Original Contributions A Mixed-Methods Evaluation of Health-Related Quality of Life for Male Veterans with and without Intestinal Stomas Robert S. Krouse, M.D., 1 Marcia Grant, R.N., D.N.Sc., 2 Christopher S. Wendel, M.S., 3 M. Jane Mohler, Ph.D., M.P.H., 3,4 Susan M. Rawl, Ph.D., 5 Carol M. Baldwin, Ph.D., 6 Stephen Joel Coons, Ph.D., 7 Ruth McCorkle, Ph.D., 8 Clifford Y. Ko, M.D., 9 C. Max Schmidt, M.D., Ph.D. 10 1 Southern Arizona Veterans Affairs Health Care System, University of Arizona College of Medicine, Tucson, Arizona 2 Department of Nursing Research and Education, City of Hope National Medical Center, Duarte, California 3 Southern Arizona Veterans Affairs Health Care System, Tucson, Arizona 4 University of Arizona Colleges of Medicine, Public Health, and Pharmacy, Tucson, Arizona 5 Center for Nursing Research, Indiana University School of Nursing, Indianapolis, Indiana 6 Arizona State University College of Nursing, Southwest Borderlands, Phoenix, Arizona 7 Division of Social and Administrative Sciences, University of Arizona College of Pharmacy, Tucson, Arizona 8 Yale University School of Nursing, New Haven, Connecticut 9 VA Greater Los Angeles Healthcare System, UCLA Center for Health Sciences, Los Angeles, California 10 Richard L. Roudebush VA Medical Center, Department of Surgery, Indiana University School of Medicine, Indianapolis, Indiana PURPOSE: Intestinal stomas have a major impact on Cases_ lives. It is essential to better understand the areas in which interventions may help to minimize the negative consequences. METHODS: This was a case-control survey study using validated instruments (City of Hope Quality of Life-Ostomy and Short Form 36 for Veterans). Cases were accrued from Veterans Affairs Medical Centers in Tucson, Indianapolis, and Los Angeles. Eligibility included a major intra-abdominal surgical procedure that led to an ostomy (cases), or a similar procedure that did not mandate a stoma (controls). Analysis included quantitative and qualitative responses. RESULTS: The response rate was 48 percent (511/1063). Cases and controls had relatively similar demographic characteristics. Because of low numbers of female respondents (13 cases and 11 controls), only results for males are reported. Based on both the City of Hope Quality of Life-Ostomy and Short Form 36 for Veterans, cases reported significantly poorer scores on scales/ domains reflecting psychologic and social functioning and well being. Additionally, cases reported poorer scores on Short Form 36 for Veterans scales reflecting physical functioning and significantly lower scores on multiple Supported by a grant from the Veterans Affairs Health Services Research & Development Service (HSR&D Service) IIR 02-221-2: Health Related Quality of Life in VA Cases with Intestinal Stomas. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs. The funder had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, or preparation, review, or approval of the manuscript. Reprints are not available. Correspondence to: Robert S. Krouse, M.D., Southern Arizona VA Health Care System, Surgical Care Line, 2-112, 3601 S. 6th Avenue, Tucson, AZ 85723, e-mail: [email protected] Dis Colon Rectum 2007; 00: 1–12 DOI: 10.1007/s10350-007-9004-7 * The American Society of Colon and Rectal Surgeons

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OriginalContributions
A Mixed-Methods Evaluationof Health-Related Quality of Lifefor Male Veteranswith and without Intestinal StomasRobert S. Krouse, M.D.,1 Marcia Grant, R.N., D.N.Sc.,2 Christopher S. Wendel, M.S.,3
M. Jane Mohler, Ph.D., M.P.H.,3,4 Susan M. Rawl, Ph.D.,5 Carol M. Baldwin, Ph.D.,6
Stephen Joel Coons, Ph.D.,7 Ruth McCorkle, Ph.D.,8 Clifford Y. Ko, M.D.,9
C. Max Schmidt, M.D., Ph.D.10
1 Southern Arizona Veterans Affairs Health Care System, University of Arizona College of Medicine,
Tucson, Arizona2 Department of Nursing Research and Education, City of Hope National Medical Center, Duarte, California3 Southern Arizona Veterans Affairs Health Care System, Tucson, Arizona4 University of Arizona Colleges of Medicine, Public Health, and Pharmacy, Tucson, Arizona5 Center for Nursing Research, Indiana University School of Nursing, Indianapolis, Indiana6 Arizona State University College of Nursing, Southwest Borderlands, Phoenix, Arizona7 Division of Social and Administrative Sciences, University of Arizona College of Pharmacy, Tucson, Arizona8 Yale University School of Nursing, New Haven, Connecticut9 VA Greater Los Angeles Healthcare System, UCLA Center for Health Sciences, Los Angeles, California10 Richard L. Roudebush VA Medical Center, Department of Surgery, Indiana University School of Medicine,
Indianapolis, Indiana
PURPOSE: Intestinal stomas have a major impact onCases_ lives. It is essential to better understand the areasin which interventions may help to minimize the negative
consequences. METHODS: This was a case-control surveystudy using validated instruments (City of Hope Quality ofLife-Ostomy and Short Form 36 for Veterans). Cases wereaccrued from Veterans Affairs Medical Centers in Tucson,Indianapolis, and Los Angeles. Eligibility included a majorintra-abdominal surgical procedure that led to an ostomy(cases), or a similar procedure that did not mandate a stoma(controls). Analysis included quantitative and qualitativeresponses. RESULTS: The response rate was 48 percent(511/1063). Cases and controls had relatively similardemographic characteristics. Because of low numbers offemale respondents (13 cases and 11 controls), only resultsfor males are reported. Based on both the City of HopeQuality of Life-Ostomy and Short Form 36 for Veterans,cases reported significantly poorer scores on scales/domains reflecting psychologic and social functioning andwell being. Additionally, cases reported poorer scores onShort Form 36 for Veterans scales reflecting physicalfunctioning and significantly lower scores on multiple
Supported by a grant from the Veterans Affairs Health ServicesResearch & Development Service (HSR&D Service) IIR 02-221-2:Health Related Quality of Life in VA Cases with Intestinal Stomas.The views expressed in this article are those of the authors and donot necessarily reflect the position or policy of the Department ofVeterans Affairs. The funder had no role in the design and conduct ofthe study, collection, management, analysis, and interpretation of thedata, or preparation, review, or approval of the manuscript.
Reprints are not available.
Correspondence to: Robert S. Krouse, M.D., Southern ArizonaVA Health Care System, Surgical Care Line, 2-112, 3601 S. 6thAvenue, Tucson, AZ 85723, e-mail: [email protected]
Dis Colon Rectum 2007; 00: 1–12DOI: 10.1007/s10350-007-9004-7* The American Society of Colon and Rectal Surgeons

items in the social domain of the City of Hope Quality ofLife-Ostomy compared with controls. Two-thirds of casesreplied to an open-ended question on their Bgreatestchallenge^ related to their ostomy, which led to furtherclarification of major issues. CONCLUSIONS: Multiplehealth-related quality of life problems were reported bymale veterans with intestinal stomas. The greatest differ-ences between cases and controls were observed in thesocial and psychologic domains/scales. Findings from thisstudy provide a greater understanding of the challengesfaced by ostomates and will inform the development andevaluation of urgently needed intervention strategies. [Keywords: Ostomy; Focus groups; Quality of life; Stomas]
T he number of persons with an intestinal stoma
(ostomy) is estimated to be > 1,000,000 in the
United States and Canada, with numbers increasing
at an annual rate of more than 100,000.1 Intestinal
stomas, or ostomies, are the surgical exteriorization
of the bowel to the anterior abdominal wall. This
may include the small (ileostomy) or large (colosto-
my) bowel, depending on the objective or site of the
stoma. Intestinal stomas are required in various
medical conditions and situations. These include
cancers, most frequently rectal cancer, and benign
etiologies, most commonly diverticulitis or inflam-
matory bowel disease. Intestinal stomas may be
placed on a temporary or a permanent basis based
on issues, such as the urgency of the procedure or
the status of the underlying disease. In addition,
there are variations of ileostomies that are placed
with intent for continence that may provide the
patient with the opportunity to control bowel move-
ments and avoid wearing a bag. Ostomies, nonethe-
less, in the vast majority of cases result in the loss of
control of intestinal contents, both stool and gas.
