1 v2 updated 28 November 2016 A GUIDE TO THE EMERGENCY CARE ADVANCED CLNICAL PRACTITIONER PILOT CREDENTIALING PROJECT November 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
v2 updated 28 November 2016
A GUIDE TO THE
EMERGENCY CARE ADVANCED
CLNICAL PRACTITIONER
PILOT CREDENTIALING PROJECT
November 2016
2
v2 updated 28 November 2016
Preface
This edition of “A Guide for Emergency Care Advanced Clinical Practitioner Pilot Credentialing
Project” provides guidance to trainee Advanced Clinical Practitioners (ACPs), assessors and
other stakeholders on the arrangements for the pilot for Emergency Care ACP credentialing.
This edition is a consolidation of all earlier versions of the Reference Guide and is applicable
to all trainee ACPs undertaking the pilot credentialing process in June 2016. This edition
replaces all previous editions with immediate effect.
The standards and requirements for the advanced clinical practitioner are set out in the
Emergency Care ACP Curriculum, which is available on the Royal College of Emergency
Medicine website and Health Education England website. The curriculum has been endorsed
by the Royal College of Nursing and the College of Paramedics.
The development of this Reference Guide has been through an iterative process of feedback
from Health Education England, Royal College of Emergency Medicine (as co-producers of
the Emergency Care ACP Curriculum) and other key stakeholders.
The Guide is published in electronic format and will be available via the Royal College of
Emergency Medicine website.
It is noted that the June 2016 and April 2017 credentialing process is a pilot. Evaluation of the
pilot will assist in developing the process and a further edition of this guide
The purpose of the Reference Guide is to assist stakeholders in understanding the pilot
process and documentation to be used. The Reference Guide is as the title states, a Guide,
and as such practices, processes and paperwork may be altered at the discretion of Health
Education England, Royal College of Emergency Medicine and credentialing panel assessors.
To access the curriculum and other information, please visit:
http://www.rcem.ac.uk/Training-Exams/Emergency%20Care%20ACP

3
v2 updated 28 November 2016
Contents
Preface .................................................................................................................................... 2
Section 1: Introduction and Background .................................................................................. 4
Section 2: Employer Support and Evidence Collation .............................................................. 5
Section 3: The Pilot Credentialing Process .............................................................................. 6
Appendix One: Checklist of Evidence ...................................................................................... 7
Adult Emergency Care ACP ................................................................................................. 9
Paediatric Competences if the ACP is Adult and Paediatric ................................................12
Paediatric Emergency Care ACP ........................................................................................13
Appendix Two: Assessment Descriptors and Assessment Forms for Emergency Care
Advanced Clinical Practitioners ..............................................................................................15
Consultant-Led Mini-Clinical Evaluation Exercise - Mini- CEX ................................................16
Mini-CEX Descriptors .............................................................................................................17
Emergency Care ACP Mini-CEX Summative Descriptors for Major Presentations ..............19
Mini-CEX Summative Descriptors for Acute Presentations ..................................................25
Consultant-Led Case based Discussion CbD .........................................................................30
CbD Descriptors ..................................................................................................................31
Direct Observation of Procedural Skills – DOPs ......................................................................32
Practical Procedures DOPs Descriptors ..................................................................................33
ACAT-EM Descriptors ............................................................................................................37
Instructions for Use of ACAT-EM ........................................................................................37
The Acute Care Assessment Tool (ACAT-EM) Form ...............................................................38
Multi-Source Feedback (MSF) Form .......................................................................................39
Patient Survey Tool .................................................................................................................40
Mini-CEX Summative Descriptors for PEM ACP .....................................................................41
Acute Presentations ................................................................................................................41
Paediatric Practical Procedures DOPs Descriptors .................................................................45
Structured Training Report for ACP ........................................................................................48
Appendix Three: Self-Declaration Form ..................................................................................50
Appendix Four: Credentialing Outcome Form .........................................................................54
Appendix Five: Credentialing Feedback Form ........................................................................56

4
v2 updated 28 November 2016
Section 1: Introduction and Background
1.1. This Guide sets out the arrangements for the pilot Emergency Care Advanced Clinical
Practitioner (ACP) credentialing process, as agreed by Health Education England (HEE) and
Royal College of Emergency Medicine (RCEM).
1.2 The pilot credentialing process is a mechanism whereby trainee ACPs in Emergency Care
will present evidence of their achievements and competences to be evaluated against the
Emergency Care ACP curriculum.
1.3 Trainee ACPs will be required to collect evidence, as per the curriculum, through use of
the RCEM e-portfolio for ACPs.
1.4 To access the curriculum, information about e-portfolio access and other information
relating to Emergency Care ACP developments, please visit: http://www.rcem.ac.uk/Training-
Exams/Emergency%20Care%20ACP.
1.5 ACPs who successfully credential against the curriculum will be awarded a certificate and
their details will be held on a new register of successfully credentialed ACPs held by RCEM.
1.6 The Emergency Care ACP credentialing process is a pilot in June 2016 and April 2017, as
such the paperwork and processes are likely to change at any stage after the first or second
pilot is completed.
1.7 Individuals interested in applying for the credentialing process, or wishing to join the
‘Emergency Care ACP mailing list’ should contact [email protected]; likewise any questions
may be sent to this email address.
1.8 All time periods referred to within this document (and other Emergency Care ACP
paperwork) are full-time equivalent.

5
v2 updated 28 November 2016
Section 2: Employer Support and Evidence Collation
2.1. Evidence should be collected as per the pilot process and curriculum requirements; this
should be saved on the RCEM e-portfolio.
2.2 For RCEM e-portfolio technical support, please contact: [email protected].
2.3 Individuals considering undertaking ACP credentialing should have support from their
employers.
2.4 At least one individual involved in assessing trainee ACPs at the local department should
have completed the appropriate Emergency Care ACP mandatory assessor training. The local
individual who has had the mandatory assessor training will be responsible for ensuring other
colleagues involved in assessing the trainee ACP understand the requirements. Where
relevant, the WBA must be a consultant in Emergency Medicine who has undertaken training
for workplace based assessment and is accredited by the General Medical council as an
educational supervisor or named clinical supervisor.
2.5 Trainee ACPs and those assessing ACPs should review the curriculum and checklist
regularly to ensure they understand the requirements, processes and paperwork. Any queries
should be directed to [email protected].
2.6 Trainee ACPs and those assessing ACPs should pay particular attention to
Appendix 1, which is a checklist of assessments provided as evidence required for pilot
credentialing process.
2.7 Trainee ACPs and those assessing ACPs should pay particular attention to
Appendix 2, which extracts details of assessment descriptors and forms.

6
v2 updated 28 November 2016
Section 3: The Pilot Credentialing Process
3.1. All credentialing panel members will be appointed and trained by the Royal College of
Emergency Medicine.
3.2 The credentialing panel will be responsible for reviewing the e-portfolio and agreeing an
outcome.
3.3 For the pilot, the panel will consist of up to 6 assessors. For the ACP feedback session,
the panel will nominate 2 representatives of which one must be a Fellow in good standing of
the RCEM.
3.4 For the pilot, Trainee ACPs will be required to submit their evidence 8 weeks prior to the
credentialing panel date. This allows the credentialing panel to review evidence remotely well
in advance prior to the credentialing panel meeting. This means that evidence submitted within
8 weeks of the panel date will not be considered (with the exception of evidence as detailed in
Section 3.5)
3.5 Trainee ACPs will be required to submit their Self-Declaration form (Appendix Three) to
[email protected] at least one week prior to the credential panel meeting.
3.6 There are two possible outcomes at the credentialing panel: Successful – credential OR
Further evidence required (see Appendix Four – Credentialing Outcome Form).
3.7 Outcomes will be recorded on a Credentialing Outcome Form (Appendix Four). Those who
have successfully met the curriculum requirements will receive a certificate and will be added
to the register of credentialed Emergency Care ACPs.
3.8 The credentialing panel members will provide feedback to trainee ACPs via the
Credentialing Feedback Form (Appendix Five). For those who have not met the requirements,
detailed feedback, including potential timescales for re-submission, will be provided.
3.9 In the pilot, there is no mechanism for appeal against the credentialing panel’s decision.
Candidates who have not met the credentialing requirements may re-submit the evidence in
future to be considered in subsequent processes.

7
v2 updated 28 November 2016
Appendix One: Checklist of Evidence
Emergency Care Advanced Clinical Practitioner
Curriculum and Assessment
Checklist of assessments provided as evidence required for pilot credentialing process
The ACP is required to present evidence that demonstrates the competences developed over
their training and experience. This evidence should be mapped to the ACP curriculum so that
every competence in the curriculum is associated with appropriate evidence of attainment.
Evidence required
There are two types of evidence:
1. Formal assessments: these will be a mixture of assessments by a consultant and those undertaken by senior ACPs and consultant nurses, and senior EM trainees. There are a minimum number of assessments that MUST be completed by a consultant on a summative assessment form. An assessment should take the form of formal observation of clinical activity with feedback from the supervisor/assessor and reflection. We would suggest consultants should usually use summative assessment forms as these clearly identify whether satisfactory performance is displayed. The other formative forms can be used by consultants and other assessors and these are useful to indicate where any weaknesses are or suggestions for further development. ACPs are also required to complete at least 1 ACAT–EM where they are observed over a period of time with a number of patients – we recommend up to three ACAT–EMs may be useful as demonstrating multi-tasking with multiple patients. Additional assessments that are required include successful completion of life support courses, satisfactory multisource feedback.
2. Other evidence. Not every presentation or competence in the curriculum must have a formal assessment/evaluation by other clinicians to demonstration competence. Other evidence that can be presented includes case reflections, evidence of attendance at courses (with reflection), teaching others or e-learning. In addition the ACP will be expected to have evidence of successful completion and conduct of an audit with reflection on the impact their role in the audit.
ACPs should read the guidance on reflection available from their regulatory body, as evidence
of appropriate reflection on the role and attributes would be important to demonstrate the ACP
is performing at the expected level and standard.
8
v2 updated 28 November 2016
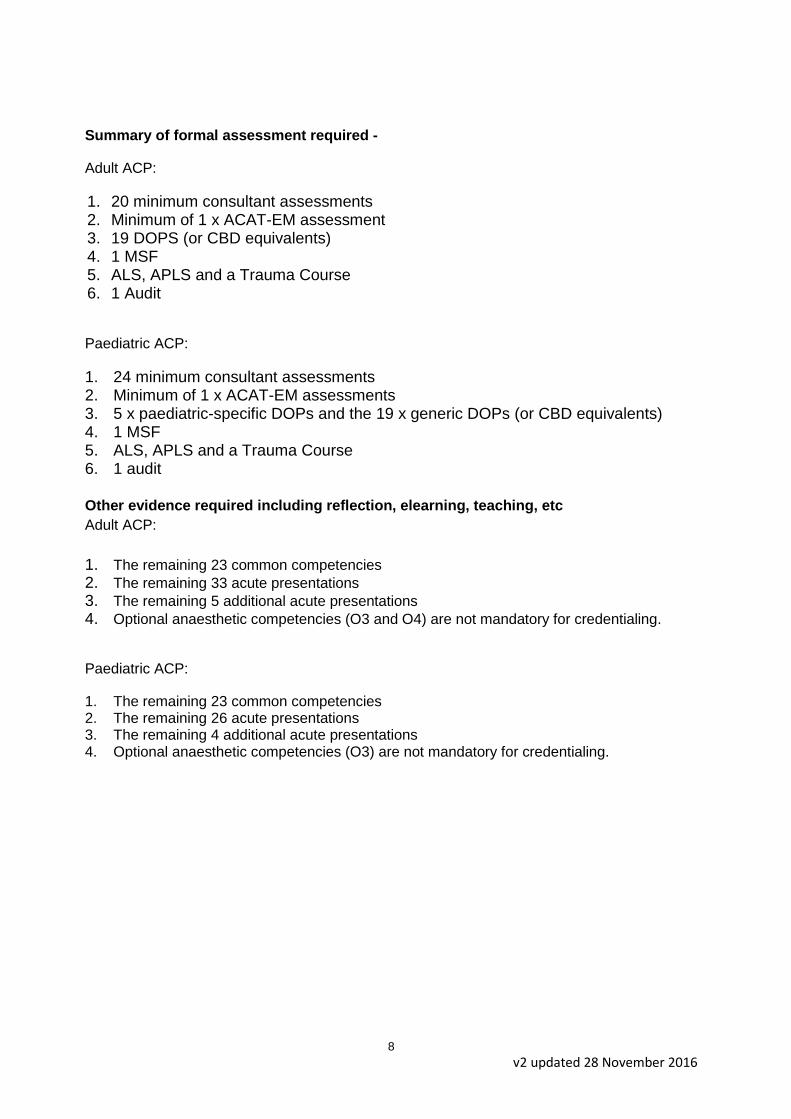
Summary of formal assessment required -
Adult ACP:
1. 20 minimum consultant assessments 2. Minimum of 1 x ACAT-EM assessment 3. 19 DOPS (or CBD equivalents) 4. 1 MSF 5. ALS, APLS and a Trauma Course 6. 1 Audit
Paediatric ACP:
1. 24 minimum consultant assessments 2. Minimum of 1 x ACAT-EM assessments 3. 5 x paediatric-specific DOPs and the 19 x generic DOPs (or CBD equivalents) 4. 1 MSF 5. ALS, APLS and a Trauma Course 6. 1 audit
Other evidence required including reflection, elearning, teaching, etc
Adult ACP:
1. The remaining 23 common competencies 2. The remaining 33 acute presentations 3. The remaining 5 additional acute presentations 4. Optional anaesthetic competencies (O3 and O4) are not mandatory for credentialing.
Paediatric ACP:
1. The remaining 23 common competencies 2. The remaining 26 acute presentations 3. The remaining 4 additional acute presentations 4. Optional anaesthetic competencies (O3) are not mandatory for credentialing.

