World J. Surg. 1,675,681, 1977 O 1977 by the Soci6t~ Internationale de Chirurgi e CASE REPORTS A Case of Fistula of the Colon and Fatal Salmonella Sepsis in Advanced Hodgkin's Lymphoma M. ZER, M.D., U. MINTZ, M.D., D. KAZNELSON, M.D., D.M.D., and M. DINTSMAN, M.D. Department of Surgery A and Department of Oncology, Beilinson Medical Center, Petah Tiqva, and The Sackler School of Medicine, Tel-Aviv University, Tel-Aviv, Israel A case of rapidly progressing Hodgkin's lymphoma is de- scribed in which two uncommon complications were observed. Perforation of the cecum due to lymphomatous invasion oc- curred with subsequent cec0sigmoid fistula and pelvic abscess. Salmonella paratyphi B septicemia, refractory to all treat- ment, caused death of the patient approximately 2 years after initial diagnosis. The relevant literature is reviewed and the possible role of impaired function of immunological mecha- nisms due to both the malignancy and its treatment in ex- posing the patient to "opportunistic" infections is discussed. Although the complications in this patient were treated by further radiation therapy, antibiotics and supportive mea- sures, early surgical intervention is probably the treatment of choice for complications of lymphomatous invasion of the gastrointestinal tract, so as to reduce undue exposure to the dangers of septic complications. A definite relationship between advanced Hodg- kin's lymphoma (HL) and severe, even fatal, re- fections due to a variety of microorganisms has been well established [1-6]. It has been observed that pa- tients with advanced HL are especially susceptible to infection by Salmonella strains, and septicemia caused by Salmonella has been reported in such pa- tients [1, 6]. It has been postulated that these "op- portunistic" infections develop as a result of impaired function of immunological defense mechanisms. The contribution of irradiation and chemotherapy to en- Reprint requests." Professor M. Dintsman. Chief. Depart- ment of Surgery A. Beilinson Hospital. Petah Tiq va. Israel. 675 hancement of susceptibility to infection is con- troversial. Wolf et al. [6] observed that 85.5% of pa- tients with malignant lymphoma !n whom Salmonella sepsis occurred had received irradiation and/or chemotherapy. Others [2, 5] have denied the existence of a causal relationship between susceptibility to in- fection and any therapeutic method employed in ma- lignant lymphoma. The susceptibility to severe in- fections following splenectomy in infancy and child- hood is a well-established phenomenon [7-9]. With this in mind, Nixon and Aisenberg [3] and Ravry et al. [4] suggested that splenectomy performed as a part of the staging procedure in HL might play a ma- jor role in exposing the patient tO '!opportunistic" in- fections. On the other hand, Schimpff et al. [5] con- cluded that splenectomy in itself does not cause an in- crease' either in incidence or in severity of infections in adultsl In add!tion, DiBella et al. [10] reported that splenectomy in patients with HL enhances hemato- logic tolerance to irradiation therapy. Sutherland et a!.[ll] found that variou's means of therapy in HL (splenectomy, irradiation, and chemotherapy) caused a long-term decrease in the number and function of lymphocytes in the periphera ! blood, and impairment of cell-mediated immunity. However, no evidence was found that this had a del~rimental influence on prognosis. In some cases of Salmonella sepsis in patients with HL, the port of entry of the infection is obviously the gastrointestinal tract, but in many cases the origin of the infection cannot be determined [2]. Involvement of the gastrointestinal tract by HL is not uncommon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
World J. Surg. 1 ,675 ,681 , 1977
O �9 1977 by the Soci6t~ Internationale de Chirurgi e
CASE REPORTS
A Case of Fistula of the Colon and Fatal Salmonella Sepsis in Advanced Hodgkin's Lymphoma M. ZER, M.D., U. MINTZ, M.D., D. KAZNELSON, M.D., D.M.D., and M. DINTSMAN, M.D.
