A longitudinal study of neurocognitive function in individuals at-risk for psychosis Richard S.E. Keefe a, ⁎ , Diana O. Perkins b , Hongbin Gu b , Robert B. Zipursky c , Bruce K. Christensen c , Jeffery A. Lieberman d a Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine, Durham, NC, USA b Department of Psychiatry, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA c Department of Psychiatry, University of Toronto School of Medicine, Toronto, ON, Canada d Department of Psychiatry, Columbia University School of Medicine, New York, NY, USA Received 15 March 2006; received in revised form 27 June 2006; accepted 28 June 2006 Available online 22 August 2006 Abstract Introduction: Clinically defined prodromal diagnostic criteria identify at-risk individuals with a 35–40% likelihood of developing a psychotic disorder within a year. The time course and predictive value of cognitive deficits in the development of psychosis has not been established. Methods: A comprehensive neurocognitive battery and clinical assessments were administered to 37 subjects meeting Criteria of Prodromal States (COPS) criteria for being at risk for psychosis, and two comparison groups: 59 first episode and 47 healthy subjects. Subjects were also evaluated at 6-month and 1-year follow-up periods. Primary analyses used a neurocognitive composite score derived from individual neurocognitive measures, including measures of vigilance, verbal memory, working memory, and processing speed. Results: At-risk subjects performed more poorly than healthy subjects (t = 2.93, P = 0.01), but better than first episode subjects (t = 4.72, p b 0.0001). At-risk subjects were particularly impaired on measures of vigilance and processing speed. Cognitive composite scores were significantly lower in at-risk subjects who progressed to psychosis (N = 11; z = - 1.2), while those at-risk subjects who did not progress to psychosis (N = 17) performed better (z = - 0.5), and not significantly different from controls. Poor CPT performance combined with better WAIS-R digit symbol performance predicted progression to psychosis. Severity of neurocognitive deficits was not related to duration of prodrome or to time to development of psychosis and neurocognitive function improved in all subjects except those who progressed to psychosis. Conclusion: Neurocognitive impairment emerges early in the course of psychotic illness. Performance on tests of neurocognition may prove to be an early risk predictor for subsequent development of psychotic disorders. © 2006 Elsevier B.V. All rights reserved. Keywords: Neurocognition; Prodrome; Psychosis; Schizophrenia; First episode; Development 1. Introduction Deficits in neurocognitive function are a core feature of schizophrenia. Almost all patients with schizophrenia have some degree of cognitive impairment compared to Schizophrenia Research 88 (2006) 26 – 35 www.elsevier.com/locate/schres ⁎ Corresponding author. Box 3270, Duke University Medical Center, Durham, NC 27710, USA. Tel.: +1 919 684 4306; fax: +1 919 684 2632. E-mail address: [email protected] (R.S.E. Keefe). 0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2006.06.041

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
88 (2006) 26–35www.elsevier.com/locate/schres
Schizophrenia Research
A longitudinal study of neurocognitive function in individualsat-risk for psychosis
Richard S.E. Keefe a,⁎, Diana O. Perkins b, Hongbin Gu b, Robert B. Zipursky c,Bruce K. Christensen c, Jeffery A. Lieberman d
a Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine, Durham, NC, USAb Department of Psychiatry, University of North Carolina at Chapel Hill, Chapel Hill, NC, USAc Department of Psychiatry, University of Toronto School of Medicine, Toronto, ON, Canadad Department of Psychiatry, Columbia University School of Medicine, New York, NY, USA
Received 15 March 2006; received in revised form 27 June 2006; accepted 28 June 2006Available online 22 August 2006
Abstract
Introduction: Clinically defined prodromal diagnostic criteria identify at-risk individuals with a 35–40% likelihood of developing apsychotic disorder within a year. The time course and predictive value of cognitive deficits in the development of psychosis has notbeen established.Methods: A comprehensive neurocognitive battery and clinical assessments were administered to 37 subjects meeting Criteria ofProdromal States (COPS) criteria for being at risk for psychosis, and two comparison groups: 59 first episode and 47 healthysubjects. Subjects were also evaluated at 6-month and 1-year follow-up periods. Primary analyses used a neurocognitive compositescore derived from individual neurocognitive measures, including measures of vigilance, verbal memory, working memory, andprocessing speed.Results: At-risk subjects performed more poorly than healthy subjects (t=2.93, P=0.01), but better than first episode subjects(t=4.72, pb0.0001). At-risk subjects were particularly impaired on measures of vigilance and processing speed. Cognitivecomposite scores were significantly lower in at-risk subjects who progressed to psychosis (N=11; z=−1.2), while those at-risksubjects who did not progress to psychosis (N=17) performed better (z=−0.5), and not significantly different from controls. PoorCPT performance combined with better WAIS-R digit symbol performance predicted progression to psychosis. Severity ofneurocognitive deficits was not related to duration of prodrome or to time to development of psychosis and neurocognitive functionimproved in all subjects except those who progressed to psychosis.Conclusion: Neurocognitive impairment emerges early in the course of psychotic illness. Performance on tests of neurocognitionmay prove to be an early risk predictor for subsequent development of psychotic disorders.© 2006 Elsevier B.V. All rights reserved.
Keywords: Neurocognition; Prodrome; Psychosis; Schizophrenia; First episode; Development
⁎ Corresponding author. Box 3270, Duke University MedicalCenter, Durham, NC 27710, USA. Tel.: +1 919 684 4306; fax: +1919 684 2632.
E-mail address: [email protected] (R.S.E. Keefe).
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.06.041
1. Introduction
Deficits in neurocognitive function are a core featureof schizophrenia. Almost all patients with schizophreniahave some degree of cognitive impairment compared to

27R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
the level of cognitive function that would be expected ofthem based upon premorbid factors (Keefe et al., 2005;Reichenberg et al., 2005). Neurocognitive impairment ispresent at first treatment contact and the severity of thesedeficits remains relatively stable over the lifetime courseof illness (Heaton et al., 2001).
