I The earliest reference to spinal cord injury (SCI) is found in the Edwin Smith Surgical Papyrus, written between 2500 and 3000 S.c., where it is described as "an ailment not to be treated" (1). Much has changed in spinal cord care over the centuries, partic- ularly in the last 50 years as it relates to increasing survival, life expectancy, community reintegration, and quality of life. Major advances include the specialized spinal cord centers of care, model SCI centers funded by the National Institute on Disability and Rehabilitation Research (NIDRR) in the United States De- partment of Education, establishment and growth of organiza- tions and journals dedicated to SCI care, and the development of the subspecialty of SCI medicine in 1998. This subspedalty ad- dresses the prevention, diagnosis, treatment, and management of traumatic and nontraumatic etiologies of spinal cord dysfunc- tion (2). The advances of the last 20 years alone have been dra- matic in terms of the understanding of the pathology of the ini- tial and secondary aspects of the injury, and the barriers that must be overcome to enhance recovery. Newer techniques to im- prove function and intervene at the cellular level for possible cure are being developed. These will further allow individuals I who sustain an SCI to be more independent in the future. I t EPIDEMIOLOGY OF TRAUMATIC SPINAL CORD INJURY I Incidence and Prevalence The National Spinal Cord Injury Statistical Center (NSCISC) 1 . database consists of data contributed by model.SCI systems (3). This database captures approximately 15% of all new traumatic 1 1 SOs that occur in the United States each year, and has been i used to develop an epidemiological profile (4-6). When com- I pr1red to population-based studies, persons in this database are I representative of all SCIs except that more severe injuries, per- t Sons of color, and injuries due to acts of violence are slightly ! overrepresented (4). ; The overall incidence of traumatic SCI in the U.5. has re- I mained relatively constant, at approximately 40 new cases per r million population, or just over 11,000 cases per year. The inci- j (l .. nce of SCI in the rest of the world is consistently lower than I in the U.S. (7). The prevalence of SCI is estimated to be approx- 250,00 persons by 20D.!, with the growth resulting from .mproved life expL'c.[,mcy rather than any increase in incidence. CHAPTER 79 Rehabilitation of Spinal Cord Injury Steven Kirshblum Age, Gender, Race, Marital, and Occupational Status The mean age at injury is 32.1 years, with the most common age at injury being 19 years (Table 79-1). Approximately 60% of all persons enrolled in the NSCISC database are 30 y.ears of age or younger at the time of injury. The percentage of new persons injured who are older than 60 has increased tq over 10% in the last decade. Men suffer traumatic SCI much more commonly than women, at a 4:1 ratio. State registries and NSCISC data re- veal higher incidence rates of SCI for African Americans than whites, which is predominately due to injuries that result from acts of violence. Approximately 50% of persons enrolled in the NSCISC database have never been married at the time of their injury. ApprOXimately 60% of persons enrolled between the ages of 16 and 59 are employed at the time of injury. Etiology and Time of Injury Motor vehicle crashes (MVCs) rank first (accounting for 38.5% of cases since 1990), followed by acts of violence (primarily gunshot wounds, or GSWs), falls, and recreational sporting ac- tivities. MVCs cause a lower percentage of cases among men than women while men have a higher percentage ofSCI due to GSW, diving mishaps, and motorcycle crashes. MVCs have de- creased, while SCI caused by GSWs almost doubled (from 12.7% to 24.1%) among men from the mid 1970s to the early 1990s, before declining slightly in subsequent years. Diving mishaps account for the majority of SCls due to recreational sports, followed by snow skiing, surfing, wrestling, and foot- ball. MVC is the leading cause of SCI until age 45; however, be- ginning with the 46- to 60-year-old age group, falls represent the leading cause of SCI. Recreational sports and acts of vio- lence decrease with advancing age as a cause of injury. Traumatic SCI occurs with greater frequency on weekends, with the greatest incidence on Saturday. Seasonal variation ex- ists, with peak incidence occurring in July followed closely by August and June. The seasonal pattern in incidence is more pronounced in the northern part of the U.5. where seasonal variation in climate is greatest.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
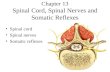
I The earliest reference to spinal cord injury (SCI) is found in the Edwin Smith Surgical Papyrus, written between 2500 and 3000 S.c., where it is described as "an ailment not to be treated" (1). Much has changed in spinal cord care over the centuries, particularly in the last 50 years as it relates to increasing survival, life expectancy, community reintegration, and quality of life. Major advances include the specialized spinal cord centers of care, model SCI centers funded by the National Institute on Disability and Rehabilitation Research (NIDRR) in the United States Department of Education, establishment and growth of organizations and journals dedicated to SCI care, and the development of the subspecialty of SCI medicine in 1998. This subspedalty addresses the prevention, diagnosis, treatment, and management of traumatic and nontraumatic etiologies of spinal cord dysfunction (2). The advances of the last 20 years alone have been dramatic in terms of the understanding of the pathology of the initial and secondary aspects of the injury, and the barriers that must be overcome to enhance recovery. Newer techniques to improve function and intervene at the cellular level for possible cure are being developed. These will further allow individuals I who sustain an SCI to be more independent in the future. I t EPIDEMIOLOGY OF TRAUMATIC SPINAL CORD INJURY I Incidence and Prevalence The National Spinal Cord Injury Statistical Center (NSCISC) 1. database consists of data contributed by model.SCI systems (3). This database captures approximately 15% of all new traumatic 11 SOs that occur in the United States each year, and has been i used to develop an epidemiological profile (4-6). When comI pr1red to population-based studies, persons in this database are I representative of all SCIs except that more severe injuries, pert Sons of color, and injuries due to acts of violence are slightly ! overrepresented (4). ; The overall incidence of traumatic SCI in the U.5. has re-I mained relatively constant, at approximately 40 new cases per r million population, or just over 11,000 cases per year. The incij (l ..nce of SCI in the rest of the world is consistently lower than I in the U.S. (7). The prevalence of SCI is estimated to be approx 250,00 persons by 20D.!, with the growth resulting from .mproved life expL'c.[,mcy rather than any increase in incidence. CHAPTER 79 Rehabilitation of Spinal Cord Injury Steven Kirshblum Age, Gender, Race, Marital, and Occupational Status The mean age at injury is 32.1 years, with the most common age at injury being 19 years (Table 79-1). Approximately 60% of all persons enrolled in the NSCISC database are 30 y.ears of age or younger at the time of injury. The percentage of new persons injured who are older than 60 has increased tq over 10% in the last decade. Men suffer traumatic SCI much more commonly than women, at a 4:1 ratio. State registries and NSCISC data reveal higher incidence rates of SCI for African Americans than whites, which is predominately due to injuries that result from acts of violence. Approximately 50% of persons enrolled in the NSCISC database have never been married at the time of their injury. ApprOXimately 60% of persons enrolled between the ages of 16 and 59 are employed at the time of injury. Etiology and Time of Injury Motor vehicle crashes (MVCs) rank first (accounting for 38.5% of cases since 1990), followed by acts of violence (primarily gunshot wounds, or GSWs), falls, and recreational sporting activities. MVCs cause a lower percentage of cases among men than women while men have a higher percentage ofSCI due to GSW, diving mishaps, and motorcycle crashes. MVCs have decreased, while SCI caused by GSWs almost doubled (from 12.7% to 24.1%) among men from the mid 1970s to the early 1990s, before declining slightly in subsequent years. Diving mishaps account for the majority of SCls due to recreational sports, followed by snow skiing, surfing, wrestling, and football. MVC is the leading cause of SCI until age 45; however, beginning with the 46- to 60-year-old age group, falls represent the leading cause of SCI. Recreational sports and acts of violence decrease with advancing age as a cause of injury. Traumatic SCI occurs with greater frequency on weekends, with the greatest incidence on Saturday. Seasonal variation exists, with peak incidence occurring in July followed closely by August and June. The seasonal pattern in incidence is more pronounced in the northern part of the U.5. where seasonal variation in climate is greatest. 