264 Consult Management Anthony Zollo MD (Lufkin, Texas) Philip B. Irwin, PA-C (Gainesville, Florida) Ako D. Bradford, M.D. (Amarillo, Texas) Harold D. Bonds MT (ASCP) SC (Jackson, Mississippi)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

264Consult Management
Anthony Zollo MD (Lufkin, Texas)Philip B. Irwin, PA-C (Gainesville, Florida)Ako D. Bradford, M.D. (Amarillo, Texas)
Harold D. Bonds MT (ASCP) SC (Jackson, Mississippi)

2
Consult Management: A Tool for Improved Performance
Anthony Zollo, MDChief Medical Officer
Charles Wilson Outpatient ClinicLufkin, Texas
Michael E. DeBakey VAMCHouston, Texas
South Central VA Health Care Network

3
“Physicians who meet in consultation must never quarrel or jeer at one
another”
HippocratesPrecepts VIII

4
A Primary Care Visit: A to-do list

5
Before seeing the patient
• Review vital signs and today’s nursing assessment
• Review recent lab, x-ray, other results
• Review all notes from other clinicians since last visit
• Review any outside records

6
During the visit with the patient
• Greet the patient• Take a focused history and review of systems• Perform focused physical exam• Satisfy all due clinical reminders• Review medications and renew, change, add,
delete as needed• Communicate and provide patient education
on diagnoses, prognosis, key issues and changes in therapy, medications or instructions
• Elicit from the patient and address remaining unaddressed questions or issues
• Discuss plans for future visits

7
After the patient leaves
• Order future testing and visits• Write as detailed a progress note as
possible • Request needed consultation visits in
CPRS• Return calls, review abnormal labs,
process view alerts, etc, etc, etc…

8
And, by the way, do it all in 20 minutes or less!!

9
That leaves about 0.75 minutes to enter a consultation request. Anything more and the next patient will not be seen within the 20 minute time of the
performance measure, and patient satisfaction will suffer.

10
Factors for a “best practice” consult request
• Provides easy way for communication of main questions/reason for consult
• Utilizes pick lists, templates, etc. to minimize the need for typing on the part of the requestor
• Does not ask the requestor to retype information that is available elsewhere in the CPRS chart
• Clearly communicates the specialty’s preferences for prerequisites (testing, etc.)
• Is flexible with prerequisites and scheduling depending on patient’s unique situation
11
Consultant Factors for a “best practice” consult reply
• Do not repeat (especially cut and paste) extensive information that is not critical to answering the reason for the consult
• Provide clear-cut, specific, reasonable recommendations in the assessment and plan
• Explain how to obtain any unusual tests or treatments recommended
• Clearly communicate what the consultant’s role will be in the future (if any)

12
Requestor Factors for “best practice” consult requests
• Clearly communicate reason for consult• Clearly communicate urgency of consult• Clearly communicate any unusual
patient factors (i.e., travel restrictions, location, preferences)
• Clearly define whether the requestor would like ongoing follow-up by the consultant (co-managed care) or a one-time visit
13
Requestor behaviors to avoid
• Not being explicit and clear with the questions or reason for consult
• Not providing information that is not available to the consultant in the CPRS chart (i.e.; outside records)

14
The 10 Commandments of Consultation
1. Determine and communicate the question
2. Establish the urgency of the consultation
3. Personally assess the patient (do not rely on others)
4. Be as brief as appropriate5. Be specific (in questions and
recommendations)

15
The 10 Commandments of Consultation
6. Provide contingency plans7. Honor thy turf8. Teach with tact9. Talk is cheap and effective10.Follow-up is essential
(Goldman, L et al, Arch Int Med, 1983)

16
1. Determine the Question
• Study showed in 15% of cases the requestor and consultant had totally different impressions of the reason for the consult
• Another study in diabetics reported no specific question was asked in 24% of cases and consultants ignored the question being asked in another 12%
• Requestor should communicate the question clearly• Consultant should communicate back to the requestor if
there are any doubts or confusion• Studies have shown that consult requestors who clearly
communicate the reasons for the consult are more likely to be satisfied with the result
• Requests to “evaluate and treat” are too vague, inappropriate and unlikely to lead to the best outcome for either party
• CPRS consult templates can facilitate or impede this communication depending on design

17
2. Establish Urgency
• Facilitated by CPRS• Emergent or truly urgent requests
should be accompanied by direct clinician to clinician communication
• Communication from the consultant should explain any unusual issues or anticipated delays in completing a consult
18
3. Personally assess the patient (do not rely on others)
• One study showed that only 9% of consults were requested to obtain assistance in interpreting data already in the chart
• Consultants bring a unique expertise and a different view of a patient’s condition
• Consultants may extract overlooked information by repeating subjective and objective data collection and assessment

19
4. Be as brief as appropriate
• Requestors and Consultants should not pull available data from other parts of CPRS into the consult request or response
• Separate the wheat from the chaff
20
5. Be specific (in questions and recommendations)
• Except for the purpose of facilitating academic training, consultation reports should be brief and goal oriented
• Otherwise, key points and recommendations can be lost in a sea of less important musings
• Suggestions that follow should be explicit and clearly related to the matter at hand
• Studies have shown that leaving a long list of suggestions decreased the likelihood that any of them would be followed
• Consultants should resist the temptation to suggest tests that are not crucial to the case

21
6. Provide contingency plans
• Consultants should remember that patient situations change and initial recommendations might prove irrelevant with time
• Try to anticipate potential problems or changes
• Try to offer diagnostic and therapeutic options for contingencies

22
7. Honor thy turf
• Less of a problem in VHA than in private sector• Requestor should communicate any desire or
expectation for ongoing follow-up• Avoid comments (and especially arguments) in
the notes regarding other subjects or areas outside the consultant’s area of expertise
• Often more than one strategy will likely succeed. If a strategy chosen by the requestor is as likely to succeed as one favored by the consultant, agreement is more appropriate than steadfast insistence on an alternate but equivalent strategy

23
8. Teach with tact
• Although brevity and clarity is important, sharing expertise without condescension is often appreciated
• References to key articles may be appreciated but should not replace focused discussion of the recommendations in the case

24
9. Talk is cheap- and effective
• There is no substitute for direct person-to-person communication
• This is especially the case if there are unusual circumstances before, during or after the consult

25
10. Follow-up is essential
• Consultant should recognize the appropriate time to sign off on a case
• Available mechanisms for communication down the road should be explained (telephone extension, email, new consult, etc.)

