in the in vitro bio- physical and in vivo physiologic activities.l-6 Infasuff (ONY, Inc., Amherst, N.Y.; investigational new drug No. 27,169) is a natural surfactant that is extracted from safine lavage fluid of calf lungs. 7-9 Compared with Exosurf Neonatal (Burroughs Wellcome Co., Research Triangle Park, N.C.), Infasurf has superior surface tension-lowering abilities at an air-liquid interface and greater resistance to inhibitors such as plasma proteins that can degrade biophysical performance in vivo. 2, 3, 5, 6 In excised rat lungs made surfactant deficient by saline lavage, Infasurf instillation almost fully restores lung mechanical properties, whereas Exosurf has little effect. 2 Infasurf produces better gas exchange, lung compli- ance, and survival rates than does Exosurf when adminis- tered to premature lambs with respiratory distress syn- drome. 4
Therefore we performed a multicenter, randomized, masked trial designed to compare the efficacy and safety of Exosurf and Infasurf in the treatment of infants with a pri- mary respiratory diagnosis of RDS. We hypothesized that, in comparison with Exosurf, Infasurf treatment of neonates with RDS would improve acute respiratory status, reduce air leak complications associated with RDS, and possibly de- crease RDS mortality rates.
M E T H O D S
Study centers. The trial was conducted at 21 neonatal in- tensive care units between February 1991 and June 1993. Nine centers (hereafter referred to as Infasurf centers) had previously participated in clinical trials of Infasurf. At the other 12 centers (Exosurf centers), Exosurf had been the most commonly used surfactant. The study protocol and an informed consent form were approved by the institutional review board at each center. The coordinating center for the study was located at the Children's Hospital of Buffalo.
a/A P02 BPD CLD FI02 IVH MAP RDS
Arterial to alveolar partial pressure of oxygen Bronchopulmonary dysplasia Chronic lung disease Fraction of inspired oxygen Intraventricular hemorrhage Mean airway pressure Respiratory distress syndrome
Eligibility and enrollment. Infants were eligible for the trial if the following criteria were met: (1) clinical and radiologic findings consistent with a primary respiratory di- agnosis of RDS; (2) respiratory distress severe enough to re- quire endotracheal intubation and mechanical ventilation; (3) a ratio of arterial to alveolar partial pressure of oxygen during mechanical ventilation of less than or equal to 0.22; (4) age less than 72 hours; and (5) written informed consent

3 9 8 Hudak et al. The Journal of Pediatrics March 1996
by a parent or guardian. Infants were not eligible if they had previously received an exogenous surfactant, had a congen- ital anomaly or proven chromosomal abnormality for which aggressive intervention was deemed futile, had physiologic instability (e.g., hypotension, bradycardia, or hypoglyce- mia), or had a persistent pneumothorax or pneumopericar- dium. Once physiologic stability had been attained, air leaks controlled, or both, infants could be enrolled if they met el- igibility criteria. Infants with valid informed consent were considered to be enrolled in the study at the time of random-
ization. Randomization and masking of treatment assignment.
Unique randomization codes were generated for each center by applying the Moses-Oakford algorithm to a random se- quence of block lengths of 4, 6, 8, and 10. l° Treatment as- signments were recorded on index cards sealed within sequentially numbered opaque envelopes.
Surfactant randomization and preparation were performed either in the nursery by a research assistant (a nurse or res- piratory therapist) or off site by a research pharmacist. Pro- cednres specific to each center were prospectively designed to safeguard masking of the surfactant treatment. Aliquots of surfactant were drawn up into syringes that were covered with cloth tape or a black plastic sheath to ensure that the color, consistency, and volume of surfactant were not ap- parent to other clinical caretakers. Surfactant administration was accomplished by the research assistant in the presence of the bedside nurse and either a respiratory therapist or a physician, according to the prospectively written protocol at each study center. The research assistant did not participate in the clinical care of the infant for a minimum of 5 days thereafter.
Snrfactant treatment. Exosurf Neonatal is a protein-free synthetic surfactant that contains a single phospholipid (di- palmitoylphosphatidylcholine), hexadecanol, tyloxapol, and sodium chloride. Each vial of lyophilized powder was reconstituted with sterile water in accordance with the instructions on the drug package insert) I Infasurf is a sur- factant preparation purified from a chloroform-methanol extract of a saline lavage of calf lung. Infasurf contains snr- factant proteins B and C (approximately 2% by weight). 1~ Each vial of lnfasurf suspension was warmed to room tem- perature and gently agitated by inversion before aliquot
preparation. Each infant received an initial dose of surfactant (Exosurf,
5 ml/kg; Infasurf, 3 ml/kg) after randomization. A second dose was administered 12 hours later if intubation continued and the attending physician approved. Two crossover treat- ments administered 12 hours apart were permitted after two study treatments if the following criteria were met: (1) the a/A Po 2 ratio was less than or equal to 0.10 on two consec- utive arterial blood gas studies; (2) the infant was less than or equal to 96 hours of age; (3) a minimum of 4 hours had
passed since the previous surfactant treatment; and (4) the attending physician judged that treatment was of potential
benefit. Both surfactants were administered via the side port of the
endotracheal tube adapter as recommended on the Exosurf package insert. By protocol, the mechanical ventilatory rate was increased to a minimum of 30 breaths/min. Heart rate, transcutaneous arterial oxygen saturation, and chest excur- sion were monitored continuously. A decrease in heart rate or arterial saturation, or evidence of airway obstruction, ne-
cessitated slowing or cessation of surfactant delivery; an in- crease in inspired oxygen concentration, ventilator rate, and/or mechanical pressure support; and/or initiation of manual ventilation as judged necessary by tile surfactant ad- ministration team. Occurrences of bradycardia (heart rate <100 beats/rain), airway obstruction (a requirement for in- creased ventilatory pressure or rate support or a requirement for manual ventilation), arterial desaturation (an increase in the fraction of inspired oxygen of >--0.05 to maintain ade- quate oxygenation), and other unusual complications were recorded.
Data collection and auditing. Maternal demographics and the obstetric history of the index pregnancy, labor, and delivery were abstracted from the mother's medical record. Information about surfactant administration was transcribed from standardized procedure notes in the infant's medical record. Ventilator and oxygen requirements before and for the first 168 hours after the initial surfactant treatment and neonatal outcomes through hospital discharge were ab- stracted from the infant's medical record. Mean airway pressure was calculated on the basis of a square respiratory pressure waveform. 13 Chest radiographs obtained before study entry, 1 and 3 days after initial surfactant treatment, at day 28, and at 36 weeks of postconceptional age, as well as chest radiographs that supported the presence of air leak, were sent to the coordinating center and evaluated by a ra- diology reading committee consisting of three pediatric ra- diologists. Cranial sonograms were also sent to the coordi- nating center and were evaluated by a single neurosonolo- gist (D. J. M.). Cause(s) of death were assigned by the principal investigators with the use of study definitions. For each death, relevant portions of the medical record, includ- ing a final autopsy report, were reviewed by the study chair- man. When the cause of death assigned by the study chair- man and by a principal investigator differed, the final assignment of the cause of death was made by a steering committee comprising the principal investigators from five of the participating centers. Research assistants, principal investigators, and the study radiologists and neurosonologist were masked to treatment assignment during data collection and outcome detemainations.
