National Team pleased with ‘encouraging’ response to Leadership Development Framework The National Team state that they have had ‘an exceptionally high quality response’ to the Framework from providers in the field of leadership, organisatonal development and NHS commissioning. As you will know, the Framework was launched in July to provide ‘a single overarching framework for the leadership development of all staff in health and care, irrespective of discipline, role or function.’ Included in this PDF Introducing the NHS Leadership Framework Page 2 Supporting Tools Page 2 NHS Leadership Framework - Full Document Pages 3 - 84 1ST ISSUE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
National Team pleased with
‘encouraging’ response to
Leadership Development Framework
The National Team state that they havehad ‘an exceptionally high qualityresponse’ to the Framework fromproviders in the field of leadership,organisatonal development and NHScommissioning. As you will know, theFramework was launched in July toprovide ‘a single overarching frameworkfor the leadership development of allstaff in health and care, irrespective ofdiscipline, role or function.’
Included in this PDF
Introducing the NHS Leadership Framework Page 2
Supporting Tools Page 2
NHS Leadership Framework - Full Document Pages 3 - 84
1STISS
UE

360° Feedback
Introducing the
NHS Leadership Framework The NHS Leadership Framework provides a consistent approach to leadership development for staff in health and care irrespective of discipline, role or function, and represents the foundation of leadership behaviour throughout the NHS. It sets out a single model of leadership for all NHS staff should aspire.
It will be imperative that frontline clinicians and the wider workforce have the leadership knowledge, skills and behaviours to drive radical service redesign and improvement. This will involve working in collaboration across health systems, in developing new models of care, and further developing the skills of the entire workforce. The ability to influence and manage change at the frontline will be central to delivering this.
To enable this change to take place successfully and to support staff in this very important role we will need to further develop the leadership capability within the system.
The NHS Leadership Framework is based on the concept that leadership is not restricted to people who hold designated
leadership roles and where there is a shared responsibility for the success of the organisation, services or care being delivered. Acts of leadership can come from anyone in the organisation and as a model it emphasises the responsibility of all staff in demonstrating appropriate behaviours, in seeking to contribute to the leadership process and to develop and empower the leadership capacity of colleagues.
The NHS Leadership Framework integrates the Medical Leadership Competency Framework (MLCF) and Clinical Leadership Competency Framework (CLCF) and supercedes the Leadership Qualities Framework (LQF). Please visit www.nhsleadership.org.uk/framework.asp to learn more about the framework and how it can be used and applied. Supporting tools
There are a number of supporting tools already available, with more on the way in the coming months.
LeAD is a free and engaging e-learning resource to help clinicians develop their understanding of how their role contributes to managing and leading health services. The sessions are grouped into modules for ease of reference, however they are designed to stand alone providing an open learning pathway to meet individual development needs and interests. LeAD is appropriate for all clinical staff regardless of profession, specialty, or stage of training and offers one
component of an overall leadership training and development programme. There is also an Additional Educational Material area which holds videos, articles and other resources to further augment learning. To register for LeAD, please visit http://www.e-lfh.org.uk/projects/lead/register.html 360° feedback is a powerful tool to help individuals identify where their leadership strengths and development needs lie. The process includes getting confidential feedback from line managers, peers and direct reports. As a result, it gives an individual an insight into other people’s perceptions of their leadership abilities and behaviour. The new Leadership Framework online 360° feedback tool is in the process of being road tested and will be available to colleagues in the service from October 2011 onwards. If you would like to register your interest in the tool, please contact [email protected].
A free self assessment tool helps individuals identify where their leadership strengths and development needs lie, to assist with personal development. For further information and access to the self assessment tool, please visit the Supporting Tools section of the NHS Leadership Framework website.
Colleagues working in the higher education institutions or in workplace training facilities may find the Guidance for Integrating the Clinical Leadership Competency Framework into Education and Training very useful. This document describes the knowledge, skills, attitudes and behaviours required for each domain and provides suggestions for appropriate learning and development activities to be delivered throughout education and training, as well as possible methods of assessment. Please visit the Supporting Tools section of the NHS Leadership Framework website to download.

NHS Leadership Framework

© 2011 Department of Health. All rights reserved.
The NHS Leadership Framework is published on behalf of the Department of Health by NHS Institute forInnovation and Improvement, Coventry House, University of Warwick Campus, Coventry, CV4 7AL.
Publisher: NHS Institute for Innovation and Improvement, Coventry House, University of Warwick Campus,Coventry, CV4 7AL.
This publication may be reproduced and circulated free of charge for non-commercial purposes only by andbetween NHS-funded organisations in England, Scotland, Wales and Northern Ireland staff, and their relatednetworks and officially contracted third parties. This includes the right to reproduce, distribute and transmit thispublication in any form and by any means, including e-mail, photocopying, microfilming, and recording. Noother use may be made of this publication or any part of it except with the prior written permission andapplication for which should be in writing and addressed to the Director of Leadership (and marked ‘re.permissions’). Written permission must always be obtained before any part of this publication is stored in aretrieval system of any nature, or electronically. Reproduction and transmission of this publication must beaccurate, must not be used in any misleading context and must always be accompanied by this Copyright Notice.
Warning: Unauthorised copying, storage, reproduction, adaptation or other use of this publication or any part ofit is strictly prohibited. Doing an unauthorised act in relation to a copyright work may give rise to civil liabilitiesand criminal prosecution.
The Clinical Leadership Competency Framework was created with the agreement of the NHS Institute forInnovation and Improvement and the Academy of Medical Royal Colleges from the Medical LeadershipCompetency Framework which was created, developed and is owned jointly by the NHS Institute for Innovationand Improvement and the Academy of Medical Royal Colleges.
NHS Institute for Innovation and Improvement and Academy of Medical Royal Colleges (2010) MedicalLeadership Competency Framework, 3rd edition, Coventry: NHS Institute for Innovation and Improvement.
© NHS Institute for Innovation and Improvement and Academy of Medical Royal Colleges 2010

Page
Foreword 5
The NHS Leadership Framework 6
Application of the NHS Leadership Framework 11
1. Demonstrating Personal Qualities 131.1 Developing Self Awareness 141.2 Managing Yourself 151.3 Continuing Personal Development 161.4 Acting with Integrity 17
2. Working with Others 192.1 Developing Networks 202.2 Building & Maintaining Relationships 212.3 Encouraging Contribution 222.4 Working within Teams 23
3. Managing Services 253.1 Planning 263.2 Managing Resources 273.3 Managing People 283.4 Managing Performance 29
4. Improving Services 314.1 Ensuring Patient Safety 324.2 Critically Evaluating 334.3 Encouraging Improvement and Innovation 34 4.4 Facilitating Transformation 35
5. Setting Direction 375.1 Identifying the Contexts for Change 38 5.2 Applying Knowledge and Evidence 395.3 Making Decisions 405.4 Evaluating Impact 41
6. Creating the Vision 436.1 Developing the Vision for the Organisation 446.2 Influencing the Vision of the Wider Healthcare System 456.3 Communicating the Vision 466.4 Embodying the Vision 47
7. Delivering the Strategy 497.1 Framing the Strategy 507.2 Developing the Strategy 517.3 Implementing the Strategy 527.4 Embedding the Strategy 53
Acknowledgements 55
Relevant reading 57
Appendix I: The Knowledge and Skills Framework (KSF) 60
Appendix II: Tables combining the indication of behaviours at different 61leadership stages from each domain
Table of Contents
3NHS Leadership Framework


NHS Leadership Framework 5
ForewordI am delighted to introduce the NHS Leadership Framework; it provides a single overarching framework forthe leadership development of all staff in health and care, irrespective of discipline, role or function.
It is underpinned by a consistent set of guiding principles, contained in the NHS Constitution, which reflectthe values of health and care staff. It therefore represents the foundation of leadership behaviour for staffthroughout the NHS, to support all staff to improve quality for our patients.
This is a unique period in the NHS and a time of significant change for health and care services in England,with an unprecedented level of responsibility being devolved to frontline staff. Building on our successes aswe design the future requires bold and thoughtful leadership, rethinking how we work, challenging currentpractice and thinking outside of our own organisational and professional interests.
It will be imperative that frontline clinicians and the wider workforce have the leadership knowledge, skillsand behaviours to drive radical service redesign and improvement. This will involve working in collaborationacross health systems, in developing new models of care, and further developing the skills of the entireworkforce. The ability to influence and manage change at the frontline will be central to delivering this. Thereis no doubt that we must continue to develop the leadership capability within the system. It is on this basisthat the NHS Leadership Framework has been designed.
Based on research and created through extensive consultation, the NHS Leadership Framework has beentailored to the specific needs and environment of the NHS, and is applicable to all staff at any stage of theircareer. It sets out the expectations of leaders at every level of our system and provides guidance to those whocommission leadership development.
The National Leadership Council (NLC) has led this work and I would like to thank everyone who hascontributed to the development of the NHS Leadership Framework.
Sir David NicholsonNHS Chief Executive

The NHS Leadership Framework
IntroductionThe NHS Leadership Framework provides a consistent approach to leadership development for staff in health andcare and represents the foundation of leadership behaviour throughout the NHS. It sets out a single model ofleadership for all NHS staff working in both clinical and non-clinical roles to which all NHS staff should aspire. It isintended as a developmental framework and there are a number of ways the NHS Leadership Framework can beapplied to develop leadership skills and behaviours across the service and to foster a shared understanding ofwhat leadership means in the NHS. The NHS Leadership Framework integrates the Medical LeadershipCompetency Framework (MLCF) and Clinical Leadership Competency Framework (CLCF) and supercedes theLeadership Qualities Framework (LQF).
The NHS Leadership Framework is made up of seven domains which describe leadership knowledge, skills andbehaviour. Staff will exhibit a range of leadership behaviours across these seven domains dependent on thecontext in which they operate, described in four stages. These are defined by their sphere of influence, extent ofresponsibility and accountability, and their impact on services.
Development of the NHS Leadership FrameworkThe National Leadership Council (NLC) commissioned the NHS Leadership Framework in 2010. Fundamental to itsdevelopment was a desire to create a single overarching leadership framework for all staff groups to enable themto understand their progression as a leader and to support the NHS to foster and develop talent.
In developing the NHS Leadership Framework detailed research and consultation with a wide cross section of staffand stakeholders has been undertaken including those with a patient perspective, and those involved inhealthcare outside of the NHS. These include professional bodies, academics, regulators and policy makers – a fulllist is available on page 56.
Those consulted embraced the concept of the NHS Leadership Framework because it affords a common andconsistent approach to professional and leadership development, based on shared values and beliefs which areconsistent with the principles and values of the NHS Constitution1.
1 Department of Health (2010) The NHS Constitution: the NHS belongs to us all. The NHS Constitution can be accessed viahttp://www.nhs.uk/choiceintheNHS/Rightsandpledges/NHSConstitution/Pages/Overview.aspx
NHS Leadership Framework6

NHS Leadership Framework 7
Underpinning leadership principles of the NHS Leadership FrameworkPeople understand the term ‘leadership’ in many different ways. Perhaps the most common stereotypic ideais of the individual, powerful, charismatic leader with followers clearly in subordinate roles. Such situations doexist but are quite limited, rather outdated and by the very rarity of charismatic qualities make it a poor modelfor leadership development. This way of thinking tends to focus on the individual as a leader rather than theprocesses of leadership.
A more modern conceptualisation sees leadership as something to be used by all but at different levels. This model of leadership is often described as shared, or distributed, leadership and is especially appropriatewhere tasks are more complex and highly interdependent – as in healthcare. It is a universal model such thatall staff can contribute to the leadership task where and when their expertise and qualities are relevant andappropriate to the context in which they work. Not everyone is necessarily a leader but everyone cancontribute to the leadership process by using the behaviours described in the five core domains of the NHSLeadership Framework: demonstrating personal qualities, working with others, managing services, improvingservices and setting direction.
The National Health Service (NHS) principles and valuesThe NHS Constitution establishes the principles and values of the NHS in England. The Constitution setsout rights to which patients, public and staff are entitled, and pledges which the NHS is committed toachieve, together with responsibilities which the public, patients and staff owe to one another to ensurethat the NHS operates fairly and effectively.
1.The NHS provides a comprehensive service, available to all irrespective of gender, race, disability, age,sexual orientation, religion or belief.
2. Access to NHS services is based on clinical need, not an individual’s ability to pay.
3. The NHS aspires to the highest standards of excellence and professionalism – in the provision of high-quality care that is safe, effective and focused on patient experience.
4. NHS services must reflect the needs and preferences of patients, their families and their carers.
5. The NHS works across organisational boundaries and in partnership with other organisations in theinterest of patients, local communities and the wider population.
6. The NHS is committed to providing best value for taxpayers’ money and the most effective, fair andsustainable use of finite resources.
7. The NHS is accountable to the public, communities and patients that it serves.
These seven key principles guide the NHS in all it does and they are underpinned by the following corevalues. Patients, public and staff have helped develop this expression of values that inspire passion in theNHS and should guide it in the 21st century.
The NHS values provide common ground for co-operation to achieve shared aspirations:
Respect and dignity Commitment to quality of care Compassion Improving lives Working together for patientsEveryone counts.

As a model it emphasises the responsibility of all staff, in demonstrating appropriate behaviours, to seek tocontribute to the leadership process and to develop and empower the leadership capacity of colleagues.
The final two domains of the NHS Leadership Framework, creating the vision and delivering the strategy,recognise that a relatively small group of people do hold designated senior positional roles, and are requiredto act as leaders in formal hierarchical positions. These two domains therefore focus more on the contributionof individual leaders rather than the general leadership process.
Evolution of the NHS Leadership FrameworkThe NHS Leadership Framework has been designed to build on learning of the following internationally recognisedbest practice standards for leadership development. It was also informed by analysis of existing NHS leadershipdata and a review of contemporary leadership literature.
• The Leadership Qualities Framework (LQF)2. The LQF 360° tool has been used extensively by staff in roles aboveand beyond the executive population that the original LQF research was based upon. The NHS LeadershipFramework addresses this by describing leadership behaviours for all staff depending on their role and thecontext in which they work.
• The Medical Leadership Competency Framework (MLCF)3. Jointly developed by The Academy of Medical RoyalColleges and the NHS Institute for Innovation and Improvement, the MLCF describes the leadershipcompetencies doctors need to become more actively involved in the planning, delivery and transformation ofservices for patients. It applies to all medical students and doctors throughout their careers.
• The Clinical Leadership Competency Framework (CLCF)4. The NLC commissioned the NHS Institute to test theleadership competencies in the MLCF to see whether they could be applied to all healthcare professionals.These have been endorsed by the clinical professions and will be progressively embedded within professionalregulation and into education and training.
NHS Leadership Framework8
2 NHS Institute for Innovation and Improvement (2005) NHS Leadership Qualities Framework http://www.nhsleadershipqualities.nhs.uk
3 NHS Institute for Innovation and Improvement and Academy of Medical Royal Colleges (2010) Medical Leadership CompetencyFramework. 3rd ed. NHS Institute for Innovation and Improvement: Coventry.
4 Department of Health (2011). Clinical Leadership Competency Framework. NHS Institute for Innovation and Improvement: Coventry.
SettingDirection
PersonalQualities
Delivering theService
Broadscanning
Seizingthe future
Intellectualflexibility
Politicalastuteness
Drive forresults
Collaborativeworking
Effectiveand strategicinfluencing
Leading changethrough people
Self beliefSelf awareness
Self managementDrive for improvement
Personal integrity
Holding toaccount
Empoweringothers
LQF CLCF and MLCF NHS Leadership Framework
The five domains of the CLCF and the MLCF were informed by the LQF, and are shared with the core five domainsof the NHS Leadership Framework to create a single overarching leadership framework.
NHS Leadership Framework 9
Design and structure of the NHS Leadership FrameworkThe NHS Leadership Framework provides a standardised and consistent approach to leadership development forNHS staff and represents the foundation of leadership behaviour throughout the NHS. The needs of the peoplewho use services have always been central to healthcare. However, if we are going to transform services, acting onwhat really matters to patients and the public is essential and involves the active participation of patients, carers,community representatives, community groups and the public in how services are planned, delivered andevaluated5.
Delivering services to patients, service users, carers and the public is therefore at the heart of the NHS LeadershipFramework. All staff work hard to improve services for people.
The NHS Leadership Framework is comprised of seven domains. Within each domain there are four categoriescalled elements and each of these elements is further divided into four descriptors. These statements describethe leadership behaviours which are underpinned by the relevant knowledge, skills and attributes all staff shouldbe able to demonstrate radiating out from those of the individual to those within the wider system.
We use the word ‘patient’ throughout the NHS Leadership Framework to generically cover patients, serviceusers, and all those who receive healthcare. Similarly, the word ‘other’ is used to describe all colleagues fromany discipline and organisation, as well as patients, service users, carers and the public.
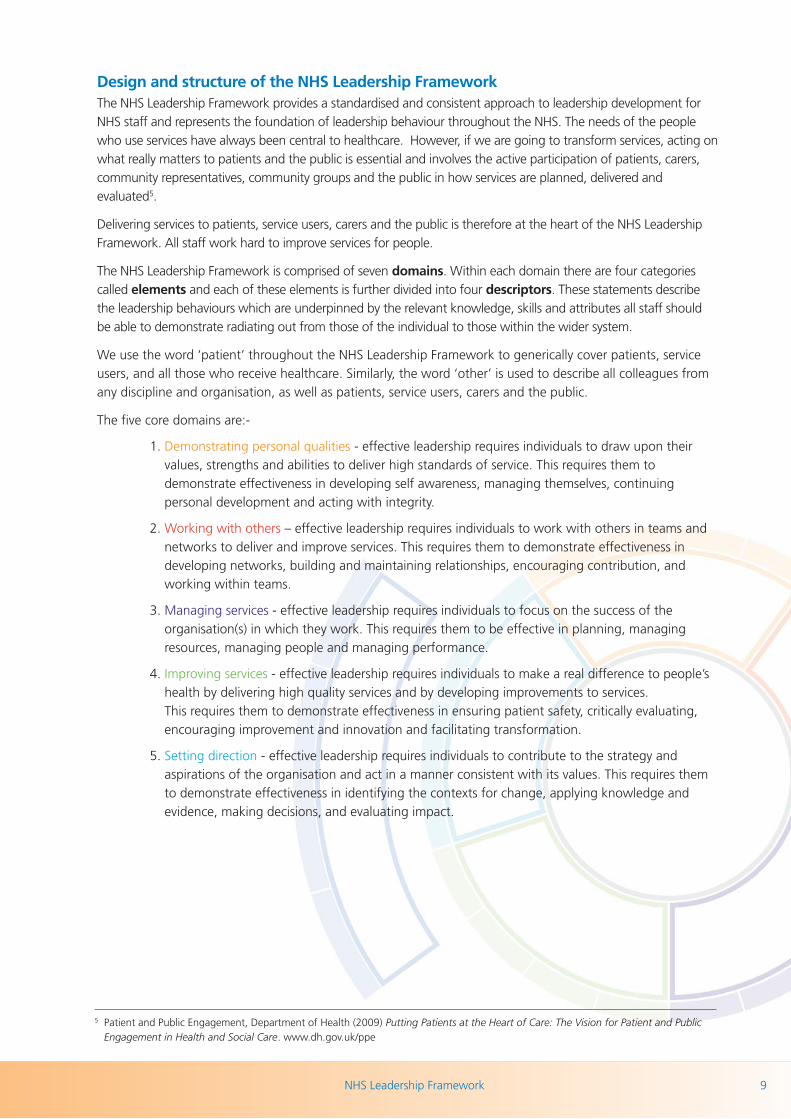
The five core domains are:-
1. Demonstrating personal qualities - effective leadership requires individuals to draw upon theirvalues, strengths and abilities to deliver high standards of service. This requires them todemonstrate effectiveness in developing self awareness, managing themselves, continuingpersonal development and acting with integrity.
2. Working with others – effective leadership requires individuals to work with others in teams andnetworks to deliver and improve services. This requires them to demonstrate effectiveness indeveloping networks, building and maintaining relationships, encouraging contribution, andworking within teams.
3. Managing services - effective leadership requires individuals to focus on the success of theorganisation(s) in which they work. This requires them to be effective in planning, managingresources, managing people and managing performance.
4. Improving services - effective leadership requires individuals to make a real difference to people’shealth by delivering high quality services and by developing improvements to services. This requires them to demonstrate effectiveness in ensuring patient safety, critically evaluating,encouraging improvement and innovation and facilitating transformation.
5. Setting direction - effective leadership requires individuals to contribute to the strategy andaspirations of the organisation and act in a manner consistent with its values. This requires themto demonstrate effectiveness in identifying the contexts for change, applying knowledge andevidence, making decisions, and evaluating impact.
5 Patient and Public Engagement, Department of Health (2009) Putting Patients at the Heart of Care: The Vision for Patient and PublicEngagement in Health and Social Care. www.dh.gov.uk/ppe

