South East London Sector A meeting of NHS Bromley Governing Body Clinical Commissioning Group ENCLOSURE 7A QUALITY NARRATIVE REPORT QUARTER 3 SUMMARY: The quarterly Quality Narrative Report contains Provider reports relating to Kings College Hospitals, specifically PRUH; Oxleas Mental Health Trust and Bromley Healthcare. This report also contains any quality issues relating to the CCG’s other commissioned providers. The main Provider reports include information gathered from CQRGs including main agenda items/deep dives; information from quarterly Patient Outcomes; Patient Safety and Patient Experience Reports, if available, plus any issues of Concern raised by BCCG. The Report also includes any internal or external reviews; national data published in the quarter and updates on any live CQC Action plans. Below is a summary of the Key Issues within the report and discussed at the Quality Assurance Subcommittee. KEY ISSUES: Kings • Elderly Care & Dementia: The Trust confirms that all patients 75+ are screened for dementia/delirium. Both sites have clinical leads for dementia; specialist dementia wards and specific old age psychiatric liaison. Of concern is the fact that DH is supported by 3 WTE specialist nurses, however, despite the PRUH’s elderly population this site only has 1WTE specialist nurse (currently under recruitment). Therefore the PRUH are struggling to achieve the target for identification of cases • Workforce: Reduction in agency spend across the Trust in this period. Physician assistant posts being rolled out at PRUH (already in place at DH) Medical vacancies at PRUH 20% and DH 1.5% - this stark difference has been questioned at CQRG. • Quality Issues: Complaints: response rates challenged with KCH by BCCG Director of Governance Cancer of Unknown Primary: Notification of Concern letter re non-adherence to NICE guidance Clinical Chair: Dr Andrew Parson 1 Chief Officer: Dr Angela Bhan

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
South East London Sector
A meeting of NHS Bromley Governing Body Clinical
Commissioning Group
ENCLOSURE 7A
QUALITY NARRATIVE REPORT QUARTER 3 SUMMARY: The quarterly Quality Narrative Report contains Provider reports relating to Kings College Hospitals, specifically PRUH; Oxleas Mental Health Trust and Bromley Healthcare. This report also contains any quality issues relating to the CCG’s other commissioned providers. The main Provider reports include information gathered from CQRGs including main agenda items/deep dives; information from quarterly Patient Outcomes; Patient Safety and Patient Experience Reports, if available, plus any issues of Concern raised by BCCG. The Report also includes any internal or external reviews; national data published in the quarter and updates on any live CQC Action plans. Below is a summary of the Key Issues within the report and discussed at the Quality Assurance Subcommittee. KEY ISSUES: Kings
• Elderly Care & Dementia: The Trust confirms that all patients 75+ are screened for dementia/delirium. Both sites have clinical leads for dementia; specialist dementia wards and specific old age psychiatric liaison. Of concern is the fact that DH is supported by 3 WTE specialist nurses, however, despite the PRUH’s elderly population this site only has 1WTE specialist nurse (currently under recruitment). Therefore the PRUH are struggling to achieve the target for identification of cases
• Workforce: Reduction in agency spend across the Trust in this period. Physician assistant posts being rolled out at PRUH (already in place at DH) Medical vacancies at PRUH 20% and DH 1.5% - this stark difference has been questioned at CQRG.
• Quality Issues: Complaints: response rates challenged with KCH by BCCG Director of Governance Cancer of Unknown Primary: Notification of Concern letter re non-adherence to NICE guidance
Clinical Chair: Dr Andrew Parson 1 Chief Officer: Dr Angela Bhan
Fractured NOF: continued improvement Diagnostics Performance: Overall 99.27% of Bromley residents seen for diagnostics within 6 weeks (October 2016) – despite this BCCG continue to have concerns regarding MSK MRI turnaround times and shortage of Radiologists at PRUH.
• KCH Quality Alert Report: Bromley CCG remains highest reporters of QAs • Cancer: PRUH below target at 90.8% (mainly skin and colorectal). Gynaecology
referrals at PRUH increased by over 26% and Trustwide +26% for skin tumours. Contract leads reviewing with Trust.
Oxleas
• CQC Update: Update on Action plan provided in Easy-Read format • Early Intervention in Psychosis (EIP): Trust delivering Part 1 of the Standard in all 3
boroughs (target >50%). Out of the 8 audit standards Oxleas are not meeting 3: 14 day access; physical health screening and offering physical health interventions e.g. smoking cessation Green Parks House Enquiry: Action plan developed in line with recommendations
• Workforce: Overall vacancy rate of 13% (April-October 2016) but vacancies for Band 5 nurses 17% (in line with Londonwide picture)
• Mortality Surveillance Update: Mortality Surveillance Committee in place to review all deaths and identify learning. Audit completed and ongoing work outlined
• Quality Issues: Concern re patients being held within ED until a bed is available following CQC recommendations Provision of mental health ‘specials’ continues to be discussed between KCH and Oxleas Following 3 borough Directors writing to express concerns regarding data and quality of Serious Incident process the Trust has responded and this is being considered in January 17.
Bromley Healthcare • All 3 CQRGs in this period were truncated due to CQC inspections. • Bladder and Bowel service outlined service developments and challenges: of note
considerable increase in caseload; aim to reduce waiting times from 10 weeks to 28 days and creation of a user group.
• CQC inspections at Global House; Lauriston House and Beckenham Beacon during this period. CQC reports awaited.
Other Providers
• Greenbrook quality metrics and reporting template agreed and in use complimented by themed analyses on a monthly basis. Quality Assurance Sub-Committee received an example of reports.
• BMI – CCG/CSU discussions underway regarding responsibilities in relation to quality monitoring at local BMI sites
• LAS monthly report highlighted one SI in November relating to a Bromley resident
Clinical Chair: Dr Andrew Parson 2 Chief Officer: Dr Angela Bhan
COMMITTEE INVOLVEMENT: • Quality Assurance Subcommittee RECOMMENDATIONS: The Governing Body is asked to:- • Note the report. ACRONYMS QAS – Quality Assurance Sub-Committee IGC – Integrated Governance Committee DIRECTORS CONTACT: Name: Sonia Colwill E-Mail: [email protected] AUTHOR CONTACT: Name: Gill Holden E-Mail: [email protected] Telephone: 01689 866548 GP CLINICAL LEAD: Name: Dr M Selby
Clinical Chair: Dr Andrew Parson 3 Chief Officer: Dr Angela Bhan
Narrative Quality Report
Quarter 3 2016/17 October-December 2016
Authors
Gill Holden Patient Safety, Governance, Risk & Quality Lead Sonia Colwill Director of Quality, Governance & Patient Safety
1

Introduction
Bromley CCG is responsible for ensuring providers deliver safe, high quality, clinically effective services, whilst providing patients with the most positive experience possible.
The larger providers are required to attend a Clinical Quality Review Group (CQRG) run by the CCG and, in Bromley, supported by the South East Commissioning Support Unit (SECSU) for acute providers. The CQRG is responsible for receiving data and information from the Trust for scrutiny, challenge and assurance. This information is triangulated with information available to the CCG about the provider in the form of complaints; themes via our Quality alert system and also with soft intelligence from patient feedback or through external agencies eg Healthwatch. External scrutiny is provided through CQC and NHS Improvement.
The Quarterly Quality Report provides a narrative update on the most up to date position with regards to quality assurance and issues of concern at the end of the quarter. In some instances comparisons over time are included as appropriate. Whilst 3 months data is provided this may not be for the full current quarter: the quantifiable data reflects the most recent available.
Provider Reports Kings College Hospital (PRUH)
The information provided relates to the PRUH and Bromley KCH sites (including Queen Mary’s; Orpington; Beckenham Beacon) unless stipulated otherwise.
In Q3 2016/17 the CQRG (October and November) discussed the following as deep dive subjects:
• Respiratory/COPD • Elderly Care and Dementia • Medicines Management • Workforce
December 2016: Due to unforeseen circumstances this meeting was postponed until January 2017. Respiratory/COPD
The deep dive focussed on the Respiratory Service at DH. It was agreed that a report on this service at PRUH would come to Dec/Jan CQRG
Elderly Care & Dementia
All patients aged over 75 years admitted as emergencies to KCH sites are screened for dementia and delirium using the 4-AT screening tool which allows identification of cognitive problems and appropriate management (part of the National Dementia CQUIN and reported on by the Trust).
• The clinical teams at both sites have different models of care for patients with dementia
• both sites have clinical leads for dementia and delirium • both sites have dementia specialist wards.
2

• both sites have specific old age psychiatric liaison
This is supported by 3 WTE dementia specialist nurses at DH and previously 1 WTE dementia specialist nurse at PRUH (currently being recruited to). PRUH have struggled to achieve the target for identification but have continued to achieve the investigation and follow up of patients. Outpatient memory services for the PRUH are delivered within the community as part of older persons mental health services.
Mental Capacity: There is clear Trust guidance, policy and resources
Patient Engagement: • There is a Trust-wide Older Person’s Committee with non-executive governor. • There are annual public forums which allow patient, carer and local service
engagement and feedback. • The Trust conducts monthly dementia carer surveys. • All clinical staff undergo mandatory dementia and delirium training and a rolling
training programme to include foundation doctors across both sites. • There is a multidisciplinary training programme which incorporates dementia friends
training and simulation training. • In May 2016 the Trust completed a year-long “Train the Trainers” dementia and
delirium training programme with HESL monies on the PRUH site that trained 78 clinical staff with a bespoke 1 day training programme which would allow staff to train staff in their clinical area on dementia and delirium awareness and be dementia and delirium champions (a further 106 staff trained).
• All patients with dementia have a “This is me” document completed with the help of their carer to help staff deliver patient centred care.
• The Trust has implemented ‘John’s campaign’ which gives relatives and carers the right to visit and help provide support and care for their relatives in hospital.
• Work is supported by carer passports, posters and a carers resource page for staff on the Trust intranet.
Learning from Incidents: • The Trust ensure that staff have support and training to deliver care to patients with
dementia and manage behaviours that might challenge. • Inappropriate antipsychotic use in patients with dementia is reviewed through audit
(locally collected data presented nationally at British Geriatrics Society) and data from National Dementia Audit demonstrates low level of antipsychotic drug use.
• Use of high fidelity simulation programmes in the Trust helps improve care of patients with acute mental and physical health disorders.
Facilitating and promoting functional independence for in-patients with dementia: • Use of patient centred care plans including “This is me” and involving family and
friends (John’s campaign). • Ensuring timely discharge from hospital and access to intermediate care and
community services to facilitate this.
