Reprinted from CLINICAL PHARMACOLOGY AND THERAPEUTICS. St. Louis Vol. 30. No. 2, Pages 239-245, August. 1981 (Printed in the U. S. A.) (Copyright 0 1981 by The C. V. Mosby Company) A method for estimating the probability of adverse drug reactions Plrc, o.~ri~rrtrriorr 111. rlrc, ~,rohtrhilin. rlrtrr tr tlr.rr,q c.crrr.sc~tl trrr trth.c,rsc, 1 lirtic~trl c,~.orrr i.v rt.srroll\ h(r.cc~tl orr c.lirric~rr1 /rtc,qrrrc,rrr. L~rc k of tr rrrc~rl~otlfi~r t~>rtrhli.slrirr,q I crct.\trlir\ ,qc2rrortrrc~.s Itrr.gc, /~c~r~~~c~c~r~-~~crr(~r.s crrrrl ~~irlrirr-~.(rrc,r.s ~~trritrl~iliry irr trs.\r~.\.~rtcorrr. Lr.\irr,qrhc, (.r~ri\~t~r~~ior~crI c.rtrc,,qor.ic..s trrrtl rlt:/irririorr.s of rlt,f~~rir(,. /)rohrr/J/~. ~)o.s.\ihlr, trrrtl ~/orrl)t/irl trtl\.or.\r, clr.rrg r.c~trc~riorr.s (A DR.\). rlrc, hcrn~oc~rr-r.trrt~r.c cr,qr~c~c~t~rc~rrr II~III,II ~~lr\.sic~itr~r.s trrrtl/i)irr ~,I~trr.~r~trc~i.srs \~.lro iricl(~/)c.rrtlc~rrr!\. trssc,.s.\otl 63 r.trrrtlorrr1~~ .\ol(,c.rt,tl trl/(,gc,tl A1)R.v \~.tr.s 38% ro 63%. ktrpl~tr ( K, tr c~l~tr~rc~t~-(~orrc~r~r(~(l irrt10.v I!( tr,qr.t,c,r~~c,~rt) ~~trr~/c~tl,/i.orrr 0.2 I 11) 0.40. trrrtl rlrr, irrrr.trc~ltrs.s ~~~~rroltrriorr c.oc;ffific.ic,rrr I!( r.clitrhiliry (R[osr]) wtrs 0.49. Si.v (~r~.\rirrg) trrr(1 -72 11.k (rt,rcsrirrg) Itrrc,r rlrc, .\trriit~ ohsrjr-~.c,r.s irrtlt~pc~rrrlt~rrr!\. rc~trrrtr1~:t~tl rlic~ 6 3 r.rr.\r,.\ /I! tr\.\i,qrrirr,q tr 11.t~ig11rotl .sc.orcJ(.-1DR ~ ~ r o l ~ r r l ) i l i r \ >c,(rlt,) ro c~trc.lr I!/ rlrt, c~orrrporrorrrs rlrtrr rrrrr.\r /I(, r~or~.si(I(~r~r~rl 111 o.s~(/l~li,slri~~,q (~trr(.s(rI cr.s,~o(.itr~io~~> I~c,r~~~t,t,ri t/r.rr,q/> 1 trrr(1 (r(I\~c,r,cc, 01~1~11r.s ((,.~q., rc,~~~l~~r(/l srPclrr('rr~.c,j. 7'/i(, c.tr.sc,s ~~,c.rc, rzrrrtloriii:orl 111 ririrrirrri:r rho ir!j/rrorrc~c~ (!f'I(~r~rrrirr~. Tlir cJ~~c,rtr 11 c1.s tr.s.si,qrrr,cl tr ~~r.ohtrl>iliry c,trrc,,qoy fiorrr I//(,tortrl sc~~rc,. 7'110 I~c~r~t~c~c~rr-rtrr~~r~s rcl/itrhi/ih (,rrrr$c': ~X,I'~.('III ~,qr(~c~~irr~~ir = X.Zc'4 ro 92'%; K = 0.69 10 0.86: r = 0.91 10 0.05; R(c..sl) = 0.92) crtrtl ~~.irlrirr-t~trrt~r-.v r.c~Iio/~ili~\ (rrrrrgo: I,r8rc.c,rrr tr~rt,c,r~rc,rrr = SOr/r ro 97'2: K = 0.64 lo 0.9-5; r = 0.91 ro 0.981 irtrpro\~c,tl (1) < O.oi)IJ. 7'111, h(,r\~.c,c,rr-~.trrc.rs rolirr1)ili~. \\.ti> rrrtrirrrtrirrc~tl orr rc,rc~.srirr,q (rtrrrgc8: r = 0.84 ro 0.94: R((,.\rj = 0.871. Tlrc~ hcri~~c~t~rr-t~trr(~r.~ rc,litrhilir~ (?/' rIrrc,o trrrc,rrclitrg ~)li\~.vic~itrri.s 11'1ro itrtlol~t~rrtlt~rrrl~ tr.\sc,.s.\c,cl 28 orlrc,r ~)ro.sl,c,c.ri~.c,!\. (.ollt,t.rc.tl c,tr.sc,s (I( trllo,qc.d .4DRs 11.tr.s \.or\. lriglr (rcrrrgc,: r = 0.76 ro 0.87; R(t,.sr) = O.XO). 11 \\.tr.v ctlso .slro~\~rr rlrtcr rlrr ADR ~>rolxrhilih .sc,trlc 11tr.s c~~rrsc~rr.\rrtrl. c~orrrc~~rr, curt1 ~.~~rrc.rrrr-orrr ~.trli~lih. T1ri.s s\~.\rc,rrrtrric rrrc,rl~otl(
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Reprinted from C L I N I C A L PHARMACOLOGY A N D T H E R A P E U T I C S . S t . Louis Vo l . 30. No. 2 , Pages 239-245, August . 1981 (Printed in the U . S . A . ) (Copyright 0 1981 by The C . V . Mosby Company)
A method for estimating the probability of adverse
drug reactions
Plrc, o.~ri~rrtrriorr 111. rlrc, ~,rohtrhi l in. rlrtrr tr tlr.rr,q c.crrr.sc~tl t r r r trth.c,rsc, 1 lirtic~trl c,~.orrr i.v rt.srroll\ h(r.cc~tl
orr c.lirric~rr1 /rtc,qrrrc,rrr. L~rc k of tr r r rc~r l~o t l f i~ r t~>rtrhli.slrirr,q I crct.\trlir\ ,qc2rrortrrc~.s Itrr.gc, / ~ c ~ r ~ ~ ~ c ~ c ~ r ~ - ~ ~ c r r ( ~ r . s
crrrrl ~~irlrirr-~.(rrc,r.s ~~t r r i t r l~ i l i r y irr trs.\r~.\.~rtcorrr. Lr.\irr,q rhc, ( . r ~ r i \ ~ t~ r~~ io r~c r I c.rtrc,,qor.ic..s trrrtl rlt:/irririorr.s of
r l t , f~~rir(,. / ) r oh r r / J /~ . ~)o.s.\ihlr, trrrtl ~/orrl)t/irl trtl\.or.\r, clr.rrg r.c~trc~riorr.s (A DR.\). rlrc, hcrn~oc~rr-r.trrt~r.c
cr,qr~c~c~t~rc~rrr I I ~ I I I , I I ~~lr\.sic~itr~r.s trrrt l / i) irr ~,I~trr.~r~trc~i.srs \~. l ro iricl(~/)c.rrtlc~rrr!\. trssc,.s.\otl 63 r.trrrtlorrr1~~
.\ol(,c.rt,tl trl/(,gc,tl A1)R.v \~ . t r . s 38% ro 63%. ktrpl~tr ( K , tr c ~ l ~ t r ~ r c ~ t ~ - ( ~ o r r c ~ r ~ r ( ~ ( l irrt10.v I!( tr,qr.t,c,r~~c,~rt)
~~trr~/c~tl,/ i .orrr 0 .2 I 11) 0 .40. trrrtl rlrr, irrrr.trc~ltrs.s ~~~~ r ro l t r r i o r r c.oc;ffific.ic,rrr I!( r.clitrhiliry (R[osr]) wtrs
0 .49 . Si.v (~r~.\r irrg) trrr(1 -72 11.k (rt,rcsrirrg) Itrrc,r rlrc, .\trriit~ ohsrjr-~.c,r.s irrtlt~pc~rrrlt~rrr!\. rc~trrrtr1~:t~tl rlic~