Whereas surgical standards of care attempt to
preserve bowel continuity for most conditions, many
people will continue to require stomal placement
each year in this country. Since the classic article by
Sutherland et al.2 was published in 1952, which
highlighted psychologic needs of ostomates, rela-
tively little research focusing on health-related
quality of life (HR-QOL) has been directed at this
group of Cases. This has created a huge gap in care
where time and resources need to be focused.
Clinicians and researchers increasingly regard HR-
QOL as an important end point for chronic disease
and cancer management.3 HR-QOL is a complex,
multidimensional concept, which involves a person_s
appraisal of his level of well-being, satisfaction with
life, and ability to perform various tasks.4 HR-QOL
can be viewed as encompassing perceptions of both
positive and negative aspects of physical, emotional,
social, cognitive, and spiritual functioning and well-
being, as well as the discomfort and symptoms
produced by disease or its treatment.5–7 This defini-
tion considers the patient as the ultimate authority
regarding his or her own HR-QOL; hence data are
derived from patient responses to HR-QOL measures.
Stomas have been associated with lower levels of
HR-QOL in multiple domains, irrespective of the type
or reason for the ostomy.8–10 For Cases with colosto-
mies and ileostomies, HR-QOL has been shown to
improve with time as noted by Jenks et al.11 and M.
Grant (unpublished data, 2000), although this finding
is not consistent.12 The many issues that impact HR-
QOL include problems with travel, intimacy, and
satisfaction with appearance. Several studies have
documented additional problem areas, including
sexuality,13–19 psychologic well being2,20–23 and inter-
ference with work, recreational, and sporting activi-
ties19,23,24 (also M. Grant, unpublished data, 2000).
Although all potential losses in functioning and
well being experienced by ostomates may not be
remediable, the evidence from the literature suggests
that more can be done. To understand better the
levels of HR-QOL experienced by veterans living
with intestinal stomas, the VA Ostomy Health-Related
Quality of Life Study was undertaken.25 The results of
this study are intended to provide the basis for
developing and evaluating clinical interventions
designed to mitigate ostomy-related HR-QOL defi-
cits.8 The purpose of this article is to report the main
study findings regarding the self-reported HR-QOL of
veterans who had a major gastrointestinal procedure
that resulted in an intestinal stoma compared with
veterans who experienced similar procedures for
which an ostomy was not required. In addition, we
report responses to an open-ended question asking
about ostomy-specific challenges, which further
illustrated the experience and the potential for
targeted interventions. We hypothesized that there
would be differences in the HR-QOL domains as well
as individual HR-QOL items (such as satisfaction with
appearance, anxiety, ability to travel, and the
ability to be intimate). In addition, we believed
that Cases would explicate their experience to help
understand better all issues related to living with
an ostomy from their personal experiences. These
findings have potential to guide development of
targeted interventions to improve HR-QOL for
ostomates and can be used by health care pro-
KROUSE ET AL Dis Colon Rectum, 2007

viders to improve care for those Cases as they
adapt to living with an ostomy.
MATERIALS AND METHODS
An in-depth presentation of the mixed-methods
design of the VA Ostomy Health-Related Quality of
Life Study has been published elsewhere.25 Briefly, all
subjects were veterans receiving care at VA Medical
Centers in Tucson, Indianapolis, or Los Angeles.
Subjects included 239 Cases with known intestinal
stomas (cases), and 272 Cases who had similar
procedures that did not lead to an ostomy (controls).
Cases who had an ostomy reversed were excluded
from both cases and controls. A mailed survey included
the City of Hope Quality of Life Ostomy-specific
(mCOH-QOL-Ostomy) questionnaire26 and the Medi-
cal Outcomes Study (MOS) Short Form 36 for Veterans
(SF-36V), a measure of general HR-QOL adapted for
use in veteran populations27,28 from the widely used
MOS SF-36.29 The mCOH-QOL-Ostomy has demo-
graphic, nonscaled and scaled items (on an ordinal
scale from 0 = poor to 10 = excellent QOL), along
with several open-ended questions to allow Cases the
opportunity to provide comments about living with an
ostomy. The nonscaled items address the areas of
marital status, work, health insurance, sexual activity,
psychologic support, and diet. The scaled items are
reported based on individual domains (physical,
psychologic, social, and spiritual well being), which
were mapped based on psychometric analysis.30 The
SF-36V retains the original SF-36 measurement model,
which includes eight multi-item scales (i.e., physical
function, role limitations as a result of physical
problems, bodily pain, general health perceptions,
vitality, social functioning, role limitations as a result
of emotional problems, and mental health) as well as
physical (PCS) and mental component summary
(MCS) scores. The subscales and component summary
scores have a possible range of 0 to 100, with higher
scores reflecting better functioning and/or well being.
The overall survey response rate was 48 percent
(511/1,063), including 51 percent of cases (239/467)
and 45 percent of controls (272/596). There are
multiple Cases within the VA system with addresses
that were found or suspected to be incorrect. For
Cases ascertained to have received the mailings, the
response rate was 69 percent. Of the veterans who
completed the survey instrument, 68 percent of the
ostomy Cases (n = 163) chose to write in an essay
response to describe their greatest challenges. As
reported earlier, the estimated internal consistency
reliability coefficients (i.e., Cronbach_s alpha) ranged
from 0.8 to 0.96 and 0.71 to 0.94 for the scales of the
mCOH-QOL-Ostomy and SF-36V questionnaires, re-
spectively.25
Medical history items obtained from VA administra-
tive databases and electronic charts included type of
stoma, reason for stoma, length of time since surgery,
preoperative marking by a stoma nurse, type of
operation, operative findings, and other medical prob-
lems. The Charlson-Deyo comorbidity index31 was
constructed from ICD-9 codes from the VA Patient
Treatment File (admissions) and Outpatient Encounter
(reasons for visits) databases during the year before
the index surgery. For Cases whose reason for an
ostomy was cancer, the type of tumor was confirmed
to the extent possible from the tumor registry.
Scales were scored and missing data were handled
according to the instrument developers_ scoring
algorithms. The SF-36V scale scores were coded as
missing if more than half of the responses for the
scale_s items were missing. Responses were rarely
missing in the mCOH-QOL-Ostomy questionnaire;
the most common missing items were those assessing
intimacy, personal spiritual activities, and religious
activities.
Statistical Analysis
We compared demographic and clinical charac-
teristics between cases and controls by using the
Student_s t-test for continuous measures and the chi-
squared test for categorical measures. In the event of
a significant chi-squared for a categorical variable,
a two-sample test of proportions was performed
for each category. Differences between cases and
controls on measures from the mCOH-QOL-Ostomy
and SF-36V were determined with multivariate
regression, adjusting for subject age, time since
index surgery, and an indicator for Charlson-Deyo
index > 2; these are all variables that had been
hypothesized a priori as potential confounders
based on clinical literature and experience. Other
variables assessed in multivariate models for po-
tential confounding between ostomy status and
HR-QOL outcomes were transformations of time
since surgery, married/partnered status, cancer as
the reason for the ostomy or surgery, race/ethnicity,
ostomy type (ileostomy vs. colostomy), income,
education, and distance from home to VA medical
center.
QUALITY OF LIFE FOR VETERANS WITH STOMAS

The mCOH-QOL-Ostomy and SF-36V domains/
scales and total/summary scores were modeled with
multiple linear regression, whereas individual items
from the COH-QOL-Ostomy were modeled with
maximum-likelihood ordered logit estimation in Stata
version 8.2. Comparisons of individual measures
within an instrument were subjected to a Bonferroni
adjustment. In addition to testing for statistical differ-
ence, we used the empirical rule effect size (ERES)
method to judge minimally important differences
(MID) in outcome measures.32 The ERES defines a
minimally important (or Bclinically significant^) differ-
ence as equivalent to 8 percent of the HR-QOL tool_s
theoretical range, which for the mCOH-QOL-Ostomy
is 0.88 and for the SF-36V is 8 units.