Study definitions. The severity of early respiratory dis- ease was quantitated as the average inspired FIo2 and mean

The Journal of Pediatrics Hudak et al. 3 9 9 Volume 128, Number 3
airway pressure for the first 72 hours after initial surfactant
treatment. Death was attributed to RDS if death occurred as a result of respiratory failure in the first 14 days of life and causes of respiratory failure other than RDS had been excluded. A diagnosis of pulmonary air leak was assigned if an air leak (i.e., pneumothorax; pulmonary interstitial em- physema; pneumomediastinum; pneumopericardium; sub- cutaneous emphysema) resulting from lung parenchymal disease was verified by the radiology reading committee, or if a clinical diagnosis of air leak resulted in a therapeutic in- tervention (e.g., thoracentesis or pericardiocentesis, place- ment of a thoracostomy or pericardiostomy, or both) with-
out preceding radiographic documentation. Right and left lungs were evaluated separately for air leak.
Bronchopulmonary dysplasia was defined as a require- ment for supplemental oxygen and a chest radiograph with a Toce-Edwards score greater than or equal to 4.14 BPD was assessed both at 28 days after birth and near term (at 36 weeks for infants with gestational age -<32 weeks and at 28 days after birth for infants with gestational age >32 weeks). Death was attributed to BPD if (1) death occurred primarily as a result of cardiorespiratory failure after 14 days of age, (2) the chest radiograph demonstrated findings consistent with BPD, and (3) another primary cause of cardiorespira-
tory failure could not be proved. To broaden the comparison of pulmonary outcomes, the following two definitions of chronic lung disease were evaluated at 28 days after birth and near term: (1) the requirement for any supplemental ox- ygen and (2) an 1~o2 requirement greater than 0.30. All def- initions were developed and recorded before initiation of the study but were not revealed to masked personnel until ter- mination of the trial.
Pulmonary hemorrhage was defined prospectively as the finding of bright red blood in the endotracheal tube, associ- ated with a deterioration in clinical status that prompted therapeutic intervention. The severity of intraventricular hemorrhage was graded with the use of the definitions of Papile et al. 15 applied to sonograms or to autopsy findings. A diagnosis of periventricular leukomalacia was made if sonograms demonstrated postnatal development of multiple cystic echolucencies in cerebral white matter. Congenital sepsis was defined as the isolation of a pathogen from blood or cerebrospinal fluid cultured within the first 24 hours of life. All congenital anomalies were screened and are reported as significant if consistent with written definitions developed before study initiation.
Study outcomes. The four primary study outcome mea- sures of efficacy were (1) the incidence of pulmonary air leak caused by lung parenchymal disease that occurred after the initial surfactant treatment and before 7 days of age, (2) the severity of initial respiratory disease as quantitated by the average FIo2 and MAP for 72 hours after the initial surfac- rant treatment, (3) the incidence of death caused by RDS, and
(4) the incidence of survival without BPD at 28 days after birth.
Secondary outcome measures of efficacy included (1) crossover surfactant treatment under protocol or treatment with a nonstudy surfactant after study withdrawal, (2) sur- vival at 28 days after birth and to hospital discharge, (3) sur- vival without CLD at 28 days after birth and near term, (4)
duration of assisted ventilation and supplemental oxygen therapy, and (5) duration of hospitalization. Secondary out- come measures of safety included acute surfactant adminis- tration complications as well as the incidences of serious morbidities of prematurity.
Sample size determination. The incidence of pulmonary air leak was reported to be 34% in infants with birth weights between 700 and 1350 gm treated with two doses of Exo- suff. 16 A sample size of 400 in this birth weight group was
required to detect a 37% decrease (from 34% to 21%) in the incidence of pulmonary air leak associated with Infasuff treatment with a type II error of 0.20 (power of 80%) and a type I error of 0.05 (two-tailed). The total sample size was determined by the relative rates of accrual of the target birth
weight (700 to 1350 gm) and the two nontarget birth weight (<700 gm; >1350 gin) groups.
Statistical analysis and data management. Both cate-
gorical and continuously distributed primary end points of efficacy were first compared with appropriate regression techniques. By design, statistical models were to include terms for surfactant treatment, birth weight, and center, and terms for the interactions of surfactant treatment with birth weight and center, as well as terms for other important base- line variables that might be found to be significantly differ- ent between the two treatment groups. Data from centers with fewer than 10 infants in either treatment group were combined and analyzed a s a single site. In practice, all inter- action terms were not significant (p >0.05) and were deleted from the final analysis. The final logistic regression model (with terms for surfactant treatment, birth weight, center, and
gestational age) identified the independent effect of surfac- tant treatment.
Groups were compared by means of the two-tailed Student t test (normal distributions) or the Wilcoxon rank-sum test (non-normal distributions) for continuous variables and the chi-square, Fisher Exact, or Mantel-Haenszel test for cate- gorical variables. The point estimate of the relative risk ratio (the ratio of the probability of an outcome among infants treated with Infasurf to the probability of that outcome among infants treated with Exosurf) and the 95% confidence intervals were calculated by means of the Mantel-Haenszel chi-square test stratified by center and by the three birth weight groups.
The average FIO2 and MAP for the first 72 hours after ini- tial surfactant treatment were calculated as the area under the- curve with the use of the trapezoidal approximation. In cases
4 0 0 Hudak et al. The Journal of Pediatrics March 1996
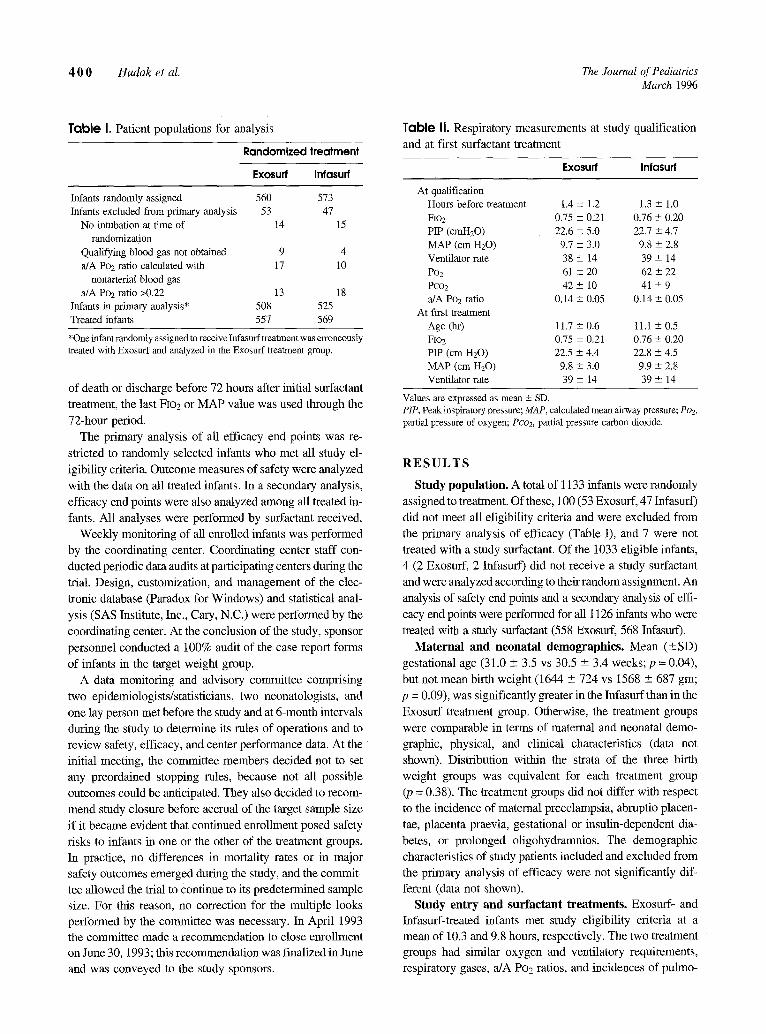
Table I. Patient populations for analysis
Randomized treatment
Exosurf Infasurf
Infants randomly assigned 560 573 Infants excluded from primary analysis 53 47
No intubation at time of 14 15 randomization
Qualifying blood gas not obtained 9 4 a/A Po2 ratio calculated with 17 10
nonarterial blood gas a/A Poz ratio >0.22 13 18
Infants in primary analysis* 508 525 Treated infants 557 569
*One infant randomly assigned to receive Infasurf treatment was erroneously treated with Exosurf and analyzed in the Exosurf treatment group.
