1416 • Renal cell carcinoma (RCC) accounts for 3% of malignancies in adults. • Cigarette smoking (in more than 20% of cases) and obesity (in more than 30%) are established causal factors for RCC. • Four percent of cases of RCC arise from hereditary syndromes. • Different subtypes of RCC are characterized by distinct clinical behavior, genetic abnormalities, and molecular signatures. • Clear cell RCC is the most common histologic subtype, representing approximately 70% of all sporadic RCCs. • The von Hippel-Lindau tumor suppressor gene is genetically and epigenetically altered in more than 75% of sporadic cases of clear cell RCC. • Prognosis for RCC is dependent on tumor histologic type, grade, and stage. • Nephron-sparing surgery has become the gold standard, when feasible. • Follow-up guidelines for resected RCC include history, physical examination, periodic metabolic panels, and abdominal and chest computed tomography (CT) studies 4 to 6 months after surgery. • High-dose bolus interleukin-2 (IL-2), though toxic and of limited use in selected patients, remains a therapeutic option for clear cell RCC because of its potential for durable complete response. Additional immunotherapeutic approaches under development and promising results have been reported with the immunocheckpoint inhibitor PD-1 antibody. Identification of predictors of response to immunotherapies is undergoing. • Antiangiogenesis drugs have become the new standard of care in the first-line setting for clear cell RCC. Clinical benefit has also been shown with vascular endothelial growth factor and mammalian target of rapamycin inhibitors in subsequent lines of therapies. Novel targets for therapeutic interventions have been identified and are being exploited in clinical testing. • Optimal treatment for non–clear cell RCC remains a challenge because of the genetic differences and little knowledge of the dysregulated molecular biology driving these cancers. Rational preclinical and clinical testing is needed. SUMMARY OF KEY POINTS 82 Cancer of the Kidney Roberto Pili, Eric Kauffman, and Ronald Rodriguez INTRODUCTION Renal cell carcinoma (RCC) accounts for approximately 3% of adult malignancies. Tumors that arise in the kidney exhibit a variety of histologic patterns that may be benign or malignant. Tumors of benign histology include oncocytomas, angiomyolipomas, fibromas, lipomas, lymphangiomas, and hemangiomas. Historically, RCC was widely known as hypernephroma. This term was coined originally by Grawitz in 1883 in the mistaken belief that these tumors arose from the adrenal gland, as the malignancies often exhibited clear cyto- plasm, a feature that was prominent in benign adrenal cortical tissue. Subsequently, it was determined that the clear cell carcinoma of the kidney (the dominant tumor type) was actually derived from mature renal tubular cells and the tumor was more appropriately referred to as renal cell adenocarcinoma. RCC exists in sporadic and hereditary forms. The sporadic form of the disease is usually first seen in the fifth decade or later in life. The clinical presentation of RCC has been described with the classic triad of symptoms of hematuria, flank pain, and fever. With the increased general use of imaging techniques, however, the vast majority of kidney tumors are now being detected incidentally. Improved surgical techniques for treatment of localized disease and recently developed novel systemic therapies for metastatic RCC (mRCC) have changed the management of this condition. INCIDENCE AND RISK FACTORS FOR SPORADIC RENAL CELL ADENOCARCINOMA The estimated new cases of kidney and renal pelvis tumors for 2012 was 64,770. 1 A predominance of cases in male patients has been reported, with an estimated 40,250 men developing disease in 2012, compared with 24,520 women. The estimated number of deaths in 2013 is 13,570 for both sexes (8,650 in men and 4,920 in women). The increasing incidence of RCC observed in the past had been attributed to increased detection as a result of the widespread use of imaging modalities such as computed tomography (CT), ultrasonog- raphy, and magnetic resonance imaging (MRI). 2,3 Although a decrease in the size of diagnosed renal cell tumors over time has been noted, an increasing incidence of large and late-stage RCC has also been observed, and partly accounts for the overall increase in incidence. 3 In the United States, increases in incidence have been more rapid among women than among men and among African Americans than among whites, leading to a shift in excess from among whites to among African Americans. 4 Cigarette smoking and obesity are the most consistently estab- lished causal risk factors, accounting for more than 20% and 30% of renal cell cancers, respectively. 4,5 Hypertension, rather than antihy- pertensive drugs, appears to influence renal cell cancer development,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1416
• Renalcellcarcinoma(RCC)accountsfor3%ofmalignanciesinadults.
• Cigarettesmoking(inmorethan20%ofcases)andobesity(inmorethan30%)areestablishedcausalfactorsforRCC.
• FourpercentofcasesofRCCarisefromhereditarysyndromes.
• DifferentsubtypesofRCCarecharacterizedbydistinctclinicalbehavior,geneticabnormalities,andmolecularsignatures.
• ClearcellRCCisthemostcommonhistologicsubtype,representingapproximately70%ofallsporadicRCCs.
• ThevonHippel-Lindautumorsuppressorgeneisgeneticallyandepigeneticallyalteredinmorethan75%ofsporadiccasesofclearcellRCC.
• PrognosisforRCCisdependentontumorhistologictype,grade,andstage.
• Nephron-sparingsurgeryhasbecomethegoldstandard,whenfeasible.
• Follow-upguidelinesforresectedRCCincludehistory,physicalexamination,periodicmetabolicpanels,andabdominalandchestcomputedtomography(CT)studies4to6monthsaftersurgery.
• High-dosebolusinterleukin-2(IL-2),thoughtoxicandoflimiteduseinselectedpatients,remainsatherapeuticoptionforclearcellRCCbecauseofitspotentialfordurablecompleteresponse.AdditionalimmunotherapeuticapproachesunderdevelopmentandpromisingresultshavebeenreportedwiththeimmunocheckpointinhibitorPD-1
antibody.Identificationofpredictorsofresponsetoimmunotherapiesisundergoing.
• Antiangiogenesisdrugshavebecomethenewstandardofcareinthefirst-linesettingforclearcellRCC.Clinicalbenefithasalsobeenshownwithvascularendothelialgrowthfactorandmammaliantargetofrapamycininhibitorsinsubsequentlinesoftherapies.Noveltargetsfortherapeuticinterventionshavebeenidentifiedandarebeingexploitedinclinicaltesting.
• Optimaltreatmentfornon–clearcellRCCremainsachallengebecauseofthegeneticdifferencesandlittleknowledgeofthedysregulatedmolecularbiologydrivingthesecancers.Rationalpreclinicalandclinicaltestingisneeded.
S U M M A R Y O F K E Y P O I N T S
82 Cancer of the KidneyRobertoPili,EricKauffman,andRonaldRodriguez
INTRODUCTIONRenal cell carcinoma (RCC) accounts for approximately 3% of adult malignancies. Tumors that arise in the kidney exhibit a variety of histologic patterns that may be benign or malignant. Tumors of benign histology include oncocytomas, angiomyolipomas, fibromas, lipomas, lymphangiomas, and hemangiomas. Historically, RCC was widely known as hypernephroma. This term was coined originally by Grawitz in 1883 in the mistaken belief that these tumors arose from the adrenal gland, as the malignancies often exhibited clear cyto-plasm, a feature that was prominent in benign adrenal cortical tissue. Subsequently, it was determined that the clear cell carcinoma of the kidney (the dominant tumor type) was actually derived from mature renal tubular cells and the tumor was more appropriately referred to as renal cell adenocarcinoma. RCC exists in sporadic and hereditary forms. The sporadic form of the disease is usually first seen in the fifth decade or later in life. The clinical presentation of RCC has been described with the classic triad of symptoms of hematuria, flank pain, and fever. With the increased general use of imaging techniques, however, the vast majority of kidney tumors are now being detected incidentally. Improved surgical techniques for treatment of localized disease and recently developed novel systemic therapies for metastatic RCC (mRCC) have changed the management of this condition.
INCIDENCE AND RISK FACTORS FOR SPORADIC RENAL CELL ADENOCARCINOMAThe estimated new cases of kidney and renal pelvis tumors for 2012 was 64,770.1 A predominance of cases in male patients has been reported, with an estimated 40,250 men developing disease in 2012, compared with 24,520 women. The estimated number of deaths in 2013 is 13,570 for both sexes (8,650 in men and 4,920 in women). The increasing incidence of RCC observed in the past had been attributed to increased detection as a result of the widespread use of imaging modalities such as computed tomography (CT), ultrasonog-raphy, and magnetic resonance imaging (MRI).2,3 Although a decrease in the size of diagnosed renal cell tumors over time has been noted, an increasing incidence of large and late-stage RCC has also been observed, and partly accounts for the overall increase in incidence.3 In the United States, increases in incidence have been more rapid among women than among men and among African Americans than among whites, leading to a shift in excess from among whites to among African Americans.4
Cigarette smoking and obesity are the most consistently estab-lished causal risk factors, accounting for more than 20% and 30% of renal cell cancers, respectively.4,5 Hypertension, rather than antihy-pertensive drugs, appears to influence renal cell cancer development,

1417CanceroftheKidney • CHAPTER82
PATHOLOGYKidney tumors usually are unilateral but may be bilateral in 2% to 4% of cases.9 These tumors tend to grow into the renal vein and may form a tumor thrombus that extends into the vena cava and even the right atrium. Vascular involvement is present in 4% to 10% of patients at the time of presentation.10 From a pathological and surgi-cal prospective, it is important to distinguish a tumor thrombus form a positive margin at the vascular surface, as a true positive margin (with actual invasion into the wall of the vessel) portends a poor prognosis.
RCC is a clinically and pathologically heterogeneous disease.11 The 2004 World Health Organization (WHO) classification for renal neoplasms recognizes several distinct histologic subtypes of RCC (Table 82-1). These subtypes include clear cell RCC, papillary RCC, chromophobe RCC, hereditary cancer syndromes, multilocular cystic RCC, collecting duct carcinoma, medullary carcinoma, mucinous tubular and spindle cell carcinoma, neuroblastoma-associated RCC, Xp11.2 translocation–TFE3 carcinoma, and unclassified lesions.12,13 Clear cell RCC is the most common adult RCC, representing 70% of all RCCs. Papillary type I and type II RCC account for 10% to 15%, chromophobe RCC for 4% to 6%, collecting duct carcinoma for less than 1%, and unclassified lesions for 4% to 5% of RCCs. Tumors may be composed of mixed histologic subtypes, and each subtype may feature high-grade sarcomatoid characteristics. Histo-logic differentiation of most subtypes of RCC can be accomplished with hematoxylin-and-eosin staining techniques. The conventional histologic pattern is the most common, characterized by large clear cells with abundant cytoplasm. The chromophobe pattern is granular with abundant mitochondria. The papillary or tubulopapillary variant may represent a different type of tumor, because they tend to be smaller with fewer anaplastic features. The most widely used
although the mechanism is unknown.4,5 This was the conclusion of a large study of 363,992 Swedish men who received at least one physical examination between 1971 and 1992 and who were followed up until death or until the end of 1995.5 The relative risk for RCC was 1.3 for former smokers and 1.6 for current smokers. The relative risk for renal pelvis cancer was even higher at 1.6 for former smokers and 3.5 for current smokers. With regard to obesity, patients with a body mass index in the highest one-eighth of the cohort had a relative risk of 1.9 when compared with patients in the leanest subgroup. Hypertension was confirmed as a third risk factor for RCC. A study tested whether smoking is associated with mutations in the von Hippel-Lindau tumor suppressor gene (VHL) in 337 cases of sporadic RCC among 120,852 people over a mean follow-up period of 11.3 years; the findings suggest that smoking causes RCC independently of VHL mutations.6
Patients with end-stage renal disease have an increased incidence of RCC when compared with the general population. Patients receiv-ing prolonged dialysis tend to develop acquired renal cystic disease, possibly as a result of disordered proliferation within the native kidney. In these patients, the tumors often are bilateral and multifo-cal, with a papillary histology.7 Accordingly, these patients should be monitored regularly with renal ultrasound examinations or noncon-trast MRI. If the patient is on dialysis, then nephrectomy is typically preferred, even when the tumor is smaller than 4 cm, providing the risk of surgery is reasonable.
Additional evidences suggest a potential role in RCC for alcohol consumption, occupational exposure to trichloroethylene, and high parity among women. However, further research is needed into the potential causal effects of genetic factors and their interaction with environmental exposures. Large studies employing genome-wide scanning technology are in progress to provide novel discoveries in renal carcinogenesis.8
Table 82-1 Histologic Classification of Renal Cell Carcinoma
SPORADIC RCC 2004 WHO CLASSIFICATION
Histologic Tumor Type Prevalence (%) Cytogenetic Findings
Clear cell RCC 70 3p25-26 (VHL)
Papillary RCC 10-15 Trisomy of chromosomes 7 and 17, loss of Y chromosome, 7q34 (c-Met)
Chromophobe RCC 4-6 Loss of multiple chromosomes: 1, 2, 6, 10, 13, 17, 21
Multilocular cystic RCC <1 Extracellular matrix gene
Collecting duct carcinoma <1 Loss of multiple chromosomes: 1, 6, 8, 13, 14
Medullary carcinoma <1 Sickle cell trait
Mucinous tubular and spindle cell carcinoma <1
Neuroblastoma-associated RCC <1
Xp11.2 translocation–TFE3 carcinoma 1-2 Translocations involving Xp11.2 (TFE3)
Unclassified lesions 4-5
HEREDITARY RCC: SYNDROMES AND HISTOLOGIC TUMOR TYPES
Hereditary SyndromeChromosome (Gene) Abnormality
Histologic Type of Renal Tumor Systemic Manifestations
von Hippel-Lindau 3p26 (VHL) Clear cell RCC Retinal angiomas, central nervous system hemangioblastomas, pheochromocytoma
Hereditary papillary RCC 7q34 (Met) Type 1 papillary RCC None
Hereditary leiomyoma RCC 1q42–43 (FH) Type 2 papillary RCC Cutaneous and uterine leiomyomas
Birt-Hogg-Dube syndrome 17p11.2 (BHD) Chromophobe RCC, oncocytoma, hybrid tumors
Skin lesions, lung cysts
Adapted from Prasad SR, Humphrey PA, Catena JR, et al. Common and uncommon histologic subtypes of renal cell carcinoma: imaging spectrum with pathologic correlation. RadioGraphics 2006;26:1795–1806.
RCC, renal cell carcinoma; WHO, World Health Organization.

PartIII:SpecificMalignancies1418
grading system for RCC is the nuclear grading system developed by Fuhrman and colleagues.14 This system assigns a grade from I to IV, based on nuclear size, roundness, and other morphologic features, such as the prominence of nucleoli and the presence or absence of clumped chromatin. Patients with tumors of high Fuhrman grade tend to have poorer clinical outcomes. However, many pathologists omit Fuhrman grade when the apparent aggressiveness of the histol-ogy is not related to prognosis (e.g., chromophobe carcinoma, which tends to have a favorable prognosis even when the cellular character-istics appear aggressive).
GENETICS AND EPIGENETICS OF RENAL CELL CARCINOMAUntil recently, RCC was thought to represent a monomorphic disease arising from a probable common precursor cell but with different histologic and clinical manifestations. Genetic characterization based on cytogenetics and molecular biology has established that different subtypes of RCCs are characterized by distinct genetic abnormalities and molecular signatures reflecting the differences in the cell type, biology, and underlying molecular mechanisms.15 Addi-tional tumor metabolic pathways may explain the biological diversity of RCC.
Sporadic Renal Cell CarcinomaClear Cell Renal Cell CarcinomaA common genetic feature signature of sporadic clear cell RCC is the loss of chromosome 3p, suggesting the presence of one or more RCC tumor suppressor genes at this site. The von Hippel-Lindau tumor suppressor gene (VHL), which resides on chromosome 3p25, is mutated or silenced in greater than 50% of sporadic clear cell RCCs.16,17 Germline VHL mutations give rise to von Hippel-Lindau syndrome, which is characterized by an increased risk of blood vessel tumors (hemangioblastomas), endocrine tumors and RCC. The VHL gene product, pVHL, is the substrate recognition module of an E3 ubiquitin ligase that targets the hypoxia-inducible factor (HIF) α transcription factors (HIF1α, HIF2α, and HIF3α) for destruction in the presence of oxygen. Hypoxic cells, or cells lacking pVHL (“pseu-dohypoxic”), accumulate high levels of HIF, which activates the tran-scription of a variety of genes, including vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF-3) B, and transforming growth factor alpha (TGF-2). Restoration of pVHL function in VHL−/− mutant renal carcinoma cells suppresses their ability to form tumors experimentally by reducing HIFα levels.18,19 Inhibition of HIFα is necessary and sufficient for tumor suppression by pVHL in RCC nude mouse xenograft assays. This provides a rationale for treating VHL−/− RCC with inhibitors of HIFα or its downstream targets. While the HIF1α isoform was initially believed to be more important, increasing literature supports HIF2α as the more important HIFα member in mediating tumorigenesis.18,19 Although most investigation has focused on the role of HIFα iso-forms, the pVHL protein also has several other targets in addition to HIFα, postulated by some to contribute to tumorigenesis. Elucidat-ing these targets will lead to further knowledge of how pVHL sup-presses tumor growth. Analysis of mutations in exon 3 of the VHL gene may be useful in refining the diagnostic criteria for conventional RCC versus chromophobe RCC with clear cell features.20
A recent work from Dr. Rathmell’s group have generated gene expression microarray data using software that implements iterative unsupervised consensus clustering algorithms to identify the optimal molecular subclasses. A Consensus Cluster analysis identified two distinct subtypes of clear cell RCC within the training set, designated clear cell type A (ccA) and B (ccB). In each subtype the analysis of data defined a small, highly predictive gene set. A validation data set of 177 tumors was analyzed. Tumors designated ccA had improved disease-specific survival compared with ccB (median survival of 8.6
vs. 2.0 years). These preliminary data suggest that a cluster subtype classification is possible in RCC as performed in other diseases such as breast cancer. Prospective clinical studies will be necessary to vali-date these important findings.21
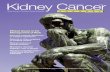
The genetic studies in familial RCC have led to the identification of specific molecular signatures in non–clear cell histotypes as well, such as Met hyperactivation in papillary type I, fumarate hydratase mutation in papillary type II, and c-Kit overexpression in chromo-phobe RCC (see “Papillary Types I and II Renal Cell Carcinoma”). Preliminary results from ongoing genetic studies have shown the possibility of clustering different histotypes based, for example, on kinase expression (Fig. 82-1A).22
DNA, histones, and nonhistone proteins are condensed into a highly complex nucleoprotein structure known as chromatin that acts as a prototype for all of the genetic information. Chromatin confor-mation can be in a heterochromatin form, a highly compact structure, associated primarily with transcriptionally inactive genes, or a euchro-matin form, consisting of a more open or relaxed structure, associated with transcriptionally active genes.23 Epigenetic mechanisms medi-ated by histone deacetylases (HDACs), histone acetyltransferases, and histone methyltransferases play critical roles in various biological and cellular processes, including cell proliferation, angiogenesis, hypoxia-related effects, and cell-cycle regulation. Histones on the N-terminal are altered by acetylation, methylation, phosphorylation, ubiquitina-tion, sumoylation, deamination, or adenosine diphosphate ribosyl-ation.24,25 The different histone residues and their modifications result in either transcriptionally active or repressive marks. For example, histone H3 lysine 4 (designated as H3K4), H3K36, and H3K79 are associated with active marks, whereas H3K9, H3K27, and H4K20 are associated with repressive marks.26
Several studies have recently reported SETD2, a histone methyl-transferase, as a tumor suppressor gene in RCC.27,28 An initial study consisting of a large-scale next-generation sequencing of primary RCC genomes identified somatic truncating mutations in SETD2 (approximately 3%).28 These mutations are associated with a decrease in H3K36 trimethylation levels in several clear cell renal carcinoma cell lines, VHL mutations and/or hypoxic phenotype (determined by a panel of hypoxia-related genes) in clinical samples, as well as a chromatin remodeling complex protein PBRM1.29 It is also impor-tant to note that SETD2 and PBRM1 are located on the short arm of the human chromosome 3 (3p21.31), in close proximity to the VHL gene and the 3p region is frequently altered in clear cell RCCs30 (see Fig. 82-1B). Although mutations in enzymes governing chroma-tin remodeling are often found in advanced stage disease, these mutations have not been correlated to survival.31 The H3K27 meth-yltransferase EZH2 (which is associated with aggressiveness in breast cancer and overexpressed in metastatic prostate cancer)32 is overex-pressed in renal tumor patient samples compared with their normal adjacent.33 Conversely, histone demethylases governing H3K27 methylation status UTX and JMJD3 are overexpressed in clear cell RCCs compared with the adjacent nontumor tissue, which corre-sponds to the decreased H3K27 methylation in clear cell RCC.34 These preliminary evidences suggest that alterations in histone-modifying genes may be associated with RCC and could be exploited for therapeutic interventions.
More recently, the BAP1 protein, a nuclear deubiquitinase, has been reported to be inactivated in 15% of clear cell RCCs. BAP1 mediates suppression of cell proliferation, ubiquitinates the histone 2A lysine 119, and its loss sensitizes RCC cells in vitro to genotoxic stress. Initial evidences suggest that BAP1 loss is associated with high tumor grade and poor prognosis. Interestingly, mutations in BAP1 and PBRM1 appear to be mutually exclusive. These preliminary results provide a rationale for future integrated pathological and molecular genetic classification of RCC that will likely lead to subtype specific treatments.35
Intratumor heterogeneity has always been considered a potential major clinical hurdle to develop personalized-medicine strategies that

1419CanceroftheKidney • CHAPTER82
Figure 82-1 • Genetic signatures in RCC. Determining the genetic signature in renal tumors not only has advanced the tumor classification but also will contribute to the optimal selection of therapies. A, Kinase expression in RCC. These data show the gene expression of approximately 80 kinases (of 518) that have differential expression across the subtypes, with red meaning strong expression. Recognition of c-Met and c-Kit expression allows clustering the samples in specific subtypes. These types of data will guide the selection of patients undergoing treatment with kinase inhibitors. Chromo, Chromophobe; Onco, oncocytoma; PapI, papillary type I, PapII, papillary type II. B, Summary of the common 3p deletion/5q amplification signature that characterizes clear cell carcinoma. Interestingly, the 3p region that harbors the VHL gene also contains histone modifying genes that have been recently reported to be commonly mutated in this histotype. (A adapted from Teh B: Kinome in renal cell carcinoma: mutation analysis of 518 kinases and expression in 400 tumors. J Clin Oncol 2007 ASCO Annual Meeting Proceedings 2007;25[18S]:5013.)
c-Met
c-Kit
1p1q2p2q3p3q4p4q5p5q6p6q7p7q8p8q9p9q10p10q11p11q12p12q13p13q14p14q15p15q16p16q17p17q18p18q19p19q20p20q21p21q22p22qXpXqYpYq
Clear cellgood prognosis
Clear cellpoor prognosis
ChromoOnco Papl
A
Mutations:
SETD2, UTX, JARID1C, BAP1 (~15% in ccRCC)PBMR1 (~40% in ccRCC)
VHL
B
Papll

PartIII:SpecificMalignancies1420
dysregulated transcriptional TFE3 activity. Immunohistochemical detection of nuclear TFE3 expression is suggestive of the underlying fusion mutation43; however, definitive diagnosis requires genetic con-firmation by karyotype, fluorescence in situ hybridization, or poly-merase chain reaction (PCR).
Rarely, fusions between the related transcription factor gene, TFEB, and the MALAT1/Alpha gene also are found in renal cancers. Less than 30 cases have thus far been reported. The histology of these tumors appears to be distinct from TFE3-fusion tumors. TFEB-fusion cancers similarly occur in younger patients, but in contrast to TFE3-fusion cancers, appear to confer an excellent prognosis. The function of the TFEB transcription factor is unknown, but a central role in lysosome biogenesis and autophagy regulation has been suggested.44
Familial Renal Cell CarcinomaIn a small percentage (5%) of cases, RCC is a feature of one of several hereditary syndromes.15,45 Such syndromes are associated with dis-tinct histologic subtypes of RCC, and in each case patients have increased risk of multifocal tumor development.15,45 Management is dependent on preservation of renal function. Close surveillance and minimization of surgical procedures constitute the mainstay of treatment.
von Hippel-Lindau syndrome is a disorder of autosomal dominant inheritance that occurs in 1 in 40,000 births. The mean age at onset is in the fourth decade of life. The syndrome is inherited as a result of a germline mutation in a single allele of the VHL gene tumor suppressor gene located on chromosomal band 3p25–26.15,45,46 Spo-radic loss of the remaining wild-type VHL allele provides the “second hit” necessary for tumorigenesis, most commonly via chromosome 3p deletion. Multifocal tumorigenesis is observed in multiple organ systems, with each tumor harboring an independent second VHL mutation. Renal manifestations include cysts and clear cell RCC tumors. Both tend to be multifocal and bilateral, and are found in the majority of patients with von Hippel-Lindau disease.15,45,46 Hun-dreds of independent clear cell cancers may be present in a single kidney, including dozens of macroscopic tumors. VHL syndrome patients are at high risk for chronic renal insufficiency because of the lifelong risk of multifocal RCC tumor development and need for repeat renal surgeries. As a result, VHL patients should undergo active surveillance until the largest tumor reaches 3 cm, at which time attempts may be made to resect all tumors in that kidney. Resection by enucleation without clamping of the main renal artery is recom-mended to maximize nephron sparing. Surgical candidates, particu-larly those with numerous tumors, are counseled as to the high possibility of local recurrence from de novo tumor formation and future ipsilateral surgery. The discovery of the VHL gene in hereditary clear cell RCC enabled the subsequent identification of a VHL muta-tion in sporadic clear cell RCC tumors (see above).47
In addition to renal cysts and cancer, common manifestations of the VHL syndrome include benign vascular tumors of the spinal cord, cerebellum and retina, presenting as neurologic and visual symptoms. The endocrine system may also be affected by adrenal pheochromocytomas and pancreatic neuroendocrine tumors, in addi-tion to pancreatic cysts. Benign papillary cystadenomas of the epi-didymis or broad ligament also develop in a minority of patients, which, when bilateral are pathognomonic for von Hippel-Lindau disease. Firm epididymal nodules on physical should prompt scrotal ultrasound and with a family history of VHL provides easy method to confirm the diagnostic suspicion. Endolymphatic sac tumors of the inner ear also may be seen.
Birt-Hogg-Dubé syndrome is a disorder of autosomal dominant inheritance. Signs and symptoms usually manifest in the fifth decade of life and include renal tumors and cysts, benign skin tumors (fibro-folliculomas) and pulmonary cysts, which can lead to spontaneous pneumothorax. The renal neoplasms may be multifocal and bilateral
depend on results from single-tumor biopsy samples. A recent report has now shown very elegantly that intratumor heterogeneity is a reality.36 Different techniques, including exome sequencing, chromo-some aberration analysis, and ploidy profiling on multiple spatially separated samples obtained from primary renal carcinomas and asso-ciated metastatic sites, determined that 63% to 69% of all somatic mutations were not detectable across every tumor region. Mutational intratumor heterogeneity was seen for multiple tumor suppressor genes and chromatin remodeling genes, including SETD2, PTEN, and KDM5C. Gene-expression signatures associated with good and poor prognosis were detected in different regions of the same tumor. These new intriguing findings, combined with the complex genomic landscape, make us rethink the common assumption that a single genomic test might guide therapy. The timing and location of the tumor sample acquisition remain a challenge, but there is still an opportunity to make personalized medicine a goal to achieve in the future for the treatment of cancer, and RCC in particular.
Papillary Types I and II Renal Cell CarcinomaAs with clear cell RCC, genetic studies in familial RCC have led to the identification of genes responsible for non–clear cell histotypes as well. However, unlike clear cell RCC, gene mutations identified in hereditary non–clear cell RCC are absent in the vast majority of sporadic cases. Activating mutations in the Met oncogene responsible for hereditary papillary RCC (see “Familial Renal Cell Carcinoma”) are found in only approximately 10% of sporadic papillary type I RCC cases.37 The Met tyrosine kinase receptor localizes to the cell membrane where it binds its extracellular ligand, hepatocyte growth factor, triggering intracellular activation of the Akt, Rac, and MAP kinase signaling pathways, promoting cell proliferation and migra-tion. Hyperactivation of Met signaling is believed to promote tumori-genesis by upregulation of these downstream pathways. Both Met and hepatocyte growth factor localize to chromosome 7, which is com-monly amplified in sporadic papillary type I RCC.
The fumarate hydratase gene encoding a Krebs cycle enzyme and mutated in hereditary papillary type II RCC (as part of hereditary leiomyomatosis and RCC syndrome; see “Familial Renal Cell Carci-noma”) has not been identified in sporadic papillary type II.38 However, increased activity of the NRF2 transcription factor result-ing from fumarate hydratase loss in hereditary papillary type II has also been demonstrated in sporadic papillary type II renal cancers.39,40
Chromophobe Renal Cell CarcinomaAs with papillary types of RCC, the genetic mutations underlying sporadic chromophobe RCC tumorigenesis remain to be elucidated, and appear to have little mutational overlap with hereditary chromo-phobe RCC. The folliculin gene mutated in the most common type of hereditary chromophobe RCC (Birt-Hogg-Dubé; see “Familial Renal Cell Carcinoma”) is rarely mutated (0% to 10%) in sporadic chromophobe RCC tumors.41 While PTEN has been implicated in a rarer type of hereditary chromophobe RCC, its mutation is yet to be identified in the sporadic disease.42
TFE3-Fusion Renal Cell CarcinomaAlso known as Xp11 translocation kidney cancer, TFE3-fusion RCC represents <1% of all sporadic renal cell cancers. It is the most recently designated histologic subtype of RCC by the WHO. TFE3-fusion RCC occurs in younger patients and is the most common mutation in pediatric RCC tumors. These tumors are clinically aggressive and commonly present with metastasis, particularly to regional lymph nodes. These tumors harbor a pathognomonic fusion between the TFE3 gene of chromosome Xp11.2 and one of a number of possible fusion partners on various chromosomes, most commonly PRCC, ASPRC1, and SFPQ. The TFE3 gene encodes a transcription factor involved in the regulation of many proteins implicated in carcino-genesis, including TGF, Met, Rb, Folliculin, Ets, and E-cadherin. It is believed that the fusion promotes tumorigenesis by causing