NHS Leadership Framework10
There are two additional domains which apply particularly but not exclusively to individuals in seniorpositional leadership roles.
6. Creating the vision - those in senior positional leadership roles create a compelling vision for thefuture, and communicate this within and across organisations. This requires them to demonstrateeffectiveness in developing the vision for the organisation, influencing the vision of the widerhealthcare system, communicating the vision and embodying the vision.
7. Delivering the strategy – those in senior positional leadership roles deliver the strategic vision bydeveloping and agreeing strategic plans and ensuring that these are translated into achievableoperational plans. This requires them to demonstrate effectiveness in framing the strategy,developing the strategy, implementing the strategy and embedding the strategy.
The leadership contextThe application and opportunity to demonstrate leadership will differ and the context in which competencecan be achieved will become more complex and demanding with career progression. We have therefore usedfour stages to describe this and to help staff understand their progression and development as a leader. They are:
Stage 1 Own practice/immediate team - is about building personal relationships with patients andcolleagues, often working as part of a multi-disciplinary team. Staff need to recognise problems and workwith others to solve them. The impact of the decisions staff take at this level will be limited in terms of risk.
Stage 2 Whole service/across teams - is about building relationships within and across teams, recognisingproblems and solving them. At this level, staff will need to be more conscious of the risks that their decisionsmay pose for self and others for a successful outcome.
Stage 3 Across services/wider organisation - is about working across teams and departments within thewider organisation. Staff will challenge the appropriateness of solutions to complex problems. The potentialrisk associated with their decisions will have a wider impact on the service.
Stage 4 Whole organisation/healthcare system - is about building broader partnerships across and outsidetraditional organisational boundaries that are sustainable and replicable. At this level leaders will be dealingwith multi-faceted problems and coming up with innovative solutions to those problems. They may lead at anational/international level and would be required to participate in whole systems thinking, finding new waysof working and leading transformational change. Their decisions may have significant impact on thereputation of the NHS and outcomes and would be critical to the future of the NHS.

NHS Leadership Framework 11
Application of the NHS LeadershipFramework and supporting toolsThe NHS Leadership Framework sets out the standard for leadership to which all staff in health and careshould aspire. It is intended for use as a developmental framework and there are many ways it can beapplied, for example:
• To raise awareness that effective leadership is needed across the whole organisation
• To underpin a talent management strategy
• As part of an existing leadership development programme
• To inform the design and commissioning of training and development programmes
• To develop individual leadership skills
• As part of team development
• To enhance existing appraisal systems
• To inform an organisation’s recruitment and retention processes.
The NHS Leadership Framework is structured to assist the user to understand how they relate to each of theseven domains. Staff will exhibit a range of leadership behaviours across these seven domains dependent onthe context in which they operate. To improve the quality and safety of health and care services, it is essentialthat staff are competent in each of the five core leadership domains: demonstrating personal qualities,working with others, managing services, improving services and setting direction. The two other domains ofthe NHS Leadership Framework, creating the vision and delivering the strategy, focus more on the role andcontribution of individual leaders.
To help users understand and apply the NHS Leadership Framework each domain is divided into fourelements and each of these elements is further divided into four descriptive statements which describe thebehaviours all staff should be able to demonstrate.
To assist users there are a number of indicators across a variety of work place situations which illustrate the typeof activity staff could be demonstrating relevant to each element and stage as well as examples of behaviours ifthey are not. These indicators are intended to be examples and only apply to part of each element.
The CLCF and MLCF are also available to specifically provide staff with clinically based examples and learningand development scenarios across the five core domains shared with the NHS Leadership Framework.
Supporting toolsA self assessment and 360° feedback tool support the NHS Leadership Framework; in addition an onlinedevelopment guide signposts development opportunities for each of the seven domains. The 360° is apowerful tool to help individuals identify where their leadership strengths and development needs lie. The process includes getting confidential feedback from line managers, peers and direct reports. As a result, itgives an individual an insight into other people’s perceptions of their leadership abilities and behaviour.
To assist with integrating the competencies into postgraduate curriculaand learning experiences, there is the LeAD e-learning resource. LeAD isa range of more than 50 short e-learning sessions that support theknowledge base of the MLCF and the CLCF. Examples and contexts
range across various different fields and specialties, all aimed at improving patient care and services. LeAD addresses how clinicians can develop their leadership contribution in clinical settings. Originally it was

produced to support medical trainees, however new sessions are being added to broaden out the learning toall clinical professions. In addition the resources section of each session includes examples of the MLCF andCLCF in practice and ideas for further development, useful to both the individual learner and also to trainersor supervisors.
LeAD is available on the National Learning Management System and through e-Learning for Healthcare(www.e-lfh.org.uk/LeAD).
How the NHS Leadership Framework fits with other career and skills based frameworks The NHS Leadership Framework is designed to be used in conjunction with career or skills based frameworkslike the Nursing Careers Framework and the NHS Knowledge and Skills Framework (KSF).
For example, a line manager may use the KSF to support an appraisal and development review whereas staffmay use the NHS Leadership Framework to understand where their leadership strengths and developmentneeds lie - for further information on the KSF see Appendix I on page 60.
The full NHS Leadership Framework follows, complete with examples in practice and work-placeindicators to demonstrate the practical application of the framework. Please note the indicators areexamples only and intended as a guide across part of the relevant element.
NHS Leadership Framework12

Dem
onst
rati
ng P
erso
nal Q
ualit
ies
DemonstratingPersonal Qualities


NHS Leadership Framework 13
1. Demonstrating Personal Qualities
Effective leadership requires individuals to draw upon their values, strengths and abilities to deliver highstandards of service. To do so, they must demonstrate effectiveness in:
• Developing Self Awareness
• Managing Yourself
• Continuing Personal Development
• Acting with Integrity.

NHS Leadership Framework14
1. Demonstrating Personal Qualities1.1 Developing Self Awareness
Leaders develop self awareness: being aware of theirown values, principles and assumptions and by beingable to learn from experiences.
Competent leaders:
• Recognise and articulate their own values andprinciples, understanding how these may differ fromthose of other individuals and groups
• Identify their own strengths and limitations, theimpact of their behaviour on others, and the effect ofstress on their own behaviour
• Identify their own emotions and prejudices andunderstand how these can affect their judgment andbehaviour
• Obtain, analyse and act on feedback from a variety ofsources.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Reflects on how factors such as own values, prejudices and emotions influence theirjudgement, behaviour and self belief. Uses feedback from appraisals and other sources toconsider personal impact and change behaviour. Understands personal sources of stress.
Appreciates the impact they have on others and the impact others have on them.Routinely seeks feedback and adapts their behaviour appropriately.
Reflects on their interactions with a wide and diverse range of individuals and groups fromwithin and beyond their immediate service/organisation. Challenges and refreshes ownvalues, beliefs, leadership styles and approaches. Overtly role models the giving andreceiving of feedback.
Uses sophisticated tools and sources to continuously learn about their leadership impact inthe wider health and care community and improve their effectiveness as a senior leader.Understands how pressures associated with carrying out a high profile role impact on themand their performance.
Contextual Indicators

NHS Leadership Framework 15
1. Demonstrating Personal Qualities1.2 Managing Yourself
Leaders manage themselves: organising andmanaging themselves while taking account of theneeds and priorities of others.
Competent leaders:
• Manage the impact of their emotions on theirbehaviour with consideration of the impact onothers
• Are reliable in meeting their responsibilities andcommitments to consistently high standards
• Ensure that their plans and actions are flexible, andtake account of the needs and work patterns ofothers
• Plan their workload and activities to fulfil workrequirements and commitments, withoutcompromising their own health.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Plans and manages own time effectively and fulfils work requirements and commitmentsto a high standard, without compromising own health and wellbeing. Remains calm andfocused under pressure.
Ensures that own work plans and priorities fit with the needs of others involved indelivering services. Demonstrates flexibility and sensitivity to service requirements andremains assertive in pursuing service goals.
Successfully manages a range of personal and organisational demands and pressures.Demonstrates tenacity and resilience. Overcomes setbacks where goals cannot be achievedand quickly refocuses. Is visible and accessible to others.
Remains focused on strategic goals when faced with competing and, at times, conflictingdemands arising from differing priorities. Identifies where they need to personally getinvolved to achieve the most benefit for the organisation and wider healthcare system.
Contextual Indicators

NHS Leadership Framework16
1. Demonstrating Personal Qualities1.3 Continuing Personal Development
Leaders actively engage in continuing personaldevelopment: learning through participating incontinuing professional development and fromexperience and feedback.
Competent leaders:
• Actively seek opportunities and challenges forpersonal learning and development
• Acknowledge mistakes and treat them as learningopportunities
• Participate in continuing professional developmentactivities
• Change their behaviour in the light of feedback andreflection.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Takes responsibilities for own personal development and seeks opportunities for learning.Strives to put learning into practice.
Puts self forward for challenging assignments and projects which will develop strengthsand address development areas.
Acts as an exemplar for others in managing their continuous personal development.Facilitates the development of a learning culture.
Develops through systematically scanning the external environment and exploring leadingedge thinking and best practice. Applies learning to build and refresh the service. Treats challenge as a positive force for improvement.
Contextual Indicators

NHS Leadership Framework 17
1. Demonstrating Personal Qualities1.4 Acting with Integrity
Leaders act with integrity: behaving in an open,honest and ethical manner.
Competent leaders:
• Uphold personal and professional ethics and values,taking into account the values of the organisationand respecting the culture, beliefs and abilities ofindividuals
• Communicate effectively with individuals,appreciating their social, cultural, religious andethnic backgrounds and their age, gender andabilities
• Value, respect and promote equality and diversity
• Take appropriate action if ethics and values arecompromised.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Behaves in an open, honest and inclusive manner, upholding personal and organisationalethics and values. Shows respect for the needs of others and promotes equality and diversity.
Acts as a role model for others in demonstrating integrity and inclusiveness in all aspects oftheir work. Challenges where organisational values are compromised.
Creates an open, honest and inclusive culture in accordance with clear principles andvalues. Ensures equity of access to services and creates an environment where people fromall backgrounds can excel.
Assures standards of integrity are maintained across the service and communicates theimportance of always adopting an ethical and inclusive approach.
Contextual Indicators

NHS Leadership Framework18
1. Demonstrating Personal QualitiesGeneric behaviours observed if individual is not yet demonstrating this domain:• Does not understand own emotions or recognise the impact of own behaviour on others• Approaches tasks in a disorganised way and plans are not realistic• Unable to discuss own strengths and development needs and spends little time on development• Demonstrates behaviours that are counter to core values of openness, inclusiveness, honesty and equality• Lacks confidence in own abilities to deliver results.
Examples in Practice for Demonstrating Personal Qualities:
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Radiotherapy Physicist X needed to focus her attention on her own professional development in order to meetthe state registration criteria with the Health Professionals Council. Accreditation required her to create aportfolio of evidence for various aspects of her work that demonstrated how she has developed the necessaryskills and experience to meet the standards set for registration. Radiotherapy Physicist X recognised the need tomanage her own workload with her educational and Continual Professional Development (CPD) requirementsto ensure that her professional goals were met without impacting on her day-to-day responsibilities.
Surgical Ward Sister C noted that her junior team was in awe of her and not always comfortable questioningwhat she said. She asked the team to challenge her more if they disagreed with her and admitted that she didhave a strong personality which might be seen as intimidating at times. In subsequent meetings sheencouraged openness by not reacting as defensively when nurses began to question what she said. She praised them when their ideas would benefit patients and thanked them when their comments wouldenable her to make improvements to her own performance. Surgical Ward Sister C set up a 360-degreefeedback process for the team designed to encourage the sharing of perspectives so that team members couldgain insight from some personal feedback on their performance. Despite her heavy workload she made thetime to sit with them and discuss their feedback one-to-one.
Associate Directorate Manager E recognised that he needed to spend time increasing his knowledge and self-awareness in order to make himself a more rounded leader at this level. Before moving into the AssociateDirector role, he undertook a number of secondments in different areas of the organisation to strengthen hisknowledge outside of his own functional specialism. He regularly requested feedback on his own leadershipstyle in order to gain insight into what he could do better. Feedback was that others were not always clearabout his expectations. To counter his natural tendency to leave the details to others, Associate DirectorateManager E spent time discussing his expectations with others. This not only helped build strong trustingrelationships, but enabled Associate Directorate Manager E to understand his team’s working methods andalign his approach with their preferences.
Chief Executive Officer Y knows how important it is to operate with a high level of emotional intelligence, selfconfidence and integrity at a senior level, particularly when balancing national and regional considerations,weighing up the competing needs of organisations, and considering the views of Members of Parliament. Thisis especially relevant when interacting with the Secretary of State, Members of Parliament, Counsellors andsenior officials within the Department of Health. Chief Executive Officer Y used his skills when two Trusts putforward a business case for a new specialist unit to be located on their patch when rationalisation meant thatfunding would only be available for one unit. He was required to adopt an objective perspective and includeother factors in the final decision that linked to how the decision would be aligned with national priorities at astrategic level including QIPP and diversity considerations. This then needed to be communicated sensitively toall parties involved. He took the time to speak to politicians and affected groups in person pointing out howthe decision taken would benefit all members of the community. He spent many hours negotiating counteroffers and compromises between senior executives when each of the parties raised equally valid points whichmade achieving a win-win outcome particularly challenging.