Department of Surgery A and Department of Oncology, Beilinson Medical Center, Petah Tiqva, and The Sackler School of Medicine, Tel-Aviv University, Tel-Aviv, Israel
A case of rapidly progressing Hodgkin's lymphoma is de- scribed in which two uncommon complications were observed. Perforation of the cecum due to lymphomatous invasion oc- curred with subsequent cec0sigmoid fistula and pelvic abscess. Salmonella paratyphi B septicemia, refractory to all treat- ment, caused death of the patient approximately 2 years after initial diagnosis. The relevant literature is reviewed and the possible role of impaired function of immunological mecha- nisms due to both the malignancy and its treatment in ex- posing the patient to "opportunistic" infections is discussed. Although the complications in this patient were treated by further radiation therapy, antibiotics and supportive mea- sures, early surgical intervention is probably the treatment of choice for complications of lymphomatous invasion of the gastrointestinal tract, so as to reduce undue exposure to the dangers of septic complications.
A definite relationship between advanced Hodg- kin's lymphoma (HL) and severe, even fatal, re- fections due to a variety of microorganisms has been well established [1-6]. It has been observed that pa- tients with advanced HL are especially susceptible to infection by Salmonella strains, and septicemia caused by Salmonella has been reported in such pa- tients [1, 6]. It has been postulated that these "op- portunistic" infections develop as a result of impaired function of immunological defense mechanisms. The contribution of irradiation and chemotherapy to en-
Reprint requests." Professor M. Dintsman. Chief. Depart- ment of Surgery A. Beilinson Hospital. Petah Tiq va. Israel.
675
hancement of susceptibility to infection is con- troversial. Wolf et al. [6] observed that 85.5% of pa- tients with malignant lymphoma !n whom Salmonella sepsis occurred had received irradiation and/or chemotherapy. Others [2, 5] have denied the existence of a causal relationship between susceptibility to in- fection and any therapeutic method employed in ma- lignant lymphoma. The susceptibility to severe in- fections following splenectomy in infancy and child- hood is a well-established phenomenon [7-9]. With this in mind, Nixon and Aisenberg [3] and Ravry et al. [4] suggested that splenectomy performed as a part of the staging procedure in HL might play a ma- jor role in exposing the patient tO '!opportunistic" in- fections. On the other hand, Schimpff et al. [5] con- cluded that splenectomy in itself does not cause an in- crease' either in incidence or in severity of infections in adultsl In add!tion, DiBella et al. [10] reported that splenectomy in patients with HL enhances hemato- logic tolerance to irradiation therapy. Sutherland et a!.[ll] found that variou's means of therapy in HL (splenectomy, irradiation, and chemotherapy) caused a long-term decrease in the number and function of lymphocytes in the periphera ! blood, and impairment of cell-mediated immunity. However, no evidence was found that this had a del~rimental influence on prognosis.
In some cases of Salmonella sepsis in patients with HL, the port of entry of the infection is obviously the gastrointestinal tract, but in many cases the origin of the infection cannot be determined [2]. Involvement of the gastrointestinal tract by HL is not uncommon

676 World J. Surg. Vol. 1, No. 5, September, 1977
[12], but is usually limited to minor neoplastic infil- tration. Perforation of the gastrointestinal tract due to gross lymphomatous invasion of the intestine in cases of HL is rare.
In this report a case is presented of fulminating, fa- tal Salmonella paratyphi B septicemia in a patient with advanced HL. Lymphomatous infiltration of the cecum caused perforation, pelvic abscess, and fistula to the rectosigmoid.