of death or discharge before 72 hours after initial surfactant
treatment, the last FIo2 or MAP value was used through the
72-hour period. The primary analysis of all efficacy end points was re-
stricted to randomly selected infants who met all study el-
igibility criteria. Outcome measures of safety were analyzed
with the data on all treated infants. In a secondary analysis, efficacy end points were also analyzed among all treated in-
fants. All analyses were performed by surfactant received. Weekly monitoring of all enrolled infants was performed
by the coordinating center. Coordinating center staff con-
ducted periodic data audits at participating centers during the trial. Design, customization, and management of the elec-
tronic database (Paradox for Windows) and statistical anal-
ysis (SAS Institute, Inc., Cary, N.C.) were performed by the
coordinating center. At the conclusion of the study, sponsor
personnel conducted a 100% audit of the case report forms
of infants in the target weight group. A data monitoring and advisory committee comprising
two epidemiologists/statisticians, two neonatologists, and
one lay person met before the study and at 6-month intervals
during the study to determine its rules of operations and to review safety, efficacy, and center performance data. At the
initial meeting, the committee members decided not to set any preordained stopping rules, because not all possible outcomes could be anticipated. They also decided to recom-
mend study closure before accrual of the target sample size
if it became evident that continued enrollment posed safety
risks to infants in one or the other of the treatment groups. In practice, no differences in mortality rates or in major safety outcomes emerged during the study, and the commit- tee allowed the trial to Continue to its predetermined sample size. For this reason, no correction for the multiple looks performed by the committee was necessary. In April 1993 the committee made a recommendation to close enrollment on June 30, 1993; this recommendation was finalized in June and was conveyed to the study sponsors.
Table II. Respiratory measurements at study qualification and at first surfactant treatment
Exosurf Infasurf
At qualification Hours before treatment 1.4 + 1.2 1.3 ± 1.0 FIO2 0.75 -- 0.21 0.76 + 0.20 PIP (cmH20) 22.6 ± 5.0 22.7 ± 4.7 MAP (cm H20) %7 ± 3.0 9.8 ± 2.8 Ventilator rate 38 -+ 14 39 -+ 14 Po2 61 -+ 20 62 ± 22 Pco2 42 -+ l0 41 +_ 9 a/A Po2 ratio 0.14 ± 0.05 0.14 + 0.05
At first treatment Age (hr) 11.7 ± 0.6 11.1 ± 0.5 FIO2 0.75 -+ 0.21 0.76 ± 0.20 PIP (cm H20) 22.5 ± 4.4 22.8 ± 4.5 MAP (cm H20) 9.8 ± 3.0 9.9 -+ 2.8 Ventilator rate 39 ± 14 39 -+ 14
Values are expressed as mean _+ SD. PIP, Peak inspiratory pressure; MAP, calculated mean airway pressure; Poe, partial pressure of oxygen; Pco2, partial pressure carbon dioxide.
RESULTS
Study population. A total of 1133 infants were randomly
assigned to treatment. Of these, 100 (53 Exosuff, 47 Infasurf) did not meet all eligibility criteria and were excluded from
the primary analysis of efficacy (Table I), and 7 were not treated with a study suffactant. Of the 1033 eligible infants,
4 (2 Exosuff, 2 Infasurf) did not receive a study suffactant and were analyzed according to their random assignment. An
analysis of safety end points and a secondary analysis of effi- cacy end points were performed for all 1126 infants who were
treated with a study surfactant (558 Exosnrf, 568 Infasnrf).
Maternal and neonatal demographics. Mean (_+SD) gestational age (31.0 -+ 3.5 vs 30.5 -+ 3.4 weeks; p = 0.04), but not mean birth weight (1644 + 724 vs 1568 -+ 687 gin;
p = 0.09), was significantly greater in the Infasuff than in the
Exosuff treatment group. Otherwise, the treatment groups were comparable in terms of maternal and neonatal demo-
graphic, physical, and clinical characteristics (data not shown). Distribution within the strata of the three birth weight groups was equivalent for each treatment group (p = 0.38). The treatment groups did not differ with respect
to the incidence of maternal preeclampsia, abruptio placen-
tae, placenta praevia, gestational or insulin-dependent dia- betes, or prolonged oligohydramnios. The demographic characteristics of study patients included and excluded from
the primary analysis of efficacy were not significantly dif-
ferent (data not shown). Study entry and surfactant treatments. Exosurf- and
Infasuff-treated infants met study eligibility criteria at a mean of 10.3 and 9.8 hours, respectively. The two treatment groups had similar oxygen and ventilatory requirements, respiratory gases, a/A Po2 ratios, and incidences of pulmo-
The Journal of Pediatrics Hudak et al. 4 0 1 Volume 128, Number 3
80 :!:!:i:i:~:";i:;!:i:i - - E x o s u r f
ii:iii:ii:iii:i:i.i~:ii~ - - Infasur f E.ii.i:?]:;~:;~) ' x
6 0 :':.:' . . . . . . . . . . . . . . . . ! :?: "!:i'~:i'i:!'i:?i ::::::::::::::::::::::::: ~ ~ _
0 " 40 - - ""
20
0 ' ' [[ J | |
12 ........................ . , . . . . . . , . . . . . . . . . . . . . . ,:.:.:.:.::,:.:,:.:.:.:
10 .?;?i.. " ..... .:.:.:.:.:.:,:.:.:-:.:,: ~
8 ~ - ~ - ~ - ~ - ~ - - _ ~ , -::'::'::'::'::':: - i I I " - ~.