Update on recruitment of community geriatricians and developing the Frailty Unit at Orpington: Joint working with Bromley CCG, together with specific funding, has led to development of two ward areas on the Orpington site specifically for frailer patients. The 38 beds/chairs in this unit are on schedule to open in January 2017. They will provide both step-down beds and step-up beds/chairs. This unit is designed to provide medical, nursing and therapy
3

support for patients whose needs are not best met in the acute hospital or in their own homes. Medicines Management The Trust gave a detailed presentation re January-September 2016. The highlights for PRUH were: Incidents:
• No Never Events in Medicines Management • 10 fold- errors
o 7 prescribing o 6 administration o 3 dispensing o 1 information o 1 other
• Contraindicated due to allergies: 8 incidents (DH reporting 25 incidents) • Omissions are the most commonly reported incident type: 246/1562 (188 @DH) • 9/19 harms arising from Omissions: most commonly associated with patient harm
Re: Oxygen performance commissioners noted that performance was below the national average although the data was relatively old so this position may not reflect current performance. Bromley CCG queried PRUH oxygen performance. Trust noted that oxygen prescribing performance has improved and is better at the PRUH than DH although exact figures were not available at the meeting
The Chief Pharmacist at DH has confirmed that he is at PRUH site 2 days per week
Patient Satisfaction: • 5 formal complaints: four via quality alerts.
o 4 relating to discharge prescriptions, o 1 relating to an outpatient.
No recent Outpatient satisfaction survey completed at the PRUH. Next is due Jan 2017. Workforce The presented report was not finalised due to internal miscommunication about the requirements. The Trust made a commitment to submit a completed in January 2017 that fully meets the commissioner specification. Commissioners noted some areas for detailed discussion including data on vacancy rates and reduction trajectories.
• The Trust noted reductions in agency spend for the Trust in the last 2-3 months. • Overseas recruitment: It was noted that overseas nurse recruitment represents a
small proportion of overall trust nursing recruitment: now there is clarity around the Home Office recruitment process there will be adequate time built into any overseas recruitment initiative.
• Commissioners queried ‘hotspot’ vacancy areas, including clinical scientists. • The Trust noted medic ‘hotspot’ vacancy areas are being looked at including
radiographers and clinical scientists. • Medical Vacancies: differential between PRUH (c.20%) and DH (c.1.5%) vacancy
rates is very stark and concerning. Trust reps acknowledged that PRUH medical vacancy rate is concerning and described their plans to map/scope working and education patterns.
4
• Commissioners queried whether there is a ‘red shift’ risk assessment for medics as
well as nurses: Trust noted that this is being worked on but it will be a rota-based RAG system rather than the shift based one for nurses.
• The Trust noted that Physician assistant posts (Band 4) are being rolled out at the PRUH; they are already established at DH. Advanced nurse practitioners are also being looked at by the Trust.
QUALITY ISSUES: Quarter 3 2016/17
Complaints
The 2015/16 Patient Complaints Annual Report was received in October Kings Quality & Governance Committee. Of note:
• The Trust received 803 complaints (464 DH/339 PRUH) • 20% reduction in complaints at DH and 14 % reduction at Bromley sites • 10% increase in PALS contacts • End of Year performance in responding to complaints within 25 working days = 45% • 2% of complaints were referred to the Ombudsman
The Director of Quality & Governance is writing to the Director of Nursing to request an improvement plan around response rates.
Maternal Death Review
KCH commissioned St George’s to conduct an external review following 4 deaths of patients cared for at KCH during 2015. All cases were DH based and 3 of the 4 cases were tertiary referrals. The CCG, via the GP Quality Lead for Maternity and the Senior Commissioning Manager, were involved in the discussions regarding the findings with Kings. The conclusion was that there were no consistent threads to suggest systemic issues with regards to maternity care at KCH.
Cancer of Unknown Primary (CUP) External Review
October CQRG was advised of a Notification of Risk letter received from NHSE Quality Surveillance Team outlining the following:
Immediate Risk There is no designated CUP MDT in place which does not comply with NICE guidance or the Manual of Cancer Services. In addition named CUP staff who undertake initial assessments are not core members of MDT. This is likely to lead to significant delays in the patient pathway and have an adverse outcome for these patients.
Serious Concern The CUP at PRUH does not have robust or sustainable cover arrangements in place.
This notification was discussed and the Trust response/actionplan noted. The Trust indicated that this relates to a small number of patients and provided reassurance that these patients are being tracked. The Trust will include a stocktake on CUP issues Cancer is discussed as a main agenda item in 2017.
KCH Fractured Neck of Femur Update – November 2016
• Continued Improvement
5

• PRUH and DH results indicate how the sustained effects of cohorting patients,
prioritising surgery and a condition-based approach have had a positive impact on patient outcomes
• KCH now ranks favourable with regards to SHMI, hours to surgery and 30 day mortality rate
• Despite shorter length of stay readmission rates are low
6

7
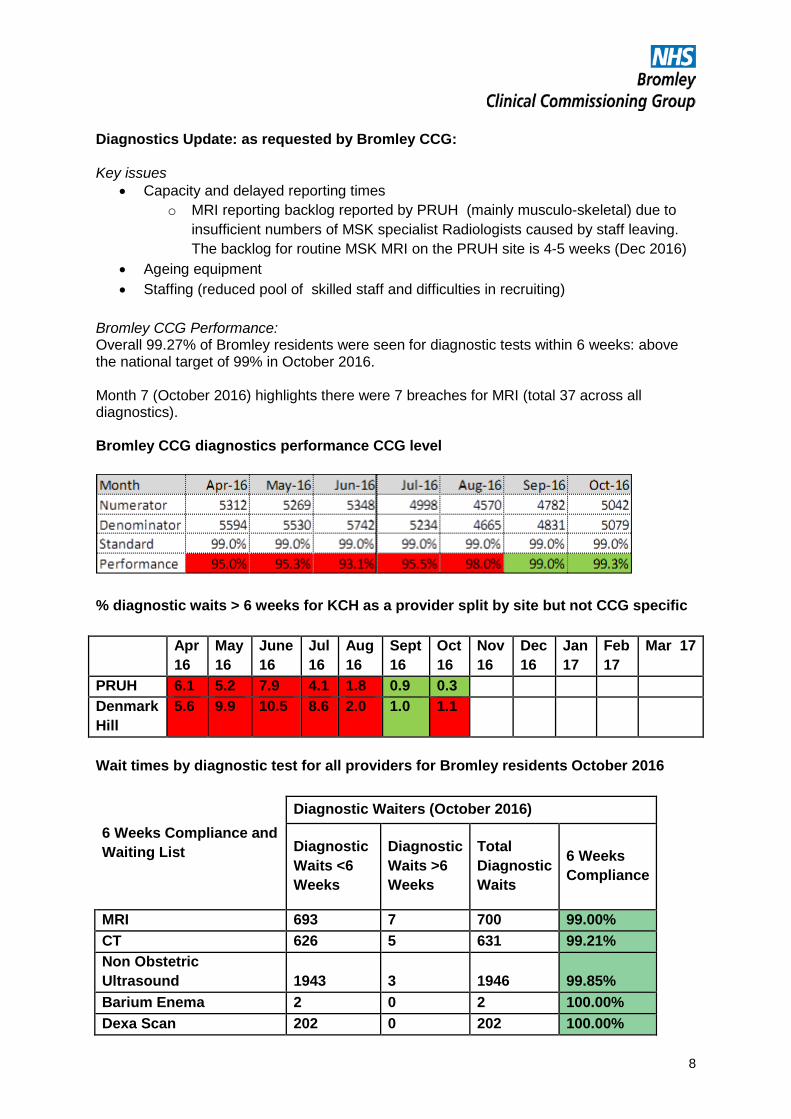
Diagnostics Update: as requested by Bromley CCG: Key issues
• Capacity and delayed reporting times o MRI reporting backlog reported by PRUH (mainly musculo-skeletal) due to
insufficient numbers of MSK specialist Radiologists caused by staff leaving. The backlog for routine MSK MRI on the PRUH site is 4-5 weeks (Dec 2016)
• Ageing equipment • Staffing (reduced pool of skilled staff and difficulties in recruiting)
Bromley CCG Performance: Overall 99.27% of Bromley residents were seen for diagnostic tests within 6 weeks: above the national target of 99% in October 2016. Month 7 (October 2016) highlights there were 7 breaches for MRI (total 37 across all diagnostics). Bromley CCG diagnostics performance CCG level
% diagnostic waits > 6 weeks for KCH as a provider split by site but not CCG specific Apr
16 May 16
June 16
Jul 16
Aug 16
Sept 16
Oct 16
Nov 16
Dec 16
Jan 17
Feb 17
Mar 17
PRUH 6.1 5.2 7.9 4.1 1.8 0.9 0.3 Denmark Hill
5.6 9.9 10.5 8.6 2.0 1.0 1.1
Wait times by diagnostic test for all providers for Bromley residents October 2016
Diagnostic Waiters (October 2016)
6 Weeks Compliance and Waiting List Diagnostic
Waits <6 Weeks
Diagnostic Waits >6 Weeks
Total Diagnostic Waits
6 Weeks Compliance
MRI 693 7 700 99.00% CT 626 5 631 99.21% Non Obstetric Ultrasound 1943 3 1946 99.85% Barium Enema 2 0 2 100.00% Dexa Scan 202 0 202 100.00%
8
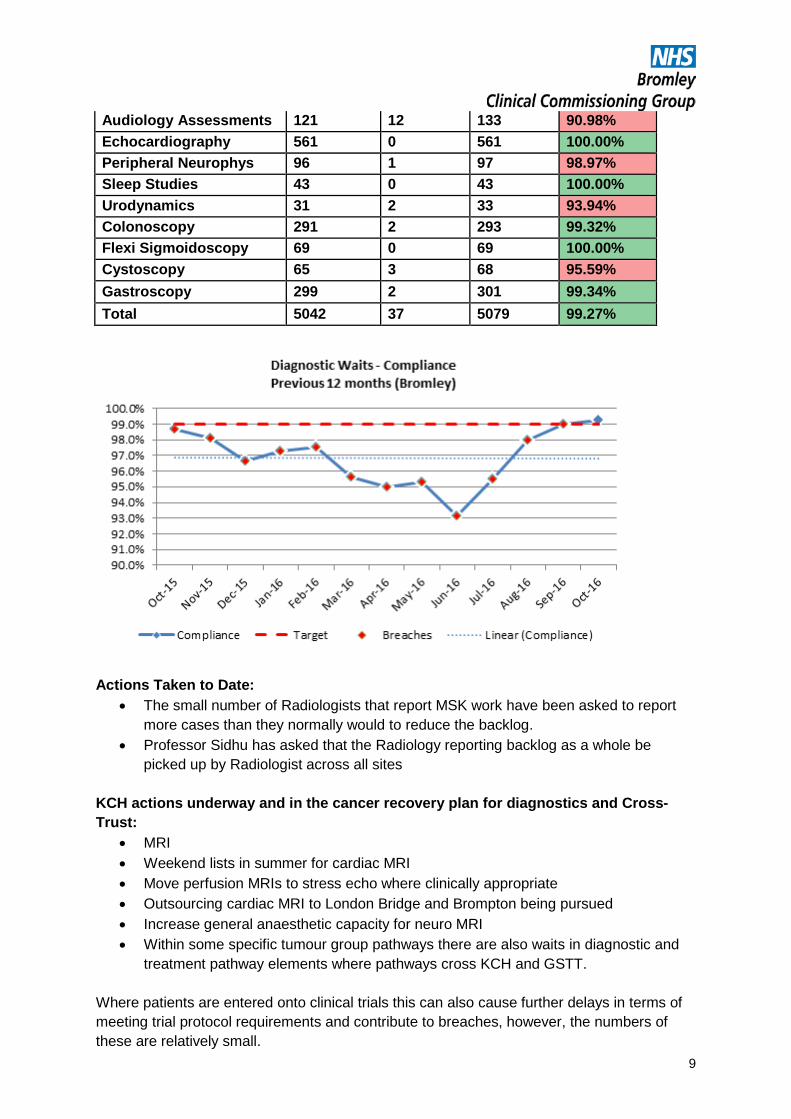
Audiology Assessments 121 12 133 90.98% Echocardiography 561 0 561 100.00% Peripheral Neurophys 96 1 97 98.97% Sleep Studies 43 0 43 100.00% Urodynamics 31 2 33 93.94% Colonoscopy 291 2 293 99.32% Flexi Sigmoidoscopy 69 0 69 100.00% Cystoscopy 65 3 68 95.59% Gastroscopy 299 2 301 99.34% Total 5042 37 5079 99.27%
Actions Taken to Date:
• The small number of Radiologists that report MSK work have been asked to report more cases than they normally would to reduce the backlog.