1716 IV: SPECIFIC CONDITIONS TABLE 791. Epidemiology ofTraumatic Spinal Cord Injury (Since 1990) Incidence: Approximately 11 ,OOO/y Prevalence: 200,000-250,000 Average age: 32.1 Gender: 80.5% male ..... Etiology: Motor vehicle accidents (38.5%); followed by violence (primarily GSW)i falls; and sports Current Percentage Classification, 1. Incomplete tetraplegia (29.6%) 2. Complete paraplegia (27.3%) 3. Incomplete paraplegia (20.6%) 4. Complete tetraplegia (18.6%) ASIA, American Spinal Injury Association; GsW, gun shot wounds. . From Facts and figures: National Spinal Cord Injury Statistical Center. J Spinal Cord Med 2002;25:139-140. Associated Injuries SCls are often accompanied by other significant injuries. The most common include broken bones (29.3%), loss of consciousness (28.2%), traumatic pneumothorax (17.S%), and head injury sufficient to. affect cognitive or emotional functioning (11.5%) (4). The nature and frequency of these injuries is significantly associated with the etiology of the SCL For example, pneumothorax occurs more frequently with GSWs as compared with other causes of SCl. Neurological Level and Extent of Lesion Traumatic SCI most commonly causes cervical lesions (approximately 50%) followed by thoracic and then lumbosacral lesions. The C5 segment is the most common lesion level, followed by C4, C6, n2, C7, and L1 at the time of discharge from inpatient rehabilitation programs (7). At time of discharge from inpatient rehabilitation, 4S.6% of persons have neurologically complete injuries [American Spinal Injury Association (ASIA) A classification], followed by incomplete injuries of ASIA D, C, B, and E classifications (7). The etiology of injury is strongly associated with level and severity of the injury. Most recreational sports-related injuries, falls, and approximately 50% of MVCs result in tetraplegia, whereas acts of violence usually result in paraplegia. Neurologically complete injuries are more likely to occur as a result of acts of violence and among younger age grouPs. Thoracic injuries are the most likely to be neurologically complete while most lower level lesions are incomplete injuries. Cervical injuries are most commonly classified as either ASIA A or ASIA D. There has been a trend toward increased likelihood of cervical injury since 1994 (5). Marital and Occupational Status after Spinal Cord Injury The annual marriage rate after SCI is below average for the general population and the annual divorce rate is higher (S,9). ApprOXimately 25/., of persons with SCI are employed, but the percentage varies substantially by neurological level and extent of injury (10). The higher the level of and the more severe the injury, the less chance one has of returning to gainful ployment. Most employed individuals with SCI have ..un . .....rather part-time jobs. gredictors .of to work' elude bemg of younger age, male, white, Wlth a greater education and being employed at the time of injury- havI...l greater motivation to return to work; having a -:.. jury etiology; being able to drive; and greater time postin (11-13). Persons who return to work within the first year Ju;1 jury usually return to the same job with the same employ while those who return to work after more than 1 year .: elapsed usually acquire a different job with a different ell\ployer, often after retraining. Professional/technical and clerical/sales jobs are the most common. ! Discharge Placement !Model SCI systems have a higher percentage of persons discharged to the community relative to nonmodel system centers (6-14). Approximately 90% of -pe.rsons discharged from " model system are discharged to a private residence within the Icommunity; 5% being discharged to a nursing home, and 3% tdying during hospitalization. Predictors of nursing home placement include ventilator dependence, older age, cervical level of injury with non-useful motor recovery, being unmarried and unemployed, and having either Medicaid or health maintenance organization (HMO) insurance (15). There has been a significant trend toward an increasing percentage of persons being discharged to nursing homes since 1995 with the advent of shorter inpatient rehabilitation lengths of stay (15,16). Life Expectancy Life expectancy of persons with SCI has improved significantly over the past few decades but remains below normal. Predictors of mortality after injury include male gender, advanced age, ventilator dependence, injury sustained by an act of violence, high injury level (particularly C4 or above), neurologi .. cally complete injury, poor self-rated adjustment to disability, and having either Medicare or Medicaid third-party sponsorship of care (17,lS). Life expectancy estimates are typically based on neurological level of injury, degree of injury completeness, age at injury, and ventilator dependence. Estimates from the NSCISC database appear in Table 79-2. Causes of Death Diseases of the respiratory system are the leading cause of death following SCI, with pneumonia being the most common. Heart disease ranks second, followed by septicemia associated with pressure ulcers, urinary tract, or respiratory Illfections) and cancer. The most common location of cancer is the lung, followed by bladder, prostate, and colon/rectum. Pneumonia is by far the leading cause of death for . with tetraplegia while heart disease, septicemia, and sUlClde are more common among persons with paraplegia (19). Among persons with incomplete motor-function (ASIA D) at any neurological level, heart disease again ranks as the cause of death (24.1%), followed by pneumonia (11.0%). Whi e ' genitourinary disease (Le., renal failure) was the leading of death 30 years ago, this has declined dramatically, m05 likely due to improved care. 79: REHABILITATION OF SPINAL CORD INJURY 1717 TABLE 79-2. Life Expectancy (years) for Postinjury by Severity of Injury and Age at Injury (for Persons Surviving at Least 1-Year Postinjury) Motor Ventilator-Age at Injury NoSCI Functional at Any Level Para Low Tetra (CSCS) High Tetra (C1C4) Dependent at Any level 20 57.2 52.5 46.2 41.2 37.1 26.8 40 38.4 34.3 28.7 24.5 21.2 13.7 60 21.2 18.1 13.7 10.6 8.4 4.0 SCI, spinal cord injury. From Facts and figures: National Spinal Cord Inju ry Statistical Center. JSpinal Cord Med 2002;25:1 39-140. Lifetime Costs Data are available from the model system that include only the direct costs of the SCI, with the indirect costs (Le., lost wages, fringe benefits) not included in these estimates (6). Costs vary by year postinjury (first year versus subsequent years), by the level of injury, and severity of injury. Estimates of the total annual costs of SCI are $9.73 billion (12). This includes first-year direct costs estimated at $2.58 billion (based on 10,600 new cases), recurring direct costs of $4.55 billion, and $2.59 billion in lost productivity. ACUTE MEDICAL AND SURGICAL MANAGEMENT OF SPINAL CORD INJURY Aft.:r injury prompt resuscitation, stabilization of the injury, and avoidance of additional neurological injury and medical complications are of greatest importance. During the first seconds after SCI there is release of catecholamines with an initial hypertensive phase. This is rapidly followed by a state of spinal shock, defined as flaccid paralysis and extinction of muscle stretch reflexes below the injury level (20), although this may not occur in all patients. The cardiovascular