Journal o/'the Neurological Sciences, 1983, 59:371 382 371 Elsevier A FAMILY WITH ADULT SPINAL AND BULBAR MUSCULAR ATROPHY, X-LINKED INHERITANCE AND ASSOCIATED TESTICULAR FAILURE TXOMIN ARBIZU 1, JOAN SANTAMAR]A l, JOSE MANUEL GOMEZ 2, ANGEL QUiLEZ l and JAUME PERES SERRA 1 Sections o/' 1Neurology and 2Endocrinology, Ciudad Sanitaria "Principes de E,wa~a ", Hospitalet, Barcelona (Spain) (Received 11 October, 1982) (Accepted 15 December, 1982) SUMMARY A family with adult spinal and bulbar muscular atrophy with X-linked recessive inheritance (Kennedy's disease) is described. Affected members presented at age 20 with muscle cramps followed insidiously by gynaecomastia, partial loss of secondary sexual traits, loss of libido and inability to maintain an erection. Three had also testicular atrophy and severe oligospermia was found in two patients. Testicular biopsy in one case showed germinal failure with almost normal Leydig cells. Hormonal tests were suggestive of a primary testicular failure. Etiologic possibilities are considered. Key words: Spinal muscular atrophy - Kennedy's disease Testicular.failure INTRODUCTION The spinal muscular atrophies are a clinically variable group of inherited disorders involving the spinal motor neurons and those of the lower cranial nerves with sparing of the corticospinal and sensory tracts. The main features used to classify these disorders are age of onset, duration of the illness, distribution of the weakness and mode of inheritance (Emery 1971 ; Marsden 1975). There is a wide degree of variation that ranges from the severe acute infantile form of Werdnig- Hoffmann to the benign chronic adult type of Smith and Patel (Smith et al. 1965). Autosomal recessive inheritance is the most usual mode of transmission (Emery Correspondence should be addressed to : Jaume Peres Serra, M.D., Secci6n de Neurologia. Ciudad Sanitaria "Principes de Espafia" Hospitalet, Barcelona, Spain. 0022-510X/83/$03.00 © 1983 Elsevier Science Publishers B.V.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal o/'the Neurological Sciences, 1983, 59:371 382 371 Elsevier
A F AMILY WITH A D U L T SPINAL A N D BULBAR M U S C U L A R ATROPHY, X-LI NKED I N H E R I T A N C E AND ASSOCIATED TESTICULAR F A ILU RE
TXOMIN ARBIZU 1, JOAN SANTAMAR]A l, JOSE M A N U E L GOMEZ 2, ANGEL QUiLEZ l and J A U M E PERES SERRA 1
Sections o/' 1Neurology and 2Endocrinology, Ciudad Sanitaria "Principes de E,wa~a ", Hospitalet, Barcelona (Spain)
(Received 11 October, 1982) (Accepted 15 December, 1982)
S U M M A R Y
A family with adult spinal and bulbar muscular atrophy with X-linked recessive inheritance (Kennedy's disease) is described. Affected members presented at age 20 with muscle cramps followed insidiously by gynaecomastia, partial loss of secondary sexual traits, loss of libido and inability to maintain an erection. Three had also testicular atrophy and severe oligospermia was found in two patients. Testicular biopsy in one case showed germinal failure with almost normal Leydig cells. Hormonal tests were suggestive of a primary testicular failure. Etiologic possibilities are considered.
Key words: Spinal muscular atrophy - Kennedy's disease Testicular.failure
INTRODUCTION
The spinal muscular atrophies are a clinically variable group of inherited disorders involving the spinal motor neurons and those of the lower cranial nerves with sparing of the corticospinal and sensory tracts. The main features used to classify these disorders are age of onset, duration of the illness, distribution of the weakness and mode of inheritance (Emery 1971 ; Marsden 1975). There is a wide degree of variation that ranges from the severe acute infantile form of Werdnig- Hoffmann to the benign chronic adult type of Smith and Patel (Smith et al. 1965). Autosomal recessive inheritance is the most usual mode of transmission (Emery
Correspondence should be addressed to : Jaume Peres Serra, M.D., Secci6n de Neurologia. Ciudad Sanitaria "Principes de Espafia" Hospitalet, Barcelona, Spain.
0022-510X/83/$03.00 © 1983 Elsevier Science Publishers B.V.
372
et al. 1976b). Wi th in the adul t form several pedigrees have been publ ished suggesting
an X-l inked recessive inher i tance (Kennedy et al. 1968; Tsukagoshi et al. 1970;
Stefanis et al. 1975; Ringel et al. 1978; Schoenen et al. 1979; Barkhaus et al. 1982),
in some with associated endocr ine dis turbances such as diabetes (Kennedy et al.
1968; Schoenen et al. 1979; Barkhaus et al. 1982), sterility (Stefanis et al. 1975;
Schoenen et al. 1979) and gynaecomast ia (Kennedy et al. 1968; Tsukagoshi et al.
1970; Stefanis et al. 1975 ; Ringel et al. 1978 ; Schoenen et al. 1979). Detai led studies
of the last two abnormal i t ies have not been done except in one previous case
(Schoenen et al. 1979). We describe a Spanish family in which several male members
through four generat ions were affected by chronic spinal and bu lbar muscular
a t rophy suggesting an X-l inked recessive inheri tance. Late hypogonad i sm and
gynaecomast ia were found in 6 members . Endocr inological studies poin ted to a
pr imary testicular dysfunct ion.
