2019 PROVIDER MANUAL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2019
PROVIDER
MANUAL

TABLE OF CONTENTS
RENAISSANCE PHYSICIANS OVERVIEW ..................................................................................................... A
RENAISSANCE PHYSICIANS ......................................................................................................................... A
Renaissance Physicians Structure ........................................................................................................................................................A
Service Area Map ..................................................................................................................................................................................B
Renaissance Physician Line of Business Quick Reference Guide ....................................................................................................... C
PATIENT INFORMATION ................................................................................................................................. 1
Eligibility Verification .............................................................................................................................................................................. 1
Eligibility Guarantee Form ..................................................................................................................................................................... 1
Maximum Out-of-Pocket (MOOP).......................................................................................................................................................... 1
Patient Hold Harmless ........................................................................................................................................................................... 1
Patient Confidentiality ............................................................................................................................................................................ 1
Patient Rights and Responsibilities ....................................................................................................................................................... 2
Advance Medical Directives................................................................................................................................................................... 4
Benefits and Services ............................................................................................................................................................................ 4
Emergency Services and Care After Hours ........................................................................................................................................... 4
Excluded Services ................................................................................................................................................................................. 5
Grievance and Appeal Process ............................................................................................................................................................. 6
Eligibility Guarantee Form ..................................................................................................................................................................... 7
Forma de Garantía de Elegibilidad ........................................................................................................................................................ 8
PROVIDER INFORMATION .............................................................................................................................. 9
Providers Designated as Primary Care Physicians (PCPs) .................................................................................................................. 9
The Role of the Primary Care Physician (PCP) .................................................................................................................................... 9
The Role of the Specialist Physician ..................................................................................................................................................... 9
Administrative, Medical, and Reimbursement Policy Changes .............................................................................................................. 9
Communication among Providers .......................................................................................................................................................... 9
Provider Marketing Guidelines............................................................................................................................................................. 10
Provider Participation .......................................................................................................................................................................... 10
PHYSICIAN RIGHTS AND RESPONSIBILITIES ........................................................................................... 11
Patient Assignment to New PCP ......................................................................................................................................................... 12
Closing Patient Panels ........................................................................................................................................................................ 12
Medical Record Standards .................................................................................................................................................................. 13
Access and Availability Standards for Providers ................................................................................................................................ 13
Plan Notification Requirements for Providers ..................................................................................................................................... 13
Provision of Health Care Services ....................................................................................................................................................... 14
Inpatient Manager Program ................................................................................................................................................................. 14
Dispute Resolution .............................................................................................................................................................................. 14
STARS GUIDANCE ........................................................................................................................................ 15
Star Rating Components ..................................................................................................................................................................... 16
Healthcare Plan Effectiveness Data Information Set (HEDIS®) .......................................................................................................... 16
Renaissance Medicare Advantage CPT II Code Guide ....................................................................................................................... 17
PROVIDER REQUEST FOR PATIENT TO TRANSFER CARE TO ANOTHER PROVIDER ......................... 20
Procedure ............................................................................................................................................................................................ 20
EXCHANGE OF ELECTRONIC DATA .......................................................................................................... 24
Experience the Ease of HSConnect .................................................................................................................................................... 24

Register for HSConnect Access .......................................................................................................................................................... 25
CREDENTIALING AND RECREDENTIALING PROGRAM ............................................................................ 37
Practitioner Selection Criteria .............................................................................................................................................................. 37
Application Process ............................................................................................................................................................................. 37
Credentialing and Recredentialing Process ......................................................................................................................................... 37
Office Site Evaluations ........................................................................................................................................................................ 37
Practitioner Rights ............................................................................................................................................................................... 38
Organizational Provider Selection Criteria ........................................................................................................................................... 38
Organizational Provider Application and Requirements ..................................................................................................................... 38
Credentialing Committee and Peer Review Process .......................................................................................................................... 38
Non-discrimination in the Decision-making Process ........................................................................................................................... 38
Provider Notification ............................................................................................................................................................................ 39
Appeals Process and Notification of Authorities ................................................................................................................................. 39
Confidentiality of Credentialing Information ......................................................................................................................................... 39
Ongoing Monitoring ............................................................................................................................................................................. 39
Initial Contracting/Credentialing Information Checklist ........................................................................................................................ 40
REIMBURSEMENT ......................................................................................................................................... 41
Primary Care Physician Capitation ...................................................................................................................................................... 41
Specialist Capitation ............................................................................................................................................................................ 41
Copays ................................................................................................................................................................................................ 41
Primary Care Physician Capitation Detail ............................................................................................................................................ 42
Specialist Capitation Summary ............................................................................................................................................................ 43
CLAIMS .......................................................................................................................................................... 44
Claims Submission .............................................................................................................................................................................. 44
ICD-10 Diagnosis and Procedure Code Reporting ............................................................................................................................. 46
Dual Eligible Patients ........................................................................................................................................................................... 46
Cost-sharing Chart .............................................................................................................................................................................. 47
Coordination of Benefits and Subrogation Guidelines ........................................................................................................................ 47
Worker's Compensation ...................................................................................................................................................................... 49
Subrogation ......................................................................................................................................................................................... 49
Appeals................................................................................................................................................................................................ 49
Reconsiderations ................................................................................................................................................................................. 50
HEALTH SERVICES ....................................................................................................................................... 52
Goals ................................................................................................................................................................................................... 52
Departmental Functions ...................................................................................................................................................................... 52
Prior Authorization ............................................................................................................................................................................... 52
Outpatient Prior Authorization Department .......................................................................................................................................... 53
ICD-10 Diagnosis and Procedure Code Reporting ............................................................................................................................. 53
Request and Time Frames .................................................................................................................................................................. 55
Retrospective Review .......................................................................................................................................................................... 55
Discharge Planning and Acute Care Management ............................................................................................................................. 55
Adverse Determinations ...................................................................................................................................................................... 55
REFERRAL PROCESS ................................................................................................................................... 57
Referral Guidelines .............................................................................................................................................................................. 57
Self Referrals ....................................................................................................................................................................................... 57
Primary Care Physician's Referral Responsibilities ............................................................................................................................ 57
Specialist Physician's Referral Responsibilities .................................................................................................................................. 58
HSConnect Quick Reference Guide .................................................................................................................................................... 24

PHARMACY QUALITY PROGRAMS ............................................................................................................. 59
Narcotic Case Management ................................................................................................................................................................ 59
Medication Adherence Strategy........................................................................................................................................................... 59
Medication Therapy Management ....................................................................................................................................................... 59
Drug Utilization Review ....................................................................................................................................................................... 59
QUALITY CARE MANAGEMENT PROGRAM................................................................................................ 60
Mission Statement ............................................................................................................................................................................... 60
Quality Principles ................................................................................................................................................................................. 61
Quality Management Program Goals .................................................................................................................................................. 62
Embedded Care Coordination ............................................................................................................................................................. 63
HEALTH PLANS ............................................................................................................................................. 64
Overview of Healthplans ...................................................................................................................................................................... 64
Cigna-HealthSpring ............................................................................................................................................................................. 64
Renaissance Physicians Health Plan Election to Participate Form ..................................................................................................... 73
Arcadia Population Health Tool ........................................................................................................................................................... 75
Cigna-HealthSpring ID Card ................................................................................................................................................................ 81
Cigna Collaborative Accountable Care ................................................................................................................................................ 82
Cigna City of Houston .......................................................................................................................................................................... 85
CIN ...................................................................................................................................................................................................... 88
BLUE Medicare Advantage HMO (MAPD) ........................................................................................................................................ 168
BLUE Value Based Incentive Plan (VBIP) ......................................................................................................................................... 175
APPENDIX ....................................................................................................................................................... 200
Prior Authorization List ...................................................................................................................................................................... 201
Case Management Programs ............................................................................................................................................................ 220
Advance Directive: Texas .................................................................................................................................................................. 221
Do Not Resuscitate English/Spanish ................................................................................................................................................. 227
Medical Power of Attorney English/Spanish ...................................................................................................................................... 229

RENAISSANCE PHYSICIANS
OVERVIEW
Renaissance Physicians is an Independent Physicians Association (IPA) that is a physician-run organization with local groups of primary care physicians (PCPs) and a full specialist network. The goal is to grow and maintain a highly desired managed health care delivery system in which the IPA accepts responsibility for a wide range of medical services, including primary care, specialty care, laboratory, part B drugs, and diagnostic procedures.
Renaissance Physicians is a PCP-driven delivery system, which allows the PCP to take the lead on coordinating care both of a preventive nature as well as chronic conditions with collaborative engagement from preferred specialist network. Due to the vast geography of the IPA, providers are grouped into a geographic networks called a POD (Physician Organized Delivery systems) centralized around a group of hospitals with full set of PCPs and Specialists who have enhanced relationships and aligned incentives.
This manual contains the operating policies and procedures of the IPA as well as plan related details as they relate to the day-to-day participating physicians and their patients. The IPA requires continual communication between the physicians and the management company, CareAllies, to ensure a consistent working relationship and timely notification of any and all practice related changes. You will receive updates to this manual as changes to the policies and procedures occur.
RENAISSANCE PHYSICIANS
Renaissance Physicians
• Non-profit corporation
• Renaissance contracts with health plans
• Renaissance contracts with LLCs and providers
• City-wide specialty panel
• Board comprised of PCPs and specialists
• Physician owned and led
Advantages of Renaissance
• One integrated contracting unit
• Physicians/providers set metrics and performance standards
• Ability to contract with PPOs through Clinically Integrated Network
• City-wide specialty network
• Superior physician satisfaction
• Greater physician-involvement and best practice sharing
• Aligned incentives with engaged management company
Renaissance Commitment
• Focus on greater Houston and Golden Triangle market
• Consistency with health plan relationships
• Financial matrix consistency
• Financial reserve discipline
• Robust physician reporting
• Ongoing physician and staff education
Improved capitation rates
• Value based capitation rates for PCPs
• Sub specialty capitation contracts
• Specialists brought up to net-city-wide utilization
• PCP driven delivery system
• Surplus funds distributed based on IPA criteria per contractual requirements
• Improved physician representation with LLCs
Duties of Renaissance
• Maintains Ultimate financial risk
• Credentialing
• Utilization/Quality management
• Creation of guiding principles
• Contracting and Physician reimbursement
Duties of LLC
• Provider network development
• Management of LLC utilization
• Communication
• Surplus distribution
• Provider satisfaction
• Problem resolution
A

1. Central Houston 2. Conroe 3. Eastside 4. Merit
5. Metropolitan 6. Northwest Suburban
7. Pasadena 8. Southeast Associates Baytown
9. Southwest 10. Space Center 11. West Houston 12. Eastex Physician Organization
NETWORK MAP
B

Renaissance Physicians
Lines of Business Quick Reference Guide
Service Cigna-HealthSpring Blue Cross Medicare Advantage (HMO)Cigna City of Houston
Cigna Surefit
Cigna CAC: LocalPlus,
Open Access Plus
VBIP: Blue Choice PPO,
Blue Advantage HMO (BAV)
Behavorial Health Behavioral Health: 866-780-8546
Mental Health
Provider Finder: www.magellanhealth.com
Magellan Internal Renaissance Physicians
Phone Number: 800-327-9251
Mental Health: 800-882-4462Behavioral Health: 800-926-2273
CignaforHCP.com
Blue Choice PPO Members:
Behavioral Health: 800-528-7264
Blue Advantage HMO Members:
Magellan Behavioral Health at
800-729-2422
www.cignaforHCP.com
Referral Requests:
HSConnect Online Portal
https://healthspring.hsconnectonline.com/HSConnect
713-437-3060
Inpatient Authorization and Case Management
Programs: 800-882-4462
For all referrals, verification of benefits:
www.availity.com
Pre-cert: iExchange Web application:
https://www.bcbstx.com/provider/tools/iexchange_index.h
tml
or iExchange System: 800-451-0287
Medical Care Management: 855-896-2701
Prime (Pharmacy) Therapeutics:
800-289-1525
For Additional Services:
Please see reference guide in BCBS VBIP manual provided
by your Network Operations representative.
Customer Service: 877-774-8592
Provider Service: 844-343-9753
TTY/TDD: 711
Member Verification: 877-774-8592
For additional benefits please contact Blue Cross Blue
Shield. Also, see the reference guide provided to you by
your Network Operations Representative.
Coding: Chaun Tatum-Williams
Phone: 713-936-6022
Fax: 888-856-3959
Contact Cigna directly for Referrals:
www.cignaforHCP.com
Medical Management (including pre-cert):
800-882-4462
For patients with GWH-Cigna or "G" ID cards:
866-494-2111
Sleep Mgmt Services:
Care Centrix: 877-877-9899
Cigna.SleepCCX.com
Please access www.cignaforHCP.com for full listing
of member specific benefits.
Amplifon Hearing Health Care:
855-531-4695
amplifonusa.com/cigna
For Additional Benefits: www.cignaforHCP.com
Silver Sneakers: 888-423-4632
Eye Med: 866-939-3633
Dental Networks of America: 855-557-5491
Transportaion (LogistiCare): 844-452-9383
Tru Hearing: 877-248-4040
For additional benefits please contact Blue
Cross Blue Shield.
Referral Requests:
HSConnect Online Portal:
https://healthspring.hsconnectonline.com/HSConn
ect
713-437-3060
Urgent Admissions:
800-441-9188
Medical Care Management:
855-390-6573
Prime (Pharmacy) Therapeutics:
877-277-7898
Customer Service: 800-451-0287
Eligibility and Benefit Information: availity.com
Commercial RiskProduct Type
https://www.bcbstx.com/provider/www.myhealthspring.comhttps://www.bcbstx.com/provider/network/bma_
hmo.html
Medicare Advantage Plans Commercial Incentive Program
www.cignaforHCP.comWebsite for Provider
Resourceswww.cignaforHCP.com
All Claims must be submitted directly to Blue Cross Blue
Shield. Please contact BCBS for further details.
All Claims must be submitted directly to Cigna. Please
refer to member's ID card.
Phone: 800-882-4462
Provider Customer Service: 800-230-6138
TTY/TTD: 877-893-1504
Member Verification: 832-553-3480
Financial Assistance (LIS): 877-236-4471
Member Customer Service: 800-668-3818
Provider/Customer
Service
Provider Service Line: 844-343-9753
Customer Service: 800-882-4462
Member Verification: www.cignaforHCP.com
Cigna Cigna of Houston Customer Service:
800-997-1406
Customer Service: 800-882-4462
Member Service: www.cignaforHCP.com
Electronic Payor ID
(Electronic Medical Claims
Submission)
Coding Department
Health Services
(Pre-Cert)
Supplemental Benefits
Enhanced Encounter/Coding:
Chaun Tatum-Williams
Phone: 713-936-6022
Fax: 888-856-3959
Submit Professional Claims to RPO
Availity: RENGQ (for HCFA only)
Emdeon: 76066 (for HCFA and UB-04)
Submit Professional Claims to RPO
Availity: RENGQ (for HCFA only)
Emdeon: 76066 (for HCFA and UB-04)
Submit Professional Claims to RPO
Availity: RENGQ (for HCFA only)
Emdeon: 76066 (for HCFA and UB-04)
Silver and Fit: 877-427-4788
www.silverandfit.com
Transportation (Access2Care):
866-214-5126
Superior Vision: 800-879-6901
Hearing Care Solutions: 866-872-1001
DentaQuest: 866-288-1573
Referral Requests: HSConnect Online Portal:
https://healthspring.hsconnectonline.com/HSConnect
Phone: 713-437-3060
Pre-Cert (Direct Admits): 832-553-3456
Medical Directors, Dr. Ramapriya Suresh:
713-437-3145
Clinical Pharmacy Manager, Esteban Gallardo:
832-553-3314
Pharmacy/Mail Order Prescriptions:
800-331-6293
Acute Admissions: Sue Chiampi: 770-779-3842
SNF: Pam Parsons: 770-779-6946
LTAC: Amber Hill: 770-779-6246
Case Management: 888-501-1116
*This is a summary of Renaissance Physicians' collaborative agreements. For the complete list, please visit our website www.myrpo.com or contact your Provider Relations Representative at 832-553-3300. Updated as of 02/25/2
C

Service Cigna-HealthSpring Blue Cross Medicare Advantage (HMO)Cigna City of Houston
Cigna Surefit
Cigna CAC: LocalPlus,
Open Access Plus
VBIP: Blue Choice PPO,
Blue Advantage HMO (BAV)
In-Network Provider/Facility
Search
In network providers can be found via the HSConnect
Portal:
https://healthspring.hsconnectonline.com/HSConnect
In network professional providers:
https://healthspring.hsconnectonline.com/HSConnec
t
In network institutional providers:
https://public.hcsc.net/providerfinder/search-
action.do?corpEntCd=TX1&custGrp=MADVANTAGEH
MOTX&alpha=MCH&ntwkdisplayId=MCHTX
In Network RPO Providers:
https://myrpo.com/providers/find-a-provider
In Network Cigna Providers:
https://hcpdirectory.cigna.com/web/public/providers
In Network RPO Providers:
https://myrpo.com/providers/find-a-provider
In Network Cigna Providers:
https://hcpdirectory.cigna.com/web/public/providers
In Network RPO Providers:
https://myrpo.com/providers/find-a-provider
In Network BCBS Providers:
https://public.hcsc.net/providerfinder/search.do?corpEntCd=
TX1&nextPage=networkplan&residencestate
Preferred Ancillary ProvidersDME/Home Health: 832-553-3456
Encompass Home Health
Dialysis Davita and Fresenius
https://www.bcbstx.com/medicare/mapd_provider.html DME/Home Health: 800-882-4462
DME/HomeHealth:
Care Centrix: 877-466-0164
www.carecentrixportal.com
Dialysis: Davita (800-244-0680) and
Fresenius (800-662-1237)
Please see reference guide in BCBS VBIP manual provided by your
Network Operations representative.
Surgery Center/
Urgent Care
Urgent Care: NextLevel Urgent Care
Conroe Surgery Center, Bay Area Endoscopy, Cyfair
Surgery Center, HMU Surgical Center, Pearland, Surgery
Center, Sugarland Surgery Center
**Contact provider rep for full listing**
Urgent Care: NextLevel Urgent Care
BCBS Facility/Center Search:
https://www.bcbstx.com/medicare/
mapd_provider.html
Urgent Care: NextLevel Urgent Care
Cigna Facility/Center Search:
https://hcpdirectory.cigna.com/web/
public/providers/
Urgent Care: NextLevel Urgent Care
Cigna Facility/Center Search:
https://hcpdirectory.cigna.com/web/
public/providers/
Urgent Care: NextLevel Urgent Care
BCBS Facility/Center Search:
https://public.hcsc.net/providerfinder/search.do?corpEntCd=
TX1&nextPage=networkplan&residencestate
Product Type Medicare Advantage Plans Commercial Risk
Cigna Home Delivery Pharmacy:
800-285-4812
Specialty Pharmacy Services: Speciality meds via
injection/infusion: 800-351-3606
BAV/HMO & PPO Members:
HCA
IASIS
Harris County Hospital District
CHI St. Luke's Hospitals
PPO Members ONLY:
The Methodist Hospitals
Walgreens
HEB
Walmart
Randalls
SAMS
Commercial Incentive Program
Quest Diagnostics Quest Diagnostics Quest Diagnostics Quest Diagnostics Quest Diagnostics
CHI St. Luke's
Memorial Hermann Health Systems
EviCore
High-tech radiology, diagnostic cardiology, musculoskeletal:
Phone: 888-693-3297
For Precertification: www.eviCore.com
Radiation therapy:
Phone: 866-688-9250
eviCore.com/Cigna/Pages/Radiology.aspx
Blue Choice PPO members: contact AIM Specialty Health to obtain
a Radiology Quality Initiative (RQI) for the following services: CT/CTA
scans, MRI/MRA scans, SPECT/Nuclear Cardiology studies, PET
scans. To obtain an RQI, contact AIM
aimspecialtyhealth.com
Blue Advantage HMO Members: Use provider search for in-
network BAV imaging center.
Preferred Hospitals
HCA
The Methodist
IASIS
Tenet
CHI St. Luke's
Christus
HCA
The Methodist
IASIS
Tenet
CHI St. Luke's
Christus
HCA
IASIS
Tenet
CHI St. Luke's
Christus
HCA
Harris County Hospital District
CHI St. Luke's Hospitals
Methodist Community
Memorial Hermann Community
Preferred Imaging
Member ID Card
CHI St. Luke's
Memorial Hermann Health Systems
Laboratory Provider
Preferred Pharmacy
Albertsons, Brookshire, HEB, Kroger, Randalls, Walgreens,
Walmart
Mail Order: Postal Prescription Services (PPS)
Phone: 1-800-552-6694, Option 3
Fax: 1-800-723-9023
Albertsons, HEB, Kroger, Tom Thumb, Randalls,
Walgreens
Home Delivery: Alliance Rx Walgreens Prime
Phone: 1-800-345-1036, Option 1
Fax: 1-800-332-9581
CHI St. Luke's
Memorial Hermann Health Systems
Cigna Home Delivery Pharmacy:
800-285-4812
Please access www.cignaforHCP.com for more information.
BA
V,
HM
O
D

PATIENT INFORMATION
Eligibility Verification
All participating providers are responsible for verifying a patient’s eligibility at each and every visit.
You can verify patient eligibility the following ways:
Call the Health Plan – You must call the Health Plan to verify eligibility when the patient cannot present identification or does not appear on your monthly eligibility list.
Please note: the Health Plan should have the most updated information, therefore, call the Health Plan for accuracy.
• HSConnect – The IPA’s web portal, HSConnect, allows our providers to verify patient eligibility online
• Ask to see the patient’s Identification Card – Each patient is provided with an individual patient identification card. Noted on the ID card is the patient’s identification number, plan code, name of PCP, copayment, and effective date. Since changes do occur with eligibility, the card alone does not guarantee the patient is eligible.
• Pursue additional proof of identification – Each PCP and specialist office is provided with a monthly Eligibility Report upon request, which lists new and current IPA’s patients with their effective dates. Please be sure to refer to the most current month’s Eligibility Report.
• See ID Cards in Health Plan sections.
Eligibility Guarantee Form
If your office decides to see a patient that does not have identification, you should have the patient sign an Eligibility Guarantee form. Please keep a copy of the signed form in patient’s file. Forms at end of Patient Information section
Maximum Out-of-Pocket (MOOP)
The Maximum Out-of-Pocket (MOOP) benefit is now a part of all benefit plans. Patients have a limit on the amount they will be required to pay out-of-pocket each year for medical services, which are covered under Medicare Part A and Part B. Once this Maximum Out-of-pocket expense has been reached, the patient no longer is responsible for any out-of-pocket expenses, including any cost shares, for the remainder of the year for covered Part A and Part B services (excluding the patient’s Medicare Part B premium and the IPA’s plan premium).
Patient Hold Harmless
Participating providers are prohibited from balance billing the IPA’s patients including, but not limited to, situations involving non-payment by IPA, insolvency of IPA, or IPA’s breach of its Agreement. Provider shall not bill, charge, collect a deposit from, seek compensation or reimbursement from, or have any recourse against patients or persons, other than the
IPA, acting on behalf of patients for Covered Services provided pursuant to the Participating Provider’s Agreement. The provider is not, however, prohibited from collecting copayments, coinsurances or deductibles for covered services in accordance with the terms of the applicable patient’s Benefit Plan.
Patient Confidentiality
We know our patients’ privacy is extremely important to them, and we respect their right to privacy when it comes to their personal information and health care. We are committed to protecting our patients’ personal information. IPA does not disclose patient information to anyone without obtaining consent from an authorized person(s), unless we are permitted to do so by law. Because you are a valued provider to the IPA, we want you to know the steps we have taken to protect the privacy of our patients. This includes how we gather and use their personal information. The privacy practices apply to all of IPA’s past, present, and future patients.
When a patient joins a Medicare Advantage plan, the patient agrees to give IPA access to Protected Health Information. Protected Health Information (“PHI”), as defined by the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), is information created or received by a health care provider, health plan, employer or health care clearinghouse, that: (i) relates to the past, present, or future physical or behavioral health or condition of an individual, the provision of health care to the individual, or the past, present or future payment for provision of health care to the individual; (ii) identifies the individual, or with respect to which there is a reasonable basis to believe the information can be used to identify the individual; and (iii) is transmitted or maintained in an electronic medium, or in any form or medium. Access to PHI allows IPA to work with providers, like yourself, to decide whether a service is a Covered Service and pay your clean claims for Covered Services using the patients’ medical records. Medical records and claims are generally used to review treatment and to do quality assurance activities. It also allows IPA to look at how care is delivered and carry out programs to improve the quality of care patients receive. This information also helps manage the treatment of diseases to improve our patients’ quality of life.
Patients have additional rights over their health information.
They have the right to:
• Send IPA a written request to see or get a copy of information about them, or amend their personal information that they believe is incomplete or inaccurate. If we did not create the information, we will refer patient to the source of the information. Request that we communicate with them about medical matters using reasonable alternative means or at an alternative address, if communications to their home address could endanger them.
1

• Receive an accounting of IPA’s disclosures of their medical information, except when those disclosures are for treatment, payment, or health care operations, or the law otherwise restricts the accounting.
As a Covered Entity under HIPAA, providers are required to comply with the HIPAA Privacy Rule and other applicable laws in order to protect patient PHI. To discuss any breaches of the privacy of our patients, please contact the CareAllies Privacy Steward at [email protected].
Patient Rights and Responsibilities
Patients have the following rights:
The right to be treated with dignity and respect
Patients have the right to be treated with dignity, respect, and fairness at all times. IPA must obey laws against discrimination that protect patients from unfair treatment. These laws say that IPA cannot discriminate against patients (treat patients unfairly) because of a person’s race, disability, religion, gender, sexual orientation, health, ethnicity, creed, age, or national origin. If patients need help with communication, such as help from a language interpreter, they should be directed to call Customer Service. Customer Services can also help patients file complaints about access to facilities (such as wheelchair access). Patients can also call the U.S. Department of Health and Human Services’ Office for Civil Rights at 1-800-368-1019 or TTY/TDD 1-800-537-7697, or the Office for Civil Rights in their area for assistance.
The right to the privacy of medical records and personal health information
There are federal and state laws that protect the privacy of patient medical records and personal health information. IPA keeps patients’ personal health information private as required under these laws. Any personal information that a patient gives is protected. IPA staff will make sure that unauthorized people do not see or change patient records. Generally, we will get written permission from the patient (or from someone the patient has given legal authority to make decisions on their behalf) before we can give patient health information to anyone who is not providing the patient’s medical care. There are exceptions allowed or required by law, such as release of health information to government agencies that are checking on quality of care.
The laws that protect patient privacy give them rights related to getting information and controlling how their health information is used. All Plans are required to provide patients with a notice that tells them about these rights and explains how the IPA protects the privacy of their health information. For example, patients have the right to look at their medical records, and to get copies of the records at no additional charge. Patients also have the right to ask plan providers to make additions or corrections to their medical records (if patients ask plan providers to do this, they will review patient requests and figure out whether the changes
are appropriate). Patients have the right to know how their health information has been given out and used for routine and non-routine purposes. If patients have questions or concerns about privacy of their personal information and medical records, they should be directed to call Customer Services. The IPA will release patient’s information, including prescription drug event data, to Medicare, which may release it for research and other purposes that follow all applicable federal statutes and regulations.
The right to see participating providers, get covered services, and get prescriptions filled within a reasonable period of time
Patients will get most or all of their health care from participating providers, that is, from doctors and other health providers who are part of IPA. Patients have the right to choose a participating provider (IPA will work with patients to ensure they find physicians who are accepting new patients). Patients have the right to go to a women’s health specialist (such as a gynecologist) without a referral. Patients have the right to timely access to their providers and to see specialists when care from a specialist is needed. Patients also have the right to timely access to their prescriptions at any network pharmacy. “Timely access” means that patients can get appointments and services within a reasonable amount of time. The Evidence of Coverage explains how patients access participating providers to get the care and services they need. It also explains their rights to get care for a medical emergency and urgently needed care.
The right to know treatment choices and participate in decisions about their health care
Patients have the right to get full information from their providers when they receive medical care, and the right to participate fully in treatment planning and decisions about their health care. Providers must explain things in a way that patients can understand. Patients have the right to know about all of the treatment choices that are recommended for their condition including all appropriate and medically necessary treatment options, no matter what their cost or whether they are covered by IPA. This includes the right to know about the different medication management treatment programs offers and those in which patients may participate. Patients have the right to be told about any risks involved in their care. Patients must be told in advance if any proposed medical care or treatment is part of a research experiment and be given the choice to refuse experimental treatments. Patients have the right to receive a detailed explanation from IPA if they believe that a plan provider has denied care that they believe they are entitled to receive or care they believe they should continue to receive. In these cases, patients must request an initial decision. “Initial decisions” are discussed in the patients’ Evidence of Coverage.
Patients have the right to refuse treatment. This includes
2

the right to leave a hospital or other medical facility, even if their doctor advises them not to leave. This also includes the right to stop taking their medication. If patients refuse treatment, they accept responsibility for what happens as a result of refusing treatment.
The right to use advance directives (such as a living will or a power of attorney)
Patients have the right to ask someone such as a family patient or friend to help them with decisions about their health care. Sometimes, people become unable to make health care decisions for themselves due to accidents or serious illness. If a patient wants to, he/she can use a special form to give someone they trust the legal authority to make decisions for them if they ever become unable to make decisions for themselves. Patients also have the right to give their doctors written instructions about how they want them to handle their medical care if they become unable to make decisions for themselves. The legal documents that patients can use to give their directions in advance of these situations are called “advance directives.” There are different types of advance directives and different names for them. Documents called “living wills” and “powers of attorney for health care” are examples of advance directives.
If patients decide that they want to have an advance directive, there are several ways to get this type of legal form. Patients can get a form from their lawyer, from a social worker, from IPA, or from some office supply stores. Patients can sometimes get advance directive forms from organizations that give people information about Medicare. Regardless of where they get this form, keep in mind that it is a legal document. Patients should consider having a lawyer help them prepare it. It is important for the patient to sign this form and keep a copy at home. Patients should give a copy of the form to their doctor and to the person they name on the form as the one to make decisions for them if they cannot. Patients may want to give copies to close friends or family patients as well.
If patients know ahead of time that they are going to be hospitalized and they have signed an advance directive, they should take a copy with them to the hospital. If patients are admitted to the hospital, the hospital will ask them whether they have signed an advance directive form and whether they have it with them. If a patient has not signed an advance directive form or does not have a copy available during admission, the hospital has forms available and will ask if the patient wants to sign one.
Remember, it is a patient’s choice whether he/she wants to fill out an advance directive (including whether they want to sign one if they are in the hospital). According to law, no one can deny them care or discriminate against them based on whether or not they have signed an advance directive. If patients have signed, an advance directive and they believe that a doctor or hospital has not followed the instructions in it; patients may file a complaint with their State Board of
Medicine or appropriate state agency (this information can be found in the patient’s Evidence of Coverage).
The right to make complaints
Patients have the right to make a complaint if they have concerns or problems related to their coverage or care. Patients or an appointed/authorized representative may file “Appeals,” “grievances,” concerns and Coverage Determinations. If patients make a complaint or file an appeal or Coverage Determination, IPA must treat them fairly (i.e., not discriminate against them) because they made a complaint or filed an appeal or Coverage Determination. To obtain information relative to appeals, grievances, concerns and/or Coverage Determinations, patients should be directed to call Customer Service.
The right to get information about their health care coverage and cost
The Evidence of Coverage tells patients what medical services are covered and what they have to pay. If they need more information, they should be directed to call Customer Services. Patients have the right to an explanation from IPA about any bills they may get for services not covered by IPA. The IPA must tell patients in writing why IPA will not pay for or allow them to get a service and how they can file an appeal to ask IPA to change this decision. Staff should inform patients on how to file an appeal, if asked, and should direct patients to review their Evidence of Coverage for more information about filing an appeal.
The right to get information about IPA, plan providers, drug coverage, and costs
Patients have the right to get information about the IPA and operations. This includes information about our financial condition, about the services we provide, and about our health care providers and their qualifications. Patients have the right to find out from us how we pay our doctors. To get any of this information, patients should be directed to call Customer Service. Patients have the right to get information from us about their Part D prescription coverage. This includes information about our financial condition and about our network pharmacies. To get any of this information, staff should direct patients to call Customer Service.
The right to get more information about patients’ rights Patients have the right to receive information about their rights and responsibilities. If patients have questions or concerns about their rights and protections, they should be directed to call Customer Service. Patients can also get free help and information from their State Health Insurance Assistance Program (SHIP).
The right to take action if a patient thinks they have been treated unfairly or their rights are not being respected
3

• If patients think they have been treated unfairly or their rights have not been respected, there are options for what they can do.
• If patients think they have been treated unfairly due to their race, color, national origin, disability, age, or religion, we must encourage them to let us know immediately. They can also call the Office for Civil Rights in their area.
• For any other kind of concern or problem related to their Medicare rights and protections described in this section, patients should be encouraged to call Customer Service. Patients can also get help from their State Health Insurance Assistance Program (SHIP).
Patients have the following responsibilities:
Along with certain rights, there are also responsibilities associated with being a patient of the IPA. Patients are responsible for the following:
• To become familiar with their IPA’s coverage provider.
• To give their doctors and other providers the information they need to provide care for them and to follow the treatment plans and instructions that they and their doctors agree upon. Patients must be encouraged to ask questions of their doctors and other providers whenever the patient has them.
• To act in a way that supports the care given to other patients and helps the smooth running of their doctor’s office, hospitals, and other offices.
• To pay their plan premiums and any copayments or coinsurances they may have for the Covered Services they receive. Patients must also meet their other financial responsibilities that are described in their Evidence of Coverage.
• To let IPA know if they have any questions, concerns, problems, or suggestions regarding their rights, responsibilities, coverage, and/or IPA’s operations.
• To notify Customer Service and their providers of any address and/or phone number changes as soon as possible.
• To use their IPA only to access services, medications and other benefits for themselves.
Advance Medical Directives
The Federal Patient Self-Determination Act ensures the patient’s right is to participate in health care decision-making, including decisions about withholding resuscitative services or declining/withdrawing life sustaining treatment. In accordance with guidelines established by the Centers for Medicare & Medicaid Services (CMS), and our own policies and procedures, IPA requires all participating providers to have a process in place pursuant to the intent of the Patient Self Determination Act.
The patient may inform all providers contracted directly or indirectly with IPA that the patient has executed, changed,
or revoked an advance directive. At the time a service is provided, the provider should ask the patient to provide a copy of the advance directive to be included in his/her medical record.
If the Primary Care Physician (PCP) and/or treating provider cannot as a matter of conscience fulfill the patient’s written advance directive, he/she must advise the patient and IPA. The IPA and the PCP and/or treating provider will arrange for a transfer of care. Participating providers may not condition the provision of care or otherwise discriminate against an individual based on whether the individual has executed an advance directive. However, nothing in The Patient Self-Determination Act precludes the right under state law of a provider to refuse to comply with an advance directive as a matter of conscience.
To ensure providers maintain the required processes to Advance Directives, IPA conducts periodic patient medical record reviews to confirm that required documentation exists. See Appendix for a copy of the Texas Advance Directives.
Benefits and Services
All patients receive benefits and services as defined in their Evidence of Coverage (EOC). Each month, the IPA makes available to each participating Primary Care Physician a list of their active patients. Along with the patient’s demographic information, the list includes the name of the plan in which the patient enrolled. Please be aware that recently terminated patients may appear on the list. (See “Eligibility Verification” section of this manual).
• The IPA encourages its patients to call their Primary Care Physician and the rules they must follow to get care as a patient. Patients can use their Evidence of Coverage and other information that we provide them to learn about their coverage, what we have to pay, and the rules they need to follow. Patients should always be encouraged to call Patient Services if they have any questions or complaints.
• To advise IPA if they have other insurance coverage.
• To notify providers when seeking care (unless it is an emergency) that they are enrolled with IPA and present their plan enrollment card to the to schedule appointments. However, if an IPA’s patient calls or comes to your office for an unscheduled non-emergent appointment, please attempt to accommodate the patient and explain to them your office policy regarding appointments. If this problem persists, please contact IPA.
Emergency Services and Care After Hours
Emergency Services
An emergency is defined as the sudden onset of a medical condition with acute symptoms. A patient may reasonably believe that the lack of immediate medical attention could result in:
4

• Permanently placing the patient’s health in jeopardy
• Causing serious impairments to body functions
• Causing serious or permanent dysfunction of any body organ or part
In the event of a perceived emergency, patients have been instructed to first contact their Primary Care Physician for medical advice. However, if the situation is of such a nature that it is life threatening, patients have been instructed to go immediately to the nearest emergency room facility. Patients who are unable to contact their PCP prior to receiving emergency treatment have been instructed to contact their PCP as soon as is medically possible or within forty-eight (48) hours after receiving care. The PCP will be responsible for providing and arranging any necessary follow-up services.
For emergency services within the service area, the PCP is responsible for providing, directing, or authorizing a patient’s emergency care. The PCP or his/her designee must be available twenty-four (24) hours a day, seven (7) days a week to assist patients needing emergency services. The hospital may attempt to contact the PCP for direction. Patients have a copayment responsibility for outpatient emergency visits unless an admission results.
For emergency services outside the service area, IPA will pay reasonable charges for emergency services received from non-participating providers if a patient is injured or becomes ill while temporarily outside the service area. Patients may be responsible for a copayment for each incident of outpatient emergency services at a hospital’s emergency room or urgent care facility.
Urgent Care Services
Urgent Care services are for the treatment of symptoms that are non-life threatening but that require immediate attention. The patient must first attempt to receive care from his/her PCP. IPA will cover treatment at a participating Urgent Care Center without a referral.
Continue or Follow-up Treatment
Continuing or follow-up treatment, except by the PCP, whether in or out of service area, is not covered by IPA unless specifically authorized or approved by IPA. Payment for covered benefits outside the service area is limited to medically necessary treatment required before the patient can reasonably be transported to a participating hospital or returned to the care of the PCP.
Special Needs Plan Medicare Advantage Special Needs Plans (SNPs) are designed for specific groups of customers with special health care needs. These plans were developed by Medicare and ensure that a plan’s most vulnerable populations receive additional benefits and services based on their individual health care need. There are three SNP types.
• Condition-SNP is for members who have specific conditions, like Diabetes. This plan is focused on disease management. Therefore, in addition to receiving Medicare covered services, members will also receive benefits and services that are specific to the disease state.
• Dual Eligible-SNP is for members who have both Medicare and Medicaid coverage. This plan offers lower copayments and out of pockets costs and typically offer transportation benefits.
• Institutional SNP is for members who reside in an institutional setting.
Excluded Services
In addition to any exclusion or limitations described in the patient’s EOC, the following items and services are not covered under Original Medicare Plan or by IPA:
• Services that are not reasonable and necessary, according to the standards of the Original Medicare Plan, unless these services are otherwise listed by our plan as a covered service.
• Experimental or investigational medical and surgical procedures, equipment, and medications, unless covered by the Original Medicare Plan or unless, for certain services, the procedures are covered under an approved clinical trial. The Centers for Medicare & Medicaid Services (CMS) will continue to pay through Original Medicare for clinical trial items and services covered under the September 2000 National Coverage Determination that are provided to plan patients. Experimental procedures and items are those items and procedures determined by our plan and the Original Medicare Plan to not be generally accepted by the medical community.
• Surgical treatment of morbid obesity unless medically necessary or covered under the Original Medicare Plan.
• Private room in a hospital, unless medically necessary.
• Private duty nurses.
• Personal convenience items, such as a telephone or television in a patient’s room at a hospital or skilled nursing facility.
• Nursing care on a full-time basis in a patient’s home.
• Custodial care unless it is provided in conjunction with covered skilled nursing care and/or skilled rehabilitation services. This includes care that helps people with activities of daily living like walking, getting in and out of bed, bathing, dressing, eating, using the bathroom, preparation of special diets, and supervision of medication that is usually self-administered.
• Homemaker services.
• Charges imposed by immediate relatives or patients of the patient’s household.
5

