Neurosurgery department, Vajira hospital Evaluation and Management Craniocervical Dissociation Atlantoaxial Rotatory Subluxation Transverse Ligament Injury Chapter 313 and 314 YOUMANS Neurological Surgery sixth edition

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Neurosurgery department, Vajira hospital
Evaluation and Management Craniocervical Dissociation Atlantoaxial Rotatory Subluxation Transverse Ligament Injury
Chapter 313 and 314
YOUMANS Neurological Surgery sixth edition

Craniocervical Dissociation

Anatomy of craniovertebral junction
✤ Ligaments of craniovertebral junction (CVJ)
✤ Skull to atlas group
✤ Articular capsule ligaments
✤ Anterior and posterior atlanto-occipital ligament
✤ Lateral atlanto-occipital ligament
✤ Cruciate ligament

Skull to atlas group

Anatomy of craniovertebral junction
✤ Ligaments of craniovertebral junction (CVJ)
✤ Skull to axis group
✤ Alar ligament
✤ Tectorial membrane
✤ Apical dental ligament
✤ Ligamentum nuchae

Skull to axis group

Stability of CVJ
✤ Mainly from skull to axis group of ligaments
✤ Alar ligament
✤ Connect odontoid process to occipital condyles and lateral mass of atlas
✤ Control axial rotation of neck and limit lateral flexion and AP translation
✤ Tectorial membrane (continuation of PLL)
✤ Connect dorsal surface of odontoid process to ventral surface of foramen magnum
✤ Limit hyperextension of neck
✤ Odontoid process to foramen magnum limits hyperflexion of neck

Stability of CVJ

Stability of CVJ
Mechanism of injury
✤ Mechanisms
✤ Hyperextension
✤ Hyperflexion
✤ Lateral flexion
✤ Combined forces

Mechanism of injury
✤ Most common is hyperextension combined with extreme lateral flexion
✤ Hyperextension cause rupture of tectorial membrane
✤ Extreme lateral flexion cause alar ligament injury
✤ Anterior dislocation of cranium to cervical spine
✤ Children are susceptibility to AOD because of
✤ Less stiffness of ligaments
✤ Larger head to body ratio

Clinical findings✤ Most common causes are high-speed motor vehicles accident and
pedestrians injury
✤ Wide range of injury from dead to minor injury
✤ Brainstem injury
✤ Cranial nerve deficit
✤ Spinal cord injury
✤ Cervical nerve roots injury
✤ Anterior spinal a., vertebral a. or carotid a. injury

Clinical findings✤ Steel rules of third at C1 spinal canal
✤ Odontoid process
✤ Spinal cord
✤ CSF space
✤ Cruciate paralysis
✤ Weakness of hands and arms with sparing of lower extremities
✤ True mechanism is still unknown but there are theories
✤ Selective damage to neural areas
✤ Injury to ventral corticospinal tracts

Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Basilar line of Wackenheim
✤ Line from posterior surface of clivus to caudal extension
✤ Normal line is attached to posterior tip of odontoid process and not altered by flexion and extension
Wackenheim’s line

Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Dens-basion interval
✤ Normal range is below 5mm in adult and 10mm in infant
✤ Unreliable due to wide range of variability in normal population

Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Craniovertebral relationships distances (Powers ratio)
✤ BC/OA ratio more than 1.0 indicate AOD (normal is 0.77)
✤ Unreliable in congenital anomaly or atlas fracture
Basion
Posterior arch of C1
Opisthion
Anterior arch of C1
Powers ratio

Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Basion-posterior axial line interval (BAI) and basion-dental interval (BDI) (Harris rule-of-12)
✤ Abnormal is more than 12mm (~95%)
✤ Universally acceptable and most accuracy
✤ BDI is unreliable in age below 13 years
BAI
BDI
Harris rule-of-12
Children atlantooccipital dissociation (AOD) By Pang and colleagues
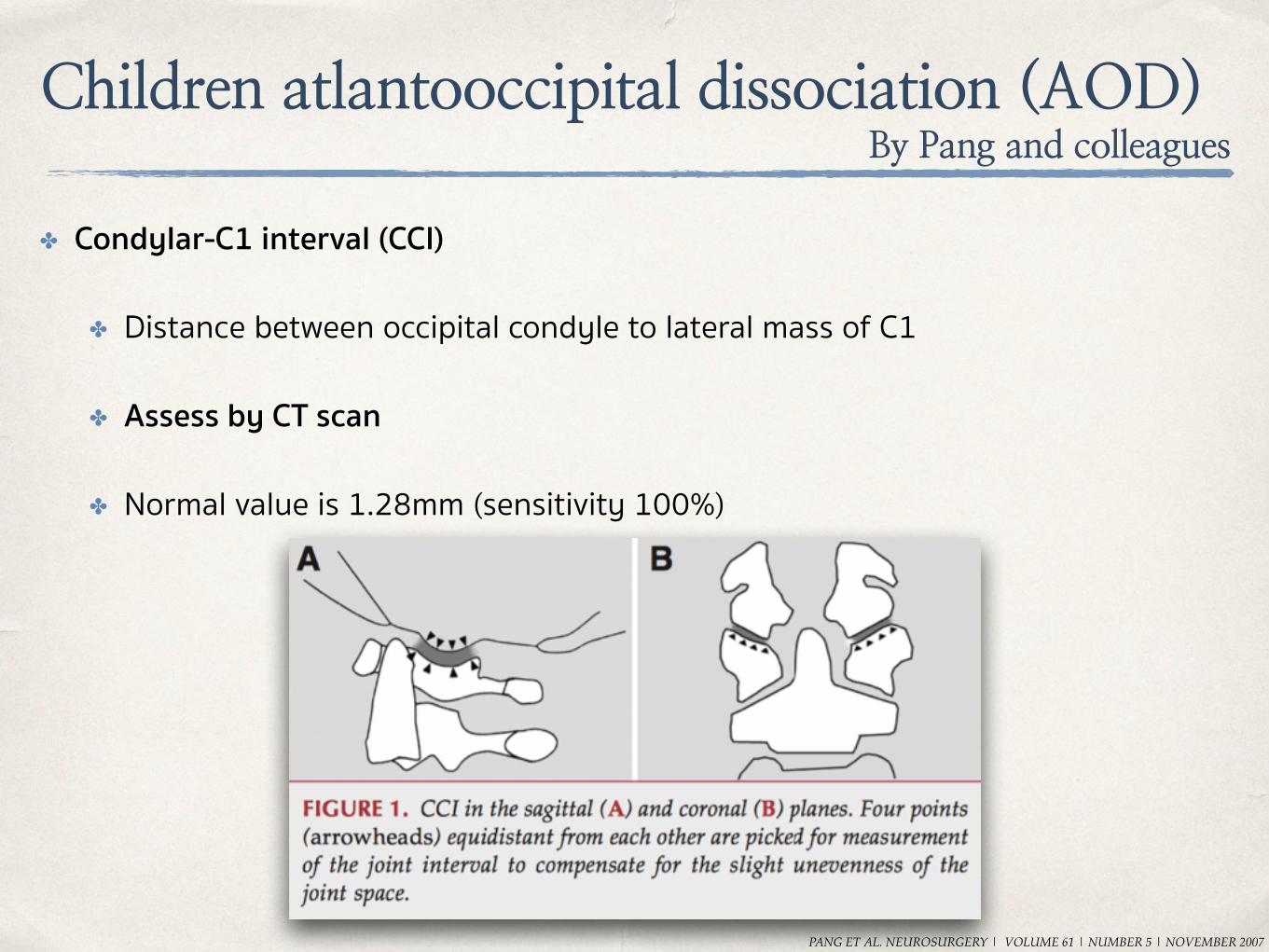
✤ Condylar-C1 interval (CCI)
✤ Distance between occipital condyle to lateral mass of C1
✤ Assess by CT scan
✤ Normal value is 1.28mm (sensitivity 100%)
PANG ET AL. NEUROSURGERY | VOLUME 61 | NUMBER 5 | NOVEMBER 2007