CASE REPORTS
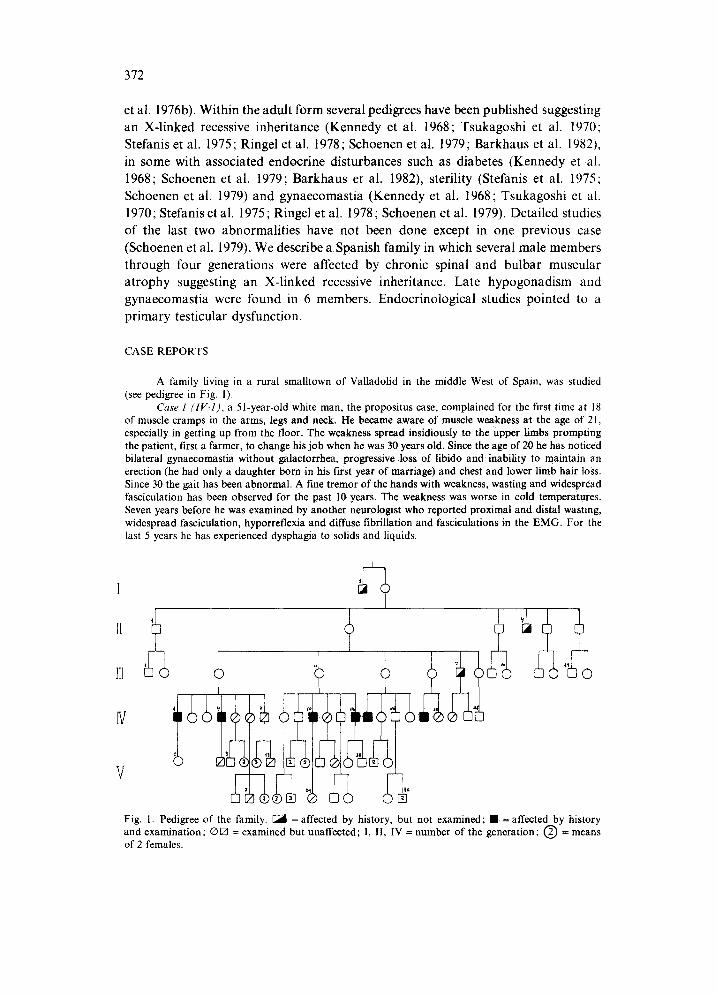
A family living in a rural smalltown of Valladolid in the middle West of Spain, was studied (see pedigree in Fig. 1).
Case 1 ( IV- l ) , a 51-year-old white man, the propositus case, complained for the first time at 18 of muscle cramps in the arms, legs and neck. He became aware of muscle weakness at the age of 21, especially in getting up from the floor. The weakness spread insidiously to the Upper limbs prompting the patient, first a farmer, to change his job when he was 30 years old. Since the age of 20 he has noticed bilateral gynaecomastia without galactorrhea, progressive loss of libido and inability to maintain an erection (he had only a daughter born in his first year of marriage) and chest and lower limb hair loss. Since 30 the gait has been abnormal. A fine tremor of the hands with weakness, wasting and widespread fasciculation has been observed for the past 10 years. The weakness was worse in cold temperatures. Seven years before he was examined by another neurologist who reported proximal and distal wasting, widespread fasciculation, hyporreflexia and diffuse fibrillation and fasciculations in the EMG. For the last 5 years he has experienced dysphagia to solids and liquids.
I +
V
Fig. 1. Pedigree of the family. ~ = affected by history, but not examined; • = affected by history and examination; ® [] = examined but unaffected; I, II, IV = number of the generation; (~) = means of 2 females.
373
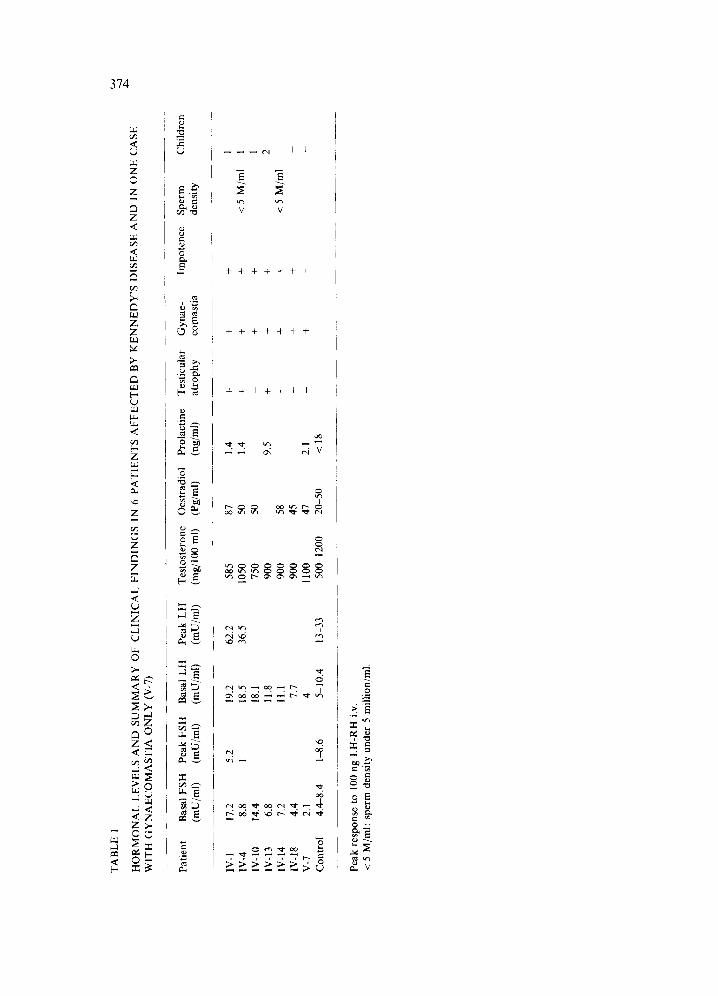
He appeared well; the skin was normal with complete absence of hair in axillae, t runk and limbs. The testes were small (2.5 cm in longitudinal diameter). Blood pressure was normal. There was slight facial diplegia, marked wasting and fasciculation of the tongue and weakness of head turning. Wasting, weakness and fasciculation were also observed in trapezius, shoulder girdle, arm, forearm and hand muscles bilaterally in a decreasing degree of involvement, more marked on the left. Deep tendinous reflexes (DTR) were present but diminished. The lower limbs were also weak with a pre- dominant proximal distribution, the wasting and fasciculation being mainly located on anterior-external and posterior muscle groups of both legs. The plantar reflexes were flexor. The rest of the neurologic examination was normal. Films of the chest, skull and cervical spine and hematologic profile were normal. Technicon Smac-20 only revealed a slight elevation in CK levels. Cerebrospinal fluid (CSF) gave normal glucose and protein values with no cells. The EMG showed fibrillation, positive waves, fasciculations, high-frequency discharges and giant motor neuron potentials (5-15 mV) in proximal and distal muscles, especially the former. Motor and sensory conduction velocities on the sural, peroneal, median and radial nerves were in the normal limits. Sural nerve biopsy was normal. A gastrocnemius muscle biopsy showed an important degree of muscular atrophy with isolated atrophic fibers and small and large group atrophy. The atrophic fibers had an increased oxidative activity and type fiber grouping was present. Type fiber predominance or target fibers were not seen. Hormonal tests including T 4, T~, TSH, cortisol rhythm and 17-ketosteroids were normal. The rest of the endocrinological studies are detailed in Table 1. Cariotype was normal 46, XY.
