Management of convulsions after the neonatal period

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of convulsions afterthe neonatal period
ObjectivesObjectives
• To review the properties of commonlyTo review the properties of commonly available drugs and their safety– Diazepamp– Phenobarbitone
• To consider a rational approach to their use in ppthe convulsing child
• To understand the need for appropriate pp psupportive care.
DiazepamDiazepam
• Half‐life, 10‐20 hours, longer in newborns.– Danger of accumulationDanger of accumulation
• Predominantly inactivated in the liver
C b i b i d l• Can be given by iv and rectal routes

Diazepam (2)Diazepam (2)io
nnc
entra
ti
Level required
ood
con
to control seizures
pam
blo
Dia
zep
Time after giving diazepam
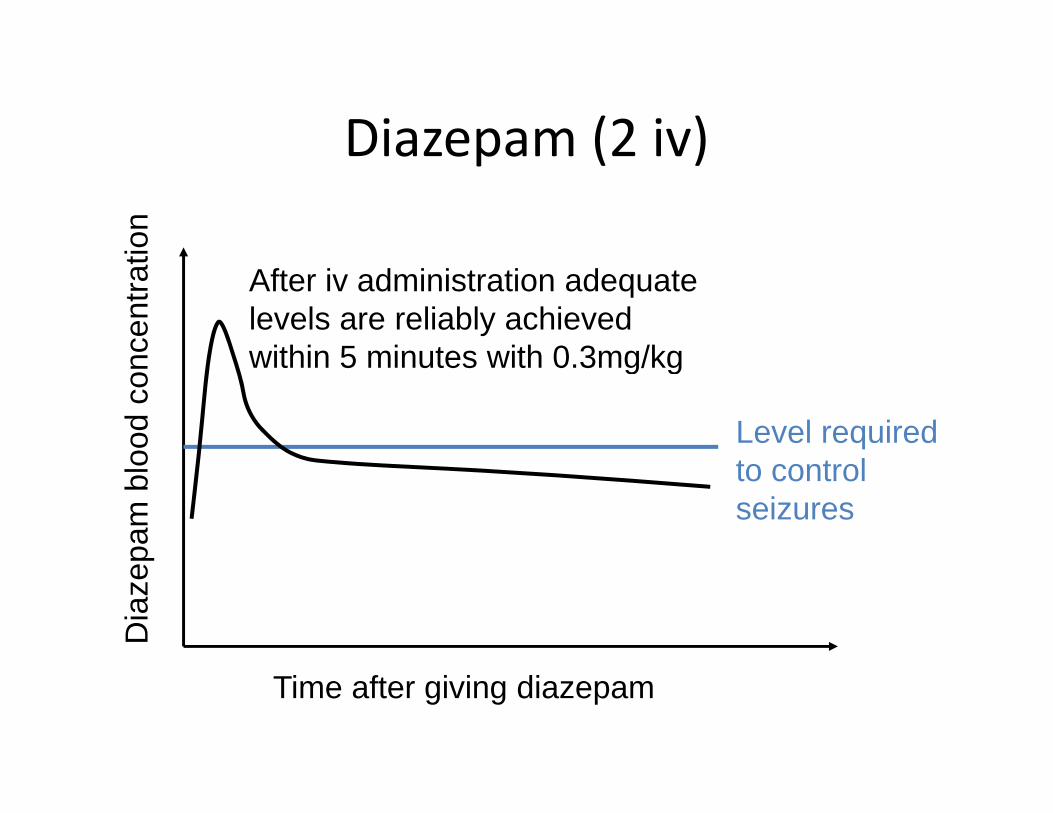
Diazepam (2 iv)Diazepam (2 iv)io
nnc
entra
ti
After iv administration adequate levels are reliably achieved within 5 minutes with 0 3mg/kg
Level required
ood