manifestation of spinal shock is neurogenic shock, consisting of hypotension, bradycardia, and hypothermia. Hypotension is especially common in persons with a neurological level of injury (NU) at or above T6. The para sympathetic influences on the heart rate are unopposed in persons with a level of injury above Tl; thus heart rates are typically less than 60 per minute. Treatment of hypotension involves fluid resuscitation to produce adequate urine output of more than 30 cc/hour, however, in neurogenic shock further fluid administration must proceed cautiously, as the patient is at risk for neurogenic pulmonary eckma. The use of vasopressors is preferred in order to maintain a mean arterial blood pressure above 85 mm Hg, as this has been associated with enhanced neurological outcome (21). Bradycardia is common in the acute period in cervical spinal injury and may be treated, if symptomatic, with intravenous atropine, or prevented with atropine given prior to any maneuver that may cause further vagal stimulation (such as nasotracheal suctioning). In cases of severe bradycardia that may Jead to cardiac arrest; temporary cardiac pacing, as well as permanent pacemakers, may be required (22,23). While most ~ pronounced in the first few weeks after injury, by 6 weeks the . : rhythm usually returns to normal. Respiratory assessment is critical for acute SCI patients and should include arterial blood gases and measurement of forced vital capacity (VC) as an assessment of respiratory muscle strength. A VC of less than 1 L indicates ventilatory compromise, and the patient usually: ...requires assisted ventilation. Close serial assessments should be obtained for those with borderline values. A nasogastric tube should be inserted during the initial assessment period to prevent emesis and potential aspiration. Aspiration occurs in apprOXimately 5% of all SCI individuals, with a higher risk in patients over the age of 60, those who have undergone anterior approach spine surgery, or in the presence of a tracheostomy (24,25). A Foley catheter should be inserted for urinary drainage and will allow for an accurate assessment of output. . . Once the initial resuscitative measures have been taken, attention is turned to spinal realignment. A full initial neurological assessment should be documented, and provides a baseline on which changes in neurological status can be gauged. A standard trauma series includes cross-table laterals and anteroposterior views of the cervical and thoracolumbar spine. There is a 12% incidence of noncontiguous fractures, therefore once one fracture is identified careful inspection of the rest of the spine is imperative (26). Forty-seven percent of patients with spine trauma and 64% of patients with SCI have concomitant injuries, including head, chest, and long bone fractures (27). Computerized tomography (CT scanning) can help evaluate for the presence of cervical fractures most often at the Cl or C7 levels, provide information for surgical stabilization or decompression, and facilitate selection of appropriately sized hardware for operative stabilization. Magnetic resonance imaging (MRI) is helpful in cases in which a ruptured disc or epidural hematoma is suspected. In addition, an MRI is usually recommended prior to attempting closed reduction after cervical spine injury to identify disc herniation and its potential for neurological worsening with manipulation. Closed cervical reduction is accomplished with traction. The patient is placed in either a Stryker frame (Stryker Corp., Kalamazoo, MI) or a RotoRest bed (Kinetic Concepts Inc., San Antonio, TX). Gardner-Wells tongs or a Halo ring are applied. Once reduction is confirmed, 10 to 15 pounds of weight is used to maintain reduction. The patient can later be brought to the operating room for open stabilization. The indications for and types of spinal orthotic devices are discussed in Chapter 62. Stab wounds and GSWs generally do not produce spinal instability and therefore may not require surgical stabilization or orthotic immobilization. Plain films and CT are used not only to assess the extent of bony injury, but to provide information regarding the location and path of the bullet and bone fragments, and the extent of soft-tissue/vascular damage, in which case angiography would also be required. Objects that are em1 1 1718 IV: SPECIFIC CONDIT10NS bedded around the spinal canal (i.e., knife) should be left in place with removal performed in the operating room under direct visualization of the spinal canal. Bullets that pass through the abdominal viscera are treated with broad-spectrum antibiotics and tetanus prophylaxis (28,29). Bullets do not have to be removed, however, they can be removed if accessible while performing another surgical procedure. In most trauma centers IF III 3'r ' ba (lid; is given after an acute SCI. Mechanisms of action for MP include improving blood flow to the spinal "Cord, preventing lipid peroxidation, being a free radical scavenger, and having antiinflamInatory function. The National Acute Spinal Cord Injury Study (NASCIS) 2 demonstrated that MP given within 8 hours of injury (30 mg/kg bolus and 5.4 mg/kg/hour for 23 hours) marginally improves neurological recovery at 6 weeks, 6 months, and 1 year, although functional recovery was not clearly studied (30). The NASCIS 3 reported that if MP is initiated within 3 hours of SCI, it should be continued for 24 hours, whereas if MP is initiated 3 to 8 hours after SCI it should be continued for 48 hours (31). The administration of MP is not given beyond 8 hours from sel or to those with sel due to penetrating injuries as they have shown no benefit and their use is associated with a higher incidence of spinal and extraspinal infections (32,33). Because. of some limitations of the NASCIS studies and that these findings have not been consistently replicated, these specific recommendations have not been universally adopted (34-36). Sygen (GM-I) is a ganglioside that is present in high concentrations in the central nervous system (CNS) and forms the major component of cell membranes. An initial small study treating patients within 48 hours of injury for an average of 26 days found greater mean recovery at 1 year including some .. , ' , . \' proved recovery in muscles with no strength at entry of study (37). A subsequent large muIticenter study reported. trend toward improvement in neurological recovery in ASlA: ., : ' individuals at 26 weeks after being treated for 8 weeks. No nificant effect however was noted at the principal 26 weeks-in the total group of patients studied (38). Role of Surgery Animal model evidence suggests that early decompressive SUrgery leads to improved neurological recovery after SCI (39). However, the role and timing of cervical decompression has not been substantiated in patients with sel since most studies . have failed to demonstrate any significant neurological recovery among patients with complete or 'incomplete deficits (40). While there is no conclusive evidence in humans with sel supporting the benefit of "early" versus "late" surgery (40-42), select patients with incomplete Sel, such as those with cervical facet fracture dislocations, may experience improved neurological recovery if early decompreSSion is' performed within 8 hours (43). In the thoracic and thoracolumbar spine, surgery for patients with complete injuries has not been shown to have significantly improved neurological function after decompres.sion, while those with incomplete injuries do benefit from surgical intervention (44). The indication for emergent surgical treatment is progressive neurological deterioration, due to compression or an expanding epidural hematoma. Despite uncertainty regarding the appropriate timing of surgery, the safety of early surgery after sel has been validated, and is not TABLE 79-3. Glossary of Key Terms e i' t Key muscle groups: Ten muscle groups that are tested as part of the standardized spinal cord examination. Root Level MusdeGroup Root Level Muscle Group CS Elbow flexors L2 Hip flexors C6 Wrist extensors L3 Knee extensors C7 Elbow extensors L4 Ankle dorsi flexors CB Long finger flexors L5 Long toe extensor T1 Small finger abductors Sl Ankle plantarflexors Motor level: The most caudal key muscle group that is graded 3/5 