9
Adult Emergency Care ACP
Area of curriculum Evidence required In library or
certificates? Date, type of assessment and name of assessor
Logbook output All competences/presentations/procedures evaluated by supervisor
Not Applicablei wonder if we should specifcy the supervisor should comment as well as confirm competence
All curriculum elements have evidence linked to them
Not Applicable I wonder if we should specify that the ACP should self evaluate here as well as confirm the competence level
Common competences
Level 2 for all CCs – self and supervisor assessment CbD or MiniCEX led by consultant for: CC4 - time management and decision making CC8 - team working and patient safety
Major presentations
Consultant assessment for: Anaphylaxis Cardiac arrest (or ALS) Major Trauma Sepsis Shocked patient Unconscious patient
Acute presentations
Consultant assessment for: Chest pain Abdominal pain Breathlessness Mental health Head injury
Alternatively an ACAT (by a consultant) may be utilised which covers 3 or more presentations of which these may be 1 or 2.
Additional Major Presentation
Consultant assessments for (or ATLS/ATNC/ETC with reflection): Major trauma chest Major trauma abdominal injury Major trauma spine Major trauma maxfax Major trauma burns (one patient – two injuries may be appropriate)
10
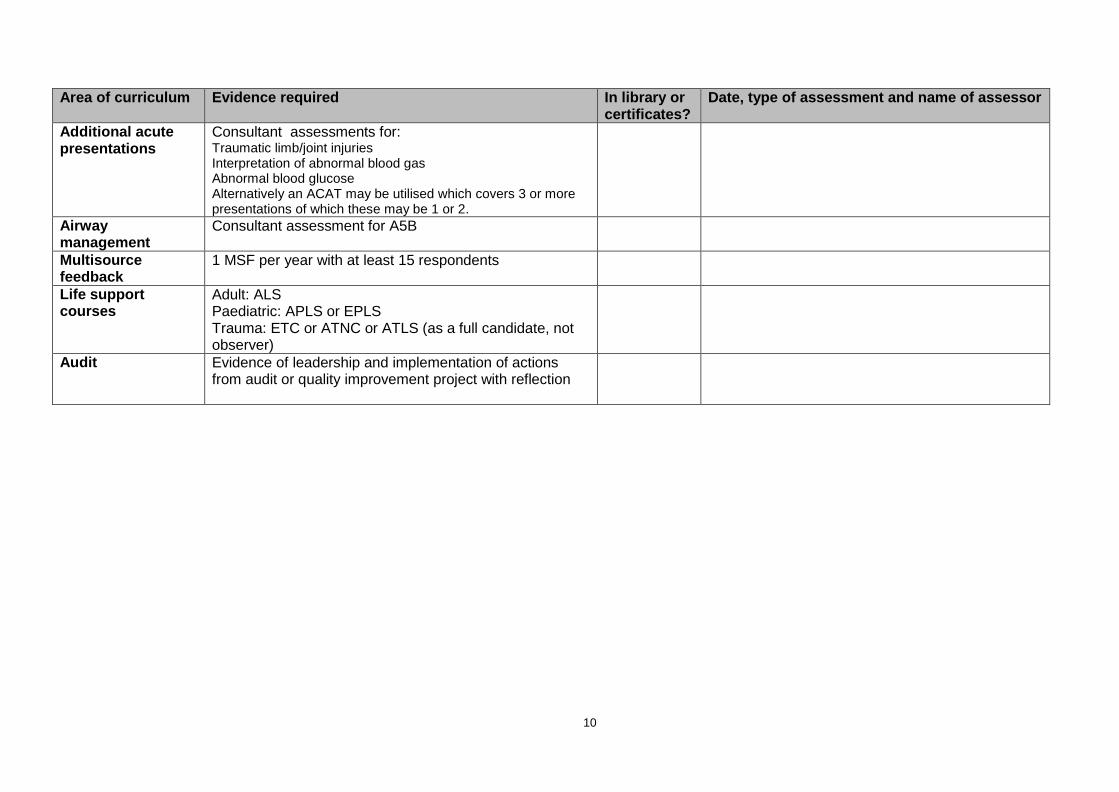
Area of curriculum Evidence required In library or certificates?
Date, type of assessment and name of assessor
Additional acute presentations
Consultant assessments for: Traumatic limb/joint injuries Interpretation of abnormal blood gas Abnormal blood glucose Alternatively an ACAT may be utilised which covers 3 or more presentations of which these may be 1 or 2.
Airway management
Consultant assessment for A5B
Multisource feedback
1 MSF per year with at least 15 respondents
Life support courses
Adult: ALS Paediatric: APLS or EPLS Trauma: ETC or ATNC or ATLS (as a full candidate, not observer)
Audit Evidence of leadership and implementation of actions from audit or quality improvement project with reflection

11
Area of curriculum Evidence required In library or certificates?
Date, type of assessment and name of assessor
Practical procedures
Where the department or work environment does not offer the opportunity for the ACP to personally undertake or practice procedures, a CbD with a consultant is sufficient (one per procedure). At least 10 procedures in total must be directly observed as a procedure.
1. Arterial cannulation (CBD) 2. Peripheral venous cannulation 3. Central venous cannulation (CBD) 4. Arterial blood gas sampling 5. Lumbar puncture (CBD) 6. Pleural tap and aspiration (CBD) 7. Intercostal drain – Seldinger (CBD) 8. Intercostal drain – Open (CBD) 9. Airway protection* 10. Basic and advanced life support 11. DC cardioversion 12. Knee aspiration 13. Temporary pacing (external) 14. Reduction of dislocation/fracture* 15. Large joint examination 16. Wound management* 17. Trauma primary survey* 18. Initial assessment of the acutely unwell 19. Secondary assessment of the acutely unwell
*For these procedures RCEM have developed specific descriptors which are available in this guide.

12
Paediatric Competences if the ACP is Adult and Paediatric
Area of curriculum Evidence required In library or
certificates? Date, type of assessment and name of assessor
Paediatric Major presentations
Consultant assessment (or APLS) for all presentations: Anaphylaxis Apnoea stridor and airway obstruction Cardiorespiratory arrest (or APLS) Major trauma Shocked child Unconscious child
Paediatric Acute presentations
Consultant assessment for: Abdominal pain Breathing difficulties Acute life threatening event Concerning presentation Head injury Mental health ACAT may be utilised which covers 3 or more presentations.
Paediatric procedures
Consultant assessment for: Venous access in children* Airway assessment and maintenance Safe sedation in children Paediatric equipment and guidelines in the resuscitation room* Primary survey in a child*

13
Paediatric Emergency Care ACP
Area of curriculum Evidence required Number of consultant
assessments (number of other assessments)
Date, type of assessment and name of assessor
Common competences Level 2 for all CCs – self and supervisor assessment CbD or MiniCEX led by consultant for: CC4 - time management and decision making CC8 - team working and patient safety
Paediatric Major Presentations
Consultant assessment for: All 6 presentations Cardiac arrest may be assessed by successful completion of APLS/EPLS
Paediatric Acute presentations
6 consultant summative assessments for: Abdominal pain Breathing difficulties Acute life threatening event Concerning presentation Head injury Mental health
Alternatively an ACAT (by a consultant) may be utilised which covers 3 or more presentations.
Additional Major Presentations
Consultant assessments for: All 5 major trauma competences. One patient may cover up to two competences if appropriate. Or ATLS, ATNC or ETC with reflection.
Additional acute presentations
Consultant assessments for: Traumatic limb/joint injuries Interpretation of abnormal blood gas Abnormal blood glucose
14
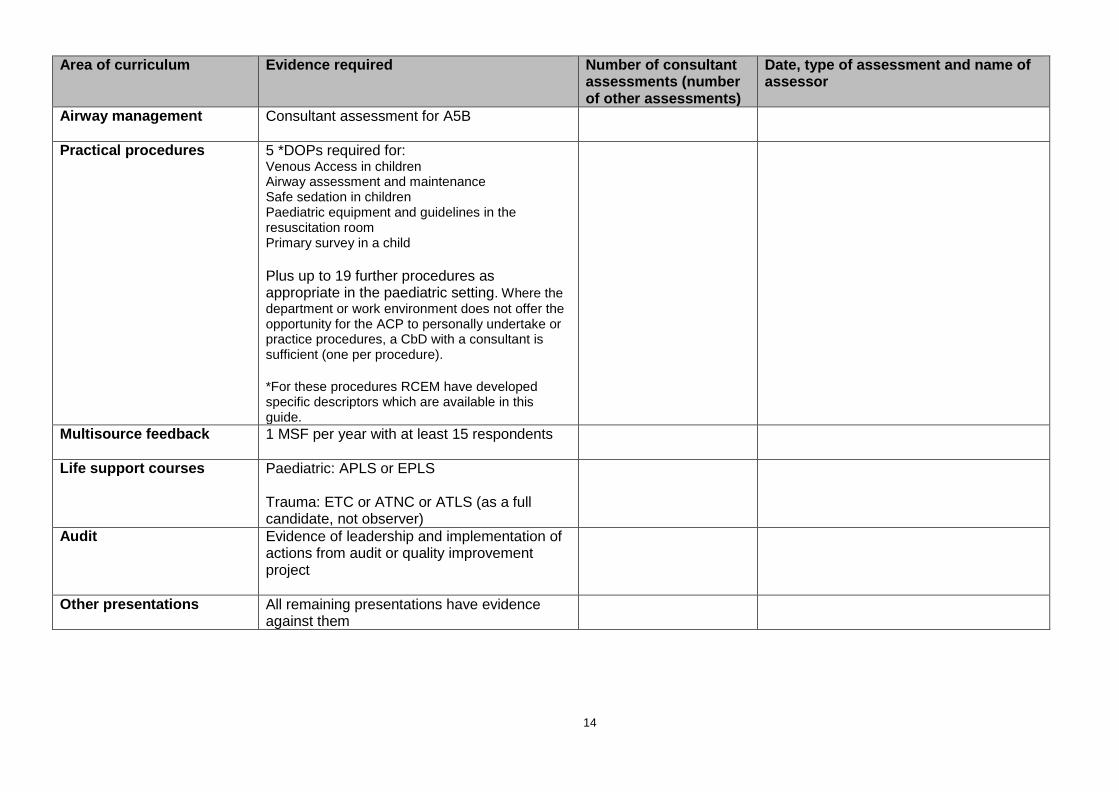
Area of curriculum Evidence required Number of consultant assessments (number of other assessments)
Date, type of assessment and name of assessor
Airway management Consultant assessment for A5B
Practical procedures 5 *DOPs required for: Venous Access in children Airway assessment and maintenance Safe sedation in children Paediatric equipment and guidelines in the resuscitation room Primary survey in a child
Plus up to 19 further procedures as appropriate in the paediatric setting. Where the
department or work environment does not offer the opportunity for the ACP to personally undertake or practice procedures, a CbD with a consultant is sufficient (one per procedure). *For these procedures RCEM have developed specific descriptors which are available in this guide.
Multisource feedback 1 MSF per year with at least 15 respondents
Life support courses Paediatric: APLS or EPLS Trauma: ETC or ATNC or ATLS (as a full candidate, not observer)
Audit Evidence of leadership and implementation of actions from audit or quality improvement project
Other presentations All remaining presentations have evidence against them

