A 29 A 29 - - YEAR OLD WOMAN WITH YEAR OLD WOMAN WITH BILATERAL VISUAL LOSS, BILATERAL VISUAL LOSS, AMENORRHEA AND AMENORRHEA AND HYPERPROLACTINEMIA HYPERPROLACTINEMIA University of Florida College of Medicine and Florida State College of Medicine M. Tariq Bhatti, MD Anthony Yachnis, MD Steven Roper, MD Charles G. Maitland, MD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
A 29A 29--YEAR OLD WOMAN WITH YEAR OLD WOMAN WITH BILATERAL VISUAL LOSS, BILATERAL VISUAL LOSS,
AMENORRHEA AND AMENORRHEA AND HYPERPROLACTINEMIAHYPERPROLACTINEMIA
University of Florida College of Medicineand
Florida State College of Medicine
M. Tariq Bhatti, MDAnthony Yachnis, MD
Steven Roper, MDCharles G. Maitland, MD
HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
• Oct 2004: Transient visual loss OU – lasting 2-3 seconds followed by 5 seconds of whitening vision and blurred vision OD
• Over next few months noticed a progressive decline in vision OD
• Jan 2005: Saw a local ophthalmologist- remembers being told that “something was pale”. Brain MRI normal.
• April 2005: Transient visual loss OU – lasting 2-3 seconds, followed by several seconds of “whitening” and “fuzzy vision”. Eye pain OD for 5 minutes
• April 2005: Saw a local ophthalmologist Hand motions OD and 20/70 OS Bilateral optic nerve atrophy
29-year-old AAF referred for progressive vision loss OD>OS
HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
MRI: 1. Pituitary adenoma2. Enhancement of intracranial portions of the optic nerves, optic chiasm and optic tracts