Case Report
A 39-year-old male was admitted to another hospi- tal in September, 1972 because of a space-occupying lesion in the nasopharynx. The lesion was surgically removed and on histopathological examination a di- agnosis of adenoid tissue was made. The post- operative course was uneventful. Ten months later the patient was readmitted because of a sub- mandibular mass. The mass was excised and the his- tological diagnosis was Hodgkin's lymphoma, mixed cellularity type. Review of the previous specimen r e- sulted in a retrospective diagnosis of HL, lymphocy- tic predominance type. Physical examination and routine laboratory investigations were normal and the patient was referred to the surgical department at Beilinson Medical Center for staging laparotomy. This was performed in August, 1973 and revealed lymphomatous involvement of the mesenteric lymph nodes in the region of the terminal ileum. Histologic typing at this time was that of lymphocytic dePletion type. During this admission, a transient fever up to 38.5~ was noted for the first time. The final diagno- sis following the staging procedure was Hodgkin's lymphoma, lymphocytic depletion type, stage III B, and treatment was administered accordingly by com- bined chemotherapy and irradiation with Co 60. The chemotherapy consisted of repeated courses of MOPP, and the radiation therapy consisted of 2000 rad each to the neck, nasopharynx, and right lower abdomen.
Remission of symptoms occurred promptly and the patient was well until August, 1974, when mild fe- ver reappeared and enlarged lymph nodes became palpable in the left inguinal region. An additional (ninth) course of MOPP was administered and 3000 rad of Co 6~ irradiation was given to the region of the enlarged lymph nodes. However, in October, 1974 all treatment was suspended due to the appearance of herpes zoster infection. Three months later the pa- tient was readmitted to the department because of high fever, abdominal pain, and weight loss. On physical examination the liver was palpable 6 cm be- low the costal margin and a 6 • 6 cm mass was pal- pated in the right lower quadrant of the abdomen. Laboratory investigation yielded normal results ex-
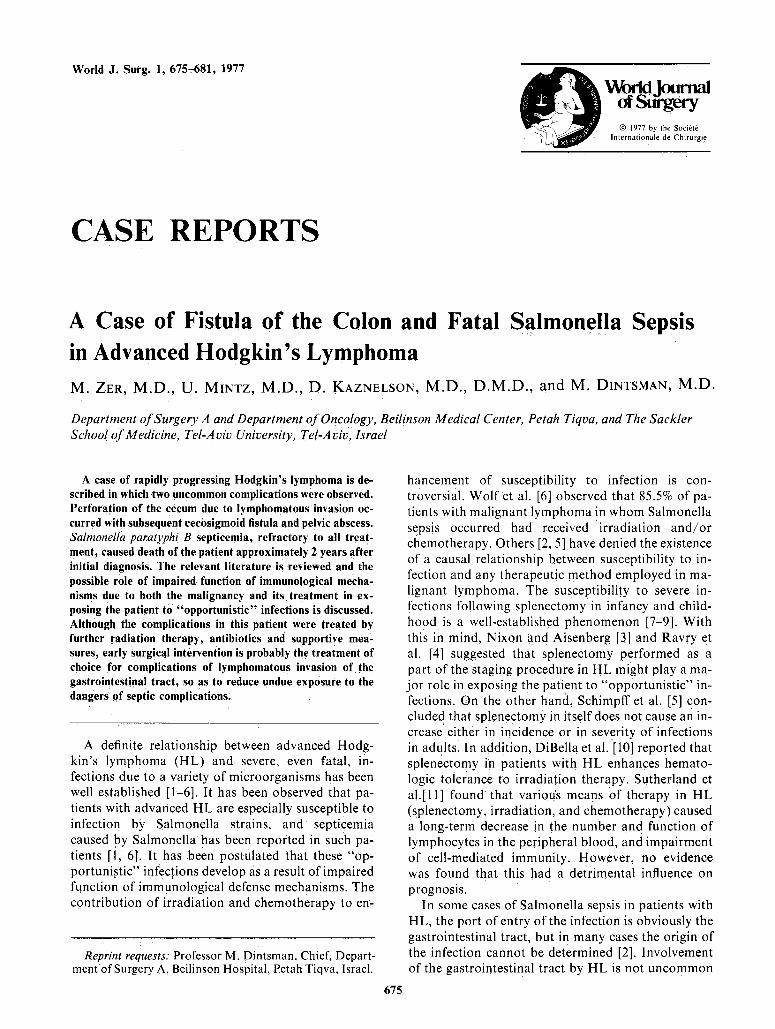
cept for an elevated erythrocyte sedimentation rate of 53/76 mm (Westergren) and an elevation of the leu- kocyte alkaline phosphatase score (300-330 vs. a nor- mal of 30-70). Bacteriological examination of blood, urine, and feces showed no growth. Chest roentgeno- grams, liver scan, and bone marrow biopsy yielded normal findings. However, barium enema x-rays showed compression of the terminal ileum and ce- cum, and a cecosigmoid fistula (Fig. 1). This finding was attributed to neoplastic involvement of the in- testine and additional irradiation (4000 rad of Co 6~ was given to the area, resulting in prompt resolution of the palpable mass. In addition, another course of chemotherapy was given, this time with CCNU.
