-
8/3/2019 3.9 a Reliable Method of Establishing the Level of the Fetal Head in Obstetrics. d. Crichton
1/4
7840& G 22
S.A. MED ICAL JOURNAL(Supplfment-South African lournal of Obstetrics and Gynaecology)
17 April 1974
AReliable Method of Establishing the Level of theFetal Head in ObstetricsD. CRICHTON
SUMMARYA method of assessing the level of the head clinically in'fifths of the head above the pubic symphysis' is des-cribed, i llustrated, and commented upon. I ts val ue in de-l ineating the descent of the head in problem cases, andas a guide t o whether or not the. head can be deliveredsafely from below, has been proved in thousands of casespresenting w ith problems of disproportion at KingEdward VIII Hospital, Durban. Confirmatory evidence byradiographic examination has been forthcoming in a largepercentage of cases.
The traditional methods of assessing the level of thehead, by i ts 'stat ion' and 'engagement', are described andsubjected to criticism. They are theoretically unsound, andpractically misleading, especial ly in problem cases.S. Afr. Med. l . 48, 784 (1974).
Hitherto only the term 'engagement' or 'station' of thehead has been employed universal ly to describe and assessthe level of the fetal head in clinical obstetrics. The practical significance, however, of engagement is so nebulousthat an examiner can be guaranteed the following definition if he asks a candidate to define this term in a finalmedical examination. 'When the largest diameter for that"articular presentation has passed through the brim of theoelvis'. Should an examiner ask a candida te to correlatethis definit ion with the fetal head in i ts clinical relat ionship to the maternal pelvis, he will find i t dif ficult to do so.
The potential dangers in mistaking the level of the headdeserve emphasis and elaboration, and the need to establishuniformity and an accurate method for describing thelevel o f t he head in the pelvis is the purpose of this article.
In pursuance of th is , a method of assessing the level ofthe head, the fifths of the head above pubic symphysismethod, is described. This and other established methods(of engagement and station of the head) are subjected to acritical analysis whereby the reliability of each is assessedand each is compared.
REQmREMENTS OF ANY METHOD INASSESSING THE LEVEL OF THE HEADThe point selected must be easy to palpate, have obstetricsignificance, and be unchanged by the pressures of difficultDepartment of Gynaecology and Obstetrics, University ofNat al and King Edward VllI Hospital, DumanD. CRICHTO_ , M.B. CH.B., D.PmL. , F.R.C.S., F.R.C.O.G.Paper presented at the Interim Congress of the Socie ty of Obstetricians~ ' 1 d G r n a e c o l o ~ i s t s held in Port Elizabeth on 23 September 1 9 6 ~ .
labour on both the fetal head and maternal pelvis. Thesefindings should be easily and reliably carried out by bothmedical and nursing staffs. These being the requirements,they consti tute the best yards ticks whereby the merits ofavailable methods of assessing the level of the head canbe evaluated and compared.
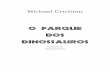
FIFTHS OF THE HEAD ABOVE THEPUBIC SYMPHYSISThis is defined as that proportion of the head (described infifths) which lies above the level of the pubic symphysis.Thus the head completely above the level of t he puo icsymphysis is described as five-fifths above, and the headdeep in the pelvis (with neither s inciput no r occiput palpable abdominally) is nought-fifths above. The occiputcan only be just tipped when the head is two-fifths above(engaged). Only the sinciput can be just tipped when ahead is one-fifth above (Fig. 1).
Landmarks on the Fetal HeadThese are the occiput and sinciput and, if the head ishigh, the midpoint on an imaginary line is drawn betweenthem. These points are easily defined by different observers.
Neither moulding no r caput of the fetal head can prejudice the accuracy of assessing their level because theylie along the base of the skull.
Landmark on the PelvisThis is the upper border of the pubic symphysis. The
landmark is easily palpable in all cases and can be reliablycarried out by different observers. .