26
8 Strategies to improve the requestor’s compliance with recommendations
• Perform the consult within 24 hours of the request
• Frequent, regular follow-up, with notes in the chart
• Verbal contact and a positive, professional interaction with the referring physician/service
• Limit recommendations to no more than five (if possible)

27
8 Strategies to improve the requestor’s compliance with recommendations
• Recommendations should be directly related to the reason for the consultation
• Phrase recommendations as definitive statements
• Assert the importance of the recommendations• Give precise information about how to order
the recommended diagnostic test and how to administer any recommended treatment
Kammerer & Gross: Medical Consultation, 1988

Examples in CPRS

29
What doesn’t work

30
What doesn’t work

31
Getting better

32
Getting better

33
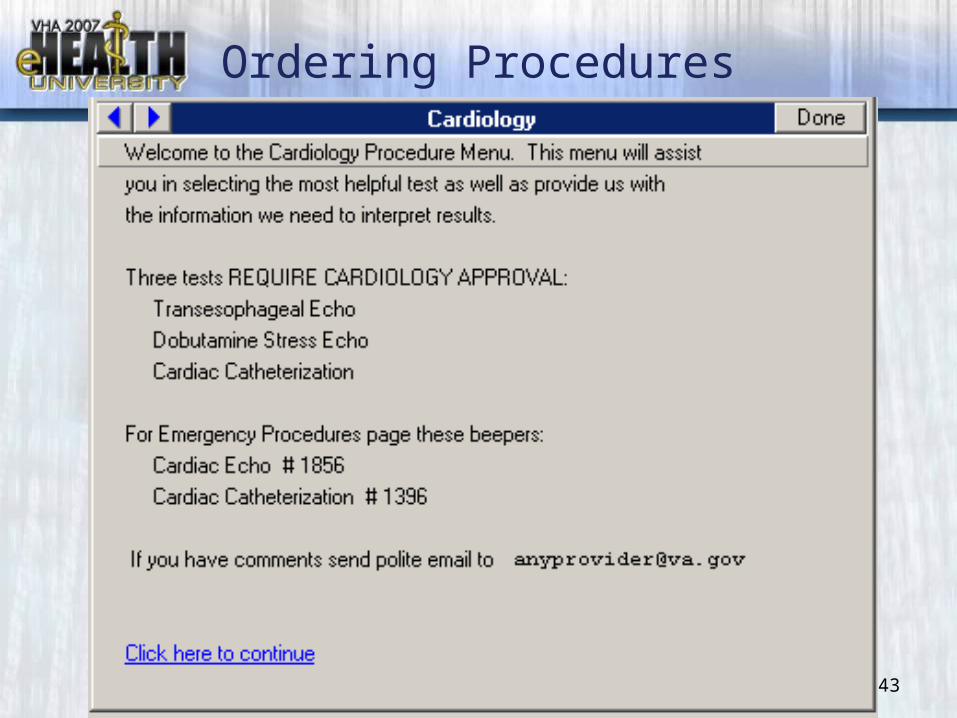
A Success: Cardiology

34




38
Key information provided on common diagnoses

39
Key information provided on common diagnoses

40
Less common conditions also covered

41

42
For simpler questions not requiring a patient visit, no more curbside consults, but recommendations will be documented in
the CPRS chart
43
Ordering Procedures