6 :Gi:!:!:!:!:!:i:i:i ~ ' ~ I<.M. ~
4 :iii:iii:iii:!ii:iii:ii) i:.:?.:>t':)':>
a !i{!!i{iiiiiiii!iii!iii!i
................. t l 0 ~i l i ' i ] i ' : : ] ' ] : i ' : l I I I ]¢ 1 I J
e,i
0.5
0.4
0.3
0.2
0.1
0
i:!:!:!:!:i:i:i:i;i:i:!:i: ::::::::::::::::::::::::::::::::::: ::::::::::::::::::::::::::::::::: .~
? ~ i ~ : ~ i l ] i i i i i : i i i i i i : . . ~ _ ~r- "
:::::::::::::::::::::::: ~ _ ~ - ~ - ~ - -
:::::::::::::::::::::::::::: ;?;.?I.?97~G?:. ?;?;!.!:?~:?;?;-. ~:!:!:!;!:!I!:I;:L ~ I
0 1 2 2 4 3 6
• E ~
I I
4 8 6 0 7 2 11 1 6 8
H o u r s A f t e r T r e a t m e n t
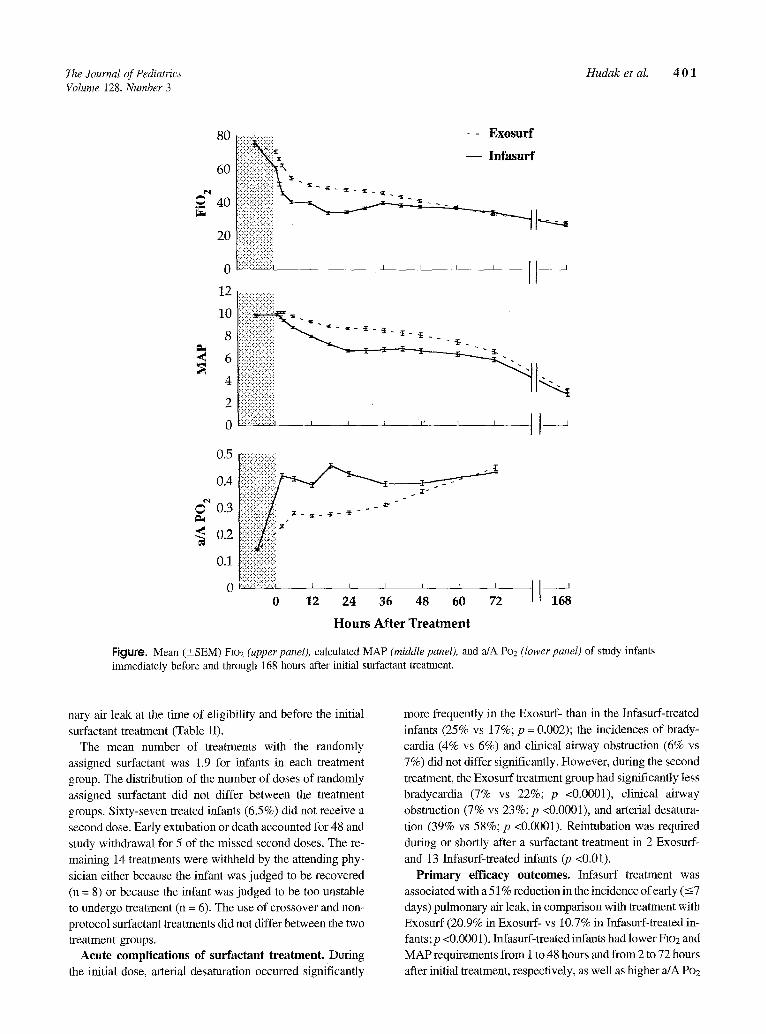
Figure. Mean (_+SEM) F]o2 (upper panel), calculated MAP (middle panel), and a/A Po2 (lower panel) of study infants immediately before and through 168 hours after initial surfactant treatment.
nary air leak at the time of eligibility and before the initial surfactant treatment (Table II).
The mean number of treatments with the randomly assigned surfactant was 1.9 for infants in each treatment group. The distribution of the number of doses of randomly assigned surfactant did not differ between the treatment groups. Sixty-seven treated infants (6.5%) did not receive a second dose. Early extubation or death accounted for 48 and study withdrawal for 5 of the missed second doses. The re- maining 14 treatments were withheld by the attending phy- sician either because the infant was judged to be recovered (n = 8) or because the infant was judged to be too unstable to undergo treatment (n = 6). The use of crossover and non- protocol surfactant treatments did not differ between the two treatment groups.
A c u t e complications of surfactant treatment. During the initial dose, arterial desaturation occurred significantly
more frequently in the Exosurf- than in the Infasurf-treated infants (25% vs 17%; p = 0.002); the incidences of brady- cardia (4% vs 6%) and clinical airway obstruction (6% vs 7%) did not differ significantly. However, during the second treatment, the Exosurf treatment group had significantly less bradycardia (7% vs 22%; p <0.0001), clinical airway obstruction (7% vs 23%; p <0.0001), and arterial desatura- tion (39% vs 58%; p <0.0001). Reintubation was required during or shortly after a surfactant treatment in 2 Exosurf- and 13 Infasurf-treated infants (p <0.01).
P r i m a r y e f f i c a c y o u t c o m e s . Infasurf treatment was associated with a 51% reduction in the incidence of early (-<7 days) pulmonary air leak, in comparison with treatment with Exosurf (20.9% in Exosuff- vs 10.7% in Infasurf-treated in- fants; p <0.0001). Infasurf-treated infants had lower FIO2 and MAP requirements from 1 to 48 hours and from 2 to 72 hours after initial treatment, respectively, as well as higher a/A Po2
4 0 2 Hudak et al. The Journal of Pediatrics March 1996
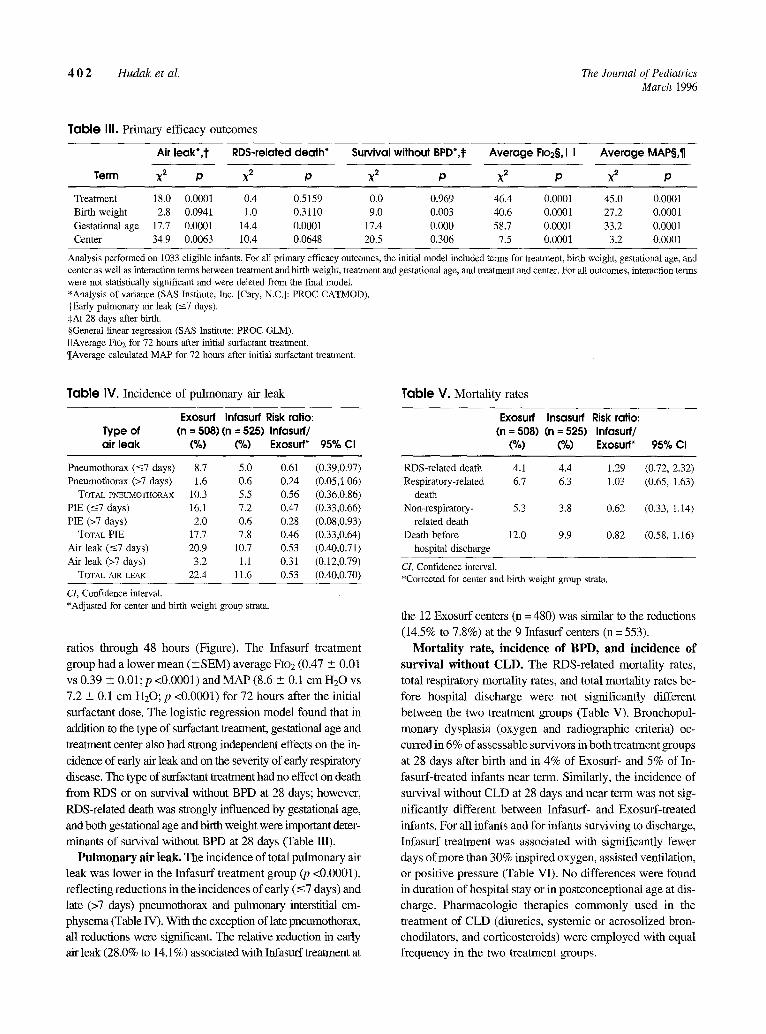
Table III. Primary efficacy outcomes
Air leak*,'J" RDS-related death* Survival without BPD*,~ Average Flo2§, I I Average MAP§,¶
Term ×2 p X2 p X2 p X2 p X2 p
Treatment 18.0 0.0001 0.4 0.5159 0.0 0.969 46.4 0.0001 45.0 0,0001 Birth weight 2.8 0.0941 1.0 0.3110 9.0 0.003 40.6 0.0001 27.2 0,0001 Gestational age 17.7 0.0001 14.4 0.0001 17.4 0.000 58.7 0.0001 33.2 0.0001 Center 34.9 0.0063 10.4 0.0648 20.5 0.306 7.5 0.0001 3.2 0.0001
Analysis performed on 1033 eligible infants. For all primary efficacy outcomes, the initial model included terms for treatment, birth weight, gestational age, and center as well as interaction terms between treatment and birth weight, treatment and gestational age, and treatment and center. For all outcomes, interaction terms were not statistically significant and were deleted from the final modal. *Analysis of variance (SAS Institute, Inc. [Cary, N.C.]: PROC CATMOD). -~Early pulmonary air leak (-<7 days). SAt 28 days after birth. §General linear regression (SAS Institute: PROC GLM). I IAverage F~oz for 72 hours after initial surfactant ixeatment. q[Average calculated MAP for 72 hours after initial surfactant treatment.