1421CanceroftheKidney • CHAPTER82
Hereditary renal cell cancer associated with melanoma has been recently described. The TFE3 gene mutated in sporadic RCC (see “Diagnosis of Renal Cell Carcinoma”) is one of four members of the MiT family of transcription factors; although TFE3 mutations have not been identified in hereditary RCC syndromes, the related MiT member, MiTF, was shown to have a specific amino acid substitution associated with hereditary RCC tumors associated with melanoma.55 This substitution confers hyperactivation of MiTF transcriptional activity by preventing its sumoylation and degradation. Histologic features of these MiTF renal cancers are yet to be characterized.
DIAGNOSIS OF RENAL CELL CARCINOMAAs the use of imaging methods has become more widespread, the frequency of incidental detection of RCC has increased. Patients with RCC typically present with a mass involving the kidney that is suggestive of the diagnosis. Nephrectomy is the most effective therapy for RCC that is confined to the kidney and should be used both diagnostically and therapeutically in most patients who are suitable surgical candidates. In certain clinical settings, percu-taneous biopsy of a renal mass should be considered. In a retro-spective study of 115 consecutive percutaneous biopsies performed on renal masses in 113 patients, investigators found percutaneous biopsy to be of high sensitivity in three clinical groups: patients with a known malignancy (N = 55), patients with no known malignancy and suspected unresectable tumor (N = 36), and non-surgical patients with a mass suspected to be a resectable RCC (N = 8).57 Percutaneous biopsy of renal masses appears to be safe, carrying only a minimal risk of tumor spread. Urologists should consider increasing the indications for renal biopsy of small renal masses that appear to be RCC, especially in elderly and surgically unfit patients. The standardization of a sheathed biopsy technique by interventional radiology has alleviated fears of tumor seeding through the biopsy tract. With more experience and follow-up preoperative biopsy, this strategy has the potential to decrease unnecessary treatment, because up to a third of small renal masses are now reported to be benign at surgery. Percutaneous biopsy also may allow better selection of renal tumors for active surveillance and minimally invasive ablative therapies. However, there are certain histologic subtypes that cannot be easily distinguished by percuta-neous biopsy. Oncocytoma for instance can only be diagnosed by resection, as rarely clear cell carcinoma may harbor regions of oncocytic cells, which are indistinguishable from oncocytoma with a single-needle core. In cases where oncocytoma may be suspected (e.g., in a patient with prior multifocal oncocytomas in the con-tralateral kidney), several staged biopsies of the mass can be per-formed to increase the confidence in the diagnosis. A RCC is unlikely to have three separate biopsies all positive for oncocytic cells only without any clear cell components. Finally, initial therapy for mRCC may potentially be stratified by histologic subtype and, in the future, molecular characteristics.
STAGING SYSTEMS FOR RENAL CELL CARCINOMAThe tumor–node–metastasis (TNM) system is a dynamic staging method that continually changes on the basis of new evidence from clinical studies (Table 82-2).58 This staging system is a method of stratifying patients with cancer and is based on data from large mul-ticenter studies with large numbers of patients and a good level of evidence. Despite continual revisions to the methodology to incor-porate new clinical evidence, however, the optimal RCC patient stratification using the TNM staging system remains controversial, and further revisions probably will be needed. Revision of the TNM staging system for RCC is likely to result in the simultaneous update of the integrated prognostic systems currently used with this tradi-tional method of staging.
tumors and most often have pure chromophobe histology or a “hybrid” mixture of chromophobe and oncocytoma; infrequently, pure oncocytoma tumors may be present. Patients can present with several different tumor types within the same kidney and the presence of benign (oncocytoma) and malignant tumors within the same kidney should immediately prompt the suspicion of Birt-Hogg-Dubé (BHD) syndrome. The BHD gene mutated in this syndrome encodes the protein Folliculin and is located on chromosome 17p11.2.15,45,46,48,49 The BHD gene appears to have the characteristics of a loss-of-func-tion tumor suppressor gene.50 Folliculin has unknown function but is found in complexes with adenosine monophosphate-activated protein kinase, the major sensor of cell energy and a negative regula-tor of the mammalian target of rapamycin (mTOR) pathway. Recently, multiple studies have implicated Folliculin in adherens junction formation and signaling.51,52
Tuberous sclerosis is a syndrome of autosomal dominant inheri-tance, with two genes identified, TSC1, located on 9q34, and TSC2, located on 16p13.3. It affects 1 in 6000 people and is usually diag-nosed at birth.15,45,46 This syndrome encompasses multiple organ systems, including dermatologic, cardiac, pulmonary, and renal. Skins lesions include facial angiofibromas, periungual fibroma, shagreen patches, and hypopigmented macules. Patients also develop cardiac rhabdomyomas, pulmonary lymphangioleiomyomatosis, retinal hamartomas, subependymal nodules, and giant cell astrocyto-mas. The renal manifestations include bilateral and multifocal angio-myolipomas (AMLs) and less commonly clear cell renal carcinoma. In contrast with spontaneous AML, AML in this setting can be associated with a low risk of occult RCC (1%). The TSC1 and TSC2 gene products inhibit activation of mTOR signaling, a major pro-moter of protein synthesis and cell growth.
Hereditary papillary renal cell carcinoma (HPRCC), inherited as an autosomal dominant trait, is caused by mutations in Met protoonco-gene on chromosomal band 7q31–34.15,46,53 It is characterized pri-marily by bilateral, multifocal papillary type I RCC. These tumors are not aggressive and rarely metastasize. Age at onset is around the fifth decade. The Met oncogene encodes a membrane tyrosine kinase that, in HPRCC, harbors an activating mutation in the kinase domain. Hyperactivation of the Met oncoprotein leads to upregula-tion of several intracellular signaling pathways involving Akt, Rac, and MAP kinase.
Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) is a disease of autosomal dominant inheritance. The gene for this disorder localizes to chromosomal band 1q42.3–43 and has been identified as fumarate hydratase (FH).15,45,46 Age at onset is between the third and fourth decades of life. The syndrome consists of cutaneous leiomyo-mas, uterine leiomyomas (fibroids), and papillary type II RCC tumors with high metastatic potential, even when small in size. Unlike the VHL patients, in whom delay in surgical treatment is usually the rule until the largest tumor reaches 3 cm, there should be no delay in treatment of solid renal lesions in these patients. Cystic lesions in these patients should be followed with close surveillance and early surgical intervention for any radiographic development of a poten-tially solid component. Thirty percent of patients have solitary and unilateral renal tumors.45,46
The FH gene functions as a tumor suppressor, with loss of the second allele detected in kidney tumors. The wild-type gene encodes an enzyme in the Krebs cycle catalyzing fumarate conversion into malate. Loss of the FH enzyme leads to accumulation of fumarate, which has been suggested to promote carcinogenesis through indirect stabilization of transcription factors HIFα and NRF2.39,40,54
Distinct from HPRCC and HLRCC, Malchoff and colleagues have described a three-generation family with five cases of papillary thyroid carcinoma and two cases with papillary renal neoplasia.53 With the use of linkage analysis, these investigators demonstrated that the fPTC/PRN phenotype was linked to 1q21.53 They characterized a distinct inherited tumor syndrome that may establish a link between papillary RCC and familial papillary thyroid carcinoma.53

PartIII:SpecificMalignancies1422
no survival difference between stage I and stage II tumors at the 2.5-cm breakpoint, although a significant difference was identified at the 7.5-cm breakpoint. In 1997, the American Joint Committee on Cancer (AJCC)62 and the International Union Against Cancer (UICC)63 published an updated version of the TNM system. The result of this international collaboration was a more uniform catego-rization of RCC based on improved clinical evaluation and manage-ment. In this version, the breakpoint between pT1 and pT2 was increased from 2.5 cm to 7.0 cm. In addition, the requirement for the T3a classification was more precisely defined as invasion of the adrenal gland by direct extension of the tumor or invasion of peri-nephric fat. The subcategories of venous tumor extension (pT3) were revised so that venous tumor extension above the diaphragm was classified as T3c, whereas venous tumor extension limited to the vena cava below the diaphragm was classified as T3b. This reflected the decreased adverse prognostic significance of venous tumor extension alone. The classification of lymph node metastasis also was simplified to include involvement of a single lymph node (N1) or multiple lymph nodes (N2), with the stipulation that four to eight nodes should be analyzed before assigning the pN0 classification.64
In the most recent (2010) 7th edition to the AJCC staging for RCC,65 T2 lesions are now subclassified as T2a (>7 cm up to 10 cm) and T2b (>10 cm), while ipsilateral adrenal involvement is now staged based on type of invasion: T4 if contiguous, M1 if not contigu-ous. In addition, renal vein involvement is reclassified as T3a, and
The first TNM staging system for RCC was developed in 1978.59 In this system, tumors are characterized on the basis of the degree of local extension of the tumor at the primary site (T), the involvement of regional lymph nodes (N), and the presence or absence of distant metastases (M). The addition of numbers to each of the TNM com-ponents allows one to more precisely categorize the extent of malig-nant disease at the primary, lymph node, and metastatic sites, respectively. The classification may be clinical (cTNM) or histopatho-logical (pTNM). In the case of RCC, the regional lymph nodes are defined as the hilar, abdominal paraaortic, and paracaval nodes. Lat-erality does not affect N categories. A retrospective study (N = 252) conducted to validate this system found that survival was most depen-dent on the local extent of the primary tumor, with 5-year overall survival rates of 100% for pT1, 91% for pT2, 58% for pT3, and 25% for pT4.60 The system also resulted in poor stratification of patients, with few patients in the pT1 (N = 7) and pT4 (N = 9) categories.
In the 1987 revision of the TNM system, a value of 2.5 cm was chosen to distinguish pT1 from pT2 tumors, and an entirely new set of criteria was introduced to evaluate lymph node status. Perhaps most important, comprehensive stage groupings were introduced to define more precisely the impact of TNM characteristics on survival. Again, however, very few patients were stratified to stage I, with only 11 of 872 patients classified in this category in one study.60,61 Fur-thermore, a study of 337 RCC tumors confined to the kidney found
Table 82-2 Tumor–Node–Metastasis (TNM) Staging System for Renal Cell Carcinoma
Staging Classification 1987 1997 2002
Tumor T1 Tumor ≤2.5 cm, limited to kidney
Tumor ≤7 cm, limited to kidney NA
T1a NA NA Tumor ≤4 cm, limited to kidneyT1b NA NA Tumor >4 cm and ≤7 cm, limited
to kidneyT2 Tumor >2.5 cm, limited to
kidneyTumor >7 cm, limited to kidney Tumor >7 cm, limited to kidney
T3 Tumor extends into major veins or invades adrenal or perinephric tissues, but not beyond Gerota fascia
Tumor extends into major veins or invades adrenal or perinephric tissues, but not beyond Gerota fascia
Tumor extends into major veins or invades adrenal or perinephric tissues, but not beyond Gerota’ fascia
T3a Perinephric or adrenal extension
Perinephric or adrenal extension Perinephric or sinus fat or adrenal extension
T3b Renal vein involvement Renal vein or vena cava involvement below diaphragm
Renal vein or vena cava involvement below diaphragm
T3c Vena cava involvement below diaphragm
Vena cava involvement above diaphragm
Vena cava involvement above diaphragm
T4 Outside Gerota’s fascia Outside Gerota fascia Outside Gerota’ fasciaT4a Vena cava involvement above
diaphragmNA NA
T4b NA NA NA
Node Nx Regional lymph nodes cannot be assessed
Regional lymph nodes cannot be assessed
Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
No regional lymph node metastasis
No regional lymph node metastasis
N1 Metastases in one lymph node ≤2 cm in greatest dimension
Metastases in one regional lymph node
Metastases in one regional lymph node
N2 Metastases in one lymph node >2 cm, but not >5 cm in greatest dimension
Metastases in more than one regional lymph node
Metastases in more than one regional lymph node
N3 Metastases in one lymph node >5 cm in greatest dimension
NA NA
Metastasis Mx Distant metastasis cannot be assessed
Distant metastasis cannot be assessed
Distant metastasis cannot be assessed
M0 No distant metastases No distant metastases No distant metastasesM1 Distant metastases Distant metastases Distant metastases
From Ficarra V, Galfano A, Mancini M, et al: TNM staging system for renal-cell carcinoma: current status and future perspectives. Lancet Oncol 2007;8:554–558.

1423CanceroftheKidney • CHAPTER82
with sarcomatoid (N = 45) and collecting duct tumors (N = 3) had worse prognosis. Survival rates for patients with clear cell and chro-mophobe histologic patterns were similar. The UISS uses five strati-fication groups (I through V) that incorporate variables commonly used in clinical practice, including 1997 TNM stage, ECOG perfor-mance status, and Fuhrman grade. The projected 5-year survival rates published by the UISS group were as follows: 94% for group I, 67% for group II, 39% for group III, 23% for group IV, and 0% for group V. The original UCLA integrated staging system has since been modi-fied so that patients are grouped into two general categories: those with nonmetastatic disease at the time of diagnosis and those with metastatic disease.78 Each category is then divided into high-, inter-mediate-, and low-risk subcategories, based on the 1997 TNM staging system, the Fuhrman grade, and the ECOG performance status.
To confirm the ability of the UISS to stratify patients with local-ized and mRCC into risk groups, an international multicenter study was conducted.73 A total of 4202 patients from eight academic centers were classified according to the UISS. The UISS stratified both local-ized and mRCC cases into three different risk groups. For localized RCC, the 5-year survival rates were 92%, 67%, and 44% for low-, intermediate-, and high-risk groups, respectively. A trend toward a higher risk of death was observed in all centers for increasing UISS risk category. For mRCC, the 3-year survival rates were 37%, 23%, and 12% for low-, intermediate-, and high-risk groups, respectively. In six of eight centers, a trend toward a higher risk of death was observed for increasing UISS risk category. A greater variability in survival rates among centers was observed for high-risk patients. These results suggest that the UISS is an accurate predictor of survival for patients with localized RCC, applicable to external databases. Although the UISS may be useful for patients with mRCC, it may be less accurate in this subset of patients because of the heterogeneity of patients and treatments.
A retrospective, single-institution review of 24 consecutive clinical trials conducted at Memorial Sloan-Kettering Cancer Center using cytokines or chemotherapy for the treatment of advanced RCC (N = 670) identified a small subgroup of patients (N = 30) who were long-term survivors after nephrectomy and treatment with interferon-α, interleukin (IL)-2, or surgical resection of metastasis.79 The five most prominent negative prognostic factors that were identi-fied by multivariate analysis included low Karnofsky performance status (less than 80%), elevated lactate dehydrogenase (greater than 1.5 times the upper limit of normal), low serum hemoglobin (below the lower limit of normal), high corrected serum calcium (greater than 10 mg/dL), and absence of nephrectomy. Patients with zero risk factors were assigned a favorable-risk status; those with one or two risk factors, an intermediate-risk status; and those with three or more risk factors, a poor-risk status. All long-term survivors in this study were in either good- or intermediate-risk groups.
In an additional study from the Memorial Sloan-Kettering Cancer Center, the relationship between pretreatment clinical features and survival was assessed in 251 patients with advanced RCC treated during 29 consecutive clinical trials between 1975 and 2002.80 Clini-cal features were first examined in univariate analyses, and then a stepwise modeling approach based on Cox regression was used to form a multivariate model. The median survival time for the 251 patients was 10.2 months and differed according to year of treatment, with patients whose tumor was treated after 1990 showing longer survival. In this group, the median overall survival time was 12.7 months. Because the purpose of this analysis was to establish prog-nostic factors for present-day clinical trial design, prognostic factor analysis was performed on data for these patients. Pretreatment fea-tures associated with a shorter survival in the multivariate analysis were low Karnofsky performance status, low hemoglobin level, and high corrected serum calcium. These features were used as risk factors to categorize patients into three different groups. The median time to death in patients with zero risk factors was 22 months. The median
nodal involvement is simplified to either N0 or N1, with the N2 stage dropped. In the previous (2002) edition of the manual, the key change was the subdivision of T1 lesions into T1a and T1b. The rationale was based on evidence from studies of patients undergoing partial nephrectomy, a procedure commonly used for tumors that are 4 cm or smaller. It has been reported that patients who undergo partial nephrectomy for RCC tumors smaller than 4 cm have equiva-lent survival to those undergoing radical nephrectomy.66 In a separate study of 485 patients undergoing nephron-sparing surgery for RCC with a mean follow-up period of 47 months, patients were divided into four groups based on the size of the primary.67 Patients in group 1 (tumors less than 2.5 cm in diameter) and those in group 2 (tumors 2.5 to 4.0 cm) had equivalent survival, although survival was signifi-cantly greater for groups 1 and 2 than for group 3 (tumors 4 to 7 cm) and group 4 (tumors greater than 7 cm). These findings were similar to those previously published in a separate series of 394 patients.68
Since the last revision of the system in 2002, data from several studies have provided issues for discussion in the next revision of the system.58 New data are available from large multicenter studies that recruited adequate numbers of patients with level 2 or 3 evidence.69-71 Prognostic systems include not only anatomical features but also other clinical and pathological variables, but will also eventually provide more accurate information for patient counseling, follow-up planning, patient selection for clinical trials, and adequate assessment of the results.58 Integrated systems are less widely used than the TNM system, because they are difficult to apply and contain several inad-equately defined clinical and histopathological variables. The TNM system will become a more refined and advanced instrument used by all clinicians and researchers involved in the management of RCC.
PROGNOSTIC FACTORS FOR RENAL CELL CARCINOMAAlthough TNM stage, Fuhrman grade, and Eastern Cooperative Oncology Group (ECOG) performance status are the most widely recognized prognostic factors in RCC, research continues to deter-mine strong and easily available prognostic parameters that may help to classify patients in groups with different risks for death from renal cancer. The prognosis for patients with RCC is dependent primarily on disease stage. Patients with histopathological stage pT1 or pT2 (organ confined) disease have the best prognosis, with 5-year cancer-specific survival rates after nephrectomy ranging from 71% to 97%.72 For patients with locally advanced tumors, 5-year cancer-specific survival rates after nephrectomy decrease by 20% to 53%, and once RCC has metastasized, the 5-year survival rate is less than 10%.
Numerous models exist to predict disease recurrence after nephrec-tomy for all histologic types and specifically for clear cell RCC.73 The natural history and risk group stratification have also been evaluated in those with newly diagnosed mRCC and in patients with previously treated metastatic disease. Currently, RCC histologic sub-types are classified according to the UICC and AJCC recommenda-tions.74 These recommendations are based on the Heidelberg classification system,75 which categorizes RCCs as clear cell, papillary, chromophobe, collecting duct, and unclassified RCC subtypes. Recent studies have suggested that stratification by histologic subtype could lend prognostic value.76,77
The University of California at Los Angeles (UCLA) Integrated Staging System (UISS) was developed for the purpose of improving the prognostic accuracy of the 1997 TNM staging system by incor-porating clinical variables.72 The study was based on the analysis of data for patients with RCC treated at a single institution between 1989 and 1999 (N = 661). All patients underwent radical or partial nephrectomy, and most patients with metastatic disease received recombinant IL-2-based immunotherapy within the context of 11 clinical trials. The median follow-up period was 37 months. Patients with papillary tumors (N = 42) showed a trend toward improved prognosis that did not achieve statistical significance, whereas patients

PartIII:SpecificMalignancies1424
addition of platelet and neutrophil counts to establish a prognostica-tor algorithm for overall survival in patients with mRCC treated with vascular endothelial growth factor (VEGF) inhibitors.83 In their latest report, the authors conducted an external validation and comparison with existing databases in RCC patients treated with VEGF inhibi-tors in the first-line setting at 13 institutions members of the Con-sortium’s database.84 They compared the Database Consortium model with the Cleveland Clinic Foundation, the International Kidney Cancer Working Group, the French, and the Memorial Sloan-Kettering Cancer Center models. A total of 1028 patients were assessed, with the majority having complete data. Median overall survival was 18.8 months. The previously defined prognostic factors (anemia, thrombocytosis, neutrophilia, hypercalcemia, Karnofsky performance status <80%, and <1 year from diagnosis to treatment) were independent predictors of reduced survival in this external vali-dation set. The results showed that median overall survival was 43.2 months in the favorable-risk group (no risk factors), 22.5 months in the intermediate-risk group (one to two risk factors), and 7.8 months in the poor-risk group (three or more risk factors). The concordance index of the Database Consortium with the other models ranged between 0.636 and 0.687. Now that this Database Consortium model has been externally validated, it can be applied to stratify patients by risk in clinical trials involving anti-VEGF therapies and to counsel patients about prognosis.
MANAGEMENT OPTIONS FOR LOCALIZED DISEASEThe gold-standard treatment for RCC localized to the kidney is surgi-cal resection, the only known curative treatment in this setting. Resection is performed by radical nephrectomy, with removal of the entire kidney and tumor en bloc, or partial nephrectomy, with removal of the tumor alone, maximizing preservation of renal func-tion. Locally advanced tumors may require additional resection of tumor in the renal vein and vena cava and/or partial resection of surrounding organs. The operation can be performed open or lapa-roscopically, the latter with or without robotic assistance, and using either a transperitoneal or retroperitoneal anatomic approach. Regional lymphadenectomy in the absence of lymphadenopathy remains controversial and is at present not routinely performed. In patients with significant comorbidity, advanced age, small tumor size, and/or low-risk tumor histology, or who are otherwise unwilling to undergo surgery, less-invasive options include thermal ablation and active surveillance. However, long-term outcomes supporting the oncologic safety of these alternatives are unclear and these options are currently reserved for select patients with greater operative than oncologic risk.
Radical NephrectomyRadical nephrectomy is the traditional gold-standard treatment for localized RCC. Long-term cancer-specific survival for pT1a, pT1b, pT2, and pT3 lesions can be approximated at greater than 90%, 80%, 70%, and 60%, respectively. Historically, a radical nephrec-tomy has included resection of the ipsilateral adrenal gland. However, adrenal resection increases the risk of life-threatening adrenal insufficiency (addisonian crisis) should the contralateral adrenal gland require resection or become otherwise functionally compromised. Today, it is common practice to limit adrenalectomy to the setting of large or upper pole renal tumors, given a low risk of adrenal involvement with smaller RCC tumors. Even in this setting, ipsilateral adrenalectomy has been challenged by recent studies sug-gesting that negative CT imaging of the ipsilateral adrenal gland can effectively rule out RCC involvement.85 Although still controversial, in the setting of negative cross-sectional imaging, adrenal gland pres-ervation should be considered to avoid long-term risk of addisonian crisis.
survival time in patients with one of these prognostic factors was 11.9 months. Patients with two or three risk factors had a median survival time of 5.4 months. These results suggest that the Memorial Sloan-Kettering Cancer Center risk categories (proposed by Motzer and coworkers80) can be used in clinical trial design and interpretation.
The natural history and risk group stratification also have been evaluated in patients with newly diagnosed mRCC. For patients diagnosed with disease recurrence, no specific risk stratification tools have been available at the time of recurrence. A retrospective study sought to evaluate the usefulness of the prognostic score suggested by Motzer and coworkers.80 From January 1989 to July 2005, patients with localized RCC treated by nephrectomy in whom recurrent disease subsequently developed were identified. Each patient was given a total risk score of 0 to 5, with 1 point for each of five prog-nostic variables (recurrence at less than 12 months after nephrectomy, serum calcium concentration greater than 10 mg/dL, hemoglobin concentration less than the lower limit of normal, lactate dehydroge-nase level greater than 1.5 times the upper limit of normal, and Karnofsky performance status less than 80%). Patients were catego-rized into low- (score = 0), intermediate- (score = 1 to 2), and high-risk subgroups (score = 3 to 5). The final cohort included 118 patients, with a median survival time of 21 months from the time of recurrence. Median duration of follow-up for survivors was 27 months. Overall survival was associated with risk group category. Low-risk, intermediate-risk, and high-risk criteria were fulfilled in 34%, 50%, and 16% of patients, respectively. Median survival times for low-risk, intermediate-risk, and high-risk patients were 76, 25, and 6 months, respectively. Two-year overall survival rates for low-risk, intermediate-risk, and high-risk patients were 88%, 51%, and 11%, respectively. These additional data support the use of a scoring system based on objective clinical and laboratory data to achieve meaningful risk stratification for both patient counseling and clinical trial entry.
The Memorial Sloan-Kettering Cancer Center and UCLA prog-nostic systems are similar in several ways. First, both systems are based on a series of consecutive clinical trials for RCC conducted at single institutions. Second, good performance status was found to correlate with lower risk in both systems. Third, cytoreductive nephrectomy for metastatic disease before immunotherapy was found to confer a more favorable prognosis (Memorial Sloan-Kettering Cancer Center) or was used as standard therapy (UCLA) in both systems. In 2007, Karakiewicz and associates proposed a nomogram for prediction of RCC-specific survival in nonmetastatic and metastatic disease, using a development cohort of 2530 patients and an external validation cohort of 1422 patients.81 The nomogram differs from the UISS with respect to one predictor. The symptom classification replaces the ECOG performance system within the nomogram. Moreover, the nomogram provides individual estimation of RCC-specific survival, instead of grouping patients within discrete strata. Direct comparison of the nomogram with the UISS strata, within an external validation cohort, demonstrated higher accuracy for the nomogram, with 89% and 87%, respectively, at 2 and 5 years, compared with 86% and 82% for UISS. A recent publication reports the results from an international, comprehensive database of more than 3500 patients that includes previously reported clinical prognostic factors. Three risk groups were identified and the model was validated using an independent data set of 645 patients treated with tyrosine kinase inhibitor (TKI) therapies. The results show that median survival in the favorable-, intermediate-, and poor-risk groups was 26.9 months, 11.5 months, and 4.2 months, respectively. Performance status, number of metastatic sites, time from diagnosis to treatment, and pretreatment hemoglobin, white blood count, lactate dehydrogenase, alkaline phosphatase, and serum calcium remain important prognos-tic factors. The model showed good concordance when tested among patients treated with TKI therapies.82
Heng et al. reported a novel model that validates components of the Memorial Sloan-Kettering Cancer Center model with the

