ANTITUBERCULAR DRUGS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ANTITUBERCULAR DRUGS

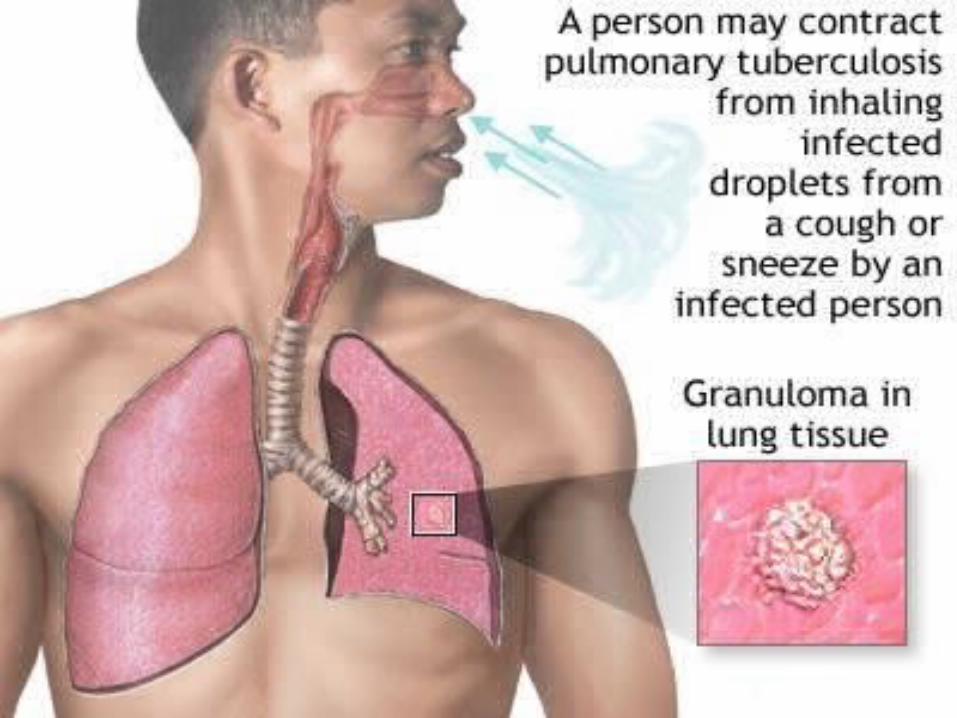
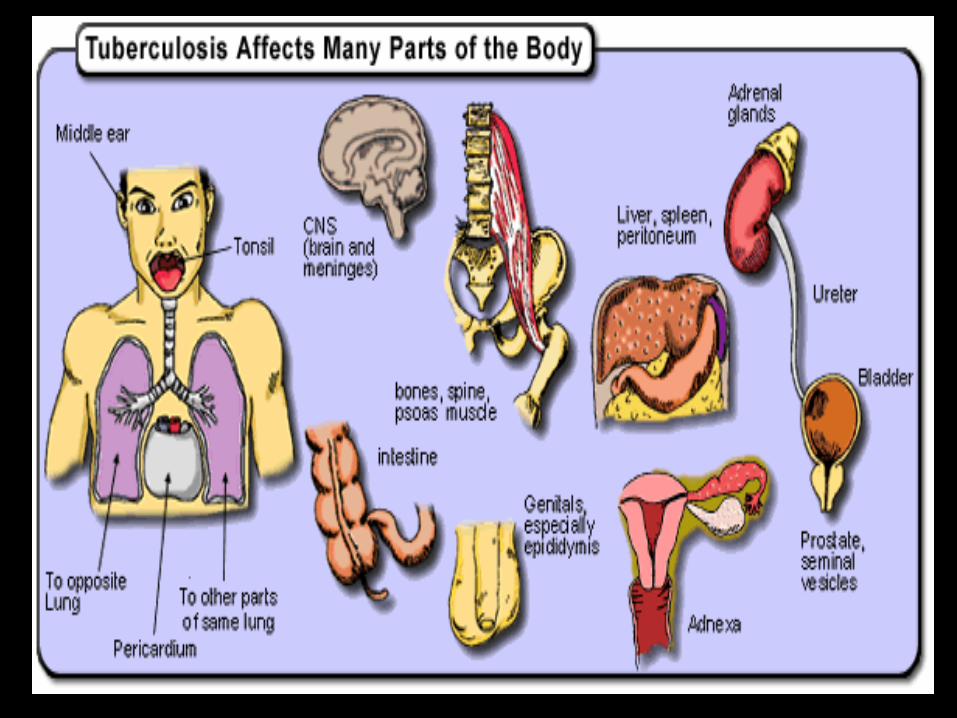
• Tuberculosis is a chronic granulomatous disease caused by Mycobacterium tuberculosis
• A major health problem in developing countries

Aims of treatment
• To kill the dividing bacilli & to destroy the persisters in order to prevent relapse and ensure complete cure
To prevent development of drug resistance. To decrease transmission to others.
