4/16/17 1 An Orthopedic View of a Pelvic Floor Patient Lila BartkowskiAbbate, PT, DPT, MS, OCS, WCS, PRPC New Dimensions Physical Therapy 75 Plandome Road 611 Broadway – Suite 503 Manhasset, NY 11030 New York, NY 10023 Lila BartkowskiAbbate, Copyright 2017 History of Women’s Health Problems: • World Health Organization: • Conceptualization of health: considers health to be a state of complete physical, mental, and social wellbeing. • How does that apply to women? Haven’t women been considered all along? Lila BartkowskiAbbate, Copyright 2017 • US Public Health Service identifies 5 criteria that a disease or condition must meet in order to be a women’s health condition. • Eg: Pregnancy or Menopause • Osteoporosis Lila BartkowskiAbbate, Copyright 2017 • Examples of Women’s Health Issues: 1.Reproductive health 2.Gynecologic disorders 3.Eating disorders 4.Osteoporosis 5.Breast cancer / lymphedema 6.Lung cancer, other gynecologic cancer 7.Sports medicine injuries specific to women or that are prevalent in women 8.Chronic pain / fibromyalgia 9.Issues of domestic violence and sexual abuse and torture to women 10.Heart disease Lila BartkowskiAbbate, Copyright 2017 What is the reality of a Women’s Health Therapist and who do we treat? • Men • Women • Children Lila BartkowskiAbbate, Copyright 2017 Recognition in Women’s Health • APTA created the Women’s Health Certification Specialty in 2011 (WCS) • In the literature, we are now being addressed as pelvic health therapists • PRPC – Pelvic Health Rehabilitation Practitioner, Certified (Herman & Wallace) • CAPP Certificate of Achievement in Pelvic Physical Therapy (APTA) Lila BartkowskiAbbate, Copyright 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

4/16/17
1
An Orthopedic View of a
Pelvic Floor Patient
Lila Bartkowski-‐Abbate, PT, DPT, MS, OCS, WCS, PRPCNew Dimensions Physical Therapy
75 Plandome Road 611 Broadway – Suite 503Manhasset, NY 11030 New York, NY 10023
Lila Bartkowski-‐Abbate, Copyright 2017
History of Women’s Health Problems:
• World Health Organization:• Conceptualization of health: considers health to be a state of complete physical, mental, and social well-‐being.
• How does that apply to women? Haven’t women been considered all along?
Lila Bartkowski-‐Abbate, Copyright 2017
• US Public Health Service identifies 5 criteria that a disease or condition must meet in order to be a women’s health condition.
• Eg: Pregnancy or Menopause• Osteoporosis
Lila Bartkowski-‐Abbate, Copyright 2017
• Examples of Women’s Health Issues:1.Reproductive health2.Gynecologic disorders3.Eating disorders4.Osteoporosis5.Breast cancer / lymphedema6.Lung cancer, other gynecologic cancer7.Sports medicine injuries specific to women or that are prevalent in women8.Chronic pain / fibromyalgia9.Issues of domestic violence and sexual abuse and torture to women10.Heart disease
Lila Bartkowski-‐Abbate, Copyright 2017
What is the reality of a Women’s Health Therapist and who do we treat?
• Men
• Women
• Children
Lila Bartkowski-‐Abbate, Copyright 2017
Recognition in Women’s Health
• APTA created the Women’s Health Certification Specialty in 2011 (WCS)
• In the literature, we are now being addressed as pelvic health therapists
• PRPC – Pelvic Health Rehabilitation Practitioner, Certified (Herman & Wallace)
• CAPP -‐ Certificate of Achievement in Pelvic Physical Therapy (APTA)
Lila Bartkowski-‐Abbate, Copyright 2017
4/16/17
2
What types of dysfunction do we see?
