New New Cervical Cancer Cervical Cancer Screening Screening Recommendations Recommendations Management of Abnormal Management of Abnormal Results Results Walter Kinney M.D. Walter Kinney M.D. Division of Gynecologic Oncology Division of Gynecologic Oncology The Permanente Medical Group The Permanente Medical Group Clinical Professor of Ob/Gyn, U.C. Clinical Professor of Ob/Gyn, U.C. Davis Davis Sacramento, California Sacramento, California

56 th Annual Ob-Gyn Update New Cervical Cancer Screening Recommendations Management of Abnormal Results 56 th Annual Ob-Gyn Update New Cervical Cancer.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

5656thth Annual Ob-Gyn Update Annual Ob-Gyn Update
New New Cervical Cancer ScreeningCervical Cancer ScreeningRecommendationsRecommendations
Management of Abnormal ResultsManagement of Abnormal Results
Walter Kinney M.D.Walter Kinney M.D.Division of Gynecologic OncologyDivision of Gynecologic OncologyThe Permanente Medical GroupThe Permanente Medical Group
Clinical Professor of Ob/Gyn, U.C. DavisClinical Professor of Ob/Gyn, U.C. DavisSacramento, CaliforniaSacramento, California

Cervical Screening Guidelines Timeline: 2011-14Cervical Screening Guidelines Timeline: 2011-14
Slide courtesy of Dr. Hormuzd Katki, NCI
ASCCP/KP 2012: Why bother?ASCCP/KP 2012: Why bother?
1) ASCCP just approved 5 year screening! The
phrase “return to routine screening” in the 2007 Guidelines now means not annual but 5 years later! Who is at low enough risk to go to 5 years after an abnormal?
2) Cotesting is now recommended, so the results that providers start with will be fundamentally different. Examples: HPV negative HSIL or ASC-H or LSIL
3) Recommendations are too complicated! Nobody knows them, not even the “experts”


ASCCP 2012 ASCCP 2012 Goals and PrinciplesGoals and Principles
Goals
Define management of abnormals that did not exist before cotesting
Define which combinations of test results after an abnormal permitted “safe” return to routine, i.e. 5 year screening
Reflect new data on management of specific results (ASC-US and LSIL < 25; ECC CIN1 for example)
Principles Management by risk – similar risk means similar
management Immediate risk determines immediate management; risk
over time determines followup interval

ASCCP 2012 ASCCP 2012 Principles and MethodsPrinciples and Methods
Principles (continued)
High or low risk population doesn’t matter: Provide management consistent with what you are providing currently for results with like risks
Methods Examination of cotest results and histology outcomes
over time in 1.4 million cotested women followed up to 9 years
Risk similar to risks found after negative cytology at 3 years or negative cotesting at 5 years are considered acceptable
Outcome measures: Use what you have. Anything is better than nothing, which is what we have had up to this point. Cancer if you have it, CIN3+ if not, even CIN2+. Real EBM – use the best data that you have.

Castle PE et al, AJOG 2007Castle PE et al, AJOG 2007

Pap Risks Over Time – Not Stratified by HPV Status
Katki et al , JLGTD, 2013

High Grade Pap Risks by HPV Status
Katki et al , JLGTD, 2013

Monograph contentsMonograph contents1.1. Using risk to develop guidelinesUsing risk to develop guidelines
2.2. HPV & Equivocal PapsHPV & Equivocal Paps
3.3. HPV & Low-grade PapsHPV & Low-grade Paps
4.4. HPV & High-grade PapsHPV & High-grade Paps
5.5. HPV & negative PapsHPV & negative Paps
6.6. Risks for women under age 25Risks for women under age 25
7.7. Risks after non-precancer biopsiesRisks after non-precancer biopsies
8.8. Risks following treatment for Risks following treatment for precancerprecancer
Katki et al, Katki et al, J Low Genit Tract DisJ Low Genit Tract Dis, 2013, 2013

ASCCP 2012 - What We LearnedASCCP 2012 - What We Learned
Risks are not evenly distributed. Thankfully they fall into a few bands that facilitate assigning management. Nothing is perfect – risks are not identical, and some judgment is unavoidable about what is a clinically meaningful difference.
Risk order is almost always similar between immediate and long term risks. Hence 5 year risk was the default comparator
Endpoints matter more than we wanted them to. Cancer is the only ideal endpoint for screening schemes. CIN3+ is right for comparing test characteristics but not ideal for screening plans
Cotesting is better – by a LOT – for followup. Totally different from screening and totally counter- intuitive. Neg cotest = longer interval.

ASCCP 2012 - Example of Pap ASCCP 2012 - Example of Pap vs HPV vs Cotest Risksvs HPV vs Cotest Risks
In every clinical circumstance, negative cotesting provides greater reassurance and thus longer followup intervals than negative cytology alone or negative HPV testing alone. Examples: After a minimal abnormality (Pap negative HPV positive x 2,
ASC-US or LSIL) followed by a colposcopy with negative or CIN1 histology, women with a single negative cotest at 1 year had a 5 year risk of CIN2+ of 1.1%, versus 1.8% with 2 negative HPV tests or 4.0% with 2 negative Paps.
Women with ASC-H or HSIL followed by a negative or CIN1 colposcopy and a negative cotest had a 5 year risk of CIN2+ of 2.2% versus 4.4% after a negative HPV test and 7.0% after a negative Pap