May 2005: Evaluated by Neuro-ophthalmologist: Hand motions OD and 20/50 OS Right RAPDOptic atrophy OD>OS
Admitted to hospital
HOSPTIAL WORKHOSPTIAL WORK--UPUP
•LP: opening pressure 25 cm H2O, no chemistries performed •CBC: Hg 11.8 d/l•Electrolytes: normal•ACE: 58 U/L (9-67 U/L)•CT Chest: normal•ESR: 41 mm/hr•TSH: 2.420 UIU/mL•FSH: 2.8 MIU/mL•LH: <0.1 MIU/mL•Growth hormone: 0.2 ng/mL (<10 ng/mL)•Serum electrophoresis: 0.19 g/dl decreased alpha-1 fraction •Prolactin: 83.1 ng/mL (normal [non-pregnant woman] 3-30 ng/mL)
HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
4 days of IV Solumedrol followed by oral prednisone taper4 days of IV Solumedrol followed by oral prednisone taper
June 2005: followJune 2005: follow--up visit after hospitalizationup visit after hospitalizationHand motion OD and 20/50 OSHand motion OD and 20/50 OS
Referred for consideration of chiasmal biopsyReferred for consideration of chiasmal biopsy
Three pregnancies resulting in nonviable fetusesThree pregnancies resulting in nonviable fetusesHeart murmur since birthHeart murmur since birthNo previous ocular historyNo previous ocular history
Past neurological history: migrainesPast neurological history: migrainesPast surgical history: One D&C, 3 years agoPast surgical history: One D&C, 3 years ago
Current medications: Current medications: Prednisone 80 mg Prednisone 80 mg qdqdAciphexAciphexTylenolTylenol
PAST MEDICAL HISTORYPAST MEDICAL HISTORY
Family history: mother with Family history: mother with sarcoidosissarcoidosis