• Meals delivered to the patient’s home.
• Elective or voluntary enhancement procedures, services, supplies, and medications including but not limited to: weight loss, hair growth, sexual performance, athletic performance, cosmetic purposes, anti-aging, and mental performance unless medically necessary.
• Cosmetic surgery or procedures, unless needed because of accidental injury or to improve the function of a malformed part of the body. All stages of reconstruction are covered for a breast after a mastectomy, as well as for the unaffected breast to produce a symmetrical appearance.
• Routine dental care (i.e. cleanings, fillings, or dentures) or other dental services unless otherwise specified in the EOC. However, non-routine dental services received at a hospital may be covered.
• Chiropractic care is generally not covered under the plan with the exception of manual manipulation of the spine and is limited according to Medicare guidelines.
• Routine foot care is generally not covered under the plan and is limited according to Medicare guidelines.
• Orthopedic shoes unless they are part of a leg brace and included in the cost of the brace. Exception: orthopedic or therapeutic shoes are covered for people with diabetic foot disease.
• Supportive devices for the feet. Exception: orthopedic or therapeutic shoes are covered for people with diabetic foot disease.
• Hearing aids and routine hearing examinations unless otherwise specified in the EOC.
• Eyeglasses, with the exception of after cataract surgery, routine eye examinations, radical keratotomy, LASIK surgery, vision therapy, and other low vision aids and services unless otherwise specified in the EOC.
• Self-administered prescription medication for the treatment of sexual dysfunction, including erectile dysfunction, impotence, and anorgasmy or hyporgasmy unless otherwise included in the patient’s Part D benefit. Please see the formulary for details.
• Reversal of sterilization measures, sex change operations, and non-prescription contraceptive supplies.
• Acupuncture
• Naturopath services
• Services provided to veterans in Veterans Affairs (VA) facilities. However, in the case of emergency situations received at a VA hospital, if the VA cost-sharing is more than the cost-sharing required under the plan, the plan will reimburse veterans for the difference. Patients are still responsible for our plan cost-sharing amount.
Any of the services listed above that are not covered will
remain not covered even if received at an emergency facility. For example, non-authorized, routine conditions that do not appear to a reasonable person to be based on a medical emergency are not covered if received at an emergency facility.
Grievance and Appeal Process
All telephonic inquiries received by IPA’s Medicare Advantage Customer Service Department will be resolved on an informal basis, except for inquiries that involve “appealable” issues. Appealable issues will be routed through either the standard or expedited appeal process. In situations where a patient is not in agreement with the informal resolution, the patient must submit a written request for reconsideration. All other written correspondence received by IPA will be documented and routed through the appropriate appeal or grievance channels.
Patients have the right to file a complaint, also referred to as a grievance, regarding any problems they observe or experience with the health plan. Situations for which a grievance may be filed include but are not limited to:
• Complaints about services in an optional Supplementary Benefit package.
• Dissatisfaction with the office experience such as excessive wait times, physician behavior or demeanor, or inadequacy of facilities.
• Involuntary disenrollment situations.
• Poor quality of care or service received.
Patients have the right to appeal any decision about IPA’s failure to provide what they believe are benefits contained in the basic benefit package. These include:
• Reimbursement for urgently needed care outside of the service area or Emergency Services worldwide.
• A denied claim for any health services furnished by a non-participating provider or supplier they believe should have been provided, arranged for, or reimbursed by IPA.
• Services not received, but believed to be the responsibility of IPA.
• A reduction or termination of a service a patient feels medically necessary.
In addition, a patient may appeal any decision related to a hospital discharge. In this case, a notice will be given to the patient with instructions for filing an appeal. The patient will remain in the hospital while the appeal documentation is reviewed. The patient will not be held liable for charges incurred during this period, regardless of the outcome of the review. Please refer to the Evidence of Coverage (EOC) for additional benefit information.
6

ELIGIBILITY GUARANTEE FORM
_______________ Date I, _______________________________ hereby certify that I am eligible for Health Plan Member Name Coverage with ______________________ as of ___________________________ Health Plan Name Month/Day/Year through ___________________________________.
Employer Group (if applicable) I have chosen _______________________________________ Physician’s Name to be my Primary Care Physician. I understand that if the above is not true or if I am not eligible under the terms of my Medical and Hospital Subscriber Health Insurance Agreement, I am liable for all charges for the services rendered. In addition, if the above is not true, I agree to pay in full for all services received within 30 days of receiving a bill from the above noted medical provide. _____________________________ ________________________ Signature of Member (or Guardian) Office Personnel _____________________________ Printed Name of Member (or Guardian)
Eligibility Guarantee Form
7

FORMA DE GARANTÍA DE ELEGIBILIDAD
_______________ Fecha El suscrito, __________________________________________ por este medio certifico que soy elegible para Nombre del miembro la cobertura del plan de atención médica de _________________________________ a partir del _________ Nombre del Plan de atención médica Mes/Día/Año A través de ___________________________________. He elegido a _______________________ ____ Grupo empleador (si aplica) Nombre del médico para que sea mi médico de cabecera. Entiendo que si la información anterior es falsa, o si no soy elegible de conformidad con los términos de mi
Contrato de seguro de atención médica y hospitales, seré responsable de pagar el costo de los servicios que
haya recibido. Además, si la información anterior no es verdadera, acuerdo pagar el costo total de los servicios
que reciba en un término de 30 días después de recibir la factura del proveedor médico arriba indicado
_____________________________ ________________________ Firma del miembro (o Tutor) Personal de la oficina _________________________________ Nombre completo del miembro (o Tutor)
Forma de Garantía de Elegibilidad
8

PROVIDER INFORMATION
Providers Designated as Primary Care Physicians (PCPs)
The IPA recognizes Family Medicine, General Practice, Geriatric Medicine, and Internal Medicine physicians as Primary Care Physicians (PCPs). Any employed mid-level practitioners rendering services must be listed on contracts and will not be assigned patients but will have data aggregated at their level for purposes of reporting.
The IPA may recognize Infectious Disease Physicians as PCPs for patients who may require a specialized physician to manage their specific health care needs.
All contracted credentialed providers participating with IPA are listed in the region-appropriate Provider Directory, which is provided to patients and made available to the public.
The Role of the Primary Care Physician (PCP)
Each patient must select an IPA Participating Primary Care Physician (PCP) at the time of enrollment. The PCP is responsible for managing all the health care needs of patients as follows:
• Manage the health care needs of patients who have chosen the physician as their PCP.
• New Patients Initial visits should be scheduled with provider (physician) within 90 days of enrollment,
• On the Member’s first visit to the provider office and within 60 days of enrollment, patient should be seen by the physician, if prior visits have been handled by PA or NP.
• Physician is to be available for questions at all scheduled visits when supervising a PA or NP and to review all referrals and coding and quality initiatives before submission to ensure accuracy and appropriateness.
• All visits and care should abide by CMS guidelines.
• Ensure that patients receive treatment as frequently as is necessary based on the patient’s condition.
• Develop an individual treatment plan for each patient.
• Submit accurately and timely claims and encounter information for clinical care coordination.
• Comply with pre-authorization and referral procedures.
• Refer patients to designated IPA participating providers.
• Comply with Quality Management and Utilization Management programs.
• Participate in health plan directed Coding and Quality Initiatives.
• Use appropriate health plan designated ancillary and facility providers.
• Comply with emergency care procedures.
• Comply with access and availability standards as outlined in this manual, including after-hours care.
• Bill on the CMS 1500 claim form, preferably electronically, in accordance with billing procedures.
• Ensure that, when billing for services provided, coding is specific enough to capture the acuity and complexity of a patient’s condition and ensure that the codes submitted are supported by proper documentation in the medical record.
• Comply with health plan Preventive Screening and Clinical Guidelines.
• Adhere to medical record standards as outlined in this manual.
The Role of the Specialist Physician
Each patient is entitled to see a Specialist Physician for certain services required for treatment of a given health condition. The Specialist Physician is responsible for managing all the health care needs of a Participating Plan’s patient as follows:
• Provide specialty health care services to patients as needed.
• Collaborate with the patient’s Primary Care Physician to enhance continuity of health care and appropriate treatment.
• Provide consultative and follow-up reports to the referring physician within 72 hours of encounter.
• Comply with access and availability standards as outlined in this manual including after-hours care.
• Comply with pre-authorization and referral process.
• Comply with Quality Management and Utilization Management programs.
• Bill on the CMS 1500 claim form in accordance with billing procedures.
• Ensure that, when billing for services provided, coding is specific enough to capture the acuity and complexity of a patient’s condition and ensure that the codes submitted are supported by proper documentation in the medical record.
• Refer patients to designated IPA participating providers.
• Use appropriate health plan designated ancillary and facility providers.
• Submit encounter information accurately and timely.
• Adhere to medical record standards as outlined in this manual.
Administrative, Medical, and Reimbursement Policy Changes
From time to time, the IPA may amend, alter, or clarify its policies. Examples of this include, but are not limited to, regulatory changes, changes in medical standards, and
9

modification of Covered Services. Specific IPA policies and procedures may be obtained by calling our Provider Services Department at 1-832-553-3300.
The IPA’s will communicate changes to the Provider Manual using a variety of methods including but not limited to:
• Annual Provider Manual Updates
• Letter
• Facsimile
• Provider Newsletters
Providers are responsible for the review and inclusion of policy updates in the Provider Manual and for complying with these changes upon receipt of these notices.
Communication among Providers
• The PCP should provide the Specialist Physician with relevant clinical information regarding the patient’s care at the time of referral.
• The Specialist Physician must provide the PCP with information about his/her visit with the patient within 72 hours of encounter.
• The PCP must document in the patient’s medical record his/her review of any reports, labs, or diagnostic tests received from a Specialist Physician.
Provider Marketing Guidelines
The general guidelines assist Plan providers who have contracted with multiple Medicare Advantage plans and accept Medicare FFS patients determine what marketing and patient outreach activities are permissible under the CMS guidelines. CMS has advised Medicare Advantage plans to prohibit providers from steering, or attempting to steer an undecided potential enrollee toward a specific plan, or limited number of plans, offered either by the plan sponsor or another sponsor, based on the financial interest of the provider or agent. Providers should remain neutral parties in assisting plans to market to beneficiaries or assisting in enrollment decisions.
Provider Can:
• Mail/call their patient panel to invite patients to general IPA’s sponsored educational events to learn about the Medicare and/or Medicare Advantage program. This is not a sales/marketing meeting. No sales representative or plan materials can be distributed. Sales representative cards can be provided upon request.
• Mail an affiliation letter one time to patients listing only IPA.
• Have additional mailings (unlimited) to patients about participation status but must list all participating Medicare Advantage plans and cannot steer towards a specific plan. This letter may not quote specific plan benefits without prior CMS approval and the agreement of all plans listed.
• Notify patients in a letter of a decision to participate in an IPA’s sponsored programs.
• Utilize a physician/patient newsletter to communicate information to patients on a variety of subjects. This newsletter can have an IPA corner to advise patients of IPA’s information.
• Provide objective information to patients on specific plan formularies, based on a patient’s medications and health care needs.
Refer patients to other sources of information, such as the State Health Insurance Assistance Program (SHIP), IPA’s marketing representatives, state Medicaid, or 1-800-Medicare
to assist the patient in learning about the plan and making a health care enrollment decision.
• Display and distribute in provider offices IPA’s MA and MAPD marketing materials, excluding application forms. The office must display or offer to display materials for all participating MA plans.
• Notify patients of a physician’s decision to participate exclusively with an IPA for Medicare Advantage or to close panel to original Medicare FFS if appropriate.
• Record messages on our auto dialer to existing IPA’s patients as long as the message is not sales related or could be construed as steerage. IPA’s Legal /Government programs must review the script.
• Have staff dressed in clothing with the Participating Plan’s logo.
• Display promotions items with the IPA logo.
• Allow IPA to have a room/space in provider offices completely separate from where patients have a prospect of receiving health care, to provide beneficiaries’ access to an IPA’s sales representative.
Provider Cannot:
• Quote specific health plan benefits or cost share in patient discussions.
• Urge or steer towards any specific plan or limited set of plans.
• Collect enrollment applications in physician offices or at other functions.
• Offer inducements to persuade beneficiaries to enroll in a particular plan or organization.
• Health Screen potential enrollees when distributing information to patients, as health screening is prohibited.
• Expect compensation directly or indirectly from the plan for beneficiary enrollment activity.
• Call patients who are disenrolling from the health plan to encourage re-enrollment in a health plan.
• Mail notifications of health plan sales meetings to patients.
• Call patients to invite patients to sales, and marketing activity of a health plan.
10

• Advertise using IPA’s name without IPA’s prior consent and potentially CMS approval depending upon the content of the advertisement.
Provider Participation
Providers must be contracted with and credentialed by IPA according to the following guidelines:
Provider Status Action
New to plan and not previously credentialed
Practicing in a solo practice
Requires a signed contract and initial credentialing
New to plan and not previously credentialed
Joining a participating group practice
Requires initial credentialing
Already participating and credentialed
Leaving a group practice to begin a solo practice
Does not require credentialing; however a new contract is required and the previous group practice affiliation is terminated
Already participating and credentialed
Leaving a participating group practice to join another participating group practice
Does not require credentialing yet the group practice affiliation will be amended
Already participating and credentialed
Leaving a participating group practice to join a non-participating group practice
The provider’s participation is terminated unless the non-participating group signs a contract with IPA. Credentialing is still valid until re-credentialing due date
PHYSICIAN RIGHTS AND RESPONSIBILITIES Physician Rights:
• IPA encourages your feedback and suggestions on how service may be improved within the organization.
• If an acceptable patient-physician relationship cannot be established with an IPA patient who has selected you
as his/her Primary Care Physician, you may request that IPA have that patient removed from your care.
• You may request claims reconsideration on any claims submissions in which you feel are not paid according to payment policy.
• You may request an appeal on any claims submission in which you feel are not paid in keeping with the level of care rendered or clinical guidelines.
• You may request to discuss any referral request with the Medical Director or Chief Medical Officer after various times in the review process, before a decision is rendered or after a decision is rendered.
Physician Responsibilities:
• You have agreed to treat all IPA patients the same as all other patients in your practice, regardless of the type or amount of reimbursement.
• Primary Care Physicians must provide continuous 24 hours, 7 days a week access to care for Health Plan patients. During periods of unavailability or absence from the practice, you must arrange coverage for your members. Please notify the IPA of the physician who is providing coverage for your practice.
• Primary Care Physicians shall use best efforts to provide patient care to new patients within three (3) months of enrollment with IPA.
• Primary Care Physicians shall use best efforts to provide follow-up patient care to patients that have been in the hospital setting within ten (10) days of hospital discharge.
• Primary Care Physicians are responsible for the coordination of routine preventive care along with any ancillary services that need to be rendered with authorization.
• All providers are required to code to the highest level of specificity necessary to describe a patient’s acuity level. All coding should be conducted in accordance with CMS guidelines and all applicable state and federal laws.
• All providers are required to actively promote and participate in all quality initiatives inclusive of any and all chart audits, patient preventive care, and patient satisfaction activities.
• Specialists must provide specialty services upon referral from the Primary Care Physician and work closely with the referring physician regarding the treatment the patient is to receive. Specialists must also provide continuous 24 hour, 7 days a week access to care for patients.
• Specialists are required to coordinate the referral process (i.e. obtain authorizations) for further care that they recommend. This responsibility does not revert back to the Primary Care Physician while the care of the patient is under the direction of the Specialist.
11

• In the event you are temporarily unavailable or unable to provide patient care or referral services to an IPA patient, you must arrange for another IPA physician to provide such services on your behalf. This coverage cannot be provided by an Emergency Room. For capitated physicians, the covering physician must agree to seek payment for services rendered to your patients from you only, but submit an encounter to the IPA with proper notation for covering services.
• You have agreed to treat Participating Plan’s patients the same as all other patients in your practice, regardless of the type or amount of reimbursement.
• You have agreed to provide continuing care to participating patients.
• You have agreed to utilize IPA participating physicians/facilities when services are available and can meet your patient’s needs. Approval prior to referring outside of the contracted network of providers may be required.
• You have agreed to participate in IPA’s peer review activities as they relate to the Quality Management/Utilization Review program.
• You have agreed to allow IPA Inpatient Managers to follow your patients in the hospital and other inpatient settings.
• You may not balance bill a patient for providing services that are covered by IPA. This excludes the collection of standard copays. You may bill a patient for a procedure that is not a covered benefit if you have followed the appropriate procedures outlined in the “Claims” section of this manual.
• You have agreed to provide the IPA Encounter Data for all services outlined in the “Encounter Data” section of this manual. Such data must be received within 95 days from the date of service. Any data received after 95 days will not be included in true-up or any other financial calculations.
• All claims must be received within 95 days from the date of service or the timeframe specified in your contract.
• Required adoption and usage of portals and software applications available to physicians for quality and cost management as well as care coordination.
Patient Assignment to New PCP
IPA’s Primary Care Physicians have a limited right to request a patient be assigned to a new Primary Care Physician. A provider may request to have a patient moved to the care of another provider due to the following behaviors:
• Fraudulent use of services or benefits
• The patient is disruptive, unruly, threatening, or uncooperative to the extent that patient seriously impairs IPA’s or the provider’s ability to provide services to the patient or to obtain new patients and the
aforementioned behavior is not caused by a physical or behavioral health condition.
• Threats of physical harm to a provider and/or office staff.
• Non-payment of required copayment for services rendered.
• Receipt of prescription medications or health services in a quantity or manner, which is not medically beneficial or not medically necessary.
• Repeated refusal to comply with office procedures essential to the functioning of the provider’s practice or to accessing benefits under the managed care plan.
• The patient is steadfastly refusing to comply with managed care restrictions (e.g., repeatedly using the emergency room in combination with refusing to allow the managed care organization to coordinate treatment of the underlying medical condition).
The provider should make reasonable efforts to address the patient’s behavior, which has an adverse impact on the patient/physician relationship, through education and counseling, and if medically indicated referral to appropriate specialists.
If the patient’s behavior cannot be remedied through reasonable efforts, and the PCP feels the relationship has been irreparably harmed, the PCP should complete the patient transfer request form and submit it to IPA.
IPA will research the concern and decide if the situation warrants requesting a new PCP assignment. If so, IPA will document all actions taken by the provider and IPA to cure the situation. This may include patient education and counseling. An IPA PCP cannot request a disenrollment based on adverse change in a patient’s health status or utilization of services medically necessary for treatment of a patient’s condition.
Procedure
• Once the IPA Medical Director has reviewed the PCP’s request and determined that the physician/patient relationship has been irreparably harmed, the patient will receive a minimum of thirty (30) days’ notice that the physician/patient relationship will be ending. Notification must be in writing, by certified mail, and IPA must be copied on the letter sent to the patient.
• The physician will continue to provide care to the patient during the thirty (30) day period or until the patient selects or is assigned to another physician. The IPA will assist the patient in establishing a relationship with another physician.
• The physician will transfer, at no cost, a copy of the medical records of the patient to the new PCP and will cooperate with the patient’s new PCP in regard to transitioning care and providing information regarding the patient’s care needs.
A patient may also request a change in PCP for any reason. The PCP change that is requested by the patient will be
12

effective the first (1st) of the month following the receipt of the request, unless circumstances require an immediate change.
Closing Patient Panels
When a participating Primary Care Physician elects to stop accepting new patients, the provider’s patient panel is considered closed. If a participating Primary Care Physician closes his or her patient panel, the decision to stop accepting new patients must apply to all patients regardless of insurance coverage. Providers may not discriminate against patients by closing their patient panels for IPA’s patients only, nor may they discriminate among patients by closing their panel to certain product lines. Providers who decide that they will no longer accept any new patients must notify the Network Management Department, in writing, at least 60 days before the date on which the patient panel will be closed or the time frame specified in your contract.
Medical Record Standards
The IPA requires the following items in patient medical records:
• Identifying information of the patient.
• Identification of all providers participating in the patient’s care and information on services furnished by these providers.
• A problem list, including significant illnesses and medical and psychological conditions.
• Presenting complaints, diagnoses, and treatment plans.
• Prescribed medications, including dosages and dates of initial or refill prescriptions.
• Information on allergies and adverse reactions (or a notation that the patient has no known allergies or history of adverse reactions).
• Information on advanced directives.
• Past medical history, physical examinations, necessary treatments, and possible risk factors for the patient relevant to the particular treatment.
Note: Unless otherwise specifically stated in your provider services agreement, medical records shall be provided at no cost to IPA and IPA patients.
Access and Availability Standards for Providers
A Primary Care Physician (PCP) must have their primary office open to receive patients five (5) days and for at least 20 hours per week. The PCP must ensure that coverage is available 24 hours a day, seven days a week. PCP offices must be able to schedule appointments for patients at least two (2) months in advance of the appointment. A PCP must arrange for coverage during absences with another participating provider in an appropriate specialty, which is documented on the Provider Application and agreed upon in the Provider Agreement.
Primary Care Access Standards
Appointment Type Access Standard
Urgent Immediately
Non-Urgent/Non-Emergent Within one (1) week
Routine and Preventive Within 30 Business Days
On-Call Response (After Hours) Within 30 minutes for emergency
Waiting Time in Office 30 minutes or less
Specialist Access Standards
Appointment Type Access Standard
Urgent Immediately
Non-Urgent/Non-Emergent Within one (1) week
Elective Within 30 days
High Index of Suspicion of Malignancy
Less than seven (7) days
Waiting time in office 30 minutes or less
Behavioral Health Access Standards
Appointment Type Access Standard
Emergency Within 6 hours of the referral
Urgent/Symptomatic Within 48 hours of the referral
Routine Within ten (10) business days of the referral*
After-hours Access Standards
All participating providers must return telephone calls related to medical issues. Emergency calls must be returned within 30 minutes of the receipt of the telephone call. Non-emergency calls should be returned within a 24-hour time period. A reliable 24 hours a day/7 days a week answering service with a beeper or paging system and on-call coverage arranged with another participating provider of the same specialty is preferred.
Plan Notification Requirements for Providers
Participating providers must provide written notice to IPA no less than 60 days in advance of any changes to their practice or, if advance notice is not possible, as soon as possible thereafter.
The following is a list of changes that must be reported to
13

by contacting your Network Operation Representative:
• Practice address
• Billing address
• Fax or telephone number
• Hospital affiliations
• Practice name
• Providers joining or leaving the practice (including retirement or death)
• Provider taking a leave of absence
• Practice mergers and/or acquisitions
• Adding or closing a practice location
• Tax Identification Number (please include W-9 form)
• NPI number changes and additions
• Changes in practice office hours, practice limitations, or gender limitations
By providing this information in a timely manner, you will ensure that your practice is listed correctly in the Provider Directory.
Please note: Failure to provide up to date and correct information regarding demographic information regarding your practice and the physicians that participate may result in the denial of claims for you and your physicians.
Provision of Health Care Services
Participating providers shall provide health care services to all patients, consistent with the benefits covered in their policy, without regard to race, ethnicity, national origin, religion, sex, age, mental or physical disability or medical condition, sexual orientation, claims experience, medical history, evidence of insurability (including conditions arising out of acts of domestic violence), genetic information, source of payment, or any other bases deemed unlawful under federal, state, or local law.
Participating providers shall provide covered services in a culturally competent manner to all patients by making a particular effort to ensure those with limited English proficiency or reading skills, diverse cultural and ethnic backgrounds, and physical or mental disabilities receive the health care to which they are entitled. Examples of how a provider can meet these requirements include but are not limited to: translator services, interpreter services, teletypewriters or TTY (text telephone or teletypewriter phone) connection.
IPA offers interpreter services and other accommodations for the hearing-impaired. Translator services are made available for non-English speaking or Limited English Proficient (LEP) patients. Providers can call IPA customer service at 832-553-3300 to assist with translator and TTY services if these services are not available in their office location.
Inpatient Manager Program
IPA requires that in certain IPA PODs, patients admitted to participating health care facilities should be assigned to the designated Inpatient Manager (IPM) for coordination of care throughout the entire stay. Health care facilities will receive notice of the designated Inpatient Manager and are required to follow the proper protocol of assigning patients to the designated Inpatient Manager.
Dispute Resolution
Any controversy, dispute or claim arising out of or relating to your Provider Agreement (“Agreement”) or the breach thereof, including any question regarding its interpretation, existence, validity or termination, that cannot be resolved informally, shall be resolved by arbitration in accordance with this Section, provided however that a legal proceeding brought by a third party against IPA, an Affiliate, provider, or any provider (“Defendant”), any cross-claim or third party claim by such Defendant against IPA, an Affiliate, provider, or any provider Facility shall not be subject to arbitration. In the event arbitration becomes necessary, such arbitration shall be initiated by either Party making a written demand for arbitration on the other Party. The arbitration shall be conducted in the county were the majority of the services are performed, in accordance with the Commercial Arbitration Rules of the American Arbitration Association, as they are in effect when the arbitration is conducted, and by an arbitrator knowledgeable in the health care industry. The Parties agree to be bound by the decision of the arbitrator. The Parties further agree that the costs, fees and expenses of arbitration will be borne by the non-prevailing party. Notwithstanding this Agreement to arbitrate IPA, an Affiliate, provider, or any provider Facility may seek interim and/or permanent injunctive relief pursuant to this Agreement in the county were the majority of the services are performed in any court of competent jurisdiction. With respect to disputes arising during the life of this Agreement, this Section shall survive the termination or expiration of the Agreement.
14

STARS GUIDANCE The Centers for Medicare & Medicaid Services (CMS) uses the Five-Star Quality Rating System to determine how much to compensate Medicare Advantage plans and educate consumers on health plan quality. The Star Ratings system consists of over 50 measures from five different rating systems. The cumulative results of these measures make up the Star rating assigned to each health plan.
Star Ratings have a significant impact on the financial outcome of Medicare Advantage health plans by directly influencing the bonus payments and rebate percentages received. CMS will award quality-based bonus payments to high performing health plans based on their Star Ratings performance. For health plans with a four star or more rating, a bonus payment is paid in the form of a percentage (maximum of five percent) added to the county benchmark. (A county benchmark is the amount CMS expects it to cost to provide hospital and medical insurance in the state and county.) After 2015, any health plans with Star Ratings below four will no longer receive bonus payments.
Star Rating Components
The Star Rating is comprised of over 50 different measures from six different rating systems:
Star Rating System:
• HEDIS-The Health Care Effectiveness Data and Information Set is a set of performance measures developed for the managed care industry. All claims are processed regularly to extract the NCQA (National Committee for Quality Assurance) defined measures. For example, this allows the health plan and CMS to determine how many enrollees have been screened for high blood pressure.
• CAHPS- Consumer Assessment of Health Care Providers and Systems is a series of patient surveys rating health care experiences performed on behalf of CMS by an approved vendor.
• CMS- Centers for Medicare & Medicaid Services rates each plan on administrative type metrics, such as, beneficiary access, complaints, call center hold times, and percentage of patients choosing to leave a plan.
• PDE- Prescription Drug Events is data collected on various medications related events, such as high-risk medications, adherence for chronic conditions, and pricing.
• HOS- Health Outcomes Survey is a survey that uses patient-reported outcomes over a 2.5-year time span to measure health plan performance. Each spring a random sample of Medicare beneficiaries is drawn from each participating Medicare Advantage Organization (MAO) that has a minimum of 500 enrollees and is surveyed. Two years later, these same respondents are surveyed again (i.e., follow up measurement).
• IRE- Medicare Advantage plans are required to submit all denied enrollee appeals (Reconsiderations) to an Independent Review Entity (MAXIMUS Federal Services).
These systems rate the plans based on six domains:
1. Staying healthy: screenings, tests and vaccines
2. Managing chronic (long term) conditions
3. Patient experience with health plan
4. Patient complaints, problems getting services, and improvement in the health plan’s performance
5. Health plan customer service
6. Data used to calculate the ratings comes from surveys, observation, claims data, and medical records.
CMS continues to evolve the Star Ratings system by adding, removing and adjusting various measures on a yearly basis.
CMS weights each measure between one and three points. A three-point measure, or triple weighted measure, are measures that CMS finds most important and should be a focus for health plans. The composition of all rating systems is indicated below.
Health Reform
The Patient Protection and Affordable Care Act (PPACA) requires that Medicare Advantage (MA) plans be awarded quality-based bonus payments beginning in 2012, as measured by the Star Ratings system. Bonus payments are provided to MA plans that receive four or more stars.
CMS assigns a benchmark amount to each county within a state, which is the maximum amount CMS will pay to provide hospital and medical benefits. All MA plans submit a bid, which is the projected cost to operate MA within the county. The spread between the bid and original benchmark is called the rebate. A bonus payment is the percentage added to the county benchmark, which increases the spread and the amount of revenue received by the health plan.
15

Healthcare Plan Effectiveness Data Information Set (HEDIS®) HEDIS (a standardized data set) is developed and maintained by the National Committee for Quality Assurance (NCQA), an accrediting body for managed care organizations. The HEDIS measurements enable comparison of performance among managed care plans. The sources of HEDIS data include administrative data (claims/encounters) and medical record review data. HEDIS measurements include measures such as Comprehensive Diabetes Care, Adult Access to Ambulatory and Preventive Care, Glaucoma Screening for Older Adults, Controlling High Blood Pressure, Breast Cancer Screening, and Colorectal Cancer Screening.
Plan-wide HEDIS measures are reported annually and represent a mandated activity for health plans contracting with the Centers for Medicare & Medicaid Services (CMS). Each spring, the Participating Plan Representatives will be required to collect from practitioner offices copies of medical records to establish HEDIS scores. Selected practitioner offices will be contacted and requested to assist in these medical record collections.
All records are handled in accordance with Participating Plan’s privacy policies and in compliance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy rules. Only the minimum necessary amount of information, which will be used solely for the purpose of this HEDIS initiative, will be requested. HEDIS is considered a quality-related health care operation activity and is permitted by the HIPAA Privacy Rule [see 45 CFR 164.501 and 506].
Participating Plan’s HEDIS results are available upon request. Contact the Health Plan’s Quality Improvement Department to request information regarding those results.
HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
Star Measure Weighting
Individual Star measures can be single-weighted, 1.5-weighted or triple-weighted, with higher weight being given to those measures that CMS deems most important by which to measure plan quality. Triple-weighted measures are typically outcomes measures that measure a health plan’s ability to manage chronic illnesses and keep patients healthy. Certain disease states appear in multiple measures. For example, diabetes directly impacts 7 measures and cardiovascular conditions directly impact 4 measures.
Following is a summary of the weighting of all Star measures:
Part C Star Rating Measure Weight Breast Cancer Screening (HEDIS) 1
Colorectal Cancer Screening (HEDIS) 1
Annual Flu Vaccine (CAHPS) 1
Improving/Maintaining Physical Health (HOS) 3
Monitoring Physical Activity (HOS) 1
Adult BMI Assessment (HEDIS) 1
Care For Older Adults -- Medication Review (HEDIS) 1
Care For Older Adults -- Pain Screening (HEDIS) 1
Care For Older Adults -- Functional Status (HEDIS 1
Osteoporosis Fracture Management (HEDIS) 1
Comprehensive Diabetes Care -- Eye Exam (HEDIS) 1
Comprehensive Diabetes Care -- Kidney Disease (HEDIS) 1
Comprehensive Diabetes Care -- HBA1C ≤ 9 (HEDIS) 3
Controlling Blood Pressure (HEDIS) 3
Rheumatoid Arthritis Management (HEDIS) 1
Reducing Risk Of Falling (HOS) 1
Managing Urinary Incontinence 1
Plan All Cause Readmissions (HEDIS) 3
Medication Reconciliation Post Discharge (HEDIS) 1
Getting Needed Care Without Delays (CAHPS) 1.5
Getting Appointments And Care Quickly (CAHPS) 1.5
Customer Service (CAHPS) 1.5
Overall Rating Of Health care Quality (CAHPS) 1.5
Overall Rating Of Plan (CAHPS) 1.5
Care Coordination (CAHPS) 1.5
Complaints About The Health Plan (CTM) 1.5
Beneficiary Access And Performance Problems (CMS) 1.5
Patients Choosing To Leave The Plan (CMS) 1.5
Improvement (CMS) 3
Plan makes Timely Decisions About Appeals (IRE) 1.5
Reviewing Appeals Decisions (IRE) 1.5
Foreign language Interpreter and TTY/TDD Availability (Call Center)
1.5
Part D Star Rating Measure
Foreign language Interpreter and TTY/TDD Availability (Call Center)
1.5
Appeals Autoforward (IRE) 1.5
Appeals Upheld (IRE) 1.5
Complaints About The Health Plan (CTM) 1.5
Beneficiary Access And Performance Problems (CMS) 1.5
Patients Choosing To Leave The Plan (CMS) 1.5
Improvement (CMS) 3
Rating Of Drug Plan (CAHPS) 1.5
Getting Needed Prescription Drugs (CAHPS) 1.5
MPF Pricing Accuracy (PDE) 1
High Risk Medications (PDE) 3
Diabetes Treatment (PDE) 3
Medication Adherence For Oral Diabetes Medications (PDE) 3
Medication Adherence For Hypertension (PDE) 3
Medication Adherence For Cholesterol (PDE) 3
16

Star Rating Timeline
The Star rating process follows a unique lag timeline that must be iterated. Each year, CMS publishes health plan ratings in October which encompass data collected in the previous year. After ratings are determined, bonuses payments can be included in the bid process for the following year. This means that actions taken to affect Stars in a given year take almost three years to realize financially. For example:
Year 1 Year 2 Year 3 Year 4 Year 5
CY2017 CY2018 CY2019 CY2020 CY2021
2019 Star Rating (Publish Oct. 2018)
Quality Activities to Impact 2019 Rating
2019 Rating Published (Oct.)
2019 Rating Included in 2020 Bid Process
2019 Rating Bonuses Distributed
N/A
Please bill CPT II codes for all contracted Medicare Advantage plans—Cigna HealthSpring and BCBS MA
Using CPT II codes will limit the number of charts requested from your office the following calendar year.
MEDICARE ADVANTAGE HEDIS CPT II CODES
BLOOD PRESSURE (SYSTOLLIC)
CPT II Description
3074F BP < 130 mmHg
3075F BP 130-139 mmHg
3077F BP > = 140mmHg
CARE OF OLDER ADULTS
SUB MEASURE CPT II Description
PAIN SCREEN 1125F Pain present
1126F No pain present
MEDICATION REVIEW
*(Both 1159F and 1160F should be billed together
1159F* Medication list documented in medical record
1160F* Review of all medications by prescriber documented in
MEDICATION RECONCILIATION POST-DISCHARGE
CPT II Description
1111F Medication Reconciliation after discharge
BLOOD PRESSURE (DIASTOLLIC)
CPT II Description
3078F BP < 80 mmHg
3079F BP 80-89 mmHg
3080F BP > = 90mmHg
17

to the measure) medical record
FUNCTIONAL STATUS 1170F Patient functional status assessed
ADVANCE CARE
PLANNING
1157F Advanced Care Plan or similar legal document
1158F Advanced Care Plan discussion documented in the medical
record
COMPREHENSIVE DIABETES CARE
SUB MEASURE CPT II Description
A1C 3044F Most recent A1C < 7.0%
3045F Most recent A1C between 7.0 – 9.0%
3046F Most recent A1c > 9.0%
RETINAL EYE EXAM
(CPT Code 2022F should be billed with CPT 92250 by the PCP performing fundus photography)
3072F Low risk for retinopathy current year
2022F Dilated retinal eye exam interpreted by an
ophthalmologist/optometrist 2024F 7 standard filed stereoscopic
photos w/interpretation by eye care professional
documented/reviewed 2026F Eye imaging validated to match
diagnosis from 7 standard stereoscopic photos results
documented/reviewed ATTENTION FOR NEPHROPATHY
3060F Positive microalbuminuria test result documented
3061F Negative microalbuminuria test result documented
3062F Positive microalbuminuria test result documented (confirm + with lab results)
3066F Documentation of treatment for nephropathy (dialysis, ESRD, CRF, ARF, renal insufficiency, nephrologist visit)
18

4010F ACEI or ARB therapy prescribed or currently being taken
19

PROVIDER REQUEST FOR PATIENT TO TRANSFER CARE TO ANOTHER PROVIDER
The providers in the IPA strive to promote the health and wellness of the patients in managed care plans through participation in a quality, comprehensive, preventive, and therapeutic health care delivery system.
A strong physician/patient relationship is one of the most important factors necessary to accomplish that mission. When there is a breakdown in the patient/physician relationship, it may be in the best interest of all concerned to have the patient transfer to another provider. Having an expedient process for handling such requests, and effecting transfers when appropriate, should have a positive impact on both patient satisfaction and provider morale.
The requesting provider needs to take the appropriate steps to ensure that the transferring patient has continued access to care during the transitional period.
Procedure
A provider may request to have a patient transfer to another provider due to the following behaviors:
• Fraudulent use of services or benefits.
• Threats of physical harm to a provider or office staff.
• Non-payment of required copay for services rendered.
• Receipt of prescription medications or health services in a quantity or manner, which is not medically beneficial or medically necessary.
• Refusal to accept a treatment or procedure recommended by the provider. If refusal is incompatible with the continuation of the patient/physician relationship, the provider should indicate if he/she believes that no professionally acceptable alternative treatment or procedure exists.
• Repeated refusal to comply with office procedures essential to the functioning of the provider’s practice or to accessing benefits under the managed care plan
• Other behavior that has resulted in serious disruption of the patient/ physician relationship.
• The provider should make reasonable efforts to address patient behavior that has an adverse impact on the patient/physician relationship, through education and counseling, and, if medically indicated, referral to appropriate specialists. Such efforts, including efforts to educate the patient regarding office procedures and treatment recommendations, should be carefully
documented. A sample letter to address patient education is provided.
A provider who wants to request that a patient transfer to the care of another provider should submit the following to the IPA office: • Completed form: Physician Requests Transfer of
Patient from Panel
• Attach all supporting documentation indicating efforts that have been made to counsel/educate the patient on the importance of being compliant (i.e., letter to patient, medical records, chart notes, documentation of missed appointments, and calls/reminders to the patient).
• Send the form and all supporting documentation to the Provider Relations Representative of the IPA.
• The IPA Medical Advisor reviews all provider requests for adequacy and appropriateness.
The IPA forwards provider requests to the managed care plan for action. The IPA office logs and tracks the provider requests and follows up once a week with the managed care plan.
During the period the provider’s request is being processed by the IPA/managed care plan, the provider should continue to provide care to the patient. It is expected that the managed care plan will respond to a provider’s request within seven (7) calendar days of receipt. The provider should be aware that the managed care plan may share the provider’s request/documentation with the affected patient. If the managed care plan is not able to salvage the relationship, the IPA will be notified. At that time, the requesting provider may, if they choose, notify the patient in writing of thirty (30) day notice to select another provider in accordance with State law.
Generally, it is the responsibility of the managed care plan to send the patient notice that he or she must transfer to another provider. It is expected that the managed care plan will send a copy of such notice to both the IPA and the requesting provider. The IPA expects the managed care plan to instruct the patient to select a new provider within thirty (30) days of receiving the notice (transitional period).
The requesting physician must provide care to the patient during the thirty (30) day transitional period. When the patient selects a new provider, the managed care plan will promptly inform the requesting provider so proper measures can be made to complete the transfer process. If the patient fails to pick a new provider after the thirty (30) day transitional period, the managed care plan will assign the patient to a new provider.
20

PHYSICIAN REQUESTS TRANSFER OF MEMBER FROM PANEL Physician Name: ___ POD: _____________________________ The member referenced below is not following the accepted standards set by our office in order to maintain an effective treatment plan or a satisfactory patient/physician relationship. The information below is provided so that the Health Plan can notify the member of such termination request advising his/her to select a new Primary Care Physician. MEMBER NAME: ID# HEALTH PLAN: Renaissance Physicians (RP) This member has displayed the following behavior:
Fraudulent use of services or benefits.
Threats of physical harm to a physician or his or her office staff.
Non-payment of required co-payment for services rendered.
Receipt of prescription medications or health services in a quantity or manner which is not medically beneficial or not medically necessary.
Refusal to accept a treatment or procedure recommended by the physician, if such refusal is incompatible with the continuation of the patient/physician relationship. The physician should also indicate if he or she believes that no professionally acceptable alternative treatment or procedure exists.
Repeated refusal to comply with office procedures essential to the functioning of the physician's practice or to accessing benefits under the managed care plan.
Other behavior which has resulted in serious disruption of the patient/physician relationship.
COMMENTS TO SUBSTANTIATE THE ABOVE BEHAVIOR: _____________________ ____________ _________________________________________________________________________________________ DATE(S) MEMBER WAS COUNSELED/EDUCATED: ______________ ______________________________________________________________________________ SUPPORTING DOCUMENTATION MUST BE ATTACHED TO SUBSTANTIATE THAT THE MEMBER WAS COUNSELED/EDUCATED ON THE ISSUES DESCRIBED ABOVE. (i.e., medical records, chart notes, incident reports, that documents the member was called and reminded of the appointment; documentation of no shows; documentation of recommended treatment plan, counseled, etc.) The above member has been counseled and educated and there has not been any improvement or progress. It is necessary for this member to be removed from my panel and to seek medical services elsewhere. I will continue to provide treatment for 30-45 days to allow the Health Plan to assist the member in the selection of another PCP. SIGNATURE OF REQUESTING PCP: TYPE OR PRINT NAME: DATE:
21

