A descriptive study of weight loss maintenance: 6 and 15 year follow-up of initially overweight adults S Sarlio-La ¨hteenkorva 1 *, A Rissanen 2 and J Kaprio 1,3 1 Department of Public Health, University of Helsinki, Helsinki, Finland; 2 Obesity Research Group, Helsinki University Central Hospital, Helsinki, Finland; 3 Department of Mental Health and Alcohol Research, National Public Health Institute, Helsinki, Finland OBJECTIVE: To describe factors associated with long-term maintenance of weight loss. DESIGN AND SUBJECTS: We identified initially overweight individuals (body mass index > 27 kg=m 2 , n 911) from the nationwide Finnish Twin Cohort and studied those who lost at least 5% of their body weight between 1975 and 1981. Subjects who had maintained weight loss until 1990 (38 men, 17 women) were compared to both re-gainers (28 men, 26 women) and the other overweight subjects in the cohort. MEASUREMENTS: Self-report data on weight, height, health behaviours and perceived well-being; self-report and register-based data on health status and use of medication. RESULTS: Only 6% of all overweight individuals lost and maintained at least 5% weight loss. In men weight loss maintenance was associated with a low level of stress and health-promoting behaviours but also with medical problems. Failure to maintain weight loss seemed to be associated with stressful life and past high alcohol intake. In women weight loss maintenance was associated with low initial well-being and health-compromising behaviours that improved after weight loss. CONCLUSION: Long-term weight loss maintenance is rare. Predictors of weight loss maintenance are different between women and men. International Journal of Obesity (2000) 24, 116–125 Keywords: overweight; weight loss maintenance; health; behaviour; well-being Introduction The weight of many obese individuals varies. Weight changes in adults appear to be determined mainly by environmental effects, 1 including health promoting behaviours such as regular exercise, 2–6 restricting diets 2 – 4,7 and high vegetable consumption. 8 Some potentially health damaging behaviours such as smok- ing, 5 drinking habits 9 and ill health may also be associated with weight loss. Both intentional and unintentional weight loss contribute to weight varia- bility. The importance on focusing on intentional weight loss has been recognized, 10 – 13 but assessing intentionality of weight loss, however, is problematic. Most intentional attempts to lose weight fail and prospective studies have shown that dieting even increases the risk of long-term weight gain. 4,14 More- over, it is possible that environmental or behavioural changes leading to altered lifestyle can result in sustained weight loss, even without a primary ‘inten- tion’ to lose weight. Various environmental 15 and psycho-social issues, 3,16 – 17 including perceived level of stress 16,18 – 19 and general life satisfaction 19 may be important for weight development, but these factors have rarely been studied. Indeed, characteristics of those overweight subjects who maintain weight loss, either intentionally or unintentionally, are incomple- tely understood. Long-term prognosis of weight reduction is poor and factors associated with sustained weight loss are inadequately understood. 10 Studies focusing on rare individuals that have been successful at losing excess weight and keeping it off provide one way of increas- ing our knowledge on weight loss maintenance. Exist- ing studies using this approach are treatment studies 20 or subjects are volunteers recruited from media and mailings to weight loss programmes. 2,15,21 Both approaches suffer from selection bias: overweight subjects seeking treatment or volunteering probably differ from the overweight population in general. In addition, studies on successful volunteers are retro- spective and treatment studies end up with small numbers of subjects. Although there are population- based retrospective studies on weight loss mainten- ance, 5 prospective studies focusing on subjects suc- cessful in weight loss maintenance have not been published. This prospective, population-based study describes the relationship between weight loss maintenance and (1) health status and use of medication, (2) health- related behaviours, and (3) indicators of subjective *Correspondence: S Sarlio-La ¨ hteenkorva, Department of Public Health, PO Box 41, FIN-00014, University of Helsinki, Helsinki, Finland. E-mail: sirpa.sarlio-lahteenkorva@helsinki.fi. Received 3 February 1999; revised 3 June 1999; accepted 27 July 1999 International Journal of Obesity (2000) 24, 116–125 ß 2000 Macmillan Publishers Ltd All rights reserved 0307–0565/00 $15.00 www.nature.com/ijo

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A descriptive study of weight loss maintenance:6 and 15 year follow-up of initially overweightadults
S Sarlio-LaÈhteenkorva1*, A Rissanen2 and J Kaprio1,3
1Department of Public Health, University of Helsinki, Helsinki, Finland; 2Obesity Research Group, Helsinki University Central Hospital,Helsinki, Finland; 3Department of Mental Health and Alcohol Research, National Public Health Institute, Helsinki, Finland
OBJECTIVE: To describe factors associated with long-term maintenance of weight loss.DESIGN AND SUBJECTS: We identi®ed initially overweight individuals (body mass index> 27 kg=m2, n� 911) fromthe nationwide Finnish Twin Cohort and studied those who lost at least 5% of their body weight between 1975 and1981. Subjects who had maintained weight loss until 1990 (38 men, 17 women) were compared to both re-gainers (28men, 26 women) and the other overweight subjects in the cohort.MEASUREMENTS: Self-report data on weight, height, health behaviours and perceived well-being; self-report andregister-based data on health status and use of medication.RESULTS: Only 6% of all overweight individuals lost and maintained at least 5% weight loss. In men weight lossmaintenance was associated with a low level of stress and health-promoting behaviours but also with medicalproblems. Failure to maintain weight loss seemed to be associated with stressful life and past high alcohol intake. Inwomen weight loss maintenance was associated with low initial well-being and health-compromising behavioursthat improved after weight loss.CONCLUSION: Long-term weight loss maintenance is rare. Predictors of weight loss maintenance are differentbetween women and men.InternationalJournal of Obesity (2000) 24, 116±125
Keywords: overweight; weight loss maintenance; health; behaviour; well-being
Introduction
The weight of many obese individuals varies. Weightchanges in adults appear to be determined mainly byenvironmental effects,1 including health promotingbehaviours such as regular exercise,2 ± 6 restrictingdiets2 ± 4,7 and high vegetable consumption.8 Somepotentially health damaging behaviours such as smok-ing,5 drinking habits9 and ill health may also beassociated with weight loss. Both intentional andunintentional weight loss contribute to weight varia-bility. The importance on focusing on intentionalweight loss has been recognized,10 ± 13 but assessingintentionality of weight loss, however, is problematic.Most intentional attempts to lose weight fail andprospective studies have shown that dieting evenincreases the risk of long-term weight gain.4,14 More-over, it is possible that environmental or behaviouralchanges leading to altered lifestyle can result insustained weight loss, even without a primary `inten-tion' to lose weight. Various environmental15 andpsycho-social issues,3,16 ± 17 including perceived level
of stress16,18 ± 19 and general life satisfaction19 may beimportant for weight development, but these factorshave rarely been studied. Indeed, characteristics ofthose overweight subjects who maintain weight loss,either intentionally or unintentionally, are incomple-tely understood.