1425CanceroftheKidney • CHAPTER82
(exophytic vs. endophytic) may be a better determinant than tumor size. With either larger size or more endophytic location, ischemic time can be expected to increase, along with complications related to bleeding and collecting system injury (urinary leak).92-94 The indica-tions for nephron-sparing surgery are partly dependent on the experi-ence and skill of the surgeon.
The primary oncologic concern with nephron-sparing surgery is the risk or recurrence in the same kidney, avoided with radical nephrectomy. Ipsilateral intrarenal recurrence occurs in 1% to 6% of patients after partial nephrectomy, and may result from either primary tumor multifocality (including de novo tumor formation) or positive surgical margins.95 However, it remains controversial whether positive surgical margins during partial nephrectomy increase the risk of RCC recurrence or have no prognostic significance. Many series support good local recurrence-free survival for patients with positive margins and intermediate-term follow up. Furthermore, immediate or delayed radical nephrectomy most often fails to reveal any residual disease in these patients. In a recent description of a large single-institutional series, Kwon et al. found no relation between margin status after partial nephrectomy and primary tumor risk (metastatic potential).96 However, local recurrence occurred in 4% of patients with a positive compared to only 0.5% of patients with negative surgical margins, and all cases of local recurrence in both groups were from high-risk primary tumors. The authors concluded that local recurrence may be more likely when positive surgical margins occur in the specific setting of high-risk primary tumor histology, whereas positive margins with low-risk primary tumors may have no significance. Current practice generally assumes no prognostic significance of positive sur-gical margins.
Given the benefit of nephron preservation and potential insignifi-cance of positive margins, the necessity of a 1-cm resection margin proposed by Vermooten in 1950 has come under question.97 Margin width during partial nephrectomy has thus been increasingly reduced over time.98,99 Several recent partial nephrectomy series show no association between disease recurrence and margin size.98-100 Some urologists now advocate a zero-margin tumor “enucleation,” taking advantage of a natural plane between the renal parenchyma and tumor pseudocapsule, a histologically confirmed structure ranging from 0.04 mm to 0.79 mm in width.101 In a series of 232 patients undergoing enucleation of tumors smaller than 4 cm, Carini et al. reported 97% and 95% 5- and 10-year cancer-specific survival rates, respectively, with no cases of positive margins or recurrences in the resection bed.102 According to these investigators, even though pseu-docapsular microinfiltration is frequent (33%) in enucleated tumors, positive margins are still avoided because of a surrounding chronic inflammatory layer that is, on average, 1 mm in width.101 In addition to optimizing renal preservation, tumor enucleation enables the surgeon to work in a relatively avascular plane and may reduce blood loss during resection and risk of collecting system injury. The reduc-tion in bleeding may allow resection without clamping of the main renal artery, avoiding renal ischemia.103
A large volume of existing retrospective literature now suggests survival benefits of partial nephrectomy over radical nephrectomy, but suffers from an uncertain selection bias. In a meta-analysis of more than 40,000 patients undergoing radical or partial nephrec-tomy, the latter was associated with a significant benefit in both survival and renal function; however, the quality of pooled studies was judged to be low.104 Recently, a large multiinstitutional random-ized trial from EORTC comparing partial and radical nephrectomy for tumors 5 cm or smaller has challenged current thinking on the role of nephron sparing.105 A total of 541 patients were enrolled in this study and median follow-up was more than 9 years. Based on an intention-to-treat analysis, the radical nephrectomy group cohort showed better overall survival compared with patients assigned to partial nephrectomy. Because there were very few cancer-specific deaths in either cohort, the benefit in overall survival for radical nephrectomy was attributed to a reduction in non–cancer-related
The role of regional lymphadenectomy at the time of radical nephrectomy is also controversial. The most common regional landing sites for RCC are the paracaval, interaortocaval, and retroca-val nodes for the right kidney, and the paraaortic, interaortocaval, and preaortic nodes for the left kidney. In the presence of radio-graphic or palpable lymphadenopathy, a lymph node dissection is justified. In the absence of such findings, the role of lymphad-enectomy is prognostic only, with no level 1 evidence to support a therapeutic benefit. Some series suggest a therapeutic role for lymphadenectomy specifically in patients without lymphadenopathy if their primary tumors are otherwise high risk, but these series are limited by retrospective nature and sample size. The European Orga-nization for Research and Treatment of Cancer (EORTC) 30881 trial has provided the only prospective randomized trial investigating radical nephrectomy (N = 772) with or without lymphadenectomy, but showed no benefit with regional lymphadenectomy at a median follow up of 12.6 years.86 This trial has been criticized for its inclusion of patients with predominantly low tumor stage and thus a low rate of nodal positivity (4%), suggesting insufficient power to detect a therapeutic benefit. In the absence of level 1 evidence supporting such a role, most urologists continue to avoid lymphadenectomy at nephrectomy, given the significant risk for hemorrhage during dis-section along the aorta and vena cava.
Nephron-Sparing SurgeryRadical nephrectomy has been shown to cause significant decreases in renal function, raising the risk of chronic renal insufficiency and dialysis, and chronic renal insufficiency, in turn, raises the risk of cardiovascular events, hospitalization, and overall mortality.87 Acknowledging the detrimental impact of chronic renal insufficiency on overall health, urologists have increasingly strived over the past 2 decades to preserve renal function in RCC patients. With increasing sensitivity and use of imaging studies leading to detection of smaller renal tumors, partial nephrectomy has become an effective alternative to radical nephrectomy for patients with localized RCC, resulting in low morbidity and good oncologic outcomes.
Traditional indications for partial nephrectomy have included conditions in which radical resection would leave the patient anephric (bilateral RCC, a horseshoe kidney, or a solitary kidney), requiring immediate dialysis; and unilateral RCC with a contralateral kidney at risk for compromised function, as in diabetes, hypertensive neph-rosclerosis, renal artery stenosis, renal calculi, and chronic pyelone-phritis. Initial outcomes under such indications supported operative feasibility and oncologic safety of a nephron-sparing approach. Patient selection quickly expanded to include localized primary tumors with diameter of 4 cm or less and exophytic location, regard-less of renal function.88 Although the risk of local recurrence is neces-sarily increased with a nephron-sparing approach, risk of cancer-specific mortality appears similar to a radical approach. Perioperative compli-cations are, however, more common with partial nephrectomy, due largely to increased bleeding/transfusion and urinary leaks related to collecting system injury.
Indications for partial nephrectomy have expanded to include select larger tumors.89 Several studies have now retrospectively com-pared partial and radical nephrectomy for larger tumors up to 7 cm, demonstrating similar oncologic outcomes.90,91 Leibovich and associ-ates compared outcomes in 91 patients managed with nephron-sparing surgery and 841 patients who underwent radical nephrectomy for 4- to 7-cm tumors.90 These investigators found no statistical dif-ference in cancer-specific survival and distant metastases between the two groups. Becker similarly compared 196 patients undergoing partial (N = 45) or radical nephrectomy (N = 151) for clear cell RCC tumors of 4 to 7 cm. They observed no differences in oncologic outcomes between the two groups, but noted better postoperative renal function at 3 months for patients undergoing nephron sparing.91 With regard to feasibility of partial nephrectomy, tumor location

PartIII:SpecificMalignancies1426
high-volume laparoscopic surgeon, similar operative outcomes were observed for laparoscopic resection of tumors larger than 4 cm (N = 58) compared to smaller tumors (N = 367), with the exception of a 6- to 8-minute increase in ischemic time.115 Central tumors resected laparoscopically were associated with increases in both ischemic and overall operative times, but not bleeding. An experienced surgeon can thus perform technically challenging laparoscopy with good surgical and oncologic outcomes.116
The advent of the daVinci robot has simplified the most difficult technical portion of the operation, namely intracorporeal suturing and reconstruction of the resection defect. This has translated to improvements in several key operative outcomes for minimally inva-sive partial nephrectomy, in addition to a quicker learning curve. In one experienced minimally invasive surgeon’s series of 492 laparo-scopic (N = 231) or robotic (N = 261) partial nephrectomies, the latter approach correlated with a significant reduction in operative time, ischemia time, positive margins, and perioperative complica-tions, despite greater patient comorbidity and tumor complexity.117 Other retrospective series indicate reduced blood loss with the robotic approach as well.118,119
The single remaining concern for laparoscopic and robotic nephron-sparing surgery is the amount of warm ischemic time and resulting loss of renal function. Precooling of the kidney prior to renal arterial clamping during open partial nephrectomy is believed to reduce ischemic injury but has thus far not been feasible with a laparoscopic approach. Warm ischemic times during laparoscopy in excess of 20 minutes have been suggested to result in irreversible injury. For this reason, complex resections, including large, endo-phytic or multifocal tumors, may require alternative methods, including either open resection using cold ischemia, or resection of the tumor without main renal artery clamping. The latter approach increases blood loss and the likelihood of transfusion, but optimizes preservation of renal function. Recently, renal hypoperfusion by pharmacologically induced hypotension has been proposed to avoid main renal artery clamping, but the safety and efficacy requires further study.120 Newer methods include superselective segmental renal artery clamping, with or without administration of near infra-red dyes to visualize clamping impact. Such strategies may allow resection without putting the entire kidney through an ischemic insult.121,122 However, immediate and long-term efficacy of these technical innovations are still under active investigation.
When open surgery is required, the choice of anatomic approach also is dictated by the surgeon’s training and experience, and by the location and extent of disease. Resection of tumors with thrombus extending into the inferior vena cava above the level of the hepatic veins usually is performed through a midline incision to allow exten-sion to a sternotomy, if required. Tumors with thrombus extending into the inferior vena cava, but below the hepatic veins, often can be accessed by a thoracoabdominal approach, if the primary lesion is on the right side. For other, less extensive tumors, laparoscopy is the preferred approach when nephrectomy is deemed necessary.
Although most laparoscopic surgeons prefer a transperitoneal (transabdominal) approach for this operation, many surgeons opt for a retroperitoneal approach. The difference in approach seems to matter relatively little to the patient, but rather is a technical issue for the surgeon. The transabdominal approach allows complete visu-alization of the viscera with multiple landmarks and visual cues for orientation, but does require more anterior and anteromedial dissec-tion. Surgery through the retroperitoneal approach can be faster in the hands of an experienced laparoscopic surgeon, but many visual cues and landmarks to ensure dissection in the proper planes are lacking with this procedure. Regardless of approach, however, current surgical practice in the United States is to perform nephrectomy robotically or laparoscopically (with or without hand assistance), except when an excessively large tumor, locally advanced disease, local adenopathy, or tumor thrombus is present. Even in these situations, it is often beneficial to start a case laparoscopically and then complete
deaths. This unexpected outcome has come under intense scrutiny and the study has been heavily criticized because of underaccrual and its intention-to-treat analysis with frequent study arm crossover. Perhaps unduly, these findings have been largely dismissed by the urology community.
With the standardization of staging and earlier diagnosis of the disease, a more tumor-specific surgical management has proved to be advantageous to maximizing the preservation of functional renal tissue. With increased evidence of the need for long-term dialysis in patients undergoing total nephrectomy, maintenance of renal func-tion in both kidneys represents the strongest argument for nephron-sparing surgery in patients with RCC who have the best chance for cure.
Surgical ApproachAn open incision has provided the traditional approach to resection of localized kidney cancers. More recently, laparoscopy has gained widespread popularity as a result of its potential for lower morbidity and faster convalescence. Whether an open or laparoscopic surgical approach is performed depends in large part on the extent of localized disease, including tumor size and location, and the training and experience of the surgeon. For lesions that appear to be locally exten-sive with potential involvement of neighboring organs, open surgery is still preferred, particularly if a colectomy, splenectomy, or distal pancreatectomy is anticipated. In addition, local adenopathy or tumor thrombus extension into the renal vein and vena cava provides a relative indication for open surgery. Even in such situations, however, laparoscopic and robotic resection may be possible, but should be reserved for specialists with experience in such techniques, as the morbidity can be quite high.
For cancers confined to the kidney requiring radical nephrec-tomy, a laparoscopic approach is generally preferred based on its tendency for lower blood loss, faster inpatient and outpatient recov-ery, and similar oncologic outcomes relative to an open approach, although these differences are inferred largely from retrospective comparisons.106-110 In a prospective randomized comparison between these two approaches among patients with tumors up to 8 cm, Burgess et al. found that laparoscopic radical nephrectomy achieved significantly better postoperative pain scores and convalescence, but no reduction in hospitalization.111
While laparoscopy is suitable for most radical nephrectomies, large renal tumors often are best approached in open fashion. In some instances, however, even large tumors can be approached laparoscopi-cally if the local anatomy is favorable, although intraoperative mobi-lization of the kidney may become more difficult. In a retrospective comparison of open and laparoscopic radical nephrectomy for T2 tumors with a mean size of 10 cm, Hemal et al. observed lower blood loss, less narcotic use, and quicker recovery with laparoscopy, at the expense of a longer mean operative time.112 In another retrospective study involving tumors larger than 7 cm, complications were more common with laparoscopic than open radical nephrectomy.103 Con-version from laparoscopy to open can be expected at higher frequency with large tumors. Gong et al. reported open conversion in 12% of laparoscopic nephrectomies for T2 tumors compared with only 1% for T1 tumors, although postoperative recovery was no different.114
In contrast to radical nephrectomy, the gold standard approach to partial nephrectomy remains an open incision. However, with increas-ing usage of minimally invasive therapies and enhanced dexterity afforded by robotic assistance, the indications for laparoscopy are expanding to include partial nephrectomy in select patients. Today, the choice between open and robotic or laparoscopic partial nephrec-tomy depends on anatomic location of the tumor, body habitus, and ability to tolerate pneumoperitoneum. The optimal tumor for lapa-roscopic partial nephrectomy is small (<4 cm) and peripheral/exophytic, although experienced laparoscopists may take on larger and more centrally located lesions. In a study from a single

1427CanceroftheKidney • CHAPTER82
ischemic injury caused by occlusion of the microvasculature during the thaw phase creates stasis within blood vessels, leading to end-tissue infarction. These ensuing insults to renal tissue lead to liquefac-tive necrosis.130
In most cases, the cryoprobes used are 2.4 mm in diameter. The usual procedure is percutaneous CT guidance cryotherapy, in which each lesion is treated with a double freeze–thaw cycle, with active freeze at 100% efficiency for a minimum of 10 minutes and a passive thaw of 8 minutes.128 These cycle times consistently deliver the lethal freeze of −4° C within 1 cm of the ice ball edge.128 The critical threshold for necrosis has been reported as between −19.4° C and −40° C.128 The number of probes used is specific to the size and shape of the lesion, with freeze margins of 0.5 to 1 cm of the lesion.
Advantages to CT-guided cryotherapy include general availability and its excellent capability to differentiate among the visceral organs. It also provides visualization of the entire ice ball while differentiating between frozen and unfrozen tissue. In addition, it provides real-time guidance in the CT fluoroscopy mode. One major disadvantage with CT guidance is the constant radiation exposure to the patient and the surgeon, which can be avoided with adequate and appropriate protection.
Numerous studies of cryoablation support adequate oncologic efficacy with short- and intermediate-term patient follow-up. However, there are at present sparse long-term data available. Gill and colleagues recently provided the first 10-year oncologic outcomes for cryotherapy using a laparoscopic approach. The mean tumor size was 2.3 cm and cancer specific survival at 10 years was 83%, com-parable but slightly lower than would be expected for surgical resec-tion of renal cancers of this size.135 Because the renal tumor is not excised and histopathological margins are unknown, whether the entire tumor has been extirpated remains uncertain.128 This challenge forces frequent CT and MRI follow-up studies on patients who receive this therapy.
Radiofrequency ablation (RFA) provides an alternative method of renal tumor ablation. This approach employs a 150- to 200-W gen-erator to create a high-frequency alternating current (460 to 500 Hz), causing frictional heating and protein denaturation. Electrode needles with or without tines are placed in the tumor laparoscopically or percutaneously under ultrasound or CT guidance. Temperatures of 60° C to 105° C are generated in the tumor, causing immediate cell death. Heating may be cycled, with each cycle approximately 5 to 12 minutes each. Probes may be inserted into the surrounding normal parenchyma for thermal monitoring. A margin of 0.5 to 1.0 cm is typically achieved.
Potential complications of RFA are similar to cryoablation, and include urinary leak/fistula, ureteral stricture or obstruction as a result of tissue sloughing, and injury to adjacent organs. Bleeding complica-tions are infrequently encountered with RFA and make this proce-dure an attractive option for poor surgical candidates on blood thinning medication. Allaf and colleagues reported increased pain with RFA compared to cryoablation, attributing this to a potential analgesic effect of the latter.136
As with cryotherapy, numerous studies now support effective short-to-intermediate–term oncologic efficacy of RFA; however, longer-term outcomes data are, at present, sparse.137-140 Psutka and colleagues documented oncologic outcomes for 185 RFA patients with a median tumor size of 3 cm and a median follow-up of 6.3 years. Only 2.2% and 1.6% of patients developed metastasis and died, respectively, although 8% and 24% of T1a and T1b patients, respectively, were not disease-free.141 The low rate of metastasis and death is promising, and validation of these longer-term outcomes is now awaited.
Active SurveillanceActive surveillance has emerged has an alternative approach to extir-pative or ablative management of small renal masses. Approximately
it in a controlled open fashion. Such a strategy can result in a smaller incision, often in the midline, with less pain and morbidity than if the entire case is performed in open fashion.
The common benefits of cosmesis and pain control with minimally invasive surgery is partly compromised during laparoscopic radical nephrectomy by the substantial skin/fascial incision needed to extract the kidney and surrounding Gerota’s fat en bloc. Some laparoscopists have accordingly advocated morcellation of the specimen as an alter-native to removing the kidney as a whole. An intact extraction has the benefit of maintaining kidney and tumor integrity for more precise histopathological evaluation, decreases the chance of tumor seeding of the port sites or renal fossa, and requires shorter surgery time.123 Pautler and colleagues compared the histopathological diagnosis of their operative needle biopsy before morcellation with the morcellated specimen.124 They found adequate histopathologic material for diag-nosis but were unable to stage most cases.124 Although it has been argued that lack of pathological tumor staging information does not affect management of the patient, the tumor stage is in fact the major determinant of current risk-based postoperative surveillance regi-mens.125 Hence, although there was initially great enthusiasm among the laparoscopic surgeons to remove the kidneys and tumors through morcellation, this practice has been abandoned and nearly all urologic surgeons now prefer intact extraction of the kidney and mass for accurate histopathological diagnosis and staging.
Thermal Ablation for Renal Cell CarcinomaUrologists pioneered minimally invasive surgery and have been con-stantly searching for less-invasive techniques. With the advent of energy-based ablative alternatives to open and laparoscopic surgeries in selected patients, it is now possible to achieve cancer-specific sur-vival with decreased surgical morbidity. Two types of ablation are currently performed, cryoablation and radiofrequency ablation. Although either can be performed laparoscopically under direct vision, ablation is most often performed percutaneously under ultra-sound or CT guidance. While the usefulness of ablative therapies is still being evaluated by many groups, the American Urological Asso-ciation consensus guidelines considers the efficacy of ablative tech-niques to be slightly less than surgical resection and should be reserved primarily for patients who decline surgery or who are not good surgi-cal candidates but who desire treatment.126
Renal cryoablation has been developed for the treatment of small renal tumors as an alternative to nephron-sparing surgery, with the goal of reducing operative morbidity. Use of standard cryoprobes of 3 to 8 mm can cause rupture of the renal capsule and parenchyma, resulting in significant bleeding. The use of multiple 2.4-mm cryo-probes under intraoperative real-time ultrasound guidance may decrease the risk of bleeding and make this technique a more feasible approach.127 Increasing evidence suggests that cryoablation is an acceptable surgical alternative to traditional open and laparoscopic nephrectomy.128-132 In addition to shorter hospital stay and less mor-bidity, cryoablation has been shown to be an effective nephron-sparing cancer therapy.132 Patients selected for this option tend to have peripheral lesions 5 cm or less in diameter.128-132 Minimally invasive therapy without the sequelae of open or laparoscopic surgery may be reasonable in these situations, particularly in morbid or elderly patients who are poor surgical candidates. Cryoablation surgery has been described in the literature with open, laparoscopic, and, more recently, imaging-guided percutaneous approaches.133,134
Multiple theories have been proposed for the mechanism of action of cryoablative surgery. The most accepted theory postulates direct cellular injury leading to coagulative necrosis.130,131 Injury to the cancer cells occurs as a result of intracellular ice crystal formation during the freezing phase of the treatment.130,131 The freezing process causes protein damage, which injures the cell membrane and essential enzymatic processes.130 Ice crystals that form within the cell disrupt intracellular organelles and membranes. Additionally, indirect

PartIII:SpecificMalignancies1428
reviewed data for 187 patients with pT1 to pT3 disease who under-went radical nephrectomy at their center.151 These investigators found that 80% of metastatic cancers were diagnosed within 3 years after surgery.151 It has been documented that Furman nuclear grade, TNM stage, ECOG status, and DNA ploidy are good predictors of tumor progression and tumor recurrence.159 T1 tumors recur between 38 and 45 months; T3 tumors recur between 17 and 28 months.159 Furman grades 1 through 4 tumors are associated with risk of metas-tasis of 9%, 61%, 79%, and 87%, respectively. Diploid tumors carry a decreased risk of recurrence compared with aneuploid tumors.151
Imaging for surveillance is based largely on risk of metastasis by anatomic site. The major metastatic sites, in order of frequency, include lung (3% to 16%), bone (2% to 8%), regional lymph nodes, liver (1% to 7%), ipsilateral adrenal, contralateral kidney, and brain (2% to 4%). Currently, a history and physical examination (H&P), serum studies (calcium level, alkaline phosphatase level, and liver transaminases), and imaging studies (chest plain radiographs or chest CT scan and abdominal CT scan) done at time points when disease recurrence is likely are used for surveillance.160 The lung has the great-est incidence of metastasis, so early diagnosis is pertinent.160 Chest radiography has been shown to detect up to 90% of lung metastases.159 Although chest CT is more sensitive than chest radiography, it yields more false positives, and its role in surveillance is still unknown.159 In the case of bone metastasis, however, only palliative therapies are available, therefore screening bone scintigraphy and radiographs are not warranted.160 Abdominal CT and liver transaminase determina-tion are an integral part of surveillance because of treatment options available for local recurrence or liver recurrence.160
Levy and coworkers have suggested a surveillance protocol based on TNM staging.150 For T1 disease, a 6-month H&P and serum studies are performed annually for 3 years. For T2 disease, 3-month H&P and semiannual chest radiographs and serum studies are per-formed; at 24 and 60 months an abdominal CT is recommended. For T3 disease, 3-month follow-up visits that include serum studies and chest x-ray are suggested. Then at 24 and 60 months, a CT scan of the abdomen is recommended. Close follow-up is suggested for T4 disease, including H&P, CT of the abdomen, chest radiographs, and serum studies every 3 months for 2 years and every 4 months for the third and fourth years. Complete follow-up is indicated semi-annually in year 5 and then annually.
Zisman and coworkers, in an attempt to standardize RCC staging and management protocol, developed the UISS, described earlier.161 This system incorporates histologic grade, ECOG status, and TNM stage to improve prognostication for RCC.161 With this system, they created a surveillance protocol for patients grouped according to recurrence risk. For the low-risk group, these investigators recom-mend H&P, serum laboratory studies, and chest CT scan annually. At 2 and 4 years after surgery, the patient should have an abdominal CT scan. The intermediate-risk group is recommended to have H&P, serum laboratory studies, and chest CT scan semiannually for 3 years and then annually for 10 years. They should also have an abdominal CT annually for 2 years and then every 2 years up to 10 years post-surgery. The high-risk group should have H&P, serum studies, and chest CT semiannually for 3 years and then annually for 10 years. These patients also should have an abdominal CT scan semiannually for 2 years and then annually for 5 years and then every 2 years up until 10 years. Throughout the protocol, after 3 years of surveillance, the chest CT can alternate with chest radiography.
According to the National Comprehensive Cancer Network (NCCN) guidelines, follow-up evaluation for patients with com-pletely resected disease includes abdominal and chest CT scans obtained approximately 4 to 6 months after the surgery to serve as baseline and then as clinically indicated. Patients are seen periodically, and each visit should include a history, physical examination, and comprehensive metabolic panel (i.e., determination of blood urea nitrogen, serum creatinine, calcium levels, lactate dehydrogenase, and liver enzymes).
30% of renal tumors are benign when 4 cm or less in diameter. Among small renal masses with malignant histology, the vast majority (75% to 85%) are low grade and clinically indolent. Hence, the American Urological Association now recommends consideration of active surveillance for small renal masses in select patients willing to accept a low risk of metastasis. Such management may be ideal for select patients with poor renal function or high operative risk, such as the elderly, or comorbid disease, and those with high tumor complexity.
The precise risk of metastasis with active surveillance is unclear, but appears to be around 1% to 2% based on current literature.142,143 However, follow up in these studies is mostly short- or intermediate-term only, thus this long-term rate may be an underestimate, particu-larly given the 5% to 10% rate of metastasis expected after surgical resection of pT1a tumors. In addition, reporting bias may further underestimate the rate of metastasis on active surveillance. During patient selection for active surveillance, the metastatic risk must be weighed in light of both the patient’s willingness to undergo treat-ment and the patient’s operative risk, including general health/performance status, renal function, and tumor complexity. Percutane-ous tumor biopsy at present does not play a routine role during patient selection, probably because of concerns of common under-grading and a historically high nondiagnostic rate, although accuracy of 80% to 90% is described in most contemporary biopsy series.
Presently, there are no standardized guidelines for surveillance regimens and thresholds for implementation of delayed treatment. A number of studies have attempted to identify clinical predictors of metastasis for patients on active surveillance, but are limited by low metastatic case number. In many cases of metastasis on active surveil-lance, the primary tumor has progressed to greater than 4 cm. Accordingly, tumor size may provide a useful trigger for intervention. Increasingly, tumor growth rate is also being used as a trigger. Although growth rate of small renal masses does not differ between malignant and benign tumors (0.2 to 0.3 cm/year), high-grade and particularly metastatic primary tumors appear to grow faster, with the latter ranging from 1.3 to 2.9 cm/year.142,144-147 A growth rate of more than 0.5 cm/year has accordingly been implemented by some urolo-gists as a threshold for intervention. This approach has been chal-lenged by the fact that oncocytomas commonly demonstrate rapid growth rates.148
SURVEILLANCE AFTER TREATMENT OF LOCALIZED RENAL CELL CARCINOMA
Sporadic Renal Cell CarcinomaA need has been recognized for standardization of surveillance pro-tocols after nephrectomy for sporadic RCC. Multiple surveillance protocols have been proposed.71,149-151 An important consideration in determining the appropriate frequency of surveillance imaging after surgery is the ability to provide curative or palliative salvage therapy. Because improved survival can be achieved for certain subsets of patients with recurrent disease, an active approach to surveillance is warranted. For instance, patients with solitary metachronous metas-tases treated aggressively with surgical resection have a 5-year survival rate of 20% to 44%.152-155 Extended survival (21 to 136 months) also can be achieved in as many as 33% of patients who undergo resection of an isolated local recurrence in the retroperitoneum.156,157 Follow-up imaging after curative therapy has been challenged on the basis of survival benefit and cost-effectiveness.158
No current randomized trials exist, so little evidence on the appro-priate follow-up after surgery is available. Too much surveillance places a financial and psychological burden on the patient, whereas too little surveillance may increase morbidity and mortality. Patients are risk stratified, and a follow-up schedule is determined on the basis of stage and grade of the disease. Most recurrence occurs within 3 to 5 years after nephrectomy.159 Ljungberg and colleagues prospectively

1429CanceroftheKidney • CHAPTER82
Adjuvant TherapiesA role for adjuvant therapy after nephrectomy remains to be estab-lished, and to date, observation remains the standard of care outside a clinical trial. Clinical studies with immunotherapies have failed to demonstrate a clinical benefit. One randomized, multicenter, pro-spective study has reported on the efficacy of adjuvant interferon alfa-2b given after nephrectomy to patients with Robson stages II and III RCC.173 Patients randomized to receive interferon alfa-2b were given a dose of 6 million IU intramuscularly 3 times per week for 6 months, starting within 1 month of surgery. Patients in the observation-only group who relapsed were given interferon alfa-2b, 10 million IU intramuscularly, 3 times per week, or the best available treatment at the time of relapse. Treatment groups were well matched at baseline for patient and tumor characteristics. No significant dif-ferences were observed in overall or event-free survival for patients randomized to management by observation (N = 124) and patients receiving interferon alfa-2b (N = 123). This study did not support the use of adjuvant interferon alfa-2b after nephrectomy. An analyzed and reported phase III study of interferon-α as adjuvant treatment for resectable RCC by the ECOG/Intergroup showed that adjuvant treatment with interferon did not contribute to better overall survival or relapse-free survival.174
As new drugs have become available for the treatment of meta-static disease, a rationale has arisen for testing these agents in micro-metastatic disease. A large, randomized, double-blind phase III study conducted by the ECOG (E2805) has been completed. Currently accruing patients who have undergone nephrectomy for kidney cancer. Patients with lesions staged as above T1c or Fuhrman grade of 3 or higher (or both) were randomly assigned to a placebo group or to either a sorafenib or sunitinib treatment group. Treatment was to continue for 1 year with close monitoring. The primary clinical end point was time to tumor progression among the three groups. The goal of this important study is to identify a possible role for VEGF receptor (VEGFR) TKI in the adjuvant setting; confirmation of a positive effect will establish a new standard of care after nephrec-tomy for patients with risk for recurrence. Additional adjuvant studies involving other antiangiogenic drugs are ongoing.
CYTOREDUCTIVE NEPHRECTOMY FOR PATIENTS WITH METASTATIC RENAL CELL CARCINOMAApproximately one third of patients diagnosed with RCC present with metastatic disease.175 The role of nephrectomy in patients with metastatic disease at the time of diagnosis has long been the subject of debate. A general consensus exists that noncurative nephrectomy is appropriate when symptoms produced by the primary tumor require palliation, when the metastatic tumor burden is less than that of the primary tumor, and when the patient wishes to receive treatment with high-dose IL-2. With the approval of multiple systemic targeted therapies, nephrectomy is now considered the standard of care in patients who are of good performance status with a resectable primary lesion and who are able to receive small molecule inhibitors for RCC.
Cytoreductive surgery with systemic therapy has been shown to induce clinical benefit.175 The Southwest Oncology Group (SWOG) conducted a randomized study in which patients who were acceptable candidates for nephrectomy either underwent radical nephrectomy followed by therapy with interferon alfa-2b (N = 120) or received interferon alfa-2b alone (N = 121). The primary end point was sur-vival, with objective response (OR) as the secondary end point. The patients were stratified by SWOG performance status (0 or 1), the presence or absence of lung metastases only, and the presence or absence of at least one measurable metastatic lesion in the region not to be resected. After randomization, patients either underwent imme-diate radical nephrectomy followed by interferon alfa-2b or were
Lifelong surveillance is necessary for patients with RCC. Late recurrence is arbitrarily defined as a recurrence more than 10 to 20 years after nephrectomy. In sporadic RCC, recurrences have been documented as long as 45 years after initial surgical resection.162 The appropriate intensity of follow-up after 5 years remains to be estab-lished. Approximately 85% of recurrences, however, will be detected in the first 3 years after resection of the primary.163
von Hippel-Lindau Disease and Other Familial Renal Cell CarcinomasPatients with von Hippel-Lindau RCC or other familial forms of RCC are at high risk for local recurrence after nephron-sparing surgery and require close lifelong surveillance. More than 80% of patients with von Hippel-Lindau disease treated with nephron-sparing surgical resection will have a recurrence in the ipsilateral kidney within 10 years, and lesions will develop in the contralateral kidney, if they have not done so already.164 This is because multiple microscopic lesions are present throughout the kidneys, despite the grossly normal appearance of the parenchyma.165 A diagnosis of von Hippel-Lindau disease should be considered in any patient with early onset or multifocal RCC or RCC in conjunction with the following: a history of visual or neurological symptoms; a family history of blindness, central nervous system (CNS) tumors, or RCC; or coexist-ing pancreatic cysts, epididymal lesions, or inner ear tumors.166,167 Standard recommendations for surveillance in patients with von Hippel-Lindau disease include (a) CT of the abdomen and pelvis every 6 months in patients with solid renal lesions and every 12 months in patients without solid renal lesions, with alternating MRI and CT in younger patients to avoid secondary malignancies associ-ated with prolonged use of the former, (b) annual physical and ophthalmologic evaluations, (c) estimation of urinary catecholamines every 1 to 2 years, (d) MRI of the CNS every 2 years, and (e) periodic auditory examinations. Molecular genetic and clinical screening should be offered to appropriate family members based on an autosomal-dominant pattern of inheritance.164,167,168
PERIOPERATIVE MEDICAL THERAPIES
Neoadjuvant TherapiesPresurgical approaches in RCC are currently under investigation based on the evidence that therapies targeting the VEGF axis have shown clinical benefit in the metastatic setting.169 The rationale for the use of VEGF inhibitors in this setting is to downsize locally advanced or nonresectable tumor and offer either organ-sparing surgery or radical nephrectomy, respectively. The use of antiangiogenic therapies perioperatively would also have a potential role in controlling early micrometastatic disease. To date, small, single-institution studies have shown that this approach appears feasible in terms of safety and may achieve meaningful tumor response.170,171
The presurgical approach is also being tested in the setting of cytoreductive nephrectomy to assess the response to antiangiogenics and determine the optimal candidates for debulking surgery. For example, a recent study assessed the safety and efficacy of presurgical bevacizumab in patients with mRCC. In this single-arm, phase II trial, patients received bevacizumab plus erlotinib (23 patients) or bevacizumab alone (27 patients) for 8 weeks followed by restaging. Forty-two patients underwent nephrectomy. Median progression-free survival and overall survival were 11 and 25.4 months, respectively. The conclusions from this study were that presurgical treatment with bevacizumab therapy yields clinical outcomes comparable with post-surgical treatment with antiangiogenic therapy in patients with mRCC, but it may result in wound-healing delays.172 At this time, a neoadjuvant therapeutic approach should only be considered in a clinical trial setting.