COUNSELING/EDUCATION LETTER TO MEMBER DATE Name Address City, State Zip
RE: Patient Name ID#:
Dear As your primary care physician, my goal is to advocate and support activities which contribute to your health and wellness. This can be accomplished through a partnership with you in a patient/physician relationship that is based on mutual trust, cooperation and adherence to accepted office procedure. It has been brought to my attention that this relationship has been threatened by the following: This behavior is unacceptable and will not be tolerated. The accepted office policy(s)/procedure(s) are: Unless you are willing to correct this behavior, I will have no choice but to request that you be removed from my panel. A response is requested from you within 14 days of receipt of this letter. Sincerely, PCP
22

CONTRACT EXCLUSIONS IPA retains the right to deliver certain services through a vendor or contractor. Should IPA elect to deliver certain services for which you are currently contracted to provide through a vendor or contractor, you will be provided a minimum of thirty (30) day’s advance notice and your contract terms will be honored during that notice period. After such time and notification, IPA retains the right to discontinue reimbursement for services provided by the vendor or contractor.
23

EXCHANGE OF ELECTRONIC DATA Information Protection Requirements and Guidance
IPA follows all applicable laws, rules, and regulations regarding the electronic transmittal and reception of Patient and Provider information. As such, if an electronic connection is made to facilitate such data transfer, all applicable laws must be followed. At all times, a provider must be able to track disclosures, provide details of data protections, and respond to requests made by IPA regarding information protection.
When an electronic connection is needed, relevant connection details will be provided to a patient by the IT Operations team who will engage with provider’s staff to appropriately implement the connection. Any files placed for receipt by provider staff must be downloaded in 24 hours, as all data is deleted on a fixed schedule. If the files
are unable to be downloaded, then alternate arrangements for retransmission must be made. The provider and provider’s staff will work collaboratively with IPA to ensure information is adequately protected and secure during transmission.
Experience the Ease of HSConnect
• View patient eligibility
• Create referrals and precertification
• Search authorizations
• Search claims
Need More Help? Contact the HSConnect Help Line: 1-866-952-7596 or e-mail [email protected] To register for HSConnect, visit: www.hsconnectonline.com
24

Register for HSConnect Access
25


Review Recent and Draft Authorizations
27

Locate a Member
28

Summary of Member’s Benefits
29

Create and Submit a Referral part 1
30

Create and Submit a Referral part 2
31

Create and Submit a Referral part 3
32

Create and Submit a Precertification
33

Create and Submit a Precertification part 2
34

Create and Submit a Precertification part 3
35

Search for Claims and View Claim Detail
36

CREDENTIALING AND RECREDENTIALING PROGRAM All practitioner and organizational applicants to IPA must meet basic eligibility requirements and complete the credentialing process prior to becoming a participating provider. Once an application has been submitted, the provider is subject to a rigorous verification process that includes primary and secondary source verifications of all applicable information for the contracted specialty(s). Upon completion of the verification process, providers are subject to a peer review process whereby they are approved or denied participation with the plan. No provider can be assigned a health plan effective date or be included in a provider directory without undergoing the credentialing verification and peer review process. All providers who have been initially approved for participation are required to recredential at least once every three years in order to maintain their participating status.
Practitioner Selection Criteria
IPA utilizes specific selection criteria to ensure that practitioners who apply to participate meet basic credentialing and contracting standards. At minimum these include, but are not limited to:
• Holds appropriate, current and unencumbered licensure in the state of practice as required by state and federal entities.
• Holds a current, valid, and unrestricted federal DEA and state controlled substance certificate as applicable.
• Is board-certified or has completed appropriate and verifiable training in the requested practice specialty.
• Maintains current malpractice coverage with limits commensurate with the community standard in which practitioner practices.
• Participates in Medicare and has a Medicare number and/or a National Provider Identification number.
• Has not been excluded, suspended, and/or disqualified from participating in any Medicare, Medicaid, or any other government health related program.
• Is not currently opted out of Medicare.
• Has admitting privileges at a participating facility as applicable.
Application Process
• Submit a completed state mandated credentialing application, CAQH Universal Credentialing Application form or CAQH ID, with a current signed and dated Attestation, Consent, and Release form that is less than 90 days old.
• If any of the Professional Disclosure questions are answered yes on the application, supply sufficient additional information and explanations.
• Provide appropriate clinical detail for all malpractice cases that are pending, or resulted in a settlement or other financial payment.
Submit copies of the following:
• All current and active state medical licenses, DEA certificate(s), and state controlled substance certificate as applicable.
• Evidence of current malpractice insurance that includes the effective and expiration dates of the policy and term limits.
• Five years of work history documented in a month/year format either on the application or on a current curriculum vitae. Explanations are required for any gaps exceeding six (6) months.
• If a physician, current and complete hospital affiliation information on the application. If no hospital privileges and the specialty require hospital privileges, a letter detailing the alternate coverage arrangement(s) or the name of the alternate admitting physician should be provided.
Credentialing and Recredentialing Process
Once a practitioner has submitted an application for initial consideration, IPA’s Credentialing Department will conduct primary source verification of the applicant’s licensure, education and/or board certification, privileges, lack of sanctions or other disciplinary action, and malpractice history by querying the National Practitioner Data Bank. The credentialing process generally takes up to ninety (90) days to complete, but can in some instances take longer. Once credentialing has been completed and the applicant has been approved, the practitioner will be notified in writing of their participation effective date.
To maintain participating status, all practitioners are required to recredential at least every three (3) years. Information obtained during the initial credentialing process will be updated and re-verified as required. Practitioners will be notified of the need to submit recredentialing information at least 4 months in advance of their three-year anniversary date. Three (3) separate attempts will be made to obtain the required information via mail, fax, email, or telephonic request. Practitioners who fail to return recredentialing information prior to their recredentialing due date will be notified in writing of their termination from the network.
Office Site Evaluations (if applicable)
Office site surveys and medical record keeping practice reviews may be required when it is deemed necessary as a result of a patient complaint, quality of care issue, and/or as otherwise mandated by state regulations.
37

Practitioner offices will be evaluated in the following categories:
• Physical appearance and accessibility
• Patient safety and risk management
• Medical record management and security of information
• Appointment availability
Providers who fail to pass the area of the site visit specific to the complaint or who score less than 90% on the site evaluation overall will be required to submit a corrective action plan and make corrections to meet the minimum compliance score. A follow up site evaluation will be done within sixty (60) days of the initial site visit if necessary to ensure that the correction action has been implemented.
Practitioner Rights
• Review information obtained from any outside source to evaluate their credentialing application with the exception of references, recommendations or other peer-review protected information. The provider may submit a written request to review his/her file information at least thirty days in advance at which time the Plan will establish a time for the provider to view the information at the Plan’s offices.
• Right to correct erroneous information when information obtained during the credentialing process varies substantially from that submitted by the practitioner. In instances where there is a substantial discrepancy in the information, Credentialing will notify the provider in writing of the discrepancy within thirty (30) days of receipt of the information. The provider must submit a written response and any supporting documentation to the Credentialing Department to either correct or dispute the alleged variation in their application information within thirty (30) days of notification.
• Right to be informed of the status of their application upon request. A provider may request the status of the application either telephonically or in writing. The Plan will respond within two business days and may provide information on any of the following: application receipt date, any outstanding information or verifications needed to complete the credentialing process, anticipated committee review date, and approval status.
Organizational Provider Selection Criteria
When assessing organizational providers, IPA utilizes the following criteria:
• Must be in good standing with all state and federal regulatory bodies.
• Has been reviewed and approved by an accrediting body.
• If not accredited, can provide appropriate evidence of successfully passing a recent state or Medicare site review, or meets other plan criteria.
• Maintains current professional and general liability insurance as applicable.
• Has not been excluded, suspended, and/ or disqualified from participating in any Medicare, Medicaid, or any other government health related program.
Organizational Provider Application and Requirements
1. A completed Ancillary/Facility Credentialing Application with a signed and dated attestation.
2. If responded “Yes” to any disclosure question in the application, an appropriate explanation with sufficient details/information is required.
3. Copies of all applicable state and federal licenses (i.e. facility license, DEA, Pharmacy license, etc.).
4. Proof of current professional and general liability insurance as applicable.
5. Proof of Medicare participation.
6. If accredited, proof of current accreditation.
7. Note: Current accreditation status is required for DME, Prosthetic/Orthotics, and non-hospital based high tech radiology providers who perform MRIs, CTs and/or Nuclear/PET studies.
8. If not accredited, a copy of any state or CMS site surveys that occurred within the last three years including evidence that the organization successfully remediated any deficiencies identified during the survey.
Credentialing Committee and Peer Review Process
All initial applicants and recredentialed providers are subject to a peer review process prior to approval or re-approval as a participating provider. The Medical Director may approve providers, who meet all of the acceptance criteria. Providers who do not meet established thresholds are presented to the Credentialing Committee for consideration. The Credentialing Committee is comprised of contracted primary care and specialty providers, and has the authority to approve or deny an appointment status to a provider. All information considered in the credentialing and recredentialing process must be obtained and verified within one hundred eighty (180) days prior to presentation to the Medical Director or the Credentialing Committee. All providers must be credentialed and approved before being assigned a participating effective date.
Non-discrimination in the Decision-making Process
IPA’s credentialing program is compliant with all guidelines from the National Committee for Quality Assurance (NCQA), Centers for Medicare & Medicaid Services (CMS), and state regulations as applicable. Through the universal application of specific assessment
38
criteria, ensures fair and impartial decision-making in the credentialing process, and does not make credentialing decisions based on an applicant’s race, gender, age, ethnic origin, sexual orientation, or due to the type of patients or procedures in which the provider specializes.
Provider Notification
All initial applicants who successfully complete the credentialing process are notified in writing of their plan effective date. Providers are advised to not see IPA’s patients until they receive notification of their plan participation and effective date. Applicants who are denied by the Credentialing Committee will be notified via a certified letter within sixty (60) days of the decision outcome detailing the reasons for the denial/term and any appeal rights to which the provider may be entitled.
Appeals Process and Notification of
Authorities
In the event that a provider’s participation is limited, suspended, or terminated, the provider is notified in writing within sixty (60) days of the decision. Notification will include a) the reasons for the action, b) outline of the appeals process or options available to the provider, and c) the time limits for submitting an appeal. A panel of peers will review all appeals. When termination or suspension is the result of quality deficiencies, the appropriate state and
federal authorities, including the National Practitioner Data Bank (NPDB) are notified of the action.
Confidentiality of Credentialing Information
All information obtained during the credentialing and recredentialing process is considered confidential and is handled and stored in a confidential and secure manner as required by law and regulatory agencies. Confidential practitioner credentialing and recredentialing information will not be disclosed to any person or entity except with the written permission of the practitioner or as otherwise permitted or required by law.
Ongoing Monitoring
IPA conducts routine, ongoing monitoring of license sanctions, Medicare/Medicaid sanctions, and the CMS Opt Out list between credentialing cycles. Participating providers who are identified as having been sanctioned, are the subject of a complaint review, or are under investigation for or have been convicted of fraud, waste, or abuse are subject to review by the Medical Director or the Credentialing Committee who may elect to limit, restrict or terminate participation. Any provider who’s license has been revoked or has been excluded, suspended, and/or disqualified from participating in any Medicare, Medicaid, or any other government health related program or who has opted out of Medicare will be (automatically terminated from the plan.
39

Initial Contracting/Credentialing Information Checklist
Initial Contracting/Credentialing Information Checklist
PHYSICIAN NAME:
PLEASE MAKE SURE TO INCLUDE THE FOLLOWING ITEMS:
� CAQH Provider ID #: ___________________________ o Please re-attest to information in CAQH and verify application & documentation are current (not expired) o Please grant access to Renaissance to view your application
� Signed attestation pages (pages 11 & 12) – signature & dates must be within 90 days of receipt. The top of Page 11 must indicate Renaissance Physicians. OR
� Completed 2007 Texas Standardized Credentialing Application (older versions will not be accepted) o Forms also available for download at http://www.tdi.state.tx.us/hmo/crform.html o Pages 11 & 12 – signature & dates must be within 90 days of receipt. The top of Page 11 must indicate
Renaissance. AND
� Copy of current DEA & DPS Certificates � Copy of Board State Medical Permit/License � Copy of current Malpractice Insurance (with limits & expiration date) � Copy of Board Certificate (if applicable) � Complete history of all malpractice claims & complete work history in month/year format (with no unexplained
gaps) � Completed W-9 Form � Signed Contracts (2) � Election to Participate (if applicable) � Facility Audit Scheduled/Completed (RP PCP, RP OB/GYN) *if applicable
Additional Required Information
Specialty: ______________________________________ Individual NPI#: _________________________
Address: _______________________________________ Group NPI#:____________________________
_______________________________________ Medicare #: ____________________________
_______________________________________
Phone #: _______________________________________ Medicaid #: _____________________________
Fax #: _________________________________________
Hospital Affiliations: ________________________________________________________________________________
2800 North Loop West, Ste. 600
Houston, Texas 77092
Telephone: (832) 553-3300
Fax: (832) 553-3418
40

REIMBURSEMENT Capitation reimbursement will vary according to an actuarial calculation of service requirements based on the age and gender of the patient.
• Payments to Primary Care Physicians (PCP’s) will be made on or before the 22nd day of each month for all patients under a PCP’s care on the first (1st) day of such month.
• Capitated specialists will receive capitation for all patients enrolled in the respective POD(s).
If a patient is added to a PCP’s roster on or before the fifteenth (15th) day of a month, a full month’s payment will be made retroactively during the month subsequent. There will be no retroactive payment for patients added after the fifteenth (15th) day of the month.
• Capitation will be paid each month to the physician whether or not the patient receives services that month.
• Capitation amounts are updated with practice and cost trends as experience dictates. See samples of capitation reports.
Primary Care Physician Capitation
The capitation payments the PCP receives will be accompanied by a computer report titled “Capitation Summary.” The capitation report is intended for use as a tool to assist in identifying those patients for whom the physician is responsible for providing services.
The report contains a summary of membership by health plan in alphabetical order with the following information:
• Patient name
• Phone number
• ID number
• Gender
• Date of birth
• Copay
• Patient group number
• Product description
• Effective date
• Termination date
• Member months
• Capitation rate
• Risk score
• Last PCP visit
Patients who terminate that month have a date in the termination column. Patients who change PCP’s, or whose coverage terminates will not appear on the following month’s
report. When such retroactivity occurs, the “Member months” column indicates the number of months adjusted for payment purposes.
Capitated services for Primary Care Physicians include:
Office visits for the diagnosis and treatment of an illness or injury.
• Periodic health assessments and routine physical examinations (performed at the discretion of the PCP as medically recommended for the age and gender of the patient, based on apparent medical condition and history of the patient. (This does not include school physicals, employment physicals, sports physicals, or other examinations requested by a third party, which are not medically required, as these are not covered under the health plan).
• Well-baby examinations.
• Vision and hearing screening.
• Voluntary family planning counseling and services if provided by the PCP (except artificial insemination)
• Miscellaneous services (i.e. removal of warts, lesions, etc.) considered by the PCP to be medically vital for removal.
Specialist Capitation
Specialist capitation includes a one-page summary illustrating the payment calculation and a single, consolidated POD(S) membership list in alphabetical order by health plan.
See samples of this report at the end of the section.
For questions about the capitation checks or report, call Provider Relations at 1-832-553-3300.
Copays
It is the responsibility of the physician’s office to collect the basic office visit copay at the time of the patient’s visit. If the copay is NOT collected from the patient, the IPA will NOT reimburse the physician’s office for that payment amount. The IPA would like to be notified of those patients who routinely do not pay their copay. Failure to make the required copay is grounds for possible termination of the patient from the health plan. The copay is a legal debt, owed by the patient to the physician, and can be collected as such.
How is the amount of copay determined?
The amount of the copay is determined by the benefit plan the employer selects.
Maximum Copays
The patient’s maximum copay per contract year for any individual and family varies depending on the health plan coverage chosen. Therefore, in some cases, a patient’s copay may change during the year.
41

Primary Care Physician Capitation Detail
Renaissance Physician
Sorted by Line of Business, Health Plan, and Member Name
PCP Cap Detail ReportJanuary 2016
Pod Name
PCP: www.xxxxxx
Member Name Member ID Sex DOB Copay Product Description EffectiveDate TermDate MemberGroup # DiseaseState Disease
Mgmt
Prg
RiskScore
Health Plan: Blue Cross MA, Cigna HealthSpring
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F XX/21/42 $0.00 Cigna-HealthSpring
Preferred (HMO)
01/01/16 TX025*MA Disabled 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx M 5/11/XX $0.00 Cigna-HealthSpring
Advantage (HMO)
01/01/16 TX009*M Medi/Medi 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F 2/XX/30 $0.00 Blue Cross
Medicare
Advantage Basic
(HMO)
01/01/16 TX010*QME Medi/Medi 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F XX/7/44 $0.00 Total Care 01/01/16 TX001*MA Other 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx M 2/XX/43 $0.00 Healthy Advantage
Preferred
01/01/16 TX010*ME Disabled 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F XX/9/50 $0.00 Blue Cross
Medicare
Advantage Basic
(HMO)
01/01/16 BC001 Other 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F 7/15/XX $0.00 Blue Cross
Medicare
Advantage Basic
(HMO)
01/01/16 BC001 Disabled 0.00
YYYYYYYY, ZZZZZZZZ - (555) 555-5555 xxxxxxxx-xx F 10/XX/27 $0.00 Blue Cross
Medicare
Advantage Basic
(HMO)
01/01/16 BC001 Other 0.00
42

43

CLAIMS Claims Submission
While IPA prefers electronic submission of claims, both electronic and paper claims are accepted. If interested in submitting claims electronically, contact Provider Relations for assistance.
All completed claims forms should be forwarded to the address noted below:
Renaissance Physicians Attn: Claims PO Box 2888 Houston, TX 77252-2888
RP Professional Claims Electronic Payment ID Numbers:
Availity - RENGQ (all caps) - as payor ID for HCFA only
Emdeon - 76066 - payor ID for HCFA and UB-04
Timely Filing
As a participating provider, you have agreed to submit all claims within 90 days of the date of service. Claims submitted with dates of service beyond 90 days are not reimbursable.
Claim Format Standards
Standard CMS required data elements must be present for a claim to be considered a clean claim and can be found in the CMS Claims Processing Manuals. The link to the CMS Claims Processing Manuals is: https://www.cms.gov/manuals/downloads/clm104c12.pdf
The IPA can only pay claims, which are submitted accurately. The provider is at all times responsible for an accurate claims submission. While IPA will make its best effort to inform the provider of claims errors, the claim accuracy rests solely with the provider.
Physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician. If more than one service is provided on the same day to the same patient by the same physician or more than one physician in the same specialty in the same group, they must bill and be paid as though they were a single physician. For example, only one evaluation and management service may be reported unless the evaluation and management services are for unrelated problems. Instead of billing separately, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level.
Physicians in the same group practice, but who are in different specialties may bill and be paid without regard to their patient in the same group.
Claim Payment
The IPA pays clean claims according to contractual requirements and the Centers for Medicare & Medicaid Services (CMS) guidelines. A clean claim is defined as a claim for a Covered Service that has no defect or impropriety. A defect or impropriety includes, without limitation, lack of data fields required by IPA or substantiating documentation, or a particular circumstance requiring special handling or treatment, which prevents timely payment from being made on the claim. The term shall be consistent with the Clean Claim definition set forth in applicable federal or state law, including lack of required substantiating documentation for non-participating providers and suppliers, or particular circumstances requiring special treatment that prevents timely payment from being made on the claim. If additional substantiating documentation involves a source outside of IPA, the claim is not considered clean.
Offsetting
As a contracted provider, you will be informed of any overpayments or other payments you may owe us within 365 days of the date on the Explanation of Benefits or within the timeframe as noted in your Agreement. You will have sixty (60) days from receipt of notification seeking recovery to refund us. We will provide you with the patient’s name, patient’s identification number, and claim number, your patient account number, date of service, a brief explanation of the recovery request, and the amount or the requested recovery. If you have not refunded us within the sixty (60) days recovery notice period, we will offset the recovery amounts identified in the initial notification, or in accordance with the terms of your Agreement.
Pricing
Original Medicare typically has market-adjusted prices by code (i.e. CPT or HCPCS) for services that Original Medicare covers. However, there are occasions where IPA offers a covered benefit for which Medicare has no pricing. In order to expedite claims processing and payment in these situations, the IPA will work to arrive at a fair market price by researching other external, publicly available pricing sources, such as other carriers, fiscal intermediaries, or state published schedules for Medicaid. The IPA requests that you make every effort to submit claims with standard coding. As described in this Manual and/or your Agreement, you retain your rights to submit a Request for Reconsideration if you feel the reimbursement was incorrect.
Claims Encounter Data
Providers who are being paid under capitation must submit claims in order to capture encounter data as required per your IPA’s Provider Agreement.
Explanation of Payment (EOP)/Remittance Advice (RA)
44

The EOP/RA statement is sent to the provider after coverage and payment have been determined by IPA. The statement provides a detailed description of how the claim was processed.
Non Payment/Claim Denial
Any denials of coverage or non-payment for services by IPA will be addressed on the Explanation of Payment (EOP) or Remittance Advice (RA). An adjustment/denial code will be listed per each billed line if applicable. An explanation of all applicable adjustment codes per claim will be listed below that claim on the EOP/RA. Per your contract, the patient may or may not be billed for services denied by IPA.
The patient may not be billed for a covered service when the provider has not followed the IPA’s procedures. In some instances, providing the needed information may reverse the denial (i.e. referral form with a copy of the EOP/RA, authorization number, etc.). When no benefits are available for the patient, or the services are not covered, the EOP/RA will alert you to this and you may bill the patient.
Processing of Hospice Claims
When a Medicare Advantage (MA) patient elects hospice care, but chooses not to dis-enroll from the plan, the patient is entitled to continue to receive any MA benefits which are not responsibility of the hospice through the IPA. Under such circumstances the premium the IPA receives from the Centers for Medicare and Medicaid Services (CMS) is adjusted to hospice status. As of the day the patient is certified as hospice, the financial responsibility for that patient shifts from IPA to Original Medicare. During a hospice election, Original Medicare covers all Medicare–covered services rendered with cost-sharing of Original Medicare. IPA will remain financially responsible for any benefits above Original Medicare benefits that are non-hospice related. Non-Medicare covered services, such as vision eyewear allowable, prescription drug claims, and medical visit transportation will remain the responsibility of IPA. Plan cost-sharing will apply to IPA covered services. If the patient chooses original Medicare for coverage of covered, non-hospice-care, original Medicare services and also follows MA plan requirements, then, the patient pays plan cost-sharing and original Medicare pays the provider. IPA will pay the provider the difference between original Medicare cost-sharing and plan cost-sharing, if applicable. Plan rules must still be followed and apply for both professional and facility charges. An HMO patient who chooses to receive services out of network has not followed plan rules and therefore is responsible to pay FFS cost-sharing; A PPO patient who receives services out of network has followed plan rules and is only responsible for plan cost-sharing. The patient need not communicate to the plan in advance his/her choice of where services are obtained.
When a patient revokes hospice care, financial responsibility for Medicare-covered services will return to the plan on the first of the month following the revocation. The following are the submission guidelines for Medicare Advantage patients enrolled in Hospice: Hospice-Related Services
• Submit the claim directly to CMS.
Medicare hospices bill the Medicare fee-for-service contractor for patients who have coverage through Medicare Advantage just as they do for patients, or beneficiaries, with fee-for-service coverage. Billing begins with a notice of election for an initial hospice benefit period, and followed by claims with types of bill 81X or 82X. If the patient later revokes election of the hospice benefit, a final claim indicating revocation, through use of occurrence code 42 should be submitted as soon as possible so the patient’s medical care and payment is not disrupted. Medicare physicians may also bill the Medicare fee-for-service contractor for patients who have coverage through Medicare Advantage as long as all current requirements for billing for hospice beneficiaries are met. These claims should be submitted with a GV or GW modifier as applicable. Medicare contractors process these claims in accordance with regular claims processing rules. When these modifiers are used, contractors are instructed to use an override code to assure such claims have been reviewed and should be approved for payment by the Common Working File in Medicare claims processing systems.
As specified above, by regulation, the duration of payment responsibility by fee-for-service contractors extends through the remainder of the month in which hospice is revoked. MA plan patients that have elected hospice may revoke hospice election at any time, but claims will continue to be paid by fee-for-service contractors as if the beneficiary were a fee-for-service beneficiary until the first day of the month following the month in which hospice was revoked.
Non-Hospice Services • For Part A services not related to the patient’s
terminal condition, submit the claim to the fiscal
intermediary using the condition code 07.
• For Part B services not related to the patient’s
terminal condition, submit the claim to the Medicare
carrier with a “GW” modifier.
• For services rendered for the treatment and
management of the terminal illness by a non-hospice
employed attending physician, submit the claim to the
fiscal Intermediary/ Medicare carrier with a “GV”
modifier.
45
Additional & Supplemental Benefits • Submit the claim to IPA.
For additional detail on hospice coverage and payment guidelines, please refer to 42 CFR 422.320-Special Rules for Hospice Care. Section (C) outlines the Medicare payment rules for patients who have elected hospice coverage. The Medicare Managed Care Manual, Chapter 11, Sections 40.2 and 50, and the CMS Program Memorandum AB-03-049 also outline payment responsibility and billing requirements for hospice services. This documentation is also available online at the CMS website: www.cms.gov.
ICD-10 Diagnosis and Procedure Code Reporting
In January 2009, the U.S. Department of Health and Human Services (HHS) published a final rule requiring the use of International Classification of Diseases version 10 (ICD-10) for diagnosis and hospital inpatient procedure coding. (The rule initially was set to go into effect on October 1, 2013, but was later postponed to an October 1, 2014 effective date.) The rule impacts the health care industry – including health plans, hospitals, doctors, and other health care professionals, as well as vendors and trading partners.
ICD-10 (International Classification of Diseases, 10th Edition, Clinical Modification /Procedure Coding System) consists of two parts:
• ICD-10-CM for Diagnosis coding is for use in all U.S. health care settings. Diagnosis coding under ICD-10-CM uses 3 to 7 characters
• ICD-10-PCS for Inpatient Procedure coding is for use in U.S. inpatient hospital settings only. ICD-10-PCS uses 7 alphanumeric characters. Coding under ICD-10-PCS is much more specific.
Note: Procedure codes are only applicable to inpatient claims and not prior authorizations.
ICD-10 will affect diagnosis and inpatient procedure coding for everyone covered by the Health Insurance Portability Accountability Act (HIPAA), not just those who submit Medicare or Medicaid claims. The change to ICD-10 does not affect CPT or HCPCS coding for outpatient procedures.
Billable vs. Non-billable Codes
• A billable ICD-10 code is defined as a code that has been coded to its highest level of specificity.
• A non-billable ICD-10 code is defined as a code that has not been coded to its highest level of specificity. If a claim is submitted with a non-billable code, the claim will be rejected.
• The following is an example of a billable ICD-10 code with corresponding non-billable codes:
Billable ICD-10 Codes Non-billable ICD-10 Codes
M1A.3110 - Chronic gout due to renal impairment, right shoulder, without tophus
M1A.3 - Chronic gout due to renal impairment
M1A.311 - Chronic gout due to renal impairment, right shoulder
• It is acceptable to submit a claim using an unspecified code when sufficient clinical information is not known or available about a particular health condition to assign a more specific code.
Billable Unspecified ICD-10 Codes
I50.9 - Heart Failure, unspecified
J18.9 - Pneumonia, unspecified organism
Questions Concerning ICD-10
If you have a question as it pertains to ICD-10, please consult with your Network Operations Representative.
Dual Eligible Patients
Many of your patients may have an IPA as their primary insurance payer and Medicaid as their secondary payer. This will require you to coordinate the benefits of these “dual eligible” patients by determining whether the patient should be billed for the deductibles and copayments, or coinsurances associated with their benefit plan. Providers may not assess a QMB (Qualified Medicare Beneficiary) or QMB-Plus for copayments, coinsurances, and/or deductibles.
Providers will accept as payment in full IPA’s payment and will not seek additional payment from the state or dual eligible patients. Additional information concerning Medicaid provider participation is available at www.myrpo.com .
A patient’s level of Medicaid eligibility can change due to their medical and financial needs. The IPA encourages you to verify patients’ Medicaid eligibility when rendering services, which will help you determine if the patient owes a deductible or copay.
Medicaid eligibility can be obtained by using the Medicaid telephonic Eligibility Verification System. If you do not have access to the system, please contact your State Medicaid provider for additional information.
Please note: Each state varies in their decision to cover the cost-share for populations beyond QMB and QMB+.
46

Cost-sharing Chart
Patient’s Medicaid Plan
Patient’s liability Patient owes deductibles and copayments associated with benefit plan
Medicaid provides benefits Patient not liable for deductibles and copayments associated with benefit plan
Medicaid (FBDE) No Yes
QMB Only No Yes
QMB+ No Yes
SLMB Yes No
SLMB+ Yes No
QI-1 Yes No
QDWI Yes No
Coordination of Benefits and Subrogation Guidelines
General Definitions
Coordination of Benefits (COB): is the process of determining and reconciling individual payor liability for reimbursement when a patient is eligible for benefits coverage under more than one insurance company or other payor type (e.g., Medicare / Medicaid). Terms and conditions within the Summary of Benefits for each plan will generally dictate which payor is primary or secondary and any mathematical formula associated for calculating each payor's portion of coverage. Coordinating payment of these plans will provide benefit coverage up to but not exceeding one hundred (100) percent of the allowable amount. The respective primary and secondary
payment obligations of the two coverages are determined by the Order of Benefits Determination Rule contained in the National Association of Insurance Commissioners (NAIC) COB Model Regulations Guidelines.
Order of Benefit Determination Rule: Rules which, when applied to a particular patient covered by at least two plans, determine the order of responsibility each plan has with respect to the other plan in providing benefits for that patient. A plan will be determine to have Primary or Secondary responsibility for a person’s coverage with respect to other plans by applying the NAIC rules.
Primary: This carrier is responsible for costs of services provided up to the benefit limit for the coverage or as if no other, coverage exists.
Secondary: This carrier is responsible for the total allowable charges, up to the benefit limit for the coverage less the primary payment not to exceed the total amount billed (maintenance of benefits).
Allowable Expense: Any expense customary or necessary, for health care services provided as well as covered by the patient’s health care plan.
Conclusion: COB is applying the NAIC rules to determine which plan is primarily responsible and plan would be in a secondary position when alternate coverage exists. If COB is to accomplish its purpose, all plans must adhere to the structure set forth in the Model COB regulations.
Basic NAIC Rules for COB
Birthday Rule: The primary coverage is determined by the birthday that falls earliest in the year, understanding both spouses are employed and have coverage. Only the day and month are taken into consideration. If both patients have the same date of birth, the plan which covered the patient the longest is considered primary.
General Rules: The following table contains general rules to follow to determine a primary carrier:
If the Patient/Beneficiary The Below Conditions Exists
Then the Below Program Pays First
The Below Program Pays Secondary
Is age 65 or older, and is covered by a Group Health Plan (GHP) through current employment or a family patient’s current employment
The employer has more than 20 employees, or at least one employer is a multi-employer group that employs 20 or more employees
The Group Health Plan (GHP) pays primary
IPA/Medicare pays secondary
47

If the Patient/Beneficiary The Below Conditions Exists
Then the Below Program Pays First
The Below Program Pays Secondary
Is age 65 or older and is covered a Group Health Plan (GHP) through current employment or a family patients current employment
The employer has less than 20 employees
IPA /Medicare pays primary
Group Health Plan (GHP) pays secondary
Is entitled based on disability and is covered by a Large Group Health Plan (LGHP) through his/her current employment or through a family patients current employment
The employer has 100 or more employees or at least one employer is a multi-employer group that employs 100 or more employees
The Large Group Health Plan (LGHP) pays primary
IPA /Medicare pays secondary
Is entitled based on disability and is covered by a Large Group Health Plan (LGHP) through his/her current employment or through a family patients current employment
The employer employs less than 100 employees
IPA /Medicare pays primary
Large Group Health Plan (LGHP) pays secondary
Is age 65 or older or entitled based on disability and has retirement insurance only
Does not matter the number of employees
IPA /Medicare pays primary
Retirement Insurance pays secondary
Is age 65 or older or is entitled based on disability and has COBRA coverage
Does not matter the number of employees
IPA/Medicare pays primary
COBRA pays secondary
Becomes dually entitled based on age/ESRD
Had insurance prior to becoming dually entitled with ESRD as in block one above
The Group Health Plan (GHP) pays primary for the first 30 months
IPA/Medicare pays secondary (after 30 months IPA pays primary)
Becomes dually entitled based on age/ESRD but then retires and keeps retirement insurance
Had insurance prior to becoming dually entitled with ESRD as in block one above and then retired
The Retirement Insurance pays primary for the first 30 months
IPA/Medicare pays secondary (after 30 months IPA pays primary)
Becomes dually entitled based on age/ESRD but then obtains COBRA insurance through employer
Had insurance prior to becoming dually entitled with ESRD as in block one above and picks up COBRA coverage
COBRA insurance would pay primary for the first 30 months (or until the patient drops the COBRA coverage
IPA/Medicare pays secondary (after 30 months IPA pays primary)
Becomes dually entitled based on disability/ESRD
Had insurance prior to becoming dually entitled with ESRD as in block three above
The Large Group Health Plan (LGHP) pays primary
IPA/Medicare pays secondary (after 30 months IPA pays primary)
48

If the Patient/Beneficiary The Below Conditions Exists
Then the Below Program Pays First
The Below Program Pays Secondary
Becomes dually entitled based on disability/ESRD but then obtains COBRA insurance through employer
Had insurance prior to becoming dually entitled with ESRD as in block three above and picks up the COBRA coverage
COBRA insurance would pay primary for the first 30 months or until the patient drops the COBRA coverage
IPA/Medicare pays secondary (after 30 months IPA pays primary)
Basic Processing Guidelines for COB
For the IPA to be responsible as either the primary or the secondary carrier, the patient must follow all HMO rules (i.e. pay copays and follow appropriate referral process).
When the IPA is the secondary insurance carrier:
• All IPA’s guidelines must be met in order to reimburse the provider (i.e. pre-certification, referral forms, etc.).
• The provider collects only the copayments required.
• Be sure to have the patient sign the “assignment of benefits” sections of the claim form.
• Once payment and/or EOB are received from the other carriers, submit another copy of the claim with the EOB of IPA for reimbursement. Be sure to note all authorization numbers on the claims and attach a copy of the referral form if applicable.
When IPA is the primary insurance carrier:
• The provider collects the copayment required under the patient’s plan.
• Submit the claim to the IPA first
• Be sure to have the patient sign the “assignment of benefits” sections of the claim form.
• Once payment and/or remittance advise (RA) has been received from IPA, submit a copy of the claim with the RA to the secondary carrier for adjudication.
• Please note that the IPA is a total replacement for Medicare.
• Medicare cannot be secondary when patients have an IPA.
• Medicaid will not pay the copay for the Participating Plan’s patients.
Worker's Compensation
The IPA does not cover worker’s compensation claims.
When a provider identifies medical treatment as related to an on-the-job illness or injury, the IPA must be notified. The provider will bill the worker’s compensation carrier for all services rendered, not the IPA.
Subrogation
Subrogation is the coordination of benefits between a health insurer and a third party insurer (i.e. property and casualty insurer, automobile insurer, or worker’s compensation carrier), not two health insurers.
Claims involving Subrogation or Third Party Recovery (TPR) will be processed internally by the IPA’s Claims Department. COB protocol, as mentioned above, would still apply in the filing of the claim.
Patients who may be covered by third party liability insurance should only be charged the required copayment. The bill can be submitted to the liability insurer. The provider should submit the claim to the IPA with any information regarding the third party carrier (i.e. auto insurance name, lawyers name, etc.). All claims will be processed per the usual claims procedures.
The IPA uses an outside vendor for review and investigation of all possible subrogation cases. This vendor coordinates all requests for information from the patient, provider and attorney’s office and assists with settlements. For claims related questions, please contact Provider Customer Service at 1-832-553-3300. A Provider Representative will gladly provide assistance.
Appeals
An appeal is a request for the IPA to review a previously made decision related to medical necessity, clinical guidelines, or prior authorization and referral requirements. You must receive a notice of denial, or remittance advice before you can submit an appeal. Please do not submit your initial claim in the form of an appeal. Appeals can take up to 90 days for review and determination. Timely filing requirements are not affected or changed by the appeal process or by the appeal outcome. If an appeal decision results in approval of payment contingent upon the filing of a corrected claim, the time frame is not automatically extended and will remain consistent with the timely filing provision in the IPA agreement.
You may appeal a previous decision not to pay for a service. For example, claims denied for no authorization or no referral, including a decision to pay for a different level of care; this includes both complete and partial denials. Examples of partial denials include denials of certain levels of care, isolated claim line items, or a decreased quantity of office or therapy visits. Total and partial denials of payment may be appealed
49

using the same appeal process. Your appeal will receive an independent review by the IPA’s representative not involved with the initial decision. Requesting an appeal does not guarantee that your request will be approved or that the initial decision will be overturned. The appeal determination may fully or partially uphold the original decision.
Appeals can take up to 60 days for review and determination. Timely filing requirements are not affected or changed by the appeal process or by the appeal outcome. If an appeal decision results in approval of payment contingent upon the filing of a corrected claim, the time frame is not automatically extended and will remain consistent with the timely filing provision in the IPA’s agreement. An appeal is a request for IPA to review a previously made decision related to medical necessity or clinical guidelines. You must receive a notice of denial, of medical non-coverage, or remittance advice before you can submit an appeal. Please do not submit your initial claim in the form of an appeal.
You should submit your appeal using the “Request for Appeal or Reconsideration” form and medical records. There are several ways to submit your appeal to the IPA. You may fax the appeal request to our secure fax line at 1-832-553-3418. Alternatively, for large medical record files, you may mail the appeal request form attached.
Part C Appeals Address and Fax Number:
Renaissance Physicians Attn: Appeals Unit PO Box 2888 Houston, TX 77252-2888
Phone: 1-832-553-3300
Fax: 1-832-553-3418
Reconsiderations
You have up to 180 days to request reconsideration of a claim. You may request claim reconsideration if you feel your claim was not processed appropriately according to the IPA’s claim payment policy or in accordance with your provider agreement. A claim reconsideration request is appropriate for disputing denials such as coordination of benefits, timely filing, or missing information. Payment retractions, underpayments/overpayments, as well as coding disputes should also be addressed through the claim reconsideration process. The IPA will review your request, as well as your provider record, to determine whether your claim was paid correctly. You may request reconsideration by submitting the completed request form to:
Renaissance Physicians Attn: Reconsiderations PO Box 2888 Houston, TX 77252-2888
Fax: 1-832-553-3418
50

APPEALS AND RECONSIDERATION REQUEST FORM Complete the top section of this form completely and legibly. Check the box that most closely describes your appeal or reconsideration reason. Be sure to include any supporting documentation, as indicated below. Requests received without required information cannot be processed. Request for appeal or reconsideration Customer first name: MI: Customer last name: Customer ID #: Customer date of birth (MM/DD/YYYY): Claim #: Date of service (MM/DD/YYYY): Provider name/contact name: Provider NPI: Provider phone #: Provider’s contact email address: Appeals Reason for appeal: __Medical necessity __Notification/precertification • Include precertification/prior authorization number __Referral denial __Payer policy
Reconsiderations Reason for reconsideration: __Payment issue __Duplicate claim __Retraction of payment __Request for medical records • Include copy of letter/request received __Request for additional information • Include copy of letter/request received • Provide missing or incomplete information • Coding dispute • Timely filing • Remittance Advice (RA), Explanation of Benefits (EOB), or other documentation of filing original claim __Coordination of Benefits Note: If you have multiple reconsideration requests for the same health care professional and payment issue, please indicate this in the notes below and include a list of the following: Customer ID #, Claim #, and date of service. If the issue requires supporting documentation as noted above, it must be included for each individual claim. If no additional documentations required for your appeal or reconsideration request, fax in only this completed coversheet. You may use the space below to briefly describe your reason for appeal or reconsideration. Definitions Payment issue: Was not paid in accordance with the negotiated terms Coordination of benefits: Could not fully be processed until information from another insurer has been received Duplicate claim: The original reason for denial was due to a duplicate claim Medical necessity: Medical clinical review Pre-certification/notification of prior-authorization or reduced payment: Failure to notify or pre-authorize services or exceeding authorized limits Payer policy clinical: Incorrectly reimbursed because of the payers payment policy Referral denial: Invalid or missing primary care physician (PCP) referral Request for additional information: Missing or incomplete information *reply via sender* Request for medical records: Please include copy of letter/request received Retraction of payment: Retraction of full or partial payment Timely filing: The claim whose original reason for denial was untimely filing
Submit Appeals to: Renaissance Physicians Attn: Appeals Unit PO Box 2888 Houston, TX 77252-2888 Phone: 1-832-553-3300 Fax: 1-832-553-3418
Submit reconsiderations to: Renaissance Physicians Attn: Reconsiderations PO Box 2888 Houston, TX 77252-2888 Fax: 1-832-553-3418
51

