Update on Acute Update on Acute Renal Failure 2.0 Renal Failure 2.0 Kenneth Chen, M.D.

25 chen acute renal failure
Jun 03, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on Acute Renal Update on Acute Renal Failure 2.0Failure 2.0
Kenneth Chen, M.D.

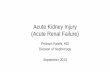
Cases of ARF Among Medicare Inpatients
10
15
20
25
30
35
40
Cas
es p
er 1
000
dis
char
ges
Year
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
JASN 17:1135-1142, 2006

Incidence of Non-Dialysis ARF Incidence of Non-Dialysis ARF
Kidney Int 2007

Incidence of Dialysis-Requiring ARFIncidence of Dialysis-Requiring ARF
KI 2007

KI 74:101, 2008

0
5
10
15
20
25
30
35
40
45
No Dialysis
Dialysis
YearJASN 17:1143, 2006
1988 1990 1992 1994 1996 1998 2000 2002
Mort
alit
y (
%)
Inpatient Mortality - ARF

Inpatient Mortality From ARFInpatient Mortality From ARF
0
10
20
30
40
50
60
1988-1992 1993-1997 1998-2002
Mor
talit
y (%
)
CI 0
CI 1
CI 3
CI 5
JASN 17:1143, 2006

Inpatient Mortality From ARF-DInpatient Mortality From ARF-D
05
101520253035404550
1988-1992 1993-1997 1998-2002
Mor
talit
y (%
)
CI 0
CI 1
CI 3
CI 5
JASN 17:1143, 2006

Increase in Total Cost of Hospitalization
Increase in Serum Creatinine from Baseline
JASN 2005;16:3365

RIFLE and AKIN staging criteria for AKIRIFLE and AKIN staging criteria for AKI____________________________________________________________________________________________________________________________
RIFLE AKIN Serum Cr Urine OutputRIFLE AKIN Serum Cr Urine Output
Stage Stage Criteria CriteriaStage Stage Criteria Criteria
____________________________________________________________________________________________________________________________
Risk 1 Increase in Scr of 1.5-2x < 0.5 ml/kg/hrRisk 1 Increase in Scr of 1.5-2x < 0.5 ml/kg/hr
baseline or increase >0.3 for 6 hrsbaseline or increase >0.3 for 6 hrs
Injury 2 Increase in Scr of 2-3x < 0.5 ml/kg/hrInjury 2 Increase in Scr of 2-3x < 0.5 ml/kg/hr
baseline for 12 hrsbaseline for 12 hrs
Failure 3 Increase in Scr of more < 0.3 ml/kg/hrFailure 3 Increase in Scr of more < 0.3 ml/kg/hr
than 3x baseline or Scr >4 for 24 hrthan 3x baseline or Scr >4 for 24 hr
with an acute rise of > 0.5 orwith an acute rise of > 0.5 or
anuria for 12 anuria for 12 hrhr
LossLoss Persistent renal failure > 4 wk Persistent renal failure > 4 wk
ESRD Persistent renal failure > 3 moESRD Persistent renal failure > 3 mo

Causes of Hospital-Acquired AKICauses of Hospital-Acquired AKI
ATN (45%)ATN (45%) Prerenal (21%)Prerenal (21%) Acute on Chronic (13%)Acute on Chronic (13%) Postrenal (10%)Postrenal (10%) Renal Vascular (3%)Renal Vascular (3%) Glomerulonephritis (3%)Glomerulonephritis (3%) AIN (2%)AIN (2%) Atheroemboli (1%)Atheroemboli (1%) Kidney Int 50:811, 1996Kidney Int 50:811, 1996

Causes of Community-Acquired Causes of Community-Acquired AKIAKI
1% of hospital admissions:1% of hospital admissions:
70% prerenal azotemia70% prerenal azotemia
17% obstruction17% obstruction
11% intrinsic (mostly drug- 11% intrinsic (mostly drug-
induced)induced)
Kaufman AJKD 1991Kaufman AJKD 1991