63 r.rr.\r,.\ /I! tr\.\i,qrrirr,q t r 11.t~ig11rotl .sc.orcJ (.-1DR ~ ~ r o l ~ r r l ) i l i r \ >c,(rlt,) ro c~trc.lr I!/ rlrt, c~orrrporrorrrs rlrtrr
rrrrr.\r / I(, r~or~.s i ( I (~r~r~r l 111 o.s~(/l~l i ,slr i~~,q (~trr(.s(rI cr.s,~o(.i tr~io~~> I~c,r~~~t,t,r i t/r.rr,q/> 1 trrr(1 (r(I\~c,r,cc, 01~1~11r.s ( ( , .~q . ,
r c , ~ ~ ~ l ~ ~ r ( / l srPclrr('rr~.c,j. 7'/i(, c.tr.sc,s ~~,c.rc, rzrrrtloriii:orl 111 ririrrirrri:r rho ir!j/rrorrc~c~ ( ! f ' I ( ~ r ~ r r r i r r ~ . T l i r cJ~~c,rtr
1 1 c1.s tr.s.si,qrrr,cl tr ~~r.ohtrl>i l iry c,trrc,,qoy fiorrr I / / ( , tortrl sc~~rc, . 7'110 I ~c~r~ t~c~c~r r - r t r r~~r~s rc l / i t rh i / ih (,rrrr$c':
~X, I '~ . ( ' I I I ~ , q r ( ~ c ~ ~ i r r ~ ~ i r = X.Zc'4 ro 92'%; K = 0.69 10 0 .86 : r = 0.91 10 0.05; R(c..sl) = 0.92) crtrtl
~~.irlrirr-t~trrt~r-.v r .c~ I io /~ i l i~ \ (rrrrrgo: I,r8rc.c,rrr tr~rt,c,r~rc,rrr = SOr/r ro 97'2: K = 0.64 l o 0.9-5; r = 0.91
ro 0.981 irtrpro\~c,tl (1) < O.oi)IJ. 7'111, h(,r\~.c,c,rr-~.trrc.rs ro l i r r1) i l i~. \\.ti> rrrtrirrrtrirrc~tl orr rc,rc~.srirr,q
(rtrrrgc8: r = 0.84 ro 0.94: R((,.\rj = 0.871. Tlrc~ hcr i~~c~t~r r - t~ t r r (~r .~ rc,litrhilir~ ( ? / ' rIrrc,o trrrc,rrclitrg
~)li\~.vic~itrri.s 11'1ro i t r t lo l~t~rr t l t~rrr l~ tr.\sc,.s.\c,cl 28 orlrc,r ~)ro.sl,c,c.ri~.c,!\. (.ollt,t.rc.tl c,tr.sc,s (I( trllo,qc.d .4DRs
11.tr.s \.or\. lriglr (rcrrrgc,: r = 0.76 ro 0.87; R(t,.sr) = O.XO). 11 \\.tr.v ctlso .slro~\~rr rlrtcr rlrr ADR
~>ro l x rh i l i h .sc,trlc 11tr.s c~~rrsc~rr.\rrtrl. c~orrrc~~rr, curt1 ~.~~rrc.rrrr-orrr ~ . t r l i ~ l i h . T1ri.s s\~.\rc,rrrtrric rrrc,rl~otl (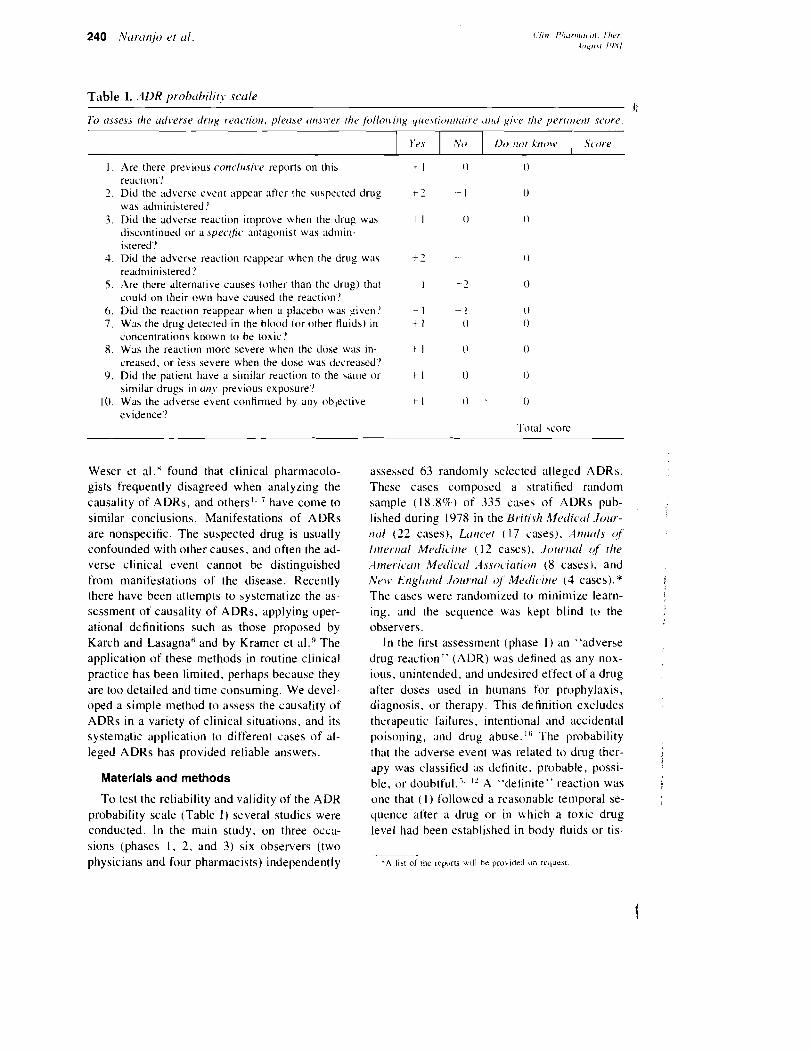
Table I . .4DR p r o h ~ b i l i y scule II
7h trssess /\re trdverse tlrrrg t-twc,rior~, plecrse trrr.s;~.rr rhr fbllo~virrg qrtr.\riot~r~trirr ~rtrll ,yir.c rhc' perrrrirr~r score.
( Yrs I ,"\.') 1 11)) ,lor Xtlon 1 Score
I . Are there previous conc.lrisire reports on this reaction'!
2 . Did the adverse event appear after the uspected drug was adn~inistered!
3. Did the adverse reaction improve when the drug mas discontinued or a spec,~/ic ~lntagonist was admin- istered?
1. Did the adverse reaction reappear when the tlrug was readministered!
5. Are there alternative causes (other than the drug) that could on their own have caused the reaction'!
6 . Did the reaction reappear when ;i placebo was given'! 7. Was the drug detected in the blood (or other Huids) In
concentrations known to be toxic'? 8. Was the reaction more severe when the close was in-
creased. or less severe when the dose was decreased'? 9. Did the patient have a similar reaction to the same or
similar drugs in ( ~ t i j . previous exposure? 10. Was the adverse event confirmed by any objective
evidence'? 'Total c o r e
Weser et al.' found that clinical pharmacolo- gists frequently disagreed when analyzing the causality of ADRs, and others1. ' have come to similar conclusions. Manifestations of ADRs are nonspecific. The suspected drug is usually confounded with other causes, and often the ad- verse clinical event cannot be distinguished from manifestations of the disease. Recently there have been attempts to systematize the as- sessment of causality of ADRs, applying oper- ational definitions such as those proposed by Karch and Lasagna6 and by Kramer et al.!' The application of these methods in routine clinical practice has been limited, perhaps because they are too detailed and time consuming. We devel- oped a simple method to assess the causality of ADRs in a variety of clinical situations, and its systematic application to different cases of al- leged ADRs has provided reliable answers.
Materials a n d methods
To test the reliability and validity of the ADK probability scale (Table I ) several studies were conducted. In the main study, on three occa- sions (phases 1 , 2. and 3) six observers (two physicians and four pharmacists) independently
assessed 63 randomly selected alleged ADRs. These cases composed a stratified random sample ( 1 8 . 8 9 ) of 335 cases of ADRs pub- lished during 1978 in the U~Yrish hfr,rlic,trl Jo~rr - tltrl ( 2 2 cases), Ltr~lc,rr r 17 cases), A11r1~1ls of
I~irrrrrul Mc~tlici~ir ( 1 2 cases), .lorrr11~/1 of rlir . - I I N C ~ ~ L . L I I I M ~ d i c ~ r I . 1 ~ ~ o c . i ~ r i o r i ( 8 cases), and Nrlr) Engltrtitl Jorrrrlul (4' Mrtlir.ir~r ( 4 cases).* i The cases were randomized to minimize learn- ing. and the sequence was kept blind tv the observers.