Long-term prognosis of weight reduction is poorand factors associated with sustained weight loss areinadequately understood.10 Studies focusing on rareindividuals that have been successful at losing excessweight and keeping it off provide one way of increas-ing our knowledge on weight loss maintenance. Exist-ing studies using this approach are treatment studies20
or subjects are volunteers recruited from media andmailings to weight loss programmes.2,15,21 Bothapproaches suffer from selection bias: overweightsubjects seeking treatment or volunteering probablydiffer from the overweight population in general. Inaddition, studies on successful volunteers are retro-spective and treatment studies end up with smallnumbers of subjects. Although there are population-based retrospective studies on weight loss mainten-ance,5 prospective studies focusing on subjects suc-cessful in weight loss maintenance have not beenpublished.
This prospective, population-based study describesthe relationship between weight loss maintenance and(1) health status and use of medication, (2) health-related behaviours, and (3) indicators of subjective
*Correspondence: S Sarlio-LaÈ hteenkorva, Department of PublicHealth, PO Box 41, FIN-00014, University of Helsinki, Helsinki,Finland. E-mail: sirpa.sarlio-lahteenkorva@helsinki.®.Received 3 February 1999; revised 3 June 1999; accepted 27 July1999
International Journal of Obesity (2000) 24, 116±125ß 2000 Macmillan Publishers Ltd All rights reserved 0307±0565/00 $15.00
www.nature.com/ijo
well-being among overweight subjects before andafter weight loss. The goal is to characterize weightlosers and potential changes in their responsesthroughout the study. We hypothesize that differentfactors may be pertinent during various phases ofweight reduction. These may include factors that arerelevant when still obese, possible changes afterweight loss and potential outcomes of weight lossmaintenance.
Subjects
The Finnish Twin Cohort and selection of subjects for
the present study
The adult Finnish Twin Cohort was compiled in 1974from the Finnish Central Population Register in orderto study the relative importance of genetic and envir-onmental effects on chronic diseases.22 The baselinecohort comprised all same-sex twin pairs born inFinland before 1958 and alive in 1967. Subjectswere mailed similar questionnaires in 1975 and1981, and the response rates were 89% and 84%,respectively. An additional questionnaire was mailedin 1990 to twins born between 1930 and 1957, andwith both co-twins alive and in Finland in 1987, witha response rte of 77%.19
Complete information about current weight andheight from all three questionnaires was obtainedfrom 11,284 subjects. Our study focused on subjectswho were clearly overweight (body mass index,BMI> 27 kg=m2) at baseline in 1975 (n� 968).From this overweight sample the following exclusionswere made: 24 women who were pregnant at baselineby a linkage to the National Hospital DischargeRegister,23 two men and one woman diagnosed witha malignant cancer before 1983 by linkage to theFinnish Cancer Registry, as well as 20 men and ninewomen who reported being on a disability pension in1975. After these exclusions the ®nal sample con-sisted of 332 women and 579 men.
Weight loss maintainers
Subjects were classi®ed as weight loss maintainers ifthey had lost at least 5% of their body weight between1975 and 1981 and were still at least 5% below theiroriginal weight in 1990. The cut point of 5% waschosen on the basis of the literature.10 Since the 1990questionnaire asked respondents to also report theirlifetime maximum (non-pregnant) weight, weexcluded one woman and one man on the basis ofthis information: they reported weights that wereinconsistent with their earlier weight history. In addi-tion, the subjects were in 1990 asked to give theirweight 12 months and 5 years previously, and wewere also able to exclude subjects with obviousweight ¯uctuation: 13 women and 16 men whoreported weights that were not below their original
weight in 1975. We found 55 subjects (17 women, 38men) who met the criteria for weight loss mainte-nance. There were only two twin pairs among menwho maintained weight loss (one monozygotic, otherwith unknown zygosity) and none among women, andhence the analysis was done with no regard for twin-ship or zygosity.
Comparison groups
Two comparison groups were selected for both menand women:
1. Overweight. Originally this comparison groupconsisted of all other initially overweight subjectsin our cohort. In the analysis all men in this group(n� 540) were used. For women we had to useanother strategy since we found weight lossmaintainers to be markedly younger than over-weight women at large (birth year 1946 vs 1939,P< 0.0001), with a very skewed age distribution.Therefore, we selected at random four overweightcontrols from the same age group (same or nextbirth year) for each woman maintainer.
2. Re-gainers. This comparison group consists ofthose initially overweight subjects who lost atleast 5% of their body weight between 1975 and1981, but had regained more than they initiallylost by 1990. This group consists of 28 men and26 women.
Methods
Body mass and dieting
Subjects reported their weight in kilograms and heightin centimetres, which were rounded to nearest integralnumber. In addition, subjects were asked in 1990 torecall their weight 1 and 5 y previously, their lifetimemaximum (non-pregnant) weight, weight at the age of20 and 30 as well as weight and height of their spouse.BMI (weight in kilograms=height in metres squared)was used as a measure of relative weight. At baselinesubjects were asked if they were currently trying tolose weight, and in 1990 subjects were asked if theyhad ever dieted or tried to lose weight. Those admit-ting dieting either in 1975 or 1990 were classi®ed ashaving intentional weight loss attempts in the past.
Background variables
Educational attainment was obtained from the 1975questionnaire, employment and marital status from allthree (1975, 1981 and 1990) questionnaires. In addi-tion, subjects were asked whether they had eitherschoolchildren or younger children in their householdsin 1990.
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
117
International Journal of Obesity

Health status and use of medication
Information about current or past physician-diagnoseddiabetes, myocardial infarction or hypertension anduse of tranquillizers, sleeping pills and pain killerswithin past 12 months was obtained in all threequestionnaires. Information on the right to reimbur-sable medication for selected chronic diseases (suchas cardiovascular diseases, diabetes, asthma, psy-choses), and information about current or past appli-cations for disability pensions were obtained from theSocial Insurance Institution of Finland in 1987. Therecord linkage was done using the personal identi®ca-tion code assigned to all residents of Finland.
Health-related behaviour
Smoking, alcohol use and physical activity were usedas indicators of health-related behaviours in all threequestionnaires. In addition, selected dietary habitswere enquired into in 1975 and 1981. Data on pastand current smoking habits included questions aboutthe daily number of cigarettes and the age of startingsmoking among regular smokers.24 Alcohol use wasrecorded as beverage-type speci®c items (beer, wine,spirits) with frequency and quantity, and convertedinto grams of absolute alcohol per day as previouslyreported.25 The baseline questionnaire included addi-tional questions about possible previous greater alco-hol intake, and frequency as well as quantity of thisgreater intake. Current leisure-time physical activitywas evaluated with identical questions in 1975 and1981, but the 1990 questionnaire included physicalactivity during the travelling to and from work as apart of leisure-time physical activity. As previously,26
leisure physical activity index (MET h=d) was calcu-lated from the products of intensity � duration �monthly frequency. In addition, leisure time activityduring the past 5 y was asked for in 1981. Dietaryquestions included daily intake of coffee and tea in1975 and 1981 as well as the amount of sugar used onaverage in these beverages. In addition, frequency ofincluding vegetables or fruits in meals, daily intake ofhigh salt food items and type of spread on bread wereasked in 1981.