Case 2 (IV-4), a 47-year-old farmer man, brother of case 1, first noticed muscle cramps at age 18. At 30 he became aware of weakness on climbing stairs that slowly spread to the upper limbs. He also observed bilateral painful gynaecomastia. Since age 35 he has had hand tremor. For 7 years he has suffered a decrease in libido, with difficulty in maintaining an erection (he had only a son), and experienced occasional dysphagia, with severe bouts of cough when drinking. Cold temperature worsened his symptoms. On examination weakness and wasting were prominent in shoulders, arms, forearms and hands, as well as in the hips, thighs and legs with an asymmetric distribution. Fasciculations were present in the tongue, face and proximal upper and lower limbs. D T R were diminished. CK and aldolase levels were slightly elevated. Pubic hair was feminoid and hair loss was evident in t runk and limbs. Testes were small (2.5 cm in the longitudinal diameter). EMG and nerve conduction velocities as well as muscle biopsy were similar to case 1. Functional respiratory tests disclosed a residual volume increase (132% of the expected volume). Hormonal studies including T 3, T4, TSH, prolactin, cortisol rhy thm and 17-ketosteroids were normal. The rest of the endocrine data is detailed in Table 1. A seminogram showed a greatly diminished count of spermatozoids (3.995.000/ml in 0.50 ml of ejaculate), 85% of them being immobile. Testicular biopsy was done showing a microcystic albuginea and a pallid parenchyma. Morphologic studies (Fig. 2) disclosed normal-sized tubules with spermatogenesis inter- ruption at the spermatide level, spermatozoids being very sparse. Occasional clustering of the Leydig cells, otherwise normal, was seen.
Four other men were also affected and the clinical history, neurological examination and EMG studies were similar to cases IV-1 and IV-4. Some findings are emphasized below.
Case IV-IO, a 45-year-old farmer man presented muscle cramps first at 16 and bilateral gynaecomastia has been observed since 18 years old. Since the age of 30 he has noticed libido decrease.
Case IV-13, a 37-year-old clerk, the brother of case IV-10, has been living in a distant city from the other affected members since he was a child. He first complained of muscle cramps at 25 and, since 30 he has slowly presented decrease in the libido, inability to maintain an erection, t runk and limb hair loss and gynaecomastia.
Case IV-14, a 45-year-old farmer has noticed muscle cramps and bilateral gynaecomastia with trunk and limb hair loss since 18. He was studied in another hospital some years before, because he had had no children. The only information available to us is that he had severe hypospermia.
Case IV-18, a 34-year-old farmer man, began to notice muscle cramps at 22. Since then he has presented gynaecomastia and a feminoid hair distribution, libido decrease and difficult erections. He was used to drinking alcohol moderately. Distal hypaesthesia with a sock-and-glove distribution was found. He refused EMG examination. Endocrinological studies of these cases are summarized in Table 1.
Cases IV-5, IV-6, 1V-7, 1V-II, IV-15, IV-lg, 11/-20, V-2, V-7, V-IO, V-24, and V-26 were also examined and blood collected for analytical studies (Technichon Samc-20, estradiol, testosterone and gonadotrophins) . No abnormalit ies were found. No one unaffected male had sexual complaints. In patient IV-6, an obligate carrier, E M G disclosed no abnormalities. Her son (V-7), a 16-year-old boy, also showed no EMG abnormalities. He had gynaecomastia but endocrinological studies were normal
TA
BL
E
1 w
p”
HO
RM
ON
AL
L
EV
EL
S A
ND
SU
MM
AR
Y
OF
CL
INIC
AL
FI
ND
ING
S IN
6
PAT
IEN
TS
AFF
EC
TE
D
BY
K
EN
NE
DY
’S
DIS
EA
SE
AN
D
IN
ON
E
CA
SE
WIT
H
GY
NA
EC
OM
AST
IA
ON
LY
(V
-7)
Patie
nt
Bas
al
FSH
Pe
ak
FSH
B
asal
L
H
Peak
L
H
Tes
tost
eron
e O
estr
adio
l
(mu/
ml)
(m
u/m
l)
(mu/
ml)
(m
U/m
l)
(mg/
l00
ml)
(P
g/m
l)
___~
._
- ~.
.__
___
~_
.___
- ~
...~
IV-
1 17
.2
5.2
19.2
62
.2
585
87
IV-4
8.
8 1
18.5
36
.5
1050
50
IV
-IO
14
.4
18.1
75
0 50
IV
-13
6.8
11.8
90
0 IV
-14
7.2
11.1
90
0 58
IV
-18
4.4
7.7
900
45
v-7
2.1
4 11
00
47
Con
trol
4.
4-8.
4 l-
8.6
5-10
.4
13-3
3 50
@ 1
200
20-5
0
.--.
~
_. ~
. ___
_~
~__
~
_~~
.
Peak
re
spon
se
to
100
ng
LH
-RH
i.v
. <
5 M
/ml:
sper
m
dens
ity
unde
r 5
mill
ion/
ml.