44
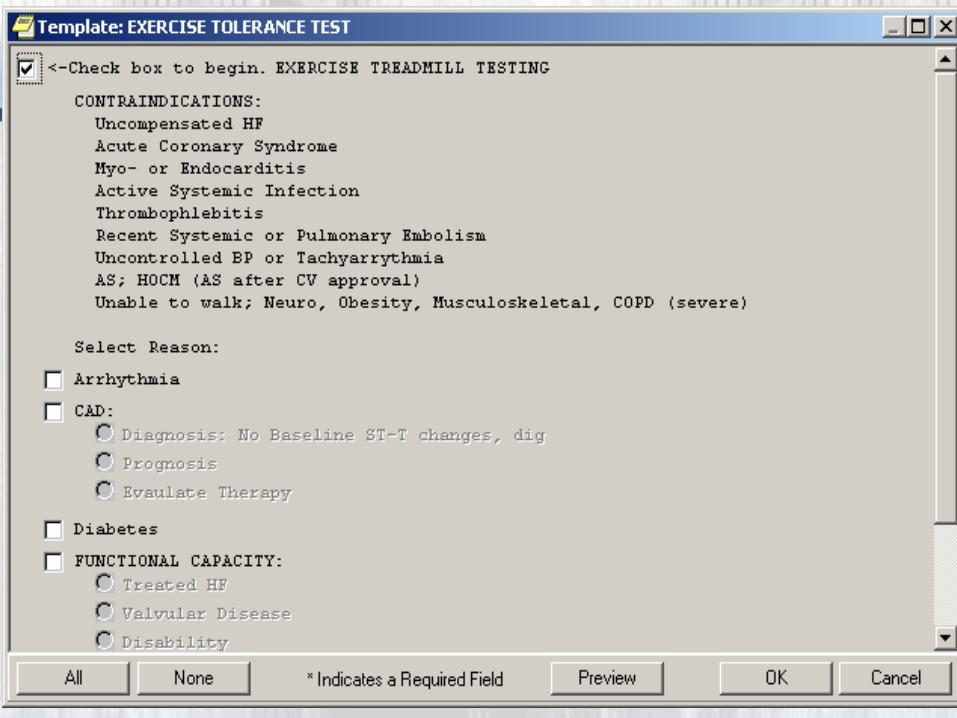
45

46

47
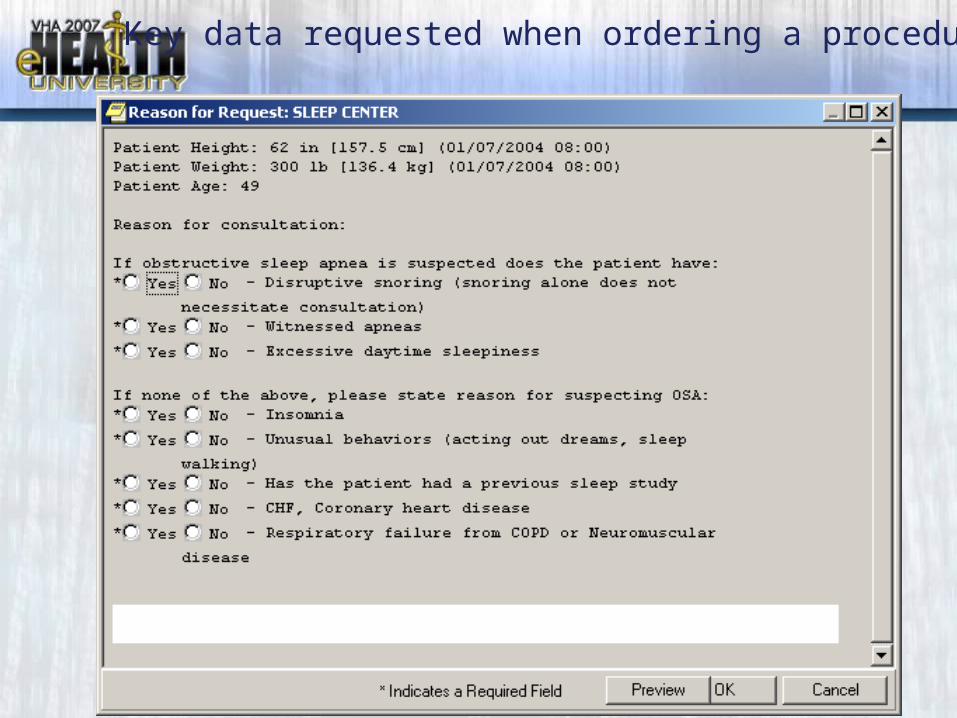
48
Key data requested when ordering a procedure

49
Consultation success!

50
SURGICAL SPECIALTY CONSULTS
Philip B. Irwin, PA-CVascular Surgery
North Florida/South Georgia VAMCGainesville, Florida
Consult Management for Success: Part 2

51
Process ImprovementIdentification of the problem
• Surgical specialty care has seen a dramatic increase in requests for service as primary care has expanded
• There are limited resources to address the consults (providers, space, OR utilization)
• Feedback loop was lacking

52
Reviewing Consults
• With a high initial rejection rate:– Makes the primary care referring
provider look foolish (they were just asking for help!)
– Makes the specialty care service look stingy (we are refusing to help!)
– Confuses the patient (they just want help!)

53
Specialty Care Council Charge 2002
• Charged with developing service contracts
• Open door communication between primary care and specialty care
• CBOCs included in process• Broad applications• Limited impact on actual requests

54
Methods of contacting a Consultant
• Phone calls (takes a personal touch)• E-mail (takes knowledge)• By electronic Consult (the new e-
mail)

55
Consults
• Request exists apart from the clinic referral guidelines
• Generally are “blank” pieces of paper• Current use of the prerequisite field
is too large and gets ignored

56
Fundament Change the Process was needed
• Current process – Service Specific• New Process – Problem Specific• Create a dialog between the services
via the Prerequisite Fields of CPRS