• Professor Sidhu has asked that the Radiology reporting backlog as a whole be picked up by Radiologist across all sites
KCH actions underway and in the cancer recovery plan for diagnostics and Cross-Trust:
• MRI • Weekend lists in summer for cardiac MRI • Move perfusion MRIs to stress echo where clinically appropriate • Outsourcing cardiac MRI to London Bridge and Brompton being pursued • Increase general anaesthetic capacity for neuro MRI • Within some specific tumour group pathways there are also waits in diagnostic and
treatment pathway elements where pathways cross KCH and GSTT. Where patients are entered onto clinical trials this can also cause further delays in terms of meeting trial protocol requirements and contribute to breaches, however, the numbers of these are relatively small.
9

BCCG will continue to monitor this via the Contract Monitoring Board and CQRG Quality Alerts Report Q2 16/17 This was presented at the November CQRG. King’s has received 94 GP quality alerts in Q2 from Southwark, Lambeth & Bromley 65 of which were from Bromley Practices. BCCG has agreed to start the roll-out of reverse quality alerts in early 2017.
Planned Improvements as a result of QAs:
Discharge Communication • New electronic discharge notification is now live in the new Sunrise EPR; some
technical issues but the Trust has worked with GPs to resolve these as they arise.
4 6 6
21 21 21
1 6
2 2 2 8
2 4
12
5
0
10
20
30
40
50
60
201607 201608 201609
QAs raised July - September 2016
Bexley
Bromley
Greenwich
Lambeth
Lewisham
Southwark
1
28
3 1
3
8 4
2 5 6
2 1 3
1 1 3
1 2
9
1 3
1 2 3
0
5
10
15
20
25
30
Themes July - September 2016
Bromley
Lambeth
Southwark
10

• Recommendations for GPs: now in a separate bold box, reasons drugs stopped and
reasons drugs changed added, responsibility to arrange further tests and follow ups made clearer.
• ‘missing/unsent ‘eDNs’ will be performance managed. Reports will be sent out daily. This was delayed due to new EPR report generation issue.
• Wards that have the most ‘unsent’ eDN’s are visited to raise awareness. • Training session at junior doctors induction programme. Slide pack presentation and
guidance handout produced. Subsequent training sessions with GP involvement to be rolled out.
• PRUH ward visits to Medical/Surgical wards re: process management of unsent eDNs. Plan to attend PRUH sisters meeting to raise awareness.
• Reiterate the importance of sending eDNs for deceased patients. • Annual Discharge Marketplace Event taking place.
Other Plans
• Fitness for work certificates: GP update regarding fit notes added to October GP e-Newsletter. Process piloted with a small group of junior doctors first week of November. Training to be incorporated into the junior doctors’ teaching programme in the weeks beginning 7th and 14th November. Working in parallel with Clinical Leads to establish local processes and specialty/procedure- specific guidelines. Target roll out week beginning 28th November ahead of the December junior doctors change over.
• Consultant to Consultant referrals: guidance added to Trust Access Policy. The guidance is in-line with the requirements detailed in the NHS standard contract for hospitals for onward referrals. Guidance continues to be reiterated with clinical teams via email communication.
• Recent GP survey highlighted Cardiology as a priority for GP education event in March 17.
CQC Trust-wide Actionplan Update: 12 October 2016 (PRUH)
A progress report against the CQC Action Plan was shared at CQRG in October. It was noted that the CQC undertook an unannounced ‘revisit’ the previous week which appeared to be a follow up on the Trust’s previously agreed actions. The Trust advised that the revisit focused on action plan areas only with 3 CQC staff members attending. PRUH DNA Cardio Pulmonary Resuscitation was a focus of the visit (documentation availability and quality of the documentation) and RCAs relating to infections.
Emergency Department
ED Recovery Plan approved with NHSI, NHSE and CCGs. There are specific actions for PRUH with bed capacity being cross-site delivery. The Plan measures system performance with 3 areas of focus:
• Out of Hospital Care: Strengthen integrated working • In Hospital Care: Review and re-design of urgent care
pathway to optimise flow • Bed Capacity: Increase and reconfigure
This is underpinned by a 7 point ‘in-hospital’ actionplan for PRUH:
• Clean Sheet Re-design/patient flow
11
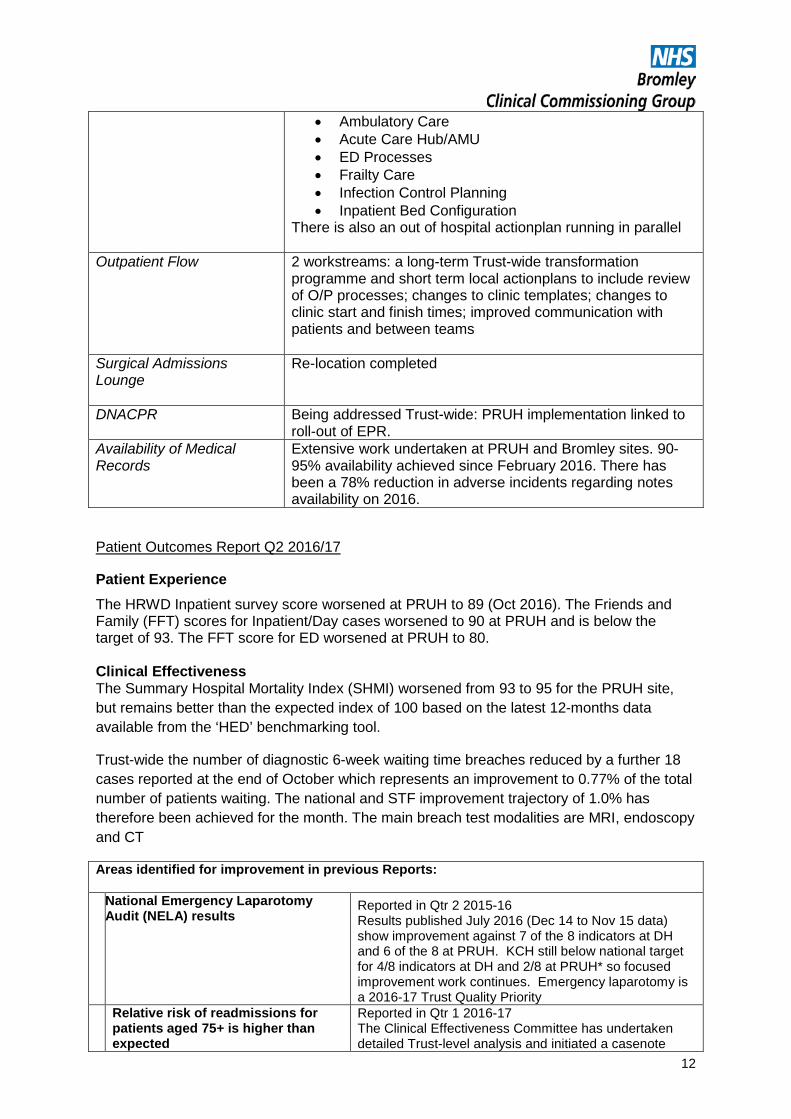
• Ambulatory Care • Acute Care Hub/AMU • ED Processes • Frailty Care • Infection Control Planning • Inpatient Bed Configuration
There is also an out of hospital actionplan running in parallel
Outpatient Flow
2 workstreams: a long-term Trust-wide transformation programme and short term local actionplans to include review of O/P processes; changes to clinic templates; changes to clinic start and finish times; improved communication with patients and between teams
Surgical Admissions Lounge
Re-location completed
DNACPR
Being addressed Trust-wide: PRUH implementation linked to roll-out of EPR.
Availability of Medical Records
Extensive work undertaken at PRUH and Bromley sites. 90-95% availability achieved since February 2016. There has been a 78% reduction in adverse incidents regarding notes availability on 2016.
Patient Outcomes Report Q2 2016/17
Patient Experience The HRWD Inpatient survey score worsened at PRUH to 89 (Oct 2016). The Friends and Family (FFT) scores for Inpatient/Day cases worsened to 90 at PRUH and is below the target of 93. The FFT score for ED worsened at PRUH to 80. Clinical Effectiveness The Summary Hospital Mortality Index (SHMI) worsened from 93 to 95 for the PRUH site, but remains better than the expected index of 100 based on the latest 12-months data available from the ‘HED’ benchmarking tool.