con within 5 minutes with 0.3mg/kg
to control seizures
pam
blo
Dia
zep
Time after giving diazepam

Diazepam (2 pr)Diazepam (2 pr)io
nnc
entra
ti After pr administration adequate levels are usually achieved within 5 minutes with 0 5mg/kg
Level required
ood
con 5 minutes with 0.5mg/kg
to control seizures
pam
blo
Dia
zep
Time after giving diazepam
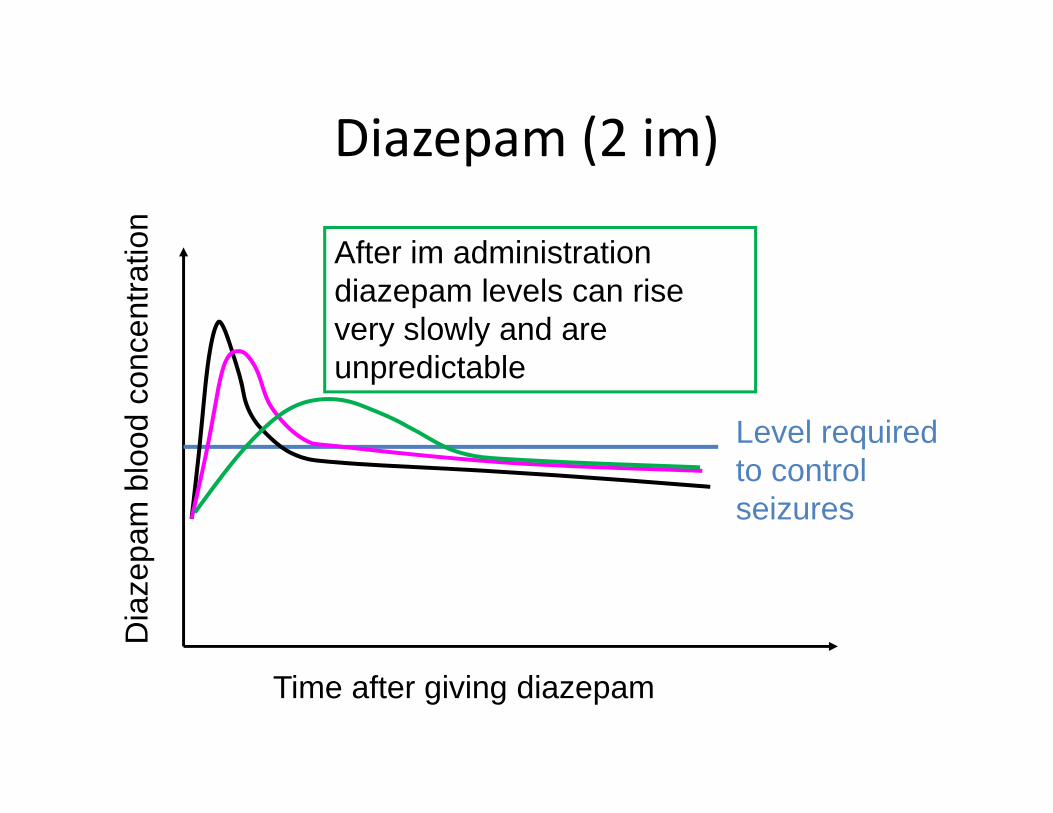
Diazepam (2 im)Diazepam (2 im)io
n
After im administration
ncen
trati After im administration
diazepam levels can rise very slowly and are
di bl
Level required
ood
con unpredictable
to control seizures
pam
blo
Dia
zep
Time after giving diazepam
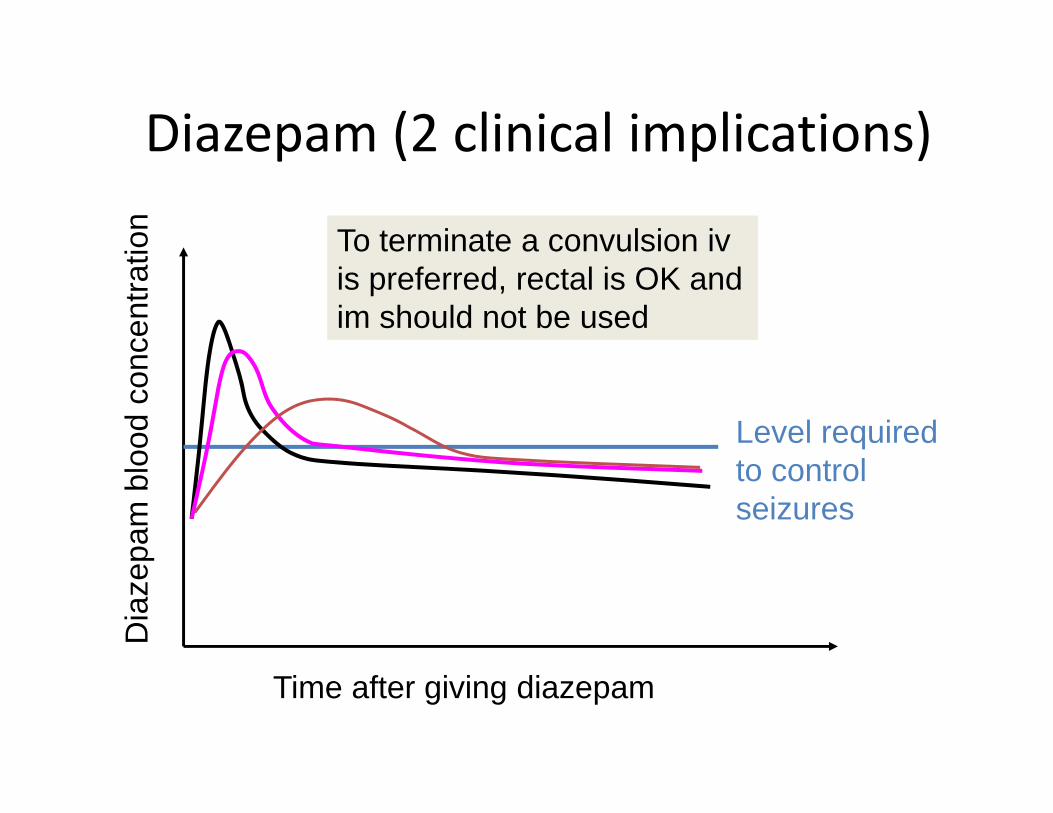
Diazepam (2 clinical implications)Diazepam (2 clinical implications)io
n To terminate a convulsion iv
ncen
trati
is preferred, rectal is OK and im should not be used
Level required
ood
con
to control seizures
pam
blo
Dia
zep
Time after giving diazepam

Diazepam (2 clinical implications)Diazepam (2 clinical implications)io