Indicators of well-being
Life satisfaction, perceived stress and selected symp-toms (sleep quality, breathlessness, musculoskeletalpains) were used as indicators of subjective well-being. Life satisfaction according to Allardt27 wasmeasured with a four-item scale on levels of interest,happiness, easiness and loneliness of life.19 The rangeof the total score was 4 ± 20, higher scores indicating aless satisfying life. Those with scores of 12 ± 20 wereclassi®ed as very dissatis®ed.28 Stress of daily activ-ities was assessed by a four-item scale19,29 and totalstress score was obtained by reversing the scale andsumming scores of all items. Thus, higher scoresindicate more stress in daily activities. Those withscores below 6 were classi®ed as stress-free.
The subjects were also asked whether they usuallyget short of breath when walking on level ground at anordinary pace with people of their own age or whenwalking uphill, climbing stairs or hurrying on levelground.30 In addition, sleep quality31 was questionedin 1975 and repeated in 1981. The questionnaire in1990 assessed insomnia32 and sleep disturbances. Ahistory of back, shoulder and=or neck pain causingdif®culties at work during recent years was includedin 1975 and 1981.
Statistical methods
Differences between weight loss maintainers andcomparison groups were tested with a Mann ± Whit-ney-U, two-way t-test or Pearson's chi-square test.Changes over time within a group were tested withWilcoxon's matched pairs signed-rank sum test. Allanalyses were computed with the SPSS 7.0 programand done separately for women and men.
Results
Only 5.1% of all initially overweight women and6.6% of men lost and maintained at least 5% weightloss. The women who maintained weight loss wereless often married at baseline than the re-gainers (35%vs 81%, P� 0.003), but there were no other differ-ences between the maintainers and the comparisongroups in the background variables (Table 1), includ-ing educational attainment, employment status,weight of their spouses, maximum weight duringlifetime and weight in twenties or thirties. However,the men who maintained weight loss had initiallyhigher BMI (30.0 kg=m2) than either the re-gainers(28.9 kg=m2, P� 0.018) or the overweight men(28.8 kg=m2, P< 0.0001), and they also lost moreweight than the re-gainers (9.7 vs 7.3 kg, P� 0.007).Subjects who were successful in weight loss main-tenance had signi®cantly lower BMIs than the com-parison groups in 1985, 1989 and 1990. Intentionalweight loss attempts were reported by nearly allwomen and three quarters of men irrespective of®nal weight loss outcome.
Health status and use of medication
Among men, no differences were found in self-reported health status or use of medication betweenthe maintainers and the comparison groups at baselinein 1975 (Table 2). However, the maintainers reportedmore diabetes than the overweight men in 1981 (8%vs 2%, P� 0.035) and in 1990 (22% vs 8%,P� 0.003). Also compared to the re-gainers, themaintainers had more diabetes (22% vs 4%,P� 0.038) and more hypertension (41% vs 18%,P� 0.05) in 1990. In addition, the use of medicationfor chronic diseases was more common among the
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
118
International Journal of Obesity

maintainers, of whom 42% had obtained the right forreimbursed medication for a chronic disease by 1987compared to only 23% of the overweight (P� 0.007)and 11% of the re-gainer men (P� 0.005). On theother hand, the maintainers reported use of tranquil-lizers less often than the re-gainers in 1981 (0% vs16%, P� 0.019) and in 1990 (3% vs 26%, P� 0.009).
A history of myocardial infarction was slightlymore common among women who maintained theirweight loss than among other women. There was alsosome indication of increased use of some drugsamong maintainer women. In 1981, they reportedmore use of sleeping pills than the overweightwomen (24% vs 2%, P� 0.001) and more pain killersthan the re-gainers (94% vs 68%, P� 0.043). No otherdifferences in the health status or use of medicationwere observed between the women who maintainedtheir weight loss and comparison groups
Health-related behaviour
Some gender-speci®c differences in health-relatedbehaviours between the weight loss maintainers andcomparison groups were observed already at baseline(Table3). Only 3% of the maintainer men reportedhaving had a higher alcohol intake in the past com-pared to 19% of the overweight men (P� 0.01) and43% of the re-gainers (P< 0.0001). In addition, themaintainers consumed less sugar in coffee and teathan the overweight men (5.1 vs 8.6 lumps daily,P� 0.01) and those who smoked had taken up the
habit at later age than the re-gainers. More health-promoting habits could be detected in 1981: morefrequent use of vegetables than the overweight men(P< 0.0001) or the re-gainers (P� 0.041), more fre-quent leisure time physical activity (P� 0.033),higher MET values (P� 0.001) and more frequentintensive physical activities during the previous 4 ± 5 y(P� 0.001) than the overweight men, however thesedifferences were not seen in 1990. In addition, therewere no differences in alcohol use between groups inany of the three questionnaires. The overweight menincreased their alcohol consumption from 1981 to1990 (P� 0.02), but otherwise changes in alcoholconsumption were not signi®cant. Both the maintai-ners (P� 0.004) and the overweight men (P� 0.008)increased their coffee consumption from 1975 to1981. A decreased intake of sugar in coffee and teafrom 1975 to 1981 was reported by the overweightmen (P< 0.0001) and the re-gainers (P� 0.008).Leisure-time MET values increased from 1975 to1981 in all groups of men.