Prerenal ARFPrerenal ARF Volume depletionVolume depletion Decreased Effective Circulating Decreased Effective Circulating
Volume – cirrhosis, CHF, nephrotic Volume – cirrhosis, CHF, nephrotic syndrome, sepsissyndrome, sepsis
Altered Intrarenal Hemodynamics – Altered Intrarenal Hemodynamics – NSAIDS, Hypercalcemia, hepatorenal NSAIDS, Hypercalcemia, hepatorenal syndrome, ACEI, ARB, calcineurin syndrome, ACEI, ARB, calcineurin inhibitorsinhibitors

Urinary IndicesUrinary Indices
Prerenal – UPrerenal – UNaNa < 20 mEq/L < 20 mEq/L
FEFENaNa< 1% < 1%
FEFEureaurea<35% (PPV 98%)<35% (PPV 98%)
ATN – UATN – UNaNa > 40 mEq/L > 40 mEq/L
FEFENaNa>2%>2%
Kidney Int 2002;62:2223 Kidney Int 2002;62:2223

Intrinsic AKIIntrinsic AKI ATN – ischemic (bypass, arrest, sepsis, ATN – ischemic (bypass, arrest, sepsis,
shock) or toxic (drug-induced or pigment shock) or toxic (drug-induced or pigment nephropathy)nephropathy)
AIN – drugs, herbs, infections, malignancyAIN – drugs, herbs, infections, malignancy Acute GN – post-infectious GN, vasculitis, Acute GN – post-infectious GN, vasculitis,
endocarditis, HUS/TTPendocarditis, HUS/TTP Acute vascular syndromes – Acute vascular syndromes –
atheroembolic dz, renal artery atheroembolic dz, renal artery thromboembolism, renal artery dissection, thromboembolism, renal artery dissection, renal vein thrombosisrenal vein thrombosis

Diagnosis of ATNDiagnosis of ATN
Granular castsGranular casts Very little or no proteinuriaVery little or no proteinuria High FENa > 2% (exception contrast)High FENa > 2% (exception contrast) Consistent clinical scenario i.e. Consistent clinical scenario i.e.
sepsis, contrast, hypotensionsepsis, contrast, hypotension

““Muddy” (Pigmented) Granular Muddy” (Pigmented) Granular CastsCasts

RBC CastRBC Cast

Dysmorphic RBCsDysmorphic RBCs

Acute Phosphate NephropathyAcute Phosphate Nephropathy
Complication of phosphate Complication of phosphate containing bowel cleansing regimens containing bowel cleansing regimens e.g. Fleet’s, Visicol, tablet formse.g. Fleet’s, Visicol, tablet forms
Risk factors – elderly (mean age 64), Risk factors – elderly (mean age 64), hx of HTN, ACEI or ARBhx of HTN, ACEI or ARB
Can present 1 mo after colonoscopyCan present 1 mo after colonoscopy Normocalcemia and bland urinary Normocalcemia and bland urinary
sedimentsediment JASN 16:3389, 2005JASN 16:3389, 2005


NephrotoxinsNephrotoxins
Afferent arteriolar constriction –Afferent arteriolar constriction –
NSAIDsNSAIDs
ContrastContrast
Amphotericin BAmphotericin B
VancomycinVancomycin
NorepinephrineNorepinephrine
Efferent arteriolar dilation – Efferent arteriolar dilation –
ACEIACEI
ARBARB

NephrotoxinsNephrotoxinsCrystalluria – sulfonamidesCrystalluria – sulfonamides
methotrexatemethotrexate acyclovir (risk 19%)acyclovir (risk 19%)
triamterene triamterene ethylene glycolethylene glycol
indinavirindinavirPigmenturia – myoglobinuriaPigmenturia – myoglobinuria hemoglobinuriahemoglobinuriaGlomerulonephritis – hydralazineGlomerulonephritis – hydralazineHUS/TTP – gemcitabine, quinine, clopidogrel, HUS/TTP – gemcitabine, quinine, clopidogrel,
cyclosporine, tacrolimuscyclosporine, tacrolimus

