1 APPENDIX A: ASSESSMENT OF THE PELVIS AND ASSOCIATED MUSCULOSKELETAL SYSTEMS: GUIDE FOR MEDICAL PRACTITIONERS This appendix will provide a basic description of the associated musculoskeletal system anatomy and function of the pelvis as well as an assessment of these structures. Assessment of posture, gait, lumbar spine, sacroiliac joint, pubic symphysis, abdomen, iliacus, psoas, and pelvic and shoulder alignment will be reviewed. Associated Musculoskeletal Systems Anatomy and Function The bony pelvis is comprised of the sacrum and the two innominate bones (separated into the ilia, pubic bones, and ischia). The anterior superior iliac spine, posterior superior iliac spine, and the iliac crest are important landmarks for locating and assessing pelvic asymmetries common in patients with CPP. 1 The sacrum and ilium form the bilateral sacroiliac joint posteriorly while the pubic bones, along with a fibrocartilaginous disc, form the pubic symphysis anteriorly. In addition, the femoral head, acetabulum, pelvic muscles, ligaments, and fascia create the hip joint and contribute similarly to overall pelvic function. The acetabulum, formed by the fusion of the ilium, ischium, and pubic bones, creates the concave surface that articulates with the femoral head. 2 See Figure 2 in the main body of document and Figure A1 and A2. The hip muscles most frequently involved in pelvic conditions are the iliopsoas, gluteus medius, obturator internus, piriformis, and adductors. Many of these muscles are found to have trigger points and elevated tenderness. 3 Each facilitates hip motion, but the iliopsoas and gluteus medius are particularly important as they assist with overall trunk stability. The coccyx articulates with the sacrum to form the sacrococcygeal joint, which is stabilized by the sacrotuberous and sacrospinous ligaments. The sacroiliac joints have the strongest ligamentous support in the body, mainly through the interosseous sacroiliac and

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
APPENDIX A: ASSESSMENT OF THE PELVIS AND ASSOCIATED MUSCULOSKELETAL SYSTEMS: GUIDE FOR MEDICAL PRACTITIONERS
This appendix will provide a basic description of the associated musculoskeletal system anatomy and
function of the pelvis as well as an assessment of these structures. Assessment of posture, gait, lumbar
spine, sacroiliac joint, pubic symphysis, abdomen, iliacus, psoas, and pelvic and shoulder alignment will
be reviewed.
Associated Musculoskeletal Systems Anatomy and Function
The bony pelvis is comprised of the sacrum and the two innominate bones (separated into the ilia, pubic
bones, and ischia). The anterior superior iliac spine, posterior superior iliac spine, and the iliac crest are
important landmarks for locating and assessing pelvic asymmetries common in patients with CPP.1 The
sacrum and ilium form the bilateral sacroiliac joint posteriorly while the pubic bones, along with a
fibrocartilaginous disc, form the pubic symphysis anteriorly. In addition, the femoral head, acetabulum,
pelvic muscles, ligaments, and fascia create the hip joint and contribute similarly to overall pelvic function.
The acetabulum, formed by the fusion of the ilium, ischium, and pubic bones, creates the concave surface
that articulates with the femoral head.2 See Figure 2 in the main body of document and Figure A1 and A2.
The hip muscles most frequently involved in pelvic conditions are the iliopsoas, gluteus medius, obturator
internus, piriformis, and adductors. Many of these muscles are found to have trigger points and elevated
tenderness.3 Each facilitates hip motion, but the iliopsoas and gluteus medius are particularly important
as they assist with overall trunk stability. The coccyx articulates with the sacrum to form the
sacrococcygeal joint, which is stabilized by the sacrotuberous and sacrospinous ligaments. The sacroiliac
joints have the strongest ligamentous support in the body, mainly through the interosseous sacroiliac and
2
posterior (dorsal) sacroiliac ligaments. Blending with fibers of the posterior sacroiliac ligament, the
sacrotuberous ligament passes posterior to the sacrospinous ligament. The pudendal nerve passes
between these two ligaments where it can become entrapped by localized inflammation or pelvic
instability and lead to perineal pain. Sacroiliac joint dysfunction can manifest clinically as radiculopathy
with sciatica-like symptoms, which can be the result of compression of lower extremity nerve roots over
the joint. Nearly 50% of patients with an MSK diagnosis are found to have sciatica-like pain with
palpation.4,5 See Figure A2.
The sacrum and fifth lumbar vertebrae articulate to form the lumbosacral junction, which is stabilized by
the iliolumbar ligament, lumbar fascia, and multifidi muscles. Progressing cephalad, the thoracolumbar
fascia is critically important in load transfer between the trunk and lower extremities.2 This load transfer
is supported by multiple muscles, including the transverse abdominis, internal and external obliques,
gluteus maximus, latissimus dorsi, and multifidi muscles.6 The abdominal muscles play a significant role
in stability and can influence pelvic symptoms, including pelvic pain, back pain, urgency, and urinary
incontinence. Patients with CPP demonstrated more trigger points and elevated tenderness throughout
the pelvis, hips, and abdomen compared to controls.3
The pelvic girdle, formed by numerous joints, muscles, ligaments, and fascia, is a dynamic structure that
works in concert to allow everyday function. The lumbopelvic-hip complex assists in overall stability and
mobility, bowel and bladder function, and sexual function. Thirty-five muscles attach directly to the
sacrum and/or innominate bone; together with ligaments and fascia, they contribute to motion control
and pelvic girdle function.2
Muscles, fascia, ligaments, and bony structures within and around the pelvis help support the body and
abdominal and pelvic viscera. There is evidence that fascia may not only be comprised of connective tissue
but may actively contract much like smooth muscle and consequently influence MSK dynamics.7 The