Data on women show a different pattern. Adversehabits were associated with weight loss maintenance.Baseline data reveal that the maintainers had startedsmoking very young (mean 14 y) compared to theoverweight women (19 y, P� 0.008) or the re-gainers(21 y, P� 0.023). The maintainers also had a higherconsumption of cigarettes than the re-gainers (17 vs 9cigarettes daily, P� 0.013). At baseline the maintai-ners also exercised less frequently than the overweightwomen (P� 0.006) and had somewhat more fre-
Table 1 BMI, weight changes (means, standard deviations) and background variables (%) by weight change category in men andwomen
Men Women
Maintainers Overweight Re-gainers Maintainers Overweight Re-gainers(n�38) (n�540) (n�28) (n�17) (n�68) (n�26)
BMI (kg=m2),1975 30.0 (1.9) 28.8 (1.7)*** 28.9 (1.5)* 29.2 (2.5) 29.0 (1.8) 29.3 (1.4)BMI,1981 27.0 (1.8) 29.2 (2.4)*** 26.6 (1.6) 25.8 (3.3) 30.4 (3.5)*** 26.8 (1.6)
about 1985 26.9 (2.3) 29.8 (2.9)*** 28.9 (2.9)** 26.3 (3.5) 30.9 (3.7)*** 29.5 (2.3)**about 1989 26.8 (1.8) 30.2 (3.0)*** 30.2 (2.6)*** 25.7 (2.6) 31.7 (3.7)*** 31.6 (2.2)***
BMI, 1990 26.9 (1.9) 30.1 (2.9)*** 30.5 (2.5)*** 25.2 (2.2) 31.5 (3.7)*** 32.0 (2.4)***
Weight change from 1975 to Ð 81 (kg) 79.7 (3.6) � 1.2 (5.3)*** 7 7.3 (3.2)** 7 9.6 (6.1) �3.4 (7.2)*** 76.8 (2.3)Weight change from 1975 to Ð 90 (kg) 79.9 (4.6) � 3.9 (7.9)*** � 5.1 (4.9)*** 7 11.7 (5.2) �6.2 (9.3)*** 6.7 (4.6)***
Weight in 20s (kg) 76.7 (10.6) 74.7 (9.8) 77.1 (8.1) 67.5 (9.6) 64.9 (11.0) 69.9 (7.0)Weight in 30s (kg) 84.7 (13.6) 83.6 (11.7) 83.4 (9.8) 71.7 (13.4) 75.6 (13.2) 70.2 (8.9)
Partner's weight (kg) 66.6 (9.5) 69.1 (13.8) 66.5 (10.4) 83.8 (21.2) 83.3 (12.5) 87.3 (10.2)
Maximum lifetime weight (kg) 98.1 (12.6) 103.6 (56.7) 100.5 (11.8) 87.7 (15.4) 90.3 (11.4) 86.5 (7.8)
Currently dieting, 1975 (%) 42.1 36.2 46.4 58.8 64.7 61.5Intentional weight loss attempts in
the past (%)76.3 72.0 82.1 100 95.6 92.3
Birth year 1941.1 (6.4) 1940.8 (6.7) 1943.7 (7.1) 1946.2 (8.9) 1945.9 (8.2) 1940.9 (8.4)
Basic education or less (%) 60.5 52.3 46.4 47.1 45.6 73.1
Employed (%)1975 100 96.5 92.9 58.8 57.4 69.21981 97.4 93.9 92.9 64.7 69.1 69.21990 80.0 72.4 74.1 52.9 64.7 53.8
Married or cohabiting (%)1975 65.8 75.7 67.9 35.3 54.4 80.8**1981 71.1 79.6 78.6 58.8 72.1 80.81990 76.3 80.4 89.3 52.9 75.0 73.1
Mann ± Whitney-U or two-way t-test for BMI, weight changes and birth year, Pearson's chi-square test for background variables:*P<0.05; **P<0.01; ***P<0.001 (maintainers compared with overweight subjects and re-gainers).
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
119
International Journal of Obesity

quently a history of higher alcohol intake in the past.In 1981, the maintainers reported more heavy drinking(18% vs 0%, P� 0.025) and lower daily intake ofsalty foods (P� 0.003) than the re-gainers. Both themaintainers and the re-gainers increased their physicalactivity from 1975 to 1981 (P� 0.002 and P� 0.003,respectively). Increased coffee consumption from1975 to 1981 was reported by the maintainers only(P� 0.022), whereas the overweight womendecreased their intake of sugar in coffee and tea(P� 0.004). There were no other differences inhealth-related behaviours between the maintainersand the comparison groups in 1981 or 1990.
Perceived well-being
Gender-speci®c differences were also seen in indicatorsof perceived well-being (Table 4). At baseline themaintainer men more often had a stress-free life thanoverweight men (50% vs 27%, P� 0.005) and lowerscores for stress than the re-gainers in 1981 (6.7 vs 8.6,P� 0.01) and in 1990 (6.2 vs 7.9, P� 0.014). The stressscores did not change among the maintainers duringfollow-up, but stress decreased among the re-gainers(P� 0.044) and he overweight men (P< 0.0001) from1981 to 1990. The maintainers reported less breath-lessness than the overweight men when walking in 1981(0% vs 9.7%, P� 0.044) and climbing uphill (16% vs39%, P� 0.005) in 1981 and in 1990 (21% vs 40%,P� 0.020). In 1990 the re-gainers reported morebreathlessness than the maintainers when walking(25% vs 5.3%, P� 0.021) or climbing uphill (52% vs
21%, P� 0.01). There were no differences in lifesatisfaction scores between the men who maintainedeight loss and the comparison groups.
Again, the pattern was different in women. Atbaseline, the maintainers were more often very dis-satis®ed with their life compared with the overweightwomen (35% vs 13%, P� 0.033), and had highermean scores which indicated a less satisfying lifecompared with the overweight women (P� 0.017) orhe re-gainers (P� 0.048). Loneliness was reported by69% of the maintainers compared to only 22% of there-gainers (P� 0.003) and the overweight women(P< 0.0001). In addition, the maintainers reportedmore breathlessness when climbing uphill than eitherthe overweight women (88% vs 63%, P� 0.044) or there-gainers (88% vs 54%, P� 0.019). Compared to theoverweight women, the maintainers also had morebreathlessness when walking on level ground (35%vs 14%, P� 0.039) and they were less likely to reportthat they usually sleep well (18% vs 46%, P� 0.035).In 1981, there were no longer differences in lifesatisfaction, but the maintainers continued to haveproblems with sleep: only 12% slept well comparedto 50% of the overweight women (P� 0.004) and 46%of the re-gainers (P� 0.019). There were no differ-ences in stress scores between the women who main-tained weight loss and comparison groups.
Among both men and women, there were nodifferences between the maintainers and the compar-ison groups in the history of back, shoulder or neckpain in 1975 or 1981. In addition, there were no
Table 2 Health status and use of medication by weight change category in men and women
Men Women
Maintainers Overweight Re-gainers Maintainers Overweight Re-gainers(n�38) (n�540) (n�28) (n�17) (n�68) (n�26)
Hypertension (%)1975 20.0 18.5 21.4 37.5 20.9 16.01981 28.9 23.6 25.0 23.5 23.9 15.41990 40.5 32.1 17.9* 18.8 29.4 28.0
Diabetes (%)1975 0 0.8 0 0 0 41981 7.9 2.2* 0 11.8 3.0 01990 22.2 7.8** 3.7* 12.5 6.1 0
Myocardial infarction (%)1975 0 0.4 0 6.3 0* 01981 0 0.9 0 5.9 0* 01990 0 5.4 3.7 6.3 1.5 0
Pain killers during previous year (%)1975 54.1 53.2 64.3 70.6 61.8 57.71981 63.9 52.1 65.4 94.1 71.9 68.0*1990 66.7 64.1 75.0 93.3 82.1 84.0
Sleeping pills during previous year (%)1975 2.7 3.2 10.7 5.9 4.4 3.81981 3.1 4.9 12.5 25 1.7* 9.51990 9.1 7.5 25.9 7.1 7.6 13.0
Tranquillizers during previous year (%)1975 5.4 5.1 17.9 5.9 8.8 7.71981 0 6.6 16.0* 0 6.7 9.51990 3.0 9.0 25.9** 13.3 15.2 19.0
Reimbursable medication for a chronic disease (%) 42.1 22.8** 10.7** 35.3 22.1 23.1Receives or has applied for disability pension (%) 7.9 9.6 17.9 11.8 10.3 19.2
Pearson's chi-square test: *P< 0.05; **P< 0.01; ***P< 0.001 (maintainers compared with overweight subjects and re-gainers).