15
Appendix Two: Assessment Descriptors and Assessment Forms for Emergency Care Advanced Clinical Practitioners

16
Royal College of Emergency Medicine
Consultant-Led Mini-Clinical Evaluation Exercise - Mini- CEX
Name of trainee:
Year of Training:
Assessor: GMC/NMC/HCPC No:
Grade of assessor:
Date / /
Case discussed (brief description) Diagnosis
Focus of assessment –
Examination
Diagnosis
Management
Communication History
Please TICK to indicate the standard of the
trainee’s performance in each area
Not observed
Further core
learning needed
Demonstrates good practice Demonstrates
excellent practice
Must address learning points
highlighted below
Should address learning points
highlighted below
Initial approach
History and information gathering
Examination
Investigation
Clinical decision making and judgment
Communication with patient, relatives, staff
Overall plan
Professionalism
For summative Mini-CEX
Unsuccessful
Successful
Things done particularly well
Learning points
Action points
Assessor Signature: Trainee Signature:
17
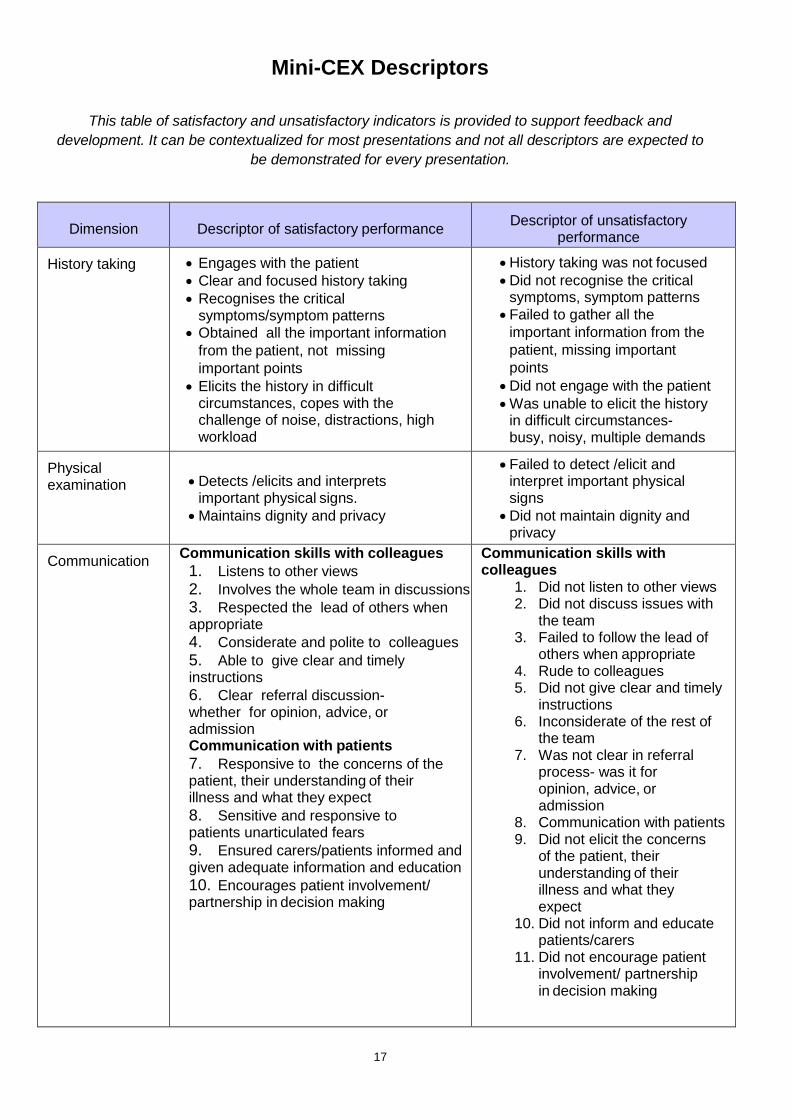
Mini-CEX Descriptors
This table of satisfactory and unsatisfactory indicators is provided to support feedback and
development. It can be contextualized for most presentations and not all descriptors are expected to
be demonstrated for every presentation.
Dimension Descriptor of satisfactory performance Descriptor of unsatisfactory
performance
History taking Engages with the patient
Clear and focused history taking
Recognises the critical symptoms/symptom patterns
Obtained all the important information
from the patient, not missing
important points
Elicits the history in difficult circumstances, copes with the challenge of noise, distractions, high workload
History taking was not focused
Did not recognise the critical symptoms, symptom patterns
Failed to gather all the
important information from the
patient, missing important
points
Did not engage with the patient
Was unable to elicit the history in difficult circumstances- busy, noisy, multiple demands
Physical examination Detects /elicits and interprets
important physical signs.
Maintains dignity and privacy
Failed to detect /elicit and interpret important physical signs
Did not maintain dignity and privacy
Communication Communication skills with colleagues
1. Listens to other views
2. Involves the whole team in discussions
3. Respected the lead of others when appropriate
4. Considerate and polite to colleagues
5. Able to give clear and timely instructions
6. Clear referral discussion- whether for opinion, advice, or admission Communication with patients
7. Responsive to the concerns of the patient, their understanding of their illness and what they expect
8. Sensitive and responsive to patients unarticulated fears
9. Ensured carers/patients informed and given adequate information and education
10. Encourages patient involvement/ partnership in decision making
Communication skills with colleagues
1. Did not listen to other views 2. Did not discuss issues with
the team 3. Failed to follow the lead of
others when appropriate 4. Rude to colleagues 5. Did not give clear and timely
instructions 6. Inconsiderate of the rest of
the team 7. Was not clear in referral
process- was it for opinion, advice, or admission
8. Communication with patients 9. Did not elicit the concerns
of the patient, their understanding of their illness and what they expect
10. Did not inform and educate patients/carers
11. Did not encourage patient involvement/ partnership in decision making

18
Dimension Descriptor of satisfactory performance Descriptor of unsatisfactory
performance
Clinical judgement-clinical decision making
Identifies the most likely diagnosis in a given situation
Appropriately judicial in the use of diagnostic tests
Able to construct a comprehensive and likely differential diagnosis
Able to correctly identify those who
need admission and those who can be
safely discharged.
Recognised atypical presentation
Able to recognise the urgency of the case
Able to select the most effective treatments
Made decisions in a timely fashion
Decisions reflected clear understanding of underlying principles
Reassessed the patient
Anticipated interventions and responded with alacrity
Reviewed the effect of interventions and took appropriate action
Did not identify the most likely diagnosis in a given situation
Was not discriminatory in the use of diagnostic tests
Did not construct a comprehensive and likely differential diagnosis
Did not correctly identify those
who need admission and those
who can be safely discharged.
Did not recognise atypical presentation
Did not recognise the urgency of the case
Did not select the most effective treatments
Did not make decisions in a timely fashion
Decisions did not reflect clear understanding of underlying principles
Did not reassess the patient
Did not anticipate interventions and slow to respond
Did not review effect of interventions
Professionalism Respected confidentiality
Protect the patients dignity
Sensitive and respectful of patients opinions/hopes/fears
Explained plan and risks in a way
the patient could understand
Did not respect confidentiality
Did not protect the patients dignity
Insensitive to patients opinions/hopes/fears
Did not explain plan and risks in
a way the patient could
understand
Organisation and efficiency
Demonstrated efficiency in progressing the case
Was slow to progress the case
Overall care Ensure patient was in a safe monitored environment
Anticipated or recognised complications
Focused sufficiently on safe practice
Was aware of and followed published standards guidelines or protocols
Follow infection control measures
Safe Prescription and provision of therapeutics
Did not ensure patient was in a safe monitored environment
Did not anticipate or recognise complications
Did not focus sufficiently on safe practice
Did not follow published standards guidelines or protocols
Did not follow infection control measures
Did not safely prescribe/provide therapeutics

19
Emergency Care ACP Mini-CEX Summative Descriptors for Major Presentations
Anaphylaxis
Unconscious/Altered Mental State
Shock
Trauma
Sepsis
1 Anaphylaxis
Expected behaviours
Initial approach ABCD approach, including GCS
Asks for vital signs including SPaO2, blood sugar
Requests monitoring
Recognises physiological abnormalities
Looks for obvious cause of shock (e.g. bleeding)
Secures iv access
History Obtains targeted history from patient
Obtains collateral history form friends, family, paramedics- cover PMH
Recognises the importance of treatment before necessarily getting all information
Obtains previous notes
Examination Detailed physical examination which must include physical signs that would differentiate between haemorrhagic, hypovolaemic , cardiogenic and septic causes for shock
Investigation Asks for appropriate tests-
arterial blood gas or venous gas and lactate
FBC,
U&Es,
clotting studies,
LFTs, toxicology,
Cross match as indicated
blood and urine culture,
CK and troponin,
ECG,
CXR,
Familiar with use of US to look for IVC compression and cardiac tamponade
Clinical decision making and judgement
Forms diagnosis and differential diagnosis including:
Trauma-haemorrhagic, blood loss control form direct pressure, pelvic splintage, emergency surgery or interventional radiology
Gastrointestinal - upper and lower GI bleed, or fluid loss form D&V
Cardiogenic - STEMI, tachy and brady dysrhythmia
Infection- sepsis, knows sepsis bundle
Endocrine - Addison’s disease, DKA
Neurological - neurogenic shock
Poisoning - TCAs, cardio toxic drugs
Communication Effectively communicates with both patient and colleagues
Organisation and efficiency
Manages time well – does not appear rushed but completes critical tasks in a timely way.
Uses staff and delegates appropriately
Overall plan Identifies immediate life threats and readily reversible causes
Stabilises and prepares for further investigation, treatment and admission
Professionalism Behaves in a professional manner
20
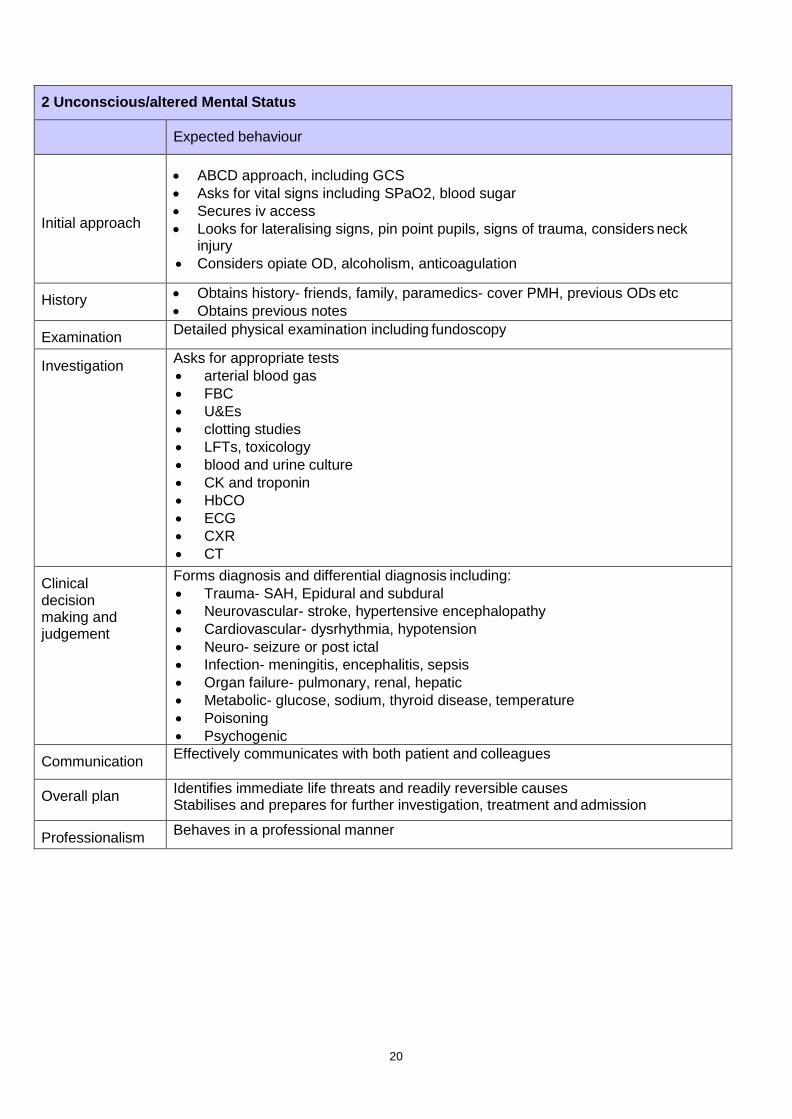
2 Unconscious/altered Mental Status
Expected behaviour
Initial approach
ABCD approach, including GCS
Asks for vital signs including SPaO2, blood sugar
Secures iv access
Looks for lateralising signs, pin point pupils, signs of trauma, considers neck injury
Considers opiate OD, alcoholism, anticoagulation
History Obtains history- friends, family, paramedics- cover PMH, previous ODs etc
Obtains previous notes
Examination Detailed physical examination including fundoscopy
Investigation Asks for appropriate tests
arterial blood gas
FBC
U&Es
clotting studies
LFTs, toxicology
blood and urine culture
CK and troponin
HbCO
ECG
CXR
CT
Clinical decision making and judgement
Forms diagnosis and differential diagnosis including:
Trauma- SAH, Epidural and subdural
Neurovascular- stroke, hypertensive encephalopathy
Cardiovascular- dysrhythmia, hypotension
Neuro- seizure or post ictal
Infection- meningitis, encephalitis, sepsis
Organ failure- pulmonary, renal, hepatic
Metabolic- glucose, sodium, thyroid disease, temperature
Poisoning
Psychogenic
Communication Effectively communicates with both patient and colleagues
Overall plan Identifies immediate life threats and readily reversible causes Stabilises and prepares for further investigation, treatment and admission
Professionalism Behaves in a professional manner