Qualitative Analysis
Qualitative analysis was conducted on answers
identified in the open-ended question at the end of
the mCOH-QOL-Ostomy questionnaire: BMany people
have shared stories about their lives with an ostomy.
Please share with us the greatest challenge you have
encountered in having an ostomy.^ The investigators
individually reviewed the responses by using content
analysis.33 This was performed on the transcriptions of
the written correspondence using four linked pro-
cesses: processing the raw data, data reduction, data
display, and conclusion drawing/verification.34,35 The
data were analyzed by using the four domains of the
mCOH-QOL-Ostomy model: physical, psychologic,
social, and spiritual well being.
Original data were deidentified and assigned a
subject identification (ID). Investigators, trained in
qualitative content analysis, read and examined all data
to identify units of analysis, which were defined as a
paragraph, sentence, verb phrase, or single word that
conveyed a single meaning, idea or concept.34,35
Responses frequently had several themes within an
essay. Thus, some responses were divided into two or
more themes, but individual statements were not
double coded. Each essay was coded by at least three
investigators. Differences were discussed with the
entire investigative team, and the group as a whole
decided final coding. Data within each of these
themes were compared by using thematic analysis.
All of the themes were identified and validated
through discussion, review, verification, and consen-
sus by the authors. This review occurred during
weekly conference calls with the investigative team.
Units that corresponded to a theme in the mCOH-
QOL-Ostomy questionnaire were bracketed and dis-
played in a table organized according to the QOL
themes encompassed by the physical, psychologic,
social, or spiritual domains. Units that did not
correspond to a QOL theme but were deemed
significant based on repetition and emphases through-
out the data were bracketed, and two additional
themes were identified: ostomy-specific content and
health care issues content. Final review was then
performed by two investigators to ensure consistency,
clarity, and any discrepancies were identified.
RESULTS
There were 239 cases and 272 controls who
returned completed survey instruments. They were
noted to be similar based on demographic and
clinical characteristics, including no significant differ-
ence in the Charlson comorbidity index (Tables 1
and 2). Fourteen percent of ostomy subjects believed
that their stoma was placed on a temporary basis.
The Btemporary^ subgroup did not show statistically
significant differences in outcome measures com-
pared with other cases, and thus these Cases were
not analyzed separately in this report. The major
clinical differences noted were a longer time since
surgery in cases (11.2 vs. 4.1 years; P < 0.001) and
significantly different proportions of reasons for
surgery. Time since surgery was significantly longer
for subjects with reason for surgery of inflammatory
bowel disease or benign tumor compared with other
reasons (13 vs. 5.7 years; P < 0.001), and this contrast
was more pronounced in cases (20 vs. 8 years;
P < 0.001) than controls (4.8 vs. 3.9 years; P < 0.05).
Cases and controls had similar frequencies of colo-
rectal cancer but within that cases had significantly
more rectal cancer. Cases also had significantly fewer
subjects with benign tumors and acute inflammatory/
infections and significantly more subjects with in-
flammatory bowel disease. The higher percentage of
married/partnered status in preoperative cases was
gone by the time of the surgery, showing that 6
percent of the ostomates had lost their married/
partnered status. Because of the small number of
females in the sample (13 cases and 11 controls) and
the known differences in QOL between males and
females, we report results from analyses that includ-
ed only male respondents.
Stratified analysis by reason for surgery revealed a
demarcation in QOL outcomes between two subgroups:
Group A (colorectal cancer, acute inflammatory/
KROUSE ET AL Dis Colon Rectum, 2007
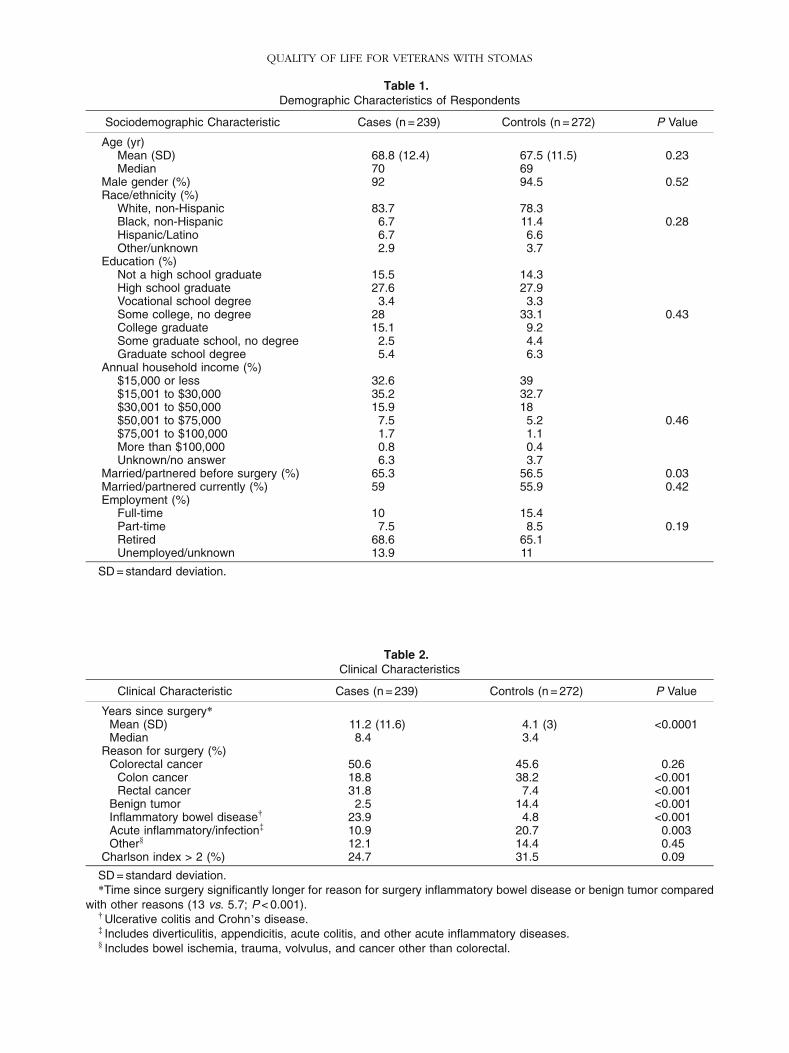
Table 1.Demographic Characteristics of Respondents
Sociodemographic Characteristic Cases (n = 239) Controls (n = 272) P Value
Age (yr)Mean (SD) 68.8 (12.4) 67.5 (11.5) 0.23Median 70 69
Male gender (%) 92 94.5 0.52Race/ethnicity (%)
White, non-Hispanic 83.7 78.3Black, non-Hispanic 6.7 11.4 0.28Hispanic/Latino 6.7 6.6Other/unknown 2.9 3.7
Education (%)Not a high school graduate 15.5 14.3High school graduate 27.6 27.9Vocational school degree 3.4 3.3Some college, no degree 28 33.1 0.43College graduate 15.1 9.2Some graduate school, no degree 2.5 4.4Graduate school degree 5.4 6.3
Annual household income (%)$15,000 or less 32.6 39$15,001 to $30,000 35.2 32.7$30,001 to $50,000 15.9 18$50,001 to $75,000 7.5 5.2 0.46$75,001 to $100,000 1.7 1.1More than $100,000 0.8 0.4Unknown/no answer 6.3 3.7
Married/partnered before surgery (%) 65.3 56.5 0.03Married/partnered currently (%) 59 55.9 0.42Employment (%)
Full-time 10 15.4Part-time 7.5 8.5 0.19Retired 68.6 65.1Unemployed/unknown 13.9 11
SD = standard deviation.