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
120
International Journal of Obesity
differences in the prevalence of insomnia or presenceof children in the household in 1990 (data not shown).
Discussion
This study shows that weight loss of overweightpersons is rarely maintained. Only 5% of the initially
overweight women and 7% of the men succeeded inmaintaining at least 5% weight loss during a 9 yperiod. Our ®ndings con®rm clinical observationsabout the dif®culty of weight maintenance20,33 andextend them to a general population.
In men, weight loss maintenance was associatedwith health-related issues. Both before and afterweight loss the maintainers had a low level of stress
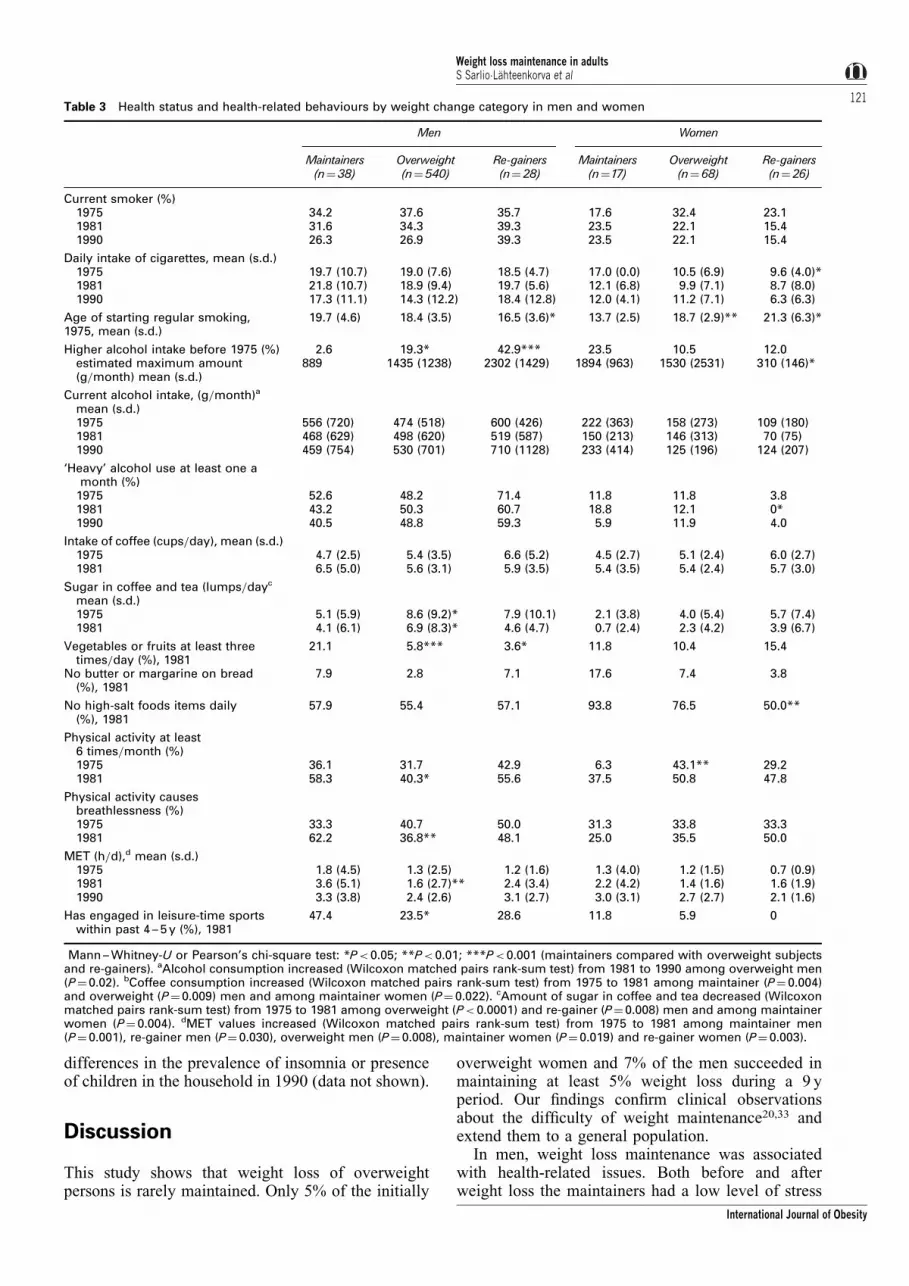
Table 3 Health status and health-related behaviours by weight change category in men and women
Men Women
Maintainers Overweight Re-gainers Maintainers Overweight Re-gainers(n�38) (n�540) (n�28) (n�17) (n�68) (n�26)
Current smoker.(%)1975 34.2 37.6 35.7 17.6 32.4 23.11981 31.6 34.3 39.3 23.5 22.1 15.41990 26.3 26.9 39.3 23.5 22.1 15.4
Daily intake of cigarettes, mean.(s.d.)1975 19.7.(10.7) 19.0.(7.6) 18.5.(4.7) 17.0.(0.0) 10.5.(6.9) 9.6.(4.0)*1981 21.8.(10.7) 18.9.(9.4) 19.7.(5.6) 12.1.(6.8) 9.9.(7.1) 8.7.(8.0)1990 17.3.(11.1) 14.3.(12.2) 18.4.(12.8) 12.0.(4.1) 11.2.(7.1) 6.3.(6.3)
Age of starting regular smoking,1975, mean.(s.d.)
19.7.(4.6) 18.4.(3.5) 16.5.(3.6)* 13.7.(2.5) 18.7.(2.9)** 21.3.(6.3)*
Higher alcohol intake before 1975.(%) 2.6 19.3* 42.9*** 23.5 10.5 12.0estimated maximum amount(g=month) mean.(s.d.)