PartIII:SpecificMalignancies1430
involvement or recurrence in two or more sites was considered to constitute multiple sites. Surgery for metastatic disease was consid-ered curative if metastases were curatively resected and noncurative if gross tumor was left behind. Of the 278 patients who underwent initial curative nephrectomy, recurrence was solitary in 155 patients and multiple in 123 patients, with a median time to first recurrence of 25 months. The overall 5-year survival rate of patients who under-went curative resection for the first recurrence was 44% (N = 141), 14% for those who received noncurative resection (N = 70), and 11% for those who were treated nonsurgically (N = 67). Favorable predic-tors of survival by multivariate analysis included a single site of first recurrence, curative resection of the first metastasis, a disease-free interval of more than 12 months, and a metachronous presentation with recurrence. Curative resection of isolated metastases to glandular tissue (thyroid, salivary gland, pancreas, adrenal, ovary) was associ-ated with the best 5-year overall survival rate (63%), followed by resection of isolated lung metastases (54%). In this study, resection of solitary brain metastases, however, was associated with poor outcome, with an 18% 5-year overall rate. The 5-year overall survival rates of 46% and 44%, respectively, for patients who underwent second (N = 62) or third curative resection (N = 22) of subsequent metastases after initial curative metastasectomy were not significantly different from those for patients who received only initial curative metastasectomy (44%; N = 141). Thus patients who undergo com-plete resection of metastatic disease in a solitary site after a disease-free interval of longer than 12 months may experience long-term survival. As with previous reports, complete resection is the important factor, rather than the number of sites resected, even in patients who have undergone prior metastectomy.184,185
Brain metastases from RCC raise specific therapeutic problems because they are relatively unresponsive to whole-brain radiation therapy and tend to bleed. Stereotactically guided high-precision irradiation (radiosurgery) has shown promising results in selected patients with brain metastases from RCC.186 Radiosurgery appears attractive owing to its low risk of toxicity and minimal invasiveness. Multiple lesions can be treated at the same time, and retreatment can be performed for local or distant recurrences.
Lymphadenectomy in Locally Advanced DiseaseThe role of lymphadenectomy in RCC remains controversial. Nodal disease has been found to be a predictor of poor prognosis even with M0 disease, although, there is very little evidence to support the value of lymph node dissection.187-189 The decision for lymph node dissec-tion should be based on multiple factors. The need for accurate staging, decreased local recurrence rates, and improved survival should be weighed against risk of morbidity and mortality.187,190 One argument against lymph node dissection is that the kidney is drained hematologically and lymphatically through multiple pathways.187 Owing to the unpredictable pathways of spread accurate staging may not be possible. From 58% to 95% of patients with lymph node disease also have synchronous metastasis.191 consequently, the likeli-hood of finding patients with localized disease is low at 2% to 9%. Canfield and associates did a retrospective study supporting the need for aggressive nodal resection in the presence of positive lymph nodes without evidence of metastasis.191 Blom and coworkers of the EORTC Genitourinary Group conducted a large randomized trial comparing radical nephrectomy with lymph node dissection and radical nephrec-tomy alone.189 At 5-year follow-up evaluation, these workers found no significant difference in morbidity and mortality between the two groups after surgery. They also found no significant difference in survival. A small subset of patients may benefit from lymph node dissection. Pantuck and associates have shown improved survival in patients found to have disease-positive lymph nodes who undergo cytoreductive nephrectomy and postoperative immunotherapy.190 The literature is variable on the benefits of lymph node dissection in
immediately given interferon alfa-2b without surgery. Interferon alfa-2b was then continued until disease progression. The median survival time was 11.1 months for patients who received nephrec-tomy plus interferon alfa-2b, and 8.1 months for patients who received interferon alfa-2b alone (P = 0.05). Nonetheless, interpreta-tion of these data is difficult in light of the poor median survival seen in both arms of this study.176
The patients benefiting the most from cytoreductive surgery appear to be those who have a good ECOG performance status (0 or 1) and preferably with metastasis limited to the lungs.177 Risk and benefits, however, need to be weighed in the decision to perform cytoreductive surgery. Patients with poor performance status and a large metastatic disease burden (greater than the tumor in the kidney) are less likely to derive benefit from surgery. Frequently, patients with metastatic disease can undergo resection laparoscopically. This is always preferred when technically feasible, because it allows a shorter recovery interval until starting systemic therapy.
Mickisch and colleagues, in the EORTC randomized trial, com-pared radical nephrectomy plus immunotherapy with immunother-apy alone.178 These investigators found that nephrectomy plus immunotherapy delayed time to progression of the disease and improved survival. Bromwich and associates found a mean survival benefit of 4 to 10 months.179 Of the 268 patients selected for the study, only 20 (7%) were selected for cytoreductive nephrectomy. Owing to the associated risks of the surgery, recovery time, and adverse reactions of the immunotherapy, they concluded after careful patient selection that cytoreductive surgery may only be beneficial to a small segment of renal cell patients.
Rabets and coworkers compared outcomes data for laparoscopic and for open cytoreductive nephrectomy.180 The selection criteria for laparoscopic surgery were presence of lesions 15 cm or less in diam-eter and confined to the kidney. These investigators found no statisti-cally significant survival benefits between the surgical modalities. Laparoscopic nephrectomy was found to have fewer morbidities, including less operative blood loss and shorter hospital stay. They concluded that even with advanced disease, laparoscopic nephrec-tomy is a safe alternative to open nephrectomy in metastatic disease. With proper patient selection patients with mRCC may still benefit from laparoscopic surgery.175,177,180,181
Laparoscopic techniques offer the possibility of lower morbidity and faster recovery, to minimize the delay in starting treatment with systemic targeted therapy.
A recent retrospective study reviewed baseline characteristics and outcomes of 314 patients with mRCC to assess the impact of cyto-reductive nephrectomy on overall survival. (The impact of cytoreduc-tive nephrectomy on survival of patients with mRCC receiving VEGF-targeted therapy.182 The authors concluded that cytoreductive nephrectomy was independently associated with prolonged overall survival (19.8 months vs. 9.4 months) favoring the patients who underwent surgery and received subsequent anti-VEGF therapies. An ongoing randomized trial (CARMINA study) is randomizing patients with newly diagnosed mRCC to either undergo surgery and then sunitinib treatment or directly to sunitinib and it will hopefully answer the question whether cytoreductive nephrectomy should remain the standard of care in the TKI’s era.
Resection of Metastases in Renal Cell CarcinomaResection of solitary metastases from RCC is associated with improved survival, although the selection criteria have been poorly defined. This issue was addressed in a retrospective, single-institution analysis of patients with recurrent RCC (N = 278) at the Memorial Sloan-Kettering Cancer Center.183 Recurrent disease was defined as solitary if it recurred within the resected renal bed or if one organ system or site was involved. Multiple unilateral lesions in the lung were consid-ered to represent a solitary site of metastasis. Bilateral lung

1431CanceroftheKidney • CHAPTER82
intravenous IL-2 should remain the preferred therapy for appropri-ately selected patients with access to such therapy. In view of the toxicity and limited efficacy of high-dose intravenous IL-2 therapy, however, additional efforts should be directed at better defining the patient population for whom this therapy is appropriate.200
Use of interferon-α as a single agent has resulted in only a modest survival benefit in the randomized setting, although combination of this agent with low-dose IL-2 (and perhaps with fluorouracil) may lead to an improved response rate, but evidence of survival benefit in a prospective randomized trial is lacking.201-203 Although interferon-α has been the outpatient treatment of choice in most of Europe and the United States until recently, benefit again appears to be restricted to patients with good prognostic risk.204
Predictors of Response to Cytokine TherapiesResponses to immunotherapy most frequently are seen in patients with RCC of clear cell histology.205-208 This observation was detailed in a retrospective analysis of pathology specimens obtained from 231 patients (163 primary and 68 metastatic tumor specimens) who had received IL-2 therapy in Cytokine Working Group clinical trials.208 For patients with primary tumor specimens available for review, the response rate to IL-2 was 21% (30 of 146) for patients with clear cell histology primary tumors, compared with 6% for patients with non-clear cell histology (1 responder in 17 patients). Among the patients with clear cell carcinoma, response to IL-2 was also associated with the presence of alveolar features and the absence of papillary or granular features. The response rate in patients whose primary tumors had “good” predictive features (e.g., greater than 50% alveolar and no granular or papillary features) was 39% (14 of 36). Patients with tumors that contained “poor” predictive features (e.g., greater than 50% granular or any papillary features) had a response rate of 3% (1 of 33). When this model was then applied to the 68 patients with specimens from metastatic sites, those patients who were treated without resection of their primary tumors, five tumor responses were seen in the 20 patients with “good” predictive features, whereas no tumor responses were seen in the 16 patients in the “poor” predictive group, thus supporting the validity of the model developed from the primary kidney tumor specimens. As a result of these data, it may be appropriate for patients whose primary tumor is of non–clear cell histologic type, or of clear cell histologic type but with “poor” predic-tive features, to forgo IL-2-based treatment altogether. Even in the most favorable predictive group, however, more than 50% of patients failed to respond to IL-2 therapy, so additional investigations to identify tumor-associated predictors of responsiveness to IL-2 are still necessary.205
Some investigators have begun to examine tumor tissue to identify immunohistochemical markers that may predict the outcomes for patients with RCC. Carbonic anhydrase IX (CAIX) has been identified as one potential marker. Bui and colleagues used a mono-clonal antibody designed to detect CAIX expression to perform an immunohistochemical analysis of paraffin-embedded RCC speci-mens. These investigators showed that greater than 90% of RCCs express CAIX, and that its expression decreases with advancing stage.209 In their analysis, high CAIX expression in primary tumors was seen in 79% of patients and was associated with improved sur-vival and possibly improved response to IL-2-based therapy. Building on this work, Atkins and coworkers performed a nested case-control study within the larger cohort of patients for whom the histopatho-logical findings were analyzed.210 CAIX expression levels were cor-related with response to IL-2, pathological risk categorization, and survival. Median survival times were 3 years and 1 year for high and low CAIX expressors, respectively. Although tumor response was seen in six patients with low CAIX staining, survival beyond 5 years was seen only in the patients with high-CAIX–expressing tumors. High-CAIX staining was associated with better histopathological features but remained an independent predictor of response. Additional
patients with renal neoplasms. Overall, lymphadenectomy provides little staging information and confers no clear benefit in decreasing risk of recurrence or in survival.
Immunotherapies for Advanced DiseaseHigh-Dose Interleukin 2Inpatient high-dose bolus IL-2 received FDA approval for treatment for patients with stage IV RCC in 1992 based on data presented on 255 patients who were entered into seven phase II clinical trials.192,193 In these studies, patients received 600,000 to 720,000 IU/kg of recombinant human IL-2 by 15-minute infusion every 8 hours during two 5-day courses (maximum: 14 doses per course) separated by 5 to 9 days of rest. Stable or responding patients received 2 to 5 courses of therapy at 8- to 12-week intervals and then were observed while not receiving any additional therapy. ORs were seen in 37 (15%) of the 255 patients, including 17 complete responses (CRs; 7%) and 20 partial responses (PRs; 8%). The median duration of response was 54 months for all of the responders and 20 months for partial responders; the median has not yet been reached for complete responders. The median survival was 16 months for all 255 patients. Most patients who achieved a CR that lasted longer than 30 months and those with PRs after resection resulting in “no evidence of disease” after a response to high-dose IL-2 were unlikely to experience disease progression and may actually be cured.
Although the inpatient high-dose bolus IL-2 regimen produces favorable outcomes in a handful of patients, it also is associated with significant toxic effects and cost and is not universally available. Low-dose IL-2 regimens (with or without interferon-α) have produced similar response rates and survival in nonrandomized phase II trials, but responses appeared to be less durable than those seen with high-dose IL-2.194-197
In an effort to determine the value of outpatient subcutaneous IL-2 and interferon-α relative to high-dose intravenous IL-2, the Cytokine Working Group did a phase III trial in which patients were randomized to receive either outpatient IL-2 and interferon-α every 6 weeks or standard high-dose inpatient IL-2 every 12 weeks.198,199 Of the 193 patients who were enrolled, 192 were evaluable for toxic-ity and tumor response. The response rate for high-dose IL-2 was 23%, versus 10% for IL-2 and interferon-α. Eight patients achieved a CR while taking high-dose IL-2, versus only three patients taking low-dose IL-2 and interferon-α. The median response durations were 24 months for high-dose IL-2 and 15 months for IL-2 and interferon-α. Median overall survival times were 17.5 and 13 months, favoring high-dose IL-2. Ten patients (nine major responders) who received high-dose IL-2 were progression free at 3 years, versus three patients (two major responders) who received IL-2 and interferon-α. Of note, responses to high-dose IL-2 were seen with equal frequency across the stratification criteria, whereas low-dose IL-2 and interferon-α seemed to produce fewer responses in patients with liver or bone metastases and in those who had not undergone prior nephrectomy to remove the primary tumor. For patients with bone or liver metastases, or with unresected primary tumor, survival was superior with high-dose IL-2 compared with IL-2 and interferon-α, whereas no significant survival differences between the two treatments were noted for patients who had undergone prior nephrectomy or who were without bone or liver metastases.
Taken together, these studies suggest that high-dose intravenous bolus IL-2 is superior in terms of response rate and possibly response quality to regimens that involve either low-dose IL-2 and interferon-α, intermediate- or low-dose IL-2 alone, or interferon-α alone.199 The superiority of high-dose IL-2 is particularly apparent in patients with tumor metastases in immune-sequestered sites, such as liver or bone, or whose primary tumor has not been resected, or who fall into the intermediate-risk or poor-risk group defined by the French Immuno-therapy Group. Consequently, although low-dose cytokine therapy has a limited role in mRCC, it must be concluded that high-dose

PartIII:SpecificMalignancies1432
Two subsequent multicenter phase I clinical trials with anti–PD-1 (BMS-936558)217 and anti–PD-L1 (BMS-936559)218 antibodies were carried out in a large cohort of patients with several types of highly refractory cancers. Two hundred and ninety-six patients enrolled in the anti–PD-1 study were intravenously administered a 1 to 10 mg per kilogram dose of anti–PD-1 antibody every 2 weeks for up to 12 cycles (2 years) or until a CR or disease progression occurred. The study was designed to assess the safety, antitumor activity, and pharmacokinetics of BMS-936558. Cumulative response rates among patients with RCC was 27% (9 of 33 patients), with ORs in 4 of 17 patients (24%) treated with 1 mg/kg and 5 of 16 (31%) treated with 10 mg/kg. Stable disease lasting 24 weeks or more was observed in 9 patients (27%) and 5 of 8 patients (63%) with ORs had a response that lasted 1 year or more. Adverse events reported in all patients were primarily immune-related, with 41 of the 296 (14%) patients exhibit-ing serious toxicities, including thyroid abnormalities, colon inflam-mation, and three deaths from pneumonitis. The majority of the patients had less severe toxicities, such as rash, fatigue, and itching.
Interestingly, immunohistochemical analysis of PD-L1 in tumor specimens of patients in the anti–PD-1 trial showed a positive rela-tionship between PD-L1 expression on tumor cells and OR (36% of patients with PD-L1 positive tumors exhibited tumor shrinkage as compared to none of the patients with PD-L1 negative tumors), suggesting that the expression of this molecular marker could poten-tially be used to predict clinical response.
The companion multicenter phase I clinical trial (CA210-001) with the anti–PD-L1 antibody (BMS-936559)218 included 207 patients with advanced disease, with 17 of the participants having RCC. The objectives of the study were to assess the safety, pharma-cokinetics, and antitumor activity of BMS-936559. Participants were intravenously administered escalating doses of the anti–PD-L1 anti-body ranging from 0.3 to 10 mg per kilogram every 2 weeks for up to 16 cycles or until disease progression or a CR occurred. Two of 17 (12%) of these patients had an OR, all lasting 4 to 17 months, with seven of the 17 (41%) having stable disease lasting at least 24 weeks, and the rate of progression free survival at 24 weeks at 53%. Patients obtained a durable response across multiple tumor types without significant toxicity, with most adverse events being grade 1 or 2. Grade 3 or 4 events occurred in only 19 of the 207 (9%) patients.
The positive results generated from the two phase I studies led to a randomized, blinded, phase II dose-ranging anti–PD-1 (BMS-936558, nivolumab) trial (NCT01354431) that has enrolled 150 patients with metastatic clear cell RCC who have received prior antiangiogenic therapy. Participants were administered 0.3 mg/kg, 2.0 mg/kg, or 10.0 mg/kg of nivolumab intravenously every 3 weeks until toxicity or progressive disease occurs. The study was designed to measure progression-free survival, tumor response rate, and overall survival across the three treatment arms. The results from this study are still pending. A randomized phase III study comparing everolimus and nivolumab in patients who have progressed on TKIs is currently accruing patients.
The data from these and other studies suggest that antibody-mediated blockade of CTLA-4 and PD-1 holds a promise as an important immunotherapeutic approach in RCC and that the effec-tiveness of this type of therapy could potentially be further enhanced by combining it with other anticancer treatments, including cyto-kine, vaccine, and VEGF-targeted therapies. A phase I study combin-ing nivolumab with sunitinib, pazopanib, or ipilimumab in subjects with mRCC is currently accruing patients (NCT01472081).
FDA-APPROVED DRUGS FOR RECURRENT RENAL CELL CARCINOMA
Angiogenesis InhibitorsInhibiting the development of new blood vessels (antiangiogen-esis) has been demonstrated as a valid approach to cancer
studies to explain these preliminary observations and correlate results with previously described clinical features are necessary.205
The Cytokine Working Group has completed the high-dose IL-2 “Select” Trial. The primary objective of this study was to determine, in a prospective fashion, if the predictive model proposed by Atkins and associates can identify a group of patients with advanced RCC who are significantly more likely to respond to high-dose IL-2-based therapy (“good” risk) than a historical, unselected patient population. New factors (including baseline immune function, immunohisto-chemical markers, and gene expression patterns) that might be associ-ated with response to high-dose IL-2 therapy have been explored in an attempt to more narrowly limit the application of IL-2 to those patients most likely to benefit.205
In this multicenter prospective study, patients with histologically confirmed RCC that was metastatic or unresectable, ECOG PS 0 to 1 and adequate organ function received high-dose IL-2 (600,000 U/kg/dose intravenously every 8 hours on days 1 through 5 and 15 to 19 [maximum 28 doses] every 12 weeks). The primary end point of the study was to determine the major response rate and associated “good” predictive features. One hundred twenty eligible patients were accrued between 2007 and 2009. The majority of patients (approximately 70%) had an ECOG performance status of 0 and were Memorial Sloan-Kettering Cancer Center intermediate risk. At the time of the analysis the investigator assessed, relative risk was 30% in clear cell RCC with six complete remissions. Response to IL-2 was not associated with any pretreatment clinical factor and was not seen in patients with non–clear cell histology. Preliminary analysis of CAIX staining did not show correlation with outcome. Additional analyses are still ongoing.211
IMMUNOCHECKPOINT INHIBITORSCytotoxic T-lymphocyte antigen 4 (CTLA-4), a key negative regula-tor of T-cell responses, has been shown to impair antitumor immune response. Ipilimumab (MDX-010) is a fully human, monoclonal antibody that, by inhibiting CTLA-4, overcomes T-cell suppression to enhance the immune response against tumors. A phase II study of ipilimumab was conducted in patients with metastatic renal cell cancer with a primary end point of OR.212 Patients enrolled in two sequential cohorts received either 3 mg/kg followed by 1 mg/kg or 3 mg/kg every 3 weeks. Major toxicities observed were enteritis and endocrine deficiencies. Five of 40 patients at the higher dose had partial responses and did not have prior response to IL-2. One-third of the patients experienced a grade III or IV immune-mediated toxic-ity with significant association between autoimmune events and tumor regression.
The programmed death-1 (PD-1) pathway has emerged as a promising immune-checkpoint–targeted cancer therapy. The pathway includes two principal components, PD-1 and PD-L1. PD-1 (B7-1) is an inhibitory T-cell receptor expressed on the surface of activated T-cells that was first discovered in 1992 by Honjo and colleagues,213 and has since been shown to play an integral role in modulating immune response and in long-term antigen exposure, as occurs in cancer.214 PDL-1 (programmed death ligand-1, also known as B7-H1 and CD274) is a PD-1 ligand found primarily in the tumor micro-environment that has been shown to be highly expressed in aggressive RCC tumors215
When PD-1 and PDL-1 bind together, the ability of the T-cell to target and lyse the tumor cell is dampened, thus blockade of interac-tions between PD-1 and PDL-1 can stimulate an immune response against tumor cells. The first phase I multiinstitutional, open-label, dose-escalation clinical trial with a fully humanized immunoglobulin G4 anti-PD-1 antibody (MDX-1106, also known as ONO-4538 and BMS-936558) was reported by Brahmer and colleagues in 2008216 and showed safety, tolerability, and clinical efficacy in patients with advanced RCC and other cancers that provided impetus for other studies.

1433CanceroftheKidney • CHAPTER82
twice daily were diarrhea, fatigue, and skin toxicity.222,223 A multi-center, placebo-controlled, randomized, discontinuation trial was performed to determine whether sorafenib inhibits tumor growth in patients with metastatic solid tumors who maintain stable disease after a 12-week run-in period.224 Patients initially received oral sorafenib 400 mg twice daily during the initial period. After 12 weeks, patients with changes in bidimensional tumor measurements that were less than 25% from baseline were randomly assigned to receive sorafenib or placebo for an additional 12 weeks; patients with 25% or greater tumor shrinkage continued open-label sorafenib treat-ment; patients with 25% or greater tumor growth discontinued treat-ment. The primary end point was the percentage of randomly assigned patients remaining progression free at 24 weeks after the initiation of sorafenib. Of 202 patients who received treatment during the run-in period, 73 patients had tumor shrinkage of 25% or greater. Sixty-five patients with stable disease at 12 weeks were randomly assigned to receive sorafenib (N = 32) or placebo (N = 33). At 24 weeks, 50% of the patients in the sorafenib treatment group were progression free, versus 18% of those in the placebo group. Median progression-free survival from randomization was sig-nificantly longer with sorafenib (24 weeks) than with placebo (6 weeks). Median overall progression-free survival was 29 weeks for the entire population of patients with RCC (N = 202). Sorafenib was readministered in 28 patients whose disease progressed during placebo treatment; these patients continued on sorafenib until further pro-gression, for a median period of 24 weeks. Common adverse events were skin rash or desquamation, hand-foot skin reaction, and fatigue; 9% of patients discontinued therapy, and no patients died from toxic-ity. These data supported the conclusion that sorafenib has significant disease-stabilizing activity in mRCC carcinoma and is tolerable with chronic daily therapy.
therapy—particularly for RCC. The discovery of the VHL gene–HIF-1α connection in kidney cancers has further intensified interest in drug development for approaches aimed at the disruption of angiogenesis in the treatment of RCC.
Thus far, VEGF is the best-characterized proangiogenic factor. It is virtually ubiquitous in human tumors, and higher levels have been correlated with more aggressive disease in kidney cancer. VEGF-A is a potent stimulator of angiogenesis because its binding to VEGF receptors (VEGFRs) has been shown to promote endothelial cell migration and proliferation, two vital features required for the devel-opment of new tumor-induced blood vessels. In addition, VEGF-A increases vascular permeability, which also may contribute to angio-genesis and tumor growth. HIF-1α regulates the activation of VEGF gene expression. Several approaches are being taken to block the HIF-1/VEGF axis (Fig. 82-2). Clinical efficacy of antiangiogenic therapy in RCC has led to the recent approval of five antiangiogenesis drugs by the FDA for the treatment of advanced kidney cancer (Fig. 82-3, Table 82-3).
SorafenibSorafenib (BAY 43–9006) is an oral kinase inhibitor targeting both tumor cells and the tumor vasculature. It was originally developed as an inhibitor of Raf-1, a member of the Raf/MEK/ERK signaling pathway.219,220 Sorafenib was subsequently found to have activity against B-Raf, VEGFR-2, platelet-derived growth factor receptor (PDGFR), Fms-like tyrosine kinase-3 (Flt-3), and stem cell growth factor (c-Kit).221 In phase I studies investigating various oral dosing schedules, sorafenib generally was well tolerated; the recommended dose for future trials was 400 mg twice daily continuously. Dose-limiting toxic effects seen at continuous doses higher than 400 mg
Figure 82-2 • Molecular targets for clear cell RCC. Several steps in the process of tumor angiogenesis are being targeted for therapeutic purposes. Depicted are both the drugs already approved and some of the agents in clinical development.
TemsirolimusEverolimus
Pericytesurvival
Plasmamembrane
Bevacizumab
EverolimusTemsirolimus
Endothelial/Tumor cellsurvival
Endothelial/Tumor cellproliferation/Genetranscription
Vascularpermeability
Sorafenib
SunitinibSorafenib
AxitinibPazopanib
Intracellular
Extracellular
BKM120
Dovitinib
BEZ235
Cabozantinib
Aflibercept
Vorinostat
Tivozanib
Akt/PKB
P13K
Casp 9
BAD
eNOS
P P
P P
P P
P P
P P
P P
P P
P P
PDGF
PDGFR VEGFR c-MET
FGFHGF
VEGF
Tumor suppressor gene silencing/hypoxia
mTOR
RAF
MEK
ERK
RAS
SPK
PKC
PLC�
PDGF FGF
FGFR
VEGF HGF

PartIII:SpecificMalignancies1434
progression-free survival in January 2005 showed a statistically sig-nificant benefit of sorafenib over placebo. Consequently, crossover was permitted from placebo to sorafenib, beginning in May 2005. Partial responses were reported as the best response in 10% of patients receiving sorafenib and in 2% of those receiving placebo. Diarrhea, rash, fatigue, and hand-foot skin reactions were the most common adverse events associated with sorafenib. Hypertension and cardiac ischemia were rare serious adverse events that were more common in
The positive results from the phase II study led to a phase III randomized, double-blind, placebo-controlled trial of sorafenib in patients with advanced clear cell RCC.225 From November 2003 to March 2005, 903 patients with RCC that was resistant to cytokine therapy were randomly assigned to receive either continuous treat-ment with oral sorafenib (at a dose of 400 mg twice daily) or placebo. A total of 451 patients received sorafenib; 452 received placebo. The primary end point was overall survival. A single planned analysis of
Figure 82-3 • National Comprehensive Cancer Network (NCCN) 2012 guidelines for the treatment of metastatic renal cell carcinoma (RCC). NCCN treatment guidelines show the incorporation of approved antiangiogenic agents into standard treatment regimens. IFN, Interferon; IL-2, interleukin-2. *Tem-sirolimus indicated for poor-prognosis patients, defined as those with three or more predictors of short survival. †Best supportive care can include palliative radiation therapy, metastasectomy, or bisphosphonates for bone metastases. (Adapted from The NCCN Kidney Cancer Guideline. Clinical Practice Guidelines in Oncology [Version 2012]. © 2012 National Comprehensive Cancer Network, Inc. Available at: http://www.nccn.org. Accessed December 30,2012. To view the most recent and complete version of the guideline, go online to www.nccn.org.)
First-Line Therapy Subsequent Therapy
Predominantclear cellhistology
Progression
Non–clear cellhistology
Relapseor
Metastatic RCCor
Unresectable RCC
Clinical trialorSunitinib (category 1)orTemsirolimus for poor-prognosispatients* (category 1)orBevacizumab + IFN (category 1)or Pazopanib (category 1)High dose IL-2 for selected patientsorSorafenib for selected patientsandBest supportive care†
Clinical trialorTargeted therapy:
orCytokine therapy
andBest supportive care†
• After tyrosine kinase inhibitor therapy
• IL-2 (category 2B)
• Everolimus (category 1)• Axitinib (category 1)• Sorafenib (category 2A)• Sunitinib (category 2A)• Temsirolimus (category 2B)• Bevacizumab (category 2B)• Pazopanib (category 3)
• After cytokine therapy• Axitinib (category 1)• Sorafenib (category 1)• Sunitinib (category 1)• Pazopanib (category 1)• Temsirolimus (category 2A)• Bevacizumab (category 2A)
Clinical trial (preferred)orTemsirolimus (category 1 for poor prognosis,*category 2A for other risk groups)orSorafeniborSunitinibPazopanib (category 3)orErlotinib (category 3)orAxitinib (category 3)andBest supportive care†
1st-LineTherapy
Setting Phase III data Alternative
2nd-LineTherapy
PriormTOR inhibitor Clinical trials
Clinical trials
Sunitinib
Temsirolimus
Pazopanib
PazopanibBevacizumab - IFN�
Sunitinibor Bevacizumab
Sunitinib
HD IL-2
Sorafenib
Axitinib
Axitinib
Everolimus
Good orintermediate
risk
Poor risk
Prior cytokine
Prior VEGFRinhibitor

