19 October 1974 S.A. MEDICAL JOURNAL 2139 Asphyxia Neonatorum - Assessment of the Infant at Birth C. D. MOLTENO, A. F. MALAN, H. DE V. HEESE SUMMARY Asphyxia neonatorum is defined as failure of a newborn infant to establish sustained respiration after its com- plete delivery. In 206 asphyxiated infants reviewed, details of the Apgar scores, to susta:ned respiration and resuscitation required, were documented. The value of each of these observations, as well as that of the heart rate and acid-base status birth, is assessed. From the findings definite for the routine assessment of the infant at birth are made. S. Afr. Med. J., 48, 2139 (1974). The term asphyxia is derived from the Greek word meaning 'pulseless' «(I = negative + sphyxis = pulse). Since the presence of a heartbeat is often the only sign of life in a depressed infant at birth, the literal application of the term is not appropriate. Physiologically, the condition of hypoxia associated with hypercapnia is implied. As a working definition of asphyxia neonatorum, failure of a newborn infant to establish sustained respiration after its com- plete delivery is recommended, because it may be applied in the delivery room. An accurate clinical assessment is fundamental to the efficient management of the asphyxiated infant. Tot only is it important in resuscitation, but careful factual docu- mentation of conditions at birth is essential in the future developmental assessment of the child. To be practical, the methods used must not be beyond the score of routine practice. The purpose of this article is to discuss these methods; and to make recommendations regarding their use. PATIENTS AND MEmODS All deliveries from 1 April 1971 to 31 March 1972 in the Groote Schuur Maternity Hospital were included in a prospective study. A carefully recorded Apgar score' at 1 and 5 minutes; the time to sustained respiration (TSR), and details of the resuscitation carried out, were documented on each infant. The TSR was taken as the time in minutes between delivery and when the infant begins to maintain reasonably regular and adequate ven- tilatory activity without recurrent stimulation.' Asphyxia Department of Paedia rics and Child Health, University of Cape Town C. D. 10LTENO, F.e.p. (S.A.) "Ll\lED. (PAED.), D.C.H. A. F. MALA:"!, M.MED. (P.. U:D.), M.D., DIP.l\IID.c.o.G. H. DE V. HEESE, B.SC., M.D., F.R.C.P., D.C.H. Date r"""ived: 10 July 1974. neonatorum was diagnosed if the Apgar score at 1 minute was 0 - 3, or if assisted respiration was needed in the first 10 minutes of life. Each asphyxiated infant was examined neurologically by the methods prescribed by Prechtl and Beintema. ' Intact neonatal survival was considered when an infant survived the neonatal period without evidence of gross neurological abnormality. In selected patients continuous heart rate tracings were obtained with a cardiotachograph, commencing within 30 seconds of birth. One hour after delivery, all babies had blood taken for acid-base measurements by heel stab after warming, precautions being taken to ensure the correct collection of samples: and to prevent crying before and during the procedure. Further samples were taken at inter- vals during the first 24 hours. In all cases acid-base values were determined by the Astrup method." Statistical methods employed in the study were the comparison of sample means by the unpaired t-test, and the chi-square test. RESULTS During the period of study 206 (6,6%) of the total live births (3 167) suffered from asphyxia neonatorum, as judged by the criteria mentioned above. The distribution of 1- and 5-minute Apgar scores is given in Figs 1 and 2. The 13 infants with a I-minute score of greater than 3 were included because they required positive pressure ventilation in the first 10 minutes of life. Exactly half of the asphyxiated infants had a score of 1 - 6 by 5 minutes. From Fig. 3 it can be seen that approximately a third of the infants established sustained respiration by 5 minJltes, and two-thirds by 10 minutes. Thirteen infants took longer than 20 minutes to start breathing sponta- neously. There is a significant correlation between intact neonatal survival as defined above, and TSR, and a very strong correlation between intact neonatal survival and the 5-minute Apgar score (Tables I and II). During