57
Third Generation
• Use the prerequisite functionality of CPRS to create a DIALOG
• Initiate consults by PROBLEM

Third Generation Problem List

59
AAA by ultrasound
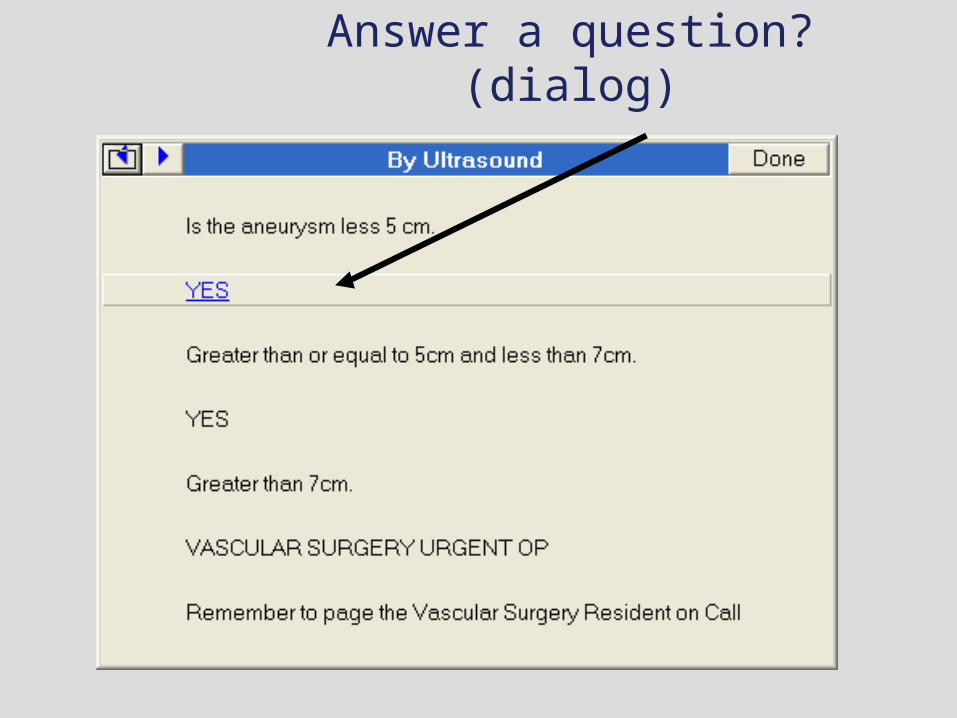
Answer a question? (dialog)

61
Immediate Feedback!

Larger AAA by U/S

63
Pre-clinical testing is included

64
Procedure and history

Urgent/routine pathway

66
After 3 clicks, here is the consult

67
Results for Vascular
• Electronic consult evaluated May 20, 2003
• Turnkey process transparent to requestor
• Now allowed for urgent and routine consults to be handled differently

68
Prior to change 4/2003
N=208
30
111
36
31
DC
Complete
Scheduled
Denied
DC 14%Comp 53%Sched 17%Denied 15%

69
Results June 2003
First Month, N=160
24
51
58
27
DC
Complete
Scheduled
DeniedDC 15%Comp 32%Sched 36%Denied 17%

70
Improvements
Four Months later, N = 159
18
69
53
19
DC
Complete
Scheduled
DeniedDC 11%
Complete 43%
Scheduled 33%
Denied 12 %

71
Results
• Saw a 20% reduction in total consults requested per month (208 – 160)
• Saw a 10% reduction in the number of consults denied or discontinued (32% to 23%)
• Easy to use, broad application

72
Results (part 2)
• Reduction in the need for a “second visit”
• Increase in the number of patients being appropriately followed in primary care
• Reduce the number of inadequate studies (i.e. CT scans in wrong format)
• Ultimately improves access to specialty care

73
Ordering a new consult still begins with the Service…

74
Audiology Problem List

75
Primary care/specialty care contracts enforced by default

76
Established patients screened

77
Contact information provided

78
Pick a problem

79
Ear pain gets re-routed….

80
… to ENT

81
Dental can include…

82
…service connection triage…

83
…with information

84
ENT problem list…

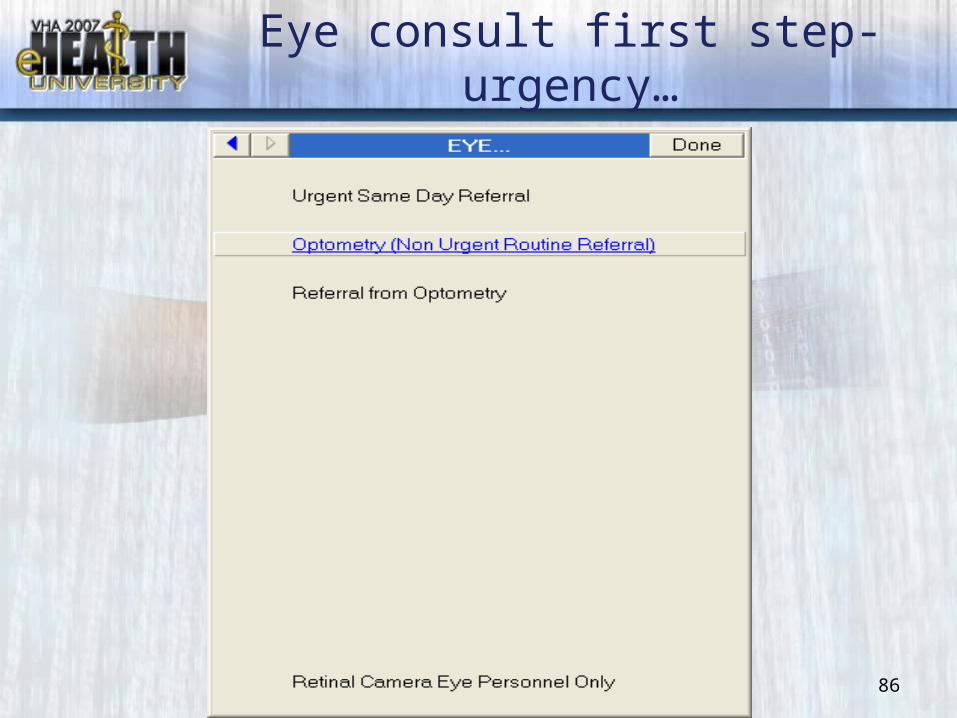
86
Eye consult first step-urgency…

87
…and routes to Optometry
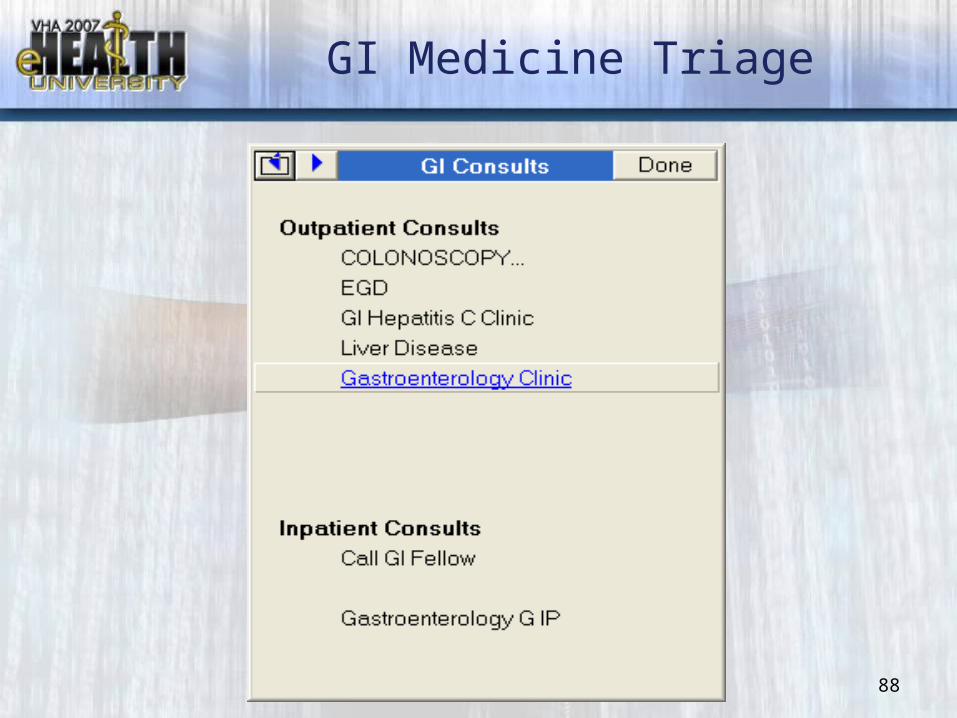
88
GI Medicine Triage