NephrotoxinsNephrotoxins
Tubular toxicity – aminoglycosidesTubular toxicity – aminoglycosides
cisplatincisplatin
vancomycinvancomycin
pentamidinepentamidine
contrastcontrast
amphotericin Bamphotericin B
heavy metalsheavy metals
tenofovir (Viread), didanosine (Videx), tenofovir (Viread), didanosine (Videx), lamivudine (Epivir), stavudine (Zerit)lamivudine (Epivir), stavudine (Zerit)

AINAIN
Drug related in 92% of casesDrug related in 92% of cases Oliguria (51%), arthralgia (45%), Oliguria (51%), arthralgia (45%),
peripheral eosinophilia (36%), fever peripheral eosinophilia (36%), fever (30%), rash (21%)(30%), rash (21%)
Urine eosinophils (40%) – PPV 38%Urine eosinophils (40%) – PPV 38% Proteinuria - 0.7 g/dayProteinuria - 0.7 g/day No proven benefit from steroids No proven benefit from steroids
Nephrol Dial Transplant 2004;19:2778Nephrol Dial Transplant 2004;19:2778


AINAIN

Causes of Interstitial NephritisCauses of Interstitial Nephritis
NSAIDs and 5-aminosalicylates NSAIDs and 5-aminosalicylates
Aristolochic Acid (Chinese herb nephropathy)Aristolochic Acid (Chinese herb nephropathy)
Lymphoma, sarcoidosis, Sjogren’sLymphoma, sarcoidosis, Sjogren’s
Antibiotics – Nafcillin, rifampin, PCN, Antibiotics – Nafcillin, rifampin, PCN, cephalosporins, bactrim, ciprofloxacin, cephalosporins, bactrim, ciprofloxacin, vancomycin, indinavirvancomycin, indinavir
Dilantin, phenobarbital, carbamazepineDilantin, phenobarbital, carbamazepine
Allopurinol, H2-blockers, PPIsAllopurinol, H2-blockers, PPIs
Sulfonamides – HCTZ, bactrim, LasixSulfonamides – HCTZ, bactrim, Lasix

CINCIN 33rdrd leading cause of inpatient ARF – leading cause of inpatient ARF –
12%12% Overall incidence 1.6-2.3% but in Overall incidence 1.6-2.3% but in
patients with CKD 15-50%patients with CKD 15-50% 13-50% requiring HD after contrast 13-50% requiring HD after contrast
remain on dialysis permanentlyremain on dialysis permanently Risk factors include CKD, DM, Risk factors include CKD, DM,
diuretics, hypovolemia, CHF, diuretics, hypovolemia, CHF, proteinuriaproteinuria
JAMA 2006;295(23):2765 and NEJM 2006;354:379JAMA 2006;295(23):2765 and NEJM 2006;354:379

CINCIN
Omnipaque (iohexol) – low-osmolar Omnipaque (iohexol) – low-osmolar (400-850 mOsm/kg), nonionic(400-850 mOsm/kg), nonionic
Visipaque (iodixanol) – iso-osmolar Visipaque (iodixanol) – iso-osmolar (290 mOsm/kg), nonionic(290 mOsm/kg), nonionic

% Incidence of CIN% Incidence of CIN
NEJM 2003;348(6):491
J Am Coll Cardiol 2006;48(4):692

CINCIN
Arch Intern Med 2002;162:329

CINCIN
NEJM 2000;343:180

CINCIN
Eur Heart J 2004;25:206

CINCIN
NEJM 2006;354:2773

CINCIN
JAMA 2004;291(19):2328

CINCIN
Clin J Am Soc Nephrol 2008;3:10

CINCIN
A meta-analysis of 41 controlled trials A meta-analysis of 41 controlled trials examining various prophylactic agents examining various prophylactic agents showed only NAC reduced the risk for showed only NAC reduced the risk for CIN (RR 0.62) over saline aloneCIN (RR 0.62) over saline alone
Furosemide increased the risk of CIN Furosemide increased the risk of CIN (RR 3.27)(RR 3.27)
Ann of Int Med 2008;148:284Ann of Int Med 2008;148:284