resuscitation, those infants who did not start breathing after clearing of the airway and application of peripheral stimulation, were intubated and given positive pressure ventilation. This form of treatment was necessary in 140 of the 206 asphyxiated infants, including all 10 who were neurologically abnormal, and 20 of the 27 who died in the neonatal period. Fig. 4 compares the means of the heart rates of asphyxi- ated infants in minutes after the establishment of sustained respiration with those of infants who breathed immediately after birth. The asphyxiated group had significantly lower heart rates at 1, 2 and 3 minutes, but not at 4 minutes after the commencement of sustained respiration. In addi- tion, the heart rate at I minute after birth, prior to respi-

4.5 Asphyxia Neonatorum - Assessment of the Infant Birth. c.d. Molteno, A.f. Malan and h. de v. h
Dec 18, 2015
nn
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
19 October 1974 S.A. MEDICAL JOURNAL 2139
Asphyxia Neonatorum - Assessment of theInfant at Birth
C. D. MOLTENO, A. F. MALAN, H. DE V. HEESE
SUMMARY
Asphyxia neonatorum is defined as failure of a newborninfant to establish sustained respiration after its com-plete delivery. In 206 asphyxiated infants reviewed, detailsof the Apgar scores, tim~ to susta:ned respiration andresuscitation required, were documented. The value ofeach of these observations, as well as that of the heartrate and acid-base status aft~r birth, is assessed. Fromthe findings definite recomm~ndat[ons for the routineassessment of the infant at birth are made.
S. Afr. Med. J., 48, 2139 (1974).
The term asphyxia is derived from the Greek word meaning'pulseless' (I = negative + sphyxis = pulse). Since thepresence of a heartbeat is often the only sign of life in adepressed infant at birth, the literal application of the termis not appropriate. Physiologically, the condition of hypoxiaassociated with hypercapnia is implied. As a workingdefinition of asphyxia neonatorum, failure of a newborninfant to establish sustained respiration after its com-plete delivery is recommended, because it may be appliedin the delivery room.
An accurate clinical assessment is fundamental to theefficient management of the asphyxiated infant. Tot onlyis it important in resuscitation, but careful factual docu-mentation of conditions at birth is essential in the futuredevelopmental assessment of the child. To be practical, themethods used must not be beyond the score of routinepractice. The purpose of this article is to discuss thesemethods; and to make recommendations regarding theiruse.
PATIENTS AND MEmODS
All deliveries from 1 April 1971 to 31 March 1972 in theGroote Schuur Maternity Hospital were included in aprospective study. A carefully recorded Apgar score'at 1 and 5 minutes; the time to sustained respiration(TSR), and details of the resuscitation carried out, weredocumented on each infant. The TSR was taken as thetime in minutes between delivery and when the infantbegins to maintain reasonably regular and adequate ven-tilatory activity without recurrent stimulation.' Asphyxia
Department of Paedia rics and Child Health, University ofCape Town
C. D. 10LTENO, F.e.p. (S.A.) "Ll\lED. (PAED.), D.C.H.A. F. MALA:"!, M.MED. (P..U:D.), M.D., DIP.l\IID.c.o.G.H. DE V. HEESE, B.SC., M.D., F.R.C.P., D.C.H.Date r"""ived: 10 July 1974.
neonatorum was diagnosed if the Apgar score at 1 minutewas 0 - 3, or if assisted respiration was needed in the first 10minutes of life. Each asphyxiated infant was examinedneurologically by the methods prescribed by Prechtl andBeintema.' Intact neonatal survival was considered whenan infant survived the neonatal period without evidenceof gross neurological abnormality.
In selected patients continuous heart rate tracings wereobtained with a cardiotachograph, commencing within 30seconds of birth. One hour after delivery, all babies hadblood taken for acid-base measurements by heel stab afterwarming, precautions being taken to ensure the correctcollection of samples: and to prevent crying before andduring the procedure. Further samples were taken at inter-vals during the first 24 hours. In all cases acid-base valueswere determined by the Astrup method."
Statistical methods employed in the study were thecomparison of sample means by the unpaired t-test, andthe chi-square test.