In the first assessment (phase I ) an 'adverse drug reaction" (ADR) was defined as any nox- ious, unintended, and undesired effect of a drug after doses used in humans for prophylaxis, diagnosis, or therapy. This definition excludes therapeutic failures, intentional and accidental poisolling, and drug abuse. '" The probability that the adverse event was related to drug ther- apy was classified as definite. probable, possi-
i
ble, or doubtful.", I% '"delinite" reaction was j one that ( 1 ) followed a reasonable temporal se- quence after a drug or in which a toxic drug level had been established in body fluids o r tis-

sues, (2) followed a recognized response to the suspected drug. and (3) was contirmed by im- provement on withdrawing the drug and reap- peared on reexposure. A "probable" reaction ( 1 ) followed a reasonable temporal sequence after a drug. (2) followed a recognized response to the suspected drug, (3) was confirmed by withdrawal but not by exposure to the drug, and (4) could not be reasonably explained by the known characteristics of the patient's clinical state. A "possible" reaction (I) followed a temporal sequence after a drug. (2) possibly fol- lowed a recognized pattern to the suspected drug. and (3) could be explained by charac- teristics of the patient's disease. A reaction was defined as "doubtful" i f it was likely related to factors other than a drug.
Six weeks later the 63 c;laes were reordered randomly and reanalyzed (phase 2). The observ- ers independently assigned a weighted score to the components used to establish a causal asso- ciation betwecn drugs and adverse events (tem- poral sequence. pattern of response. withdrawal, reexposure, alternative causes, placebo re- $ponse, drug levels in body fluids or tissues, dose-response relationship. previous patient ex- perience with the drug, and confirmation by ob-
1 jective evidence). These factors were analyzed and scored using the ADR probability scale (Table I ) . Each question could be answered positive (yes), negative (no). or unknown or inapplicable (do not know). The raters were in- structed to use the questionnaire for about 20 min.* The ADR was assigned to a probability category from the total score as follows: definite 2-9, probable 5 to 8, possible 1 to 4, doubtful 5 0 . The between-raters reliability to use the categorical classification of ADR probability was measured using percent agreement and kappa ( K , a chance-corrected inde .~ of agree- ment).'-' Kappa was calculated as follows:
P,, - P,. K = - I - P,.
where P , = proportion of observed agreement
*.4n a p p n d l x with instructions for using o u r ADR pmbab~lity scale will be supplied with reprints and will 3lw he available from the National A u x ~ l i a r y Publication Service. American Society of Inl;?rmation Services. 1010 16th St. N.W.. Washinelon, D.C. 20036.
and P, = proportion of agreement expected by chance. Kappa ranged from - 1 (complete dis- agreement) to + l (perfect agreement). Correla- tion coefficients between ADR scores were also used to test between-raters and within-raters re- liability in phases 2 and 3. The intraclass corre- lation coefficient of reliability (R[est]) was also calculated:
where Sg = variance from the cases, S: =
variance generated by the raters, and S: = re- sidual variance or error. This coefficient is the ratio of the variance associated with true case- to-case variability to the sum of all the compo- nents of variance. R(est) varies from zero ( i .e . , no intercase variation is detected by the ratings, the ratings are the result only of measurement error and between-rater differences) to a maxi- mum of unity ( i .e . , intercase variation is cor- rectly detected by the ratings, there is no contam- ination by measurement error or rater-to-rater variation). I - ' The R(est) was calculated in phase 1 , assuming a score of 1 (doubtful), 2 (possi- ble), 3 (probable), or 4 (definite). The actual ADR scores were used in phases 2 and 3 .
T o determine whether the improvement in reliability found in phase 2 had occurred by chance the cases were again reordered randomly and reanalyzed independently by the six raters 4 mo later (phase 3). This allowed us to assess within-rater and between-rater retest reliability. The between-rater reliability of practicing phy- sicians was also tested. Three attending physi- cians independently rated 28 other prospec- tively collected cases of alleged ADR observed in the Toronto Western Hospital.
Validity. T o establish validity comparison with a standard is necessary. Because there is no method that can determine which adverse events are truly ADR, we studied the validity of the ADR probability scale in several ways. Consensual validity was tested as follows. ( 1 ) The consensus assessment of three "experts" ( C . A. N . , E. M. S . , D. J . G . ) using the con- ventional categories of ADR probabilities was the external standard with which physicians- pharmacists assessments were compared. Their expertise is supported by p ~ b l i c a t i o n s . ~ l o . l 2
Clin. Phurmocol. Ther Augrrsr I Y X l
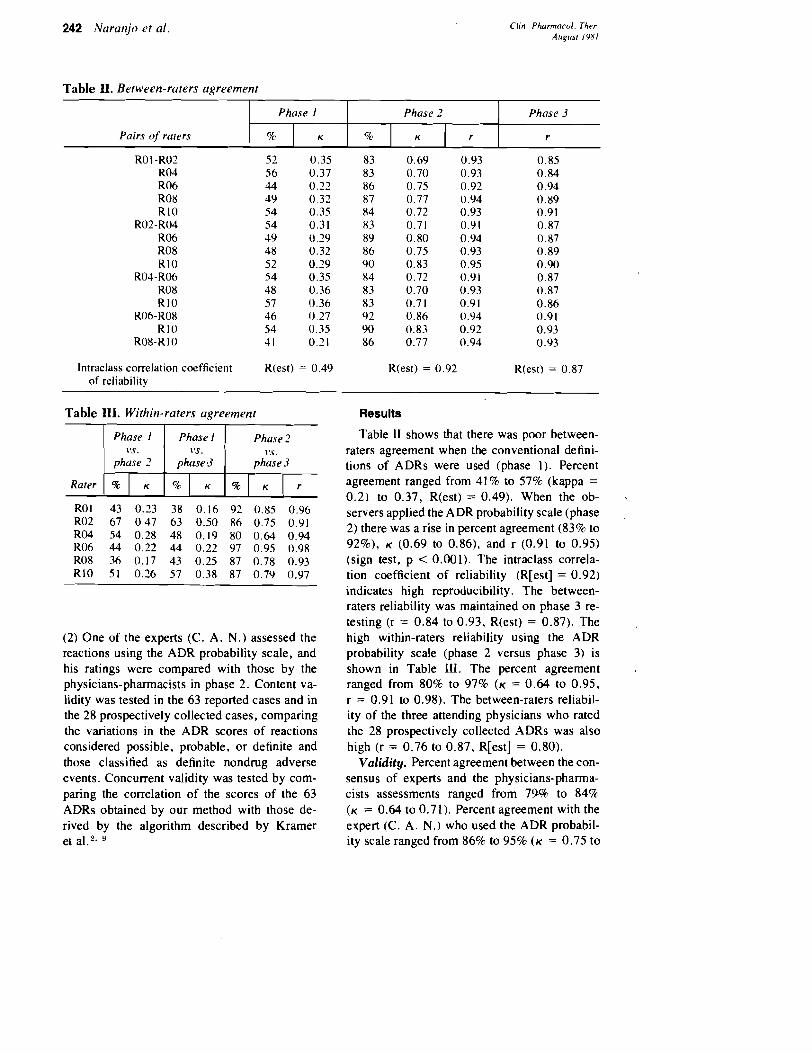
Table 11. Between-rc~rers agreement
lntraclass correlation coefficient R(est) = 0.49 of reliability
Pairs of raters
Table 111. Within-raters agreement
Phuse 2
phase 3
Rater
(2) One of the experts (C. A. N.) assessed the reactions using the ADR probability scale, and his ratings were compared with those by the physicians-pharmacists in phase 2. Content va- lidity was tested in the 63 reported cases and in the 28 prospectively collected cases, comparing the variations in the ADR scores of reactions considered possible, probable, or definite and those classified as definite nondrug adverse events. Concurrent validity was tested by com- paring the correlation of the scores of the 63 ADRs obtained by our method with those de- rived by the algorithm described by Kramer et
Phase I
Results
%
Table I1 shows that there was poor between- raters agreement when the conventional defini- tions of ADRs were used (phase 1). Percent agreement ranged from 41% to 57% (kappa =
0.21 to 0.37, R(est) = 0.49). When the ob- %.
servers applied the ADR probability scale (phase 2) there was a rise in percent agreement (83% to 92%), K (0.69 to 0.86), and r (0.91 to 0.95) (sign test, p < 0.001). The intraclass correla- tion coefficient of reliability (R[est] = 0.92) indicates high reproducibility. The between- raters reliability was maintained on phase 3 re- testing (r = 0.84 to 0.93, R(est) = 0.87). The high within-raters reliability using the ADR probability scale (phase 2 versus phase 3) is shown in Table 111. The percent agreement ranged from 80% to 97% ( K = 0.64 to 0.95, r = 0.91 to 0.98). The between-raters reliabil- ity of the three attending physicians who rated the 28 prospectively collected ADRs was also high (r = 0.76 to 0.87, R[est] = 0.80).