3
coccygeus muscles attach bilaterally, helping form the pelvic diaphragm, and assist the LA in providing
support of the pelvic viscera. Although they no longer “wag our tail,” they can become overactive and
tight, causing buttock and coccygeal pain. Pelvic asymmetries can be the result of repetitive daily
activities, pregnancy and delivery, and injury or trauma.8 Overall core support integrates the PFMs (the
“floor of the core”); abdominal, back, and buttock musculature; and the respiratory diaphragm.4
Guide to Assessment of Associated Musculoskeletal Systems
Preparation for the Assessment of Musculoskeletal Systems
Before beginning the MSK examination it is important to be aware of potential neurologic involvement. A
complete and thorough lower extremity neurologic evaluation might be important if there is concern for
an overlapping neurologic diagnosis or if the patient reports any of the following: trauma, progression of
a known neurologic disease, headache, blurry vision, change in behavior, fatigue, change in balance or
coordination/gait, numbness/tingling, weakness, tremor or new onset of bladder or bowel incontinence.
Components of a neurologic examination that may be relevant are myotomal (strength) or manual muscle
strength testing, dermatomal (sensory) testing by light touch or pinprick, deep tendon reflexes,
assessment for lower extremity tone, upper motor neuron signs (Babinski reflex), coordination, balance
and/or gait assessment.
Assessment of Posture
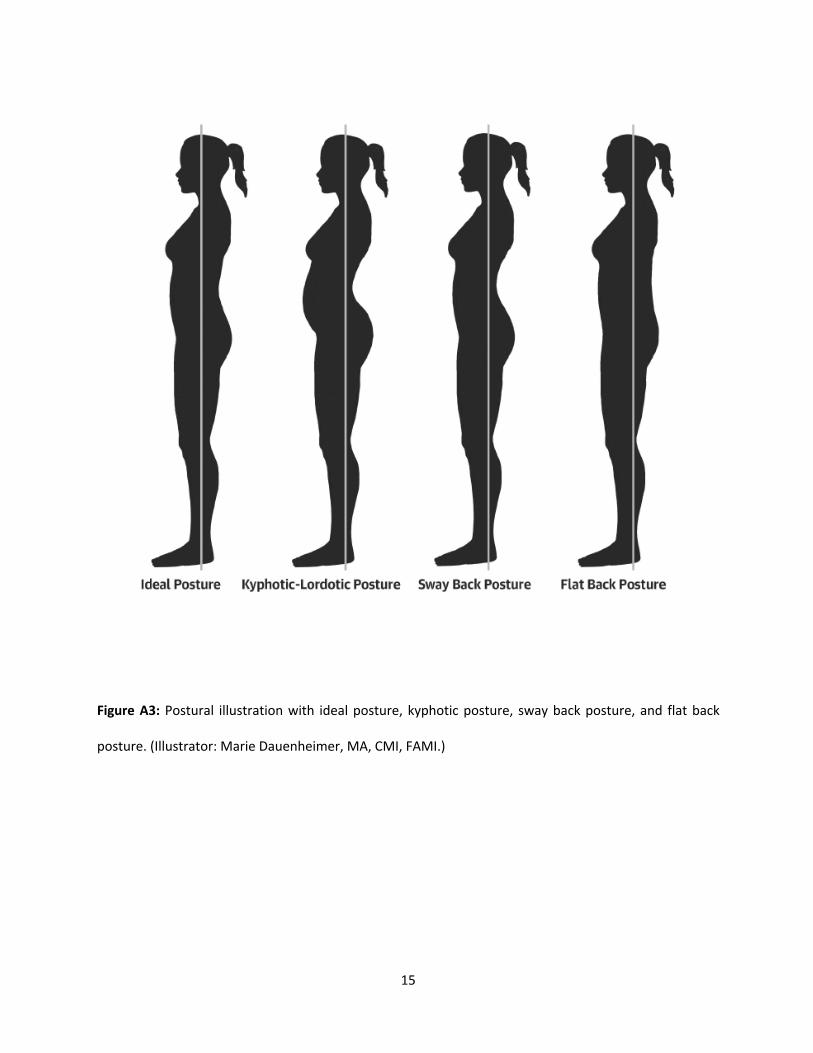
Postural changes, whether preceding the onset of pain or occurring as a consequence, predispose women
to pelvic instability and guarding.1 The human body reflexively finds a way to compensate for weakness,
imbalance in flexibility and pain. For example, when one unconsciously favors one side of the body over
the other, our posture gradually adapts to the imbalance. With time, chronic postural changes force the