“Lesser abnormalities”: HPV+/ASCUS or LSIL orPap- HPV x2
“Greater abnormalities”: HSIL or ASC-H or AGC
<CIN2: normal, metaplasia, CIN1
1 negative cotest over 1 year – retest in 3 years2 negative cotests over 2 years – retest in 5 years
2 negative cotests over 2 years – retest in 3 years
Untreated CIN2 or CIN2/3
2 negative Paps and colposcopies over 1 year (ASCCP 2006)AND one negative cotest in another 1 year– retest in 3 years
Treated CIN2, CIN2/3, CIN3, AIS
2 negative cotests over 2 years– retest in 3 years
Summary of Followup Recommendations 25+
ASCCP 2012 ASCCP 2012 What we got wrong and howWhat we got wrong and how
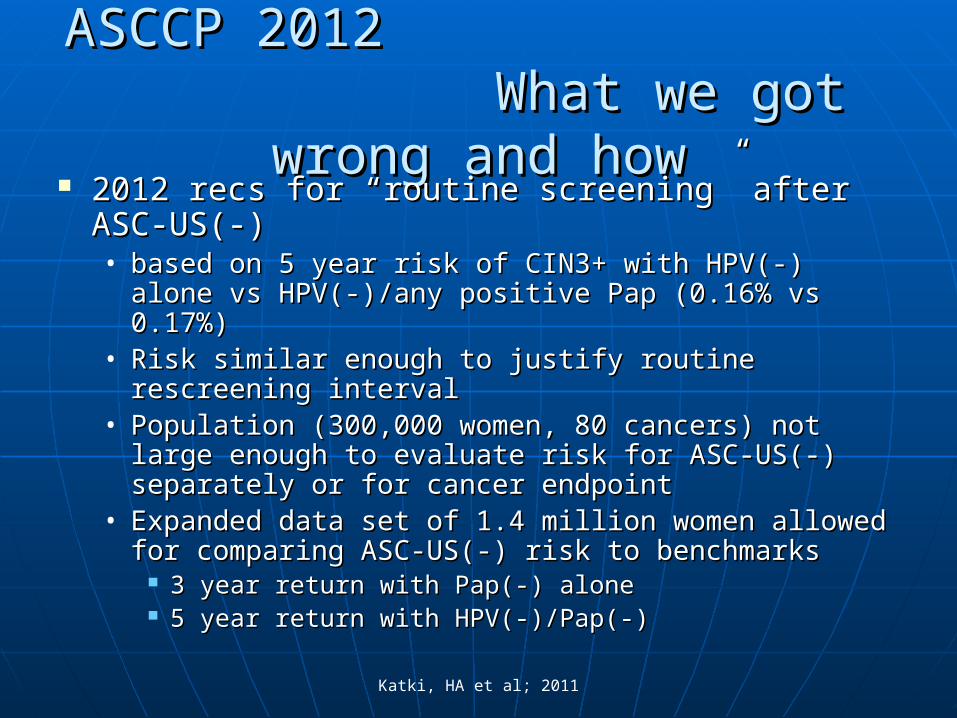
2012 recs for “routine screening” after ASC-2012 recs for “routine screening” after ASC-US(-) US(-) • based on 5 year risk of CIN3+ with HPV(-) alone vs based on 5 year risk of CIN3+ with HPV(-) alone vs
HPV(-)/any positive Pap (0.16% vs 0.17%) HPV(-)/any positive Pap (0.16% vs 0.17%) • Risk similar enough to justify routine rescreening Risk similar enough to justify routine rescreening
interval interval • Population (300,000 women, 80 cancers) not large Population (300,000 women, 80 cancers) not large
enough to evaluate risk for ASC-US(-) separately or enough to evaluate risk for ASC-US(-) separately or for cancer endpointfor cancer endpoint
• Expanded data set of 1.4 million women allowed for Expanded data set of 1.4 million women allowed for comparing ASC-US(-) risk to benchmarkscomparing ASC-US(-) risk to benchmarks
3 year return with Pap(-) alone3 year return with Pap(-) alone 5 year return with HPV(-)/Pap(-)5 year return with HPV(-)/Pap(-)
Katki, HA et al; 2011
ASCCP 2012ASCCP 2012Fix for ASC-US (-) with more dataFix for ASC-US (-) with more data
• 1.4 million women and 388 cancers instead of 300,000 1.4 million women and 388 cancers instead of 300,000 women and 80 cancers permits examination of ASC-US women and 80 cancers permits examination of ASC-US (-) risks specifically including cancer risk(-) risks specifically including cancer risk
• Risk at 5 years of CIN3+ with an ASC-US(-) is similar to Risk at 5 years of CIN3+ with an ASC-US(-) is similar to that of a negative Pap alone at 3 years (0.43% vs that of a negative Pap alone at 3 years (0.43% vs 0.26%); cancer risk at 5 years was also similar to that of 0.26%); cancer risk at 5 years was also similar to that of a negative Pap at 3 yearsa negative Pap at 3 years
• But risk of cancer at 5 years was 5 times greater with But risk of cancer at 5 years was 5 times greater with ASC-US(-) than with Pap(-)HPV(-) (0.050% vs 0.011%)ASC-US(-) than with Pap(-)HPV(-) (0.050% vs 0.011%)
• With recommendations of rescreen with Pap(-) alone at 3 With recommendations of rescreen with Pap(-) alone at 3 years the updated 2013 recommendations are for years the updated 2013 recommendations are for rescreening ASC-US(-) at 3 year intervalsrescreening ASC-US(-) at 3 year intervals
Massad LS et al. 2013.

ASCCP 2012ASCCP 2012What was totally made upWhat was totally made up
• Any recommendation for return to 5 year screening for Any recommendation for return to 5 year screening for any abnormality greater than “lesser abnormalities” any abnormality greater than “lesser abnormalities” (ASC-US, LSIL, Pap negative HPV positive times 2), (ASC-US, LSIL, Pap negative HPV positive times 2), followed by any biopsy <CIN2followed by any biopsy <CIN2
• No path to 5 year rescreening with low enough risk could No path to 5 year rescreening with low enough risk could be discerned from the available data for any abnormality be discerned from the available data for any abnormality > ASC-US, LSIL or Pap negative HPV positive OR any > ASC-US, LSIL or Pap negative HPV positive OR any biopsy >CIN1biopsy >CIN1
• Everything else is “expert opinion”Everything else is “expert opinion”
QuizQuiz
1.1. What is the clinical management for What is the clinical management for a.a. Pap negative HPV positivePap negative HPV positiveb.b. ASC-US HPV negative?ASC-US HPV negative?c.c. LSIL HPV negative?LSIL HPV negative?d.d. ASC-H HPV negative?ASC-H HPV negative?e.e. HSIL HPV negative?HSIL HPV negative?f.f. AGC-NOS HPV negative?AGC-NOS HPV negative?g.g. AGC-NEO HPV negative?AGC-NEO HPV negative?
2.2. What does it take to get back to 3 year screening after a <=CIN1 What does it take to get back to 3 year screening after a <=CIN1 colpo and colpo and a.a. Pap negative HPV positive x 2Pap negative HPV positive x 2b.b. ASC-US HPV positive?ASC-US HPV positive?c.c. LSIL HPV positive?LSIL HPV positive?d.d. ASC-H HPV negative?ASC-H HPV negative?e.e. HSIL HPV negative?HSIL HPV negative?f.f. AGC-NOS HPV negative?AGC-NOS HPV negative?g.g. AGC-NEO HPV negative?AGC-NEO HPV negative?