Validity. Percent agreement between the con- sensus of experts and the physicians-pharma- cists assessments ranged from 7% to 84% (K = 0.64 to 0.71). Percent agreement with the expert (C. A. N.) who used the ADR probabil- ity scale ranged from 86% to 95% (K = 0.75 to
Phase 3
r K
Phase 2
% K r
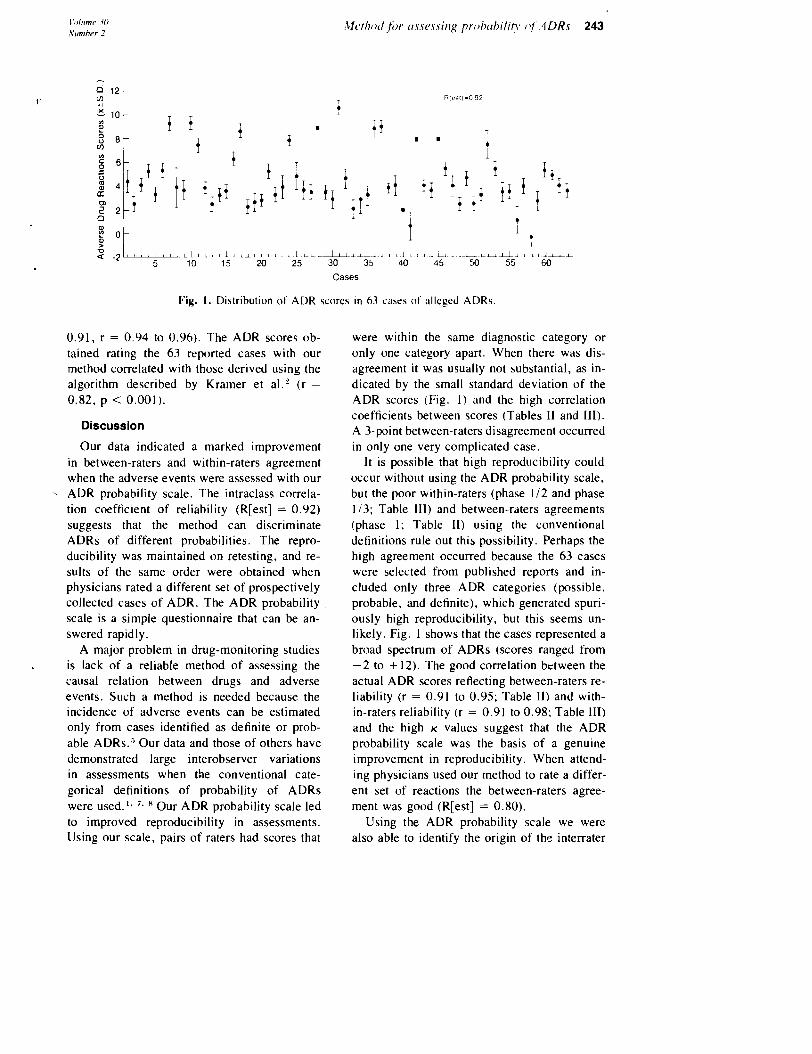
Cases
Fig. I. Distribution of ADR scores in 63 cases of alleged ADRs.
0.91. r = 0.94 to 0.96). The ADR scores ob- tained rating the 63 reported cases with our method correlated with those derived using the algorithm described by Kramer et al.' (r =
0.82, p < 0.001).
Discussion
Our data indicated a marked improvement in between-raters and within-raters agreement when the adverse events were assessed with our ADR probability scale. The intraclass correla- tion coefficient of reliability (R[est] = 0.92) suggests that the method can discriminate ADRs of different probabilities. The repro- ducibility was maintained on retesting, and re- sults of the same order were obtained when physicians rated a different set of prospectively collected cases of ADR. The ADR probability scale is a simple questionnaire that can be an- swered rapidly.
A major problem in drug-monitoring studies is lack of a reliable method of assessing the causal relation between drugs and adverse events. Such a method is needed because the incidence of adverse events can be estimated only from cases identified as definite or prob- able ADRs." Our data and those of others have demonstrated large interobserver variations in assessments when the conventional cate- goricaI definitions of probability of ADRs were used." '. Our ADR probability scale led to improved reproducibility in assessments. Using our scale, pairs of raters had scores that
were within the same diagnostic category or only one category apart. When there was dis- agreement it was usually not substantial, as in- dicated by the small standard deviation of the ADR scores (Fig. 1 ) and the high correlation coefficients between scores (Tables I1 and 111). A 3-point between-raters disagreement occurred in only one very complicated case.
It is possible that high reproducibility could occur without using the ADR probability scale, but the poor within-raters (phase 112 and phase 113; Table 111) and between-raters agreements (phase 1: Table 11) using the conventional definitions rule out this possibility. Perhaps the high agreement occurred because the 63 cases were selected from published reports and in- cluded only three ADR categories (possible, probable, and definite), which generated spuri- ously high reproducibility, but this seems un- likely. Fig. 1 shows that the cases represented a broad spectrum of ADRs (scores ranged from -2 to + 12). The good correlation between the actual ADR scores reflecting between-raters re- liability (r = 0.91 to 0.95; Table 11) and with- in-raters reliability (r = 0.91 to 0.98; Table 111) and the high K values suggest that the ADR probability scale was the basis of a genuine improvement in reproducibility. When attend- ing physicians used our method to rate a differ- ent set of reactions the between-raters agree- ment was good (R[est] = 0.80).
Using the ADR probability scale we were also able to identify the origin of the interrater
dis;ipreenlmts. The :r>s~:>alrlent (lf quebtion 5 (aitern:itive ~, ; iuszr) led to the most disagree- !,lent. In view of the cunlplex clir~ical situatiolls :~nd the differences in triiir~ing o f the observers, this should have been ;~nticipated. Pharmacists in general n.ere more likely to ansuer "I d o not k ~ ~ o w " to this question. Hutchinson et al. ' !clund that this c o ~ ~ l d he a ~ n i ~ j o r source of dis- aqeerrlent evcn though \.cry 8.letaileti instruc- tions were given. In $oms complicated cases n o i~lgori th~n can snhstitute for clinical experience.
Evcn though the repruducibilitv of ;In instru- r r~er~t is ilnportant. its validity rnust also he con5itlered. The ohservers could agree among thelr~sclves, but they cnuld also all be wrong. In cases of ;ldverse events there is no definite stan- dard again\t which to test the validity of new operational definitions of XDRs. We therefore assessed the validity of our AI>R probability sc;~le in several \bays. The agreement of the six raters mith the consensus o f three experts was \cry high, suggesting that our instrument has consensual validity. Although the experts may not always accurately classify reactions. the probability that the consensus of three experts would be corr~pletely wrong all the time is small. The high agreement between the physi- cians-pharmacists and one o f the experts using the RDR probability scale also indicates con- sensual validity. The concurrent validity of our instrument is suggested by the good correlation between the ADR scores generated by our method and those of another recently pl~blished a l g o r i t h m . T h e negative scores in the definite nondrug adverse events and the positive scores in the "true" ADR indicate that our method had content validity. Our tindings indicate that our hl1R probability scale is reliable and valid.
Important potential ;~pplications of the ADK probability scale are the analysis of adverse $drug-related events published in medical jour- nals as well as the assessment of reports submit- ted to national tlrllg monitoring centers. Many countries ore interested in developi~ig postmar- keting drug surveilla~ice programs.'' The reli- ability of the ADR assessments in case studies could improve if operational delinitions such as ours and similar procedures are used." Advan- tages of our method are simplicity and wide applilvability. Sonie minor modifications rriay be
required in special circumstances. In analyzing adverse drug interactions suspect interacting 4 drugs rather than a particular drug must be as- sessed. When a patient receives several drugs at the same time the ADR scale must be applied to each of the possible causes: the most likely will he the drug with the highest score. In reactions that appear during drug withdrawal. withdrawal corresponds to reinstituting treatment and rep- etition corresponds to disccntinuing the suspect drug.