4
body to use muscles improperly, often causing muscle spasm, bony changes, and movement dysfunction,
all of which can contribute to pain. See Figure A3.
Postural assessment is an important part of the physical examination. The patient’s posture can provide
insight into presenting complaints, either mild or more severe, such as traumas, injuries, and pathologies.
Posture can allow us a first glimpse of the patients’ overall demeanor which can reveal valuable
information including their self-esteem, level of confidence, energy, and mood. It is important to assess
both static and dynamic postures to ascertain the patient's functional movement.
Ideal standing posture can be measured by examining the patient in the sagittal plane and using an
imaginary line passing down through the middle of the earlobe, mastoid process, shoulder and hip joints,
and slightly in front of the knee and ankle joints. While assessing in the sitting position, the same line runs
through the hip joint. Deviations observed in standing may include a forward head (earlobes in front of
shoulders), a greater curve in the thoracic kyphosis (creating concavity in the upper chest), rounded
shoulders, or a decreased lordosis (tucking of the tailbone and flattening of the lumbar spine causing a
posterior pelvic tilt). From a sagittal view, the dominant shoulder is often depressed (lower) and slightly
protracted (rounded forward). See Figure A3. Changes in alignment and posture can indicate improper
use of muscles and joints which in turn contribute to pelvic symptoms. In addition, it can indicate that
more than just the pelvic floor is involved in the patient’s condition and further assessment is warranted
by a physical therapist.
Assessment of Gait
Observing a patient walk in and out of the clinic can provide valuable information as well. A normal gait
pattern begins with the heel striking the ground rather than the entire foot or toes. The pelvis should
remain level or horizontal, arms should swing with the contralateral (opposite) leg, and there should be