Trust-wide the number of diagnostic 6-week waiting time breaches reduced by a further 18 cases reported at the end of October which represents an improvement to 0.77% of the total number of patients waiting. The national and STF improvement trajectory of 1.0% has therefore been achieved for the month. The main breach test modalities are MRI, endoscopy and CT
Areas identified for improvement in previous Reports: National Emergency Laparotomy
Audit (NELA) results Reported in Qtr 2 2015-16 Results published July 2016 (Dec 14 to Nov 15 data) show improvement against 7 of the 8 indicators at DH and 6 of the 8 at PRUH. KCH still below national target for 4/8 indicators at DH and 2/8 at PRUH* so focused improvement work continues. Emergency laparotomy is a 2016-17 Trust Quality Priority
Relative risk of readmissions for patients aged 75+ is higher than expected
Reported in Qtr 1 2016-17 The Clinical Effectiveness Committee has undertaken detailed Trust-level analysis and initiated a casenote
12
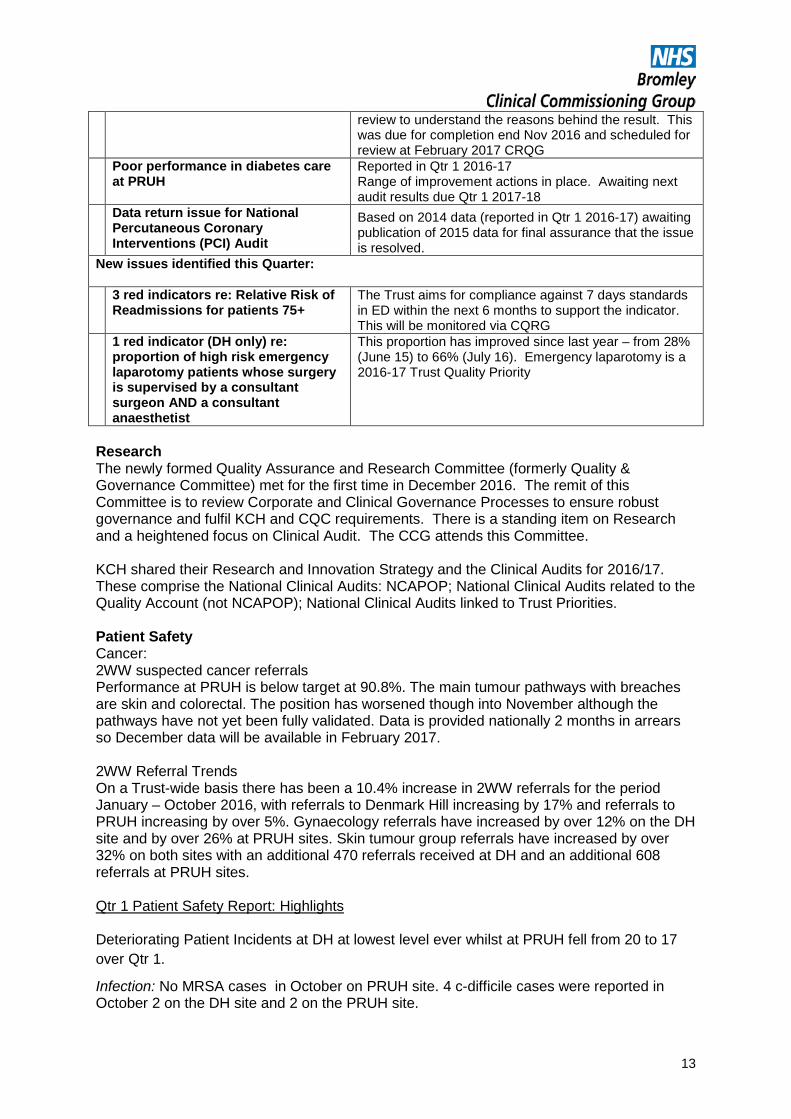
review to understand the reasons behind the result. This was due for completion end Nov 2016 and scheduled for review at February 2017 CRQG
Poor performance in diabetes care at PRUH
Reported in Qtr 1 2016-17 Range of improvement actions in place. Awaiting next audit results due Qtr 1 2017-18
Data return issue for National Percutaneous Coronary Interventions (PCI) Audit
Based on 2014 data (reported in Qtr 1 2016-17) awaiting publication of 2015 data for final assurance that the issue is resolved.
New issues identified this Quarter: 3 red indicators re: Relative Risk of
Readmissions for patients 75+ The Trust aims for compliance against 7 days standards in ED within the next 6 months to support the indicator. This will be monitored via CQRG
1 red indicator (DH only) re: proportion of high risk emergency laparotomy patients whose surgery is supervised by a consultant surgeon AND a consultant anaesthetist
This proportion has improved since last year – from 28% (June 15) to 66% (July 16). Emergency laparotomy is a 2016-17 Trust Quality Priority
Research The newly formed Quality Assurance and Research Committee (formerly Quality & Governance Committee) met for the first time in December 2016. The remit of this Committee is to review Corporate and Clinical Governance Processes to ensure robust governance and fulfil KCH and CQC requirements. There is a standing item on Research and a heightened focus on Clinical Audit. The CCG attends this Committee. KCH shared their Research and Innovation Strategy and the Clinical Audits for 2016/17. These comprise the National Clinical Audits: NCAPOP; National Clinical Audits related to the Quality Account (not NCAPOP); National Clinical Audits linked to Trust Priorities. Patient Safety Cancer: 2WW suspected cancer referrals Performance at PRUH is below target at 90.8%. The main tumour pathways with breaches are skin and colorectal. The position has worsened though into November although the pathways have not yet been fully validated. Data is provided nationally 2 months in arrears so December data will be available in February 2017. 2WW Referral Trends On a Trust-wide basis there has been a 10.4% increase in 2WW referrals for the period January – October 2016, with referrals to Denmark Hill increasing by 17% and referrals to PRUH increasing by over 5%. Gynaecology referrals have increased by over 12% on the DH site and by over 26% at PRUH sites. Skin tumour group referrals have increased by over 32% on both sites with an additional 470 referrals received at DH and an additional 608 referrals at PRUH sites. Qtr 1 Patient Safety Report: Highlights Deteriorating Patient Incidents at DH at lowest level ever whilst at PRUH fell from 20 to 17 over Qtr 1.
Infection: No MRSA cases in October on PRUH site. 4 c-difficile cases were reported in October 2 on the DH site and 2 on the PRUH site.
13

Hand Hygiene audits at PRUH have improved slightly to 86% in October but this is still below 95% target. The Director of Nursing at KCH has committed to improving this total.
Endoscopy: Criteria for sedation and GA in endoscopy being clarified cross-site. Risk assessment regarding the transfer of complex patients to DH undertaken until anaesthetic support is established at PRUH. This is being monitored via CQRG.
Staffing: Capacity in Neurosciences still significant challenge. Nursing and medical staffing shortages at PRUH stroke Unit.
Vacancy rate at PRUH was 14.7% in September 2016, however, no data was available for October. Particular vacancy pressures in Medical 5 and AMU wards (nursing)
Diagnostics: See above
Falls: 47 falls across CCU/M8 at PRUH April-September 2016 – this is being monitored via the Safer Care Group
Pressure Ulcers: Increase in Grade 3 PUs related to plaster casts at PRUH due to a shortage of permanent plaster technicians and lack of information for patients on taking action due to discomfort. This is being monitored via the Safer Care Group.
CTG (fetal) monitoring: The CCGs are awaiting a Deep Dive report on SIs (both DH and PRUH) where CTG monitoring is a contributory factor to the incident. There has been robust discussions at the Serious Incident Committees to which the CCG have contributed and this has led to immediate improvements in terms of guidance to staff and a revised training programme for nursing and medical staff, however, the formal actionplan will be shared with the CCGs by March 2017.
Oxleas
BCCG continues to work closely with Bexley and Greenwich CCGs around quality monitoring at Oxleas. In addition there is now a quality review as part of the Bromley contract monitoring process.
Oxleas CQC Inspection Update:
CQC Inspection of Oxleas Foundation trust was published in September 2016. Overall the Trust was rated as ‘requires improvement’. However, in the acute in-patient and psychiatric intensive care services the Trust was rated Inadequate
The final CQC action plans were submitted to the CQC on the 3rd of November 2016. Further detail on flow of patients in and out of the acute services has been requested by the CQC. A response was sent back on the 29th of November 2016. The CQC actionplan is monitored via CQRG monthly and the following Update was provided at CQRG in December.
14
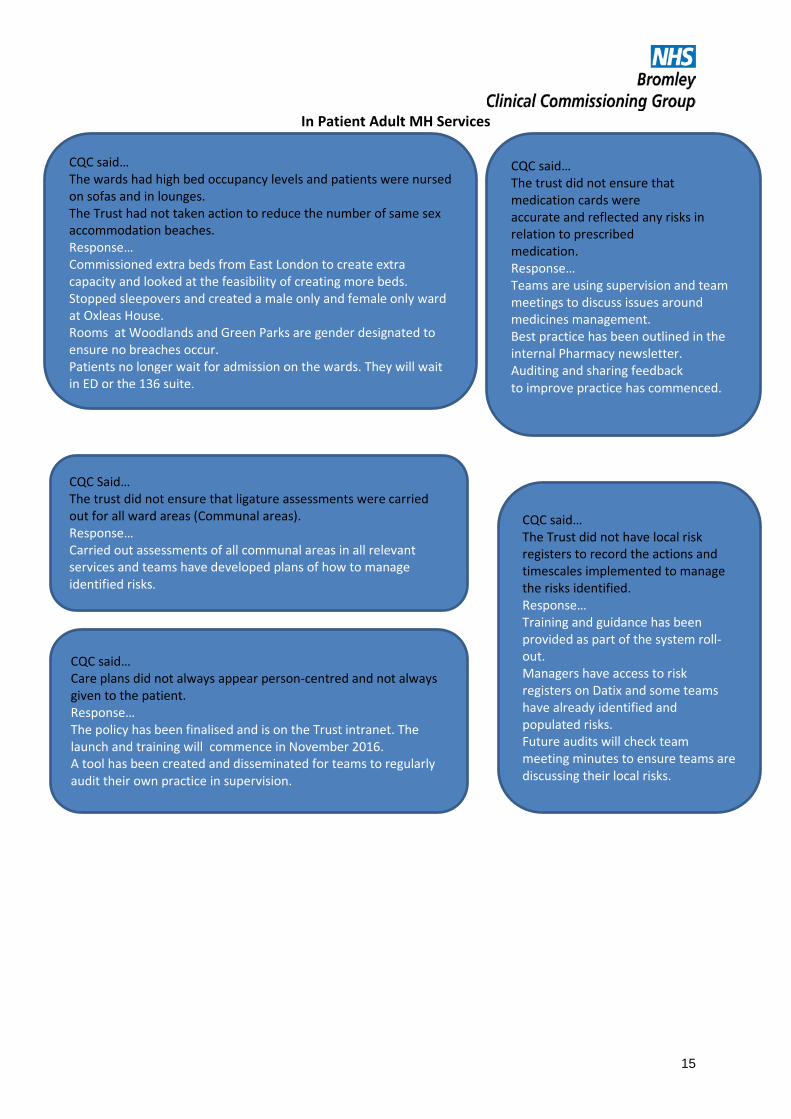
In Patient Adult MH Services
CQC said… The wards had high bed occupancy levels and patients were nursed on sofas and in lounges. The Trust had not taken action to reduce the number of same sex accommodation beaches. Response… Commissioned extra beds from East London to create extra capacity and looked at the feasibility of creating more beds. Stopped sleepovers and created a male only and female only ward at Oxleas House. Rooms at Woodlands and Green Parks are gender designated to ensure no breaches occur. Patients no longer wait for admission on the wards. They will wait in ED or the 136 suite.