Table 2.Clinical Characteristics
Clinical Characteristic Cases (n = 239) Controls (n = 272) P Value
Years since surgery*Mean (SD) 11.2 (11.6) 4.1 (3) <0.0001Median 8.4 3.4
Reason for surgery (%)Colorectal cancer 50.6 45.6 0.26
Colon cancer 18.8 38.2 <0.001Rectal cancer 31.8 7.4 <0.001
Benign tumor 2.5 14.4 <0.001Inflammatory bowel disease. 23.9 4.8 <0.001Acute inflammatory/infection- 10.9 20.7 0.003Other` 12.1 14.4 0.45
Charlson index > 2 (%) 24.7 31.5 0.09
SD = standard deviation.*Time since surgery significantly longer for reason for surgery inflammatory bowel disease or benign tumor compared
with other reasons (13 vs. 5.7; P < 0.001).. Ulcerative colitis and Crohn_s disease.- Includes diverticulitis, appendicitis, acute colitis, and other acute inflammatory diseases.` Includes bowel ischemia, trauma, volvulus, and cancer other than colorectal.
QUALITY OF LIFE FOR VETERANS WITH STOMAS

infection, and Bother^) and Group B (inflammatory
bowel disease and benign tumor). Table 3 shows mean
differences between cases and controls in the domains
of the mCOH-QOL-Ostomy, separately by reason for
surgery and adjusted for age, time since surgery, and
Charlson comorbidity score. In Group A, all differences
suggest lower QOL for cases and reach statistical
significance for the social domain subscale, total QOL
scores, and in the psychologic subscale score for
colorectal cancer cases. By contrast, in Group B, most
differences suggest higher QOL for cases, but none
reach statistical significance.
When analysis was limited to Cases with CRC, we
found that mCOH-QOL-Ostomy domains subscale
and total QOL scores did not differ between Cases with
rectal and Cases with colon cancer, when adjusted for
age, time since surgery, and comorbidity score. For the
115 cases with CRC, the difference of a score of 10
favored rectal cancer by only 0.06 (P =0.85), and for
the 116 controls, the difference favored colon cancer
by only 0.09 (P = 0.83).
Adjusted mean scores for the domains of the
mCOH-QOL-Ostomy were compared between cases
and controls for Groups A and B separately (Table 4).
Statistically significant differences were found in
Group A for the total score, as well as the psychologic
and social domains. When comparing scores for
potentially meaningful differences regardless of statis-
Table 3.City of Hope Quality of Life-Ostomy Domain Score* Adjusted. Mean Difference Between Cases and Controls
for Male Veterans by Reason for Surgery
Group A Group B
City of Hope Quality ofLife-Ostomy Domain
Other-
(n = 60)Acute Inflammatory`
(n = 79)Colorectal Cancer
(n = 231)Benign Tumor
(n = 45)IBDË
(n = 65)
Total QOL 1.03{ 0.95{ 0.63{ j0.03 j0.39Physical 0.18 0.48 0.22 j0.72 j0.56Psychologic 0.94# 0.81 0.71{ 0.66 j0.54Social 1.93{ 1.91{ 1.10{ j0.12 j0.55Spiritual 0.93 0.34 0.41 j0.31 0.14
QOL = quality of life; IBD = inflammatory bowel disease.*Based on a response scale of 0 to 10, with higher scores reflecting more positive outcomes.. Difference adjusted for age, time since surgery, and comorbidity score (positive number indicates lower QOL for cases).- Includes bowel ischemia, trauma, volvulus, and cancer other than colorectal.` Includes diverticulitis, appendicitis, acute colitis, and other acute inflammatory diseases.Ë Ulcerative colitis and Crohn_s disease.{P < 0.05.# P = 0.055.
Table 4.City of Hope Quality of Life-Ostomy Domain Scores* for Male Veterans
Reason for Surgery Group A. Reason for Surgery Group B.
City of Hope Quality ofLife-Ostomy Domain
Cases(n = 176)
Controls(n = 218)
AdjustedMean Diff-
AdjustedP Value-
Cases(n = 63)
Controls(n = 52)
AdjustedMean Diff-
AdjustedP Value-
Total QOL 6.3 (2.0) 6.8 (1.8) 0.77 <0.001` 7.2 (1.9) 6.8 (1.8) j0.08 0.86Physical domain 6.6 (2.1) 6.6 (2.3) 0.23 0.33 7.2 (1.9) 6.7 (2.3) j0.42 0.39Psychologic domain 6.4 (2.1) 6.9 (1.9) 0.77 <0.001Ë 7.2 (2.0) 6.8 (1.9) j0.06 0.90Social domain 6.0 (2.6) 7.0 (2.6) 1.45{ <0.001Ë 7.0 (2.4) 6.9 (2.6) j0.32 0.58Spiritual domain 6.3 (2.3) 6.7 (2.3) 0.51 0.043 7.2 (2.4) 6.8 (2.3) j0.30 0.61
QOL = quality of life; diff = difference.Data are means with standard deviations in parentheses unless otherwise indicated.*Based on a response scale of 0 to 10, with higher scores reflecting more positive outcomes.. Group A includes colorectal cancer, acute inflammatory/infection, and other; Group B includes inflammatory bowel
disease and benign tumor.- Difference adjusted for age, time since surgery, and comorbidity score (positive number indicates lower QOL for cases).` Statistically significant (P < 0.05) with no Bonferroni adjustment.Ë Statistically significant after Bonferroni adjustment (adjusted alpha = 0.05/4 = 0.0125).{Exceeds Minimally Important Difference (empirical rule effect size).
KROUSE ET AL Dis Colon Rectum, 2007
tical significance, only the social domain exceeded the
estimated MID.
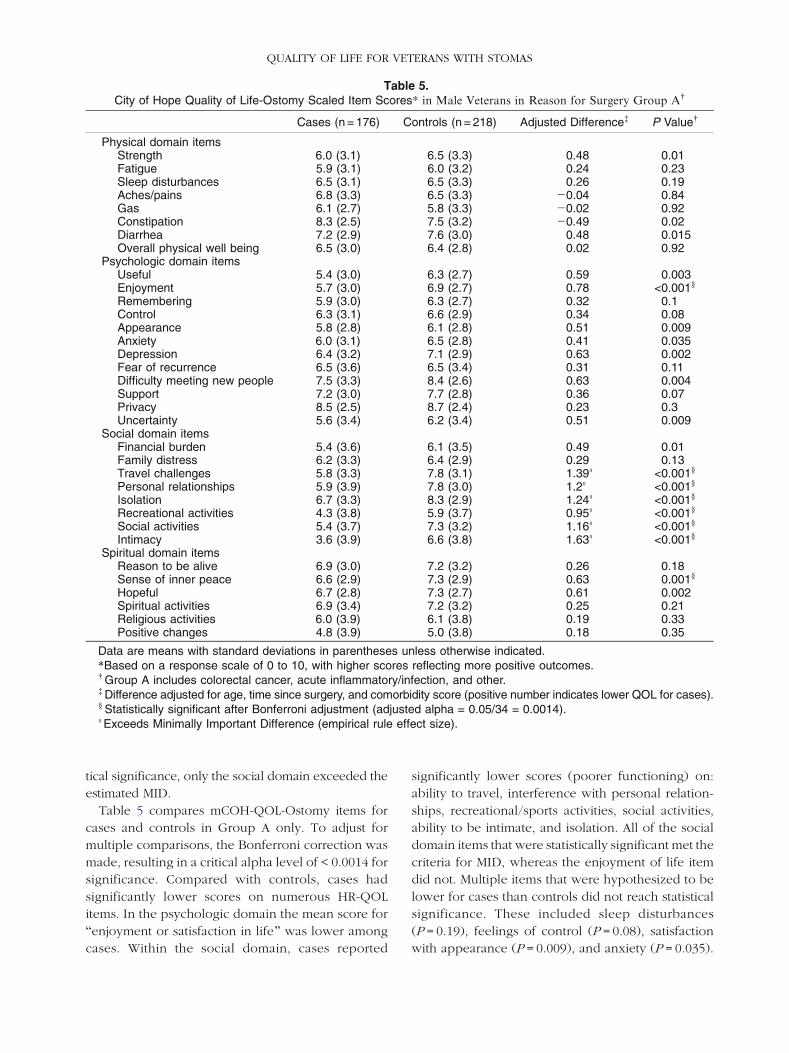
Table 5 compares mCOH-QOL-Ostomy items for
cases and controls in Group A only. To adjust for
multiple comparisons, the Bonferroni correction was
made, resulting in a critical alpha level of < 0.0014 for
significance. Compared with controls, cases had
significantly lower scores on numerous HR-QOL
items. In the psychologic domain the mean score for
Benjoyment or satisfaction in life^ was lower among
cases. Within the social domain, cases reported
significantly lower scores (poorer functioning) on:
ability to travel, interference with personal relation-
ships, recreational/sports activities, social activities,
ability to be intimate, and isolation. All of the social
domain items that were statistically significant met the
criteria for MID, whereas the enjoyment of life item
did not. Multiple items that were hypothesized to be
lower for cases than controls did not reach statistical
significance. These included sleep disturbances
(P = 0.19), feelings of control (P = 0.08), satisfaction
with appearance (P = 0.009), and anxiety (P = 0.035).