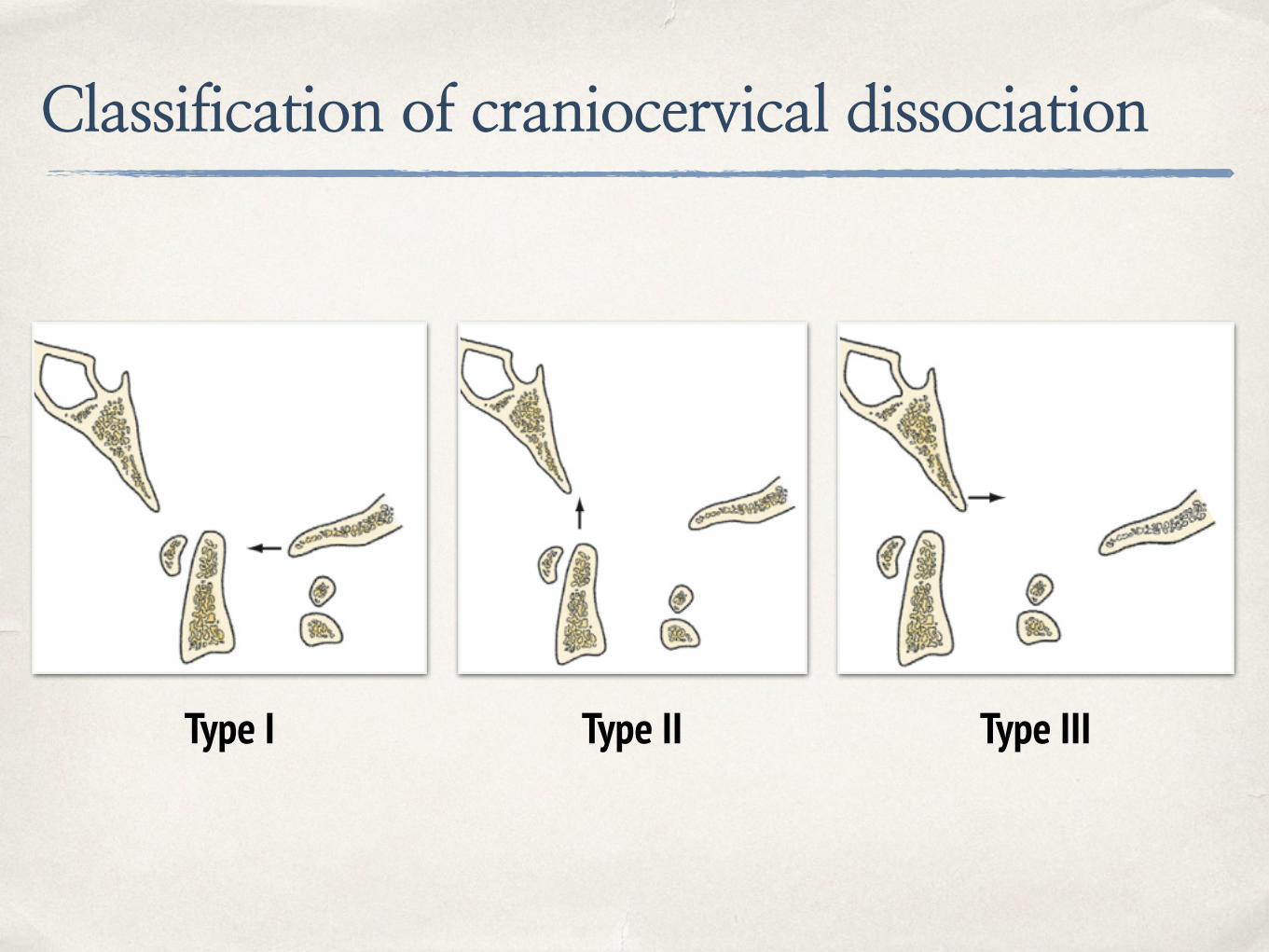
Classification of craniocervical dissociation
✤ Assess by lateral C-spine plain film or CT scan
✤ 3 types
✤ Type I : Anterior displacement of occiput to atlas
✤ Type II : Longitudinal distraction with seperation of occiput to atlas
✤ Type III : Posterior displacement of occiput to atlas
Classification of craniocervical dissociation
Type I Type II Type III
Treatment considerations
✤ Emergency considerations
✤ Awareness of craniocervical dissociation
✤ Cardiopulmonary support
✤ Spinal immobilisation
✤ Surgical removal of hematoma at CVJ (rare condition) if hematoma associated with neurological deficit