21
3 Shock
Expected behaviour
Initial approach ABCD approach, including GCS
Asks for vital signs including SPaO2, blood sugar
Requests monitoring
Recognises physiological abnormalities
Looks for obvious cause of shock e.g. bleeding
Secures iv access
History Obtains targeted history from patient
Obtains collateral history form friends, family, paramedics- cover PMH
Recognises the importance of treatment before necessarily getting all information
Obtains previous notes
Examination Detailed physical examination which must include physical signs that would different between haemorragic, hypovolaemic , cardiogenic and septic causes for shock
Investigation Asks for appropriate tests
Arterial blood gas or venous gas and lactate
FBC
U&Es
clotting studies
LFTs, toxicology
Cross match as indicated
blood and urine culture
CK and troponin
ECG
CXR
Familiar with use of US to look for IVC compression and cardiac tamponade
Clinical decision making and judgement
Forms diagnosis and differential diagnosis including:
Trauma-haemorrhagic, blood loss control form direct pressure, pelvic splintage, emergency surgery or interventional radiology
Gastrointestinal - upper and lower GI bleed, or fluid loss form D&V
Cardiogenic - STEMI, tachy and brady dysrhythmia,
Infection- sepsis, knows sepsis bundle
Endocrine - Addison’s disease, DKA
Neurological - neurogenic shock
Poisoning - TCAs, cardio toxic drugs
Communication Effectively communicates with both patient and colleagues
Overall plan Identifies immediate life threats and readily reversible causes Stabilises and prepares for further investigation, treatment and admission
Professionalism Behaves in a professional manner

22
4 Major Trauma
Expected behaviour
Initial approach Knows when to activate the trauma team (based on local guidelines)
Able to perform a rapid primary survey, including care of the c spine and oxygen delivery
Can safely log roll patient off spinal board
Able to assess disability, using AVPU or GCS
Asks for vital signs
Able to request imaging at end of primary survey
Knows when to request specialty opinion and/or further imaging
History Obtains history of mechanism of injury from paramedics
Able to use AMPLE history
Examination After completing a primary survey is able to perform detailed secondary survey
Investigation Asks for appropriate tests
Primary survey films
CT imaging
arterial blood gas
FBC
U&Es
clotting studies
PT
toxicology
ECG
FAST
UO by catheterisation
Appropriate use of NG
Clinical decision making and judgement
Forms differential diagnosis and management plan based on:
Able to identify and mange life threatening injuries as part of primary survey
Able to identify the airway that may be at risk
Can identify shock, know it classification and treatment
Safely prescribes fluids, blood products and drugs.
Can identify those patients who need urgent interventions or surgery before imaging or secondary survey
Can safely interpret imaging and test results
Demonstrates safe disposition of trauma patient after secondary survey
Able to identify those patients that be safely discharged home
Communication Effectively communicates with both patient and other members of the trauma team
Overall plan Identifies immediate life threats and readily reversible causes. Stabilises and prepares for further investigation, treatment and admission
Professionalism Behaves in a professional manner

23
5 Sepsis
Expected behaviour
Initial approach Initial approach based on ABCD system- ensuring early monitoring of vital signs including temperature,SPaO2, blood sugar
Can interpret early warning medical score as indicators of sepsis (EMEWS or similar)
Aware of systemic inflammatory response criteria (SIRS), and that 2 or more may indicate sepsis o T>38 or < 36
o HR > 90 o RR > 20 o WCC > 12 or < 4
History Obtains history of symptoms leading up to illness
Able to take a collateral history, form paramedics, friends and family
Able to use AMPLE history
Looks specifically for conditions causing immunocompromise
Examination Able to perform a competent examination looking for 1. Possible source of infection 2. Secondary organ failure
Investigation Asks for appropriate tests
FBC
U&Es
clotting studies
ABGs or VBGs
Lactate, ScVo2
Blood cultures
ECG
CXR
Urinalysis +/- catheterisation
Other interventions which may help find source of sepsis o Swabs o PCR o Pus
Considers need for further imaging

24
Clinical decision making and judgement
Form a management plan with initial interventions being:
Oxygen therapy
Fluid bolus, starting with 20 mls/Kg
IV Antibiotics, based on likely source of infection
Documentation of a physiological score, which can be repeated
Be able to reassess Recognises and is able to support physiological markers of organ dysfunction, such as:-
Systolic BP < 90 mm Hg
PaO2 < 8 Kpa
Lactate > 5
Reduced GCS
Urine output < 30 mls/hr Demonstrates when to use invasive monitoring, specifically
CVP line
Arterial line
Demonstrates when to start inotropes, Noradrenaline v dopamine Demonstrates how to set up an inotrope infusion
Communication Effectively communicates with both patient and other members of the acute care team
Overall plan Identifies sepsis Implements sepsis bundle Stabilises patient, reassesses and able to inform and/or hand over to critical care team
Professionalism Behaves in a professional manner

25
Mini-CEX Summative Descriptors for Acute Presentations Chest pain
Abdominal pain
Breathlessness
Mental Health
Head Injury
1 Chest Pain
Expected behaviours
Initial approach Ensures monitoring, i.v. access and defibrillator nearby.
Ensures vital signs are measured including SpO2
History Takes focused history (having established conscious with patent airway) of chest pain including
o site o severity o onset o nature o radiation o duration o frequency o precipitating and relieving factors o Previous similar pains and associated symptoms
Systematically explores for symptoms of life threatening chest pain
Assesses ACS risk factors
Specifically asks about previous medication and past medical history
Seeks information from paramedics, relatives and past medical notes including previous ECGs
Examination On examination has ABCD approach with detailed cardiovascular and respiratory examination including detection of peripheral pulses, blood pressure measurement in both arms, elevated JVP, palpation of apex beat, auscultation e.g. for aortic stenosis and incompetence, pericardial rub, signs of cardiac failure, and pleural rubs
Investigation Ensures appropriate investigation
ECG (serial)
ABG
FBC, U&Es
troponin and d dimer if indicated
Chest x-ray
Communication Effectively communicates with both patient and colleagues
Prescribing Able to relieve pain by appropriate prescription
Clinical decision making and judgement
Able to formulate a full differential diagnosis and the most likely cause in this case.
Overall plan Stabilises and safely prepares the patient for further treatment and investigation
Professionalism Behaves in a professional manner

26
2 Abdominal Pain
Expected behaviours
Initial approach Ensures appropriate monitoring in place and iv access
Establishes that vital signs measured
History Takes focused history of abdominal pain including o site o severity o onset o nature o radiation o duration o frequency o precipitating and relieving factors o previous similar pains and associated symptoms
Systematically explores for symptoms of life threatening abdominal pain
Specifically asks about previous abdominal operations
Considers non abdominal causes- MI, pneumonia, DKA, hypercalcaemia, sickle, porphyria
Seeks information from paramedics, relatives and past medical notes
Examination Able to undertake detailed examination for abdominal pain (ensuring adequate exposure and examining for the respiratory causes of abdominal pain) including 1. Inspection, palpation, auscultation and percussion of the abdomen 2. Looks for herniae and scars 3. Examines loins, genitalia and back 4. Undertakes appropriate rectal examination
Investigation Ensures appropriate investigation-
ECG
ABG
FBC
U&Es
LFTs
amylase
erect chest x-ray
and abdominal x-rays if obstruction or perforation suspected
Clinical decision making and judgement
Able to formulate a full differential diagnosis and the most likely cause in this case
Communication Effectively communicates with both patient and colleagues
Prescribing Able to relieve pain by appropriate prescription
Overall plan Stabilises (if appropriate)and safely prepares the patient for further treatment and investigation
Professionalism Behaves in a professional manner