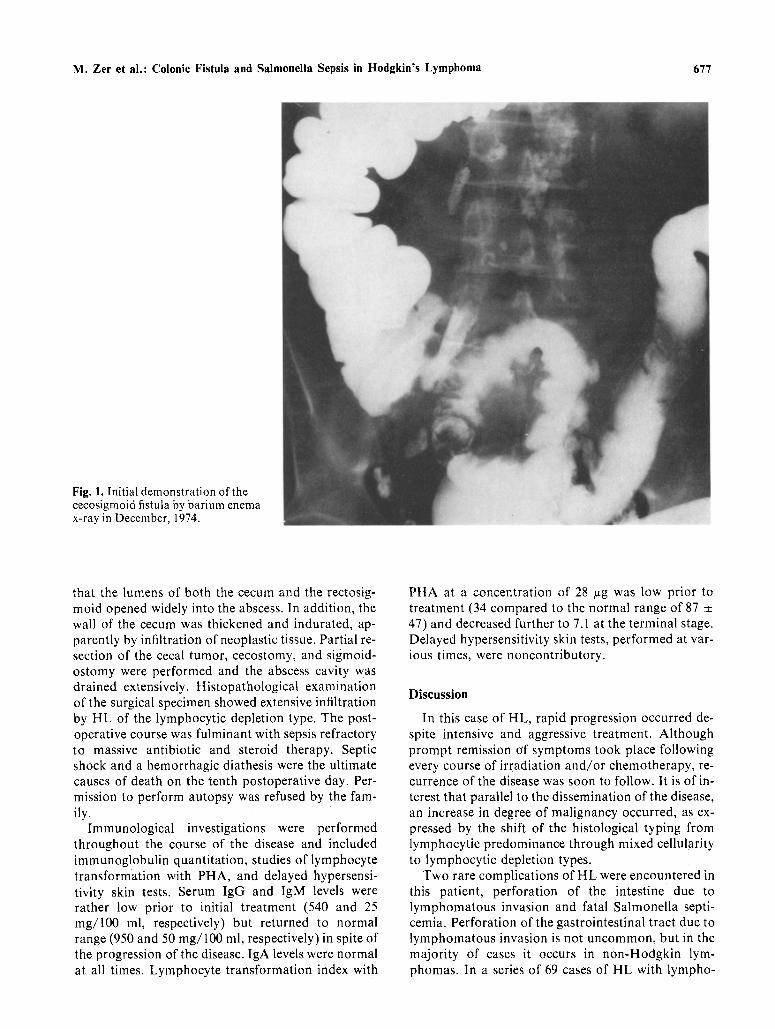
Three months later the patient was readmitted to the hospital because of high fever, severe abdominal pain, and progressive weight loss. The abdominal mass had reappeared and was even larger than at the previous admission. In addition, marked anemia (he- moglobin 8.2 g/100 ml) and leukocytosis (17,100/mm s) were found. Repeated blood cultures were sterile, but Salmonella paratyphi B was found in stool cultures for the first time. Barium enema x-rays demonstrated irregularity of the walls and partial ob- struction of the lumen in the rectosigmoid and en- largement of the existing cecosigmoid fistula (Fig. 2). Intensive antibiotic and supportive therapy resulted in improvement of the patient's general condition and the body temperature returned to normal. An ad- ditional course of irradiation (4000 rad of Co 6~ was given to the left lower quadrant of the abdomen. However, high fever and abdominal pain soon reap- peared and the patient had intermittent diarrhea, from which Salmonella paratyphi B was repeatedly cultured. Notwithstanding in vitro sensitivity of the Salmonella to gentamicin, this antibiotic had no clin- ical effect on the infection.