CQC said… The trust did not ensure that medication cards were accurate and reflected any risks in relation to prescribed medication. Response… Teams are using supervision and team meetings to discuss issues around medicines management. Best practice has been outlined in the internal Pharmacy newsletter. Auditing and sharing feedback to improve practice has commenced.
CQC Said… The trust did not ensure that ligature assessments were carried out for all ward areas (Communal areas). Response… Carried out assessments of all communal areas in all relevant services and teams have developed plans of how to manage identified risks.
CQC said… The Trust did not have local risk registers to record the actions and timescales implemented to manage the risks identified. Response… Training and guidance has been provided as part of the system roll-out. Managers have access to risk registers on Datix and some teams have already identified and populated risks. Future audits will check team meeting minutes to ensure teams are discussing their local risks.
CQC said… Care plans did not always appear person-centred and not always given to the patient. Response… The policy has been finalised and is on the Trust intranet. The launch and training will commence in November 2016. A tool has been created and disseminated for teams to regularly audit their own practice in supervision.
15
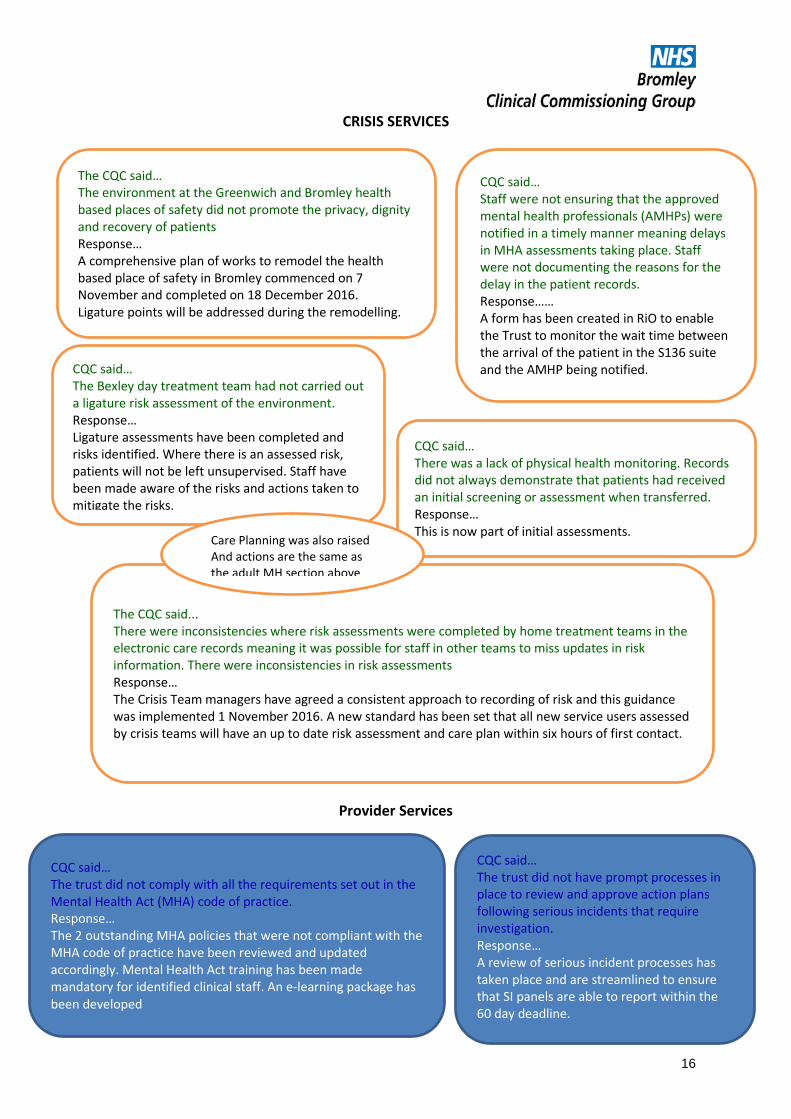
CRISIS SERVICES
Provider Services
The CQC said… The environment at the Greenwich and Bromley health based places of safety did not promote the privacy, dignity and recovery of patients Response… A comprehensive plan of works to remodel the health based place of safety in Bromley commenced on 7 November and completed on 18 December 2016. Ligature points will be addressed during the remodelling.
CQC said… The Bexley day treatment team had not carried out a ligature risk assessment of the environment. Response… Ligature assessments have been completed and risks identified. Where there is an assessed risk, patients will not be left unsupervised. Staff have been made aware of the risks and actions taken to mitigate the risks.
CQC said… Staff were not ensuring that the approved mental health professionals (AMHPs) were notified in a timely manner meaning delays in MHA assessments taking place. Staff were not documenting the reasons for the delay in the patient records. Response…… A form has been created in RiO to enable the Trust to monitor the wait time between the arrival of the patient in the S136 suite and the AMHP being notified.
The CQC said... There were inconsistencies where risk assessments were completed by home treatment teams in the electronic care records meaning it was possible for staff in other teams to miss updates in risk information. There were inconsistencies in risk assessments Response… The Crisis Team managers have agreed a consistent approach to recording of risk and this guidance was implemented 1 November 2016. A new standard has been set that all new service users assessed by crisis teams will have an up to date risk assessment and care plan within six hours of first contact.
CQC said… There was a lack of physical health monitoring. Records did not always demonstrate that patients had received an initial screening or assessment when transferred. Response… This is now part of initial assessments.
Care Planning was also raised And actions are the same as the adult MH section above
CQC said… The trust did not comply with all the requirements set out in the Mental Health Act (MHA) code of practice. Response… The 2 outstanding MHA policies that were not compliant with the MHA code of practice have been reviewed and updated accordingly. Mental Health Act training has been made mandatory for identified clinical staff. An e-learning package has been developed
CQC said… The trust did not have prompt processes in place to review and approve action plans following serious incidents that require investigation. Response… A review of serious incident processes has taken place and are streamlined to ensure that SI panels are able to report within the 60 day deadline.
16
CQRG Main Agenda items
The last 3 months CQRGs have focussed on:
• Service Presentation: Restraint, Sedation and Rapid Tranquillisation • Evaluation of Community Mental Health Redesign • Clinical Information Systems Improvements • EIP (Early Intervention in Psychosis) • Maternity Peri-Natal Mental Health Services (Bromley)
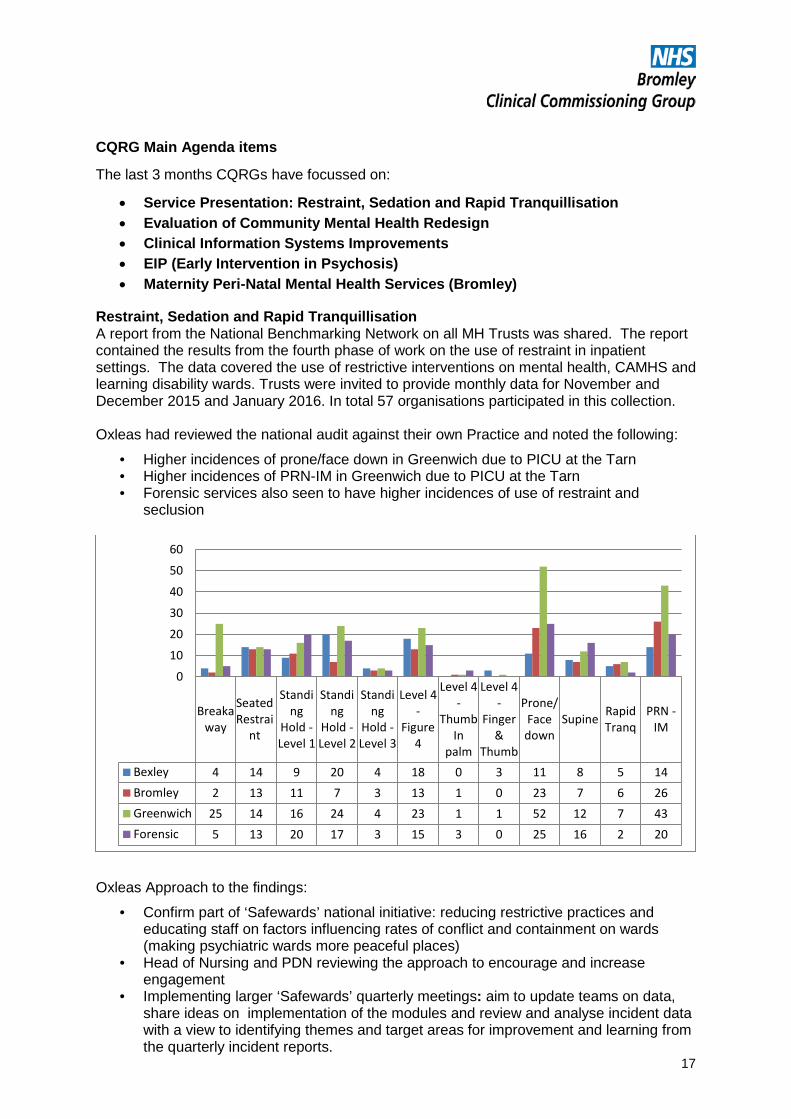
Restraint, Sedation and Rapid Tranquillisation A report from the National Benchmarking Network on all MH Trusts was shared. The report contained the results from the fourth phase of work on the use of restraint in inpatient settings. The data covered the use of restrictive interventions on mental health, CAMHS and learning disability wards. Trusts were invited to provide monthly data for November and December 2015 and January 2016. In total 57 organisations participated in this collection. Oxleas had reviewed the national audit against their own Practice and noted the following:
• Higher incidences of prone/face down in Greenwich due to PICU at the Tarn • Higher incidences of PRN-IM in Greenwich due to PICU at the Tarn • Forensic services also seen to have higher incidences of use of restraint and
seclusion
Oxleas Approach to the findings:
• Confirm part of ‘Safewards’ national initiative: reducing restrictive practices and educating staff on factors influencing rates of conflict and containment on wards (making psychiatric wards more peaceful places)
• Head of Nursing and PDN reviewing the approach to encourage and increase engagement
• Implementing larger ‘Safewards’ quarterly meetings: aim to update teams on data, share ideas on implementation of the modules and review and analyse incident data with a view to identifying themes and target areas for improvement and learning from the quarterly incident reports.