• Stress Incontinence, Urinary Urge Incontinence, Urinary retention• Pre-‐natal & Post-‐partum symptoms• Fecal Incontinence & Chronic Constipation• Abdominal Pain• Pelvic Pain: vaginismus, vulvodynia, post-‐pelvic fractures, MVA• Coccyx Pain/SIJ Dysfunction• Sexual Dysfunction: erectile dysfunction, penetrative pain, ejaculation pain, testicular pain • Sitting Pain: Coccyx pain, ischial tuberosity pain
Lila Bartkowski-‐Abbate, Copyright 2017
Parallels and Differences of Traditional vs. Pelvic PT• Understanding of pelvic anatomy
• Looking above and below a joint
• Relationship of lumbar spine/LE to the pelvis
• Muscle dysfunction – muscle problem, just in a different place
• Muscles get too weak = incontinence, or too tight = pain & spasm
Lila Bartkowski-‐Abbate, Copyright 2017
Bony Landmarks1. Symphysis pubis 4. Pubic rami2. Ischial tuberosities 5. Sacrotuberous ligament3. Coccyx
Lila Bartkowski-‐Abbate, Copyright 2017
Modalities
• Heat, Ice• Ultrasound• Interferential for pain• TENS for pain• Real-‐time Ultrasound (RTUS)
Lila Bartkowski-‐Abbate, Copyright 2017
Manual Therapy Techniques
• Cyriax Cross-‐Friction Massage• Traditional Massage Technqiues• Connective-‐Tissue Mobilization vs Skin Rolling
• External and Internal Work• Intra-‐vaginal• Intra-‐rectal
Lila Bartkowski-‐Abbate, Copyright 2017
Neuromuscular Re-‐education
• Deep Breathing Exercises
• Squat & Drop – muscle release
• Retraining muscles for proper coordination
• Biofeedback training
• RTUS
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
3
Therapeutic Exercise
• Strengthening Exercises – for those who are weak
• Stretching Exercises – for those who are tight
• Understanding when to do each – takes understanding of condition
Lila Bartkowski-‐Abbate, Copyright 2017
Cycle of the Problem:
PELVIC FLOOR COMPONENT
ORTHOPEDIC COMPONENT
Lila Bartkowski-‐Abbate, Copyright 2017
Orthopedic Component
• Postural Screen:• Pelvic stability starts at the cranium and ends at the feet
• How much does forward head, thoracic kyphosis and lumbar lordosis play a role in pelvic stability?
Lila Bartkowski-‐Abbate, Copyright 2017
Does normalizing bony landmarks create pelvic stability?
Lila Bartkowski-‐Abbate, Copyright 2017
Core Strength
What does that mean for pelvic stability?
• Term of the past???
• Poor coordination• Weakness = Pain • How do our patients view core strength?
Lila Bartkowski-‐Abbate, Copyright 2017
How are PTs determining strength and pelvic stability? What is normal?
• Objective measures that we can use:• Palpation of Diastesis Recti – using calipers or RTUS• One-‐legged standing test (OLS)• Active straight leg raise (ASLR)
• addresses core coordination• pelvic floor muscle weakness• gives the therapist a good place to start
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
4
What is normal arthrokinematics& muscle coordination for pelvic stability?
Lila Bartkowski-‐Abbate, Copyright 2017
Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers
• Preactivation of the TrA, Oblique Internus, Multifidus, Pubococcygeus and Glut Max induce posterior rotation of the ilium relative to the sacrum• Increases tension on the posterior SI ligaments and posterior thoracolumbar fascia before load transfer onto the supporting leg• Co-‐activation of the trunk and hip muscles increases spinal stiffness and increases compression and stiffness of the SIJ
Lila Bartkowski-Abbate, Copyright 2017Hungerford,Gilleard,Lee 2004
Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers
• Posterior rotation of the (ilium) inominate in relation to the sacrum is a position for stability during transfer load• Anterior rotation occurred in symptomatic subjects during weight bearing. • Anterior rotation is a non-‐optimal pattern• Abnormal articular and neuromyofascial function during increased vertical loading through the pelvis.
Lila Bartkowski-Abbate, Copyright 2017Hungerford,Gilleard,Lee 2004
Optimal Pelvic Stability
• Normalized biomechanical movement, along with appropriate muscle coordination paired with optimal strength create core strength and stability.
Lila Bartkowski-‐Abbate, Copyright 2017
Pelvic Floor Muscles & SIJ
• Subjects with SIJ pain syndrome were different in their activation of the pelvic floor muscles, so:
A.Is it the joint problem that caused the PFM dysfunction?
B.Is it the PFM dysfunction that caused a deficit in the force closure mechanism of the SIJ?