or greater with the segments cephalad graded normal (5/5) strength. Motor index score: Calculated by adding the muscle scores of each key muscle group; a total score of 100 is possible. Sensory level: The most caudal dermatome to have normal sensation for both pinprick/dull and light touch on both sides. Sensory index score: Calculated by adding the scores for each dermatome; a total score of 112 is possible for each pinprick and light touch. Neurological level of injury (NU): The most caudal level at which both motor and sensory modalities are intact. Complete injury: The absence of sensory and motor function in the lowest sacral segments. Incomplete injury: Preservation of motor or sensory function below the neurological level that includes the lowest sacral segments. Skeletal level: The level at which, by radiological examination, the greatest vertebral damage is found. Zone of partial preservation (ZPP): Used only with complete injuries, refers to the dermatomes and myotomes caudal to the neurological level that remain partially innervated. The most caudal segment with some sensory or motor function defines the extent of the ZPP. From Kirshblum se, O'Connor K. Levels of injury and outcome in traumatic spinal cord injury, Phys Med Rehabil Clin North Am 2000;11 :1-27, '. associated with greater than expected complications (40,45). Early surgery may contribute to a shorter rehabilitation length stay and a similar frequency of medical complications than ,lOse undergoing surgery beyond 24 hours from injury (46). NEUROLOGICAL ASSESSMENT The most accurate way to document impairments in a person with a new SCI is by performing a standardized neurological examination as endorsed by the International Standards for Neurological Classification of Spinal Cord Injury Patients (47). These standards provide basic definitions of the most common terms used by clinicians in the assessment of SCI and describe the neurological examination. Key terms are defined in Table 79-3. The examination has two main components, sensory and motor. The information from this neurological examination is recorded on a standardized flow sheet (Fig. 79-1), and helps determine the sensory and motor index scores; the sensory, motor, and NU; the completeness of the injury; and to classify the impairment. For the sensory examination, there are 28 key dermatomes, each tested for pinprick and light touch on each side of the 79: REHABILITATION OF SPINAL CORD INJURY 1719 body. A 3-point scale (range 0 to 2) is used, with the face as the normal control point. Absent pinprick, a score 9f zero, is the inability to distinguish between the sharp and dull edge of the pin. Impaired pin sensation, a score of 1, is assignl,'!d when the patient can distinguish between the sharp and dull edge of the pin, but the pin is not felt as sharp as on the face. Normal or intact sensation, a score of 2, is assigned only if the pin is felt as sharp in the tested dermatome as when tested on the face. For light touch, a cotton tip applicator is used, and scored as follows: intact, same sensation as on the face; impaired, less than on the face; and absent, no sensation. To test for deep anal sensation, a rectal digital examination is performed. The patient is asked to report any sensory awareness, touch, or pressure, with firm pressure of the examiner's digit on the rectal wall. Deep anal sensation is recorded as either present or absent. The required elements of the, motor examination consist of strength grading of ten key muscles bilaterally: five in the upper limb (C5-Tl myotomes) and five in the lower limb (L2-S1) on each side of the body (see Table 79-3). Testing is performed with the patient in the supine position. is graded on a 6-point scale (range 0 to 5). Voluntary anal contraction is tested by sensing contraction of the external anal sphincter around the examiner's finger and graded as either present or absent. STANDARD NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY LIGHT PINMOTOR TOUCH PRICK R L KEY MUSCLES R l R L C2 ,....., C3 t.... C4 Elbow flexors CS Wrist extensors C6 Elbow extensors C7 Finger flexors (distal phalanx 01 middle linger) CB SENSORY KEY SENSORY POINTS . . 0= absent t impaired 2= normal /liT", not testable .. ' ..
... .0'" Finger abductors (little finger) !;,.::::1,. 0 = total paralysis 1 = palpable or viSible contraction r"! 2 = active movement, gravity eliminated ,.."" 3 = active movement, l,,,j against gravity " . . 4 = active movement. r:1 against some resistance 5 = active movement, :"'''1 against full resistance ,t:::J .' NT = not testable Ankle dorsiflexors Long toe extensors Ankle plantar flexors T1 T5 T6 TT91 0 T11 T12 L4 lS Sl Any anal sensation (Yes/No) [}[] = c:::J PIN PRICK SCORE (max: 112) TOTALS 0 + 0 = c:=:J MOTOR SCORE 1---...... = c:::J LIGHT TOUCH SCORE (max: 112) t::J c=::::J Voluntary anal contraction (VeS/No) !!.S (MAXIMUM) (50) (50) (100) (MAXIMUM) (56) (56) (56) (56) NEUROLOGICAL R L COMPLETE OR INCOMPLETE? ZONE OF PARTIAL R LEVEL SENSORY 0 0 JncompJste:::; Any sensory or motor functIOn in S4-S5 PRESERVATION SENSORY Cl 0 The. most caudal segmem MOTOR DD Partially innerv.'ed segments MOTOR Cl 0 With normallvndion ASIA IMPAIRMENT SCALE This form may be copied freely but should not be altered without permiSSion from the American Spinal Injury Association, Figure 79-1. American Spinal Injury Association (ASIA) neurological flow sheet. L 1720 IV: SPECIFIC CONDITIONS TABLE 79-4. Summary of the Steps in Classifying an Individual with a Spinal Cord Injury 1. Perform sensory exam in 28 dermatomes bilaterally for pinprick and light touch including the 54/5 dermatome and test for anal sensation on rectal examination. 2. Determine sensory level (right and left) and total sensory score. 3. Perform motor exam in the 10 key muscle groups including voluntary anal contraction on rectal examination. 4. Determine motor level (right and left) and motor index score. 5. Determine the neurological level of injury (NU). 6. Classify injury as complete or incomplete. 7. Categorize American 5pinallnjury Association (ASIA) Impairment Scale (A through E). 8. Determine zone of partial preservation if A51A A. From Kirshblum SC, Donovan WHo Neurologic assessment and classification of traumatic spinal cord injury. In; Kirshblum se, Campagnolo D, Delisa JE, eds. Spinal cord medicine. Philadelphia: Lippincott Williams & Wilkins, 2002:82-95. The NU is the most caudal level at which both motor and sensory modalities are intact on both sides of the body. The motor and sensory levels are the same in less than 50% of complete injuries, and the motor level may be multiple levels below the sensory level at I-year postinjury (48). In cases where there is no key muscle available (i.e., cervical levels at and above C4; T2-L1; and sacral levels S2-5), the neurological level is that which corresponds to the sensory level. The motor level and upper extremity motor index score better reflect the degree of function as well as the severity of impairment and disability, relative to the NU, after motor complete tetraplegia (48). Table 79-4 lists a summary of the steps to be followed in classifying an individual with an SCI (49). In 1982, the American Spinal Injury Association (ASIA) first published Standards for Neurological Classification of SCI, adopting the Frankel Scale (50). These standards were refined with the Frankel Scale being replaced in 1992 by the ASIA Impairment Scale (51), revised in 1996 (52), and again in 2000 (53), with reprinting in 2002 (47). The ASIA Impairment Scale describes five categories of SCI (Table 79-5). TABLE 79-5. American Spinal Injury Association (ASIA) Impairment Scale A= Complete; No motor or sensory function is preserved in the sacral segments 54-SS. B = Incomplete: Sensory but not motor function preserved below the neurological level and includes the sacral segments 54-SS. C = Motor function is preserved below the neurological level, and more than half of the key muscles below the neurological level have a muscle grade less than 3. D= Incomplete: Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more. E= Normal; Motor and sensory function are normal. Note: For an individual to receive a grade of Cor D, he/she must be incomplete, that is, have sensory or motor function in the sacral segments