27
3 Breathlessness
Expected behaviours
Initial approach Ensures monitoring, iv access gained, O2 therapy
Ensures vital signs are measured including Spa O2
History If patient able, trainee takes focused history of breathlessness including onset,
o severity o duration o frequency o precipitating and relieving factors o previous similar episodes o associated symptoms
Systematically explores for symptoms of life threatening causes of breathlessness
Takes detailed respiratory history
Specifically asks about medication and past medical history
Seeks information from paramedics, relatives and past medical notes including previous chest x-rays and blood gases
Examination On examination has ABCD approach with detailed cardiovascular and
respiratory examination including, work of breathing, signs of
respiratory distress
detection of wheeze
crepitations
effusions
areas of consolidation
Investigation Ensures appropriate investigation
ECG
ABG
FBC
U&Es
troponin and d dimer if indicated
Chest x-ray
Able to interpret chest x-ray correctly
Clinical decision making and judgement
Able to formulate a full differential diagnosis and the most likely cause in this case Knows BTS guidelines for treatment of Asthma and PE
Communication Effectively communicates with both patient and colleagues
Prescribing Able to prescribe appropriate medication including oxygen therapy, bronchodilators, GTN, diuretics
Able to identify which patients would benefit from NIV
Overall plan Stabilises and safely prepares the patient for further treatment and investigation
Professionalism Behaves in a professional manner
28
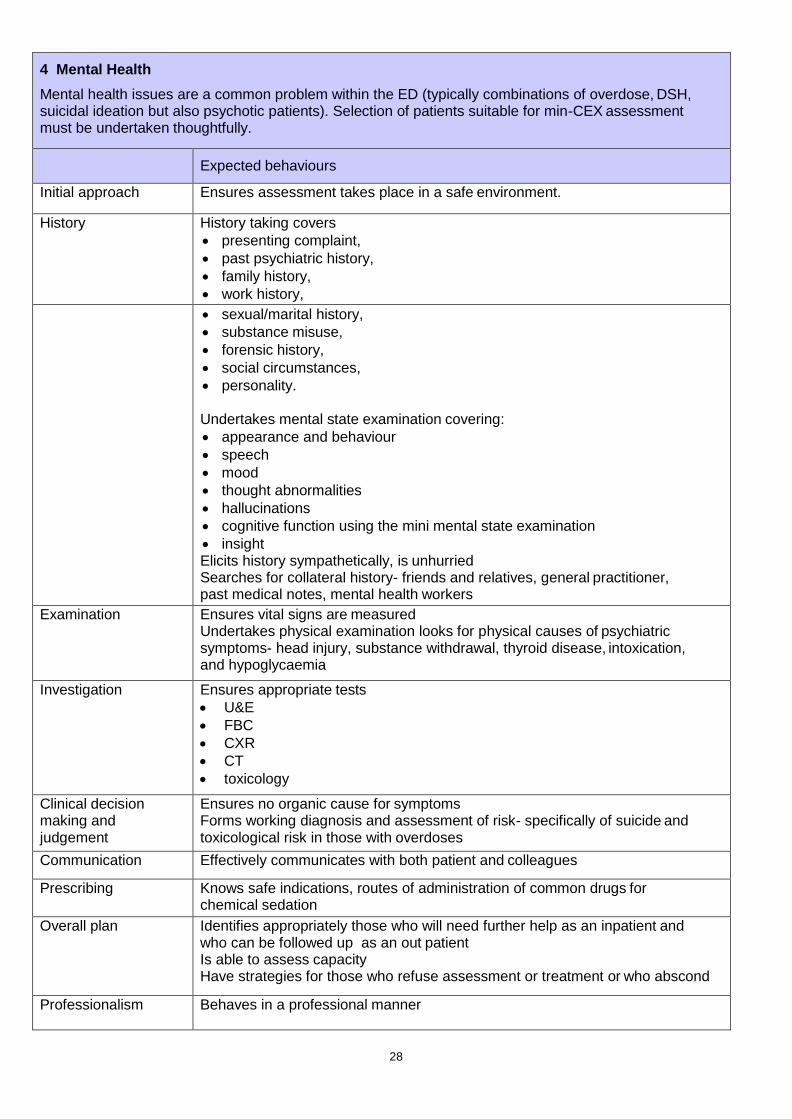
4 Mental Health
Mental health issues are a common problem within the ED (typically combinations of overdose, DSH, suicidal ideation but also psychotic patients). Selection of patients suitable for min-CEX assessment must be undertaken thoughtfully.
Expected behaviours
Initial approach Ensures assessment takes place in a safe environment.
History History taking covers
presenting complaint,
past psychiatric history,
family history,
work history,
sexual/marital history,
substance misuse,
forensic history,
social circumstances,
personality.
Undertakes mental state examination covering:
appearance and behaviour
speech
mood
thought abnormalities
hallucinations
cognitive function using the mini mental state examination
insight Elicits history sympathetically, is unhurried Searches for collateral history- friends and relatives, general practitioner, past medical notes, mental health workers
Examination Ensures vital signs are measured Undertakes physical examination looks for physical causes of psychiatric symptoms- head injury, substance withdrawal, thyroid disease, intoxication, and hypoglycaemia
Investigation Ensures appropriate tests
U&E
FBC
CXR
CT
toxicology
Clinical decision making and judgement
Ensures no organic cause for symptoms Forms working diagnosis and assessment of risk- specifically of suicide and toxicological risk in those with overdoses
Communication Effectively communicates with both patient and colleagues
Prescribing Knows safe indications, routes of administration of common drugs for chemical sedation
Overall plan Identifies appropriately those who will need further help as an inpatient and who can be followed up as an out patient Is able to assess capacity Have strategies for those who refuse assessment or treatment or who abscond
Professionalism Behaves in a professional manner

29
5 Head Injury
Expected behaviours
Initial approach Ensures ABC is adequate and that neck is immobilised in the unconscious patient and those with neck pain. Ensures BM done
History Establishes history- o mechanism of injury o any loss of consciousness and duration o duration of any amnesia o headache o vomiting o associated injuries especially facial and ocular
Establishes if condition is worsening
Gains collateral history from paramedics, witnesses, friends/relatives and medical notes
Establishes if taking anticoagulants, is epileptic
Examination After ABC undertakes systematic neuro examination including
GCS
papillary reactions and size
cranial nerve and peripheral neurological examination
and seeks any cerebellar signs
Looks for signs of basal skull fracture
Examines scalp
Looks for associated injuries- neck, facial bones including jaw
Actively seeks injuries elsewhere
Investigation Is able to identify the correct imaging protocol for those with potentially significant injury -specifically the NICE guidelines
Clinical decision making and judgement
Is able to refer appropriately with comprehensive and succinct summary Knows which patients should be referred to N/surgery Is able to identify those patients suitable for discharge and ensures safe discharge.
Communication Effectively communicates with both patient and colleagues
Prescribing Able to safely relieve pain in the head injured patient
Overall plan Stabilises and safely prepares the patient for further treatment and investigation or safely discharges patient
Professionalism Behaves in a professional manner

30
Consultant-Led Case based Discussion CbD
Name of trainee:
Regulatory Body and Registration Number:
Assessor:
Case discussed (brief description) Diagnosis
Date of Discussion
Please TICK to indicate
the standard of the trainee’s performance in
each area
Not observed
Further core
learning needed
Demonstrates good practice
Demonstrates excellent practice
Must address learning points
highlighted below
Should address learning points
highlighted below
Record keeping
Review of investigations
Diagnosis
Treatment
Planning for subsequent care (in patient or discharged patients)
Clinical reasoning
Patient safety issues
Overall clinical care
Things done particularly well
Learning points
Action points
Assessor’s Signature: Trainee’s Signature:

31
CbD Descriptors
Domain Descriptor
Record keeping Records should be legible and signed. Should be structured and include provisional and differential diagnoses and initial investigation & management plan. Should record results and treatments given.
Review of investigations Undertook appropriate investigations. Results are recorded and correctly interpreted. Any Imaging should be reviewed in the light of the trainees interpretation
Diagnosis The correct diagnosis was achieved with an appropriate differential diagnosis. Were any important conditions omitted?
Treatment Emergency treatment was correct and response recorded. Subsequent treatments appropriate and comprehensive
Planning for subsequent care (in patient or discharged patients)
Clear plan demonstrating expected clinical course, recognition of and planning for possible complications and instructions to patient (if appropriate)
Clinical reasoning Able to integrate the history, examination and investigative data to arrive at a logical diagnosis and appropriate treatment plan taking into account the patients co morbidities and social circumstances
Patient safety issues Able to recognise effects of systems, process, environment and staffing on patient safety issues
Overall clinical care The case records and the trainees discussion should demonstrate that this episode of clinical care was conducted in accordance with good clinical practice and to a good overall standard

32
Direct Observation of Procedural Skills – DOPs
Name of trainee:
Regulatory Body and Registration Number:
Assessor:
Procedure observed (including indications)
Date of Assessment
Please TICK to indicate the standard of the trainee’s performance in each area
Not observed
Further
core learning needed
Demonstrates good practice
Demonstrates excellent practice
Must address learning points
highlighted below
Should address learning points
highlighted below
Indication for procedure discussed with assessor
Obtaining informed consent
Appropriate preparation including monitoring, analgesia and sedation
Technical skills and aseptic technique
Situation awareness and clinical judgement
Safety, including prevention and management of complications
Care /investigations immediately post procedure
Professionalism, communication and consideration for patient, relatives and staff
Documentation in the notes
Completed task appropriately
Things done particularly well
Learning points
Action points
Assessor’s Signature: Trainee’s Signature:

33
Practical Procedures DOPs Descriptors • Basic airway • Trauma - primary survey • Wound management • Fracture manipulation and joint reduction
1 Basic airway management including adjuncts e.g. BVM, oxygen delivery
Observed behaviour Task Completed
1. Is able to assess the adult airway and in the obstructed patient provide a patent airway by simple manoeuvres and the use of adjuncts and suction.
2. Undertakes this in a timely and systematic way.
3. Assesses depth of respiration and need for BVM.
4. Can successfully BVM.
5. Knows and can show how to deliver high flow 02
6. Knows other O2 delivery systems typically in ED- fixed concentration masks, nasal specs, Mapleson C circuits.
7. Consents the patient
2 Perform a primary survey of a potentially multiple injured trauma patient
Observed behaviour Task Completed
1. Ensures safe transfer of patient onto ED trolley
2. Assesses airway, establishes if obstructed, corrects and ensures delivery of 100%O2
3. Concurrently ensures cervical spine immobilisation (using collar, sandbags and tape)
4. Exposes chest identified raised respiratory rate, chest asymmetry, chest wall bruising, air entry (anteriorly and laterally) and percussion (laterally). Identifies life threatening problems and correctly carries out associated procedures
5. Examines for signs of shock, ensures monitoring established and has gained iv accessX2
6. If shocked looks for potential sites of blood loss- abdomen, pelvis and limbs.
7. Can formulate differential for shocked patient
8. Establishes level of consciousness and seeks lateralising signs
9. Examines limbs, spine and rectum ensuring safe log roll.
34
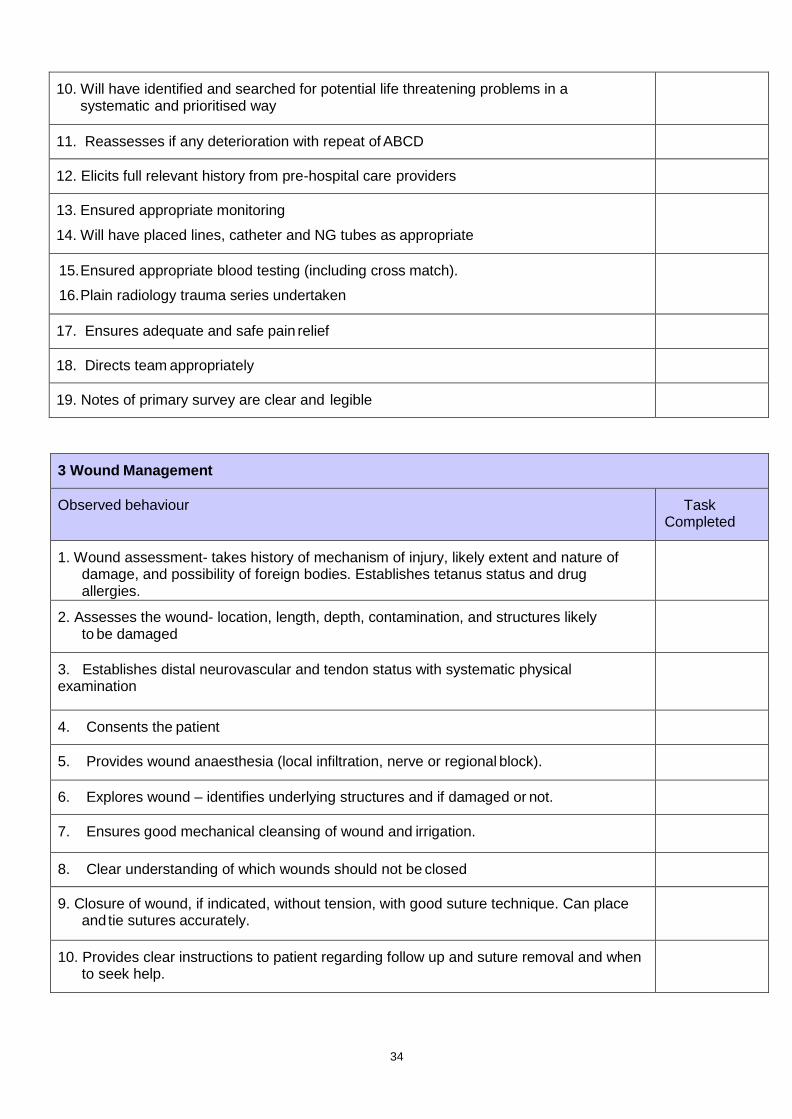
10. Will have identified and searched for potential life threatening problems in a systematic and prioritised way
11. Reassesses if any deterioration with repeat of ABCD
12. Elicits full relevant history from pre-hospital care providers
13. Ensured appropriate monitoring
14. Will have placed lines, catheter and NG tubes as appropriate
15. Ensured appropriate blood testing (including cross match).
16. Plain radiology trauma series undertaken
17. Ensures adequate and safe pain relief
18. Directs team appropriately
19. Notes of primary survey are clear and legible
3 Wound Management
Observed behaviour Task Completed
1. Wound assessment- takes history of mechanism of injury, likely extent and nature of damage, and possibility of foreign bodies. Establishes tetanus status and drug allergies.
2. Assesses the wound- location, length, depth, contamination, and structures likely to be damaged
3. Establishes distal neurovascular and tendon status with systematic physical examination
4. Consents the patient
5. Provides wound anaesthesia (local infiltration, nerve or regional block).
6. Explores wound – identifies underlying structures and if damaged or not.
7. Ensures good mechanical cleansing of wound and irrigation.
8. Clear understanding of which wounds should not be closed
9. Closure of wound, if indicated, without tension, with good suture technique. Can place and tie sutures accurately.
10. Provides clear instructions to patient regarding follow up and suture removal and when to seek help.
35
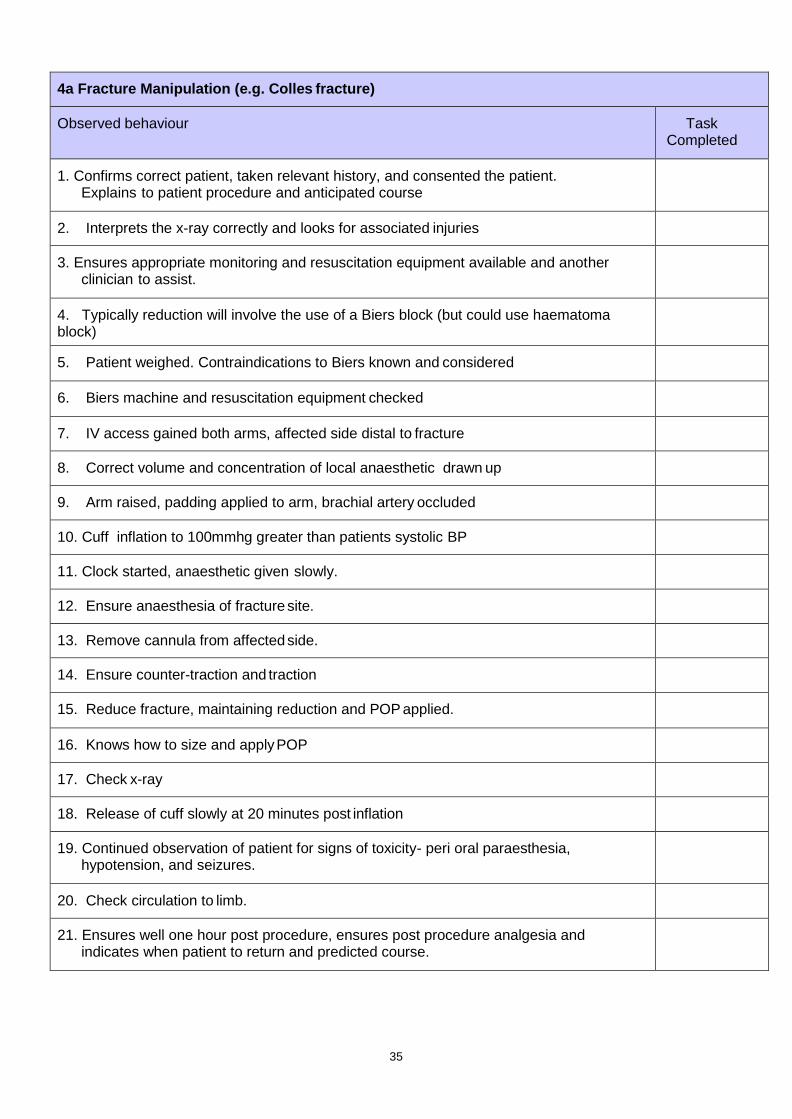
4a Fracture Manipulation (e.g. Colles fracture)
Observed behaviour Task Completed
1. Confirms correct patient, taken relevant history, and consented the patient. Explains to patient procedure and anticipated course
2. Interprets the x-ray correctly and looks for associated injuries
3. Ensures appropriate monitoring and resuscitation equipment available and another clinician to assist.
4. Typically reduction will involve the use of a Biers block (but could use haematoma block)
5. Patient weighed. Contraindications to Biers known and considered
6. Biers machine and resuscitation equipment checked
7. IV access gained both arms, affected side distal to fracture
8. Correct volume and concentration of local anaesthetic drawn up
9. Arm raised, padding applied to arm, brachial artery occluded
10. Cuff inflation to 100mmhg greater than patients systolic BP
11. Clock started, anaesthetic given slowly.
12. Ensure anaesthesia of fracture site.
13. Remove cannula from affected side.
14. Ensure counter-traction and traction
15. Reduce fracture, maintaining reduction and POP applied.
16. Knows how to size and apply POP
17. Check x-ray
18. Release of cuff slowly at 20 minutes post inflation
19. Continued observation of patient for signs of toxicity- peri oral paraesthesia, hypotension, and seizures.
20. Check circulation to limb.
21. Ensures well one hour post procedure, ensures post procedure analgesia and indicates when patient to return and predicted course.