Prol
actin
e T
estic
ular
@g/
ml)
at
roph
y
1.4
+
1.4
+ _
9.5
+ _ -
2.1
-
< 18
_~~
Gyn
ae-
com
astia
Impo
tenc
e Sp
erm
de
nsity
C
hild
ren
+
1
+ <5
M
/ml
1
+ I
f 2
+ ~5
M
/ml
-
+ _
_ _
375
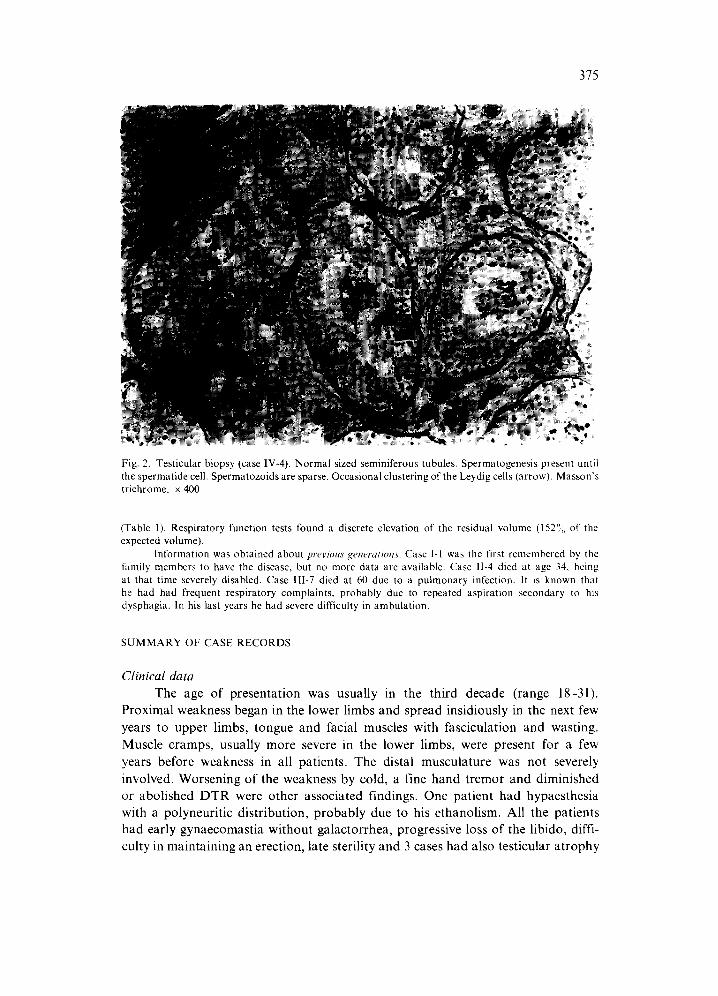
Fig. 2. Testicular biopsy (case IV-4). Normal sized seminiferous tubules. Spermatogenesis present until the spermatide cell. Spermatozoids are sparse. Occasional clustering of the Leydig cells (arrow). Masson ' s trichrome, x 400.
(Table 1). Respiratory function tests found a discrete elevation of the residual volume (152°; of the expected volume).
Information was obtained about previous generations. Case 1-1 was the first remembered by the family members to have the disease, but no more data are available. Case 1I-4 died at age 34, being at that time severely disabled. Case 1II-7 died at 60 due to a pulmonary infection, it is known that he had had frequent respiratory complaints, probably due to repeated aspiration secondary to his dysphagia. In his last years he had severe difficulty in ambulation.
S U M M A R Y OF CASE R E C OR DS
Clinical data The age of presentation was usually in the third decade (range 18-31).
Proximal weakness began in the lower limbs and spread insidiously in the next few years to upper limbs, tongue and facial muscles with fasciculation and wasting. Muscle cramps, usually more severe in the lower limbs, were present for a few years before weakness in all patients. The distal musculature was not severely involved. Worsening of the weakness by cold, a fine hand tremor and diminished or abolished DTR were other associated findings. One patient had hypaesthesia with a polyneuritic distribution, probably due to his ethanolism. All the patients had early gynaecomastia without galactorrhea, progressive loss of the libido, diffi- culty in maintaining an erection, late sterility and 3 cases had also testicular atrophy
376
(Table 1). No sphincteric disturbances were found. No one relative male had gynaecomastia, except case V-7, or sexual complaints. The course of the disease was slowly progressive, usually more than 30 years, and not severely disabling.
Laboratory data Only a slight elevation of the CK and aldolase levels was found. The glucose
and triglycerides were normal. Endocrine studies showed (Table 1): (a) Elevated basal LH and FSH (high FSH in 2 patients and high LH in 5).
LH response to the stimulation by LH-RH was exaggerated in the 2 cases in which it was done.
(b) Normal testosterone values in all cases. (c) Estradiol elevation in 2 cases. (d) Severe oligospermia in 2 patients. (e) Testicular biopsy with spermatogenesis arrest at the spermatide level and
normal, occasionally clustered, Leydig cells (Fig. 2). (f) Normal values ofFSH, LH testosterone and estradiol in unaffected males. EMG in 3 cases showed a pattern compatible with a motor neuron lesion in
all muscles tested. Nerve conduction was normal in the cases examined. In 2 un- affected members (IV-6 and V-7) there were no EMG abnormalities. Nerve and muscle biopsy was done in 2 cases. The muscle biopsy suggested chronic denervation with collateral reinervation. Nerve biopsy was normal. In 2 cases examined, the respiratory function tests showed elevation in the residual volume.
Inheritance The disease through four generations affected only males in a nondominant
form, making females the probable carriers. These facts favor an X-linked recessive mode of inheritance.
DISCUSSION
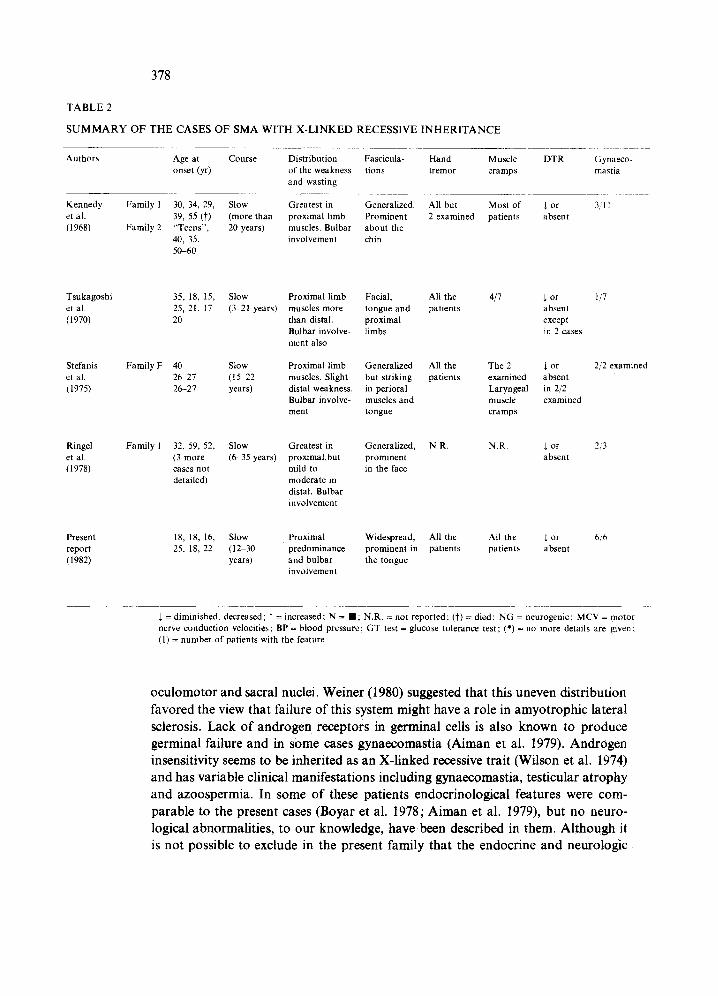
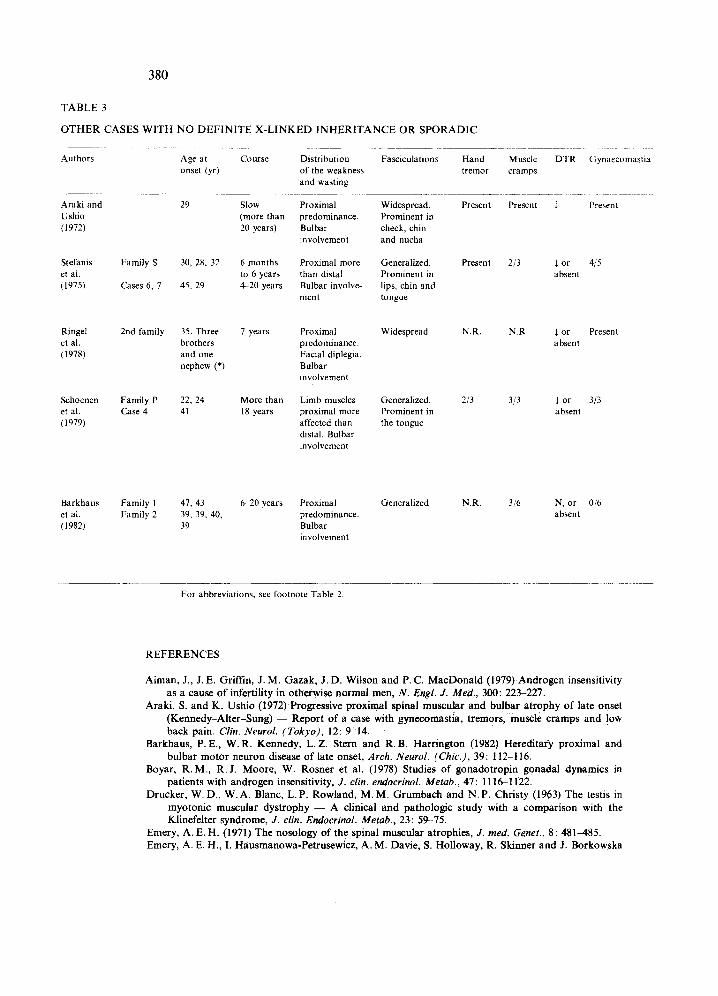