The time course of the emergence of neurocognitivedeficits is not well understood. Prospective studies ofindividuals “at-risk” for schizophrenia defined as havingan affected first degree relative generally find cognitivefunctions, especially attention, in childhood to be lowerthan the general population (Cornblatt et al., 1999;Niemi et al., 2003). While academic performance inchildhood is not dramatically different for individualswho later develop schizophrenia compared to those whodo not, and future adult schizophrenia is not identifiablein children based on scholastic achievement, individualswho later develop schizophrenia demonstrate decline intheir academic performance from childhood to adoles-cence (Cannon et al., 1999, 2002; Fuller et al., 2002;Isohanni et al., 1998; Jones et al., 1994; Zammit et al.,2004). Young people identified as being at risk forpsychosis, and who develop psychosis as adults havebeen found to have IQ declines from baseline evaluationcompared to those at-risk subjects with no psychoticsymptoms (Cosway et al., 2000). Thus, available evi-dence suggests that at least some cognitive deficits arepresent premorbidly, but that there may be decline incognitive function and/or impairments in normal cogni-tive maturation with adolescence.
Prior to developing psychosis, about 85% of indi-viduals experience prodromal symptoms, which includesub-clinical attenuated positive symptoms, negative sym-ptoms, mood symptoms and increasing functional impair-ments (Yung and McGorry, 1996). There is preliminaryevidence that neurocognitive deficits may also be presentin individuals experiencing prodromal symptoms. Indi-viduals meeting criteria for prodromal symptoms (Milleret al., 2003) have been found to have deficits in vigilance,visual working memory, executive function and memorycompared with published norms from healthy individuals(Hawkins et al., 2004). Compared to healthy controls andpatients with schizophrenia, individuals at high risk forpsychosis based on subjective “basic symptoms” (Klos-terkotter et al., 2001) demonstrated impairments inattention, memory, and verbal fluency compared to heal-thy comparison subjects and better performance than theschizophrenia patients on all domains (Hambrecht et al.,2002). Particularly noteworthy are the deficits in olfactoryidentification and memory that may predict which at riskindividuals eventually progress to psychosis (Brewer etal., 2003; Brewer et al., 2005).
To better understand the neurocognitive deficits pres-ent in individuals at-risk for schizophrenia as defined bythe experience of attenuated sub-clinical psychotic sym-ptoms, we compared the performance of “at-risk”subjects to that of healthy subjects and subjects expe-riencing a first episode of psychosis using the samecomprehensive neurocognitive test battery. To evaluatethe onset and time course of cognitive deficits in schizo-phrenia we examined the one year course of neurocog-nitive function and the relationship of neurocognitivefunction with duration of prodrome and time to devel-opment of a psychotic disorder in individuals experi-encing symptoms meeting at-risk criteria for psychosis.We also determined whether in at-risk subjects the se-verity of neurocognitive deficits at study entry predicteddevelopment of a psychotic disorder during the 1-yearfollow-up period.
2. Method
2.1. Subjects
All study subjects were recruited from researchprograms at the University of North Carolina at ChapelHill, and the University of Toronto. Both sites estab-lished Prevention through Risk Management and Edu-cation (PRIME) Clinics, and at-risk subjects wererecruited through these clinical programs. Five of theat-risk subjects participating from the UNC site and allof the subjects participating from the Toronto site werealso participating in a randomized, double-blind placebocontrolled clinical trial of olanzapine to prevent devel-opment of psychosis (Lilly pharmaceutical protocolF1D-MC-HGGF). Placebo-treated patients were includ-ed in this report, but because antipsychotic treatmentmay reduce psychosis, risk data from those individualsreceiving olanzapine were included in the baseline ana-lyses only, before antipsychotic treatment had begun,and not included in the longitudinal analysis. At-risksubjects met the Criteria of Prodromal States (COPS), asevaluated using the Structured Interview for ProdromalSymptoms (SIPS) (Miller et al., 2003). All study sub-jects met Attenuated Positive Symptom State criteria,which included emergence or worsening over the pastyear of a non-psychotic disturbance of thought content,thought process, or perceptual abnormality. Baselinecognitive data were available for 37 at-risk subjects.Thirteen of the 32 untreated at-risk subjects progressedto psychosis during the yearlong follow-up period. Foursubjects developed schizophrenia, two schizoaffectivedisorder, five psychosis NOS, one delusional disorder,and one brief psychotic disorder. Baseline data from 12

28 R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
of the at-risk subjects were also included in a previouspublication (Hawkins et al., 2004).
Fifty-nine first episode subjects participated at theUNC and Toronto sites of a multi-center, double-blindplacebo controlled trial of olanzapine and haloperidol inthe treatment of first episode psychosis (Lilly protocolF1D-MC-HGDH). The multi-center treatment resultsfrom this study have been published previously (Keefeet al., 2004, 2006; Lieberman et al., 2003), including adescription of cognitive performance and treatment-re-lated changes. First episode subjects were between ages16 and 40, had onset of psychotic symptoms before age25, met DSM-IV criteria for schizophrenia, schizophreni-form disorder, or schizoaffective disorder, experiencedpsychotic symptoms for at least 1 but not more than60 months, were seriously ill as evaluated by the PANSSand CGI, and had been treated less than 16 cumulativeweeks with an antipsychotic prior to entry into the study.
Forty-seven healthy comparison subjects did notmeet DSM IV criteria for any disorder, were medicallyhealthy, and did not have a first degree relative with aDSM IV disorder.
