EPILPSY “8” Presented By: Dr. Raed Ahmed MBChB , FIBMS Neurologist 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EPILPSY“8”
Presented By:Dr. Raed Ahmed MBChB , FIBMSNeurologist
1
First Seizure
• Whether to treat first seizure is controversial
• 16-62% will recur within 5 years
• Increased risk of relapse
1-Abnormal imaging 2-Abnormal EEG 3-Family history of epilepsy
•Currently, most patients are not treated for the first seizure unless there is an increased risk for relapse
Medical treatment of epilepsy When do we start antiepileptic medication
(AED)? Which AED to choose? When and how do we switch AEDs? When is polytherapy needed? When can AEDs be discontinued? Pregnancy Driver’s licence
4
Guidelines for anticonvulsant therapy• More than one non-provoked, well-documented seizure• Aim: maximal seizure control, minimal side effects• Monotherapy : start with one first-line drug • Start at a low dose; gradually increase dose until
effective control of seizures is achieved or side-effects develop
• Optimise compliance (use minimum number of doses/d) • • If first drug fails (seizures continue or side-effects
develop), start second first-line drug, followed if possible by gradual withdrawal of first
5
Therapeutic principles
• If second drug fails start second-line drug in combination with preferred first-line drug at maximum tolerated dose • If this combination fails replace second-line drug with alternative second-line drug• If this combination fails, check compliance and reconsider diagnosis (Are events seizures? Occult lesion? • Consider alternative, non-drug treatments (e.g. epilepsy surgery, vagal nerve stimulation)

AEDsOld
Primidon Phenobarbital Phenytoin Clobazam Clonazepam Ethosuximid Valproate Carbamazepine
New Lamotrigine Oxcarbazepine Topiramate Gabapentin Vigabatrin Levatiracetam Zonisamide Tiagabin

Mechanism of action of AEDs
Inhibition of voltage gated Na, Ca channels
Na: phenytoin, carbamazepine, oxcarbazepine, lamotrigine, valproate, topiramate, felbamate, zonisamideCa: ethosuximid, valproate lamotrigine, topiramate, zonisamide
Potentiaton of GABA mediated inhibition
phenobarbital, benzodiazepins, vigabatrin, tiagabine, topiramate, valproate, gabapentin, felbamate
Decrease of glutamate mediated excitation
felbamate, topiramate
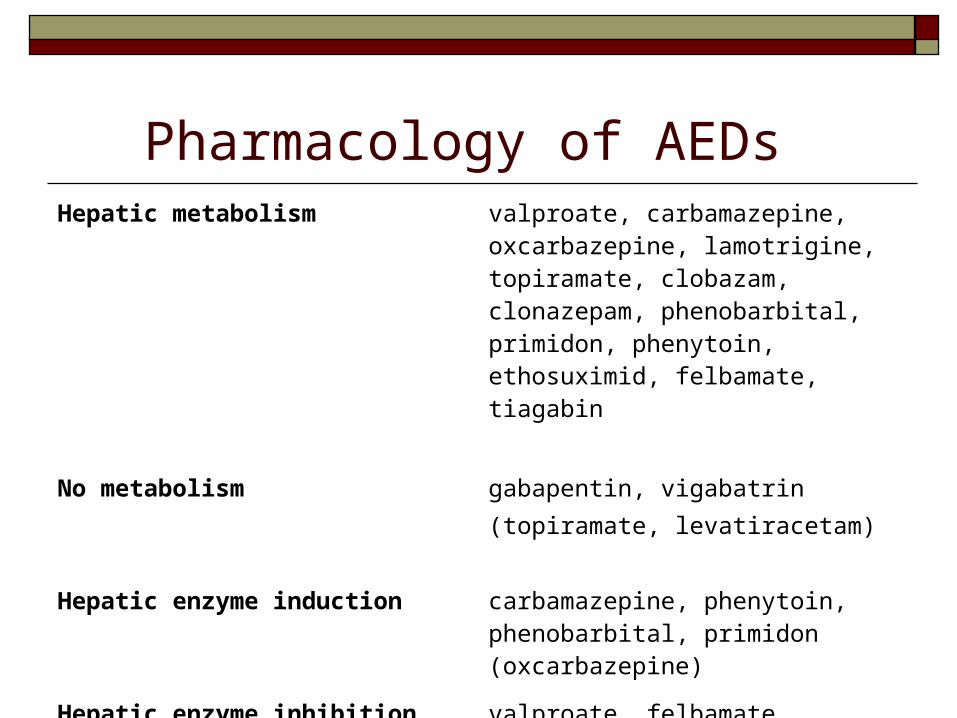
Pharmacology of AEDs Hepatic metabolism valproate, carbamazepine,
oxcarbazepine, lamotrigine, topiramate, clobazam, clonazepam, phenobarbital, primidon, phenytoin, ethosuximid, felbamate, tiagabin
No metabolism gabapentin, vigabatrin(topiramate, levatiracetam)
Hepatic enzyme induction carbamazepine, phenytoin, phenobarbital, primidon (oxcarbazepine)
Hepatic enzyme inhibition valproate, felbamate