36
4b Reduction of a dislocated joint (e.g. shoulder, ankle)
Observed behaviour Task Completed
1. Confirms correct patient, takes focused history and consents the patient.
2. Takes focused history and examination to establish that sedation is safe.
3. Undertakes examination to confirm dislocation and assesses distal neurovascular function
4. Interprets the x-ray correctly and looks for associated injuries
5. Ensures appropriate monitoring and resuscitation equipment available and another clinician to assist.
6. Gains IV access, and has correct volume of opiate, benzodiazepine or other
agent e.g. Ketamine, in correctly labelled syringes.
7. Knows the pharmacology of these drugs and their antagonists
8. Explains to patient procedure and anticipated course.
9. Ensures another clinician present
10. Gives drugs in controlled way in monitored environment with patient receiving oxygen.
11. Establishes sedated- still responsive to verbal commands.
12. Undertakes reduction in gentle and controlled manner.
13. Confirms reduction by physical examination and checks distal neurovascular function
14. Immobilises - sling, pop correct patient, taken relevant history, and consented the patient. Explains to patient procedure and anticipated course
15. Gets check x-ray- checks reduced and no additional fractures detected.
16. Ensures observed and monitored until fully recovered.
17. Rechecks neurovascular function
18. Ensures well one hour post procedure, ensures post procedure analgesia and indicates when patient to return and predicted course.
37
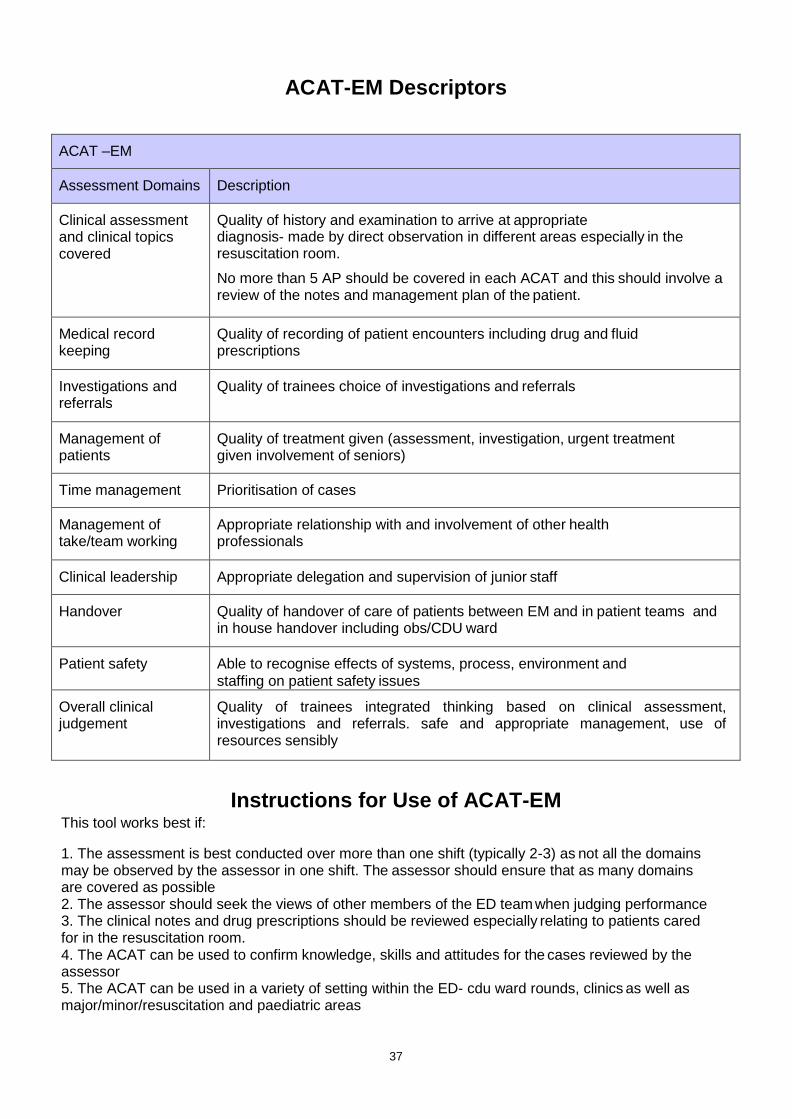
ACAT-EM Descriptors
ACAT –EM
Assessment Domains Description
Clinical assessment and clinical topics covered
Quality of history and examination to arrive at appropriate diagnosis- made by direct observation in different areas especially in the resuscitation room.
No more than 5 AP should be covered in each ACAT and this should involve a review of the notes and management plan of the patient.
Medical record keeping
Quality of recording of patient encounters including drug and fluid prescriptions
Investigations and referrals
Quality of trainees choice of investigations and referrals
Management of patients
Quality of treatment given (assessment, investigation, urgent treatment given involvement of seniors)
Time management Prioritisation of cases
Management of take/team working
Appropriate relationship with and involvement of other health professionals
Clinical leadership Appropriate delegation and supervision of junior staff
Handover Quality of handover of care of patients between EM and in patient teams and in house handover including obs/CDU ward
Patient safety Able to recognise effects of systems, process, environment and
staffing on patient safety issues
Overall clinical judgement
Quality of trainees integrated thinking based on clinical assessment, investigations and referrals. safe and appropriate management, use of resources sensibly
Instructions for Use of ACAT-EM This tool works best if:
1. The assessment is best conducted over more than one shift (typically 2-3) as not all the domains may be observed by the assessor in one shift. The assessor should ensure that as many domains are covered as possible 2. The assessor should seek the views of other members of the ED team when judging performance 3. The clinical notes and drug prescriptions should be reviewed especially relating to patients cared for in the resuscitation room. 4. The ACAT can be used to confirm knowledge, skills and attitudes for the cases reviewed by the assessor 5. The ACAT can be used in a variety of setting within the ED- cdu ward rounds, clinics as well as major/minor/resuscitation and paediatric areas

