03/17/22 [email protected] 1 Evidence based Evidence based Emergency Medicine Emergency Medicine Dr Jaycen Cruickshank Director of Emergency Medicine, Ballarat Health Services Senior Lecturer, Rural Clinical School, University of Melbourne

6/3/2015 [email protected] 1 Evidence based Emergency Medicine Dr Jaycen Cruickshank Director of Emergency Medicine, Ballarat Health Services Senior Lecturer,
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
04/18/[email protected]
Evidence based Emergency Evidence based Emergency MedicineMedicine
Dr Jaycen Cruickshank
Director of Emergency Medicine, Ballarat Health Services
Senior Lecturer, Rural Clinical School, University of Melbourne

04/18/[email protected]
Introduction Introduction
Evidenced based Emergency Medicine is using validated clinical decision rules.
The audience will learn in this session– What evidence is available and easy to use
– How to find the evidence
– Evidence from the patient’s point of view
– Patient fact sheets There is too much to remember - students are
now taught how to find it.

04/18/[email protected]
Overview Overview
Big picture - these mostly ignoredExplain how all the individual topics fit
togetherX-ray?Admit?IV or oral?CT?
Pittsburgh
Syncope
What next?
TIMICURB-65
PSI
Wells
OttawaABCD2

04/18/[email protected]
AgendaAgenda
Topics Medical, trauma/injury Resources: www.patient.co.uk www.betterhealth.vic.gov.au www.scaphoidfracture.com.au http://emedicine.medscape.com/ Google www.mdcalc.com
04/18/[email protected]
Clinical Decision RulesClinical Decision Rules
TIA - ABCD2
Pneumonia– PSI
– CURB-65 PE - Wells
criteria DVT - Wells
criteria San francisco
syncope rule
Ottawa ankle and foot rules Pittsburg knee rules Canadian neck rules vs
Nexus guidelines NICE guidelines
– Head injury RCH guidelines http://www.rch.org.au/clinicalguide/cpg.cfm RWH guidelines

ABCD2 algorithm identifies risk of stroke after TIA
People who have had a suspected TIA (that is, they have no neurological symptoms at the time of assessment [within 24 hours]) should be assessed as soon as possible for their risk of subsequent stroke using a validated scoring system, such as ABCD2
Score >=4 – Admit, aspirin, specialist
and imaging early (<24 hrs) Score <4
– Discharge, Review within 1 week
– General preventative measures
A - age (>=60 years, 1 point)
B - blood pressure at presentation (>=140/90 mmHg, 1 point)
C - clinical features – (unilateral weakness, 2
points; – speech disturbance without
weakness, 1 point) D - Duration of symptoms
– >= 60 minutes, 2 points; – 10-59 minutes, 1 point
Diabetes (1 point) ABCD2 is calculated based
on:total scores range from 0 (low risk) to 7 (high risk).

General prevention of stroke control of risk factors: smoking, lack of exercise hypertension - target blood pressure for patients with a TIA or stroke
is <130/<80 mmHg hyperlipidaemia - ideal targets? treatment of symptomatic vascular disease such as giant cell arteritis antiplatelet therapy is most effective in patients in sinus rhythm: the combination of modified-release (MR) dipyridamole and aspirin is
recommended for people who have had an ischaemic stroke or a transient ischaemic attack (TIA) for a period of 2 years from the most recent event. Thereafter, or if MR dipyridamole is not tolerated, preventative therapy should revert to standard care (including long-term treatment with low-dose aspirin)
clopidogrel - clopidogrel alone (within its licensed indications) is recommended for people who are intolerant of low-dose aspirin
anticoagulant therapy is effective in patients in atrial fibrillation and can reduce the likelihood of further vascular events
there is no place for anticoagulant therapy in managing patients with a stroke or TIA in the absence of atrial fibrillation.
carotid endarterectomy - highly beneficial in symptomatic patients with 70-99% stenosis of the internal carotid
ACE inhibitition - using a combination of long-acting ACE inhibitor (e.g. perindopril or ramipril) and a thiazide diuretic (e.g.indapamide) has been suggested
04/18/[email protected]
CURB-65 (pneumonia)CURB-65 (pneumonia)
Pneumonia is not a particularly difficult diagnosis to make
Assessment of severity of disease influences
TreatmentAdmit or dischargeOutcomesDo we agree on severity?