889 1435.(1238) 2302.(1429) 1894.(963) 1530.(2531) 310.(146)*
Current alcohol intake,.(g=month)a
mean.(s.d.)1975 556.(720) 474.(518) 600.(426) 222.(363) 158.(273) 109.(180)1981 468.(629) 498.(620) 519.(587) 150.(213) 146.(313) 70.(75)1990 459.(754) 530.(701) 710.(1128) 233.(414) 125.(196) 124.(207)
`Heavy' alcohol use at least one amonth.(%)
1975 52.6 48.2 71.4 11.8 11.8 3.81981 43.2 50.3 60.7 18.8 12.1 0.*1990 40.5 48.8 59.3 5.9 11.9 4.0
Intake of coffee.(cups=day), mean.(s.d.)1975 4.7.(2.5) 5.4.(3.5) 6.6.(5.2) 4.5.(2.7) 5.1.(2.4) 6.0.(2.7)1981 6.5.(5.0) 5.6.(3.1) 5.9.(3.5) 5.4.(3.5) 5.4.(2.4) 5.7.(3.0)
Sugar in coffee and tea.(lumps=dayc
mean.(s.d.)1975 5.1.(5.9) 8.6.(9.2)* 7.9.(10.1) 2.1.(3.8) 4.0.(5.4) 5.7.(7.4)1981 4.1.(6.1) 6.9.(8.3)* 4.6.(4.7) 0.7.(2.4) 2.3.(4.2) 3.9.(6.7)
Vegetables or fruits at least threetimes=day.(%), 1981
21.1 5.8*** 3.6* 11.8 10.4 15.4
No butter or margarine on bread(%), 1981
7.9 2.8 7.1 17.6 7.4 3.8
No high-salt foods items daily(%), 1981
57.9 55.4 57.1 93.8 76.5 50.0**
Physical activity at least6 times=month.(%)1975 36.1 31.7 42.9 6.3 43.1** 29.21981 58.3 40.3* 55.6 37.5 50.8 47.8
Physical activity causesbreathlessness.(%)1975 33.3 40.7 50.0 31.3 33.8 33.31981 62.2 36.8** 48.1 25.0 35.5 50.0
MET.(h=d),d mean.(s.d.)1975 1.8.(4.5) 1.3.(2.5) 1.2.(1.6) 1.3.(4.0) 1.2.(1.5) 0.7.(0.9)1981 3.6.(5.1) 1.6.(2.7)** 2.4.(3.4) 2.2.(4.2) 1.4.(1.6) 1.6.(1.9)1990 3.3.(3.8) 2.4.(2.6) 3.1.(2.7) 3.0.(3.1) 2.7.(2.7) 2.1.(1.6)
Has engaged in leisure-time sportswithin past 4 ± 5 y.(%), 1981
47.4 23.5* 28.6 11.8 5.9 0
Mann ± Whitney-U or Pearson's chi-square test: *P<0.05; **P<0.01; ***P<0.001.(maintainers compared with overweight subjectsand re-gainers). aAlcohol consumption increased.(Wilcoxon matched pairs rank-sum test) from 1981 to 1990 among overweight men.(P�0.02). bCoffee consumption increased.(Wilcoxon matched pairs rank-sum test) from 1975 to 1981 among maintainer.(P� 0.004)and overweight.(P�0.009) men and among maintainer women.(P� 0.022). cAmount of sugar in coffee and tea decreased.(Wilcoxonmatched pairs rank-sum test) from 1975 to 1981 among overweight.(P< 0.0001) and re-gainer.(P�0.008) men and among maintainerwomen. (P� 0.004). dMET values increased. (Wilcoxon matched pairs rank-sum test) from 1975 to 1981 among maintainer men.(P�0.001), re-gainer men.(P� 0.030), overweight men.(P�0.008), maintainer women.(P�0.019) and re-gainer women.(P� 0.003).
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
121
International Journal of Obesity

and showed more health-promoting behaviours thanthe comparison groups. Weight loss was greater thanamong the re-gainers, and it was accompanied byseveral health-promoting behaviours, includingincreased physical activity and more vegetables inhe diet. The importance of physical exercise and otherhealth-promoting behaviours for weight maintenancehas also been found in previous studies.2,4 ± 8 Notsurprisingly, men who were successful in weightloss maintenance also reported better physical condi-tion than comparison groups after weight loss.Healthy behaviours among some maintainers couldprobably be explained by chronic diseases. There wasan increased incidence of diabetes and more registeredrights for reimbursed medication for chronic diseases.It is possible that getting diabetes or other chronichealth problems initially triggered weight lossattempts or motivated maintainers to keep weightlevel down. Part of he weight loss may have beenunintentional given the insidious course of diabetes;the disease may have been present years beforediagnosis was made.
The men who regained weight had many health-compromising behaviours prior to weight loss, such asa history of high alcohol intake and long exposure tocigarettes. Despite parallel improvements in thesebehaviours and weight there was no change inhealth status, however. On the contrary, both afterweight loss and regain these men reported use oftranquillizers more often and had higher levels ofstress than the maintainers, suggesting psychologicaldistress and reduced well-being. Both weight gain19
and weight ¯uctuation16 have also been associatedwith stress previously. Stress, alcohol and smokingmay stimulate the hypothalamic ± pituitary ± adrenalaxis, causing endocrine abnormalities that promotevisceral obesity.34
In women, a different picture emerged. When stilloverweight, the maintainers were often living withouta partner, suffered from loneliness and were lesssatis®ed with life than the other women. They alsoseemed to have slightly more medical problems andreported poor physical condition, low level of exer-cise, a long smoking history and poor sleep. Weight
Table 4 Indicators of perceived well-being by weight change category in men and women
Men Women
Maintainers Overweight Re-gainers Maintainers Overweight Re-gainers(n�38) (n�540) (n�28) (n�17) (n�68) (n�26)
Stress of daily activities, mean scores (s.d.)a
1975 6.8 (3.1) 7.7 (2.8) 8.2 (3.3) 7.9 (2.6) 7.4 (2.7) 7.4 (3.0)1981 6.7 (2.5) 7.6 (2.8) 8.6 (3.2)* 7.4 (2.1) 6.7 (2.2) 7.5 (3.5)1990 6.2 (2.2) 6.8 (2.6) 7.9 (3.0)* 6.7 (2.6) 7.2 (2.4) 7.2 (3.3)
No stress at all (%)1975 50.0 27.3** 26.1 17.6 28.8 40.01981 42.9 27.7 20.0 21.4 31.1 37.51990 47.2 38.3 26.9 43.8 24.6 34.8
Life satisfaction, mean scores (s.d.)1975 8.6 (2.5) 8.4 (2.7) 8.8 (3.1) 10.6 (4.0) 8.2 (2.8)* 8.4 (2.3)*1981 8.3 (2.4) 8.6 (2.9) 8.6 (3.4) 9.4 (3.7) 8.3 (2.5) 8.7 (3.2)1990 8.1 (2.5) 8.4 (2.8) 8.7 (3.4) 9.3 (3.7) 8.5 (2.4) 9.4 (3.4)
Very dissatis®ed with life (%)1975 13.2 13.2 21.4 35.3 13.2* 15.41981 13.2 16.1 11.1 23.5 13.2 19.21990 10.8 14.6 21.4 25.0 14.1 23.1
Feels very=fairly lonely (%)1975 17.1 13.9 26.9 68.8 21.9*** 21.7**1981 21.6 17.8 15.4 31.3 16.7 13.61990 17.1 20.4 29.6 26.7 22.2 24.0
Usually sleeps well (%)1975 50.0 48.1 32.1 17.6 45.6** 38.51981 39.5 44.1 42.9 11.8 50.0** 46.2*
Usually has undisturbed sleep (%)1990 86.8 83.6 85.2 64.7 84.8 80.8
Breathlessness while walking on level ground (%)1975 10.5 6.8 21.4 35.3 13.6* 28.01981 0 9.7* 7.1 5.9 20.9 12.01990 5.3 13.6 25.0* 5.9 23.5 26.9
Breathlessness when hurrying, climbing stairs, going uphill, etc. (%)1975 34.2 38.3 53.6 88.2 62.7* 53.8*1981 15.8 38.8** 32.1 52.9 58.2 57.71990 21.1 40.1* 51.9** 37.5 63.2 61.5
Mann ± Whitney-U, two-way t-test or Pearson's chi-square test: *P< 0.05; **P<0.01; ***P< 0.001 (maintainers compared withoverweight subjects and re-gainers). aStress scores decreased (Wilcoxon matched pairs rank-sum test) from 1981 to 1990 amongoverweight (P< 0.0001) and re-gainer men (P� 0.044).