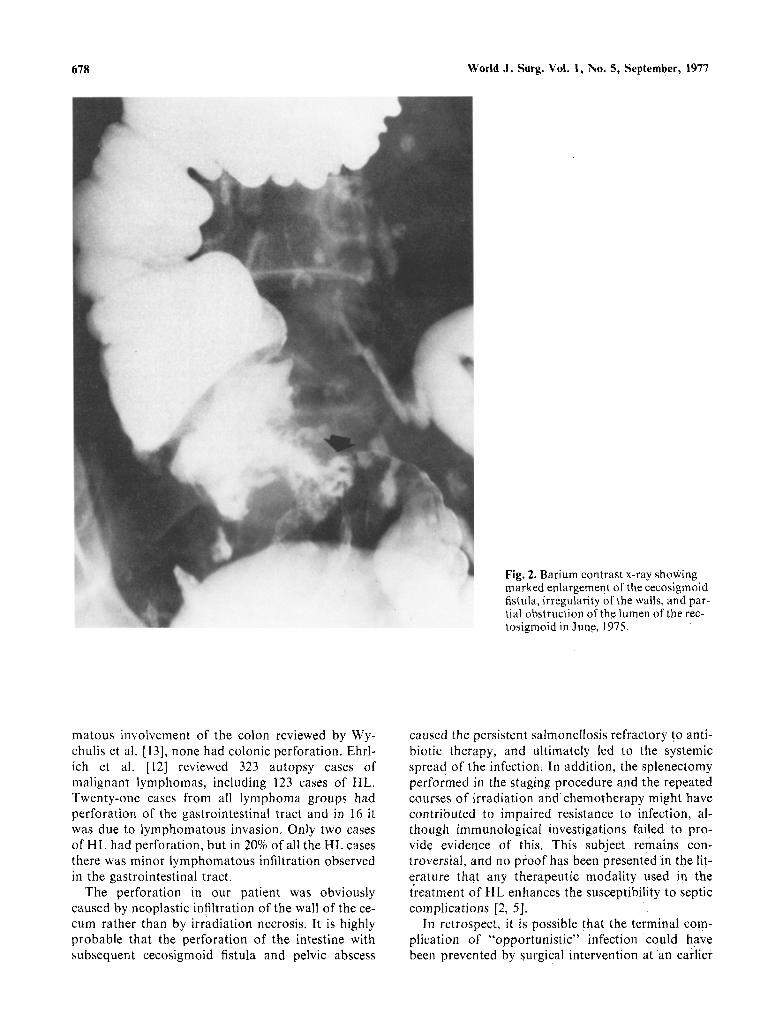
In September, 1975 further deterioration in the pa- tient's condition occurred, with high fever, abdomi- nal pain, and dyspnea. Salmonella paratyphi B septi- cemia was found in addition to the intestinal salmo- nellosis. Severe anemia (hemoglobin of 7.5 g/100 ml) and hypoalbuminemia (1.8 g/100 ml) were present. The WBC ranged from 4,200 to 9,700/mm 8. Barium enema x-rays demonstrated a large pelvic abscess cavity in the area of the previously identified cecosig- moid fistula (Fig. 3). Intensive antibiotic and suppor- tive therapy, including steroids, were administered with only temporary improvement. Two weeks later the patient suddenly developed an acute surgical ab- domen and an emergencY laparotomy was per- formed. At exploration, general peritonitis was found due to rupture of a right pelvic, paracolic, fecal ab- scess that had been walled off by the cecum, rectosig- moid~ and several loops of small intestine. Following evacuation of the abscess Cavity, it became evident
M. Zer et al.: Colonic Fistula and Salmonella Sepsis in Hodgkin's Lymphoma 677
Fig. 1. Initial demonstration of the cecosigmoid fistula by barium enema x-ray in December, 1974.