HEALTH SERVICES The Health Services Department coordinates health care services to ensure appropriate utilization of health care resources. This coordination assures promotion of the delivery of services in a quality-oriented, timely, clinically appropriate, and cost-effective manner for the patients.
The Utilization Management staff base their utilization-related decisions on the clinical needs of patients, the patient’s Benefit Plan, Interqual Criteria, Milliman Guidelines, the appropriateness of care, Medicare National Coverage Guidelines, health care objectives, and scientifically based clinical criteria and treatment guidelines in the context of provider and/or patient-supplied clinical information and other such relevant information.
The IPA in no way rewards or incentivizes, either financially or otherwise, practitioners, utilization reviewers, clinical care managers, physician advisers or other individuals involved in conducting utilization review, for issuing denials of coverage or service, or inappropriately restricting care.
Goals
• To ensure that services are authorized at the appropriate level of care and are covered under the patient’s health plan benefits.
• To monitor utilization practice patterns of IPA’s contracted physicians, hospitals, ancillary services, and specialty providers.
• To provide a system to identify high-risk patients and ensuring that appropriate care is accessed.
• To provide utilization management data for use in the process of re-credentialing providers.
• To educate patients, physicians, contracted hospitals, ancillary services, and specialty providers about IPA’s goals for providing quality, value-enhanced managed health care.
• To improve utilization of IPA’s resources by identifying patterns of over- and under-utilization that have opportunities for improvement.
Departmental Functions
• Prior authorization
• Concurrent review
• Discharge planning
• Case management and disease management
• Continuity of care
Prior Authorization
The Primary Care Physician (PCP) or Specialist is responsible for requesting prior authorization of all scheduled admissions or services/procedures, for referring a patient for an elective admission, outpatient service, specialist referral and for requesting services in the home. The IPA recommends requesting prior authorization at least seven (7) days in advance of the admission, procedure, or service. Requests for prior authorization are expeditiously as the patient’s health condition requires. For prior authorizations, providers should call 1-800‑‑‑‑511-6932. You may also submit most requests via our online portal 24 hours per day, 7 days per week at: https:// www.hsconnectonline.com
Services requiring prior authorization are listed in the appendix or Health Plan section of this manual, as well as on IPA’s website. The presence or absence of a service or procedure on the list does not determine coverage or benefits. Log in to HSConnect or contact customer service to verify benefits, coverage, and patient eligibility.
The Prior Authorization Department, under the direction of licensed nurses, clinical pharmacists, and medical directors, documents and evaluates requests for authorization, including:
• Verification that the patient is eligible for services with IPA at the initial start of care
• Verification that the requested service is a covered benefit under the patient’s benefit package.
• Determination of the appropriateness of the services (medical necessity).
• Verification that the service is being provided by the appropriate provider and in the appropriate setting.
The Prior Authorization Department documents and evaluates requests utilizing CMS guidelines and nationally recognized accepted criteria, processes the authorization determination, and notifies the provider of the determination.
Examples of information required for a determination include, but are not limited to:
• Patient name and identification number
• Location of service (e.g., hospital or surgi-center setting)
• Primary Care Physician name along with Tax Identification Number (TIN) or Provider Identification Number (PIN)
• Servicing/attending physician name
• Date of service
• Diagnosis
• Service/procedure/surgery description and CPT or HCPCS code
• Clinical information supporting the need for the service to be rendered
For patients who go to an emergency room for treatment,
52

an attempt should be made in advance to contact the PCP unless it is not medically feasible due to a serious condition that warrants immediate treatment.
If a patient appears at an emergency room for care, which is non-emergent, the PCP should be contacted for direction. The patient may be financially responsible for payment if the care rendered is non-emergent. The IPA also utilizes urgent care facilities to treat conditions that are non-emergent but require immediate treatment.
Emergency admissions must be pre-certified by IPA within twenty-four (24) hours, or the next business day, of admission. Please be prepared to discuss the patient’s condition and treatment plan with our nurse coordinator.
Prior Authorization is a determination of medical necessity and is not a guarantee of claims payment. Claim reimbursement may be impacted by various factors including eligibility, participating status, and benefits at the time the service is rendered.
Outpatient Prior Authorization Department
Intake Unit:
• Consists of non-clinical personnel
• Receives faxes, provider portal submission and phone calls for services that require prior authorization
• Handles issues that can be addressed from a non-clinical perspective:
� Did you receive my fax? � Does this procedure/service
require prior authorization?
� Setting up “shells” for services that must be forwarded to clinical personnel for determination
� Creates and validates cases for services that must be forwarded to clinical personnel for medical necessity determination
Prior Authorization Unit:
• Consists of RN’s and LPN’s
• Performs medical necessity review of clinical requests for services such as:
� Infusion � Outpatient Surgical Procedures � DME / O&P
� Ambulance transports
� Outpatient Diagnostic Testing � Outpatient Therapy
• Maintains clinical decision-making documentation
• Coordinates Medical Director Review of cases requiring secondary review
• Notifies customer and provider of Prior Authorization determination
ICD-10 Diagnosis and Procedure Code Reporting
In January 2009, the U.S. Department of Health and Human Services (HHS) published a final rule requiring the use of International Classification of Diseases version 10 (ICD-10) for diagnosis and hospital inpatient procedure coding. The rule impacts the health care industry – including health plans, hospitals, doctors and other health care professionals, as well as vendors and trading partners.
ICD-10 (International Classification of Diseases, 10th Edition, Clinical Modification /Procedure Coding System) consists of two parts:
ICD-10-CM for Diagnosis coding is for use in all U.S. health care settings. Diagnosis coding under ICD-10-CM uses 3 to 7 characters adding more specificity.
ICD-10-PCS for Inpatient Procedure coding is for use in U.S. inpatient hospital settings only. ICD-10-PCS uses 7 alphanumeric characters
Coding under ICD-10-PCS is much more specific
ICD-10 will affect diagnosis and inpatient procedure coding for everyone covered by the Health Insurance Portability Accountability Act (HIPAA), not just those who submit Medicare or Medicaid claims. The change to ICD-10 does not affect CPT or HCPCS coding for outpatient procedures.
ICD-10 Authorization Guidelines
Health care professionals must be prepared to comply with the transition to ICD-10 by the new compliance date. The IPA will strictly adhere to the following guidelines:
• Prior authorizations and referrals for date of service or admission on or after the new compliance date must be submitted with ICD-10 diagnosis codes.
• Prior authorizations and referrals will only accept code type ICD-10 based on date of service or admission.
53

Billable vs. Non-billable Codes
• A billable ICD-10 code is defined as a code that has been coded to its highest level of specificity.
• A non-billable ICD-10 code is defined as a code that has not been coded to its highest level of specificity. If a claim is submitted with a non-billable code, the claim will be rejected.
• The following is an example of a billable ICD-10 code with corresponding non-billable codes:
Billable ICD-10 Codes Non-billable ICD-10 Codes
M1A.3110 - Chronic gout due to renal impairment, right shoulder, without tophus
M1A.3 - Chronic gout due to renal impairment
M1A.311 - Chronic gout due to renal impairment, right shoulder
• It is acceptable to submit a claim using an unspecified code when sufficient clinical information is not known or available about a particular health condition to assign a more specific code.
Billable Unspecified ICD-10 Codes
I50.9 - Heart Failure, unspecified
J18.9 - Pneumonia, unspecified organism
Questions Concerning ICD-10
If you have a question as it pertains to ICD-10, please consult with your Provider Coding Educator.
Requests and Time Frames
Emergency - Authorization is not required
An Emergency Medical Condition is a medical condition manifesting itself by acute symptoms of sufficient severity (including severe pain) such that a prudent layperson, with an average knowledge of health and medicine, could reasonably expect the absence of immediate medical attention to result in:
• Serious jeopardy to the health of the individual
• Serious impairment to bodily functions;
• Or, serious dysfunction of any bodily organ or part.
Expedited:
An expedited request can be requested when you
as a physician believe that waiting for a decision under the routine time frame could place the patient’s life, health, or ability to regain maximum function in serious jeopardy. Expedited requests will be determined within 72 hours or as soon as the patient’s health requires.
An expedited request may not be requested for cases in which the only issue involves a claim for payment for services that the patient has already received.
Routine:
A routine or standard Prior Authorization request will be determined as expeditiously as the health condition requires, but no later than 14 calendar days after receipt of the request.
Approval: Once the Precertification Department receives the request for authorization, we will review the request using nationally recognized industry standards or local Coverage Determination criteria. If the request for authorization is approved, the IPA will assign an authorization number and enter the information in our medical management system. This authorization number can be used to reference the admission, service or procedure. Approval notification is provided to the patient and the provider.
Retrospective Review
Retrospective review is the process of determining coverage for clinical services by applying guidelines/criteria to support the claim adjudication process after the opportunity for precertification or concurrent review timeframe has passed. The only scenarios in which retrospective requests can be accepted are:
• Authorizations for claims billed to an incorrect carrier
� As long as you have not billed the claim to IPA and received a denial, you can request a retro authorization from Health Services within 2 business days of receiving the RA from the incorrect carrier.
� If the claim has already been submitted to IPA and you have received a denial, the request for retro authorization then becomes an appeal and you must follow the guidelines for submitting an appeal.
• Services/Admissions after hours, weekends, or holidays
� IPA will retrospectively review any medically necessary services provided to IPA’s patients after hours, holidays, or weekends. The IPA does require the retro authorization request and applicable clinical information to be submitted to the Health Services dept. within 2 business days of providing the service or admitting the patient.
� In accordance with IPA’s policy, retrospective requests for authorizations not meeting the scenarios listed above may not be accepted and these claims may be denied for payment.
� After confirming the patient’s eligibility and the availability of benefits at the time the service
54

was rendered, providers should submit all supporting clinical documentation with the request for review and subsequent reimbursement via fax to 1-832-553-3420. Please refer to the Prior Authorization Grid in the appendix section on your specific service for authorization guidelines and/or requirements.
� The requesting provider has the responsibility of notifying the patient that services are approved and documenting the communication in the medical record.
Discharge Planning and Acute Care Management
Discharge Planning is a critical component of the process that begins with an early assessment of the patient’s potential discharge care needs in order to facilitate transition from the acute setting to the next level of care. Such planning includes preparation of the patient and his/her family for any discharge needs along with initiation and coordination of arrangements for placement and/or services required after acute care discharge. The IPA will coordinate with the facility discharge planning team to assist in establishing a safe and effective discharge plan.
In designated contracted facilities, IPA also employs ACCMs to assist with the process, review the inpatient medical record, and complete face-to-face patient interviews to identify patients at risk for readmission, in need of post-discharge complex care coordination and to aid the transition of care process. This process is completed in collaboration with the facility discharge planning and acute care management team patients and other IPA staff. When permissible by facility agreement, the ACCM also completes the Concurrent Review process onsite at assigned hospitals. The role of the ACCM onsite reviewer then also includes the day-to-day functions of the Concurrent Review process at the assigned hospital by conducting timely and consistent reviews and discussing with an IPA medical director as appropriate. The reviewer monitors the utilization of inpatient patient confinement at the assigned hospitals by gathering clinical information in accordance with hospital rules and contracting requirements including timelines for decision-making. All clinical information is evaluated utilizing nationally accepted review criteria.
The ACCM onsite reviewer will identify discharge-planning needs and be proactively involved by interacting with attending physicians and hospital case managers in an effort to facilitate appropriate and timely discharge. The onsite reviewer will follow the policies and procedures consistent with the guidelines set forth by IPA Health Services Department and the facility.
Adverse Determinations
Rendering of Adverse Determinations (Denials)
The Utilization Management staff is authorized to render an administrative denial decision to participating providers based only on contractual terms, benefits, or eligibility.
Every effort is made to obtain all necessary information, including pertinent clinical information and original documentation from the treating provider to allow the Medical Director to make appropriate determinations.
Only an IPA Medical Director may render an adverse determination (denial) based on medical necessity but he/she may also make a decision based on administrative guidelines. The Medical Director, in making the initial decision, may suggest an alternative Covered Service to the requesting provider. If the Medical Director makes a determination to deny or limit an admission, procedure, service, or extension of stay, the IPA notifies the facility or provider’s office of the denial of service. Such notice is issued to the provider and the patient, when applicable, documenting the original request that was denied and the alternative approved service, along with the process for appeal.
The IPA’s employees are not compensated for denial of services. The PCP or attending physician may contact the Medical Director by telephone to discuss adverse determinations.
Notification of Adverse Determinations (Denials)
The reason for each denial, including the specific utilization review criteria with pertinent subset/information or benefits provision used in the determination of the denial, is included in the written notification and sent to the provider and/or patient as applicable. Written notifications are sent in accordance with CMS and NCQA requirements to the provider and/or patient as follows:
• For non-urgent pre-service decisions – within 14 calendar days of the request.
• For urgent pre-service decisions - within 72 hours or three calendar days of the request.
• For urgent concurrent decisions – within 24 hours of the request.
• For post-service decisions – within 30 calendar days of the request.
*Denotes initial oral notification of the denial decision is provided with electronic or written notification given no later than 3 calendar days after the oral notification
Peer-to-Peer information is provided.
The IPA complies with CMS requirements for written notifications to patients, including rights to appeal and grievances. For urgent care requests, the IPA notifies the provider(s) only of the decision since the treating or attending practitioner is acting as the patient’s representative. If the denial is either concurrent or post service (retrospective) and the patient is not at financial risk, the patient is not routinely notified.
55

An Advanced Beneficiary Notice (ABN) may not be used to hold patients liable for services unless a preservice organization determination has already been rendered.
Appeals
An appeal is a request for the IPA to review a previously made
decision related to medical necessity, clinical guidelines, or
prior authorization and referral requirements. You must receive
a notice of denial, or remittance advice before you can submit
an appeal.
You may appeal a health services or Utilization Management denial of a service not yet provided, on behalf of a patient. The patient must be aware that you are appealing on his or her behalf. Patient appeals are processed according to Medicare guidelines.
An appeal must be submitted within 60 days of the original decision unless otherwise stated in your provider agreement. With your appeal request, you must include a copy of your denial, any medical records that would support the medical necessity for the service, hospital stay, or office visit, and a copy of the insurance verification completed on the date of service.
Appeals can take up to 60 days for review and determination. Timely filing requirements are not affected or changed by the appeal process or by the appeal outcome. If an appeal decision results in approval of payment contingent upon the filing of a corrected claim, the time frame is not automatically extended and will remain consistent with the timely filing provision in the IPA’s agreement. An appeal is a request for IPA to review a previously made decision related to medical necessity or clinical guidelines. You must receive a notice of denial, of medical non-coverage, or remittance advice before you can submit an appeal. Please do not submit your initial claim in the form of an appeal.
56

REFERRAL PROCESS The Primary Care Physician (PCP) is the patient’s primary point of entry into the health care delivery system for all outpatient specialist care.
The PCP is required to obtain a referral for most outpatient specialist visits for IPA’s patients.
Referrals can be requested through several methods, such as:
• HSConnect
• Phone
Likewise, the specialist is required to ensure that a referral is in place prior to scheduling a visit (except urgent/emergent visits, which do not require referral). The specialist is also required to communicate to the PCP via consultation reports any significant findings, recommendations for treatment and the need for any ongoing care.
Electronic submission/retrieval of referrals through HSConnect helps to ensure accurate and timely processing of referrals.
All referrals must be obtained prior to services being rendered. No retro-authorizations of referrals will be accepted. Please note that we value the PCP’s role in taking care of our IPA’s patients and that the PCP has a very important role in directing the patient to the appropriate specialist based on your knowledge of the patient’s condition and health history. It is also absolutely essential that patients are directed to participating providers only. In order to ensure this, please refer to our online directory or contact Customer Service for assistance.
Remember: An authorization number does not guarantee payment – services must be a covered benefit. Please verify benefits before providing services.
Referral Guidelines
• PCPs should refer only to IPA’s participating specialists for outpatient visits.
• Non-participating specialist’s visits require prior authorization by IPA.
• Referrals must be obtained PRIOR to specialist services being rendered.
• PCPs should not issue retroactive referrals.
• Most referrals are valid for 180 days starting from the issue date.
• All requests for referrals must include the following information:
� Patient Name, Date of Birth, patient ID � PCP Name
� Specialist Name
� Date of Referral � Number of visits requested
If a patient is in an active course of treatment with a specialist at the time of enrollment, The IPA will evaluate requests for continuity of care. A PCP referral is not required, but an authorization must be obtained from IPA’s Prior Authorization Department. For further details, please refer to the Continuity of Care section in Health Services.
Please note: A specialist may not refer the patient directly to another specialist unless within scope of treatment. If a patient needs care from another specialist, he/she must obtain the referral from his/her PCP.
Self Referrals
Patients have open access to certain specialists, known as self-referred visits/services; these include but are not limited to:
• Emergency medicine (emergency care as defined in the provider contract)
• Obstetric and Gynecological care (routine care, family planning)
Please refer to IPA’s website to view the current provider directory for Participating Specialists. If a patient has a preference, the PCP should accommodate this request if possible. The only exceptions where the patient may self-refer are:
• To a Participating Gynecologist for annual gynecological exam except for infertility and to see a non-participating OB/GYN. The PCP may perform the annual exam if agreed upon by the patient.
Primary Care Physician's Referral Responsibilities
A PCP is responsible for ensuring a patient has a referral prior to the appointment with the specialist.
There are two ways a PCP can obtain referral to specialists:
• Log in to HSConnect.
• Submit all referrals through HSConnect
• Call in to the Referral Department: If the referral is an emergency, or you simply would like to speak with a referral department representative, you may obtain a referral by phone by calling:
• Precert: Local: 1-713-497-3060 Toll Free Fax: 1-855-700-2928 Local Fax: 1-832-553-3420
57

Specialist Physician's Referral Responsibilities
Specialists must have a referral from a PCP prior to seeing a patient if the patient’s plan requires a referral. Claims will be denied if a specialist sees a patient without a referral when the health plan requires a referral. The IPA is unable to make exceptions to this requirement. If a referral is not in place, specialists must contact the patient’s PCP before the office visit. In order to verify that a referral has been made, the specialist may log in to HSConnect or the specialist may call to verify.
Instructions for a Specialist to Obtain Referrals:
The specialist can obtain referrals directly for the patient to another Specialist with the following limits:
1. The PCP referred the patient to the specialist
2. The following five (5) conditions must be met:
� Diagnosis must be related to the specialty and/or service to be obtained;
� Diagnosis must be related to reason PCP referred to referring Specialist;
� Must be a covered benefit of the health plan;
� The patient must be currently under the care of the referring specialist;
� And, Referral must be made to a participating provider.
3. The specialist provides follow-up documentation to the PCP for all referrals obtained for further specialty care.
4. Referrals for the following specialty care are excluded from this process and must be referred back to the PCP to obtain referral: Non-participating providers, Chiropractor, Dermatology, Otolaryngology, Maxillofacial Surgeon, Podiatry, Optometry, Transplant Specialist, and Reconstructive (Plastic) Surgeon with the exception of breast reconstruction.
5. The referral must be obtained prior to the services being rendered.
Note: If all elements within the limits above cannot be met, the specialist must defer back to the PCP for further services.
The specialist may obtain referrals via HSConnect or telephone.
*Please refer to page 24 of provider manual for examples on how to utilize HSCONNECT.
58

PHARMACY QUALITY PROGRAMS Narcotic Case Management The Narcotic Case Management Program is designed to identify patterns of inappropriate opioid utilization with the goal to enhance patient safety through improved medication use. Monthly reports are generated using an algorithm that identifies customers at risk of potential opioid overutilization based on the number of prescribers, pharmacies, and calculated morphine milligram equivalent (MME) per day. Any individual with cancer or on hospice care is excluded from the program. The IPA clinical staff review claims data of all identified customers who meet the established criteria and determine whether further investigation with prescribers is warranted. If intervention is deemed appropriate, clinical staff will send written notification by fax to the prescribers involved in the customer’s care requesting information pertaining to the medical necessity and safety of the current opioid regimen. The IPA will reach out to discuss the case with the customer’s opioid prescriber(s) in an attempt to reach a consensus regarding the customer’s opioid regimen. If clinical staff is able to engage with prescribers, then action will be taken based on an agreed upon plan. In the most severe cases, clinical staff may collaborate with the prescriber(s) to implement customer-specific limitations to assist with control of inappropriate utilization or overutilization of opioid medications. The limitations may require customers to use only selected pharmacies or prescribers for opioid medications or limit the amount of opioid medication covered by the health plan. If the IPA does not receive a response from the prescribers, despite multiple outreach attempts, then limitations may be invoked based on the decision of an internal, multi-disciplinary team.
Medication Therapy Management The Medication Therapy Management program is designed to help improve medication therapy outcomes by identifying gaps in care, addressing medication adherence, and recognizing potential cost savings opportunities. The program is designed for customers that satisfy all three of the following criteria:
• Have at least three of the following conditions: Chronic Heart Failure (CHF), Diabetes, Dyslipidemia, Hypertension, and Osteoporosis
• Take at least seven Part D prescription drugs from select classes; and
• Are likely to incur annual costs for covered drugs great than or equal to $4,044
Eligible customers are automatically enrolled into the program and sent a welcome letter encouraging each customer to call to complete their Comprehensive Medication Review (CMR) before their annual wellness visit with their
primary care provider, so the customer can take their medication list to the appointment. A comprehensive medication review is a personal review of prescriptions, OTC medications, herbal therapies, and dietary supplements with a clinical pharmacist. After the completion of the CMR, any potential drug therapy problems (DTPs) that were identified are sent to the prescribing provider and/or primary care provider by mail or fax. Along with DTPs, the provider also receives an updated list of the customer’s medication history through the previous 4 months. Also, an individualized letter, which includes a personal medication record of all medications discussed and a medication action plan, is mailed to the customer. If the customer has any questions or comments about the medication action plan, a phone number is provided for follow up.
In addition to the CMR, customers also receive targeted medication reviews (TMRs) quarterly. The TMRs are automatically generated and completed electronically to review for specific DTPs. If any DTPs are identified, a letter may be mailed or faxed to the prescribing provider and/or primary care provider.
There is no additional cost for participation in the MTM program. Refer eligible customers to the MTM program at 1-800-625-9432 to complete their annual CMR.
Drug Utilization Review The IPA completes a monthly review of prescription drug claims data to assess dispensing and use of medications for our customers. Drug Utilization Review (DUR) is a structured and systematic attempt to identify potential issues with drug therapy coordination among prescribers, unintentional adverse drug events (including drug interactions), and non-adherence with drug regimens among targeted classes of drugs. Retrospective Drug Utilization Review (rDUR) evaluates past prescription drug claims data, and concurrent Drug Utilization Review (cDUR) ensures that a review of the prescribed drug therapy is performed before each prescription is dispensed. cDUR is typically performed at the point-of-sale, or point of distribution, by both the dispensing pharmacist and/or through automated checks that are integrated in the pharmacy claims processing system. The IPA tracks and trends all drug utilization data on a regular basis to enable our clinical staff to determine when some type of intervention may be warranted, whether it is customer-specific or at a population level. Targeted providers and/or customers identified based on DUR activity will receive information regarding the quality initiative by mail or fax. rDUR studies that may be communicated to customers and/or providers include:
• Failure to refill prescribed medications
• Drug-drug interactions
• Therapeutic duplication of certain drug classes
• Narcotic safety including potential abuse or misuse
59

• Use of medications classified as High Risk for use in the older population
• Use of multiple antidepressants, antipsychotics, or insomnia agents concurrently
• Multiple prescribers of the same class of psychotropic drug
Letters to customers will focus on topics such as the importance of appropriate medication adherence or safety issues. Letters to providers will include the rationale for any of the particular concerns listed above that are the subject of the initiative. Provider letters will also include drug claims data for the selected calendar period applicable to the initiative. If you (as a provider) receive a letter indicating that you prescribed a medication that you did not, in fact, prescribe, please notify the IPA using the contact information on the letter. A multidisciplinary team determines the direction of pharmacy quality initiatives for the DUR program. The pharmacy quality initiative concepts originate from a variety of sources, including but not limited to, claims data analysis and trends, the Centers for Medicare and Medicaid Services (CMS) guidance, Pharmacy Quality Alliance (PQA) measures and initiatives, Food and Drug Administration (FDA) notifications, clinical trials or clinical practice guidelines, and other relevant healthcare quality publications.
Important Opioid cDUR Changes for 2019 Opioid initiatives for 2019 focus on strategies to help prevent and combat opioid overuse among our beneficiaries through the use of cDUR. Safety controls will be implemented at point-of-sale, including “soft” and “hard” cDUR edits, which will both reject the claim. The dispensing pharmacy may override a “soft” rejection by entering the appropriate pharmacy professional service (PPS) codes upon consulting the prescriber and/or determining safe and appropriate use of the medication. “Hard” rejections may not be overridden at point-of-sale, and in order to request coverage of the medication(s), a coverage determination must be initiated. Listed below are the opioid changes that will occur in 2019, which are in line with CMS guidance on required and recommended changes to utilization management of opioid prescriptions:
• Opioid prescriptions will be limited to a maximum of a 1-month supply OR a 7-day supply in opioid naïve patients. The IPA defines “opioid naïve” as patients who have not had an opioid medication filled within the past 120 days. This is a “hard” cDUR edit and will require a coverage determination for coverage under the beneficiary’s part D plan if a day supply exceeding these limits is needed.
• Opioid prescriptions for patients who have claims exceeding a total of 90 morphine milligram equivalents (MME) per day AND have 2 or more
opioid prescribers will receive a “soft” rejection at point-of-sale. A coordination of care between the prescriber and dispensing pharmacist is encouraged. Upon consulting the prescriber and receiving approval, the dispensing pharmacist may use pharmacy professional service (PPS) codes to override the “soft” rejection.
• Opioid prescriptions will “soft” reject at point-of-sale if an interaction with a benzodiazepine is detected. The dispensing pharmacist may override the denial with PPS codes if the pharmacist consults with the prescriber, provides patient counseling, and/or determines that it is safe to dispense the medication(s).
• Opioid prescriptions for long-acting opioid medications will “soft” reject at point-of-sale if a duplication of therapy is detected between 2 or more long-acting opioid medications. The dispensing pharmacist may override the denial with PPS codes if the pharmacist consults with the prescriber, provides patient counseling, and/or determines that it is safe to dispense the opioid medication(s).
Prescription Drug Monitoring Programs Nearly all states currently require pharmacies and other dispensers to submit records of certain prescription drugs dispensed on a daily to monthly basis. These data are compiled into state-run databases, termed prescription drug monitoring programs (PDMPs), and made available in a searchable format to prescribers and pharmacists for use in monitoring drug utilization and abuse. In their landmark 2016 Guideline for Prescribing Opioids for Chronic Pain, the CDC features PDMPs prominently in their final recommendations:
Clinicians should review the patient’s history of controlled substance prescriptions using state prescription drug monitoring program (PDMP) data to determine whether the patient is receiving opioid dosages or dangerous combinations that put him or her at high risk for overdose. Clinicians should review PDMP data when starting opioid therapy for chronic pain and periodically during opioid therapy for chronic pain, ranging from every prescription to every 3 months. As part of our ongoing partnership with providers to decrease the unnecessary use and diversion of controlled substances, The IPA encourages prescribers and pharmacists to fully utilize their state’s PDMP. You may find your state’s PDMP at: http://www.pdmpassist.org/content/state-pdmp-websites.
MedWatch: The FDA Adverse Event Reporting Program
60
The Food & Drug Administration (FDA) MedWatch is a safety information and adverse event reporting program that allows both clinicians and consumers to report serious issues with human medical products and receive safety information updates. The FDA relies on clinicians to report medical adverse events after a drug product is marketed, as clinical trials may not elucidate all potential safety concerns for patients.
It is appropriate to report issues related to prescription and over-the-counter medications, biologics, medical devices, combination products, special nutritional products (infant formulas, medical foods), cosmetics, and foods/beverages to FDA’s MedWatch Adverse Event Reporting Program. Types of events to report include: serious adverse events, product quality problems, product use/medication errors, therapeutic inequivalence/failure, and counterfeit medical products. Clinicians may submit a report using Form 3500, available online at www.fda.gov/medwatch/report.htm, or by downloading and mailing (5600 Fishers Lane, Rockville, MD 20852-9787) or faxing the form (fax number 1-800-332-0178). Questions about the form can be answered at 1-800-332-1088.
Safety problems with tobacco, vaccines, investigational study drugs, veterinary products, and dietary supplement problems should not be reported to FDA MedWatch. Adverse events with vaccines can be reported through the Vaccines Adverse Event Reporting System (VAERS) at https://vaers.hhs.gov/reportevent.html. For additional information on where to submit adverse event reports for the other product types, visit https://www.accessdata.fda.gov/scripts/medwatch/index.cfm?action=reporting.home.
Voluntary adverse event reporting is critical to maintain FDA surveillance of product safety. One single report could prompt a product safety investigation that could result in product label updates, Medication Guide inclusion criteria, product recalls, and/or product design, process, packaging, or distribution changes. Additionally, subscribing to MedWatch Safety Alerts via Email (MedWatch E-list), Twitter (@FDAMedWatch), or RSS provides a consumer-friendly platform by which to easily stay updated with recent alerts, and in turn, help improve the overall care and safety of patients.
QUALITY CARE MANAGEMENT PROGRAM Mission Statement
IPA is dedicated to improving the health of the community we serve by delivering the highest quality and greatest value in health care benefits and services.
Values
• Integrity – We always conduct ourselves in a professional and ethical manner.
• Respect – We all have value and will treat others with dignity and esteem.
• Team – We recognize that employees are our main asset and encourage their continued development.
• Communications – We encourage the free exchange of thoughts and ideas.
• Balance – We manage both our personal and company priorities.
• Excellence – We continuously strive to exceed our patients’ expectations.
• Prudence – We always use the company’s financial resources wisely.
Quality Principles
IPA shall apply the guiding values described above to its oversight and operation of its system and:
• Provide services that are clinically driven, cost effective and outcome oriented.
• Provide services that are culturally informed, sensitive and responsive.
• Provide services that enable patients to live in the least restrictive, most integrated community setting appropriate to meet their health care needs.
• Ensure that guidelines and criteria are based on professional standards and evidence-based practices that are adapted to account for regional, rural and urban differences.
• Foster an environment of quality of care and service within the IPA, the Senior Segment of IPA and through our provider partners.
• Promote patient safety as an over-riding consideration in decision-making.
The Quality Improvement program provides guidance for the management and coordination of all quality improvement and quality management activities throughout the IPA and its affiliates.
The program describes the processes and resources to continuously monitor, evaluate and improve the clinical care and service provided to enrollees for both their physical and behavioral health. The program also defines the methodology for identifying improvement opportunities and for developing and implementing initiatives to impact opportunities identified.
• All aspects of physical and behavioral care including accessibility, availability, level of care, continuity, appropriateness, timeliness and clinical effectiveness of care and services provided through IPA and contracted providers and organization.
• All aspects of provider performance relating to access to care, quality of care including provider
61

credentialing, confidentiality, medical record keeping and fiscal and billing activities.
• All services covered.
• All professional and institutional care in all settings including hospitals, skilled nursing facilities, outpatient and home health.
• All providers and any delegated or subcontracted providers.
• Management of behavioral health care and substance abuse care and services.
• Aspects of IPA’s internal administrative processes which are related to service and quality of care including credentialing, quality improvement, pharmacy, health education, health risk assessments, clinical guidelines, utilization management, patient safety, case management, disease management, special needs, complaints, grievances and appeals, customer service, provider network, provider education, medical records, patient outreach, claims payment and information systems
Quality Management Program Goals
The primary objective of the Quality Improvement program is to promote and build quality into the organizational structure and processes to meet the organization’s mission of improving the health of the community we serve by delivering the highest quality and greatest value in health care benefits and services.
The goals the organization has established to meet this objective are:
• Maintain an effective quality committee structure that:
� Fosters communication across the enterprise;
� Collaboratively works towards achievement of established goals;
� Monitors progress of improvement efforts to established goals;
� And, provides the necessary oversight and leadership reporting.
• Ensure patient care and service is provided according to established goals and metrics.
• Ensure identification and analysis of opportunities for improvement with implementation of actions and follow-up as needed.
• Promote consistency in quality program activities.
• Ensure the QI program is sufficiently organizationally separate from the fiscal and administrative management to ensure that fiscal and administrative management does not unduly influence decision-making regarding organizational determinations and/or appeals of adverse determinations of covered benefits.
• Assure timely access to and availability of safe and appropriate physical and behavioral health services for the population served by IPA.
• Ensure services are provided by qualified individuals and organizations including those with the qualifications and experience appropriate to service patients with special needs.
• Promote the use of evidence-based practices and care guidelines.
• Improve the ability of all IPA’s staff to apply quality methodology through a program of education, training, and mentoring.
• Establish a rigorous delegation oversight process.
• Ensure adequate infrastructure and resources to support the Quality Improvement program.
• Assure provider involvement in maintaining and improving the health of IPA’s patients, through a comprehensive provider partnership.
62

Embedded Care Coordination
The CareAllies Embedded Care Coordination (ECC) Program provides onsite practice support to assist Physicians in providing quality care and achieving better clinical outcomes. The Embedded Care Coordinator (ECC) is typically a CareAllies employed RN or LVN. The ECC is a dedicated resource that is embedded in the IPA Physician’s office. Responsibilities of the ECC include but are not limited to:
• Prompt Physician for standard of care alerts/
measures due for MA and Commercial patients
• Meet with Physician and office staff contact person on
a routine basis to discuss STAR ratings, progress,
opportunities, missed opportunities, and complex
patients.
• Abstract data from medical records to close quality
gaps
• HEDIS – gather and submit medical records to close
open HEDIS chases MA and Commercial patients
• Communicate daily admits/discharges to ensure
patient is seen for post discharge follow up and
medication reconciliation
• Participate in Complete Health Team rounds and
Interdisciplinary Care Team meetings as needed to
discuss needs for identified patients.
CODING AND PERFORMANCE MANAGEMENT INITIATIVES CIGNA-HEALTHSPRING ENHANCED ENCOUNTER:
For Cigna-HealthSpring patients, Lumeris is an accountable care delivery innovation company offering health systems, payers, and provider’s operational support, technology, and consulting services. Lumeris’ innovative solutions help health care organizations design, build, operate, measure, and optimize any accountable care model to accomplish the Triple Aim Plus One: improved quality, cost, and patient and physician satisfaction. An Enhanced Encounter is a comprehensive patient exam designed to accurately and compliantly document a patient’s health history, current conditions, quality measures and future risk areas. The Enhanced Encounter program is used in conjunction with the Audit Tool. As Enhanced Encounter forms are submitted they are incorporated into the Audit Tool and reviewed, and can result in feedback to the providers. For
63

HEALTH PLANS CIGNA
• Cigna-HealthSpring (MAPD)
• Cigna Collaborative Accountable Care Legacy
• Clinically Integrated Network (CIN) Cigna Collaborative Accountable Care
• Cigna HMO (City of Houston)
BLUE CROSS BLUE SHIELD TX
• Blue Advantage HMO (MAPD)
• Blue Value Based Incentive Plan (VBIP)
Cigna-HealthSpring
Transportation Benefit
Patients may schedule transportation with Access2Care 24 hours a day, seven days a week by calling toll-free 1-866-214-5126. To schedule transportation:
To a doctor's visit
Patient should call Access2Care:
• By 4:00 pm, 24 hours in advance, to schedule a trip.
• 72 hours in advance to schedule trip to plan’s Patient Orientation Meeting.
• If someone will accompany them (limited to one adult).
• If they will be using a wheelchair.
Important: Patient must be ready for pick-up at LEAST one hour before their medical appointment. Driver will arrive at patient’s residence up to one hour before scheduled medical appointment. To cancel, patient must call AT LEAST three hours before scheduled pick-up time.
From a doctor's visit
Patient should:
• Call the phone number on the card that the driver gives them upon arrival at appointment
� Call when they are ready for their return trip. � Driver will arrive within one hour of the call. � Do not call Access2Care.
To a pharmacy on the way home
Patient should call Access2Care:
• Before the driver picks up patient for the return trip
• Pharmacy trips are allowed after a medical appointment or hospital discharge
• Pharmacy trips are not allowed as a stand-alone trip
Please note:
• Each trip is limited to 70 miles one way from patient’s residence or Adult Day Care to health care professional’s office.
• Transportation to health care professional’s office and transportation to return home (round trip) is considered two trips.
• Patient must check their benefits to determine eligibility and number of trips available per benefit year.
Case Management Services
Participating Plan’s case management program is an administrative and clinically proactive process that focuses on coordination of services for patients with multiple comorbidities, complex care needs and/or short-term requirements for care. The program is designed to work as a partnership between patients, providers, and other health services staff. The goal is to provide the best clinical outcomes for patients. The central concept is early identification, education, and measurement of compliance with standards of care. The case management staff strives to enhance the patient’s quality of life, facilitates provision of services in the appropriate setting, and promotes quality cost effective outcomes. Staff patients with specific clinical expertise provide support services and coordination of care in conjunction with the treating provider.
Case Management Program Goals
The Health plan has published and actively maintains a detailed set of program objectives available upon request in our case management program description. These objectives are clearly stated, measurable, and have associated internal and external benchmarks against which progress is assessed and evaluated throughout the year. Plan demographic and epidemiologic data, and survey data are used to select program objectives, activities, and evaluations.
Case Management Approach
The Participating Plan’s has multiple programs in place to promote continuity and coordination of care, remove barriers to care, prevent complications and improve patient quality of life. It is important to note that the Health plan treats disease management as a component of the case management continuum, as opposed to a separate and distinct activity. In so doing, we are able to seamlessly manage cases across the care continuum using integrated staffing, content, data resources, risk identification algorithms, and computer applications.
The Health plan employs a segmented and individualized case management approach that focuses on identifying, prioritizing, and triaging cases effectively and efficiently. Our aim is to assess the needs of individual patients, to secure their agreement to participate, and to match the scope and intensity of our services to their needs. Results from health risk assessment surveys, eligibility data, retrospective claims data,
64

and diagnostic values are combined using proprietary rules, and used to identify and stratify patients for case management intervention. The plan uses a streamlined operational approach to identify and prioritize patient outreach, and focuses on working closely with patients and family/caregivers to close key gaps in education, self-management, and available resources. Personalized case management is combined with medical necessity review, ongoing delivery of care monitoring, and continuous quality improvement activities to manage target patient groups.
Patients are discharged from active case management under specific circumstances, which many include stabilization of symptoms or a plateau in disease processes, the completed course of therapy, patient specific goals obtained; or the patient has been referred to Hospice. A patient’s case may be re-initiated based on the identification of a transition in care, a change in risk score, or through a referral to case management.
How to Use Services
Patients that may benefit from case management are identified in multiple ways, including but not limited to: utilization management activities, predictive modeling, and direct referrals from a provider. If you would like to refer a patient for case management services, please call 1-888-501-1116. In addition, our patients have access to information regarding the program via a brochure and website and may self refer. Our case management staff contacts patients by telephone or face-to-face encounter. The patient has the right to opt out of the program. If the patient opts in, a letter will be sent to the patient and you as the provider. Once enrolled, an assessment is completed with the patient and a plan of care with goals, interventions, and needs is established.
SPECIAL NEEDS PLAN
In 2008, CMS issued the final regulation “Medicare Improvements for Patients and Providers Act of 2008,” known as “MIPPA.” This regulation mandated that all Special Needs Plans have a filed and approved Model of Care by January 1, 2010. The Patient Protection and Affordable Care Act reinforced the importance of the SNP Model of Care as a fundamental component by requiring NCQA review and approval.
Special Needs Plan Eligibility Criteria Special Needs Plans (SNPs) are designed for specific groups of customers with special health care needs. Only customers meeting the following criteria may join the SNP plan. CMS defined these SNP types as follows.
The three SNP specific groups are:
• Dual eligible SNP (D-SNP): (for individuals who eligible for Medicaid and Medicare)
• Chronic conditions SNP (C-SNP): for individuals with chronic conditions that are substantially disabling or life-threatening
• Institutional SNP (I-SNP): for individuals who reside in a long-term care facility
CMS mandates that each SNP type have a Model of Care (MOC). The MOC is an evidenced-based care management program which facilitates the early and on-going assessments, the identification of health risks and major changes in the health status of SNP customers. The SNP MOC provides structure and describes the coordination of care and benefits and services targeted to improve the overall health of our SNP customers. The MOC also serves as also serves to ensure that the unique needs of our SNP customers are identified and appropriately addressed.
The SNP MOC identifies four key care management components:
• SNP population – provides a description of the unique characteristics of our overall and most vulnerable SNP customers.
• Care coordination – describes our SNP staff structure, the Health Risk Assessment (HRA), Individualized Care plan (ICP), Interdisciplinary Care Team (ICT) and Care Transition process, all of which identify the services and benefits offered through this plan and are available to our SNP customers. The wide range of services is targeted to help our SNP customers achieve their optimal health and improve the connection to care.
• Provider Network – describes the Specialized Expertise providers who participate in our SNP program, Clinical Practices guidelines, and Care Transition protocols. The SNP MOC Training is also addressed this section.
• MOC Quality Measurement and Performance Improvement – this section describes the quality improvement plan and identifies goals for the SNP population; this section of the MOC includes clinical and customer satisfaction goals, as well as on-going performance evaluation of the SNP MOC.
SNP MOC Process The SNP MOC care management process focuses on the unique needs of our SNP customers. The MOC includes key program components, including conducting an initial and/or annual HRA, the development of an ICP by the ICT team and with a change in the health status, performing Care Transition coordination. These benefits and services are provided to ensure appropriate care coordination and care management. The IPA also utilizes risk stratification methodology to identify our most vulnerable SNP customers. These members include those who are frail/disabled, customers with multiple chronic illnesses and those at the end of life. The risk stratification process includes input from the provider, customer, and data analysis. The goal is to
65

identify interventions, care coordination and care transitions needs, barriers to care, education, early detection, and symptom management.
• Health Risk Assessment (HRA) – Health plan will conduct an HRA to identify care needs. SNP customers will have a Health Risk Assessment (HRA) completed within 90 days of enrollment and then annually, within 365 days of the last HRA.
• Individualized Care Plan (ICP) – HRA results and evidence-based clinical protocols are utilized to develop an ICP. The Interdisciplinary Care Team is responsible for the development of an ICP.
• Interdisciplinary Care Team – An ICT is composed of key stakeholders, including the PCP and case managers. The ICT help to develop the ICP.
o Primary Care Providers (PCPs) who treat SNP customers are core participants of the Interdisciplinary Care Team (ICT) as they are the primary care giver. However, ICT participants can also include practitioners of various disciplines and specialties, based on the customer’s individual needs. The customer may participate in the ICT meetings, as may health care providers.
• Care Transition – a change in health status could result in new care management needs. As a result, our case management teams provide support to address the specific needs of our SNP population.
o As a provider, your participation is required for the coordination of care, care plan management and in identifying additional health care needs for our Special Needs program customers.
PCP - Your Participation is needed at the ICT meetings. The IPA will invite you to participate in an ICT meeting when your SNP customer requires care management. We encourage you to participate in the ICT meeting and to collaborate in the care planning and identification of care plan goals for your SNP customer. SNP programs are geared support our customers and you by providing the benefits and services required and by supporting care management and customer goal self-management. Additionally, care transitions, whether planned or unplanned, are monitored, and PCPs are informed accordingly. PCP communication to promote continuity of care and ICT involvement is a critical aspect of care transitions protocols. Implementation of the SNP Model of Care is supported through feedback from you, as well as systems and information sharing between the health plan, health care providers and the customer. The SNP Model of Care includes periodic analysis of effectiveness, and all activities are supported by the Stars & Quality department.
SNP Contact Information: When a SNP customer completes a Health Risk Assessment (HRA), a care plan is generated. A copy of the HRA can be obtained by calling: our Health Risk Assessment department at 1-800-331-6769 based on the HRA responses. The customer and assigned PCP will receive a copy of the customer's care plan. A copy of the HRA can be obtained by calling: our Health Risk Assessment department at 1-800-331-6769 To discuss and/or request a copy of the care plan, refer an SNP customer for an Interdisciplinary Care Team meeting or to participate in an Interdisciplinary Care Team
meeting at 1-888-501-1116.
Behavioral Health
The Health plan provides comprehensive mental health and substance abuse coverage to its patients. Its goal is to treat the patient in the most appropriate, least restrictive level of care possible, and to maintain and/or increase functionality.
The Participating Plan’s network is comprised of mental health and substance abuse services and providers who identify and treat patients with behavioral health care needs.
Integration and communication among behavioral health and physical health providers is most important. The Health plan encourages and facilitates the exchange of information between and among physical and behavioral health providers. Patient follow-up is essential. High risk patients are evaluated and encouraged to participate in Participating Plan’s behavioral health focused case management program where education, care coordination, and support is provided to increase patient’s knowledge and encourage compliance with treatment and medications. The Health plan works with its providers to become part of the strategy and the solution to provide quality behavioral health services.
Behavioral Health Services
Behavioral Health services are available and provided for the early detection, prevention, treatment, and maintenance of the patient’s behavioral health care needs. Behavioral health services are interdisciplinary and multidisciplinary: a patient may need one or multiple types of behavioral health providers, and the exchange of information among these providers is essential. Mental health and substance abuse benefits cover the continuum of care from the least restrictive outpatient levels of care to the most restrictive inpatient levels of care.
Behavioral Health services include:
• Access to Participating Plan’s customer Service for orientation and guidance.
• Routine outpatient services to include psychiatrist, addicitionologist, licensed psychologist and LCSWs, and psychiatric nurse practitioners. PCPs may provide behavioral health services within his/her scope of practice.
• Initial evaluation and assessment.
66