2.2. Clinical and neurocognitive assessment
At-risk and first episode subjects were evaluatedclinically at baseline and at least every month for 1 year.Healthy controls and at-risk subjects were given neuro-cognitive assessments at baseline and every 6 monthsthereafter. The first episode patients were given neuro-
Table 1Neurocognitive assessment battery
Neurocognitivedomain
Test Description
Verbal fluency Controlled Oral AssociationTest (29)
Subjects are askedand S in three sepa
Category instancegeneration (29)
Subjects are askedthree categories (an
Attention Continuous PerformanceTest, Identical Pairs Version (27)
Subjects are askedon a computer screkey whenever the n
Verbal memoryand learning
California Verbal LearningTest (30)
Subjects are askedread aloud by the t
Processing Speed WAIS-R digit–symbol test (26) Each numeral (1 this asked to copy as
Working Memory Dot Test of VisuospatialWorking Memory (31)
Subjects are shownand are asked eitheafter a delay of 10calculated as a mea
Letter–Number SequencingTest (32)
Clusters of letters cand the subject is afrom lowest to high
Motor speed Finger Oscillation Test (33) Subjects are askedfor five trials is cal
cognitive assessments at baseline, 12 weeks, 6 months,and 1 year post-baseline.
The neurocognitive test battery is listed in Table 1. Thetest procedures were identical for all study subjects, andsupervision of test administration was conducted by thesame study investigator (RSEK) for all groups at bothsites. Study subjects were recruited contemporaneously.A summary cognitive score was calculated as the firstprincipal component from 7 tests based upon previouswork using this battery in patients with schizophrenia(Keefe et al., 2004). The first principal component anal-ysis produced a set of weights for constructing the com-posite score from the following tests: CPT, Verbal Recall,Finger Oscillation, Digit–Symbol, Verbal Fluency (cate-gory instances and letter fluency), WorkingMemory (DotTest and Letter–Number Span). A summary score was notcalculated if any score was missing.
2.3. Statistical analysis
We first examined data compatibility by testing study(Prodromal Study versus First Episode Study) and site(Toronto versus UNC) differences among healthy sub-jects controlling for age, gender and race. Neither wasfound significant in cognitive summary score (pN0.50).Data were pooled for all the following analysis.
The valid analysis sample included subjects with non-missing cognitive summary scores at baseline. Becauseantipsychotics may reduce the risk of psychosis in at-risk subjects (Phillips et al., 2002; Woods et al., 2003),
to generate as many words as possible beginning with F, A,rate trials of 60 s.to name as many words as possible in 60 s within each ofimals, fruits, vegetables).to respond to a series of 450 four-digit numbers presenteden at a rate of one per second by lifting a finger from a mouseumber is identical to the previous number in the series.to recall as many words as possible from a list of 16 wordsester. The procedure is repeated five times.rough 9) is associated with a different simple symbol, and the subjectmany symbols associated with the numerals as possible in 90 s.a series of dots at different locations on separate pieces of paperr to copy the location of the dot or recall the position of the dotor 20 s. The difference between the copy and recall trials issure of “working memory deficit.”ombined with numbers (e.g., N6G2) are read aloud by the tester,sked to reorganize the cluster so that the numbers are listed first,est, followed by the letters in alphabetical order.to tap the index finger as quickly as possible for 10 s. An averageculated for each hand.
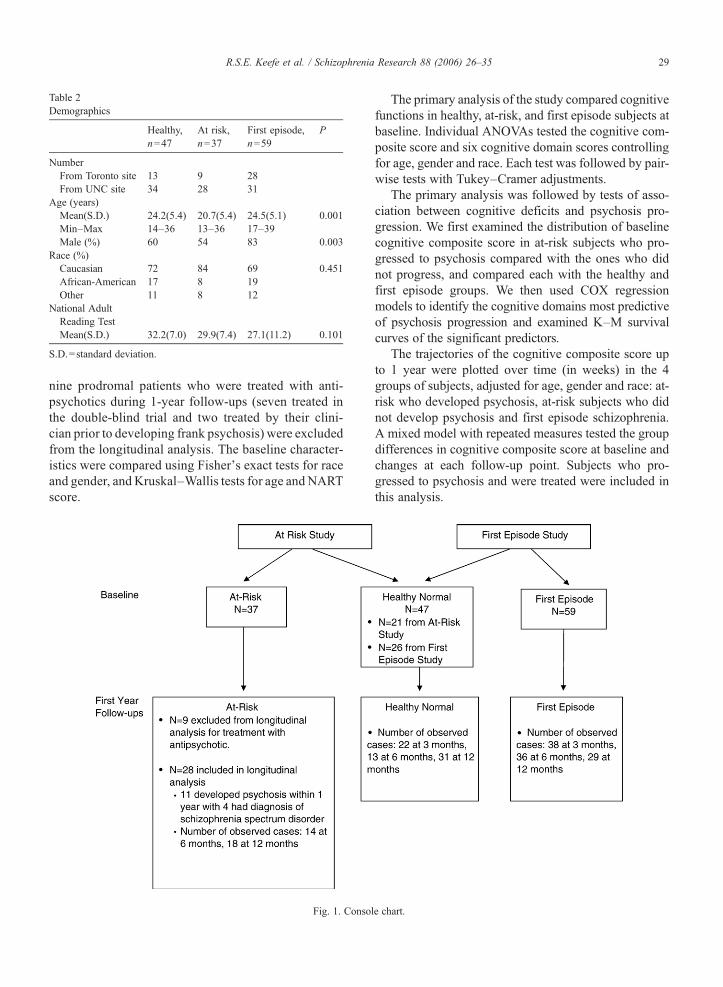
Table 2Demographics
Healthy,n=47
At risk,n=37
First episode,n=59
P
NumberFrom Toronto site 13 9 28From UNC site 34 28 31
Age (years)Mean(S.D.) 24.2(5.4) 20.7(5.4) 24.5(5.1) 0.001Min–Max 14–36 13–36 17–39Male (%) 60 54 83 0.003
Race (%)Caucasian 72 84 69 0.451African-American 17 8 19Other 11 8 12
National AdultReading TestMean(S.D.) 32.2(7.0) 29.9(7.4) 27.1(11.2) 0.101
S.D.=standard deviation.