89
Start with brief guidelines…

90
…initial workup…

91
…and then consult

92
Home health care…

93
…with listed resources

94
Nutrition…

95
…has multiple entries

96
Podiatry Problem List
97
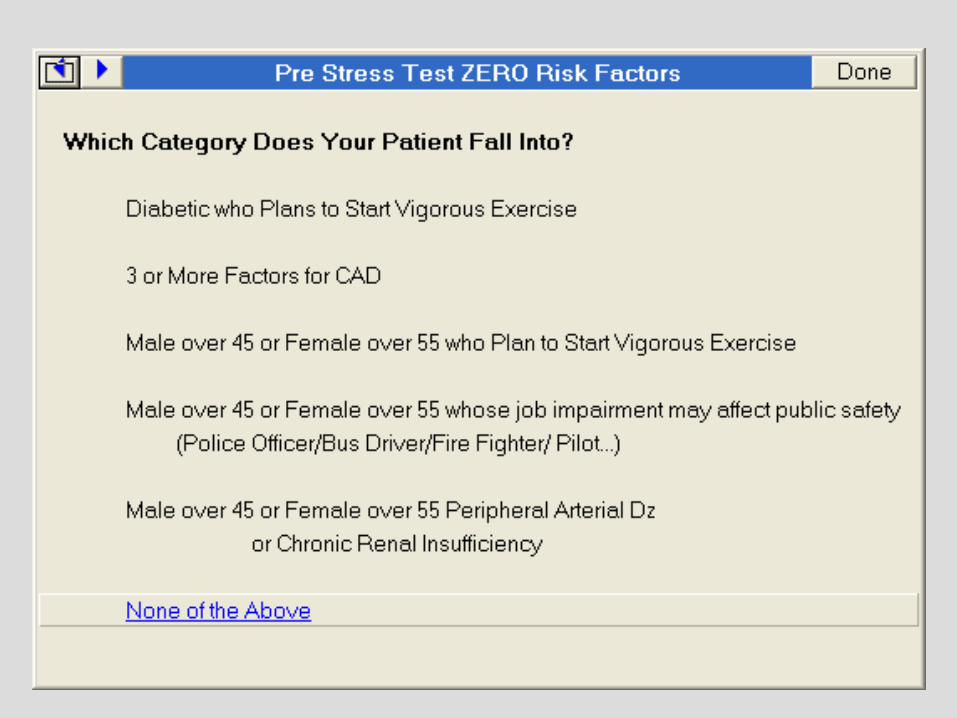
Decision Tree
• Nuclear medicine stress testing was being over utilized
• Unable to meet demand• Cardiology presented in-service
training on workup, had limited change in practice pattern
• Used CPRS to help manage stress testing


100




104

105

106

107

108

109

110

111

112


114

115
Things to Avoid
• The worst thing that can happen is an unnecessary visit– Makes the patient mad– Wastes clinician’s time– Interferes with sicker patients

116
In conclusion
• Problem-oriented patient diagnosis best fit into a problem-oriented consultation system
• CPRS with the use of the prerequisite fields is aptly suited to facilitate the process
• Groundwork must be set out by the service handling the consult

117
Conclusion continued
• Refining the questioning process is a worthwhile task
• Helps the Sender and the Receiver

118
References
• “Reducing Wait Times for Cardiac Consultation” Federal Practitioner Feb 2005 pp 24-28
• “Why we don’t come: patient perceptions on no-shows” Ann Family Medicine 2004;2:541-545
• Advanced Clinic access portal vaww.vccsportal.med.va.gov/aca/

119
Consultations and the Inpatient Provider – A Brief Overview of
Placing the Consult AND Being the Consultant
Ako D. Bradford, M.D.Internal Medicine / Hospitalist
Thomas E. Creek VAMCAmarillo, TX
Southwest VA Health Care Network (VISN 18)
Consult Management for Success: Part 3

120
Inpatient Consults – cont.
• PLACING THE CONSULT
• BEING THE CONSULTANT
•WOMEN’S HEALTH CONSULTS
• An excellent reference text: Kammerer and Gross’ Medical Consultation: The Internist on Surgical, Obstetric, and Psychiatric Services, 3rd ed. (1998). Gross and Caputo, Ed.