Table 5.City of Hope Quality of Life-Ostomy Scaled Item Scores* in Male Veterans in Reason for Surgery Group A.
Cases (n = 176) Controls (n = 218) Adjusted Difference- P Value.
Physical domain itemsStrength 6.0 (3.1) 6.5 (3.3) 0.48 0.01Fatigue 5.9 (3.1) 6.0 (3.2) 0.24 0.23Sleep disturbances 6.5 (3.1) 6.5 (3.3) 0.26 0.19Aches/pains 6.8 (3.3) 6.5 (3.3) j0.04 0.84Gas 6.1 (2.7) 5.8 (3.3) j0.02 0.92Constipation 8.3 (2.5) 7.5 (3.2) j0.49 0.02Diarrhea 7.2 (2.9) 7.6 (3.0) 0.48 0.015Overall physical well being 6.5 (3.0) 6.4 (2.8) 0.02 0.92
Psychologic domain itemsUseful 5.4 (3.0) 6.3 (2.7) 0.59 0.003Enjoyment 5.7 (3.0) 6.9 (2.7) 0.78 <0.001`
Remembering 5.9 (3.0) 6.3 (2.7) 0.32 0.1Control 6.3 (3.1) 6.6 (2.9) 0.34 0.08Appearance 5.8 (2.8) 6.1 (2.8) 0.51 0.009Anxiety 6.0 (3.1) 6.5 (2.8) 0.41 0.035Depression 6.4 (3.2) 7.1 (2.9) 0.63 0.002Fear of recurrence 6.5 (3.6) 6.5 (3.4) 0.31 0.11Difficulty meeting new people 7.5 (3.3) 8.4 (2.6) 0.63 0.004Support 7.2 (3.0) 7.7 (2.8) 0.36 0.07Privacy 8.5 (2.5) 8.7 (2.4) 0.23 0.3Uncertainty 5.6 (3.4) 6.2 (3.4) 0.51 0.009
Social domain itemsFinancial burden 5.4 (3.6) 6.1 (3.5) 0.49 0.01Family distress 6.2 (3.3) 6.4 (2.9) 0.29 0.13Travel challenges 5.8 (3.3) 7.8 (3.1) 1.39Ë <0.001`
Personal relationships 5.9 (3.9) 7.8 (3.0) 1.2Ë <0.001`
Isolation 6.7 (3.3) 8.3 (2.9) 1.24Ë <0.001`
Recreational activities 4.3 (3.8) 5.9 (3.7) 0.95Ë <0.001`
Social activities 5.4 (3.7) 7.3 (3.2) 1.16Ë <0.001`
Intimacy 3.6 (3.9) 6.6 (3.8) 1.63Ë <0.001`
Spiritual domain itemsReason to be alive 6.9 (3.0) 7.2 (3.2) 0.26 0.18Sense of inner peace 6.6 (2.9) 7.3 (2.9) 0.63 0.001`
Hopeful 6.7 (2.8) 7.3 (2.7) 0.61 0.002Spiritual activities 6.9 (3.4) 7.2 (3.2) 0.25 0.21Religious activities 6.0 (3.9) 6.1 (3.8) 0.19 0.33Positive changes 4.8 (3.9) 5.0 (3.8) 0.18 0.35
Data are means with standard deviations in parentheses unless otherwise indicated.*Based on a response scale of 0 to 10, with higher scores reflecting more positive outcomes.. Group A includes colorectal cancer, acute inflammatory/infection, and other.- Difference adjusted for age, time since surgery, and comorbidity score (positive number indicates lower QOL for cases).` Statistically significant after Bonferroni adjustment (adjusted alpha = 0.05/34 = 0.0014).Ë Exceeds Minimally Important Difference (empirical rule effect size).
QUALITY OF LIFE FOR VETERANS WITH STOMAS

Several items on the mCOH-QOL-Ostomy were
not included in the survey for controls because they
had no relevance. Although these items have no
control comparison, they do give further insight into
life with a stoma. These items addressed problems
with skin surrounding the ostomy (mean = 6.4),
leaking from the pouch (or around the appliance;
mean = 6.4), privacy when traveling for conducting
ostomy care (mean = 6.4), difficulty adjusting to the
ostomy (mean = 6), embarrassment from ostomy
(mean = 6.2), difficulty looking at the ostomy
(mean = 8.3), and difficulty in caring for the ostomy
(mean = 7.5).
Nonscaled items showed few differences between
cases and controls with two important exceptions.
Compared with controls, higher proportions of
ostomates reported having felt depressed (52 vs. 36
percent; P < 0.01) and having had suicidal ideation
(12 vs. 5 percent; P < 0.01) after their operations.
There were no significant differences between
Groups A and B in these contrasts.
Comparisons of cases and controls revealed mul-
tiple differences on the SF-36V scales among Group
A patients (Table 6). Significant differences between
cases and controls were observed on mean scores on
seven of the eight scales and the PCS and MCS.
Differences between the groups exceeded the MID
for the seven significant scales.
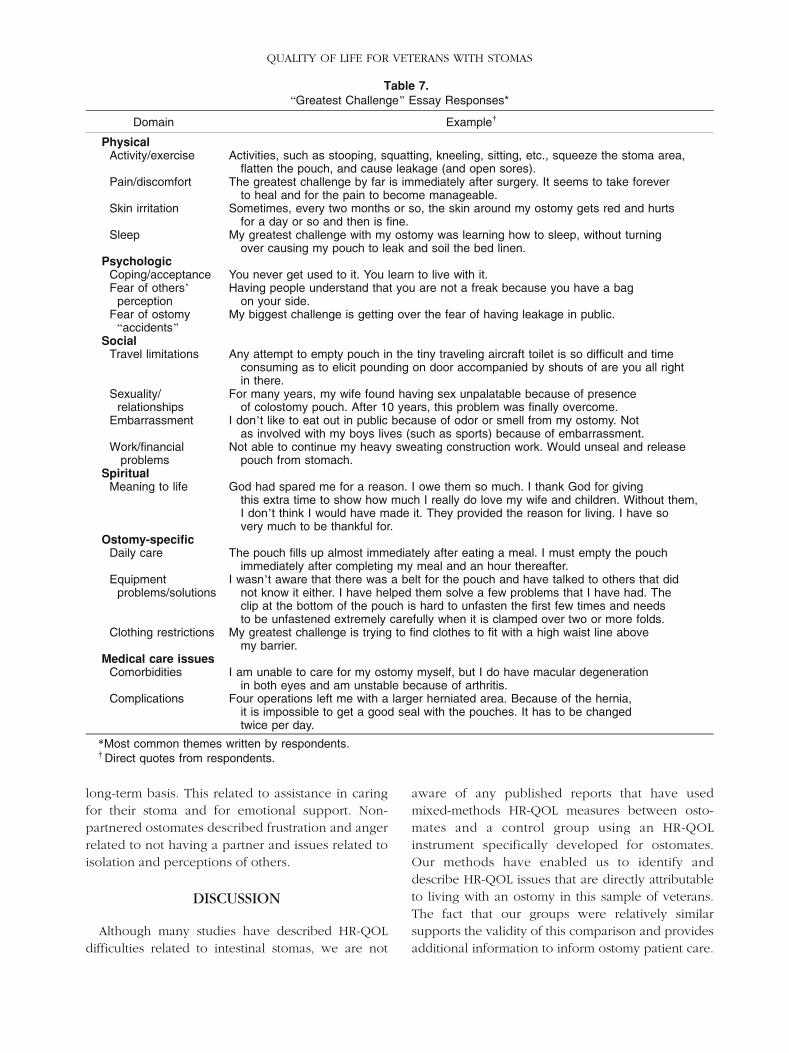
Sixty-eight percent of ostomates took the oppor-
tunity to expand on the final qualitative statement
asking to share Bthe greatest challenge you have
encountered in having an ostomy.^ Themes were
coded by using the four domains of the mCOH-QOL-
Ostomy model of HR-QOL. Two additional themes
emerged that were separated into new Bdomains^:1) ostomy-specific issues, and 2) medical care issues.