Working with Others
Wo
rkin
g w
ith
Oth
ers


NHS Leadership Framework 19
2. Working with Others
Effective leadership requires individuals to work with others in teams and networks to deliver and improveservices. To do so, they must demonstrate effectiveness in:
• Developing Networks
• Building and Maintaining Relationships
• Encouraging Contribution
• Working within Teams.
NHS Leadership Framework20
2. Working with Others2.1 Developing Networks
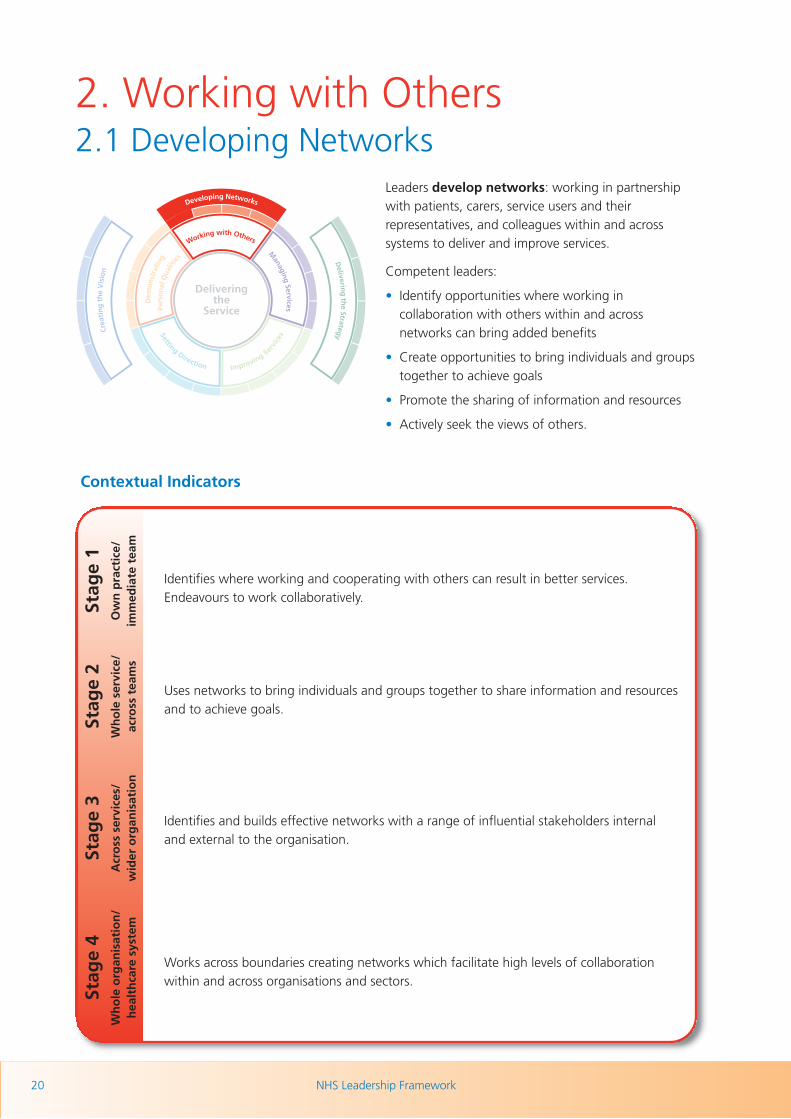
Leaders develop networks: working in partnershipwith patients, carers, service users and theirrepresentatives, and colleagues within and acrosssystems to deliver and improve services.
Competent leaders:
• Identify opportunities where working incollaboration with others within and acrossnetworks can bring added benefits
• Create opportunities to bring individuals and groupstogether to achieve goals
• Promote the sharing of information and resources
• Actively seek the views of others.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Identifies where working and cooperating with others can result in better services.Endeavours to work collaboratively.
Uses networks to bring individuals and groups together to share information and resourcesand to achieve goals.
Identifies and builds effective networks with a range of influential stakeholders internaland external to the organisation.
Works across boundaries creating networks which facilitate high levels of collaborationwithin and across organisations and sectors.
Contextual Indicators

NHS Leadership Framework 21
2. Working with Others2.2 Building and Maintaining Relationships
Leaders build and maintain relationships: listening,supporting others, gaining trust and showingunderstanding.
Competent leaders:
• Listen to others and recognise different perspectives
• Empathise and take into account the needs andfeelings of others
• Communicate effectively with individuals andgroups, and act as a positive role model
• Gain and maintain the trust and support ofcolleagues.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Communicates with and listens to others, recognising different perspectives. Empathises andtakes into account the needs and feelings of others. Gains and maintains trust and support.
Builds and maintains relationships with a range of individuals involved in delivering theservice. Manages sensitivities between individuals and groups.
Builds and nurtures trusting relationships at all levels within and across services andorganisational boundaries.
Builds and maintains sustainable strategic alliances across the system and other sectors.Has high impact when interacting with others at all levels.
Contextual Indicators

NHS Leadership Framework22
2. Working with Others2.3 Encouraging Contribution
Leaders encourage contribution: creating anenvironment where others have the opportunity tocontribute.
Competent leaders:
• Provide encouragement, and the opportunity forpeople to engage in decision-making and tochallenge constructively
• Respect, value and acknowledge the roles,contributions and expertise of others
• Employ strategies to manage conflict of interest anddifferences of opinion
• Keep the focus of contribution on delivering andimproving services to patients.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Seeks and acknowledges the views and input of others. Shows respect for thecontributions and challenges of others.
Creates a supportive environment which encourages others to express diverse opinions andengage in decision- making. Constructively challenges suggestions and reconcilesconflicting views.
Integrates the contributions of a diverse range of stakeholders, being open and honestabout the extent to which contributions can be acted upon.
Creates systems which encourage contribution throughout the organisation. Invites contribution from different sectors to bring about improvements.
Contextual Indicators

NHS Leadership Framework 23
2. Working with Others2.4 Working within Teams
Leaders work within teams: to deliver and improveservices.
Competent leaders:
• Have a clear sense of their role, responsibilities andpurpose within the team
• Adopt a team approach, acknowledging andappreciating efforts, contributions and compromises
• Recognise the common purpose of the team andrespect team decisions
• Are willing to lead a team, involving the right peopleat the right time.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Understands roles, responsibilities and purpose within the team. Adopts a collaborativeapproach and respects team decisions.
Helps lead others towards common goals, providing clear objectives and offeringappropriate support. Shows awareness of team dynamics and acts to promote effectiveteam working. Appreciates the efforts of others.
Takes on recognised positional leadership roles within the organisation. Builds high performinginclusive teams that contribute to productive and efficient health and care services. Promotesautonomy and empowerment and maintains a sense of optimism and confidence.
Contributes to and leads senior teams. Enables others to take on leadershipresponsibilities, building high level leadership capability and capacity from a diverse rangeof backgrounds.
Contextual Indicators

NHS Leadership Framework24
2. Working with OthersGeneric behaviours observed if individual is not yet demonstrating this domain:• Fails to network with others and/or allows relationships to deteriorate• Fails to win the support and respect of others• Does not encourage others to contribute ideas• Does not adopt a collaborative approach.
Examples in Practice for Working with Others:
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Student social worker B is on a practice placement with a qualified social worker in a large inner city GPpractice. Whilst working with an elderly Asian man who has been newly diagnosed with diabetes she becomesconscious of the culture and familial factors affecting the man’s treatment and maintenance. Her supervisorsuggests that she explores what other support might be available to him. B approaches Diabetes UK, the localCVS and seeks advice from a contact at the Gurdwara. She is able to put her client in touch with a self-helpgroup for people with diabetes and a worker at the local Indian community centre. Together they start aweekly luncheon group for Asian elders which provides help and support on a number of health issues. Thisgreatly improves the patient’s response to his illness and helps maintain good diabetes care.
Chief Speech and Language Therapist G spent time maintaining good working relationships with her team oftherapists by providing support and guidance. One of the ways she did this was organising monthly meetingsto share information and discuss issues. At one such meeting she encouraged a team member to share someservice descriptions which he had written up. She suggested these were used as a blueprint for writing up thistype of information in the future. Speech and Language Therapist G also identified an opportunity for amember of her team to work with her on a new assignment involving video fluoroscopy. It was an area thatthe team member had previously expressed an interest in and provided the individual with the opportunity totake a leading role on the assignment.
Associate Medical Director M supported Lead Clinicians, PCT Medical Directors, Medical Advisors andDirectorate Managers both within and outside the Trust in setting up an Acute Stroke Unit. Associate MedicalDirector M was involved in leading and chairing meetings to develop the business plan for the initiative. Heworked closely with colleagues over whom he had limited authority and was required to use his influencingskills to persuade people as to the benefits of the proposal. By communicating the Trust’s vision, explaininghow individuals and teams could contribute to the strategy, clarifying roles and drawing on his expertise, hewas able to help them understand how the new stroke unit would enable them to achieve their owndepartmental goals. When a difference of opinion arose as to how the Acute Stroke Unit should be co-ordinated, Associate Medical Director M set up a meeting to allow all stakeholders to discuss their perspectivesand debate alternative strategies rationally. He facilitated the discussion and mediated between conflictingopinions in such a way that a successful outcome was ultimately achieved.
Chief Allied Health Professions Officer Z’s role requires her to focus on external issues, collaborate withGovernment Ministers and translate policy into practical strategies for the delivery of allied health professionalservices across the Service. She engenders trust and support from others who may not report into her directlyby drawing on her personal credibility and superior influencing skills. She met with the allied healthprofessional leads within each of the regional strategic health authorities on a six weekly basis to share insightsand discuss issues around government policy. Working in partnership with these leads, Chief Allied HealthProfessions Officer Z guided them though the process of creating a narrative outlining how a governmentwhite paper was likely to impact on allied health professionals and the services they offered. She influencedthe leads by outlining the benefits arising from the white paper for patients and staff and the long-termconsequences of remaining with the status quo. She also talked through the drivers that were making changeinevitable. Chief Allied Health Professions Officer Z encouraged all allied health professional leads to worktogether and link up with general practitioner consortia to proactively demonstrate the value they could offerto patients.

Man
agin
g S
ervi
ces
Managing Services


NHS Leadership Framework 25
3. Managing Services
Effective leadership requires individuals to focus on the success of the organisation(s) in which they work.
To do so, they must be effective in:
• Planning
• Managing Resources
• Managing People
• Managing Performance.

NHS Leadership Framework26
3. Managing Services3.1 Planning
Leaders engage in planning: actively contributing toplans to achieve service goals.
Competent leaders:
• Support plans for services that are part of thestrategy for the wider healthcare system
• Gather feedback from patients, service users andcolleagues to help develop plans
• Contribute their expertise to planning processes
• Appraise options in terms of benefits and risks.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Contributes ideas to service plans, incorporating feedback from others - including a diverserange of patients, service users and colleagues.
Works collaboratively to develop business cases and service plans that supportorganisational objectives, appraising them in terms of benefits and risks.
Leads service design and planning processes. Communicates and keeps others informed ofstrategic and operational plans, progress and outcomes.
Anticipates the impact of health trends and develops strategic plans that will have asignificant impact on the organisation and wider healthcare system. Ensures strategicobjectives are translated into operational plans.
Contextual Indicators

NHS Leadership Framework 27
3. Managing Services3.2 Managing Resources
Leaders manage resources: knowing what resourcesare available and using their influence to ensure thatresources are used efficiently and safely, and reflect thediversity of needs.
Competent leaders:
• Accurately identify the appropriate type and level ofresources required to deliver safe and effectiveservices
• Ensure services are delivered within allocatedresources
• Minimise waste
• Take action when resources are not being usedefficiently and effectively.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Understands what resources are available and organises the appropriate type and level ofresources required to deliver safe and efficient services.
Identifies resource requirements associated with delivering services. Manages resources andtakes action to ensure their effective and efficient use.
Forecasts resource requirements associated with delivering complex services efficiently andeffectively. Manages resources taking into account the impact of national and local policiesand constraints.
Strategically manages resources across the organisation and wider healthcare system.
Contextual Indicators

NHS Leadership Framework28
3. Managing Services3.3 Managing People
Leaders manage people: providing direction,reviewing performance, motivating others, andpromoting equality and diversity.
Competent leaders:
• Provide guidance and direction for others using theskills of team members effectively
• Review the performance of the team members toensure that planned service outcomes are met
• Support team members to develop their roles andresponsibilities
• Support others to provide good patient care andbetter services.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Supports others in delivering high quality services and excellence in health and care.
Provides others with clear purpose and direction. Helps others in developing their roles andresponsibilities.
Motivates and coaches individuals and teams to strengthen their performance and assistthem with developing their own capabilities and skills. Aligns individual developmentneeds with service goals.
Inspires and supports leaders to mobilise diverse teams that are committed to and alignedwith organisational values and goals. Engages with and influences senior leaders and keystakeholders to deliver joined up services.
Contextual Indicators

NHS Leadership Framework 29
3. Managing Services3.4 Managing Performance
Leaders manage performance: holding themselvesand others accountable for service outcomes.
Competent leaders:
• Analyse information from a range of sources aboutperformance
• Take action to improve performance
• Take responsibility for tackling difficult issues
• Build learning from experience into future plans.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Uses information and data about performance to identify improvements which willstrengthen services.
Works with others to set and monitor performance standards, addressing areas whereperformance objectives are not achieved.
Establishes rigorous performance measures. Holds self, individuals and teams to accountfor achieving performance standards. Challenges when service expectations are not beingmet and takes corrective action.
Promotes an inclusive culture that enables people to perform their best, ensuring thatappropriate performance management systems are in place and that performance data issystematically evaluated and fed into future plans.
Contextual Indicators

NHS Leadership Framework30
3. Managing ServicesGeneric behaviours observed if individual is not yet demonstrating this domain:• Disorganised or unstructured approach to planning• Wastes resources or fails to monitor them effectively• Does not effectively manage and develop people• Fails to identify and address performance issues.
Examples in Practice for Managing Services:
Stag
e 4
S
tag
e 3
S
tag
e 2
Sta
ge
1
Biomedical Scientist Z was asked to get involved in trialling a new Clostridium difficile kit that would result inthe strengthening of service outcomes for patients. She conducted a risk assessment on the kit and analysedthe strengths and weaknesses of the product. This included assessing factors such as the speed and accuracyof diagnosis provided by the kit thereby helping to ensure that a cost effective, high quality product waspurchased. Biomedical Scientist Z used feedback from colleagues when considering how to test the efficiencyof the equipment. She compared the performance of the new kit with performance data from old kits andconducted a literature review on alternative options available to ensure she was up to date with the latestdevelopments in the field. Following the trial, the new kit was put into operation and the speed and accuracywith which patients were diagnosed improved significantly.
Deputy Physiotherapist Manager E undertook a service review of the Medical Assessment unit. By looking atdata on the types and numbers of patients seen and the staff cover required, she took the decision to split theunit into two sections. She met with the Medical Directorate team to ensure this met with their requirements.She created a business case for recruiting an additional team leader. Deputy Physiotherapist Manager E thensupported a member of her staff who volunteered to take on the role of team leader in the interim. She provided advice and encouragement to the individual who appeared to lack sufficient confidence dealingwith the complexities of the situation. When a misunderstanding occurred between two members of the team,Deputy Physiotherapist Manager E worked with the interim team manager to manage the situation before itescalated and impacted on service delivery.
After taking up his post, Head of Operations P found a disparate group of directorates each operatingindependently in ‘silos’ and not managing services in a joined up manner. Head of Operations P introducedweekly Business Operational and Performance (BOPS) meetings where he spent time listening to the views ofthe team and demonstrated that each had a valuable perspective which could benefit others in terms ofconsidering efficiencies. He noted that silo behaviour existed largely because the culture previously washierarchical and revolved around the professional status of each area. Head of Operations P developed a‘decision tree’ tool to assist team members with challenging their own thinking and helped them realise that asa group they were able to achieve more than they could on their own. As the team began to trust him andunderstood what he was trying to achieve he began to challenge them more as part of their ongoingdevelopment. Together the team began to jointly prioritise actions and looked at opportunities for sharingresources to help one another deliver a better quality service to patients.
Chief Nursing Officer P is involved in an initiative to increase the number of health professionals. This was inresponse to changing government policy brought about by an ageing UK population creating more demandfor services. She worked with colleagues to gather information from a range of parties including politicians,special advisors, trade union representatives and health visitors, to further understand governmentrequirements and establish future resourcing strategies. Her first priority was to formulate a governance modelto clearly communicate the purpose of the initiative. Chief Nursing Officer P then looked at developing asuccession planning strategy designed to co-ordinate future resourcing requirements with regional needs. This included debating and refining future strategic imperatives, establishing performance expectations andreviewing resources across regions.
Improving Services
Imp
rovi
ng
Ser
vice
s


NHS Leadership Framework 31
4. Improving Services
Effective leadership requires individuals to make a real difference to people’s health by delivering high qualityservices and by developing improvements to services. To do so, they much demonstrate effectiveness in:
• Ensuring Patient Safety
• Critically Evaluating
• Encouraging Improvement and Innovation
• Facilitating Transformation.

