26 Jan 2006 26 Jan 2006 Workshop on ADHD in Workshop on ADHD in Third Level students Third Level students Fiona McNicholas Consultant Lucena Clinic, Rathgar & Our Lady’s Hospital for Sick Children, Crumlin Professor Child & Adolescent Psychiatry, UCD Martin O’Sullivan Consultant Child and Adolescent Psychiatrist Mater Hospital and St Vincent’s Hospital Fairview

26 Jan 2006 Workshop on ADHD in Third Level students Fiona McNicholas Consultant Lucena Clinic, Rathgar & Our Ladys Hospital for Sick Children, Crumlin.
Mar 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

26 Jan 200626 Jan 2006
Workshop on ADHD in Third Workshop on ADHD in Third Level studentsLevel students
Fiona McNicholas
Consultant Lucena Clinic, Rathgar & Our Lady’s Hospital for Sick Children, Crumlin
Professor Child & Adolescent Psychiatry, UCD
Martin O’Sullivan
Consultant Child and Adolescent Psychiatrist
Mater Hospital and St Vincent’s Hospital Fairview

26 Jan 200626 Jan 2006
Overview of TalkOverview of Talk
• ADHD in children• ADHD in adults• Treatment of ADHD

26 Jan 200626 Jan 2006
InattentionInattention HyperactivityHyperactivity
ImpulsivityImpulsivity
ADHD- as we know it!ADHD- as we know it!

26 Jan 200626 Jan 2006
Diagnostic criteriaDiagnostic criteria(ICD/DSM)(ICD/DSM)
• Over activity • Inattention• Impulsivity • Symptoms before age 7
(6 ICD) • Pervasive across
situation • Cause impairment of
social or educational functioning.
• Not due to PDD, Psychotic or other mental disorder (anxiety, depression)

26 Jan 200626 Jan 2006
Inattention: (6/9)Inattention: (6/9)
– Fails to give close attention to details or makes careless errors in schoolwork, or other activities
– Difficulty sustaining attention in tasks or play activities– Does not seem to listen when spoken to directly– Does not follow through on instructions and fails to finish school
work, chores or duties (not due to oppositional behaviour or failure to understand)
– Difficulty organising tasks/activities– Avoids, dislikes or reluctant to engage in tasks that require
sustained mental effort– Loses things necessary for tasks– Easily distracted by extraneous stimuli– Forgetful in daily activities

26 Jan 200626 Jan 2006
Hyperactivity/Impulsivity (6/9)Hyperactivity/Impulsivity (6/9)
• Fidgets with hands or feet or squirms in chair
• Leaves seat in classroom or other in which sitting is expected
• Runs about, climbs excessively in situations in which it is inappropriate (restless)
• Difficulty playing in activities quietly• ‘On the go’ or ‘driven by a motor’• Talks excessively• Blurts out answers• Difficulty awaiting turn• Interrupts or intrudes on others

26 Jan 200626 Jan 2006
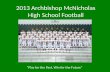
Common Associated Common Associated ComorbiditiesComorbidities
(%)
Milberger et al. Am J Psychiatry 1995; 152: 1793–1799Biederman et al. J Am Acad Child Adolesc Psychiatry 1997; 36: 21–29Castellanos. Arch Gen Psychiatry 1999; 56: 337–338Goldman et al. JAMA 1998; 279: 1100–1107Szatmari et al. J Child Psychol Psychiatry 1989; 30: 219–230
60
40
20
0Oppositional
defiant disorder
Anxiety disorder
Learning disorder
Mood disorder
Conductdisorder
Substance use disorder
Tics

26 Jan 200626 Jan 2006
PrevalencePrevalence
• ICD 1-2 % or DSM IV 3-5%
• 30-50% of children referred to child psychiatry clinics have ADHD
• Diagnosed in boys 3-4 often than in girls
• Persists in 30-50% of patients into adolescence and adulthood (symptom profile may change)
• Prevalence in Adults: 2%

26 Jan 200626 Jan 2006
Associated problemsAssociated problems
• School:• Language impairment 15-
75%• Learning Disability 15-
40%• Low Self esteem• Poor social skills• Labelled
‘trouble maker’
• Poor relationship with parents – often secondary and
improves with appropriate intervention
• Family History ADHD