n Levels stay moderately high for
ncen
trati many hours – multiple doses can
result in very high, potentially dangerous levels
Level required
ood
con dangerous levels
to control seizures
pam
blo
Dia
zep
Time after giving diazepam

Diazepam (2 clinical implications)Diazepam (2 clinical implications)io
n Give the right dose – iv / pr d idl lt i
ncen
trati overdoses can rapidly result in
very high levels that have serious side effects
Level required
ood
con
to control seizures
pam
blo
Dia
zep
Time after giving diazepam
Diazepam – side effectsDiazepam side effects
• Respiratory depression• Respiratory depression– ↑ pCO2, worsens acidosis and can cause an increase in intra‐cranial pressure (ICP) possibly p ( ) p yprecipitating coning and respiratory arrest.
– ↓ pO2, worsening oxygen delivery to the btissues and brain
• After a single (correct) dose of diazepam up t 10% f hild h di blto 10% of children have discernable respiratory depression
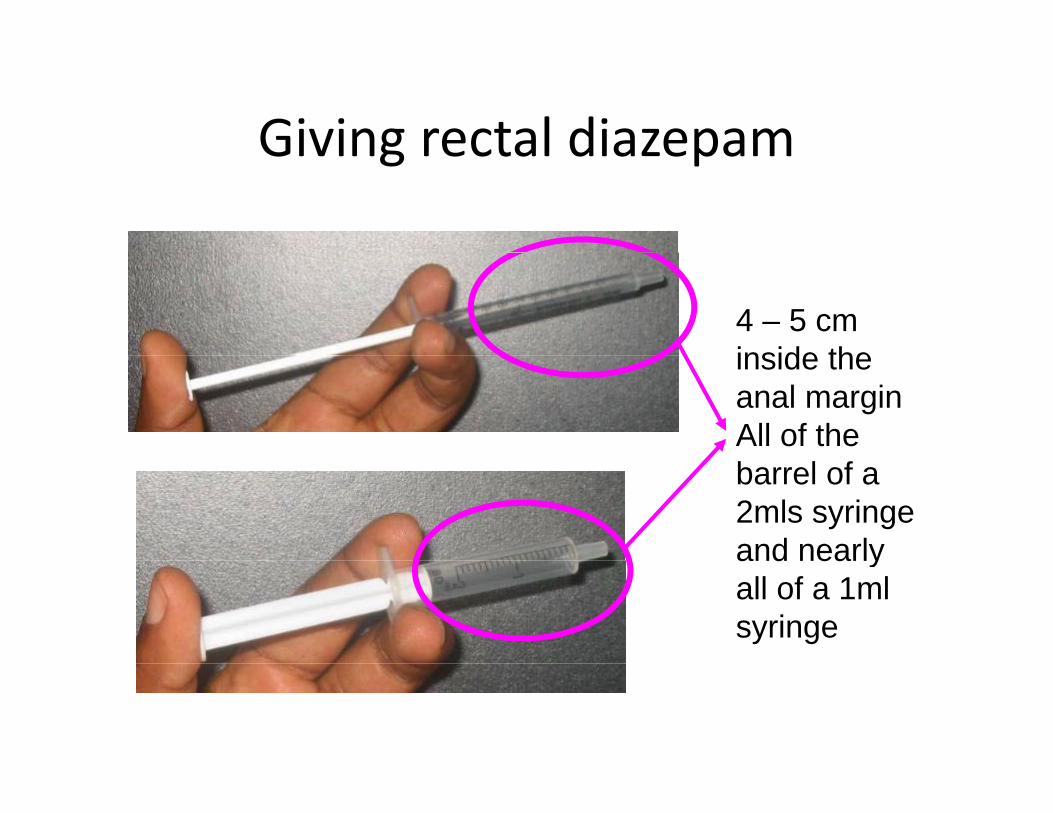
Giving rectal diazepamGiving rectal diazepam
4 – 5 cm inside theinside the anal margin All of the barrel of a 2mls syringe and nearlyand nearly all of a 1ml syringe
PhenobarbitonePhenobarbitone
• Half life, ≥ 2 daysHalf life, ≥ 2 days– Danger of accumulation
• Eliminated by the liverEliminated by the liver• Can be given:
– Deep im injection– Deep im injection– Slow iv infusion (max 1mg/kg/min – 15min for loading dose!)g )
– iv bolus doses are contraindicated.

Phenobarbitone (2)Phenobarbitone (2)io
non
cent
rat
After 10 minutes adequate levels are reliably achieved with a loading dose of 15mg/kg im
Level required blo
od c
o a loading dose of 15mg/kg im
to control seizures
barb
itone
Phe
nob
Time after giving Phenobarbitone
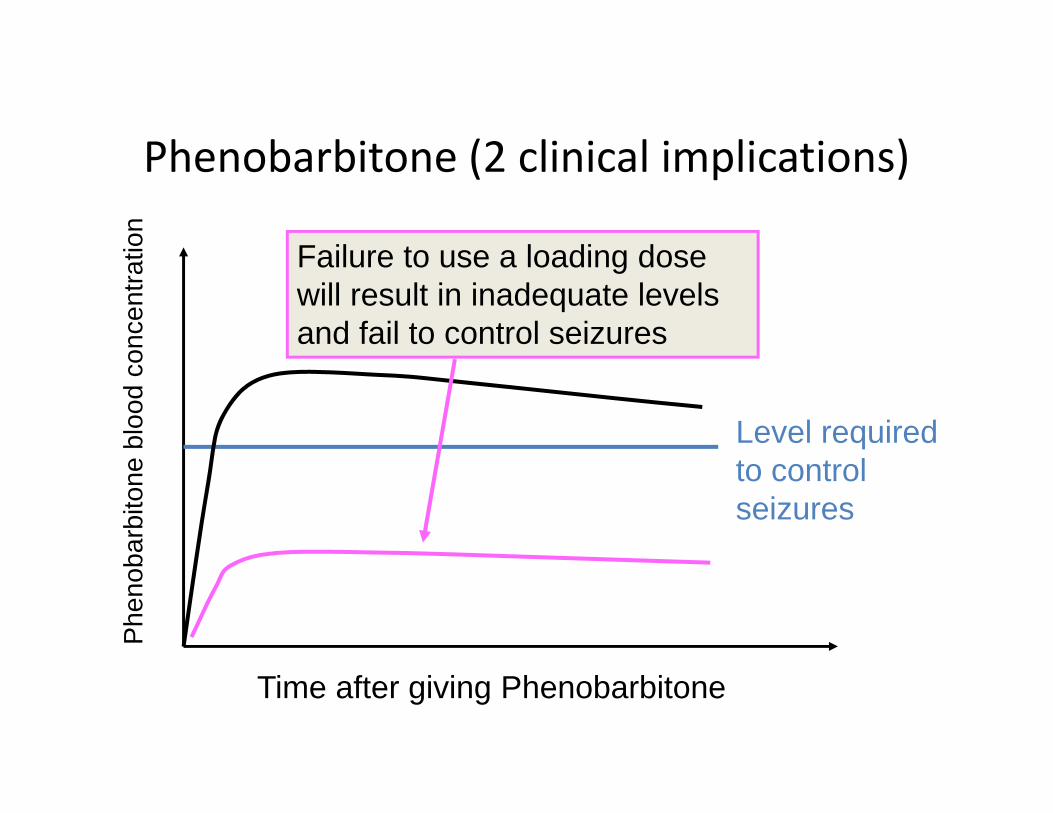
Phenobarbitone (2 clinical implications)Phenobarbitone (2 clinical implications)io
n
Failure to use a loading dose
once
ntra
t Failure to use a loading dose will result in inadequate levels and fail to control seizures