Treatment considerations
✤ Skull traction
✤ Recommended in patients of Type I and III dislocation with neurological deficit
✤ Fluoroscopic-guided for applied traction is recommended
✤ Traction weight below 5 lb.
✤ If clinical improved >> decrease weight to 1-2 lb. or halo vest applied
✤ Contraindication in Type II dislocation and rotatory subluxation

Treatment considerations
✤ Surgical management
✤ Posterior fusion of occiput to C2 is recommended in most cases of AOD
✤ Main injury is ligaments and stability cannot maintain after external fixation
✤ Should be done after medically stable
✤ Some surgeon recommended posterior fusion without skull traction first


Atlantoaxial Rotatory Subluxation and Transverse Ligament Injury

Anatomy and Biomechanics of Atlantoaxial joint
✤ Atlantoaxial joint is mainly functionally as neck rotation
✤ Facet joint of C1-2 is horizontal
✤ Stability of C1-2 joint is from ligamentous structures
✤ Transverse ligament : Prevent excessive translation of atlas to axis
✤ Alar ligament : Limit rotation of atlas on axis and secondary translation stabiliser (from transverse ligament)
✤ Vertebral artery runs in transverse foramenSchmidek & Sweet operative neurosurgical techniques
Diagnosis
✤ Sign and symptom of AARS
✤ “Cock-robin” position of neck : head tilted one side and rotated to contralateral side with flexion of neck
✤ Occipital pain from compression of occipital nerve or C2 nerve root
✤ Posterior fossa syndrome from stretching or kinking of vertebral arteries


Diagnosis
✤ Imaging
✤ Open-mouth plain film show asymmetrical of lateral of C1 to odontoid process
✤ Lateral plain film show lateral mass of C1 projecting anterior to odontoid process >> “wink” sign

Diagnosis
✤ Imaging
✤ Cervical spine CT is recommended for diagnosis of AARS
✤ Contrast injection for evaluating of vertebral artery
✤ MRI can be used for evaluating of transverse ligament and cord compression