04/18/[email protected]
CURB-65 predicts mortalityCURB-65 predicts mortality
1 point each Confusion Urea > 7mmol/L Resp rate >20, pCO2 <32 Blood pressure
<90mmHg 65 - Age >65 http://
www.mdcalc.com/mdcalc/wordpress/curb-65
Mortality Score 0 = 0.7% 1 = 3.2% 2 = 13% 3 = 17% 4 = 42% 5 = 57%
04/18/[email protected]
Pneumonia Severity Index – also Pneumonia Severity Index – also called PORT score or CAP riskcalled PORT score or CAP risk Class/mortality/Where/What 1- 0.1% -home - oral antis 2 - 0.3% -home-HITH - oral/IV 3- 0.9%- ?? admit/IV antis 4 - 9%- admit/IV antis 5 - 30%- ICU/IV antis
Details in Victorian Antibiotic guidelines
BHS compliance 27%!
CURB -65 1 2 3 4 5

04/18/[email protected]
Well’s criteria -PEWell’s criteria -PE
Radiologists in Ballarat feel too many CTPAs are done, and feel that there is a lack of appropriate use and understanding of history, exam, and tests - ECG, CXR, D-Dimer
They have a case, but sometimes … “no CT without a D-Dimer”
Big man, 30’s, wife, 2 year old, trip to south africa, new diagnoses of calf strain and then asthma
He died. He should not have died.
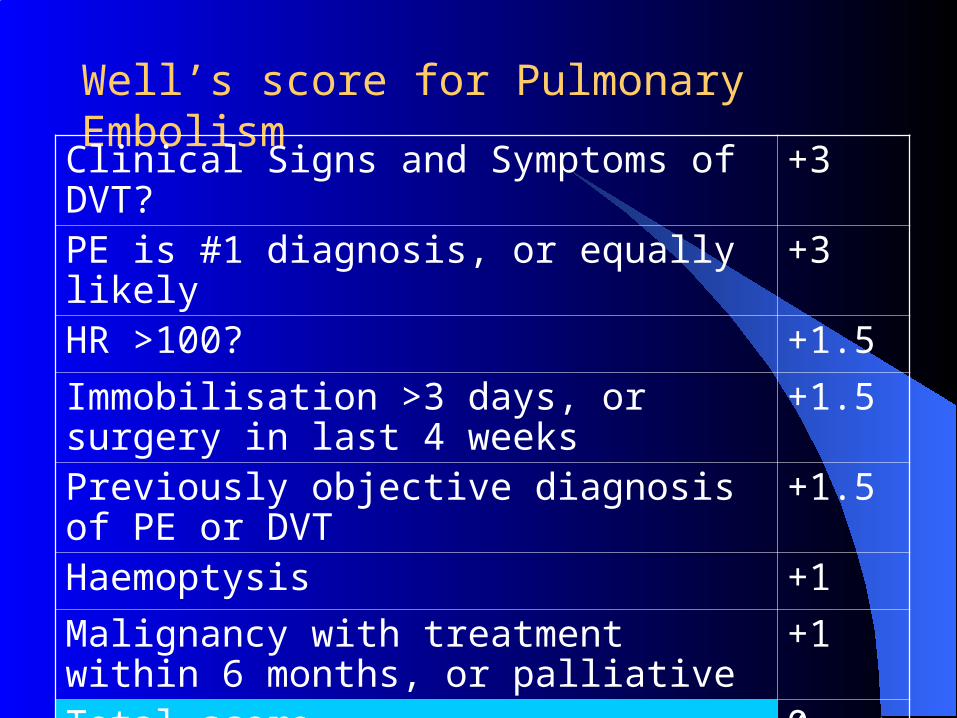
Well’s score for Pulmonary EmbolismClinical Signs and Symptoms of DVT? +3
PE is #1 diagnosis, or equally likely +3
HR >100? +1.5
Immobilisation >3 days, or surgery in last 4 weeks
+1.5
Previously objective diagnosis of PE or DVT +1.5
Haemoptysis +1
Malignancy with treatment within 6 months, or palliative
+1
Total score 0-12.5
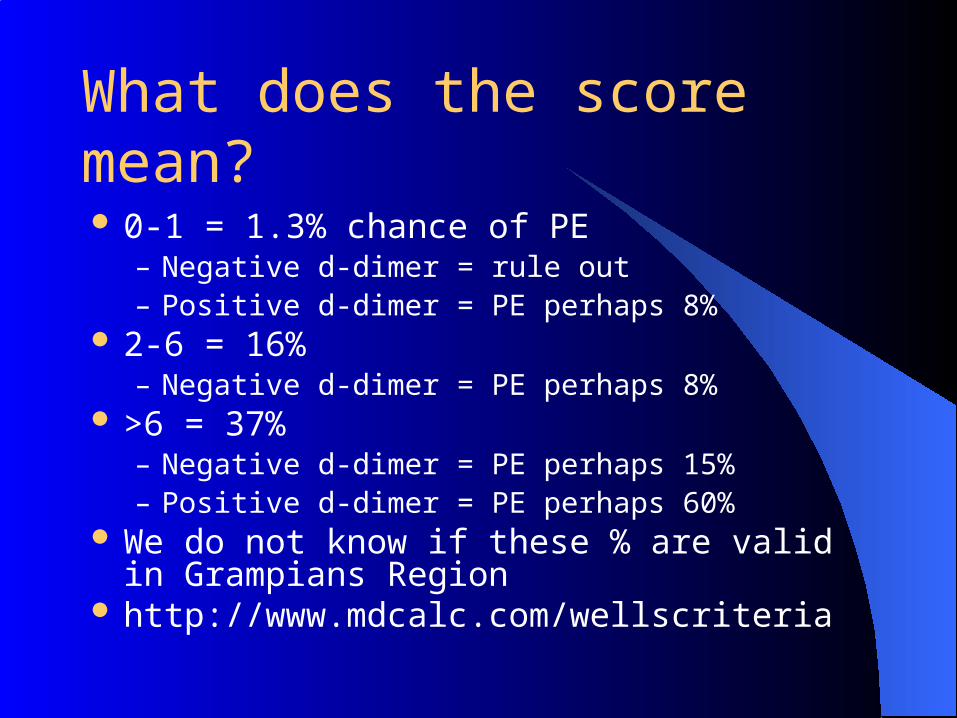
What does the score mean?
0-1 = 1.3% chance of PE– Negative d-dimer = rule out– Positive d-dimer = PE perhaps 8%
2-6 = 16% – Negative d-dimer = PE perhaps 8%
>6 = 37% – Negative d-dimer = PE perhaps 15%– Positive d-dimer = PE perhaps 60%
We do not know if these % are valid in Grampians Region
http://www.mdcalc.com/wellscriteria