Avery 2000
Lila Bartkowski-Abbate, Copyright 2017
Evidence of Altered Lumbo-‐Pelvic Muscle Recruitmentin the Presence of SIJ Pain
• Delayed onset in patients with SIJ pain:• Internal Oblique• Multifidus • Glut max in the supporting leg during hip flexion with SEMG
• Alteration in strategy for lumbopelvic stabilization • Disruption load transference through the pelvis
Lila Bartkowski-Abbate, Copyright 2017Hungerford 2003

4/16/17
5
Analyze the findings:
• Internal Oblique• Multifidus • Glut max in the supporting leg during hip flexion with SEMG
• IO firing was poor secondary to rib flare, over-‐dominant rectus?• Poor multifidi firing pattern secondary to increased lumbar lordosis, poor TA strength, lumbar vertebrae positioned into rotations creating poor firing patterns?• Glut max – does the patient have normalized hip extension, normal capsular ROM or stiffness into relative anterior translation?
Lila Bartkowski-‐Abbate, Copyright 2017
Pelvic Joint ControlPosteriorly:Sacral position stabilized by: Multifidus (to S4)Coccygeus (ischiococcygeus)
Anteriorly:Pubic symphysis stabilized by:PubococcygeusTrAInternal oblique
Lee 2005
Lila Bartkowski-Abbate, Copyright 2017
Posteriorly:Sacral position stabilized by • Multifidus (to S4)• Coccygeus (ischiococcygeus)
Anteriorly:Pubic symphysis stabilized by • Pubococcygeus• TrA• Internal oblique
• The orthopedic therapist can address >50% of muscle firing patterns• Pelvic health therapist will further look at:• Coccyx deviations: internal & external• Internal pelvic floor muscle assessment
Lila Bartkowski-‐Abbate, Copyright 2017
• Viewed as the composite function of three systems:• Osseo-‐ligamentous system -‐ provides a passive subsystem• Muscular system -‐ provides an active subsystem• Neural control system -‐ controls the subsystems
Lila Bartkowski-Abbate, Copyright 2017
Spinal Segmental Stabilization (Hodges)
Local Stabilizing System
• Intertransversarii• Interspinals• Longissimus thoracis
• Iliocostalis lumborum• Multifidus
• Quadratus (medial)• Transversus abdominus
• Internal oblique• Pelvic floor muscles
• includes deep muscles which have origin or insertion on the lumbar vertebrae and the pelvic floor muscles of the pelvis
Hodges
Lila Bartkowski-Abbate, Copyright 2017
Global Stabilizing System
• Longissimus thoracis• Iliocostalis lumborum• Quadratus (lateral)• Rectus abdominus• External oblique• Internal oblique • Global stabilizing system-‐ large, superficial
muscles of the trunk that move the spine and transfer the load from the thoracic to the pelvis
Hodges
Lila Bartkowski-Abbate, Copyright 2017
4/16/17
6
CHECK FOR ABDOMINAL FUNCTION
Lila Bartkowski-‐Abbate, Copyright 2017
What is diastesis recti?Thinning or splitting of the linea alba which is the connective tissue connecting two ends of the rectus abdominus
Linea alba 1. Thins2. Splits
Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-‐Abbate, Copyright 2017
Causation and contributing factors?
1. Abdominal laparoscopic surgery
2. Abdominal full-‐thickness surgery
3. Umbilical hernia4. Pregnancy5. Genetic connective tissue
make-‐up6. Poor abdominal coordination7. What is keeping the ends of
the rectus apart? Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-Abbate, Copyright 2017
Diastasis Recti Controversy
• Measurement by finger widths is unreliable
• Much of the time it was incorrect when compared to Real-‐Time Ultrasound (RTUS) measurements
• What’s the best way to measure it in the clinic? Depends upon your clinic’s goals. Finger-‐width is easy for the patient to self-‐measure.
Diastesis Rectus Abdominus (DRA) Prevelance
• 66% of women have a DRA in their third trimester and 53% persist immediately post-‐partum.• 36% remain AbN widened @ 7 wks (Boissonnault & Blaschat, 1998)• No change at 1 year post-‐partum (Coldron, et al 2008)• 52% of women with PFD (SUI or POP) have a DRA (Spintznagle ,et al 2007)
Lee, Lecture Discover the Pelvis, 2010
• We take this idea and transfer it to the more global population: why are men and children becoming urinary incontinent and/or have long-‐lasting low back pain?