26 Jan 200626 Jan 2006
ADHD more likely than norms toADHD more likely than norms to
• Drop out of school 32-40%
• Rarely complete college 5-10%
• Under-perform at work 70-80%
• Have few or no friends 50-70%
• Engage in antisocial activities 40-50%
• Experience teen pregnancy 40%
• Sexually transmitted disease 16%
• Speed or have car accidents
• Suffer from depression 20-30%
• Have a personality disorder 18-25%

26 Jan 200626 Jan 2006
Assessment: History & ObservationsAssessment: History & Observations
• Symptoms of ADHD– Home– School– After school activities
• Co-morbidity– LD– Motor– ODD/CD– Other child psychiatric
disorders
• Perpetuating factors– Family– Temperament– Environment
• Informants– Parents– Child– Teacher, Coach, play
school, clubs etc
• Tests– Physical examination
Rating scales– Formal assessments
NEPS, SALT, OT, hearing, vision

26 Jan 200626 Jan 2006
ADHD in Adults?ADHD in Adults?
• ADHD child grown up
• Parent of newly diagnosed ADHD child
• Adult recognizing symptoms of ADHD for the first time
• New onset ADHD symptoms-’secondary ADHD’

26 Jan 200626 Jan 2006
Issues re Adult ADHDIssues re Adult ADHD
• DSM IV diagnosis valid for children• ? Natural History• Assessment process
– Retrospective recall – Multi rater– Inappropriate wording -new scales
• Self referral versus childhood continuation• Developmental disorder PDD or Psychiatric
disorder such as Depression

26 Jan 200626 Jan 2006
Diagnosis of Adult ADHDDiagnosis of Adult ADHD
• Criteria:– Childhood criteria
meet– Current symptoms– Impairment
• Assessment:– Clinical interview– Collateral– Childhood records– Rating Sclaes

26 Jan 200626 Jan 2006
The UTAH Criteria for adult ADHDThe UTAH Criteria for adult ADHD
• Childhood history
• Adult symptoms of– Motor hyperactivity– Attention deficits
• Plus two of the following:– Affective lability– Hot tempers, explosive and
short lived outbursts– Emotional over reactivity– Disorganisation, inability to
complete tasks– Impulsivity
• DDx: schizophrenia, borderline PD or SUD
• Associated features – Marital instability– Sub-optimal academic and
vocational success, – Alcohol or drug misuse,– Family history of ADHD,– Antisocial personality
disorder– Atypical response to
psychoactive medications.

26 Jan 200626 Jan 2006
Adult ADHD Rating ScalesAdult ADHD Rating Scales
• Conner’s 4 dimensions– Cognitive Dysfunction
• Inattention, disorganization, procrastination, poor memory, poor time management
– Hyperactivity• Predominantly inner restlessness, impatience
– Emotional Impulsivity• Rages, tempers, anger management issues, mood
lability, frustration
– Self Esteem & Self worth

26 Jan 200626 Jan 2006
Adult Rating ScalesAdult Rating Scales
• Brown Adult & Adolescent rating Scale– Self report and significant other
• ADHD Rating Scale– Developed by Adler et al, Boston group– DSM IV items reworded for adults
• How often have you had difficulty in wrapping up the final details of a project once the challenging parts have been done?
• ASRS-V1.1 www.adultadd.com

26 Jan 200626 Jan 2006
Adult Self Report Scale Adult Self Report Scale (WHO)(WHO)
• How often do you have trouble wrapping up the final details of a project, once the challenging parts have been done?
• How often do you have difficulty getting things in order when you have to do a task that requires organization?
• How often do you have problems remembering appointments or obligations?
• When you have a task that requires a lot of thought, how often do you avoid or delay getting started?
• How often do you fidget or squirm with your hands or your feet when you have to sit down for a long time?
• How often do you feel overly active and compelled to do things, like you were driven by a motor?