ASCCP Algorithms ASCCP Algorithms Mobile AppMobile App
The ASCCP App is a historic The ASCCP App is a historic step forward for teaching step forward for teaching and communicating and communicating guidelines guidelines
Can the App improveCan the App improve• Understanding of the evidence Understanding of the evidence
underlying a guideline?underlying a guideline?• Acceptance of guidelines?Acceptance of guidelines?
Could presenting the logic of Could presenting the logic of “Equal Management of Equal “Equal Management of Equal Risks” help?Risks” help?
5-yr CIN3+ risk: 0.08% 0.26% 2.6% 5.2% 25% HPV-/NILM NILM ASC-US LSIL AGC/ASC-H/HSIL Management: 5-year 3-year 1-year Colposcopy Colposcopy
Risk for this result: 6.8%

A “A “Risk BarRisk Bar”” for the App for the App
““Equal Management of Equal Risks” logic must be Equal Management of Equal Risks” logic must be obviously and immediately apparentobviously and immediately apparent
The risk calculation underlying the recommendation is The risk calculation underlying the recommendation is displayed on the continuumdisplayed on the continuum
““Why is the recommendation for HPV-negative/ASC-US Why is the recommendation for HPV-negative/ASC-US a 3-year return?”a 3-year return?”• ““Oh, the data say it’s just like a negative Pap. I get it.”Oh, the data say it’s just like a negative Pap. I get it.”
5-year CIN3+ risk: 0.08% 0.26% 2.6% 5.2% 25%
Management-defining Result: HPV-/Pap- Pap- ASC-US LSIL AGC/ASC-H/HSIL Management: 5-year return 3-year return 1-year return Colposcopy Colposcopy
Risk for this result: 0.43%

Recent Changes In National Recent Changes In National Screening Screening
RecommendationsRecommendations
- American Cancer Society and ACOG- Annual cytology or 3 year cotesting changed
to 3 year cytology or 5 year cotesting- Cotesting preferred
- US Preventive Services Task Force- 3 year cytology changed to 3 year cytology
or 5 year cotesting- No preference
Primary Screening with HPV Only Primary Screening with HPV Only FDA Approved April 2014FDA Approved April 2014
April 2014: US FDA approved a single HPV assay (Roche) for primary screening April 2014: US FDA approved a single HPV assay (Roche) for primary screening among women age 25-65 following 3 year 47,000 woman registration trial “Athena”among women age 25-65 following 3 year 47,000 woman registration trial “Athena”
““Candidate Algorithm” Primary HPV with immediate colpo for 16/18 positive and Candidate Algorithm” Primary HPV with immediate colpo for 16/18 positive and cytology triage of other HPV starting at age 25cytology triage of other HPV starting at age 25
Compared in the FDA registration trial to Compared in the FDA registration trial to
Cytology at 3 year intervals: “More sensitive and at least equally specific”Cytology at 3 year intervals: “More sensitive and at least equally specific”
Cytology at 3 year intervals 25-29 followed by cotesting at 3 year intervals 30-Cytology at 3 year intervals 25-29 followed by cotesting at 3 year intervals 30-64. One year followup of Pap negative HPV positive, and not 16/18 triage. 64. One year followup of Pap negative HPV positive, and not 16/18 triage. “More sensitive than cotesting”“More sensitive than cotesting”
Large number of CIN3 in 25-29, more than half of which were Pap negativeLarge number of CIN3 in 25-29, more than half of which were Pap negative
Significant loss to followup for Pap negative HPV positive women in the cotesting armSignificant loss to followup for Pap negative HPV positive women in the cotesting arm
ACS/ASCCP/ASCP (Saslow et al. J Low Genit Tract 2012)ACOG (Practice Bulletin # 131, Obstet Gynec, 2012)

Why Is It time For Screening Why Is It time For Screening Cytology To Go Away?Cytology To Go Away?
HPV Plus Cytology HPV Plus Cytology “Cotesting”“Cotesting”
HPV First, HPV First, p16/Ki67 Secondp16/Ki67 Second
Cytology ManualCytology Manual Both AutomatedBoth Automated
Cytology EquivocalCytology Equivocal Result DichotomousResult Dichotomous
Cytology IrreproducibleCytology Irreproducible ReproducibleReproducible
Sensitivity = Sensitivity = Sensitivity = Sensitivity =
Less SpecificLess Specific More SpecificMore Specific
More ColpoMore Colpo Less ColpoLess Colpo

ASCCP vs KPNC andASCCP vs KPNC andConduct of ColposcopyConduct of Colposcopy
The recommendations are a LOT closer than we
were in 2008. Where there are differences we are (with rare exceptions) slightly more aggressive and those differences result from one of 3 issues We concur with the literature that “colposcopic impression” is
completely irreproducible and of no clinical value. If we take someone to colposcopy we want to know what the histologic answer is – every patient, every time.
We have had access to more of our data for longer and in greater granularity
The committee writing this document felt that a different balance of risk of cancer versus risk of overscreening was more advantageous to the women members of KPNC
Interobserver Agreement in the Evaluation Interobserver Agreement in the Evaluation of Digitized Cervical Imagesof Digitized Cervical Images
ConclusionsConclusions ““The agreement among the whole group of The agreement among the whole group of
evaluators was poor.”evaluators was poor.” ““Colposcopic diagnosis using static images is Colposcopic diagnosis using static images is
poorly reproducible poorly reproducible andand mightmight reflect reflect similar problems in clinical practice.”similar problems in clinical practice.”
Jeronimo J et al for the NIH-ASCCP Research Group, Obstet Gynecol 2007;110:833