Respondents identified problems related to sexuality
and intimacy, travel, clothing, equipment, and other
common issues that they faced. Comments and
themes that represent the most frequent challenges
faced by these males are presented in Table 7.
Common issues included coping and acceptance of
their stoma, comorbidities, travel limitations, sexual
issues, embarrassment, and daily care. Challenges
were frequently ostomy-specific rather than direct
comparisons to the control group in the quantitative
data. In addition, some issues, such as sleep chal-
lenges, pain, and financial difficulties, that were not
significant in the quantitative comparison data were
still important challenges for ostomates. Importantly,
many ostomates described relying on their partners
during the immediate postoperative period or for a
Table 6.Short Form 36 for Veterans_ Scale Scores* for Male Veterans
Reason for Surgery Group A. Reason for Surgery Group B.
SF-36V ScalesCases
(n = 176)Controls(n = 218)
AdjustedMean Diff-
AdjustedP Value-
Cases(n = 63)
Controls(n = 52)
AdjustedMean Diff-
AdjustedP Value-
Physical function 43.2 (29.4) 54.4 (30.8) 11.6` <0.001Ë 63.1 (29.9) 54.7 (33.8) 0.99 0.89General health 48.4 (25.1) 56.9 (24.1) 10.0` <0.001Ë 57.0 (25.8) 46.9 (24.9) j4.0 0.51Vitality 38.5 (23.8) 45.2 (25.2) 8.0` 0.003Ë 51.4 (29.2) 43.8 (26.7) j3.2 0.65Mental health 63.6 (23.5) 71.7 (22.9) 9.7` <0.001Ë 76.4 (21.9) 68.8 (23.2) j1.6 0.78Role-Physical 47.5 (30.7) 58.0 (30.4) 12.1` <0.001Ë 62.7 (31.8) 57.9 (34.1) 1.4 0.86Role-Emotional 57.4 (30.7) 69.5 (29.8) 13.8` <0.001Ë 74.7 (28.5) 67.8 (30.1) 1.3 0.85Social function 60.4 (31.3) 72.7 (29.7) 13.3` <0.001Ë 73.0 (30.4) 68.6 (27.8) 0.96 0.89Bodily pain 44.7 (29.2) 47.8 (27.6) 2.7 0.40 52.7 (29.2) 43.6 (29.1) j3.8 0.60PCS 34.2 (10.6) 37.3 (10.4) 3.3 0.006{ 39.1 (10.6) 35.7 (11.6) 0.03 0.99MCS 45.4 (12.0) 50.4 (10.9) 5.8 <0.001{ 51.2 (11.0) 47.3 (11.6) j0.76 0.80
diff = difference; PCS = Physical Component Summary score; MCS = Mental Component Summary score.Data are means with standard deviations in parentheses unless otherwise indicated.*Scale and summary scores can range from 0 to 100, with higher scores reflecting better functioning and/or well-
being. Unlike the individual SF-36V scale scores, the PCS and MCS scores are standardized to reflect a mean of 50 anda standard deviation of 10 in the general adult U.S. population.
. Group A includes colorectal cancer, acute inflammatory/infection, and other; Group B includes inflammatory boweldisease and benign tumor.
- Difference adjusted for age, time since surgery, and comorbidity score (positive number indicates lower QOL for cases)` Exceeds Minimally Important Difference (empirical rule effect size).Ë Statistically significant after Bonferroni adjustment (adjusted alpha = 0.05/8 = 0.00625).{Statistically significant (P < 0.05) with no Bonferroni adjustment.
KROUSE ET AL Dis Colon Rectum, 2007
long-term basis. This related to assistance in caring
for their stoma and for emotional support. Non-
partnered ostomates described frustration and anger
related to not having a partner and issues related to
isolation and perceptions of others.
DISCUSSION
Although many studies have described HR-QOL
difficulties related to intestinal stomas, we are not
aware of any published reports that have used
mixed-methods HR-QOL measures between osto-
mates and a control group using an HR-QOL
instrument specifically developed for ostomates.
Our methods have enabled us to identify and
describe HR-QOL issues that are directly attributable
to living with an ostomy in this sample of veterans.
The fact that our groups were relatively similar
supports the validity of this comparison and provides
additional information to inform ostomy patient care.
Table 7.BGreatest Challenge^ Essay Responses*
Domain Example.
PhysicalActivity/exercise Activities, such as stooping, squatting, kneeling, sitting, etc., squeeze the stoma area,
flatten the pouch, and cause leakage (and open sores).Pain/discomfort The greatest challenge by far is immediately after surgery. It seems to take forever
to heal and for the pain to become manageable.Skin irritation Sometimes, every two months or so, the skin around my ostomy gets red and hurts
for a day or so and then is fine.Sleep My greatest challenge with my ostomy was learning how to sleep, without turning
over causing my pouch to leak and soil the bed linen.Psychologic
Coping/acceptance You never get used to it. You learn to live with it.Fear of others_
perceptionHaving people understand that you are not a freak because you have a bag
on your side.Fear of ostomyBaccidents^
My biggest challenge is getting over the fear of having leakage in public.
SocialTravel limitations Any attempt to empty pouch in the tiny traveling aircraft toilet is so difficult and time
consuming as to elicit pounding on door accompanied by shouts of are you all rightin there.
Sexuality/relationships
For many years, my wife found having sex unpalatable because of presenceof colostomy pouch. After 10 years, this problem was finally overcome.
Embarrassment I don_t like to eat out in public because of odor or smell from my ostomy. Notas involved with my boys lives (such as sports) because of embarrassment.
Work/financialproblems
Not able to continue my heavy sweating construction work. Would unseal and releasepouch from stomach.
SpiritualMeaning to life God had spared me for a reason. I owe them so much. I thank God for giving
this extra time to show how much I really do love my wife and children. Without them,I don_t think I would have made it. They provided the reason for living. I have sovery much to be thankful for.
Ostomy-specificDaily care The pouch fills up almost immediately after eating a meal. I must empty the pouch
immediately after completing my meal and an hour thereafter.Equipment
problems/solutionsI wasn_t aware that there was a belt for the pouch and have talked to others that did
not know it either. I have helped them solve a few problems that I have had. Theclip at the bottom of the pouch is hard to unfasten the first few times and needsto be unfastened extremely carefully when it is clamped over two or more folds.
Clothing restrictions My greatest challenge is trying to find clothes to fit with a high waist line abovemy barrier.
Medical care issuesComorbidities I am unable to care for my ostomy myself, but I do have macular degeneration
in both eyes and am unstable because of arthritis.Complications Four operations left me with a larger herniated area. Because of the hernia,
it is impossible to get a good seal with the pouches. It has to be changedtwice per day.