Breakaway
SeatedRestrai
nt
Standing
Hold -Level 1
Standing
Hold -Level 2
Standing
Hold -Level 3
Level 4-
Figure4
Level 4-
ThumbIn
palm
Level 4-
Finger&
Thumb
Prone/Facedown
Supine RapidTranq
PRN -IM
Bexley 4 14 9 20 4 18 0 3 11 8 5 14Bromley 2 13 11 7 3 13 1 0 23 7 6 26Greenwich 25 14 16 24 4 23 1 1 52 12 7 43Forensic 5 13 20 17 3 15 3 0 25 16 2 20
0
10
20
30
40
50
60
17
Evaluation of Community MH Redesign – Update The service redesign went live across all 3 boroughs in September 2015 with an overall aim to provide service users and patients with access to high quality care and support through better liaison with primary care and via dedicated care pathways offering quicker assessment and specialised support. A 12 month IPC support programme began November 2015 to work with the Trust to develop the outcomes evaluation framework. The programme, due to be completed by November 2016, will produce a final draft Service Delivery Plan; individual locality plans and an associated performance evaluation framework which can support the service to assess its progress against the original aims and objectives of the service re-design. An update is due at CQRG in February 17. Performance Evaluation Review: IPC also mapped the original aims and objectives with identified benefits and proposed monitoring measures. Through this work it was agreed service level objectives and priorities for the service would be distilled into 5 key service level objectives as follows:
• Ensure high quality support and treatment is delivered by highly skilled practitioners • Support service users to build resilience to manage their own health and wellbeing • Services to fully adopt a recovery culture for all service users • Staff to work as part of MDTs to provide expert support and interventions • To use resources efficiently to ensure sustainability of the service
Clinical Information System Improvements Infrastructure Investment:
• Wi-fi: available to staff at all Trust locations • Remote access via ipads • Managed Print Service: ‘Follow me’ printing plus significant savings • Migration to NHS mail 2: Improved functionality and cost savings • Continued Investment in Wide Area Network (WAN) • IT Helpdesk: Focus on customer service and immediate resolution of issues
Investment in New Technology:
• Rio- Integrated MH and Community system: Deployed to over 3500 staff. • Docman: Successfully deployed across BBG • Digital dictation: improve ‘turnaround’ time for correspondence • Mobile working: Trustwide rollout of iPads to > 1100 community clinicians • 2 clinical apps launched (MIA and SAF): Online/offline Rio to support mobile working • Care Connect: access to patient records across the borough of Greenwich & working
with Bromley CCG on Local Care record • Ifox: Real time reporting: Team dashboards, clinical tasklists, activity/performance
reports and bed management reports 1700 users Next Steps: Implementation of SEL STP Digital Roadmap plus
• Improved resilience and availability of IT infrastructure • Provide staff access to performance information they need in their roles • Support staff to make the best use of the data/technology available • Ensure staff have skills and training to make the most of new technology • Improved resource Management/productivity • Greater patient engagement and digital interaction
18
Early Intervention in Psychosis (EIP) Presentation
October 2014 announcement by DH of new standards in EIP: “Achieving Better Access to Mental Health Services by 2020”.
• Go live 1st April 2016. • 2 part standard
o delivering timely care (14 day RTT target to assess and allocate patients within EIP)
o followed by: delivering NICE concordant care • Target is to achieve >50% against the standard • Pathway is ageless (although interpreted to 65)
Oxleas Performance: Part 1:
• Develop a dashboard on Ifox; since January 16 submitting monthly UNIFY reports • Oxleas are meeting more than 50% in all 3 Boroughs
Part 2: • Assessed by Royal College of Psychiatrist Centre for Quality Improvement (CCQI)
using a National audit in December 2015 • Re-audit submitted to CCQI on 30 September 2016
Data Summary:
• Oxleas returned 49 cases after data cleansing from the 3 Adult EIP teams plus a service level report for each team
• Out of the 8 audit standards Oxleas performed better than the National average for all but the 14 day waiting time target (National 33% Oxleas 31%)
• In December 2015 Oxleas meeting 5/8 of the standards
Not achieving: • 14 day access/RTT • Physical health screening • Offering physical health interventions where indicated
Next Steps: • Embed ‘wellbeing’ within EIP • Facilitated 4 patient focus groups and are working closely with the Trust PEG and the
Greenwich Institute of Integrated Care. • Hoping to run a clinical trial (RCT) looking at the use or ‘wearable technology’
(Fitbits) in conjunction with an 8 week intensive lifestyle/wellbeing/physical health program.
• Re-audit which included CAMHS was submitted on 30 September and results awaited.
• Oxleas has good representation at London-wide EIP groups • On-going training being offered by HEE particularly extending this offer into CAMHS
Maternity Peri-Natal MH Services (Bromley)
Bromley CCG commissioned service from July 2016
Designed to focus on:
19

• Integrated care and multiagency partnership working • Early detection and prediction of risk and promotion of mental health and wellbeing • Rapid access to intervention • Access to perinatal psychological therapies • Parity of physical health and mental health care
Interventions provided:
• Specialist assessment of mental health • Specialist assessment of mother and infant attachment • Preconception counselling for woman planning a pregnancy with previous mental
illness during the perinatal period. • Medication reviews • Perinatal psycho education and therapeutic engagement • Psychosocial & Cognitive Behavioural Interventions • Attendance/input to safeguarding meetings
Qtr 1 data:
82% of Q1 cases seen within 14 days of referral 92% reported that their quality of life had improved as a result of the care and treatment. Automated referral form on GP EMIS system Focus on raising service profile across the Trust and other local agencies Green Parks House: Enquiry Actions Following 5 serious incidents in Green Parks House (GPH) in 2016 the Oxleas Board commissioned an independent review of clinical practice within the unit. The results of the review were presented to the Executive on 27 September 2016; to the Oxleas Board in November and to CQRG in December. The report identified a number of areas for review and improvement in relation to:
• Multi-disciplinary working, including a MDT formulation of each patient's condition • Care planning • Risk assessment and management • The involvement of families while their relative is on the ward • Ward leadership and ward round management
The executive established a 12 week quality improvement programme (QIP) in each unit to address the recommendations and progress will be reported to CQRG. Oxleas Workforce Report: December CQRG Supervision
20
The trust has been working to ensure that all staff receive supervision at least once every six weeks. The trust target is 80% compliance. This allows for a margin for annual leave, sickness, maternity leave etc. The performance against this target is detailed below April May June July August September October 88% 74% 82% 81% 75% 82% 83% Audits of the quality of supervision have been carried out for Nursing and AHPs. The audits have given strong assurance of the quality of supervision being delivered. This has been supported by evidence from staff surveys. Appraisal The trust requires all staff to be appraised on an annual basis with reviews throughout the year. All staff are RAG rated at their appraisal with those who are rated as RED being denied incremental progression if that were available. Appraisal is recorded on the trust learning system and as with appraisal this is monitored in real time. The target for compliance is 80%. April May June July August September October 93% 91% 91% 91% 91% 90% 90% Staff survey data has consistently demonstrated that Oxleas staff have one of the highest satisfaction scores with the quality of their appraisal compared with other mental health trusts. Vacancy and Recruitment Recruitment, particularly of nursing staff, continues to pose a significant and on-going challenge. Areas of greatest challenge are in recruiting band 5 nurses to prisons and adult mental health inpatient units. The trust has changed its recruitment practices to be more efficient for candidates and the trust. Saturday morning interviews for up to 50 candidates at a time have proven to be an effective means of encouraging candidate attendance. These Saturday morning recruitment events are now being run on a regular basis every month. At the beginning of the year the trust trialled an alternative pay offer for band 5 nursing staff whereby staff could chose to receive the employer pension contribution directly in lieu of membership of the NHS pension scheme. The scheme was adopted by a third of external applicants joining as a result of that campaign. There was considerable opposition from national trade union bodies to the approach and as a result the trust decided to close the scheme with a view to reviewing its impact. Oxleas is continuing to run campaigns for nursing staff and is working with the London Capital Nurse programme and locally with the University of Greenwich to streamline the entry of newly qualified nursing students into the workforce. In partnership with SLAM and South West London & St. George’s, Oxleas has been identified as a follow on implementer of the band 4 nurse associate role. These roles will be trained using the apprenticeship model and it is hoped will alleviate some of the recruitment difficulties relating to band 5 nursing staff.