I
II
IV
III
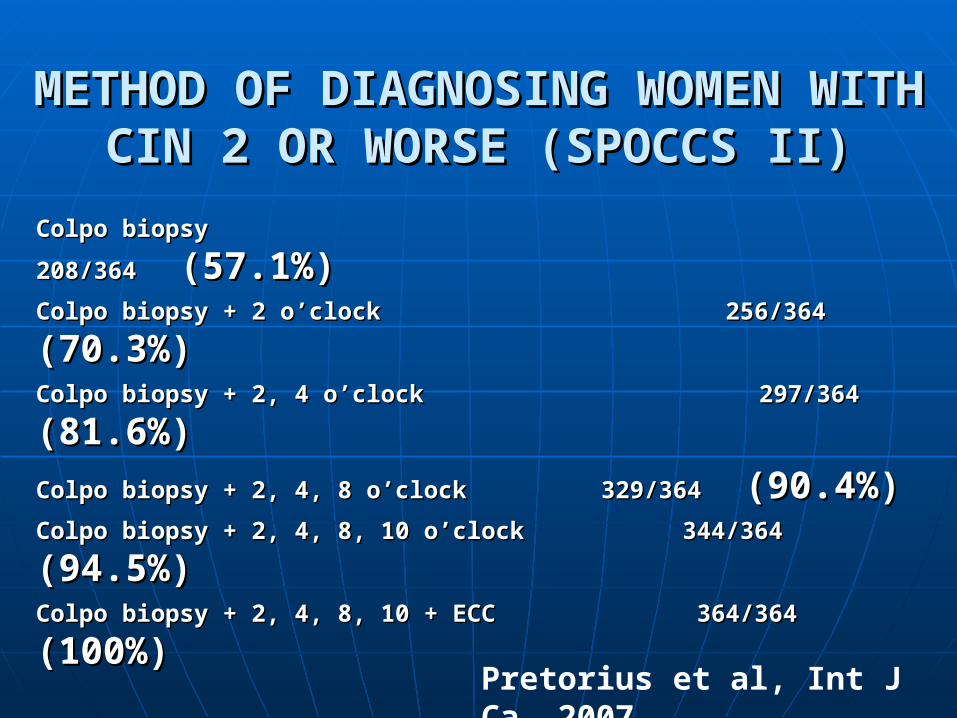
METHOD OF DIAGNOSING WOMEN METHOD OF DIAGNOSING WOMEN WITH CIN 2 OR WORSE (SPOCCS II)WITH CIN 2 OR WORSE (SPOCCS II)
Colpo biopsy 208/364 Colpo biopsy 208/364 (57.1%)(57.1%)
Colpo biopsy + 2 o’clock 256/364 Colpo biopsy + 2 o’clock 256/364 (70.3%)(70.3%)
Colpo biopsy + 2, 4 o’clockColpo biopsy + 2, 4 o’clock 297/364 297/364 (81.6%)(81.6%)
Colpo biopsy + 2, 4, 8 o’clockColpo biopsy + 2, 4, 8 o’clock 329/364 329/364 (90.4%)(90.4%)
Colpo biopsy + 2, 4, 8, 10 o’clock 344/364 Colpo biopsy + 2, 4, 8, 10 o’clock 344/364 (94.5%)(94.5%)
Colpo biopsy + 2, 4, 8, 10 + ECC 364/364 Colpo biopsy + 2, 4, 8, 10 + ECC 364/364 (100%)(100%)
57.1% vs. 70.3% vs. 81.6% vs. 90.9% vs. 94.5% vs. 100%, Chi-57.1% vs. 70.3% vs. 81.6% vs. 90.9% vs. 94.5% vs. 100%, Chi-Square = 326, df=5, P<.001Square = 326, df=5, P<.001
Pretorius et al, Int J Ca, 2007