1435CanceroftheKidney • CHAPTER82
weeks without treatment) or interferon-α at a dose of 9 million U given subcutaneously 3 times weekly.227 The primary end point was progression-free survival. Secondary end points included the OR rate, overall survival, patient-reported outcomes, and safety. The median progression-free survival was significantly longer in the sunitinib group (11 months) than in the interferon-α group (5 months), cor-responding to a hazard ratio of 0.42. Sunitinib was also associated with a higher OR rate than was interferon-α. The proportion of patients with grade 3 or 4 treatment-related fatigue was significantly higher in the interferon-α treatment group, whereas diarrhea was more frequent in the sunitinib group. Patients in the sunitinib group reported a significantly better quality of life than did patients in the interferon-α treatment group. Progression-free survival was longer and response rates were higher in patients with metastatic renal cell cancer who received sunitinib than in those receiving interferon-α. Update analysis of the phase III study showed that sunitinib induced a longer survival compared to interferon-α plus improvement in response and progression-free survival in the first-line treatment of patients with mRCC, highlighting an improved prognosis in patients with clear cell RCC in the era of targeted therapies.228
BevacizumabBecause of the mechanistic link between VEGF overexpression and VHL inactivation in clear cell RCC, a randomized, placebo-controlled, double-blind study of bevacizumab in patients with mea-surable metastatic clear cell RCC was conducted.229,230 The two bevacizumab doses selected were 3 mg/kg (predicted by pharmacoki-netics to produce a serum level equal to the optimally effective level in nude mice bearing human tumor xenografts) and 10 mg/kg (the
patients receiving sorafenib than in those receiving placebo. As com-pared with placebo, treatment with sorafenib prolonged progression-free survival in patients with advanced clear cell RCC in whom previous therapy has failed. On the basis of these data, the FDA approved sorafenib in December 2005 for the treatment of advanced kidney cancer.
SunitinibSunitinib (SU11248) is a multitargeted receptor TKI of VEGFRs and PDGFRs. Patients with mRCC who demonstrated progression on first-line cytokine therapy were enrolled into a multicenter phase II trial.226 SU11248 monotherapy was administered in repeated 6-week cycles of daily oral therapy for 4 weeks, followed by 2 weeks off. Overall response rate was the primary end point, and time to progres-sion and safety were secondary end points. Twenty-five (40%) of 63 patients who received SU11248 achieved PRs; 17 additional patients (27%) demonstrated stable disease with duration of 3 months or longer. Median time to progression in the 63 patients was 8.7 months. Dosing generally was tolerated well, with manageable toxicities. SU11248 demonstrated antitumor activity in mRCC as second-line therapeutic agent. Based on the phase II study results, the FDA approved sunitinib for the treatment of advanced kidney cancer in early 2006.
Because sunitinib has shown activity in two uncontrolled studies in patients with mRCC, a comparison of the drug with interferon-α in a phase III trial was warranted. A total of 750 patients with previ-ously untreated, mRCC were enrolled in a multicenter, randomized phase III trial to receive either repeated 6-week cycles of sunitinib (at a dose of 50 mg given orally once daily for 4 weeks, followed by 2
Table 82-3 Efficacy of Approved Targeted Therapies for mRCC in Pivotal Phase III Clinical Trials
Sorafenib SunitinibBevacizumab + IFN-α Temsirolimus Everolimus Pazopanib Axitinib
Patient population
Clear cell mRCC; PD after 1 systemic therapy
Clear cell mRCC; no previous systemic therapy
AVOREN and CALGB 90206; clear cell mRCC; no prior systemic therapy
Poor-prognosis mRCC; no prior systemic therapy
Clear cell mRCC; prior VEGFR TKI therapy
Advanced RCC/mRCC; with or without prior cytokine-based systemic therapy
Advanced RCC/mRCC; prior VEGFR TKI, cytokine-based systemic therapy
Comparator Placebo IFN-α A, IFN-α + placebo; C IFN-α
INF-α Placebo Placebo Sorafenib
PFS COMPARATOR, MONTHS
Median 5.5 vs. 2.8 11 vs. 5 A, 10.2 vs. 5.4; C, 8.5 vs. 5.2
T, 3.8 vs. 1.9; T + IFN, 3.7 vs. 1.9
4.9 vs. 1.9 9.2 vs. 4.2 6.7 vs. 4.7
HR (95% CI) 0.44 (0.35–0.55)
0.42 (0.32–0.54)
A, 0.63 (0.52–0.75); C, 0.71 (0.61-0.83)
NR 0.33 (0.25–0.43)
0.46 (0.34–0.62)
0.67 (0.54–0.81)
ORR versus comparator, %
~10 vs. 2 47 vs. 12 A, 31 vs. 13; C, 25.5 vs. 13.1
T, 8.6 vs. 4.8; T + IFN, 8.1 vs. 4.8
1.8 vs. 0 30 vs. 3 19 vs. 9
OS VERSUS COMPARATOR, MONTHS
Median 17.8 vs. 15.2
26.4 vs. 21.8
A, 23.3 vs. 21.3; C, 18.3 vs. 17.4
T, 10.9 vs. 7.3; T+IFN, 8.4 vs. 7.3
14.8 vs. 14.4 Not reached Not available yet
HR (95% CI) 0.88 (0.74–1.04)
0.818 (0.669–0.999)
A, 0.91 (0.76–1.10); C, 0.85 (0.74–1.01)
T, 0.73 (0.58–0.92); T + IFN, 0.96 (0.76–1.20)
0.87 (0.65–1.17)
A, AVOREN, C, CALGB (Cancer and Leukemia Group B); CI, confidence interval; HR, hazard ratio; IFN-α, interferon-α; mRCC, metastatic renal cell carcinoma; NR, not reported; ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; T, temsirolimus; TKI, tyrosine kinase inhibitor; VEGFR, vascular endothelial growth factor receptor.

PartIII:SpecificMalignancies1436
on bevacizumab plus interferon-α had a significantly improved progression-free survival and overall survival versus patients without hypertension.233
Both studies demonstrated that the combination of bevacizumab with interferon-α as first-line treatment in patients with mRCC results in a significant improvement in progression-free survival, com-pared with interferon-α alone.
PazopanibPazopanib is a potent and selective multitargeted receptor TKI (of VEGFR-1, VEGFR-2, VEGFR-3, PDGFR-α/β, and c-Kit) that blocks tumor growth and inhibits angiogenesis. In a phase II random-ized discontinuation trial, the effects of pazopanib on tumor growth in patients with RCC was assessed after 12 weeks of treatment.234 Patients with cytokine-naive and cytokine-refractory (as indicated by failure to respond to 1 previous cycle of a cytokine- or bevacizumab-containing regimen) RCC, ECOG stages 1 and 2, were enrolled. Pazopanib 800 mg was given orally once daily. In the first 60 patients, response at week 12 by independent review showed PR in 24 (40%); stable disease in 25 (42%); disease progression in 5 (8%); unknown response in 2 (3%); and withdrawal before week 12 in 4 (7%). On the basis of findings on investigator review at week 12, 27 (45%) patients were randomized for treatment. Total disease control rate was 82% (PR plus stable disease). Approximately 67% of patients were treatment naive, and the remaining 33% had failed to respond to one previous treatment regimen. Most common adverse effects or labora-tory abnormalities in all patients were alanine and aspartate amino-transferase elevations, diarrhea, fatigue, nausea, hair depigmentation, and hypertension. Grade 3 or 4 adverse effects occurred in 26% of patients; most common were hypertension (8%) and an increase in alanine transaminase (8%). Interim analysis of findings in this phase II study demonstrated that pazopanib treatment resulted in a PR rate at week 12 of 40% among patients with RCC and an acceptable toxicity profile.
A randomized, double-blind, placebo-controlled, phase III study evaluating the efficacy and safety of pazopanib in 435 treatment-naive and cytokine-pretreated patients with advanced RCC was recently completed.235 Data showed that progression-free survival was signifi-cantly prolonged with pazopanib compared with placebo in the overall study population (median: 9.2 months vs. 4.2 months), in the treatment-naive subpopulation (11.1 months vs. 2.8 months), and in the cytokine-pretreated subpopulation (median: 7.4 months vs. 4.2 months). The OR rate was 30% with pazopanib compared with 3% with placebo. The most common adverse events were diarrhea, hyper-tension, hair color changes, nausea, anorexia, and vomiting. The final analysis showed that the difference in final overall survival between pazopanib- and placebo-treated patients was not statistically signifi-cant (22.9 months vs. 20.5 months, respectively). However, the cross-over from placebo to pazopanib might have confounded the final overall survival analysis.236
AxitinibAG13637 (axitinib) is a potent inhibitor of VEGFRs 1, 2, and 3, and showed substantial efficacy in a phase II study in patients with cytokine-refractory RCC.237 The activity of AG13637 in mRCC patients refractory to prior TKI therapy was recently evaluated.237 Patients with sorafenib-refractory RCC were enrolled in this multi-center, open-label phase II study. All patients received a starting dose of AG13637 5 mg orally twice daily, titrated according to tolerance. The primary end point was RECIST (Response Evaluation Criteria in Solid Tumors)-defined OR, with a null hypothesis of OR = 8%, versus OR = 20% under the alternative hypothesis. Partial response was observed in 6 of 42 evaluable patients (14%), stable disease was noted in 15 patients (36%), 12 patients (29%) experienced progres-sive disease, and 9 patients (21%) withdrew because of adverse effects.
maximum dose in the phase I trial, although limiting toxicity was not reached). Beginning 1 week after a loading dose of 150% of the assigned dose, treatment was given by intravenous infusion every 2 weeks. The primary end points were time to tumor progression (by WHO criteria) and response rate. Survival was a secondary end point, because crossover from placebo to 3 mg/kg of bevacizumab was allowed for patients with disease progression on placebo. Minimal toxic effects were seen, with hypertension and asymptomatic protein-uria predominating. The trial was stopped after the interim analysis met the criteria for early stopping. With 116 patients randomly assigned to treatment groups (40 to placebo, 37 to low-dose antibody, and 39 to high-dose antibody), a significant prolongation of the time to progression of disease was found for the high-dose antibody group, compared with the placebo group (hazard ratio: 2.55). A small dif-ference, of borderline significance, was observed between the time to progression of disease in the low-dose antibody group and that in the placebo group (hazard ratio: 1.26). The probability of being progression-free for patients given high-dose antibody, low-dose anti-body, and placebo was 64%, 39%, and 20%, respectively, at 4 months, and 30%, 14%, and 5%, respectively, at 8 months. In this trial, four partial responses occurred for a 10% response rate, and time to tumor progression was substantially prolonged in patients receiving the higher dose of bevacizumab. No major responses to the 3 mg/kg dose were noted, and the effect on time to progression was minimal and of borderline statistical significance. No difference in survival was shown. A substantial number of patients taking bevaci-zumab showed evidence of mixed tumor responses. Because sensitive criteria for tumor progression were used (a 25% increase in the product of perpendicular diameters of any lesion; even a single lesion increasing in diameter by 12% could meet this criterion), protocol therapy was truncated in some patients who may have been experi-encing a net benefit from bevacizumab. No significant differences in overall survival between groups were found.
In view of the positive results from the phase II study, two phase III trials were conducted to evaluate the efficacy and safety of beva-cizumab in combination with interferon-alfa as first-line treatment in mRCC. In the AVOREN study, 649 patients with previously untreated mRCC were randomized to receive interferon alfa-2a (9 MIU subcutaneously 3 times weekly) and bevacizumab (10 mg/kg every 2 weeks; n = 327) or placebo and interferon alfa-2a (n = 322). The primary end point was overall survival.231 Median duration of progression-free survival was significantly longer in the bevacizumab plus interferon alfa group than it was in the control group (10.2 months vs. 5.4 months). Increases in progression-free survival were observed with bevacizumab plus interferon alfa irrespective of risk group or whether reduced-dose interferon alfa was received. The most commonly reported grade 3 or worse adverse events were fatigue (12% patients in the bevacizumab group vs. 8% in the control group) and asthenia (10% vs. 7%).
In a parallel study (CALGB 90206) patients with previously untreated, metastatic clear cell RCC were randomly assigned to receive either bevacizumab (10 mg/kg intravenously every 2 weeks) plus interferon (9 million U subcutaneously 3 times weekly) or the same dose and schedule of interferon monotherapy.232 The primary end point was overall survival and secondary end points were progression-free survival, OR rate, and safety. The median progression-free survival was 8.5 months in patients receiving bevacizumab plus interferon versus 5.2 months in patients receiving interferon mono-therapy (log-rank P < 0.0001; adjusted hazard ratio: 0.71). Bevaci-zumab plus interferon had a higher OR rate as compared with interferon (25.5% vs. 13.1%). Overall toxicity was greater for beva-cizumab plus interferon, including grade 3 hypertension (9% vs. 0%), anorexia (17% vs. 8%), fatigue (35% vs. 28%), and proteinuria (13% vs. 0%). The final analysis of the study showed a median overall survival time of 18.3 months for bevacizumab plus interferon-α and 17.4 months for interferon-α monotherapy (unstratified log-rank P = 0.097). Interestingly, patients who developed hypertension

1437CanceroftheKidney • CHAPTER82
was 85%, and median progression-free survival was 11.7 months. Forty-five percent of patients experienced hypertension, with grades 3/4 hypertension in 12% of the patients. Dysphonia was reported in 22% of participants. Overall, tivozanib was shown to be well toler-ated with minimal off-target toxicities.
An additional phase II open-label, single-arm, multicenter study of tivozanib in 2011-2012 enrolled 100 patients (stratified by clear cell vs. non–clear cell histology) with advanced RCC who had a nephrectomy, no prior VEGF- or mTOR-targeted therapy, and 0 or 1 prior systemic treatment. The trial (NCT01297244, known as BATON) is designed to evaluate biomarkers (including, but not limited to, VEGF-A, VEGF-B, VEGF-C, VEGF-D, CD68, HIF-1, HIF-2, CAIX, and PLGF) in the blood and tumor tissue and their correlation with clinical activity and toxicity of tivozanib. Participants will receive 1.5 mg of tivozanib once daily for 3 weeks, followed by 1 week off.241 Data generated from this study will allow for the opti-mization of patient selection for treatment.
The positive results of previous trials led to the TIVO-1 (Tivoza-nib Versus Sorafenib in First-line Advanced RCC) global (86 centers), randomized, open-label, superiority phase III clinical trial. The study was designed to evaluate the safety and efficacy of tivozanib compared with sorafenib in 517 patients with advanced clear cell RCC who had no prior VEGF- or mTOR-targeted therapy and who had undergone a nephrectomy. Patients were randomly assigned to treatment with tivozanib (1.5 mg/day, 3 weeks on/1 week off, n = 260) or sorafenib (400 mg twice/day in a 4 week cycle, n = 257). The primary end point of the study was progression-free survival. The results, pre-sented in 2012,242 showed a statistically significant improvement in progression-free survival with tivozanib (12.7 months) over sorafenib (9.1 months), and is the first agent to demonstrate greater than 1 year progression-free survival in treatment-naive advanced RCC patients. Objective response rate for tivozanib was 33% compared to 23% for sorafenib (P = 0.01). There was less drug-related toxicity reported in tivozanib-treated patients (tivozanib, 67.6% vs. sorafenib, 83.3%), with the rate of dose reductions for tivozanib as 14% com-pared to 44% for sorafenib. However, more serious adverse events were seen following tivozanib treatment, with hypertension (grade 3 or higher) as the most frequent adverse event (23.6% tivozanib vs. 15.2% sorafenib). Overall survival data are expected to be presented in 2013.
Data from all studies suggest that tivozanib should be considered as a first-line treatment option for those with RCC. In the last quarter of 2012, AVEO (makers of tivozanib), submitted a New Drug Appli-cation (NDA) to the FDA for approval for therapy.
DovitinibDovitinib is a potent, oral, selective TKI that has been shown to have clinical benefit in several types of solid tumor types, including RCC. Unlike other TKIs, dovitinib (also known as TKI258) inhibits VEGFR-1, -2, and -3, PDGFR-β, and fibroblast growth factor recep-tor (FGFR)-1, -2, and -3. The FGFR, in particular, has been shown to be overexpressed in renal cell carcinoma243 and associated with RCC progression and tumor vascularity, and direct inhibition is postulated to facilitate an escape from TKI resistance.
In a phase I, dose escalation portion of a multicenter, open-label phases I/II study (NCT00715182), the safety and efficacy of dovi-tinib was evaluated in 20 patients with advanced RCC or mRCC with predominant clear cell histology who no longer responded to standard therapy.244 Participants were given a 500- or 600-mg/day dose of dovitinib on a 5-days-on/2-days-off schedule in 28-day cycles. Treatment continued until patients experienced disease progression or toxicity. Two patients achieved a partial response (500-mg cohort) and 12 had stable disease, with two patients (500-mg cohort) expe-riencing greater-than-a-year disease stabilization. Eight (53%) of the patients in the 500-mg cohort and 1 (20%) patient in the 600-mg cohort had dose delays or interruptions. The most common treatment-related adverse events were mild (grade 1 or 2), with asthenia (50%),
Overall, 57% of patients experienced some degree of tumor regres-sion. With a median follow-up period of 5.3 months, the median progression-free survival was not reached. Preliminary analysis indi-cates an overall median progression-free survival longer than 7.1 months. No ORs have yet been observed in patients who received prior sunitinib treatment, although tumor regression was demon-strated in 55% of patients with median progression-free survival longer than 6.1 months. Treatment-related grade 3 or 4 adverse events included hypertension (16%), fatigue (14%), and hand-foot syndrome (14%).
The treatment of advanced RCC has been revolutionized by targeted therapy with drugs that block angiogenesis. So far, no phase III randomized trials comparing the effectiveness of one targeted agent against another have been reported. Rini et al. did a random-ized phase III study comparing axitinib, a potent and selective second-generation inhibitor of VEGFRs, with sorafenib, an approved VEGFR inhibitor, as second-line therapy in patients with metastatic renal cell cancer. We included patients coming from 175 sites (hos-pitals and outpatient clinics) in 22 countries age 18 years or older with confirmed clear cell RCC who progressed despite first-line therapy containing sunitinib, bevacizumab plus interferon-α, tem-sirolimus, or cytokines. Patients were stratified according to ECOG performance status and type of previous treatment and then ran-domly assigned (1 : 1) to either axitinib (5 mg twice daily) or sorafenib (400 mg twice daily). Axitinib dose increases to 7 mg and then to 10 mg, twice daily, were allowed for those patients without hypertension or adverse reactions above grade 2. Participants were not masked to study treatment. The primary end point was progression-free survival and was assessed by a masked, independent radiology review and analyzed by intention to treat. This trial was registered on ClinicalTrials.gov, number NCT00678392. A total of 723 patients were enrolled and randomly assigned to receive axitinib (n = 361) or sorafenib (n = 362). The median progression-free survival was 6.7 months with axitinib compared to 4.7 months with sorafenib (hazard ratio: 0.665; 95% confidence interval [CI], 0.544 to 0.812; one-sided P < 0.0001). Treatment was discontinued because of toxic effects in 14 (4%) of 359 patients treated with axitinib and 29 (8%) of 355 patients treated with sorafenib. The most common adverse events were diarrhea, hypertension, and fatigue in the axitinib arm, and diarrhea, palmar-plantar erythro-dysesthesia, and alopecia in the sorafenib arm. Conclusion: Axitinib resulted in significantly longer progression-free survival compared with sorafenib. Axitinib is a treatment option for second-line therapy of advanced RCC.238
Other Angiogenesis Inhibitors in DevelopmentOver the past years additional agents targeting the VEGF axis and other angiogenesis-related proteins have shown activity in preclinical models and are in advanced clinical development for RCC.239
TivozanibTivozanib is an investigational, potent, oral, once-daily, long half-life, selective, small molecule TKI of VEGFR-1, -2, and -3 that, unlike currently available angiogenesis inhibitors, has shown to have a very tolerable safety profile.
In a phase II, multicenter, randomized discontinuation study designed to evaluate the safety and efficacy of tivozanib (also known as AV-951), 272 patients with advanced/mRCC and no prior VEGF-targeted therapy received 1.5 mg/day of open-label tivozanib for 16 weeks.240 After which, 118 patients with less than 25% tumor change were randomly assigned to receive placebo or tivozanib, 78 patients with 25% or greater tumor shrinkage continued to take tivozanib, and patients with 25% or greater tumor growth were discontinued. Study end points were OR rate at 16 weeks and progression-free survival. In the overall study population, 84% of the patients had stable disease or PR by week 16, overall response rate was 30%, DCR

PartIII:SpecificMalignancies1438
one-third of RCC patients eventually develop bone metastatic lesions, cabozantinib could be especially valuable in this population. Ran-domized phase II trials comparing the efficacy of cabozantinib with standard RCC therapy are planned for 2013.247
AMG 386Preclinical studies suggest that endothelial induction of Ang1 and Ang2 in tumors may regulate vessel stability. Thus targeting the Ang-/Tie2 axis may represent an effective novel antiangiogenic therapy for clear cell RCC patients. AMG 386 is an investigational peptide-Fc fusion protein that inhibits angiogenesis by disrupting the angiopoietin/Tie2 axis.248 The safety and efficacy of AMG 386 in combination with sunitinib in patients with mRCC was evaluated in an open-label multicenter phase II study.248
Eighty-five treatment-naive participants were administered either sunitinib 50 mg PO QD (4 weeks on, 2 weeks off ) and AMG 386 at 10 mg/kg (Arm A) or 15 mg/kg (Arm B) intravenously weekly. The primary end point was safety and tolerability. AMG 386 discon-tinuations because of adverse events were 16% (Arm A) and 29% (Arm B), and grade 3 or greater treatment-related adverse events occurred in 72% (Arm A) and 74% (Arm B), attributed all to suni-tinib. The median progression-free survival was 13.9 months in Arm A and not yet mature in Arm B. Objective response rate was 58% in Arm A and 59% in Arm B. Atkins and colleagues concluded that in patients with advanced RCC, administration of AMG 386 at 10 and 15 mg/kg combined with sunitinib, appeared to be tolerable. The efficacy results also suggest potential benefit for the addition of AMG 386 to sunitinib treatment.
Another randomized study evaluated the safety and antitumor activity of AMG 386 in combination with sorafenib in 152 treatment-naive patients with clear cell mRCC.249 Participants were randomized 1 : 1 : 1 to receive sorafenib 400 mg orally twice daily plus intravenous AMG 386 at 10 mg/kg (Arm A) or 3 mg/kg (Arm B) or placebo (Arm C) once weekly. Patients in Arm C received open-label AMG 386 at 10 mg/kg weekly plus sorafenib following disease progression. The primary end point of the study was progression-free survival. Median progression-free survival was 9.0, 8.5, and 9.0 months in Arms A, B, and C, respectively. The OR rate for Arms A, B, and C, respectively, was 38%, 37%, and 25%. Common adverse events included diarrhea (56% to 70%), palmar-plantar erythrodysesthesia syndrome (47% to 54%), alopecia (45% to 50%), and hypertension (42% to 49%). Grade 4 adverse events were reported in 15 patients. Overall, AMG 386 did not significantly improve progression-free survival as compared with placebo plus sorafenib.
CediranibCediranib is another pan-VEGFR inhibitor that has shown promis-ing activity in preclinical models. In a preliminary single-arm phase II study of cediranib in 32 treatment-naive RCC patients 12 evalu-able patients achieved partial response.250
In a randomized, double-blind, phase II trial, 71 patients with RCC were randomized 3 : 1 to cediranib or placebo.2 Following 3 months of treatment, a significant difference in mean percentage change in tumor size between the study and control groups was observed. Of the patients in the placebo arm that crossed over to cediranib the majority had some tumor reduction. The OR rate was 34% in the cediranib arm. Adverse events were similar to other anti-VEGFR drugs. However, the majority of patients (87%) required a dose reduction or a temporary interruption because of toxicities, including diarrhea and hypertension.
RamucirumabRamucirumab is a fully human, high-affinity monoclonal antibody to the extracellular domain of VEGFR-2.251 Its binding prevents ligand binding. A phase II trial evaluating ramucirumab in TKI-refractory RCC completed accrual in 2011. The final report on this important study is not yet available.
diarrhea (70%), vomiting (70%), and nausea (75%). Serious adverse events (sinus bradycardia, hypertensive crisis, pyrexia) were only reported in three of the 20 patients (15%). The study established the maximum tolerated dose of dovitinib as 500 mg/day.
The results of the phase I study led to a phase II dose expansion with 59 unresectable or mRCC patients who had been previously treated with VEGF and mTOR inhibitors. The primary objective of the study was to assess the efficacy of a 500-mg/day dose of dovi-tinib.245 Median progression-free survival and overall survival were 6.1 and 16 months, respectively. Eight percent of patients had PR, 37% had stable disease for 4 months or longer, and 22% had progres-sive disease. Of the patients who were refractory to VEGF and/or mTOR inhibitor therapy, 10% had PR, 42% had stable disease for 4 months or longer, and 19% had progressive disease. Overall, dovi-tinib was well tolerated, with the most common adverse events being nausea (73%), diarrhea (64%), vomiting (56%), decreased appetite (48%), asthenia (36%), and fatigue (36%).
A randomized, open-label, multicenter phase III clinical trial (NCT01223027) is designed to compare the safety and effectiveness of dovitinib versus sorafenib in 550 patients with mRCC from more than 26 countries who failed previous VEGF- and mTOR-targeted (antiangiogenesis) therapies.246 Participants will receive dovitinib (500 mg/day on a 5-days-on/2-days-off schedule) or sorafenib (400 mg twice/day). The end points of the study will include progression-free survival, overall survival, response rates, and inci-dence of adverse events. The study is expected to complete accrual in 2013.
Data from these studies suggest that dovitinib may be especially clinically beneficial to patients with advanced disease, such as mRCC, who no longer respond to standard therapeutic options. With its shown effectiveness and low toxicity profile, a combinatorial approach with this compound may prove to be even more efficacious.
CabozantinibCabozantinib is a potent, orally bioavailable, multitargeted, small-molecule inhibitor of VEGFR-2 and c-MET. The clinical efficacy of cabozantinib (trade name Cometriq, also known as XL184) in mul-tiple tumor types, including mRCC, is associated with disruption of tumor vasculature and invasiveness, blockade of metastases, and extensive tumor cell apoptosis. Very encouraging findings as to the effectiveness of cabozantinib in heavily pretreated patients has been demonstrated in recent clinical trials and is postulated to be because of its ability to overcome resistance to VEGF through inhibition of the c-MET kinase pathway.
A phase Ib drug–drug interaction multicenter study was designed to evaluate the safety, tolerability, and efficacy of a 140-mg/day dose of cabozantinib plus rosiglitazone (a CYP2C8 substrate) in 25 meta-static, treatment refractory RCC patients. Sixty-four percent of which had received 2 or more prior therapies, with 88% having had anti-VEGF therapy, and 60% having received prior mTOR inhibitors. A partial response was reported in seven of the 25 patients (28%), 13 (52%) had stable disease, and only one patient demon-strated progressive disease. A median progression-free survival was 14.7 months, with tumor shrinkage seen in 19 of 21 (90%) patients evaluated. The rate of disease control at 16 weeks for all patients was 72%. Dramatic responses in bone metastases were observed, with a partial bone scan resolution reported in one patient and a complete resolution of pain reported in another. Overall, treatment with cabo-zantinib was found to be relatively safe, with the most frequently reported grade 3 or greater adverse events being hypophosphatemia (36%), hyponatremia (20%), fatigue (16%), diarrhea (12%), and proteinuria (8%).
These encouraging phase I data have demonstrated the clinical effectiveness of cabozantinib in patients who are refractory to stan-dard therapeutic treatments and hence could be a particularly ideal therapeutic for those with advanced RCC. Additionally, existing RCC therapies have little impact on bone disease and given that

