UROGENITAL NEOPLASMS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UROGENITAL NEOPLASMS
KIDNEY•Grawitz /Adenocacinoma / Renal cell carcinoma
•Willm’s / Nefroblastoma
Grawitz Tumor• Parenchymal• From Proximal tubules epithelial cell
• Most kidney cancer in adults, about 90%
• 50-70 years old• Men : Woman 2:1
Etiology & Risk Factor• Etio ? Multifactor
Risk :• Smoke• Arsenic, asbestos,• Obesity, esterogen
Histopathology1.Clear cell carcinoma2.Papillary carcinoma3.Chromophobe renal carcinoma4.Collecting duct carcinoma
DiagnosisSign & Symptom :• Back Pain• Hematuria• Abdominal mass
Imaging :• IVP distortion• CT Scan
Nefroblastoma• From blastemal cell• Mostly in children, < 10 years, most 2-5 years
• Unilateral, 10% bilateral
Symptom:• Asymptomatic• Hematuria
Imaging USG, IVP
Histopathology• Anaplastic Poor Prognosis
Ureteral Cancer
• Ureteral cancer is cancer of the ureters rare < 1%
• Ureteral cancer is usually transitional cell carcinoma. Transitional cell carcinoma is "a common cause of ureter cancer and other urinary (renal pelvic) tract cancers.
• Risk factor : smoking
• Sign and symptoms : hematuria,diminished urine stream, nocturia, itching, incontinence, dysuria, recurrent urinary tract infection, urethral discharge and swelling.
• Diagnosis : - PIV filling defect- Urinary cytology- Urteroscopy to show in the lumen of ureter and guiding biposy.
• Treatment : Treatment methods include surgery, chemotherapy,
radiation therapy and medication
Bladder Cancer
Bladder cancer:Epidemiology
• Incidence: 20/100000/year (Europe)• Mortality: 8-9/100000/year
• Fourth most common cancer in men– Incidence: 31.1 mortality: 12.1
• Seventh most common cancer in women– Incidence: 9.5 mortality: 4.5
• At diagnosis >70%: > 65 y of age
Bladder cancer: Histology
• 90-95% transitional-cell carcinoma
• 3% squamos-cell carcinoma• 2% adenocarcinoma• <1% small-cell carcinoma