The accuracy of colposcopic biopsy: analyses from the placebo arm of the Gardasil clinical trials
Stoler MH et al, Int J Cancer, 2010
NegNeg CIN1CIN1 CIN2CIN2 CIN3/CIN3/AISAIS
NegNeg 195195 8282 2929 5454
CIN1CIN1 1212 6565 2828 1717
CIN2CIN2 11 22 2121 2525
CIN3/CIN3/AISAIS
77 44 33 4949
TotalTotal 215215 153153 8181 145145
Colpo Directed Biopsy
LEEP Histology
CIN2+ called CIN1 or Neg 128/226 (57%)CIN3/AIS called CIN1 or Neg 71/145 (49%)
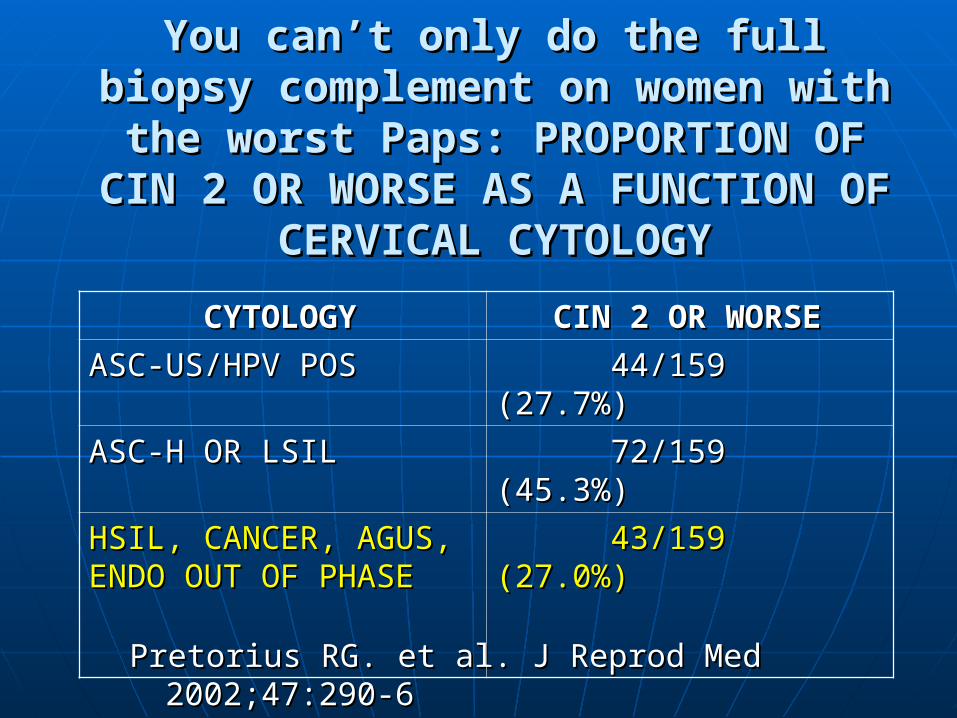
You can’t only do the full biopsy You can’t only do the full biopsy complement on women with the worst complement on women with the worst
Paps: PROPORTION OF CIN 2 OR Paps: PROPORTION OF CIN 2 OR WORSE AS A FUNCTION OF CERVICAL WORSE AS A FUNCTION OF CERVICAL
CYTOLOGYCYTOLOGY
Pretorius RG. et al. J Reprod Med 2002;47:290-6Pretorius RG. et al. J Reprod Med 2002;47:290-6
CYTOLOGYCYTOLOGY CIN 2 OR WORSECIN 2 OR WORSE
ASC-US/HPV POSASC-US/HPV POS 44/159 (27.7%)44/159 (27.7%)
ASC-H OR LSILASC-H OR LSIL 72/159 (45.3%)72/159 (45.3%)
HSIL, CANCER, AGUS, HSIL, CANCER, AGUS, ENDO OUT OF PHASEENDO OUT OF PHASE
43/159 (27.0%)43/159 (27.0%)
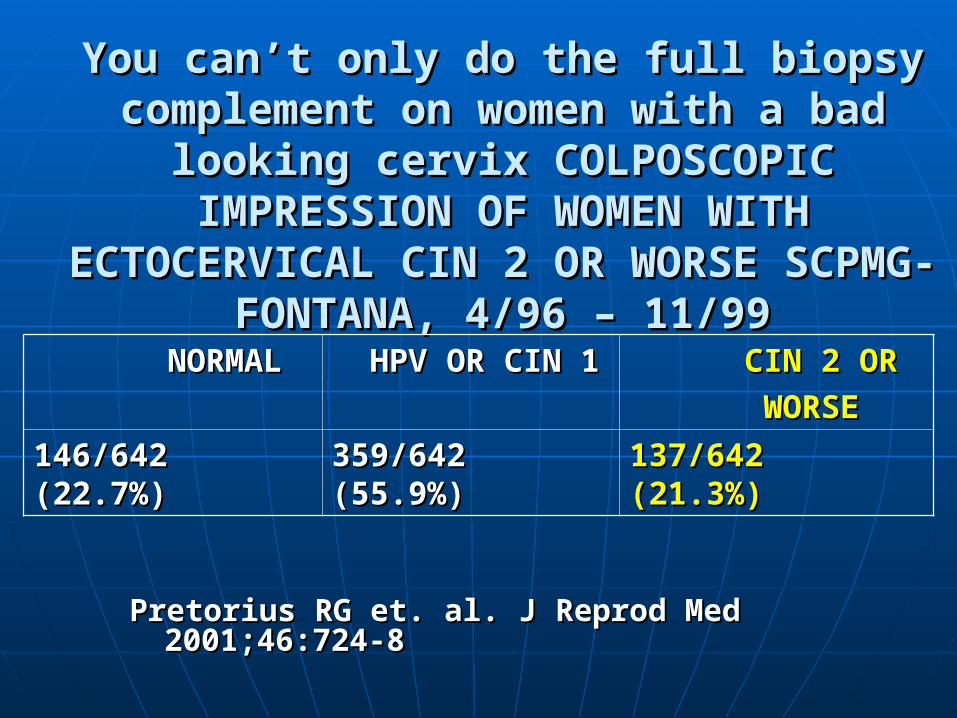
You can’t only do the full biopsy You can’t only do the full biopsy complement on women with a bad looking complement on women with a bad looking
cervix COLPOSCOPIC IMPRESSION OF cervix COLPOSCOPIC IMPRESSION OF WOMEN WITH ECTOCERVICAL CIN 2 OR WOMEN WITH ECTOCERVICAL CIN 2 OR WORSE SCPMG-FONTANA, 4/96 – 11/99WORSE SCPMG-FONTANA, 4/96 – 11/99
Pretorius RG et. al. J Reprod Med Pretorius RG et. al. J Reprod Med 2001;46:724-82001;46:724-8
NORMALNORMAL HPV OR CIN 1HPV OR CIN 1 CIN 2 ORCIN 2 OR
WORSEWORSE
146/642 146/642 (22.7%)(22.7%)
359/642 359/642 (55.9%)(55.9%)
137/642 137/642 (21.3%)(21.3%)