29R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
nine prodromal patients who were treated with anti-psychotics during 1-year follow-ups (seven treated inthe double-blind trial and two treated by their clini-cian prior to developing frank psychosis) were excludedfrom the longitudinal analysis. The baseline character-istics were compared using Fisher's exact tests for raceand gender, and Kruskal–Wallis tests for age and NARTscore.
Fig. 1. Consol
The primary analysis of the study compared cognitivefunctions in healthy, at-risk, and first episode subjects atbaseline. Individual ANOVAs tested the cognitive com-posite score and six cognitive domain scores controllingfor age, gender and race. Each test was followed by pair-wise tests with Tukey–Cramer adjustments.
The primary analysis was followed by tests of asso-ciation between cognitive deficits and psychosis pro-gression. We first examined the distribution of baselinecognitive composite score in at-risk subjects who pro-gressed to psychosis compared with the ones who didnot progress, and compared each with the healthy andfirst episode groups. We then used COX regressionmodels to identify the cognitive domains most predictiveof psychosis progression and examined K–M survivalcurves of the significant predictors.
The trajectories of the cognitive composite score upto 1 year were plotted over time (in weeks) in the 4groups of subjects, adjusted for age, gender and race: at-risk who developed psychosis, at-risk subjects who didnot develop psychosis and first episode schizophrenia.A mixed model with repeated measures tested the groupdifferences in cognitive composite score at baseline andchanges at each follow-up point. Subjects who pro-gressed to psychosis and were treated were included inthis analysis.
e chart.
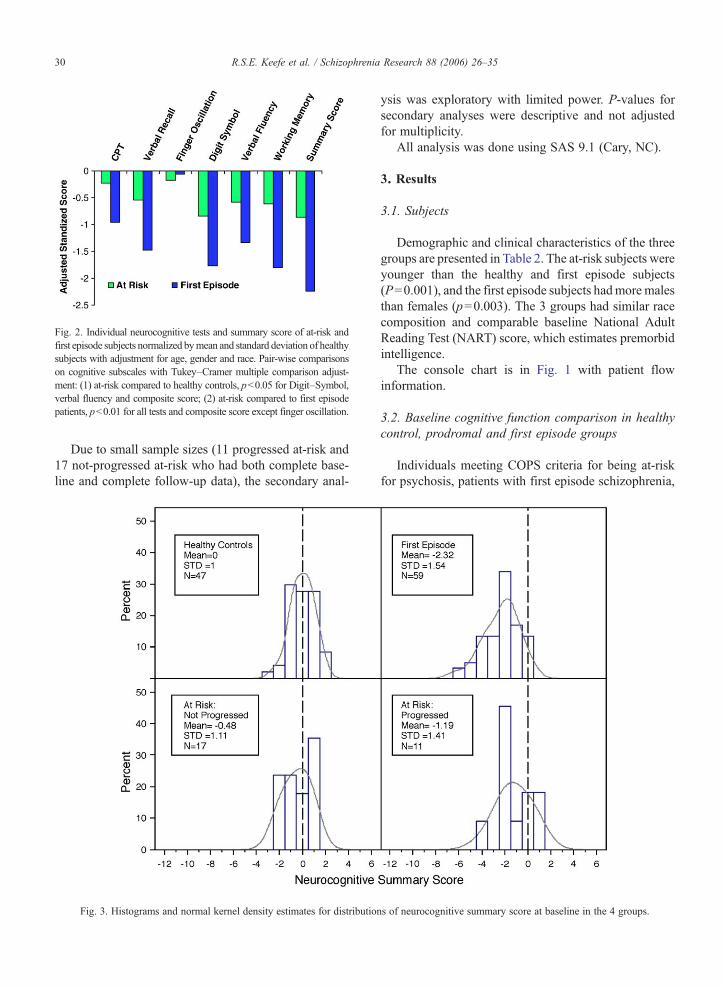
Fig. 2. Individual neurocognitive tests and summary score of at-risk andfirst episode subjects normalized bymean and standard deviation of healthysubjects with adjustment for age, gender and race. Pair-wise comparisonson cognitive subscales with Tukey–Cramer multiple comparison adjust-ment: (1) at-risk compared to healthy controls, pb0.05 for Digit–Symbol,verbal fluency and composite score; (2) at-risk compared to first episodepatients, pb0.01 for all tests and composite score except finger oscillation.
30 R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
Due to small sample sizes (11 progressed at-risk and17 not-progressed at-risk who had both complete base-line and complete follow-up data), the secondary anal-
Fig. 3. Histograms and normal kernel density estimates for distributio
ysis was exploratory with limited power. P-values forsecondary analyses were descriptive and not adjustedfor multiplicity.
All analysis was done using SAS 9.1 (Cary, NC).
3. Results
3.1. Subjects
Demographic and clinical characteristics of the threegroups are presented in Table 2. The at-risk subjects wereyounger than the healthy and first episode subjects(P=0.001), and the first episode subjects hadmore malesthan females (p=0.003). The 3 groups had similar racecomposition and comparable baseline National AdultReading Test (NART) score, which estimates premorbidintelligence.
The console chart is in Fig. 1 with patient flowinformation.
3.2. Baseline cognitive function comparison in healthycontrol, prodromal and first episode groups
Individuals meeting COPS criteria for being at-riskfor psychosis, patients with first episode schizophrenia,
ns of neurocognitive summary score at baseline in the 4 groups.