Bladder cancer: Entities
• 75-85% superficial bladder cancerpTa, pTis, pT1
• 10-15% muscle-invasive bladder cancer
pT2, pT3, pT4• 5% metastatic bladder cancer
N+, M+
• Classification, ISUP (international society of urologic pathology).– Benign
• Urothelial papilloma– Malignant
• Papillary– Papillary urothelial neoplasm of low malignant potential
– Papillary urothelial carcinoma – low grade– Papillary urothelial carcinoma – high grade
• Flat– Urothelial carcinoma in-situ– Invasive urothelial carcinoma
– Squamous cell carcinoma
Bladder cancer:Classification
Bladder cancer:Clinical
• Clinical:– Painless hematuria– 50-70 year, men 3x>women– Risk factors
•Smoking•Industrial solvent, hydrocarbons, dyes
•Cystitis•Schistosomiasis•cyclophosphamide
Bladder cancer:Clinical
• Clinical:– High recurrence rate– Fatal by ureteric obstruction– Overall survival 5y: 57%– Ureteric carcinoma 5y survival: 10%
Bladder cancer: Stage and Prognosis
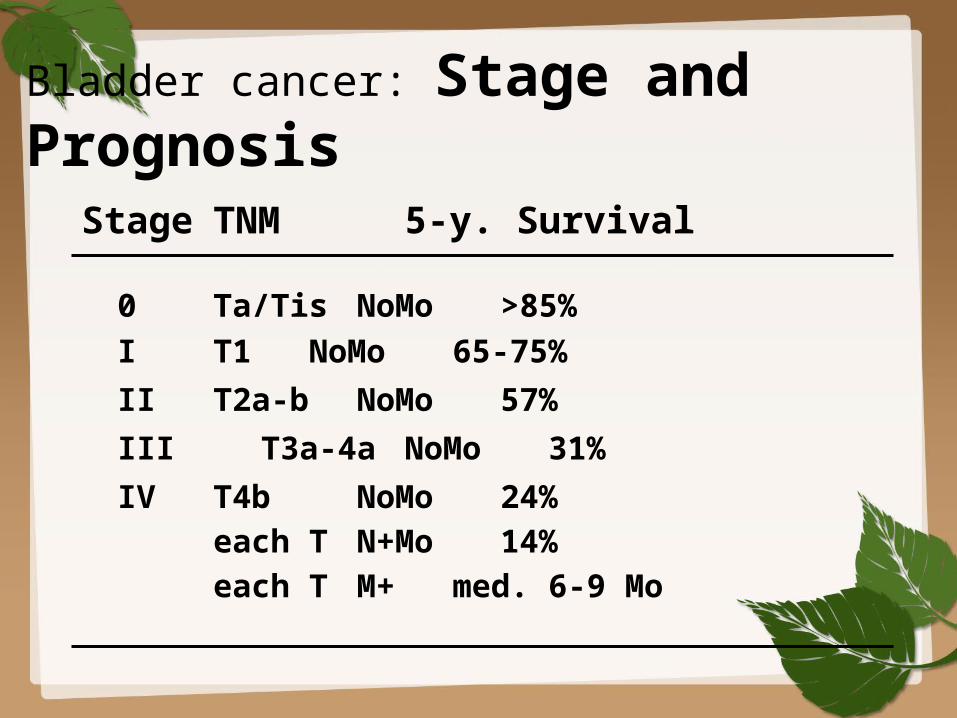
Stage TNM 5-y. Survival
0 Ta/Tis NoMo >85%I T1 NoMo 65-75%II T2a-b NoMo 57%III T3a-4a NoMo 31%IV T4b NoMo 24%
each T N+Mo 14%each T M+ med. 6-9 Mo
Superficial Bladder CancerpTa, pT1, Tis
• Standard of care=intravesical Therapy transurethral resection
• Relapse rate:70% adjuvant therapy
Superficial Bladder Cancer
• Histological grading is importantG1G2G3
Relapse rate 42% 50% 80%
Progression rate 2%11% 45%
Superficial Bladder CancerAdjuvant Therapy
• Reduces relpase rate by 30-80%
– Doxorubicin weekly 6-8 w. / monthly 6-12
– Mitomycin C weekly 6-8 w. / monthly 6-12
– BCG weekly 6-8 w. /Mo 3 and 6
Invasive bladder cancer
• Standard of care = Radical cystectomy with pelvic lymphadenectomy
Only about 50% of patients with high-grade invasive disease are cured
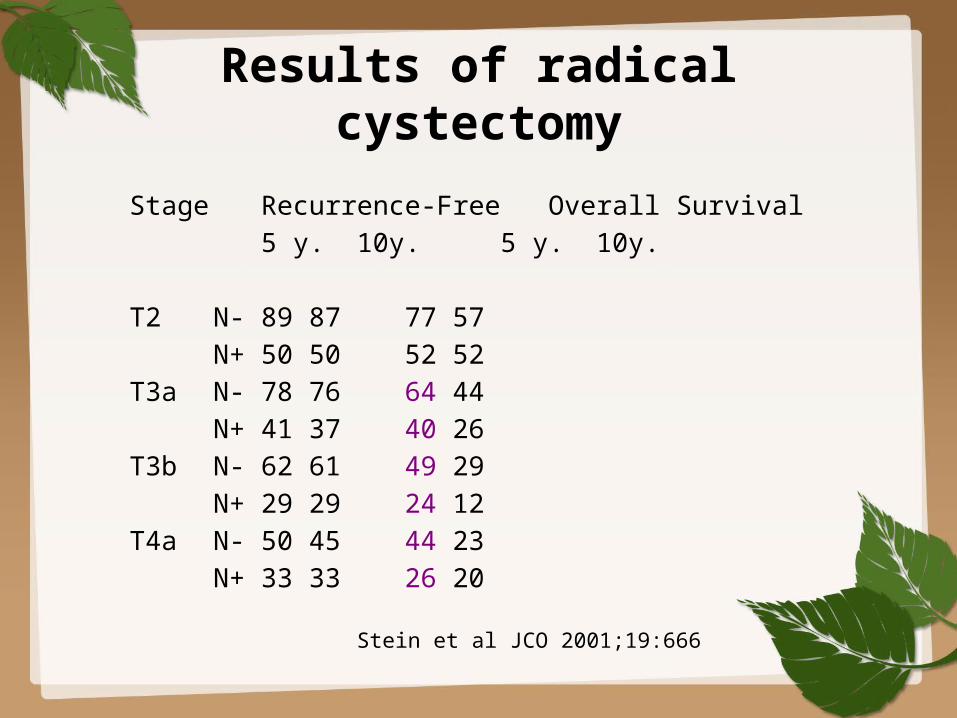
Results of radical cystectomy
Stage Recurrence-Free Overall Survival5 y. 10y. 5 y. 10y.