1439CanceroftheKidney • CHAPTER82
temsirolimus alone had longer overall survival (hazard ratio for death: 0.73) and progression-free survival than did patients who received interferon-α alone. Overall survival in the combination therapy group did not differ significantly from that in the interferon group (hazard ratio: 0.96). Median overall survival times in the interferon group, the temsirolimus group, and the combination therapy group were 7.3, 10.9, and 8.4 months, respectively. Rash, peripheral edema, hyperglycemia, and hyperlipidemia were more common in the tem-sirolimus group, whereas asthenia was more common in the interferon-α group. There were fewer patients with serious adverse events in the temsirolimus group than in the interferon-α treatment group. Compared with interferon-α, temsirolimus improved overall survival among patients with mRCC and a poor prognosis. The addi-tion of temsirolimus to interferon-α did not improve survival. These data led the FDA to approve temsirolimus for the treatment of advanced kidney cancer in July 2007.
EverolimusEverolimus (RAD001) is an oral mTOR inhibitor. A phase II study with 41 patients enrolled was conducted.261 Of the 41 patients, 37 were evaluable for response and toxicity. Twelve patients had PRs; 19 patients were stable for longer than 3 months. Median duration of therapy is greater than 8 months (range: 1 to 20 months). Treatment-related adverse effects included mucositis, skin rash, pneumonitis, hypophosphatemia, hyperglycemia, hypertriglyceridemia, hypercho-lesterolemia, thrombocytopenia, anemia, and elevated liver enzymes. Positron emission tomography scans demonstrated decreased meta-bolic activity in responding or stable patients. Median overall survival was 11.5 months (range: 1 to 20 months or longer). A phase III randomized trial of everolimus versus supportive care in patients with mRCC has been completed in patients with mRCC whose disease had progressed on VEGF-targeted therapy.262
Patients with mRCC that had progressed on sunitinib, sorafenib, or both, were randomly assigned in a 2 : 1 ratio to receive everolimus 10 mg once daily (n = 272) or placebo (n = 138), in conjunction with best supportive care. The primary end point was progression-free survival, assessed via a blinded, independent central review. The study was halted at the second interim analysis as a significant differ-ence in efficacy between arms was observed. A median progression-free survival of 4.0 versus 1.9 months favoring the everolimus arm was observed with an hazard ratio of 0.30. Stomatitis (40%), rash (25%), and fatigue (20%) were the most commonly reported adverse events in the everolimus-treated patients, but were mostly mild or moderate in severity. Pneumonitis was detected in 8% patients in the everolimus group. This study has led to the approval of everolimus, for it has shown to prolong progression-free survival relative to placebo in patients with mRCC that had progressed on other targeted therapies, including VEGF inhibitors and cytokine therapies.
Additional targeting agents aimed to inhibit the PI3K/Akt and mTOR pathways concomitantly have been shown to have preclinical activity and are under clinical testing. For example, a dual inhibitor of PI3K/mTOR, BEZ235, had a greater inhibitory activity of RCC as compared to lines both in vitro and in vivo more effectively than inhibition of TORC1 alone with rapamycin.263
These evidences suggest that the development of targeted agents aimed to inhibit signaling pathways with a direct antitumor effect represent a valid therapeutic strategy in RCC.
FUTURE DIRECTIONS FOR ANTIANGIOGENESIS THERAPIESAlthough small molecule and antibodies targeting VEGF have added greatly to the therapeutic armamentarium for patients with advanced renal cancer, as single agents, these drugs produce PRs rather than CRs, require long-term administration for continued disease control, and have side effects. The term targeted with respect to therapies in kidney cancer raises several questions: (a) Can the selected target be
AfliberceptAflibercept is a soluble decoy receptor incorporating domains of both VEGFR-1 and -2 fused to the Fc region of human IgG1 that, as compared to bevacizumab, binds all isoforms of VEGF-A and pla-cental growth factor. This VEGF blocker has been shown to have significant preclinical activity, including in a RCC model.251,252 Aflibercept has been approved in combination with chemotherapy in the treatment of colorectal cancer. A randomized phase II study (E4805) testing 2 doses of aflibercept is currently accruing patients with previously treated clear cell RCC and is expected to be com-pleted by 2014.
Inhibitors of the Mammalian Target of Rapamycin PathwayTemsirolimusTemsirolimus (CCI-779) is a mammalian target of rampamycin (mTOR) kinase inhibitor administered intravenously. It has been shown to bind with high affinity to the immunophilin FKBP, and this complex inhibits mTOR kinase activity as evidenced by inhibi-tion of phosphorylation of the eukaryotic translation initiation factor 4E–binding protein-1 and the 40S ribosomal protein p70 S6 kinase, the primary downstream effectors of mTOR.253-255 The upstream activator of mTOR is the serine-threonine kinase Akt. Akt activity is, in turn, regulated by phosphoinositol-3 (PI3)-kinase and the PTEN tumor suppressor gene. Although mutations in PTEN have not been detected in RCC, PTEN gene expression often is downregu-lated.256,257 In addition, the mTOR pathway appears to be involved in the development of a hereditary form of RCC seen in patients with tuberous sclerosis.
Activation of mTOR increases HIF-1α gene expression at the levels of both messenger RNA translation and protein stabilization.258 Thus, inhibition of mTOR by CCI-779 could also prevent the enhanced angiogenesis associated with sporadic RCC and loss of VHL function.
In a phase II study, 111 patients were randomly assigned to receive 25, 75, or 250 mg of CCI-779 weekly as a 30-minute intravenous infusion.259 Patients were evaluated for tumor response, time to tumor progression, survival, and adverse events or effects. Blood samples were collected to determine CCI-779 pharmacokinetics. CCI-779 produced an OR rate of 7% (one CR and seven PRs) and minor responses in 26% of these patients with advanced RCC. Median time to tumor progression was 5.8 months, and the median survival time was 15.0 months. The most frequently occurring CCI-779–related adverse effects of all grades were maculopapular rash (76%), mucositis (70%), asthenia (50%), and nausea (43%). The most frequently occurring grade 3 or 4 adverse effects were hyperglycemia (17%), hypophosphatemia (13%), anemia (9%), and hypertriglyceridemia (6%). Neither toxicity nor efficacy was signifi-cantly influenced by CCI-779 dose level. Patients were retrospectively classified into good-, intermediate-, or poor-risk groups on the basis of criteria used by Motzer and colleagues for a first-line study popula-tion with mRCC treated with interferon-α. Within each risk group, the median survival rates of patients at each dose level were similar. In patients with advanced RCC, CCI-779 showed antitumor activity, encouraging survival, and generally was well tolerated over the three dose levels tested.
The promising data from the phase II study led to a multicenter phase III trial in which 626 patients with previously untreated, poor-prognosis mRCC were randomly assigned to receive 25 mg of intra-venous temsirolimus weekly, 3 million U of interferon-α (with an increase to 18 million U) subcutaneously 3 times weekly, or combina-tion therapy with 15 mg of temsirolimus weekly plus 6 million U of interferon-α 3 times weekly.260 The primary end point was overall survival in comparisons of the temsirolimus group and the combina-tion therapy group with the interferon group. Patients who received

PartIII:SpecificMalignancies1440
strategy of sequential inhibition of angiogenesis by means of treat-ment with aflibercept, a neutralizing decoy consisting of VEGFRs 1 and 2, after TKI failure (Fig. 82-4). A second strategy, pursued in E2804, is to administer duplets of agents that target the VEGF by blocking the ligand, inhibiting the receptor, or affecting HIF with an mTOR inhibitor to test concomitant inhibition (Fig. 82-4). HDAC inhibitors have been shown to reduce HIF-1α protein expression both in tumor and endothelial cells.267,268 The combination of HDAC inhibitors with VEGF inhibitors has an additive antiangiogenic and antitumor activity in animal models, and may achieve a “vertical” inhibition of the VEGF pathway.267 Our group has completed a trial combining bevacizumab with vorinostat a small-molecule inhibitor of HDAC, in patients with mRCC. Vorinostat is a potent inhibitor of HDAC, and can be administered orally with good bioavailabil-ity.269 The study showed a 18% OR rate and a median progression-free survival of 5.4 months in patients with prior antiangiogenic therapies.270
Despite the preclinical evidence and a strong scientific rationale for combining VEGF TKIs, VEGF blockers, and mTOR inhibitors, the results to date have been disappointing. The expected increased clinical benefit has not been observed but rather increased toxicities. The following studies are representative examples.
In the open label, multicenter randomized phase II study (TORAVA trial), the investigators aimed to assess the potential syn-ergistic or additive effect of the combination of bevacizumab and temsirolimus in mRCC. Patients were randomly assigned (2 : 1 : 1) to receive the combination of bevacizumab (10 mg/kg every 2 weeks) and temsirolimus (25 mg weekly; group A), or one of the standard treatments: sunitinib (50 mg/day for 4 weeks followed by 2 weeks off; group B), or the combination of interferon-α (9 mIU 3 times per week) and bevacizumab (10 mg/kg every 2 weeks; group C). The primary end point was progression-free survival at 48 weeks. 171 patients were randomly assigned. Median progression-free survival was 8.2 months in group A, 8.2 months in group B, and 16.8 months in group C. More than 50% of patients in group A stopped treatment for reasons other than progression. Grade 3 or worse adverse events were reported in 77% of patients in group A versus 60% in group B and 70% in group C. These results revealed that the toxicity of the
effectively inhibited? (b) Is the target the same in each patient? (c) Is the therapy endothelial cell or tumor cell specific? New clinical tools to determine whether a patient is going to respond to a certain target-ing agent or whether the inhibition of an alternative target will lead to a greater clinical benefit are urgently needed.
Treatment resistance typically develops within 1 year. Reasons for these results can be multifold: (a) optimal dosing has not been achieved; (b) the signaling pathway is not sufficiently understood; or (c) tumor heterogeneity may be responsible for different dependence from the targeted pathway among patients. Combination therapies have been proposed as a way of potentially producing greater and more durable benefit as compared to single agents. Although critically important, testing of combination regimens must proceed cautiously because of the potential for synergistic toxicity or countervailing activity inherent with use of these multitargeted agents.264 Approaches to combination therapy that have been investigated include “vertical” combinations, in which the HIF/VEGF pathway is blocked at several steps, and “horizontal” combinations, in which multiple separate signaling pathways are blocked simultaneously.265
The vast majority of patients eventually progress through anti-VEGF therapies. Different hypotheses for the resistance mechanisms have been proposed. A recent report suggests that in a transgenic mouse model of pancreatic cancer, an early phase of response to anti-VEGF therapy leads to decrease in blood vessel formation and consequent hypoxia with induction of HIF-1α with downstream overexpression of proangiogenesis growth factors.266 It is conceivable that overexpression of HIF-1α is responsible for increased levels of VEGF that cannot be counteracted by VEGF TKI, or that such overexpression induces alternative growth factors such as placental growth factor and basic fibroblast growth factor. Clinical evidence also indicates that circulating VEGF levels are increased in patients receiving TKIs. Taken together, these observations suggest that the anti-VEGF therapy “escape” may be neutralized with a therapeutic strategy aimed to achieve a “vertical” inhibition of the VEGF pathway. For example, inhibition of tumor cell adaptation to hypoxia induced by TKIs may be achieved with HDAC or mTOR inhibitors that block the HIF pathway. These hypotheses can be tested in rationally designed clinical trials. The ECOG study (E4805) is testing the
Figure 82-4 • Strategies targeting the tumor microenvironment. Dysregulation of the HIF pathway is likely to contribute to the development of renal cell carcinoma. Therefore drugs that inhibit HIF or its downstream targets warrant testing for treatment of this disease. EGFR, epithelial growth factor recep-tor; HIF, hypoxia-inducible factor; PDGF, placenta-derived growth factor; PDGFR, platelet-derived growth factor receptor; TGF-α, transforming growth factor-α; TKIs, receptor tyrosine kinase inhibitors; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor.
mTOR inhibitorsTemsirolimusEverolimus
BEZ235ink128
Ang/c-MET/DII4 inhibitors
AMG386Cabozantinib
REGN421
Vascular disrupting agents
Endothelial cell Immune cellTumor cell
BNCP105
Immunotherapies
AldesleukinBMS-936558VEGF inhibitors
SunitinibSorafenib
BevacizumabPazopaninib
AxitinibDovitinibTivozanibAflibercept

1441CanceroftheKidney • CHAPTER82
AGS-003 (Argos Therapeutics), based on a dendritic cell-based strategy, is generated using RNA comprised of unique and mutated antigens from a patient tumor specimen that is inserted directly into dendritic cells that trigger a tumor-specific immune response. Unlike targeted therapies, this approach addresses the heterogeneity of indi-vidual tumors with an immune response to the whole tumor. A phase I clinical trial with AGS-003 included 22 newly diagnosed, synchro-nous mRCC patients given AGS-003 as a single agent. Clinical benefit (one PR and seven stable disease) was shown in 40% of patients with a favorable safety profile.275,276 The second trial, a phase II combination study of AGS-003 plus sunitinib, followed 21 newly diagnosed, unfavorable risk mRCC patients with an expected overall median survival of 15 months. Treatment consisted of one or two initial cycles of sunitinib (4 weeks on/2 weeks off ), followed by intradermal injections of 5 doses of AGS-003 every 3 weeks, and then a booster shot given every 12 weeks until disease progression. Immune responses correlated directly with prolonged survival. Fifty percent of patients survived longer than 30 months after initiating therapy (median progression-free survival of 11.2 months, final median overall survival of 30.2 months), with 33% of the patients alive after nearly 4 years or longer on the study. Grade 1 injection site reactions were reported in approximately 50% of the patients in the study. The survival benefit for the AGS-003 plus sunitinib combination regimen did not result in added toxicity.275,276
The positive results from the phase II study led to a pivotal phase III randomized, multicenter, open-label clinical trial called Autolo-gous Dendritic Cell Immunotherapy (AGS-003) Plus Standard Treatment of Advanced Renal Cell Carcinoma (ADAPT), and the fast track designation of AGS-003 by the FDA. In 2013, approxi-mately 120 global sites enrolled 450 newly diagnosed unfavorable risk mRCC patients who will receive AGS-003 plus standard RCC therapy (e.g., sunitinib) or standard therapy alone, with a primary end point being overall survival. Secondary end points will include safety, overall response, immune response, and progression-free survival.
IMA901 (immatics) is the first therapeutic multipeptide vaccine for the treatment of RCC that is comprised of 10 different tumor-associated peptides (TUMAPs) found to be highly overexpressed in RCC patients. TUMAPs are expressed in tumor tissue and shown to activate cytotoxic T-cells against tumor cells, hence stimulation of TUMAPs can lead to a highly specific immune response that has a long-term benefit with limited side effects. The safety, immunogenic-ity, and efficacy of IMA901 was tested in a multicenter, open-label, single-arm phase I study with 28 advanced mRCC, leukocyte A (HLA-A)*02-positive patients receiving up to eight IMA901 vaccina-tions, each preceded by administration of granulocyte-macrophage colony-stimulating factor as an immunomodulator.277 At a 3-month follow-up, one patient had partial response (4%), 11 (39%) had stable disease, and 16 (57%) had progressive disease. Seventy-four percent of patients showed a vaccine-induced T-cell response to at least one TUMAP, with 30% of patients responding to multiple TUMAPs. In addition, it was found that patients who responded to multiple TUMAPs were significantly (P = 0.019) more likely to experience partial response or stable disease than patients who responded to one or no TUMAPs. No treatment-related serious adverse events or deaths occurred during the study period.
In a randomized phase II trial that followed, 68 mRCC, leukocyte A (HLA-A)*02-positive patients received IMA901 alone or in com-bination with single-dose cyclophosphamide (immunomodulator) administered before the first of 17 vaccinations.277 As seen in the phase I trial, T-cell response was shown to be significantly associated with clinical benefit. Improved efficacy of IMA901 was found when combined with cyclophosphamide (median overall progression-free survival of 23.5 months vs. 14.8 months), presumably as a result of decreased numbers of regulatory T-cells. The disease control rate within all treated patients was 31% in those with prior cytokine treatment and 14% in patients with prior TKI treatment. In addition,
temsirolimus and bevacizumab combination was much higher than anticipated and clinical activity was low compared with the benefit expected from sequential use of each targeted therapy.271
The “BEST” trial (E2804) also did not show that combination therapies were significantly better than single agents. In this study, 361 treatment-naive RCC patients were randomized to receive beva-cizumab (10 mg/kg every 2 weeks), temsirolimus (25 mg every week) + bevacizumab(10 mg/kg), bevacizumab (5 mg/kg every 2 weeks) + sorafenib (200 mg PO 5 days on/2 days off ), or sorafenib (200 mg every day) + temsirolimus (25 mg every week) until disease progres-sion or unacceptable toxicity. The study was designed to detect a 67% improvement in median progression-free survival on the combination arms, compared to single-agent bevacizumab (median: 9 months vs. 15 months). The results showed that the median progression-free survival was 8.7 months for bevacizumab versus 7.3 months for beva-cizumab + temsirolimus, 11.3 months for bevacizumab + sorafenib, and 7.7 months for sorafenib + temsirolimus. The response rates were 12%, 28%, 30%, and 27%, respectively. No difference in overall survival was observed. Grades 3/4 adverse events and dose reductions were more common in the combination arms CTT.272
The targeted agents for the treatment of RCC have increased overall survival, but patients tend to be treated continuously for long periods of time. Management of the side effects is becoming more challenging. A recent comprehensive review interrogated five data-bases. A total of 107 articles were identified that describe monitoring tools of adverse events and interventions for adverse event manage-ment. The authors identified and summarized clear recommenda-tions for the management of dermatologic, gastrointestinal, thyroid, cardiovascular, and other adverse events. Adverse events were based predominantly on expert opinion. However, there is a need for further systematic investigation of management strategies for adverse events.273
Even though combination strategies have shown similar activity but increased toxicities as compared to single-agent therapy, sequen-tial therapies with anti-VEGF and mTOR inhibitors remain the common practice. The optimal sequence remains unclear, but future prospective studies with associated molecular characterizations will likely identify the subset of patients who might benefit from one therapy sequence versus another therapy sequence.
VACCINE STRATEGIES FOR RENAL CELL CARCINOMAMany cancer vaccines are in various stages of preclinical and clinical development. These vaccines are based on the assumption that tumor-associated antigens (TAAs) are inherently weakly immuno-genic or functionally nonimmunogenic, and that effective vaccines will enhance the efficacy of presentation of TAAs to the immune system, resulting in dramatically increased activation of host T cells. To “break tolerance” against TAAs is the common purpose of antigen presentation by vaccination. Strategies for the development of cancer vaccines include (a) identifying novel TAAs for RCC reactive cyto-toxic T lymphocytes; (b) improving modes of antigen delivery and antigen presentation by using dendritic cells; (c) enhancing antigen immunogenicity (e.g., alternating vaccine prime and boost, enhanc-ing T-cell costimulation, and engineering amino acid sequences in peptide TAAs); (d) improving systemic T-cell dissemination; (e) enhancing destruction of tumor cells (effector phase); (f ) improving T-cell memory; and (g) enhancing the adaptive response to tumor variants (e.g., use of cytokines as vaccine adjuvants).
RCC has long been shown to be an immunogenic-responsive cancer. However, therapeutic cancer vaccines have historically had little proven effect in the area of RCC, with reported response rates ranging from 1.9% to 9.5%.274 In recent years, this has changed with a more specific, personalized, immunotherapeutic approach. Two vaccines in particular, AGS-003 and IMA901, have shown very promising patient survival benefit.

PartIII:SpecificMalignancies1442
have a better prognosis than clear cell carcinomas, the percentage of metastatic non–clear cell carcinomas is much lower.282,283 Less than 10% of patients who receive treatment in clinical trials have non–clear cell histologic characteristics and, consequently, data on response rates for non–clear cell RCC are relatively limited.207,208,284 This is not only because of the rarity of these variants in the metastatic setting, but also because in the past, studies have not typically reported on response by subtype. The Cytokine Working Group reported that only 1 of 17 patients with non–clear cell tumors responded to high-dose IL-2,208 and in the Memorial Sloan-Kettering Cancer Center series, only 1 of 37 responded to interferon-based therapy,178 suggest-ing that immunotherapy should not be offered to patients with non–clear cell RCC.
Sarcomatoid differentiation in RCC indicates an aggressive subtype of renal parenchymal tumors, and is associated with a poor prognosis.285,286 Some evidence suggests that mRCC with sarcoma-toid differentiation do not respond to immunotherapy and should be treated with combination chemotherapy.287 Based on the anti-tumor activity of doxorubicin and gemcitabine in collecting duct carcinoma of the kidney, Nanus and coworkers have tested this combination for treatment in selected patients with sarcomatoid or rapidly progressing RCC.288 Eighteen patients with RCC (56% sar-comatoid; 44% other) were treated at two institutions. Seven patients had received previous treatment with interferon or IL-2. Sites of metastases included the lung, soft tissue, bone, liver, and brain, with 88% of patients presenting with three or more sites of disease. Treat-ment consisted of doxorubicin (50 mg/m2) and gemcitabine (1500 or 2000 mg/m2) every 2 to 3 weeks with granulocyte colony-stimulating factor support. A median of 5 courses was administered (range: 2 to 12 cycles). Therapy was well tolerated with no grade 4 toxicity. Two patients had a CR, five had a PR, three had a mixed response, and one had stable disease. The median duration of response was 5 months (range: 2 to 21 months or longer). These data suggested that the combination of doxorubicin and gemcitabine has antitumor activity in patients with sarcomatoid RCC or with rapidly progressing RCC. An ongoing ECOG study is testing this combination in patients with sarcomatoid RCC.
As a follow up to this study, the ECOG conducted a phase II trial of doxorubicin 50 mg/m2 IV push and gemcitabine 1500 mg/m2 IV over 30 minutes every 2 weeks in 39 patients with locally advanced or mRCC with sarcomatoid features. Ten patients (26%) had grade 3 toxicity, and four patients (11%) had grade 4 toxicities. Although most toxicity was from myelosuppression, one patient died while on the study from cardiac dysfunction after a cumulative dose of 450 mg/m2 doxorubicin. Six (16%) patients experienced responses (5 partial responses and 1 CR), and 10 (26%) patients had stable disease. The median overall survival was 8.8 months, and the median progression-free survival was 3.5 months. The investigators con-cluded that the combination of doxorubicin and gemcitabine, has clinical activity in patients with RCC with sarcomatoid features, but they recognized the toxicity. Additional prospective studies with rational combination strategies involving cytotoxic agents, signal transduction inhibitors and other targeted therapies are needed to make a difference in this unfortunate subset of RCC patients.289
Collecting duct RCC is a rare and aggressive neoplasm of the distal collecting duct system for which no effective therapy has been established. In a case report, a 37-year-old woman with metastatic collecting duct RCC demonstrated 80% reduction in her tumor burden, including complete regression of lymph node metastases and significant shrinkage of the primary, after treatment with paclitaxel and carboplatin. The patient was subsequently rendered free of disease by nephrectomy without evidence of recurrence on follow-up evaluation at 20 months.290 A number of case reports have described responses of collecting duct carcinoma to gemcitabine- or taxane-based therapies similar to those used in transitional cell carci-noma.291,292 This finding is consistent with expression data suggesting that these tumors are closely related to transitional cell cancers.230,293
an analysis of more than 300 pretreatment patient samples identified two serum biomarkers, apolipoprotein A-1 and chemokine (C-C motif ) ligand 17 (CCL17), to be positively correlated with response and overall survival. Noteworthy was that patients pretreated with sunitinib had a lower frequency of regulatory T cells, supporting the idea that sunitinib may have not only a direct effect on tumor cells, but also an immunomodulatory one. Treatment with IMA901 was found to be safe and well tolerated. Most drug-related adverse events were mild local site reactions, with two patients experiencing systemic or grade 3 localized allergic reactions.
These data provided the impetus for the IMPRINT (IMA901 Multi-Peptide vaccine Randomized INTernational study) random-ized phase III study. Patient recruitment of approximately 345 patients across the United States and Europe with metastatic and/or locally advanced RCC was completed in November 2012 and the vaccine was granted U.S. orphan designation by the FDA. The trial is designed to compare the overall survival benefit of IMA901 in combination with sunitinib to sunitinib alone, with the initial results expected in the first half of 2014. The secondary end points will include safety and tolerability, progression-free survival, and immune response to the peptides in IMA901.
Although vaccine therapy is still in an investigational stage, these aforementioned personalized cancer vaccines address the issues seen with previous vaccines of immunosuppressive related toxicity and lack of identified specific tumor-associated targets, and thus hold much promise as adjuvant therapy for patients with RCC. Data generated from the ADAPT and IMPRINT studies will provide confirmatory evidence of the effectiveness of a combinatorial approach of vaccine therapy with standard targeted treatments.
Future vaccine investigations could incorporate concomitant modulation of proinflammatory and immune inhibitory pathways that have hindered generation of tumor-specific immunity. Promising preclinical approaches include the combination of vaccines with agents that deplete CD25+ T-regulatory cells or block the generation of arginase-expressing tumor-associated myeloid cells. In addition, combinations of dendritic cell vaccines with immunocheckpoint inhibitors such as PD-1 antibody may produce more clinical benefit in patients with RCC
CHEMOTHERAPY FOR ADVANCED RENAL CELL CARCINOMAConventional cytotoxic agents generally offer little benefit to patients with RCC. The response rates for a wide variety of chemotherapeutic agents in phase II trials generally have been in the range of 6% to 20%. Although these responses are durable on occasion, no improve-ment in median survival has been reported.278 In a review of 83 trials of a variety of chemotherapeutic regimens published from 1983 to 1993, Yagoda and colleagues reported a 6% overall response rate for 4093 patients with advanced RCC.279 Data from a multiinstitutional phase II trial of gemcitabine and 5-FU suggested that this regimen could be active for patients with advanced RCC.280 Another multi-institutional study with gemcitabine and capecitabine, however, showed only modest activity in patients with metastatic renal cancer, and the degree of clinical benefit and its associated toxicity did not support further evaluation in a phase III trial in unselected patients.281 More focused investigations to identify patients most likely to benefit from chemotherapy or to enhance activity with additional agents such as anti-VEGF drugs would be worthwhile.
Treatment of Kidney Cancers with Nonconventional Histologic FeaturesThe incidence of non–clear cell carcinoma of the kidney has been reported as approximately 20% to 30%. These percentages, however, reflect data from surgical series of patients undergoing primary nephrectomy. Because primary non–clear cell carcinomas tend to

1443CanceroftheKidney • CHAPTER82
therapies to be developed for the specific histologic subtypes. Surgical resection remains the principal therapeutic modality when RCC is confined to the kidney and in selected cases of metastatic disease. Surgical techniques continue to be refined through the growing use of laparoscopic and robotic procedures aimed, when feasible, at nephron-sparing resections that result in less morbidity, preservation of renal function, and comparable therapeutic outcomes. Overall survival remains influenced by stage, performance status, Fuhrman grade, and histologic subtype (e.g., sarcomatoid feature is associated with poor prognosis). Patients at high risk for recurrence after nephrectomy include those with positive lymph nodes, high Fuhrman grade, extension beyond the Gerota fascia, or extension into the renal vein or vena cava. To date, no approved adjuvant therapy is available for these patients. However, the results from the completed adjuvant trials with different TKIs will answer the question whether early exposure to these drugs has a clinical benefit in this setting. Cytore-ductive nephrectomy for patients with metastatic disease may enhance responsiveness to high-dose IL-2 and also remains the standard treat-ment modality for patients receiving antiangiogenesis drugs. Ongoing clinical trials will address this clinical question. Metastasectomy is considered acceptable if all disease can be resected, which, in some instances, may be curative.
Recent years have witnessed the approval of new systemic thera-peutic options that have confirmed the role of VEGF as a critical target for effective therapeutic interventions for recurrent RCC. High-dose IL-2 remains an important therapeutic option in appro-priately selected patients with excellent performance status, normal pulmonary and cardiac functions, and limited disease burden, but new immunotherapy approaches such as the use of immunocheck-point PD-1 inhibitors will likely represent a new standard of care in the near future.
Great progress in the treatment of renal cancer has been made. Three distinct therapeutic approaches (targets) remain the main stem of therapeutic intervention for recurrent RCC: VEGF/VEGFR blockade/inhibition, mTOR inhibition, and immunotherapies. However, these approaches alone are not sufficiently active to achieve durable clinical benefit in the majority of patients. Continued explo-ration of molecular pathways and investigations to identify prognos-tic and predictive markers in this disease remain critical. The genetic studies of RCC have unveiled the potential role of chromatin remod-eling genes. Future studies will shed additional light on the possible biological mechanisms driven by the dysregulation of histone-modifying genes and on novel therapies with chromatin remodeling agents. Physician encouragement of patient participation in clinical trials will dictate the pace of progress in the development of novel, rationally designed, and more effective therapeutic strategies.
The activity of sunitinib and sorafenib in non–clear cell histologic tumor types was recently evaluated.189 Clinical features at study entry and treatment outcomes were evaluated in all patients with metastatic papillary and chromophobe RCC who received either sunitinib or sorafenib as their initial TKI treatment at one of five different cancer centers in France and the United States between 2002 and 2006. Overall response rate, progression-free survival, and overall survival for the entire cohort were 10%, 8.9 months, and 12.2 months, respectively. Twenty (38%) and 33 (62%) patients received sunitinib and sorafenib, respectively. Three of 12 patients (25%) with chromo-phobe histology had an OR, versus two of 41 (4.8%) with papillary histology. Progression-free survival for patients with chromophobe histology was 9.3 months, compared with 6.6 months for those with papillary histology. Overall survival was not different across histologic types and types of TKIs received. Patients who received sunitinib had an overall response rate of 15% and progression-free survival of 11.9 months, compared with 6% and 5.5 months, respectively, for patients who received sorafenib. Other factors found to be associated with shorter progression-free survival include ECOG performance status greater than 0 and subnormal hemoglobin concentration. These pre-liminary results suggest that TKI may have activity in metastatic chromophobe RCC, similar to what is seen with tumors of clear cell histology. Minimal activity, however, was noted in papillary RCC, justifying continued investigations of novel agents for treatment of this histologic tumor type.
A recent single-arm phase 2 trial was recently conducted in patients with non–clear cell RCC and ccRCC with equal to or greater than 20% sarcomatoid histology and no prior treatments with VEGF inhibitors.294 Patients were treated with standard dose and schedule sunitinib. Primary end points were OR rate and progression-free survival. Fifty-seven patients were eligible with different histologic RCCs, including papillary, chromophobe, collecting duct or medul-lary carcinoma, and sarcomatoid. Median progression-free survival for 55 evaluable patients was only 2.7 months. Two patients with chromophobe and one patient with unclassified histology had a con-firmed PR (5% OR rate). Median progression-free survival for patients with papillary histology was 1.6 months. Median progression-free survival for patients with chromophobe histology was 12.7 months. Median overall survival for all patients was 16.8 months. In this small study, the differential response of chromophobe histology to sunitinib suggests a therapeutically relevant biological heterogene-ity exists within non–clear cell RCC.
Two clinical trials (the ASPEN study—NCT01108445 and NCT01185366) are currently testing which single agent has greater clinical benefit between sunitinib and everolimus in patients with advanced non–clear cell carcinoma.
SUMMARYRecent advances in the molecular characterization of RCC using techniques such as next-generation sequencing will lead to new clas-sification of kidney cancer and, in the near future, to novel targeted
R E F E R E N C E S1. Siegel R, Naishadham D, Jemal A. Cancer statistics
2012. CA Cancer J Clin 2012;62(1):10–29.3. Hollingsworth JM, et al. Rising incidence of small
renal masses: a need to reassess treatment effect. J Natl Cancer Inst 2006;98(18):1331–4.
15. Linehan WM, et al. Genetic basis of cancer of the kidney: disease-specific approaches to therapy. Clin Cancer Res 2004;10(18 Pt 2): 6282S–9S.
16. Iliopoulos O, et al. Tumour suppression by the human von Hippel-Lindau gene product. Nat Med 1995;1(8):822–6.
17. Kaelin Jr WG. The von Hippel-Lindau tumor suppressor protein and clear cell renal carcinoma. Clin Cancer Res 2007;13(2 Pt 2):680s–4s.
28. Dalgliesh GL, et al. Systematic sequencing of renal carcinoma reveals inactivation of histone modifying genes. Nature 2010;463(7279):360–3.
36. Gerlinger M, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 2012;366(10):883–92.
58. Ficarra V, et al. TNM staging system for renal-cell carcinoma: current status and future perspectives. Lancet Oncol 2007;8(6):554–8.
79. Motzer RJ, et al. Effect of cytokine therapy on survival for patients with advanced renal cell carci-noma. J Clin Oncol 2000;18(9):1928–35.
The complete reference list is available online at www.expertconsult.com.