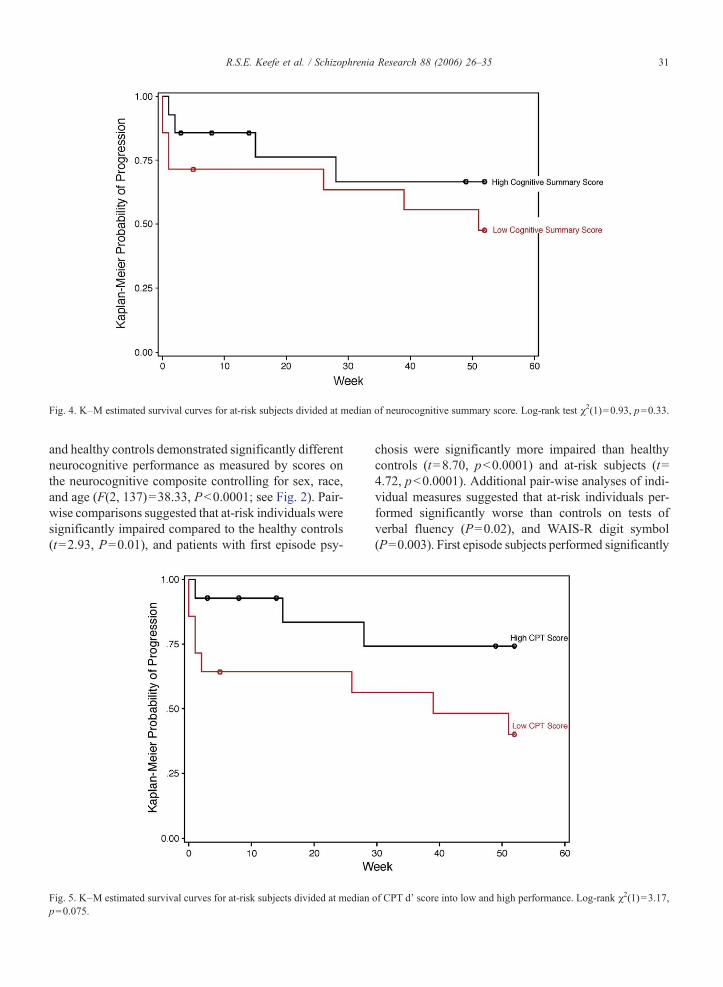
Fig. 4. K–M estimated survival curves for at-risk subjects divided at median of neurocognitive summary score. Log-rank test χ2(1)=0.93, p=0.33.
31R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
and healthy controls demonstrated significantly differentneurocognitive performance as measured by scores onthe neurocognitive composite controlling for sex, race,and age (F(2, 137)=38.33, Pb0.0001; see Fig. 2). Pair-wise comparisons suggested that at-risk individuals weresignificantly impaired compared to the healthy controls(t=2.93, P=0.01), and patients with first episode psy-
Fig. 5. K–M estimated survival curves for at-risk subjects divided at medianp=0.075.
chosis were significantly more impaired than healthycontrols (t=8.70, pb0.0001) and at-risk subjects (t=4.72, pb0.0001). Additional pair-wise analyses of indi-vidual measures suggested that at-risk individuals per-formed significantly worse than controls on tests ofverbal fluency (P=0.02), and WAIS-R digit symbol(P=0.003). First episode subjects performed significantly
of CPT d' score into low and high performance. Log-rank χ2(1)=3.17,
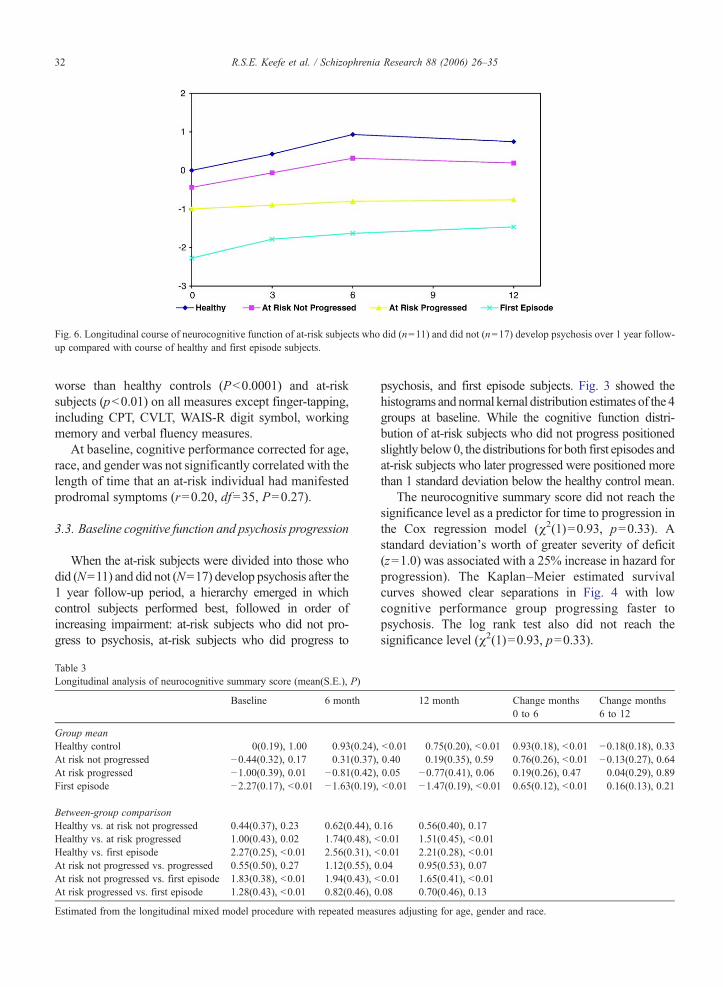
Fig. 6. Longitudinal course of neurocognitive function of at-risk subjects who did (n=11) and did not (n=17) develop psychosis over 1 year follow-up compared with course of healthy and first episode subjects.
32 R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
worse than healthy controls (Pb0.0001) and at-risksubjects (pb0.01) on all measures except finger-tapping,including CPT, CVLT, WAIS-R digit symbol, workingmemory and verbal fluency measures.
At baseline, cognitive performance corrected for age,race, and gender was not significantly correlated with thelength of time that an at-risk individual had manifestedprodromal symptoms (r=0.20, df=35, P=0.27).