T2 N- 89 87 77 57N+ 50 50 52 52
T3a N- 78 76 64 44N+ 41 37 40 26
T3b N- 62 61 49 29N+ 29 29 24 12
T4a N- 50 45 44 23N+ 33 33 26 20
Stein et al JCO 2001;19:666
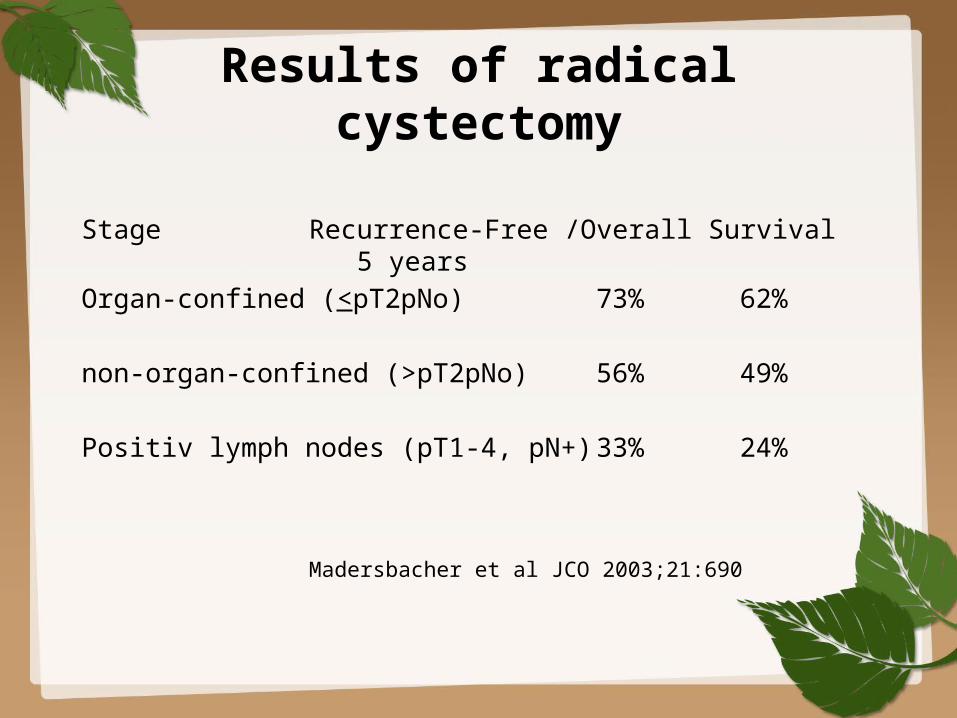
Results of radical cystectomy
Stage Recurrence-Free /Overall Survival5 years
Organ-confined (<pT2pNo) 73% 62%
non-organ-confined (>pT2pNo) 56% 49%
Positiv lymph nodes (pT1-4, pN+)33% 24%
Madersbacher et al JCO 2003;21:690
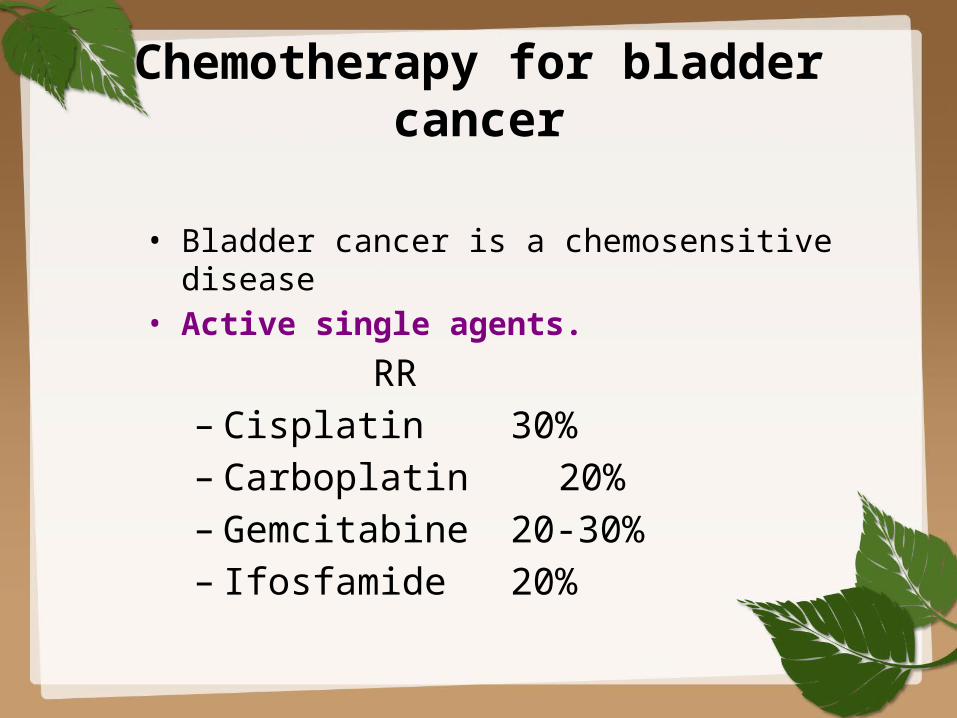
Chemotherapy for bladder cancer
• Bladder cancer is a chemosensitive disease
• Active single agents.RR
– Cisplatin 30%– Carboplatin 20%– Gemcitabine 20-30%– Ifosfamide 20%
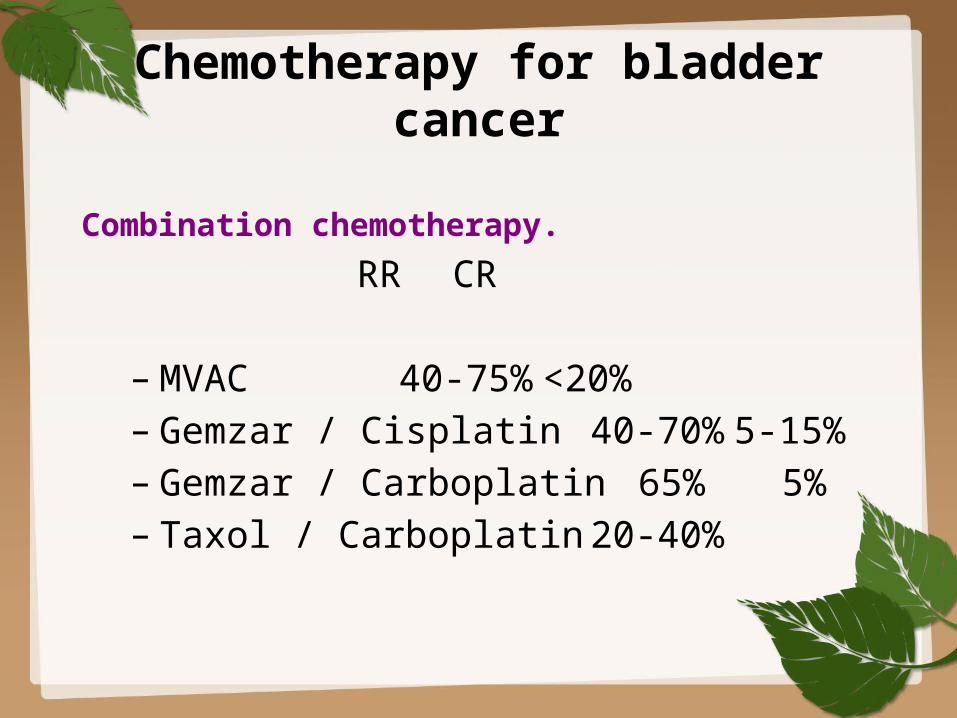
Chemotherapy for bladder cancer
Combination chemotherapy.RR CR
– MVAC 40-75% <20%– Gemzar / Cisplatin 40-70% 5-15%– Gemzar / Carboplatin 65% 5%– Taxol / Carboplatin20-40%