S455. In addition, the individual must have either (a) voluntary anal sphincter contraction or (b) sparing of motor function more than 3 levels below the motor level. From American Spinal Injury Association. Intemationa! standards for neuro!ogiC,1! ci.mification of spina! cord injury. Chicago: A5IA, 2002. A complete injury is defined as the absence of sensory motor function in the lowest sacral segments, and injury defined as preservation of motor function or SetlSaliciq. below the NU that includes the lowest sacral segmenli (termed sacral sparing). Sacral sparing is tested by light lQUch. and pin sensation at the anal mucocutaneous junction (54/5 dermatome), on both sides, as well as testing VOluntarY allal contraction and deep anal sensation as part of the rectal examj.. nation. If any of these are present, whether intact or impaired . individual has sacral sparing and therefore an inJury. There were three main revisions to the standards in 2000 (53). First there was clarification that for an individual to receive an ASIA classification of "motor incomplete" (ASIA Cor D), the patient must have either (a) voluntary anal sphincter contraction or (b) have sensory sacral sparing with sparing of motor function more than three levels below the motor level. Previously, an individual only needed to have sparing more than two levels below the motor level. Secondly, the zone ofpartial preservation (ZPP) should as the most caudal segment with some sensory or motor function bilaterally, rather than all areas spared. Lastly, in the 2000 revision, the Functional Independence Measure (FJM) was eliminated from the standards. Incomplete Spinal Cord Injury Syndromes Incomplete SCI syndromes include central cord, BrownSequard, anterior cord, conus medullaris, and cauda equina syndromes. The most common of the incomplete syndromes is central cord syndrome (CCS), which applies almost exclusively to cervical injuries and is characterized by motor weakness in the upper extremities greater than the lower extremities, in association with sacral sparing (54). Bladder dysfunction and varying sensory loss below the level of the lesion may also be present. CCS most frequently occurs in older persons with cervical spondylosis who suffer a hyperextension injury, but may occur in persons of any age and is associated with other etiologies, predisposing factors, and injury mechanisms. The postulated mechanism of injury involves compression of the cord both anteriorly and posteriorly by degenerative changes of the bony structures, with inward bulging of the flavum during hyperextension in an already narrowed spmal canal (55). CCS usually has a favorable prognosis. Recovery occurs earliest and to the greatest extent in the lower extremities, fol lowed by bowel and bladder function, proximal upper extremity, and then distal hand function. Prognosis for functional recovery of ambulation, activities of daily living bowel and bladder function is dependent upon the patIent.s age (less than or greater than 50 years of age), with a less ?ptlmistic prognosis in older patients relative to younger patients (56-58). Older, newly injured individuals however, with a classification of ASIA D tetraplegia, have a good prognosis for recovery of independent ambulation (58). Bro'Wn-Seqllard syndrome (BSS) involves a hemisection of spinal cord, consisting of asymmetric paresis with hypalgeSia more marked on the less paretic side and accounts for 2% to 4% of all traumatic seIs (59-61). In the classic presentation of aSS, there is (a) ipsilateral loss of all sensory modalities at the level of the lesion; (b) ipsilateral flaccid paralysis at the level of the ( lesion; (c) ipsilateral loss of position sense and vibration below the lesion; (d) contralateral loss of pain and temperature beloW the lesion; and (e) ipsilateral motor loss below the level of lesion. This is due to the crossing of the spinothalamic tracts In the spinal cord, as opposed to the corticospinal and dorsal columns that cross in the brainstem. The pure form of B5S is rare; Brown-Sequard plus syndrome (BSPS) is much more com(62) and refers to a relative ipsilateral hemiplegia with a relative contralateral hemianalgesia. Although BSS has traditionally been associated with knife injuries, a variety of etiologies, including those that result incIosed spinal injuries with or \\,ithout vertebral fractures may be the cause (62,63). Recovery usually takes place in the ipsilateral proximal extensors and then the distal flexors (64,65). Motor recovery of any extremity having a pain/temperature sensory deficit occurs before the opposite extremity and these patients may expect functional gait recovery by 6 months. Overall, patients Irith BSS have the greatest prognosis for functional outcome and potential for ambulation of the incomplete syndromes, as 7 5 ~ ; ' to 90% of patients ambulate independently at discharge from rehabilitation and nearly 70% perform functional skills and ADLs independently (60,62). Recovery of bowel and bladder function is also favorable. The anterior cord syndrome involves a lesion affecting the anterior two-thirds of the spinal cord while preserving the posterior columns. It may occur with retropulsed disc or bone fragments (66), direct injury to the anterior spinal cord, or with lesions of the anterior spinal artery which provides the blood supply to the anterior spinal cord (67). There is a variable loss of motor as well as pinprick sensation with a relative preservation of light touch, proprioception, and deep-pressure sensation. Patients usually have a 10% to 20% chance of muscle recovery (68). CONUS MEDULLARIS AND CAUDA EQUINA INJURIES The conus medullaris, which is the terminal segment of the dult spinal cord, lies at the inferior aspect of the L1 vertebrae. 'he segment above the conus medullaris is termed the epiCOIIIIS, consisting of spinal cord segments L4-S1. Lesions of the epiconus will affect the lower lumbar roots supplying muscles of the lower part of the leg and foot, with sparing of reflex function of sacral segments. The bulbocavernosus reflex and micturition reflexes are preserved, representing an upper motor neuron (UMN) or suprasacral lesion. Spasticity will most likely develop in sacral innervated segments (toe flexors, ankle plantarflexors, and hamstring muscles). Recovery is similar to other UMN SCIs. Conus medullaris lesions affecting neural segments 52 and below will present with lower motor neuron (LMN) deficits of the anal sphincter and bladder due to damage of the anterior horn cells of 52-54. Bladder and rectal reflexes are diminished Or absent, depending on the exact level and extent of the lesion. Motor strength in the legs and feet may remain intact if the nerve roots (13-52) are not affected (Le., "root escape"). Injuries below the L1 vertebral level usually affect the cauda equina or nerve rootlets supplying the lumbar and sacral segments producing motor weakness and atrophy of the lower extremities (L2-S2) with bowel and bladder involvement (52-54), 3.nd areflexia of the ankle and plantar reflexes. Often the patIent may have spared sensation in the perineum or lower extremities, but still have paralysis. In cauda equina injuries there IS loss of anal and bulbovernosus reflexes, as well as impotence. Cauda equina injuries have a better prognosis for recove : ~ 1110st likely due to the fact that the nerve roots are more resllIttlt to injury. Cauda equina injuries may represent a 01fopraxia or axonotmesis and demonstrate progressive re'ery over. a course of weeks and months. As the cauda .'lIina rootlets arehistologically peripheral nerves, regeneratIon can occur. Separation of cauda equina and conus lesions in clinical practice is difficult, because some of the clinical features of 79: REHABILITATION OF SPINAL CORD INJURY 1721 these lesions overlap. Pain is uncommon in conus lesions but is frequently a complaint in cauda equina lesions. Sensory abnormalities occur in a saddle distribution in conus lesions and, if there is sparing, there is usually dissociated loss with a greater loss of pain and temperature while sparing touch sensation. In cauda equina lesions, sensory loss occurs more in a root distribution and is not dissociated. THE FUNCTIONAL EVALUATION Numerous attempts have been made to correlate impairment with