5
minimal torso (trunk) rotation. Abnormal gait patterns arise from traumatic injuries, diseases, or
conditions of neurologic or MSK origin. Even when using assistive devices, such as a walker or cane, the
gait should not deviate too far from the normal pattern unless other impairments are present.
There are two distinct characteristics that suggest tightness resulting from decreased range of motion in
the deep lateral rotators of the hip (piriformis and obturator internus muscles). One important sign is the
duck walk when the patient walks with toes pointed outward in either one or both feet. The second
characteristic is a posterior pelvic tilt observed during the postural assessment.
The most obvious gait deviation due to hip weakness (primarily in the gluteus medius and minimus
muscles) is the Trendelenburg gait. A non-compensated Trendelenburg pattern is visible when the
contralateral hip (ie, right hip) drops because the ipsilateral hip (ie, left hip) abductors are too weak to
stabilize the pelvis and keep it level in stance. A compensated Trendelenburg pattern is observed when
there is an excessive lateral lean in which the shoulders are thrust laterally to keep the center of gravity
over the stance leg. See Figure A4.
Assessment of General strength
Performing manual muscle testing to assess for strength is the preferred method of quantification by PTs;
however, there are functional or transitional movements that can be performed quickly to assess global
strength by all practitioners. Our core includes the pelvic floor, back, gluteal, and abdominal muscles as
well as the respiratory diaphragm. These structures work together to provide support and locomotion for
our entire body; weakness within the core can influence the patient’s overall functional ability. For
example, observing how the patient stands up from the chair can provide information on their lower
extremity strength.

6
● Are they able to stand up from the chair without using their hands? Do their knees come together
(genu valgus) when they are attempting to stand?
● Do they lean forward in a normal pattern (nose over toes) or do they lean backward?
● Are they able to get off the examination table independently?
All of these suggest weakness specifically of core, gluteal, and quadricep muscles. For additional
information, the patient can perform a squat or step up onto a step stool while assessing form for
compensation similar to the items listed above. See Table 3 in the main body of document.
Guide for the Assessment of the Lumbar Spine, and Pelvic Girdle, and
Hips
Preparation for Assessment of the Lumbopelvic and Core Complex
Physical therapists who specialize in women’s and pelvic health are well trained in detailed MSK
examinations; however, this may not be the case in other medical professions. The following information
is presented to educate readers on how to perform brief, external MSK assessments through observation
and/or examination. Assessment should include all or parts of the following: mid-body structures,
including the lumbar spine, sacroiliac joint, pubic symphysis, hip joints, abdomen, and alignment of the
pelvis; posture, both sitting and standing; gait; and general strength testing.9 The findings will provide vital
pieces to the diagnostic puzzle when used in conjunction with standard physical examination. There is
mounting evidence to support the external musculoskeletal assessment, however, greater research on
validation, reliability, and correlation with PFDs is needed. Comprehensive examination as described in
Table 3 in the main body of the document is strongly recommended along with referral and further
evaluation to orthopedic/physical medicine and rehabilitation/physical therapy providers as indicated.

7
Assessment of the Lumbar Spine, Sacroiliac Joint, Pubic Symphysis
Screening the lumbar spine for pain or limitations in movements may indicate mechanical MSK
dysfunction. This includes standing trunk flexion (bending forward), extension (bending backward), lateral
(side) bending and rotation. The degree and quality of motion are equally important to note. Palpation
at/of the lumbar spine can reveal muscular tightness and/or tenderness, which may be primary or
secondary pain generators. As the lower lumbar and sacral nerve roots innervate the PFMs and lower
extremities, it is beneficial to be aware that lumbar spine impairment may compress nerve roots
potentially creating radiculopathy or referred pain.9 See Table 3 in the main body of document.
The sacroiliac joint and pubic symphysis provide stability to the pelvic girdle and help to offset the load
of the trunk to the lower extremities. Reduction in strength and flexibility can influence an individual’s
ability to perform their usual daily activities at their accustomed level. The sacroiliac joints can be
examined through a cluster of special tests established by Laslett et al.10 To rule in a sacroiliac
joint dysfunction, at least 2 test results need to be positive. Pain at the pubic symphysis is best assessed
by direct palpation.11 Another reliable and valid functional test is the Active Straight Leg Raise (ASLR)
test, which assesses the difficulty of the leg raise and the ability of the PF and core muscles to stabilize
the pelvis during weight-bearing. It is performed with the patient supine.12 The quality of movement,
pain, compensations through the lumbar spine, contralateral hip or pelvis and/or change in breathing
pattern are all assessed as the patient lifts one leg 20 cm off the surface. Additionally, the P4/Thigh
Thrust, Faber, or Posterior Pelvic Pain Provocation Test13 can be used. Upon referral to physical therapy,
patients receive a thorough and complete assessment, which may include many of the tests listed here.
See Table 3 in the main body of document.