38
The Acute Care Assessment Tool (ACAT-EM) Form
Name of Trainee:
Regulatory Body and Registration Number:
Assessor
Setting, ED, CDU, Clinic, other
Date
Timing, duration and level of responsibility
Acute presentations covered (5 max for EM)
Please TICK to indicate the standard of the trainee’s performance in each area
Not observed
Further core
learning needed
Demonstrates good practice
Demonstrates excellent practice Must
address learning points
highlighted below
Should address
learning points highlighted
below Clinical Assessment
Medical record keeping
Time management
Management of the team
Clinical leadership
Patient safety
Handover
Overall Clinical Judgement
Which aspects were done well Learning points
Unsatisfactory AP? Plan for further AP assessment, specify WPBA tool and review date
Trainees Comments Action points
Assessor’s Signature: Trainee’s Signature:
39
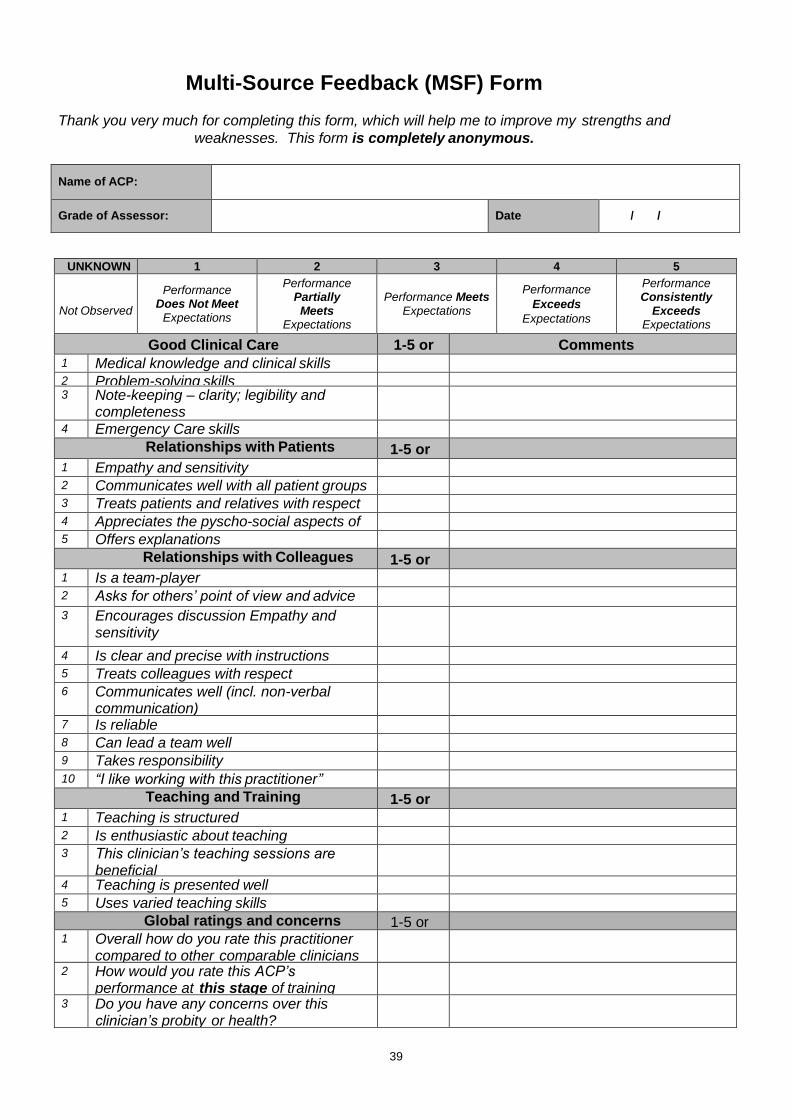
Multi-Source Feedback (MSF) Form
Thank you very much for completing this form, which will help me to improve my strengths and
weaknesses. This form is completely anonymous.
Name of ACP:
Grade of Assessor:
Date / /
UNKNOWN 1 2 3 4 5
Not Observed
Performance Does Not Meet
Expectations
Performance Partially Meets
Expectations
Performance Meets Expectations
Performance
Exceeds
Expectations
Performance Consistently
Exceeds Expectations
Good Clinical Care 1-5 or UK
Comments 1 Medical knowledge and clinical skills 2 Problem-solving skills 3 Note-keeping – clarity; legibility and
completeness
4 Emergency Care skills
Relationships with Patients 1-5 or UK
1 Empathy and sensitivity 2 Communicates well with all patient groups 3 Treats patients and relatives with respect 4 Appreciates the pyscho-social aspects of
patient care
5 Offers explanations
Relationships with Colleagues 1-5 or UK
1 Is a team-player 2 Asks for others’ point of view and advice
3 Encourages discussion Empathy and sensitivity
4 Is clear and precise with instructions 5 Treats colleagues with respect 6 Communicates well (incl. non-verbal
communication)
7 Is reliable 8 Can lead a team well 9 Takes responsibility
10 “I like working with this practitioner”
Teaching and Training 1-5 or UK
1 Teaching is structured 2 Is enthusiastic about teaching 3 This clinician’s teaching sessions are
beneficial
4 Teaching is presented well 5 Uses varied teaching skills
Global ratings and concerns 1-5 or UK
1 Overall how do you rate this practitioner
compared to other comparable clinicians
2 How would you rate this ACP’s performance at this stage of training
3 Do you have any concerns over this clinician’s probity or health?

40
Patient Survey Tool
Communication with patients is a very important part of quality medical care. We would like to know how you feel about the way your practitioner communicated with you. Your answers are completely confidential, so please be as open and as honest as you can. Thank you very much for your help and co-operation.
The Clinician Poor Fair Good Very Good
Excellent
Greeted me in a way that made me feel comfortable
1 2 3 4 5
Treated me with respect 1 2 3 4 5
Showed interest in my ideas about my health
1 2 3 4 5
Understood my main health concerns 1 2 3 4 5
Paid attention to me (looked at me and listened carefully)
1 2 3 4 5
Let me talk without interruptions 1 2 3 4 5
Gave as much information as I wanted 1 2 3 4 5
Talked in terms I could understand 1 2 3 4 5
Checked to be sure I understood everything 1 2 3 4 5
Encouraged me to ask questions 1 2 3 4 5
Involved me in decisions as much as I wanted
1 2 3 4 5
Discussed next steps including any follow up plans
1 2 3 4 5
Showed care and concern 1 2 3 4 5
Spent the right amount of time with me 1 2 3 4 5
Clinician’s Name:
Validated by:

41
Mini-CEX Summative Descriptors for PEM ACP
Acute Presentations 1. Abdominal pain 2. Fever 3. Breathlessness 4. Pain
1 Abdominal pain
Expected behaviour
Initial approach ABCD approach
Asks for vital signs
History Obtains history-patient, friends, family, paramedics- cover PMH
Obtains previous notes
Examination General appearance – listlessness, features of dehydration and shock
Detailed physical examination including assessment of dehydration
Abdominal examination for guarding and distention
Inguinal and testicular examination
Investigation Asks for appropriate tests
FBC,
U&Es,
LFTs,
blood and urine culture
Abdominal x-ray for those with? obstruction
Clinical decision making and judgement
Forms diagnosis and differential diagnosis for D&V including:
Intussusception
Bacterial and viral gastroenteritis
Food poisoning
Pyelonephritiss for abdominal pain
hernia,
intussusception,
pyloric stenosis,
appendicitis,
UTI,
viral URTI,
lower lobe pneumonia
Communication Effectively communicates with both patient and colleagues
Overall plan identifies immediate life threats and readily reversible causes
Able to classify degree of dehydration and prescribe appropriately
Stabilises and prepares for further investigation, treatment and admission.
Identifies which patients can be safely discharged
Professionalism Behaves in a professional manner

42
2 Assessment of the febrile child
Expected behaviour
Initial approach ABCD approach, including GCS
Asks for vital signs including o SPaO2, o temperature, o blood sugar.
Identifies patient that needs resuscitation
History Obtains history- parents, friends, paramedics- cover PMH,
Obtains previous notes
Identifies if immune deficient/ high risk-sickle, DM, CSF shunts, cardiac patients
Examination General appearance
Detailed physical examination focus on looking for causes of fever- o ENT, o neck stiffness, o chest for resp and cardiac causes, o abdomen, o CNS, o joints, o Skin/rash
Investigation Asks for appropriate tests
arterial blood gas
FBC,U&Es, o clotting studies, o LFTs, o toxicology, o blood and urine culture
Appropriate imaging including Chest x-ray
Clinical decision making and judgement
Forms diagnosis and differential diagnosis including: Infection Bacterial
otitis media,
UTI,
pneumonia,
meningitis,
cellulitis,
joint infection,
appendicitis Viral
chickenpox,
gastroenteritis Others
neoplastic,
salicylates,
hyperthyroidism Demonstrates knowledge of NICE guidelines for management of febrile child
Communication Effectively communicates with both child, parents and colleagues
Overall plan Stabilizes and prepares for further investigation, treatment and admission
Professionalism Behaves in a professional manner

43
3 Assessment of the breathless child
Expected behaviour
Initial approach ABCD approach focusing on o airway patency, o effort and efficacy of breathing, o effects of inadequate respiration o and cardiovascular status.
Ensures patent airway and high flow oxygen. Ensures monitoring
History Obtains history- parents, paramedics
Examination General appearance
Detailed physical examination with detection of stridor & wheeze,
Signs of heart failure
Investigation Asks for appropriate tests- o arterial blood as, o FBC, o U&Es, o clotting studies, o blood and urine culture, o blood sugar
Appropriate imaging Cxray
Clinical decision making and judgement
Forms diagnosis and differential diagnosis including:
Stridor: croup/epiglottitis
Wheeze: asthma/bronchiolitis
Fever :pneumonia Demonstrates knowledge of guidelines e.g. NICE for management of asthma. Knows of croup scoring system
Communication Effectively communicates with both child, parents and colleagues
Overall plan Stabilises and prepares for further investigation, treatment and admission. Seeks senior help early and appropriately
Professionalism Behaves in a professional manner

44
4 Assessment of the child in pain
Expected behaviour
Initial approach Recognises child in pain including behavioural and physiological changes
History Obtains history of the condition causing pain
Elicits past history of painful experiences and successful relieving measures
Examination Able to determine the cause of pain
Able to undertake pain assessment including the use of pain ladder and faces scale
Investigation Appropriate to the presentation
Clinical decision making and judgement
Ensures parent involvement
Selects most appropriate analgesic and route of administration
Demonstrates comprehensive knowledge of drugs and dosages
Calculates dosage correctly
Considers use of distractive techniques
Communication Communicates effectively to both the child and parents. Sensitive and reassuring
Overall plan Ensures effective analgesia by repeated assessment and additional treatment if needed
Professionalism Behaves in a professional manner

45
Paediatric Practical Procedures DOPs Descriptors 1. Venous access 2. Airway assessment and maintenance 3. Paediatric equipment and guidelines in the resuscitation room 4. Primary survey in a child
1 Venous access in children
Trainee should identify suitable sites for cannulation in a child- specifically
the dorsum of the hand and foot,
cubital fossae,
external jugular,
scalp veins,
femoral vein,
IO. S/he should select appropriate route depending on the clinical case
For the fully conscious patient:
Should ensure adequate pain relief if appropriate- using topical anaesthetic
Should ensure clean site and use aseptic technique
Prepares equipment- cannulae, connections, steristrips, flush and blood collection bottles
Immobilisation of limb using other members of staff
Gains access, takes samples, connects, secures and flushes to ensure correct position
Splints limb
Writes up fluid to be administered (if any).
For those undergoing resuscitation (this DOPs will be unplanned but should not stop this valuable learning opportunity from being missed) a. femoral vein cannulation
Demonstrates correct anatomy and proposed site of puncture
Should ensure clean site and use aseptic technique
Prepares equipment- cannulae, connections, steristrips, flush and blood collection bottles
Immobilisation of limb using other members of staff
Gains access, takes samples, connects, secures and flushes to ensure correct position
b. Intraosseous insertion using either IO needle or EZ drill
Demonstrates correct anatomy and proposed site of insertion over the medial tibia.
Should ensure clean site and use aseptic technique
Prepares equipment- IO needle, connections, flush and syringe for collection of marrow blood
Successfully inserts, confirms secure and patent. Connects to giving set and three way tap, and gives fluid bolus
Knows complications of IO insertion If trainees cannot do IO needle insertion on real patient then they must demonstrate to their trainer they can do so using a mannequin

46
2 Basic airway manoevers in children
Preparation- can size nasophrayngeal and oral airways
Can select appropriate BVM
On arrival assesses airway for patency
Established if obstructed or not.
Uses suction, adjuncts and positioning appropriately
Ensures patent airway
Administers high flow oxygen with appropriate mask
Supports ventilation with BVM
Ensures concurrent monitoring including SpAO2, ECG
Correctly identifies those that will need intubation
Works effectively with medical and nursing colleagues to deliver effective care
3 Equipment and guidelines in the resuscitation room.
This is designed to ensure the trainee is familiar with and can access important paediatric resuscitation information and equipment
The trainee must demonstrate that:
Can calculate the child’s weight, defibrillation energy, ETT size, fluid bolus, dose of adrenaline, dose of 10% dextrose to correct hypoglycaemia
Can attach paediatric defibrillation paddles to adult paddles
Can size and use o/p, n/p airways and use BVM
They can find IO needle set
That they know/ can find the normal range of physiological variables
Can immediately access and know the common paediatric protocols- for cardiac arrest, seizures and anaphylaxis
They can interpret limb x-rays- specifically recognise epiphyses, joint effusions.
That they can interpret lat cspine (age <10)
That they recognise the normal paediatric ECG and how it changes