• Individual and group therapy.
• Psychological testing according to established guidelines and needs.
• Inpatient hospitalization.
• Medication management.
• Partial hospitalization programs.
Responsibilities of Behavioral Health Providers
The Health plan encourages behavioral health providers to become part of its network. Their responsibilities include but are not limited to:
• Provide treatment in accordance with accepted standards of care.
• Provide treatment in the least restrictive level of care possible.
• Communicate on a regular basis with other medical and behavioral health practitioners who are treating or need to treat the patient.
• Direct patients to community resources as needed to maintain or increase patient’s functionality and ability to remain in the community.
Responsibilities of the Primary Care Physician:
The PCP can participate in the identification and treatment of their patient’s behavioral health needs. His/her responsibilities include:
• Screening and early identification of mental health and substance abuse issues.
• Treating patients with behavioral health care needs within the scope of his/her practice and according to established clinical guidelines. These can be patients with co-morbid physical and minor behavioral health problems or those patients refusing to access a mental health or substance abuse provider, but requiring treatment.
• Consultation and/or referral of complex behavioral health patients or those not responding to treatment.
• Communication with other physical and behavioral health providers on a regular basis.
Patients may access behavioral health services as needed:
• Patients may self-refer to any in-network behavioral health provider for initial assessment and evaluation, and ongoing outpatient treatment.
• Patients may access their PCP and discuss their behavioral health care needs or concerns and receive treatment that is within their PCP’s scope of practice. They may request a referral to a behavioral health practitioner. Referrals however, are not required to receive most in-network mental health or substance abuse services.
• Patients and providers can call the Participating Plan’s Behavioral Health Patient Service to receive orientation on how to access behavioral health services, provider information, and prior authorizations. (See Quick Reference Guide for phone numbers in the Appendix.)
Medical Record Documentation
When requesting prior authorization for specific services or billing for services provided, behavioral health providers must use the DSM-IV multi-axial classification system and document a complete diagnosis. The provision of behavioral health services require progress note documentation that correspond with day of treatment, the development of a treatment plan, and discharge plan as applicable for each patient in treatment.
Continuity of Care
Continuity of Care is essential to maintain patient stability. Behavioral health practitioners and PCPs, as applicable, are required to:
• Evaluate patient if he/she was hospitalized for a behavioral health condition within 7 days post-discharge.
• Provide patients receiving care with contact information for any emergency or urgent matter arising that necessitates communication between the patient and the provider.
• Evaluate patient needs when the patient is in acute distress.
• Communicate with the patient’s other health care providers.
• Identify those patients necessitating follow-up and refer to Participating Plan’s behavioral health focused case management program as necessary.
• Discuss cases as needed with a peer reviewer.
• Make request to Health plan for authorization for patient in an active course of treatment with a non-participating practitioner.
Utilization Management
The Participating Plan’s Health Services Department coordinates behavioral health care services to ensure appropriate utilization of mental health and substance abuse treatment resources. This coordination assures promotion of the delivery of services in a quality-oriented, timely, clinically-appropriate, and cost-effective manner for the patients.
The Participating Plan’s Utilization Management staff base their utilization-related decisions on the clinical needs of patients, the patient’s Benefit Plan, Interqual Criteria, the appropriateness of care, Medicare National Coverage Guidelines, health care objectives, and scientifically-based clinical criteria and treatment guidelines in the context of provider and/or patient-supplied clinical
67

information and other relevant information. For requests for behavioral health services that require authorization, the Health plan will approve the request or issue a notice of denial if the request is not medically necessary.
Concurrent Review
Concurrent Review is the process of initial assessment and continual reassessment of the medical necessity and appropriateness of inpatient care during an acute care hospital admission, rehabilitation admission or skilled nursing facility or other inpatient admission in order to ensure:
• Covered services are being provided at the appropriate level of care;
• And, services are being administered according to the individual facility contract.
The Health plan requires admission notification for the following:
• Elective admissions
• ER and Urgent admissions
• Transfers to Acute Rehabilitation, LTAC and SNF admissions *These levels of care require pre-authorization*
• Admissions following outpatient procedures or observation status
• Observation status
• Newborns remaining in the hospital after the mother is discharged.
Emergent or urgent admission notification must be received within twenty-four (24) hours of admission or next business day, whichever is later, even when the admission was prescheduled. If the patient’s condition is unstable and the facility is unable to determine coverage information, Health plan requests notification as soon as it is determined, including an explanation of the extenuating circumstances. Timely receipt of clinical information supports the care coordination process to evaluate and communicate vital information to hospital professionals and discharge planners. Failure to comply with notification timelines or failure to provide timely clinical documentation to support admission or continued stay could result in an adverse determination.
The Participating Plan’s Health Services department complies with individual facility contract requirements for concurrent review decisions and timeframes. The Participating Plan’s nurses, utilizing CMS guidelines and nationally accepted, evidence-based review criteria, will conduct medical necessity review. The Health plan is responsible for final authorization.
Participating Plan’s preferred method for concurrent review is a live dialogue between our Concurrent Review nursing staff and the facility’s UM staff within 24 hours of notification or on the last covered day. If clinical information is not received within 72 hours of admission or last covered day, the case will be reviewed for medical necessity with
the information health plan has available. If it is not feasible for the facility to contact health plan via phone, facilities may fax the patient’s clinical information within 24 hours of notification to 1-832-553-3420. Skilled Nursing Facility (SNF) Reviews should be faxed to 1-713-437-3130. For SNF admission requests, a recent PM&R or physical, occupational and/or speech therapy consult is requested along with the most recent notes for therapy(ies) or recent medical status and expected skilled treatment and service requirements.
Following an initial determination, the concurrent review nurse will request additional updates from the facility on a case-by-case basis. The health plan will render a determination within 24 hours of receipt of complete clinical information. Participating Plan’s nurse will make every attempt to collaborate with the facility’s utilization or case management staff and request additional clinical information in order to provide a favorable determination. Clinical update information should be received 24 hours prior to the next review date.
The health plan’s Medical Director reviews all acute, rehab, LTAC, and SNF confinements that do not meet medical necessity criteria and issues a determination. If the health plan’s Medical Director deems that the inpatient or SNF confinement does not meet medical necessity criteria, the Medical Director will issue an adverse determination (a denial). The Concurrent Review nurse or designee will notify the provider(s) e.g. facility, attending/ordering provider verbally and in writing of the adverse determination via notice of denial. The criteria used for the determination is available to the practitioner/facility upon request. To request a copy of the criteria on which a decision is made. Call 1-832-553-3333.
In those instances where the attending provider does not agree with the determination, the provider is encouraged to contact Participating Plan’s Medical Director for Peer-to-Peer discussion. The telephone number to contact our Medical Director for the discussion call is 1-832-553-3333.
Following the Peer-to-Peer discussion, the Medical Director will either reverse the original determination and authorize the confinement or uphold the adverse determination.
For patients receiving hospital care and for those who transfer to a Skilled Nursing Facility or Acute Inpatient Rehabilitation Care, the health plan will approve the request or issue a notice of denial if the request is not medically necessary. The health plan will also issue a notice of denial if a patient who is already receiving care in an Acute Inpatient Rehabilitation Facility has been determined to no longer require further treatment at that level of care. This document will include information on the patients’ or their Representatives’ right to file an expedited appeal, as well as instructions on how to do so if the patient or patient’s physician does not believe the denial is appropriate.
The health plan also issues written Notice of Medicare Non-Coverage (NOMNC) determinations in accordance with CMS guidelines. This notice will be sent by fax to the SNF or HHA.
68

The facility is responsible for delivering the notice to the patient or their authorized representative/power of attorney (POA) and for having the patient, authorized representative or POA sign the notice within the written time frame listed in the Adverse Determination section of the provider manual. The facility is requested and expected to fax a copy of the signed NOMNC back to Health Services at the number provided. The NOMNC includes information on patients’ rights to file a fast track appeal.
Readmission
The Health Services Department will review all readmissions occurring within 31 days following discharge from the same facility, according to established processes, to assure services are medically reasonable and necessary, with the goal of high quality cost effective health care services for health plan patients.
The Health Services Utilization Management (UM) staff will review acute Inpatient and Observation readmissions. If admissions are determined to be related; they may follow the established processes to combine the two confinements.
The Role of the ACCM
(Acute Care Case Manager)
Health plan Acute Care case managers (ACCMs) are registered nurses. All ACCMs are expected to perform at the height of their license. They understand Participating Plan’s plan benefits and utilize good clinical judgment to ensure the best outcome for the patient.
The Acute Care Case Manager has two major functions:
• Ensure the patient is at the appropriate level of care, in the appropriate setting, at the appropriate time through utilization review.
• Effectively manage care transitions and length of stay (LOS).
Utilization review is performed utilizing evidence-based guidelines (Interqual) and collaborating with Primary Care Physicians (PCP), attending physicians, and Participating Plan’s Medical Directors.
The ACCM effectively manages all transitions of care through accurate discharge planning and collaboration with facility personnel to prevent unplanned transitions and readmissions via interventions such as:
• Medication reconciliation.
• Referral of patients to Participating Plan’s programs such as: CHF CCIP Program, Respiratory Care Program, and Fragile Fracture Program.
• Appropriate coordination of patient benefits.
• Obtaining needed authorizations for post-acute care services or medications.
• Collaborating with attending physician and PCP, as needed.
• Introducing and initiating CTI (Care Transition Intervention).
• Addressing STAR measures, as applicable: Hgb A1C and foot care, LDL, colorectal cancer screening, osteoporosis management in women who had a fracture, falls, emotional health, flu and pneumonia vaccines and medication adherence.
• Facilitating communication of care level changes to all parties.
• The goals of the ACCM are aligned with the goals of acute care facilities.
• Patients/patients receive the appropriate care, at the appropriate time, and in the most appropriate setting.
• Readmissions are reduced and LOS is managed effectively.
We strive for Primary Care Physicians (PCP), attending physicians, and acute care facility personnel to view the Participating Plan’s ACCM as a trusted resource and partner in the care of our patients (your patients).
Special Needs Plan - Model of Care
Medicare Advantage Special Needs Plans (SNPs) are designed for specific groups of patients with special health care needs.
The three specific groups are:
• “Dual eligible” beneficiaries (individuals who are eligible for both Medicaid & Medicare);
• Individuals with Chronic conditions;
• And, individuals who are residents of long-term care facilities or require that level of care and reside in the community.
In 2008, Congress passed the statute “Medicare Improvements for Patients and Providers Act of 2008,” known as “MIPPA.” This regulation mandated that all Special Needs Plans have a filed and approved Model of Care by January 1, 2010.
The Model of Care is an evidenced-based process by which we integrate benefits and coordinate care for patients enrolled in Participating Plan’s Special Needs Plans. The Model of Care facilitates the early assessment and identification of health risks and major changes in the health status of patients with complex care needs, as well as the coordination of care to improve their overall health.
Special Needs Plan Model of Care has the following goals:
• Improve access to medical, mental health, and social services.
• Improve access to affordable care.
• Improve coordination of care through an identified point of contact.
69

• Improve transitions of care across health care settings and providers.
• Improve access to preventive health services.
• Assure appropriate utilization of services.
• Improve beneficiary health outcomes.
Importantly, the Model of Care focuses on the individual SNP patient. SNP patients receive a health risk assessment within 90 days of enrollment and then, annually, within one year of completion of the last HRA. Based on the results of this assessment, an individualized care plan is developed using evidence-based clinical protocols. All SNP patients must have an individualized care plan. Interdisciplinary care teams are responsible for care management, support the assessment, and care planning process.
PCPs that treat Special Needs Plan patients are core participants of their Interdisciplinary Care Teams and oversee clinical care plan development and maintenance. Interdisciplinary care team participants include PCPs as well as practitioners of various disciplines and specialties, based on the needs of the patient. The patient may participate in the care team meetings, as may all health care providers. The plan-developed individualized care plan is recorded centrally so that it may be shared with all patients of the interdisciplinary care team, as indicated. All providers are encouraged to participate in the SNP Model of Care and interdisciplinary care teams.
The health plan uses a data-driven process for identifying the frail/disabled, patients with multiple chronic illnesses and those at the end of life. Risk stratification and protocols for interventions around care coordination, care transitions, barriers to care, primary care givers, education, early detection, and symptom management are also components of the Model of Care. Based on the needs of plan patients, a specialized provider network is available to assure appropriate access to care, complementing each patient’s primary care provider.
The health plan uses care transitions protocols and specific programs to support patients through transitions, connect patients to the appropriate providers, facilitate the communication process between settings, promote patient self-management and reduce the risk for readmissions. Care transitions, whether planned or unplanned, are monitored, and PCPs are informed accordingly. PCP communication to promote continuity of care and interdisciplinary care team involvement is a critical aspect of Participating Plan’s care transitions protocols.
Implementation of the Model of Care is supported by systems and processes to share information between the health plan, health care providers and the patient. The SNP Model of Care includes periodic analysis of effectiveness, and the Quality Improvement Program supports all activities.
For Dual SNP patients:
Providers may contact our Health Risk Assessment department to request patients’ HRA results at 1-800-331-6769.
To discuss and/or request a copy of a patient’s care plan, refer a patient for an Interdisciplinary Care Team meeting or participate in an Interdisciplinary Care Team meeting, please contact our Case Management department at 1-888-501-5116.
For Chronic SNP patients:
Providers may contact our Health Risk Assessment department to request patients’ HRA results at 1-800-331-6769.
To discuss and/or request a copy of a patient’s care plan, refer a patient for an Interdisciplinary Care Team meeting or participate in an Interdisciplinary Care Team meeting, please contact our Case Management department at 1-888-501-1116.
Fraud, Waste, and Abuse
In order to protect Medicare trust funds from fraud, waste and abuse, to ensure Part D drugs are prescribed only by qualified suppliers, and to follow the recommendations from the Office of Inspector General (OIG); the Centers for Medicare & Medicaid Services (CMS) proposed changes to the Medicare participation requirements related to Drug Enforcement Administration (DEA) certification of registration.
Pharmacy Prescription Benefit
Part D Drug Formulary
Formulary listings, utilization management criteria, and formulary changes for formularies can be found at: http://www.cigna.com/medicare/resources/drug-list-formulary.
The health plan utilizes the USP classification system to develop Part D drug formularies that include drug categories and classes covering all disease states. Each category must include at least two drugs, unless only one drug is available for a particular category or class. The health plan includes all or substantially all drugs in protected classes, as defined by CMS. All formularies are reviewed for clinical appropriateness by the health plan’s Pharmacy and Therapeutics (P&T) Committee, including the utilization management edits placed on formulary products. Health plan submits all formulary changes to CMS according to the timelines designated by CMS.
A Part D drug is a drug that meets the following criteria: may be dispensed only by prescription; is approved by the FDA; is used and sold in the US; is used for a medically accepted indication; includes FDA-approved uses; includes uses approved for inclusion in the American Hospital Formulary Service Drug Information (AHFS DI), Micromedex, National Comprehensive Cancer Network (NCCN), Clinical Pharmacology, plus other authoritative compendia that the Secretary of Health and Human Services identifies, as off-label
70

uses described in peer-reviewed literature are insufficient on their own to establish a medically accepted indication; and finally includes prescription drugs, biologic products, vaccines that are reasonable and necessary for the prevention of illness, insulin, and medical supplies associated with insulin that are not covered under Parts A or B (syringes, needles, alcohol, swabs, gauze, and insulin delivery systems).
Drugs excluded under Part D include the following: drugs for which payment as so prescribed or administered to an individual is available for that individual under Part A or Part B; drugs or classes of drugs, or their medical uses, which may be excluded from coverage or otherwise restricted under Medicaid (with the exception of smoking cessation products); drugs for anorexia, weight loss or weight gain; drugs to promote fertility; drugs for cosmetic purposes and hair growth; drugs for symptomatic relief of coughs and colds; vitamins and minerals (except for prenatal vitamins and fluoride preparations); non-prescription drugs; outpatient prescriptions for which manufacturers require the purchase of associated tests or monitoring services as a condition for getting the prescription (manufacturer tying arrangements); agents used for treatment of sexual or erectile dysfunction (ED) (except when prescribed for medically-accepted indications such as pulmonary hypertension).
Part D Utilization Management
Health plan’s formularies include utilization management requirements that include prior authorization, step therapy and quantity limits.
• Prior Authorization (PA): For a select group of drugs, the health plan requires the patient or their physician to get approval for certain prescription drugs before the patient is able to have the prescription covered at their pharmacy.
• Step Therapy (ST): For a select group of drugs, the health plan requires the patient to first try certain drugs to treat their medical condition before covering another drug for that condition.
• Quantity Limits (QL): For a select group of drugs, the health plan limits the amount of the drug that will be covered without prior approval.
The Centers for Medicare & Medicaid Services (CMS), in collaboration with the Pharmacy Quality Alliance (PQA), has identified certain medications as high risk when used in the elderly. This list is based upon the American Geriatrics Society (AGS) 2012 Updated Beers Criteria. All medications on the list are ones for which the AGS Expert Panel strongly recommends avoiding use of the medication in older adults. Use of these medications in the elderly may result in increased rates of adverse drug events, potential drug toxicity, and an increased risk of falls and/or fractures. Due to these safety concerns, the health plan requires prior authorization for these medications in all patients aged 65 and older in order to confirm that the benefits outweigh the risks, and that safer
alternatives cannot be used.
How to file a Coverage Determination A Coverage Determination (CD) is any decision that is made by or on behalf of a Part D plan sponsor regarding payment or benefits to which an enrollee believes he or she is entitled. Coverage Determinations may be received orally or in writing from the patient’s prescribing physicians.
For the Provider Call Center, please call 1-877-813-5595 or fax 1-866-845-7267. The mailing address is: Coverage Determination & Exceptions PO Box 20002 Nashville, TN 37202
The Provider Call Center is open from 7 a.m. CST to 8 p.m. CST Monday through Friday. Any call received after 8 p.m. CST will be routed to a voicemail box and processed daily. To ensure timely review of a CD and that the prescriber is aware of what requires for the most commonly requested drugs, forms are available online at http://www.cigna.com/medicare/resources/2015-customer-forms or by requesting a fax when calling 1-877-813-5595. A provider will receive the outcome of a Coverage Determination by fax no later than seventy-two (72) hours after receipt for standard requests or receipt of the supporting statement and no later than twenty-four (24) hours after receipt for urgent requests or receipt of the supporting statement. The following information will be provided: 1) the specific reason for the denial taking into account the patient’s medical condition, disabilities and special language requirements, if any; 2) information regarding the right to appoint a representative to file an appeal on the patient’s behalf; and 3) a description of both the standard and expedited redetermination processes and timeframes including conditions for obtaining an expedited redetermination and the appeals process. The fax cover sheet includes the peer-to-peer process if a provider has questions and wants to review with a clinical pharmacist.
How to file a Part D Appeal
A Part D appeal can be filed within 60 calendar days after the date of the Coverage Determination decision, if unfavorable. The health plan will ask for a statement and select medical records from the prescriber if a patient requests a Part D appeal. For an expedited appeal, the health plan will provide a decision no later than seventy-two (72) hours after receiving the appeal, and for a standard appeal, the timeframe is seven (7) days. If the request is regarding payment for a prescription drug the patient already received, an expedited appeal is not permitted.
Part D Appeals may be received orally or in writing from the patient’s prescribing physicians by calling 1-866-845-6962 or fax 1-866-593-4482.
The mailing address is: Part D Appeals PO Box 24207
71

Nashville, TN 37202−9910
The DEA implements and enforces the Controlled Substances Act (CSA). The CSA makes possession of authority under state law to dispense controlled substances a requirement for both obtaining and maintaining a DEA certificate of registration. CMS equates a DEA certificate of registration to prescribe controlled substances as similar to a state’s requirement that a physician or eligible professional be licensed or certified by the state to furnish health care services.
To ensure additional controls are in place to protect the Medicare trust funds from any fraud, waste and abuse the following changes were finalized:
• Granting CMS the authority to deny a physician or eligible professional’s Medicare enrollment application if: (1) his or her DEA certificate is currently suspended or revoked; or (2) the applicable licensing or administrative body for any state in which the physician or eligible professional practices has suspended or revoked the physician or eligible professional’s ability to prescribe drugs, and such suspension or revocation is in effect on the date he or she submits his or her enrollment application to the Medicare contractor.
• Granting CMS the authority to revoke a physician or eligible professional’s Medicare enrollment if: (1) his or her DEA certificate is suspended or revoked; or (2) the applicable licensing or administrative body for any state in which the physician or eligible professional practices suspends or revokes his or her ability to prescribe drugs.
CMS considers the loss of the ability to prescribe drugs, via a suspension or revocation of a DEA certificate or by state action, a clear indicator that a physician or eligible professional may be misusing or abusing his or her authority to prescribe such substances. These changes are consistent with the CMS requirement that suppliers maintain compliance with all applicable licensure and certification requirements.
72

Renaissance Physicians Health Plan Election to Participate Form This Election to Participate form confirms the undersigned health care provider’s (who is referred to as "You") agreement to participate in the health plan programs listed below with Renaissance Physicians (“IPA”). Health Plan Participation Option: Answer Yes or No
Plan Option Elect to Participate
Open Panel
Closed Panel
Current Patient Only
Age Limitation Please Specify
Cigna HealthSpring
Cigna Collaborative Accountable Care (CAC)
Cigna HMO (City of Houston)
Blue Cross Blue Shield (Medicare Advantage)
Blue Value Based Incentive Plan (VBIP)
1. You understand that your participation in the Cigna-IPA CAC will become effective upon notice from IPA. 2. You understand and agree that if you are a Primary Care Physician (specialty of Family Practice, General Practice, Internal
Medicine, Pediatrics, Adolescent Medicine, and Geriatric Medicine) you may only participate in one Cigna CAC program at a time.
3. You acknowledge that your agreement through which you participate in the Cigna provider network (“Participation Agreement”) remains in full force and effect. Should your Participation Agreement terminate for any reason, your participation in the Cigna-IPA CAC program immediately and automatically terminates.
4. You acknowledge that your participation in the Cigna-IPA CAC program immediately and automatically terminates if the CAC agreement between Cigna and IPA terminates.
5. You acknowledge and agree that Cigna and IPA or its designee are authorized to exchange data specific to CAC provision of covered services to Cigna members in furtherance for the CAC to include, but not be limited to, facilitating data reporting and assessment related to the CAC.
6. Your effective date with CAC will be the 1st of the month depending upon completion of credentialing and receipt of the signed ETPF form. See below for tentative effective dates.
Your effective date with CAC will be the 1st of the month depending upon completion of credentialing and receipt of the signed ETPF form. See below for tentative effective dates.
CAC Effective Date Timeline 2019 Quarter ETPF Received by Date Effective Date with CAC LOB January 1st November 15th January 1st April 1st February 15th April 1st July 1st May 15th July 1st October 1st August 15th October 1st
Provider Printed Name: __________________________________________________ Provider Signature: ___________________ Provider Tax Identification Number: ____________________ Medicare ID Number: ___________________ Provider Address: ___________________ POD: _____________________________________________________________________ Effective Date: ______________________________________________________________
Please fax this form to:
♦ Provider Relations at 832-553-3418
73

BEHAVIORAL HEALTH SERVICES QUICK FACTS AND PHONE GUIDE
Cigna-HealthSpring is committed to providing our patients with the highest quality and greatest value in healthcare benefits and services. Managing the behavioral health benefits of our patients allows Cigna-HealthSpring the opportunity to demonstrate this commitment by recognizing overall needs and providing better care.
Cigna-HealthSpring will continue to offer the outpatient services listed below without the requirement of a prior authorization. Any service not listed will continue to utilize the standard authorization process.
Services Requiring No Authorization by Participating Provider
CPT Code DESCRIPTION Report with Psychotherapy Add-On Codes
90791 Psychiatric diagnostic evaluation (no medical services)
90792 (or New Patient E & M codes)
Psychiatric diagnostic evaluation with medical services
Out Patient 99201-99205 99211-99215
New Patient Visit (10-60 min) Established Patient (5-25 min)
Psychotherapy Add On Codes:
(when appropriate)
90833-30 min 90836-45 min 90838-60 min
Nursing Facility 99304-99306 99307-99310
New Patient Visit (10-45 min) Established Patient (10-35 min)
90832 Psychotherapy (30 min) 90834 Psychotherapy (45 min) 90837 Psychotherapy (60 min) 90846 Family Psychotherapy (without patient present) 90847 Family Psychotherapy (with patient present)
90853 Group Psychotherapy (other than of a multiple–family group) Physician’s Office Only ~ Facilities Require Prior Authorization.
Q3014 Telehealth FUNCTION PHONE/ADDRESS DESCRIPTION OF SERVICES
Member Eligibility/Benefits 800-230-6138
Verification of coverage and benefits; for facility admissions and other facility services, consult the Common Working File if member does present ID card.
Authorization Line 866-780-8546 Fax: 866-949-4846
Prior authorization is required for services not listed above.
Inpatient Admissions 866-780-8546 Fax: 866-949-4846
Notification is required within 24 hours of admissions; clinical staff available 24 hrs a day/7 days a week to assist with notifications and precertification.
Claims Submission (paper)
Cigna-HealthSpring P.O. Box 981706
El Paso, TX 79998
Claims Submission (electronic)
Clearing Houses: *Emdeon, *Relay Health, *Proxymed, *OfficeAlly * SSIGroup, * Availity *Medassets *Zirmed
*GatewayEDI Payor ID 63092
Claim Status Inquires 800-230-6138
HSConnect www.hsconnectonline.com
Access to on-line provider portal for verification of member eligibility, authorization, and claim payment review. Select Providers tab, then HSConnect to access portal.
74

ARCADIA
Arcadia is a population health management company, specializing in data aggregation, analytics, and
workflow software for value-based care. Their customers achieve financial success in their risk-sharing
contracts through Arcadia’s focus on creating the highest quality data asset, pushing expertly derived
insights to the point of care, and supporting administrative staff with data when and where they need it
with applications including care management and referral management. Arcadia has off-the-shelf
integration technology for more than 40 different physical and behavioral health EHR vendors, powered
by machine learning that combs through variations in over 50 million longitudinal patient records
across clinical, claims and operational data sources. Arcadia software and outsourced ACO services
are trusted by some of the largest risk- bearing health systems and health plans in the country to
improve the bottom line. Founded in 2002, Arcadia is headquartered outside Boston in Burlington, MA,
with offices in Seattle, Pittsburgh, Chicago, and Rockford, IL.
Home Page
The Home Page is the centralized location of the Arcadia platform where many essential components
can be easily accessed. Returning to the Home Page can be easily done by selecting the Arcadia logo in
the upper left corner from anywhere in the core platform. From this page the end user can quickly
navigate to the following:
� Search Bar: allows users to find a specific patient by searching based on name, member ID or
date of birth
� Custom Chips: globally filtered reports and lists that allow quick access to the Quality
Dashboard, Care Gaps report, Arcadia 360 Exam List, and the Member List. Chips are consistent
for all users
� Custom Reports and Lists: administrative or user created reports and lists customized to adapt
to specific population needs
75

Patient Search
Users may search for a specific patient in the Search Bar near the top of the homepage or with the
Search Icon in the upper right corner using the following:
� Name (Last Name, First Name)
� Member Number
� Date of Birth (MM-DD-YYYY or YYYY-MM-DD)
Patient Chart
The Patient Chart is the longitudinal health record of the patient. Access to the Patient Chart may be
done through a patient search or selecting a specific patient hyperlink within an Arcadia report. This
chart will help orient the clinician to the following information:
� medications
� utilization history
HELPFUL HINT!
The most accurate search results come from using the exact member number or full name.
76

� eligible and outstanding quality measure gaps
� chronic condition history
� patient demographics
� care team (Care Management users only)
From the Patient Chart, end users will have access to the following buttons and functionality (based on
individual user access rights):
� The Share button allows the patient chart to be printed or downloaded as a PDF
� The Back button returns the user to the previous report or list
� The 360 button directs the user to enter the Arcadia 360 module
� The Quality button allows access to the Hybrid Quality module
Patient Chart: Care Management User
77

In addition, end users that leverage care management functionality, will have access to the following
tabs and buttons:
� The CM Activity tab displays a scorecard view of scheduled tasks, activities and associated detail
� The CM Plan tab shows information around a set of care plan goals and actionable
interventions to achieve those goals
� The New Task button allows the user to schedule various different tasks
� The Back to Dashboard button returns the user to the CM Dashboard
User Manual
� The User Manual contains all documentation related to Arcadia Analytics and its additional
modules. Access the manual by navigating to the bottom of the page within the Arcadia
platform and selecting the User Manual button. Once in the User Manual, use the search
function at the top right of the page to search for specific terms and features or use the
navigation tree in the left sidebar to find content hierarchically.
78

Contacting Production Support
�Customer Portal: “Report Issue” button in the Web Application
�Email: [email protected]
�Phone: 888.853.8095 Please remember to never send personal or patient sensitive information via unencrypted email.
If you must provide PHI or PI, please use the customer portal or call the Production Support team
for instructions on the best way to communicate sensitive information. Depending on how you
created your request, you will receive an acknowledgement with a request number and possibly an
estimated time of resolution for your request. Please make a note of and refer to this request
number in future communications if you are not using the customer portal.
79

CARE MANAGEMENT PROGRAMS STANDING ORDER
� I would like all of my eligible CHS patients to become enrolled into any appropriate CHS care management
program if criteria has been met.
Cigna-HealthSpring (CHS) is structured to support the PCP network by targeting patients for enrollment into various care
management programs. These programs are designed to coordinate with, but not replace, the PCPs. Below are the programs
that are offered to any eligible CHS patient along with brief highlights of the program. If you agree for the Cigna-HealthSpring
health services team to automatically enroll any of your eligible CHS patients into any one of these programs, please indicate
your agreement by either, a.) checking the box next to the program(s) you choose, or b.) check the box that agrees for this
order to apply for my patient’s enrollment into ANY eligible care management program(s):
Where can I find more information?
Please contact your local Network Operations representative.
Once complete, please sign below and fax this Standing Order form to: 832-553-3423
I agree to allow Cigna-HealthSpring to refer/enroll my patients who meet criteria for any of the programs mentioned
above. My patients may be identified by the health plan Medical Directors and/or Health Services team members
(including Inpatient Review nurses, Embedded Care Coordinator nurses and Case Managers).
Please accept my signature below as a Standing Order, or opt-in, for my patients:
Physician Name (Printed Legibly): _______________________________________________________________
Physician Signature: _______________________________________________________ Date: ____________________
IPA/POD:___________ Revised: 8/2/18
� Alegis Care Complex Care Program (CCP)
• Ideal for your patients with chronic medical
conditions and/or have had recent high utilization,
such as:
� Frequent ER visits OR ≥2 admits in 3 months or
≥3 admits in 6 months (includes Observation)
� Difficulty with optimizing the medical condition
(i.e. diabetes, CHF, COPD, etc), despite multiple
efforts taken by you, the PCP.
� Aspire Palliative Care Program
• An innovative home palliative care program
committed to providing an extra layer of support for
patients with end stage conditions, such as advanced
cancer, dementia, and end stage organ disease.
Services include patient and family education, goals
of care discussions, patient symptom management
and the coordination of care with the patient’s
current provider.
� Comprehensive Case Management
• An Episodic, Telephonic and Community program to
support those patients with chronic diseases
resulting in higher utilization. Management and
intervention is telephonic with home, office or
hospital face-to-face visits when necessary.
� Diabetes Empowerment and Education Program (DEEP)
• A 6-week program providing self-management
education to patients with diabetes. The program is
structured to meet within the community and
designed to empower patients with strategies to
better manage their diabetes. Patients who graduate
from the program are enrolled in our Episodic
Diabetes Case Management program.
� Respiratory Program
• Designed to impact quality care and decrease
utilization for patients with respiratory conditions.
Patients with a diagnosis of COPD, Asthma, or
Emphysema with home respiratory equipment and
who had ≥2 admissions or with disease specific
medications qualify for this program. These patients
have an initial home evaluation and respiratory
assessment by a Registered Respiratory Therapist
(RRT) and are then followed telephonically by a RRT
Case Manager.
� Alegis Care In-Home 360 Program
• This program focuses on completing in-home 360’s
for patients who have NOT been seen by you in the
past year, and/or who have not responded to your
office staff outreaching to schedule the 360.
80

Cigna-HealthSpring ID Card
81

Cigna Commercial Cigna Local Access Plus
Access Standards
A physician group (hereinafter collectively “Provider”) entering into a Collaborative Accountable Care (CAC) relationship with Cigna with their Local Access Plus product must meet the following, minimum standards when providing care:
• Daily acute care: Provider shall extend daily hours as needed until last urgent care patient is seen. Urgent care services may be delivered in an alternate facility, but Provider will use best efforts to ensure care is delivered in a Provider facility;
• Telephonic triage: Provider shall provide clinically capable evening and weekend telephonic consultation and triage service;
• Evening and weekend acute care: Provider shall provide evening and weekend office hours, which may be provided on a regional basis or other reasonable limited location basis;
• Access to care: Provider shall ensure that Cigna Participants receive physician access equal to or better than that of any other payer.
Assignment of Aligned CAC Participants
Aligned CAC Participants will be identified at minimum every three (3) months using the methodology described below. A Participant becomes an Aligned CAC Participant once the Participant is listed on the Aligned CAC Participant list, except for purposes of determining Provider’s TMC and the Market’s TMC or TMC Performance Index, in which case when a Participant becomes an Aligned CAC Participant, the Participant is considered an Aligned CAC Participant for the entire Measurement Period or for the time during the Measurement Period in which the Aligned CAC Participant was a Participant, whichever is longer. Participants with Cigna Connect, Cigna Focus or Cigna SureFit networks, and Shared Administration, Strategic Alliances, patients under a capitation arrangement Payer Solutions, and Cigna International plans will not be included as CAC Participants. Also, excluded are Participants in Benefit Plans which have elected to not participate in the CAC program and when the Benefit Plan that is insured or administered by Cigna is not primary.
• Cigna uses twenty-four (24) months of retrospective medical claim data.
• Records are selected for a specific market(s); claim records are assigned a market based on the servicing physician’s zip code.
The alignment uses records where:
• Servicing physician is a primary care physician (PCP) (specialty of Family Practice - FP, General Practice - GP, Internal medicine -
IM, pediatrics – PD, Adolescent Medicine – AM, Geriatric Medicine - GE*)
• 29 evaluation and management (E&M) codes are used for alignment:
� Office Visit E&M, New & Established (99201 – 99205; 99211 – 99215)
� Office Visit Preventive, New & Established (99381 – 99387; 99391 – 99397)
� Office Consult (99241 – 99245)
• Alignment – Step 1 (most recent twelve (12) months)
� Services for the 29 established E&M codes and totaled by Participant and PCP (sorted by Participant and number of visits).
� Participant is assigned to the PCP with the most visits.
� If there is a tie for the number of visits (to multiple PCPs), assignment is to the PCP with the most recent visit.
• Alignment – Step 2 (prior twelve (12) months)
� For Participants NOT aligned for the most recent 12 months (no PCP visit), services for the 29 E&M codes for the prior 12 months (sorted by service date).
� Participant is assigned to the PCP with the most recent visit.
� If Participant is no longer an active Participant with Cigna in the most recent 12 months, they will be excluded.
• Claim Assignment (most recent twelve (12) months)
� All Participant claim activity occurring nationwide over the most recent 12 month period attributed to the aligned PCP.
� If a Participant’s zip code is greater than 100 miles from the aligned PCP, Participant is aligned to the “next best” aligned PCP within 100 miles. If there is no other service to an aligned PCP within 100 miles, the Participant is not aligned.
*Alignment to OB/GYN’s, Nurse Practitioners (NP), and Physician Assistants (PA) will occur when Participants do not have a visit with one of the physician specialties described above. In order for this to occur, OB/GYNs, NPs, and PAs must be included in the CAC roster, and NPs and PAs must be credentialed to provide primary care services.
Patient Level Actionable Reports
The following reports will be provided to the group:
• Monthly Report: A combined report that includes Previse, Well Informed Gaps in Care and Monthly Closed Case Referral reports. It also includes pharmacy and other pertinent patient detail information helpful in managing high risk patients. Please refer to the below descriptions for more detail on each section.
82