disability in SCI. The most conunonlyused disability measures in SCI are the Functional Independence Measure (FIM), the Modified Barthel Index (MBn, and the Quadriplegia Index of Function (QIF) (69-71). A review of the scales and their reliability and validity have been covered elsewhere (49, 72). The Craig Handicap and Reporting Technique (CHART) is an excellent measure of handicap (limitation of activity) for individuals with SCI (73,74). The FIM is highly predictive of hours of assistance received by individuals after discharge from inpatient rehabilitation, but the cognitive domain may be inappropriate for use in 5CI (75,76). While the FIM was added to the Standards in 1992, it was removed in the 2000 revisions (53). There is good correlation between a seven-item short version and the total motor FIM for persons with SCI (77). The QIF is more sensitive and a better indicator of motor recovery as compared to the FIM, since it can reflect small gains in function that parallel small strength gains (78). Another scale described is the Capabilities of Upper Extremity instrument (CUE) that measures upper extremity functional limitations in individuals with tetraplegia (79). To more precisely measure physical assistance and devices required for walking after 5CI, the Walking Index for. Spinal Cord Injury (WISCI) has been developed and has shown good validity and reliability (80,81). This is currently being used in research studies. PROGNOSTICATING RECOVERY AFTER TRAUMATIC SPINAL CORD INJURY Fundamental to predicting outcome is the knowledge and skill of performing an accurate examination based on the International Standards. The use of radiological and neurophysiological tests can aid and supplement in the diagnosis and prognosis for recovery (f$2-84). The keys to prognosticating recovery from traumatic SCI depend on the initial level of injury, the initial strength of the muscles, and most importantly, whether the injury is complete or incomplete as determined by physical examination. While the initial examination establishes a baseline, testing over a period of days and at 72 hours is superior to a single early examination (85). Vertebral displacement of less than 30% and age under 30 years at the time of injury is associated with improved recovery (86). No correlation has been found between other variables such as the degree of vertebral wedging or type of fracture. The etiology of the injury only plays a role in determining whether the injury is more likely to be neurologically complete or not (87). The types of injuries that are more likely to cause a complete injury include bilateral cervical facet dislocation, thoracolumbar f1exionl rotation injuries, and transcanal bull et locations. 1722 IV: SPECifiC CONDITIONS TABLE 79-6. Summary of Recovery in CompleteTetraplegia A. Patients (300/0-80%) regain one mOtor level from 1 wk to 1 y. B. At 72 h to 1 wk, recovery of the next m()tor level to at least 3/5 at 1 y depends on the motor level and initral . Approximately300/0-400k offirst 0/5 mllsdes 70%-90% of muscles 1 or 2/5' '....., ..... Presence of sensation at that leVel increases chances ofrecovery c. At 1 mo ... recovery at 1 y:. , . .' . Greater than 9S% of 1 or 2/5 fullsclesrec0vt:r to 3/5 50%...60% of first O/S muscles retover,to }IS. '. .'" Approximately 25% of first O/S muscle,s recover to < less than 10% of second 0/5 muscles recoverto l/5... . ' Approximately 1 % of seCond O/Srrtuscle,sfeeov.ers t031S D. The initial strength of the muscle, IS a achieving antigravity strength and its rate of recQvery.' .... . . E. The faster an initial 0/5 muscle starts torecQvksCime strength, the betterthe prognosis for recovery. ' .....' . , .,' ..... . >" '.F. Mostupper extremity recovery QCcurs duringthe first 6 /'nos; with the greatest rate of change during the 0105. G. Mostpatients with some initial PClwer plateau at .an earlier time .. and at a higher level than patients,withn!:,m()tor power. Motc:>r . recoVery can continue, with lesser seen In the secorid year, . espeCially for patients with initially 0/5 strength. From DitunnoJ. Flanders A, Kirshblum SC, et al. Predicting outcome in traumatic spinal cord injury. In: Kirshblum SC, Campagnolo 0, Delisa jE, eds. , Spinal cord medicine. Philadelphia: llppincott WUllams & Wilkins, 2002:108-122. Complete Tetraplegia It has frequently been stated that patients with complete cervical lesions recover one root level of function (SS). Table 79-6 lists certain generalizations regarding recovery patterns in patients with complete tetraplegia. The initial strength of a muscle is a significant predictor of achieving antigravity strength at the level caudal to the NU, as well as the rate of recovering antigravity strength (S9,9O). The faster recovery begins the greater the chance of recovering anti gravity strength (91). Recovery at the C4 level to the CS level, both motor and sensory, may be less and slower than at the lower cervical segments, especially if there is initially no strength at the CS myotome (76,92). Most upper extremity (UE) motor recovery occurs during the first 6 months after injury; with the greatest rate of change during the initial 3 months. Overall, the mean total motor score improvement for persons with complete tetraplegia between 1 and 6 months postinjury is 6.6 4.7; between 1 month and 1 year, S.6 4.7; and during the. second year, 1.7 1.9 (90). In patients with no motor strength at the first caudal level, recovery may continue for up to 2 years after injury (92). Only a small percentage of subjects have motor recovery below the first caudallevel from the NU (90). . Incomplete Tetraplegia Persons with incomplete tetraplegia have a better prognosis for recovery. UE motor recovery is approximately twice as great as in complete tetraplegia, with the potential for varying degrees of lower extremity (LE) motor recovery and functional ambulation. For patients who are sensory incomplete initially, the prognosis for motor recovery is more favorable in those with sparing of pin sensation rather than light touch sensation alone. Studies using the Frankel Scale found that for Frankel B patients with pin sensation initially intact, the prognosis for ombul'tion is 66% to89%, while fo, th"", with only I:' intact it was 11% to 14% (93-95). The basis of a more favo' outcome for pinprick sparing in the initially sensory ir. plete patient may be explained by the close anatomical t,,: . tionship of the motor tracts (mediated through the / .....cospinal tract), which are just dorsal to the sensory (lateral spinothalamic tract) carrying pain and tern' " fibers. A sensory incomplete motor complete patient .' at 1 month may still regain LE muscle recovery if bila ' sacral pin sensation is present, although the prognosis for coI:' munity ambulation is poor (96). Functional and neurolosiCil recovery is more favorable for patients with an initial motoriit!: complete injury (93-98).,i For UE motor recovery, the total motor score improvemerit from 1 month to 1 year is 10.6 6.9, with improvement in second year of 1.1 2.3 (96). The majority of functional ery is within the first 6 months after injury and the early' appearance of motor function suggests a better functional outcome (85,94,96,98). A greater percentage of key muscles recover antigravity strength orbetteri,as well as earlier, distal to the NU in individuals with motor incomplete tetraplegia thanJIL those with motor complete injuries (99,100). The mean LE motor recovery in incomplete tetraplegics is 13.5 7 from 1 month to 1 year and 1.8 3.1 in the second year (96). Motor recovery in the UE and LE occur concurrently, rather than sequentially. Complete Paraplegia Recovery from injuries resulting in paraplegia has not been studied to the same degree of tetraplegia. For persons complete injury with a NU at TS or above, Waters and \ leagues found that none regained any LE motor function. Tht: potential for LE motor recovery improves with lower initial neurological levels of injury; 15% of patients with an NU between T9-Tll and 55% of those with an initial NU below T12 gain some recovery. Most movement gained is in the proximal LE musculature (101). This improvement may represent recovery of partially injured lumbar roots or "root escape" (102). Incomplete Paraplegia Individuals with incomplete paraplegia have the best prognosis for LE motor recovery and ambulation (103,104). Eighty percent of individuals with incomplete paraplegia regain antigravity hip flexors and knee extensors at 1 year. Individuals with no LE strength at 1 month may still show significant return by 1 year. Conversion from Complete to Incomplete Status While it has been reported that up to 10% of patients with an initial Frankel A classification can progress to Frankel D or E, Maynard and associates prospectively demonstrated that jects with this degree of change had sustained closed head 111juries with cognitive impairment and were incorrectly initially diagnosed as Frankel A (105). Model systems data report that up to 16% of initially neurological complete (Frankel or A) patients improve at least one classification grade, from 1Il0 tial early examination to the I-year follow-up, but only up . 