A A DVANCES DVANCES IN IN I I NFLAMMATORY NFLAMMATORY B B OWEL OWEL D D ISEASE ISEASE presented by The Foundation for Clinical Research in Inflammatory Bowel Disease 2004

A DVANCES IN I NFLAMMATORY B OWEL D ISEASE presented by The Foundation for Clinical Research in Inflammatory Bowel Disease .
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AADVANCESDVANCES ININ
IINFLAMMATORYNFLAMMATORY
BBOWELOWEL DDISEASEISEASE
presented by
The Foundation for Clinical Research in Inflammatory Bowel Disease
www.clinicalresearchinibd.org
2004

AADVANCESDVANCES ININ
IINFLAMMATORYNFLAMMATORY
BBOWELOWEL DDISEASEISEASE
presented by
The Foundation for Clinical Research in Inflammatory Bowel Disease
www.clinicalresearchinibd.org
2004

AADVANCESDVANCES ININ
IINFLAMMATORYNFLAMMATORY
BBOWELOWEL DDISEASEISEASE
presented by
The Foundation for Clinical Research in Inflammatory Bowel Disease
www.clinicalresearchinibd.org
2004

Inflammatory Bowel Disease (IBD) vs.
Irritable Bowel Syndrome (IBS)
• IBD = Inflammatory Bowel Disease– Chronic intestinal inflammation – Crohn’s disease, Ulcerative Colitis
• IBS = Irritable Bowel Syndrome– No tissue abnormality
• Change in bowel habits– Diarrhea/ Constipation/ Alternating bowel patterns
• Pain relieved with bowel movement• Increased sensitivity to intestinal motility
IBD: Overview
• Total number of cases– More than 1 million cases estimated in
United States– Ulcerative Colitis: 50%– Crohn’s disease: 50%
• Number of new cases annually– 10 new cases per 100,000 people per year– Peak onset occurs between ages of 10 and 19– Young children: 2%
IBD: Overview
• Scope of the disorder (United States)– 700,000 physician visits per year– 100,000 hospitalizations per year
• Long-term outlook– Chronic, lifelong disease without medical cures– Surgery for 50% to 80% of Crohn’s disease patients – Surgery for 20% of Ulcerative Colitis patients
• Most patients live normal, productive lives!
UCUC CDCD
Indeterminate colitis
The Spectrum of IBD
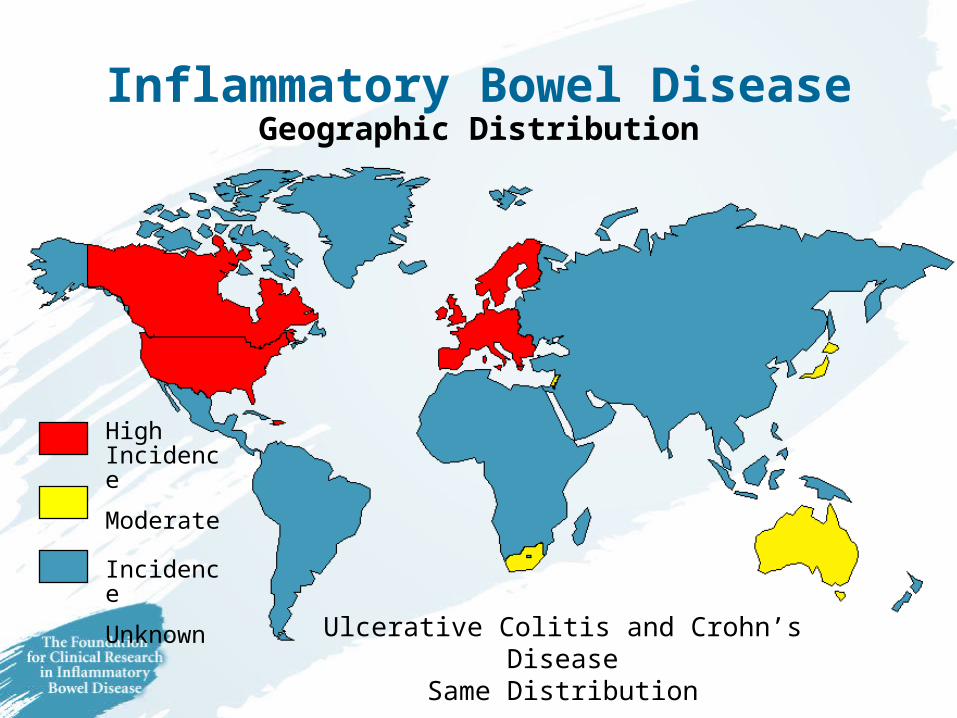
Inflammatory Bowel DiseaseGeographic Distribution
Ulcerative Colitis and Crohn’s DiseaseSame Distribution
High Incidence
Moderate Incidence
Unknown

Potential Causes of IBD
Genetics ImmuneSystem
Environment

Do All Causes Contribute Equally?
Genetics ImmuneSystem
Environment
GeneticsImmuneSystem
Genetics
Environment
Environment
ImmuneSystem