21
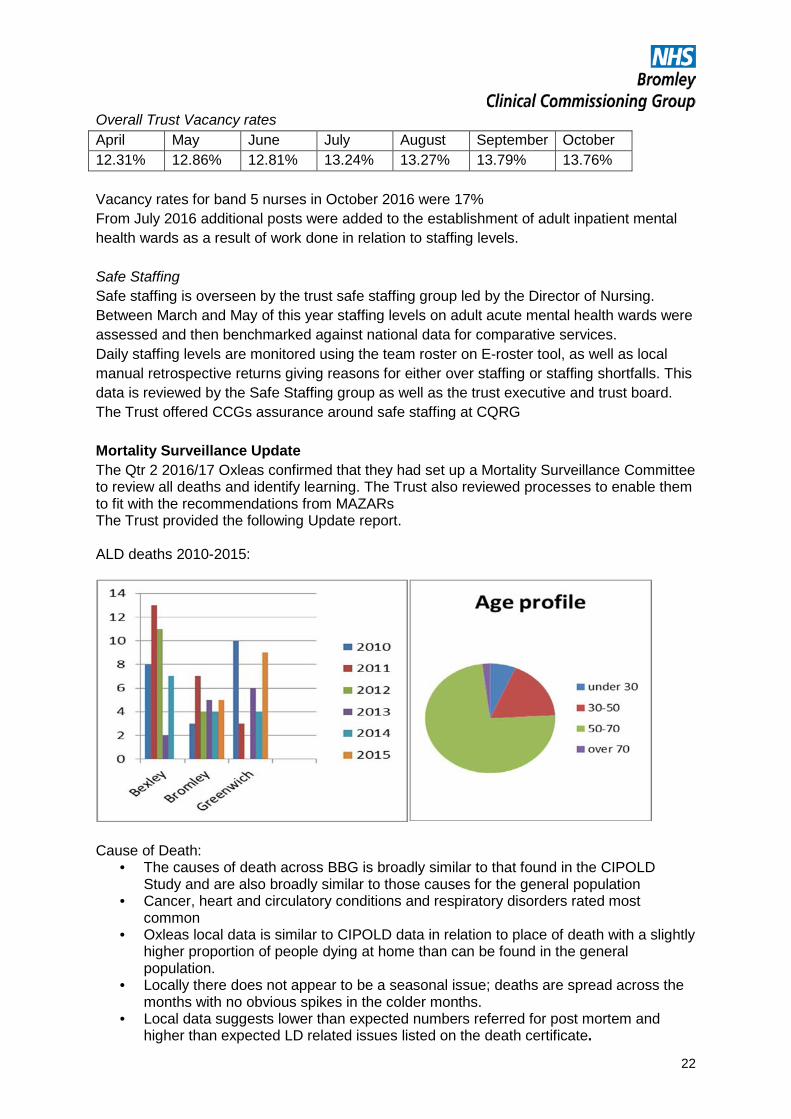
Overall Trust Vacancy rates April May June July August September October 12.31% 12.86% 12.81% 13.24% 13.27% 13.79% 13.76% Vacancy rates for band 5 nurses in October 2016 were 17% From July 2016 additional posts were added to the establishment of adult inpatient mental health wards as a result of work done in relation to staffing levels. Safe Staffing Safe staffing is overseen by the trust safe staffing group led by the Director of Nursing. Between March and May of this year staffing levels on adult acute mental health wards were assessed and then benchmarked against national data for comparative services. Daily staffing levels are monitored using the team roster on E-roster tool, as well as local manual retrospective returns giving reasons for either over staffing or staffing shortfalls. This data is reviewed by the Safe Staffing group as well as the trust executive and trust board. The Trust offered CCGs assurance around safe staffing at CQRG Mortality Surveillance Update The Qtr 2 2016/17 Oxleas confirmed that they had set up a Mortality Surveillance Committee to review all deaths and identify learning. The Trust also reviewed processes to enable them to fit with the recommendations from MAZARs The Trust provided the following Update report. ALD deaths 2010-2015:
Cause of Death:
• The causes of death across BBG is broadly similar to that found in the CIPOLD Study and are also broadly similar to those causes for the general population
• Cancer, heart and circulatory conditions and respiratory disorders rated most common
• Oxleas local data is similar to CIPOLD data in relation to place of death with a slightly higher proportion of people dying at home than can be found in the general population.
• Locally there does not appear to be a seasonal issue; deaths are spread across the months with no obvious spikes in the colder months.
• Local data suggests lower than expected numbers referred for post mortem and higher than expected LD related issues listed on the death certificate.
22
Age of Death:
• The cohort was 247 people for who the median age of death was 64 years. • Oxleas sampled over a longer time period and covered 3 London Boroughs with a
median age of 60 years. This remains higher than the average life expectancy of someone with a learning disability which stands at 57 but is still lower than for the general population where life expectancy currently stands at 78 for men and 83 for women.
• Within the local cohort there were 2 deaths of people deemed to be of a significantly old age for a person with LD: a 95 year old who died in Bromley in 2012 and a 91 year old who died in Greenwich in 2015.
• Oxleas have tried to identify if any local deaths would have been considered as premature using the same definition used by CIPOLD( “without a specific event that formed part of the pathway that led to death it was probable that the person would have lived for at least one more year”). Currently there is only one case in 2011 where this was considered to apply (not Bromley patient).
• Oxleas were assured that all of the deaths in younger people i.e. those under 30 years were exclusively service users who had multiple complex needs including life-limiting conditions that were well understood.
Oxleas Adult Learning Disability Mortality Reporting Process
• Death reported to Datix and ALD database • 2 mortality reviewers named as investigators on Datix • All ALD deaths are investigated • Report written and shared with teams • Monthly ALD report to Oxleas Committee and ALD PSG • On-going work with Local Authorities, SGVA groups and CCGs to develop multi-
agency processes Ongoing Work:
• Use of personal health profiles to maintain a person centred record of health needs • Acute liaison • Reducing avoidable admissions - this involves working intensively with people with
complex multiple needs to manage on going health issues and keep them out of hospital therefore reducing the risk of complications.
• Continue work around end of life care and DNACPR guidance including forward • Planning tool for people with life limiting conditions. • Nutrition: low weight is as much of a problem for LD as obesity. 17% of people with
an LD are thought to be underweight compared to 2% in the general population. Nurses are trained in enteral feeding and work closely with dietetics to ensure a healthy weight can be achieved and maintained.
• Downs Syndrome and dementia: there is a high prevalence of early onset dementia in people with Downs syndrome some diagnosed as early as their late thirties.
• Diagnostic overshadowing: this is huge challenge in the LD population especially with services users who challenge services and are nonverbal.
• Staff are vigilant for physical health issues being the rationale for an increase in challenging behaviours.
• Service Users admitted to a Mental Health bedded service receive a full physical health check.
There was no Qtr 3 2016/17 Quality Report tabled in this period.
Other Issues of Concern:
• Oxleas post-CQC inspection decision that patients requiring beds are held in ED until a bed is available. This has the potential for patients being kept in an unsuitable
23
environment leading to safety concerns, poor patient satisfaction and pressures on ED and will be monitored.
• LD service: Oxleas advised that yeoman House is in the process of moving to QMH. Following a request by the CCG for a full Equality Impact Assessment to be undertaken Oxleas have shared this with commissioners and this is being discussed at the Performance and Quality meetings.
• Provision of MH ‘Specials’ to Kings: Oxleas have provided assurances that they will continue to support this function whilst financial arrangements are agreed and the Trust are continuing to explore options.
• The 3 Directors of Quality at Bromley, Bexley and Greenwich CCGs have written to Oxleas Medical Director to voice concerns regarding the quality serious incident investigation reports and poor data quality. The Trust has responded and this is being considered in January 2017.
Bromley Healthcare
In Qtr 3 the CQRG had truncated agendas due to CQC inspections in October/November/December and an extended focus on the MRT report in November. There was only one service deep dive: on the Bladder and Bowel Service in November. In addition the following reports were received during Qtr 3:
• MRT Q2 Report • Qtr 2 Patient Experience Report • Qtr 2: Quality Report
Deep Dive: Bladder & Bowel service (previously the Continence Service) The service provides:
• Assessments and treatment to patients (adults and children)with bladder or bowel symptoms
• 35 nurse led clinics per month around the borough (over 1/3rd self-referrals) +16 paediatric clinics
• A monthly joint paediatric clinic with Consultant • Support to HVs, DNs, Community Paediatrics and School Nursse with complex
patients seen in their own homes/ schools • Clinical leadership and training for internal and external staff on bladder and bowel
health/ catheterisations • Manage the operational service of assessment through to delivery/ monitoring budget
for pads which are delivered to approximately 2800 patients every 8-12 weeks
Service Improvements 2016/17:
• Implement centralised booking for all appointments • Develop community continence team to provide timely quality continence
assessments for housebound patients. • EMIS spring clean ie patients who never reply to “contact us”. Add read codes • Use of mobile EMIS for community team. • Patient agreed goals can be monitored
Patient Feedback:
24

Service Challenges:
• Administration support not fully effective at present; gap analysis after centralised appointments
• An increase in B&B caseload size (approx extra 2500) with new staff recruited • Deliver enuresis clinics from Oct 16 • Increased demand; 1in 10
What is Working Well:
• Reduced referrals to secondary care : 5% referred in 15/16 (41/738) • Integrated working with CCG, Consultants and GPs • Positive patient experience and feedback • Cost effective control on containment expenditure. 0.8% decrease on total spend
despite 9% increase in patients (14/15- 15/16) • Good networking regionally. Chair of SE Thames Bladder and Bowel Specialist
Nurse group/shared working.
Objectives for next 12 months:
• Move to a centralised booking system/ text • Reduce waiting times from 10 weeks to 28 days • Provide an effective community continence team working within each hub • Incorporate the enuresis service into Bladder and Bowel team • Complete and implement a continence formulary for GPs and nurses • Continuing to work with CCG and Urology to complete care pathways and integrated
care • Increase training throughout the Borough: internal/external • Implement TOMS across the service to give more accurate picture of patients’
progress. • Create a user group/support group
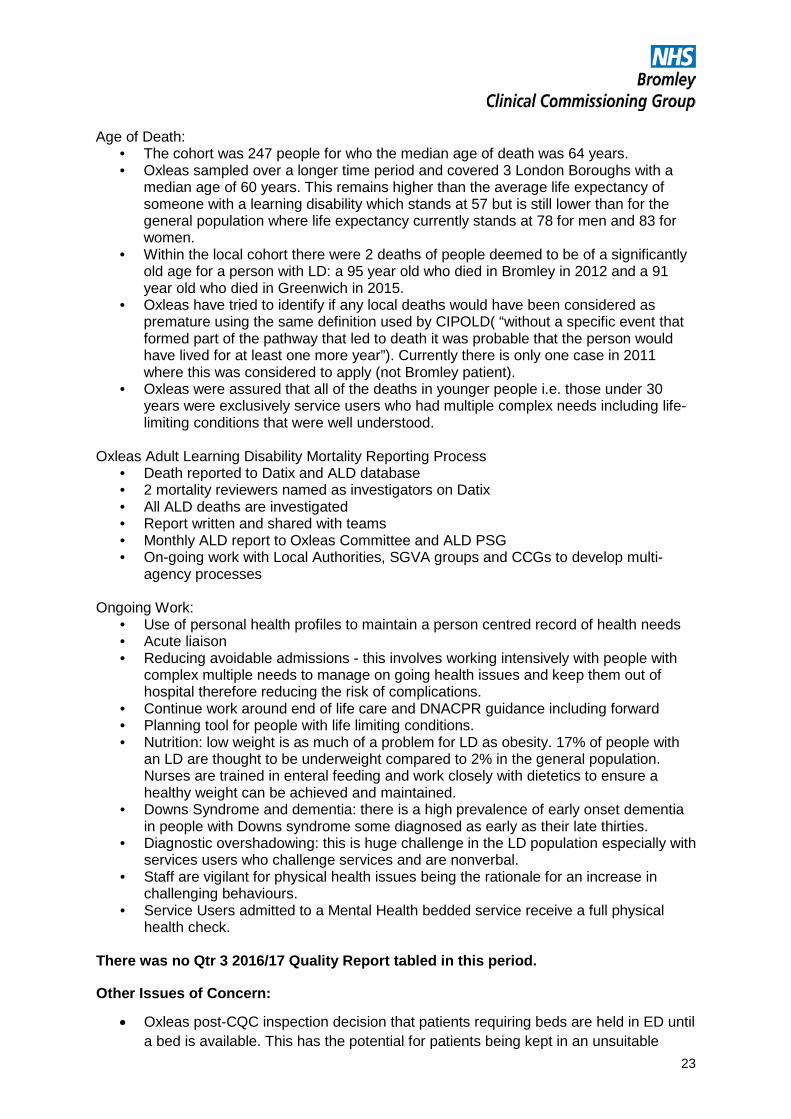
Qtr 2 Quality Report Patient Experience: BHC continues to perform strongly in the National FFT survey. Total responses received during August 2016 show that of the 196 responses 100% of clients were either likely or extremely likely to recommend BHC. Patient Opinion postings are also largely positive.