Social history: no smoking or drinkingSocial history: no smoking or drinking
Review of systems: Review of systems: No fever, chills or weight lossNo fever, chills or weight loss
10% hearing loss in the left ear, constant headache and 10% hearing loss in the left ear, constant headache and excessive thirst excessive thirst
Amenorrhea for 23 months, decreased libido, no abnormal Amenorrhea for 23 months, decreased libido, no abnormal lactation (evaluated by endocrinologist)lactation (evaluated by endocrinologist)
PAST MEDICAL HISTORYPAST MEDICAL HISTORY
PATIENT PRESENTATION: EXAMPATIENT PRESENTATION: EXAM
Visual acuity: counting fingers OD and 20/100 OSVisual acuity: counting fingers OD and 20/100 OS
Color vision: no control plate OUColor vision: no control plate OU
Pupils: Equal, sluggish OU, subtle R RAPDPupils: Equal, sluggish OU, subtle R RAPD
Eye movements: full OUEye movements: full OU
Slit lamp examination: normal OUSlit lamp examination: normal OU
IOP: 14 OD, 15 OSIOP: 14 OD, 15 OS
Cranial nerves: normalCranial nerves: normal
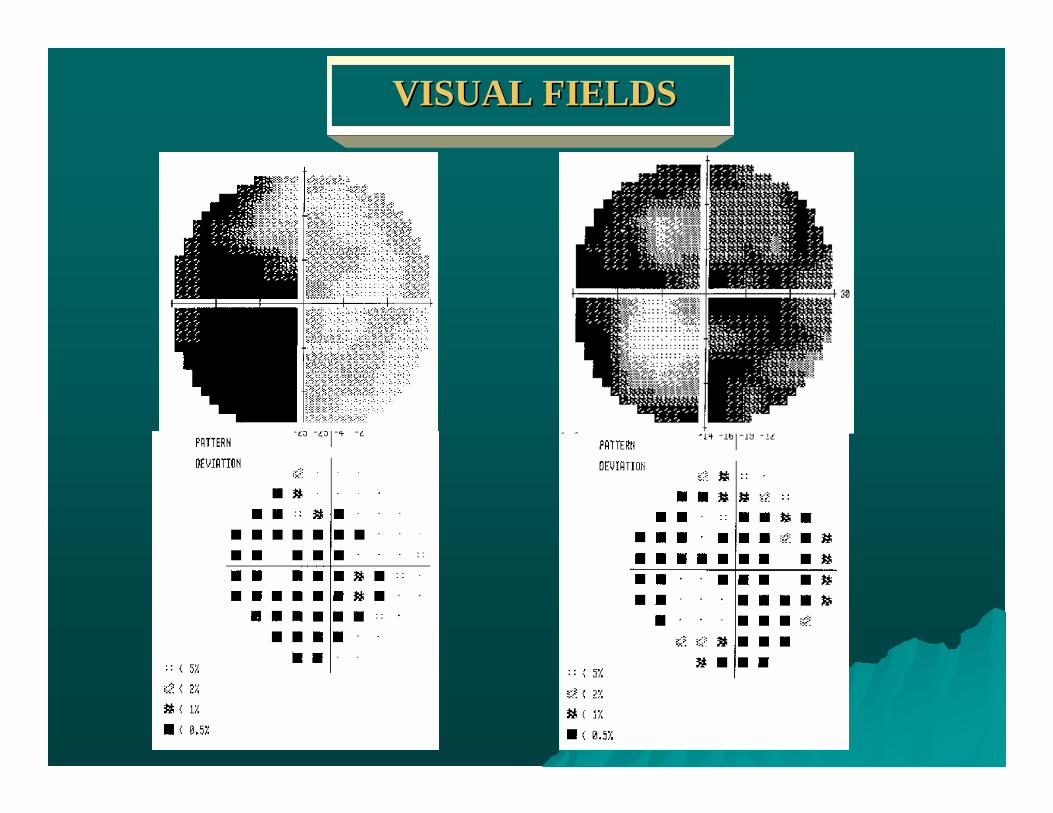
VISUAL FIELDSVISUAL FIELDS
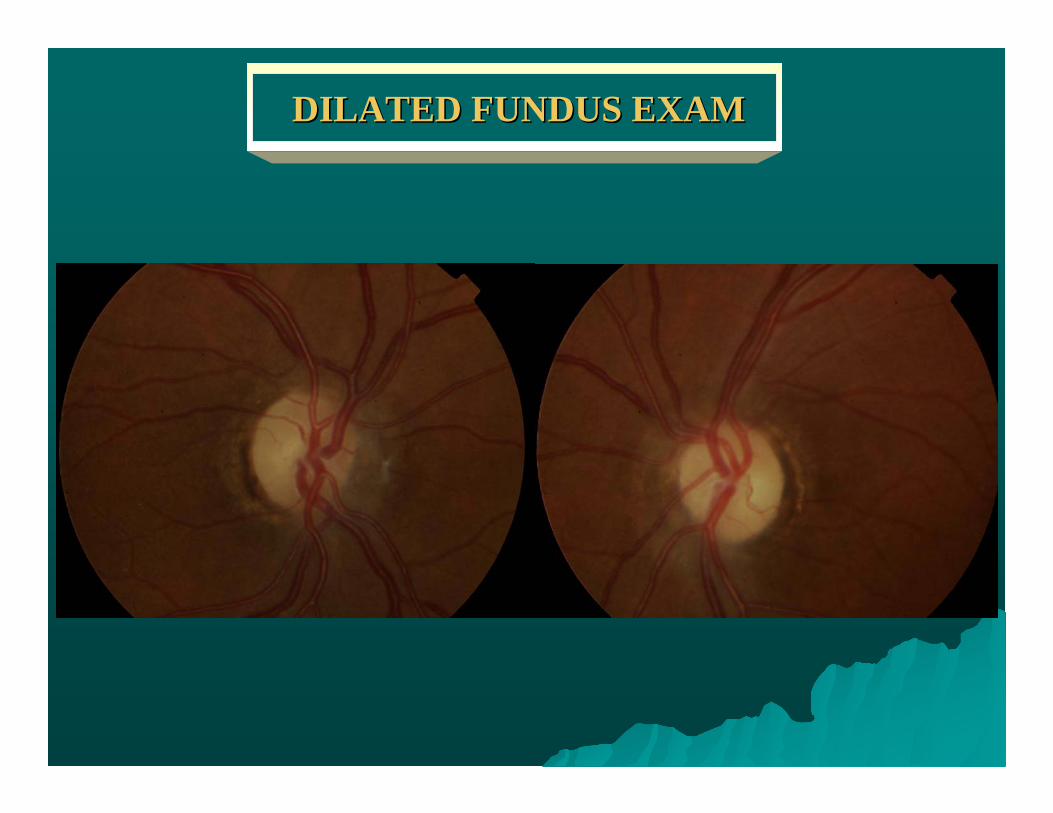
DILATED FUNDUS EXAMDILATED FUNDUS EXAM
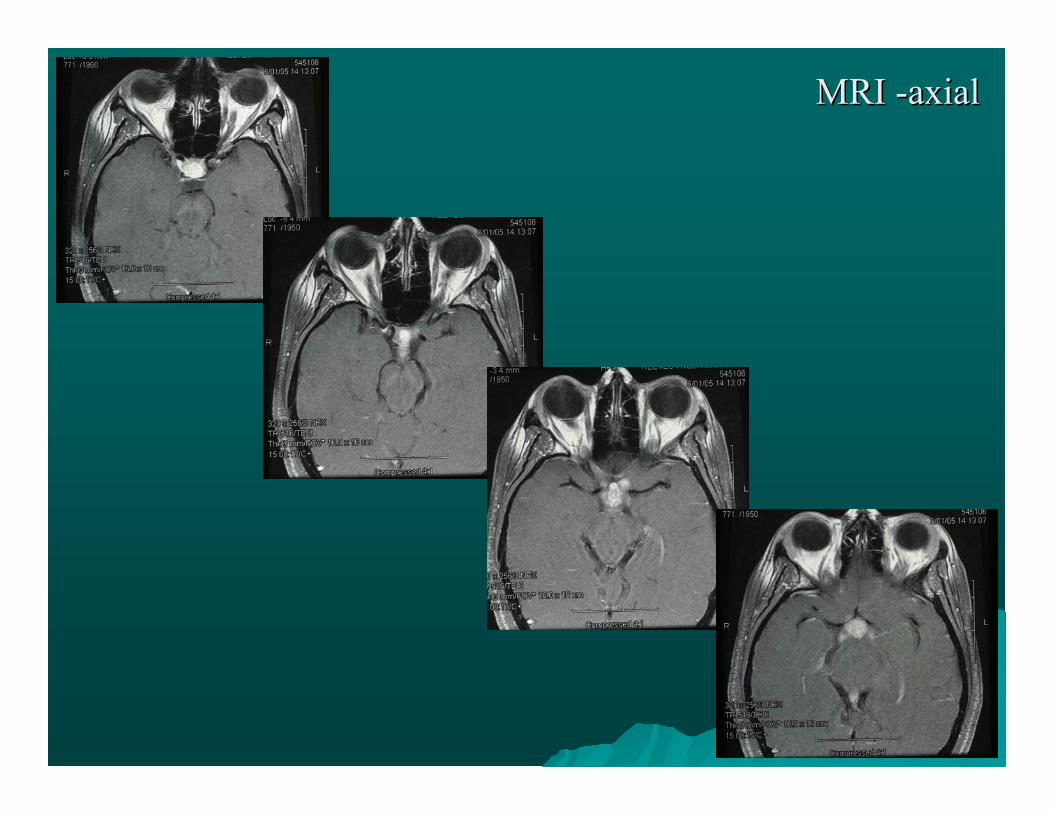
MRI MRI --axialaxial
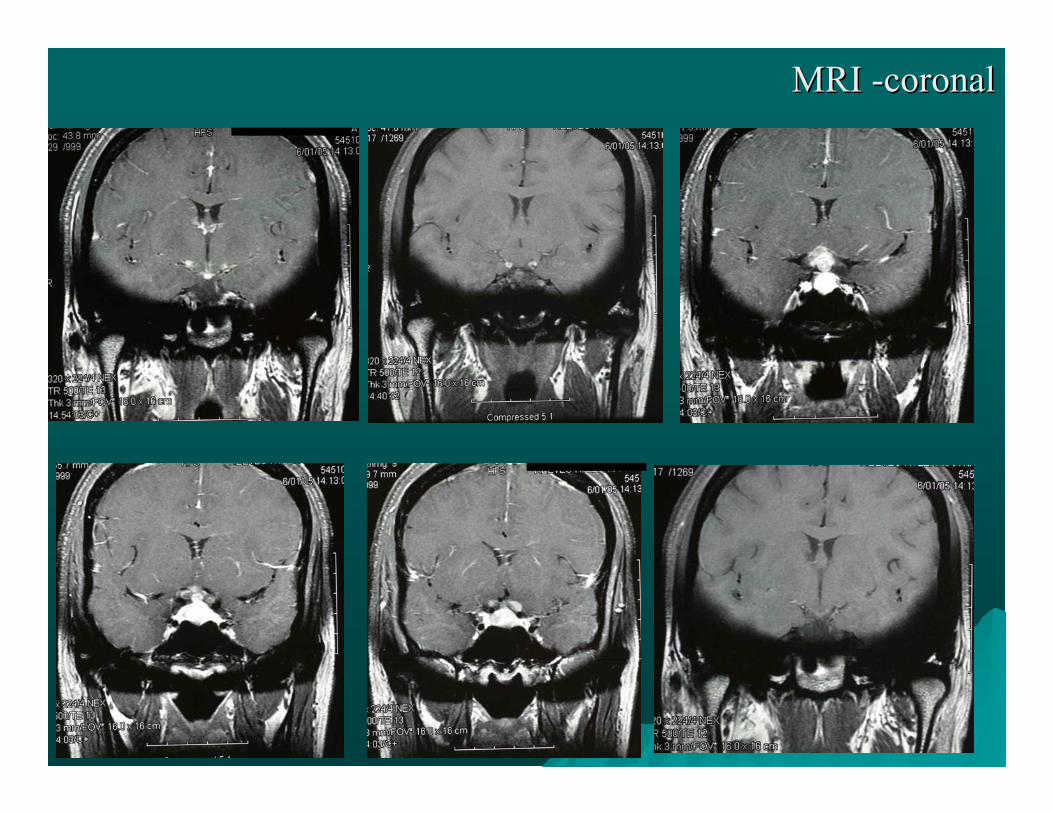
MRI MRI --coronalcoronal
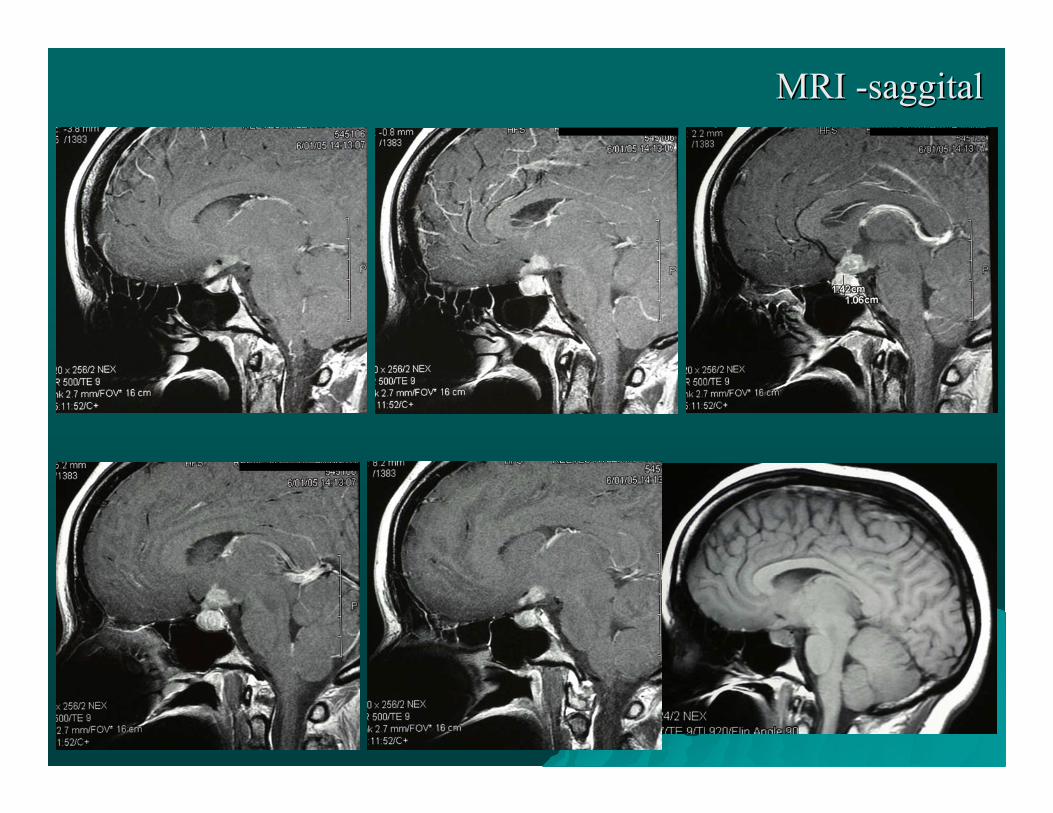
MRI MRI --saggitalsaggital
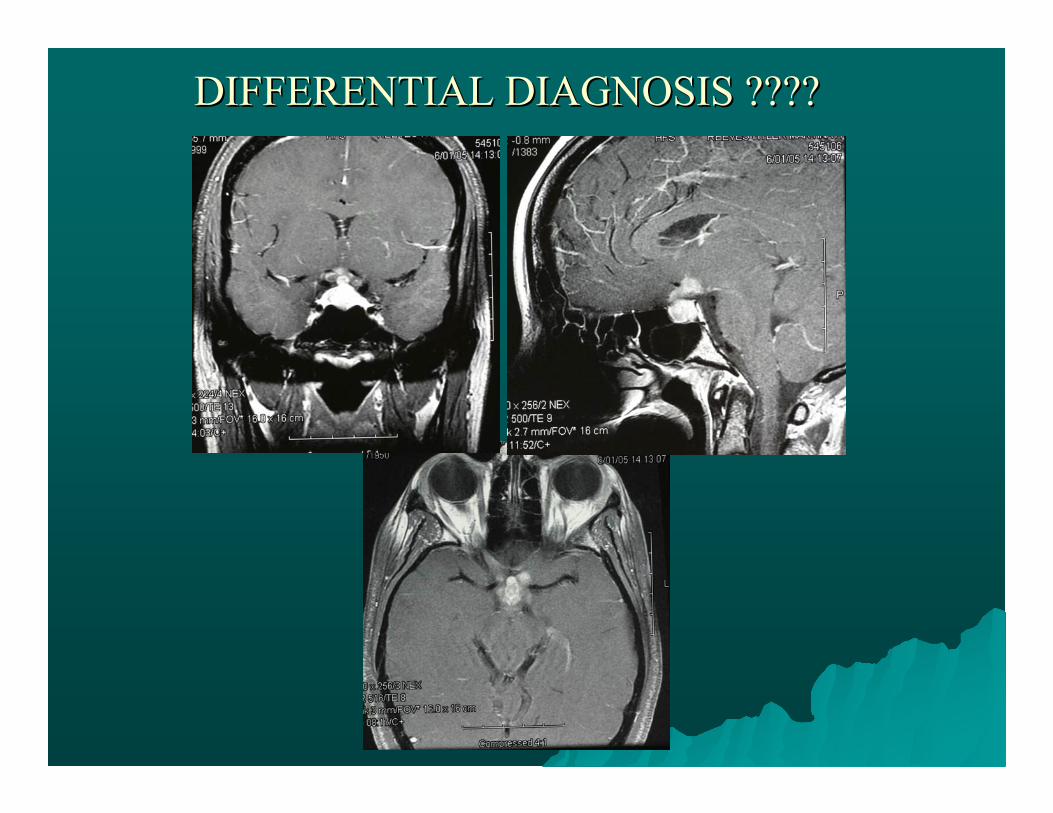
DIFFERENTIAL DIAGNOSIS ????DIFFERENTIAL DIAGNOSIS ????