121
Inpatient Consults – cont.
• PLACING THE CONSULT – Daily vs. periodic involvement– Expectations of the Consultant: what do
you want them to do?– Establishing follow-up after discharge– Consult vs. Referral
122
Inpatient Consults – cont.
• PLACING THE CONSULT: Daily vs. periodic involvement
– May be affected by how the problem is stated
– May be affected by how your hospital provides more specialized / invasive services
– Is this addressed in the service agreement?
– Remember the 9th Consult Commandment?• Talk is cheap – and effective!
123
Inpatient Consults – cont.
• PLACING THE CONSULT: “Whaddaya want?!?”
– Do you want them to do something... to make the diagnosis... or, to support / refute the diagnosis that YOU have already made?
– How aggressive / proactive is your consultant?
– Is this addressed in the service agreement?
– But, remember the 7th Commandment?• Honor thy turf

124
Inpatient Consults – cont.
•PLACING THE CONSULT: Establishing hospital follow-up
– May depend upon extent of consultant involvement
– 10th Commandment?• Follow-up is essential

125
Inpatient Consults – cont.
•PLACING THE CONSULT: Consult vs. Referral
• “A consultation is strictly defined as requesting another physician to give his or her opinion on diagnosis or management. A referral means to request another physician to assume direct responsibility for a portion or for all of the patient’s care.”
– Kammerer and Gross’ Medical Consultation: The Internist on Surgical, Obstetric, and Psychiatric Services, 3rd ed. (1998).

126
Inpatient Consults – cont.
• BEING THE CONSULTANT– To admit or to consult?– What do they want you to do? – Pre-op evaluation– Resident-managed Consultation Service– Signing Off

127
Inpatient Consults – cont.
• BEING THE CONSULTANT: To admit or to consult? (A.K.A. “To be, or not to
be…”)
– What is the patient’s primary issue? How is this issue best addressed for their safety?
– Communication and collegiality are essential!

128
Inpatient Consults – cont.
• BEING THE CONSULTANT: “Whaddaya want?!?”
•The 1st Commandment?– “Determine and communicate the
question”
– “Medical issues” or “follow along” are inappropriate
– How aggressive / proactive do they want you to be?

129
Inpatient Consults – cont.
• BEING THE CONSULTANT: Pre-op Evaluation
• You do not “clear” a patient; you assess their peri- / intra- / post-operative risks.– Goldman Criteria
• L Goldman et. al. “Multifactorial index of cardiac risk in noncardiac surgical procedures” NEJM 297 (16):845-850. October 20, 1977.
– Qaseem A et. al. “Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: A guideline from the American College of Physicians”. Ann Intern Med. 2006 Apr 18;144(8):575-80.

130
Inpatient Consults – cont.
• BEING THE CONSULTANT: Resident-managed Consult Service
• One of the greatest benefits: availability– 3rd Commandment?
• Personally assess the patient (do not rely on others)
• Less likely to request a “curbside consult”

131
Inpatient Consults – cont.
• BEING THE CONSULTANT: Signing off (or, “Like Nike – Just do it!”)
• Professionally courteous.
• Consults can always be re-requested; but, what if it’s for the same thing as before?

132
Inpatient Consults – cont.
WOMEN’S HEALTH CONSULTS**In the Military . .
• 212,000: Total number of active duty women in the military, as of Sept. 30, 2004. Of that total, 35,100 women were officers and 177,000 were enlisted.(Source: Statistical Abstract of the United States: 2006, Table 501.)
• 15%: Proportion of members of the armed forces who were women, as of Sept. 30, 2004. In 1950, women comprised fewer than 2 percent.(Source: Statistical Abstract of the United States: 2006, Table 501.)
• 1.7 million: The number of military veterans who are women. (Source: Statistical Abstract of the United States: 2006, Table 510.)

133
Inpatient Consults – cont.
So, what’s the bottom line?• The success of many inpatient
consultations depends upon your relationship with your consultants.
• Don’t be afraid to pick up the phone
• Remember the 10 Consult Commandments

134
264 Consult Management: Monitoring for
Performance improvement
Harold D. Bonds MT (ASCP) SCHealth Systems SpecialistG. V. Montgomery VAMC
Jackson, Mississippi
Consult Management for Success: Part 4

135
#264 – Consult Management Monitoring for Performance improvement
• Reasons for monitoring consult from a referring service perspective:
– Provider Utilization• Appropriateness of request (consult reason for
request)• Provider training needs (over utilization vs.
underutilization)
– Timeliness of Response by Consultant for quality patient care
136
#264 – Consult Management Monitoring for Performance improvement
• Reasons for monitoring consult requests from a consultant perspective
– Provider Utilization• Appropriateness of request (consult reason for
request)• Provider utilization (over utilization vs. under
utilization)
– Monitor Supply and Demand• Demand for services • Timeliness of Care • Clinic Capacity and Utilization • Staffing effectiveness and utilization

137
#264 – Consult Management Monitoring for Performance improvement
• Data for Monitoring may be collected from several sources:
– VistA Consult Package Reporting Options– Care Management Query Tool– VistA Fileman templates (requires some
programming knowledge for obtaining information from the files)
– VistA Ambulatory Care Reporting Package Options
– National Reports called KLF reports from the Austin Automation Center generated with software created by Kathie Lee Frisbee.

138
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:
– ST Completion Time Statistics– PC Service Consults Pending Resolution– SH Service Consults Schedule-Management
Report– CC Service Consults Completed– CP Service Consults Completed or Pending Resolution– IFC Interfacility (IFC) Requests– IP Interfacility (IFC) Requests By Patient– IR Interfacility (IFC) Requests by Remote Ordering
Provider– NU Service Consults with Consults Numbers– PI Print Interfacility (IFC) Requests– PL Print Consults by Provider, Location, or
Procedure– PM Consult Performance Monitor Report– PR Print Service Consults by Status– SC Service Consults By Status– TS Print Completion Time Statistics Report

139
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:– SH Service Consults Schedule-Management
Report• Benefits of this option are:
– Status of the consults:– Service Connection Percentage (Priority
Scheduling)– Total consult numbers at a single glance– Patient appointment linked with consult
• Pitfalls of this option:– Ordering Provider not listed– Reason for Request not indicated– Completion, Cancellation, and Discontinued data
not available