3.3. Baseline cognitive function and psychosis progression
When the at-risk subjects were divided into those whodid (N=11) and did not (N=17) develop psychosis after the1 year follow-up period, a hierarchy emerged in whichcontrol subjects performed best, followed in order ofincreasing impairment: at-risk subjects who did not pro-gress to psychosis, at-risk subjects who did progress to
Table 3Longitudinal analysis of neurocognitive summary score (mean(S.E.), P)
Baseline 6 month
Group meanHealthy control 0(0.19), 1.00 0.93(0.24),At risk not progressed −0.44(0.32), 0.17 0.31(0.37),At risk progressed −1.00(0.39), 0.01 −0.81(0.42),First episode −2.27(0.17), b0.01 −1.63(0.19),
Between-group comparisonHealthy vs. at risk not progressed 0.44(0.37), 0.23 0.62(0.44), 0Healthy vs. at risk progressed 1.00(0.43), 0.02 1.74(0.48), bHealthy vs. first episode 2.27(0.25), b0.01 2.56(0.31), bAt risk not progressed vs. progressed 0.55(0.50), 0.27 1.12(0.55), 0At risk not progressed vs. first episode 1.83(0.38), b0.01 1.94(0.43), bAt risk progressed vs. first episode 1.28(0.43), b0.01 0.82(0.46), 0
Estimated from the longitudinal mixed model procedure with repeated meas
psychosis, and first episode subjects. Fig. 3 showed thehistograms and normal kernal distribution estimates of the 4groups at baseline. While the cognitive function distri-bution of at-risk subjects who did not progress positionedslightly below0, the distributions for both first episodes andat-risk subjects who later progressed were positioned morethan 1 standard deviation below the healthy control mean.
The neurocognitive summary score did not reach thesignificance level as a predictor for time to progression inthe Cox regression model (χ2(1)=0.93, p=0.33). Astandard deviation's worth of greater severity of deficit(z=1.0) was associated with a 25% increase in hazard forprogression). The Kaplan–Meier estimated survivalcurves showed clear separations in Fig. 4 with lowcognitive performance group progressing faster topsychosis. The log rank test also did not reach thesignificance level (χ2(1)=0.93, p=0.33).
12 month Change months0 to 6
Change months6 to 12
b0.01 0.75(0.20), b0.01 0.93(0.18), b0.01 −0.18(0.18), 0.330.40 0.19(0.35), 0.59 0.76(0.26), b0.01 −0.13(0.27), 0.640.05 −0.77(0.41), 0.06 0.19(0.26), 0.47 0.04(0.29), 0.89b0.01 −1.47(0.19), b0.01 0.65(0.12), b0.01 0.16(0.13), 0.21
.16 0.56(0.40), 0.170.01 1.51(0.45), b0.010.01 2.21(0.28), b0.01.04 0.95(0.53), 0.070.01 1.65(0.41), b0.01.08 0.70(0.46), 0.13
ures adjusting for age, gender and race.

33R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
To explore the cognitive domains most predictive ofthe conversion to psychosis, we used a Cox regressionmodel to select significant predictors from the demo-graphic variables of age, race, gender and the six cognitivetest scores in a backwardmodel selection procedure. Race(African-American) (χ2(1)=3.93, p=0.05), poor CPTperformance (χ2(1)=5.40, p=0.02), and good WAIS-Rdigit symbol performance(χ2(1)=3.94, p=0.05) pre-dicted eventual conversion to psychosis. The K–Msurvival curves for low and high CPT patients (mediansplit) showed faster progression for lowCPT performancepatients in Fig. 5. The log-rank test result were marginal(χ2(1)=3.17, p=0.075).
3.4. Longitudinal cognitive function comparison inhealthy control, prodromal progressed, prodromal not-progressed and first episode groups
After adjustment for age, gender and race, the least-square means of the neurocognitive summary score ateach follow-up visit for the 4 groupswere plotted in Fig. 6.Over all, group differences were significant over the entirefollow-up period (F(3, 191)=30.30, pb0.0001), and therewas no significant evidence for different trajectory pat-terns of cognitive score change over time (F(7, 191)=1.24,p=0.2804).
Detailed group least-square means and between-group comparisons at each time point are listed inTable 3. Both the healthy subjects and at-risk subjectswho did not develop psychosis showed significant gainsat the 3-month and 6-month retests from baseline(pb0.01), and leveled afterwards (pN0.30). First epi-sode subjects, who were receiving treatment, had signi-ficant cognitive improvement at 3 months (pb0.01), andleveled at the 3-month assessment and beyond. Thegroup of at-risk subjects who did develop psychosis wasthe only group to retain the same level of deficit withoutsignificant change throughout the course (pN0.40).
The at-risk subjects who did not develop psychosiswere not significantly different from the healthy controls(pN0.15), but performed significantly better than thefirst episode subjects (pb0.01) at all the follow-up visits.The at-risk subjects who developed psychosis performedbetter than the first episode subjects (pb0.01) at base-line, but the difference was not statistically significant bythe end of the follow-up period (p=0.13).
4. Discussion
The results of this study confirm the notion thatneurocognitive deficits are present during the prodromalstage of illness, prior to developing psychosis (Brewer et
al., 2003, 2005; Hambrecht et al., 2002; Hawkins et al.,2004). Specifically, the neurocognitive performance ofsubjects who subsequently developed a psychoticdisorder was similar to that of first episode subjectsand significantly worse than that of healthy subjects.Although not significantly worse than at-risk subjectswho did not develop a psychotic disorder, the z-scoredifference between these groups (0.6) was larger thanwhat is considered to be a medium effect size, andimproved in each group except those subjects whoprogressed to psychosis.