Evidence for Genetic Susceptibility to IBD
• Racial and ethnic risks of IBD
• Multiple family members with IBD
• Patterns of IBD in identical vs. fraternal twins
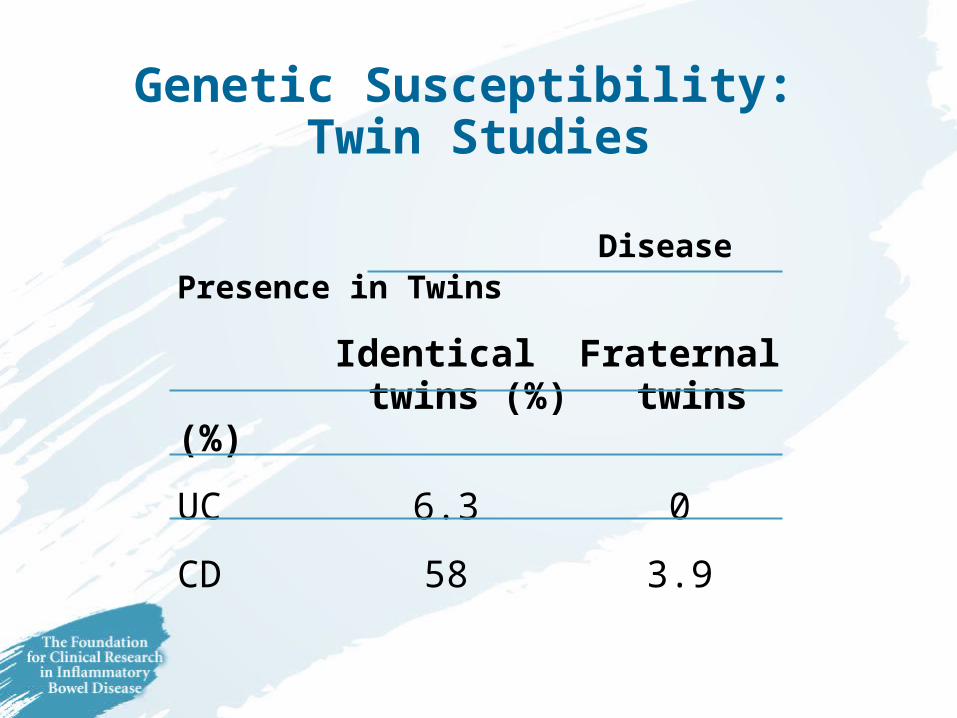
Genetic Susceptibility: Twin Studies
Disease Presence in Twins
Identical Fraternal twins (%) twins (%)
UC 6.3 0
CD 58 3.9
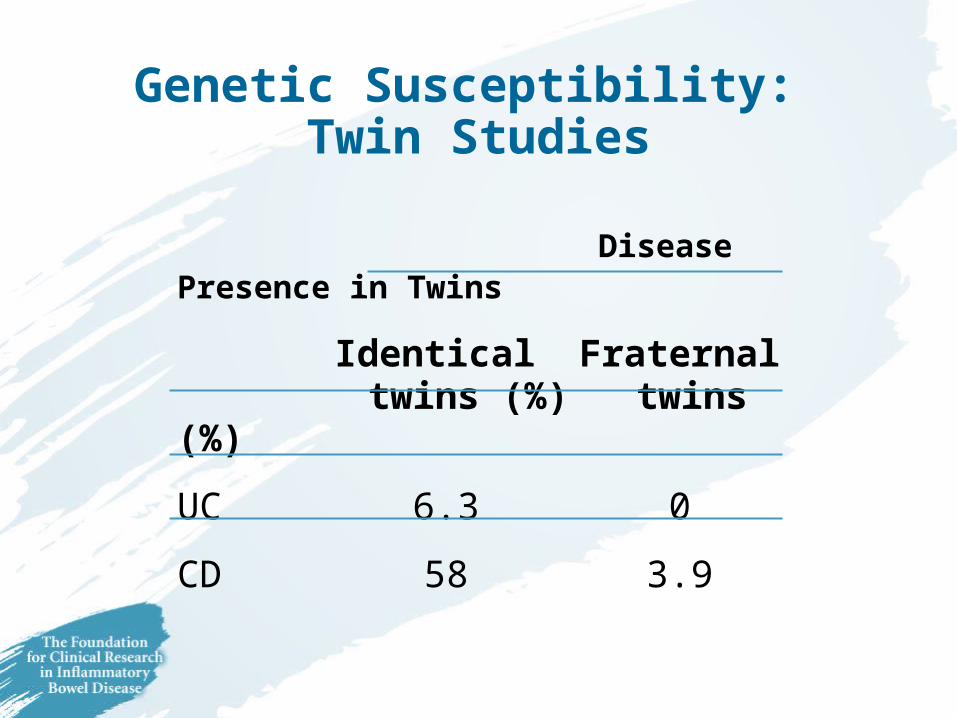
Genetic Susceptibility: Twin Studies
Disease Presence in Twins
Identical Fraternal twins (%) twins (%)
UC 6.3 0
CD 58 3.9

Searching for IBD Genes
• Candidate Gene Approach– Based on “hunch”– Investment low, likelihood
of success low
• Genome Wide Screen– Better in families with
multiply members affected– Looking for evidence of “linkage”

Searching for IBD Genes
• Candidate Gene Approach– Based on “hunch”– Investment low, likelihood
of success low
• Genome Wide Screen– Better in families with
multiply members affected– Looking for evidence of “linkage”
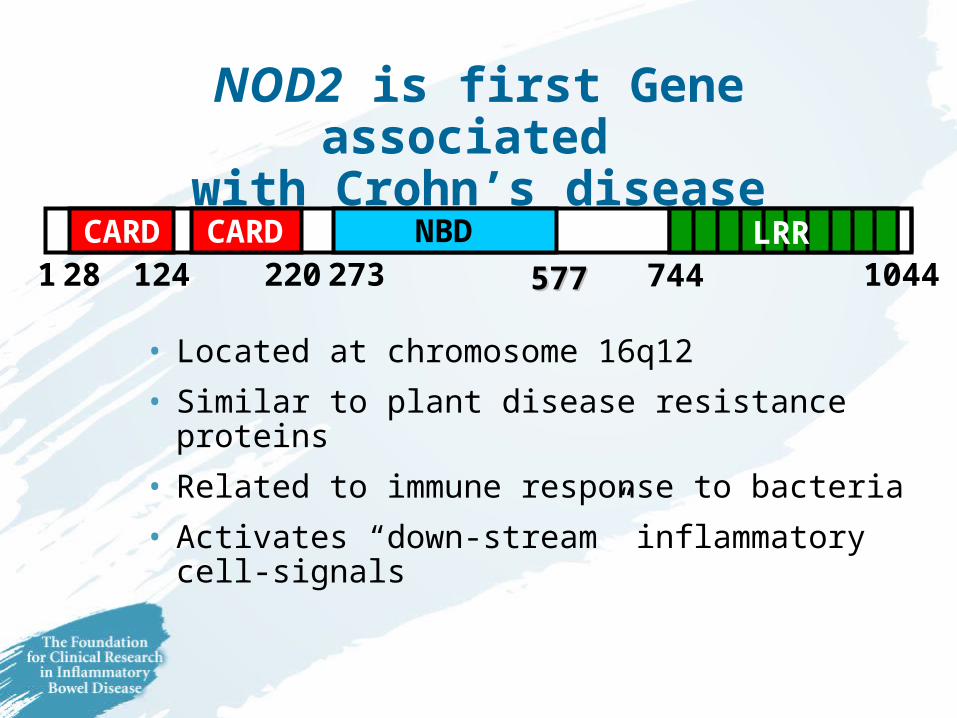
NOD2 is first Gene associated with Crohn’s disease
• Located at chromosome 16q12
• Similar to plant disease resistance proteins
• Related to immune response to bacteria
• Activates “down-stream” inflammatorycell-signals
1 28 124 220 273 577577 744 1044LRRCARD CARD NBD
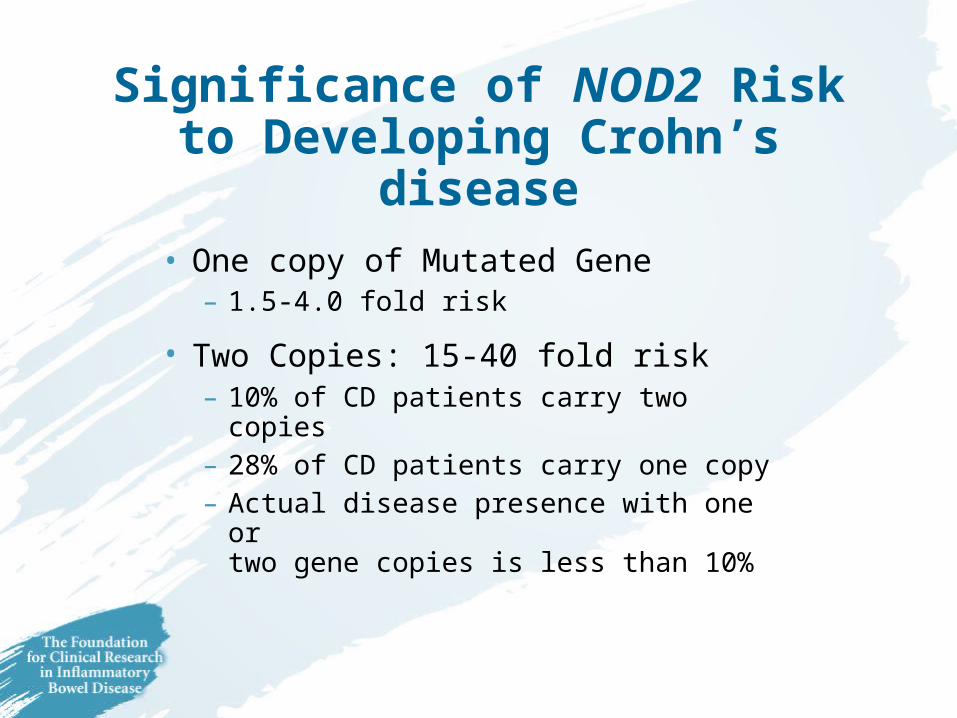
Significance of NOD2 Risk to Developing Crohn’s disease
• One copy of Mutated Gene– 1.5-4.0 fold risk
• Two Copies: 15-40 fold risk – 10% of CD patients carry two copies– 28% of CD patients carry one copy– Actual disease presence with one or
two gene copies is less than 10%