that the lumens of both the cecum and the rectosig- mold opened widely into the abscess. In addition, the wall of the cecum was thickened and indurated, ap- parently by infiltration of neoplastic tissue. Partial re- section of the cecal tumor, cecostomy, and sigmoid- ostomy were performed and the abscess cavity was drained extensively. Histopathological examination of the surgical specimen showed extensive infiltration by HL of the lymphocytic depletion type. The post- operative course was fulminant with sepsis refractory to massive antibiotic and steroid therapy. Septic shock and a hemorrhagic diathesis were the ultimate causes of death on the tenth postoperative day. Per- mission to perform autopsy was refused by the fam- ily.
Immunological investigations were performed throughout the course of the disease and included immunoglobulin quantitation, studies of lymphocyte transformation with PHA, and delayed hypersensi- tivity skin tests. Serum IgG and IgM levels were rather low prior to initial treatment (540 and 25 rag/100 ml, respectively) but returned to normal range (950 and 50 rag/100 ml, respectively) in spite of the progression of the disease. IgA levels were normal at all times. Lymphocyte transformation index with
PHA at a concentration of 28 ~g was low prior to treatment (34 compared to the normal range of 87 :t: 47) and decreased further to 7.1 at the terminal stage. Delayed hypersensitivity skin tests, performed at var- ious times, were noncontributory.
Discussion
In this case of HL, rapid progression occurred de- spite intensive and aggressive treatment. Although prompt remission of symptoms took place following every course of irradiation and/or chemotherapy, re- currence of the disease was soon to follow. It is of in- terest that parallel to the dissemination of the disease, an increase in degree of malignancy occurred, as ex- pressed by the shift of the histological typing from lymphocytic predominance through mixed cellularity to lymphocytic depletion types.
Two rare complications of HL were encountered in this patient, perforation of the intestine due to lymphomatous invasion and fatal Salmonella septi- cemia. Perforation of the gastrointestinal tract due to lymphomatous invasion is not uncommon, but in the majority of cases it occurs in non-Hodgkin lym- phomas. In a series of 69 cases of HL with lympho-
678 World J. Surg. Vol. 1, No. 5, September, 1977
Fig. 2. Barium contrast x-ray showing marked enlargement of the cecosigmoid fistula, irregularity of the walls, and par- tial obstruction of the lumen of the rec- tosigmoid in June, 1975.
matous involvement of the colon reviewed by Wy- chulis et al. [13], none had colonic perforation. Ehrl- ich et al. [12] reviewed 323 autopsy cases of malignant lymphomas, including 123 cases of HL. Twenty-one cases from all lymphoma groups had perforation of the gastrointestinal tract and in 16 it was due to lymphomatous invasion. Only two cases of i lL had perforation, but in 20% of all the HL cases there was minor lymphomatous infiltration observed in the gastrointestinal tract.
The perforation in our patient was obviously caused by neoplastic infiltration of the wall of the ce- cum rather than by irradiation necrosis. It is highly probable that the perforation of the intestine with subsequent cecosigmoid fistula and pelvic abscess
caused the persistent salmonellosis refractory t ~ anti- biotic therapy, and ultimately led to the systemic spread of the infection. In addition, the splenectomy performed in the staging procedure and the repeated courses of irradiation and chemotherapy might have contributed to impaired resistance to infection, al- though immunological investigations failed to pr o - vide evidence of this. This subject remains con- troversial, and no proof has been presented in the lit- erature that any therapeutic modality used in the treatment of HL enhances the susceptibility to septic complications [2, 5].