Analysis of the ConceptA basovertical diameter' extending from the base of the
skull to the most distant point of the vertex measures onlyslightly less than the biparietal diameter which is just over9 cm in an average 3,182-kg baby. Therefore, 2 cm on thisline represents roughly one-fifth of the head.As regards the selection of reliable landmarks on thepelvis, i t might be said that the level of the pubic symphysisis not the level of the brim of the pelvis. From a practicalstandpoint, however, the correlation between the levels issufficient to render the level of the pubic symphysis acceptable as all index of the level of the brim, for clinical
-
8/3/2019 3.9 a Reliable Method of Establishing the Level of the Fetal Head in Obstetrics. d. Crichton
2/4
17 April 1974 S . -A . M E D IE SE T YD S KR IF(Byvoegscl-Suid-Afrikaanse Tydskrif vir Obsrerrie en Ginekologie)
7850 & G 23
Sinciput +++++Occiput ++++ ABDOMEN
Sinciput ++Occiput + I t i J ; : ~ 1 Sinciput +t i i ~ 1
Occiput Nil......__ . . . .,.............._ PUBICSYMPHYSIS
CAESAREAN SECnON a. Symphysiotomyb. Craniotomy
TRIALFORCEPS
MIDFORCEPS
LOWFORCEPS
Fig. 1 . Level of tbe bead in f if tbs above pubis symphysis.
purposes. Theoret ical ly, special allowances could be madein cases with very high or low assimilation pelves, butduring an experience of problems of disproportion noneof my staff have found correction clinically advantageous,even though it would have been easy to do so, fo r theinterpretation of radiographs taken during trials of labouris undertaken exclusively by the obstetric staff conductingthe trial o f l abou r in ou r unit. Thus, correlation of theclinical level of the head with the precise level seen onradiographs taken at that time, has been forthcoming ina high percentage of cases.
Practical Application of the MethodThe clear definition of the levels of the sinciput and
occiput as well as the upper margin of the pubic symphysis,the bladder naturally being empty, is essential. The levelof the upper margin of the pubic symphysis shou ld bemarked with an indelible line.The sinciput and occiput levels are most accuratelydefined by the 'second pelvic grip'. Mistakes are commonwhen the hands are not maintained almost in line with theforearms and when palp at ion commences too low, tooanterior, and too forcefully, with fingers, as opposed to thegentle pressure with the flat of the hand. The fingers mustbe held almost paral lel to the surface of the abdomen,with a little additional pressure being applied at times,by slight flexion of the metacarpophalangeal joints (notinterphalangeal joints) (Fig. 2). There is no force likegentleness fo r this palpation.Occas iona lly difficulty is exper ienced when the occ iputlies posterior and when the lower abdomen is prohibitivelyresistant to palpation. A combined abdominovaginalexamination will help to clarify the position, for the fingersin the vagina are able to impart small degrees of move-ment to the sinciput and occiput, which renders theirlevel more easily appr ec ia ted by the fingers on theabdomen (Fig. 3). A better appreciation of the size ofthe fetal head is an additional advantage.The levels of the sinciput and occiput can be marked
on the anterior abdominal wall, and a line drawn between
Fig. 2. Second pelvic grip--correct positioning of forearms,hands and fingers.
them would indica te the degree of flex ion and the level ofthe base of the skull; but special care mus t be taken notto dis tort the level of the abdominal skin in marking thesepoints. This prac tice has proved helpful in teaching and
-
8/3/2019 3.9 a Reliable Method of Establishing the Level of the Fetal Head in Obstetrics. d. Crichton
3/4
7860& G 24
S.A. MED ICAL JOURNAL(Supplemeni-Solllh African Journal of Obstetrics and Gynaecology)
17 April 1974
THUMB RESTING ONUPPER MARGIN OF
PUBIC SYMPHYSIS:--.-
ESTIMATING LEVEL OF THE HEAD BYABDOMINAL-PELVIC EXAMINATION
Fig. 3. Abdominopelvic method of assessing head level.
checking upon the accuracy achieved by students and staff.It is also helpful as a guide to radiographers undertakingintrapartum radiography, fo r they are thereby able toavoid omitting part of the head from radiographs.
It has recently been suggested' that this method couldbe modified by placing the fingers of the right hand suprapubical ly while palpating the sinciput and occiput wit h aleft-hand reversed Paulic's grip. This method, however, isactua lly not a modif ication, but a different method whichwas evaluated some years ago in ou r Unit and found tooinaccurate to use. The reasons are as follows:Alt hough the reversed Paulic's g rip is supposed to besuperimposed on points previously established by thesecond pelvic grip, all too soon the staff lapsed into'establ ishing' the level of the head with the reversedPaulic's grip, whether a preliminary second pelvic grip
had been done or not. Whereas the inaccuracy is notserious when the head is more than three-fifths above, inaccuracy when the head is three-fifths or less above(especially when the occiput is posterior) is often disastrousat levels which have greatest obstetric importance. Further,when it comes to assessing the level of th e h ead as beingone- or two-fifths above, this is assessed with the breadthof I or 2 fingers above the pubic symphysis in the suggested modification; but these head levels are well abovethose employed in my method (i.e. sinciput just tippedone-fifth above, and occiput just tipped-two-fifths above).