Table IV. Incidence of pulmonary air leak T a b l e V. Mortality rates
Exosurf Infasurf Risk ratio: Exosurf Insasurf Risk ratio: Type of (n = 508) (n = 525) Infasurf/ (n = 508) (n = 525) Infasurf/ air leak (%) (%) Exosurf* 95% CI (%) (%) Exosurf* 95% Cl
Pneumothorax (-<7 days) 8.7 5.0 0.61 (0 .39,0 .97) RDS-related death 4.1 4.4 1.29 Pneumothorax (>7 days) 1.6 0.6 0.24 (0 .05,1 .06) Respiratory-related 6.7 6.3 1.03
TOTAL etCEUMOTHORAX 10.3 5.5 0.56 (0.36,0.86) death PIE (-<7 days) 16.1 7.2 0.47 (0 .33,0 .66) Non-respiratory- 5.3 3.8 0.62 PIE (>7 days) 2.0 0.6 0.28 (0.08,0.93) related death TOTAL PIE 17.7 7.8 0.46 (0.33,0.64) Death before 12.0 9.9 0.82
Air leak (-<7 days) 20.9 10.7 0.53 (0.40,0.71) hospital discharge
Air leak (>7 days) 3.2 1.1 0.31 (0.12,0.79) CI, Confidence interval. TOTAL AIR LEAK 22.4 11.6 0.53 (0.40,0.70) *Corrected for center and birth weight group strata.
cI, Confidence interval. *Adjusted for center and birth weight group strata.
ratios through 48 hours (Figure). The Infasurf treatment
group had a lower mean (-+SEM) average FIo2 (0.47 -+ 0.01
vs 0.39 ,+ 0.01;p <0.0001) and MAP (8.6 -+ 0.1 cm H20 vs
7.2 _+ 0.1 cm H20; p <0.0001) for 72 hours after the initial
surfactant dose. The logistic regression model found that in
addition to the type of surfactant treatment, gestational age and
treatment center also had strong independent effects on the in-
cidence of early air leak and on the severity of early respiratory
disease. The type of surfactant treatment had no effect on death
from RDS or on survival without BPD at 28 days; however,
RDS-Mated death was strongly influenced by gestational age,
and both gestational age and birth weight were important deter-
minants of survival without BPD at 28 days (Table HI).
Pulmonary air leak. The incidence of total pulmonary air
leak was lower in the Infasurf treatment group (p <0.0001),
reflecting reductions in the incidences of early (-<7 days) and
late (>7 days) pneumothorax and pulmonary interstitial em-
physema (Table W). With the exception of late pneumothorax,
all reductions were significant. The relative reduction in early
air leak (28.0% to 14.1%) associated with Infasurf treatment at
(0.72, 2.32) (0.65, 1.63)
(0.33, 1.t4)
(0.58, 1.16)
the 12 Exosurf centers (n = 480) was similar to the reductions
(14.5% to 7.8%) at the 9 Infasurf centers (n = 553).
Mortality rate, incidence of BPD, and incidence of survival without CLD. The RDS-related mortality rates,
total respiratory mortality rates, and total mortality rates be-
fore hospital discharge were not significantly different
between the two treatment groups (Table V). Bronchopul-
monary dysplasia (oxygen and radiographic criteria) oc-
curred in 6% of assessable survivors in both treatment groups
at 28 days after birth and in 4% of Exosuff- and 5% of In-
fasurf-treated infants near term. Similarly, the incidence of
survival without CLD at 28 days and near term was not sig-
nificantly different between Infasurf- and Exosuff-treated
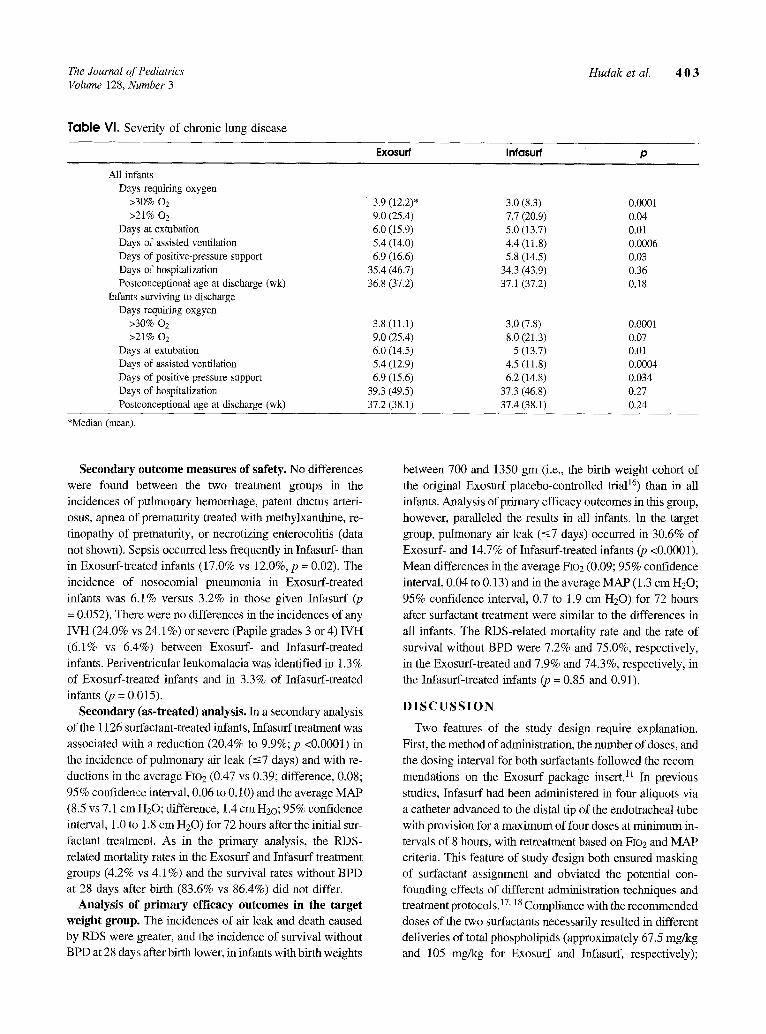
infants. For all infants and for infants surviving to discharge,
Infasurf treatment was associated with significantly fewer
days of more than 30% inspired oxygen, assisted ventilation,
or positive pressure (Table VI). No differences were found
in duration of hospital stay or in postconceptional age at dis-
charge. Pharmacologic therapies commonly used in the
treatment of CLD (diuretics, systemic or aerosolized bron-
chodilators, and corticosteroids) were employed with equal
frequency in the two treatment groups.