In retrospect, it is possible that the terminal com- plication of "opportunistic" infection could have been prevented by surgical intervention at an earlier
M. Zer et ai.: Colonic Fistula and Salmonella Sepsis in Hodgkin's Lymphoma 679
Fig. 3. Barium contrast x-ray showing a large abscess cavity at the site of the cecosigmoid fistula in September, 1975. Partial destruction of the walls of the ce- cum and rectosigmoid is evident.
stage, when the abdominal mass reappeared and be- fore the formation of the pelvic abscess. Should a similar case occur in the future, we will probably op- erate on the patient, rather than pursuing a con- servative course of radiation therapy.
R6sum6
Pr6sentation d'un cas de lymphome type Hodgkin 6volution rapide et avec deux complications in-
habituelles: (1) perforation du caecum par infiltration lymphomateuse, avec fistule caeco-sigmo'fdienne et abc6s pelvien; (2) septic6mie ~ Salmonella para-B r6sistant ~ tout traitement et responsable du d6c6s 2 ans apr6s le diagnostic. La litt6rature est revue: il est possible que la d6pression immunitaire due tant h la
tumeur qu'au traitement favorise les infections "op- portunistes" chez ce type de malades. Dans notre cas, les complications ont ~t6 trait6es par radioth6rapie et antibiotiques. Mais l 'op6ration pr6coce est vraisem- blablement le traitement de choix des complications dues & l'atteinte lymphomateuse du tube digestif: elle r6duira le danger de complications infectieuses.
References
1. Abeloff, M.D., Densen, P., Lenhard, R.E., Jr.: Salmonella empyema and Hodgkin's disease. South. Med. J. 68:363, 1975
2. Casazza, A.A., Duvall, C.P., Carbone, P.P.: Summary of infectious complications in patients with Hodgkin's disease. Cancer Res. 26:1290, 1966
680 World J. Surg. Vol. 1, No. 5, September, 1977
3. Nixon, D.W., Aisenberg, A.C.: Fatal hemophilus in- fluenza sepsis in an asymptomatic splenectomized Hodgkin's disease patienL Ann. Intern. Med. 77:69, 1972
4. Ravry, M., Maldonado, H., Velez-Garcia, E., Mon- talvo, J., Santiago, P.J.: Serious infection after sple- nectomy for the staging of Hodgkin's disease. Ann. In- tern. Med. 77:11, 1972
5. Schimpff, S.C., O'Connell, M.J., Greene, W.H., Wier- nik, P.H.: Infections in 92 splenectomized patients with Hodgkin's disease. Am. J. Med. :59:695, 1975
6. Wolf, M.S., Armstrong, D., Louria, D.B., Blevins~ A.: Salmonellosis in patients with neoplastic disease. Arch. Intern. Med. 128:546, 1971
7. Gofstein, R., Gellis, S.S.: Splenectomy in infancy and childhood. The question of overwhelming infection following operation. J. Dis. Child. 91:566, 1956
8. King, H., Shumaker, H.B.: Splenic studies. I. Suscepti-
bility of infection after splenectomy performed in in- fancy. Ann. Surg. 136:239, 1952
9. Smith, C.H., Erlandson, M., Schulman, I.: Hazard of severe infections in splenectomized infants and chil- dren. Am. J. Med. 22:390, 1957
10. DiBella, N.J., Blom, J., Slawson, R.G.: Splenectomy and hematologic tolerance to irradiation in Hodgkin's disease. Radiology 107:195, 1973
11. Sutherland, R.M., McCredie, J.A., Inch, W.R.: Effect of splenectomy and radiotherapy on lymphocytes in Hodgkin's disease. Clin. Oncol. 1:275, 1975
12. Erhlich, A.N., Stadler, G., Geller, W., Sherlock, P.: Gastrointestinal manifestations of malignant lym- phoma. Gastroenterology 54: I 115, 1968
13. Wychulis, A.R., Beahrs, O.H., Woolner, L.B.: Malig- nant lymphoma of the colon. A study of 69 cases. Arch. Surg. 93:215, 1966
INVITED COMMENTARY
PAUL SHERLOCK, M.D.