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
122
International Journal of Obesity

loss was accompanied by positive behaviouralchanges such as increased physical activity andfewer cigarettes, and by less loneliness, improvedlife satisfaction and better physical condition. VanGemert et al35 reported that low initial self-esteem isassociated with long-term success among surgicallytreated subjects. The authors suggest that those whosuffer most from obesity are best motivated to loseweight.35 This kind of phenomen could explain ourresults for weight loss maintainers as well. However,the maintainers continued to have problems with sleepand reported more use of sleeping pills, pain killersand `heavy' alcohol intake after weight loss. Thecauses for these problems and potential risk behaviourare open to speculation. They may re¯ect some formof health-related problems that we were unable tocapture with our survey, such as disordered eating,substance abuse or mental problems. Nevertheless, alldifferences between maintainers and comparisongroups had diminished by the last survey, as themaintainer women reached a similar level of well-being as the other overweight women. Compared withwomen who maintained weight loss, those whoregained weight were more often living with a partnerat baseline and enjoyed a somewhat healthier lifestylewith better physical condition and greater life satisfac-tion. It is possible that overweight women withoutserious weight-related problems may be less moti-vated to maintain weight loss.
Gender-speci®c factors behind successful weightloss maintenance may re¯ect different dimensions ofweight-related problems. Women with excess weightare more likely to be stigmatized and disadvantaged inour modern societies,36 whereas men seldom sufferfrom such problems. Previous studies2,21 indicate thatwomen often report emotional or lifestyle triggers as aprecursor of successful weight loss, whereas menreport more medical reasons. It is possible that lowsubjective well-being may have acted as a trigger tosuccess among our women as well. In men weight lossmaintenance seems to be centred in medical problemsand health-oriented behaviour only. However, menand women who succeeded in weight loss mainte-nance seemed to achieve either physical or psycho-social bene®ts after weight loss, whereas theserewards appear to be absent among those who hadnot maintained the weight loss. It seems obvious thatin order to succeed in weight loss maintenance, therehas to be some amelioration in the quality of life.
The presence of health-related problems andadverse habits among those with weight loss raisesquestions about causes and consequences of weightloss in our sample. We excluded subjects with malig-nant cancers and severe disabilities but it is never-theless possible that, whether the intent to lose weightwas reported or not, the weight loss was partly causedby an underlying illness such as poorly controlleddiabetes in diabetic men with weight loss. Similarly,some weight loss may have ensued from adversehabits such as longer history of smoking in maintainer
women. These unfavourable characteristics of sub-jects with weight loss could help to explain theperplexing ®nding that both unintentional and inten-tional weight loss are associated with increased dis-ease prevalence37 and weight loss is associated withincreased mortality.11
Both intentional and unintentional weight loss con-tribute to long-term weight changes. We chose not tocon®ne our analyses to those with reported intentionalweight loss since we wanted to get a comprehensivepicture of those who achieve sustained weight loss ina population, irrespective of intentionality. The ques-tions about intentional weight loss or `dieting' areproblematic for several reasons. First, weight lossattempts reported by a great majority of our studysubjects were not related to weight loss outcome. Forinstance, attempts to lose weight were equally com-monly reported by diabetic persons who maintainedthe weight loss as among the diabetics who did notmaintain it (data now shown). Furthermore, the valid-ity of questions focusing on past dieting attempts isnot established and the interpretation of questionsconcerning dieting may differ according to gender,education and weight status.38 Also, intentional diet-ing has been associated with subsequent weightgain.5,14
The main strength of this study is a unique long-term follow-up of a large unselected populationsample, even if the ®nal analysis involved only asmall number of subjects. We could identify gender-speci®c patterns of behaviour, health and subjectivewell-being that differed between maintainers andcomparison groups. However, because of wide rangeof variables examined, individual ®ndings must beevaluated with caution. Other limitations include useof self-report data, lack of information about weight¯uctuation and many possible causes of weight loss. Itis well known that self-report data underestimate theprevalence of overweight and result in `¯at slopesyndrome' i.e. overweight subjects tend to underreporttheir BMI, whereas thin people do the reverse.39,40
This phenomenon would lead to the underestimationof overweight and reduce the number of subjectschosen for our study, so the effect is likely to beconservative. Self-reported weight history was used asan additional selection criterion for weight maintain-ers, and subjects with obvious weight ¯uctuationcould be excluded. Although this type of categoriza-tion discriminates weight cyclers from weight losersbetter than statistical measures of weight variability,41
it is possible that the data still include maintainerswho had temporarily regained weight. Finally, thecauses of weight loss are not known. However, asour purpose was just to characterize those rare indi-viduals who show sustained weight loss in this pro-spective, population-based sample of overweightadults, further studies are clearly needed to evaluatecausal relationships.
In conclusion, predictors of successful weight lossmaintenance appear to be gender-speci®c. In men,
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
123
International Journal of Obesity
medical problems and in women psycho-social issuesappear to be important for weight loss maintenance.High prevalence of medical problems or health-com-promising behaviour among those who lose weightmay partly explain the increased mortality found insome weight loss studies. More prospective long-termstudies are clearly needed to evaluate determinantsand consequences of sustained weight loss.
Acknowledgement
Supported in part by grants from the Academy ofFinland (nos 42022 and 37800).
References1 Korkeila M, Kaprio J, Rissanen A, Koskenvuo M. Consistency
and change of body mass index and weight. A study on 5967adult Finnish twin pairs. Int J Obes 1995; 19: 310 ± 317.
2 Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. Adescriptive study of individuals successful at long-term main-tenance of substantial weight loss. Am J Clin Nutr 1997; 66:239 ± 246.
3 Coakley EH, Rimm EB, Colditz G, Kawachi I, Willet W.Predictors of weight change in men: Results from the healthprofessionals follow-up study. Int J Obes 1998; 22: 89 ± 96.
4 French SA, Jeffery RW, Forster JL, McGovern PG, Kelder,SH, Baxter JE. Pridictors of weight change over two yearsamong a population of working adults: The Healthy WorkerProject. Int J Obes 1994; 18: 145 ± 154.
5 French SA, Jeffery RW, Folsom AR, McGovern P, William-son DF. Weight loss maintenance in young adulthood: pre-valence and correlations with health behavior and disease in apopulation-based sample of women aged 55 ± 69 years. Int JObes 1996; 20: 303 ± 310.
6 Hunter GR, Weinsier RL, Bamman MM, Larson DE. A role ofhigh intensity exercise on energy balance and weight control.Int J Obes 1998; 22: 489 ± 493.
7 Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO.Psychological symptoms in individuals successful at long-termmaintenance of weight loss. Health Psychol 1998; 17: 336 ±345.