0
0.05
0.1
0.15
0.2
0.25
0 1 2 3 4 5 6
Biopsies in addition to colpo-directed biopsy
Yie
ld o
f C
IN 3
or
Can
cer
per
co
lpo
sco
py
Doc 1, r=.959, p=.0025
Doc 2, r=.921, p=.009
Doc 3, r=.958, p=.003
Doc 4, r=.995, p<.001
Doc 5, r=.645, p=.17
Doc 6, r=.983, p<.001
Doc 7, r=.943, p=.005
Pretorius RG et al, JLGTD, 2011
Changes for 2012Changes for 2012
Age 21-24: No colposcopy for ASC-US and LSIL• KPNC publication drives the national recommendations• No colpo for ASC HPV positive means ASC-US triage not needed for
ages 21-24• Goal: reduce screening now in a population that does not benefit;
eventually start screening at 25 No colposcopy for LSIL HPV negative at any age
• KPNC publication drives national recommendations• Goal: save colposcopy for women more likely to benefit
No colposcopy for a single Pap negative HPV positive even if previous abnormal• KPSC unpublished data • Clinical history can’t identify women at risk unless their previous
abnormality was not evaluated• Goal: abandon an unsuccessful triage strategy; save colposcopy
for women more likely to benefit
Changes for 2012Changes for 2012
No more annual returns for ASC-US HPV negative• KPNC data drives the national recommendations (again)KPNC data drives the national recommendations (again)• Note that risk does not permit a 5 year return!Note that risk does not permit a 5 year return!
• For access this is For access this is HUGEHUGE 300,000 Paps/year @4% ASC-US = 12,000. 2/3 HPV 300,000 Paps/year @4% ASC-US = 12,000. 2/3 HPV
negative means that there are 8,000 followup negative means that there are 8,000 followup appointments in a year that we are no longer going appointments in a year that we are no longer going to do, plus all of the followup that those tests would to do, plus all of the followup that those tests would generategenerate
• We redid the cancer risks ourselves to make 100% sure We redid the cancer risks ourselves to make 100% sure that this was OKthat this was OK
ECC CIN1 no longer mandates excision• Dr. Littell drives the national recommendations (again)Dr. Littell drives the national recommendations (again)
Cotesting 25-65: RationaleCotesting 25-65: Rationale
1.1. There is invasive cervical cancer in women age 25-29. Risk for women age 25-There is invasive cervical cancer in women age 25-29. Risk for women age 25-2929 in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of 5/100,000/year. 5/100,000/year.
2.2. Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in the late 20sthe late 20s
3.3. To make any progress against adenocarcinoma and adenosquamous carcinoma, To make any progress against adenocarcinoma and adenosquamous carcinoma, HPV testing will have to be included in screening.HPV testing will have to be included in screening.
4.4. Simplification of Guidelines aids complianceSimplification of Guidelines aids compliance
5.5. All of the current management recommendations for abnormals are 21-24 and All of the current management recommendations for abnormals are 21-24 and 25+, not 21-29 and 30+25+, not 21-29 and 30+
6.6. Screening is going to stop under 25Screening is going to stop under 25
7.7. ASC-US triage “store and sort” will no longer be necessaryASC-US triage “store and sort” will no longer be necessary
8.8. Cotesting permits enhanced cytology QCCotesting permits enhanced cytology QC
9.9. Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus 10.1% for women 25-29.10.1% for women 25-29.
10.10. Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not lumped together with CIN3 as “histologic HSIL”lumped together with CIN3 as “histologic HSIL”

KP Regional Lab 2012 CIN3 By Age
AGE PATIENTS CIN III % CIN III
21-24 30,805 1 0.003%
25-29 40,045 191 0.477%
30-34 42,746 222 0.519%
35-39 38,695 110 0.284%
0
50
100
150
200
250
21-24 25-29 30-34 35-39
CIN3
Kinney et al, IPV Abstract, 2014

ATHENA 25-29 CIN3+
0
5
10
15
20
25
30
35
40
21-24 25-59 30-39 40-49 50+
% of all CIN3+ diagnosed
Wright, AJOG, 2011
0
10
20
30
40
50
60
25-29 30-39 40-49 50+
% of all CIN3+ Pap Neg HPV Pos
Huh, Abstract,IPV, 2011
Cotesting 25-65: RationaleCotesting 25-65: Rationale
1.1. There is invasive cervical cancer in women age 25-29. Risk for women age 25-There is invasive cervical cancer in women age 25-29. Risk for women age 25-2929 in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of 5/100,000/year. 5/100,000/year.
2.2. Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in the late 20sthe late 20s
3.3. To make any progress against adenocarcinoma and adenosquamous carcinoma, To make any progress against adenocarcinoma and adenosquamous carcinoma, HPV testing will have to be included in screening.HPV testing will have to be included in screening.
4.4. Simplification of Guidelines aids complianceSimplification of Guidelines aids compliance
5.5. All of the current management recommendations for abnormals are 21-24 and All of the current management recommendations for abnormals are 21-24 and 25+, not 21-29 and 30+25+, not 21-29 and 30+
6.6. Screening is going to stop under 25Screening is going to stop under 25
7.7. ASC-US triage “store and sort” will no longer be necessaryASC-US triage “store and sort” will no longer be necessary
8.8. Cotesting permits enhanced cytology QCCotesting permits enhanced cytology QC
9.9. Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus 10.1% for women 25-29.10.1% for women 25-29.
10.10. Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not lumped together with CIN3 as “histologic HSIL”lumped together with CIN3 as “histologic HSIL”

Cotest Cotest ResultResult
SquamousSquamous NonsquamousNonsquamous Total Number Total Number of Womenof Women
Cotest +Cotest + 5050 46 (72%)46 (72%) 96 (71%)96 (71%)
Pap + Pap + HPV-HPV-
99 2 (3%)2 (3%) 1111
Pap- Pap- HPV+HPV+
1414 28 (44%)28 (44%) 4242
Pap+ Pap+ HPV+HPV+
2727 16 (25%)16 (25%) 4343
Cotest -Cotest - 2222 18 (28%)18 (28%) 40 (29%)40 (29%)
TotalTotal 7272 6464 136136
Cancer Antecedents: 136 Women Cotested 6 to 42 Months Prior to Diagnosis 2003-2009
Dinkelspiel et al, WAGO Abstract, 2011

AIS Antecedents: 172 Women Cotested 6 to 42 Months Prior to Diagnosis 2003-2010
Dinkelspiel et al, SGO Abstract, 2012
Pap neg HPV pos is by far the most important screening diagnosis prior to AIS
Screening Results
First cotest 6-42 Months Prior to AIS
Cotests +
Pap+ HPV- 8 (4.7%)
Pap- HPV+ 91 (52.9%) Pap+ HPV+ 53 (30.8%)
Cotests - 20 (11.6%)
Total 172

CIN 3/AIS by year in facilities served CIN 3/AIS by year in facilities served continuously by the Regional Labcontinuously by the Regional Lab
Continuous FacilitiesContinuous Facilities
2003-2012 2003-2012 CIN3CIN3 AISAIS
20032003 186186 1010
20042004 226226 2121
20052005 205205 2727
20062006 319319 4646
20072007 397397 5959
20082008 425425 5757
20092009 457457 6868
20102010 332332 6464
20112011 394394 5555
20122012 364364 6565
KPNC Unpublished, 2013