The conventional classilicntion of definite. probable, possible, and doubtful ADRs. as pro- posed by Seidl et al."' in 1966, assumes four discrete categories For which there is no empiri- cal demonstration, It is therefore reasonable to postulate that some of the unreliability of the conventional detinitions or operational detini- tions of ADRs could result. because such cate- gories are not unique ( i . e . , the unreliability could reflect the overlap between nondiscrete categories). Thus the higher correlation co- cfticients of the actual ADR scores (r = 0.91 to 0.94), as compared with the kappa values when using four categories ( K = 0.69 to 0.83) (Table 11). support this view and indic,ate the need to characterize the probability spectrum of ADRs empirically. We suggest that it is preferable 1 ,: !
to classify the prohability using the actuaI ADR scores by our and \imilar operational methods.
Notwithstanding our encouraging results, it is unrealistic to expect that our relatively simple procedure will solve all the complex problems of identification and classification of ADRs. Further experience will provide the rationale for refinements and improvements and will confirm its utility in clinical practice. Our findings sug- gest that its systematic application can improve the quality of the assessment of ADRs in a va- riety of clinical situations.
The collaboration of Doctors M. Spino. H . Wang. and M . Rudyk and of S. Schachter. B .Sc.. in some of the phases of the study i s grnteti~lly itcknowledged.
Rufirur~cua I . Blanc S, Leuenberger P. Berger JP. Brooke EM.
Schelliny JL: Judgments of trained observers on adverse drug reaction<. C1.i~ PH A R M ~ C O L THER 25:493-498. 1979.
1. B u t o I!. ?I :~r~ ln jo C"4. Sellera ELI: i ~ ~ i ~ p a r r : ~ ~ ) ~ ~ 1 o l two recen~ly published .ilgorithr~ls to .iare,s
the prcibabrlit). a d ~ c r s e drug rcai;:tloils. C I IS
P~~.-\KzI-\~oI ' ~ ~ I E R 20:2.3h. I'jR1 3 . Gross F t i , Inrnan WtiW: Dl-11s i n ~ c i n ~ t o ~ - i i ~ g . ?.I?:+-
YOI-k. 1077. .\c;idcn~~i;: Press. 1. Flut~~hinst111 T.A. l.e\.cnthal J h l . K~,ur~i;:r >IS.
K;~ri;:h t.E. I.rplnan .A(;. F;c'in\tc.in .AR: .An al- ~ o r i t h m lo r rhe ~ ~ p e l a t i o n a l d>sesblllent o i .IJ- \else tlr-ug ~cacriona. 11. I)crnt)nsrr;irion of 1.2-
pr~ ldt lc ih i l i ty JII~ \ a l i J i t y . JX?rlA 242:hi i h3X. 1979.
5 . Karch FE. L.,I\,I~II~ 1-: :\d\c~.,e drug rt.ii~.tlona: 1 crit ical revle\c. J A b I A 2.74: 1236- 12-11. 1075.
0 . Karch FE. Ldbagnlr L : 'TowarJ rhc' opc.rario~~,rl i de r~~ i r i ca t ion o i ad~c ' rbe (Ir~rg re;~ctions. Ci 1%
P I ~ ~ K M - \ ~ ~ I ~ H L - R 21:217-25-1, 1 ~ 7 7 . 7 . Karsh FE. Smith C'L. l i e r rner B. h l u ~ ~ u l l o .iM.
Weintraub 51. Laaagrra L: ,Advcrsc d n r IeaL,- ~i~,ns: A matter OF opinron. C'I..IN PIIAK~IA~ OL
T t l t . ~ 19:1X9-492. 1076. X . Koch-\Veser J. Sellers EM. Z~i;:e\t R: 'The a111-
ttiguity o l a d ~ c r s e ~ I - L I ~ rcacrionr. L!~.rr J C l l n Pharnlacol 11:7.5-78, 1977.
9 . Krluuer h I S . I.t.\;el~thal JIM, Hutchinson 'T.1. Feinsrein AR: : i n a lgor i thm for the operat io l~al ;cssc.asrnent u t adbsrse drug reactions. I . Hack- ground, drhcript ion. and instrui;:tions for LI~S. JAMA 2-42:623-631, 19.79.
i l l , * l i l l c ~ [ < I < . <~~ICL.II~;I:II~ 1 ) ) . I . j tug CI~ 'CC[ \ III I I%I \~J~- rdl irct l p d ~ c n t \ . \etv 'L'nrk. 1976. lohn \i'ilt?)'S s011r.
i I . ? q , ~ ~ . d ~ ~ l o C 1. [~II\IO I . ..',b~l .I(;. S c l l ~ r s 1131: t<mp i r r i ~ le l i~ rea t ion ,)t the probcthrlity \l,c.ctrllnl 111' < i d \ c r ~ c t1r11g I-~~IL.IIOI~~. CI ib t ' t i - \u\ l~c 01.
~ ~ I I I R 2 ~ : ~ 0 7 ~ ~ ~ ~ . lost 12 . ?,~ii~..~nlo C \. F'OIIII~O E. \ d1dcncg1-o ( '. &)n-
i * ~ I c f G. KIIIL I. BLI~II) F~~ r , ) sc~ l i i de - i r~~ I~~~ . : c i ; ~ i l ~ ~ c ~ s c iec1L~it'nh i n ~ i r ~ t i t \ a r r , ) t ' [he l i ~ . c r . L'I IS
I'II.\R!,IA\ a IL l ' i i t . ~ 25: 134- 100. ! c l ~ ' l . 13. SLILII 1 .G T'11o1.11ton (;F:. S1111th .It+'. ( l u f f 1 E;
Stuilieh on [he ep ic l c~n i~ l losy o i .icl\cr\c J ~ L I ~ ~ i ~ t i i . lil. Kc' i rc f ion~ i r ~ pdrienrs ttn a gcller:kl r ~ ~ c d i ~ . , i l ,er\.r~,c. IOIIIIS l i o ~ h i ~ ~ s 5,lcd 1 I 19:2'iLJ- 315. 19h6.
1-1. Spirter R l . . t . 1 ~ 1 5 ~ J L . E r ~ ~ i i c ~ r ~ t I: f'~.ciblt.ms r l t '
, las>~licar~urr: Re l iab i l~ ty and , l l i c l i t > . !,r l . i l)[un %lA, LIihla>cro A. K i l l i ~ r l ~ DF. etlitorh: P\y- L ~ I I L I ~ > I ~ ~ I I ~ I ~ L o I ~ I ~ ~ ; '1 g?n~r.dt ion or progress. Nc:w YOI-A. 1978. K i i \ c n Prcas. p l , 657-869.
l i . Wardel l \Vhl. Tatar~~.o \IC. .1na\.ckar SPJ. ()a\ is t I T P~)srrnarkcr~l lg >11r\ eillancs u i new dr.ug5. \I. Care \(ci<lles. J C'lin Phdrl~~ai;:ol lY:16Y-1x4. 1979.