It is unclear the extent to which these cognitivedeficits are stable, pre-morbid characteristics, orwhether these deficits emerge or worsen during earlypuberty. Recent studies that report decline in IQ and inschool performance in late childhood and earlyadolescence suggest that neurocognitive decline asso-ciated with the psychotic prodrome may occur aroundpuberty. During this time there are substantialmaturational changes occurring in frontal corticalareas of the brain (Thompson et al., 2001). RecentfMRI studies in at risk subjects find reduced activationof frontal regions in response to a visual odd ball task(Morey et al., 2005). The emerging evidence is thusconsistent with the hypothesis that the cognitiveimpairments associated with schizophrenia may resultfrom alterations in the normal trajectory of braindevelopment during early adolescence. The results ofthis study are consistent with the hypothesis that theneurocognitive deficits associated with schizophreniamay worsen during the prodromal period, as thosesubjects who progressed to psychosis did not demon-strate the same improved performance over time thatwas found in healthy controls and those at-risk subjectswho did not progress to psychosis. Severity ofneurocognitive deficits in the at-risk subjects was notrelated to duration of prodromal symptoms. Furtherresearch is needed to further define the longitudinalcourse of the neurocognitive deficits associated withschizophrenia.
The profile of neurocognitive deficits in individualsat high risk for developing psychosis has not beenestablished. In the current study, at-risk subjectsdemonstrated specific deficits on the WAIS digit–symbol test and verbal fluency, both of which measureprocessing speed. An impaired capacity to processinformation at adequate speed is a fundamentalcomponent of the cognitive deficits of schizophrenia(Nuechterlein and Dawson, 1984) and processingspeed tests are more highly correlated with neurocog-nitive composite scores than other aspects of cognitivefunctioning (30). This pattern of results may suggest

34 R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
that individuals at risk for psychosis demonstratedeficits in general cognitive functions more thanspecific mechanisms. However, the breadth of cogni-tive assessment in this study was limited, and manyspecific hypotheses regarding the neurocognitive riskfor psychosis were not tested.
The value of developing preventative treatments forschizophrenia is clear (Insel, 2006) and depends on theidentification of sensitive and specific disease markers.While statistical power to determine the predictivevalue of neurocognitive deficits for the progression topsychosis was limited in this study, the poorperformance of the at-risk subjects who later developedpsychosis is consistent with the notion that neurocog-nitive test performance may help predict whetherindividuals at high risk will progress to psychosis(Brewer et al., 2005). Post-hoc analyses suggested astatistical trend for CPT performance to predict whichpatients progressed to psychosis, and that a combina-tion of poor CPT performance and better WAIS-Rdigit–symbol performance significantly predicted psy-chosis development. Poor vigilance as measured by theCPT has previously been associated with risk forschizophrenia (Cornblatt and Keilp, 1994) and theprediction of adult schizophrenia-related psychopathol-ogy (Cornblatt et al., 1999). It is also noteworthy thatthe entire group of at-risk subjects in this studyperformed worse than controls on the WAIS digit–symbol task, yet those subjects who progressed topsychosis performed significantly better on this taskthan those who did not progress. While post-hocanalyses on small numbers of patients are potentiallyunstable and thus need to be viewed with appropriatecaution, the combination of poor vigilance and highprocessing speed may make patients particularlyvulnerable to the progression to psychosis. The devel-opment of psychosis may be associated with increasedgeneration of activity in the context of disturbedcapacity to attend to the context of these actions. Futureprospective studies are needed to determine the ability ofspecific neurocognitive assessments to enhance theprediction of psychosis in those individuals at risk.
Acknowledgements
The authors would like to thank an anonymous donor(administered through the San Francisco ResearchFoundation), the Foundation of Hope, and The StanleyFoundation for their support. Supported in part bystudies F1D-MC-HGDH and F1D-MC-HGGF fundedby Eli Lilly Pharmaceuticals. Support for this projectalso came from NIMH projects P50-MH064065 and
MH01905 (D. Perkins) and a NARSAD IndependentInvestigator Award (R. Keefe).
References
Brewer, W.J., Wood, S.J., McGorry, P.D., Francey, S.M., Phillips, L.J.,Yung, A.R., et al., 2003. Impairment of olfactory identificationability in individuals at ultra-high risk for psychosis who laterdevelop schizophrenia. Am. J. Psychiatry 160 (10), 1790–1794.
Brewer, W.J., Francey, S.M., Wood, S.J., Jackson, H.J., Pantelis, C.,Phillips, L.J., et al., 2005. Memory impairments identified inpeople at ultra-high risk for psychosis who later develop first-episode psychosis. Am. J. Psychiatry 162 (1), 71–78.
Cannon, M., Jones, P., Huttunen, M.O., Tanskanen, A., Huttunen, T.,Rabe-Hesketh, S., et al., 1999. School performance in Finnishchildren and later development of schizophrenia: a population-based longitudinal study. Arch. Gen. Psychiatry 56 (5), 457–463.
Cannon, M., Caspi, A., Moffitt, T.E., Harrington, H., Taylor, A.,Murray, R.M., et al., 2002. Evidence for early-childhood, pan-developmental impairment specific to schizophreniform disorder:results from a longitudinal birth cohort. Arch. Gen. Psychiatry 59(5), 449–456.
Cornblatt, B.A., Keilp, J.G., 1994. Impaired attention, genetics, andthe pathophysiology of schizophrenia. Schizophr. Bull. 20 (1),31–46.
Cornblatt, B., Obuchowski, M., Roberts, S., Pollack, S., Erlenmeyer-Kimling, L., 1999. Cognitive and behavioral precursors of schizo-phrenia. Dev. Psychopathol. 11 (3), 487–508.
Cosway, R., Byrne, M., Clafferty, R., Hodges, A., Grant, E.,Abukmeil, S.S., et al., 2000. Neuropsychological change inyoung people at high risk for schizophrenia: results from the firsttwo neuropsychological assessments of the Edinburgh High RiskStudy. Psychol. Med. 30 (5), 1111–1121.
Fuller, R., Nopoulos, P., Arndt, S., O'Leary, D., Ho, B.C., Andreasen,N.C., 2002. Longitudinal assessment of premorbid cognitivefunctioning in patients with schizophrenia through examination ofstandardized scholastic test performance. Am. J. Psychiatry 159(7), 1183–1189.