The Journal of Pediatrics Hudak et aL 4 0 3 Volume 128, .Number 3
Table VI. Severity of chronic lung disease
Exosurf Infasurf p
All infants Days requiting oxygen
>30% 02 >21% 02
Days at extubation Days of assisted ventilation Days of positive-pressure support Days of hospitalization Postconceptional age at discharge (wk)
Infants surviving to discharge Days requiring oxgyen
>30% 02 >21% 02
Days at extubation Days of assisted ventilation Days of positive pressure support Days of hospitalization Postconceptional age at discharge (wk)
3.9 (12.2)* 3.0 (8.3) 0.0001 9.0 (25.4) 7.7 (20.9) 0.04 6.0 (15.9) 5.0 (13.7) 0.01 5.4 (14.0) 4.4 (11.8) 0.0006 6.9 (16.6) 5.8 (14.5) 0.03
35.4 (46.7) 34.3 (43.9) 0.36 36.8 (37.2) 37.1 (37.2) 0.18
3.8 (11.1) 3.0 (7.8) 0.0001 9.0 (25.4) 8.0 (21.3) 0.07 6.0 (14.5) 5 (13.7) 0.01 5.4 (12.9) 4.5 (11.8) 0.0004 6.9 (15.6) 6.2 (14.8) 0.034
39.3 (49.5) 37.3 (46.8) 0.27 37.2 (38.1) 37.4 (38.1) 0.24
*Median (mean).
Secondary outcome measures of safety. No differences were found between the two treatment groups in the incidences of pulmonary hemorrhage, patent ductus arteri- osus, apnea of prematurity treated with methylxanthine, re- tinopathy of prematurity, or necrotizing enterocolitis (data not shown). Sepsis occurred less frequently in Infasurf- than in Exosurf-treated infants (17.0% vs 12.0%, p = 0.02). The incidence of nosocomial pneumonia in Exosurf-treated infants was 6.1% versus 3.2% in those given Infasurf (p = 0.052). There were no differences in the incidences of any
IVH (24.0% vs 24.1%) or severe (Papile grades 3 or 4) IVH (6.1% vs 6.4%) between Exosurf- and Infasurf-treated infants. Periventricular leukomalacia was identified in 1.3 % of Exosurf-treated infants and in 3.3% of Infasurf-treated infants (p = 0.015).
Secondary (as-treated) analysis. In a secondary analysis of the 1126 surfactant-treated infants, Infasurf treatment was associated with a reduction (20.4% to 9.9%; p <0.0001) in the incidence of pulmonary air leak (-<7 days) and with re- ductions in the average FIo2 (0.47 vs 0.39; difference, 0.08; 95% confidence interval, 0.06 to 0.10) and the average MAP (8.5 vs 7.1 cm H20; difference, 1.4 cm H2o; 95% confidence interval, 1.0 to 1.8 cm H20) for 72 hours after the initial sur- factant treatment. As in the primary analysis, the RDS- related mortality rates in the Exosurf and Infasurf treatment groups (4.2% vs 4.1%) and the survival rates without BPD at 28 days after birth (83.6% vs 86.4%) did not differ.
Analysis of primary efficacy outcomes in the target weight group. The incidences of air leak and death caused by RDS were greater, and the incidence of survival without BPD at 28 days after birth lower, in infants with birth weights
between 700 and 1350 gm (i.e., the birth weight cohort of the original Exosuff placebo-controlled triaP 6) than in all infants. Analysis of primary efficacy outcomes in this group, however, paralleled the results in all infants. In the target group, pulmonary air leak (-<7 days) occurred in 30.6% of Exosurf- and 14.7% of Infasurf-treated infants (p <0.0001).
Mean differences in the average FIo2 (0.09; 95% confidence interval, 0.04 to 0.13) and in the average MAP (1.3 cm H20; 95% confidence interval, 0.7 to 1.9 cm H20) for 72 hours after surfactant treatment were similar to the differences in all infants. The RDS-related mortality rate and the rate of survival without BPD were 7.2% and 75.0%, respectively, in the Exosurf-treated and 7.9% and 74.3%, respectively, in the lnfasurf-treated infants (p = 0.85 and 0.91).
D I S C U S S I O N
Two features of the study design require explanation. First, the method of administration, the number of doses, and the dosing interval for both surfactants followed the recom- mendations on the Exosurf package insert. 11 In previous
studies, Infasuff had been adininistered in four aliquots via a catheter advanced to the distal tip of the endotracheal tube with provision for a maximum of four doses at minimum in- tervals of 8 hours, with retreatment based on FIo2 and MAP criteria. This feature of study design both ensured masking of surfactant assignment and obviated the potential con- founding effects of different administration techniques and treatment protocols.IV, 18 Compliance with the recommended doses of the two surfactants necessarily resulted in different defiveries of total phospholipids (approximately 67.5 mg/kg and 105 mg/kg for Exosurf and Infasurf, respectively);

4 0 4 Hudak et al. The Journal of Pediatrics March 1996
however, an increase in the Exosurf dose to 100 mg phos- pholipid per kilogram of body weight has not been shown to confer additional efficacy. 19 Second, the provision for
crossover treatment afforded the infants with severe respira- tory failure access to both surfactants in case significant dif- ferences in efficacy did exist. The investigators judged that end points other than RDS-related death (i.e., the incidence of air leak and the severity of RDS) would provide sufficient comparative information.
Several considerations motivated the choice of total pul- monary air leak as the primary efficacy end point. Air leak may be life-threatening, require invasive treatment, or lead to implementation of different treatments or strategies of ventilation. Air leak has also been associated with an increased risk of intracranial hemorrhage. 2°' 21 For these
reasons, we believed that air leak in an individual infant would provide a more meaningful index of acute disease se- verity than would, for instance, integration of inspired oxy- gen or MAP requirements with time. Although Exosurf treatment reduced air leak in earlier trials, the incidence of air leak in treated infants was still substantial (17% and 34% in the two largest trials)) 6' 22 An extensive open-label expe-
rience with Infasurf suggested that a comparison trial might identify up to a 50% further reduction in the frequency of air leak in infants weighing 700 to 1350 gm at birth. This ex- pectation was supported by metaanalyses in which protein- containing surfactants appeared to have prevented air leak complications more effectively than did synthetic surfac- tants.23, 24 Finally, at least in infants not treated with surfac- tant, air leak has been a powerful surrogate marker for death and BPD. 25
Selection of end points used in the original placebo-con- trolled trials of Exosurf (death or survival without BPD) would have been unrealistic within the setting of the study design. The very low rates of respiratory-related death in the Exosurf treatment trials (2.9% and 7.8% for infants weigh- ing ->1250 gm and those weighing between 700 and 1350 gin, respectively) would have required a prohibitively large sample size to detect modest differences in respiratory- related mortality rates with adequate power. 16,22 Further-
more, the provision for crossover surfactant treatment was meant to minimize differences in respiratory-related mortal- ity rates between the two treatment groups.
This study did define that Infasuff treatment was associ- ated with a nearly 50% decrease in the incidence of pulmo- nary air leak. The incidence of air leak in Exosurf-treated infants with birth weights between 700 and 1350 gm was the same as that reported in the placebo-controlled trial of Ex- osurf in this birth weight group. 16 The significance of these differences is strengthened by the diagnostic consistency achieved through the assignment of radiographic air leak outcomes by an independent panel of pediatric radiologists.
Although the logistic regression model identified a signif- icant influence of treatment center on the incidence of air leak, the finding of a similar percentage of reduction in air leak associated with Infasurf treatment at both Exosurf and Infasurf centers excludes the possibility that the overall sur-
factant treatment effect was systematically influenced by center differences in familiarity with the two surfactants. The higher overall incidence of air leak at the Exosurf centers was not explained by differences in maternal or infant demo- graphics or in respiratory status at study entry. Variations in other population characteristics, in ventilation strategies, or both may have mediated the observed difference.