! 6. Wor l t l He:llrh Organiration; I ~ i t c i ~ ~ i a t i o r ~ ; ~ I dr119 111onitcrring: 'rile rc~lc. of tire hoaoital. LL 110 Tech Rep Scr No. 125. 1Y69
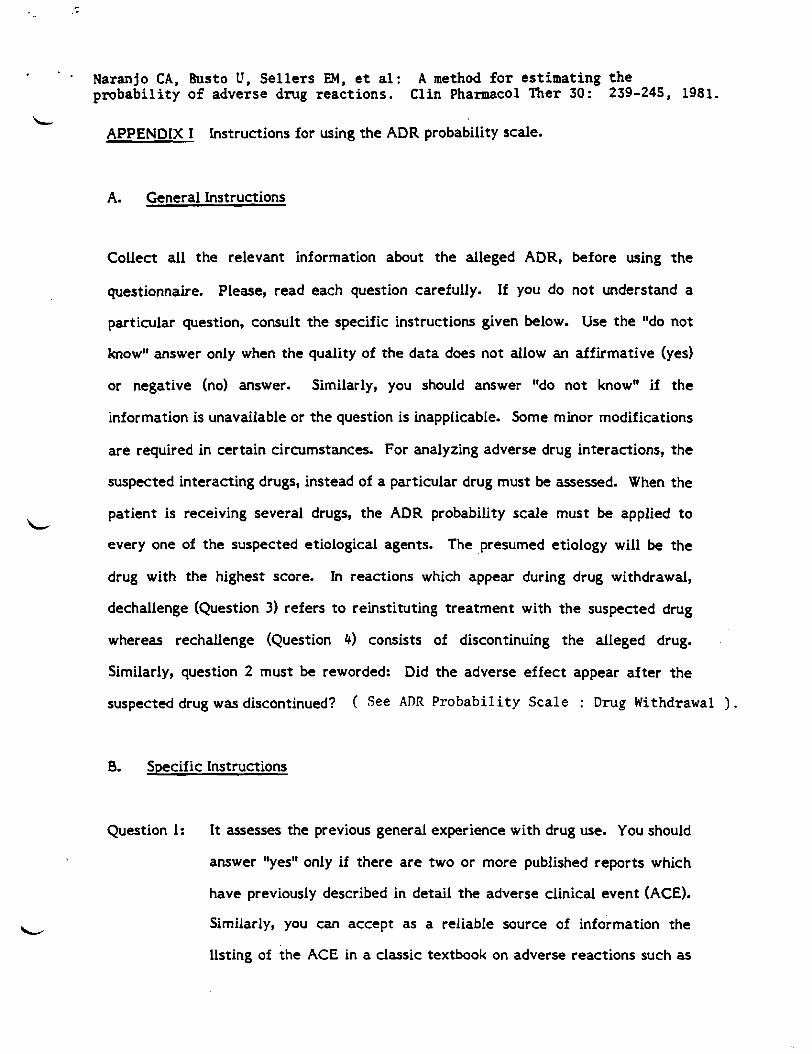
Naranjo CA, Busto U, S e l l e r s EM, e t al : A method f o r e s t ima t ing t h e p r o b a b i l i t y o f adverse drug r eac t ions . Cl in Pharmacol Ther 30: 239-245, 1981.
L APPENDIX I Instructions for using the ADR probability scale.
A. General Instructions
Collect all t he relevant information about the alleged ADR, before using the
questionnaire. Please, read each question carefully. If you do not understand a
particular question, consult the specific instructions given below. Use the "do not
knoww answer only when the quality of the data does not allow an affirmative (yes)
or negative (no) answer. Similarly, you should answer "do not know" if the
information is unavailable or the question is inapplicable. Some minor modifications
a r e required in certain circumstances. For analyzing adverse drug interactions, the
suspected interacting drugs, instead of a particular drug must be assessed. When the
patient is receiving several drugs, the ADR probability scale must be applied t o L
every one of the suspected etiological agents. The presumed etiology will be the
drug with the highest score. In reactions which appear during drug withdrawal,
dechallenge (Question 3) refers t o reinstituting treatment with the suspected drug
whereas rechallenge (Question 4) consists of discontinuing the alleged drug.
Similarly, question 2 must be reworded: Did the adverse e f fec t appear af ter the
suspected drug was discontinued? ( See ADR P r o b a b i l i t y Sca l e : Drug Withdrawal ) .
0. Specific Instructions
Question 1: It assesses the previous general experience with drug use. You should
answer "yes" only if there a r e two or more published reports which
have previously described in detail the adverse clinical event (ACE).
Similarly, you can accept as a reliable source of information the
listing of the ACE in a classic textbook on adverse reactions such as
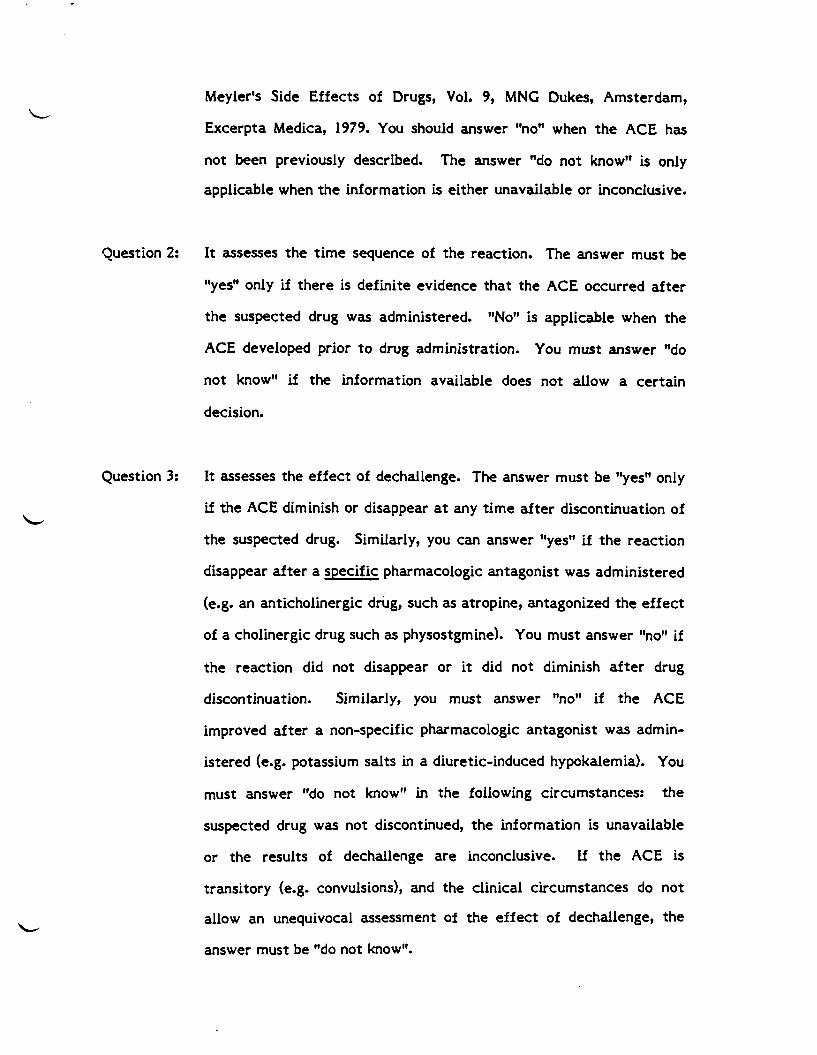
Meyler's Side Effects of Drugs, Vol. 9, MNG Dukes, Amsterdam,
Excerpta Medica, 1979. You should answer "no" when the ACE has
not been previously described. The answer "do not know" is only
applicable when the information is either unavailable or inconclusive.
Question 2: It assesses the t ime sequence of the reaction. The answer must be
"yes" only if there is definite evidence tha t the ACE occurred a f te r
the suspected drug was administered. "No" is applicable when the
ACE developed prior t o drug administration. You must answer "do
not knoww if the information available does not allow a certain
decision.
Question 3: It assesses the effect of dechallenge. The answer must be "yesw only
if the ACE diminish or disappear at any t ime af te r discontinuation of
the suspected drug. Similarly, you can answer "yes" if the reaction
disappear a f te r a specific pharmacologic antagonist was administered
(e.g. an anticholinergic drug, such as atropine, antagonized the effect
of a chalinergic drug such as physostgmine). You must answer "no" if
the reaction did not disappear or i t did not diminish a f te r drug
discontinuation. Similarly, you must answer "no" if the ACE
improved af ter a non-specific pharmacologic antagonist was admin-
istered (e.g. potassium salts in a diuretic-induced hypokalemia). You
must answer "do not know" in the following circumstances: the
suspected drug was not discontinued, the information is unavailable
or the results of dechallenge a re inconclusive. If t he ACE is
transitory (e.g. convulsions), and the clinical circumstances do not
allow an unequivocal assessment of the effect of dechallenge, the
answer must be "do not know".