*Most common themes written by respondents.. Direct quotes from respondents.
QUALITY OF LIFE FOR VETERANS WITH STOMAS

The major clinical differences that could have HR-QOL
implications (age, time since surgery, and comorbidity)
were controlled in our model, and we stratified by
reason for surgery. Sample size precluded examining
the data from females in our cohort to definitively
examine HR-QOL issues. This population will be
described separately in a future report. To account for
etiology differences, we stratified by reason for surgery,
and then combined categories with similar findings.
Although it must be recognized that there may be other
clinical differences in our ostomate and control groups,
they are all males of similar age and comorbidity profile
who have equivalent access and availability to VA
health care. Our results are generalizable for the VA
male population. Extrapolation into the general popu-
lation, especially females, can only be performed with
caution. Finally, our mixed methods allowed us to
cross-validate quantitative findings by using qualitative
data, which further specified ostomate challenges.
Qualitative and quantitative findings from this
study underscore the impact of having an intestinal
stoma, particularly in the social domain. Although
individual item analyses were conducted in an
exploratory manner, both statistically and clinically
meaningful findings were evident. Thus, specific
items that can be explored for differences include
those related to general QOL, such as fatigue, aches
and pains, or anxiety, or those more related directly
to an ostomy, such as recreational activities, travel
challenges, or dissatisfaction with appearance.30
We found a demarcation in QOL outcomes
between two subgroups of cause for stoma. There
has been some indication that ostomates with cancer
had better HR-QOL for most issues compared with
ostomates without cancer,24 but our data do not
confirm this for comparison of cancer to inflamma-
tory bowel or benign tumor as cause of stoma.
Because our study is controlled, has better access to
patient records, and recruited through primary care
providers, we believe that the present results are
likely to be more accurate. Cases with ulcerative
inflammatory bowel disease or benign tumors had
more positive HR-QOL scores than other cases; this
may be caused by greater symptom relief or cure
after surgery. Cancer Cases often have other treat-
ments that can impact HR-QOL, and those needing
emergency procedures may not look at their stomas
as Bcurative^ and remain dissatisfied that they must
endure this complication of their acute disease. Cases
with inflammatory bowel disease and benign tumors
had longer time since surgery compared with other
patients; this factor may contribute to lack of observed
impact of a stoma in these etiologic subgroups,
although we adjusted for time since surgery, but should
not bias the results that we report for Group A.
It has been reported that approximately one-
quarter of stoma Cases experience significant clinical
psychologic symptoms.36 Our quantitative analyses
provide further evidence of the overall lower emo-
tional well being of ostomates. One of the most
important findings of this study was increased self-
reported postoperative depression and suicidal ide-
ation for ostomates. We also found a trend of worse
current feelings of depression (scaled item) among
cases. Whereas others have shown depression in this
population,10,37 our findings are novel in describing
postoperative effects, including risk of suicide, which
must be addressed in the perioperative setting.
The psychologic issues of coping and acceptance
were the most frequent challenges encountered in
our qualitative analysis. Although anxiety scores
were not significantly different for ostomates com-
pared with controls, Cases with stomas frequently
described fears related to others_ perceptions of them
and fear of Baccidents^ related to their stoma.
Overcoming these fears may be difficult and lead to
greater isolation and social debilitation. These results
further suggest that early professional psychologic
evaluation for Cases who undergo intestinal stomas
is warranted. This may be especially important for
those with preoperative or perioperative psychiatric
history,36 or those who have displayed negative
reactions toward their stoma.36
The major HR-QOL differences between ostomates
and controls were related to social functioning. The
social implications of an ostomy were reported more
than 50 years ago in some detail,2,38,39 and more
recent reports also have described these deficien-
ces.10,18,19,21,23,24,37,40–44 Our study provides further
detail regarding the specific social consequences of
having an ostomy and reports results that reflect
meaningful decrements in aspects of social well-being
that should be the focus of targeted interventions.
Although it is clear that counseling and supportive
interventions could focus on these potential concerns,
improvement in some of these areas may be difficult.
Although some problems may not be easily amenable
to change (e.g., intimacy), social isolation and travel
techniques can be enhanced. If these issues are
addressed, intimacy also may improve, even if not in
a sexual sense. In fact, some Bgreatest challenges^statements, especially from nonpartnered respondents,
KROUSE ET AL Dis Colon Rectum, 2007

focused on isolation and travel concerns that keep
them from being more socially active. In addition, it is
important to consider the potential interrelationship of
the domains of HR-QOL. For example, if the ostomy
keeps Cases from participating in church, this may
impair both spiritual and social functioning. Therefore,
helping Cases who have or are likely to have social
difficulties related to their stoma could have great
impact on other domains, and importantly a patient_s
overall HR-QOL. Partnered status was not an indepen-
dent predictor of HR-QOL for ostomates. However, our
data showed that both cases and controls who were
partnered had higher HR-QOL scores (data not
shown). Qualitative data included descriptions of
ostomates_ reliance on partners for care or emotional
support and assistance in caring for their ostomy,
especially in the immediate postoperative period. This
must be considered when an ostomy is created to plan
for the training of partners and for the additional
support required by those who are not partnered or do
not have an adequate support system.
No difference was noted in the physical well-being
domain of the mCOH-QOL-Ostomy between cases
and controls, with little difference in individual items.
Others have shown more of a gas problem for
ostomates, which was not evident in our population,
but we did see less constipation for ostomates which
was in agreement with others.19 Interestingly, we did
see a difference in physical functioning and role
limitations on the SF-36V (Table 6). This is in contrast
to findings using the SF-36 in Japan when comparing
the physical functioning of ostomates vs. Japanese
norms (P = 0.37); however, they did note a difference
in role limitations (P < 0.001).45 Their study utilized
the general population as a comparison, which may
be the reason why there is no difference in physical
functioning, but the stoma may lead to role limi-
tations as a result of the stoma and its care.
Care of a stoma for older adults or persons with
multiple medical problems, such as arthritis, poor
vision, or obesity, may be even more difficult.
Challenges related to comorbidities and surgical
complications were clearly illustrated in the open-
ended essay question, with cases focusing on the
individual medical problem that added to the total
health burden of care, as well as all of the daily self-
management problems that they needed to master.
In examining ostomy-specific content, cases
reported relatively low scores on items, such as the
skin surrounding the ostomy, leaking from the pouch
(or around the appliance), privacy when traveling for
conducting ostomy care, difficulty adjusting to the
ostomy, and embarrassment from ostomy. It must be
remembered that these low scores occur in a
population averaging 11 years postoperatively; these
are obviously persistent problems that ostomates
have not been able to resolve. Practical care issues
that are clearly outlined by Cases must be addressed
early after surgery to ensure that they are facile with
supplies, have the correct equipment for them, and
know where to seek alternatives and help when
necessary. Long-term support and follow-up related
to these issues are clearly needed.
Our data show HR-QOL issues that should be a focus
for clinicians who care for Cases with intestinal stomas.
This may involve early psychologic evaluation and
subsequent follow-up to ensure emotional stability and
coping after surgery. Integrating significant others to
participate in care may lead to improved adjustment
and even save marriages and/or partnered status.
Encouraging social networking and participation in
recreational events is likely to have positive effects.
Networking with other ostomates also would be help-
ful to many Cases to clarify many issues, and limit the
lengthy trial and error approach that most Cases
experience. Finally, a clear educational strategy will
facilitate coping and adjustment to one_s stoma and
lead to improvement of multiple HR-QOL issues. Our
qualitative data have helped focus these strategies, such as
related to the importance of the timing of eating, clothing
restrictions, or specific travel restrictions. Our team is
working toward an integrative approach in a prospective
study setting to understand interventions that will best
help Cases with intestinal stomas.
REFERENCES
1. United Ostomy Associations of America, Phoenix Ostomy
Chapter. Available at: http://www.phoenixostomychapter.
org/info.html. Accessed May 8, 2006.