NHS Leadership Framework32
4. Improving Services4.1 Ensuring Patient Safety
Leaders ensure patient safety: assessing andmanaging the risk to patients associated with servicedevelopments, balancing economic considerationswith the need for patient safety.
Competent leaders:
• Identify and quantify the risk to patients usinginformation from a range of sources
• Use evidence, both positive and negative, to identifyoptions
• Use systematic ways of assessing and minimising risk
• Monitor the effects and outcomes of change.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Puts the safety of patients and service users at the heart of their thinking in delivering andimproving services. Takes action to report or rectify shortfalls in patient safety.
Reviews practice to improve standards of patient safety and minimise risk. Monitors theimpact of service change on patient safety.
Develops and maintains audit and risk management systems which will drive serviceimprovement and patient safety.
Creates a culture that prioritises the health, safety and security of patients and serviceusers. Delivers assurance that patient safety underpins policies, processes and systems.
Contextual Indicators

NHS Leadership Framework 33
4. Improving Services4.2 Critically Evaluating
Leaders critically evaluate: being able to thinkanalytically, conceptually and to identify where servicescan be improved, working individually or as part of ateam.
Competent leaders:
• Obtain and act on patient, carer and service userfeedback and experiences
• Assess and analyse processes using up-to-dateimprovement methodologies
• Identify healthcare improvements and createsolutions through collaborative working
• Appraise options, and plan and take action toimplement and evaluate improvements.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Uses feedback from patients, carers and service users to contribute to healthcareimprovements.
Engages with others to critically evaluate services and create ideas for improvements.
Synthesises complex information to identify potential improvements to services. Identifiespotential barriers to service improvement.
Benchmarks the wider organisation against examples of best practice in healthcare andother sectors. Evaluates options for improving services in line with future advances.
Contextual Indicators

NHS Leadership Framework34
4. Improving Services4.3 Encouraging Improvement and Innovation
Leaders encourage improvement and innovation:creating a climate of continuous service improvement.
Competent leaders:
• Question the status quo
• Act as a positive role model for innovation
• Encourage dialogue and debate with a wide rangeof people
• Develop creative solutions to transform services andcare.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Questions established practices which do not add value. Puts forward creative suggestionsto improve the quality of service provided.
Acts as a positive role model for innovation. Encourages dialogue and debate in thedevelopment of new ideas with a wide range of people.
Challenges colleagues’ thinking to find better and more effective ways of delivering servicesand quality. Accesses creativity and innovation from relevant individuals and groups.
Drives a culture of innovation and improvement. Integrates radical and innovative approachesinto strategic plans to make the NHS a leader in the provision of healthcare services.
Contextual Indicators

NHS Leadership Framework 35
4. Improving Services4.4 Facilitating Transformation
Leaders facilitate transformation: activelycontributing to change processes that lead to improvinghealthcare.
Competent leaders:
• Model the change expected
• Articulate the need for change and its impact onpeople and services
• Promote changes leading to systems redesign
• Motivate and focus a group to accomplish change.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Articulates the need for changes to processes and systems, acknowledging the impact onpeople and services.
Focuses self and others on achieving changes to systems and processes which will lead toimproved services.
Energises others to drive change that will improve health and care services. Activelymanages the change process, drawing on models of effective change management.Recognises and addresses the impact of change on people and services.
Inspires others to take bold action and make important advances in how services aredelivered. Removes organisational obstacles to change and creates new structures andprocesses to facilitate transformation.
Contextual Indicators

NHS Leadership Framework36
4. Improving ServicesGeneric behaviours observed if individual is not yet demonstrating this domain:• Overlooks the need to put patients at the forefront of their thinking• Does not question/evaluate current processes and practices• Maintains the status quo and sticks with traditional outdated ways of doing things• Fails to implement change or implements change for change’s sake.
Examples in Practice for Improving Services:
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Physician B has been undertaking a major piece of audit work on the management of thromboprophylaxis.Physician B worked with a local Thrombosis Committee to collect and critically evaluate data relating to care ofpatients with thrombosis and compared the results with a set of defined standards. Physician B presented the resultsto the Thrombosis Committee who had responsibility for implementing policies on the management ofthromboprophylaxis. He recommended changes suggesting that a number of adjustments be made to currentworking practices including creating risk assessment sheets for patients and modifying blood charts, to ensurepatient safety and improve patient outcomes.
Specialist Orthoptist F took responsibility for implementing a new eye screening programme aimed at providing highquality eye tests for school children with learning disabilities. He wrote a proposal on the advantages of providingclinics in schools and worked closely with school governors and head teachers to educate them of the benefits.Despite facing initial challenges, the eye screening programme was implemented. Specialist Orthoptist F evaluatedthe programme some months later, by conducting an audit. He asked parents to comment on the new set up andreceived very positive feedback. Children were seen more quickly and were less stressed due to being treated in achild friendly environment. Parents also commented on how much easier it was to attend appointments now thatthey were scheduled on school premises.
Directorate Senior Business Manager T used his experience outside of the NHS to bring a fresh perspective todealing with service delivery improvements. He encouraged clinical staff to develop a mindset that viewed patientsin a broader sense as ‘customers’ rather than as just NHS patients. Directorate Senior Business Manager Tchallenged staff by asking them if a customer in another industry would be satisfied with waiting for a product forthirty weeks. After discussions with the team he identified that there were poor data systems in place. To achieve a‘quick win’ he asked his team to implement a cost effective tracking system that documented the patient’s journeyand helped identify where there were potential bottlenecks with processing patients through the system. Thetracking system was well received by staff and patients who saw tangible benefits in terms of time and moneysavings as well as increased patient satisfaction. Other areas within the NHS have subsequently asked about howthey might make use of this cost effective, easy to design tracking system.
Associate Medical Director S led a national initiative to transform emergency care through the delivery of ambulatoryemergency care to eliminate the need for overnight stay for certain conditions. The impact and benefits of thewidespread adoption of this would be comparable to the adoption of day-case surgery which has transformedinpatient elective surgical services. Dr S observed the delivery of ambulatory emergency care in a range of hospitalsover a two year period and identified 49 clinical scenarios where early senior assessment by a competent clinicaldecision-maker would result in immediate diagnosis, treatment and rapid discharge, avoiding the need for anovernight stay. He estimated that approximately 22 per cent of current non-elective admissions with at least oneovernight stay could be managed in this way with a potential saving to the NHS of up to £350 million annually, as aconservative estimate. Dr S published these clinical scenarios in the Directory of Ambulatory Emergency Care forAdults which was adopted as one of the national quality indicators and is well supported by professional bodies as amodel of care which is deliverable. All scenarios in the directory have evidence for the concept and the evidencebase for effectiveness and safety is building over time. Dr S now also has a role as Clinical Lead of the EmergencyCare Intensive Support Team in which he supports and encourages others to transform their clinical practice inemergency services. He estimates that 60-70 per cent of units have already changed their practice and have startedto implement the concept of ambulatory emergency care as described within the Directory.

Sett
ing
Dir
ecti
on
Setting Direction


NHS Leadership Framework 37
5. Setting Direction
Effective leadership requires individuals to contribute to the strategy and aspirations of the organisation andact in a manner consistent with its values. To do so, they must demonstrate effectiveness in:
• Identifying the Contexts for Change
• Applying Knowledge and Evidence
• Making Decisions
• Evaluating Impact.

NHS Leadership Framework38
5. Setting Direction5.1 Identifying the Contexts for Change
Leaders identify the contexts for change: beingaware of the range of factors to be taken into account.
Competent leaders:
• Demonstrate awareness of the political, social,technical, economic, organisational and professionalenvironment
• Understand and interpret relevant legislation andaccountability frameworks
• Anticipate and prepare for the future by scanningfor ideas, best practice and emerging trends that willhave an impact on health outcomes
• Develop and communicate aspirations.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Understands the range of factors which determine why changes are made.
Identifies the external and internal drivers of change and communicates the rationale forchange to others.
Actively seeks to learn about external factors which will impact on services. Interprets themeaning of these for services and incorporates them into service plans and actions.
Synthesises knowledge from a broad range of sources. Identifies future challenges andimperatives that will create the need for change and move the organisation and the widerhealthcare system in new directions. Influences the context for change in the best interestsof services and service users.
Contextual Indicators

NHS Leadership Framework 39
5. Setting Direction5.2 Applying Knowledge and Evidence
Leaders apply knowledge and evidence: gatheringinformation to produce an evidence-based challengeto systems and processes in order to identifyopportunities for service improvements.
Competent leaders:
• Use appropriate methods to gather data andinformation
• Carry out analysis against an evidence-based criteriaset
• Use information to challenge existing practices andprocesses
• Influence others to use knowledge and evidence toachieve best practice.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Gathers data and information about aspects of the service, analyses evidence and uses thisknowledge to suggest changes that will improve services in the future.
Obtains and analyses information about services and pathways to inform future direction.Supports and encourages others to use knowledge and evidence to inform decisions aboutthe future of services.
Understands the complex interdependencies across a range of services. Applies knowledge to set future direction.
Uses knowledge, evidence and experience of national and international developments inhealth and social care to influence the future development of health and care services.
Contextual Indicators

NHS Leadership Framework40
5. Setting Direction5.3 Making Decisions
Leaders make decisions: using their values, and theevidence, to make good decisions.
Competent leaders:
• Participate in and contribute to organisationaldecision-making processes
• Act in a manner consistent with the values andpriorities of their organisation and profession
• Educate and inform key people who influence andmake decisions
• Contribute their unique perspective to team,department, system and organisational decisions.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Consults with others and contributes to decisions about the future direction/vision of theirservice.
Involves key people and groups in making decisions. Actively engages in formal andinformal decision-making processes about the future of services.
Remains accountable for making timely decisions in complex situations. Modifies decisionsand flexes direction when faced with new information or changing circumstances.
Ensures that corporate decision-making is rigorous and takes account of the full range offactors impinging on the future direction of the organisation and the wider healthcaresystem. Can operate without all the facts. Takes unpopular decisions when in the bestinterests of health and care in the long term.
Contextual Indicators

NHS Leadership Framework 41
5. Setting Direction5.4 Evaluating Impact
Leaders evaluate impact: measuring and evaluatingoutcomes, taking corrective action where necessaryand by being held to account for their decisions.
Competent leaders:
• Test and evaluate new service options
• Standardise and promote new approaches
• Overcome barriers to implementation
• Formally and informally disseminate good practice.
Stag
e 4
St
age
3
Stag
e 2
Stag
e 1
Wh
ole
org
anis
atio
n/
Acr
oss
ser
vice
s/W
ho
le s
ervi
ce/
Ow
n p
ract
ice/
hea
lth
care
sys
tem
wid
er o
rgan
isat
ion
acro
ss t
eam
sim
med
iate
tea
m
Assesses the effects of change on service delivery and patient outcomes. Makes recommendations for future improvements.
Evaluates and embeds approaches and working methods which have proved to beeffective into the working practices of teams and individuals.
Identifies gains which can be applied elsewhere in the organisation and incorporates these intooperational/business plans. Disseminates learning from changes which have been introduced.
Synthesises learning arising from changes which have been introduced and incorporatesthese into strategic plans. Shares learning with the wider health and care community.
Contextual Indicators

NHS Leadership Framework42
5. Setting DirectionGeneric behaviours observed if individual is not yet demonstrating this domain:• Unaware of political, social, technical, economic, organisational factors that impact on the future of the
service /organisation• Does not use an evidence-base for decision-making• Makes poor decisions about the future• Fails to evaluate the impact of previous decisions and actions.
Examples in Practice for Setting Direction:
Stag
e 4
Stag
e 3
S
tag
e 2
S
tag
e 1
Learning and Development Coordinator D learned of new national guidance regarding information governancewhich required all staff to undertake annual training in data protection. D had been aware of high profile caseswhere data protection measures had been inadequate and reported in the press, from sectors other than the NHS,and understood the importance of training to prevent similar occurrences within her trust. D identified thatcompliance with training in data protection in the trust was only 13 per cent and agreed a target to increase this to95 per cent over an eight month period. She introduced mandatory training to achieve this. She regularlymonitored attendance rates, updated managers with statistical data about uptake and worked hard to raiseawareness of the importance of training. After just six months the compliance rate reached 64 per cent and wasexpected to reach the target on time. As a result of this initiative, the uptake of statutory training overall increasedacross the trust, and training has been reconfigured to achieve even higher attendance rates.
Falls Lead K realised that the local ambulance service was ideal for identifying people prone to falling. Fromfeedback he received from physiotherapists and the falls team, he constructed a questionnaire to collect details ofthe patient and their fall. When they deal with a person who has fallen, all of the ambulance officers now fax aform to the falls team, which assesses patients and refers them to physiotherapy as needed. Providingphysiotherapy for these patients led to the number of repeat falls being reduced, close to 4,000 fewer falls victims ayear. Comprehensive risk assessments have been effective in eliminating a lot of trolley waits, bed days and returnvisits to hospital. This reduction in falls has saved the ambulance service more than £400,000 in 18 months, moneythat has been redirected into improving existing services.
Clinical services lead V is working for a community health service and has become aware that a new contract toprovide a service to tackle adult obesity among the borough’s ethnically diverse communities was being put out totender. He led work with physiotherapists, dietitians, psychologists, sports medicine clinicians and a local charity todevelop and submit a joint bid. This focused its business case on addressing obesity through community-basedactivity, optimising integrated models of care and achieving long-term financial advantages through ill-healthprevention to demonstrate value and cost-effectiveness. The central initiative within the proposal was forprofessional staff to train lay community figures within the charity to provide information on exercise to clients, andfor outcome measures to be implemented at the start and end of the programme. The joint bid was awarded atender for a year.
Dr K is a senior partner in a GP practice which had been one of the first wave pathfinder consortia for GPcommissioning. He identified the need for clinicians from across a range of professions to develop a new kind ofcollegiate network outside existing membership organisations, which would share learning and best practice duringthe early stages of GP commissioning. He was concerned that the development and implementation of GPcommissioning should be done in a way which accurately reflected policy and which used the experience ofclinicians. Dr K took on the additional role of National Clinical Commissioning Network Lead and, over a period of10 months, identified 400 clinical leaders from across the country and supported them to become activeparticipants in the network which was used to exchange views, share success stories and information about localchallenges. Stories about how services had been changed and improved through GP commissioning could beaccessed via the network very quickly, providing rapid feedback on progress, and a collective voice for primary careto speak directly to policy makers. Dr K’s success in this venture is based upon high credibility amongst his clinicalcolleagues, the respect he has earned from others, and his accessibility to those he supports within the network.

Cre
atin
g t
he
Vis
ion
Creating the Vision


NHS Leadership Framework 43
6. Creating the Vision
Effective leadership involves creating a compelling vision for the future, and communicating this within andacross organisations. This requires individuals to demonstrate effectiveness in:
• Developing the Vision for the Organisation
• Influencing the Vision of the Wider Healthcare System
• Communicating the Vision
• Embodying the Vision.

NHS Leadership Framework44
6. Creating the Vision6.1 Developing the Vision for the Organisation
Those in senior positional leadership roles develop thevision for the organisation, looking to the future todetermine the direction for the organisation. They:
• Actively engage with colleagues and key influencers,including patients and public, about the future ofthe organisation
• Broadly scan and analyse the full range of factorsthat will impact upon the organisation, to createlikely scenarios for its future
• Create a vision which is bold, innovative andreflects the core values of the NHS
• Continuously ensure that the organisation’s vision iscompatible with future developments within thewider healthcare system.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Actively engages a diverse range of key stakeholders in creating a bold, innovative, sharedvision which reflects the future needs and aspirations of the population and the futuredirection of health and care services. Thinks broadly and aligns the vision to the NHS corevalues and the values of the wider healthcare system.
Contextual Indicators

NHS Leadership Framework 45
6. Creating the Vision6.2 Influencing the Vision of the WiderHealthcare System
Those in senior positional leadership roles work withpartners across organisations to influence the visionof the wider healthcare system. They:
• Seek opportunities to engage in debate about thefuture of health and care related services
• Work in partnership with others in the healthcaresystem to develop a shared vision
• Negotiate compromises in the interests of betterpatient services
• Influence key decision-makers who determine futuregovernment policy that impacts on the NHS and itsservices.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Actively participates in and leads on debates about the future of health, wellbeing andrelated services. Manages political interests, balancing tensions between organisationalaspirations and the wider environment. Shapes and influences local, regional and nationalhealth priorities and agendas.
Contextual Indicators

NHS Leadership Framework46
6. Creating the Vision6.3 Communicating the Vision
Those in senior positional leadership rolescommunicate the vision and motivate others towork towards achieving it. They:
• Communicate their ideas and enthusiasm about thefuture of the organisation and its servicesconfidently and in a way which engages and inspiresothers
• Express the vision clearly, unambiguously andvigorously
• Ensure that stakeholders within and beyond theimmediate organisation are aware of the vision andany likely impact it may have on them
• Take time to build critical support for the vision andensure it is shared and owned by those who will becommunicating it.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Clearly communicates the vision in a way that engages and empowers others. Uses enthusiasm and energy to inspire others and encourage joint ownership of the vision.Anticipates and constructively addresses challenge.
Contextual Indicators

NHS Leadership Framework 47
6. Creating the Vision6.4 Embodying the Vision
Those in senior positional leadership roles embodythe vision by behaving in ways which are entirelyconsistent with the vision and values of theorganisation. They:
• Act as a role model, behaving in a manner whichreflects the values and principles inherent in thevision
• Demonstrate confidence, self belief, tenacity andintegrity in pursuing the vision
• Challenge behaviours which are not consistent withthe vision
• Identify symbols, rituals and routines within theorganisation which are not consistent with thevision, and replace them with ones that are.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Consistently displays passion for the vision and demonstrates personal commitment to itthrough their day-to-day actions. Uses personal credibility to act as a convincing advocatefor the vision.
Contextual Indicators

NHS Leadership Framework48
6. Creating the VisionGeneric behaviours observed if individual is not yet demonstrating this domain:• Does not involve others in creating and defining the vision• Does not align their vision with the wider health and care agenda• Misses opportunities to communicate and share understanding of the vision with others• Lacks enthusiasm and commitment for driving the vision.
Examples in Practice for Creating the Vision:
Stag
e 4
St
age
3
Stag
e 1
& 2
While the prime responsibility for Creating the Vision rests with senior leaders, it is expected that staff at all stageswill contribute to the vision of the organisation by offering their perspective and professional judgment. Staff atstages 1 and 2 are often those closest to patients and service users which puts them in a unique position to ensurethat patients’ best interests are represented in the organisation’s vision.
Deputy Director of Nursing Quality & Workforce has been working with the Executive team to help determinewhether the existing vision for her area remained relevant in the light of future changes to the way the NHS wouldoperate. This involved conducting a gap analysis to identify where her team needed to be both in the short andlonger-term and establish whether the existing vision and strategy was suitable for achieving organisational goals.Reviews were organised and different stakeholder groups were encouraged to contribute to determining whatservices should be provided to patients and how the services should be structured and run. Deputy Director ofNursing Quality & Workforce helped the groups consider the interdependencies between nursing, social servicesand the local authority and how this impacted on the provision of future services. She identified that far more focusneeded to be placed on quality and safety than had been the case in the past. She involved her staff in developingvalue and culture statements for the service to align them with the future vision and strategy. She also set up aninnovative and experimental Chief Executive blog which allowed staff to receive regular updates on the strategy.This proved to be a successful initiative as it enabled staff to access and respond to real-time messages from theChief Executive about the future of the organisation.
Director of Primary Care Improvement X has worked with the executive team on the formulation of a primary careand community services vision for the future. She outlined how she helped review the strategy ensuring that itaccounted for key themes such as patient empowerment, quality, prevention and leadership. She spent timespeaking to staff to share a national perspective on issues. Ten road shows were conducted to support local deliveryand make the strategy relevant within a regional context. Using her knowledge acquired through going to events,making visits and attending small meetings she was able to provide a unique holistic perspective on the NHS thatdemonstrated her understanding of issues at the grassroots level. Director of Primary Improvement X showedresilience when answering objections relating to issues such as uncertainty about the future and reframed them in away that made others aware of the need, and encouraged them, to take appropriate risks and operate outside oftheir comfort zones.
Del
iver
ing
th
e St
rate
gy
Delivering the Strategy


NHS Leadership Framework 49
7. Delivering the Strategy
Effective leadership involves delivering the strategy by developing and agreeing strategic plans that placepatient care at the heart of the service, and ensuring that these are translated into achievable operationalplans. This requires individuals to demonstrate effectiveness in:
• Framing the Strategy
• Developing the Strategy
• Developing the Strategy
• Embedding the Strategy.