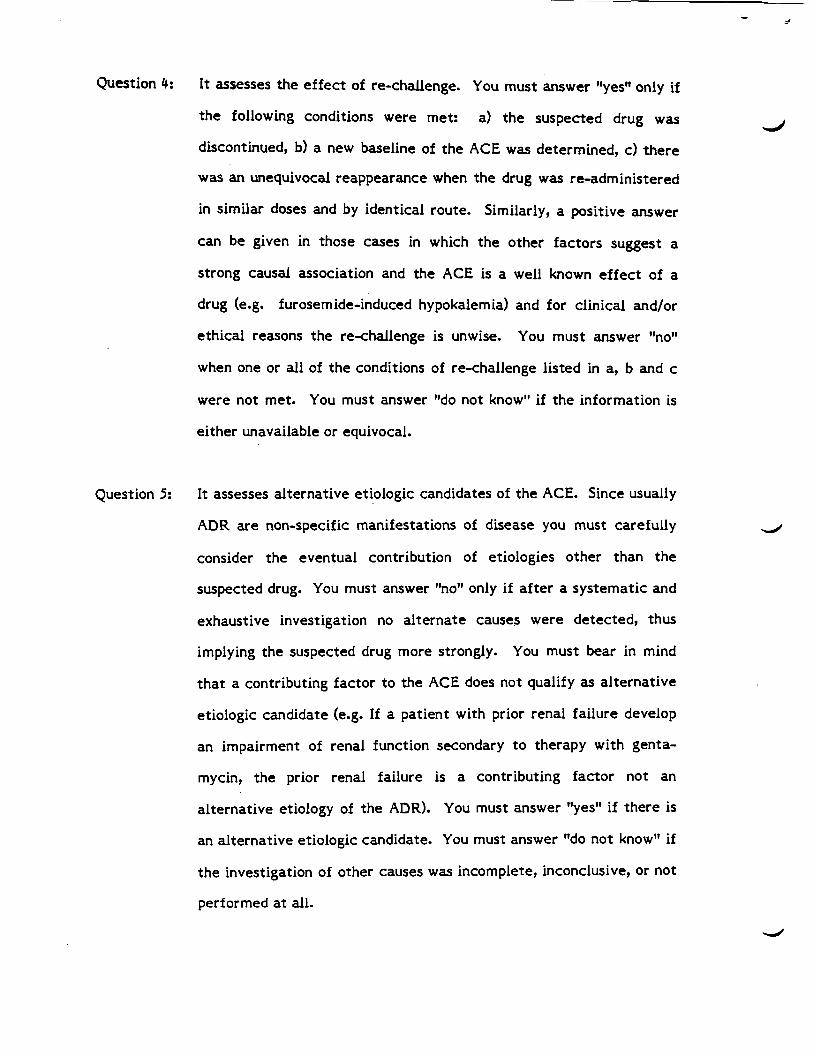
Question 4: I t assesses t h e e f f e c t of re-challenge. You must answer llyesll only if
t h e following conditions were met: a) t h e suspected drug was
discontinued, b) a new baseline of t h e ACE was determined, c ) t h e r e
was a n unequivocal reappearance when t h e drug was re-administered
in similar doses and by identical route. Similarly, a positive answer
can be given in those cases in which t h e other factors suggest a
strong causal association and t h e ACE is a well known e f f e c t of a
drug (e.g. furosemide-induced hypokalemia) and for clinical and/or
e thical reasons t h e re-challenge is unwise. You must answer "now
when one o r a l l of t h e conditions of re-challenge listed in a, b and c
were not met. You must answer "do not know" if t h e information is
ei ther unavailable o r equivocal.
Question 5: It assesses alternative etiologic candidates of t h e ACE. Since usually
ADR are non-specific manifestations of disease you must carefully
consider t h e eventual contribution of etiologies o ther than t h e
suspected drug. You must answer "no" only if a f t e r a systemat ic and
exhaustive investigation no a l t e rna te causes were detected, thus
implying t h e suspected drug more strongly. You must bear in mind
t h a t a contributing fac to r t o t h e ACE does not qualify as al ternat ive
etiologic candidate (e.g. If a patient with prior renal fai lure develop
a n impairment of renal function secondary t o therapy with genta-
mycin, t h e prior renal failure is a contributing fac to r not an
a l ternat ive etiology of t h e ADR). You must answer "yes" if the re is
an alternative etiologic candidate. You must answer "do not know" if
t h e investigation of other causes was incomplete, inconclusive, o r not
performed at all.
Question 6: It is important when the ACE is subjective. The answer must be L
l1yesl1 only if t he following conditions were met: a) the suspected
drug was discontinued, b) a new baseline of the clinical manifestation
was established, and c) there was unequivocal re-appearance of t he
ACE af te r a single or double-blind placebo administration. The
answer must be "no" if re-administration of placebo, as described
above, did not elicit the same reaction. You must answer "do not
knowv1 when a placebo test was not performed, the information is
unavailable, or t he placebo e f fec t is inconclusive.
Question 7: I t is very important in cases of dose-related ADRs, and i t assesses
the information provided by drug concentrations in blood, other body
fluids or tissues. The answer must be llyesll only if t he concentration
of the alleged drug is in the accepted toxic range. The answer must
be l1nol1 if drug concentration is below the toxic range; and the answer
must be "do not knowt1 if this information is either unavailable or t he
question is inapplicable (i.e. in ADRs which a r e not dose-related).
Question 8: I t assesses clinically the dose-response relationship. You must
answer only if t he ACE was more severe when the dose of the
alleged drug was increased. Similarly, you must answer l1yesl1 if the
ACE was less severe a f te r reduction in the dose of the alleged drug.
The answer must be llnoll if there was no clinically detectable
variation in t he ACE when the dose of the suspected drug was
changed. You must answer "do not know" when either the dose did
not change or t he information is unavailable.
Question 9: It assesses the personal experience of t he patient in previous
administrations of t h e same or chemically related drugs. You must
answer "yestt only if t h e patient report a similar ACE t o t h e drug(s).
Similarly, you must answer "yesv if there is documentation in t h e
patient's record of such prior reaction (e.g. documentation of prior
manifestations of allergy t o penicillin such as skin rash or anaphyl-
axis.) You must answer "nott when either t h e patient has no previous
exposure t o t h e drug or if in a previous exposure t o t h e same or
similar drugs t h e patient did not develop t he ACE. The answer must
be "do not knowN when either t h e information is unavailable o r it is
inconclusive.
Question 10: It assesses the quality of t he information in which we a r e supporting
our judgments. This is crucial because even though the patient's
report is a very important source of information, some patients can
be unreliable, for instance, because of memory impairment. You
must answer "yes" only in t he following circumstances: a) a
laboratory test documented t h e ADR (e.g. in t h e case of a suspected
drug-induced hepatitis, a compatible liver biopsy). b) t h e ACE was
directly observed by qualified personnel (e.g. t he attending physicians
or t h e nurses observed manifestations such as the skin rash, jaundice,
etc). The answer must be "no" when either t he laboratory tests or
t h e direct clinical observation did not document the reaction. The
answer must be "do not know" when t he ACE is subjective, t h e
information is unavailable or i t is inconclusive.
Once you have answered all t h e questions, you must add t he individuals scores. The
probability of t h e ADR i s given by t h e tota l score.
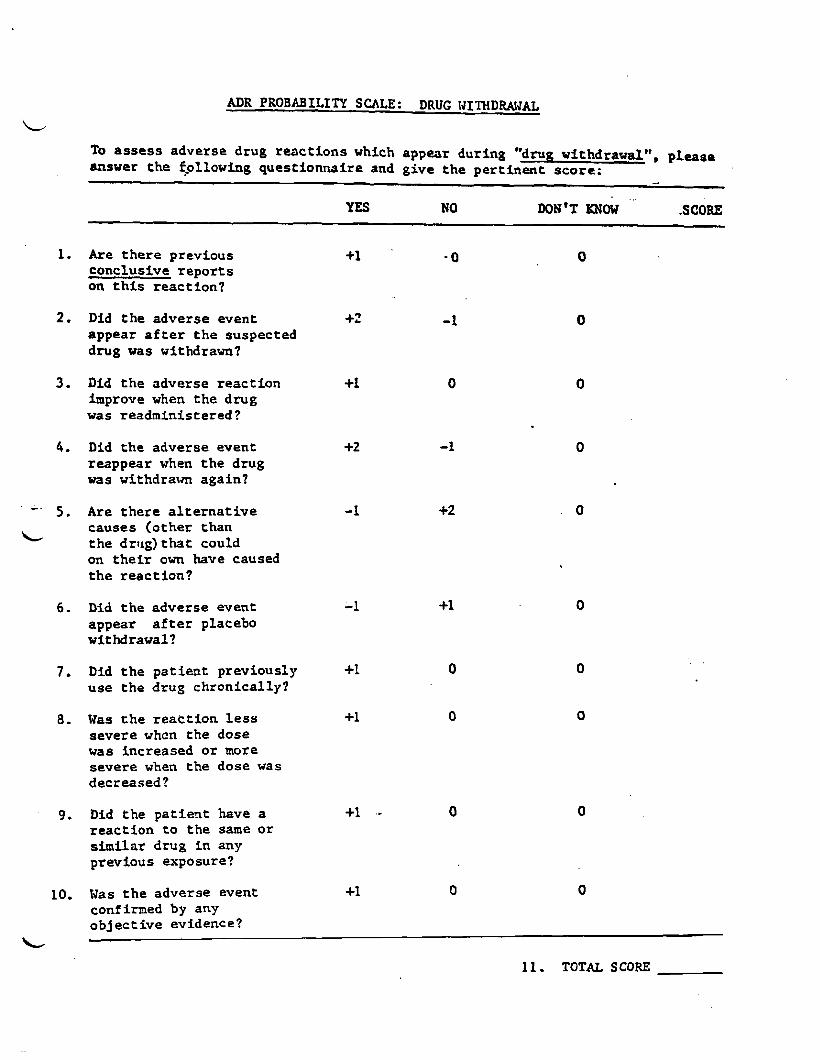
ADR PROBABILITY SCALE : DRUG IJITHDRAWAL
L To assess adverse drug reac t ions which appear during "drug withdrawal", please answer the ~_ollowing questionnaire and give the per t inent score:
... -..