An X-linked recessive mode of inheritance among the group of chronic spinal muscular atrophies was first suggested in 1957 by Kurland in a brief reference to a Japanese family. Kennedy et al. in 1968 and Tsukagoshi et al. in 1970 published several families with affected males belonging to two or three generations and having many clinical similarities, including bulbar involvement and gynaecomastia that are less frequently reported in autosomal forms (Emery et al. 1976a; Pearn et al. 1978). The concept has later arisen that kindreds with no definite X-linked recessive transmission and isolated cases, belong to the same entity (Kennedy's disease) (Araki et al. 1972; Stefanis et al. 1975; Schoenen et al. 1979). Whether or not it is a separate disease is not clear at present (see for comparison Tables 2 and 3).
The clinical picture in our patients is compatible with the previous reports of this disorder. Bulbar and proximal limb weakness, wasting and fasciculation, of late onset and slow course, preceded by muscle cramps, and gynaecomastia are

377
almost constant. Disturbances in erection were previously reported only by Ringel et al. (1978). Late hypogonadism with loss of some secondary sexual traits, testicular atrophy and oligospermia are first noticed, to our knowledge, in the present cases. Other findings such as diabetes (Kennedy et al. 1968; Schoenen et al. 1979; Barkhaus et al. 1982), hyperlipidaemia (Ringel et al. 1978: Schoenen et al. 1979), cardiac conduction abnormalities (Ringel et al. 1978), low back pain (Kennedy et al. 1968; Araki et al. 1972) and worsening of the weakness by cold (Tsukagoshi et al. 1970) are less frequently reported.
The nature of the gynaecomastia has only been investigated by two authors. Araki et al. (1972), reported that urinary gonadotrophins, testosterone and estradiol levels were normal. A detailed study by Schoenen et al. (1979) in another patient, found low testosterone levels with a positive response to stimulation by human chorionic gonadotrophin (HCG), high estradiol levels and normal serum gonado- trophins. They suggested hypothalamic hypophyseal dysfunction as the cause of the gynaecomastia, although the high estradiol levels could not be explained in this way. The endocrine studies performed in the present family showed severe oligospermia and FSH elevation, suggesting serious failure, probably irreversible, of the germinal cells, and LH increase with exaggerated response to the LH RH test. Elevated LH, with or without low testosterone, could be the result of a com- pensated failure of the Leydig cells caused by the same aetiologic t:actors damaging the seminal tubules. The above data and the normal prolactin, T,, T4, and cortisol makes hypothalamic hypophyseal dysfunction improbable in our cases. Primary testicular failure seems to be the most logical explanation for the hypogonadism. Gynaecomastia might then be due to an increase in the peripheral conversion of testosterone to estrogens induced by the elevated gonadotrophins.
Several explanations could be offered in order to explain the association of spinal muscular atrophy and testicular failure. Defective control of the testicular vessels and the cremasteric reflex, due to the spinal disease process, can produce an increase in the intrascrotal temperature and be responsible for the generalized hypoplasia of the germinal epithelium, testicular atrophy and the less severe involvement of the Leydig cells. In some paraplegic patients similar features have been described and gynaecomastia observed (Hayes et al. 1979). This nonspecific mechanism, however, would not explain why it has not been reported in the autosomal recessive forms of spinal muscular atrophy (Namba et al. 1970; Emery et al. 1976a; Pearn et al. 1978) or in the chronic forms of amyotrophic lateral sclerosis (Norris et al. 1975).
A genetically determined disorder of the gonadal cells, similar to that involving spinal and bulbar motor neurons, might also cause the testicular failure. In myotonic dystrophy, germinal failure, gynaecomastia and testicular atrophy with histological and endocrine features similar to the present cases has been reported (Drucker et al. 1963: Sagel et al. 1975).