NHS Leadership Framework50
7. Delivering the Strategy7.1 Framing the Strategy
Those in senior positional leadership roles identifystrategic options for the organisation and draw upon awide range of information, knowledge and experiencein order to frame the strategy. They:
• Take account of the culture, history and long termunderlying issues for the organisation
• Use sound organisational theory to inform thedevelopment of strategy
• Identify best practice which can be applied to theorganisation
• Identify strategic options which will deliver theorganisation’s vision.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Critically reviews relevant thinking, ideas and best practice and applies whole systemsthinking in order to conceptualise a strategy in line with the vision.
Contextual Indicators

NHS Leadership Framework 51
7. Delivering the Strategy7.2 Developing the Strategy
Those in senior positional leadership roles engage withcolleagues and key stakeholders to develop theorganisation’s strategy. They:
• Engage with key individuals and groups to formulatestrategic plans to meet the vision
• Strive to understand others’ agendas, motivationsand drivers in order to develop strategy which issustainable
• Create strategic plans which are challenging yetrealistic and achievable
• Identify and mitigate uncertainties and risksassociated with strategic choices.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Integrates the views of a broad range of stakeholders to develop a coherent, joined up andsustainable strategy. Assesses organisational readiness for change. Manages the risks,political sensitivities and environmental uncertainties involved.
Contextual Indicators

NHS Leadership Framework52
7. Delivering the Strategy7.3 Implementing the Strategy
Those in senior positional leadership roles areentrepreneurial in that they organise, manage andassume the risks of the organisation in order toimplement the strategy. They:
• Ensure that strategic plans are translated intoworkable operational plans, identifying risks, criticalsuccess factors and evaluation measures
• Identify and strengthen organisational capabilitiesrequired to deliver the strategy
• Establish clear accountability for the delivery of allelements of the strategy, hold people to accountand expect to be held to account themselves
• Respond quickly and decisively to developmentswhich require a change in strategy.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Responds constructively to challenge. Puts systems, structures, processes, resources andplans in place to deliver the strategy. Establishes accountabilities and holds people in local,regional, and national structures to account for jointly delivering strategic and operationalplans. Demonstrates flexibility when changes required.
Contextual Indicators
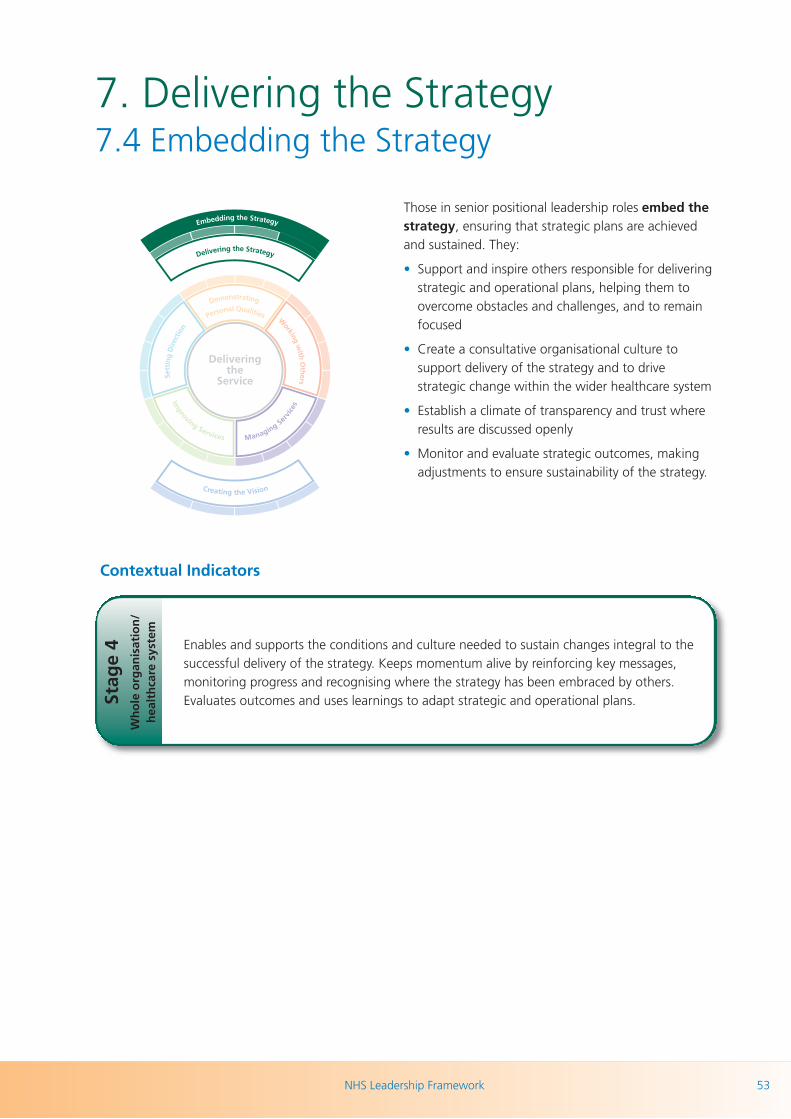
NHS Leadership Framework 53
7. Delivering the Strategy7.4 Embedding the Strategy
Those in senior positional leadership roles embed thestrategy, ensuring that strategic plans are achievedand sustained. They:
• Support and inspire others responsible for deliveringstrategic and operational plans, helping them toovercome obstacles and challenges, and to remainfocused
• Create a consultative organisational culture tosupport delivery of the strategy and to drivestrategic change within the wider healthcare system
• Establish a climate of transparency and trust whereresults are discussed openly
• Monitor and evaluate strategic outcomes, makingadjustments to ensure sustainability of the strategy.
Stag
e 4
W
ho
le o
rgan
isat
ion
/h
ealt
hca
re s
yste
m
Enables and supports the conditions and culture needed to sustain changes integral to thesuccessful delivery of the strategy. Keeps momentum alive by reinforcing key messages,monitoring progress and recognising where the strategy has been embraced by others.Evaluates outcomes and uses learnings to adapt strategic and operational plans.
Contextual Indicators

NHS Leadership Framework54
7. Delivering the StrategyGeneric behaviours observed if individual is not yet demonstrating this domain:• Does not align the strategy with local, national and/or wider health care system requirements• Works to develop the strategy in isolation without input or feedback from others• Absolves oneself of responsibility for holding others to account• Fails to enable an organisational culture that embraces the strategy.
Examples in Practice for Delivering the Strategy:
Stag
e 4
St
age
3
Stag
e 1
& 2
While the ultimate accountability for Delivering the Strategy rests with senior leaders, the actual delivery of strategyis undertaken by everyone in the organisation and it is everyone’s responsibility to ensure that their plans andactions are in line with and contribute to the organisation’s goals.
Associate Medical Director R took steps to ensure that his organisation was compliant with the Chief Executive’sstrategy to meet new national policy guidelines around best practice in delivering high quality patient care. This initiative was important as the reputation of the organisation was linked to a successful outcome. A number ofprocesses and procedures were identified as being below standard. A particular issue that proved to be challengingwas getting commitment to implement basic procedures such as using World Health Organisation (WHO)checklists. A climate existed where staff failed to recognise the importance of the issue and in some cases felt thatthe matter was not pertinent to their circumstances. Associate Medical Director R used meetings to reinforce hismessage, presented statistical results, shared real stories highlighting the impact of non-compliance on patients andencouraged professional teams to work together as a single integrated unit. His approach resonated with his targetaudience and contributed to compliance data improving with 95 per cent of WHO checklists being used effectivelyby staff. However, a further area for improvement was identified which was making effective use of checklists atthe patient checkout stage. Associate Medical Director R took prompt action and, with the support of his teams,considered devolving the checkout stage of the process to middle grade doctors and theatre staff or anaesthetistsas a possible solution. Ultimately the option chosen was successful and his overall approach was highly valued bythe Chief Executive.
Chief Executive Officer P has adopted a long term perspective on issues when reconfiguring maternity services in hisregion. Reconfiguration of maternity services involved moving from thirteen sites down to eight sites as part of arationalisation process. The rationale for this reconfiguration of services was to provide a better overall service to thecommunity and save lives as well as reduce waste. Chief Executive Officer P spent time acknowledging concernsand the perspectives of different parties in various forums. He needed to be particularly sensitive given that thedecision had a significant political dimension to it. Constituents for eight Members of Parliament (MPs) wrote toParliament and the press saying that they were unhappy about the prospect of losing their local maternity unit as aresult of the proposed reconfiguration. Chief Executive Officer P’s approach was to spend time consulting with theMPs, the local community and other interested parties and lay out the case for change based on ethical argumentsaround patient safety as well as by providing a sound business and financial rationale for his approach. ChiefExecutive Officer P described how he communicated his views in an open and honest manner and showed awillingness to meet community representatives face-to-face to discuss issues as well as face cross examination fromthe media on television. All of these actions built credibility and trust with stakeholders and ensured the processwas viewed as being consultative in nature, transparent and fair. Key to building partnerships was spending timeliaising and engaging with the wider public service and local authorities. This included finding outcomes that wouldbe of benefit to all parties and would in turn help drive the initiative forward with broad support.

NHS Leadership Framework 55
AcknowledgementsThe NLC would like to thank the many individuals who have contributed to development of the NHSLeadership Framework:
Department of HealthJan Sobieraj, Director of LeadershipStephen Collins, Deputy Director of Talent and LeadershipAnne Hackett*, Workforce Leadership Team - Policy Lead
Elizabeth Manero, Lay advisorMike Medas, Lay advisor
SHA Leadership Leads#: Martin Lewis, Caroline Wigley,Peter Lees, Deborah McKenzie, Elaine Readhead, RachelMunton, Amanda Grindall
National Leadership CouncilDr Mark Goldman, Programme Lead, Clinical LeadershipWorkstream Theresa Nelson*, Programme Director, Clinical LeadershipWorkstream Kim Orlandini*, Programme Manager, Clinical LeadershipWorkstreamSimon Bird, Associate Director, Top Leaders WorkstreamKaren Lynas, Programme Director, Top Leaders WorkstreamDeborah Chafer#, Programme Director, Emerging LeadersWorkstreamPaul Harrison#, Programme Director, Inclusion WorkstreamCaroline Stanger#, Programme Director, GP CommissioningWorkstreamDavid Baron, Programme Director Provision Workstream
Rachel Abraham, Associate Director of Education, ImperialCollege London
Christine Bamford, Director of Leadership Development,National Leadership and Innovation Agency for Healthcare,Wales
Louise Barden, Secretariat, NLC
Maree Barnett, Head of Non-Medical Revalidation, DH
Amit Bose, Policy Manager, Dental and Eye Care, DH
Andrew Butcher, Director, Workforce Strategy, Skills forHealth
Chris Caldwell, Assistant Director of Education andOrganisational Development/Assistant Chief Nurse, GreatOrmond Street Hospital for Children NHS Trust, London
Ingrid Clayden, Director for Health Workforce, Scottish Government
John Cowie, Deputy Director - Health Workforce, Scottish Government
Alison Croad, Policy Officer, Health Professions Council
Marc Davis, Associate Programme Director, CommissioningLeadership, NLC
Carolyn Davison, Emerging Leader (Nurse Consultant), NLC
David Hutton, Nursing Adviser, Nursing and MidwiferyPolicy and Standards, Nursing and Midwifery Council
Peter Gregg, Head of Education and Training Unit,Department of Health and Social Services, Northern Ireland
Patricia Hamilton, Director of Medical Education, DH
Lisa Hughes, Allied Health Professions Manager, DH
Mark Humble, Leadership Development Manager, LondonSHA
Rachel Kirkwood, Accreditation Pilot Lead, NLC/NHS WestMidlands
Penny Lewis, LeAD Manager E-learning for Healthcare,Tony and Penny Lewis Associates
Hazel Mackenzie, Health Workforce, Scottish Government
Rona McCandlish, Midwifery Professional Advisor, DH
Deborah McKenzie, Leadership Lead, London SHA
Claire Marshall, Emerging Leader (Head of PhysiotherapyServices), NLC
Debbie Mellor, Deputy Director, Workforce Education, DH
David Murphy, Senior Leadership and OrganisationDevelopment Manager, National Leadership InnovationAgency for Health Care
Simon Plint, GP Senior Clinical Advisor/Dean of MedicalCommissioning Workforce, Education & Leadership, DHMMC Team/South Central SHA
Jerry Read, Project Lead Oral Health, DH
Patricia Saunders, Programme Manager, NHS MedicalDirectorate, DH
National Leadership Council Clinical Leadership Framework and Accreditation Steering Board*
*indicates someone who also sits on the Steering Board, but is categorised under a different group above.# indicates someone who is also a SHA Leadership Lead, but is categorised under a different group above.

NHS Leadership Framework56
Leadership Framework Development Team, NHS Institute for Innovation and Improvement
Sue Mortlock*, Head of Board Development
Paul W Long*, Project Director, CLCF Project
Professor John Clark*, Director of Medical Leadership
Professor Peter Spurgeon*, Project Director, EEMLProject
Sue Balderson, Project Advisor
Tracy Lonetto*, Project Manager, CLCF Project
Sabhia Sheikh, Associate, Board Development
And colleagues from Right Management
Organisations and groups consulted
Allied Health Professions Federation
Ambulance Service Education Leads
Ambulance Training College
Ambulance Trust CEs Group
Ambulance Trust National HR Directors Group
Association of British Dispensing Opticians
Association of Clinical Scientists (ACS)
Association of Optometrists
Association of Professional Music Therapists
British and Irish Orthoptic Society
British Association of Art Therapists
British Association of Dramatherapists
British Association of Prosthetists and Orthotists
British Dental Association
British Dietetic Association
British Healthcare Trades Association (BHTA) OrthoticsSection
British Psychoanalytic Council
Centre for Pharmacy Postgraduate Education
Chartered Society of Physiotherapy
College of Occupational Therapists
College of Operating Department Practitioners
College of Optometrists
College of Paramedics
Department for Health and Social Services, Wales
Department of Health and Community Care, Scotland
Department of Health, England
Department of Health, Social Services and Public Safety,Northern Ireland
Federation of Healthcare Scientists
Federation of Ophthalmic and Dispensing Opticians
General Dental Council
General Medical Council
General Optical Council
General Pharmaceutical Council
Health Professions Council
Institute of Biomedical Science
Lead Midwife for Education Strategic Reference Group
Local Supervising Authority Midwifery Officers
Midwifery 2020
National Leadership Council Clinical LeadershipFramework and Accreditation Steering Board
National Leadership Council, England
National Skills Academy for Social Care
NHS Institute for Innovation and Improvement
Nursing and Midwifery Council
Royal College of Midwives
Royal College of Nursing
Royal College of Speech and Language Therapists
Royal Pharmaceutical Society of Great Britain
Skills for Health
Social Care Institute for Excellence
The British Psychological Society
The Council of Deans of Health
The Council of University Heads of Pharmacy
The Dental Schools Council
The Institute of Chiropodists & Podiatrists
The Society & College of Radiographers
The Society of Chiropodists & Podiatrists