PartIII:SpecificMalignancies1444
81. Karakiewicz PI, et al. Multi-institutional validation of a new renal cancer-specific survival nomogram. J Clin Oncol 2007;25(11):1316–22.
83. Heng DY, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol 2009;27(34): 5794–9.
109. Jeong W, et al. Comparison of laparoscopic radical nephrectomy and open radical nephrectomy for pathologic stage T1 and T2 renal cell carcinoma with clear cell histologic features: a multi-institutional study. Urology 2011;77(4):819–24.
116. Lane BR, Campbell SC, Gill IS. Ten-year onco-logic outcomes after laparoscopic and open partial nephrectomy. J Urol 2013.
118. Ellison JS, et al. A matched comparison of periop-erative outcomes of a single laparoscopic surgeon versus a multisurgeon robot-assisted cohort for partial nephrectomy. J Urol 2012;188(1):45–50.
126. Campbell SC, et al. Guideline for management of the clinical T1 renal mass. J Urol 2009;182(4): 1271–9.
130. Rodriguez R, et al. Renal ablative cryosurgery in selected patients with peripheral renal masses. Urology 2000;55(1):25–30.
135. Aron M, et al. Laparoscopic renal cryoablation: 8-year, single surgeon outcomes. J Urol 2010; 183(3):889–95.
144. Kunkle DA, Egleston BL, Uzzo RG. Excise, ablate or observe: the small renal mass dilemma–a meta-analysis and review. J Urol 2008;179(4):1227–33; discussion 1233–4.
169. Timsit MO, et al. Neoadjuvant treatment in advanced renal cell carcinoma: current situation and future perspectives. Expert Rev Anticancer Ther 2012;12(12):1559–69.
171. Cowey CL, et al. Neoadjuvant clinical trial with sorafenib for patients with stage II or higher renal cell carcinoma. J Clin Oncol 2010;28(9):1502–7.
172. Jonasch E, et al. Phase II presurgical feasibility study of bevacizumab in untreated patients with metastatic renal cell carcinoma. J Clin Oncol 2009;27(25):4076–81.
173. Pizzocaro G, et al. Interferon adjuvant to radical nephrectomy in Robson stages II and III renal cell carcinoma: a multicentric randomized study. J Clin Oncol 2001;19(2):425–31.
174. Messing EM, et al. Phase III study of interferon alfa-NL as adjuvant treatment for resectable renal cell carcinoma: an Eastern Cooperative Oncology
Group/Intergroup trial. J Clin Oncol 2003;21(7): 1214–22.
176. Flanigan RC, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med 2001;345(23):1655–9.
178. Mickisch GH, et al. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet 2001; 358(9286):966–70.
182. Choueiri TK, et al. The impact of cytoreductive nephrectomy on survival of patients with meta-static renal cell carcinoma receiving vascular endo-thelial growth factor targeted therapy. J Urol 2011;185(1):60–6.
183. Kavolius JP, et al. Resection of metastatic renal cell carcinoma. J Clin Oncol 1998;16(6):2261–6.
192. Fyfe G, et al. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol 1995;13(3):688–96.
199. Atkins M, Regan M, McDermott D. Update on the role of interleukin 2 and other cytokines in the treatment of patients with state IV renal cell carci-noma. Clin Cancer Res 2004;10:6342S–6S.
204. Negrier S, Perol D, Ravaud A, et al. Do cytokines improve survival in patients with metastatic renal cell carcinoma (MRCC) of intermediate prognosis? Results of the prospective reandomized PERCU Quattro trial. J Clin Oncol 2005;23:380S.
212. Yang JC, Hughes M, Kammula U, et al. Ipilim-umab (anti-CTLA4 antibody) causes regression of metastatic renal cell cancer associated with enteritis and hypophysitis. J Immunother 2007;30(8): 825–30.
214. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer 2012; 12(4):252–64.
217. Topalian SL, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 2012;366(26):2443–54.
225. Escudier B, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med 2007;356(2): 125–34.
227. Motzer RJ, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 2007;356(2):115–24.
229. Yang JC, et al. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor anti-body, for metastatic renal cancer. N Engl J Med 2003;349(5):427–34.
231. Escudier B, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carci-noma: a randomised, double-blind phase III trial. Lancet 2007;370(9605):2103–11.
235. Sternberg CN, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a ran-domized phase III trial. J Clin Oncol 2010;28(6): 1061–8.
238. Rini BI, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet 2011; 378(9807):1931–9.
239. Posadas EM, Figlin RA. Systemic therapy in renal cell carcinoma: advancing paradigms. Oncology (Williston Park) 2012;26(3):290–301.
260. Hudes G, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med 2007;356(22):2271–81.
262. Motzer RJ, et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet 2008; 372(9637):449–56.
264. Atkins MB, et al. Innovations and challenges in renal cell carcinoma: summary statement from the Second Cambridge Conference. Clin Cancer Res 2007;13(2 Pt 2):667s–70s.
265. Kaelin Jr WG. The von Hippel-Lindau tumor sup-pressor gene and kidney cancer. Clin Cancer Res 2004;10(18 Pt 2):6290S–5S.
266. Casanovas O, et al. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell 2005;8(4):299–309.
271. Negrier S, et al. Temsirolimus and bevacizumab, or sunitinib, or interferon alfa and bevacizumab for patients with advanced renal cell carcinoma (TORAVA): a randomised phase 2 trial. Lancet Oncol 2011;12(7):673–80.
272. A randomized phase II study of VEGF RAF kinase, an dmTOR combination targeted therapy CCTT) wiht bevacizumab (bev), sorafenib (sor) and tem-sirolimus (tem) in advanced renal cell carcinoma. J Clin Oncl 2013;31.
273. Eisen T, et al. Targeted therapies for renal cell car-cinoma: review of adverse event management strat-egies. J Natl Cancer Inst 2012;104(2):93–113.
274. Rosenberg SA, Yang JC, Restifo NP. Cancer immu-notherapy: moving beyond current vaccines. Nat Med 2004;10(9):909–15.
288. Nanus DM, et al. Active chemotherapy for sarco-matoid and rapidly progressing renal cell carci-noma. Cancer 2004;101(7):1545–51.

1444.e1CanceroftheKidney • CHAPTER82
R E F E R E N C E S1. Siegel R, Naishadham D, Jemal A. Cancer statistics
2012. CA Cancer J Clin 2012;62(1):10–29.2. Chow WH, et al. Rising incidence of renal cell
cancer in the United States. JAMA 1999;281(17): 1628–31.
3. Hollingsworth JM, et al. Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst 2006;98(18):1331–4.
4. Lipworth L, Tarone RE, McLaughlin JK. The epidemiology of renal cell carcinoma. J Urol 2006;176(6 Pt 1):2353–8.
5. Chow WH, et al. Obesity, hypertension, and the risk of kidney cancer in men. N Engl J Med 2000;343(18):1305–11.
6. van Dijk BA, et al. Cigarette smoking, von Hippel-Lindau gene mutations and sporadic renal cell carcinoma. Br J Cancer 2006;95(3):374–7.
7. Bretan Jr PN, et al. Chronic renal failure: a significant risk factor in the development of acquired renal cysts and renal cell carcinoma. Case reports and review of the literature. Cancer 1986;57(9):1871–9.
8. Chow WH, Dong LM, Devesa SS. Epidemiology and risk factors for kidney cancer. Nat Rev Urol 2010;7(5):245–57.
9. Moertel CG, Dockerty MB, Baggenstoss AH. Multiple primary malignant neoplasms. I. Intro-duction and presentation of data. Cancer 1961; 14:221–30.
10. Pritchett TR, Lieskovsky G, Skinner DG. Extension of renal cell carcinoma into the vena cava: clinical review and surgical approach. J Urol 1986;135(3):460–4.
11. Grubb RL, Walther MM, Linehan WM. The Genetic Basis of Cancer of the Kidney. In: Genetic Diseases of the Kidney. San Diego: Elsevier; 2005.
12. Lopez-Beltran A, et al. 2004 WHO classification of the renal tumors of the adults. Eur Urol 2006;49(5):798–805.
13. Prasad SR, et al. Common and uncommon histo-logic subtypes of renal cell carcinoma: imaging spectrum with pathologic correlation. Radiograph-ics 2006;26(6):1795–806; discussion 1806–10.
14. Fuhrman SA, Lasky LC, Limas C. Prognostic sig-nificance of morphologic parameters in renal cell carcinoma. Am J Surg Pathol 1982;6(7):655–63.
15. Linehan WM, et al. Genetic basis of cancer of the kidney: disease-specific approaches to therapy. Clin Cancer Res 2004;10(18 Pt 2):6282S–9S.
16. Iliopoulos O, et al. Tumour suppression by the human von Hippel-Lindau gene product. Nat Med 1995;1(8):822–6.
17. Kaelin Jr WG. The von Hippel-Lindau tumor suppressor protein and clear cell renal carcinoma. Clin Cancer Res 2007;13(2 Pt 2):680s–4s.
18. Maranchie JK, et al. The contribution of VHL substrate binding and HIF1-alpha to the pheno-type of VHL loss in renal cell carcinoma. Cancer Cell 2002;1(3):247–55.
19. Kondo K, et al. Inhibition of HIF is necessary for tumor suppression by the von Hippel-Lindau protein. Cancer Cell 2002;1(3):237–46.
20. Barnabas N, et al. Mutations in the von Hippel-Lindau (VHL) gene refine differential diagnostic criteria in renal cell carcinoma. J Surg Oncol 2002;80(1):52–60.
21. Brannon AR, et al. Molecular stratification of clear cell renal cell carcinoma by consensus clustering reveals distinct subtypes and survival patterns. Genes Cancer 2010;1(2):152–63.
22. Teh B. Kinome in renal cell carcinoma: mutuation analysis of 518 kinases and expression in 400 tumors. J Clin Oncol 2007.
23. Ellis L, Atadja PW, Johnstone RW. Epigenetics in cancer: Targeting chromatin modifications. Mol Cancer Ther 2009;8(6):1409–20.
24. Hake SB, Xiao A, Allis CD. Linking the epigenetic ‘language’ of covalent histone modifications to cancer. Br J Cancer 2004;90(4):761–9.
25. Wang GG, Allis CD, Chi P. Chromatin remodel-ing and cancer, Part I: Covalent histone modifica-tions. Trends Mol Med 2007;13(9):363–72.
26. Ellinger J, et al. Prognostic relevance of global histone H3 lysine 4 (H3K4) methylation in renal cell carcinoma. Int J Cancer 2010;127(10): 2360–6.
27. Duns G, et al. Histone methyltransferase gene SETD2 is a novel tumor suppressor gene in clear cell renal cell carcinoma. Cancer Res 2010;70(11): 4287–91.
28. Dalgliesh GL, et al. Systematic sequencing of renal carcinoma reveals inactivation of histone modifying genes. Nature 2010;463(7279):360–3.
29. Varela I, et al. Exome sequencing identifies frequent mutation of the SWI/SNF complex gene PBRM1 in renal carcinoma. Nature 2011; 469(7331):539–42.
30. Bodmer D, et al. Understanding familial and non-familial renal cell cancer. Hum Mol Genet 2002;11(20):2489–98.
31. Hakimi AA, et al. Clinical and pathologic impact of select chromatin-modulating tumor suppressors in clear cell renal cell carcinoma. Eur Urol 2013;63(5):848–54.
32. Kleer CG, et al. EZH2 is a marker of aggressive breast cancer and promotes neoplastic transforma-tion of breast epithelial cells. Proc Natl Acad Sci U S A 2003;100(20):11606–11.
33. Ozdag H, et al. Differential expression of selected histone modifier genes in human solid cancers. BMC Genomics 2006;7:90.
34. Shen Y, et al. Expression and significance of histone H3K27 demethylases in renal cell carcinoma. BMC Cancer 2012;12:470.
35. Pena-Llopis S, et al. BAP1 loss defines a new class of renal cell carcinoma. Nat Genet 2012;44(7): 751–9.
36. Gerlinger M, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 2012;366(10): 883–92.
37. Schmidt L, et al. Germline and somatic mutations in the tyrosine kinase domain of the MET proto-oncogene in papillary renal carcinomas. Nat Genet 1997;16(1):68–73.
38. Tomlinson IP, et al. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet 2002;30(4):406–10.
39. Adam J, et al. Renal cyst formation in Fh1-deficient mice is independent of the Hif/Phd pathway: roles for fumarate in KEAP1 succination and Nrf2 signaling. Cancer Cell 2011;20(4):524–37.
40. Ooi A, et al. An antioxidant response phenotype shared between hereditary and sporadic type 2 papillary renal cell carcinoma. Cancer Cell 2011; 20(4):511–23.
41. Gad S, et al. Mutations in BHD and TP53 genes, but not in HNF1beta gene, in a large series of sporadic chromophobe renal cell carcinoma. Br J Cancer 2007;96(2):336–40.
42. Sukosd F, et al. Allelic loss at 10q23.3 but lack of mutation of PTEN/MMAC1 in chromophobe renal cell carcinoma. Cancer Genet Cytogenet 2001;128(2):161–3.
43. Argani P, et al. Aberrant nuclear immunoreactivity for TFE3 in neoplasms with TFE3 gene fusions: a sensitive and specific immunohistochemical assay. Am J Surg Pathol 2003;27(6):750–61.
44. Settembre C, et al. TFEB links autophagy to lysosomal biogenesis. Science 2011;332(6036): 1429–33.
45. Takahashi M, et al. Familial adult renal neoplasia. J Med Genet 2002;39(1):1–5.
46. Cohen D, Zhou M. Molecular genetics of familial renal cell carcinoma syndromes. Clin Lab Med 2005;25(2):259–77.
47. Gnarra JR, Tory K, Weng Y, et al. Mutations of the VHL tumour suppressor gene in renal carcinoma. Nat Genet 1994;7(1):85–90.
48. Pavlovich CP, et al. Evaluation and management of renal tumors in the Birt-Hogg-Dube syndrome. J Urol 2005;173(5):1482–6.
49. Toro JR, et al. Birt-Hogg-Dube syndrome: a novel marker of kidney neoplasia. Arch Dermatol 1999;135(10):1195–202.
50. Khoo SK, et al. Inactivation of BHD in sporadic renal tumors. Cancer Res 2003;63(15):4583–7.
51. Medvetz DA, et al. Folliculin, the product of the Birt-Hogg-Dube tumor suppressor gene, interacts with the adherens junction protein p0071 to regu-late cell-cell adhesion. PLoS One 2012;7(11): e47842.
52. Nahorski MS, et al. Folliculin interacts with p0071 (plakophilin-4) and deficiency is associated with disordered RhoA signalling, epithelial polarization and cytokinesis. Hum Mol Genet 2012;21(24): 5268–79.
53. Malchoff CD, et al. Papillary thyroid carcinoma associated with papillary renal neoplasia: genetic linkage analysis of a distinct heritable tumor syn-drome. J Clin Endocrinol Metab 2000;85(5): 1758–64.
54. Sudarshan S, et al. Fumarate hydratase deficiency in renal cancer induces glycolytic addiction and hypoxia-inducible transcription factor 1alpha sta-bilization by glucose-dependent generation of reac-tive oxygen species. Mol Cell Biol 2009;29(15): 4080–90.
55. Bertolotto C, et al. A SUMOylation-defective MITF germline mutation predisposes to mela-noma and renal carcinoma. Nature 2011; 480(7375):94–8.
56. Teh BT, et al. Bilateral multiple renal oncocytomas and cysts associated with a constitutional transloca-tion (8;9)(q24.1;q34.3) and a rare constitutional VHL missense substitution. Genes Chromosomes Cancer 1998;21(3):260–4.
57. Rybicki FJ, et al. Percutaneous biopsy of renal masses: sensitivity and negative predictive value stratified by clinical setting and size of masses. AJR Am J Roentgenol 2003;180(5):1281–7.
58. Ficarra V, et al. TNM staging system for renal-cell carcinoma: current status and future perspectives. Lancet Oncol 2007;8(6):554–8.
59. Harmer MH. TNM Classification of Malignant Tumors. 1978.
60. Bassil B, Dosoretz DE, Prout Jr GR. Validation of the tumor, nodes and metastasis classification of renal cell carcinoma. J Urol 1985;134(3):450–4.
61. Hermanek P, Schrott KM. Evaluation of the new tumor, nodes and metastases classification of renal cell carcinoma. J Urol 1990;144(2 Pt 1):238–41; discussion 241–2.
62. Flemming ID, Cooper JS, Henson DE, et al. AJCC Cancer Staging Manual. 5th ed. Philadel-phia: Lippincott-Raven; 1997. p. 231–2.
63. Guinan P, et al. TNM staging of renal cell carcinoma: Workgroup No. 3. Union International Contre le Cancer (UICC) and the American Joint Committee on Cancer (AJCC). Cancer 1997;80(5): 992–3.
64. Gettman MT, Blute ML. Update on pathologic staging of renal cell carcinoma. Urology 2002; 60(2):209–17.
65. Edge SB, Byrd DR, Compton CC, et al, editors. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010.

PartIII:SpecificMalignancies1444.e2
66. Lee CT, et al. Surgical management of renal tumors 4 cm. or less in a contemporary cohort. J Urol 2000;163(3):730–6.
67. Hafez KS, Fergany AF, Novick AC. Nephron sparing surgery for localized renal cell carcinoma: impact of tumor size on patient survival, tumor recurrence and TNM staging. J Urol 1999;162(6): 1930–3.
68. Lerner SE, et al. Disease outcome in patients with low stage renal cell carcinoma treated with nephron sparing or radical surgery. J Urol 1996; 155(6):1868–73.
69. Patard JJ, et al. Safety and efficacy of partial nephrectomy for all T1 tumors based on an international multicenter experience. J Urol 2004;171(6 Pt 1):2181–5, quiz 2435.
70. Ficarra V, et al. Proposal for reclassification of the TNM staging system in patients with locally advanced (pT3-4) renal cell carcinoma according to the cancer-related outcome. Eur Urol 2007; 51(3):722–9; discussion 729–31.
71. Thompson RH, et al. Reclassification of patients with pT3 and pT4 renal cell carcinoma improves prognostic accuracy. Cancer 2005;104(1):53–60.
72. Zisman A, et al. Improved prognostication of renal cell carcinoma using an integrated staging system. J Clin Oncol 2001;19(6):1649–57.
73. Patard JJ, et al. Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience. J Clin Oncol 2005;23(12):2763–71.
74. Storkel S, et al. Classification of renal cell carcinoma: Workgroup No. 1. Union Internatio-nale Contre le Cancer (UICC) and the American Joint Committee on Cancer (AJCC). Cancer 1997;80(5):987–9.
75. Kovacs G, et al. The Heidelberg classification of renal cell tumours. J Pathol 1997;183(2):131–3.
76. Moch H, et al. Prognostic utility of the recently recommended histologic classification and revised TNM staging system of renal cell carcinoma: a Swiss experience with 588 tumors. Cancer 2000;89(3):604–14.
77. Amin MB, et al. Prognostic impact of histologic subtyping of adult renal epithelial neoplasms: an experience of 405 cases. Am J Surg Pathol 2002;26(3):281–91.
78. Zisman A, et al. Risk group assessment and clinical outcome algorithm to predict the natural history of patients with surgically resected renal cell carci-noma. J Clin Oncol 2002;20(23):4559–66.
79. Motzer RJ, et al. Effect of cytokine therapy on survival for patients with advanced renal cell carci-noma. J Clin Oncol 2000;18(9):1928–35.
80. Motzer RJ, et al. Prognostic factors for survival in previously treated patients with metastatic renal cell carcinoma. J Clin Oncol 2004;22(3): 454–63.
81. Karakiewicz PI, et al. Multi-institutional validation of a new renal cancer-specific survival nomogram. J Clin Oncol 2007;25(11):1316–22.
82. Manola J, et al. Prognostic model for survival in patients with metastatic renal cell carcinoma: results from the international kidney cancer working group. Clin Cancer Res 2011;17(16): 5443–50.
83. Heng DY, et al. Prognostic factors for overall sur-vival in patients with metastatic renal cell carci-noma treated with vascular endothelial growth factor-targeted agents: results from a large, multi-center study. J Clin Oncol 2009;27(34):5794–9.
84. Heng DY, et al. External validation and compari-son with other models of the International Meta-static Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol 2013;14(2):141–8.
85. Kutikov A, et al. Routine adrenalectomy is unnec-essary during surgery for large and/or upper pole renal tumors when the adrenal gland is radiograph-ically normal. J Urol 2011;185(4):1198–203.
86. Blom JH, et al. Radical nephrectomy with and without lymph-node dissection: final results of European Organization for Research and Treat-ment of Cancer (EORTC) randomized phase 3 trial 30881. Eur Urol 2009;55(1):28–34.
87. Go AS, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitaliza-tion. N Engl J Med 2004;351(13):1296–305.
88. Novick AC. Nephron-sparing surgery for renal cell carcinoma. Annu Rev Med 2002;53:393–407.
89. Simone P, et al. [The diagnosis and treatment of renal oncocytoma. Our experience]. Minerva Chir 1992;47(10):935–8.
90. Leibovich BC, et al. Nephron sparing surgery for appropriately selected renal cell carcinoma between 4 and 7 cm results in outcome similar to radical nephrectomy. J Urol 2004;171(3):1066–70.
91. Dash A, et al. Comparison of outcomes in elective partial vs radical nephrectomy for clear cell renal cell carcinoma of 4-7 cm. BJU Int 2006;97(5): 939–45.
92. Simhan J, et al. Objective measures of renal mass anatomic complexity predict rates of major com-plications following partial nephrectomy. Eur Urol 2011;60(4):724–30.
93. Patard JJ, et al. Morbidity and clinical outcome of nephron-sparing surgery in relation to tumour size and indication. Eur Urol 2007;52(1):148–54.
94. Campbell SC, et al. Complications of nephron sparing surgery for renal tumors. J Urol 1994; 151(5):1177–80.
95. Porpiglia F, et al. Laparoscopic versus open partial nephrectomy: analysis of the current literature. Eur Urol 2008;53(4):732–42; discussion 742–3.
96. Kwon EO, et al. Impact of positive surgical margins in patients undergoing partial nephrec-tomy for renal cortical tumours. BJU Int 2007;99(2):286–9.
97. Vermooten V. Indications for conservative surgery in certain renal tumors: a study based on the growth pattern of the cell carcinoma. J Urol 1950;64(2):200–8.
98. Puppo P, et al. Long term results of excision of small renal cancer surrounded by a minimal layer of grossly normal parenchyma: review of 94 cases. Eur Urol 2004;46(4):477–81.
99. Berdjis N, et al. Impact of resection margin status after nephron-sparing surgery for renal cell carci-noma. BJU Int 2006;97(6):1208–10.
100. Castilla EA, et al. Prognostic importance of resection margin width after nephron-sparing surgery for renal cell carcinoma. Urology 2002; 60(6):993–7.
101. Minervini A, et al. Histopathologic analysis of peritumoral pseudocapsule and surgical margin status after tumor enucleation for renal cell carci-noma. Eur Urol 2009;55(6):1410–18.
102. Carini M, et al. Simple enucleation for the treatment of PT1a renal cell carcinoma: our 20-year experience. Eur Urol 2006;50(6):1263–8; discussion 1269–71.
103. Kutikov A, et al. Enucleation of renal cell carci-noma with ablation of the tumour base. BJU Int 2008;102(6):688–91.
104. Kim SP, et al. Comparative effectiveness for survival and renal function of partial and radical nephrectomy for localized renal tumors: a systematic review and meta-analysis. J Urol 2012;188(1):51–7.
105. Van Poppel H, et al. A prospective, randomised EORTC intergroup phase 3 study comparing the oncologic outcome of elective nephron-sparing surgery and radical nephrectomy for low-stage renal cell carcinoma. Eur Urol 2011;59(4): 543–52.
106. Shuford MD, et al. Complications of contempo-rary radical nephrectomy: comparison of open vs. laparoscopic approach. Urol Oncol 2004;22(2): 121–6.
107. Ono Y, et al. Laparoscopic radical nephrectomy for renal cell carcinoma: a five-year experience. Urology 1999;53(2):280–6.
108. Jeon SH, et al. Comparison of laparoscopic versus open radical nephrectomy for large renal tumors: a retrospective analysis of multi-center results. BJU Int 2011;107(5):817–21.
109. Jeong W, et al. Comparison of laparoscopic radical nephrectomy and open radical nephrectomy for pathologic stage T1 and T2 renal cell carcinoma with clear cell histologic features: a multi-institutional study. Urology 2011;77(4):819–24.
110. Makhoul B, et al. Laparoscopic radical nephrec-tomy for T1 renal cancer: the gold standard? A comparison of laparoscopic vs open nephrectomy. BJU Int 2004;93(1):67–70.
111. Burgess NA, et al. Randomized trial of laparo-scopic v open nephrectomy. J Endourol 2007; 21(6):610–13.
112. Hemal AK, et al. Laparoscopic versus open radical nephrectomy for large renal tumors: a long-term prospective comparison. J Urol 2007;177(3): 862–6.
113. Hattori R, et al. Laparoscopic radical nephrectomy for large renal-cell carcinomas. J Endourol 2009; 23(9):1523–6.
114. Gong EM, et al. Laparoscopic radical nephrec-tomy: comparison of clinical Stage T1 and T2 renal tumors. Urology 2006;68(6):1183–7.
115. Simmons MN, Chung BI, Gill IS. Perioperative efficacy of laparoscopic partial nephrectomy for tumors larger than 4 cm. Eur Urol 2009;55(1): 199–207.
116. Lane BR, Campbell SC, Gill IS. Ten-year onco-logic outcomes after laparoscopic and open partial nephrectomy. J Urol 2013.
117. Khalifeh A, et al. Comparative outcomes and assessment of trifecta in 500 robotic and laparo-scopic partial nephrectomy cases: a single surgeon experience. J Urol 2013;189(4):1236–42.
118. Ellison JS, et al. A matched comparison of periop-erative outcomes of a single laparoscopic surgeon versus a multisurgeon robot-assisted cohort for partial nephrectomy. J Urol 2012;188(1):45–50.
119. Pierorazio PM, et al. Robotic-assisted versus tradi-tional laparoscopic partial nephrectomy: compari-son of outcomes and evaluation of learning curve. Urology 2011;78(4):813–19.
120. Gill IS, et al. “Zero ischemia” partial nephrectomy: novel laparoscopic and robotic technique. Eur Urol 2011;59(1):128–34.
121. Ng CK, et al. Anatomic renal artery branch micro-dissection to facilitate zero-ischemia partial nephrectomy. Eur Urol 2012;61(1):67–74.
122. Borofsky MS, et al. Near-infrared fluorescence imaging to facilitate super-selective arterial clamp-ing during zero-ischaemia robotic partial nephrec-tomy. BJU Int 2013;111(4):604–10.
123. Bishoff JT. Laparoscopic radical nephrectomy: morcellate or leave intact? Definitely morcellate! Rev Urol 2002;4(1):34–7.
124. Pautler SE, et al. Specimen morcellation after lapa-roscopic radical nephrectomy: confirmation of histologic diagnosis using needle biopsy. J Endou-rol 2002;16(2):89–92.
125. Lam JS, et al. Postoperative surveillance protocol for patients with localized and locally advanced renal cell carcinoma based on a validated prognos-tic nomogram and risk group stratification system. J Urol 2005;174(2):466–72; discussion 472; quiz 801.
126. Campbell SC, et al. Guideline for management of the clinical T1 renal mass. J Urol 2009;182(4): 1271–9.
127. Pantuck AJ, et al. Cryosurgical ablation of renal tumors using 1.5-millimeter, ultrathin cryoprobes. Urology 2002;59(1):130–3.
128. Gill IS, et al. Renal cryoablation: outcome at 3 years. J Urol 2005;173(6):1903–7.