CIN - SummaryCIN - Summary Check a Cr if hx of CKD, DM, proteinuria, Check a Cr if hx of CKD, DM, proteinuria,
renal surgery, CHF, gout, or HTNrenal surgery, CHF, gout, or HTN Hold NSAIDs and diuretics for 24 hrs Hold NSAIDs and diuretics for 24 hrs
before and after contrast, and metformin before and after contrast, and metformin the day of the procedure.the day of the procedure.
NAC 1200 mg PO bid 24 hrs before and NAC 1200 mg PO bid 24 hrs before and after contrast after contrast
NS 1 ml/kg/hr 6-12 hrs before and after NS 1 ml/kg/hr 6-12 hrs before and after contrast contrast

Approach to DiagnosisApproach to Diagnosis
History - NSAIDs, herbals, medications, History - NSAIDs, herbals, medications, contrast, UTI symptoms, prostatism?contrast, UTI symptoms, prostatism?
Physical – suprapubic Physical – suprapubic fullness/tendernessfullness/tenderness
Bladder catheterization and/or U/SBladder catheterization and/or U/S
U/A and urinary indicesU/A and urinary indices
Therapeutic trial of IVFsTherapeutic trial of IVFs

CrCl = (140-age) x IBW/(Cr x 72) x 0.85 if female
Cockcroft-Gault Equation


Treatment of ARFTreatment of ARF IVF hydrationIVF hydration Early removal of Foley cathetersEarly removal of Foley catheters General lack of benefit – mannitol, loop General lack of benefit – mannitol, loop
diuretics, low dose dopaminediuretics, low dose dopamine Renal dose medications – especially Renal dose medications – especially
antibioticsantibiotics Adjust TPN/lower K and PO4 intakeAdjust TPN/lower K and PO4 intake Avoid PICC lines – 23% initial thrombosis Avoid PICC lines – 23% initial thrombosis
risk and 38% thrombosis risk overall risk and 38% thrombosis risk overall (JVIR (JVIR 2000;11:1309)2000;11:1309)

Treatment of ARFTreatment of ARF Stop metformin if Cr > 1.5Stop metformin if Cr > 1.5 Switch from tolazamide or glyburide to Switch from tolazamide or glyburide to
glipizideglipizide Avoid gemfibrozil and statinsAvoid gemfibrozil and statins Avoid Demerol, aminoglycosides, NSAIDs, Avoid Demerol, aminoglycosides, NSAIDs,
Fleet’s enemas, Al, MgFleet’s enemas, Al, Mg Caution with morphine, insulin, fosamax, Caution with morphine, insulin, fosamax,
lmwhlmwh Avoid nitrofurantoin or probenecidAvoid nitrofurantoin or probenecid Use ½ NS for post-obstructive diuresisUse ½ NS for post-obstructive diuresis

Treatment of ARFTreatment of ARF
Indications for dialysis:Indications for dialysis:
Refractory metabolic acidosisRefractory metabolic acidosis
Refractory hyperkalemiaRefractory hyperkalemia
Pulmonary edema/volume overloadPulmonary edema/volume overload
Uremic pericarditisUremic pericarditis
Uremic symptomsUremic symptoms
Toxic ingestionsToxic ingestions

Nephrogenic Systemic FibrosisNephrogenic Systemic Fibrosis
Hardening and thickening of skin Hardening and thickening of skin overlying the trunk and extremitiesoverlying the trunk and extremities
Expansion and fibrosis of the dermis Expansion and fibrosis of the dermis in association with CD34-positive in association with CD34-positive fibrocytesfibrocytes
95% of cases associated with 95% of cases associated with gadoliniumgadolinium
Probably 5% risk in advanced RFProbably 5% risk in advanced RF