Differential Diagnosis: Suprasellar Mass Differential Diagnosis: Suprasellar Mass ((SATCHMOE)
•Sarcoidosis
•Aneurysm/Adenoma
•Teratoma
•Craniopharyngioma
•Hypothalamic glioma/Histiocytosis
•Meningioma/Metastasis
•Optic nerve glioma
•Epidermoid/Dermoid inclusion cyst

RECOMMENDATIONS ??RECOMMENDATIONS ??1 2
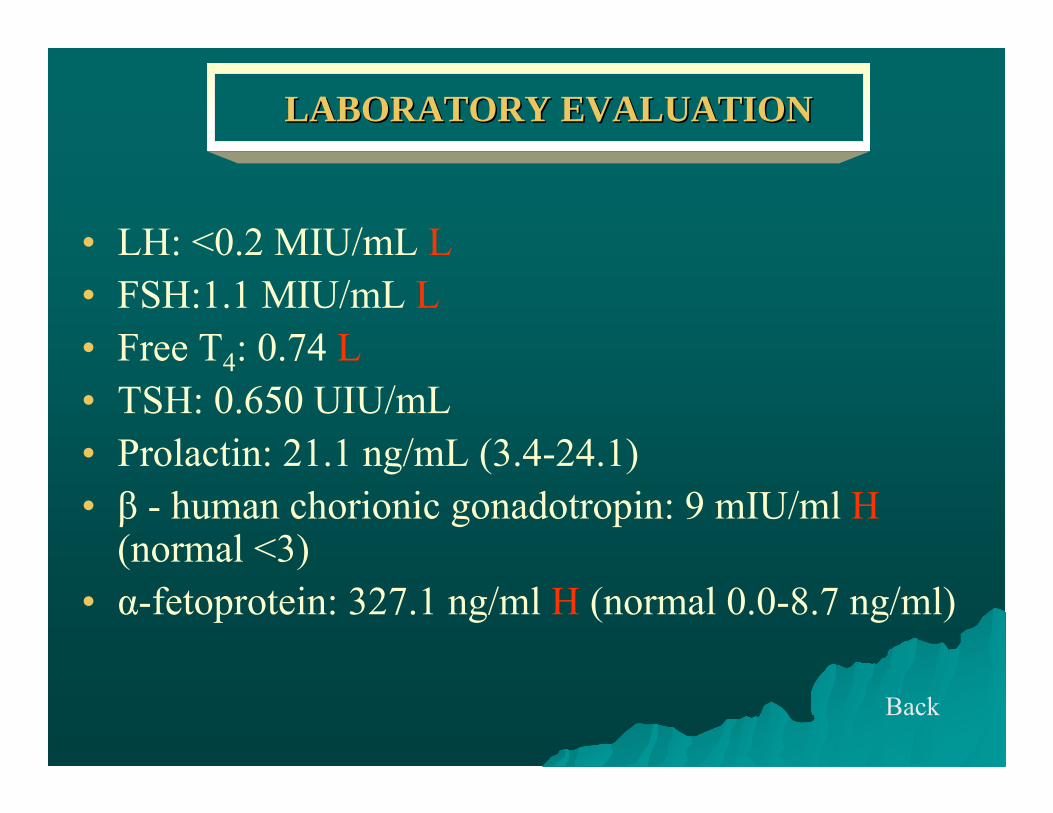
LABORATORY EVALUATIONLABORATORY EVALUATION
• LH: <0.2 MIU/mL L• FSH:1.1 MIU/mL L • Free T4: 0.74 L• TSH: 0.650 UIU/mL• Prolactin: 21.1 ng/mL (3.4-24.1)• β - human chorionic gonadotropin: 9 mIU/ml H
(normal <3)• α-fetoprotein: 327.1 ng/ml H (normal 0.0-8.7 ng/ml)
Back
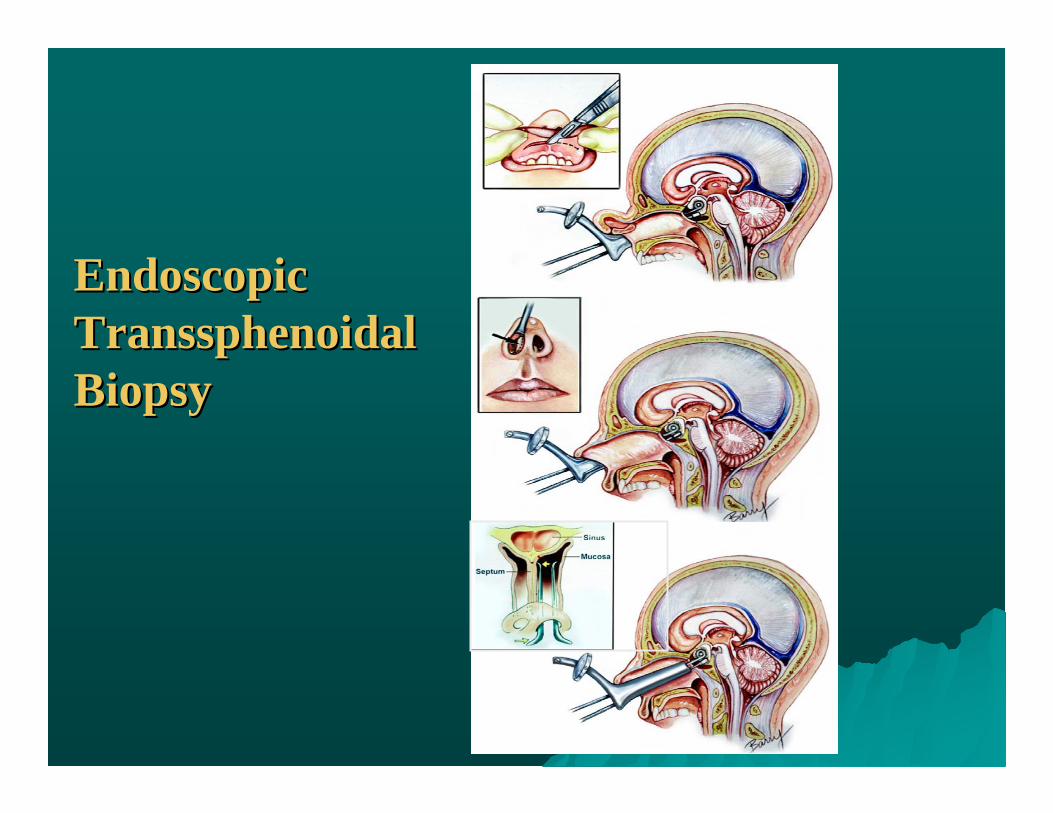
Endoscopic Endoscopic TranssphenoidalTranssphenoidalBiopsyBiopsy
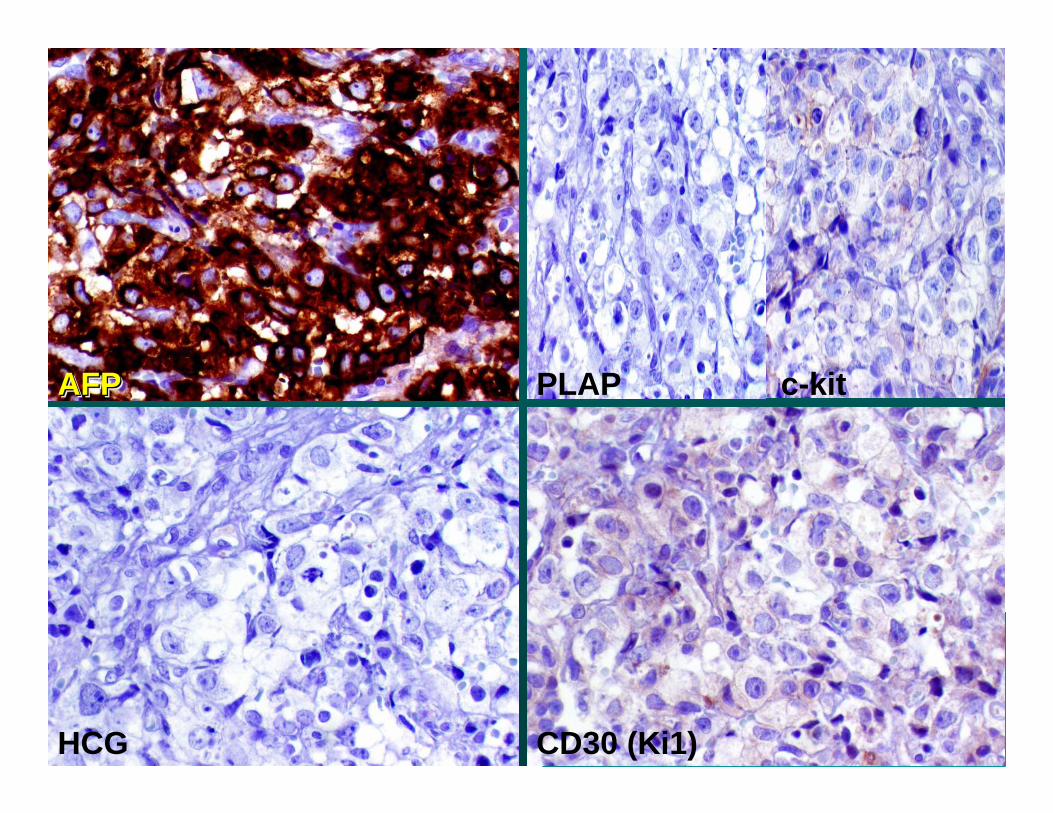
AFPAFPAFP PLAP c-kit
HCG CD30 (Ki1)
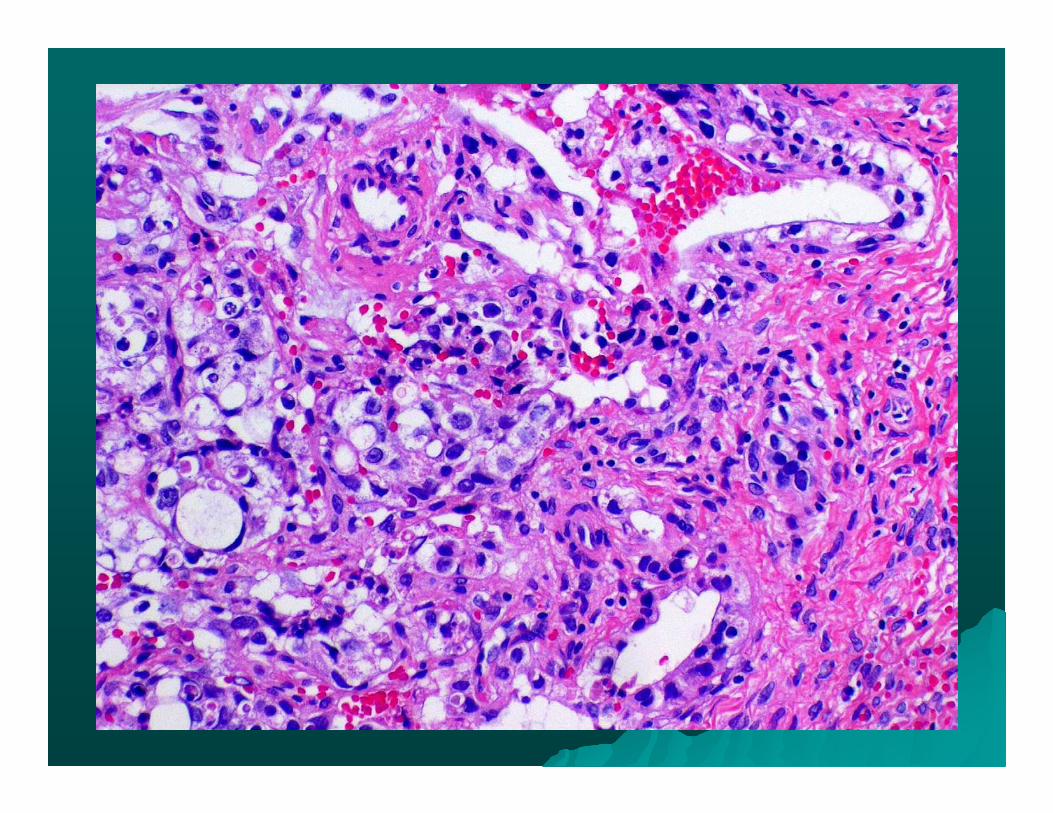
Diagnosis:Diagnosis:
YOLK SAC TUMOR (Endodermal Sinus Tumor)
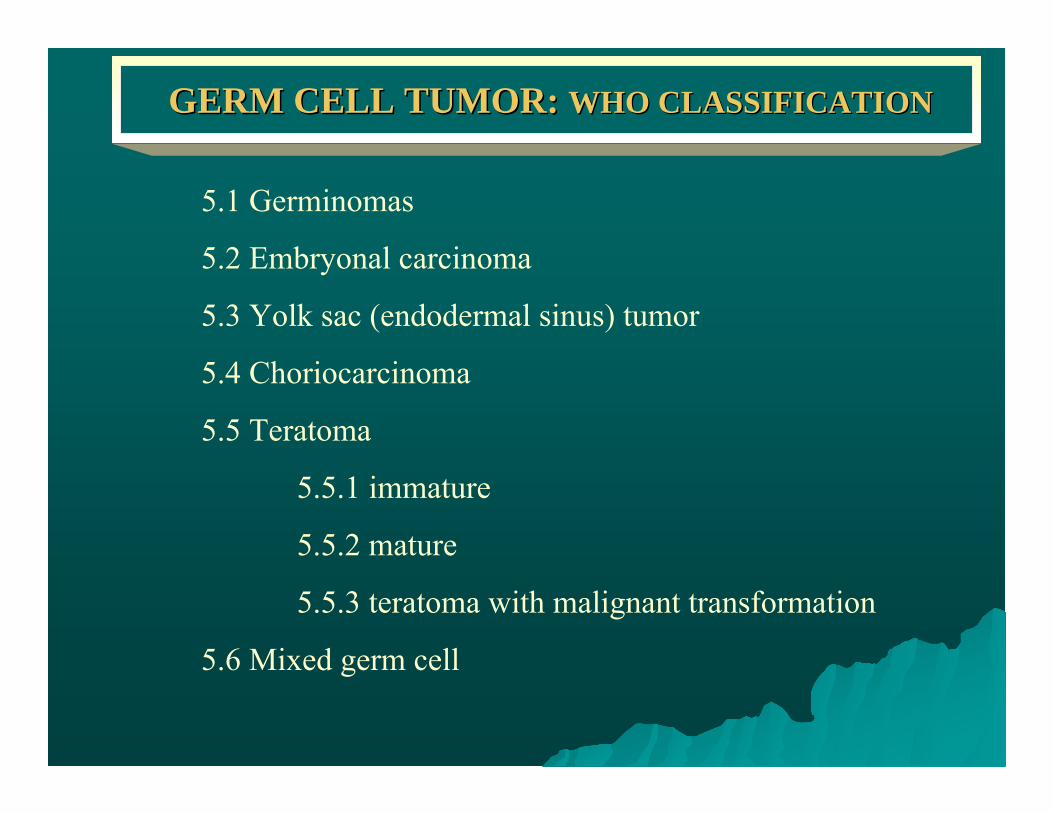
GERM CELL TUMOR: GERM CELL TUMOR: WHO CLASSIFICATIONWHO CLASSIFICATION
5.1 Germinomas
5.2 Embryonal carcinoma
5.3 Yolk sac (endodermal sinus) tumor
5.4 Choriocarcinoma
5.5 Teratoma
5.5.1 immature
5.5.2 mature
5.5.3 teratoma with malignant transformation