1444.e3CanceroftheKidney • CHAPTER82
129. Lin CH, et al. Histopathologic confirmation of complete cancer-cell kill in excised specimens after renal cryotherapy. Urology 2004;64(3):590.
130. Rodriguez R, et al. Renal ablative cryosurgery in selected patients with peripheral renal masses. Urology 2000;55(1):25–30.
131. Permpongkosol S, Nielsen ME, Solomon SB. Percutaneous renal cryoablation. Urology 2006; 68(1 Suppl):19–25.
132. Schwartz BF, et al. Cryoablation of small periph-eral renal masses: a retrospective analysis. Urology 2006;68(1 Suppl):14–18.
133. Hegarty NJ, et al. Probe-ablative nephron-sparing surgery: cryoablation versus radiofrequency abla-tion. Urology 2006;68(1 Suppl):7–13.
134. Silverman SG, et al. Renal tumors: MR imaging-guided percutaneous cryotherapy–initial experi-ence in 23 patients. Radiology 2005;236(2): 716–24.
135. Aron M, et al. Laparoscopic renal cryoablation: 8-year, single surgeon outcomes. J Urol 2010; 183(3):889–95.
136. Allaf ME, et al. Pain control requirements for per-cutaneous ablation of renal tumors: cryoablation versus radiofrequency ablation–initial observa-tions. Radiology 2005;237(1):366–70.
137. Varkarakis IM, et al. Percutaneous radio frequency ablation of renal masses: results at a 2-year mean followup. J Urol 2005;174(2):456–60; discussion 460.
138. Sung HH, et al. Comparison of percutaneous radiofrequency ablation and open partial nephrec-tomy for the treatment of size- and location-matched renal masses. Int J Hyperthermia 2012;28(3):227–34.
139. Breen DJ, et al. Management of renal tumors by image-guided radiofrequency ablation: experience in 105 tumors. Cardiovasc Intervent Radiol 2007;30(5):936–42.
140. Leveillee RJ, et al. Oncological outcomes utilizing real-time peripheral thermometry-guided radiofre-quency ablation of small renal masses. J Endourol 2013;27(4):480–49.
141. Psutka SP, et al. Long-term oncologic outcomes after radiofrequency ablation for t1 renal cell car-cinoma. Eur Urol 2013;63(3):486–92.
142. Smaldone MC, et al. Small renal masses progress-ing to metastases under active surveillance: a sys-tematic review and pooled analysis. Cancer 2012;118(4):997–1006.
143. Mason RJ, et al. Growth kinetics of renal masses: analysis of a prospective cohort of patients under-going active surveillance. Eur Urol 2011;59(5): 863–7.
144. Kunkle DA, Egleston BL, Uzzo RG. Excise, ablate or observe: the small renal mass dilemma–a meta-analysis and review. J Urol 2008;179(4):1227–33; discussion 1233–4.
145. Chawla SN, et al. The natural history of observed enhancing renal masses: meta-analysis and review of the world literature. J Urol 2006;175(2): 425–31.
146. Oda T, et al. Growth rates of primary and meta-static lesions of renal cell carcinoma. Int J Urol 2001;8(9):473–7.
147. Kato M, et al. Natural history of small renal cell carcinoma: evaluation of growth rate, histological grade, cell proliferation and apoptosis. J Urol 2004;172(3):863–6.
148. Kawaguchi S, et al. Most renal oncocytomas appear to grow: observations of tumor kinetics with active surveillance. J Urol 2011;186(4): 1218–22.
149. Sandock DS, Seftel AD, Resnick MI. A new pro-tocol for the followup of renal cell carcinoma based on pathological stage. J Urol 1995;154(1):28–31.
150. Levy DA, et al. Stage specific guidelines for surveil-lance after radical nephrectomy for local renal cell carcinoma. J Urol 1998;159(4):1163–7.
151. Ljungberg B, et al. Follow-up guidelines for nonmetastatic renal cell carcinoma based on the occurrence of metastases after radical nephrectomy. BJU Int 1999;84(4):405–11.
152. Tolia BM, Whitmore Jr WF. Solitary metastasis from renal cell carcinoma. J Urol 1975;114(6): 836–8.
153. Middleton RG. Surgery for metastatic renal cell carcinoma. J Urol 1967;97(6):973–7.
154. Klugo RC, et al. Aggressive versus conservative management of stage IV renal cell carcinoma. J Urol 1977;118(2):244–6.
155. Golimbu M, et al. Aggressive treatment of meta-static renal cancer. J Urol 1986;136(4):805–7.
156. Esrig D, et al. Experience with fossa recurrence of renal cell carcinoma. J Urol 1992;147(6):1491–4.
157. Tanguay S, et al. Therapy of locally recurrent renal cell carcinoma after nephrectomy. J Urol 1996; 155(1):26–9.
158. Edelman MJ, Meyers FJ, Siegel D. The utility of follow-up testing after curative cancer therapy. A critical review and economic analysis. J Gen Intern Med 1997;12(5):318–31.
159. Janzen NK, et al. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease. Urol Clin North Am 2003;30(4):843–52.
160. Chin AI, et al. Surveillance strategies for renal cell carcinoma patients following nephrectomy. Rev Urol 2006;8(1):1–7.
161. Zisman A, et al. Validation of the ucla integrated staging system for patients with renal cell carci-noma. J Clin Oncol 2001;19(17):3792–3.
162. Tapper H, et al. Recurrent renal cell carcinoma after 45 years. Clin Imaging 1997;21(4):273–5.
163. Rabinovitch RA, et al. Patterns of failure following surgical resection of renal cell carcinoma: implica-tions for adjuvant local and systemic therapy. J Clin Oncol 1994;12(1):206–12.
164. Steinbach F, et al. Treatment of renal cell carci-noma in von Hippel-Lindau disease: a multicenter study. J Urol 1995;153(6):1812–16.
165. Walther MM, et al. Prevalence of microscopic lesions in grossly normal renal parenchyma from patients with von Hippel-Lindau disease, sporadic renal cell carcinoma and no renal disease: clinical implications. J Urol 1995;154(6):2010–14; discus-sion 2014–15.
166. Maher ER, Kaelin Jr WG. von Hippel-Lindau disease. Medicine (Baltimore) 1997;76(6):381– 91.
167. Neumann HP, Zbar B. Renal cysts, renal cancer and von Hippel-Lindau disease. Kidney Int 1997; 51(1):16–26.
168. Zbar B, et al. Third International Meeting on von Hippel-Lindau disease. Cancer Res 1999;59(9): 2251–3.
169. Timsit MO, et al. Neoadjuvant treatment in advanced renal cell carcinoma: current situation and future perspectives. Expert Rev Anticancer Ther 2012;12(12):1559–69.
170. Hellenthal NJ, et al. Prospective clinical trial of preoperative sunitinib in patients with renal cell carcinoma. J Urol 2010;184(3):859–64.
171. Cowey CL, et al. Neoadjuvant clinical trial with sorafenib for patients with stage II or higher renal cell carcinoma. J Clin Oncol 2010;28(9): 1502–7.
172. Jonasch E, et al. Phase II presurgical feasibility study of bevacizumab in untreated patients with metastatic renal cell carcinoma. J Clin Oncol 2009;27(25):4076–81.
173. Pizzocaro G, et al. Interferon adjuvant to radical nephrectomy in Robson stages II and III renal cell carcinoma: a multicentric randomized study. J Clin Oncol 2001;19(2):425–31.
174. Messing EM, et al. Phase III study of interferon alfa-NL as adjuvant treatment for resectable renal cell carcinoma: an Eastern Cooperative Oncology
Group/Intergroup trial. J Clin Oncol 2003;21(7): 1214–22.
175. Matin SF, Madsen LT, Wood CG. Laparoscopic cytoreductive nephrectomy: the M. D. Anderson Cancer Center experience. Urology 2006;68(3): 528–32.
176. Flanigan RC, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med 2001;345(23):1655–9.
177. Flanigan RC, et al. Cytoreductive nephrectomy in patients with metastatic renal cancer: a combined analysis. J Urol 2004;171(3):1071–6.
178. Mickisch GH, et al. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet 2001; 358(9286):966–70.
179. Bromwich E, Hendry D, Aitchison M. Cytoreduc-tive nephrectomy: is it a realistic option in patients with renal cancer? BJU Int 2002;89(6):523–5.
180. Rabets JC, et al. Laparoscopic versus open cytore-ductive nephrectomy for metastatic renal cell car-cinoma. Urology 2004;64(5):930–4.
181. Walther MM, et al. Laparoscopic cytoreductive nephrectomy as preparation for administration of systemic interleukin-2 in the treatment of meta-static renal cell carcinoma: a pilot study. Urology 1999;53(3):496–501.
182. Choueiri TK, et al. The impact of cytoreductive nephrectomy on survival of patients with meta-static renal cell carcinoma receiving vascular endo-thelial growth factor targeted therapy. J Urol 2011;185(1):60–6.
183. Kavolius JP, et al. Resection of metastatic renal cell carcinoma. J Clin Oncol 1998;16(6):2261–6.
184. Rasco DW, Assikis V, Marshall F. Integrating metastasectomy in the management of advanced urological malignancies-where are we in 2005? J Urol 2006;176(5):1921–6.
185. Wente MN, et al. Renal cancer cell metastasis into the pancreas: a single-center experience and overview of the literature. Pancreas 2005;30(3): 218–22.
186. Muacevic A, et al. Treatment of brain metastases in renal cell carcinoma: radiotherapy, radiosurgery, or surgery? World J Urol 2005;23(3):180–4.
187. Freedland SJ, Dekernion JB. Role of lymphadenec-tomy for patients undergoing radical nephrectomy for renal cell carcinoma. Rev Urol 2003;5(3): 191–5.
188. Rodriguez A, Sexton WJ. Management of locally advanced renal cell carcinoma. Cancer Control 2006;13(3):199–210.
189. Blom JH, et al. Radical nephrectomy with and without lymph node dissection: preliminary results of the EORTC randomized phase III protocol 30881. EORTC Genitourinary Group. Eur Urol 1999;36(6):570–5.
190. Pantuck AJ, et al. Renal cell carcinoma with retro-peritoneal lymph nodes: role of lymph node dis-section. J Urol 2003;169(6):2076–83.
191. Canfield SE, et al. Renal cell carcinoma with nodal metastases in the absence of distant metastatic disease (clinical stage TxN1-2M0): the impact of aggressive surgical resection on patient outcome. J Urol 2006;175(3 Pt 1):864–9.
192. Fyfe G, et al. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol 1995;13(3):688–96.
193. Fisher RI, Rosenberg SA, Fyfe G. Long-term survival update for high-dose recombinant interleukin-2 in patients with renal cell carcinoma. Cancer J Sci Am 2000;6(Suppl 1):S55–S57.
194. Dutcher JP, et al. Interleukin-2-based therapy for metastatic renal cell cancer: the Cytokine Working Group experience, 1989-1997. Cancer J Sci Am 1997;3 Suppl 1:S73–S78.

PartIII:SpecificMalignancies1444.e4
195. Dutcher JP, et al. Outpatient subcutaneous interleukin-2 and interferon-alpha for metastatic renal cell cancer: five-year follow-up of the Cyto-kine Working Group Study. Cancer J Sci Am 1997;3(3):157–62.
196. Dutcher JP, et al. Phase II trial of interleukin 2, interferon alpha, and 5-fluorouracil in metastatic renal cell cancer: a cytokine working group study. Clin Cancer Res 2000;6(9):3442–50.
197. Negrier S, et al. Treatment of patients with metastatic renal carcinoma with a combination of subcutaneous interleukin-2 and interferon alfa with or without fluorouracil. Groupe Francais d’Immunotherapie, Federation Nationale des Centres de Lutte Contre le Cancer. J Clin Oncol 2000;18(24):4009–15.
198. Atkins MB, McDErmott DF. Results of the cyto-kine working group phase III trial of high dose IL-2 vs. low dose IL-2 and IFN therapy in patients with metastatic renal cell carcinoma. Cancer Invest 2003;21(Suppl 1):S87–S88.
199. Atkins M, Regan M, McDermott D. Update on the role of interleukin 2 and other cytokines in the treatment of patients with state IV renal cell carcinoma. Clin Cancer Res 2004;10:6342S–6S.
200. Parton M, Gore M, Eisen T. Role of cytokine therapy in 2006 and beyond for metastatic renal cell cancer. J Clin Oncol 2006;24(35):5584–92.
201. Coppin C, et al. Immunotherapy for advanced renal cell cancer. Cochrane Database Syst Rev 2005;(1):CD001425.
202. Interferon-alpha and survival in metastatic renal carcinoma: early results of a randomised controlled trial. Medical Research Council Renal Cancer Collaborators. Lancet 1999;353(9146):14–17.
203. Pyrhonen S, et al. Prospective randomized trial of interferon alfa-2a plus vinblastine versus vinblas-tine alone in patients with advanced renal cell cancer. J Clin Oncol 1999;17(9):2859–67.
204. Negrier S, Perol D, Ravaud A, et al. Do cytokines improve survival in patients with metastatic renal cell carcinoma (MRCC) of intermediate prognosis? Results of the prospective reandomized PERCU Quattro trial. J Clin Oncol 2005;23:380S.
205. McDermott DF. Update on the application of interleukin-2 in the treatment of renal cell carcinoma. Clin Cancer Res 2007;13(2 Pt 2): 716s–20s.
206. Cangiano T, et al. Sarcomatoid renal cell carci-noma: biologic behavior, prognosis, and response to combined surgical resection and immunother-apy. J Clin Oncol 1999;17(2):523–8.
207. Motzer RJ, et al. Treatment outcome and survival associated with metastatic renal cell carcinoma of non-clear-cell histology. J Clin Oncol 2002; 20(9):2376–81.
208. Upton MP, et al. Histologic predictors of renal cell carcinoma response to interleukin-2-based therapy. J Immunother 2005;28(5):488–95.
209. Bui MH, et al. Carbonic anhydrase IX is an inde-pendent predictor of survival in advanced renal clear cell carcinoma: implications for prognosis and therapy. Clin Cancer Res 2003;9(2):802–11.
210. Atkins M, et al. Carbonic anhydrase IX expression predicts outcome of interleukin 2 therapy for renal cancer. Clin Cancer Res 2005;11(10):3714–21.
211. McDermott DF, Ghebremichael MS, Signoretti S, et al. The high dose aldesleukin (HD IL-2) “SELECT” trial in patients with metastatic renal cell carcinoma (mRCC). J Clin Oncol 2110; 28:15s:345S (abstract 4514).
212. Yang JC, Hughes M, Kammula U, et al. Ipilimumab (anti-CTLA4 antibody) causes regres-sion of metastatic renal cell cancer associated with enteritis and hypophysitis. J Immunother 2007; 30(8):825–30.
213. Okazaki T, Honjo T. PD-1 and PD-1 ligands: from discovery to clinical application. Int Immunol 2007;19(7):813–24.
214. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer 2012;12(4):252–64.
215. Thompson RH, et al. Costimulatory B7-H1 in renal cell carcinoma patients: Indicator of tumor aggressiveness and potential therapeutic target. Proc Natl Acad Sci U S A 2004;101(49): 17174–9.
216. Brahmer JR, Topalian S, Wollner I, et al. Safety and activity of MDX-1106 (ONO-4538), an anti-PD-1 monoclonal antibody, in patients wiht selected refractory or relapsed malignancies. J Clin Oncol 2008;26(suppl):absr 3006.
217. Topalian SL, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 2012;366(26):2443–54.
218. Brahmer JR, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 2012;366(26):2455–65.
219. Wilhelm S, Chien DS. BAY 43-9006: preclinical data. Curr Pharm Des 2002;8(25):2255–7.
220. Hilger RA, Scheulen ME, Strumberg D. The Ras-Raf-MEK-ERK pathway in the treatment of cancer. Onkologie 2002;25(6):511–18.
221. Wilhelm SM, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angio-genesis. Cancer Res 2004;64(19):7099–109.
222. Awada A, et al. Phase I safety and pharmacokinet-ics of BAY 43-9006 administered for 21 days on/7 days off in patients with advanced, refractory solid tumours. Br J Cancer 2005;92(10): 1855–61.
223. Strumberg D, et al. Phase I clinical and pharma-cokinetic study of the Novel Raf kinase and vascu-lar endothelial growth factor receptor inhibitor BAY 43-9006 in patients with advanced refractory solid tumors. J Clin Oncol 2005;23(5):965–72.
224. Ratain MJ, et al. Phase II placebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma. J Clin Oncol 2006;24(16):2505–12.
225. Escudier B, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med 2007;356(2): 125–34.
226. Motzer RJ, et al. Activity of SU11248, a multitar-geted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell car-cinoma. J Clin Oncol 2006;24(1):16–24.
227. Motzer RJ, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 2007;356(2):115–24.
228. Motzer RJ, et al. Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma. J Clin Oncol 2009;27(22):3584–90.
229. Yang JC, et al. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor anti-body, for metastatic renal cancer. N Engl J Med 2003;349(5):427–34.
230. Yang JC. Bevacizumab for patients with metastatic renal cancer: an update. Clin Cancer Res 2004;10(18 Pt 2):6367S–70S.
231. Escudier B, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carci-noma: a randomised, double-blind phase III trial. Lancet 2007;370(9605):2103–11.
232. Rini BI, et al. Bevacizumab plus interferon alfa compared with interferon alfa monotherapy in patients with metastatic renal cell carcinoma: CALGB 90206. J Clin Oncol 2008;26(33): 5422–8.
233. Rini BI, et al. Phase III trial of bevacizumab plus interferon alfa versus interferon alfa monotherapy in patients with metastatic renal cell carcinoma: final results of CALGB 90206. J Clin Oncol 2010;28(13):2137–43.
234. Hutson TE, D I, Machiels JP, et al. Pazopanib (GW786034) is active in metastatic renal cell car-cinoma (MRCC). J Clin Oncol 2007;25.
235. Sternberg CN, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a ran-domized phase III trial. J Clin Oncol 2010;28(6): 1061–8.
236. Sternberg CN, et al. A randomised, double-blind phase III study of pazopanib in patients with advanced and/or metastatic renal cell carcinoma: Final overall survival results and safety update. Eur J Cancer 2013;49(6):1287–96.
237. Rini B, Rixe O, Bukowski R, et al. AG-013736, a multi-target tyrosine kinase receptor inhibitor, demonstrates anti-tumor activitiy in a phase 2 study of cytokine-refractory, metastatic renal cell carner (RCC). J Clin Oncol 2005.
238. Rini BI, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet 2011;378(9807):1931–9.
239. Posadas EM, Figlin RA. Systemic therapy in renal cell carcinoma: advancing paradigms. Oncology (Williston Park) 2012;26(3):290–301.
240. Nosov DA, et al. Antitumor activity and safety of tivozanib (AV-951) in a phase II randomized dis-continuation trial in patients with renal cell carci-noma. J Clin Oncol 2012;30(14):1678–85.
241. Hutson TE, Rathmell K, Gary R, et al. A phase II biomarker assessment of tivozanib in oncology (BATON) trial in patients (pts) with advanced renal cell carcinoma (RCC). J Clin Oncl 2012;30.
242. Motzer RJ, Nosov D, Eisen T, et al. Tivozanib versus sorafenib as initail targeted therapy for patients with advanced renal cell carcinoma: results from a Phase III randmized, open-label, multi-center trial. J Clin Oncl 2012.
243. Tsimafeyeu I, et al. Overexpression of fibroblast growth factor receptors FGFR1 and FGFR2 in renal cell carcinoma. Scand J Urol Nephrol 2011;45(3):190–5.
244. Angevin E, et al. Phase I study of dovitinib (TKI258), an oral FGFR, VEGFR, and PDGFR inhibitor, in advanced or metastatic renal cell car-cinoma. Clin Cancer Res, 2013;19(5):1257–68.
245. Angevin E, Grünwald V, Ravaud A. A phase II study of dovitinib (TKI258), an FGFR- and VEGFR-inhibitor, in patients with advanced or metastatic renal cell cancer (mRCC). J Clin Oncol 2011;29, (suppl; abstr 4551).
246. Motzer RJ, PCBG.e. Phase III trail of dovitinib (TK1258) versus sorafenib in patient siwth meta-static renal cell carcinoma after failaure of anti-angiogenic (VEGF-targeted and mTOR inhibitor) therapies. J Clin Oncl 2012;30.
247. Choueiri TK, P S, McDErmott DF, et al. Efficacy of cabozantinib (XL1840 in patients (pts) with metastatic, refractory enal cell carcinoma. J Clin Oncl 2012.
248. Atkins MB, RAGG.e. A recent open label multi-center phase II study evaluated the safety and efficacy of AMG386 in combination wiht suni-tinib in patients with adanced RCC. J Clin Oncl 2012;30.
249. Rini B, et al. AMG 386 in combination with sorafenib in patients with metastatic clear cell car-cinoma of the kidney: a randomized, double-blind, placebo-controlled, phase 2 study. Cancer 2012; 118(24):6152–61.
250. Mulders P, Hawkins R, Nathan P, et al. Final results of a phase II randomized study of cediranib (RECENTINTM) in patients with advanced renal cell carcinoma (RCC). Eur J Cancer 2009;21.
251. Holash J, et al. VEGF-Trap: a VEGF blocker with potent antitumor effects. Proc Natl Acad Sci U S A 2002;99(17):11393–8.
252. Verheul HM, et al. Vascular endothelial growth factor trap blocks tumor growth, metastasis forma-tion, and vascular leakage in an orthotopic murine

1444.e5CanceroftheKidney • CHAPTER82
renal cell cancer model. Clin Cancer Res 2007; 13(14):4201–8.
253. Dudkin L, et al. Biochemical correlates of mTOR inhibition by the rapamycin ester CCI-779 and tumor growth inhibition. Clin Cancer Res 2001;7(6):1758–64.
254. Neshat MS, et al. Enhanced sensitivity of PTEN-deficient tumors to inhibition of FRAP/mTOR. Proc Natl Acad Sci U S A 2001;98(18): 10314–19.
255. Yu K, et al. mTOR, a novel target in breast cancer: the effect of CCI-779, an mTOR inhibitor, in preclinical models of breast cancer. Endocr Relat Cancer 2001;8(3):249–58.
256. Brenner W, et al. Loss of tumor suppressor protein PTEN during renal carcinogenesis. Int J Cancer 2002;99(1):53–7.
257. Velickovic M, et al. Intragenic PTEN/MMAC1 loss of heterozygosity in conventional (clear-cell) renal cell carcinoma is associated with poor patient prognosis. Mod Pathol 2002;15(5):479–85.
258. Hudson CC, et al. Regulation of hypoxia-inducible factor 1alpha expression and function by the mam-malian target of rapamycin. Mol Cell Biol 2002;22(20):7004–14.
259. Atkins MB, et al. Randomized phase II study of multiple dose levels of CCI-779, a novel mam-malian target of rapamycin kinase inhibitor, in patients with advanced refractory renal cell carci-noma. J Clin Oncol 2004;22(5):909–18.
260. Hudes G, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med 2007;356(22):2271–81.
261. Jac J, Khan M, et al. A phase II trail of RAD001 in patients with metastatic renal cell carcinoma (MRRC). J Clin Oncl 2007.
262. Motzer RJ, et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet 2008; 372(9637):449–56.
263. Cho DC, et al. The efficacy of the novel dual PI3-kinase/mTOR inhibitor NVP-BEZ235 compared with rapamycin in renal cell carcinoma. Clin Cancer Res 2010;16(14):3628–38.
264. Atkins MB, et al. Innovations and challenges in renal cell carcinoma: summary statement from the Second Cambridge Conference. Clin Cancer Res 2007;13(2 Pt 2):667s–70s.
265. Kaelin Jr WG. The von Hippel-Lindau tumor sup-pressor gene and kidney cancer. Clin Cancer Res 2004;10(18 Pt 2):6290S–5S.
266. Casanovas O, et al. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell 2005;8(4):299–309.
267. Qian DZ, et al. The histone deacetylase inhibitor NVP-LAQ824 inhibits angiogenesis and has a greater antitumor effect in combination with the vascular endothelial growth factor receptor tyrosine kinase inhibitor PTK787/ZK222584. Cancer Res 2004;64(18):6626–34.
268. Qian DZ, et al. Targeting tumor angiogenesis with histone deacetylase inhibitors: the hydroxamic acid derivative LBH589. Clin Cancer Res 2006;12(2): 634–42.
269. Kelly WK, et al. Phase I study of an oral histone deacetylase inhibitor, suberoylanilide hydroxamic acid, in patients with advanced cancer. J Clin Oncol 2005;23(17):3923–31.
270. Hammers JH, Vilky B, et al. Phae I safety and pharmacokinetic harmacodynamic results of the histone deacetylase inhibitor vorinostat n combi-nation wiht bevacizumab in patients with kidney cancer. J Clin Oncl 2008;26.
271. Negrier S, et al. Temsirolimus and bevacizumab, or sunitinib, or interferon alfa and bevacizumab for patients with advanced renal cell carcinoma (TORAVA): a randomised phase 2 trial. Lancet Oncol 2011;12(7):673–80.
272. A randomized phase II study of VEGF RAF kinase, an dmTOR combination targeted therapy CCTT) wiht bevacizumab (bev), sorafenib (sor) and tem-sirolimus (tem) in advanced renal cell carcinoma. J Clin Oncl 2013;31.
273. Eisen T, et al. Targeted therapies for renal cell car-cinoma: review of adverse event management strat-egies. J Natl Cancer Inst 2012;104(2):93–113.
274. Rosenberg SA, Yang JC, Restifo NP. Cancer immu-notherapy: moving beyond current vaccines. Nat Med 2004;10(9):909–15.
275. Amin A, Logan T, et al. A phase II study testing the safety and activity of AGS-003 as an immuno-therapeutic in subjects with newly diagnosed advanced stage renal cell carcinoma RCC in com-bination with sunitinib. J Clin Oncl 2010;28.
276. Figlin RA. Phase II study combining personalized dendritic cell (DC)-based therapy, AGS-003 wiht sunitinib in metastatic renal cell carcinoma. J Clin Oncol 2012;30(suppl)348.
277. Walter S, et al. Multipeptide immune response to cancer vaccine IMA901 after single-dose cyclophosphamide associates with longer patient survival. Nat Med 2012.
278. Motzer RJ, Vogelzang NJ. Chemotherapy for renal cell carcinoma. Philadelphia: Lippincott-Raven; 1997;885–96.
279. Yagoda A, Abi-Rached B, Petrylak D. Chemo-therapy for advanced renal-cell carcinoma: 1983-1993. Semin Oncol 1995;22(1):42–60.
280. Rini BI, et al. Phase II trial of weekly intravenous gemcitabine with continuous infusion fluorouracil in patients with metastatic renal cell cancer. J Clin Oncol 2000;18(12):2419–26.
281. Stadler WM, et al. A phase II study of gemcitabine and capecitabine in metastatic renal cancer: a report of Cancer and Leukemia Group B protocol 90008. Cancer 2006;107(6):1273–9.
282. Stadler WM. Therapeutic options for variant renal cancer: a true orphan disease. Clin Cancer Res 2004;10(18 Pt 2):6393S–6S.
283. Beck SD, et al. Effect of papillary and chromo-phobe cell type on disease-free survival after nephrectomy for renal cell carcinoma. Ann Surg Oncol 2004;11(1):71–7.
284. Stadler WM, et al. Prognostic factors for survival with gemcitabine plus 5-fluorouracil based regimens for metastatic renal cancer. J Urol 2003;170(4 Pt 1):1141–5.
285. de Peralta-Venturina M, et al. Sarcomatoid differentiation in renal cell carcinoma: a study of 101 cases. Am J Surg Pathol 2001;25(3):275–84.
286. Cheville JC, et al. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am J Surg Pathol 2003; 27(5):612–24.
287. Mian BM, et al. Prognostic factors and survival of patients with sarcomatoid renal cell carcinoma. J Urol 2002;167(1):65–70.
288. Nanus DM, et al. Active chemotherapy for sarco-matoid and rapidly progressing renal cell carci-noma. Cancer 2004;101(7):1545–51.
289. Haas NB, et al. A phase II trial of doxorubicin and gemcitabine in renal cell carcinoma with sarcomatoid features: ECOG 8802. Med Oncol 2012;29(2):761–7.
290. Gollob JA, et al. Long-term remission in a patient with metastatic collecting duct carcinoma treated with taxol/carboplatin and surgery. Urology 2001;58(6):1058.
291. Milowsky MI, et al. Active chemotherapy for collecting duct carcinoma of the kidney: a case report and review of the literature. Cancer 2002;94(1):111–16.
292. Peyromaure M, et al. Collecting duct carcinoma of the kidney: a clinicopathological study of 9 cases. J Urol 2003;170(4 Pt 1):1138–40.
293. Yang XJ, et al. Gene expression profiling of renal medullary carcinoma: potential clinical relevance. Cancer 2004;100(5):976–85.
294. Tannir NM, et al. A phase 2 trial of sunitinib in patients with advanced non-clear cell renal cell carcinoma. Eur Urol 2012;62(6):1013–19.
Related Documents