Environmental Triggers
IBD
Antibiotics
Diet
Smoking
Infections
NSAIDs
Stress

Environmental Triggers
IBD
Antibiotics
Diet
Smoking
Infections
NSAIDs
Stress
Smoking in IBD
• Ulcerative Colitis– Smoking can protect against UC– Ex-smokers are more likely to develop UC
• Crohn’s disease– Twofold risk in current smokers– Smokers are less responsive to treatment– Smokers are more likely to develop recurrence
of disease after surgery
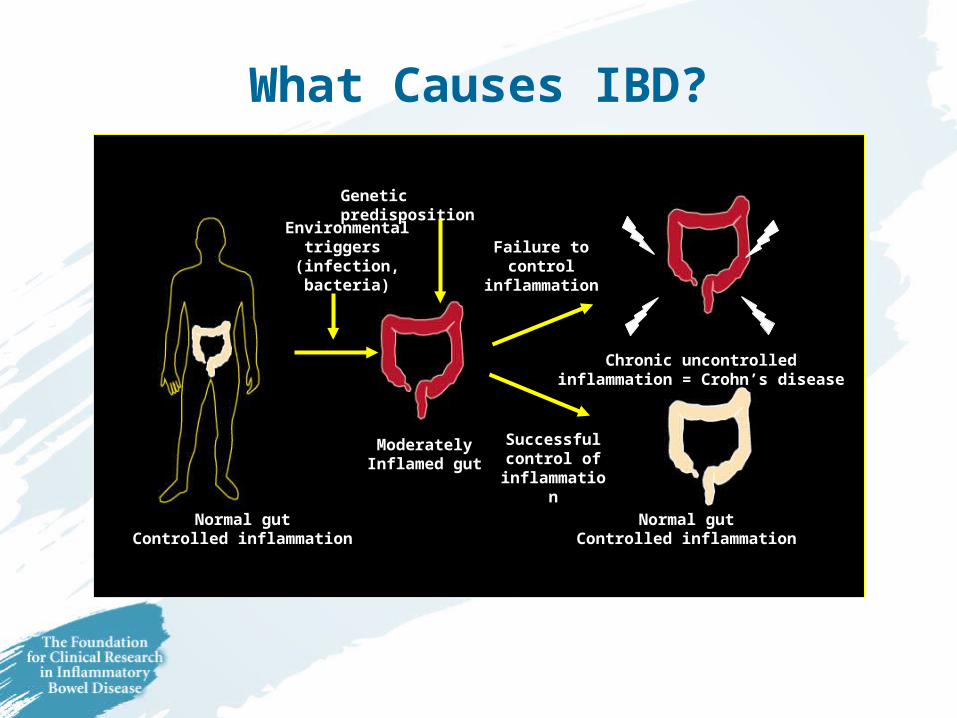
Environmentaltriggers
(infection, bacteria)
ModeratelyInflamed gut
Failure to control inflammation
Chronic uncontrolledinflammation = Crohn’s disease
Successful control of
inflammation
Normal gutControlled inflammation
Normal gutControlled inflammation
Genetic predisposition
What Causes IBD?

How IBD is Diagnosed
• Clinical history
• Physical examination
• Laboratory tests
• Endoscopy (Gastroscopy/Colonoscopy)
• X-ray findings
• Tissue biopsy (pathology)
How IBD is Diagnosed
• Clinical history
• Physical examination
• Laboratory tests
• Endoscopy (Gastroscopy/Colonoscopy)
• X-ray findings
• Tissue biopsy (pathology)
How IBD is Diagnosed
• Clinical history
• Physical examination
• Laboratory tests
• Endoscopy (Gastroscopy/Colonoscopy)
• X-ray findings
• Tissue biopsy (pathology)

Colonoscopy in IBD
• Diagnosis of IBD (UC vs. CD)– Allows visualization of large intestine
and ileum– Allows biopsies to examine colon tissue
• Determines activity of disease
• Important for pre-cancer surveillance in UC and CD
Colonoscopy in IBD
• Diagnosis of IBD (UC vs. CD)– Allows visualization of large intestine
and ileum– Allows biopsies to examine colon tissue
• Determines activity of disease
• Important for pre-cancer surveillance in UC and CD