#264 – Consult Management Monitoring for Performance improvement

#264 – Consult Management Monitoring for Performance improvement

#264 – Consult Management Monitoring for Performance improvement
143
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:– IFC Interfacility (IFC) Requests
• Benefits of this option:– List consults by Requesting or Consulting facility– List status of consults by Requesting or Consulting
facility– Provides totals for each consult service by facility and
overall totals by facility– Provides basic status of consults
• Pitfalls of this option:– Does not indicate Ordering Provider– Does not indicate Reason for Request– Does not indicate Completion, Cancellation, or
Discontinue data– No appointment data not available

#264 – Consult Management Monitoring for Performance improvement
IF Consult/Request By Status - Consulting Site FROM: ALL TO: JUN 20,2007
SERVICE: Brachytherapy Discont. PRINTED TO 6/5/2007 CPRS,PATIENTONE 1 VAMCONE
Discont. PRINTED TO 1/11/2007 CPRS,PATIENTTWO 2 VAMCTWO
Discont. PRINTED TO 11/29/2006 CPRS,PATIENTFOUR 4 VAMCTHREE
Discont. PRINTED TO 9/18/2006 CPRS,PATIENTFIVE 5 VAMCFOUR
Discont. DISCONTINUED 2/21/2006 CPRS,PATIENTEIGHT 8 VAMCFIVE
Completed COMPLETE/UPDATE 6/8/2007 CPRS,PATIENTFOURTEEN 14 VAMCTWO
Completed COMPLETE/UPDATE 6/5/2007 CPRS,PATIENTFIFTEEN 15 VAMCTHREE
Completed COMPLETE/UPDATE 5/29/2007 CPRS,PATIENTSIXTEEN 16 VAMCSIX
Completed ADDED COMMENT 5/22/2007 CPRS,PATIENTSEVENTEEN 17 VAMCONE
Completed COMPLETE/UPDATE 5/8/2007 CPRS,PATIENTTWENTYONE 21 VAMCFOUR
Completed COMPLETE/UPDATE 11/29/2006 CPRS,PATIENTFORTY 40 VAMCSEVEN
Completed COMPLETE/UPDATE 9/27/2006 CPRS,PATIENTFORTYEIGHT 48 VAMCEIGHT
Pending PRINTED TO 6/15/2007 CPRS,PATIENTONEHUNDREDSEVEN 107 VAMCONE
Scheduled ADDED COMMENT 6/5/2007 CPRS,PATIENTONEHUNDREDEIGHT 108 VAMCTHREE
Scheduled SCHEDULED 6/1/2007 CPRS,PATIENTONEHUNDREDNINE 109 VAMCTWO
Scheduled ADDED COMMENT 5/30/2007 CPRS,PATIENTONEHUNDREDTEN 110 VAMCEIGHT
Scheduled ADDED COMMENT 1/19/2007 CPRS,PATIENTONEHUNDREDELEVEN 111 VAMCONE
Incomplete INCOMPLETE RPT 12/19/2006 CPRS,PATIENTONEHUNDREDTWELVE 112 VAMCTWO
Cancelled CANCELLED 12/4/2006 CPRS,PATIENTONEHUNDREDTHIRTEEN 113 VAMCFOUR
Cancelled CANCELLED 11/22/2006 CPRS,PATIENTONEHUNDREDFOURTEEN 114 VAMCTWO
Cancelled CANCELLED 2/9/2006 CPRS,PATIENTONEHUNDREDSEVENTEEN 117 VAMCONE
Cancelled ADDED COMMENT 1/17/2006 CPRS,PATIENTONEHUNDREDNINETEEN 118 VAMCFIVE

#264 – Consult Management Monitoring for Performance improvement
To Service Brachytherapy Total Requests Discont. 13
To Service Brachytherapy Total Requests Completed 93
To Service Brachytherapy Total Requests Pending 1
To Service Brachytherapy Total Requests Scheduled 4
To Service Brachytherapy Total Requests Incomplete 1
To Service Brachytherapy Total Requests Cancelled 6
Total Requests Pending Resolution To Service Brachytherapy 6
Total Requests To Service Brachytherapy @ VAMCFIVE 2
Total Requests To Service Brachytherapy @ VAMCTHREE 34
Mean Days Completed To Service Brachytherapy @ VAMCTHREE 40
Total Requests To Service Brachytherapy @ VAMCSEVEN 3
Mean Days Completed To Service Brachytherapy @ VAMCSEVEN 26
Total Requests To Service Brachytherapy @ VAMCFOUR 31
Mean Days Completed To Service Brachytherapy @ VAMCFOUR 22
Total Requests To Service Brachytherapy @ VAMCTWO 13
Mean Days Completed To Service Brachytherapy @ VAMCTWO 33
Total Requests To Service Brachytherapy @ VAMCONE 22
Mean Days Completed To Service Brachytherapy @ VAMCONE 16
Total Requests To Service Brachytherapy @ VAMCSIX 5
Mean Days Completed To Service Brachytherapy @ VAMCSIX 10
Total Requests To Service Brachytherapy @ VAMCEIGHT 8
Mean Days Completed To Service Brachytherapy @ VAMCEIGHT 28
Mean Days Completed To Service Brachytherapy 27
Total Requests To Service Brachytherapy 118

146
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:
– PL Print Consults by Provider, Location, or Procedure• Benefits of this option:
– Consult Statistics by Ordering Provider, Location or Procedure
» Individually» System wide
• Pitfalls of this option:– Reason for Request not indicated– Completion, Cancellation, or Discontinue data not available– No appointment data not available