47
4 Perform a primary survey in a child
Expected behaviour
Preparation phase
Has calculated weight – prepared – defibrillation charge, ETT, fluid bolus, and dextrose (10%)
Has Broselow tape and knows how to use it
Transfer Ensures safe transfer of patient onto ED trolley
Examination Assesses airway, establishes if obstructed, corrects and ensures delivery of 100%O2. Appropriate use and correct sizing of airway adjuncts
Concurrently ensures cervical spine immoblisation (using collar, sandbags and tape)- able to select and apply correct collar
Exposes chest identified raised respiratory rate, chest asymmetry, chest wall bruising, air entry (anteriorly and laterally) and percussion (laterally). Identifies life threatening problems and correctly carries out associated procedures
Examines for signs of shock, ensures monitoring established and has gained iv accessX2
If shocked looks for potential sites of blood loss- abdomen, pelvis and limbs.
Can formulate differential for shocked patient
Knows protocol for fluid administration for the shocked child
Establishes level of consciousness and seeks lateralising signs
Uses paediatric GCS scale
Examines limbs, spine and rectum (if unconscious or spinal injury suspected) ensuring safe log roll.
BM done for those with altered level of consciousness
Will have identified and searched for potential life threatening problems in a systematic and prioritised way
Ensured child is kept warm
Reassesses if any deterioration with repeat of ABCD
Elicits full relevant history from prehospital care providers, witnesses and parents
Monitoring and interventions
Ensured appropriate monitoring
Will have placed lines, catheter and NG tubes as appropriate
Investigations Ensured appropriate blood testing (including cross match).
Plain radiology trauma series undertaken
Prescribing Ensures adequate and safe pain relief
Clinical decision making and judgement
Directs team appropriately
Liaises with and involves parents
Overall plan Notes of primary survey are clear and legible
Professionalism Behaves in a professional manner
48
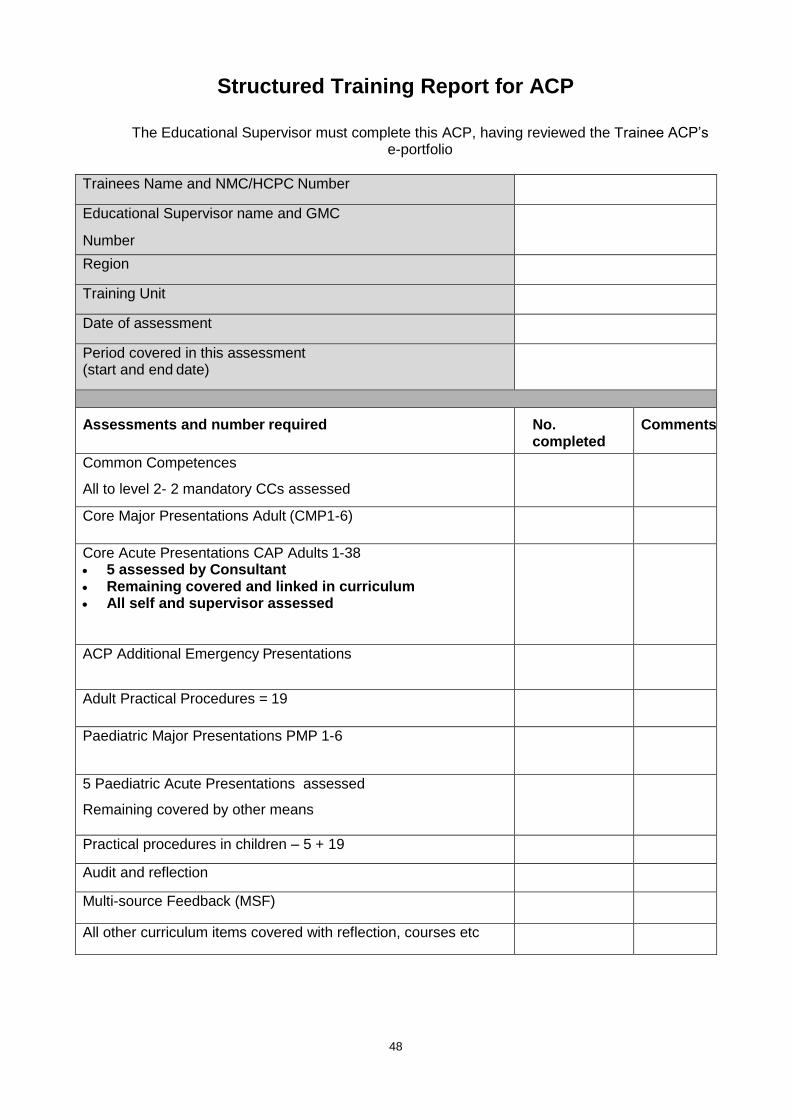
Structured Training Report for ACP
The Educational Supervisor must complete this ACP, having reviewed the Trainee ACP’s
e-portfolio
Trainees Name and NMC/HCPC Number
Educational Supervisor name and GMC
Number
Region
Training Unit
Date of assessment
Period covered in this assessment (start and end date)
Assessments and number required No. completed
Comments
Common Competences
All to level 2- 2 mandatory CCs assessed
Core Major Presentations Adult (CMP1-6)
Core Acute Presentations CAP Adults 1-38 5 assessed by Consultant Remaining covered and linked in curriculum All self and supervisor assessed
ACP Additional Emergency Presentations
Adult Practical Procedures = 19
Paediatric Major Presentations PMP 1-6
5 Paediatric Acute Presentations assessed
Remaining covered by other means
Practical procedures in children – 5 + 19
Audit and reflection
Multi-source Feedback (MSF)
All other curriculum items covered with reflection, courses etc

49
Other outcome to be considered
Activity Date Outcome Comments
Educational achievements
Evidence of reflective practice
Critical incidents
Complaints
Strengths of ACP
Development needs of ACP
Preparedness for independent practice – view of the local faculty
Names of faculty consulted:
Comments:
Supervisor’s Name and Signature Trainee ACP’s Name and Signature
Date: Date:

50
Appendix Three: Self-Declaration Form
Self-Declaration Form for Emergency Care Advanced Clinical
Practitioners
Section 1: Personal details
Forename: Surname:
Home Address:
Employer Address:
Telephone: Primary contact email address:
Current Deanery/LETB:
Section 2: Probity and Health Declaration
Convictions, finding against you and disciplinary action
In the last 12 months have you been convicted of a criminal offence? Yes No If yes, please give details:
Do you have any criminal proceedings pending against you inside or outside the UK? Yes No If yes, please give details:
Have you had any cases considered, heard and concluded against you by any of the following:
o The Nursing and Midwifery Council o The Health and Care Professions Council o Any other professional regulatory or other professional licensing body within the
UK o A professional regulatory or other professional licensing body outside the UK
Yes No If yes, please give details:

51
Health Declaration: Your own health Regulatory bodies acknowledge that nurses and paramedics who become ill deserve health and support. Advanced Clinical Practitioners (ACPs) also have to recognise that illness can impair their judgment and performance and thus put patients and colleagues at risk. The NMC and HCPC therefore encourages ACPs to reflect in their own health, seek professional advice if necessary and consider whether, for health related reasons, they should modify their professional activities in accordance with fitness to practice requirements. It is the ACP’s responsibility to report any sickness absence to their employer and they must be aware of employer policy. Sickness absence could also be recorded in the ePortfolio.
Do you have any illness or physical condition that has, in the last 12 months, resulted in your restricting or changing your professional activities?
Yes No If yes, please give details of the changes in your professional activities, which it is (or was) necessary for you to make:
Are you currently or in the last 12 months, been subject to supervision, voluntary or otherwise, and/or any restrictions voluntary or otherwise, imposed by your employer or contractor resulting from any illness or physical condition within the UK or abroad?
Yes No If yes, please give details:
Regulatory and voluntary proceedings
1) Are you, or have you been in the last 12 months, the subject of any proceedings with any of the following organisations:
a. The Nursing and Midwifery Council b. The Health and Care Professions Council c. Any other professional regulatory or other professional licensing body within the UK d. A professional regulatory or other professional licensing body outside the UK Yes No If yes, please give details:
2) In the last 12 months, have there been any disciplinary actions taken again you by your employer or your contractor (either inside the UK or outside) that have been upheld?
Yes No If yes, please give details:

52
3) In in last 12 months, has your employment contract ever been terminated or suspended (in the UK or abroad) on grounds relating to your fitness to practice (conduct, performance or health)?
Yes No If yes, please give details:
Section 3: Involvement in significant events, complaints or other investigations:
Significant Event: A significant event (also known as an untoward or critical incident) is any unintended or unexpected event, which could or did lead to harm of one or more patients. This includes incidents which did not cause harm but could have done, or where the event should have been prevented. You are required to record and reflect on Significant events with the focus on what you have learnt as a result of the event/s. Use non-identifiable patient data only.
Complaints: A complaint is a formal expression of dissatisfaction or grievance. It can be about an individual, the team or about the care of patients where you could be expected to have had influence or responsibility. As a matter of honesty & integrity you are obliged to include all complaints, even when you are the only person aware of them. You should reflect on how complaints influence your practice. Use non-identifiable patient data only.
Other investigations: In this section you should declare any on-going investigations, such as honesty, integrity, conduct, or any other matters that you feel the panel should be made aware of. Use non-identifiable patient data only.
**REMINDER: DO NOT INCLUDE ANY PATIENT-IDENTIFIABLE INFORMATION ON THIS FORM

53
Please tick/cross ONE of the following only: I do NOT have anything to declare I HAVE been involved in significant events/complaints/other investigations
If you know of any significant events/complaints/other investigations, you are required to have written a reflection on these in your ePortfolio. Please identify where in your ePortfolio the reflection(s) can be found.
Significant event: Complaint: Other investigation:
Date of entry in ePortfolio ____________ Title/Topic of Reflection/Event _________________________________
Location of entry in ePortfolio __________________________________________________________________
** Significant event: Complaint: Other investigation:
Date of entry in ePortfolio ____________ Title/Topic of Reflection/Event _________________________________
Location of entry in ePortfolio __________________________________________________________________
** Significant event: Complaint: Other investigation:
Date of entry in ePortfolio ____________ Title/Topic of Reflection/Event _________________________________
Location of entry in ePortfolio __________________________________________________________________
Section 4: Declaration
I confirm this form is a true and accurate declaration at this point in time and will immediately notify the panel and my employer if I am aware of any changes to the information provided in this form. I give permission for my past and present portfolios and / or appraisal documentation to be viewed by the panel and any appropriate person nominated.
Trainee’s Signature :
Date:
Chair of the Panel’s
Signature:
Date:

54
Appendix Four: Credentialing Outcome Form
Emergency Care Advanced Clinical Practitioner Credentialing Outcome Form
Forename: Surname: Regulatory Body and
Membership Number:
Primary Qualification (Institution and year awarded):
Master’s Degree (Institution and year awarded):
Date of Credentialing Assessment:
List all panel
members
1. 2.
3. 4.
5. 6.
Location of training/working From: (insert
dates)
To: (insert
dates)
Evidence considered by the panel and known to the trainee
1. ePortfolio 2. Structured Training Report
3. Checklist of evidence 4.
5. 6.
Panel Outcome
Successful - Credential
Achievement of all curriculum requirements
Further evidence required
Further evidence is required, see additional feedback form.

55
If further evidence is required:
Recommended time required to achieve outstanding objectives (whole time equivalent) following
discussion:
________________________________________________________________________________
Chair of Panel’s
signature: Date:
Trainee ACP’s
signature: Date
By signing this form the Chair of the panel is confirming that fitness to any practice issues have been considered. This
document should be scanned and saved in the trainee ACP’s ePortfolio. This information will also be recorded at the
Royal College of Emergency Medicine. By signing the form, the ACP is indicating that they understand and agree that
the information will be shared with other parties involved in their training as outlined above. The ACP signature on the
form indicates that they understand the recommendations arising from the credentialing assessment. It does not imply
they accept or agree with the outcome.

56
Appendix Five: Credentialing Feedback Form
Emergency Care Advanced Clinical Practitioner Credentialing Feedback Form
Forename: Surname: Regulatory Body:
Date of Credentialing Assessment:
List panel
members 1. 2.
Feedback from Credentialing Panel – Evidence Presented
ePortfolio
Structured Training Report
Checklist of evidence

57
Chair of Panel’s signature:
Date:
Trainee ACP’s signature:
Date
Feedback from Credentialing Panel – Post-Assessment
Overall Quality of Evidence
Comments on areas of ACP Progression/Developments In Role
Feedback on the Pilot
Recommended Actions (for those in who require further evidence):
Related Documents