Even though the Infasurf group had less severe RDS and
fewer air leaks, the incidence of RDS-related death was the same in both treatment groups. This finding was unlikely to have arisen from error in the assignments of cause of death. Not only were the total respiratory-related mortality rates equal in the two treatment groups, but also Kaplan-Meier survival curves for the two groups during the first 2 weeks of life were superimposable.
Attempts to infer the effect of surfactant on BPD through a cumulative review of published trials is of limited value for several reasons, including differences among studies in el- igibility criteria, in treatment protocols, in the outcome of the control groups, and in the definitions of BPD. Even defini- tions that incorporate chest radiograph findings are not nec- essarily comparable; in practice, the requirement for a Toce- Edwards score greater than or equal to 4 identifies fewer in- fants with BPD than the more general requirement for parenchymal abnormalities consistent with BPD. If the principal effect of surfactant on late pulmonary function were to prevent the very severe cases of BPD, this effect would be best demonstrated by employing a more restrictive definition tailored to identify such cases. This might be one reason why two Exosurf treatment trials reported a reduction in BPD, 16, 22 whereas other studies that adopted more inclu- sive definitions of BPD did not. 26' 27 To establish intrasur-
faetant differences in these outcomes with adequate power would have required recruitment of a number of infants greatly exceeding the time and resources available.
Two large comparison trials of Exosurf and Survanta with a similar design have been reported. 2s' 29 Both trials found
that the severity of acute respiratory disease was significantly lower in infants treated with Survanta than in those treated with Exosurf. A significantly lower incidence of pneumotho- rax was discerned in Survanta- than in Exosnrf-treated infants in the 1297 infants enrolled in the Vermont Oxford Trials Network study (9% vs 15%) but not in the 617 infants in a trial sponsored by the National Institutes of Health (9% vs 13%). The absolute rates of survival without BPD were slightly but not significantly greater in Survanta- than in Ex- osurf-treated infants in both trials. Analysis of the 220 infants

The Journal of Pediatrics Hudak et al. 4 0 5 Volume 128, Number 3
enrolled in our study who would have met all entry criteria
of the two Exosuff-Survanta trials yielded similar findings. Hence, in all three comparison trials, the two protein-
containing surfactants appear to offer an advantage com- pared with synthetic surfactant; this indicates the need for caution against interpreting too literally the metaanalyses of
controlled surfactant trialsY Placebo-controlled trials have occasionally found that
surfactant treatment is associated with significant increases or decreases in some complications of prematurity, includ- ing IVH, 3° pulmonary hemorrhage, 31 patent ductus arterio- sus, 32 sepsis, 33 and apnea. 16, 22 In this study, we identified a
significant increase in periventricular leukomalacia and sig- nificant decreases in postnatal sepsis and pneumonia in the
Infasurf treatment group. These findings may merely illus- trate the increased probability of falsely identifying a signif- icant outcome difference when large numbers of outcomes
are examined. Arterial desaturafion occurred more frequently with Exo-
surf during the first protocol treatment, whereas bradycardia, clinical airway obs~uction, and arterial desaturation were more common events for Infasurf-treated infants during the second dose. Assuming that surfactant-specific physicome- chanical events in the endotracheal tube and airways were equivalent during both doses, we offer the following spec- ulation: Instillation of Infasurf but not Exosurf into a surfac-
tant-deficient lung results in an immediate and significant rise in P02. During the initial dose, this rapid improvement in oxygenation likely compensated for effects of mechani- cal problems related to the propensity of the more surface active Infasurf to foam and partially obstruct ventilation. However, during the second dose, Infasurf-treated infants were receiving reduced oxygen and ventilatory support. Thus the relatively greater physicomechanical problems as- sociated with Infasurf treatment may have been unmasked during this dose. Previous trials of Infasurf that had used an- other administration method and stricter retreatment criteria had not reported the high rates of complications observed in this study.
We conclude that, compared with Exosurf, Infasurf reduced air leak complications and substantially improved the acute respiratory status of infants with RDS. These re- sults are consistent with preclinical comparison of the in vitro biophysical properties and the in vivo physiologic activities of the two surfactants. 1-6 In addition, Infasurf treatment was associated with improvement in some secondary outcome measures, including the number of days of using more than 30% oxygen and the number of days of using assisted ven- tilation. The trial did not have sufficient power to detect dif- ferences between rates of survival and rates of survival without BPD. We believe that Infasurf is preferable to Ex- osurf for the treatment of RDS.
We are grateful to the parents of the enrolled infants; to the nurses, respiratory therapists, house officers, and attending physicians at the participating centers; to the research associates; and to the members of the Data Monitoring and Advisory Committee. Special thanks are due to Lindy Canavan, Elizabeth Matteson, RN, NNP, Jessica Baus, RN, Karen Middleton, and Kathy Huges for their work in coordi- nating the study, and to Bonnie Hudak, MD, and Frederick C. Morin III, MD, for manuscript review.
The research associates who participated in this trial were as follows: Donna Curtis, RN, Children's Hospital of Buffalo, Buffalo, N.Y.; Jeanette M. Asselin, MS, RRT, Martha Birch, RCPT, and Margaret Wen-Chen, Rig, Oakland Children's Hospital, Oakland, Calif.; Katherine E. O'Brien, RN, and Paul C. Fitzgerald, RN, MSN, Northwestern Memorial Hospital, Chicago, Ill.; Lois V. Kimberlin, RNC, Evanston Hospital, Evanston, Ill.; Sharon E. Stroebel, BSN, MSN, Johns Hopkins Hospital, Baltimore, Md.; Kathy J. Auten, BA, Duke University Medical Center, Durham, N.C.; Mary Beth Hollinger, RN, MSN, Susan Boynton, RN, and Pauline Graziano, RN, Albany Medical Center, Albany, N.Y.; Kathleen A. Coughlin, RN, BS, North Shore University Medical Center, Manhasset, N.Y.; Sue Mackey, RRT, Miami Valley Hospital, Dayton, Ohio; Shawna Baker, RN, and Karen Osborne, RN, Primary Children's Hospital and University of Utah Medical Center, Salt Lake City, Utah; Su- san Moreland, RN, Children's Hospital of Denver, Denver, Colo.; Shirley MacKenzie, RN, MSN, Faith McNabb, RN, and Kathy Hale, BSN, University of Colorado Medical Center, Denver; Kath- leen M. Laskay, MSN, University of South Alabama, Mobile; Linda Reubens, RN, Strong Memorial Hospital, Rochester, N.Y.; Mar- garet Wen, RRT, Alta Bates Hospital, Oakland, Calif.; Catherine M. Groh, RN, Tampa General Hospital, Tampa, Fla.; Judith G. Jones, RNC, BSN, Magee Women's Hospital, Pittsburgh, Pa.; Cathy Schumer, RN, Columbus Children's Hospital and Ohio State Uni- versity Hospital, Columbus; and Mary E. Chafin, RN, BSN, NNP, West Virginia University School of Medicine, Morgantown.
The members of the Data Monitoring and Advisory Committee were Curtis Meinert, PhD (Chairman), and Richard Royall, PhD, Department of Biostatisfics and Epidemiology, Johns Hopkins School of Public Health and Hygiene, Baltimore, Md.; Lillian R. Blackmon, MD, Department of Pediatrics, University of Maryland School of Medicine, Baltimore, Md.; Billie Lou Short, MD, Department of Pediatrics, George Washington University School of Medicine, Washington D.C.; and Fr. Frank Tuchols, Department of Pastoral Care, Children's Hospital of Buffalo, Buffalo, N.Y.