Lila Bartkowski-Abbate, Copyright 2017

4/16/17
7
Linea Alba at Rest
< 45 years old
• Supraumbilical >10 mm • Umbilical Ring >27 mm • Subumbilical >9 mm
> 45 years old
>15 mm
>27 mm
>14 mm
Lila Bartkowski-Abbate, Copyright 2017 Lila Bartkowski-Abbate, Copyright 2017
Lila Bartkowski-Abbate, Copyright 2017
Diastesis = Low back pain & urinary incontinence and abdominal pain?
Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-Abbate, Copyright 2017
Diastasis Recti Correction• How do we bring the rectus abdominus ends together?
• Passive realignment of the muscle, then isolation of recruitment
• Head lift alone isolates the rectus abdominus
• Adding a posterior pelvic tilt increases the SEMG activity
Diastasis Recti Correction
Sheet wrapped around the thorax for approximation of the rectus abdominus – brings the ends of the rectus closer togetherHead lift Hold 3-5 seconds30 reps
Lila Bartkowski-Abbate, Copyright 2017

4/16/17
8
What if the first step doesn’t work?1. Check lumbar spine bony position2. Clear out myofascial restrictions that
are keeping the ends of the rectus from coming back together
3. Rectus stripping – soft-‐tissue technique
4. Check rib position and look for rib flaring
5. What are the obliques doing?6. Normalize spinal curves7. Normalize hip ROM & strength8. Teach functional positions: avoid curl
up and down with transitional movements: use log rolling
Lila Bartkowski-‐Abbate, Copyright 2017
1. Understand lumbar mechanics along with basics of flexion and extension and how to treat each dysfunction
2. Understanding of the myofascial clock and clearing out soft-‐tissue restrictions
3. Look for rib flaring and use of McConnell taping treatment
4. Basic hip mobilizations5. Basic movements that create more vs
less diastesis
What you need to do….1. Check lumbar spine bony position2. Clear out myofascial restrictions that
are keeping the ends of the rectus from coming back together
3. Rectus stripping – soft-‐tissue technique4. Check rib position and look for rib
flaring5. What are the obliques doing?6. Normalize spinal curves7. Normalize hip ROM & strength8. Teach functional positions: avoid curl
up and down with transitional movements: use log rolling
What skill-‐set you need to have….
1. Understand lumbar mechanics along with basics of flexion and extension and how to treat each dysfunction
2. Understanding of the myofascial clock and clearing out soft-‐tissue restrictions
3. Look for rib flaring and use of McConnell taping treatment
4. Basic hip mobilizations5. Understanding of basic movements
that create more vs less diastesisLila Bartkowski-‐Abbate, Copyright 2017
Testing and Assessment (Lee)Integrating Lab & Lecture
• Clinical evaluation for Hip/Pelvis/SIJ:
1. One-legged standing test (OLS)2. ASLR- raising one leg in supine and isolation of TrA, PF, Multifidus3. Decompression
Lila Bartkowski-Abbate, Copyright 2017
TESTING for SIJ StabilityOne-‐legged Standing Test (OLS)• Standing• Palpate ilium @ ASIS and hug around entire ilium• Palpate S2 using 2 finger pads of digits 2 & 3• Distance between thumbs should stay the same or get a little smaller• Ilial anterior rotation – distance is greater• Indicates lack of stability• Have patient contract:• TrA, Pelvic floor, both• Use guide wire imaging
Lila Bartkowski-Abbate, Copyright 2017
Active Straight Leg Raise (ASLR)
• Proven to be valid, reliable and specific to determine:• load transfer between the lumbosacral spine and lower extremities.
• Can identify and isolate the weakest link. • TrA• PF• Multifidus
Mens, 2006
Lila Bartkowski-Abbate, Copyright 2017
ASLR Test
• Helps clinician determine:
A.Whether it is appropriate to start exercises to increase stability.
B.Whether to start techniques to decrease compression and excessive stability.