Nephrogenic Systemic FibrosisNephrogenic Systemic Fibrosis

Nephrogenic Systemic FibrosisNephrogenic Systemic Fibrosis

Nephrogenic Systemic FibrosisNephrogenic Systemic Fibrosis

Nephrogenic Systemic FibrosisNephrogenic Systemic Fibrosis
Gd should be avoided when GFR<30Gd should be avoided when GFR<30 Dialysis should be initiated as soon Dialysis should be initiated as soon
as possible after exposure if pt is on as possible after exposure if pt is on dialysisdialysis
No proven treatment No proven treatment

Ancient Chinese Medical TextAncient Chinese Medical Text
The inferior doctor treats actual The inferior doctor treats actual illness.illness.
The mediocre doctor attends to The mediocre doctor attends to impending illness.impending illness.
The superior doctor prevents illness The superior doctor prevents illness (Kaiser Permanente!)(Kaiser Permanente!)
2600 BC - Huang Dee Nai-Chang 2600 BC - Huang Dee Nai-Chang




D’oh!

Evidence-Based MedicineEvidence-Based Medicine Eminence-Based MedicineEminence-Based Medicine Eloquence-Based MedicineEloquence-Based Medicine Vehemence-Based MedicineVehemence-Based Medicine Kaiser-Based MedicineKaiser-Based Medicine

CINCIN
NDT 2006;21(8):2120

CINCIN
Ann of Pharmacotherapy 2007;41:46

Causes of ProteinuriaCauses of Proteinuria
Selected Causes of Proteinuria by TypeSelected Causes of Proteinuria by Type
Glomerular Glomerular Primary glomerulonephropathy Minimal change disease Primary glomerulonephropathy Minimal change disease Idiopathic membranous glomerulonephritis Focal segmental Idiopathic membranous glomerulonephritis Focal segmental glomerulonephritis Membranoproliferative glomerulonephritis IgA glomerulonephritis Membranoproliferative glomerulonephritis IgA nephropathy Secondary glomerulonephropathy Diabetes mellitus Collagen nephropathy Secondary glomerulonephropathy Diabetes mellitus Collagen vascular disorders (e.g., lupus nephritis) Amyloidosis Preeclampsia vascular disorders (e.g., lupus nephritis) Amyloidosis Preeclampsia Infection (e.g., HIV, hepatitis B and C, poststreptococcal illness, syphilis, Infection (e.g., HIV, hepatitis B and C, poststreptococcal illness, syphilis, malaria and endocarditis) Gastrointestinal and lung cancers Lymphoma, malaria and endocarditis) Gastrointestinal and lung cancers Lymphoma, chronic renal transplant rejection Glomerulonephropathy associated with chronic renal transplant rejection Glomerulonephropathy associated with the following drugs: Heroin NSAIDs Gold components Penicillamine Lithium the following drugs: Heroin NSAIDs Gold components Penicillamine Lithium Heavy metals Heavy metals
TubularTubular Hypertensive nephrosclerosis Tubulointerstitial disease due to: Hypertensive nephrosclerosis Tubulointerstitial disease due to: Uric acid nephropathy Acute hypersensitivity interstitial nephritis Fanconi Uric acid nephropathy Acute hypersensitivity interstitial nephritis Fanconi syndrome Heavy metals Sickle cell disease NSAIDs, antibiotics syndrome Heavy metals Sickle cell disease NSAIDs, antibiotics
Overflow Overflow Hemoglobinuria Myoglobinuria Multiple myeloma Amyloidosis Hemoglobinuria Myoglobinuria Multiple myeloma Amyloidosis