NHS Leadership Framework 57
Relevant readingThis document is designed to be read and used in conjunction with relevant professional and servicedocuments such as policy, curricula guidance, standards and frameworks related to education andtraining, learning and development activity and performance assessment tools. A selection is included below:
British Association of Arts Therapists, Suggestions from council on curriculum content
British Dietetic Association (2008) Curriculum framework for the pre-registration education and training of dietitians
British and Irish Orthoptic Society (2008) BIOS guidelines for implementing preceptorship
British and Irish Orthoptic Society HNS KSF - outline for Orthoptist Band 5
British Psychological Society (2010) Clinical Psychology Leadership Development Framework July 2010
Charan, R, S Drotter and J Noel (2001) The Leadership Pipeline: How to Build the Leadership Powered Company
Chartered Society of Physiotherapy (2011) CSP Physiotherapy Framework
Chartered Society of Physiotherapy (2011) CSP Learning & Development Principles
College of Occupational Therapists (2006) Post Qualifying Framework: A Resource for Occupational Therapists
College of Occupational Therapists (2009 revised edition) The College of Occupational Therapists’ CurriculumGuidance for Pre-Registration Education
College of Operating Department Practitioners (2009) BSc in Operating Department Practice Curriculum Document
College of Optometrists (2009) Scheme for Registration Trainee Handbook 2009
College of Optometrists (2009) Assessment Framework Optometrists
College of Paramedics (2008) Paramedic Curriculum Guidance and Competence Framework, 2nd edition
Committee of Postgraduate Dental Deans and Directors (2006) A Curriculum for UK Dental Foundation ProgrammeTraining
College of Podiatrists and the Society of Chiropodists and Podiatrists (2008) Regulations and guidance for theaccreditation of pre-registration education programmes in Podiatry leading to eligibility for membership of TheSociety of Chiropodists and Podiatrists Handbook, Edition 2
Department of Health (2010) The NHS Knowledge and Skills Framework (NHS KSF) and the Development ReviewProcess
Department of Health (2008) High Quality Care for All: NHS Next Stage Review Final Report
Department of Health (2010) Equity and Excellence: Liberating the NHS (White Paper)
Department of Health (2009) Transforming Community Services: Enabling New Patterns of Provision
Department of Health (2010) Modernising Scientific Careers: The UK Way Forward
Department of Health (2010) Planning and Developing the NHS Workforce: The National Framework
Department of Health (2010) Building a Safe and Confident Future: Implementing the Recommendations of theSocial Work Task Force
Department of Health (2010) Pharmacy in England: Building On Strengths – Delivering the Future (White Paper)
Department of Health (2008) Modernising Allied Health Professions (AHP) Careers: a Competence-based CareerFramework
NHS Leadership Framework58
Department of Health (2010) Preceptorship Framework for Newly Registered Nurses, Midwives and Allied HealthProfessionals
General Dental Council (2010) Outcomes for Registration
General Medical Council (2009) Tomorrow’s Doctors: Outcomes and Standards for Undergraduate MedicalEducation
Gitsham, M. (2009) Developing the Global Leaders of Tomorrow. Ashridge Business School and the EuropeanAcademy of Business in Society
Gronn, P. (2008) The Future of Distributed Leadership, Journal of Educational Administration, 46(2), 141-58
Hartley, J. and Bennington, J. (2010) Leadership for Healthcare. Policy Press: Bristol
Health Professions Council (2009) Standards of Education and Training
Health Professions Council (Various) Standards of Proficiency
Health Professions Council (2008) Standards of Conduct, Performance and Ethics
Health Professions Council (2005) Standards for Continuing Professional Development July 2005
Heifetz, R. and Laurie, D. (2009) Review: The Work of Leadership by Heifetz and Laurie. The Welsh NHSConfederation
Midwifery 2010 Midwifery 2020 – Delivering Expectations
MMC Inquiry (2008) Aspiring to Excellence: Final Report of the Independent Enquiry into Modernising MedicalCareers
Mott MacDonald (2010) Literature Review: Leadership Frameworks. Mott MacDonald: Bolton
National Skills Academy Social Care (2009) Leadership and Management Prospectus
National Skills Academy Social Care (2010) Overview and Key Messages May 2010
NHS Institute for Innovation and Improvement (2006) NHS Leadership Qualities Framework
NHS Institute for Innovation and Improvement and Academy of Medical Royal Colleges (2010) Medical LeadershipCompetency Framework, 3rd edition
NHS Institute for Innovation and Improvement and Academy of Medical Royal Colleges (2010) Shared Leadership:Underpinning of the MLCF
NHS Scotland (2009) Delivering Quality Through Leadership: NHS Scotland Leadership Development Strategy
Nursing and Midwifery Council (2010) Standards for Pre-registration Nursing Education: draft for consultation
Royal College of Speech and Language Therapists (2007) Speech and Language Therapy Competency Frameworkto Guide Transition to Full RCSLT Membership
Royal College of Speech and Language Therapists CPD Framework - Human and Financial Leadership andResource Management
Skills for Care and Development (2009) Health and Social Care – National Occupational Standards
Skills for Health, Shape a Quality Nursing Workforce
Society and College of Radiographers (2007) Learning and Development Framework for Clinical Imaging andOncology
Society and College of Radiographers (2010) Education and Professional Development Strategy: New Directions
Society and College of Radiographers (2005) A Framework for Professional Leadership in Clinical Imaging andRadiotherapy and Oncology Services

NHS Leadership Framework 59
Spurgeon, P., Clark. J., and Ham, C. (2011) Medical Leadership: From the Dark Side to Centre Stage, OxfordRadcliffe Press: Oxford
Stanton, E., Lemer, C. and Mountford, J. (eds) (2010) Clinical Leadership: Bridging the divide. Quay Books: London
Tamkin, P., Pearson, G., Hirsh, W. and Constable, S. (2010) Exceeding Expectation: the Principles of OutstandingLeadership. The Work Foundation
Wilson, A., Lenssen, G., and Hind, P. (2007) Leadership Qualities and Management Competencies for CorporateResponsibility. Ashridge Business School and the European Academy of Business in Society
NHS Leadership Framework60
Appendix IThe NHS Knowledge and Skills Framework
The NHS Knowledge and Skills Framework (KSF) was re-launched in 2010 in a simplified form, designed to be aflexible tool and adaptable for local use. The new KSF focuses on the core dimensions and links to the NHSLeadership Framework particularly in the areas of communication, personal and people development, serviceimprovement, quality and equality and diversity. The KSF also includes a new optional dimension on managementand leadership (http://www.nhsemployers.org/PayAndContracts/AgendaForChange/KSF/Simplified-KSF/Pages/SimplifiedKSF.aspx) which sets out concisely the knowledge and skills required for leadership across fourlevels of the KSF and so relates well in summary form to the NHS Leadership Framework. It also includes indicatorsto help organisations identify whether the knowledge and skills of the dimension are present in the organisation.
To view a visual representation of what the KSF and the NHS Leadership Framework have in common, pleasevisit: www.nhsleadership.org.uk/framework.asp

NHS Leadership Framework 61
App
endi
x II:
The
follo
win
g ta
bles
com
bine
the
indi
catio
n of
beh
avio
urs
at d
iffer
ent
lead
ersh
ip s
tage
s fr
om e
ach
dom
ain
sect
ion.
Ple
ase
refe
r to
the
ful
l dom
ain
page
s fo
r th
e el
emen
t de
scrip
tors
. 1. D
EMO
NST
RA
TIN
G P
ERSO
NA
L Q
UA
LITI
ESEf
fect
ive
lead
ersh
ip r
equi
res
indi
vidu
als
to d
raw
upo
n th
eir
valu
es, s
tren
gths
and
abi
litie
s to
del
iver
hig
h st
anda
rds
of s
ervi
ce. T
o do
so,
the
y m
ust
dem
onst
rate
eff
ectiv
enes
s in
dem
onst
ratin
g se
lf aw
aren
ess,
man
agin
g th
emse
lves
, con
tinui
ng t
heir
pers
onal
dev
elop
men
t an
d ac
ting
with
inte
grity
.
Elem
ent
1O
wn
Prac
tice/
Imm
edia
te T
eam
2W
hole
Ser
vice
/Acr
oss
Team
s3
Acr
oss
Serv
ices
/Wid
er O
rgan
isatio
n4
Who
le O
rgan
isatio
n/W
ider
H
ealth
care
Sys
tem
1.1
Dev
elo
pin
g S
elf
Aw
aren
ess
Refle
cts
on h
ow fa
ctor
s su
ch a
s ow
nva
lues
, pre
judi
ces
and
emot
ions
influ
ence
thei
r jud
gem
ent,
beha
viou
r and
sel
f bel
ief.
Use
s fe
edba
ck fr
om a
ppra
isals
and
othe
rso
urce
s to
con
sider
per
sona
l im
pact
and
chan
ge b
ehav
iour
. U
nder
stan
ds p
erso
nal
sour
ces
of s
tres
s.
App
reci
ates
the
impa
ct t
hey
have
on
othe
rs a
nd t
he im
pact
oth
ers
have
on
them
. Rou
tinel
y se
eks
feed
back
and
adap
ts t
heir
beha
viou
r ap
prop
riate
ly.
Refle
cts
on t
heir
inte
ract
ions
with
a w
ide
and
dive
rse
rang
e of
indi
vidu
als
and
grou
ps f
rom
with
in a
nd b
eyon
d th
eir
imm
edia
te s
ervi
ce/o
rgan
isat
ion.
Cha
lleng
es a
nd r
efre
shes
ow
n va
lues
,be
liefs
, lea
ders
hip
styl
es a
nd a
ppro
ache
s.O
vert
ly r
ole
mod
els
the
givi
ng a
ndre
ceiv
ing
of f
eedb
ack.
Use
s so
phist
icat
ed to
ols
and
sour
ces
toco
ntin
uous
ly le
arn
abou
t the
ir le
ader
ship
impa
ct in
the
wid
er h
ealth
and
car
eco
mm
unity
and
impr
ove
thei
ref
fect
iven
ess
as a
sen
ior l
eade
r.U
nder
stan
ds h
ow p
ress
ures
ass
ocia
ted
with
car
ryin
g ou
t a h
igh
prof
ile ro
le im
pact
on th
em a
nd th
eir p
erfo
rman
ce.
1.2
Man
agin
g Y
ou
rsel
fPl
ans
and
man
ages
ow
n tim
e ef
fect
ivel
yan
d fu
lfils
wor
k re
quire
men
ts a
ndco
mm
itmen
ts to
a h
igh
stan
dard
, with
out
com
prom
ising
ow
n he
alth
and
wel
lbei
ng.
Rem
ains
cal
m a
nd fo
cuse
d un
der p
ress
ure.
Ensu
res
that
ow
n w
ork
plan
s an
dpr
iorit
ies
fit w
ith t
he n
eeds
of
othe
rsin
volv
ed in
del
iver
ing
serv
ices
.D
emon
stra
tes
flexi
bilit
y an
d se
nsiti
vity
to
serv
ice
requ
irem
ents
and
rem
ains
asse
rtiv
e in
pur
suin
g se
rvic
e go
als.
Succ
essf
ully
man
ages
a r
ange
of
pers
onal
and
org
anis
atio
nal d
eman
dsan
d pr
essu
res.
Dem
onst
rate
s te
naci
tyan
d re
silie
nce.
Ove
rcom
es s
etba
cks
whe
re g
oals
can
not
be a
chie
ved
and
quic
kly
refo
cuse
s. I
s vi
sibl
e an
dac
cess
ible
to
othe
rs.
Rem
ains
focu
sed
on s
trat
egic
goa
ls w
hen
face
d w
ith c
ompe
ting
and,
at t
imes
,co
nflic
ting
dem
ands
aris
ing
from
diff
erin
gpr
iorit
ies.
Iden
tifie
s w
here
they
nee
d to
pers
onal
ly g
et in
volv
ed to
ach
ieve
the
mos
t ben
efit
for t
he o
rgan
isatio
n an
dw
ider
hea
lthca
re s
yste
m.
1.3
Co
nti
nu
ing
Per
son
alD
evel
op
men
tTa
kes
resp
onsib
ility
for o
wn
pers
onal
deve
lopm
ent a
nd s
eeks
opp
ortu
nitie
s fo
rle
arni
ng.
Striv
es to
put
lear
ning
into
prac
tice.
Puts
sel
f fo
rwar
d fo
r ch
alle
ngin
gas
sign
men
ts a
nd p
roje
cts
whi
ch w
illde
velo
p st
reng
ths
and
addr
ess
deve
lopm
ent
area
s.
Act
s as
an
exem
plar
for
oth
ers
inm
anag
ing
thei
r co
ntin
uous
per
sona
lde
velo
pmen
t. F
acili
tate
s th
ede
velo
pmen
t of
a le
arni
ng c
ultu
re.
Dev
elop
s th
roug
h sy
stem
atic
ally
sca
nnin
gth
e ex
tern
al e
nviro
nmen
t and
exp
lorin
gle
adin
g ed
ge th
inki
ng a
nd b
est p
ract
ice.
App
lies
lear
ning
to b
uild
and
refr
esh
the
serv
ice.
Tre
ats
chal
leng
e as
a p
ositi
ve fo
rce
for i
mpr
ovem
ent.
1.4
Act
ing
wit
h In
teg
rity
Beha
ves
in a
n op
en, h
ones
t and
incl
usiv
em
anne
r, up
hold
ing
pers
onal
and
orga
nisa
tiona
l eth
ics
and
valu
es.
Show
s re
spec
t for
the
need
s of
oth
ers
and
prom
otes
equ
ality
and
div
ersit
y.
Act
s as
a r
ole
mod
el f
or o
ther
s in
dem
onst
ratin
g in
tegr
ity a
ndin
clus
iven
ess
in a
ll as
pect
s of
the
ir w
ork.
Cha
lleng
es w
here
org
anis
atio
nal v
alue
sar
e co
mpr
omis
ed.
Cre
ates
an
open
, hon
est
and
incl
usiv
ecu
lture
in a
ccor
danc
e w
ith c
lear
prin
cipl
es a
nd v
alue
s. E
nsur
es e
quity
of
acce
ss t
o se
rvic
es a
nd c
reat
es a
nen
viro
nmen
t w
here
peo
ple
from
all
back
grou
nds
can
exce
l.
Ass
ures
sta
ndar
ds o
f int
egrit
y ar
em
aint
aine
d ac
ross
the
serv
ice
and
com
mun
icat
es th
e im
port
ance
of a
lway
sad
optin
g an
eth
ical
and
incl
usiv
e ap
proa
ch.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• D
oes
not
unde
rsta
nd o
wn
emot
ions
or
reco
gnis
e th
e im
pact
of
own
beha
viou
r on
oth
ers
• A
ppro
ache
s ta
sks
in a
dis
orga
nise
d w
ay a
nd p
lans
are
not
rea
listic
• U
nabl
e to
dis
cuss
ow
n st
reng
ths
and
deve
lopm
ent
need
s an
d sp
ends
litt
le t
ime
on d
evel
opm
ent
• D
emon
stra
tes
beha
viou
rs t
hat
are
coun
ter
to c
ore
valu
es o
f op
enne
ss, i
nclu
sive
ness
, ho
nest
y an
deq
ualit
y•
Lac
ks c
onfid
ence
in o
wn
abili
ties
to d
eliv
er r
esul
ts

NHS Leadership Framework62
2. W
OR
KIN
G W
ITH
OTH
ERS
Effe
ctiv
e le
ader
ship
req
uire
s in
divi
dual
s to
wor
k w
ith o
ther
s in
tea
ms
and
netw
orks
to
deliv
er a
nd im
prov
e se
rvic
es. T
his
requ
ires
the
m t
o de
mon
stra
te e
ffec
tiven
ess
inde
velo
ping
net
wor
ks, b
uild
ing
and
mai
ntai
ning
rel
atio
nshi
ps, e
ncou
ragi
ng c
ontr
ibut
ion,
and
wor
king
with
in t
eam
s.
Elem
ent
1O
wn
Prac
tice/
Imm
edia
te T
eam
2W
hole
Ser
vice
/Acr
oss
Team
s3
Acr
oss
Serv
ices
/Wid
er O
rgan
isatio
n4
Who
le O
rgan
isatio
n/W
ider
H
ealth
care
Sys
tem
2.1
Dev
elo
pin
g N
etw
ork
sId
entif
ies
whe
re w
orki
ng a
nd c
oope
ratin
gw
ith o
ther
s ca
n re
sult
in b
ette
r ser
vice
s.En
deav
ours
to w
ork
colla
bora
tivel
y.
Use
s ne
twor
ks t
o br
ing
indi
vidu
als
and
grou
ps t
oget
her
to s
hare
info
rmat
ion
and
reso
urce
s an
d to
ach
ieve
goa
ls.
Iden
tifie
s an
d bu
ilds
effe
ctiv
e ne
twor
ksw
ith a
ran
ge o
f in
fluen
tial s
take
hold
ers
inte
rnal
and
ext
erna
l to
the
orga
nisa
tion.
Wor
ks a
cros
s bo
unda
ries
crea
ting
netw
orks
whi
ch fa
cilit
ate
high
leve
ls of
colla
bora
tion
with
in a
nd a
cros
sor
gani
satio
ns a
nd s
ecto
rs.
2.2
Bu
ildin
g a
nd
Mai
nta
inin
gR
elat
ion
ship
sC
omm
unic
ates
with
and
list
ens
to o
ther
s,re
cogn
ising
diff
eren
t per
spec
tives
.Em
path
ises
and
take
s in
to a
ccou
nt th
ene
eds
and
feel
ings
of o
ther
s. G
ains
and
mai
ntai
ns tr
ust a
nd s
uppo
rt.
Build
s an
d m
aint
ains
rel
atio
nshi
ps w
ith a
rang
e of
indi
vidu
als
invo
lved
inde
liver
ing
the
serv
ice.
Man
ages
sens
itivi
ties
betw
een
indi
vidu
als
and
grou
ps.
Build
s an
d nu
rtur
es t
rust
ing
rela
tions
hips
at a
ll le
vels
with
in a
nd a
cros
s se
rvic
esan
d or
gani
satio
nal b
ound
arie
s.
Build
s an
d m
aint
ains
sus
tain
able
str
ateg
ical
lianc
es a
cros
s th
e sy
stem
and
oth
erse
ctor
s. H
as h
igh
impa
ct w
hen
inte
ract
ing
with
oth
ers
at a
ll le
vels.
2.3
Enco
ura
gin
gC
on
trib
uti
on
Seek
s an
d ac
know
ledg
es th
e vi
ews
and
inpu
t of o
ther
s. S
how
s re
spec
t for
the
cont
ribut
ions
and
cha
lleng
es o
f oth
ers.
Cre
ates
a s
uppo
rtiv
e en
viro
nmen
t w
hich
enco
urag
es o
ther
s to
exp
ress
div
erse
opin
ions
and
eng
age
in d
ecis
ion-
mak
ing.
Con
stru
ctiv
ely
chal
leng
essu
gges
tions
and
rec
onci
les
conf
lictin
gvi
ews.
Inte
grat
es t
he c
ontr
ibut
ions
of
a di
vers
era
nge
of s
take
hold
ers,
bei
ng o
pen
and
hone
st a
bout
the
ext
ent
to w
hich
cont
ribut
ions
can
be
acte
d up
on.
Cre
ates
sys
tem
s w
hich
enc
oura
geco
ntrib
utio
n th
roug
hout
the
orga
nisa
tion.
Invi
tes
cont
ribut
ion
from
diff
eren
t sec
tors
to b
ring
abou
t im
prov
emen
ts.
2.4
Wo
rkin
g w
ith
in T
eam
sU
nder
stan
ds ro
les,
resp
onsib
ilitie
s an
dpu
rpos
e w
ithin
the
team
. A
dopt
s a
colla
bora
tive
appr
oach
and
resp
ects
team
deci
sions
.
Hel
ps le
ad o
ther
s to
war
ds c
omm
ongo
als,
pro
vidi
ng c
lear
obj
ectiv
es a
ndof
ferin
g ap
prop
riate
sup
port
. Sh
ows
awar
enes
s of
tea
m d
ynam
ics
and
acts
to
prom
ote
effe
ctiv
e te
am w
orki
ng.
App
reci
ates
the
eff
orts
of
othe
rs.
Take
s on
rec
ogni
sed
posi
tiona
l lea
ders
hip
role
s w
ithin
the
org
anis
atio
n. B
uild
shi
gh p
erfo
rmin
g in
clus
ive
team
s th
atco
ntrib
ute
to p
rodu
ctiv
e an
d ef
ficie
nthe
alth
and
car
e se
rvic
es.
Prom
otes
auto
nom
y an
d em
pow
erm
ent
and
mai
ntai
ns a
sen
se o
f op
timis
m a
ndco
nfid
ence
.
Con
trib
utes
to a
nd le
ads
seni
or te
ams.
Enab
les
othe
rs to
take
on
lead
ersh
ipre
spon
sibili
ties,
bui
ldin
g hi
gh le
vel
lead
ersh
ip c
apab
ility
and
cap
acity
from
adi
vers
e ra
nge
of b
ackg
roun
ds.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• F
ails
to
netw
ork
with
oth
ers
and/
or a
llow
s re
latio
nshi
ps t
o de
terio
rate
• Fa
ils t
o w
in t
he s
uppo
rt a
nd r
espe
ct o
f ot
hers
• D
oes
not
enco
urag
e ot
hers
to
cont
ribut
e id
eas
• D
oes
not
adop
t a
colla
bora
tive
appr
oach