9
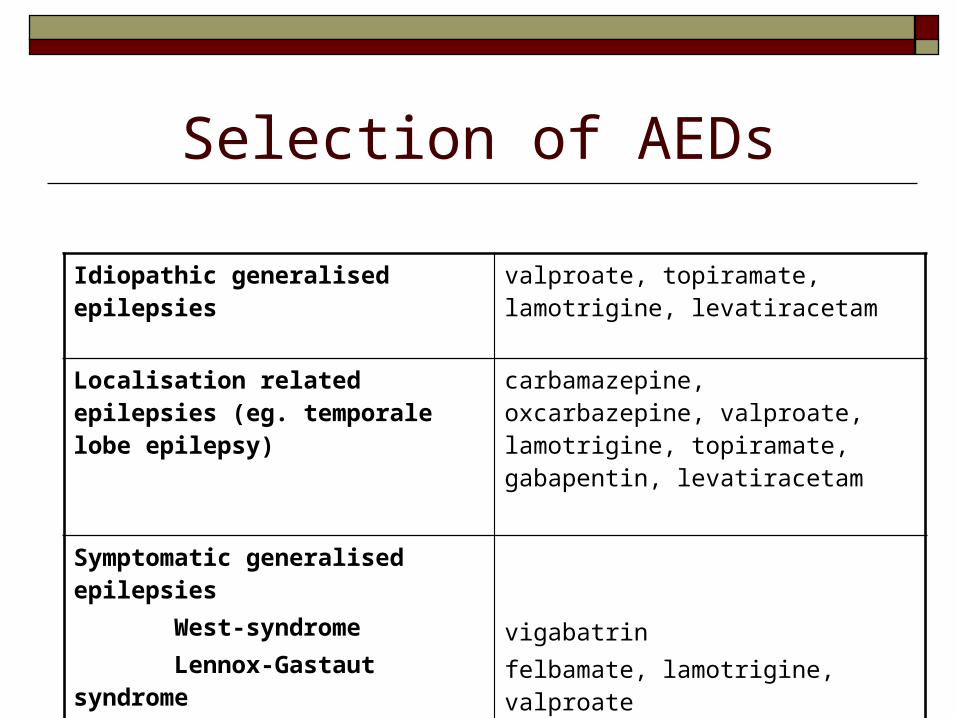
Selection of AEDs
Idiopathic generalised epilepsies valproate, topiramate, lamotrigine, levatiracetam
Localisation related epilepsies (eg. temporale lobe epilepsy)
carbamazepine, oxcarbazepine, valproate, lamotrigine, topiramate, gabapentin, levatiracetam
Symptomatic generalised epilepsies West-syndrome Lennox-Gastaut syndrome
vigabatrinfelbamate, lamotrigine, valproate

Side effects of AEDs Allergy Central nervous system side effects (dose
dependent) drowsiness, headache dizziness, dysequilibrium cognitive dysfunction (memory)
Idiosynchratic reactions / chronic SE s bone marrow suppression (CMZ) hepatic failure(Valproate) rash(CMZ) weight gain (valproate) weight loss (topiramate) tremor(valproate) polycystic ovary syndrome(valproate) visual field defect (vigabatrin)

Summary of Serious and Non-serious Adverse Events of the Newer AEDs
AED Serious Adverse Events Nonserious Adverse Events
Gabapentin None Weight gain, peripheral edema, behavioral changes
Lamotrigine Rash, including Stevens Johnson and toxic epidermal necrolysis hypersensitivity reactions, including risk of hepatic and renal failure, DIC
Tics and insomnia
Levetiracetam None Irritability/behavior change
Oxcarbazepine Hyponatremia (more common in elderly), rash None
Tiagabine Stupor or spike wave stupor Weakness
Topiramate Nephrolithiasis, open angle glaucoma, hypohidrosis (predominantly children)
Metabolic acidosis, weight loss, language dysfunction
Zonisamide Rash, renal calculi, hypohidrosis (predominantly children)
Irritability, photosensitivity, weight loss

Possible causes of AED inefficacy Inadequate dose → dose escalation Poor or Lack of compliance → measure blood AED
levels False diagnosis: the patient doesn’t have epilepsy ‘Pseudoseizures’ → precise description of seizure, EEG
/ video monitoring Inadequate selection of AED True inefficacy of AED → AED switch
Other AED on monotherapy AED combination ? Refractory patients