Lila Bartkowski-Abbate, Copyright 2017

4/16/17
9
ASLR TestAbnormal strategies cause:•Excessive joint compression•Loss of mobility•Increases in IAP •Restriction of ribcage mobility for respiration •Reduced postural control•Pain•Dysfunction
Lila Bartkowski-Abbate, Copyright 2017
ASLR Test•
Lila Bartkowski-Abbate, Copyright 2017
•Ask patient to alternatively actively lift straight leg off table approximately 12” off table.•Ask pt if it is more difficult to lift one than the other.•Observe for the following substitution strategies:Abd Wall bulgingTrunk rotationBreath holdingThoracic spine extension
Lee LJ 2006
ASLR TestMedial compression
Compression at anterior pelvis at ASIS for Transversus AbdominusCompression at anterior pelvis at pubic symphysis is Anterior Pelvic Floor Compression at posterior pelvis at ischial tuberosities is Posterior Pelvic FloorCompression at posterior pelvis at PSIS is MultifidusCompression at combinations simulates multiple musclesLook for easier lifting of leg
LEE, LJ 2006Lila Bartkowski-Abbate, Copyright 2017
ASLR Test -‐ Decompression
Lila Bartkowski-Abbate, Copyright 2017
If none of those work, patient may be too stable.
Decompression: Thoracic erector spinaeAnterior/posterior cranial
Start with myofascial release,breathing, TrP release, strain-counter strain
Lee LJ 2006
McConnell Tape for Diastesis Recti
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
10
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017
Abdominal PainVisceral & Musculoskeletal Causes and Treatment
Lila Bartkowski-‐Abbate, Copyright 2017
CONTRIBUTION OF THE VISCERA
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
11
When is the abdominal pain occuring?
Related to Food/Ingestion
• During the eating phase?
• During the digestion phase?
• 1-‐2 hours after eating?
Related to Movement/Locomotion
• Standing/walking• Where in the quadrant of the abdomen?
• Do they have a diastesis?
Lila Bartkowski-‐Abbate, Copyright 2017
Overview of the Superficial Organs
Lila Bartkowski-‐Abbate, Copyright 2017
Stomach
• The stomach is a muscular organ located on the left side of the upper abdomen. The stomach receives food from the esophagus.
• As food reaches the end of the esophagus, it enters the stomach through a muscular valve called the lower esophageal sphincter.
Lila Bartkowski-‐Abbate, Copyright 2017
Large Intestines
Lila Bartkowski-‐Abbate, Copyright 2017
1. The large intestine has four parts: cecum, colon, rectum, and anal canal.
2. Partly digested food moves through the cecum into the colon, where water and some nutrients and electrolytes are removed.
3. The remaining material, solid waste called stool, moves through the colon, is stored in the rectum, and leaves the body through the anal canal and anus.
Lila Bartkowski-‐Abbate, Copyright 2017
Function of the Sigmoid Colon
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
12
When to refer out to a pelvic health therapist? • Abdominal pain related to eating• Abdominal surgical history that seems more complicated than basic scar management can release• Abdominal pain complicated by gas and bloating• Abdominal pain relating to bowel movements• Abdominal related to sexual activity
• Refer to MD• Red flags: fever, sweats, non-‐orthopedic nature of their symptoms
Lila Bartkowski-‐Abbate, Copyright 2017
CONTRIBUTION OF THE MUSCULOSKELETAL SYSTEM TO THE CAUSATION OF ABDOMINAL PAIN
Lila Bartkowski-‐Abbate, Copyright 2017
• Abdominal posturing shifts the internal center of gravity up toward the chest: “forces man to swing between hypertension and slackness (inefficiency)”.
Durkheim, “Hara: The Vital Centre of Man”
Lila Bartkowski-‐Abbate, Copyright 2017
Shortened Psoas
1. Minimizes the passive pumping action to the bowel
2. Decreases respiration which indirectly moves the organs from a cranial to caudal motion
3. Decreases normal hip extension which decreases glut strength
Lila Bartkowski-‐Abbate, Copyright 2017
Iliopsoas
• Positioned to travel with the aorta move through the thorax and are postioned adjacent to the ascending and descending colon.• Contraction/relaxation of iliopsoas creates passive bowel motility.
Lila Bartkowski-‐Abbate, Copyright 2017
• Psoas functions as a counter-‐balance to the rectus, maintaining a centered anterior-‐posterior relationship.• However, all the abdominals muscles are directly balanced by the length of the hamstring.• The balance between the iliopsoas complex, the abdominals and the hamstrings maintain a functional relationship.
• Koch, L. The Psoas Book, 1997.