8
Assessment of the Hip
A screen of hip range of motion can be performed while the patient is in the sitting or supine position.
When in the sitting position, ask the patient to cross her legs, placing one ankle on the opposite knee.
Note the amount and quality of movement. When the patient is supine on the examination table, passive
hip range of motion can be performed by the health care provider by flexing the patient’s hip to 90
degrees, then rotating the lower leg inward and outward. Normal range of motion inward (external
rotation) is 40 degrees and motion outward (internal rotation) is 30 degrees. Note the differences in range
of motion when comparing right to left. See Figure A4.
Muscles that provide stability and allow motion of the hip include the PFMs. Disorders or pain in the hip
can cause gait adaptations that include guarding of the hip muscles, specifically the obturator internus
muscles. Guarding will affect the resting tone of the PFMs and create PFM overactivity. In this setting,
patients may complain of pain at the hip (posterior pelvis, lateral hip, or groin) in conjunction with pain in
the pelvic floor.9
Assessment of the Abdomen, Iliacus, and Psoas and Pelvic Alignment
Palpating the abdomen for tenderness, scar tissue, and restriction is helpful when evaluating pain.9 The
iliopsoas in particular can be a contributor to a number of pelvic floor symptoms. Our deep core stabilizers
(including the iliopsoas and quadratus lumborum), abdominals, lumbar and gluteal musculature along
with the pelvic floor are all extremely important components of movement and stability and work
together as a unit creating our core. Each of these muscle groups has an influence on the other and in
particular on pelvic floor functional ability. It is important to understand both the anatomy and some basic
assessment tools for examining and understanding the patient as a whole. See Table 1 and Table 3 in the
main body of the document, and Figure A1.Musculoskeletal assessment is indicated after ruling out

9
hernias and/or masses with appropriate evaluation and imaging as indicated. Palpating the iliacus and
psoas contraction during hip flexion can identify pain, tightness, or trigger points, which can impact the
PFMs and lumbar spine. Using the finger pads on both hands, gently sink deep into the abdominal cavity
medial to the anterior superior iliac spine. As the iliacus originates along the iliac crest, it can be palpated
with gentle pressure inferior on the ilium as the hip is slightly flexed. To assess the psoas, sink deeper and
more medial in the abdominal cavity during hip flexion. Abdominal trigger points can also be assessed.
Palpate multiple areas on the abdominal wall while asking the patient to slowly contract the rectus
abdominis. Myofascial pain will be exaggerated with active muscle contraction whereas visceral pain will
be diminished or unchanged.4 See Table 1 and Table 3 in the main body of document, and Figure A1 and
Figure A2.
Assessment of Pelvic and Shoulder Alignment Quick visual assessment of the patient’s overall alignment can give the practitioner insight regarding
possible overall pelvic involvement in symptoms. Assessment of pelvic and shoulder girdle alignment
can be performed from the ventral view while standing. In a study by Tu et al, women with chronic
posterior pelvic pain had more frequent abnormal MSK findings than did controls, including asymmetric
iliac crests (61% vs 25%) and pubic symphysis (50% vs 10%), and positive posterior pelvic provocation
testing (37% vs 5%).8 If the palpated points are not equal or symmetrical, the potential for pelvic
asymmetry or instability is present. Palpate the anterior superior iliac spine and shoulder positions
bilaterally, assessing for alignment right to left. From the dorsal view, palpate the posterior superior iliac
spine, iliac crest, and popliteal folds at the knees, assessing for symmetry in alignment. The dominant
shoulder should be slightly lower than the non-dominant one. If there is a dramatic difference or if the
non-dominant is lower, there may be an associated asymmetry in the pelvis. See Table 3 in the main
body of the document and Figure A4. The assessment strategies in this appendix provide the
10
practitioner with tools that may help determine if the associated pelvic structures, the pelvic floor or
both are contributing to the patient’s symptoms.
References
1. Tu FF, Holt J, Gonzales J, et al. Physical therapy evaluation of patients with chronic pelvic pain: a
controlled study. Am J Obstet Gynecol. 2008;198(3):272.e1-272.e7.
doi:10.1016/J.AJOG.2007.09.002
2. Lee D, Lee L-J, Vleeming A, et al. The Pelvic Girdle: An Integration of Clinical Expertise and
Research. 4th ed. Churchill Livingstone; 2011.
3. Sanses TVD, Chelimsky G, McCabe NP, et al. The Pelvis and Beyond: Musculoskeletal Tender
Points in Women with Chronic Pelvic Pain. Clin J Pain. 2016;32(8):659-665.
doi:10.1097/AJP.0000000000000307
4. Lamvu G, Carrillo J, Witzeman K, et al. Musculoskeletal Considerations in Female Patients with
Chronic Pelvic Pain. Semin Reprod Med. 2018;36(2):107-115. doi:10.1055/s-0038-1676085
5. Visser LH, Nijssen PGN, Tijssen CC, et al. Sciatica-like symptoms and the sacroiliac joint: clinical
features and differential diagnosis. Eur Spine J. 2013;22(7):1657-1664. doi:10.1007/s00586-013-
2660-5
6. Sapsford RR, Hodges PW, Richardson CA, Cooper DH, Markwell SJ, Jull GA et al. Co-activation of
the abdominal and pelvic floor muscles during voluntary exercises. Neurourol Urodyn.
2001;20(1):31-42. http://www.ncbi.nlm.nih.gov/pubmed/11135380. Accessed April 10, 2019.
7. Schleip R, Klingler W, Lehmann-Horn F. Active fascial contractility: Fascia may be able to contract
in a smooth muscle-like manner and thereby influence musculoskeletal dynamics. Med
Hypotheses. 2005;65(2):273-277. doi:10.1016/J.MEHY.2005.03.005