5.8% improve to grade C and 3% improve to grade D .. , Marino and colleagues reported a small difference when using the Frankel and the ASIA Impairment scales (106). . Between 4% to 10% of patients may undergo late converS1()ll (after 30 days) from complete to incomplete status which haS bet' n reported to occur years after injury (90,107,108). Motor re-seems to be slightly improved and some, usually non-LE recovery, may take place. the Effect of Reflexes fhe presence of spinal shock may play a role in prognosis; fOr the same degree of SCI the presence of spinal shock implies a lJ10re rapid evolution of injury and a worse prognosis (109). In individual lesions, especially in high level cervical SCI, the lJ10st distal sacral reflexes, including the bulbocavernosus (BC) JIld anal wink, may remain intact. The order that reflexes return in the postinjury period may help prognosticate outcome (110). The lack of the BC reflex ISJ-l roots) or the anal reflex (S2-4 roots) after the acute period 124 to 72 hours) suggests injury to the conus medullaris or cauda equina (Le., LMN injury). As such, prognosis regarding recovery and also the potential use of rehabilitation intervention (e.g., electrical stimulation) can be determined. The delaved plantar response, which may be the first of all reflexes to return, occurs within hours or days following SCI, and shows a high correlation with complete injuries and a poor prognosis for LE motor recovery and function (ambulation) {no,111). Magnetic Resonance Imaging in Predicting Outcome Numerous studies have shown a direct correlation between the appearance of the spinal cord on MRI and the degree of functional deficit at the time of injury and the capacity for neuro1 recovery. Overall, the findings on MRI that correspond to a more severe initial injury and have a poor prognosis for neurolOgical recovery include the presence and length of hemorrhage, the length of spinal cord edema, and spinal cord compression. An intramedullary hemorrhage equates with a severe initial neurological deficit, most commonly ASIA A (complete) injury on clinical examination, and carries a poor prognosis (83,112-114). The location of the hemorrhage corresponds anatomically to the level of the neurological injury. If no hemorrhage is seen on initial MRI, these individuals usually have an incomplete lesion by clinical exam and have a better prognosis for motor and functional recovery. Cord edema alone is associated with mild to moderate initial deficits. Cord edema that extends for more than the span of one vertebral segment is associated with a more severe initial injury than smaller areas of edema (114,115). In the chronic stage after SCI, persons with persistent signal Changes in their spinal cord on follow-up MRI exams demonstrrd injury patients: effects of PES exercise. I ReIUlbiI Res Dev 1994; 31:50-"], BeDell KK Scremin AME, Pere\l KL, et al. Effects of functional electrical stimulatiCJ)1-induced lower extremity cycling on bone density of spinal cordinjured patient. Am' Phys Med Rehabill996;75:29-34. :CS. Klose KJ, Ganz W, et al. Bone mineral density after bicycle er,o:"metry training. Arch Phys Med RehabiI 1990;71:207-279. .lo:," Rdwbil199'J;80:1166. 391. Olenik LM. Laskin H, Bumham R. et aL Efficacy of rOWing, backward wheeling and isolated scapular retr,lctor exercise as remedial strength activities 1750 IV: SPECIFIC CONDITIONS for wheelchair users: application of electromyography. Paraplegia 1995;33: 148-152. 392. Cums KA, Tyner TM, Zachary L, et al. Effect of a standard exercise protocol on shoulder pain in long-term wheelchair users. Spinal Cord 1999;37:421429. 393. Robinson MD, Hussey RW, Ha CY. Surgical decompression of impingement in the weight bearing shoulder. Arch Phys Med Rellabil 1993;74:324-327. 394. Gellman H, Chandler D, Petrasek J, et al. Carpal tunnel syndrome in paraplegic patients. I Bone It Surg (Am) 1988;70:517-519. 395. Davidoff G, Wemer R, Waring W. Compressive mononeuropathies of the upper extremity in chronic paraplegia. Paraplegia 1991;29:17-24. 396. Nemchausky BA, Ubilluz RM. Upper extremity neuropathies in patients with spinal cord injuries.J Spinal Cord Med 1995;18:95-97. 397. Kirshblum S, Druin E, Planten K. Musculoskeletal conditions in chronic spinal cord injury. Tap Spinal Cord Inj Rehabil1997;2:23-35. 398. Yerzierski RP. Pain following spinal cord injury: the clinical problem and experimental studies. Pain 1996;68: 185-194. 399. Siddahl pJ, Taylor DA, McClelland JM. et al. Pain report and the relationship of pain to physical factors in the first 6 months following spinal cord injury. Pain 1999;81:187-199. . 400. Demirel G, Ylhnaz H, Gencosmanoglu B, et al. Pain following spinal cord injury. Spinal Cord 1998;36:25-28. 401. Davidoff G, Guarradni M, Roth E, et a!. Trazodone hydrochloride in the treatment of dysesthetic pain in traumatic myelopathy: a randomized, double-blind placebo-controlled study. Pain 1987;2:151-161. 402. Putzke ID, Richard JS, DeVivo MJ. Preceptors of pain 1 year post-spinal cord injury. I Spinal Cord Med 2001;24(1):47-53. 403. Siddall PI, Loeser JO. Pain following spinal cord injury. Spinal Cord 2001; 39:63-73. 404. Stormer S, Gemer HJ, Gruninger W, et al. Chrome pain/dysaethesiae in spinal cord injury patients: results of a multicentre study. Spinal Cord 1997; 35:446-455. 405. Turner JA, Cardenas DD, Warms CA, et al. Chronic pain associated with spinal cord injuries: a community survey. Arclz Phys Med Rehab 200182(4): 501-509. 406. Siddall pJ, Yezierski RP, Loeser JD. Pain following spinal cord injury: clinical features, prevalence, and taxonomy. IASP Newslell 200()-,3-7. 407. McAdoo DJ, Xu GY, Roback G, et a!. Changes in amino add concentrations over time and space around an impact injury and their diffusion through the rat spinal cord. Exp Neuro/1999;159:538-544. 408. Eide PK, Stubhaug A, Stenehjem AE. Central dysesthesia pain after traumatic spinal cord injury is dependent on N-methyl-D-aspartate receptor activation. Neurosurgery 1995;37(6):1080-1087. 409. Hao JX, et at. Baclofen reverses the hypersensitivity of dorsal horn wide dynamic ranged neurons to mechanical stimulation after transient spinal cord ischemia: implications for a tonic GABAergic inhibitory control of myelinated fiber input. I NeurophysioI1992;68:392-396. 410. Ciom B, Meglio M, Pentimalli L, et al. Spinal cord stimulation in the treatment of paraplegic pain. I Neurosurg 1995;82:35-39. 411. Cole J, lIlis L, Sedgwick E. Intractable pain in spinal cord injury is not relieved by spinal cord stimulation. Paraplegia 1991;20:167-172. 412. Vaarwerk I, Staal M. Spinal cord stimulation in chronic pain syndromes. Spinal Cord 1998;36:671-682. 413. Oavis R, Lentini R. Transcutaneous nerve stimulation for treatment of pain in patients with spinal cord injury. Sllrg NeuroI1975;4:100-101. 414. Friedman AH, Nashold SS Jr. OREZ lesions for relief of pain related to spinal cord injury. f Neurosurg 1986;65(4):465-469. 415. To TP, Lim TC, Hill sr, et at. Gabapentin for neuropathic pain following spinal cord injury. Spinal Cord 2002;40(6):282-285. 416. Tai Q, Kirshblum 5, Tai Q, Kirshblum se, Chen B, Millis S, et a!. Treatment of neuropathic pain with gabapentin in spinal cord injury. JSpinal Cord Med 2002;25:100-105. 417. Warms CA, Turner JA, Marshall HM, et al. Treatments for chronic pain associated with spinal cord injuries: many are tried, few are helpful. Clill I Pain 2OO2;18(3):1S4-163. . 