The members of the Steering Committee were James J. Cum- mings, MD, Department of Pediatrics, Childrens Hospital of Buf- falo, Buffalo, N.Y.; Elaine E. Farrell, MD, Department of Pedlar- tics, Evanston Hospital, Evanston, Ill.; Richard L. Auten, MD, De- partment of Pediatrics, Duke University Medical Center, Durham, N.C.; August L. Jung, MD, Department of Pediatrics, University of Utah Medical Center, Salt Lake City; and Adam A. Rosenberg, MD, Department of Pediatrics, University of Colorado Health Sciences Center, Denver.
The members of the Radiology Reading Committee were Alan S. Brody, MD, Paul Montgomery, MD, and Merchline M. Riddles- berger, MD, Department of Pediatric Radiology, Children's Hospi- tal of Buffalo, Buffalo, N.Y.
4 0 6 Hudak et aI. The Journal of Pediatrics March 1996
R E F E R E N C E S
1. Jobe A, Ikegami M. Surfactant for the treatment of respiratory distress syndrome. Am Rev Respir Dis 1987;136:1256-75.
2. Notter R. Physical chemistry and physiological activity of pulmonary suffactants. In: Shapiro D, Notter R, eds. Suffac- tant replacement therapy. New York: Alan R. Liss, 1989:19- 70.
3. Schurch S. Surface tension properties of surfactant. Clin Pefi- natol 1993;20:669-82.
4. Cummings J, Holm B, Hudak M, Hudak B, Ferguson W, Egan E. A controlled clinical comparison of four different surfactant preparations in surfactant-deficient preterm lambs. Am Rev Respir Dis 1992;145:999-1004.
5. Seeger W, Grnbe C, Gunther A, Schmidt R. Surfactant inhibi- tion by plasma proteins: differential sensitivity of various sur- factant preparations. Eur Respir J 1993;6:971-7.
6. Hall SB, Venkitaraman AR, Whitsett JA, Holm BA, Notter RH. Importance of hydrophobic apoproteins as constituents of clin- ical exogenous surfactants. Am Rev Respir Dis 1992;145:24- 30.
7. Enhorning G, Shennan A, Possmayer F, Dunn M, Chen C, Milligan J. Prevention of neonatal respiratory distress syn- drome by tracheal instillation of surfactant: a randomized clin- ical trial. Pediatrics 1985;76:145-53.
8. Kattwinkel J, Bloom B, Delmore P, et al. Prophylactic admin- istration of calf lung surfactant extract is more effective than early treatment of respiratory distress syndrome in neonates of 29 through 32 weeks gestation. Pediatrics 1993;92:90-8.
9. Kwong M, Egan E, Notter R, Shapiro D. Double-blind clinical trial of calf lung surfactant extract for the prevention of hyaline membrane disease in extremely premature infants. Pediatrics 1985;76:585-92.
10. Meinert C, Tonascia S. Clinical trials: design, conduct, and analysis. New York: Oxford University Press, 1986.
11. Exosurf Neonatal (colfosceril palmitate, cetyl alcohol, tylox- apol) for intratracheal suspension [package insert]. Research Triangle Park, North Carolina: Burroughs Wellcome, 1990.
12. Mizuno K, Ikegami M, Chen C, Ueda T, Jobe A. Surfactant protein-B supplementation improves in vivo function of a modified natural surfactant. Pediatr Res 1995;37:271-6.
13. Glenski J, Marsh H, Hall R. Calculation of mean airway pres- sure during mechanical ventilation in neonates. Crit Care Med 1984;12:642-4.
14. Toce S, Farrell P, Leavitt L, Samuels D, Edwards D. Clinical and roentgenographic scoring systems for assessing broncho- pulmonary dysplasia. Arch Pediatr Adolesc Med [Am J Dis Child] 1984;138:581-5.
15. Papile L, Burstein J, Burstein R, Koffier H. Incidence and evo- lution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1500 gm. J lhZDI- ATR 1978;92:529-34.
16. Long W, Thompson T, Sundell H, et al. Effects of two rescue doses of a synthetic surfactant on mortality rate and survival without bronchopulmonary dysplasia in 700- to 1350-gram in- fants with respiratory distress syndrome. J PEDIATR 1991;118: 595-605.
17. Segerer H, van Gelder W, Angenent F, et al. Pulmonary dis- tribution and efficacy of exogenous surfactant in lung-lavaged rabbits are influenced by the instillation technique. Pediatr Res 1993;34:490-4.
18. Ueda T, Ikeganai M, Rider ED, Jobe AH. Distribution of sur- factant and ventilation in surfactant-treated preterm lambs. J Appl Physiol 1994;76:45-55.
19. Berry D, Pramanik A, Philips J, et al. Comparison of the effect of three doses of a synthetic surfactant on the alveolar-arterial oxygen gradient in infants weighing > or = 1250 grams with respiratory distress syndrome [American Exosurf Neonatal Study Group]. J PEOrATR 1994;124:294-301.
20. Hill A, Perlman J, Volpe J. Relationship of pneumothorax to occurrence of intraventricular hemorrhage in the premature newborn. Pediatrics 1982;69:144-9.
21. Wallin L, Rosenfeld C, Laptook A, et al. Neonatal intracranial hemorrhage. II. Risk factor analysis in an inborn population. Early Human Dev 1990;23:129-37.
22. Long W, Corbet A, Cotton R, et al. A controlled trial of syn- thetic surfactant in infants weighing 1250 grams or more with respiratory distress syndrome. N Engl J Med 1991;325:1696- 703.
23. Jobe A. Pulmonary surfactant therapy. N Engl J Med 1993; 328:861-8.
24. Merritt T, Soil R, Hallman M. Overview of exogenous surfac- tant replacement therapy. J Intensive Care Med 1993;8:205-28.
25. Powers W, Clemens J. Prognostic implications of age at detec- tions of air leak in very low birth weight infants requiring ven- tilatory support. J PEDIATR 1993;123:611-7.
26. Liechty E, Donovan E, Purohit D, et al. Reduction of neonatal mortality after multiple doses of bovine surfactant in low birthweight neonates with respiratory distress syndrome. Pedi- atrics 1991;88:19-28.
27. Collaborative European Multicenter Study Group. Surfactant replacement therapy for severe neonatal respiratory distress syndrome: an international randomized clinical trial. Pediatrics 1988;82:683-91.
28. Horbar J, Wright L, Soll R, et al. A multicenter randomized trial comparing two surfactants for the treatment of neonatal respi- ratopy distress syndrome. J PED~TR 1993;123:757-66.
29. The Vermont Oxford Trials Network. A multicenter random- ized trial comparing synthetic surfactant to modified bovine surfactant extract in the treatment of neonatal respiratory dis- tress syndrome. Conference proceeding: Hot Topics in Neona- tology, Washington, D.C., 1994:175.
30. Horbar J, Soll R, Schachinger H, et al. A European multicenter randomized controlled trial of single-dose surfactant therapy for idiopathic respiratory distress syndrome. Eur J Pediatr 1990; 149:416-23.
31. Raju T, Langenberg P. Pulmonary hemorrhage and exogenous surfactant therapy: a metaanalysis. J PEDIAa~ 1993; 123:603-10.
32. Raju T, Bhat R, McCulloch K. Double-blind controlled trial of single-dose treatment with bovine surfactant in severe hyaline membrane disease. Lancet 1987;1:651-6.
33. Survanta (Beractant): intratracheal suspension [package insert]. Columbus, Ohio: Ross Laboratories, 1994.
Related Documents