#264 – Consult Management Monitoring for Performance improvement
Consult# Req Date Ordering Provider Location To Service Patient SSN Status Procedure870286 1-Mar-07 CPRS,PROVIDERONE TELEPHONE-MEDICINE 1st Floor EKG Section p Outpatient EKG - 891272 18-Apr-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Bariatric Surgery dc852729 19-Jan-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Blue II PharmD Coag c846273 4-Jan-07 CPRS,PROVIDERONE TELEPHONE-MEDICINE Cardiology c846872 5-Jan-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Cardiology Procedure Section c Holter - 864685 15-Feb-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE CARVEDILOL c853849 23-Jan-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE CDTP x917365 12-Jun-07 CPRS,PROVIDERONE WALK-IN PRIMARY CARE BLUE II Chiropractic s846163 4-Jan-07 CPRS,PROVIDERONE TELEPHONE-MEDICINE CLOPIDOGREL c845001 2-Jan-07 CPRS,PROVIDERONE PC BLUE II-FLU SHOT Dental (Routine) c862449 12-Feb-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Dermatology c898586 3-May-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Diabetic Education (Outpatient) s905014 16-May-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Diabetic Eye Screening x870947 2-Mar-07 CPRS,PROVIDERONE WALK-IN PRIMARY CARE BLUE II EEG (Neurodiagnostics) c EEG856611 29-Jan-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Endocrinology (Diabetic) c916724 11-Jun-07 CPRS,PROVIDERONE TELEPHONE-MEDICINE Endocrinology (Non Diabetic) c875238 13-Mar-07 CPRS,PROVIDERONE WALK-IN PRIMARY CARE BLUE II ENT Cerumen Removal c856878 29-Jan-07 CPRS,PROVIDERONE WALK-IN PRIMARY CARE BLUE II Enterostomal Therapy (ET) c902415 10-May-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE EYEGLASS REQUEST INITIAL ORDER c861490 8-Feb-07 CPRS,PROVIDERONE TELEPHONE TRIAGE FLOMAX c898506 3-May-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Fund Approval (Outpatient) - Medical Service c845166 2-Jan-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE Gastroenterology c897524 1-May-07 CPRS,PROVIDERONE PC BLUE II-CPRSPROVIDERONE General Surgery c

#264 – Consult Management Monitoring for Performance improvement
Consult# Req Date Ordering Provider Location To Service Patient SSN Status Procedure854454 23-Jan-07 CPRSREMOTE,PROVIDERFIVE BILOXI VAMC Urology c858708 29-Jan-07 CPRSREMOTE,PROVIDERFIVE BILOXI VAMC Urology s892416 11-Apr-07 CPRSREMOTE,PROVIDERFIVE BILOXI VAMC Urology s891268 12-Apr-07 CPRSREMOTE,PROVIDERFIVE BILOXI VAMC Urology c854207 22-Jan-07 CPRSREMOTE,PROVIDERTHREE BILOXI VAMC Oncology c886279 29-Mar-07 CPRSREMOTE,PROVIDERTHREE BILOXI VAMC Oncology c853309 22-Jan-07 CPRSREMOTE,PROVIDERTHREE BILOXI VAMC Radiation Therapy c878268 17-Mar-07 CPRSREMOTE,PROVIDERTHREE BILOXI VAMC Radiation Therapy dc882240 29-Mar-07 CPRSREMOTE,PROVIDERTHREE BILOXI VAMC Radiation Therapy s

149
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:
– PM Consult Performance Monitor Report• Benefit of this option:
– Gives Consult Completion Statistics with Percentages
• Pitfalls of this option:– No Individual consult information available– No appointment data available

150
#264 – Consult Management Monitoring for Performance improvement
VistA System Consult Tracking Reports option:
– PR Print Service Consults by Status• Benefits of this option:
– Allows each status to be reviewed/printed separately or together
– Provides numbers of consults in each status– Provides patient information with ordering location
• Pitfalls of this option:– No Ordering provider information– No Reason for Request available– No Completion, Cancellation, or Discontinue data
available– No Appointment data available

#264 – Consult Management Monitoring for Performance improvement

152
#264 – Consult Management Monitoring for Performance improvement
• VistA System Consult Tracking Options:
– There is no one option in the VistA Consult Package that will provide all the information that may be obtained from all five of the reporting options described.
– There is not an option in the VistA Consult Package that will provide the Reason for Request
– There is not an option in the VistA Consult Package that will provide the Completion, Cancellation or Discontinued consult information.

153
#264 – Consult Management Monitoring for Performance improvement
• Consult cancellation reasons can be retrieved by two methods:– Manually looking at each patient’s Electronic
Medical Record from a list generated with one of the VistA Consult Tracking Options.
– Searching and printing the cancelled consults with the reason for cancellation from the consult files.

154
#264 – Consult Management Monitoring for Performance improvement
• Consult completion information can be retrieved by two methods:– Manually looking at each patient’s Electronic
Medical Record from a list generated with one of the VistA Consult Tracking Options.
– Searching and printing a list of the completed consults from the consult files with the associated results field populated.

155
#264 – Consult Management Monitoring for Performance improvement
• Care Management Query Tool:– Benefits:
• Provides report with differing criteria defined by user:– Consult Service– Ordering Provider– Ordering Location– Date Range– Directly exportable report to Microsoft Excel Spreadsheet
– Pitfalls:• Requires specific patient list for search• No Appointment data available• No Reason for Request• No Completion, Cancellation, or Discontinue data
available

#264 – Consult Management Monitoring for Performance improvement

157
#264 – Consult Management Monitoring for Performance improvement
• Ambulatory Care Reporting Package Options:– Benefits:
• Provides statistical data on patient appointments that may be compared to Consult data obtained from the VistA Consult Package
– Pitfalls:• Provides no direct consult data

158
#264 – Consult Management Monitoring for Performance improvement
• VHA Service Support Center Reports:– Benefits:
• Provides statistical data on patient appointments, wait times, delays, and missed opportunities that may be compared to Consult data obtained from the VistA Consult Package and utilized for performance improvement.
– Pitfalls:• Provides no direct consult data at this time• 5 week lag time before monthly data is
available

#264 – Consult Management Monitoring for Performance improvement
VSSC KLF Data Ambulatory Care Option Reports Consult Data

160
3 x 5 cards please