418. Biering-Sorensen F, Bohr H. Bone mineral content of the lumbar spine and lower extremities years after spinal cord lesion. Paraplegia 1988;26:293-301. . 419. Kiralti B, Smith A, Nauenberg T, et al. Bone mineral and geometric changes through the femur with immobilization due to spinal cord injury. I Rehabil Res Dev 2000;37:225-233. 420. Chow Y, Imnan C, Pollintine P, et at. Ultrasound bone densitometry and dual energy x-ray absorptiometry in patients with spinal cord injury: a cross sectional study. Spinal Cord 1996;34:736-741. 421. Needham-Shropshire B, Broton J, Klose K, et al. Evaluation of a training program for persons with SCI paraplegia using the Parastep 1 ambulation system: .Part 3. Lack of effect on bone mineral density. Arc" P"ys Med Rd,abil 1997;78:799-803. 422. Belanger M, Stein R, Wheeler G, et al. Electrical stimulation: can it increase muscle strength and reverse osteoporosiS in spinal cord injured individuals. Arcll PI,y. Med Rellabil2000;81:1090-1098. 423. Mohr T, Podenphant l, Biering-Sorensen F, et al. Increased bone mineral drnsity after prolonged electrically induced cycle training of paralyzt>d limbs in spinal cord injured man. CalcifTisslllt1997;61:22-25. 424. Harktopp A, Murphy R, Mohr T, et al. Bone fracture during electrical stimulation of the quadriceps in a spinal cord injured subject. Arcll P1Iys Med Re/IQ1>iI1998;79:1133-1136. 425. Nance P, Schryvers 0, Leslie W, et al. Intravenous pamidronate bone density loss after acute spinal cord injury. Arcll Phys Med 1999;80:243-251. 426. Luethi M, Zehnder Y, Michel D, et al. Alendronate in the treatment loss after spinal cord injury: preliminary data of a 2 year rartclorniz...t trolled trial in 60 paraplegic men. J Bone Mill Res 2oo1;16[Suppl (abst). . 427. Ragnarsson KT, Sell GH. Lower extremity fractures after spinal cord a retrospective study. Arch Phys Med Rellilbi/1981;62:416--423. .-,,;:. 428. Frisbie JH. Fractures after myelopathy. I Spitllll Cord Med 429. Garland DE. Pathologic fractures and bone mineral density at the __., ... Spinal Cord Med 1999;22:335. 430. Freehafer AA. Limb fractures in spinal cord injury. Arch Phys Med Reh4i . 1995;76:823-827. . 431. Rossier AB, Foo 0, Shillito J, et al. Post-traumatic syringomyelia: clinical electrophysiological studies, syrinx protein and results of conservative and operative treatment. Brain 1985;108:439-461. 432. El Masry W, Biyani A. Incidence, management, and outcome of post.traumatic syringomyelia.J Neurol Nellr05l1rg Psychiatry 1996;60:141-146. 433. Perrouin-Verbe B, Lenne-Aurier K, Robert R, et a!. Post-traumatic syringo. myelia and post-traumatic spinal canal stenosis: a direct relationship: review of 75 patients with a spinal cord injury. Spinal Cord 1998;36:137-141 434. Sett P, Crockard H. The value of magnetic resonance imaging (MRI) in !he follow-up management of spinal injury. Paraplegia 1991;29:396-410. 435. Backe HA, Beta RR, Mesgarzacfeh M; et'al;' Post-traumatic spinal cord cysts evaluated by magnetic resonance imaging. Paraplegia 1991;29:607-612. 436. Abel R, Gerner HJ, Smit C, et a!. Residual deformity of the spinal canal in patients with traumatic paraplegia and secondary changes of the spinal cord. Spinal Cord 1999;37:14-19. 437. Nogues MA, Gene R, Encabo H. Risk of sudden death during sleep in sy_ ringomyelia and Syringobulbia. JNeurol Nellros1trg Psycltiatry 1992;55:585589. 438. Wang D, Bodley R, Sett P, et al. A clinical magnetic resonance imaging study of the traumatised spinal cord more than 20 years following injury. Paraple gia 1996;34:65-81. 439. Little lW, Robinson LR, Goldstein B, et al. Electrophysiologic findings in posttraurnatic syringomyelia: implications for clinical management. JAm Paro Soc 1992;15:44-52. 440. Nogues MA, Stalberg E. Electrodiagnostic findings in syringomyelia. Muscle Nerve 1999;22:1653-1659. 441. Sgouros S, Williams B. Management and outcome of posttraumatic sy ringomyelia. JNeur05nrg 1996;85:197-205. 442. Dautheribes LW, POintillart V, Gaujard E, et al. Mean term follow-up of a series of posttraumatic syringomyelia patients after syringo-peritoneal shunting. Paraplegia 1995;33:241-245. 443. Levi ADO, Sonntag VKH. Management of posttraumatic syringomyelia using expansile duraplasty. Spine 1998;23:128-132. 444. Batzdorf U, KJekamp J, Johnson JP. A critical appraisal of syrinx cavity shunting procedures. I NellrOSllrg 1998;89:382-388. 445. Grant R, Handley OM, Lang 0, et al. MRI measurement of the syrinx size before and after operation. JNeurol Neurosurg Psychiatry 1987;50:1685-1687. 446. Waters RL, Muccitelli LM. Tendon transfers to impro\'e function of patienl5 with tetraplegia. In Kirshblum SC, Campagnolo D, DeLisa JE, t>ds. Spilllll cord medicine. Philadelphia: Lippincott Williams & Wilkins, 447. Pedretti LW. Occupational performance: a model for practice in dysfunction. In: Pedretti LW, ed. Occupational therapy practice skillsJor pltysrcal dysfunction, 4th ed. St. Louis: Mosby, 1996;3-12. 448. Mc Dowell CL, Moberg EA, House JH. The Second International Conference on Surgical Rehabilitation of the Upper Limb in Traumatic Quadriplegia. J Hand Surg 1986;l1A:604--608. . 449. Moberg E, Freehafer AA, Lamb DK, et al. International federation eties for surgery of the hand. A report from the committee on spinal injunes 1980. Scalld f Relzabil M,ti 1982;14:3-5. . 450. Moberg E. Surgical rehabilitation of the upper limb in tetraplegia. ParaplfglQ 1990;28:330-334. 451. Freehafer AA. Tendon transfers in patients with cervical spinal cord injury. 1 Hand Surg 1991;16A:804-809. . 452. Johnson DL, Gellman H, Waters RL, et al. Brachioradialis transfer for wnst extension in tetraplegic patients who have fifth-cervical-level neurological function. I BOlle IOi"t Sllrg 1996;78A:1063-1067. 453. Raczka R, Braun R, Waters RI.. Posterior deltoid-to-triceps transfer in quadriplegia. Cllin OrtllOp 1984;187:163-167. . 454. Revol M, Briand E, Servant JM. Biceps-to-triceps transfer in tetraplegIa. The medial route. JHallti SurS (Br) 1999;24(2):235-237. . . _ 455. Kuz lE, Van Heest AE, HouseJH. Biceps-to-triceps transfer in tetrapleglcpa, tients: report of the medial routing technique and follow-up of three case> Ha/ld SlIrg (Am) 1999;24(1):161-172. .' 456. Moberg E. TIle 1l1'1','r lilllb ill t,'tTllI'/C;;:ia. a "1/ClI' al'proacll" /() ';/IIXical ",lmMIIIl tiOIl. Stuttgart: G"orge Thieme, 1978. . . 457. Moberg EA.TIu., present state ofsurgical rehabilitation for the upper Iim td:aplegia. Parlll'i.'sia1987;25:351-356. . ce458. Rel"er TV, Waters RI.. Long term follmv up of the :Yloberg key gnp pro dure./ f/1l1I,1 SlIr)11981>;11 A:724-728. 459. W.1t"r R. K, Grabofi 5, et al. I3mchiomdi.11i, tn ne",r p,)lIids ionsgUS rgtendon transfer for active lateral pinch in tht' ,Halla u 1985;lOA(3):385-391. I f!tO House JH, Shannon M. Restoration of strong grasp and lateral pinch in . tetraplegia: a comparison of two methods of thumb control in each patient. I Hand Surg 1985;IOA(I):22-29. Gansel J, Waters RL, Geilman H. Pronator teres to flexor digitorum profun> dus transfer in quadriplegia. I BOlle loint Surg 1990;72A(3):427-432. . , la 113 SD, Gellman H, Waters R et at Single-stage reconstruction of key . pinch and extension of the elbow in tetraplegic patients. J Bone /t Surg 199-1;76(A):1451-1456. fttl. Gellman H, Kan D, Waters RL, et al. Rerouting of the biceps brachii for paraIvlic supination contracture of the forearm in tetraplegia due to trauma. / Borl 11 Surg 1994;76A:398-402. Gellman H. The hand and upper limb in tetraplegia. Curr Or/hop 1991;5: 233-238. Waters RL, Stark LZ, Gubemick I, et al. Electromyographic analysiS of brachioradialis to flexor pollicis longus tendon transfer in quadriplegia. / Hand Sltrg 1990;15A:335-339. -167. Pe(kham PH, Keith MW, Kilgore Kt, et al. Implantable Neuroprosthesis Re,earch Group. Efficacy of an implanted neuroprosthesis for restoring hand grasp in tetraplegia: a multicenter study. Arch Phys Med Rehabil 2001;82: 1380-1388. Wl. Mulcahay MJ, Beta RR, Smith BT, et al. Implanted functional electrical stimulation hand system in adolescents with spinal injuries: an evaluation. Arch Pity> Med Rehabill997;78:597-607. WJ. Hobby J, Taylor PN, Esnouf J. Restoration of tetraplegic hand function by use of the neurocontrol freehand system. JHand Surg (Br) 2001;26:459-464. 4i\J. l
Related Documents