Colonoscopy
• Requires complete “cleansing” of colon to allow visualization of bowel lining
• Preparations include:– Golytely®/Colyte® purge
• Requires drinking 1 gallon of solution
– Fleets prep®
• Small volume of purge, large volume of water
– Visicol® tablets
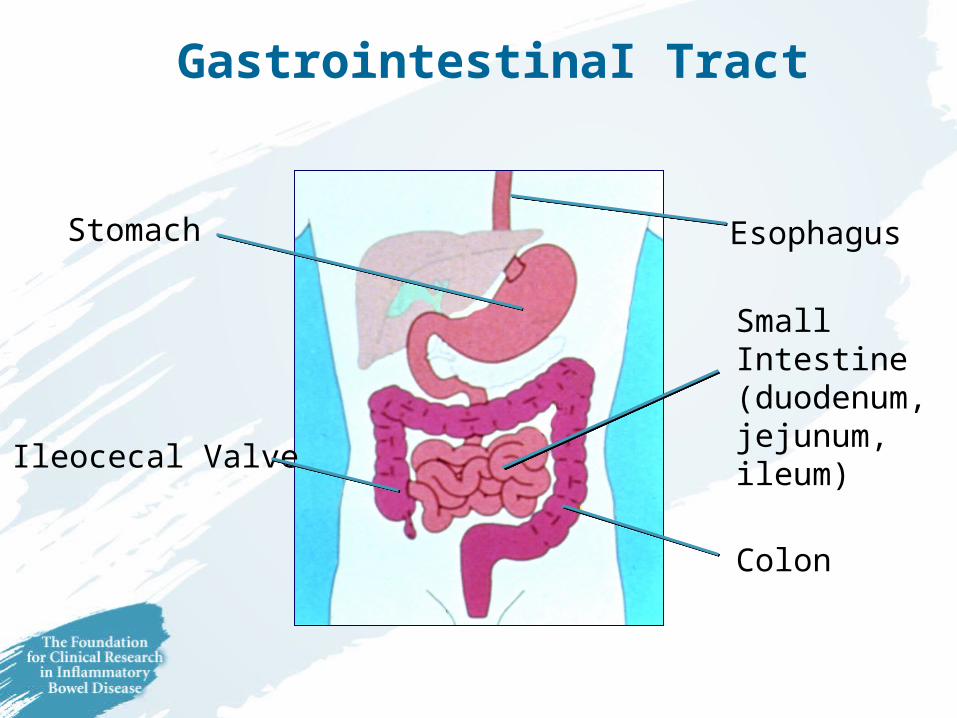
GastrointestinaI Tract
Stomach
Colon
Small Intestine(duodenum, jejunum, ileum)
Esophagus
Ileocecal Valve
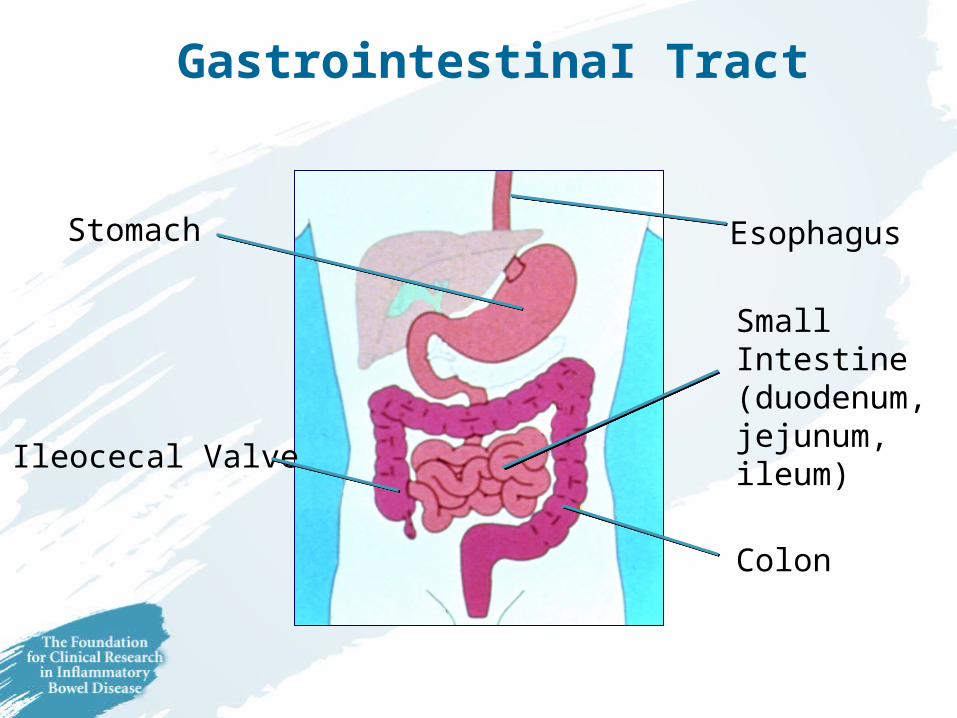
GastrointestinaI Tract
Stomach
Colon
Small Intestine(duodenum, jejunum, ileum)
Esophagus
Ileocecal Valve
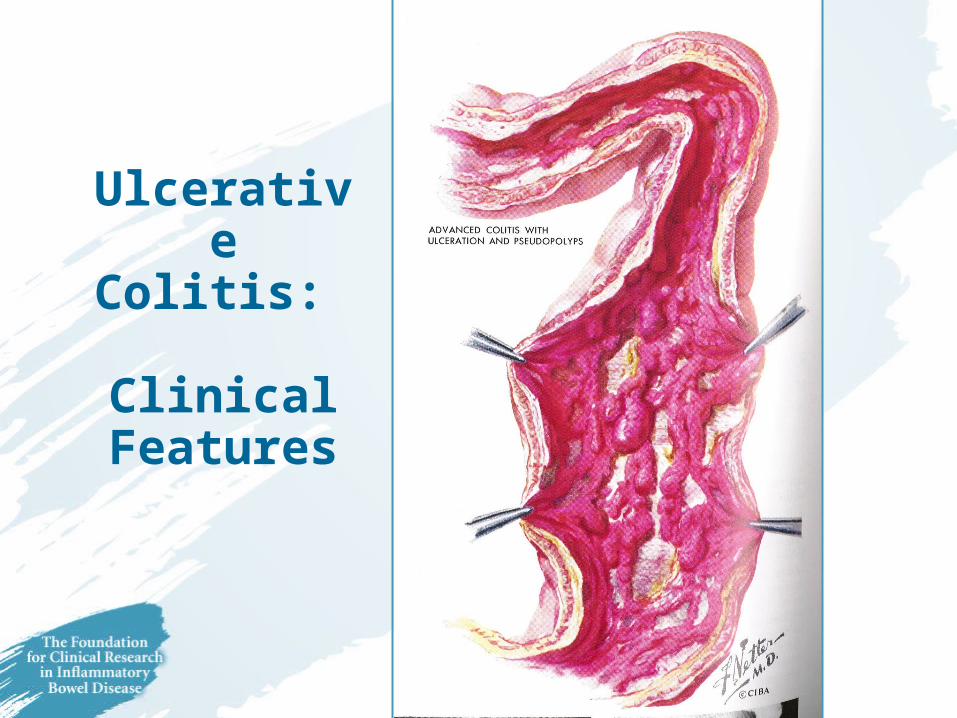
Ulcerative Colitis: Clinical
Features
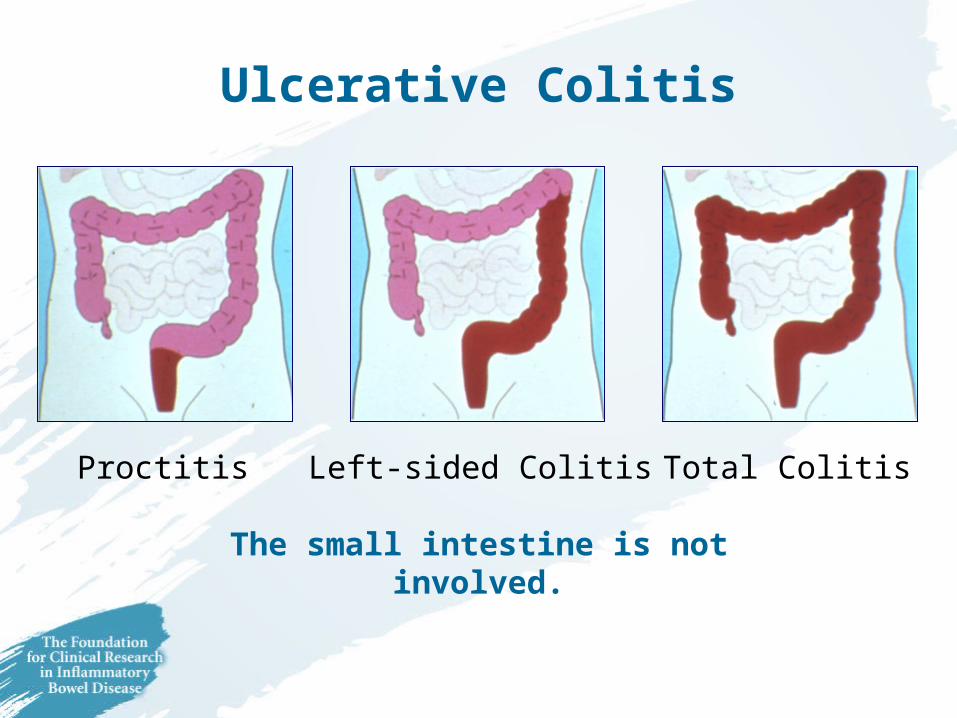
Ulcerative Colitis
Left-sided ColitisProctitis Total Colitis
The small intestine is not involved.