5.6 Mixed germ cell
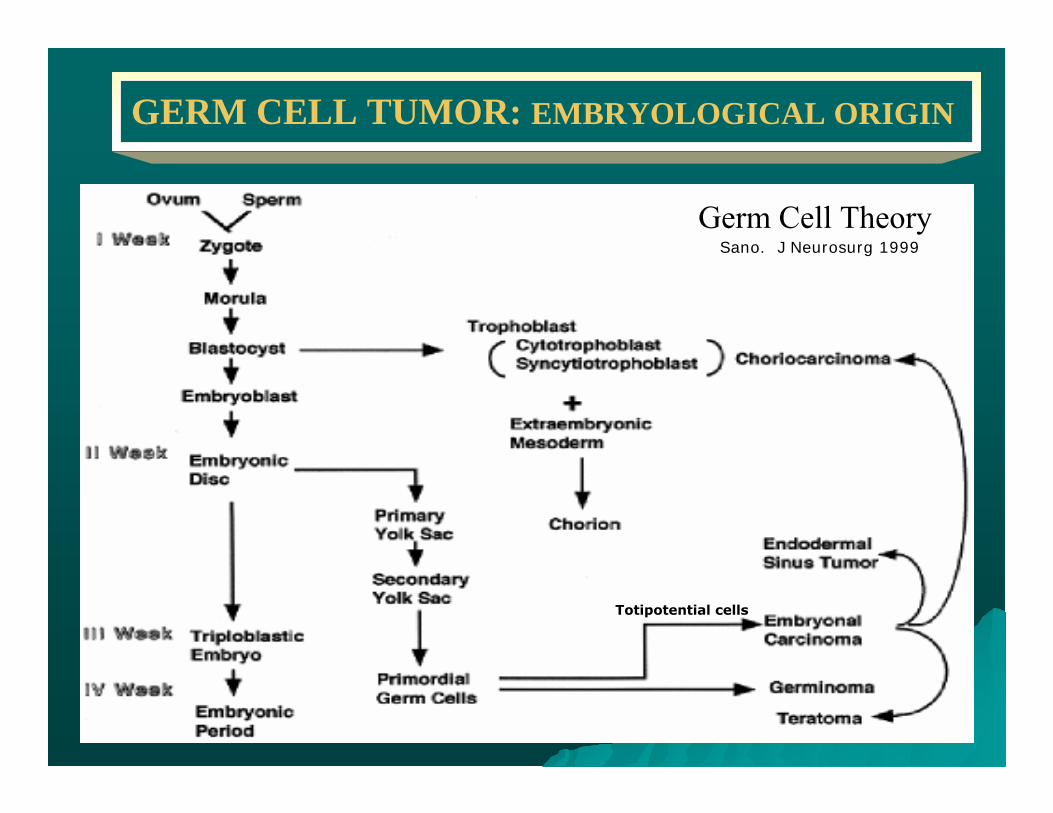
Germ Cell Theory
Totipotential cells
Sano. J Neurosurg 1999
GERM CELL TUMOR: EMBRYOLOGICAL ORIGIN
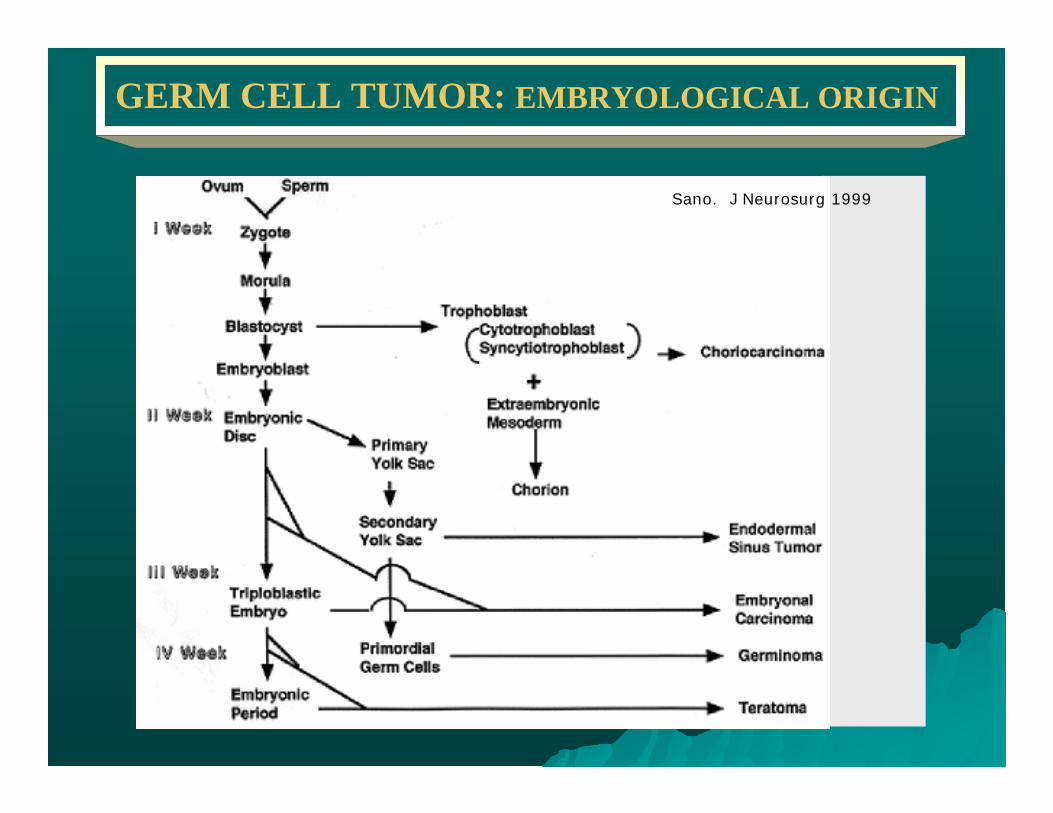
GERM CELL TUMOR: EMBRYOLOGICAL ORIGIN
Sano. J Neurosurg 1999
Intracranial Germ Cell Tumors (ICGCT): Intracranial Germ Cell Tumors (ICGCT): EPIDEMIOLOGYEPIDEMIOLOGY
• 95% of GCT occur in the gonads and 5% in extragonadal sites
• Age: 10-21 years old (70%)
• Caucasians:African Americans- ~5:1
• Male: Female- 2.24:1
• Western countries: 0.3-3.4% of primary intracranial tumors Japan: 2.1-12.7% of primary intracranial tumors
• Intracranial location (midline): pineal gland, sellar and suprasellar region, basal ganglia, and posterior fossa
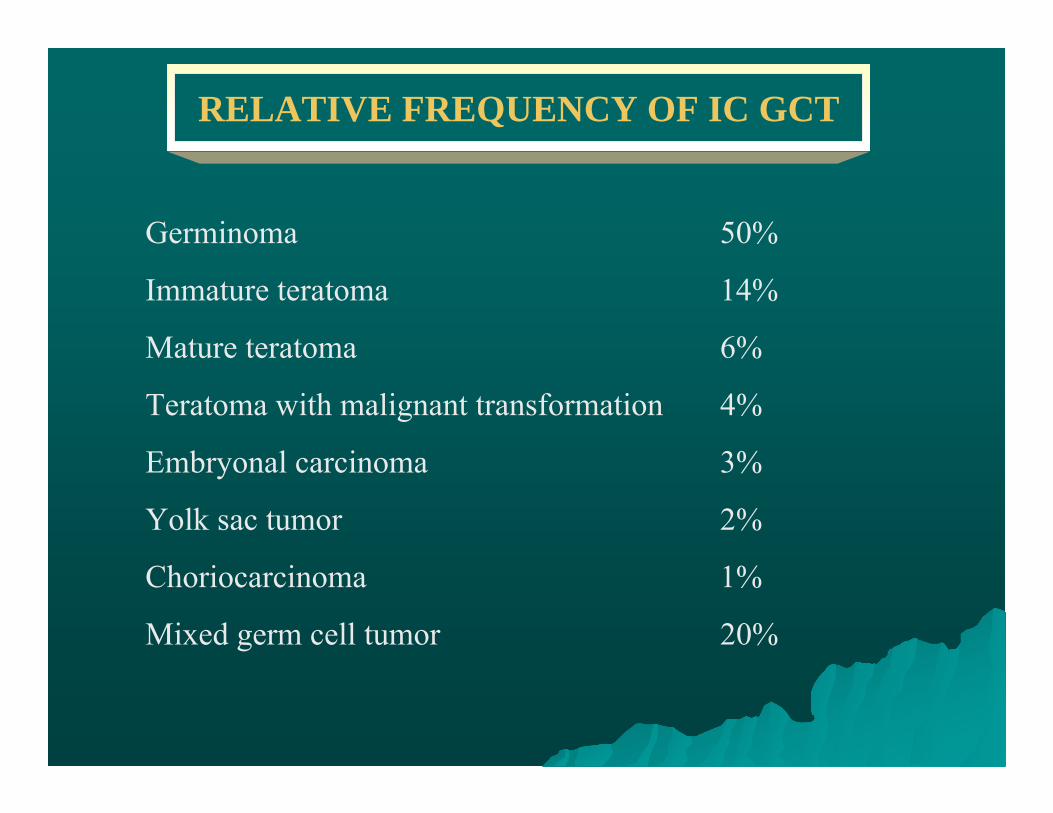
RELATIVE FREQUENCY OF IC GCT
Germinoma 50%
Immature teratoma 14%
Mature teratoma 6%
Teratoma with malignant transformation 4%
Embryonal carcinoma 3%
Yolk sac tumor 2%
Choriocarcinoma 1%
Mixed germ cell tumor 20%
IC GCT: SIGNS & SYMPTOMS
Suprasellar GCTSuprasellar GCT