Drug interactionsEnzyme inductorscarbamazepine, phenytoinphenobarbital, primidon
Increase of metabolism / decrease of efficacyvalproate, lamotrigine, topiramate, carbamazepineoral contraceptionoral anticoagulation
Enzyme inhibitorsvalproate
Decrease of metabolism / increase in efficacy - toxicitylamotrigine, carbamazepine, phenytoin
Does not cause interactionlamotrigine, gabapentin, topiramate, vigabatrin, tiagabin
Seizure-free for more than 2 years A decision of both the doctor and patient AED should be very slowly tapered, lasting
weeks- months Childhood-onset epilepsy **classical absence seizures JME : marked tendency to recur after drug withdrawal Seizures that begin in adult life, particularly those with
partial features, are also likely to recur

16
Contraception
• Some AEDs induce hepatic enzymes that metabolise synthetic hormones, increasing the risk of contraceptive failure.
• Most marked with carbamazepine, phenytoin and barbiturates, but clinically significant effects can be seen with lamotrigine and topiramate.
• If the AED cannot be changed, this can be overcome by giving higher-dose preparations of the oral contraceptive.
• Sodium valproate and levetiracetam have no interaction with hormonal contraception.
17
Epilepsy in pregnancy
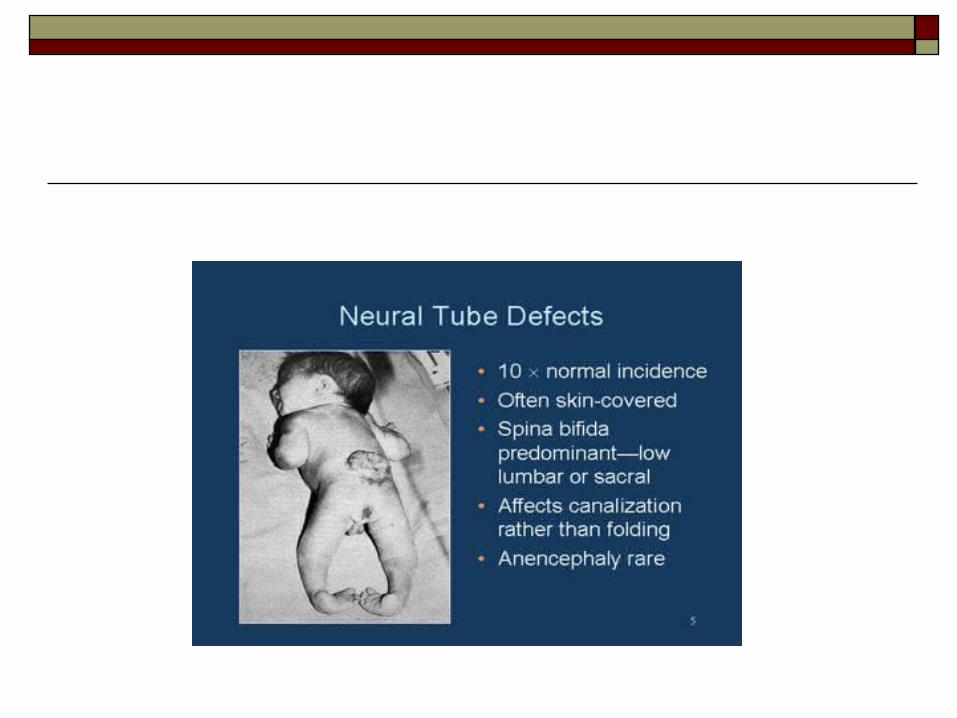
• Great concern about teratogenesis associated with AEDs.
• Background risk of severe fetal malformation in the population is 2–3%.
• Teratogenesis with sodium valproate, which, at high dose, increases the risk to around 6–7%.
• Carbamazepine and lamotrigine have the lowest incidence of major fetal malformations. Levetiracetam may be safe.
• Learning difficulties in children: IQ may be lower when children are exposed to valproate in utero