Symptoms of Ulcerative Colitis
• Symptoms depend on extent and severity of inflammation– Rectal bleeding and urgency to evacuate– Diarrhea– Abdominal cramping– Extraintestinal (systemic) symptoms
• Joint pain/swelling• Eye inflammation• Skin lesions
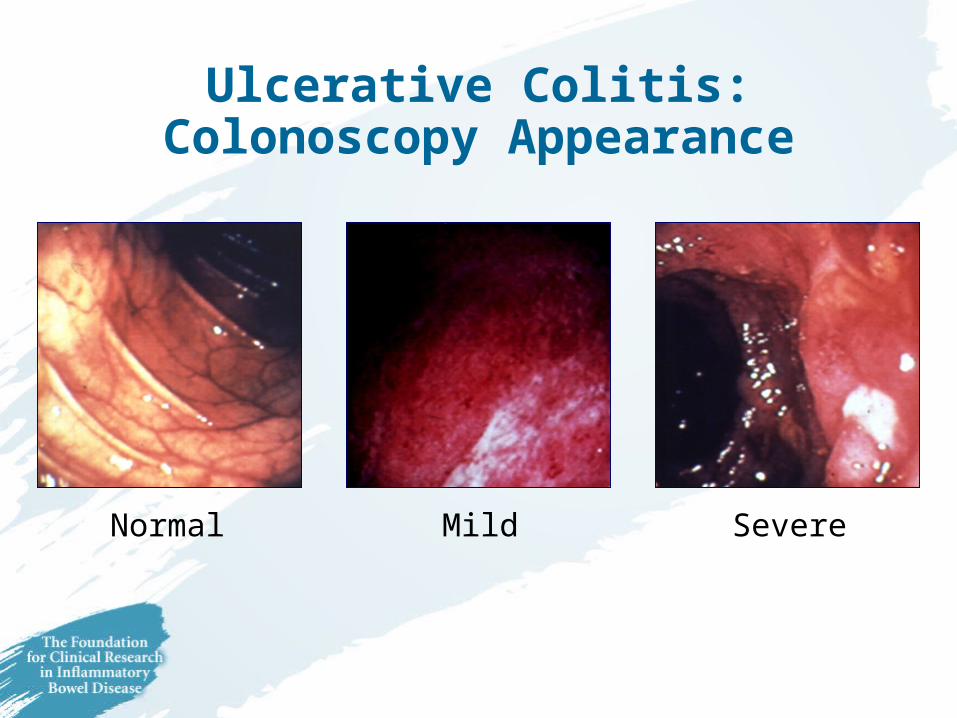
Ulcerative Colitis:Colonoscopy Appearance
MildNormal Severe
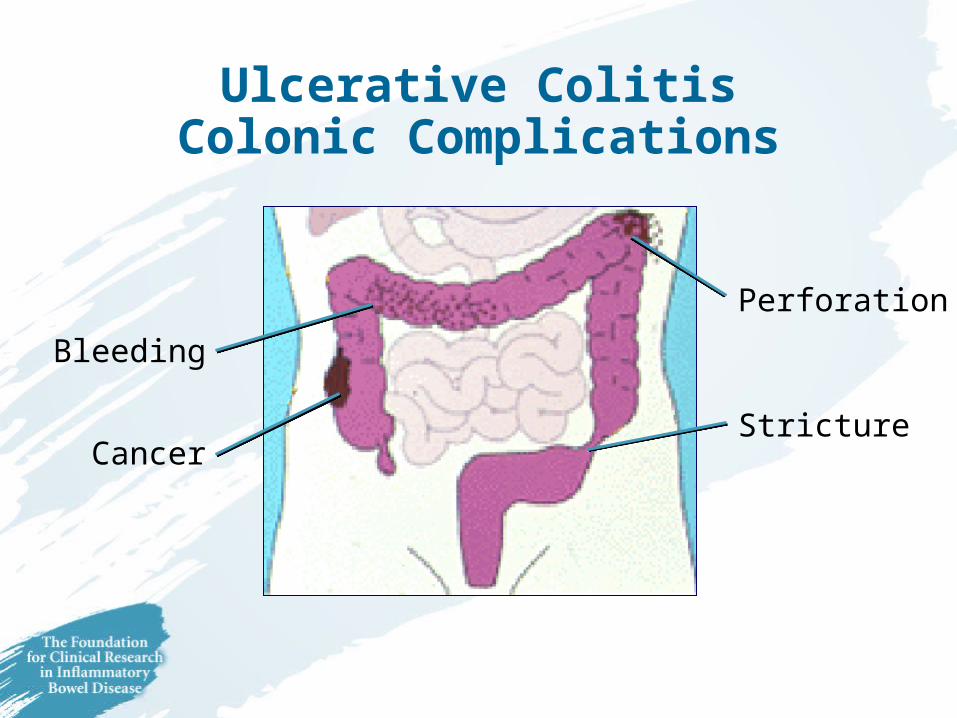
Ulcerative ColitisColonic Complications
Perforation
Stricture
Bleeding
Cancer
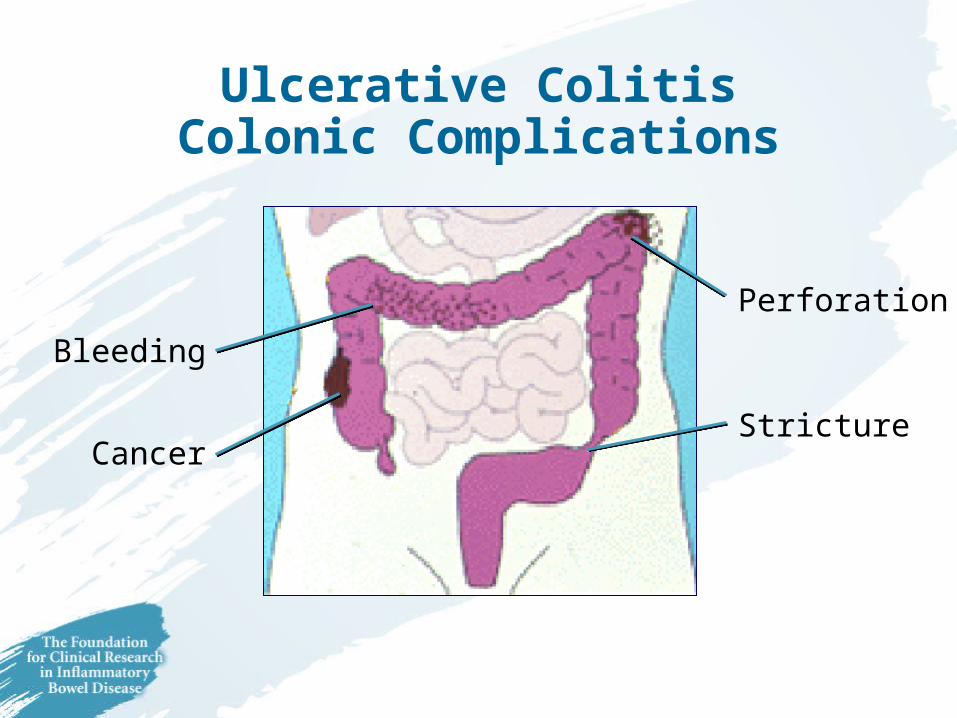
Ulcerative ColitisColonic Complications
Perforation
Stricture
Bleeding
Cancer

Crohn’s Disease:Distribution
Upper GI
Ileocolic(most common)
Colon
Small Intestine
Common Symptoms of Crohn’s Disease
• Diarrhea
• Abdominal pain and tenderness
• Loss of appetite and weight
• Fever
• Fatigue
• Rectal bleeding and anal ulcers
• Stunted growth in children
Common Symptoms of Crohn’s Disease
• Diarrhea
• Abdominal pain and tenderness
• Loss of appetite and weight
• Fever
• Fatigue
• Rectal bleeding and anal ulcers
• Stunted growth in children