11
8. Stein A, Sauder SK, Reale J. The Role of Physical Therapy in Sexual Health in Men and Women:
Evaluation and Treatment. Sex Med Rev. 2019;7(1):46-56. doi:10.1016/j.sxmr.2018.09.003
9. Prather H, Dugan S, Fitzgerald C, et al. Review of Anatomy, Evaluation, and Treatment of
Musculoskeletal Pelvic Floor Pain in Women. PM R. 2009;1(4):346-358.
doi:10.1016/j.pmrj.2009.01.003
10. Laslett M, Aprill CN, McDonald B, et al. Diagnosis of sacroiliac joint pain: validity of individual
provocation tests and composites of tests. Man Ther. 2005;10(3):207-218.
doi:10.1016/j.math.2005.01.003
11. Prather H, Camacho-Soto A. Musculoskeletal etiologies of pelvic pain. Obstet Gynecol Clin North
Am. 2014;41(3):433-442. doi:10.1016/j.ogc.2014.04.004
12. Mens JMA, Vleeming A, Snijders CJ, et al. Reliability and Validity of the Active Straight Leg Raise
Test in Posterior Pelvic Pain Since Pregnancy. Spine (Phila Pa 1976). 2001;26(10):1167-1171.
doi:10.1097/00007632-200105150-
13. Vleeming A, Albert HB, Ostgaard HC, et al. European guidelines for the diagnosis and treatment
of pelvic girdle pain. Eur Spine J. 2008;17(6):794-819. doi:10.1007/s00586-008-0602-4

12
Appendix A Figures

13
Figure A1: Posterior view of bony pelvis with lower lumbar spine and hips included. (Illustrator:
Marie Dauenheimer, MA, CMI, FAMI.)

14
Figure A2: Pelvic bony structure with pelvic core muscles including iliopsoas, psoas, iliacus, and quadratus
lumborum. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI.)
15
Figure A3: Postural illustration with ideal posture, kyphotic posture, sway back posture, and flat back
posture. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI.)

1
Figure A4: Decision tree for assessment of potential pelvic musculoskeletal conditions. Assessment categories include associated
musculoskeletal systems, pelvic floor muscle assessment, and pelvic girdle assessment.
1
Related Documents