Adjuvant chemotherapy
• Six randomised trials have compared CT with observation after cystectomy or RT
• 4x no survival benefit• 2x benefit from adjuvant CT no standard of care
– node positive disease, lymphovascular invasion, positive margins
Neoadjuvant chemotherapy
• Meta-analysis of ten randomised trials (2688 patients)
13% reduction in risk of death5% absolute benefit at 5 yearsOS increased from 45% to 50%
ABC Meta-analysis Collaboration. Lancet 2003;361:1927
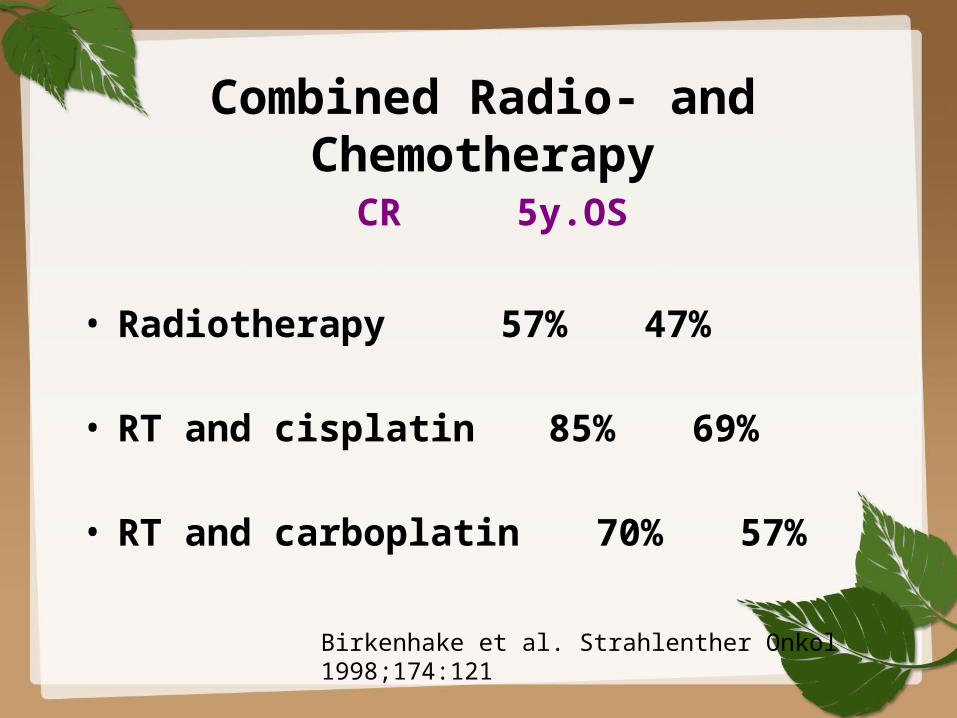
Combined Radio- and Chemotherapy
CR 5y.OS
• Radiotherapy 57% 47%
• RT and cisplatin 85% 69%
• RT and carboplatin 70% 57%
Birkenhake et al. Strahlenther Onkol 1998;174:121
Bladder-sparing therapy for invasive bladder cancer