Cotesting 25-65: RationaleCotesting 25-65: Rationale
1.1. There is invasive cervical cancer in women age 25-29. Risk for women age 25-There is invasive cervical cancer in women age 25-29. Risk for women age 25-2929 in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of 5/100,000/year. 5/100,000/year.
2.2. Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in the late 20sthe late 20s
3.3. To make any progress against adenocarcinoma and adenosquamous carcinoma, To make any progress against adenocarcinoma and adenosquamous carcinoma, HPV testing will have to be included in screening.HPV testing will have to be included in screening.
4.4. Simplification of Guidelines aids complianceSimplification of Guidelines aids compliance
5.5. All of the current management recommendations for abnormals are 21-24 and All of the current management recommendations for abnormals are 21-24 and 25+, not 21-29 and 30+25+, not 21-29 and 30+
6.6. Screening is going to stop under 25Screening is going to stop under 25
7.7. ASC-US triage “store and sort” will no longer be necessaryASC-US triage “store and sort” will no longer be necessary
8.8. Cotesting permits enhanced cytology QCCotesting permits enhanced cytology QC
9.9. Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus 10.1% for women 25-29.10.1% for women 25-29.
10.10. Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not lumped together with CIN3 as “histologic HSIL”lumped together with CIN3 as “histologic HSIL”
0.010%
0.012%
0.014%
0.016%
0.018%
0.020%
0.022%
0.024%
0.026%
0.028%
0.030%
2008 2009 2010 2011 2012
REG LAB CA % FAC LAB CA %
Cancer Rate Trend Among Previously Screened Women - Effects of “screening with prejudice” and QC review of all Pap-HPV+
KPNC 2014, Unpublished
Exclusions: Unscreened women and women screened in both Regional and Facility Labs

Cotesting 25-65: RationaleCotesting 25-65: Rationale
1.1. There is invasive cervical cancer in women age 25-29. Risk for women age 25-There is invasive cervical cancer in women age 25-29. Risk for women age 25-2929 in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of in the SEER registry is 5.1/100,000/year, similar to the overall risk in KPNC of 5/100,000/year. 5/100,000/year.
2.2. Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in Detection of CIN3 and AIS are the goals of screening. CIN3 incidence is BIG in the late 20sthe late 20s
3.3. To make any progress against adenocarcinoma and adenosquamous carcinoma, To make any progress against adenocarcinoma and adenosquamous carcinoma, HPV testing will have to be included in screening.HPV testing will have to be included in screening.
4.4. Simplification of Guidelines aids complianceSimplification of Guidelines aids compliance
5.5. All of the current management recommendations for abnormals are 21-24 and All of the current management recommendations for abnormals are 21-24 and 25+, not 21-29 and 30+25+, not 21-29 and 30+
6.6. Screening is going to stop under 25Screening is going to stop under 25
7.7. ASC-US triage “store and sort” will no longer be necessaryASC-US triage “store and sort” will no longer be necessary
8.8. Cotesting permits enhanced cytology QCCotesting permits enhanced cytology QC
9.9. Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus Cytology negative HPV positive rates in women 30-34 in KPNC are 6.1%, versus 10.1% for women 25-29.10.1% for women 25-29.
10.10. Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not Cotesting 25-29 will not lead to overuse of LEEP if CIN2 and CIN2/3 are not lumped together with CIN3 as “histologic HSIL”lumped together with CIN3 as “histologic HSIL”

Risk of Untreated CIN2 and CIN2/3Risk of Untreated CIN2 and CIN2/3KPNC 2003-2010KPNC 2003-2010
• 1,659 CIN2 and CIN2/3 age 21-29 followed with 1,659 CIN2 and CIN2/3 age 21-29 followed with
cytology without excision for an average of 25(CIN2) cytology without excision for an average of 25(CIN2) to 30 (CIN2/3) months (minimum 18), with an to 30 (CIN2/3) months (minimum 18), with an average of 3.3-3.6 Paps or biopsies during followupaverage of 3.3-3.6 Paps or biopsies during followup
• Risk of invasive cancer was – predictably - Risk of invasive cancer was – predictably - proportional to grade and age, but low in all groupsproportional to grade and age, but low in all groups• 21-24 year old21-24 year old
CIN2: 0/559(0%; CI 0.0-0.53%)CIN2: 0/559(0%; CI 0.0-0.53%) CIN2/3: 0/170(0%; CI 0.0-1.7%)CIN2/3: 0/170(0%; CI 0.0-1.7%)
• 25-29 year old25-29 year old CIN2: 1/667(0.15%; CI 0.006%-0.71%)CIN2: 1/667(0.15%; CI 0.006%-0.71%) CIN2/3: 1/263(0.38%; CI 0.016%-1.8%)CIN2/3: 1/263(0.38%; CI 0.016%-1.8%)
Ladwig-Scott et al, WAGO Abstract, 2013
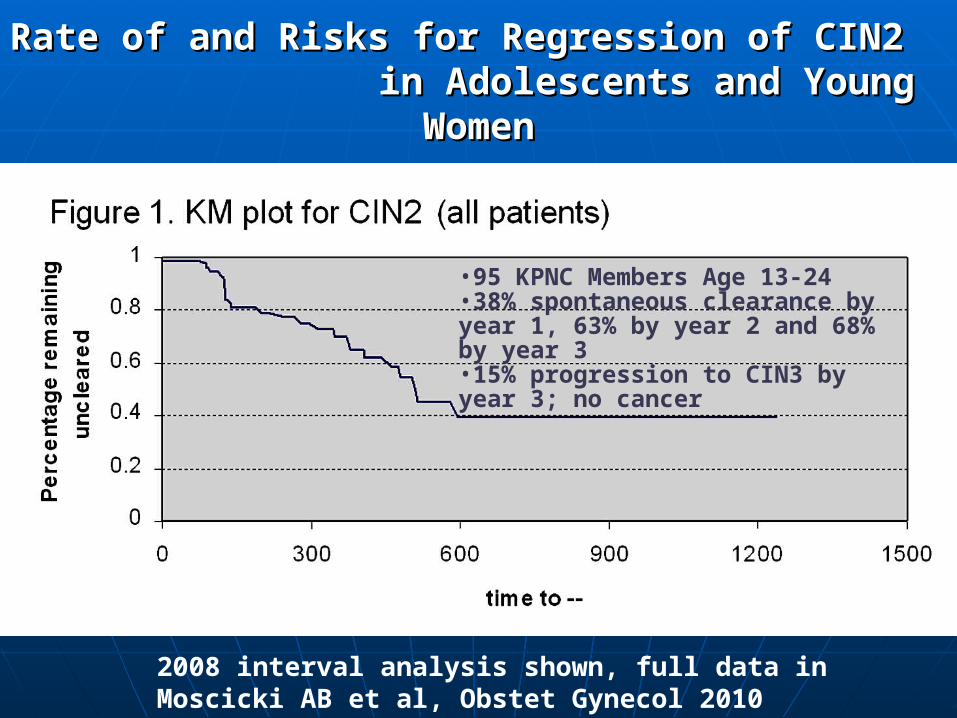
Rate of and Risks for Regression of CIN2 Rate of and Risks for Regression of CIN2 in Adolescents and Young Womenin Adolescents and Young Women
2008 interval analysis shown, full data in Moscicki AB et al, Obstet Gynecol 2010 December; 116(6):1373-1380
•95 KPNC Members Age 13-24•38% spontaneous clearance by year 1, 63% by year 2 and 68% by year 3•15% progression to CIN3 by year 3; no cancer