� PreVise: a Cigna developed predictive model, which measures the likelihood of an individual incurring high health care expenditures in a twelve-month period. The data utilized in this model includes information from medical claims, pharmacy claims, demographic data, lab results, gap scores, and episode treatment groups (ETGs).This model looks at hundreds of variables to project a risk level for every Participant.
� Well Informed Gaps in Care (Gaps in Care): This report identifies Aligned CAC Participants who may need additional services based on past claims history. Gaps are identified at a patient level on a monthly basis using clinical rule-based software. The software evaluates all the medical, pharmacy, and lab data to first identify whether or not a patient has a condition. It then identifies if there is a potential gap in care.
� Monthly Closed Case Referral Report: This is a summary of all Aligned CAC Participants in which a case management case was closed during the past month.
• Daily Report: The daily report is a combined report that includes the inpatient daily census and case management referral report. It provides real time hospital admission information on Aligned CAC Participants to facilitate transition of care activities. It includes all reported admissions, at all types of inpatient facilities and provides discharge dates contingent on Cigna obtaining that information. The case management portion of the report provides the information on all Aligned CAC Participants referred into a case management program in the prior 24 hours.
Participant Communications
Cigna expects the Provider to issue the following communications to Aligned CAC Participants:
• Initial communication with Aligned CAC Participants describing the CAC Program, data that will be exchanged and that Provider will reach out to them periodically regarding the CAC Program and its services, and periodic communications to Aligned CAC Participants.
• The availability of comprehensive, coordinated care with the Provider every six months or as otherwise mutually agreed to.
• Furthermore, Provider will communicate information regarding availability of their services at the time of each visit.
• Provider will encourage Aligned CAC Participants to enroll in Cigna disease management and other programs where there is a likely benefit to the Aligned CAC Participant.
• Provider will implement annual patient satisfaction surveys and share results with Cigna. If patient satisfaction results deteriorate, Provider will develop and share improvement plans with Cigna.
Performance Reports
Cigna may provide the following reports on a quarterly basis:
• Advanced Imaging Summary • Alignment Summary • Episode Treatment Group Cost Summary • Inpatient Facility Summary • Out of Network Activities Summary • Outpatient Emergency Department/Urgent Care
Performance • Pharmacy Utilization • Provider Drilldown Report • Quality Provider Drilldown Report • Quality Summary • Specialty Care Utilization Cost Summary • Total Medical Cost Summary • Trend Summary The types of reports may change from time to time and Cigna will provide notice of any material changes to Provider. For additional information on the purpose and specifications of these reports, please contact your Cigna contracting representatives.
Quality Multiplier
Definitions
Aligned National Participant(s) means a Participant(s) who resides in the United States and its territories that is aligned to a primary care physician using the same alignment process outlined in the section entitled "Assignment of Aligned CAC Participants". Aligned Pharmacy Participant(s) means an Aligned CAC Participant(s) who has Prescription Drug Benefits under a Cigna insured or administered Benefit Plan at any time during the Measurement Period.
Generic Drug means each single source or multisource drug or supply generally accepted as therapeutically equivalent and/or interchangeable with drugs having identical amount of the same active ingredient and as further defined by the Aligned Pharmacy Participant's Benefit Plan. Market EBM Rules Performance means the result of the sum of the successes divided by the number of opportunities incurred during that Measurement Period for every Market Aligned Participant as identified and calculated by Evidence-based medicine Connect using claims that were submitted and paid within or sixty (60) days after the Measurement Period, For purposes, of determining Market Performance, the Provider's opportunities and successes are excluded.
83

Market Pharmacy Participant(s) means Aligned Market Participant(s) who have Prescription Drug Benefits under a Cigna insured or administered Benefit Plan. Market Pharmacy Performance means the result when 1) for each therapeutic class, the number of days supply during the Measurement Period for which Generic Drug claims were submitted and paid within or sixty (60) days after the Measurement Period for Market Pharmacy Participants divided by the number of days supply during the Measurement Period for all prescription drugs for which claims were submitted and paid within or sixty (60) days after the Measurement Period for Market Pharmacy Participants (Therapeutic Class generic dispensing rate GDR) and 2) the Therapeutic Class GDR is then multiplied by Provider's Weight for each class and summed across all therapeutic classes. The Provider's Weight is determined by number of days supply for which claims were submitted for each therapeutic class divided by total number of days supply for which claims were submitted for all the therapeutic classes. For purposes of determining Market Pharmacy Performance, the Provider's experience is excluded. National EBM Rules Performance means the result of the sum of the successes divided by the number of opportunities incurred during a Measurement Period for every Aligned National Participant as identified and calculated by EBM Connect using claims that were submitted and paid within or sixty (60) days after the Measurement Period. National Pharmacy Participant(s) means Aligned National Participant(s) who have Prescription Drug Benefits under Cigna insured or administered Benefit Plan. National Pharmacy Performance means the result when 1) for each therapeutic class, the number of days supply during the Measurement Period for which Generic Drug claims were submitted and paid within or sixty (60) days after the Measurement Period for National Pharmacy Participants divided by the number of days supply during the Measurement Period all prescription drugs for which claims were submitted and paid within or sixty (60) days after the Measurement Period for National Pharmacy Participant (Therapeutic Class GDR) and 2) the Therapeutic Class GDR is then multiplied by Provider's Weight for each class and summed across all therapeutic classes. The Provider's Weight is determined by number of days supply for which claims were submitted for each therapeutic class divided by total number of days supply for which claims were submitted for all the therapeutic classes.
Quality Multiplier is determined by the Provider's performance relative to the 15 EBM Rules, the Generic Dispensing Rate, and Patient Experience Questions, collectively referred to as "Program Rules." Success Rate means the number of times a Provider successfully complied with an EBM Rule divided by the number of opportunities to comply expressed as a percentage.
Program Rules
• EBM Rules: EBM Rules are derived from rules endorsed by the National Quality Forum (NQF), Ambulatory Care Quality Alliance (AQA), Healthcare Effectiveness Data Information Set (HEDIS), or developed by physician organizations. The EBM Rules that will be used in this evaluation are listed in Exhibit A. The opportunities and successes for each EBM Rule are identified using the Optumlnsight (EBM Connect) version that is in use by Cigna at the end of a given Measurement Period, and the parties agree to abide by such calculations.
Each opportunity and success will be attributed solely to the Represented Provider to which the Aligned CAC Participant is aligned and then included in the Providers results for the CAC program in which the Representative Provider participates.
• Generic Dispensing Rate or GDR. Generic Dispensing Rate or GDR is the number of days supply during the Measurement Period for which Generic Drug claims were submitted and paid within or sixty (60) days after the Measurement Period for CAC Pharmacy Participants divided by the number of days supply during the Measurement Period using claims that were submitted and paid within or sixty (60) days after the Measurement Period for all prescription drugs for CAC Pharmacy Participants.
• Patient Experience. Each Provider will be asked to respond to the following Patient Experience Questions:
� Do you measure Patient Experience with at least seventy percent (70%) of physicians?
� Have you identified three areas of opportunity for improvement of the Patient Experience?
� Do you have action plan for improvement in the three Patient Experience areas identified in the above question reflected in your Key Focus Action Plan?
Assessment Process
• Earned Points
� EBM: For each Measurement Period, Provider will earn a maximum of one point for each Program Rule for which the Provider has at least twenty (20) opportunities during the Measurement Period and
84

85

86

87

Clinical Integration Acknowledgement
88

Clinical Integration Acknowledgement
CHARTER OF
CIN CLINICAL QUALITY SUBCOMMITTEE
A SUBCOMMITTEE OF THE UM/QM CREDENTIALING COMMITTEE, A COMMITTEE OF THE BOARD OF
DIRECTORS OF RENAISSANCE PHYSICIAN ORGANIZATION, INC. (“RPO”)
Purpose and Authority The Subcommittee shall recommend to the RPO UM/QM Credentialing Committee and the RPO CIN Program Committee processes, pathways, and bundles of care and services to ensure:
• Clinical integration across entire continuum of care • Superior quality/Patient safety • Appropriate Utilization of Resources • Improved patient outcomes
The Subcommittee shall oversee progress of the CIN Program as a whole and individual achievement of clinical quality standards and metrics:
• Performance metrics associated with these standards • Compliance with these standards • Continuous Improvement
Overall Role and Responsibilities The Subcommittee shall:
• Evaluate and modify practice patterns of CIN Participants to allow each CIN Participant to assign
and implement interventions for their population’s consumers with high priority clinical
conditions based on clinical or evidence-based practice guidelines.
• Review, recommend, develop and use patient-centered care strategies to implement evidence-
based guidelines, clinical processes and capabilities to identify the health needs of individuals
served within the contracted population.
• Review individual CIN Participant performance and rates of adoption of modified practice
patterns compared to desired performance.
• Work collaboratively with CIN Program Oversight Subcommittee to develop, monitor and
implement corrective action plans and process improvement initiatives.
• Develop policies to evaluate practice patterns, allowing each CIN Participant to assign and
implement interventions for their population’s consumers with high priority clinical conditions
that are based on clinical or evidence-based best practice guidelines.
• Establish and oversee Work Groups for management of specific diseases through the use of a
unified clinical information system and common protocols.
Meeting Frequency and Length • Quarterly or upon request of the Subcommittee Chairman, the UM/QM
Credentialing Committee, the CIN Program Committee, or the Board of Directors.
Membership, Size, and Term • The Subcommittee shall be composed of __ or more members appointed by the
UM/QM Credentialing Committee, each of whom is a participant in the CIN Program
89

Clinical Integration Acknowledgement
and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The UM/QM Credentialing Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the UM/QM Credentialing Committee and approved by the Board of Directors.
Work Groups
• The Subcommittee may establish work groups comprised of its members or CIN Participants who are not members of the Subcommittee to address designated issues related to clinical quality and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
• The Chairman of the Subcommittee shall be designated by the UM/QM Credentialing Committee and approved by the Board of Directors.
• Any member of the UM/QM Credentialing Committee, the CIN Program Committee, and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee will prepare an annual assessment of performance metrics and provide such report to the UM/QM Credentialing Committee and the CIN Program Committee. This report is to include an assessment of current performance metrics and recommendations of actions and/or changes needed to improve the provision of clinically integrated care to consumers based on identified opportunities.
• The Subcommittee shall make regular reports to the UM/QM Credentialing Committee and the CIN Program Committee, including, a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on the state of the CIN Program’s attainment of clinical quality metrics and such other matters as the UM/QM Credentialing Committee, the CIN Program Committee, or Board of Directors may request from time to time.
Evaluations
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
90

Clinical Integration Acknowledgement
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
91

Clinical Integration Acknowledgement
CHARTER OF
CIN FINANCE SUBCOMMITTEE
A SUBCOMMITTEE OF THE FINANCE COMMITTEE, A COMMITTEE OF THE
BOARD OF DIRECTORS OF RENAISSANCE PHYSICIAN ORGANIZATION, INC.
Purpose and Authority The Subcommittee will monitor, evaluate and seek processes to improve the financial performance and financial reporting of the CIN Program and will make recommendations to the RPO Finance Committee and RPO CIN Program Committee on financial matters relative to the CIN Program. Overall Role and Responsibilities
The Subcommittee shall assist the RPO Finance Committee in its responsibilities for overseeing and recommending CIN Program policies and processes related to:
• Development of financial integration programs for the purpose of improved clinical outcomes and health care cost mitigation designed to offer applicable incentives and/or disincentives for compliance with clinical guidelines and integration systems and processes, directly aligned with the CIN Program’s goals, and tracked and reported to Participants participating in the financial integration programs.
• Overall financial performance of the CIN Program. • Auditing, accounting, financial reporting processes, including the review and
recommendation of the annual budget for the CIN Program to the Finance Committee.
• Incentive reward distributions to CIN Participants. • Remaining updated and informed regarding current and emerging methods of
reimbursement for health care services in the community and nationally. • Review financial assumptions accompanying disease management and population
management as it pertains to contracting, in coordination with other CIN Program subcommittees.
• Perform such other functions and exercise such other powers as may be delegated to it from time to time by the Finance Committee.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the Finance Committee, or the Board of Directors
Membership, Size, and Term
• The Subcommittee shall be composed of __ or more members appointed by the Finance Committee, each of whom is (i) a participant in the CIN Program, (ii) a key physician or board member at the POD level, and (iii) and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
92

Clinical Integration Acknowledgement
• The Finance Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the Finance Committee and approved by the Board of Directors.
Work Groups • The Subcommittee may establish work groups comprised of its members or CIN
Participants who are not members of the Subcommittee to address designated issues related to financial aspects of the CIN Program and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
• The Chairman of the Subcommittee shall be designated by the Finance Committee and approved by the Board of Directors.
• Any member of the Finance Committee and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the Finance Committee and the CIN Program Committee with respect to the Finance Committee's discharge of its responsibilities
• and with respect to such recommendations such Committees may deem appropriate, including, a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the
Subcommittee on the state of the CIN Program’s attainment of financial goals, including
financial integration programs, and such other matters as the Finance Committee, the CIN
Program Committee, or Board of Directors may request from time to time.
Evaluations
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
• Review legal and regulatory matters that may have a material effect on financial performance of the CIN Program.
93

Clinical Integration Acknowledgement
CHARTER OF
CIN MEMBERSHIP SUBCOMMITTEE
A SUBCOMMITTEE OF THE CIN PROGRAM COMMITTEE, A COMMITTEE OF THE BOARD OF DIRECTORS
OF RENAISSANCE PHYSICIAN ORGANIZATION, INC. (“RPO”)
PurposeandAuthority The Subcommittee shall oversee, evaluate changes need and make recommendations to the
RPO CIN Program Committee regarding:
• The standards of participation for physicians who wish to join the CIN Program.
• Determining the size and composition of the network needed to serve the population served by
CIN Program.
• Ensure that current credentialing documents are maintained.
• Continually review, with RPO’s counsel, any legal matter that could have a significant
impact on CIN Program’s relationships with CIN Participants or potential
participants.
• Report to the CIN Program Committee on a regular basis regarding network needs.
OverallRoleandResponsibilities
The Subcommittee shall assist the CIN Program Committee in its responsibilities for
developing and recommending policies and processes to the Board of Directors related to
membership and in overseeing the following activities:
• Review applications and credentials for compliance with the CIN selection and participation
criteria and recommend participants as appropriate for approval by the CIN Program
Committee. [or will RPO Board be the ultimate decision-maker to approve CIN Participants?]
• Evaluate on an ongoing basis and make recommendations to the CIN Program Committee
regarding the CIN Program Selection Criteria and the CIN Program Membership Criteria, taking
into consideration the quality, safety, care coordination, patient satisfaction, access, and cost
effectiveness and efficiency standards for participation in the CIN Program.
• Maintaining relationships between CIN Program participating physicians (“CIN Participants”),
facilities and RPO and working to resolve concerns, complaints, and questions about
participation status.
• Identifying and resolving conflicts of interest of applicants and CIN Participants.
• Overseeing credentialing of CIN Participants.
• Establishing and overseeing Work Groups related to membership issues.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the CIN Program Committee, or the Board of Directors
94

Clinical Integration Acknowledgement
Membership, Size, and Term • The Subcommittee shall be composed of __ or more members appointed by the CIN
Program Committee, each of whom is a participant in the CIN Program and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The CIN Program Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the CIN Program Committee and approved by the Board of Directors.
Work Groups
• The Subcommittee may establish work groups comprised of its members or CIN Participants who are not members of the Subcommittee to address designated issues related to membership and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
• The Chairman of the Subcommittee shall be designated by the CIN Program Committee and approved by the Board of Directors.
• Any member of the CIN Program Committee and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the CIN Program Committee, including a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on the state of the CIN Program’s network and such other matters as the CIN Program Committee or Board of Directors may request from time to time.
Evaluations and Review
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
• Review legal and regulatory matters that may have a material effect on membership of the CIN Program.
95

Clinical Integration Acknowledgement
CHARTER OF
CIN COMMUNICATION AND EDUCATION SUBCOMMITTEE
A SUBCOMMITTEE OF THE CIN PROGRAM COMMITTEE, A COMMITTEE OF THE BOARD OF DIRECTORS
OF RENAISSANCE PHYSICIAN ORGANIZATION, INC. (“RPO”)
PurposeandAuthority The Subcommittee shall oversee and make recommendations to the RPO CIN Program
Committee regarding:
• Methods and processes to disseminate and educate CIN Participants on clinical protocols,
performance measures, and CIN Program goals and objectives.
• Patient education and engagement strategies and tools.
OverallRoleandResponsibilities
The Subcommittee shall assist the CIN Program Committee in its responsibilities for
developing and recommending policies and processes to the Board of Directors related to
education and communication with regard to the following activities:
• Develop, support and disseminate implementation and education of clinical protocols and
performance measures.
• Monitor, oversee and develop processes, policies and programs to facilitate communication,
cooperation and care coordination among Participants.
• Develop patient education and engagement strategies and tools.
• Work collaboratively with CIN Clinical Quality Subcommittee to identify CIN Program
communication needs and educational opportunities.
• Report to the CIN Program Committee on a regular basis regarding communication and
education objectives.
• Establish and oversee Work Groups related to CIN Program communication and education
issues.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the CIN Program Committee, or the Board of Directors
Membership, Size, and Term • The Subcommittee shall be composed of __ or more members appointed by the CIN
Program Committee, each of whom is a participant in the CIN Program and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The CIN Program Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the CIN Program Committee and approved by the Board of Directors.
96

Clinical Integration Acknowledgement
Work Groups • The Subcommittee may establish work groups comprised of its members or CIN
Participants who are not members of the Subcommittee to address designated issues related to communication and education and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
• The Chairman of the Subcommittee shall be designated by the CIN Program Committee and approved by the Board of Directors.
• Any member of the CIN Program Committee and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the CIN Program Committee, including, a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on the state of the CIN Program’s network and such other matters as the CIN Program Committee or Board of Directors may request from time to time.
Evaluations and Review
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
CHARTER OF
CIN IT INFRASTRUCTURE SUBCOMMITTEE
A SUBCOMMITTEE OF THE CIN PROGRAM COMMITTEE, A COMMITTEE OF THE BOARD OF DIRECTORS
OF RENAISSANCE PHYSICIAN ORGANIZATION, INC. (“RPO”)
PurposeandAuthority The Subcommittee shall oversee and make recommendations to the RPO CIN Program
Committee regarding:
• IT infrastructure needs of the CIN Program.
19199543v.1
97

Clinical Integration Acknowledgement
• Interfaces and platform processes needed to enhance the CIN Program, foster collaboration and
coordination of patient care, and streamline and promote tracking and reporting of CIN Program
measures and metrics.
OverallRoleandResponsibilities
The Subcommittee shall assist the CIN Program Committee in its responsibilities for
developing and recommending policies and processes to the Board of Directors related to
IT infrastructure needed to support and enhance the CIN Program, including:
• Evaluate, develop and identify IT-dependent performance improvement platform and interface
with data-based mechanisms and processes to monitor and track utilization, report on quality
measures, coordinate patient care (especially for high-cost, high-risk patients) and efficiency of
resource use to demonstrate value
• Report to the CIN Program Committee on a regular basis regarding IT infrastructure needs and
objectives.
• Establish and oversee Work Groups related to CIN Program IT infrastructure issues.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the CIN Program Committee, or the Board of Directors
Membership, Size, and Term • The Subcommittee shall be composed of __ or more members appointed by the CIN
Program Committee, each of whom is a participant in the CIN Program and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The CIN Program Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the CIN Program Committee and approved by the Board of Directors.
Work Groups
• The Subcommittee may establish work groups comprised of its members or CIN Participants who are not members of the Subcommittee to address designated issues related to IT infrastructure and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
• The Chairman of the Subcommittee shall be designated by the CIN Program Committee and approved by the Board of Directors.
• Any member of the CIN Program Committee and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any
98

Clinical Integration Acknowledgement
representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the CIN Program Committee, including a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on the state of the CIN Program’s network and such other matters as the CIN Program Committee or Board of Directors may request from time to time.
Evaluations and Review
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
19199653v.1
99

Clinical Integration Acknowledgement
CHARTER OF
CIN CONTRACTING SUBCOMMITTEE
A SUBCOMMITTEE OF THE CONTRACTING COMMITTEE, A COMMITTEE OF THE
BOARD OF DIRECTORS OF RENAISSANCE PHYSICIAN ORGANIZATION, INC.
Purpose and Authority
The Subcommittee will review, evaluate and make recommendations to the RPO Contracting Committee and RPO CIN Program Committee concerning contracting matters related to the CIN Program. Overall Role and Responsibilities
The Subcommittee shall assist the RPO Contracting Committee in its responsibilities related to:
• Evaluating, negotiating and monitoring contracts related to the CIN Program. • Working collaboratively with the CIN Program Committee, CIN Clinical Quality
Committee and CIN Finance Committee in assessing contract needs and terms, including communication of current financial integration methods and programs for documentation in contracts.
• Performing such other functions and exercise such other powers as may be delegated to it from time to time by the Contracting Committee.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the Contracting Committee, the CIN Program Committee, or the Board of Directors
Membership, Size, and Term
• The Subcommittee shall be composed of __ or more members appointed by the Contracting Committee, each of whom is a participant in the CIN Program and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The Contracting Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the CIN Contracting Committee and approved by the Board of Directors.
Work Groups • The Subcommittee may establish work groups comprised of its members or CIN
Participants who are not members of the Subcommittee to address designated issues related to CIN Program contracting and to report findings to the Subcommittee, as assigned.
Leadership and Meeting Attendance
100

Clinical Integration Acknowledgement
• The Chairman of the Subcommittee shall be designated by the Contracting Committee and approved by the Board of Directors.
• Any member of the Contracting Committee, the CIN Program Committee, and any director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the Contracting Committee and the CIN Program Committee, including, a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on matters addressing contracting issues and such other matters as the Contracting Committee, the CIN Program Committee, or the Board of Directors may request from time to time.
Evaluations
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
• Review legal and regulatory matters that may have a material effect on contracting issues related to the CIN Program.
101

Clinical Integration Acknowledgement
CHARTER OF
CIN OVERSIGHT SUBCOMMITTEE
A SUBCOMMITTEE OF THE OVERSIGHT COMMITTEE, A COMMITTEE OF THE BOARD OF DIRECTORS OF
RENAISSANCE PHYSICIAN ORGANIZATION, INC. (“RPO”)
PurposeandAuthority The Subcommittee will monitor, evaluate and make recommendations to the RPO Oversight
Committee and RPO CIN Program Committee regarding CIN Program performance and
performance of CIN Participants to meet established goals of the CIN Program.
OverallRoleandResponsibilities
The Subcommittee shall assist the Oversight Committee in its responsibilities to:
• Monitor, evaluate and provide oversight of CIN Program.
• Work collaboratively with CIN Subcommittees and the CIN Program Committee to assess overall
CIN Program performance and performance of individual Participants and to develop and
recommend changes to CIN Program elements to enhance performance.
• Monitor and evaluate the clinical performance, quality, and cost efficiency of CIN Participants
and provide support, counsel, and accountability for those CIN Participants whose clinical
outcomes do not meet CIN Program standards.
Meeting Frequency and Length
• Quarterly or upon request of the Subcommittee Chairman, the Oversight Committee, the CIN Program Committee, or the Board of Directors.
Membership, Size, and Term • The Subcommittee shall be composed of __ or more members appointed by the
Oversight Committee, each of whom is a participant in the CIN Program and free from any relationship that, in the opinion of the Board of Directors, would interfere with the exercise of his or her independent judgment as a member of the Subcommittee.
• The Oversight Committee may adjust the Subcommittee’s size and composition from time-to-time.
• The term of the Subcommittee members shall be annual, unless otherwise recommended by the Oversight Committee and approved by the Board of Directors.
Work Groups
• The Subcommittee may establish work groups comprised of its members or CIN Participants who are not members of the Subcommittee to address designated issues related to oversight of the CIN Program and to report findings to the Subcommittee, as assigned.
102

Clinical Integration Acknowledgement
Leadership and Meeting Attendance • The Chairman of the Subcommittee shall be designated by the Oversight Committee
and approved by the Board of Directors. • Any member of the Oversight Committee, the CIN Program Committee, and any
director of RPO who is not a member of the Subcommittee may attend meetings of the Subcommittee; provided, however, that such individuals may not vote on any matter coming before the Subcommittee for a vote. The Subcommittee also may invite to its meetings any representative of CareAllies and such other persons as it deems appropriate in order to carry out its responsibilities.
Reports
• The Subcommittee shall make regular reports to the Oversight Committee and the CIN Program Committee, including a description of important issues that have developed since the last report and responses thereto.
• In addition to regular reports, an annual plan and report shall be developed by the Subcommittee on matters addressing oversight activities and such other matters as the Oversight Committee, the CIN Program Committee, or the Board of Directors may request from time to time.
• At least annually, implement systematic data collection, analysis and reporting to the CIN Program Committee of measures related to established goals of the CIN Program, including: (a) appropriate utilization of health items and services, (b) outcome measures related to accepted clinical practice and/or evidence-based guidelines, quality standards and case management/care coordination programs and (c) financial measures of service delivery efficiencies and associated costs of care.
Evaluations and Review
• The Subcommittee shall periodically review and, if necessary, propose updates to the Subcommittee's charter and the CIN Program Performance Improvement Policy.
• The Subcommittee will perform an evaluation of its performance at least annually to ensure that the Subcommittee is functioning effectively.
• The Subcommittee shall regularly review policies and procedures applicable to its responsibilities.
What is a Clinically Integrated Network (CIN)
• The Department of Justice and the Federal Trade Commission define clinical integration as an active and ongoing program to evaluate and modify practice patterns by CIN participants to create a high degree of interdependence and cooperation among physicians to control costs and ensure quality patient care. While there are many factors the FTC considers in evaluating whether a program or organization is clinically integrated, the following are necessary:
103

Clinical Integration Acknowledgement
• Establishes mechanisms to monitor and control utilization of healthcare services that are designed to control costs and ensure quality of care.
• Selectively chooses CIN physicians who are likely to further these efficiency objectives.
• Utilizes investment of significant capital, both monetary and human, in the necessary infrastructure and capability to realize the claimed efficiencies.
Why Join the RPO CIN
• Allows practice independence while taking advantage of the scale of the RPO organization for shared CIN population health platform and allows for contracting FFS agreements
• Being part of a larger network of high performing providers improves leverage, minimizes participation costs, and allows for data to be managed centrally; which can help with CMS reporting, commercial payer pay-for-performance compliance, and patient tracking and management
• It is expensive to manage to metric-driven contracts, so utilizing CIN data mining across EHRs from multiple vendors helps to reduce that burden substantially.
• Access to complete patient information from all the CIN Providers • Ability to monitor patient compliance • Ability to sell combined services of network to payors, making independent practice
more viable, especially for small practices Additional Details
• IT platform required for care coordination for CIN between PCPs and Specialists. • CIN formation will allow participating physicians to negotiate enhanced FFS rates with
payers. • CIN will have to meet quality and medical cost metrics for payers to maintain increased
rates for physicians. • Each group executes a contract but every individual provider in the group must sign the
joinder agreement (Exhibit D). • Every individual provider must pay $250 annual CIN Fee.
o This is a DOJ/FTC expectation that CIN members must invest time and capital to prove engagement and active participation.
• PCP and Specialist criteria are listed in the contract Exhibit A but can be changed at the sole discretion of the CIN Committee at any time.
• Each group will need to sign a BAA Exhibit E for access to EMR/Medical records for CIN membership.
• CIN Providers will be required to accept all future CIN lines of business; however the CIN has the latitude to change this requirement for a particular plan if there is a compelling reason to do so.
• Does this CIN agreement affect my current RPO contract or any current lines of business on my RPO contract? NO, this is separate agreement that will have separate lines of business but is still part of RPO entity.
• Do all providers in a group have to participate? YES • Can Providers be in multiple CINs?
• Technically yes PCP can be with another CIN but RPO CIN will require participation with all lines of business (i.e. Cigna PPO, Blue PPO – potential
104

Clinical Integration Acknowledgement
contracts for CIN next year) however the CIN has the latitude to change this requirement for a particular plan if there is a compelling reason to do so.
• Specialists can participate in multiple CINs; membership is not aligned thru specialists.
• Is the CIN only for commercial LOBs? CIN contracts will most likely be Commercial PPO plans but could be Medicare PPO as well, etc. dependent upon payer.
• If PCP or Specialist meets criteria for CIN the provider can be extend a contract to participate throughout the year. However effective date with actual CIN plans could vary depending on plan, some plans may only update alignment quarterly.
• Provider term process will be the same for CIN contract as it is for the RPO contract, appeal panel, etc.
• Provider CIN contract states 120 days’ notice if provider intends to terminate their contract (6.2).
105

Clinical Integration Acknowledgement
RPO CIN PROGRAM
Participant AGREEMENT
This RPO CIN PROGRAM PARTICIPANT AGREEMENT (“Agreement”) is by and between RENAISSANCE PHYSICIAN ORGANIZATION, INC., a not-for-profit corporation organized under the laws of the State of Texas (“RPO”), and ___________________________, a Texas ___________________ (“Participant”) with the tax identification number (“TIN”) listed on the signature page hereto.
WHEREAS, RPO is engaged in the development and implementation of an active and ongoing program to evaluate and modify the practice patterns of a selective group of participating physicians who have demonstrated the capability of achieving a high degree of interdependence and cooperation to control costs and ensure quality (the “CIN
Program”); WHEREAS, pursuant to such CIN Program, RPO is organized to negotiate and enter into
fee-for-service contracts and participate in payment program initiatives developed by Payers, and will coordinate and enter into, on a non-exclusive basis, Program Agreements on behalf of its CIN Program participating physicians pursuant to which RPO, Participant and CIN Members may agree to work together on CIN Activities to achieve clinical efficiencies (“Program Agreement”); and
WHEREAS, on behalf of itself and its Related Providers, Participant desires to be an active participant in the CIN Program.
NOW, THEREFORE, in consideration of the covenants and promises herein, Participant and RPO agree as follows:
ARTICLE I
DEFINITIONS
For the purpose of this Agreement, the following terms will have the meanings specified below.
1.1 “Applicable Law” means all applicable federal, state and local law, including all applicable statutes, codes, regulations, ordinances and rules, including all applicable case law, administrative decisions, and agency guidelines
1.2 “CIN Activities” means the active and ongoing program of health care quality and efficiency initiatives developed and implemented by RPO to evaluate and modify practice patterns by Participants and Payers and to create a high degree of interdependence and cooperation among them to control costs and ensure quality.
1.3 “CIN Member” means Participant and each other “Participant” that has executed a CIN Participant Agreement with RPO.
1.4 “CIN Policy” means each and every standard, policy, procedure, protocol, practice, plan, process and/or guideline governing the CIN Program and CIN Activities, as approved by RPO, and made available to Participant. Unless specifically provided otherwise by RPO with respect to a specific Policy, each Policy or amendment to a previously approved Policy will become effective upon delivery by RPO to Participant (individually for an individual and to the designated representative for an entity) and shall remain in effect until RPO takes action to revise or rescind the Policy.
106

Clinical Integration Acknowledgement
1.5 “Incentive Award” means an amount to be paid to RPO by a Payer under a Program Agreement, which will be used, distributed and/or paid in accordance with the applicable Incentive Award Methodology for the achievement of Payer initiatives or the achievement of designated Performance Standards.
1.6 “Incentive Award Methodology” means the definition set forth in Section 4.4.
1.7 “Participant” means the party to this Agreement
1.8 “Payer” means a third party payer of health care services that has entered into a Program Agreement with RPO, including employers, union groups, managed care plans, insurers, HMOs, PPOs, federal, state, or government payer, applicable Medicaid program or third party administrators contracting on behalf of any such entities.
1.9 “Payer Agreement” means a contract between a Payer and a Participant that sets forth the health care benefits a covered person is entitled to receive and the terms and conditions upon which the Payer will pay the Participant for the provision of covered health care services.
1.10 “Payer Regulations” means the policies and procedures developed by a Payer and applicable to the CIN Program and CIN Members under a Payer Agreement.
1.11 “Performance Standards” means criteria or metrics for measuring clinical quality, patient satisfaction, resource utilization, and cost effectiveness with regard to the delivery of covered health care services, as set forth in an applicable Program Agreement, or as set forth in CIN Policy.
1.12 “Program” means a payment program developed by Payers which may contain incentives for meeting certain initiatives and/or Performance Standards as detailed in a Program Agreement entered into between RPO and Payer.
1.13 “Related Provider” means each licensed person or entity who bills for services under the TIN of a Participant and who has executed a Joinder Agreement in the form attached hereto as Exhibit D to this Agreement and such person or entity has been approved by RPO for participation, as evidenced by RPO executing the Joinder Agreement submitted by such person or entity. Each and every reference to “Participant” in this Agreement shall pertain to each Provider who has entered into a Joinder Agreement that has been executed by both parties.
ARTICLE II
PARTICIPATION IN CIN PROGRAM
2.1 CIN Participation. By executing this Agreement, Participant understands that Participant and Related Providers, if applicable, have been selected to participate in the CIN Program based upon meeting the CIN Program Selection Criteria, the current version which is attached hereto as Exhibit A, and which shall be a continuing obligation of Participant and Related Providers to maintain, as it may be amended by RPO from time to time. Participant and its Related Providers further agree to participate in the CIN Program on the terms and conditions contained in this Agreement, to actively participate in CIN Activities, including, but not limited
107

Clinical Integration Acknowledgement
to service on CIN Program committees and working groups, as needed, education, and CIN Program initiatives, and to uphold throughout the Term the CIN Program Membership Criteria, the current version which is attached hereto as Exhibit B, and which shall be a continuing obligation of Participant ad Related Providers to maintain, as it may be amended by RPO from time to time in its sole discretion.
2.2 Participation Fees. Upon execution of this Agreement, Participant shall remit to RPO those Participation Fees specified in Exhibit C. Such Participation Fees may be modified from time to time, as approved by RPO.
2.3 Contracting. Following RPO approval, Participant agrees to participate in designated Program Agreements effective as of the later of: the date of this Agreement, the date defined in the applicable Program Agreement, or the date approved by RPO. Participant hereby designates RPO to act as its agent in negotiations with Payers for contracts that obligate Participant to provide medical services to individuals who are beneficiaries under the health benefit plans of such Payers. It is the intent of the parties that the ability of RPO to negotiate prices on behalf of the CIN Members is subordinate and reasonably necessary for clinical efficiencies.
2.4 Standards. By executing this Agreement, Participant agrees to perform CIN Activities and to be bound by and comply with this Agreement, CIN Policy, the applicable Payer Agreements and related Payer Regulations, and Performance Standards, as applicable to such Participant and Related Provider, all of which shall be provided to Participant.
2.5 Non-exclusivity. Except as otherwise expressly provided herein, this Agreement is non-exclusive. Participant is free to contract directly or through another clinically integrated network with any payer that has not contracted with RPO, unless otherwise prohibited under one or more Program Agreements.
2.6 Covenants of Participants That are Entities. Participant, on behalf of itself and its Related Providers, as their duly authorized agent, accepts the duties of a CIN Member as set forth herein. Each and every Related Provider individually assumes and accepts the same duties as Participant and their participation hereunder is not effective until their execution of the Joinder Agreement attached as Exhibit D.
A. Participant shall deliver written notice to RPO of termination of any Related Provider’s relationship with Participant within thirty (30) days of the effective date of such termination.
B. Participant shall deliver to RPO as soon as possible an executed Joinder Agreement for any Related Provider who desires to become a Related Provider subsequent to the Effective Date, which Joinder Agreement will become effective only upon the execution by RPO.
2.7 Remedial Action. If the performance of Participant is determined by RPO to fall below the level of performance required by a CIN Policy, the CIN Membership Criteria or a
108

Clinical Integration Acknowledgement
particular Program, RPO shall notify Participant (and the affected Related Provider) of such noncompliance, and Participant or Related Provider, as applicable, shall be placed in a performance improvement plan consistent with the CIN Performance Improvement Policy. In the event Participant’s (or Related Provider’s, as applicable) performance does not sufficiently improve in accordance with the terms of the Performance Improvement Policy, RPO shall have the right to terminate Participant or the affected Related Provider from participation under the particular Program and/or the CIN Program in accordance with Section 6.4).
2.8 Provision of Services. Participant agrees only to provide health care services under the CIN Program that Participant is licensed and credentialed to provide in compliance with this Agreement and any applicable Payer Agreement. Participant agrees not to discriminate in the provision of health care services based on any legally protected status, marital status, health status, or income.
2.9 Provider/Patient Relationships. Participant shall retain sole responsibility for medical decision-making with regard to a specific patient. Nothing in this Agreement nor any policy shall be interpreted to supplant, interfere with, or impose restrictions on the traditional physician-patient relationship. No policy shall substitute for or take precedence over any Participant’s duty to render care within the standard of care and all applicable legal duties and regulatory requirements. Participant is solely responsible to each patient for all aspects of health care and treatment within the scope of Participant’s competence and license, including the quality and levels of such care and treatment.
2.10 Use of Name. During the Term, RPO shall have the right to utilize the name, trademarks, logos and symbols identifying Participant and Related Providers, consistent with and in furtherance of the CIN Program.
ARTICLE III
RECORDS, DATA AND CONFIDENTIALITY
3.1 Records. Participant shall maintain medical and other records, and collect data and information relating to services furnished in connection with the CIN Program in accordance with applicable state and federal laws and applicable CIN Policy. Except as limited by a Program Agreement, Participant agrees to provide RPO access, without charge, to all medical, claims and other data and information deemed necessary and appropriate for management of individual or population health management purposes to allow RPO to perform CIN Activities and meet applicable Performance Standards.
3.2 EHR Interoperability. Participant agrees to allow RPO access to its EMR, subject to compliance with applicable HIPAA and privacy restrictions.
3.3 Data Submission. During the Term, if required by an applicable Program, Participant agrees to prepare and submit electronically claims information, data, and/or reports about clinical encounters and such other information necessary to process and/or to verify such claims and all other data and information, including quality data, required by applicable CIN Policy and Programs.
109

Clinical Integration Acknowledgement
3.4 Access to Records and Documentation. Program Agreements may require Participants to submit to an audit to evaluate the records, data and other information created or used by the CIN Program, Participants, and other individuals or entities performing CIN Activities that pertain to a Program. Participant agrees to cooperate fully with any such requests.
3.5 Confidential Information. Participant acknowledges that all Confidential Information of the CIN Program, except medical records and any other non-aggregated information belonging to Participant, is the exclusive property of RPO, is confidential and may not be used or disclosed by Participant, except as expressly permitted herein or required by Applicable Law. In the event of a breach of this Section, RPO will be entitled to enjoin Participant from such breach and obtain an equitable remedy prohibiting Participant from disclosing in whole or in part the Confidential Information of RPO and the CIN Program. The term “Confidential Information” includes, without limitation: (a) all budgets, strategic plans, marketing plans, financial information, data, documents, records, and other materials, which contain information relating to the operation of the CIN Program; (b) all methods, techniques, and procedures utilized in providing services to patients not readily available through sources in the public domain; (c) all trademarks, trade names, and service marks of RPO and the CIN Program; (d) all proprietary computer software, programs, data files, and documentation; (e) all work product (including materials developed by Participant) prepared in connection with or resulting from the performance of services under this Agreement; (f) all CIN Policies and the methods and manner by which RPO conducts the CIN Activities; and (g) all non-public information obtained as part of this Agreement.
In the event that Participant is compelled to disclose Confidential Information pursuant to any statute, regulation, order or other form of valid legal process, Participant agrees to provide RPO with prior written notice of such compelled disclosure as soon as practicable after receiving the legal process to permit RPO to seek a protective order. If, following receipt of such written notice from Participant, RPO is unable to obtain or does not seek a protective order, and Participant is legally compelled to disclose the Confidential Information, then such disclosure of such Confidential Information under legal compulsion will be made without liability. Unless otherwise required by law, Participant agrees that, before reporting any actual or perceived violation of law, by CIN or any Participant, or other person with regard to the provision of services under this Agreement, to any governmental entity, Participant will first discuss any potential legal or compliance matter with RPO’s designated compliance officer and, unless otherwise required by law, provide RPO an opportunity to investigate and appropriately report any compliance matter brought to its attention by Participant. This Section will survive the termination of this Agreement for any reason.
3.6 HIPAA. The parties are subject to the provisions of the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) in the performance of CIN Activities, as follows: (i) to the extent that RPO and/or CIN Members perform CIN Activities for Participant, they are conducting health care operations on Participant’s behalf and are therefore a Business Associate of Participant; and (ii) to the extent that Participant performs CIN Activities for other CIN Members, Participant is conducting health care operations on behalf of such CIN Members and is therefore a Business Associate of such CIN Members. Thus, in performing CIN
110