•• Decreased visual acuityDecreased visual acuity•• Visual field defectsVisual field defects•• DiplopiaDiplopia•• ACTH deficiencyACTH deficiency•• Central hypothyroidismCentral hypothyroidism•• GH deficiencyGH deficiency•• Precocious Precocious pseudopubertypseudopuberty•• HypogonadismHypogonadism•• Excessive thirstExcessive thirst•• ObesityObesity•• PsychosisPsychosis•• ObsessiveObsessive--compulsive symptomscompulsive symptoms
Pineal GCTPineal GCT
•• PapilledemaPapilledema•• ParinaudParinaud’’ss syndromesyndrome•• HeadacheHeadache•• NauseaNausea•• VomitingVomiting•• Gait abnormalitiesGait abnormalities•• Deterioration of intellectual Deterioration of intellectual
functionsfunctions•• SphinctericSphincteric incontinenceincontinence
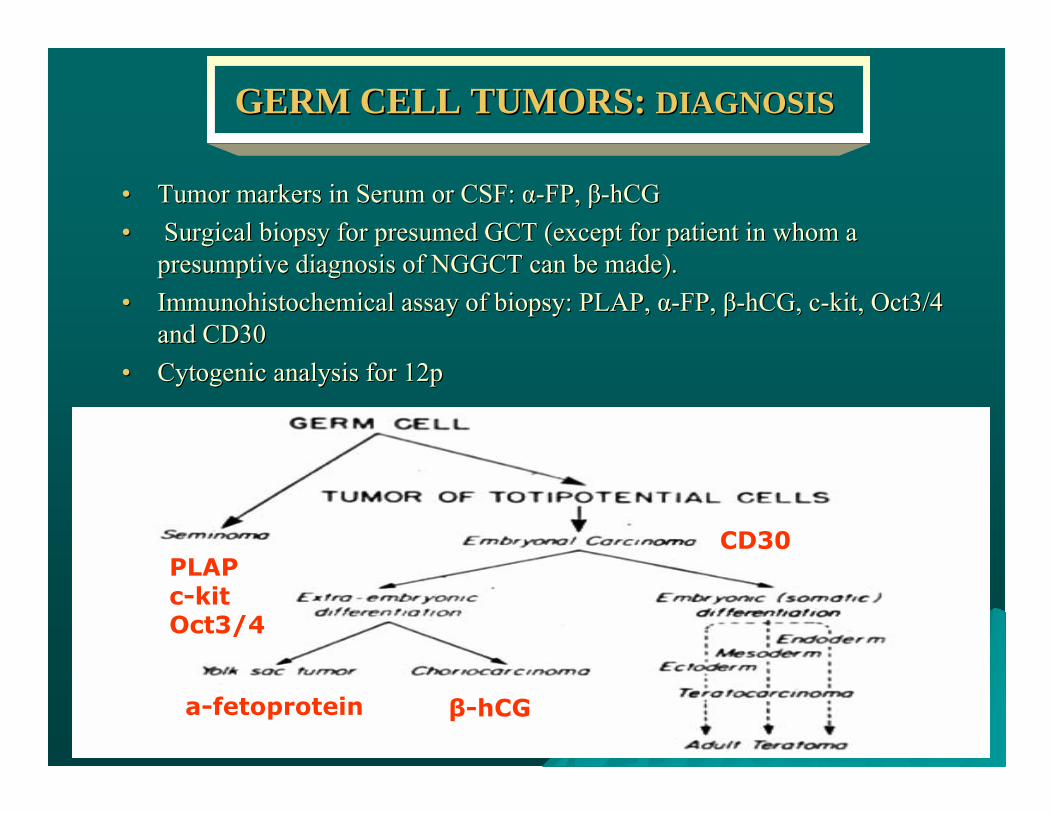
GERM CELL TUMORS: GERM CELL TUMORS: DIAGNOSISDIAGNOSIS
•• Tumor markers in Serum or CSF: Tumor markers in Serum or CSF: αα--FP, FP, ββ--hCGhCG•• Surgical biopsy for presumed GCT (except for patient in whom a Surgical biopsy for presumed GCT (except for patient in whom a
presumptive diagnosis of NGGCT can be made).presumptive diagnosis of NGGCT can be made).•• ImmunohistochemicalImmunohistochemical assay of biopsy: PLAP, assay of biopsy: PLAP, αα--FP, FP, ββ--hCGhCG, c, c--kit, Oct3/4 kit, Oct3/4