18
• Seizures may become more frequent during pregnancy (carbamazepine levels may fall in the third trimester, Lamotrigine and levetiracetam levels may fall early in pregnancy)
• Menstrual irregularities and reduced fertility are more common in women with epilepsy, and are also increased by sodium valproate.
• Patients with epilepsy are at greater risk of osteoporosis, (higher female risk).
• Haemorrhagic disease of the newborn: anticonvulsants increase risk. oral vitamin K 20 mg daily to the mother during the last month of pregnancy and give IM vitamin K 1 mg to the infant at birth.
Epilepsy and pregnancy: what to do?
Before conception: Attained the best possible seizure control with the lowest
possible (effective) AED dose, preferably in monotherapy Pre-conception treatment with folic acid (5 mg daily)
During pregnancy: During first trimester supplement folic acid Change medication only if seizure control worsens Screening of fetal malformations (ultrasound on week 16 and 20,
AFP) In case of enzyme inductor AEDs, give vitamin K
Breast feeding is not contraindicated with women on AEDs BUT
Sleep deprivation can provoke seizures

AEDs and Bone Health
Epilepsy and drivingSingle seizure Cease driving until at least 6 mths have passed
without recurrence
Epilepsy Cease driving immediately Licence restored when patient is free from all types
of seizure for 1 yr or seizures have occurred exclusively during sleep for a period of at least 3 yrs
Withdrawal of anticonvulsants Cease driving during withdrawal period and for 6
mths thereafter

Prognosis Overall, generalised seizures are more readily controlled than
focal seizures.
Presence of a structural lesion reduces the chances of freedom from seizures.
Epilepsy: outcome after 20 years 50% are seizure-free, without drugs, for the previous 5 yrs
20% are seizure-free for the previous 5 yrs but continue to take medication
30% continue to have seizures in spite of anti-epileptic therapy

About Epilepsy Drug resistant epilepsy: is defined as failure of
adequate trials of two tolerated, appropriately chosen and used antiepileptic drug schedules to achieve sustained seizure freedom.
Intractable epilepsy: additionally connotes serious impairment of quality of life by either recurrent seizures or AED adverse effects, or both.
It has been estimated that approximately 15% of persons with epilepsy are medically intractable.

Status Epilepticus Status epilepticus is a medical emergency in which
seizures occur continuously or repeatedly without intervening resumption of consciousness for 30 minutes.
However, even 5 minutes of generalized tonic-clonic seizures cause hypoxia, lactic acidosis, muscle breakdown, and neuronal damage.

Diagnosis is usually clinical and can be made on the basis of the description of prolonged rigidity and/or clonic movements with loss of awareness.
As seizure activity becomes prolonged, movements may become more subtle.
Cyanosis, pyrexia, acidosis and sweating may occur, and complications include aspiration, hypotension, cardiac arrhythmias and renal or hepatic failure.
Causes of SE In patients with pre-existing epilepsy, the most
likely cause is a fall in anti-epileptic drug levels.
In de novo SE , it is essential to exclude precipitants such as infection (meningitis, encephalitis), neoplasia and metabolic derangement (hypoglycaemia,hyponatraemia, hypocalcaemia).
MANAGEMENT OF STATUS EPILEPTICUS
General: Immediate care (ABC) Secure intravenous access. Draw blood for glucose, urea and electrolytes (including Ca
and Mg), liver function and sample for future analysis (e.g. drug misuse)
Give diazepam 10 mg intravenously (or rectally)-repeat once only after 15 mins; or lorazepam 4 mg intravenously
Transfer to intensive care area, monitoring neurological condition, blood pressure, respiration and blood gases
Correct any metabolic trigger, e.g. hypoglycaemia

If seizures continue after 30 mins
• IV infusion (with cardiac monitoring) with one of: Phenytoin: 15 mg/kg at 50 mg/min Fosphenytoin: 15 mg/kg at 100 mg/min Phenobarbital: 10 mg/kg at 100 mg/min
• Cardiac monitor and pulse oximetry
Monitor neurological condition, blood pressure, respiration;
check blood gases

If seizures still continue after 30–60 mins
• Transfer to intensive care
Start treatment for refractory status with intubation,ventilation and general
anaesthesia using propofol or thiopental
EEG monitor

Once status controlled
• Commence longer-term anticonvulsant medication with one of: Sodium valproate 10 mg/kg IV over 3–5 mins, then 800–
2000 mg/day Phenytoin: give loading dose (if not already used as above) of
15 mg/kg, infuse at < 50 mg/min, then 300 mg/day Carbamazepine 400 mg by nasogastric tube, then 400–1200
mg/day
• Investigate cause
Related Documents




![[XLS] · Web view8 6212.5 8 19478.2 8 8015 8 8597.35 8 4585 8 15861.9 8 4797.5 8 8597.35 8 15235 8 5153 8 8257.5 8 5592.2 8 19565.7 8 15861.9 8 7575 8 19947.5 8 10215 8 2970 8 15861.9](https://static.cupdf.com/doc/110x72/5bc48cb809d3f274118c1b96/xls-web-view8-62125-8-194782-8-8015-8-859735-8-4585-8-158619-8-47975.jpg)