Clinical Integration Acknowledgement
Activities, the parties agree to adhere to the requirements of HIPAA in relation to maintaining the privacy and security of PHI, and Participant agrees to execute and abide by the terms and conditions of the Business Associate Agreement, in the form attached hereto as Exhibit E.
ARTICLE IV
FINANCIAL OBLIGATIONS AND CIN PROGRAM INCENTIVE AWARDS
4.1 Relationship With Payers. During the Term, Participant agrees to maintain in effect a separate Payer Agreement with each Payer with whom RPO has entered into a Program Agreement applicable to Participant. Participant shall immediately notify RPO in the event of suspension or other termination of any such Payer Agreement. Participant understands and acknowledges that RPO or a Payer may restrict or limit the number of Participants participating in a particular Program Agreement.
4.2 Payer Obligations to Pay Claims. Except as expressly agreed in writing by RPO, each Payer has full and final responsibility and liability for payment of claims under an applicable Payer Agreement. RPO is not responsible for, does not guarantee, and does not assume liability for payment of any claim for services rendered under a Payer Agreement, and all final decisions with respect to the payment of claims are the responsibility of the applicable Payer.
4.3 Fee-Related Information. Except as necessary to achieve CIN Activities, under no circumstance may Participant share or disclose fee-related information with other CIN Members, or seek or request fee-related information regarding any other person or entity participating in the CIN Program. RPO will maintain the confidentiality of any fee-related information Participant provides and will not share or disclose specific fee-related information to any CIN Member (except as permitted by Applicable Law or as necessary for reporting purposes). It is understood that this will not limit or restrict RPO from disclosing aggregated data.
4.4 Incentive Awards. RPO may be eligible for Incentive Awards in accordance with the terms of a Program Agreement. RPO will use and/or distribute each Incentive Award in accordance with the applicable methodology adopted by RPO in its sole discretion, by which the CIN Program will use and distribute Incentive Awards received from Payers in connection with each respective Program Agreement (“Incentive Award Methodology”). To the extent RPO receives Incentive Awards and distributes all or a portion of such Incentive Awards to CIN Members, Participant shall only be entitled to receive a distribution for Programs in which Participant has participated during the applicable period.
ARTICLE V
RPO COVENANTS
5.1 Infrastructure. RPO shall assist with the development and maintenance of necessary infrastructure to operate the CIN Program.
111

Clinical Integration Acknowledgement
5.2 Clinical Guidelines and Protocols. RPO will develop and/or adopt and implement patient-centered care strategies to implement evidence-based guidelines, clinical protocols, processes, and capabilities to control costs and ensure quality.
5.3 Business Associate. RPO shall adhere to the terms of the HIPAA Business Associate Agreement attached as Exhibit D.
5.4 Transparency. RPO shall make available for review by Participant: CIN Policy, Program Agreements applicable to Participant, and certain information related to Incentive Awards and the distribution of funds received.
ARTICLE VI
TERM AND TERMINATION
6.1 Term and Renewal. The Initial Term of this Agreement shall commence on ________ 2017 (“Effective Date”) and shall expire on ____________________. Upon expiration of the Initial Term, this Agreement will automatically renew for successive one (1) year Renewal Terms unless otherwise terminate as provided herein. (Initial and Renewal Terms are collectively referred to as the “Term”.)
6.2 Termination of Agreement. Either party may terminate this Agreement for any or no reason, without penalty, upon providing the other with at least one hundred twenty (120) days’ prior written notice. The participation of each Related Provider, if any, will automatically terminate upon the termination of Participant.
6.3 Termination of a Participant/Related Provider from a Program. RPO may terminate the participation of any Participant (if an individual) or any Related Provider (if Participant is an entity) in any Program, for any or no reason, upon providing Participant with at least sixty (60) days’ advance written notice. The participation of any Related Provider will automatically terminate with respect to all Programs upon the termination of their employment or other contractual relationship with Participant.
6.4 Additional Grounds for Termination. RPO may terminate Participant or any Related Provider’s participation in the CIN Program for: (a) failure to meet and maintain the CIN Program Membership Criteria; (b) engaging in conduct inconsistent with or potentially detrimental to the delivery of quality patient care or contrary to the best interests of RPO and/or the CIN Program; or (c) material non-compliance with this Agreement, a Program Agreement or CIN Policy, provided that in lieu of terminating this Agreement RPO may terminate the participation of Participant or any Related Provider in select Programs only. Participant and its Related Provider(s), if applicable, will be provided thirty (30) days’ advance written notice prior to termination under this Section and a thirty (30) day opportunity to cure such non-compliance to the reasonable satisfaction of RPO.
6.5 Immediate Suspension. RPO may immediately suspend Participant or any Related Providers’ participation in any or all Programs pending completion of termination proceedings if RPO has a reasonable basis for concluding that Participant or such Related
112

Clinical Integration Acknowledgement
Provider poses an immediate risk to patient care or poses an undue disruption of CIN Program operations.
6.6 Review of Decision. Any and all decisions of RPO pursuant to this Article 6 are final and will not be subject to review by or appeal to any individual, committee, court, arbitrator, administrative body or other entity, unless otherwise required by Applicable Law or a Program Agreement.
6.7 Termination of Program Agreement. The termination of a given Program Agreement will automatically terminate the participation of Participant and Related Providers in that particular Program. If a Program Agreement between RPO and a Payer is terminated, for any reason, any and all financial benefits, rewards, or incentives available under the terms of such Program Agreement will be used and/or distributed in accordance with the applicable Incentive Award Methodology.
6.8 Effect of Termination. The provisions of this Agreement will be of no further force or effect after its termination but each party will remain liable for obligations or liabilities arising from activities carried on prior to the termination and under provisions which by their terms survive termination of this Agreement. Upon the termination or expiration of this Agreement, Participant shall be required to furnish all data necessary to complete the assessment of the CIN Program’s performance and address other relevant matters, as reasonably directed by RPO.
ARTICLE VII
MISCELLANEOUS
7.1 Amendment. This Agreement may be amended at any time by mutual written consent of the parties. Notwithstanding the foregoing, RPO may amend this Agreement as necessary (a) to comply with Applicable Law or (b) to implement, policies, procedures, or programs adopted by RPO.
7.2 Entire Agreement. This Agreement, together with the addenda attached hereto, constitutes the complete and exclusive statement of agreement among the parties. It supersedes all prior written and oral statements, including any prior representation, statement, condition, or warranty.
7.3 Assignment and Benefit. This Agreement may not be assigned or any duties hereunder delegated, in whole or in part, by Participant, and any such purported assignment of this Agreement or delegation shall be null, void, and of no force of effect. RPO may assign this Agreement or delegate any duties hereunder by giving Participant at least thirty (30) days advance written notice of the same.
7.4 Waiver. No waiver of or failure by either party to enforce any of the terms, conditions, or obligations herein will be construed as a waiver of any subsequent breach of such term, condition, or obligation, or of any other term, condition, or obligation hereunder, whether
113

Clinical Integration Acknowledgement
the same or different in nature. No extension of time for performance of any obligations or acts will be deemed an extension of the time for performance of any other obligations or acts.
7.5 Notices. Except where this Agreement indicates that notice will be furnished in accordance with CIN Policies, any notice required to be given hereunder will be in writing and must be personally delivered or sent by overnight mail to the addresses set forth on the execution page of this Agreement. Such notice will be effective upon delivery. Notice by CIN to Participant will be deemed to constitute notice to each of its Related Providers.
7.6 General Interpretation; Ambiguities. Ambiguities, if any, in this Agreement will be reasonably construed in accordance with all relevant circumstances including, without limitation, prevailing practices in the industry of the parties in the place where the contract is to be performed and will not be construed against either party, irrespective of which party may be deemed to have authored the ambiguous provision.
7.7 Choice of Law; Venue. This Agreement and will be construed and governed by the laws of the State of Texas irrespective of its choice-of-law principles. Venue for any action arising under this Agreement will lie in Harris County or in the federal courts for the Southern District of Texas.
7.8 Partial Invalidity. If any provision of this Agreement is found to be invalid or unenforceable by any court or other lawful forum, such provision will be ineffective only to the extent that it is in contravention of applicable laws without invalidating the remaining provisions of this Agreement, unless such invalidity or unenforceability would defeat an essential business purpose of this Agreement.
7.9 Signatures. Any individual signing this Agreement on behalf of an entity hereby represents and warrants in his/her individual capacity that he/she has full authority to do so on behalf of such entity.
7.10 Survival. Except as otherwise expressly provided in this Agreement, all covenants, agreements, representations, and warranties, expressed or implied, will survive the termination of this Agreement, and will remain in effect and binding upon the parties until they have fulfilled all of their obligations under this Agreement, and the statute of limitations will not commence to run until the time such obligations have been fulfilled.
7.11 Independent Contractors. The parties to this Agreement are independent entities, and neither party, by virtue of this Agreement, assumes any liability for any debts or obligations of a financial or legal nature incurred by the other party.
7.12 Changes in Laws. In the event there are changes to any Applicable Law, or the application thereof, or the interpretation of existing provisions or the adoption of new legislation, any of which would in the reasonable opinion of counsel to either party affect the legality of this Agreement, the parties agree to examine the Agreement and to re-negotiate those provisions which are required to be revised in order to accommodate such changes.
114

Clinical Integration Acknowledgement
[Signature Page Follows]
115

Clinical Integration Acknowledgement
IN WITNESS HEREOF, in consideration of the mutual covenants and promises stated herein and other good and valuable consideration, the undersigned have agreed to be bound by this Agreement.
PARTICIPANT: RPO:
Name: _____________________________ Renaissance Physician Organization, Inc.
Signature: __________________________ Signature: __________________________
Title: ______________________________ Title: ______________________________ Date: ______________________________ Date: ______________________________ TIN: ______________________________ Provider Number/NPI (if applicable): __________________________________ Notice Address: _________________________________ _________________________________ _________________________________
Notice Address: _________________________________ _________________________________ _________________________________
116

Clinical Integration Acknowledgement
EXHIBIT A
CIN PROGRAM SELECTION CRITERIA
For Primary Care Physicians:
· Be a member in good standing of RPO
· Credentials and history of sanctions have been verified by RPO and are satisfactory
· MA
o Part C/part D star rating
o Fund stat PMPM (Positive)
o Chronic code capture (80% or greater)
· Overall Engagement (1 Point)
o Administrator engagement rating (Engaged = Yes)
· Commercial (0.5 points each)
o Quality % for CAC (70% or greater)
o Total Medical Cost PMPM for CAC (less than $400)
For Specialist Physicians:
· Be a member in good standing of RPO
· Credentials and history of sanctions have been verified by RPO and are satisfactory
· Participates as a specialist in RPO Preferred POD network
117

Clinical Integration Acknowledgement
EXHIBIT B
CIN PROGRAM PARTICIPATION CRITERIA
• Be and remain a member in good standing of RPO
• Maintain medical staff privileges at a facility
• Act in a professional manner in relationships with patients, physicians and staff
• Actively participate in and adhere to the CIN Program’s clinical programs, evidence-based
guidelines, quality standards and care coordination programs, performance measurement and
reporting procedures and any requirements to contribute to the core goals of the CIN Program
• Be held accountable via the CIN Program’s Performance Improvement Plan, which encompasses
performance monitoring, evaluation & remediation process, inclusive of peer-to-peer
counseling and economic rewards
• Maintain connectivity with the CIN to share electronic clinical and demographic data
• Permit the CIN to review post-adjudicated claims data that are relevant to its programs
• Achieve the targeted performance levels within established protocols, pathways, and metrics as
defined for the CIN Program by RPO
• Participate in all CIN contracts approved and designated by RPO
• Demonstrate a willingness and commitment to promoting utilization of CIN Program resources
in a manner that improves care coordination, clinical quality and data transparency
• Be an active participant in leadership and oversight roles for the CIN Program
• Attend educational programs related to CIN programs & evidence-based medicine
• Meet all credentialing guidelines
118

Clinical Integration Acknowledgement
EXHIBIT C
PARTICIPATION FEE
Participants who are individuals shall remit to RPO Two Hundred Fifty Dollars ($250.00) annually as a Participation Fee. Participants who are entities shall remit ($250.00) annually as a Participation Fee for each Related Provider. Notwithstanding the foregoing, RPO may, in its sole discretion, elect to waive or remit some or all of this Participation Fee for those Participants/Related Providers whom RPO determines have devoted significant time and effort to the development and/or ongoing operations of the CIN Program.
119

Clinical Integration Acknowledgement
EXHIBIT D
JOINDER AGREEMENT
The undersigned individual desires to be considered a “Related Provider” as defined in the RPO Participant Agreement between RPO and ____________________ [fill in name of Participant] (“Agreement”) and hereby acknowledges, agrees and confirms that, if approved as a Related Provider by RPO to participate in the CIN Program, he/she: (1) has received a copy of the Agreement; (2) by execution of this Joinder Agreement, shall be bound to perform those duties and obligations assumed by Participant on Related Provider’s behalf under the terms of the Agreement; and (3) commits to be an active participant in the CIN Program, in compliance with CIN Policy and Performance Standards.
____________________________________ Print Name: __________________________ National Provider Identification: _________ Primary Specialty: ____________________ Date: _______________
Approved by RPO as a Related Provider: ____________________ ____________________ Date: _______________
120

Clinical Integration Acknowledgement
EXHIBIT E
BUSINESS ASSOCIATE AGREEMENT
This Business Associate Agreement (“Agreement”) is entered into and effective as of the ______ day of ________________, 20____ (“Effective Date”) by and between _____________________________________ (“Covered Entity”), and Renaissance Physician Organization (“Business Associate”)(collectively, the “Parties”).
WITNESSETH
WHEREAS, Covered Entity is a “covered entity” as defined in the Health Insurance Portability and Accountability Act of 1996 and the regulations promulgated thereunder (“HIPAA”), and as described in the Health Information Technology for Economic and Clinical Health Act (“HITECH”) provisions of the American Recovery and Reinvestment Act of 2009 (“ARRA”); and WHEREAS, Business Associate will provide certain quality control and reporting services (the “Services”) for Covered Entity pursuant to the terms of the RPO CIN Program Participant Agreement between the Parties, the performance of which involves exposure to certain Protected Health Information, as defined in 45 CFR 160.103 and limited to the information created or received by Business Associate from or on behalf of Covered Entity (“PHI”); WHEREAS, to the extent that Business Associate and/or other members of the clinically integrated network perform services for Covered Entity, they are conducting health care operations on Covered Entity’s’ s behalf and are therefore a Business Associate of Covered Entity;
1. WHEREAS, HIPAA requires that Covered Entity enter into written agreements with its business associates in order to regulate the use and disclosure of certain protected health information of Covered Entity; and
WHEREAS, Covered Entity and Business Associate agree to enter into this Agreement under the terms and conditions set forth herein to meet the applicable requirements for such business relationships under HIPAA.
2. NOW THEREFORE, for and in consideration of these premises, the Parties’ other mutual covenants contained herein, and other good and valuable consideration, the receipt and adequacy of which are forever acknowledged and confessed, the Parties hereto acknowledge, covenant, and agree as follows:
1. Obligations of Business Associate
1.1. Permitted Uses and Disclosures of PHI. Business Associate shall use and disclose any PHI it may receive from Covered Entity only to perform the Services and carry out the obligations of Business Associate under the Agreement, and in accordance with applicable
121

Clinical Integration Acknowledgement
federal and state laws, including but not limited to HIPAA. Business Associate may also use or disclose PHI for the proper management and administration of the Business Associate, for data aggregation services, or to carry out its legal responsibilities if such disclosure is required by law or if (i) the Business Associate obtains reasonable assurances from the person or entity to whom the information is disclosed that it will be held confidentially and used or further disclosed only as required by law or for the purpose for which it was disclosed, and (ii) the person or entity agrees to notify the Business Associate of any instances of which it is aware in which the confidentiality of the information has been breached. Business Associate shall not use or further disclose PHI other than permitted or required by this Agreement or as otherwise required by law. 1.2 Safeguards. Business Associate shall implement and use appropriate administrative, physical and technical safeguards that reasonably and appropriately protect the confidentiality, integrity, and availability of the PHI and prevent the use or disclosure of PHI other that as set forth in this Agreement or as permitted or required by law. Business Associate agrees to notify Covered Entity in the event of any breach of unsecured PHI held by or under the control of Business Associate, including the identity of the affected individual(s) and all other relevant information, within three (3) business days of becoming aware of such breach. Unless the context of the relationship specifically requires otherwise, the parties disclaim any agency relationship between Covered Entity and Business Associate. 1.3 Reporting Disclosures of PHI. In the event Business Associate, its agents, employees or contractors use or disclose PHI in violation of this Agreement, Business Associate shall report such use or disclosure to Covered Entity as soon as Business Associate becomes aware of such violation, including the circumstances surrounding the use or disclosure and a description of the PHI inappropriately used or disclosed. Business Associate shall report to Covered Entity any security incident of which it becomes aware. 1.4 Mitigation of Harmful Effects. Business Associate shall establish procedures for mitigating harmful effects of any improper use or disclosure of PHI that Business Associate reports to Covered Entity. 1.5 Third Party Agreements. Business Associate shall require all of its subcontractors and agents that receive, use or have access to PHI under this Agreement to agree in writing to adhere to the same restrictions and conditions applicable to the use or disclosure of such PHI as required herein. 1.6 Access to Information. Within ten (10) business days of a request by Covered Entity for access to PHI about an individual contained in a Designated Record Set (as defined in 45 C.F.R. 164.501) in Business Associate’s possession, Business Associate shall make available to Covered Entity such PHI for so long as such information is maintained in the Designated Record Set by Business Associate. In the event any individual requests access to his or her own PHI directly from Business Associate, Business Associate shall forward such request for access to PHI Covered Entity upon receipt of same. Business Associate shall reasonably cooperate with Covered Entity to provide an individual, at Covered Entity’s written direction, with access to the individual’s PHI in Business Associate’s possession within ten (10) business
122

Clinical Integration Acknowledgement
days of Business Associate’s receipt of written instructions for same from Covered Entity. Any denials of access to PHI requested shall be the responsibility of Covered Entity. 1.7 Amendment of PHI. Business Associate agrees to make PHI in a Designated Record Set available for amendment and to incorporate any appropriate amendments at the direction of and in the time and manner designated by Covered Entity. Business Associate further agrees to forward any request for amendment of PHI made by an individual to Covered Entity upon receipt of such request, and take no action on such request until directed by Covered Entity. 1.8 Accounting of Disclosures. Business Associate agrees to document disclosures of PHI and information related to such disclosures as would be required for Covered Entity to respond to a request by an individual for an accounting of disclosures of PHI in accordance with 45 CFR 164.528 and to provide Covered Entity with an accounting of such disclosures in the time and manner designated by Covered Entity. Business Associate further agrees to forward any request for an accounting of disclosures of PHI made by an individual to Covered Entity upon receipt of such request. To the extent Business Associate maintains PHI in an electronic health record, Business Associate agrees to account for all disclosures of such PHI upon the request of an individual for a period of at least three (3) years prior to such request (but no earlier than the effective date of this Agreement), as required by HITECH; such accounting shall be directly to the individual if requested by Covered Entity. 1.9 Access to Books and Records. Business Associate agrees to make its internal practices, books, and records relating to the use and disclosure of PHI available to the Secretary of the Department of Health and Human Services for purposes of determining compliance with the requirements of HIPAA. 1.10 Obligations under ARRA. Business Associate acknowledges that it is subject to the security and data breach provisions of HIPAA and agrees to abide thereby. Business Associate also agrees to abide by all of the privacy provisions set forth in Title XIII, Subtitle D of ARRA, including without limitation restrictions on marketing and requirements relating to limited data sets and minimum necessary disclosures. 2. Obligations of Covered Entity
2.1 Notice of Privacy Practices. Covered Entity agrees to provide Business Associate with a copy of Covered Entity’s “Notice of Privacy Practices,” required to be provided to individuals in accordance with 45 CFR 164.520, as well as any subsequent changes to such notice. 2.2 Changes to or Restrictions on Use or Disclosure of PHI. Covered Entity will provide Business Associate with any changes to, or revocation of, permission to use or disclose PHI if such changes affect Business Associate’s permitted or required uses or disclosures. Covered Entity will further notify Business Associate of any restriction to the use or disclosure of PHI agreed to by Covered Entity in accordance with the provisions of 45 CFR
123

Clinical Integration Acknowledgement
164.522, and any restriction requested by an individual which Covered Entity is required to comply with in accordance with the provisions of HITECH. 2.3 Requested Uses or Disclosures of PHI. Covered Entity shall not request Business Associate to use or disclose PHI in any manner inconsistent with state or federal law. 3. Term and Termination
3.1 Term. This Agreement shall be deemed effective on the Effective Date and shall continue in effect until all obligations of the Parties have been met, unless otherwise terminated under the terms and conditions set forth herein. 3.2 Termination for Cause. Upon Covered Entity’s knowledge of a material breach of this Agreement by Business Associate, its agents or subcontractors, this Agreement and any underlying services agreement may be immediately terminated by Covered Entity, as provided under 45 CFR 164.504(e)(2)(iii). At its option, Covered Entity may choose to (i) provide Business Associate with written notice of the existence of a material breach of this Agreement; and (ii) permit Business Associate to cure the material breach upon mutually agreeable terms. In the event Business Associate is afforded an opportunity and fails to cure the breach in accordance with such mutually agreeable terms, this Agreement and any underlying services agreement may be immediately terminated at the option of Covered Entity. In the event Covered Entity violates its obligations under HIPAA in a manner related to this Agreement, Business Associate shall provide Covered Entity with notice of such breach; if Covered Entity does not cure such breach within a reasonable period of time, Business Associate may terminate this Agreement. 3.3 Effect of Termination. Upon termination of this Agreement, Business Associate shall return or destroy all PHI created or received by Business Associate, its agents and subcontractors to the extent feasible, without retaining any copies of such PHI. If Business Associate and Covered Entity mutually agree that return or destruction of the PHI is not reasonably feasible, Business Associate agrees to extend the protections of PHI under this Agreement and limit further uses and disclosures of such PHI to those purposes that make the return or destruction infeasible. 4. Miscellaneous Provisions
4.1 Definitions and Interpretation; Indemnification. All words used herein but not defined herein shall have the meanings set out in HIPAA, and this Agreement shall be interpreted in such a fashion as to cause the parties to be in compliance with HIPAA.
4.2 Assignment. Neither party shall have the right to assign its rights or obligations under this Agreement without the prior written consent of the other party, and any such attempted assignment shall be void.
124

Clinical Integration Acknowledgement
4.3 Amendment. This Agreement shall not be modified or amended except by a written document executed by each of the parties to this Agreement, and such written modification or amendment shall be attached hereto.
4.4 Waiver of Provisions. Any waiver of any terms and conditions of this Agreement must be in writing, and signed by both Business Associate and Covered Entity. The waiver of any of the terms and conditions of this Agreement shall not be construed as a waiver of any other terms and conditions of the Agreement.
4.5 Parties In Interest; No Third-Party Beneficiaries. Except as otherwise provided in this Agreement, the terms and conditions of this Agreement shall inure to the benefit of and be binding upon the respective heirs, legal representatives, successors and permitted assigns of the parties to this Agreement. Neither this Agreement nor any other agreement contemplated in this Agreement shall be deemed to confer upon any person not a party to this Agreement any rights or remedies contained in this Agreement.
4.6 Governing Law. This Agreement, the rights and obligations of the parties hereto, and the entire relationship between the parties relating hereto shall be governed by and construed and enforced in accordance with the substantive laws (but not the rules governing conflicts of laws) of the state of Texas and with HIPAA.
4.7 Notice. Whenever this Agreement requires or permits any notice, request, or demand from one party to another, the notice, request, or demand must be in writing to be effective and shall be deemed to be delivered and received (i) if personally delivered or if delivered by telex, telegram, facsimile or courier service, when actually received by the party to whom notice is sent or (ii) if delivered by mail (whether actually received or not), at the close of business on the third business day next following the day when placed in the mail, postage prepaid, certified or registered, addressed to the appropriate party, at the address of such party set forth below (or at such other address as such party may designate by written notice to all other parties in accordance herewith):
If to Covered Entity: __________________________
__________________________ __________________________ __________________________ Attn: _________________ If to Business Associate: Renaissance Physician Organization 4.8 Authorization. The Parties executing this Agreement hereby warrant that they have the authority to execute this Agreement and that their execution of this Agreement does not violate any bylaws, rules, or regulations applicable to them.
125

Clinical Integration Acknowledgement
4.9 Counterparts. This Agreement may be executed in multiple counterparts, each of which shall be deemed an original, and all of which together shall constitute one and the same instrument.
3. IN WITNESS WHEREOF, the Parties hereto have executed this Agreement as of the date first written above.
Renaissance Physician Organization
By: Printed Name: _____________________________
Its: Date:
____________________________
By: Printed Name: _____________________________
Its:
126

Clinical Integration Acknowledgement
CLINICAL INTEGRATION ACKNOWLEDGEMENT
THIS CLINICAL INTEGRATION ACKNOWLEDGEMENT is made by and between Renaissance Physicians Organization (“RPO”) and ___________, M.D. (“Physician”). WHEREAS, Physician provides medical care to individuals pursuant to contracts arranged by RPO. WHEREAS, RPO members that have signed an RPO CIN Program Participant Agreement (the “Participant Agreement”) either as individual or through a group they are employed by or contracted with (collectively referred to herein as a “CIN Participant”), are clinically integrated and mutually interdependent providers that seek to control health care costs and ensure quality and coordination of care for patients; and WHEREAS, Physician is a CIN Participant; and WHEREAS, to ensure appropriate clinical integration in accordance with guidance on clinical integration established by the Federal Trade Commission and the Department of Justice, RPO seeks from Physician his or her acknowledgement regarding certain conditions of participation, and Physician wishes to acknowledge his obligation to comply with such conditions of participation and membership under the Participation Agreement; NOW, THEREFORE, in consideration of the mutual covenants, rights and obligations set forth herein, the benefits to be derived therefrom, and other good and valuable consideration, the receipt and sufficiency of which are hereby acknowledged, Physician acknowledges the following:
RESPONSIBILITIES OF RPO
1.1 Development of Policies. RPO agrees to develop and implement policies and procedures to ensure clinical integration of the services provided by CIN Participants, in accordance with guidelines of the Federal Trade Commission and the U.S. Department of Justice. RPO’s goal is to function as a clinically integrated independent practice organization and to promote quality, cost-effective medical services by arranging medical services to the public.
1.2 Administrative Services. RPO shall perform or cause to be performed all administrative, accounting and other functions relating to the maintenance of a clinical integration program on behalf of RPO CIN Participants.
RESPONSIBILITIES OF PHYSICIAN
2.1 Compliance with Policies. For so long as Physician is providing services under the Participant Agreement and consistent with the terms thereof, Physician agrees to comply with all clinical integration policies adopted by RPO from time to time, copies of which will be provided to Physician in advance of their effectiveness as to Physician. Specifically, Physician agrees to comply with the RPO Clinical Integration Policies, all policies and procedures contained in the RPO Provider Manual, including but not limited to the RPO CIN Performance Improvement Policy, and the RPO Clinical Integration Policies and Procedures, attached hereto as Attachment A and incorporated by reference into this Acknowledgement.
19918809v.2
127

Clinical Integration Acknowledgement
2.2 Reasonable Cooperation. Physician agrees to use his/her best efforts to provide reasonable assistance and cooperation to provide information required hereunder to RPO in a timely manner in order to facilitate the clinical integration program.
2.3 Multiple Counterparts. This Acknowledgment may be executed in one or more counterparts, each of which shall be deemed an original, but all of which together shall constitute one and the same document.
Renaissance Physician Organization
_______________________________ By: Title: Date:
Physician
________________________________ By: Date:
128
Clinical Integration Acknowledgement
ATTACHMENT A
RPO CLINICAL INTEGRATION POLICIES AND PROCEDURES
1. DEFINITIONS.
Ancillarity
The nexus between RPO’s joint contracting and collective bargaining on behalf of RPO CIN Participants and achievement of the maximum efficiency benefits of the Clinical Integration Program. In other words, the ability and necessity of RPO’s joint conduct to facilitate Clinical Integration Program efficiencies and pro-competitive benefits to consumers of RPO services.
Clinically Integrated RPO
Through RPO’s Clinical Integration Program, participating RPO CIN Participants have a high degree of interdependence and cooperation. Reports and information on Performance Measures will be provided to Participants with the intent of evaluating and modifying their clinical practice patterns as needed. The goal is to achieve efficiencies, control costs and assure the quality of Participants’ services. The Participant’s active participation in RPO’s Clinical Integration Program is a requirement for continued membership in RPO. All Participants participating in the Clinical Integration Program will participate in each contract when RPO reaches an agreement with a payor through collective negotiations.
Clinical Integration/Clinically Integrated
Partial (i.e., non-financial) integration and mutual interdependence of RPO CIN Participants as a basis for achieving RPO’s goals of enhanced efficiencies, including controlling and reducing healthcare costs and ensuring clinical quality, in part resulting from payor contracting activities undertaken by RPO on behalf of its Participant members.
Financial Integration
Sharing of financial risk among RPO Participants, either through participation in pre-paid or capitation payment formula contracts, bundling of episodes or case rates, financial withholds, or through overall economic integration and risk of operations.
Health Information Technology System (“HIT System”)
RPO’s clinical information management system that is the data repository of clinical health information collected from various sources including RPO Participants, hospitals, and independent laboratories. The HIT System is used to support the Clinical Integration Program and the quality and performance improvement initiatives of RPO.
RPO CIN Committee (the “Committee”)
The Committee is a representative group of RPO CIN Participants who in coordination with RPO staff have authority to guide RPO CIN Participants in Clinical Integration initiatives in accordance with the RPO Bylaws.
Performance Measure(s)
Evidence-based clinical performance measures, quality benchmarks, practice guidelines and protocols, utilization control mechanisms, and case and disease management programs, if applicable, and all updates thereto, as adopted by RPO from time to time.
129

Clinical Integration Acknowledgement
Participant(s)
An appropriately licensed physician or other licensed healthcare provider permitted by state law and the RPO Governing Board to provide patient care services on behalf of RPO, and who satisfies the relevant membership criteria, is approved to participate as a Participant in RPO, and who has executed a written agreement to participate with RPO’s CIN.
2. CLINICAL INTEGRATION.
2.1 These policies and procedures set forth RPO’s Clinical Integration Program requirements.
2.2 RPO is a Clinically and Financially Integrated independent practice association (“IPA”). As a condition of membership, RPO requires of all CIN Participants certain actions to ensure appropriate clinical integration in accordance with guidance on clinical integration established by the Federal Trade Commission and the Department of Justice. Participants have a high degree of interdependence and cooperation. The Participant’s active participation in RPO’s Clinical Integration Program is a requirement for continued Participant membership in RPO’s CIN.
2.3 As a Clinically and Financially Integrated IPA, RPO uses its best efforts to contract directly with managed health care companies and other payors on behalf of its CIN Participants. Absent Clinical or Financial Integration, RPO would face legal barriers to its ability to collectively bargain with managed care companies and other payors on behalf of its Participant members.
3. GOALS.
3.1 The goals of the Clinical Integration Program include, but are not limited to, the following:
3.1.1 Improve the quality, consistency and coordination of patient care;
3.1.2 Reduce and control costs and increase efficiencies in the health care provided;
3.1.3 Accelerate the adoption and common use of the HIT System by CIN Participants;
3.1.4 Ensure a valuable and competitive product will be available for consumers that would not be possible through independent actions of the Participants;
3.1.5 Reduce the cost and burden of complying with health plan requirements; and
3.1.6 Seek enhanced reimbursement for providing higher quality care.
130

Clinical Integration Acknowledgement
4. CONDITIONS OF MEMBERSHIP. As a RPO member, each individual Participant understands and agrees to comply with the following conditions of membership:
4.1 Be and remain a member in good standing of RPO 4.2 Maintain medical staff privileges at a facility 4.3 Act in a professional manner in relationships with patients, physicians and staff 4.4 Actively participate in and adhere to the CIN Program’s clinical programs, evidence-based guidelines,
quality standards and care coordination programs, performance measurement and reporting procedures and any requirements to contribute to the core goals of the CIN Program
4.5 Be held accountable via the CIN Program’s Performance Improvement Plan, which encompasses performance monitoring, evaluation & remediation process, inclusive of peer-to-peer counseling and economic rewards
4.6 Maintain connectivity with the CIN to share electronic clinical and demographic data 4.7 Permit the CIN to review post-adjudicated claims data that are relevant to its programs 4.8 Achieve the targeted performance levels within established protocols, pathways, and metrics as defined
for the CIN Program by RPO 4.9 Participate in all CIN contracts approved and designated by RPO 4.10 Demonstrate a willingness and commitment to promoting utilization of CIN Program resources in a
manner that improves care coordination, clinical quality and data transparency 4.11 Execute RPO’s Health Insurance Portability and Accountability Act business associate agreement, as
may be requested from time to time. 4.12 Participate in each payor contract executed by or on behalf of RPO.
5. PARTICIPANT PARTICIPATION.
To become or to be retained as a Participant in RPO, each CIN Participant is subject to the RPO credentialing and selection process. As a Clinically Integrated program, RPO is selective as to the individuals that are admitted to practice as CIN Participants. RPO may deny or terminate a CIN Participant’s RPO participation for failure to promote and adhere to the Clinical Integration Program.
6. OBLIGATIONS OF RPO.
6.1 RPO will provide CIN Participants and CIN Participants’ staff with educational opportunities and tools about the Clinical Integration Program and the HIT System.
6.2 RPO will provide CIN Participants with access to the RPO patient web portal where information on each RPO patient is stored, and will assist CIN Participants in interfacing with the HIT System.
6.3 RPO will provide Participants with periodic reports concerning each CIN Participant’s individual and aggregate compliance with Performance Measures.
6.4 RPO will collectively negotiate with managed care companies and other payors on behalf of CIN Participants.
7. INVESTMENT IN THE CLINICAL INTEGRATION PROGRAM.
RPO and Participants acknowledge the significant financial capital and human capital investments that are required to adequately and reasonably support the organization and operation of the Clinical Integration Program. RPO has provided sufficient and ongoing investment in support of the Clinical Integration Program, as determined by the RPO Board, including, but not limited to, infrastructure development and maintenance and provision of appropriate professional staff. CIN Participants agree to provide sufficient and ongoing human capital in support of the Clinical Integration Program as approved by the Board, including, but not limited to, CIN Participant and CIN Participants’ office staff training participation.
131

Clinical Integration Acknowledgement
8. HEALTH INFORMATION TECHNOLOGY SYSTEM.
In recognition of the importance of the HIT System to achieving and maintaining Clinical Integration through the capture of information about patient care provided to RPO patients, RPO and CIN Participants agree to the following:
8.1 CIN Participants agree to undergo initial and ongoing training regarding the HIT System as requested by RPO. CIN Participants agree that their staff will participate in HIT System training sessions as requested by RPO.
8.2 CIN Participants agree to post and share on a timely basis clinical information about RPO patients on the HIT System, and to collaborate with other RPO CIN Participants concerning common RPO patients.
8.3 CIN Participants agree that RPO will monitor Participant HIT System use and generate performance reports based in part on whether Participants appropriately utilize the HIT System.
9. EVIDENCE-BASED MEDICINE.
9.1 The Committee and the RPO Board will research, review and adopt Performance Measures for particular clinical conditions and/or diagnosis for each specialty and/or sub-specialty represented in RPO. The Committee will review and, if appropriate, adjust Performance Measures, particularly internal benchmarks as necessary, based on reported data and payor benchmarks as necessary but no less often than on an annual basis. In accordance with the RPO Bylaws, Committee members will provide insight into the medical care for the member’s particular medical specialty and patient population while taking into account the recommended course of treatment as defined by specialty associations, government entities, and other third party sources. Committee members are encouraged to consult with other CIN Participants in the selection and adoption of Performance Measures.
9.2 Once adopted by the Committee and the RPO Board, Performance Measures will be disseminated to Participants. RPO staff will contact CIN Participants directly to discuss the Performance Measures as well as how information on adherence to Performance Measures will be collected and how the Participant’s performance will be measured.
9.3 In coordination with the Committee, RPO benchmarks will be developed by reviewing and validating
reported data. In addition to establishing internal benchmarks, payors may have benchmarks for consideration that target specific areas of care.
10. ANCILLARITY.
10.1 RPO jointly contracts and collectively negotiates with managed health care companies and other payors on behalf of CIN Participants. In addition to the already established Financial Integration of RPO, achieving the goals of the Clinical Integration Program is more likely to be attained through collective efforts. Joint contracting and collective negotiation are related to, and reasonably necessary to further, the Clinical Integration Program’s integration and achievement of efficiencies and result in an overall procompetitive effect. In other words, there is ancillarity between joint contracting and achievement of RPO’s Clinical Integration goals. Factors including but not limited to RPO’s history, the substantial human and financial investments associated with the Clinical Integration Program, and the non-exclusive operation of the Clinical Integration Program, are indications that RPO’s competitive restraints are subordinate to and in furtherance of the Clinical Integration Program.
10.2 RPO recognizes that the achievement of Clinical Integration Program efficiencies is contingent upon establishment of a defined group of RPO CIN Participants who have committed to practice subject to the Clinical Integration Program’s conditions and constraints, as identified in RPO policies and procedures, and among whom referrals and other key interactions in treating patients under the Clinical Integration Program will occur. Specifically, the Clinical Integration Program’s joint contracting and collective bargaining will further RPO’s efficient operation by allowing it to: 1) establish a pre-determined panel of
132

Clinical Integration Acknowledgement
RPO CIN Participants that are easily identifiable to payors, patients, and referring physicians, 2) reinforce RPO’s in-network referral program, 3) ensure that all RPO CIN Participants are working toward the same financial and quality goals, 4) maximize opportunities for RPO to affect physicians’ practice patterns and the quality of care patients receive, 5) maximize the opportunities for collaboration in the care of patients, 6) reduce RPO’s administrative burdens, and 7) maximize transaction cost efficiencies.
11. INCENTIVES AND PENALTIES.
11.1 RPO and CIN Participants recognize the importance of compliance with and adherence to the Performance Measures for the purpose of Clinical Integration. Using a consistently applied methodology, RPO may, at its sole discretion, offer incentives to a CIN Participant for individual and/or aggregate achievement of Performance Measures; provided, however, that, if RPO makes an incentive available, RPO is not obligated to make the incentive available to each CIN Participant on the same terms as such incentive is made available to other CIN Participants. RPO may, in its sole discretion, allocate incentives based on the contributions and effort towards Clinical Integration made by various Participants.
11.2 Using a consistently applied methodology, RPO may, in its sole discretion, withhold incentives or otherwise penalize any CIN Participant for individual and/or aggregate failure to meet the Performance Measures; provided, however, that, if RPO penalizes a Participant, RPO is not obligated to penalize each Participant in the same manner as all other Participants. RPO reserves the right to penalize individual Participants based on a failure of contribution or effort towards Clinical Integration made by an individual Participant.
12. CLINICAL INTEGRATION PROGRAM.
As a condition of membership, each Participant acknowledges that he/she has received and reviewed, with counsel if desired, information concerning RPO requirements, including all current and available information related to Clinical Integration, Performance Measures and the HIT System.
13. CLINICAL QUALITY.
13.1 Compliance reports will be generated quarterly to detail Participants’ compliance with the Performance Measures. Compliance reports will be generated at the RPO aggregate and Participant level. The RPO aggregate level report will demonstrate Performance Measures compliance per the Participant’s specialty. The Participant level report will show reported patient information per Participant.
13.2 The Committee will review aggregate and Physician level compliance reports. In reviewing reports, the Committee will identify Participant(s) whose data demonstrates potential areas for improvement.
13.3 Periodically a small number of Performance Measures will be identified for targeted patient and Participant education opportunities.
14. BEHAVIOR MODIFICATION.
14.1 If the Participant level compliance report demonstrates a need for improvement as identified by the Committee, RPO staff will work with the individual Participant, the Participant’s office staff and, on occasion, patients to engage in educational opportunities with the desired result being both increased Participant and patient compliance.
14.2 The Committee will be apprised of said educational efforts and will monitor the Participant level compliance reports for those identified Participants to ensure Performance Measures compliance improves and/or is maintained in accordance with Clinical Integration Program requirements.
15. Physician acknowledges they are subject to RPO CIN Performance Improvement Policy
133