An hereditary androgen receptor failure involving mainly the spinal and bulbar motor neurons and germinal cells merits some consideration. Androgen receptors have been found in spinal and bulbar motor neurons but were absent in
378
T A B L E 2
S U M M A R Y O F T H E C A S E S O F S M A W I T H X - L I N K E D R E C E S S I V E I N H E R I T A N C E
Authors Age at Course Distribution Fascicula- Hand Muscle DTR Gynaeco- onset (yr) of the weakness tions tremor cramps mastia
and wasting
Kennedy Family 1 30, 34, 29, Slow Greatest in Generalized. All but Most of $ or 3/I 1 et al. 39, 55 (t) (more than proximal limb Prominent 2 examined patients absent (1968) Family 2 "Teens". 20 years) muscles. Bulbar about the
40, 35, involvement chin 50-60
Tsukagoshi 35, 18, 15, Slow Proximal limb Facial, All the 4/7 $ or et al. 25, 21, 17 (3-21 years) muscles more tongue and patients absent (1970) 20 than distal, proximal except
Bulbar involve- limbs in 2 cases ment also
Stefanis Family F 40 Slow Proximal limb Generalized All the The 2 ~ or et al. 26-27 (15 22 muscles. Slight but striking patients examined absent (1975) 26-27 years) distal weakness, in perioral Laryngeal in 2/2
Bulbar involve- muscles and muscle examined ment tongue cramps
Ringel Family 1 32, 59, 52, Slow Greatest in Generalized, N.R. N.R. ~t or et al. (3 more (6-35 years) proximal,but prominent absent (1978) cases not mild to in the face
detailed) moderate in distal. Bulbar involvement
Present 18, 18, 16, Slow Proximal Widespread, All the All the ~ or report 25, 18, 22 (12-30 predominance prominent in patients patients absent (1982) years) and bulbar the tongue
involvement
1 / 7
2/2 examined
2,,'3
6/6
$ = diminished, decreased ; T = increased ; N = • ; N.R. = not reported; (t) = died; NG = neurogenic; MCV = motor nerve conduction velocities; BP = blood pressure; GT test = glucose tolerance test; (*)= no more details are given; (1) = number of patients with the feature.
oculomotor and sacral nuclei. Weiner (1980) suggested that this uneven distribution favored the view that failure of this system might have a role in amyotrophic lateral sclerosis. Lack of androgen receptors in germinal ceils is also known to produce germinal failure and in some cases gynaecomastia (Aiman et al. 1979). Androgen insensitivity seems to be inherited as an X-linked recessive trait (Wilson et al. 1974) and has variable clinical manifestations including gynaecomastia, testicular atrophy and azoospermia. In some of these patients endocrinological features were com- parable to the present cases (Boyar et al. 1978; Aiman et al. 1979), but no neuro- logical abnormalities, to our knowledge, have been described in them. Although it is not possible to exclude in the present family that the endocrine and neurologic
379
Impotence
N.R.
N.R.
3/3
6/6
Muscle CSF enzymes protein
N.R. T 6 t imes In 3ca se s : (CPK) 35, 80 1 case and 100
mg/100 ml
E M G Conduct ion nerve studies
N except in 3 cases: 2 with block in median nerve at wrist; 1 with I MCV (diabetic)
N G
Sterility Endocrine studies
N.R. in fumily N.R. B in some cases. Only 1 case had no children. Family G normal
4 t imes N N G N N.R. 3 had N.R. (1). only 1 child. N in II1-V had 2. 2 cases Two had no
children
" 3 6 N R N G N: M C V N.R. but no N.R. t imes in Absent ulnar one affected 2 cases sensory termi- member had
hal potential children and H-reflex in 1 case
T 2 t imes N N G N 3 had no Thyroid in children. The function 2 cases 3 examined N N in had 6, 5 and 2 1 case children
Muscle Other Unaffected biopsy findings member
features
G r o u p a t rophy Adrenalec tomy Diabetes in sarcolemmal due to } BP. 13 cases.
nuclei. Rare Low back pain T r e m o r in degenerat ing in some cases, some. Muscle fibers Diabetes in c ramps in
3 cases several cases
Group a t rophy 3 cases had Two females BP had cramps.
Weakness of the orbicularis oculi in some
Group a t rophy 3 females internal nuclei, and 2 males N
Necrotic fibers undergoing fagocytosis
Variat ion in Very occcasional 3 females N fiber size. urinary and (obligate Type grouping, fecal inconti- carriers) Small angular nence. E C G fibers conduction
blocks in 2 cases
N to T N N G N One had 2 Pr imary Group atrophy. Worsening by One unaf- 4 t imes children, hypo- Type grouping cold fected male N Three: 1 child, gonad i sm had ]" residual (1 case) One had no volume
child. One single
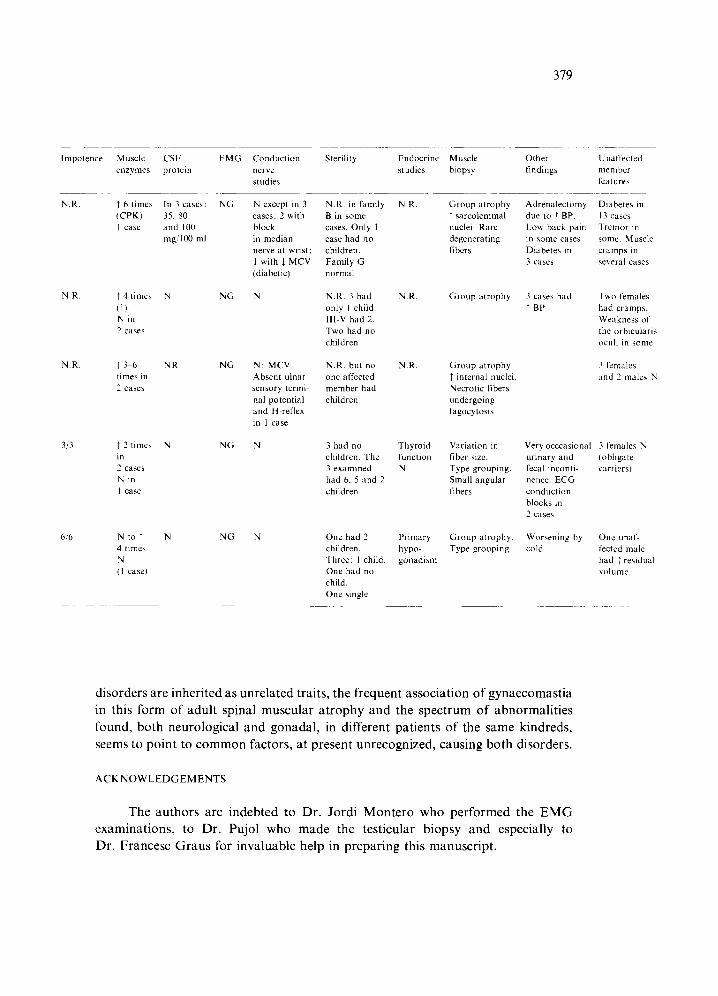
disorders are inherited as unrelated traits, the frequent association of gynaecomastia in this form of adult spinal muscular atrophy and the spectrum of abnormalities found, both neurological and gonadal, in different patients of the same kindreds, seems to point to common factors, at present unrecognized, causing both disorders.