RESULTS
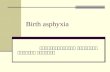
During the period of study 206 (6,6%) of the total livebirths (3 167) suffered from asphyxia neonatorum, asjudged by the criteria mentioned above. The distributionof 1- and 5-minute Apgar scores is given in Figs 1 and2. The 13 infants with a I-minute score of greater than 3were included because they required positive pressureventilation in the first 10 minutes of life. Exactly half ofthe asphyxiated infants had a score of 1 - 6 by 5 minutes.From Fig. 3 it can be seen that approximately a thirdof the infants established sustained respiration by 5minJltes, and two-thirds by 10 minutes. Thirteen infantstook longer than 20 minutes to start breathing sponta-neously. There is a significant correlation between intactneonatal survival as defined above, and TSR, and a verystrong correlation between intact neonatal survival and the5-minute Apgar score (Tables I and II).
During resuscitation, those infants who did not startbreathing after clearing of the airway and application ofperipheral stimulation, were intubated and given positivepressure ventilation. This form of treatment was necessaryin 140 of the 206 asphyxiated infants, including all 10 whowere neurologically abnormal, and 20 of the 27 who diedin the neonatal period.
Fig. 4 compares the means of the heart rates of asphyxi-ated infants in minutes after the establishment of sustainedrespiration with those of infants who breathed immediatelyafter birth. The asphyxiated group had significantly lowerheart rates at 1, 2 and 3 minutes, but not at 4 minutesafter the commencement of sustained respiration. In addi-tion, the heart rate at I minute after birth, prior to respi-
-
2140 S.-A. MEDIESE TYDSKRIF 19 Oktober 1974
-
ASPHYXIA NEONATORUMTime to Sustained Respiration
11') 0- ;! ~ +V I I 011') S2 :!! N
minuteslS.R.
60
70
80
50
'"..
'"0u 40-0g
3D-
20-,........
,........
10
Fig. 3. Time to sustained respiration.
Time to sustained respiration (min)
therefore, that in apnoeic infants the heart rate falls toapproximately 60 beats/minute. With the onset of respira-tion it then rapidly rises to a level of over 100 beats/minute. Thereafter, over a period of roughly 4 minutes,it approximates with that of an infant vigorous at birth.
TABLE I. INTACT SURVIVAL AND TIME TO SUSTAINEDRESPIRATION2 3 4 5 6 7 8 9 10
5 min Apgor Score
-r--
0
-
r--
.-
r-
--
0- -.-
40
3
i3 20'0cic
ASPHYXIA NEONATORUM
70--
-
60 r-
50
40
..
S0u 30'0
~20
10
I 11 InI r-"""'O ,-0 2 3 -4 5 6 7 8 9 10
I 1 min Apgar ScoreI
11Fig. 1. Apgar score at 1 minute.
IASPHYXIA NEONATORUM
Fig. 2. Apgar score at 5 minutes.
-
19 October 1974 S.A. MEDICAL JOURNAL 2141
HEART RATE PATTERNSMean ! one standard deviation
tfNS
Apgar 9 -10 Asphyxia after onset of resp. Prior to first brP.Olh~ Apnoea after breathing
20 -20 9 -10 Apgor
0-3 Apgor
ACID BASE STATUSAT 1 HOUR
Vaginal deliYef'"ie1
pH PC~ BE
7,40 0
7, 90
.
7, -5 ...
7,
10 0
i:~ 0oc
NS
II
p
-
2142 S.-A. MEDIESE TYDSKRIF 19 Oktober 1974
IdI
ACID BASE STATUSAT 1 HOUR
Caesarean section deliveries
pH PC02 BE7. 0
7.35.S. .0 .0
7.'Jt) 80 0 -5 .. 0
.~7.25 8
7.20 -10.0
...8
87,15 50 0
.0
7.10 0 40 ~. -15
.0
7, 30
fetal pH, and negative base excess.'"' The changes are alsoreflected in maternal arterial and umbilical vein samplesat birth." Measuring these parameters, however, is notpossible as a routine, since only a small percentage ofnewborn infants suffer from asphyxia neonatorum. Fromthis study, it is evident that changes in acid-base statuspersist for at least an hour after birth, and that the mostmarked differences between asphyxiated and normal infantscan be seen in the base excess readings. It can be concludedthat a negative base excess reading during the first hourgives an indication of the amount of hypoxia suffered bythe infant during the whole birth process.