26 Jan 200626 Jan 2006
Differences between Adult and Differences between Adult and Child cases ADHDChild cases ADHD
• Male: female ratio 3:2 vs 3:1 – 10:1
• Source of referral
• Motivation for treatment
• Who is affected by ADHD?
• Insight/ awareness

26 Jan 200626 Jan 2006
Functional ImpairmentFunctional Impairment• Weiss Functional Impairment Rating Scale (v2 2005) - Margaret D Weiss [email protected]
Domains: FamilyWork / School / CollegeLife SkillsSelf – Concept SocialRisk

26 Jan 200626 Jan 2006
WFIRS-SWFIRS-S
• Provides information on breadth and severity of impairment
• Can be used to track changes over time
• Psychometric properties of the scale currently under investigation

26 Jan 200626 Jan 2006
Brown Attention Deficit Disorder Brown Attention Deficit Disorder ScaleScale
5 important symptom clusters
• Getting organised, activating tasks
• Sustaining focus, especially reading
• Alertness, effort, processing speed, motivation
• Affect
• Working memory, memory retrieval

26 Jan 200626 Jan 2006
Clinical Vignette 1Clinical Vignette 1
Walter, 26
• Very superior IQ
• Wide variation in College scores, some papers brilliant, others failed
• Previous history of Dx ADHD + use of Ritalin – stopped aged 14
• Drops out of College year 3 – many short papers, projects not completed

26 Jan 200626 Jan 2006
Clinical Vignette 2Clinical Vignette 2
Maria, 24
• Primary school teacher trainee
• “Terrible planning, organising”
• Procrastinates, late with assignments
• Can’t keep up with the reading
• Finances in a mess – maxed out on Credit

26 Jan 200626 Jan 2006
Clinical Vignette 3Clinical Vignette 3
Anthony, 26
• 3rd attempt at third-level degree
• Makes good starts then gets bored
• Conflict with supervisors
• Regular cannabis use
• Once supportive parents losing patience

26 Jan 200626 Jan 2006
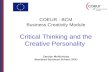
v v Storagevesicle
DA Transporter
Cytoplasmic DA
Methylphenidate blocks
reuptake
Presynaptic NeuronPresynaptic Neuron
SynapseSynapseWilens T, Spencer TJ. Handbook of Substance Abuse: Neurobehavioral Pharmacology. 1998;501-513.
Amphetamine blocks
reuptake
Amphetamine blocks
How Medication works: StimulantsHow Medication works: Stimulants

26 Jan 200626 Jan 2006
Treatment - PsychostimulantsTreatment - Psychostimulants
Methylphenidate or Amphetamine
• First line medications for the treatment of AD/HD in adults off-label
• Clinical response is dose related >1mg/kg/day
• Efficacy rates ~(25-) 70%
• Successful treatment results in diminished substance misuse

26 Jan 200626 Jan 2006
Psychostimulants IIPsychostimulants II
Possible side effects
• Insomnia, headaches,anxiety, loss of appetite
• Cardiovascular: BP 4mmHg; bpm +10

26 Jan 200626 Jan 2006
Psychostimulants IIIPsychostimulants III
• Immediate release MPH require two – three doses e.g. Ritalin, Equasym
• Extended / sustained release MPH e.g. Ritalin LA, Concerta

26 Jan 200626 Jan 2006
Psychostimulants IVPsychostimulants IV
• Immediate release Amphetamine
• E.g. Dexedrine, Adderall
• Extended or sustained release:
• E.g. Adderall XR

26 Jan 200626 Jan 2006
Non-stimulant medications- Non-stimulant medications- Atomoxetine HClAtomoxetine HCl
Strattera• Approved by FDA for treatment of adults• Potent selective NA reuptake inhibitor• Not ‘controlled’• C/I MAOI users, glaucoma• Cautions: liver problems/ cardiovascular/
depression/ suicidality• Await trials in those with depression/ anxiety • Metabolised CYP2D6 enzyme Fluoxetine,
Paroxetine and Quinidine inhibit this enzyme

26 Jan 200626 Jan 2006
Non-stimulant medications- Non-stimulant medications- OtherOther
• SSRIs not effective
• TCAs – Des., Imip, moderate effect
• MAOIs no controlled trials
• Bupropion DA NA atypical anti dep
• Venlafaxine NA 5HT blocker
• Clonidine alpha-2 NA

26 Jan 200626 Jan 2006
ConclusionsConclusions

26 Jan 200626 Jan 2006
Questions?Questions?
Related Documents