NHS Leadership Framework 63
3. M
AN
AG
ING
SER
VIC
ESEf
fect
ive
lead
ersh
ip r
equi
res
indi
vidu
als
to f
ocus
on
the
succ
ess
of t
he o
rgan
isat
ion(
s) in
whi
ch t
hey
wor
k. T
his
requ
ires
them
to
be e
ffec
tive
in p
lann
ing,
man
agin
g re
sour
ces,
man
agin
g pe
ople
and
man
agin
g pe
rfor
man
ce.
Elem
ent
1O
wn
Prac
tice/
Imm
edia
te T
eam
2W
hole
Ser
vice
/Acr
oss
Team
s3
Acr
oss
Serv
ices
/Wid
er O
rgan
isatio
n4
Who
le O
rgan
isatio
n/W
ider
H
ealth
care
Sys
tem
3.1
Plan
nin
gC
ontr
ibut
es id
eas
to s
ervi
ce p
lans
,in
corp
orat
ing
feed
back
from
oth
ers
-in
clud
ing
a di
vers
e ra
nge
of p
atie
nts,
serv
ice
user
s an
d co
lleag
ues.
Wor
ks c
olla
bora
tivel
y to
dev
elop
busi
ness
cas
es a
nd s
ervi
ce p
lans
tha
tsu
ppor
t or
gani
satio
nal o
bjec
tives
,ap
prai
sing
the
m in
ter
ms
of b
enef
its a
ndris
ks.
Lead
s se
rvic
e de
sign
and
pla
nnin
gpr
oces
ses.
Com
mun
icat
es a
nd k
eeps
othe
rs in
form
ed o
f st
rate
gic
and
oper
atio
nal p
lans
, pro
gres
s an
dou
tcom
es.
Ant
icip
ates
the
impa
ct o
f hea
lth tr
ends
and
deve
lops
str
ateg
ic p
lans
that
will
hav
ea
signi
fican
t im
pact
on
the
orga
nisa
tion
and
wid
er h
ealth
care
sys
tem
. En
sure
sst
rate
gic
obje
ctiv
es a
re tr
ansla
ted
into
oper
atio
nal p
lans
.
3.2
Man
agin
g R
eso
urc
esU
nder
stan
ds w
hat r
esou
rces
are
ava
ilabl
ean
d or
gani
ses
the
appr
opria
te ty
pe a
ndle
vel o
f res
ourc
es re
quire
d to
del
iver
saf
ean
d ef
ficie
nt s
ervi
ces.
Iden
tifie
s re
sour
ce r
equi
rem
ents
asso
ciat
ed w
ith d
eliv
erin
g se
rvic
es.
Man
ages
res
ourc
es a
nd t
akes
act
ion
toen
sure
the
ir ef
fect
ive
and
effic
ient
use
.
Fore
cast
s re
sour
ce r
equi
rem
ents
asso
ciat
ed w
ith d
eliv
erin
g co
mpl
exse
rvic
es e
ffic
ient
ly a
nd e
ffec
tivel
y.M
anag
es r
esou
rces
tak
ing
into
acc
ount
the
impa
ct o
f na
tiona
l and
loca
l pol
icie
san
d co
nstr
aint
s.
Stra
tegi
cally
man
ages
reso
urce
s ac
ross
the
orga
nisa
tion
and
wid
er h
ealth
care
sys
tem
.
3.3
Man
agin
g P
eop
leSu
ppor
ts o
ther
s in
del
iver
ing
high
qua
lity
serv
ices
and
exc
elle
nce
in h
ealth
and
car
e.Pr
ovid
es o
ther
s w
ith c
lear
pur
pose
and
dire
ctio
n. H
elps
oth
ers
in d
evel
opin
gth
eir
role
s an
d re
spon
sibi
litie
s.
Mot
ivat
es a
nd c
oach
es in
divi
dual
s an
dte
ams
to s
tren
gthe
n th
eir
perf
orm
ance
and
assi
st t
hem
with
dev
elop
ing
thei
row
n ca
pabi
litie
s an
d sk
ills.
Alig
nsin
divi
dual
dev
elop
men
t ne
eds
with
serv
ice
goal
s.
Insp
ires
and
supp
orts
lead
ers
to m
obili
sedi
vers
e te
ams
that
are
com
mitt
ed to
and
alig
ned
with
org
anisa
tiona
l val
ues
and
goal
s. E
ngag
es w
ith a
nd in
fluen
ces
seni
orle
ader
s an
d ke
y st
akeh
olde
rs to
del
iver
join
ed u
p se
rvic
es.
3.4
Man
agin
gPe
rfo
rman
ceU
ses
info
rmat
ion
and
data
abo
utpe
rfor
man
ce to
iden
tify
impr
ovem
ents
whi
ch w
ill s
tren
gthe
n se
rvic
es.
Wor
ks w
ith o
ther
s to
set
and
mon
itor
perf
orm
ance
sta
ndar
ds, a
ddre
ssin
g ar
eas
whe
re p
erfo
rman
ce o
bjec
tives
are
not
achi
eved
.
Esta
blis
hes
rigor
ous
perf
orm
ance
mea
sure
s. H
olds
sel
f, in
divi
dual
s an
dte
ams
to a
ccou
nt f
or a
chie
ving
perf
orm
ance
sta
ndar
ds. C
halle
nges
whe
n se
rvic
e ex
pect
atio
ns a
re n
ot b
eing
met
and
tak
es c
orre
ctiv
e ac
tion.
Prom
otes
an
incl
usiv
e cu
lture
that
ena
bles
peop
le to
per
form
to th
eir b
est,
ensu
ring
that
app
ropr
iate
per
form
ance
man
agem
ent s
yste
ms
are
in p
lace
and
that
perf
orm
ance
dat
a is
syst
emat
ical
lyev
alua
ted
and
fed
into
futu
re p
lans
.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• D
isor
gani
sed
or u
nstr
uctu
red
appr
oach
to
plan
ning
• W
aste
s re
sour
ces
or f
ails
to
mon
itor
them
eff
ectiv
ely
• D
oes
not
effe
ctiv
ely
man
age
and
deve
lop
peop
le•
Fai
ls t
o id
entif
y an
d ad
dres
s pe
rfor
man
ce is
sues

NHS Leadership Framework64
4. IM
PRO
VIN
G S
ERV
ICES
Effe
ctiv
e le
ader
ship
req
uire
s in
divi
dual
s to
mak
e a
real
diff
eren
ce t
o pe
ople
’s he
alth
by
deliv
erin
g hi
gh q
ualit
y se
rvic
es a
nd b
y de
velo
ping
impr
ovem
ents
to
serv
ices
. Thi
s re
quire
sth
em t
o de
mon
stra
te e
ffec
tiven
ess
in e
nsur
ing
patie
nt s
afet
y, c
ritic
ally
eva
luat
ing,
enc
oura
ging
impr
ovem
ent
and
inno
vatio
n an
d f
acili
tatin
g tr
ansf
orm
atio
n.
Elem
ent
1O
wn
Prac
tice/
Imm
edia
te T
eam
2W
hole
Ser
vice
/Acr
oss
Team
s3
Acr
oss
Serv
ices
/Wid
er O
rgan
isatio
n4
Who
le O
rgan
isatio
n/W
ider
H
ealth
care
Sys
tem
4.1
Ensu
rin
g P
atie
nt
Safe
tyPu
ts th
e sa
fety
of p
atie
nts
and
serv
ice
user
s at
the
hear
t of t
heir
thin
king
inde
liver
ing
and
impr
ovin
g se
rvic
es.
Take
sac
tion
to re
port
or r
ectif
y sh
ortf
alls
inpa
tient
saf
ety.
Revi
ews
prac
tice
to im
prov
e st
anda
rds
ofpa
tient
saf
ety
and
min
imis
e ris
k.M
onito
rs t
he im
pact
of
serv
ice
chan
geon
pat
ient
saf
ety.
Dev
elop
s an
d m
aint
ains
aud
it an
d ris
km
anag
emen
t sy
stem
s w
hich
will
driv
ese
rvic
e im
prov
emen
t an
d pa
tient
saf
ety.
Cre
ates
a c
ultu
re th
at p
riorit
ises
the
heal
th, s
afet
y an
d se
curit
y of
pat
ient
s an
dse
rvic
e us
ers.
Del
iver
s as
sura
nce
that
patie
nt s
afet
y un
derp
ins
polic
ies,
pro
cess
esan
d sy
stem
s.
4.2
Cri
tica
lly E
valu
atin
gU
ses
feed
back
from
pat
ient
s, c
arer
s an
dse
rvic
e us
ers
to c
ontr
ibut
e to
hea
lthca
reim
prov
emen
ts.
Enga
ges
with
oth
ers
to c
ritic
ally
eva
luat
ese
rvic
es a
nd c
reat
e id
eas
for
impr
ovem
ents
.
Synt
hesi
ses
com
plex
info
rmat
ion
toid
entif
y po
tent
ial i
mpr
ovem
ents
to
serv
ices
. Id
entif
ies
pote
ntia
l bar
riers
to
serv
ice
impr
ovem
ent.
Benc
hmar
ks th
e w
ider
org
anisa
tion
agai
nst e
xam
ples
of b
est p
ract
ice
inhe
alth
care
and
oth
er s
ecto
rs.
Eval
uate
sop
tions
for i
mpr
ovin
g se
rvic
es in
line
with
futu
re a
dvan
ces.
4.3
Enco
ura
gin
gIm
pro
vem
ent
and
Inn
ova
tio
n
Que
stio
ns e
stab
lishe
d pr
actic
es w
hich
do
not a
dd v
alue
. Put
s fo
rwar
d cr
eativ
esu
gges
tions
to im
prov
e th
e qu
ality
of
serv
ice
prov
ided
.
Act
s as
a p
ositi
ve r
ole
mod
el f
orin
nova
tion.
Enc
oura
ges
dial
ogue
and
deba
te in
the
dev
elop
men
t of
new
idea
sw
ith a
wid
e ra
nge
of p
eopl
e.
Cha
lleng
es c
olle
ague
s’ t
hink
ing
to f
ind
bett
er a
nd m
ore
effe
ctiv
e w
ays
ofde
liver
ing
serv
ices
and
qua
lity.
Acc
esse
scr
eativ
ity a
nd in
nova
tion
from
rel
evan
tin
divi
dual
s an
d gr
oups
.
Driv
es a
cul
ture
of i
nnov
atio
n an
dim
prov
emen
t. In
tegr
ates
radi
cal a
ndin
nova
tive
appr
oach
es in
to s
trat
egic
pla
nsto
mak
e th
e N
HS
wor
ld c
lass
in th
epr
ovisi
on o
f hea
lthca
re s
ervi
ces.
4.4
Faci
litat
ing
Tran
sfo
rmat
ion
Art
icul
ates
the
need
for c
hang
es to
proc
esse
s an
d sy
stem
s, a
ckno
wle
dgin
g th
eim
pact
on
peop
le a
nd s
ervi
ces.
Focu
ses
self
and
othe
rs o
n ac
hiev
ing
chan
ges
to s
yste
ms
and
proc
esse
s w
hich
will
lead
to
impr
oved
ser
vice
s.
Ener
gise
s ot
hers
to
driv
e ch
ange
tha
t w
illim
prov
e he
alth
and
car
e se
rvic
es.
Act
ivel
y m
anag
es t
he c
hang
e pr
oces
s,dr
awin
g on
mod
els
of e
ffec
tive
chan
gem
anag
emen
t. R
ecog
nise
s an
d ad
dres
ses
the
impa
ct o
f ch
ange
on
peop
le a
ndse
rvic
es.
Insp
ires
othe
rs to
take
bol
d ac
tion
and
mak
e im
port
ant a
dvan
ces
in h
ow s
ervi
ces
are
deliv
ered
. Re
mov
es o
rgan
isatio
nal
obst
acle
s to
cha
nge
and
crea
tes
new
stru
ctur
es a
nd p
roce
sses
to fa
cilit
ate
tran
sfor
mat
ion.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• O
verlo
oks
the
need
to
put
patie
nts
at t
he f
oref
ront
of
thei
r th
inki
ng•
Doe
s no
t qu
estio
n/ev
alua
te c
urre
nt p
roce
sses
and
pra
ctic
es•
Mai
ntai
ns t
he s
tatu
s qu
o an
d st
icks
with
tra
ditio
nal o
utda
ted
way
s of
doi
ng t
hing
s•
Fai
ls t
o im
plem
ent
chan
ge o
r im
plem
ents
cha
nge
for
chan
ge’s
sake