Hambrecht, M., Lammertink, M., Klosterkotter, J., Matuschek, E.,Pukrop, R., 2002. Subjective and objective neuropsychologicalabnormalities in a psychosis prodrome clinic. Br. J. Psychiatry 43,s30–s37 (Suppl.).
Hawkins, K.A., Addington, J., Keefe, R.S., Christensen, B., Perkins,D.O., Zipursky, R., et al., 2004. Neuropsychological status ofsubjects at high risk for a first episode of psychosis. Schizophr.Res. 67 (2–3), 115–122.
Heaton, R.K., Gladsjo, J.A., Palmer, B.W., Kuck, J., Marcotte, T.D.,Jeste, D.V., 2001. Stability and course of neuropsychologicaldeficits in schizophrenia. Arch. Gen. Psychiatry 58 (1), 24–32.
Insel, T.R., 2006. Cure therapeutics and strategic prevention: raisingthe bar for mental health research. Mol. Psychiatry 11 (1), 11–17.
Isohanni, I., Jarvelin, M.R., Nieminen, P., Jones, P., Rantakallio, P.,Jokelainen, J., et al., 1998. School performance as a predictor ofpsychiatric hospitalization in adult life. A 28-year follow-up in theNorthern Finland 1966 Birth Cohort. Psychol. Med. 28 (4),967–974.
Jones, P., Rodgers, B., Murray, R., Marmot, M., 1994. Childdevelopment risk factors for adult schizophrenia in the British1946 birth cohort. Lancet 344 (8934), 1398–1402.
Keefe, R.S.E., Seidman, L.J., Christensen, B.K., Hamer, R.M.,Sharma, T., Sitskoorn, M.M., et al., 2004. Comparative effect of
35R.S.E. Keefe et al. / Schizophrenia Research 88 (2006) 26–35
atypical and conventional antipsychotic drugs on neurocognitionin first-episode psychosis: a randomized, double-blind trial ofolanzapine versus low doses of haloperidol. Am. J. Psychiatry 161(6), 985–995.
Keefe, R.S.E., Eesley, C.E., Poe, M.P., 2005. Defining a cognitivefunction decrement in schizophrenia. Biol. Psychiatry 57 (6),688–691.
Keefe, R.S.E., Seidman, L.J., Christensen, B.K., Hamer, R.M., Sharma, T.,Sitskoorn, M.M., et al., 2006. Long-term neurocognitive effects ofolanzapine or low-dose haloperidol in first-episode psychosis. Biol.Psychiatry 59 (2), 97–105.
Klosterkotter, J., Hellmich, M., Steinmeyer, E.M., Schultze-Lutter, F.,2001. Diagnosing schizophrenia in the initial prodromal phase.Arch. Gen. Psychiatry 58 (2), 158–164.
Lieberman, J.A., Tollefson, G., Tohen, M., Green, A.I., Gur, R.E.,Kahn, R., et al., 2003. Comparative efficacy and safety of atypicaland conventional antipsychotic drugs in first-episode psychosis: arandomized, double-blind trial of olanzapine versus haloperidol.Am. J. Psychiatry 160 (8), 1396–4404.
Miller, T.J., McGlashan, T.H., Rosen, J.L., Cadenhead, K., Cannon, T.,Ventura, J., et al., 2003. Prodromal assessment with the structuredinterview for prodromal syndromes and the scale of prodromalsymptoms: predictive validity, interrater reliability, and training toreliability. Schizophr. Bull. 29 (4), 703–715.
Morey, R.A., Inan, S., Mitchell, T.V., Perkins, D.O., Lieberman, J.A.,Belger, A., 2005. Imaging frontostriatal function in ultra-high-risk,early, and chronic schizophrenia during executive processing.Arch. Gen. Psychiatry 62 (3), 254–262.
Niemi, L.T., Suvisaari, J.M., Tuulio-Henriksson, A., Lonnqvist, J.K.,2003. Childhood developmental abnormalities in schizophrenia:
evidence from high-risk studies. Schizophr. Res. 60 (2–3),239–258.
Nuechterlein, K.H., Dawson, M.E., 1984. Information processing andattentional functioning in the developmental course of schizo-phrenic disorders. Schizophr. Bull. 10 (2), 160–203.
Phillips, L.J., Yung, A.R., Yuen, H.P., Pantelis, C., McGorry, P.D.,2002. Prediction and prevention of transition to psychosis in youngpeople at incipient risk for schizophrenia. Am. J. Med. Genet. 114(8), 929–937.
Reichenberg, A., Weiser, M., Rapp, M.A., Rabinowitz, J., Caspi,A., Schmeidler, J., et al., 2005. Elaboration on premorbidintellectual performance in schizophrenia: premorbid intellectualdecline and risk for schizophrenia. Arch. Gen. Psychiatry 62(12), 1297–130.
Thompson, P.M., Vidal, C., Giedd, J.N., Gochman, P., Blumenthal, J.,Nicolson, R., et al., 2001. Mapping adolescent brain change revealsdynamic wave of accelerated gray matter loss in very early-onsetschizophrenia. Proc. Natl. Acad. Sci. U. S. A. 98 (20), 11650–11655.
Woods, S.W., Breier, A., Zipursky, R.B., Perkins, D.O., Addington, J.,Miller, T.J., et al., 2003. Randomized trial of olanzapine versusplacebo in the symptomatic acute treatment of the schizophrenicprodrome. Biol. Psychiatry 54 (4), 453–464.
Yung, A.r., McGorry, P.D., 1996. The initial prodrome in psychosis:descriptive and qualitative aspects. Aust. N. Z. J. Psychiatry 30 (5),587–599.
Zammit, S., Allebeck, P., David, A.S., Dalman, C., Hemmingsson, T.,Lundberg, I., et al., 2004. A longitudinal study of premorbid IQScore and risk of developing schizophrenia, bipolar disorder,severe depression, and other non-affective psychoses. Arch. Gen.Psychiatry 61 (4), 354–360.
Related Documents