Crohn’s Disease:Colonoscopic Appearance
CobblestoneDiscrete Ulcer Stricture(Narrowing)
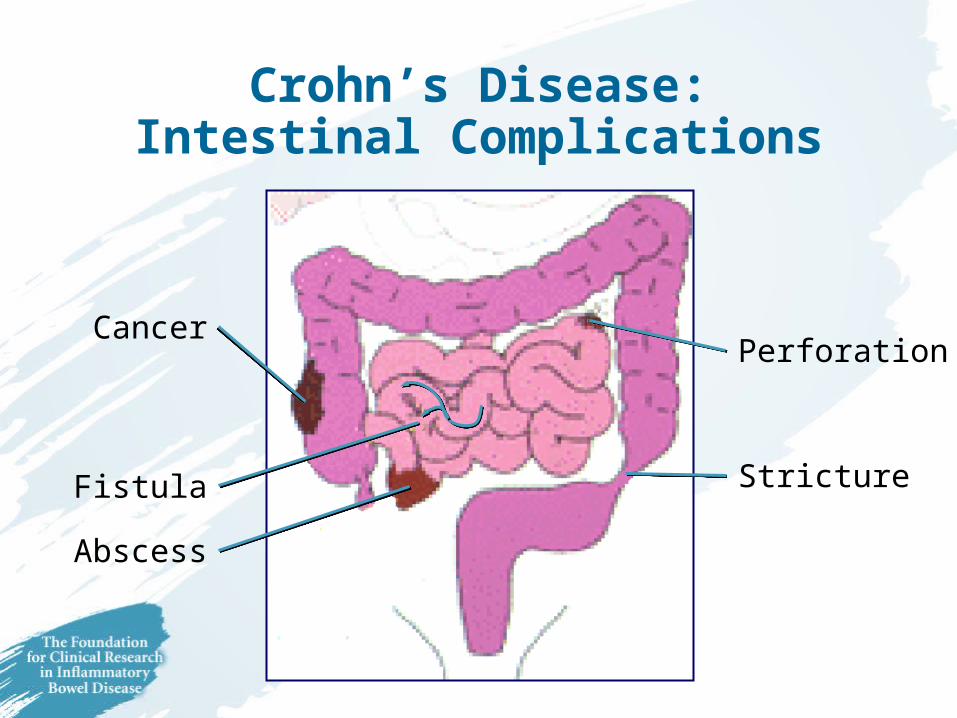
Perforation
Stricture
Cancer
Fistula
Abscess
Crohn’s Disease:Intestinal Complications
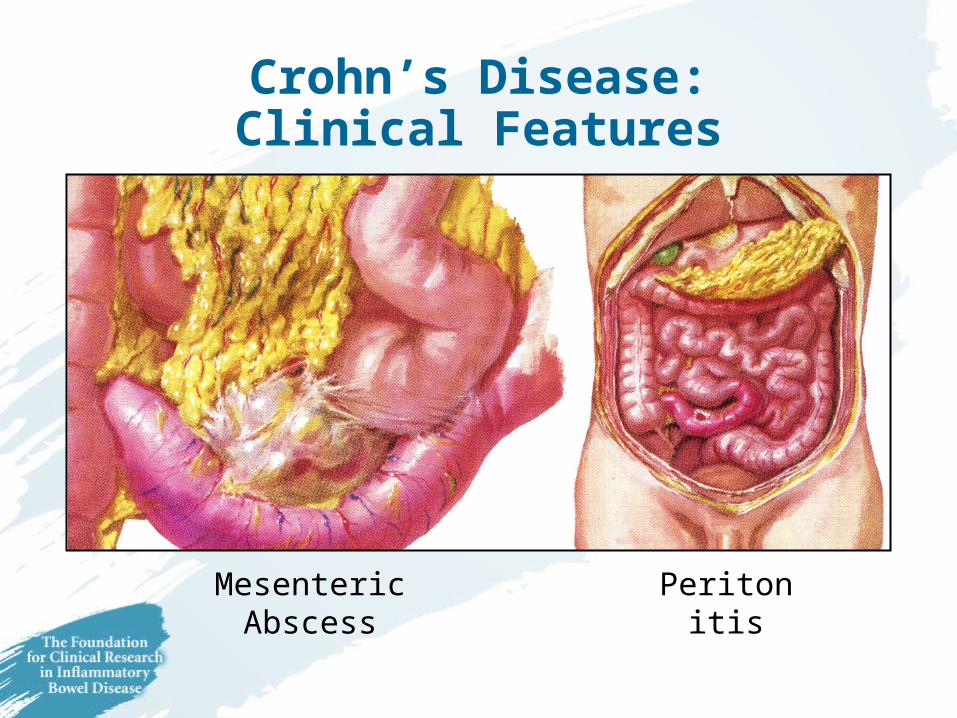
Crohn’s Disease:Clinical Features
PeritonitisMesenteric Abscess

Crohn’s Disease:Clinical Features
Internal Fistulae

Peri-Anal Fistulaeand/or Abscesses
External Fistula(via appendectomy incision)
Crohn’s Disease: Clinical Features

Fistula
Skin Tag
Abscess
Fissure
Crohn’s Disease:Perianal Problems
IBD: Extra-intestinal Manifestations
SkinEye
Bones and JointsKidneyLiver/
Gall Bladder
IBD: Extra-intestinal Manifestations
SkinEye
Bones and JointsKidneyLiver/
Gall Bladder

IBD:Skin Lesions
Erythema nodosum
Pyoderma gangrenosum

Treatment ofInflammatory Bowel Disease
Surgery
EmotionalSupport
Nutrition
Medications

IBD:Management Goals
Relievesymptoms
Treat inflammation
Treatcomplications
Address psychosocial
issues
Identify dysplasiaand detect
cancerImprove daily
functioning
Replenish nutritional
deficits
Minimize treatment toxicity
Maintain remission
EstablishDiagnosisEstablishDiagnosis

What Patients Should Expect
• Prior to diagnosis– Quick access/referral from Primary Care to
Specialist (Gastroenterologist)
• At diagnosis– Thoughtful explanation of disease with
opportunity for discussion
What Patients Should Expect
• Long-term follow-up– Continuity of care
• Primary Care Physician (if confident)• Gastroenterologist should be available
– Consideration of quality of life– Acknowledgement of problems– Access to second opinions– Maintain dignity!
What Patients Should Expect
• Hospital management– Knowledgeable MD/nursing staff– Willingness to refer to specialist center– Communication with patients/families– Encouragement of self-management– Choice in medical/surgical therapies– Access to dietitians, social workers

Medical Therapies for Inflammatory Bowel Disease
• 5-ASA agents– Asacol®
– Azulfidine®
– Colazal®
– Dipentum®
– Pentasa® – Rowasa® Enema– Canasa® Suppository

Medical Therapies for Inflammatory Bowel Disease
• Antibiotics– Cipro®
– Flagyl®
• Steroids– ACTH– Medrol®
– Prednisone– Cortenema®
– Cortifoam®