The importance of the heart rate in the newborn hasbeen stressed in the literature." The results of this studyshow that in an apnoeic infant the heart rate rapidly fallsto a level of approximately 60 beats/minute. To judge fromanimal experiments, the rate would presumably remain atthis level, unless resuscitation took place, until cardiac gly-cogen reserves became exhausted." With oxygenation ofthe myocardium, the heart rate rises rapidly to a level ofover 100 beats/minute. Thereafter, over a period of a fewminutes, it rises further to reach normal levels. The heartrate is, therefore, of importance, but recording a figure ata particular stage fails to add to information gained fromthe Apgar score itself. Continual assessment of the heartbeat does, however, give a valuable guide to the success ofthe resuscitative measures applied.
7.00 20 CONCLUSIONS
6.95
6.90 -25
9-10 Apgaro 0- 3 Apgor
Fig. 6. Acid-base status at 1hour - Caesarean section.
analeptic drugs can stimulate gasping, whereas in secon-dary apnoea, only intermittent positive pressure ventila-tion, and intravenous correction of the acidosis, can dothis. Asphyxia of the fetal monkey beyond the last gaspleads to permanent symmetrical and bilateral damage inthe brain stem nuclei." It is therefore important to recordwhich methods were required during resuscitation. In addi-tion, the Apgar score and TSR may be influenced by thetiming of these. In this study 20 of the 27 neonatal deaths,and all of those found to be neurologically abnormalrequired endotracheal intubation and positive pressureventilation.
It has long been known that the duration and severityof asphyxia are reflected in acid-base changes." Hypoxiagives rise to an accumulation of lactic acid, which resultsin i\ metabolic acidosis.'4 Intra-uterine hypoxia is accom-panied by an increasing difference between maternal and
In addition to the usual recording of the Apgar score at1 and 5 minutes and the 'resuscitation carried out, it isrecommended that the time to sustained respiration andbase excess reading on arterialised capillary blood atapproximately half an hour after birth, be recorded onevery asphyxiated infant. The heart rate, although valuableduring resuscitation, does not add significantly to theinformation recorded in the Apgar score.
'Ve wish to thank the South African Medical ResearchCouncil for financial assistance.
REFERENCES
1. Apgar, V. (1953): Anaesth. Analg. Curr. Res., 32. 260.2. Crawford. J. S. (1965): Principles and Praccice of Obstetric Anaesehe-
sia, 2nd ed .. p. 283. Oxford: Blackwell.3. Prechtl, H. and Be nrem3., D. (1964): The Neurological Examinacion
of {he Fill/-Term Newborn InfanL (Little Club Clinics in Develop-mental Med.cine No. 12) London: William Heinemann MedicalBooks.
4. Heese. H. de V., Malan, A. F., Harrison, V. C. and Evans, A.(1966): S. Mr. Med. J., 40, 660.
5. Siggaard Anderson. 0., Engel, K., J(?)rgensen, K. and Astrup, P.(1960): Scand. J. Clin. Lab. Inve"., 12, 172.
6. Apgar, V. and James, L. S. (1962): Amer. J. Dis. Child., t04. 419.7. Crawford, J. S. (1962): Develop. Med. Child Neural., 4, 441.8. James, L. S. (1962): Ibid., 4, 444.9. Drage, J. S. and Berendes, H. (1966): Pedial. Cl.n. N. Amer., 13.
61 5.10. Gupta, J. M. and Tizard, J. P. M. (1967): Lancet, 2, 55.11. Dawes, G. S. (1968): Feral and Neonaral Physiology, p. 149. Chicago:
Ye
Related Documents