San Francisco syncope rule
Congestive Heart Failure history? Yes +1Hematocrit < 30%? Yes
+1ECG Abnormal ? Yes
+1Shortness of Breath History? Yes
+1Systolic BP < 90 mmHg at Triage? Yes +1Any of these = high risk
How to use this tool?You still look for features on history - e.g micturition,
cough, posture, and on examination e.g aortic stenosis to make a diagnosis of serious or harmless cause, then use the tool when you have found nothing serious.
If you suspect subarachnoid haemorrhage, then the tool does not help you rule it out.
Note: This rule has a 96% sensitivity and 62% specificity for serious outcome. Negative predictive value: 99.2%; positive predictive value 24.8%.Serious Outcome in this study is defined as "death, myocardial infarction, arrhythmia, pulmonary embolism, stroke, subarachnoid hemorrhage, significant hemorrhage, or any condition causing a return ED visit and hospitalization for a related event."

Characteristics of Patients Who Should Characteristics of Patients Who Should Undergo Radiography After Knee TraumaUndergo Radiography After Knee Trauma
Ottawa knee rules Age >55 years Tenderness at head of fibula Isolated tenderness of
patella Inability to flex knee to 90
degrees Inability to walk four
weight-bearing steps immediately after the injury and in the emergency department
http://www.mdcalc.com/mdcalc/wordpress/ottawa-ankle-and-pittsburgh-knee-rules
Pittsburgh decision rules
Blunt trauma or a fall as mechanism of injury plus either of the following:
Age < 12 or >50 years Inability to walk four
weight-bearing steps in the emergency department
04/18/[email protected]


Canadian C-spine rules better than NEXUS to rule out neck injury http://www.aafp.org/afp/20040515/tips/10.html Canadian rules better, used in UK guidelines also Approx 7500 study with 162 clinically important injuries
– Canadian C-spine rule detected 161 of 162 clinically important injuries– NEXUS rule detected 147 of 162 (sensitivity = 99.4 percent versus 90.7 percent).
The Canadian C-spine rule more specific than the NEXUS rule (45.1 percent versus 36.8 percent).
The Canadian C-spine rule had a higher inter-rater reliability than the NEXUS rule: 0.63 versus 0.47.
Physicians were slightly more uncomfortable when applying the Canadian C-spine rule (8.0 percent versus 7.1 percent using the NEXUS rule were uncomfortable or very uncomfortable; P = .03),
Fewer patients required radiography based on the use of the Canadian C-spine rule than the NEXUS rule (56 percent versus 67 percent), reducing cost and length of stay in the emergency department.

The UK NICE guidelines.
http://www.nice.org.uk/nicemedia/pdf/CG56QuickRedGuide.pdf


04/18/[email protected]
SummarySummary
State what has been learned Some good clinical decision rules exist, to help our clinical
judgement. They are easily accessible Patients can find information
Define ways to apply training Favourites on your computers Ipod touch, other hand held device. Patient access to online information.
Request feedback of training session
04/18/[email protected]
Where to Get More InformationWhere to Get More Information
Other tools TIMI score http://www.mdcalc.com/uanstemitimiscoreList books, articles, electronic sources Emergency Medicine. Avoiding the pitfalls and improving the
outcomes - Amal Mattu & Deepti Goyal. Blackwell publishing. BMJ Books. A short book to take the step from good to expert.
Pat Standen, DHS Always helpful in providing support in the region if asked.
Related Documents