Medical Therapies for Inflammatory Bowel Disease
• Immunologic agents– Imuran® (Azathioprine)– Purinethol® (6-MP) – Neoral® (Cyclosporine)– Methotrexate
• Biologic agents– Remicade® (Infliximab)
5-ASA agents (Aminosalicylates)
• Induce remissions in mild-moderate – UC/CD
• Maintain remissions in mild-moderate UC
• Maintain remissions in CD after:– Medical treatment– Surgical resections

5-ASA agents(Aminosalicylates)
Benefits
• Well-tolerated
• Few side effects
• Relatively inexpensive
• Oral or Rectal
• Safe for all ages & pregnancy
Risks
• Rare allergies/side effects
• Not helpful in severe disease
• Not helpful after steroids (particularly CD)
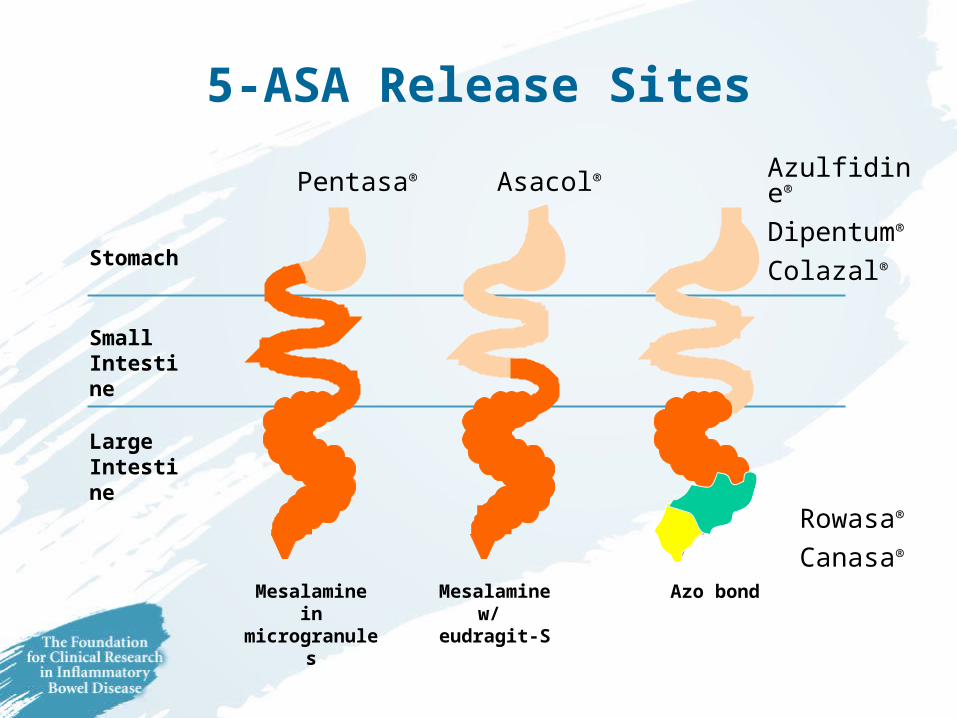
Stomach
Small Intestine
Large Intestine
Mesalamine in microgranules
Pentasa®
Mesalaminew/
eudragit-S
Asacol®
Azo bond
Azulfidine®
Dipentum®
Colazal®
5-ASA Release Sites
Rowasa®
Canasa®
Rationale for Topical Therapy5-ASA or Steroids
• Treats the inflammation directly
• Best initial choice for active ulcerative proctitis

Corticosteriods
• Prednisone, Hydrocortisone, Medrol®, Decadron®, Cortenema®, Cortifoam®, ACTH
• Administered by pill, IV or enema
• Induce remissions in UC and CD
• No maintenance benefits
Corticosteriods
Benefits
• Induces remissions in UC and CD
• Quick fix
• Inexpensive
• Oral or rectal
Risks• No long-term benefits• Numerous side effects
– Cushingoid changes– Hypertension– Diabetes– Osteoporosis– Acne– Cataracts– Depression– Growth retardation

Antibiotics
• Flagyl® (Metronidazole), Cipro® (Ciprofloxacin, Ampicillin, etc.)
• Treats mild symptoms of Crohn’s disease– Active disease when colon is involved– Peri-anal fistulae
• Intravenous to treat severe colitis or infections such as abscess
Antibiotics
Benefits
• Mild-moderate CD
• Fistula and peri-anal CD
• Reduce recurrence after surgery (?)
Risks
• Not effective in UC
• Flagyl® (Metronidazole)– Neuropathy– Coated tongue– Yeast infections
• Cipro® (Ciprofloxacin)– Yeast infections– Tendon injury

Immune-Modulators Imuran® (azathioprine) & Purinetheol® (6-MP)
• Long-term (maintenance) treatments for UC or CD– Can treat fistulas in CD over long-term
• Primarily for patients unable to get off steroids
• Requires continuous monitoring of blood counts

Immune-Modulators Imuran® (azathioprine) & Purinetheol® (6-MP)
Benefits
• “Steroid-sparing” in UC and CD
• Long-term maintenance
• Relatively inexpensive
Risks
• Can lower blood counts and “immunity”– Small risk of infections
• Requires long-term monitoring
• Occasional allergies– Pancreatitis– Fever

Immune-Modulators Imuran® (azathioprine) & Purinetheol® (6-MP)
Myths
• Dangerous drugs used to treat cancer
• Cause cancer
• Should not be used longer than 3 years
• If they don’t work over 3-6 months, they will not work
• Must be stopped before or during pregnancy
Facts
• Do not cause cancer
• Can be used for more than 3 years
• If they don’t seem to work at first, the dose needs to be reassessed
• Can be used during pregnancy,
– Must be monitored

Cyclosporine
Benefits
• Effective in severe UC
• Effective in Crohn’s disease?
• Works rapidly
Risks
• Kidney damage
• Increased infection, tumors,?
Methotrexate
• Used for many decades in Rheumatoid Arthritis
• Useful in Crohn’s disease to reduce steroids
• More effective given as injection once a week
• Common side effects– Nausea, flu-like symptoms day of injection
• Rare side effects– Liver disease and Pneumonia
• Cannot be used if attempting pregnancy!!!

Biologic Therapy: Remicade® (infliximab)
• Blocks the immune system reaction that causes inflammation
• Rapidly relieves symptoms
• Allows discontinuation of steroids without recurrence of symptoms
• Can be given repeatedly over time to maintain remission

Biologic Therapy: Remicade® (infliximab)Benefits
• Induces and maintains remissions in CD
• Rapidly relieves symptoms & fistula drainage
• Steroid-sparing
• Effective even whenother therapiesfail
Risks
• Allergic reactions to intravenous infusions
• Development of antibodies and loss of response
• Reactivation of TB and other rare infections
• Expensive
How is Remicade® administered?
• Intravenous infusion
• Allergic infusion reactions: 20% of patients– Usually manageable – Often preventable with
repeated infusions
• Discontinuation of therapy due to infusion reactions is rare
Weighing the Benefits and Risks of Treatment
Potential BenefitsPotential Risks
• Control inflammation
• Improve symptoms
• Improve quality of life
• Prevent relapse
• Reduce complications
• Reduce surgery
• Short-term side effects
• Long-term toxicity
• Cost