• High probability of subsequent distant metastasis after cystectomy or radiotherapy alone (50% within 2 years)
• Radiotherapy im comparison with cystectomy has inferior results (local control 40%)
• muscle-invasive bladder cancer is often a systemic disease
combined modality therapy
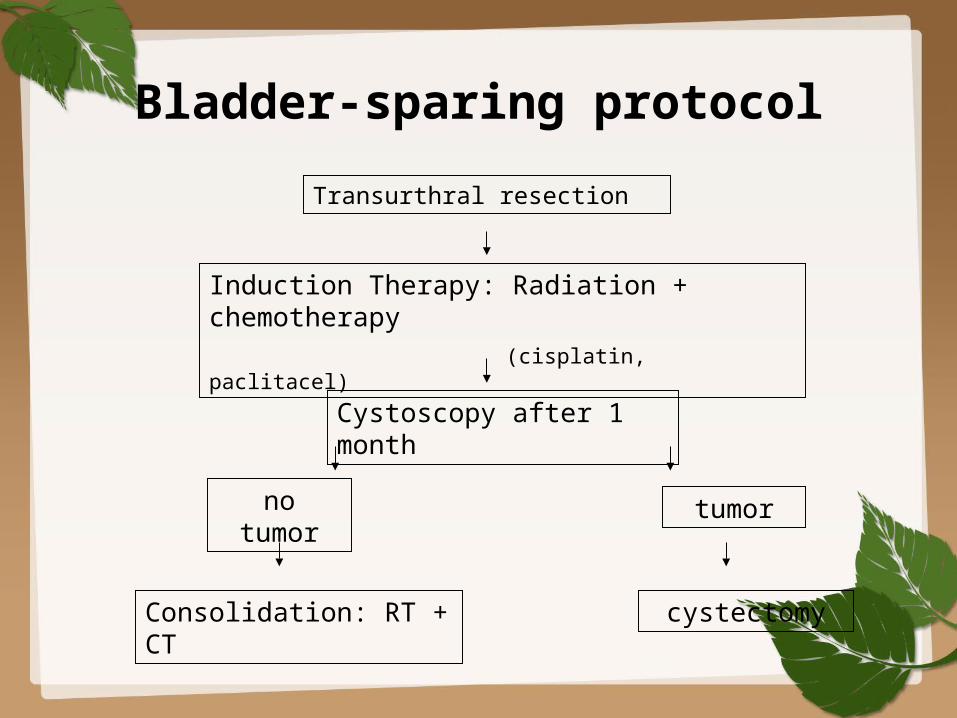
Bladder-sparing protocolTransurthral resection
Induction Therapy: Radiation + chemotherapy
(cisplatin, paclitacel)
Cystoscopy after 1 month
no tumor
tumor
Consolidation: RT + CT
cystectomy
Combined-modality treatment and organ preservation in invasive bladder
cancer
Rödel et al. JCO 2002;20:3061
415 patients with T1 high-risk, T1-4, No-1
Treatment: 1. Transurethral resection
2. RT (n=126), RCT (n=289) RT median 54 Gy, CT cisplatin week 1,
5
3. Restaging-TUR
Combined-modality treatment and organ preservation in invasive bladder
cancer
• Rödel et al. JCO 2002;20:3061
• Complete remission 72%• Local control after CR 64% (10 y.)• distant metastasis 35% (10 y.)• Disease-specific survival 42% (10 y.)• Preservation of bladder >80%
TUR and adjuvant Radio-Chemotherapy
• 5 year Survival 50-65%
• Preservation of Bladder 38-43%
Testicular tumor• Testicular cancer starts in the testicles. It typically develops in one or both testicles in young
• men, although it can occur at any age. It is a highly treatable and usually curable type of cancer
Germ cell tumors• More than 90% of cancers of the testicle develop in special cells known as germ cells. These
• are the cells that make sperm. There are 2 main types of germ cell tumors (GCTs) in men:
• Seminomas • Non-seminomas • Seminoma and non-seminoma cells look very different under a microscope.