8 Kahn HS, Tatham LM, Rodriguez C, Calle EE, Thun MJ,Heath CW, Jr. Stable behaviors associated with adults' 10-yearchange in body mass index and likelihood of gain at the waist.Am J Public Health 1997; 87: 747 ± 754.
9 Hellerstedt WL, Jeffery RW, Murray DM. The associationbetween alcohol intake and adiposity in the general popula-tion. Am J Epidemiol 1990; 132: 594 ± 611.
10 WHO. Obesity: Preventing and managing the global epi-demic. Report of a WHO consultation on obesity, 3 ± 5 June1997. World Health Organisation: Geneva, 1998.
11 Williamson DF. ``Weight cycling'' and mortality: How do theepidemiologists explain he role of intentional weight loss? JAm Coll Nutr 1996; 15: 6 ± 13.
12 Williamson DF, Pamuk E, Thun M, Flanders D, Byers T,Heath C. Prospective study of intentional weight loss andmortality in overweight white men aged 40 ± 64 years. Am JEpidemiol 1999; 149: 491 ± 503.
13 French SA, Folsom AR, Jeffery RW, Williamson DF. Pro-spective study of intentionality of weight loss and mortality inolder women: The Iowa Women's Health Study. Am J Epi-demiol 1999; 149: 504 ± 514.
14 Korkeila M, Rissanen A, Kaprio J, SoÈrensen TIA, KoskenvuoM. Attempts to lose weight and risk for major weight gain. Aprospective study on adult Finns. Am J Clin Nutr (in press).
15 Tinker JE, Tucker JA. Environmental events surroundingnatural recovery from obesity. Addictive Behav 1997; 22:571 ± 575.
16 Foreyt JP, Brunner RL, Goodrick GK, Cutter G, Brownell KD,St Jeor ST. Psychological correlates of weight ¯uctuation. Int JEating Disord 1995; 17: 263 ± 275.
17 Rumpel C, Ingram DD, Harris TB, Madans J. The associationbetween weight change and psychological well-being inwomen. Int J Obes 1994; 18: 179 ± 183.
18 Greeno CG, Wing RR. Stress-induced eating. Psychol Bull1994; 115: 444 ± 464.
19 Korkeila M, Kaprio J, Rissanen A, Koskenvuo M, SoÈrensenTIA. Predictors of major weight gain in adult Finns: Stress, lifesatisfaction and personality traits. Int J Obes 1998; 22: 949 ±957.
20 Glenny Am, O'Meara S, Melville A, Sheldon TA, Wilson C.The treatment and prevention of obesity: A systematic reviewof the literature. Int J Obes 1997; 21: 715 ± 737.
21 Colvin RH, Olson SB. A descriptive analysis of men andwomen who have lost signi®cant weight and are highlysuccessful at maintaining the loss. Addictive Behav 1983; 8:287 ± 295.
22 Kaprio J. Lessons from twin studies in Finland. Ann Med1994; 26: 135 ± 139.
23 Korkeila M, Kaprio J, Rissanen A, Koskenvuo M. Effects ofgender and age on the heritability of body mass index. Int JObes 1991; 15: 647 ± 654.
24 Kaprio J, Koskenvuo M. A prospective study of psychologicaland socioeconomic characteristics, health behavior and mor-bidity in cigarette smokers prior to quitting compared topersistent smokers and non-smokers. J Clin Epidemiol 1988;41: 139 ± 150.
25 Kaprio J, Koskenvuo M, Langinvainio H, Romanov K, Sarna,Rose RJ. Genetic in¯uences on use and abuse of alcohol: Astudy of 5638 adult Finnish twin brothers. Alcohol Clin ExpRes 1987; 11: 349 ± 356.
26 Kujala UM, Kaprio J, Sarna S, Koskenvuo M. Relationship ofleisure-time physical activity and mortality: The Finnish twincohort. JAMA 1998; 279: 440 ± 444.
27 Allardt E. About dimensions of welfare. An explanatoryanalysis of a comparative Scandinavian survey. Researchgroup for comparative sociology. University of Helsinki,Research Report 1, 1973.
28 Koivumaa-Honkanen, H.-T. Life satisfaction as a health pre-dictor. Doctoral Dissertation, D. Medical Series 143. KuopioUniversity Publications: Kuopio, 1998.
29 RaÈiha I, Kemppainen H, Kaprio J, Koskenvuo M, Sourander.Lifestyle, stress, and genes in peptic ulcer disease: a nation-wide twin cohort study. Arch Intern Med 1998; 158: 698 ±704.
30 Rose GA, Blackburn H, Gillum RF, Prineas RJ. Cardiovascularsurvey methods. World Health Organisation: Geneva, 1982.
31 Partinen M, Putkonen PT, Kaprio J, Koskenvuo M, Hilakivi.Sleep disorders in relation to coronary heart disease. Acta MedScand 1982; 660: 69 ± 83.
32 Hublin C, Kaprio J, Partinen M, HeikkilaÈ K, Koskenvuo M.Daytime sleepiness in an adult, Finnish population. J InternMed 1996; 239: 417 ± 423.
33 Kramer FM, Jeffery RW, Forster JL, Snell MK. Long-termfollow-up of behavioral treatment for obesity: Patterns ofweight regain among men and women. Int J Obes 1989; 13:123 ± 136.
34 BjoÈrntorp P. Endocrine abnormalities of obesity. Metabolism1995; 44: 21 ± 23.
35 Gemert WG van, Svereijns RM, Greve JW, Groenman N,Soeters PB. Psychological functioning of morbidly obesepatients after surgical treatment. Int J Obes 1998; 22: 393 ± 398.
36 Stunkard AJ, SoÈrensen TIA. Obesity and socioeconomicstatus Ð a complex relation. New Engl J Med 1993; 329:1036 ± 1037.
37 French SA, Jeffery RW, Folsom AR, Williamson DF, Byers T.Relation of weight variability and intentionality of weight lossto disease history and health-related variables in a population-based sample of women aged 55 ± 69 years. Am J Epidemiol1995; 142: 1306 ± 1314.
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
124
International Journal of Obesity
38 Neumark-Sztainer D, Jeffery RW, French SA. Self-reporteddieting: How should we ask? What does it mean? Associationsbetween dieting and reported energy intake. Int J EatingDisord 1997; 22: 437 ± 449.
39 Kuskowska-Wolk A, BergstroÈm R, BostroÈm G. Relationshipbetween questionnaire data and medical records of height,weight and body mass index. Int J Obes 1992; 16: 1 ± 9.
40 Jalkanen L, Tuomilehto J, Tanskanen A, Puska P. Accuracy ofself-reported body weight compared to measured body weight.A population survey. Scan J Soc Med 1987; 15: 191 ± 198.
41 French SA, Jeffery RW, Folsom AR, Williamson DF, Byers T.Weight variability in a population-based sample of olderwomen: Reliability and intercorrelation of measures. Int JObes 1995; 19: 22 ± 29.
Weight loss maintenance in adultsS Sarlio-LaÈhteenkorva et al
125
International Journal of Obesity
Related Documents