Level required blo
od c
o
to control seizures
barb
itone
Phe
nob
Time after giving Phenobarbitone
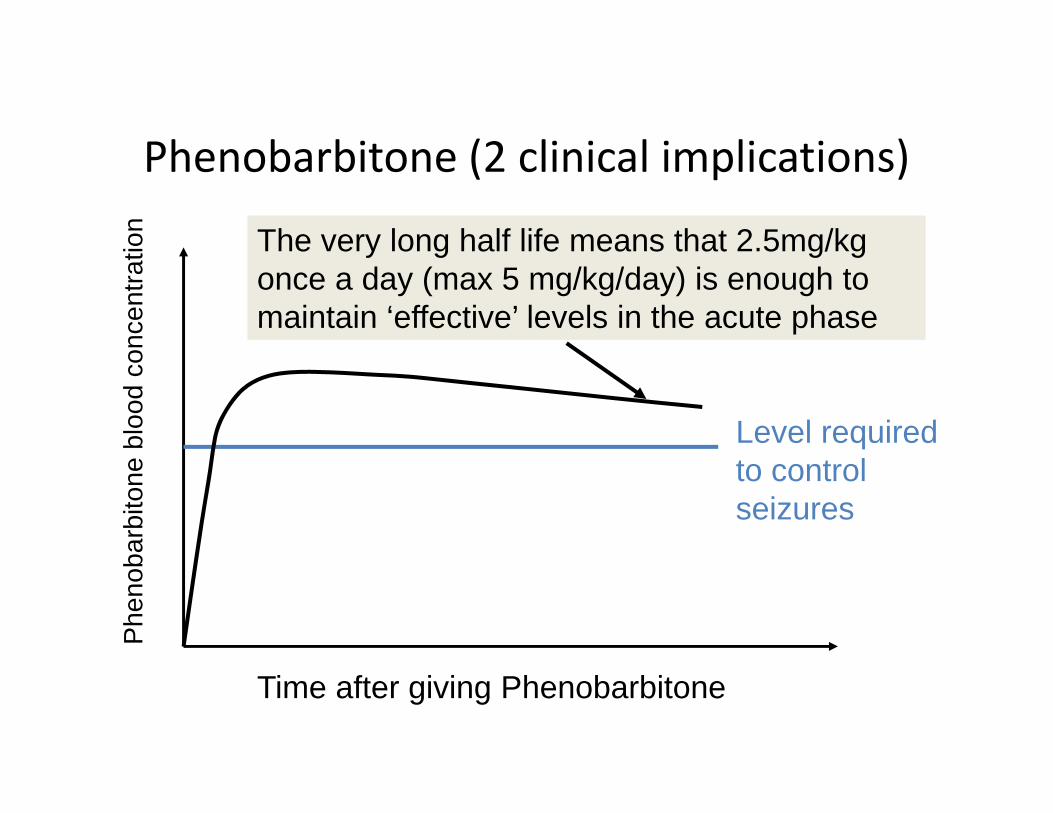
Phenobarbitone (2 clinical implications)Phenobarbitone (2 clinical implications)io
n The very long half life means that 2.5mg/kg
once
ntra
t y g g gonce a day (max 5 mg/kg/day) is enough to maintain ‘effective’ levels in the acute phase
Level required blo
od c
o
to control seizures
barb
itone
Phe
nob
Time after giving Phenobarbitone
Phenobarbitone – side effectsPhenobarbitone side effects
• Respiratory depression• Respiratory depression– ↑ pCO2, worsens acidosis and can cause an increase in intra cranial pressure (ICP) possiblyincrease in intra‐cranial pressure (ICP) possibly precipitating coning and respiratory arrest.
– ↓ pO worsening oxygen delivery to the↓ pO2, worsening oxygen delivery to the tissues and brain
• In overdose – coma and hypotension• In overdose coma and hypotension.