A C K N O W L E D G E M E N T S
The authors are indebted to Dr. Jordi Montero who performed the EMG examinations, to Dr. Pujol who made the testicular biopsy and especially to Dr. Francesc Graus for invaluable help in preparing this manuscript.
380
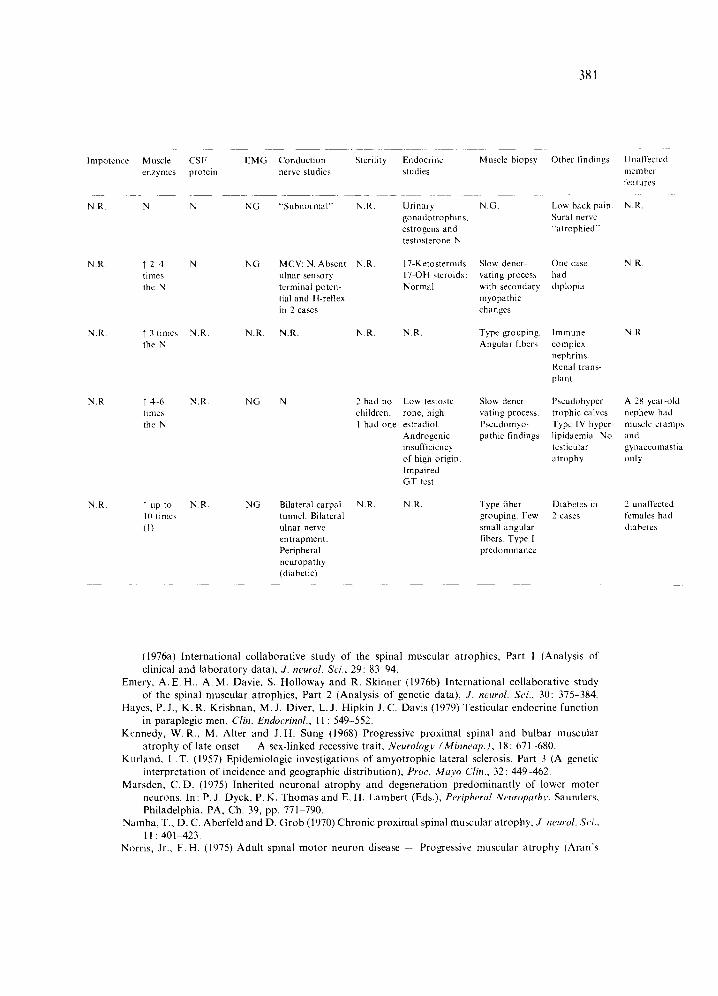
TABLE 3
OTHER CASES WITH NO DEFINITE X-LINKED INHERITANCE OR SPORADIC
Authors Age at Course Distribution Fasciculations Hand M u s c l e DTR Gynaecomastia onset (yr) of the weakness tremor cramps
and wasting
Araki and 29 Slow Proximal Widespread. Ushio (more than predominance. Prominent in (1972) 20 years) Bulbar cheek, chin
involvement and nucha
Present Present ~ Present
Stefanis Family S 30, 28, 32 6 months Proximal more Generalized. Present 2/3 ~ or 4,,5 et al. to 6 years than distal Prominent in absent (1975) Cases 6, 7 45, 29 4-20 years Bulbar involve- lips, chin and
ment tongue
Ringel 2nd family 35. Three 7 years Proximal Widespread NR. N.R. J. or et al. brothers predominance, absent (1978) and one Facial diplegia.
nephew (*) Bulbar involvement
Schoenen Family P 22, 24 More than Limb muscles Generalized. 2/3 3/3 J, or 3/3 et al. Case 4 41 18 years proximal more Prominent in absent (1979) affected than the tongue
distal. Bulbar involvement
Present
Barkhaus Family 1 47, 43 6--20 years Proximal Generalized N.R. 3/6 N, or 0/6 et al. Family 2 39, 39. 40, predominance, absent (1982) 39 Bulbar
involvement
For abbreviations, see footnote Table 2.
REFERENCES
Aiman, J., J.E. Griffin, J. M. Gazak, J .D. Wilson and P.C. MacDonald (1979) Androgen insensitivity as a cause of infertility in otherwise normal men, N. Engl. J. Med., 300: 223-227.
Araki, S. and K. Ushio (1972) Progressive proximal spinal muscular and bulbar atrophy of late onset (Kennedy-Alter-Sung) - - Report of a case with gynecomastia, tremors, muscle cramps and low back pain. Clin. Neurol. (Tokyo), 12: 9~14.
Barkhaus, P.E., W.R. Kennedy, L.Z. Stern and R.B. Harrington (1982) Hereditary proximal and bulbar motor neuron disease of late onset, Arch. Neurol. (Chic.), 39: 112-116.
Boyar, R.M., R.J. Moore, W. Rosner et al. (1978) Studies of gonadotropin-gonadal dynamics in patients with androgen insensitivity, J. clin. endocrinol. Metab., 47:1116-1122.
Drucker, W. D., W.A. Blanc, L.P. Rowland, M.M. Grumbach and N.P. Christy (1963) The testis in myotonic muscular dystrophy - - A clinical and pathologic study with a comparison with the Klinefelter syndrome, J. clin. Endocrinol. Metab., 23: 59-75.