Diagnosis
Classification system
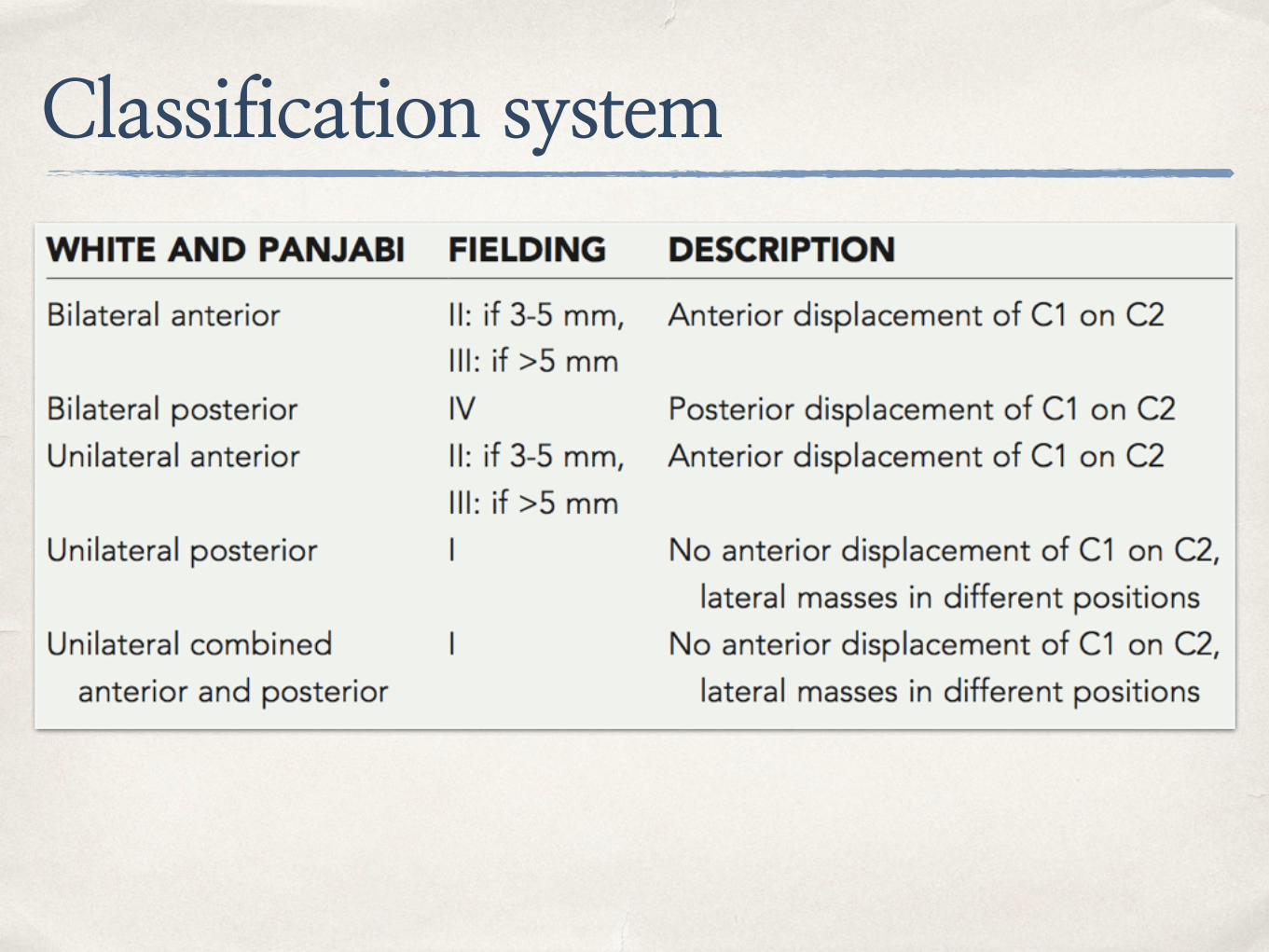
✤ Fielding system (1977)
✤ Type I : Intact odontoid and transverse ligament with disrupt of alar ligament
✤ Type II : Anterior translation of atlas on axis 3-5mm with disrupt of transverse ligament
✤ Type III : Anterior translation of atlas on axis > 5mm with disrupt of transverse ligament
✤ Type IV : Posterior displacement of atlas on axis and odontoid process is injured
Classification system
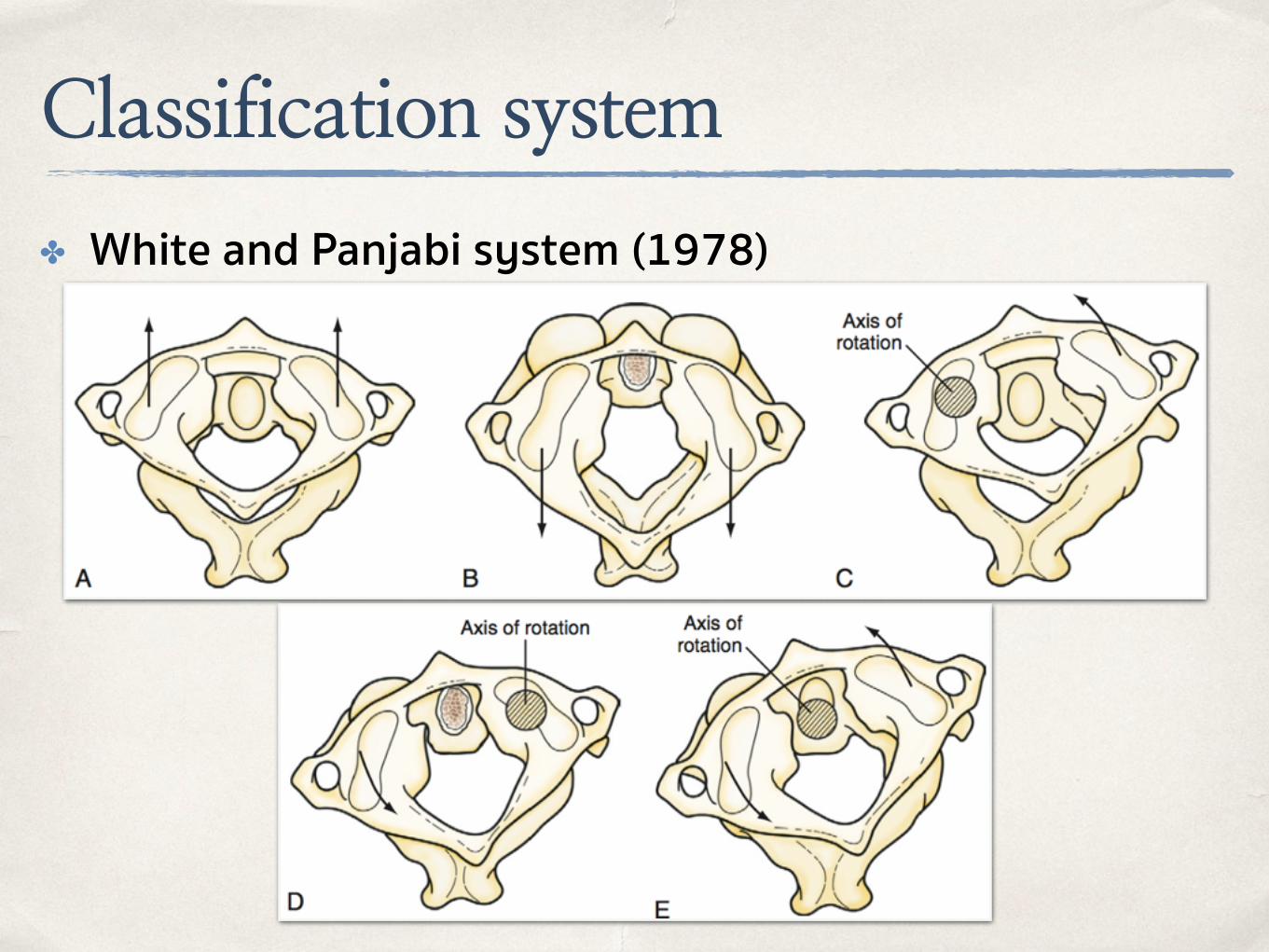
✤ White and Panjabi system (1978)
Classification system
Grisel’s Syndrome✤ Nontraumatic atlantoaxial subluxation (rare condition)
✤ Caused by infection process or head and neck procedure
✤ Edema (inflammation process) and relaxation of ligamentous structures
✤ In children with Down’s syndrome and Klippel-Feil syndrome increase risk of Grisel’s syndrome
✤ Management
✤ Reduction by cervical traction with muscle relaxant
✤ Antibiotic prophylaxis in high risk group
✤ Surgical fusion if failed conservative treatment