It will be seen, therefore, that the suggested modificationis actua lly a dif ferent method altogether, and why itsinaccuracy is dangerously misleading.
ENGAGEMENT OF THE HEADThe accepted definition of 'engagement ' is when the largestdiameter for that particular presentation has passedthrough the brim of the pelvis.
Landmark on the HeadIn clinical practice it is impossible to palpate or ascertainprecisely what is the largest diameter for that particularpresentation. Some obstetricians at temp t t o defend thisimaginary clinical l andmark by saying that it can be correlated with the lowest point of the head palpated vaginallyin relation to the ischial spines. This introduces the disadvantageous vaginal examinations, and presupposes thatthe head is not elongated by moulding (which it probably
would be in a problem case). The further assumption thatthe distance between the ischial spines and the level of thebrim is constant is also l ikely to be erroneous in problemcases.Other obstetricians try to relate this indistinct clinical
landmark on the head with the pos it ion of the biparietaldiameter (passing through the brim of the pelvis), but this,too, cannot be defined clinically, and the level of the biparietal diameter varies considerably in relat ion to otnercranial diameters, with moulding.
-
8/3/2019 3.9 a Reliable Method of Establishing the Level of the Fetal Head in Obstetrics. d. Crichton
4/4
17 April 1974 S. -A. MED I E SE T YDSKR I F(Byvoegsel-Suid-Afrikaanse Tydskrif vir Obstetrie en Ginekologie)
7870& G 25
Landmark on the PelvisThe brim of the pelvis is selected fo r this measurement.
It is impossible to determine the level of the pelvic brimby abdominal palpation. Further, variations in the angleof pelvic inclination and variations in the levels of theavailable conjugate and transverse diameters may lowerthe level of the available brim below the clinical guessesmade when this method is favoured. In practice thediversity of assessments of this plane when engagement isbeing determined is considerable.
It follows t ha t th e widely recognised fact that differentobservers (nurses or doctors) often give contradictoryestimations of engagement i n p robl em cases should nolonger arouse surprise, but fulfil expectations in the lightof the nebulous nature of landmarks selected on the fetalhead and the maternal pelvis demonstrated in this analysis.Further elaboration is superfluous to prove that the con-cept of engagement of the head constitutes one of thosemeaningless clinical definitions which have been handeddown from textbook to tex tbook; one which should berelegated to obstetric history!
STATION OF THE HEADThe station of the head is the relationship which its lowestcranial point bears to the level of the ischial spines (Fig. 4).
Landmark on the BeadIn normal cases with no disproportion, establishment ofthe level of the lowest cranial point is easy. I t is the prob-lem case, associated with disproportion in labour, in which
accurate establishment of the level assumes importance;here it is difficult, unreliable, and misleading. In trials oflabour associated with ruptured membranes and dispropor-tion, an overlying caput succedaneum will give the im-pression that the head is far lower than it really is, andwill obstruct a clear definition of the lowest cranial point.Furthermore , the greater the moulding of the head, themore i t elongates (lengthening of the basovertical dia-meter') , thus the lowest point of the cranium descends,whereas its base r emains stationary or descends moreslowly (Fig. 4).
Consequently, once again the.obstetrician can easily betempted to deliver a head vaginal ly when i ts t rue level isdangerously high, and deluded into the belief that there isprogress in a trial of labour in terms of descent of thehead when this is not so.
Landmark on the PelvisThe ischial spines are recognisable on vaginal examina-tion and establ ish the level of the bispinous diameter.
Part of the confidence placed in the selection of thislevel, however, rests upon the assumption that it bears aconstant relationship to the level of t he br im which is the
Misleading -STATION OF THE HEAD"if Caput and moulding exist
STATION OF THE HEADFig. 4. Station of head (top), and moulding and caputdestroying reliability of assessing head level by station(bottom).
main obstacle to the descending head. Unfortunately, thisis often an erroneous assumption in problem cases.
The assessment of the level of the head in terms ofstation of the head has serious shortcomings; first, theassessment cannot be made abdominally-pelvic examina-tions are essential; secondly, the landmark selected on thefetal cranium becomes incapable of clear definition dueto caput formation, and decreases in rel iabili ty propor-tionately to moulding; and thirdly, the pelvic landmark isunreliable in practice.
REFERE 'CES1. CrichlOO, D. (1962): J . Obstet. Gyn.ec. Brit. Emp., 69 , 366.2 . Notelov itz, M. (1973)' S. Afr. J. Obstet. Gyn.ec., 11, 3.