YES NO DON'T KNOW SCORE
1. Are t he r e previous conclusive r epo r t s on t h i s react ion?
2. Did t he adverse event +2 - 1 appear a f t e r t h e suspected drug was withdram?
3. Did t h e adverse react ion improve when t he drug vas readministered?
4. Did the adverse event reappear when t he drug was withdrawn again?
- 5 . Are the re a l t e r n a t i v e
L causes (other than the drug) t h a t could on t h e i r own have caused t he react ion?
6. Did t h e adverse event appear a f t e r placebo withdrawal?
7. Did t he pa t i en t previously +1 use t h e drug chronically?
8. lias t h e r e a t t i o n l e s s +1 severe whcn the dose was increased o r more severe when t he dose was decreased?
9. Did the pa t i en t have a +1 .- 0 react ion t o the same o r s imi la r drug i n any previous exposure?
10. tias t h e adverse event +1 0 0 confirmed by any ob jec t ive evidence?
L
11 . TOTAL SCORE
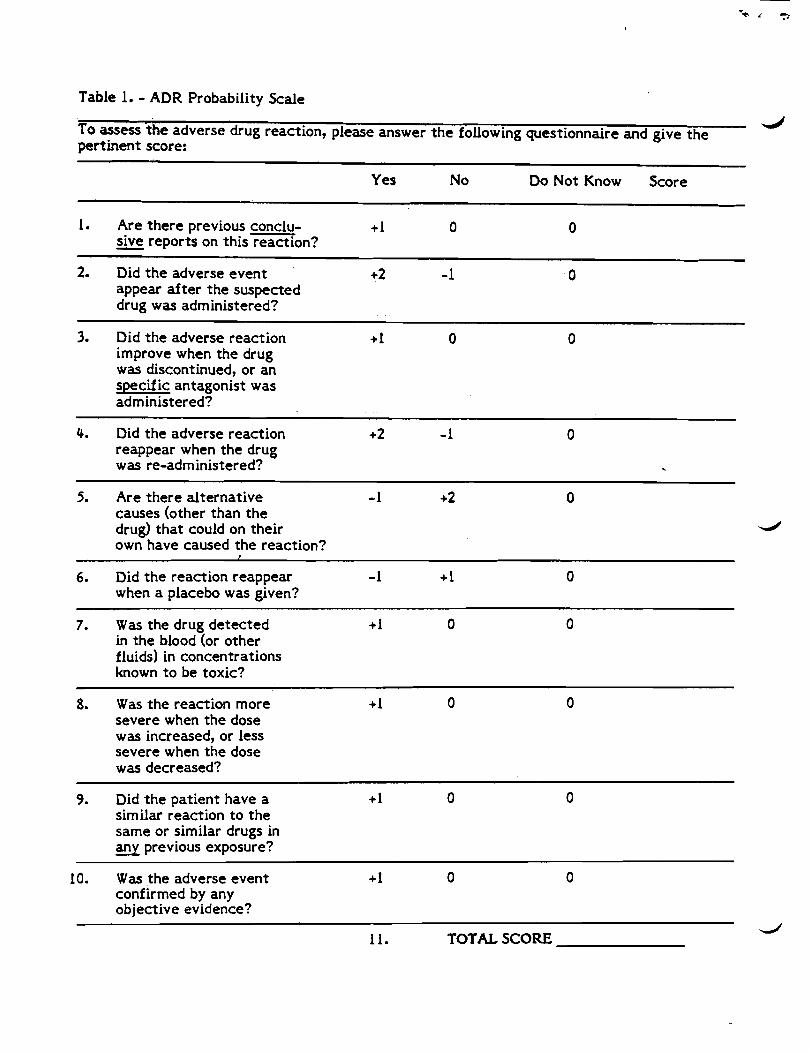
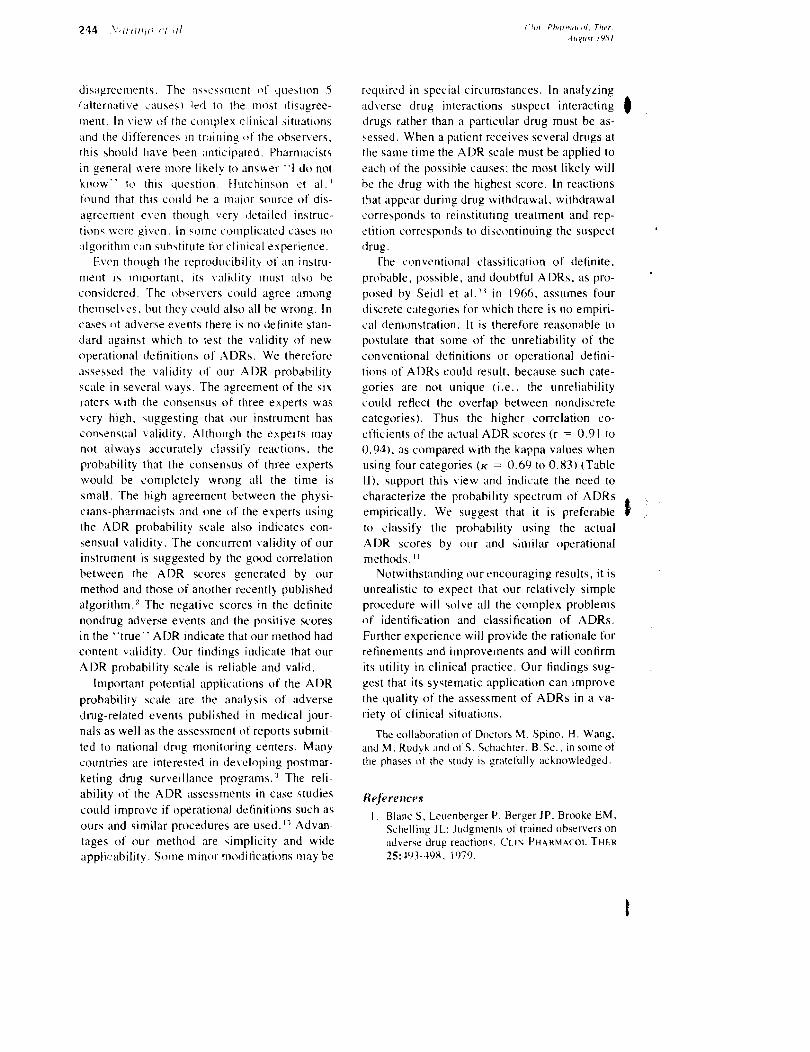
Table 1. - ADR Probability Scale
To assess t h e adverse drug reaction, please answer t h e following questionnaire and give t h e pert inent score:
Yes No Do Not Know Score
1. Are t h e r e previous conclu- + 1 0 0 sive reports on th is reaction? -
2. Did t h e adverse even t +2 - 1 0 appear a f t e r t h e suspected drug was administered?
3. Did t h e adverse reaction + 1 0 improve when t h e drug was discontinued, o r an specific antagonist was administered?
4. Did t h e adverse reaction +2 - 1 0 reappear when t h e drug was re-administered? .
5. Are t h e r e a l ternat ive -1 +2 0 causes (other than t h e drug) t h a t could on thei r d
own have caused t h e reaction? f
6. Did t h e reaction reappear - 1 + 1 0 when a placebo was given?
7. Was t h e drug de tec ted +1 0 in t h e blood (or o the r fluids) in concentrations known t o be toxic?
-
8. Was t h e reaction more +I 0 severe when t h e dose was increased, o r less severe when t h e dose was decreased?
9. Did t h e pat ient have a +I 0 similar reaction t o t h e s a m e o r similar drugs in any previous exposure?
10. W a s t h e adverse even t + 1 0 confirmed by any objective evidence?
11. TOTAL SCORE d
Related Documents