Lila Bartkowski-‐Abbate, Copyright 2017
4/16/17
13
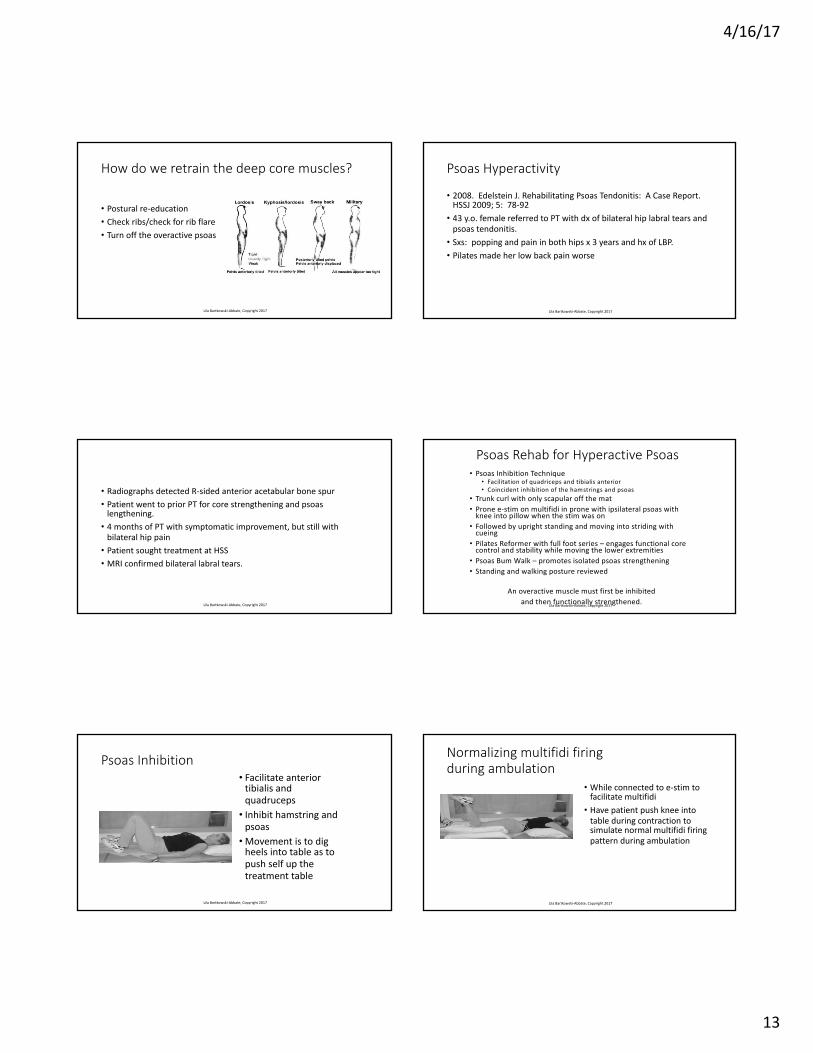
How do we retrain the deep core muscles?
• Postural re-‐education• Check ribs/check for rib flare• Turn off the overactive psoas
Lila Bartkowski-‐Abbate, Copyright 2017
Psoas Hyperactivity
• 2008. Edelstein J. Rehabilitating Psoas Tendonitis: A Case Report. HSSJ 2009; 5: 78-‐92• 43 y.o. female referred to PT with dx of bilateral hip labral tears and psoas tendonitis. • Sxs: popping and pain in both hips x 3 years and hx of LBP.• Pilates made her low back pain worse
Lila Bartkowski-‐Abbate, Copyright 2017
• Radiographs detected R-‐sided anterior acetabular bone spur• Patient went to prior PT for core strengthening and psoas lengthening.• 4 months of PT with symptomatic improvement, but still with bilateral hip pain• Patient sought treatment at HSS• MRI confirmed bilateral labral tears.
Lila Bartkowski-‐Abbate, Copyright 2017
Psoas Rehab for Hyperactive Psoas• Psoas Inhibition Technique
• Facilitation of quadriceps and tibialis anterior• Coincident inhibition of the hamstrings and psoas
• Trunk curl with only scapular off the mat• Prone e-‐stim on multifidi in prone with ipsilateral psoas with knee into pillow when the stim was on• Followed by upright standing and moving into striding with cueing • Pilates Reformer with full foot series – engages functional core control and stability while moving the lower extremities• Psoas Bum Walk – promotes isolated psoas strengthening• Standing and walking posture reviewed
An overactive muscle must first be inhibited and then functionally strengthened.