and CD30and CD30•• CytogenicCytogenic analysis for 12panalysis for 12p
PLAPc-kitOct3/4
CD30
a-fetoprotein β-hCG
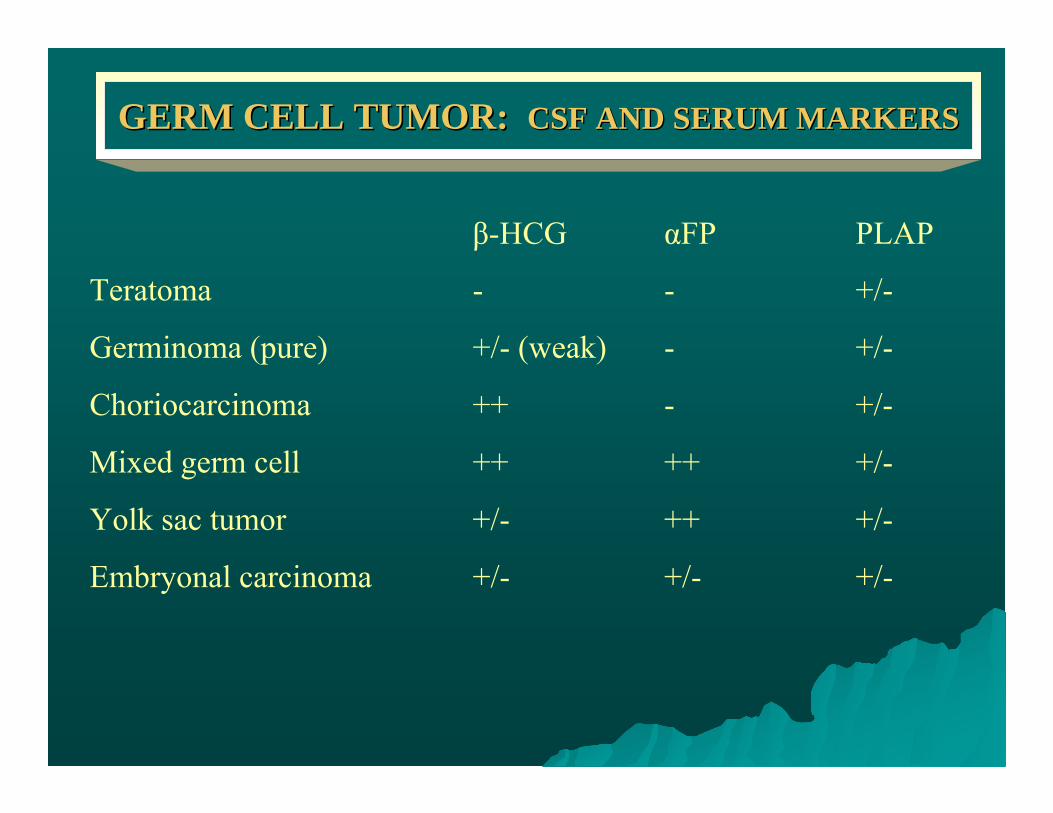
GERM CELL TUMOR: GERM CELL TUMOR: CSF AND SERUM MARKERSCSF AND SERUM MARKERS
β-HCG αFP PLAP
Teratoma - - +/-
Germinoma (pure) +/- (weak) - +/-
Choriocarcinoma ++ - +/-
Mixed germ cell ++ ++ +/-
Yolk sac tumor +/- ++ +/-
Embryonal carcinoma +/- +/- +/-
YOLK SAC TUMORYOLK SAC TUMOR
•Primitive appearing epithelial cells in a loose, variably cellular, myxoid matrix resembling extraembryonic mesoblast
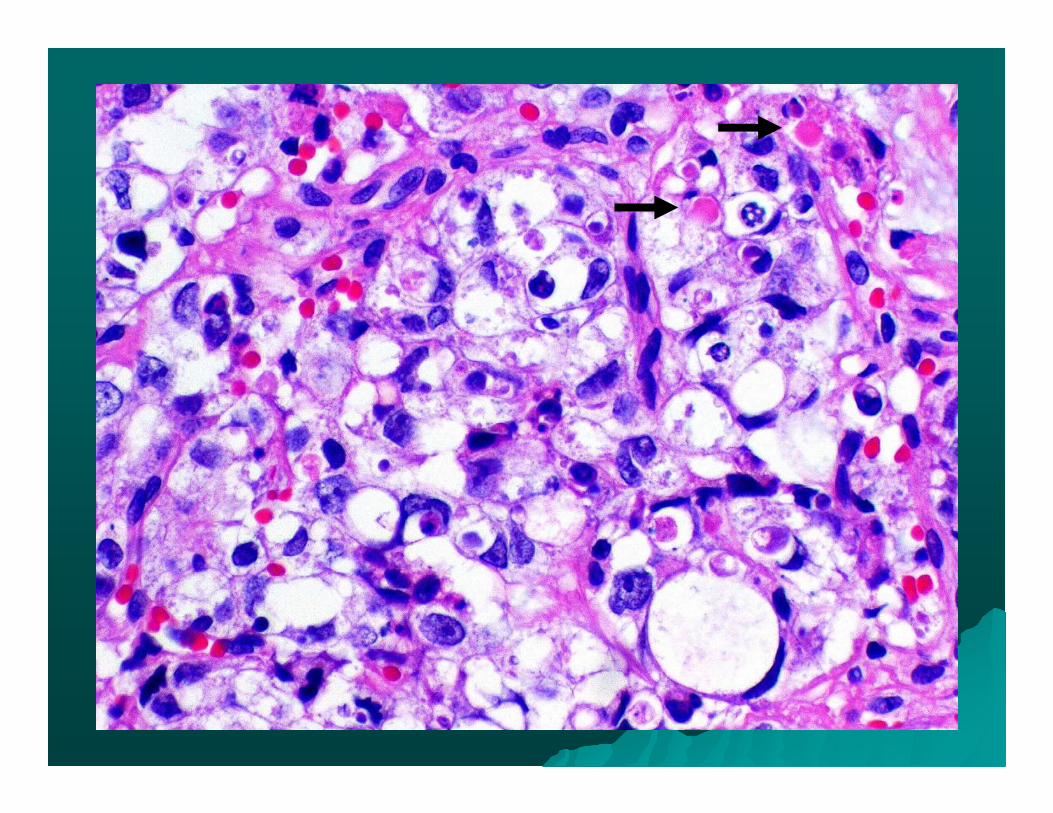
•Eosinophilic hyaline globules immunoreactive to αFP
•Epithelial elements proliferate in sheets with intervening meshwork of irregular tissue spaces
•Schiller-Duval bodies: papillae formation
•Brightly eosinophilic, PAS-positive and diastase resistant hyaline globules (inconsistent finding but diagnostic)
•Variable mitotic activity, necrosis uncommon
•Cytoplasmic immunoreactivity for αFP is characteristic
•Poor prognosis
GERM CELL TUMOR: GERM CELL TUMOR: TREATMENTTREATMENT
GERMINOMAS:• Radiosensitive
• Local radiation therapy (RT) that includes the suprasellar region, pineal gland and periventricular areas.
• Craniospinal irradiation (CSI) reserved for patients with evidence of leptomeningeal disease, multiple tumors or simultaneous pineal and suprasellar involvement.
• Greater success with protocols that use chemotherapy (cisplatin) followed by RT (event free survival rate ~92%), although no randomized trial completed.
GERM CELL TUMORS: GERM CELL TUMORS: TREATMENTTREATMENT
NONGERMINOMATOUS GCT:• Relatively radioresistant
• Chemotherapy appears to be essential for successful treatment ofintracranial NGGCTs
• Platinum-based chemotherapy (i.e., carboplatin + etoposide + bleomycin) have shown moderate effectiveness, with complete and partial response rates ~80%
• Long-term surrival rates (>50%) with combined platinum containing chemotherapy and RT.
• High incidence of leptomeningeal metastasis, hence CSI is usually recommended.
• Surgical resection for patient with residual radiographic abnormalities and normalized tumor markers following chemotherapy, because of possibility of residual teratoma.
GERM CELL TUMOR:GERM CELL TUMOR:
•Interesting and prolonged presentation
•Diagnostic dilemma
•Rarity of diagnosis
Related Documents