91.53%
8.47%
100% of our patients are extremely likely or likely to recommend B&B service to friends and
Report run from 1.4.15-31.3.16
Extremely likelyLikelyNeither likely nor unlikelyUnlikelyExtremely unlikelyDon't Know
25
Closed complaints and concerns upheld - 01 July 2016 - 30 September 2016 -
Type Total number Upheld Partially
upheld Not upheld Closed
unable to gain
consent
Information requested
but not provided
Jul-16 Complaints 4 50% 25% 0% 25% 0%
Aug-16 Complaints 4 25% 50% 25% 0% 0%
Sep-16 Complaints 3 75% 0% 25% 0% 0%
0100200300400500600700800
com
plai
nt
conc
ern
com
plim
ent
com
plai
nt
conc
ern
com
plim
ent
com
plai
nt
conc
ern
com
plim
ent
14/15 15/16 16/17
Summary of Feedback (closed)
Q4
Q3
Q2
Q1
0
1
2
3
Jul-16 Aug-16 Sep-16
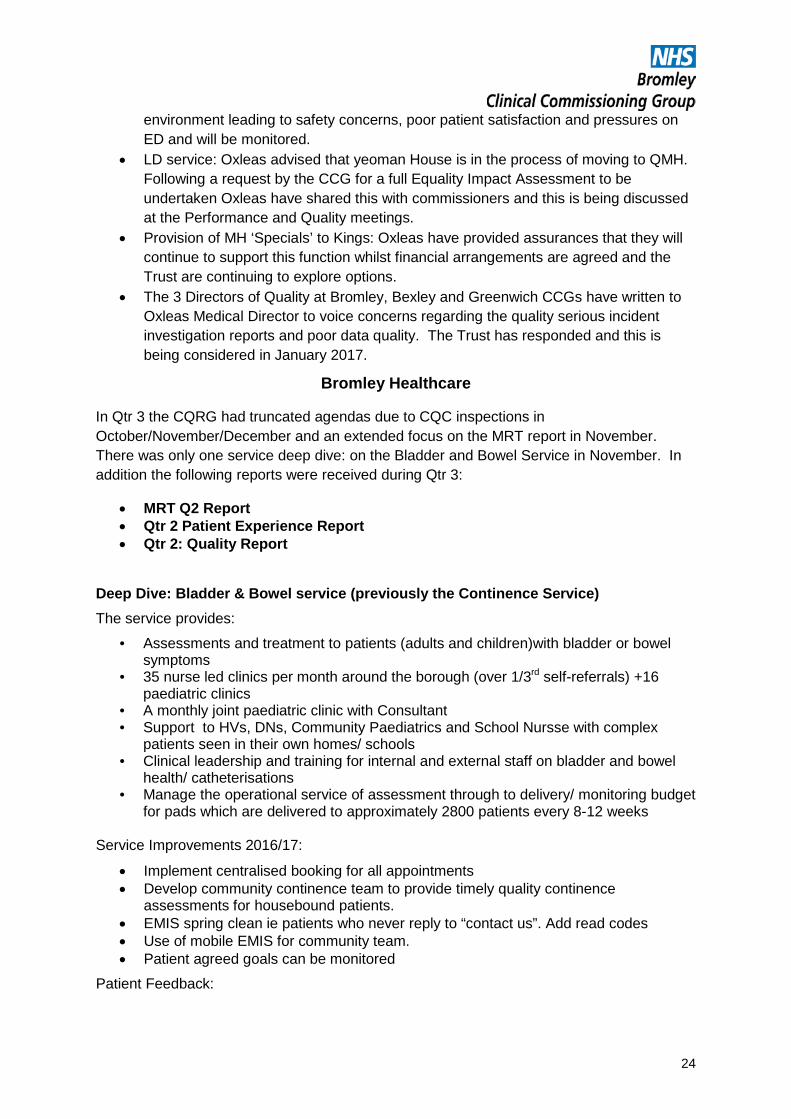
Subject of Closed Complaints, 1 July to 30 September 2016
Date for appointment
clinical treatment
Prescription
Discharge/care package
Aids/appliances/equipment
other
Communication (oral)
26
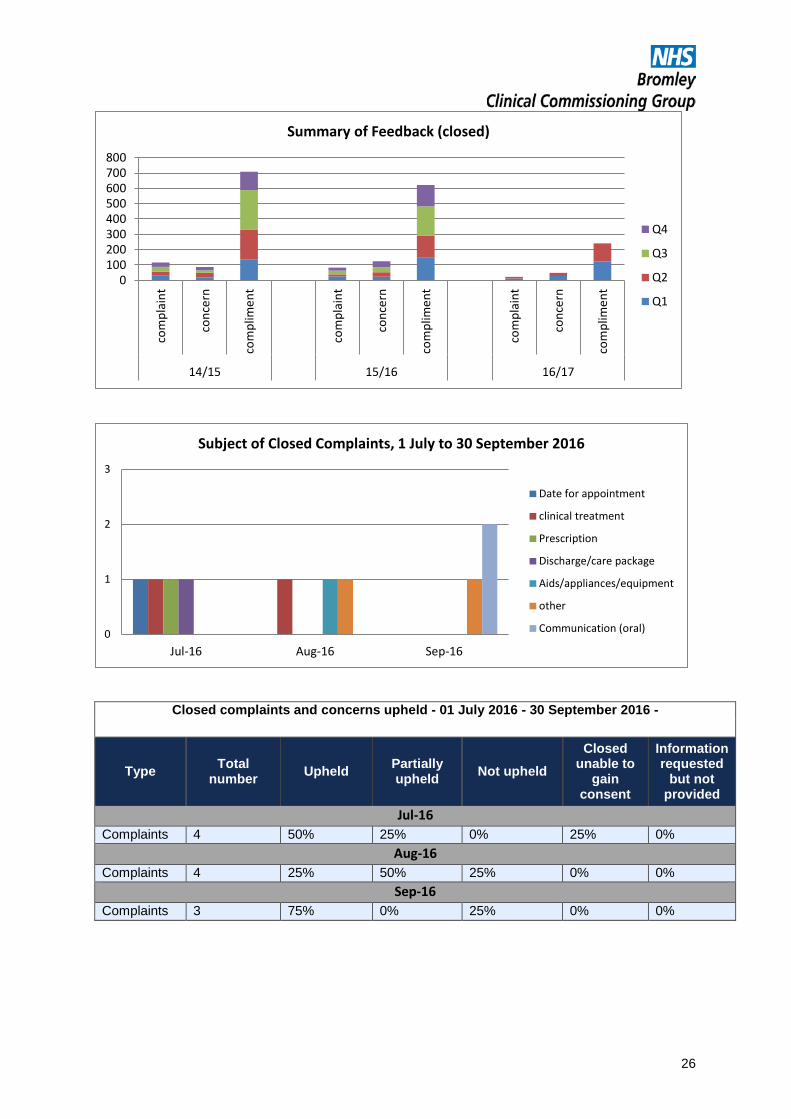
Patient Safety: Incidents:
Degree of harm
There is an overall increase in reporting no harm/low harms across the organisation.
Of note: from April 2016 infant child deaths have also been captured in the data as BHC is responsible (via the safeguarding children team) for gathering evidence of these deaths whether the child was in receipt of BHC services or not. There was one death in Quarter 2 in which a patient died within 24 hours of being discharged from PRUH. There were no concerns for BHC to investigate further.
Infection Control
There were no cases of MRSA or attributable cases of C Diff in this period. A patient who died at Lauriston House in December was discussed at the RCA review and the C diff was confirmed as community acquired, however, the report concluded that this was not contributory to the death. There have been no outbreaks within BHC bedded areas.
Other Issues The potential effect of re-procurement on staffing continues to be closely monitored via CQRG
Waiting times for housebound patients was noted and it was agreed there would be a presentation at next CQRG on this area.
The CCG was notified of inspections at:
• Global House (18/19 October) • Lauriston House (7 November) • Beckenham Beacon (13/14 December)
The CCG continue to liaise with BHC regarding the most appropriate mechanism for gaining assurance around quality of care.
27
Other Provider Exception Report
The Quality Assurance Sub-Committee has received a draft report on quality in BCCG’s other providers. Following discussion the Quality Team is in the process of re-drafting the quality report as directed by the committee and the revised template will be presented in January 2017. Quality Leads have been allocated to each workstream within Planned Care, Primary Care and each provider contract with the aim of supporting commissioning and contracting through service development, procurements and driving up quality within contract monitoring. It is proposed that all contract meetings should have a quality component on at least a quarterly basis going forward.
Community Procurement: The Quality Team are an integral part of the Procurement Working group and, in addition, a Consultant has been commissioned to undertake a validation of the quality components of the procurement. A report will be shared with the Quality Assurance Committee in February 2017.
Greenbrook Greenbrook and the CCG have agreed a quality report which will be submitted monthly. This will go to the Quality Assurance Sub-Committee for information in January 2017. Contract monitoring meetings have a quality component to review the reports and provide time for themed deep dives.
The CCG has been notified that Greenbrook UCC at Beckenham Beacon will be inspected by CQC in February 2017.
BMI Discussions are taking place between the CSU and the Director of Finance with regards to contract and quality monitoring of local BMI sites going forward. The Quality Assurance Sub-Committee will be informed of these arrangements once finalised LAS The CCG receive a Monthly SI report from LAS, however, this is only highlighted where a report has been received relating to a Bromley patient. The SI declared in November relating to a Bromley patient is as follows: 26/10/16: Patient pressed Careline button. Careline passed to LAS 00:16: categorised as unknown problem – C4 (Emergency Response Call). Approx. 2 hours later Paramedic 1 arrived and found patient in cardiac arrest already deceased for some time. Basic life support commenced. Paramedic 2 arrived 02.39; Advanced life support commenced. Recognition of Death 03.18.
LAS has advised that 2016/17 SI figures continue to be higher than 2015/16. For the financial year to end November 2016 LAS has declared 48% more SIs than the previous year.
Gill Holden Patient Safety, Quality & Risk Lead
28
Related Documents