NHS Leadership Framework 65
5. S
ETTI
NG
DIR
ECTI
ON
Effe
ctiv
e le
ader
ship
req
uire
s in
divi
dual
s to
con
trib
ute
to t
he s
trat
egy
and
aspi
ratio
ns o
f th
e or
gani
satio
n an
d ac
t in
a m
anne
r co
nsis
tent
with
its
valu
es. T
his
requ
ires
them
to
dem
onst
rate
eff
ectiv
enes
s in
iden
tifyi
ng t
he c
onte
xts
for
chan
ge, a
pply
ing
know
ledg
e an
d ev
iden
ce, m
akin
g de
cisi
ons,
and
eva
luat
ing
impa
ct.
Elem
ent
1O
wn
Prac
tice/
Imm
edia
te T
eam
2W
hole
Ser
vice
/Acr
oss
Team
s3
Acr
oss
Serv
ices
/Wid
er O
rgan
isatio
n4
Who
le O
rgan
isatio
n/W
ider
H
ealth
care
Sys
tem
5.1
Iden
tify
ing
th
eC
on
text
s fo
r C
han
ge
Und
erst
ands
the
rang
e of
fact
ors
whi
chde
term
ine
why
cha
nges
are
mad
e.Id
entif
ies
the
exte
rnal
and
inte
rnal
driv
ers
of c
hang
e an
d co
mm
unic
ates
the
ratio
nale
for
cha
nge
to o
ther
s.
Act
ivel
y se
eks
to le
arn
abou
t ex
tern
alfa
ctor
s w
hich
will
impa
ct o
n se
rvic
es.
Inte
rpre
ts t
he m
eani
ng o
f th
ese
for
serv
ices
and
inco
rpor
ates
the
m in
tose
rvic
e pl
ans
and
actio
ns.
Synt
hesis
es k
now
ledg
e fr
om a
bro
adra
nge
of s
ourc
es.
Iden
tifie
s fu
ture
chal
leng
es a
nd im
pera
tives
that
will
cre
ate
the
need
for c
hang
e an
d m
ove
the
orga
nisa
tion
and
the
wid
er h
ealth
care
syst
em in
new
dire
ctio
ns. I
nflu
ence
s th
eco
ntex
t for
cha
nge
in th
e be
st in
tere
sts
ofse
rvic
es a
nd s
ervi
ce u
sers
.
5.2
Ap
ply
ing
Kn
ow
led
ge
and
Evid
ence
Gat
hers
dat
a an
d in
form
atio
n ab
out
aspe
cts
of th
e se
rvic
e, a
naly
ses
evid
ence
and
uses
this
know
ledg
e to
sug
gest
chan
ges
that
will
impr
ove
serv
ices
in th
efu
ture
.
Obt
ains
and
ana
lyse
s in
form
atio
n ab
out
serv
ices
and
pat
hway
s to
info
rm f
utur
edi
rect
ion.
Sup
port
s an
d en
cour
ages
othe
rs t
o us
e kn
owle
dge
and
evid
ence
to in
form
dec
isio
ns a
bout
the
fut
ure
ofse
rvic
es.
Und
erst
ands
the
com
plex
inte
rdep
ende
ncie
s ac
ross
a r
ange
of
serv
ices
. A
pplie
s kn
owle
dge
to s
etfu
ture
dire
ctio
n.
Use
s kn
owle
dge,
evi
denc
e an
dex
perie
nce
of n
atio
nal a
nd in
tern
atio
nal
deve
lopm
ents
in h
ealth
and
soc
ial c
are
toin
fluen
ce th
e fu
ture
dev
elop
men
t of
heal
th a
nd c
are
serv
ices
.
5.3
Mak
ing
Dec
isio
ns
Con
sults
with
oth
ers
and
cont
ribut
es to
deci
sions
abo
ut th
e fu
ture
dire
ctio
n/vi
sion
of th
eir s
ervi
ce.
Invo
lves
key
peo
ple
and
grou
ps in
mak
ing
deci
sion
s. A
ctiv
ely
enga
ges
info
rmal
and
info
rmal
dec
isio
n-m
akin
gpr
oces
ses
abou
t th
e fu
ture
of
serv
ices
.
Rem
ains
acc
ount
able
for
mak
ing
timel
yde
cisi
ons
in c
ompl
ex s
ituat
ions
. M
odifi
esde
cisi
ons
and
flexe
s di
rect
ion
whe
nfa
ced
with
new
info
rmat
ion
or c
hang
ing
circ
umst
ance
s.
Ensu
res
that
cor
pora
te d
ecisi
on-m
akin
g is
rigor
ous
and
take
s ac
coun
t of t
he fu
llra
nge
of fa
ctor
s im
ping
ing
on th
e fu
ture
dire
ctio
n of
the
orga
nisa
tion
and
the
wid
er h
ealth
care
sys
tem
. Can
ope
rate
with
out a
ll th
e fa
cts.
Tak
es u
npop
ular
deci
sions
whe
n in
the
best
inte
rest
s of
heal
th a
nd c
are
in th
e lo
ng te
rm.
5.4
Eval
uat
ing
Imp
act
Ass
esse
s th
e ef
fect
s of
cha
nge
on s
ervi
cede
liver
y an
d pa
tient
out
com
es.
Mak
esre
com
men
datio
ns fo
r fut
ure
impr
ovem
ents
.
Eval
uate
s an
d em
beds
app
roac
hes
and
wor
king
met
hods
whi
ch h
ave
prov
ed t
obe
eff
ectiv
e in
to t
he w
orki
ng p
ract
ices
of t
eam
s an
d in
divi
dual
s.
Iden
tifie
s ga
ins
whi
ch c
an b
e ap
plie
del
sew
here
in t
he o
rgan
isat
ion
and
inco
rpor
ates
the
se in
to o
pera
tiona
l/bu
sine
ss p
lans
. Dis
sem
inat
es le
arni
ngfr
om c
hang
es w
hich
hav
e be
enin
trod
uced
.
Synt
hesis
es le
arni
ng a
risin
g fr
om c
hang
esw
hich
hav
e be
en in
trod
uced
and
inco
rpor
ates
thes
e in
to s
trat
egic
pla
ns.
Shar
es le
arni
ng w
ith th
e w
ider
hea
lth a
ndca
re c
omm
unity
.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• U
naw
are
of p
oliti
cal,
soci
al, t
echn
ical
, eco
nom
ic, o
rgan
isat
iona
l fac
tors
tha
t im
pact
on
the
futu
re o
fth
e se
rvic
e/or
gani
satio
n•
Doe
s no
t us
e an
evi
denc
e-ba
se f
or d
ecis
ion-
mak
ing
• M
akes
poo
r de
cisi
ons
abou
t th
e fu
ture
• F
ails
to
eval
uate
the
impa
ct o
f pr
evio
us d
ecis
ions
and
act
ions

NHS Leadership Framework66
6. C
REA
TIN
G T
HE
VIS
ION
Thos
e in
sen
ior
posi
tiona
l lea
ders
hip
role
s cr
eate
a c
ompe
lling
vis
ion
for
the
futu
re, a
nd c
omm
unic
ate
this
with
in a
nd a
cros
s or
gani
satio
ns. T
his
requ
ires
them
to
dem
onst
rate
effe
ctiv
enes
s in
dev
elop
ing
the
visi
on f
or t
he o
rgan
isat
ion,
influ
enci
ng t
he v
isio
n of
the
wid
er h
ealth
care
sys
tem
, com
mun
icat
ing
the
visi
on a
nd e
mbo
dyin
g th
e vi
sion
.
Elem
ent
ELEM
ENT
DES
CR
IPTO
RS
(see
als
o p
ages
43-
47)
4W
hole
Org
anis
atio
n/W
ider
Hea
lthca
re S
yste
m
6.1
Dev
elo
pin
g t
he
Vis
ion
for
the
Org
anis
atio
n•
Act
ivel
y en
gage
with
col
leag
ues
and
key
influ
ence
rs, i
nclu
ding
pat
ient
s an
d pu
blic
,ab
out t
he fu
ture
of t
he o
rgan
isatio
n
•Br
oadl
y sc
an a
nd a
naly
se th
e fu
ll ra
nge
of fa
ctor
s th
at w
ill im
pact
upo
n th
eor
gani
satio
n, to
cre
ate
likel
y sc
enar
ios
for i
ts fu
ture
•C
reat
e a
visio
n w
hich
is b
old,
inno
vativ
e a
nd re
flect
s th
e co
re v
alue
s of
the
NH
S
•C
ontin
uous
ly e
nsur
es th
at th
e or
gani
satio
n’s
visio
n is
com
patib
le w
ith fu
ture
deve
lopm
ents
with
in th
e w
ider
hea
lthca
re s
yste
m
Act
ivel
y en
gage
s ke
y st
akeh
olde
rs in
cre
atin
g a
bold
, inn
ovat
ive,
sha
red
visio
n w
hich
refle
cts
the
futu
re n
eeds
and
asp
iratio
ns o
f the
pop
ulat
ion
and
the
futu
re d
irect
ion
ofhe
alth
care
. Th
inks
bro
adly
and
alig
ns th
e vi
sion
to th
e N
HS
core
val
ues
and
the
valu
es o
fth
e w
ider
hea
lthca
re s
yste
m.
6.2
Infl
uen
cin
g V
isio
n in
th
eW
ider
Hea
lth
care
Sys
tem
•Se
ek o
ppor
tuni
ties
to e
ngag
e in
deb
ate
abou
t the
futu
re o
f hea
lth a
nd c
are
rela
ted
serv
ices
•W
ork
in p
artn
ersh
ip w
ith o
ther
s in
the
heal
thca
re s
yste
m to
dev
elop
a s
hare
d vi
sion
•N
egot
iate
com
prom
ises
in th
e in
tere
sts
of b
ette
r pat
ient
ser
vice
s
•In
fluen
ce k
ey d
ecisi
on-m
aker
s w
ho d
eter
min
e fu
ture
gov
ernm
ent p
olic
y th
at im
pact
son
the
NH
S an
d its
ser
vice
s
Act
ivel
y pa
rtic
ipat
es in
and
lead
s on
deb
ates
abo
ut th
e fu
ture
of h
ealth
, wel
lbei
ng a
ndre
late
d se
rvic
es.
Man
ages
pol
itica
l int
eres
ts, b
alan
cing
tens
ions
bet
wee
n or
gani
satio
nal
aspi
ratio
ns a
nd th
e w
ider
env
ironm
ent.
Sha
pes
and
influ
ence
s lo
cal,
regi
onal
and
natio
nal h
ealth
prio
ritie
s an
d ag
enda
s.
6.3
Co
mm
un
icat
ing
th
eV
isio
n•
Com
mun
icat
e th
eir i
deas
and
ent
husia
sm a
bout
the
futu
re o
f the
org
anisa
tion
and
itsse
rvic
es c
onfid
ently
and
in a
way
whi
ch e
ngag
es a
nd in
spire
s ot
hers
•Ex
pres
s th
e vi
sion
clea
rly, u
nam
bigu
ously
and
vig
orou
sly
•En
sure
that
sta
keho
lder
s w
ithin
and
bey
ond
the
imm
edia
te o
rgan
isatio
n ar
e aw
are
ofth
e vi
sion
and
any
likel
y im
pact
it m
ay h
ave
on th
em
•Ta
ke ti
me
to b
uild
crit
ical
sup
port
for t
he v
ision
and
ens
ure
it is
shar
ed a
nd o
wne
d by
thos
e w
ho w
ill b
e co
mm
unic
atin
g it
Cle
arly
com
mun
icat
es th
e vi
sion
in a
way
that
eng
ages
and
em
pow
ers
othe
rs.
Use
sen
thus
iasm
and
ene
rgy
to in
spire
oth
ers
and
enco
urag
e jo
int o
wne
rshi
p of
the
visio
n.A
ntic
ipat
es a
nd c
onst
ruct
ivel
y ad
dres
ses
chal
leng
e.
6.4
Emb
od
yin
g t
he
Vis
ion
•A
ct a
s a
role
mod
el, b
ehav
ing
in a
man
ner w
hich
refle
cts
the
valu
es a
nd p
rinci
ples
inhe
rent
in th
e vi
sion
•D
emon
stra
te c
onfid
ence
, sel
f bel
ief,
tena
city
and
inte
grity
in p
ursu
ing
the
visio
n
•C
halle
nge
beha
viou
rs w
hich
are
not
con
siste
nt w
ith th
e vi
sion
•Id
entif
y sy
mbo
ls, ri
tual
s an
d ro
utin
es w
ithin
the
orga
nisa
tion
whi
ch a
re n
ot c
onsis
tent
with
the
visio
n, a
nd re
plac
e th
em w
ith o
nes
that
are
Con
siste
ntly
disp
lays
pas
sion
for t
he v
ision
and
dem
onst
rate
s pe
rson
al c
omm
itmen
t to
itth
roug
h th
eir d
ay-t
o-da
y ac
tions
. Use
s pe
rson
al c
redi
bilit
y to
act
as
a co
nvin
cing
advo
cate
for t
he v
ision
.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• D
oes
not
invo
lve
othe
rs in
cre
atin
g an
d de
finin
g th
e vi
sion
• D
oes
not
alig
n th
eir
visi
on w
ith t
he w
ider
hea
lth a
nd c
are
agen
da•
Mis
ses
oppo
rtun
ities
to
com
mun
icat
e an
d sh
are
unde
rsta
ndin
g of
the
vis
ion
with
oth
ers
• L
acks
ent
husi
asm
and
com
mitm
ent
for
driv
ing
the
visi
on

NHS Leadership Framework 67
7. D
ELIV
ERIN
G T
HE
STRA
TEG
YTh
ose
in s
enio
r pos
ition
al le
ader
ship
role
s de
liver
the
stra
tegi
c vi
sion
by d
evel
opin
g an
d ag
reei
ng s
trat
egic
pla
ns th
at p
lace
pat
ient
car
e at
the
hear
t of t
he s
ervi
ce, a
nd e
nsur
ing
that
thes
e ar
e tr
ansla
ted
into
ach
ieva
ble
oper
atio
nal p
lans
. Thi
s re
quire
s th
em to
dem
onst
rate
eff
ectiv
enes
s in
fram
ing
the
stra
tegy
, dev
elop
ing
the
stra
tegy
, im
plem
entin
g th
e st
rate
gy, a
nd e
mbe
ddin
g th
e st
rate
gy.
Elem
ent
ELEM
ENT
DES
CR
IPTO
RS
(see
als
o p
ages
49-
53)
4W
hole
Org
anis
atio
n/W
ider
Hea
lthca
re S
yste
m
7.1
Fram
ing
th
e St
rate
gy
•Ta
ke a
ccou
nt o
f the
cul
ture
, hist
ory
and
long
term
und
erly
ing
issue
s fo
r the
org
anisa
tion
•U
se s
ound
org
anisa
tiona
l the
ory
to in
form
the
deve
lopm
ent o
f str
ateg
y
•Id
entif
y be
st p
ract
ice
whi
ch c
an b
e ap
plie
d to
the
orga
nisa
tion
•Id
entif
y st
rate
gic
optio
ns w
hich
will
del
iver
the
orga
nisa
tion’
s vi
sion
Crit
ical
ly re
view
s re
leva
nt th
inki
ng, i
deas
and
bes
t pra
ctic
e an
d ap
plie
s w
hole
sys
tem
sth
inki
ng in
ord
er to
con
cept
ualis
e a
stra
tegy
in li
ne w
ith th
e vi
sion.
7.2
Dev
elo
pin
g t
he
Stra
teg
y•
Enga
ge w
ith k
ey in
divi
dual
s an
d gr
oups
to fo
rmul
ate
stra
tegi
c pl
ans
to m
eet t
he v
ision
•St
rive
to u
nder
stan
d ot
hers
’ ag
enda
s, m
otiv
atio
ns a
nd d
river
s in
ord
er to
dev
elop
stra
tegy
whi
ch is
sus
tain
able
•C
reat
e st
rate
gic
plan
s w
hich
are
cha
lleng
ing
yet r
ealis
tic a
nd a
chie
vabl
e
•Id
entif
y an
d m
itiga
te u
ncer
tain
ties
and
risks
ass
ocia
ted
with
str
ateg
ic c
hoic
es
Inte
grat
es th
e vi
ews
of a
bro
ad ra
nge
of s
take
hold
ers
to d
evel
op a
coh
eren
t, jo
ined
up
and
sust
aina
ble
stra
tegy
. A
sses
ses
orga
nisa
tiona
l rea
dine
ss fo
r cha
nge.
Man
ages
the
risks
, pol
itica
l sen
sitiv
ities
and
env
ironm
enta
l unc
erta
intie
s in
volv
ed.
7.3
Imp
lem
enti
ng
th
eSt
rate
gy
•En
sure
that
str
ateg
ic p
lans
are
tran
slate
d in
to w
orka
ble
oper
atio
nal p
lans
, ide
ntify
ing
risks
, crit
ical
suc
cess
fact
ors
and
eval
uatio
n m
easu
res
•Id
entif
y an
d st
reng
then
org
anisa
tiona
l cap
abili
ties
requ
ired
to d
eliv
er th
e st
rate
gy
•Es
tabl
ish c
lear
acc
ount
abili
ty fo
r the
del
iver
y of
all
elem
ents
of t
he s
trat
egy,
hol
d pe
ople
to a
ccou
nt a
nd e
xpec
t to
be h
eld
to a
ccou
nt th
emse
lves
•Re
spon
d qu
ickl
y an
d de
cisiv
ely
to d
evel
opm
ents
whi
ch re
quire
a c
hang
e in
str
ateg
y
Resp
onds
con
stru
ctiv
ely
to c
halle
nge.
Put
s sy
stem
s, s
truc
ture
s, p
roce
sses
, res
ourc
es a
ndpl
ans
in p
lace
to d
eliv
er th
e st
rate
gy.
Esta
blish
es a
ccou
ntab
ilitie
s an
d ho
lds
peop
le in
loca
l, re
gion
al, a
nd n
atio
nal s
truc
ture
s to
acc
ount
for j
oint
ly d
eliv
erin
g st
rate
gic
and
oper
atio
nal p
lans
. D
emon
stra
tes
flexi
bilit
y w
hen
chan
ges
requ
ired.
7.4
Emb
edd
ing
th
e St
rate
gy
•Su
ppor
t and
insp
ire o
ther
s re
spon
sible
for d
eliv
erin
g st
rate
gic
and
oper
atio
nal p
lans
,he
lpin
g th
em to
ove
rcom
e ob
stac
les
and
chal
leng
es, a
nd to
rem
ain
focu
sed
•C
reat
e a
cons
ulta
tive
orga
nisa
tiona
l cul
ture
to s
uppo
rt d
eliv
ery
of th
e st
rate
gy a
nd to
driv
e st
rate
gic
chan
ge w
ithin
the
wid
er h
ealth
care
sys
tem
•Es
tabl
ish a
clim
ate
of tr
ansp
aren
cy a
nd tr
ust w
here
resu
lts a
re d
iscus
sed
open
ly
•M
onito
r and
eva
luat
e st
rate
gic
outc
omes
, mak
ing
adju
stm
ents
to e
nsur
e su
stai
nabi
lity
of th
e st
rate
gy
Enab
les
and
supp
orts
the
cond
ition
s an
d cu
lture
nee
ded
to s
usta
in c
hang
es in
tegr
al to
the
succ
essf
ul d
eliv
ery
of th
e st
rate
gy.
Kee
ps m
omen
tum
aliv
e by
rein
forc
ing
key
mes
sage
s, m
onito
ring
prog
ress
and
reco
gnisi
ng w
here
the
stra
tegy
has
bee
n em
brac
edby
oth
ers.
Eva
luat
es o
utco
mes
and
use
s le
arni
ngs
to a
dapt
str
ateg
ic a
nd o
pera
tiona
lpl
ans.
Gen
eric
beh
avio
urs
ob
serv
ed if
ind
ivid
ual
is n
ot
yet
dem
on
stra
tin
g t
his
do
mai
n:
• D
oes
not
alig
n th
e st
rate
gy w
ith lo
cal,
natio
nal a
nd/o
r w
ider
hea
lth c
are
syst
em r
equi
rem
ents
• W
orks
to
deve
lop
the
stra
tegy
in is
olat
ion
with
out
inpu
t or
fee
dbac
k fr
om o
ther
s•
Abs
olve
s on
esel
f of
res
pons
ibili
ty f
or h
oldi
ng o
ther
s to
acc
ount
• F
ails
to
enab
le a
n or
gani
satio
nal c
ultu
re t
hat
embr
aces
the
str
ateg
y

Related Documents