Managing Nutrition in IBD• Malnutrition can occur in IBD
– Decreased intake of food• Symptoms• Overly zealous restriction
– Decreased absorption of nutrients• Active disease, small intestine
– Increased needs for calories and protein
• Professional nutritional assessment
• Tailor diet to individual needs & preferences
• Dietary supplements
Managing Nutrition in IBD• Malnutrition can occur in IBD
– Decreased intake of food• Symptoms• Overly zealous restriction
– Decreased absorption of nutrients• Active disease, small intestine
– Increased needs for calories and protein
• Professional nutritional assessment
• Tailor diet to individual needs & preferences
• Dietary supplements
Surgery in IBD
Ulcerative Colitis
• Surgery (colectomy, removal of colon) is curative
• Colectomy & ileostomy
• Colectomy & ileo-anal anastomosis (J-pouch)
Crohn’s Disease
• Surgery does not cure
• Disease recurs after a resection– Less after an “ostomy”
• Resection of inflamed segments to treat complications or “refractory” disease

Surgery in IBD
Ulcerative Colitis
• Surgery (colectomy, removal of colon) is curative
• Colectomy & ileostomy
• Colectomy & ileo-anal anastomosis (J-pouch)
Crohn’s Disease
• Surgery does not cure
• Disease recurs after a resection– Less after an “ostomy”
• Resection of inflamed segments to treat complications or “refractory” disease

Ulcerative Colitis:Indications for Surgery
• Failure to control severe attacks or toxic megacolon
• Acute complications
• Chronic symptoms despite medical therapy
• Medication side effects without disease control
• Dysplasia or Cancer
Crohn’s Disease:Indications for Surgery
• Obstructing strictures
• Complicating fistula
• Peri-anal abscess
• Toxic megacolon
• Localized, unresponsive disease
Colorectal Cancer Risks in IBD
• Compared to general population– Risk is 20 times higher and– Occurs at lower age
• Risk is same for UC and CD according to:– How much of colon is affected– How long the disease is present– If patient has liver disease (PSC)
• Risk is may be related to severity/activity of disease

Preventing Colon Cancer in IBD• Compliance with maintenance medications
– 5-ASA agents
• Regular follow-up and surveillance colonoscopies– Every 1-2 years after 10 years– Every year after 20 years
• Colectomy (removal of colon) if:– Dysplasia (confirmed pre-cancerous changes)– Unwilling to continue surveillance examinations

Osteoporosis and IBD
• Bone (skeletal) disease characterized by low bone density (mass)
• Increased “fragility” of bone
• Susceptibility to breaks (fractures)– Particularly of spine
(vertebrae) and hip

Osteoporosis in IBD
Risk Factors• Steroid therapy
• Smoking
• Active disease – Crohn’s disease > Ulcerative Colitis
• Females – Small stature– Family history– Post-menopausal
Preventing Osteoporosis in IBD
• Check bone density (DEXA or heel scan)
• Control active disease
• Weight bearing exercise
• Supplement calcium and vitamin D (Crohn’s disease or steroids)
• Bisphosphonates if low bone density– Actonel® or Fosomax®
IBD & Pregnancy
• Fertility is normal if disease is controlled
• Fertility is reduced in active disease
• Pregnancy outcomes are normal – Low birth weight/prematurity if active disease– NO INCREASED RISK OF BIRTH DEFECTS
• Risk of active disease after delivery– Stay on maintenance medications
IBD Medications & Pregnancy
• Medications that are safe:– 5-ASA agents– Steroids
• Low risk of cleft palate
– Most antibiotics– Imuran® (Azathioprine) and Purinethol®
(6-MP)– Remicade®(Infliximab)
• MUST BE AVOIDED– Methotrexate

Research in IBD
Where are We Heading?
Genetic Research
• Identify the gene locations– Family studies– Correlate genes with clinical patterns
• Identify the gene(s)– Likely multiple– Protective genes/harmful genes
• Identify function of genes
• How to manipulate genes

Research in the Environment
• Identify bacteria capable of causing disease– Measles virus, Mycobacteria Paratuberculosis
• Identify “normal” bacteria that produce “abnormal” immune response– Bacterial-Epithelial interactions
• Identify gene-microorganism interactions– Do immune systems mistake “self” for bacteria?

Options for Environmental Causes
• Treat patient if “infected”
• Eradicate from the environment
• Immunize to prevent “infection”
Research in Surgery
• Ileo-anal pouches– Preventing, treating Pouchitis
• Minimal invasive surgery – Laparoscopy
• Prevention of post-operative recurrence– Select subgroups– 6-MP, 5-ASA, antibiotics, biologics(?)

IBD Summary
• Ulcerative Colitis and Crohn’s disease are chronic diseases requiring long-term medical therapy
• Quality of Life is impaired during flare-ups and should be normal during remissions
• Life expectancy is same as general population
• Surgery cures Ulcerative Colitis & treats complications in Crohn’s disease
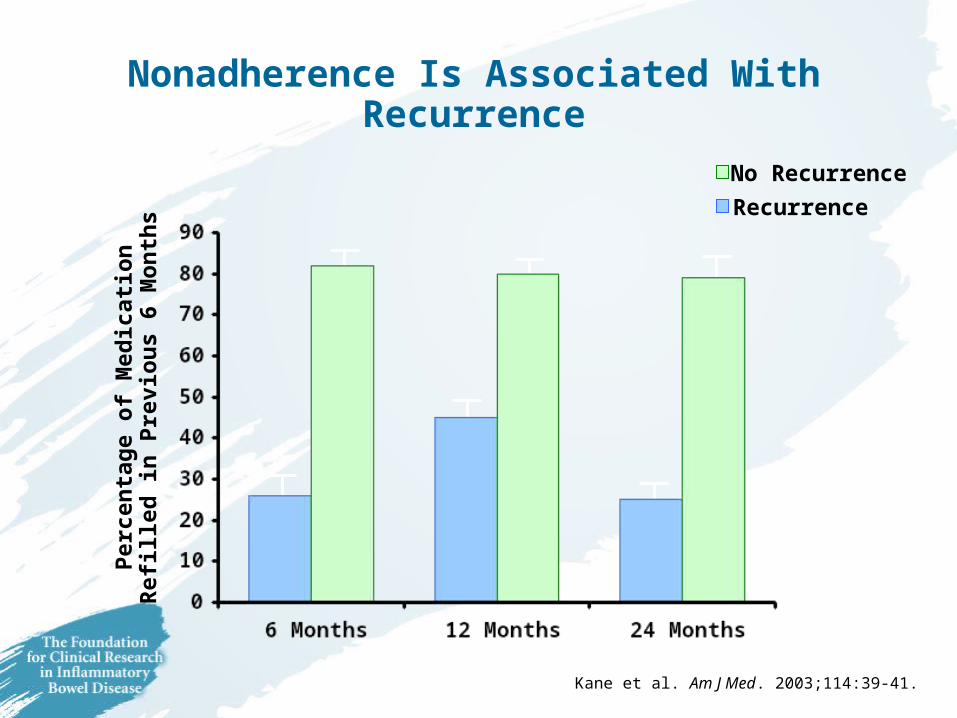
Nonadherence Is Associated With Recurrence
Follow-up
Pe
rcen
tag
e o
f M
edic
atio
nR
efill
ed in
Pre
vio
us
6 M
on
ths
No Recurrence
Recurrence
Kane et al. Am J Med. 2003;114:39-41.

Adherence Decreases Risk of Relapse
0
25
50
75
100P
erce
nta
ge
of
Pat
ien
ts (
%)
Rem
ain
ing
in R
emis
sio
n
40 36 32Adherent n =Nonadherent n = 59 32 28
Adherent
Nonadherent
0 12 24Time (months) 36
Kane et al. Am J Med. 2003;114:39-41.

for more information:
www.healthtalk.com
Related Documents