In-Hospital Mortality Rate 1992-In-Hospital Mortality Rate 1992-20012001
33% - ARF requiring dialysis33% - ARF requiring dialysis
27.5% - ARF not requiring dialysis27.5% - ARF not requiring dialysis
4.6% - no ARF4.6% - no ARF
JASN 17:1135-1142, 2006JASN 17:1135-1142, 2006

Survival in ESRDSurvival in ESRD
Life expectancy for a 40 year-old male Life expectancy for a 40 year-old male is 37.3 years, but just 7.4 yrs on is 37.3 years, but just 7.4 yrs on dialysisdialysis
Life expectancy for a 60 year-old male Life expectancy for a 60 year-old male is 20.2 years, but just 4 yrs on dialysisis 20.2 years, but just 4 yrs on dialysis
Life expectancy for a 70 year-old male Life expectancy for a 70 year-old male is 13.2 years, but just 2.8 yrs on is 13.2 years, but just 2.8 yrs on dialysisdialysis
USRDSUSRDS



Causes of Hospital-Acquired ARFCauses of Hospital-Acquired ARF
Postoperative statePostoperative state Advanced cardiovascular diseaseAdvanced cardiovascular disease Neoplastic diseaseNeoplastic disease HIV infectionHIV infection Multiple organ system failureMultiple organ system failure Systemic infectionSystemic infection Solid organ transplantationSolid organ transplantation

Increase in Serum Creatinine from Baseline
JASN 2005;16:3365

CaseCase
65 y.o. female admitted with fevers, hearing 65 y.o. female admitted with fevers, hearing loss, ear pain, neck pain, vomiting, and loss, ear pain, neck pain, vomiting, and myalgias.myalgias.
Meds – lisinopril 15 mg dailyMeds – lisinopril 15 mg daily
HCTZ 25 mg dailyHCTZ 25 mg daily
Labs – Na 139 K 3.6 Cl 101 HCO3 25 BUN 13 Labs – Na 139 K 3.6 Cl 101 HCO3 25 BUN 13 Cr 0.7 Gluc 149Cr 0.7 Gluc 149
U/A (catheter) 1.02/6/50 mg% ketones/large U/A (catheter) 1.02/6/50 mg% ketones/large bl/30 mg% prot/sm LE/5-10 sq cells/0-2 bl/30 mg% prot/sm LE/5-10 sq cells/0-2 WBC/11-25 RBCWBC/11-25 RBC

CaseCase11stst Day – ceftriaxone (2g q12, vanco (1 g), IV Day – ceftriaxone (2g q12, vanco (1 g), IV
acyclovir 10 mg/kg q8hr)acyclovir 10 mg/kg q8hr)
22ndnd day – vanco and acyclovir d/c’d day – vanco and acyclovir d/c’d
Scr 0.6Scr 0.6
33rdrd day – aspirin 162 mg daily and lisinopril day – aspirin 162 mg daily and lisinopril startedstarted
Scr 1.97 U/A 100 mg%prot/5-10 sq cells/3-Scr 1.97 U/A 100 mg%prot/5-10 sq cells/3-5 WBC/10-25 RBC5 WBC/10-25 RBC
44thth day – Scr 2.2 U/A tr prot/sm LE/3-5 day – Scr 2.2 U/A tr prot/sm LE/3-5 WBC/0-2 RBCWBC/0-2 RBC
55thth day – Scr 1.4 day – Scr 1.4

CaseCase
What was the cause of her ARF?What was the cause of her ARF?
a)a) VancomycinVancomycin
b)b) AcyclovirAcyclovir
c)c) CeftriaxoneCeftriaxone
d)d) Volume contractionVolume contraction
e)e) SepsisSepsis

90 Day Mortality Rate in 200190 Day Mortality Rate in 2001
44.8% - ARF requiring dialysis44.8% - ARF requiring dialysis 40.3% - ARF not requiring dialysis40.3% - ARF not requiring dialysis 12.1% - no ARF12.1% - no ARF
JASN 17:1135-1142, 2006JASN 17:1135-1142, 2006
Related Documents