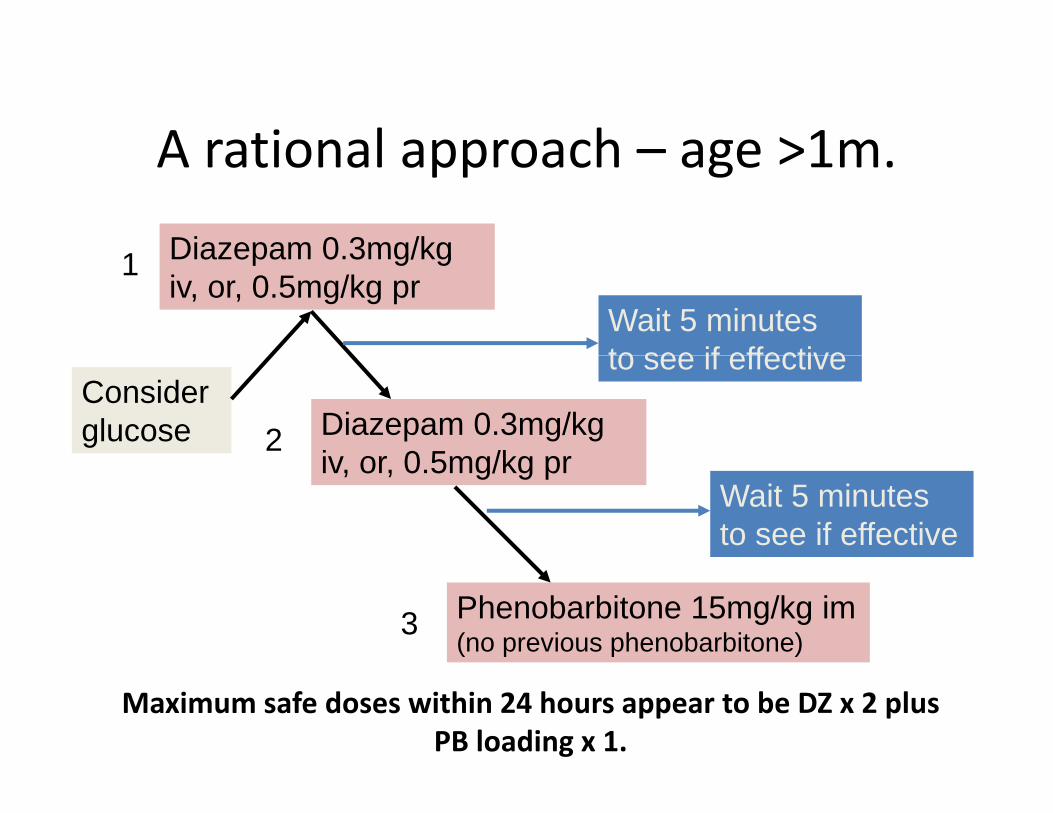
A rational approach – age >1mA rational approach – age >1m.
Diazepam 0 3mg/kg1 Diazepam 0.3mg/kg iv, or, 0.5mg/kg pr
1
Wait 5 minutes to see if effective
Diazepam 0.3mg/kg iv or 0 5mg/kg pr
2
to see if effectiveConsider glucose
iv, or, 0.5mg/kg prWait 5 minutes to see if effective
Phenobarbitone 15mg/kg im (no previous phenobarbitone)3
Maximum safe doses within 24 hours appear to be DZ x 2 plus PB loading x 1.
Clinical dilemma?Clinical dilemma?
Will treatment make things better or worse?Will treatment make things better or worse?

Managing the risks of seizures and their treatment
• Airway– Positioning– Suction– Support after seizure
• Breathing– Oxygen– Check after seizuref
• Circulation– Temperature gradient?– Severe Pallor?– Severe Pallor?
• Disability– What drugs have been
used?used?– Glucose?
Questions?Questions?
SummarySummary
• Diazepam and phenobarbitone when used• Diazepam and phenobarbitone when used appropriately are safe and usually effective.
• Overdosing (the 2.5 / 5 / 10 mg approach) or img ( / / g pp )DZ can be dangerous
• When seizures continue despite basic treatment the dr gs can become as dangero s as thethe drugs can become as dangerous as the convulsions
• Insufficient attention is paid to basic airway andInsufficient attention is paid to basic airway and respiratory support that may prevent death and brain damage.
Related Documents





![REGLAMENTO_ORGANICO _FEBRERO _2010[1]](https://static.cupdf.com/doc/110x72/577d29af1a28ab4e1ea783aa/reglamentoorganico-febrero-20101.jpg)