2. Sutherland AM, Orbach CE, Dyk RB, Bard M. The
psychological impact of cancer and cancer surgery.
Cancer 1952;5:857–72.
3. Decosse JJ. Quality of life. J Surg Oncol 1997;65:231.
4. Walker CS. Quality of life: assessment and application.
London: MTP Press, 1987.
5. Osoba D. Lessons learned from measuring health-related
quality of life in oncology. J Clin Oncol 1994;12:609–16.
6. Grant MM, Padilla GV, Ferrell BR, Rhiner M. Assess-
ment of quality of life with a single instrument. Semin
Oncol Nurs 1990;6:260–70.
7. Spilker B. Introduction. In: Spilker B, ed. Quality of life
and pharmacoeconomics in clinical trials. 2nd ed.
Philadelphia: Lippincott–Raven, 1996:1–10.
QUALITY OF LIFE FOR VETERANS WITH STOMAS

8. Grant M. Quality of life issues in colorectal cancer.
Develop Support Care 1999;3:4–9.
9. Grant M, Ferrell B, Rivera L, Dean G, Chu D, Krouse
RS. Quality of life for cancer Cases with ostomies. Qual
Life Res 1998;7:599–600.
10. Nugent KP, Daniels P, Stewart B, Patankar R, Johnson
CD. Quality of life in stoma Cases. Dis Colon Rectum
1999;42:1569–74.
11. Jenks JM, Morin KH, Tomaselli N. The influence of
ostomy surgery on body image in Cases with cancer.
Appl Nurs Res 1997;10:174–80.
12. Klopp AL. Body image and self-concept among indi-
viduals with stomas. J Enterostom Ther 1990;17:98–105.
13. Hojo K, Vernava AM III, Sugihara K, Katumata K.
Preservation of urine voiding and sexual function after
rectal cancer surgery. Dis Colon Rectum 1991;34:532–9.
14. Grunberg KJ. Sexual rehabilitation of the cancer patient
undergoing ostomy surgery. J Enterostom Ther
1986;13:148–52.
15. Ofman US, Auchincloss SS. Sexual dysfunction in
cancer Cases. Curr Opin Oncol 1992;4:605–13.
16. Fazio VW, Fletcher J, Montague D. Prospective study of
the effect of resection of the rectum on male sexual
function. World J Surg 1980;4:149–51.
17. Yeager ES, van Heerden JA. Sexual dysfunction follow-
ing proctocolectomy and abdominoperineal resection.
Ann Surg 1980;191:169–70.
18. Borweil B. The psychosexual needs of stoma Cases.
Prof Nurse 1997;12:250–5.
19. Sprangers MA, Taal BG, Aaronson NK, te Velde A.
Quality of life in colorectal cancer: stoma vs. nonstoma
Cases. Dis Colon Rectum 1995;38:361–9.
20. Thomas C. Madden F, Jehu D. Psychological effects of
stomas. I. Psychosocial morbidity one year after
surgery. J Psychosom Res 1987;31:311–6.
21. Hurny C, Holland JC. Psychosocial sequelae of osto-
mies in cancer Cases. Cancer 1985;36:170–83.
22. Keyes K, Bisno B, Richardson J, Marston A. Age
differences in coping, behavioral dysfunction and
depression following colostomy surgery. Gerontologist
1987;27:182–4.
23. Wirsching M, Druner HU, Herrmann G. Results of psycho-
social adjustment to long-term colostomy. Psychother
Psychosom 1975;26:245–56.
24. Krouse RS, Grant M, Ferrell B, Dean G, Nelson R, Chu
DZ. Quality of life outcomes in 599 cancer and
noncancer Cases with colostomies. J Surg Res
2007;138:79–87.
25. Krouse RS, Mohler MJ, Wendel C, et al. The VA Ostomy
Health-Related Quality of Life Study: objectives, methods,
and patient sample. Curr Med Res Opin 2006;22:781–91.
26. City of Hope/Beckman Research Institute Pain Re-
source Center Research Instruments. Available at:
http://www.cityofhope.org/prc/pdf/Quality%20o-
f%20Life%20Ostomy.pdf. Accessed July 20, 2006.
27. Kazis LE, Miller DR, Clark J, et al. Health-related quality
of life in Cases served by the Department of Veterans
Affairs: results from the Veterans Health Study. Arch
Intern Med 1998;158:626–32.
28. Kazis LE, Ren XS, Lee A, et al. Health status in VA
Cases: results from the Veterans Health Study. Am J
Med Qual 1999;14:28–38.
29. Ware JE Jr, Sherbourne CD. The MOS 36-item short-
form health survey (SF-36): II. Psychometric and
clinical tests of validity in measuring physical and
mental health constructions. Med Care 1992;31:247–63.
30. Grant M, Ferrell B, Dean G, Uman G, Chu D, Krouse R.
Revision and psychometric testing of the City of Hope
Quality of Life-Ostomy questionnaire. Qual Life Res
2004;13:1445–57.
31. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical
comorbidity index for use with ICD-9- CM administra-
tive databases. J Clin Epidemiol 1992;45:613–9.
32. Sloan J, Symonds T, Vargas-Chanes D, Fridley B.
Practical guidelines for assessing the clinical signifi-
cance of health-related quality of life changes within
clinical trials. Drug Information J 2003;37:23–31.
33. Krippendorff K. Content analysis. Beverly Hills: Sage,
1980.
34. Miles MB, Huberman AM. Qualitative data analysis.
Thousand Oaks: Sage, 1994.
35. Morse JM, Field PA. Qualitative research methods for
health professionals. Thousand Oaks: Sage, 1995.
36. White CA, Hunt JC. Psychological factors in postoper-
ative adjustment to stoma surgery. Ann R Coll Surg Engl
1997;79:3–7.
37. Thomas C, Madden F, Jehu D. Psychosocial morbidity
in the first three months following stoma surgery. J
Psychosomatic Res 1984;28:251–7.
38. Ewing MR. Colostomy: the patient_s point of view.
Postgrad Med J 1950;26:584–9.
39. Dukes CE. Management of a permanent colostomy:
study of 100 Cases at home. Lancet 1947;2:12–4.
40. Krouse RS, Grube B, Grant M, et al. Ostomy-related
sexual dysfunction: an important quality of life issue
[abstract]. Proc-Am Soc Clin Oncol 1999;18:599a.
KROUSE ET AL Dis Colon Rectum, 2007

41. Karada? A, Mentes BB, Ayaz S. Colostomy irrigation:
results of 25 cases with particular reference to quality
of life. J Clin Nurs 2005;14:479–85.
42. Sideris L, Zenasni F, Vernerey D, et al. Quality of life of
Cases operated on for low rectal cancer: impact of the
type of surgery and Cases_ characteristics. Dis Colon
Rectum 2005;48:2180–91.
43. McKenzie F, White CA, Kendall S, Finlayson A,
Urquhart M, Williams I. Psychological impact of
colostomy pouch change and disposal. Br J Nurs
2006;15:308–16.
44. Kuchenhoff J, Wirsching M, Druner HU, Herrmann G,
Kohler C. Coping with a stoma: a comparative study of
Cases with rectal carcinoma or inflammatory bowel
diseases. Psychother Psychosom 1981;36:98–104.
45. Ito N, Tanaka M, Kazuma K. Health-related quality of life
among persons living in Japan with a permanent colosto-
my. J Wound Ostomy Continence Nurs 2005;32:178–83.
QUALITY OF LIFE FOR VETERANS WITH STOMAS
Related Documents

![İNTESTİNAL OBSTRÜKSİYONLAR.ppt [Uyumluluk Modu]€¦ · Barsak ObstrüksiyonuTanımlama İntestinal obstrüksiyon, intestinal içeriğin gastrointestinal sistem içinde distale](https://static.cupdf.com/doc/110x72/5f603f10302e4166bd691bd7/ntestnal-obstroeks-uyumluluk-modu-barsak-obstrksiyonutanmlama-ntestinal.jpg)