TIME TO REGRESSION OF CIN 2 BY TIME TO REGRESSION OF CIN 2 BY PATHOLOGIST CONCORDANCEPATHOLOGIST CONCORDANCE
Moscicki AB, Obstet Gynecol 2010 KPNC Members Ages 13-25

The Lower Anogenital Squamous The Lower Anogenital Squamous Terminology (LAST) ProjectTerminology (LAST) Project
“Consensus” conference held in March of 2012 Recommended that histology be described as
LSIL = CIN1 HSIL = CIN2, CIN2/3 and CIN3 p16 is to be used to assign CIN2 to LSIL or HSIL. “This will result in
increased specificity of diagnosing HSIL.” NO data concerning risk for the new diagnoses was presented
Use of –SIL terminology alone was voted down. Revised motion permits the use of -IN terminology in
parentheses passed (barely) “during the transition” In place of information concerning risk, patient management is
to go forward under the new system based on “clinical judgment”, placing the risk of adverse outcomes squarely on the clinician. (Waxman et al Obstet Gynecol)
Diagnostic irreproducibility will no doubt be reduced. Whom does this benefit?
Waxman et al, Obstet Gynecol 2012;120:1465-71

SummarySummary
1.1. Cancer incidence can be decreased and outcomes can be improvedCancer incidence can be decreased and outcomes can be improved2.2. Like heart disease, understanding the causes is not enoughLike heart disease, understanding the causes is not enough3.3. It takes time and resources and will and focus and a system approachIt takes time and resources and will and focus and a system approach4.4. For cervical cancer prevention in unvaccinated women the system For cervical cancer prevention in unvaccinated women the system
includesincludesa)a) Increasing screening rates with outreach and the call center and inreach and Increasing screening rates with outreach and the call center and inreach and
tracking rates by facilitytracking rates by facilityb)b) Inclusion of HPV testing in screeningInclusion of HPV testing in screeningc)c) ““Screening with prejudice” if you are doing cotesting – show the techs the HPV Screening with prejudice” if you are doing cotesting – show the techs the HPV
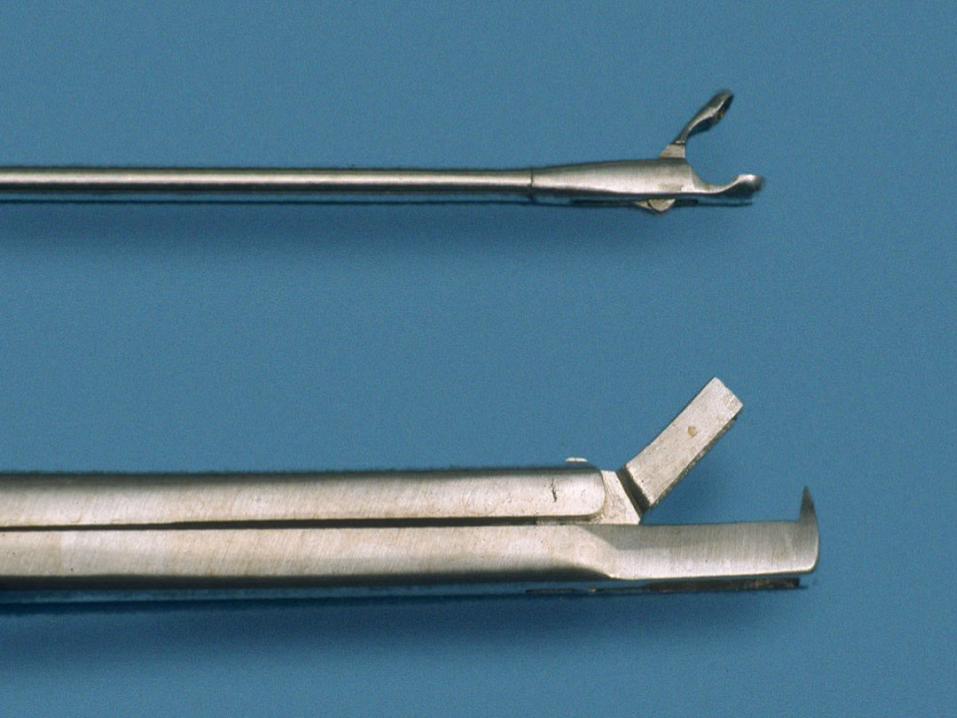
and Focal Point resultsand Focal Point resultsd)d) Tracking of abnormalsTracking of abnormalse)e) Improved colposcopy sensitivity – 4 quadrant biopsy plus ECC with 2mm Improved colposcopy sensitivity – 4 quadrant biopsy plus ECC with 2mm
punchespunchesf)f) Followup of women with abnormal cytology and histology based on data about Followup of women with abnormal cytology and histology based on data about
risk over the term until the next screenrisk over the term until the next screeng)g) Comprehensible simple dichotomous reproducible test results, not “could be Comprehensible simple dichotomous reproducible test results, not “could be
might be maybe” and variants thereonmight be maybe” and variants thereonh)h) Standards of screening and followup of abnormals that deliver cancer Standards of screening and followup of abnormals that deliver cancer
protection equivalent to annual cytology protection equivalent to annual cytology
Related Documents