Lila Bartkowski-‐Abbate, Copyright 2017
Psoas Inhibition• Facilitate anterior tibialis and quadruceps• Inhibit hamstring and psoas•Movement is to dig heels into table as to push self up the treatment table
Lila Bartkowski-‐Abbate, Copyright 2017
Normalizing multifidi firing during ambulation
• While connected to e-‐stim to facilitate multifidi• Have patient push knee into table during contraction to simulate normal multifidi firing pattern during ambulation
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
14
Psoas Bum Walk
• Developed by Erl Pettman• Without moving laterally, have patient scoot forward to strength the psoas • Patient has to advance forward only using the psoas• Alternate R to L buttock
Lila Bartkowski-‐Abbate, Copyright 2017
WHAT IS THE IMPACT OF THE PELVIC FLOOR MUSCLES?
Lila Bartkowski-‐Abbate, Copyright 2017
Referred pain patterns of abdominal pain
• Do we think about the pelvic floor muscle group as a co-‐contributor to abdominal pain? • Is abdominal pain an extension or progression of low back pain?• During your pelvic examination:• think about is there laxity in the anterior vs. posterior compartment?• Is there overactivity in the anterior vs. posterior compartments?
Lila Bartkowski-‐Abbate, Copyright 2017
HOW DO WE TREAT ABDOMINAL PAIN?
Lila Bartkowski-‐Abbate, Copyright 2017
Check List• Postural Screen – back to the basics• Are normal spinal curves present?• Are the ribs flared?• Are the rings rotated?• Does the rectus fire appropriately?• Is there diaphragmatic breathing and passive expiration?• Is there true normal hip extension?• Is the psoas overactive and uncoordinated? • Is iliacus bound down?• Diastesis present?
Lila Bartkowski-‐Abbate, Copyright 2017
To Decrease Thoracic Kyphosis
• Towel rolls• ½ foam roller• Full foam roller• Lie supine over Bosu/Ball• Medicine ball roll on SPLie over roll for 5 minutes in the AM & PM –using the low-‐load/creep theory
Pectoralis major stretch with every rest room visit
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
15
Lumbar Lordosis Correction
• Is it caused by gluteus weakness or tight hip flexors?
IT DOESN’T REALLY MATTER
• Intervention will require the correction of both
Lila Bartkowski-‐Abbate, Copyright 2017
Lack of True Hip Extension
• Compensations can be seen in many ways• Increased lumbar lordosis: tight psoas, quadriceps• Excessive sacral mobility: is ilium medially/laterally glided? Iliacus tightness, pubococcygeus tightness? Is there sacral-‐ilial disassociation?• Increased pelvic torsion during ambulation• Decreased relative hip anterior translation• Knee hyperextension• Medial/Lateral heel whip during FF push off• Obturator internus tight
Lila Bartkowski-‐Abbate, Copyright 2017
• Hip Flexor Stretch
• Use Bosu or mat/towel
• Isolation of the gluteus maximus and minimizing lumbar lordosis
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
16
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017
Lila Bartkowski-‐Abbate, Copyright 2017 Lila Bartkowski-‐Abbate, Copyright 2017
Conclusion
Lila Bartkowski-‐Abbate, Copyright 2017
• Orthopedic dysfunction is the major contributing factor to patient’s c/o:• Low back pain: core coordination training needed• Urinary Incontinence: core coordination & pelvic floor muscle training• Abdominal pain: psoas overactivity, organ dysfunction & core coordination
• When correction of many of the orthopedic components fail, it is then time to refer to a pelvic floor physical therapist:• Low back pain: core coordination training needed & pelvic floor muscle overactivity• Urinary Incontinence: core coordination & pelvic floor muscle training• Abdominal pain: psoas overactivity, organ dysfunction & core coordination
Lila Bartkowski-‐Abbate, Copyright 2017

4/16/17
17
How to find a pelvic health therapist?
• www.apta.org• Find a PT
• Women’s Health
• www.hermanwallace.org• Practitioner Directory
• abbate@nd-‐pt.com
Lila Bartkowski-‐Abbate, Copyright 2017
BREAK FOR DELEGATE MEETINGNEXT IS LAB…..
Lila Bartkowski-‐Abbate, Copyright 2017
Related Documents