Management of AARS
✤ Conservative treatment
✤ Cervical traction by Gardner-Wells tong or halo ring with conscious sedation
✤ Bone fracture must be ruled out before traction application
✤ Patient with minor ligamentous injury should be placed in halo vest for 3 months
✤ Failure of conservative treatment or gross instability, surgical fusion should be done

Management of AARS
✤ Surgical treatment
✤ Reducible deformity >> only posterior fixation with fusion
✤ Irreducible deformity >> Anterior decompression with posterior fusion
✤ Anterior decompression
✤ Transoral route with soft tissue and longus colli muscles stripped from bone with/without anterior arch of C1 resection
Posterior C1-2 fusion techniques
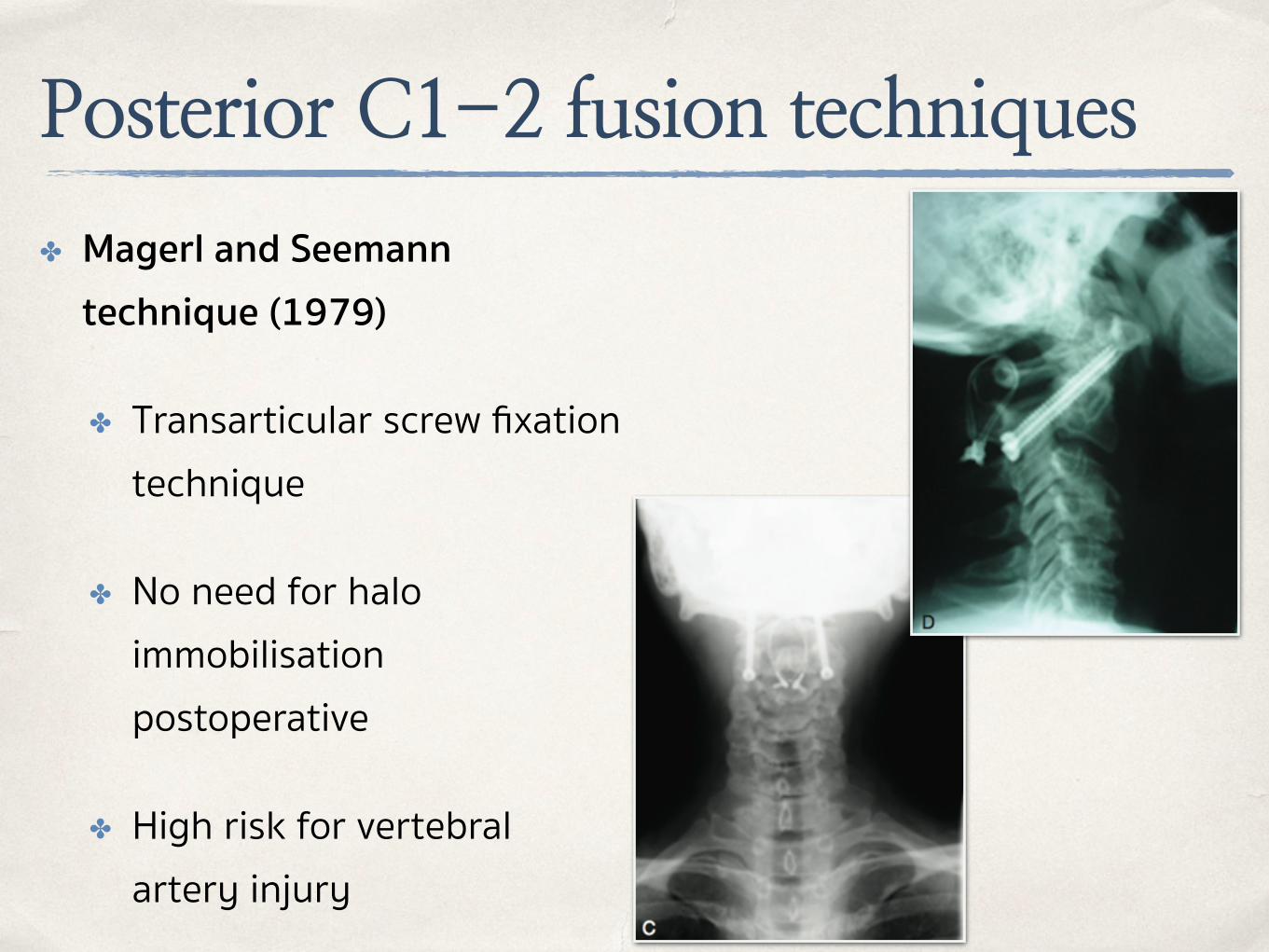
✤ Magerl and Seemann technique (1979)
✤ Transarticular screw fixation technique
✤ No need for halo immobilisation postoperative
✤ High risk for vertebral artery injury

Posterior C1-2 fusion techniques
✤ Harms and Melcher technique
✤ Lateral mass screw in C1
✤ Pedicular screw in C2
✤ Connect with rod

Posterior C1-2 fusion techniques
✤ Wright technique
✤ Translaminar fixation technique of C2
✤ Low risk for vertebral artery injury
C1
C2


Related Documents