Drugs are combined to:• Delay the development of resistance• Reduce toxicity• Shorten the course of treatmentDuration of therapy: Depends on 1.Site of disease, 2.Bacillary load, 3.Severity of disease, 4.History of treatment and resistance.
Classification
1. First line antitubercular drugs (standard drugs)• Isoniazid (H)• Rifampicin (R)• Pyrazinamide (Z)• Ethambutol (E)• Streptomycin (S)
2. Second line antitubercular drugs (Reserve drugs)
• Amikacin• Para - aminosalicylic acid• Kanamycin• Cycloserine• Ethionamide• Thiacetazone• Ciprofloxacin, moxifloxacin, gatifloxacin• Clarithromycin, azithromycin• Rifabutin, rifapentine
Newer agents
First line antitubercular drugs (standard drugs)
ISONIAZID (Isonicotinic acid hydrazide, INH)
• Mechanism: inhibits the biosynthesis of mycolic acids, which are essential constituents of the mycobacterial cell wall
Adverse Reactions:• Hepatitis - loss of appetite, nausea, vomiting,
jaundice, and right upper quadrant pain • Peripheral neuropathy (deficiency of
pyridoxine )• Fever, skin rashes , arthralgia, GI disturbances• Psychosis, optic neuritis and rarely
convulsions
RIFAMPIN• Mechanism:
inhibits bacterial DNA-dependent
RNA polymerase
inhibits RNA synthesis
Adverse effects• Hepatitis• Flu-like syndrome – fever, chills, headache,
muscle & joint pain• GI disturbances• Skin rashes, itching, & flushing• Orange-red discoloration of body fluid
secretions such as urine, tears, saliva, sweat, sputum etc - patient to be informed
ETHAMBUTOLMechanism:• Inhibits arabinosyl transferases that are
involved in mycobacterial cell wall synthesis Adverse effects:• Optic neuritis: red -green color blindness• Hyperuricaemia• Skin rashes & joint pain
PYRAZINAMIDEMechanism:•Like INH, pyrazinamide inhibits mycolic acid biosynthesis but by a different mechanism.Adverse effects :•Dose-dependent hepatotoxicity•Hyperuricaemia•Anorexia, nausea, vomiting, fever and skin rashes
Streptomycin• It was the first effective drug developed for the
treatment of tuberculosis. • Is an aminoglycoside antibiotic• Adverse effects: ototoxicity, nephrotoxicity
and neuromuscular blockade
SECOND-LINE DRUGS
In case of resistance to first-line agentsIn case of failure of clinical response to
conventional therapy In case of serious treatment limiting adverse
drug reactions
Treatment of Tuberculosis:• WHO recommends the use of multidrug
therapy (MDT) for all cases of tuberculosis. The objectives of MDT are:– To make the patient non-infectious as early as
possible by rapidly killing the dividing bacilli by using 3-4 bactericidal drugs.
– To prevent the development of drug resistant bacilli.
– To prevent relapse by killing the persisters or dormant bacilli.
– To reduce the total duration of effective therapy.
Short Course Chemotherapy (SCC)Intensive phase: • Tuberculocidal drugs used• The main objective is to render the patient
non-contagious.2HRZE:
INH RifampinPyrazinamideEthambutol
Continuation phase: • This phase helps to eliminate persisters and
prevents relapse4HR:
INH Rifampin
Antileprotic drugs
Classification:
Sulfone – Dapsone Phenazine derivative – Clofazimine Antitubercular drugs – Rifampicin EthionamideOther antibiotics – Ofloxacin Minocycline Clarithromycin
DapsoneUse : antileprotic agent
Adverse effects: Haemolytic anemia & methaemoglobinaemia – G6PD deficiency cases Sulfone syndrome – fever, dermatitis, pruritus,
anemia lymphadenopathy & hepatitis GI disturbances, headache, itching Peripheral neuropathy
2. Rifampicin – used in multidrug regimens – kills most
of the bacilli
3. Clofazimine:MOA – binds to mycobacterial DNA - inhibits its template function – anti-inflammatory effect
Use : antileprotic agent
Adverse effects: Accumulates in tissues : red-to-brown
discoloration of the skin Pigmentation of the conjunctiva & cornea GI disturbances
Treatment of LeprosyPaucibacillary :- Dapsone:100mg dailyRifampin:600mg once a month-Supervised.Duration:- 6 months.
Multibacillary Leprosy:-Dapsone:- 100mg dailyRifampin:- 600mg once a month supervisedClofazimine:- 300mg once a month supervised,50 mg
daily.Duration:- 24 Months.
Related Documents