• These 2 types occur about equally. Many testicular cancers contain both seminoma and non-seminoma cells. These mixed germ cell tumors are treated as non-seminomas because they grow and spread like non-seminomas
Seminomas • Seminomas tend to grow and spread more slowly than non-seminomas. The 2 main subtypes of these tumors are classical (or typical) seminomas and spermatocytic seminomas. Doctors can tell them apart by how they look under the microscope.
Classical seminoma:• More than 95% of seminomas are classical. These usually occur in men between 25 and 45.
Spermatocytic seminoma:• This rare type of seminoma tends to occur in older men. The average age of men diagnosed with spermatocytic seminoma is about 65. Spermatocytic tumors tend to grow more slowly and are less likely to spread to other parts of the body than classical seminomas
• Some seminomas can increase blood levels of a protein called human chorionic gonadotropin (HCG). HCG can be detected by a simple blood test and is considered a tumor marker for certain types of testicular cancer. It can be used for diagnosis and to check how the patient is responding to treatment.
Non-seminomas • These types of germ cell tumors usually occur in men between their late teens and early 30s. There are 4 main types of non-seminoma tumors:
• Embryonal carcinoma • Yolk sac carcinoma • Choriocarcinoma • Teratoma • Most tumors are a mix of 2 or more different types (sometimes with a seminoma component as well), but this does not change treatment. All non-seminoma cancers are treated the same way.
Embryonal carcinoma:This type of non-seminoma is present to some degree in about 40% of testicular tumors, but pure embryonal carcinomas occur only 3% to 4% of the time. When seen under a microscope, these tumors can look like tissues of very early embryos. This type of non-seminoma tends to grow rapidly and spread outside the testicle. Embryonal carcinoma can increase blood levels of a tumor marker protein called alpha-fetoprotein (AFP), as well as HCG.
Yolk sac carcinoma:• These tumors are so named because their cells look like the yolk sac of an early human embryo. Other names for this cancer include yolk sac tumor, endodermal sinus tumor, infantile embryonal carcinoma, or orchidoblastoma. This is the most common form of testicular cancer in children (especially in infants), but pure yolk sac carcinomas (tumors that do not contain other types of non-seminoma cells) are rare in adults. When they occur in children, these tumors usually are treated successfully. But they are of more concern when they occur in adults, especially if they are pure. Yolk sac carcinomas respond very well to chemotherapy, even if they have spread. This type of tumor almost always increases blood levels of AFP.
Choriocarcinoma:• This is a very rare and aggressive type of testicular cancer in adults. Pure choriocarcinoma is likely to spread rapidly to distant organs of the body, including the lungs, bones, and brain. More often, choriocarcinoma cells are present with other types of non-seminoma cells in a mixed germ cell tumor. These mixed tumors tend to have a better outlook than pure choriocarcinomas. This type of tumor increases blood levels of HCG.
Teratoma:• Teratomas are germ cell tumors with areas that, under a microscope, look like each of the 3 layers of a developing embryo: the endoderm (innermost layer), mesoderm (middle layer), and ectoderm (outer layer). Pure teratomas of the testicles are rare and do not increase AFP or HCG levels. More often, teratomas are seen as parts of mixed germ cell tumors.
• There are 3 main types of teratomas: Mature teratomas are tumors formed by cells similar to cells of adult tissues. They rarely spread to nearby tissues and distant parts of the body. They can usually be cured with surgery, but some come back (recur) after treatment. Immature teratomas are less well-developed cancers with cells that look like those of an early embryo. This type is more likely than a mature teratoma to grow into (invade) surrounding tissues, to spread (metastasize) outside the testicle, and to come back (recur) years after treatment. Teratoma with somatic type malignancy is a very rare cancer. These cancers have some areas that look like mature teratomas but have other areas where the cells have become a type of cancer that normally develops outside the testicle (such as a sarcoma, adenocarcinoma, or even leukemia)

Related Documents