Memorial Sloan-Kettering Cancer Center, New York, New York, U.S.A.
Hodgkin's disease rarely arises in the gastrointesti- nal tract as a primary lesion. I n all series reporting primary gastrointestinal malignant lymphoma, Hodg- kin's disease is the least frequent as compared to lymphosarcoma and reticulum Cell sarcoma. How- ever, it is not unusual for Hodgkin's disease to in- volve the gastrointestinal tract as a manifestation of the generalized lymphomatous process. In our series of 123 patients with Hodgkin's disease, 30% had gas- trointestinal involvement at autopsy [1]. Single gas- trointestinal organ involvement was more common than the multiple organ infiltrations that are seen with both lymphosarcoma and reticulum cell sar- coma. All the clinical gastrointestinal manifestations that may be seen with primary Hodgkin's disease may also be seen with disseminated Hodgkin's dis- ease that involves the gastrointestinal tract.
Secondary involvement with tumor may occur in any part of the small intestine but occurs more fre- quently in the ileum, manifesting itself clinically by intussusception, obstruction, perforation, or massive hemorrhage [2, 3]. Colicky abdominal pain, nausea, vomiting, and diarrhea occur. A malabsorption syn- drome has been reported in patients with Hodgkin's disease of the small intestine but the incidence is over- emphasized. Massive lymphatic obstruction by spread of tumor along the mesentery and mesenteric lymphatics or diffuse infiltration of the mucosa and submucosa may be responsible for the malabsorp- tion. Hodgkin's disease may be superimposed on long-standing celiac disease and the symptoms of malabsorption may worsen. When Hodgkin's disease
involves the colon it is almost always localized and may occur at any site in the large bowel. Diffuse polypoid lesions frequently seen with lymphosar- coma do not occur in Hodgkin's disease.
Spontaneous perforation of the bowel wall in pa- tients with lymphoma involving the bowel was con- sidered rare in some of the older series. However, more recent series have reflected a much higher in- cidence of this complication. The use of radiotherapy and cytotoxic agents in the treatment of malignant lymphomas possibly increases the risk of perforation because of the marked sensitivity of these tumors to these agents. Very rapid dissolution of tumor without allowing time for regeneration of normal epithelium to cover the defect caused by radio- or chemonecrosis could result in perforation. In 1962 we reported on a patient with widespread reticulum cell sarcoma who developed multiple perforations of the small bowel following mechlorethamine hydrochloride (nitrogen mustard) therapy [4].
Non-tumorous lesions of the gastrointestinal tract in patients with Hodgkin's disease are significant since symptoms and signs attributed to tumor may instead be caused by gastric erosions, secondary fungal or bacterial infection, or by the effects of radi- ation and drugs. In our series of 123 cases of Hodg- kin's disease, a total of 48% had gastrointestinal pa- thology: 20% with tumor alone; 18% with non-tumor pathology alone; 10% with both tumor and non-tu- mor pathology present [1].
Fungal and bacterial complications occur fre- quently in patients with Hodgkin's disease and other lymphomas. In an autopsy series 11% of patients with Hodgkin's disease and 13% of patients with lym- phoma had histologically proven Candida (Monilia) infection of the gastrointestinal tract [5]. Candida in- fection was most common in the esophagus but in- volved all areas of the gastrointestinal tract. The most common lesions were esophagitis, with or without
Related Documents