Emery, A. E. H. (1971) The nosology of the spinal muscular atrophies, J. reed. Genet., 8: 481-485. Emery, A. E. H., I. Hausman0wa-Petrusewicz, A. M. Davie, S. Holloway, R. Skinner and J. Borkowska
381
Impotence Muscle CSF EMG Conduction Sterility Endocrine Muscle biopsy Other findings Unaffected enzymes protein nerve studies studies member
features
N.R. N N NG "Subnormal" N.R. N.G. Low back pain. N.R. Sural nerve "atrophied"
Urinary gonadotrophins, estrogens and testosterone N
NR. "f 2 4 N NG MCV: N. Absent N.R. 17-Ketosteroids Slow dener- One case N.R. times ulnar sensory 17-OH steroids: vating process had the N terminal poten- Normal with secondary diplopia
tial and H-reflex myopathic in 2 cases changes
N.R. ~" 3 times N.R. N.R. N.R. N.R. N.R. the N
N.R. T 4 6 N.R. NG N times the N
N.R.
2 had no Low testoste- children, rone, high I had one estradiol.
Androgenic insufficiency of high origin, Impaired GT test
Type grouping. Immune N.R. Angular fibers complex
nephritis. Renal trans- plant
Slow dener- Pseudohyper- A 28-year-old vating process, trophic calves, nephew had Pseudomyo- Type IV hyper- muscle cramps pathic findings lipidaemia. No and
testicular gynaecomastia atrophy only
" up to N.R. NG Bilateral carpal NR. N.R. Type fiber Diabetes in 2 unaffected 10 times tunnel. Bilateral grouping. Few 2 cases females had (I) ulnar nerve small angular diabetes
entrapment, fibers. Type 1 Peripheral predominance neuropathy (diabetic)
(1976a) International collaborative study of the spinal muscular atrophies, Part l (Analysis of clinical and laboratory data), J. neurol. Sci., 29:83 94.
Emery, A. E. H., A.M. Davie, S. Holloway and R. Skinner (1976b) International collaborative study of the spinal muscular atrophies, Part 2 (Analysis of genetic data), J. neurol. Sci., 30: 375-384.
Hayes, P.J., K.R. Krishnan, M.J. Diver, L.J. Hipkin J. C. Davis (1979)Testicular endocrine function in paraplegic men, Clin. Endocrinol., ll : 549-552.
Kennedy, W.R., M. Alter and J .H. Sung (1968) Progressive proximal spinal and bulbar muscular atrophy of late onset - - A sex-linked recessive trait, Neurology (Minneap.), 18: 671-680.
Kurland, L.T. (1957) Epidemiologic investigations of amyotrophic lateral sclerosis, Part 3 (A genetic interpretation of incidence and geographic distribution), Proc. Mayo Clin., 32 : 449-462.
Marsden, C.D. (1975) Inherited neuronal atrophy and degeneration predominantly of lower motor neurons. In: P. J. Dyck, P. K. Thomas and E, H. Lambert (Eds.), Peripheral Neuropathy, Saunders, Philadelphia, PA, Ch. 39, pp. 771-790.
N amba, T., D. C. Aberfeld and D. Grob (1970) Chronic proximal spinal muscular atrophy, J. neurol. Set., 11:401 423.
Norris, Jr., F.H. (1975) Adult spinal motor neuron disease 4. Progressive muscular atrophy (Aran's
382
disease) in relation to amyotrophic lateral sclerosis. In: P.J. Vinken and G.W. Bruyn (Eds.), Handbook of Clinical Neurology, Vol. 22 (System Disorders and Atrophies), North-Holland Pub- lishing Co., Amsterdam, Ch. 1, pp. 1-56.
Pearn, J.H., P. Hudgson and J.H. Walton (1978) A clinical and genetic study of spinal muscular atrophy of adult onset - - The autosomal recessive form as a discrete entity, Brain, 101: 591-606.
Ringel, S. P., N. S. Lava, M. M. Treihaft, M. L. Lubs and H. A. Lubs (1978) Late onset X-linked recessive spinal and bulbar muscular atrophy, Muscle & Nerve, 1 : 297-307.
Sagel, J., L.A. Distiller, J.E. Morley, H. Isaacs, G. Kay and Van der Walt (1975) Myotonia distrophica - - Studies on gonadal function using luteinizing hormone-releasing hormone (LRH), J. clin. Endocrinol. Metab., 40: 1110-1113.
Schoenen, J., P.J. Delwaide, J.J. Legros and P. Franchimont (1979) Motoneuropathie h6r6ditaire La forme proximal de l'adulte li66 au sexe (ou maladie de Kennedy), J. neurol. Sci., 49: 343- 357.
Smith, J.B. and A. Patel (1965) The Wohlfart-Kugelberg-Welander disease, Neurology (Minneap.j, 15 : 469473.
Stefanis, C., Th. Papapetropoulos, S. Scarpalezos, G. Lygidakis and C.P. Panayiotopoulos (1975) X-linked spinal and bulbar muscular atrophy of late onset - - A separate type of motor neuron disease? J. neurol. Sci., 24: 493-503.
Tsukagoshi, H., H. Shoji and T. Furukawa (1970) Proximal neurogenic muscular atrophy in adolescence and adulthood with X-linked recessive inheritance, Neurology (Minneap.), 20:1188-1193.
Weiner, L. P. (1980) Possible role of androgen receptors in amyotrophic lateral sclerosis - - A hypothesis, Arch. Neurol. (Chic.), 37: 129-131.
Wilson, J. D., M. J. Harrod, J. L. Goldstein, D. J. Hemsell, P. C. MacDonald (1974) Familial incomplete male pseudohermaphroditism, type I - - Evidence for androgen resistance and variable clinical manifestations in a family with the Reifenstein syndrome, N. Engl. J. Med., 290:1097-1103.
ADDENDUM
Since the submission of this manuscript another paper has appeared [A. E. Harding, P.K. Thomas, M. Baraitser, P. G. Bradbury, J.A. Morgan-Hughes and J. R. Ponsford (1982) X-linked recessive bulbo- spinal neuropathy - - A report of ten cases, J. Neurol. Neurosurg. Psychiat., 45: 1012-1019]. This report emphasizes the similarities among patients with and without definite X-linked recessive inheritance and describes diminished fertility, testicular atrophy and azoospermia in several cases. A primary testicular failure is also suggested by the endocrinological studies in these patients.
Related Documents





![Perinatal Testicular · PDF filePerinatal Testicular TorsionTorsion Audrey C. Durrant, ... departments with acute scrotum. ... Neonatal Testicular Torsion.ppt [Compatibility Mode]](https://static.cupdf.com/doc/110x72/5a9f7f227f8b9a62178cccbd/perinatal-testicular-testicular-torsiontorsion-audrey-c-durrant-departments.jpg)