Clinical Integration Acknowledgement
Recommended by the RPO CIN Committee _________, 2018
Adopted by: RPO Board of Directors on _________, 2018
134

Clinical Integration Acknowledgement
EXHIBIT A
CIN PROGRAM SELECTION CRITERIA
For Primary Care Physicians:
· Be a member in good standing of RPO
· Credentials and history of sanctions have been verified by RPO and are satisfactory
· MA
o Part C/part D star rating
o Fund stat PMPM (Positive)
o Chronic code capture (80% or greater)
· Overall Engagement (1 Point)
o Administrator engagement rating (Engaged = Yes)
· Commercial (0.5 points each)
o Quality % for CAC (70% or greater)
o Total Medical Cost PMPM for CAC (less than $400)
For Specialist Physicians:
· Be a member in good standing of RPO
· Credentials and history of sanctions have been verified by RPO and are satisfactory
· Participates as a specialist in RPO Preferred POD network
135

Clinical Integration Acknowledgement
EXHIBIT B
CIN PROGRAM PARTICIPATION CRITERIA
• Be and remain a member in good standing of RPO
• Maintain medical staff privileges at a facility
• Act in a professional manner in relationships with patients, physicians and staff
• Actively participate in and adhere to the CIN Program’s clinical programs, evidence-based guidelines, quality
standards and care coordination programs, performance measurement and reporting procedures and any
requirements to contribute to the core goals of the CIN Program
• Be held accountable via the CIN Program’s Performance Improvement Plan, which encompasses performance
monitoring, evaluation & remediation process, inclusive of peer-to-peer counseling and economic rewards
• Maintain connectivity with the CIN to share electronic clinical and demographic data
• Permit the CIN to review post-adjudicated claims data that are relevant to its programs
• Achieve the targeted performance levels within established protocols, pathways, and metrics as defined for
the CIN Program by RPO
• Participate in all CIN contracts approved and designated by RPO
• Demonstrate a willingness and commitment to promoting utilization of CIN Program resources in a manner
that improves care coordination, clinical quality and data transparency
• Be an active participant in leadership and oversight roles for the CIN Program
• Attend educational programs related to CIN programs & evidence-based medicine
• Meet all credentialing guidelines
136

Clinical Integration Acknowledgement
CIN PROGRAM PERFORMANCE IMPROVEMENT POLICY Purpose To establish a process to provide support, counsel, and accountability for physicians participating in the CIN Program (“Participants”) to foster a high level of performance and delineate steps to address the failure of Participants to meet expectations. Overview On an ongoing basis, the CIN Program Oversight Subcommittee and the Clinical Quality Subcommittee will work collaboratively to monitor and evaluate the clinical performance, quality, and cost efficiency of Participants and provide support, counsel, and accountability for those Participants whose clinical outcomes do not meet CIN Program standards. Process A. On at least a quarterly basis, the Clinical Quality Subcommittee will analyze reports detailing the performance of all Participants against the measures, benchmarks and performance initiatives established for the CIN Program (“Measures”) and report its findings to the CIN Program Oversight Subcommittee. B. On a quarterly basis, the CIN Program Oversight Subcommittee will present the aggregate results to Participants. C. The CIN Program Oversight Subcommittee will follow the process outlined below for Participants who fail to meet Measures:
1. If any Participant fails to meet applicable Measures in two consecutive quarters, the CIN Program
Oversight Subcommittee will assign a physician representative of the subcommittee to contact the Participant to informally discuss barriers to success.
2. If the Participant fails to meet the same Measure(s) in the following quarter, the CIN Program
Oversight Subcommittee will send the Participant a formal notice by overnight national carrier to meet with a designated Subcommittee member.
3. If possible, the Subcommittee member will be selected on the basis of relevant practice area, peer
relationship and understanding of the goals and standards of the CIN Program. The Subcommittee member will not be a partner from the Participant’s practice.
4. Following receipt of such notice, the Participant will be expected to schedule and attend a meeting
with the Subcommittee member within 10 business days to discuss an improvement plan, which will encompass recommended quality steps, availability of resources, and a timeline for improvement with a duration of 90 days; however the Subcommittee, in its discretion, may shorten or lengthen the duration of the expected improvement based upon the nature of the clinical initiative and the time necessary to show improvement.
. 5. The Subcommittee member serving as the liaison will provide regular reports to the CIN Program
Oversight Subcommittee as to the status of all such meetings with Participants, and in turn, the Subcommittee will provide regular reports to the CIN Program Committee.
6. After the initial meeting with the Participant, the Subcommittee member and the Participant should
meet periodically, at least once a month, to evaluate progress and identify any needed support. 7. At the end of the designated timeline for improvement, the Subcommittee CIN Program Oversight
Subcommittee will evaluate the progress of the Participant and make one of the following recommendations to the CIN Program Committee:
137

Clinical Integration Acknowledgement
a. If, based on reasonable clinical judgment, the Subcommittee determines that the Participant has satisfactorily achieved identified improvement steps; the Subcommittee will recommend no further action. b. If, based on reasonable clinical judgment, the Subcommittee determines that the Participant is demonstrating significant improvement, the Subcommittee may allow the timeline for improvement to be extended, up to an additional 60 days. c. If, based on reasonable clinical judgment, the Subcommittee determines that the Participant has failed to demonstrate significant improvement, the Subcommittee will recommend a 90 day termination notice of the Participant to the CIN Program Committee.
8. Final determinations of action, taking into consideration the recommendations of the Subcommittee, will be made by the CIN Program Committee.
9. If a Participant is given a 90 day termination notice, the following appeals process is offered:
a) Administrator (CareAllies) receives appeal letter from provider
b) Administrator collects from provider a few lunch-hour dates and asks for any supplemental data (inquire who will be attending to coordinate legal if needed)
c) Provider Relations Rep to alert RPO Appeal panel (and legal if needed) of selected date via Outlook invite
d) Administrator notifies appealing provider and provides everyone a call-in number
e) Provider Relations Rep sends a reminder the day before with date, time, and number to provider and panel.
f) Hold panel discussion: (use sample script)
o First 30 minutes is provider pleading their case to panel and panel asks questions
o All disconnect from conference call and the panel and admin call back in
o Panel discusses matter
o Panel makes decision
g) Provider Relations Rep to complete minutes
h) Administrator notifies the provider of the decision via formal letter
i) Provider Relations Rep requests panel members a stipend of $250 for participation
138

Clinical Integration Acknowledgement
NETWORK OPERATIONS NETWORK OPERATIONS NETWORK OPERATIONS NETWORK OPERATIONS Provider CINProvider CINProvider CINProvider CIN Contract Appeals Contract Appeals Contract Appeals Contract Appeals ProcessProcessProcessProcess Date: 9Date: 9Date: 9Date: 9----12121212----17171717
I. Purpose: I. Purpose: I. Purpose: I. Purpose: To provide RPO CIN contract appeals process for Physicians/Providers (MD, DO) that participate in the Renaissance Physician Organization provider networks.
II. Definitions: II. Definitions: II. Definitions: II. Definitions:
1. Provider Provider Provider Provider –––– Any individual who is engaged in the delivery of health care services in a state and is licensed or certified by the state to engage in that activity in the state; and any entity that is engaged in the delivery of health care services in a state and is licensed or certified to deliver those services if such licensing or certification is required by state law or regulation.
2. Participating Provider Participating Provider Participating Provider Participating Provider –––– A participating Specialist or PCP providing covered services to members pursuant to an agreement with Renaissance Physician Organization.
III. Policy: III. Policy: III. Policy: III. Policy: In the event a provider’s CIN participation is denied or terminated by RPO, the provider must adhere to the appeals process below: 1. NOS/Admin receives appeal from provider. 2. Admin collects from provider a few lunch hour dates and asks for any supplemental data (inquire who
will be attending to coordinate legal if needed). 3. NOS to alert RPO Appeal panel (and legal if needed) of selected date via outlook invite 4. Admin notifies appealing provider and provides all a call in number 5. NOS sends a reminder the day before with date, time, and number to provider and panel. 6. Hold panel discussion: (use sample script)
a. First 30 minutes is provider pleading their case to panel and panel asks questions b. All disconnect from conference call and the panel and admin call back in c. Panel discusses matter d. Panel makes decision
7. NOS to complete minutes 8. Admin notifies the provider of the decision via formal letter 9. NOS requests panel members a stipend of $250 for participation
IV. Responsibility: IV. Responsibility: IV. Responsibility: IV. Responsibility: Network Operations is responsible for ensuring that the process is followed in order to ensure that the providers are provided the appropriate appeals process in accordance with the established guidelines.
V. Maintenance of Policy: V. Maintenance of Policy: V. Maintenance of Policy: V. Maintenance of Policy: This policy will be reviewed by Network Operations Support annually.
Appeal Panels:Appeal Panels:Appeal Panels:Appeal Panels: Appeal panel for Specialists: Dr. Hawkins, Dr. Horn and a like specialist. (Dan Hayes if needed) Appeal panel for PCPs: Dr. Hawkins, Dr. Moore, Dr. Basaldua, Dr. Orsak, Dr. Wills, Dr. Julian Gonzalez, and Dr. Vanderzyl (Dan Hayes if needed)
139

Clinical Integration Acknowledgement
RPO Medical Director: Dr. Nelson Fernandez Signature of Department Head Signature of Department Head Signature of Department Head Signature of Department Head Printed Name of Department Printed Name of Department Printed Name of Department Printed Name of Department Head Head Head Head Whitney Horak, President RPO Date Date Date Date 09/12/2017
140

Clinical Integration Acknowledgement
141

Clinical Integration Acknowledgement
Contents
Define to Delivery (D2D) Framework .................................................................................................................................. 164
Clinically Integrated Network (CIN) Guardrails ................................................................................................................. 1657
Overview ........................................................................................................................................................................... 1657
Care Coordination and Transitions of Care ..................................................................................................................... 16547
New or Established Patient Visit ................................................................................................................................. 16648
Patient Transitions from Hospitalist to PCP/Specialist ................................................................................................... 167
PCP Coordinates Patient Care with Specialist ................................................................................................................. 168
Specialist (A) Coordinates Patient Care with Specialist (B) ............................................................................................. 168
Chronic Disease Management ............................................................................................................................................ 169
Actively Managing Patients with Chronic Conditions ..................................................................................................... 170
Chronic Care Program Recommendation by PCP or Specialist ................................................................................... 17052
Reporting and Governance ............................................................................................................................................. 17153
CIN Reporting Grid ...................................................................................................................................................... 17254
Solution Evaluation ......................................................................................................................................................... 17557
Gap Analysis ................................................................................................................................................................ 17557
Appendix ......................................................................................................................................................................... 17860
• 1.Physician-to-Physician (P2P) Care Coordination Standards ............................................................................. 17860
• 2.Items to Review in Longitudinal Patient Record .............................................................................................. 17961
• 3.Glossary ............................................................................................................................................................ 17961
• 4.Icons ................................................................................................................................................................. 18062
• 5.Assumptions Related to Workflow Development ............................................................................................ 18062
Define to Delivery (D2D) Framework
The D2D framework consists of phases to progressively decompose a complex process (or program) into component
processes (or subcomponents), with each level providing increasing detail and precision to where the program can be
implemented efficiently and effectively. The framework includes:
• Requirements at a high (enterprise or context) level that provide a general understanding of a process
(program/program processes) and its relationship to other programs/processes
• At lower (operational) levels, roles and responsibilities defined, more granular activities are included and all
outcomes identified, including exceptions and alternative paths
• At the lowest (system) level, a basis for execution can be defined in the form of a project plan
The D2D Framework consists of 4 Phases that build on each other:
• Define: Evolve to our definition of the services offering
• Discovery: Discovering the agreed upon model that works for CA and the client
• Details: Determination of details required to make the service offering work and developing a plan
142

Clinical Integration Acknowledgement
• Delivery: Delivering on the plan
Clinically Integrated Network (CIN) Guardrails
Physician networks that enter joint agreements on price are exposed to antitrust risk. The FTC is unlikely to pursue
enforcement against networks with financial risk-sharing and low market share. Meaningful clinical integration can
make up for a lack of financial risk-sharing.
Clinical integration requires an active and ongoing effort to modify practice patterns in a way that creates
interdependence and cooperation among physicians to control costs and improve quality.
Indicia of clinical integration include:
• Shared information technology
• Shared clinical protocols
• Care review based on the implementation of protocols
• Mechanisms to ensure adherence to protocols
Networks should include financial risk-sharing and/or meaningful clinical integration that creates cost savings and
quality improvements that accrue to customers.
Networks should not be arrangements that focus on collective price negotiations or agreements, with only minimal or
pretextual financial or clinical integration.
Only enter into agreements on price if they are necessary to achieving the benefits or efficiencies of the integration.
Clinical Integration Guardrails (privileged).docx
Overview The following protocols are established to create standards of quality and drive initiatives that address care
coordination, disease management, and controlled cost and utilization. These protocols are put into place for all
provider types with the *Specified Physician Organization*.
In order to support the following protocols, *Specified Physician Organization* has implemented a new population
health management technology, *Asset*. This technology shall serve as a foundation for providing:
• Data to support a longitudinal, clinical patient record
• Effective coordination of care through communication tools
• Reporting on quality measures
• Tracking care costs and utilization trends
Where possible, provider workflows have been included with the protocols to guide efficient implementation and
appropriate adherence.
Care Coordination and Transitions of Care
1. The following protocols ensure a patient has quality coordination and effective
transitions of care across a spectrum of associated health care providers.
143

Clinical Integration Acknowledgement
# Protocol
1 Participating Providers (PCPs and Specialists) and/or delegates shall use the *Asset* to identify
patients covered in the CIN. Providers will use the *Asset* to collaborate to share and review the
patient’s longitudinal health record when a patient transitions between providers (PCPs and
Specialists). The 360 degree view of a patient’s health record is contained in the provided
*Asset*.
2 Participating Providers and/or delegates shall communicate using the *Asset* when coordinating
patient care between various levels of care. The minimum requirements (the minimum
requirements for each coordination interaction are available in the Appendix) include, but are not
limited to:
• Alerting providers when a patient has been admitted
• Documenting necessary clinical and medication information to the patient’s longitudinal
health record to share and collaborate with other providers
• Reviewing the longitudinal health record upon admission and post discharge
3 Participating Providers and/or delegates shall utilize the *Asset* to review and communicate
information related to a patient’s current condition and potential clinical needs to address a
particular disease state. Providers and/or delegates will add Clinical updates to the *Asset* to be
viewed by the coordinating physicians.
4 Medical Directors and CIN oversight committee shall regularly review task history reports from
the *Asset* to ensure PCPs and Specialists are actively monitoring and completing assigned
coordination activities.
New or Established Patient Visit
144

Clinical Integration Acknowledgement
Patient Transitions from Hospital to PCP/Specialist
Clinical Integration Network (CIN) – Care Coordination & Transitions of Care: Patient Transitions From Hospital to PCP/Specialist
Role--Owner
Use the *Asset* to
Communicate to the
Attributed PCP that
the Patient has Been
Admitted
Upon Discharge, Use
*Asset* to Coordinate
with the Attributed
PCP and Any Other
Indicated Specialists
with Follow-up on
Patient. Document
Necessary Discharge
Information in the
*Asset*
Log-In to *Asset* to
Review MessagesEnd
4
3
Start
Review Open Tasks
and Supporting
Documentation in
the *Asset* and
Schedule Follow-up
as Indicated
5
Access *Asset* to
Review Pertinent
Patient History
Information
2
6
See Appendix #1: P2P Care
Coordination Standards #2
See Appendix #1: P2P Care
Coordination Standards #3
See Appendix: #2. Items to Review in
Longitudinal Patient Record
If Patient Payer LOB
is in the CIN, Access
*Asset* to Locate
the Patient and
confirm is in CIN
1
145

Clinical Integration Acknowledgement
PCP Coordinates Patient Care with Specialist
Clinical Integration Network (CIN) – Care Coordination & Transitions of Care: PCP Coordinates Patient Care With Specialist
Part
icip
ati
ng P
rovid
er
(PC
P)
an
d/o
r
de
legate
Part
icip
ati
ng P
rovid
er
(Sp
eci
alist
) an
d/o
r
dele
gate
Role--Owner
Notify the Specialist
to Review Patient
Information in the
*Asset*
Access *Asset* to
Review Pertinent
Patient History
Information
Upon Receipt of Care
Coordination
Notification, Log-in to
the *Asset*. Look up
the Patient, Attest to
Medical Need for
Patient Information,
and Review the
Longitudinal Record
for History and
Attributed PCP
Documentation
End
4
If Patient Payer LOB
is in the CIN, Access
*Asset* to Locate
the Patient and
confirm is in CIN
1 2
Start
Enter appropriate Post
Patient Visit
information in the
*Asset* and Notify the
Attributed PCP to
Review and/or Perform
Additional Follow-up,
as Necessary
5
See Appendix #1: P2P Care
Coordination Standards #4
See Appendix #1: P2P Care
Coordination Standards #5
Continue
Coordination with
Specialist using the
*Asset* as
Appropriate
6
See Appendix: #2. Items to Review in
Longitudinal Patient Record
See Appendix: #2. Items to Review in
Longitudinal Patient Record
3
Specialist (A) Coordinates Patient Care with Specialist (B)
Part
icip
ati
ng P
rovi
der
(Sp
eci
alist
A)
an
d/o
r
dele
gate
Part
icip
ati
ng P
rovid
er
(Sp
eci
alist
B)
an
d/
or
dele
gate
Part
icip
ati
ng P
rovi
der
(PC
P)
an
d/o
r d
ele
gate
146

Clinical Integration Acknowledgement
CIN - Care Coordination Transitions of Care 4_13.pdf
ChronicDiseaseManagement
2. The following protocols ensure appropriate and effective use of available disease
management programs to enhance patient outcomes, proactively address gaps in care,
utilize optimal resources, and minimize needs for emergency intervention.
# Protocol
5 Participating Primary Care Providers (PCPs) and/or delegates shall use the *Asset* to identify
patients with chronic conditions and proactively address current gaps in care through patient
outreach and engagement.
6 Participating providers and/or delegates shall actively manage patients enrolled in Case
Management or available Disease Management programs, identified as those most frequently in
need of emergency interventions, following appropriate evidence based guidelines and standards
of care.
•
7 Participating Providers and/or delegates shall collaborate to evaluate a patient for chronic disease
management programs provided by the payer by utilizing the *Asset* for enrollment criteria and
coordinated communication, if appropriate.
• Either the PCP or Specialist can refer an appropriate patient to a payer chronic disease
management program and will inform the collaborating provider of the referral in the
*Asset*
147

Clinical Integration Acknowledgement
Actively Managing Patients with Chronic Conditions
Chronic Care Program Recommendation by PCP or Specialist
PC
P/O
ffic
e S
taff
Sp
eci
alist
/Off
ice
Sta
ff
148

Clinical Integration Acknowledgement
CIN - Chronic Disease Management 4_13.pdf
ReportingandGovernance
3. The following protocols ensure clinical guidelines are being adhered to in order to
increase quality, effectively coordinate patient care, improve health outcomes, and reduce
costs.
# Protocol
8 Reporting and governance shall be provided through the use of monthly UM/QM meetings,
Governance Board meetings, and regular reporting out of the *Asset*. Interventions at the
provider level will be determined by local Governance boards consistent with the larger
Governance operational guidelines, ranging from a phone call to one-on-one coaching to
termination from the CIN
9 Performance of quality measures to assess and monitor improvements and outcomes will be
tracked and reported in the following areas:
• Protocol Adherence Metrics (Regular review of number of tasks and response times, with
monthly calculation and reporting of average response times, by provider)
• Performance Metrics
o Gaps in Care Metrics, utilizing the performance dashboard within the *Asset* to
benchmark target goals and current performance throughout the year
o Utilization metrics using various reporting from the *Asset*:
� Admissions
� Re-admissions: same or similar and all-cause
� Emergency Room Utilization
10 Performance Reports shall be shared on a regular basis with each participating provider so that
providers can compare their own performance with that of their peers. Consistent reporting and
feedback shall allow providers to measure and compare clinical outcomes, efficiency, and patient
utilization, driving the desired overall quality of care.
149

Clinical Integration Acknowledgement
CIN Reporting Grid
PROTOCOL ADHERENCE MEASURES
# Report Name Brief Description Frequency Report User
1 General Usage Shows frequency of user access to system and
portions accessed.
Monthly CIN Leadership,
Clinical Leaders,
provider and CA
2 Hospitalist
Coordination
Shows Hospitalist access to Asset, admit information
sent, to whom sent, discharge information sent and
to whom sent
Monthly CIN Leadership,
Clinical Leaders,
provider and CA
3 PCP Coordination Shows PCP access to Asset, coordination information
sent and to whom sent, response time to tasks
Monthly CIN Leadership,
Clinical Leaders,
provider and CA
4 Specialist
Coordination
Shows Specialist access to Asset, coordination
information sent and to whom sent, response time
to tasks
Monthly CIN Leadership,
Clinical Leaders,
provider and CA
5 Payer Program
Referrals
Shows referrals to payer chronic care programs by
provider, CIN providers copied on referral and
outcome of referral
Monthly CIN Leadership,
Clinical Leaders,
provider and CA
PERFORMANCE METRICS
# Report Name Brief Description Frequency Report User
1 Gaps in Care Shows patient level detail (PHI approved access) by
attributed provider and benchmarks against CIN
On
Demand
CIN Leadership,
Clinical Leaders,
provider and CA
2 Admissions and
Re-admissions
Admissions, hospitalist admit and discharge note
sent (Y/N), PCP visit within (10) days (Y/N) and
facility. Matches Re-admissions to reference
admission.
On
Demand
CIN Leadership,
Clinical Leaders,
provider and CA
3 ER Utilization ER encounters to identify high utilizing patients and
overall ER utilization metrics
On
Demand
CIN Leadership,
Clinical Leaders,
provider and CA
4 Chronic Condition
Management
Able to select by target condition and shows list of
patients, date last seen, date of last admission,
enrollment status in payer program and disease
specific gaps
On
Demand
CIN Leadership,
Clinical Leaders,
provider and CA
*Note: All reports are available at provider level and CIN level. PHI visibility is determined based on user role and
need and de-identified as appropriate.
150

Clinical Integration Acknowledgement
CIN - Reporting and Governance.pdf
DATA CONTEXT MODEL
# Data Category Description
1 Claims/Encounters Medical claims and encounters are medical bills submitted to an
insurance carrier (payer) for services rendered to a customer
(patient) by a healthcare provider. Claims contain pertinent
information about the patient related to diagnoses and services
performed during the billed encounter. A customer, a
representative of the customer, or a healthcare professional or
organization may submit claims.
151

Clinical Integration Acknowledgement
2 Eligibility The status that shows a patient is enrolled in a healthcare benefit
plan at a specified time and entitled to benefits and services as
defined by that agreement.
3 Hierarchy A top-down system of layers to organize and arrange the
relationships between the entities in a healthcare network for
grouping and reporting purposes.
4 Pharmacy Prescription drug claim information for an individual submitted to
a payer or pharmacy benefit manager for payment.
5a Payer Labs Information from the Payer on the results of a procedure, usually
conducted in a laboratory, that is intended to detect, identify, or
quantify one or more significant substances, evaluate organ
functions, or establish the nature of a condition or disease for an
individual.
5b Direct Labs Diagnostic tests and results performed by laboratory initiated by
an order from a healthcare provider. Lab values can be
transmitted via claims, encounters or as supplemental data.
6 Documentation of
Protocols
Referral Information, Tasks, and Attachments documented in the
“common” *asset* as part of the CIN protocols.
7 Protocol Adherence
Metrics
Reportable data to determine adherence rates for the CIN
protocols determined by the CIN entity: number of tasks & specific
response times for activities by providers as well as average
response times and monthly calculation.
8 Performance Metrics Reportable data to determine the performance of specific quality
measures by various levels of the reporting hierarchy, such as
providers or groups, i.e., Gaps in Care, Admissions, Re-admissions
(Same or similar and all-cause), Network utilization compliance.
9 Auths Notice of service authorization from the payer of the service to the
provider who requested the authorization to be paid for the
service per the payer’s authorization policies, typically completed
before the delivery of the service and subsequent claim
10 ADT Admissions, discharges, and transfers (Formats: HL7 [Preferred] &
Other)
An ADT feed is one way an application or a provider can get
information such as Registering a patient & Discharging a patient
from a clinic or hospital information system (HIS).
11 EHR Electronic health record (EHR), or electronic medical record (EMR),
refers to the systematized collection of patient and population
electronically-stored health information in a digital format. Records
can be shared across different health care settings. Records are
shared through network-connected, enterprise-wide information
systems or other information networks and exchanges. OR: An
electronic health record (EHR) or electronic medical record (EMR)
is a digital version of a patient’s paper chart. EHRs are real-time,
patient-centered records that make information available instantly
and securely to authorized users. While an EHR does contain the
medical and treatment histories of patients, an EHR system is built
to go beyond standard clinical data collected in a provider’s office
and can be inclusive of a broader view of a patient’s care.
12 Facility Census The count of the number of patients in a facility on a given day.
The report can include member details (e.g., admission date,
admitting diagnosis, planned discharge date, etc.) and is typically
produced by the entity who authorizes and pays for the patient’s
152

Clinical Integration Acknowledgement
stay (the payer).
13 Supplemental Clinical data from sources other than claims or encounters that
comes from approved sources, such as OSCR, 360s and medical
charts.
14 HIE A Health Information Exchange (HIE) is a secure electronic
exchange that consists of health-related information between
treating physicians, hospitals, health care payers and other health
care providers involved in the care of the patient.
Solution Evaluation
Gap Analysis
# Requirement Associated
Protocol
Gap Analysis
Vendor Capability
Readiness
Comments
1 The ability to provide/display data to
support a longitudinal, clinical patient
record
Overview Currently supported
and enabled
2 The ability to enable effective
coordination of care through
communication tools
Overview Currently
supported; not
enabled
3 The ability to report on quality
measures
Overview Currently supported
and enabled
Enabled internally only, not for
PCPs
4 The ability to track care costs and
utilization trends
Overview Currently supported Would need vetting and possibly
additional development to refine
5 The ability to enable providers to share
and review the longitudinal health
record in the Asset
1 Currently supported Partially enabled. Providers can
view. The functionality to
message another user and direct
them to the health record is
supported but not enabled.
6 The ability to enable PCPs and
Hospitalists to communicate in the
Asset when coordinating between
various levels of care:
- Hospitalist message providers
when a patient is being
admitted
2 Currently
supported; not
enabled
Note: messages cannot be
tracked or reported on. Would
also need to do further testing on
how messaging works with
attestation
7 The ability to enable PCPs and
Hospitalists to communicate in the
Asset when coordinating between
various levels of care:
- PCPs and Hospitalists attach
necessary documentation and
medication information to the
patient’s longitudinal health
record
2 Currently supported
and enabled
8 The ability to enable PCPs and
Hospitalists to communicate in the
Asset when coordinating between
2 Currently
supported; not
enabled
153

Clinical Integration Acknowledgement
various levels of care:
- PCPs and Hospitalists review
the longitudinal health record
upon admission and post
discharge
9 The ability to enable PCPs and
Specialists to review and communicate
a patient’s current condition and
potential clinical needs to address a
particular disease state in the Asset
3 Currently
supported; not
enabled
10 The ability to enable Medical Directors
and UM/QM Boards to review task
history reports from the Asset (to
ensure PCPs and Specialists are actively
monitoring and closing assigned tasks)
4 Currently
supported; not
enabled
Would want to perform testing
around this functionality as it is
rather new
11 The ability to enable PCPs and
Specialists to collaborate and evaluate
a patient for chronic disease
management programs in the Asset for
enrollment criteria and coordinated
communication:
- PCPs shall review and respond
to tasks from specialists to
evaluate patients for chronic
care programs
- Specialist shall notify PCP of the
enrollment in the program if
the Specialist is recommending
it.
7 See notes The tasking to evaluate is
supported in the platform. The
requirements for chronic care
programs could be stored in the
content library. But the provider
could not make a referral into a
chronic care program from the
platform though.
12 The ability to enable PCPs and
Specialists to collaborate and evaluate
a patient for chronic disease
management programs in the Asset for
enrollment criteria and coordinated
communication:
- Specialists shall attach related
documentation to support a
program recommendation and
tasks PCP to review
7 See notes The tasking to evaluate is
supported in the platform. The
requirements for chronic care
programs could be stored in the
content library. But the provider
could not make a referral into a
chronic care program from the
platform though.
13 The ability to support regular reporting.
Performance of quality outcomes to
ensure improvement shall be tracked
and reported in the following areas:
- Regular review of number of
tasks and response times, with
monthly calculation and
reporting of average response
times, by provider
9 Partially supported Reporting on tasks and
completion is supported.
However, we need to confirm if
response time is a reportable
element.
14 The ability to support regular reporting.
Performance of quality outcomes to
ensure improvement shall be tracked
and reported in the following areas:
- STAR and HEDIS measures,
9 Currently supported
and enabled
Enabled internally only, not for
PCPs
154

Clinical Integration Acknowledgement
utilizing the performance
dashboard within the Asset to
benchmark target goals and
current performance
throughout the year
15 The ability to support regular reporting.
Performance of quality outcomes to
ensure improvement shall be tracked
and reported in the following areas:
- Utilization metrics using various
reporting from the Asset:
o Admissions
o Re-admissions: same or
similar and all-cause
o Network utilization
compliance
9 Partially supported Most of the reporting needs are
met through current
functionality. Testing would be
needed to confirm gaps and
additional development would be
needed to ensure it is user
friendly. The one reporting
element I’m not sure that exists
easily is network utilization
compliance.
16 Source (data) into the Platform
17 System produces reporting for tracking
18 Get CINs preferred network if there is
one
155

Clinical Integration Acknowledgement
Appendix
1. Physician-to-Physician (P2P) Care Coordination Standards
The following scenarios reflect the minimum CIN clinical requirements for a provider to send to another provider when
coordination of care of the patient occurs for the scenarios in the CIN workflows
1. Patient appointment in a provider office without another provider's notice (e.g., new patient, self-referral)
and the rendering provider needs to notify an attributed PCP of the patient visit
a. Date of Service
b. Presenting complaint, reason for visit
d. Test orders and results
e. Treatment Plan
2. Notification to PCP upon admission
a. Admission Date
b. Facility name
c. Admit Diagnosis
d. Expected discharge date
e. Request for PCP office to provide any clinical information that is relevant to the admitting diagnosis
3. Notification to PCP (and Specialist, when appropriate) upon discharge
a. Discharge Date
b. If referred to a Specialist, copy both PCP and Specialist
c. Discharge medications and changes from previous medication regimen
d. Home care needs
e. Treatment Plan
4. PCP notification to a Specialist when a patient is sent to Specialist
a. Date of PCP visit
a. Reason for referral to Specialist including any special circumstances
5. Specialist notes back to PCP (and Specialist, if applicable) after Specialist visit
a. Date of Specialist visit
b. Test orders and results
c. Treatment plan
156

Clinical Integration Acknowledgement
6. Specialist notification to a second Specialist (and notifies attributed PCP of same information) when a
patient is sent to another Specialist
a. Date of Specialist A visit
b. Reason for referral
c. Test orders and results
2. Items to Review in Longitudinal Patient Record
Items to review in Longitudinal Patient Record
• Patient Demographics
o DOB/Phone/Address
o Attributed Primary Provider
o Last Accountable Provider Visit
• Diagnosis History
• Services and Procedures History
• Prescriptions History
• Lab History
• Screening and Prevention History
• Program Enrollment
3. Glossary
Term Definition
D2D Define to Delivery Framework
CIN Clinically Integrated Network
Physician Network The associated group of providers, typically Primary Care Physicians
(PCPs) and Specialists that are available to care for an individual
patient, as defined by some type of agreement (e.g., payer, IPA, CIN,
etc.)
FTC Federal Trade Commission
Clinical Integration Indicia of clinical integration include:
• Shared information technology
• Shared clinical protocols
• Care review based on the implementation of protocols
• Mechanisms to ensure adherence to protocols
Specified Physician Organization As used in this document, this is the client organization that would
utilize this service
Asset As used in this document, this is the shared application used to deliver
these services
157

Clinical Integration Acknowledgement
PCP Primary Care Physician
Hospitalist A physician dedicated to the delivery of comprehensive medical care to
hospitalized patients
Specialist A physician who has completed advanced education and clinical
training in a specific area of medicine
Medical Director A physician who provides clinical guidance, leadership, oversight and
quality assurance for an organization
Governance Board An organization’s Board that is responsible for Policy Formulation,
Decision Making and Oversight related to the responsibilities of the
organization, such as its Mission, Leadership, Operations and Financial
Health
4. Icons
5. Assumptions Related to Workflow Development
# Assumption Response
1 CIN must include all PCPs and Specialists
2 Specified Physician Organization meets all other CIN
“requirements” outside of care coordination
3 CIN will only use Payer’s Chronic Disease Management
programs
4 Workflows must be flexible to address all applicable payer
types & LOBS
5 A minimum set of data will be required to execute the CIN
(Reference CIN Data Context Model)
6 All participants in the CIN would have access to same
technology (technologies)
7 PCP offices in CIN will check the Asset a minimum of once
daily to check for any messages
8 Specialists will need to be notified via a method to direct
them to check the Asset for a message. They will not be
expected to check daily, like the PCP, so will need to be
prompted to go to asset.
158

Clinical Integration Acknowledgement
Renaissance Physicians CIN Clinical Guidelines Guidelines Ambulatory Care: Renaissance Physicians CIN follows MCG Health Guidelines for Ambulatory Care. http://www.mcg.com/ Ambulatory Care offers over 760 evidence-based guidelines for the appropriate assessment, treatment, management and referral of patients with conditions typically treated in an ambulatory or outpatient setting. With Ambulatory Care, you can:
Optimize Utilization: Reference clinical indications for the appropriate use of advanced imaging services and other diagnostics to reduce overutilization, reduce costs, and improve patient safety. Reduce Denials: Reduce payment denials and protect revenue by presenting the best available evidence to establish the medical necessity of the outpatient care provided. Support Referrals: Support authorization and treatment planning for patients requiring outpatient rehabilitation or specialist referrals services by consulting evidence-based guidelines and/or industry benchmarks.
159

Clinical Integration Acknowledgement
160

Clinical Integration Acknowledgement
ANNUAL MEMBER SURVEY
To: Renaissance Physicians Member
From: Renaissance Physicians
Re: Member Satisfaction Survey
Renaissance Physicians is proud to provide coordinated care centered on you and your needs. Your Renaissance
primary care physician coordinates all of your care using enhanced information technology, more comprehensive data
from your health plan, and expert clinical staff to ensure you receive necessary care tailored to your specific needs.
In order to evaluate our commitment to youyouyouyou Renaissance Physicians is asking for your feedback by completing the
enclosed survey which will allow you to rate your physician and physician staff. Your feedback to this survey will
ultimately help improve your experience when visiting or contacting your Physician.
Please take this opportunity by completing the enclosed short survey and returning it using the self-addressed envelope
provided.
Renaissance Physicians is committed to providing quality of care and increase your overall satisfaction with the care you
receive. We look forward to working with you to help you become healthy, stay healthy and get the care and services
that are right for you.
Thank you for choosing Renaissance Physicians!
161

www.arcadiasolutions.com Arcadia Healthcare Solutions
Frequently Asked Questions
Which internet browser is most compatible with the Arcadia platform?
Use Google Chrome for optimal use. Also supported is Firefox, Safari or IE v.9 or older.
Why can’t I navigate in the platform and keep getting a message that says
“Unexpected Error”?
The platform has “timed out”. Time out occurs after 15 minutes of inactivity. You will need
to close your browser window and login again to access the Arcadia platform.
I am in the Activity Feed and unable to access my patient by selecting on the
patient’s name.
In order to access the patient’s record, you will need to do one of the following items:
• Select on the link for Patient Summary
• Navigate to the task in My Calendar and select on the patient’s name
• Use the patient search feature to locate the patient
Where are today’s tasks on My Calendar?
Today’s tasks are located under the “Overdue” heading. The oldest items will be at the
top, notated by the number of days they are overdue. Today’s tasks will be at the bottom
of the list without a number of days notated.
How do I search for my patients?
You may search for a patient by clicking on the magnifying glass in the top right of the
screen. Once you click here, a search bar will open. Patients may be searched for in any
of the following formats.
• Name
• Last First (no comma)
• Last, First
• Date of Birth
• YYYY-MM-DD
What types of documents can be uploaded in the Patient Info section and a Quick
Note?
The following documents types are accepted as attachments:
MSWord, PDF, Rich Text, Plain Text, Bitmap, Jpeg, PNG, TIF, CSV (Comma delimited)
162

Ste
ps fo
r C
om
ple
tio
n
www.arcadiasolutions.com Arcadia Healthcare Solutions
Clinically Integrated Network: Logging In
1. Visit the CareAllies homepage: https://CareAllies.com
2. Navigate to the LOGIN link in the upper right corner to log-in to the CareAllies Population
Health Management tool
3. Provide log-in credentials using your email address as your user name
4. You will then be routed to the Arcadia home page
163
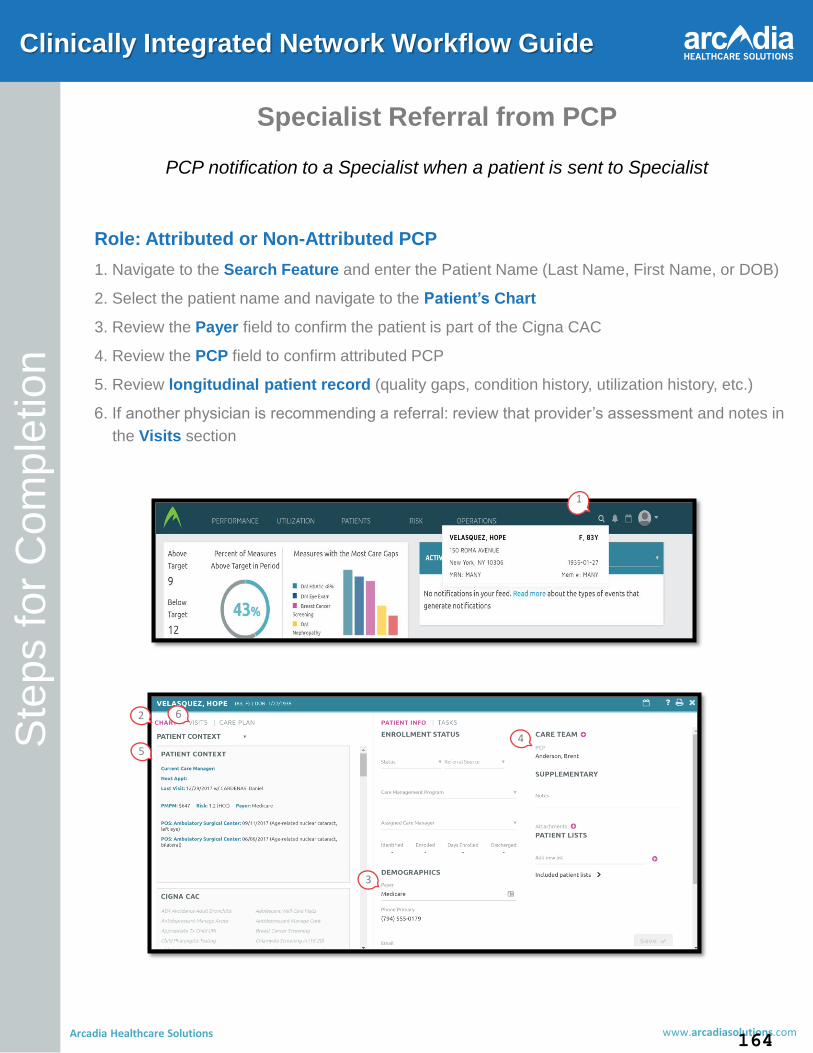
Ste
ps fo
r C
om
ple
tio
n
www.arcadiasolutions.com Arcadia Healthcare Solutions
Clinically Integrated Network Workflow Guide
Specialist Referral from PCP
PCP notification to a Specialist when a patient is sent to Specialist
Role: Attributed or Non-Attributed PCP
1. Navigate to the Search Feature and enter the Patient Name (Last Name, First Name, or DOB)
2. Select the patient name and navigate to the Patient’s Chart
3. Review the Payer field to confirm the patient is part of the Cigna CAC
4. Review the PCP field to confirm attributed PCP
5. Review longitudinal patient record (quality gaps, condition history, utilization history, etc.)
6. If another physician is recommending a referral: review that provider’s assessment and notes in
the Visits section
1
2
3
4 5
6
164

Ste
ps fo
r C
om
ple
tio
n
www.arcadiasolutions.com Arcadia Healthcare Solutions
Clinically Integrated Network Workflow Guide
Specialist Referral from PCP continued…
7. Navigate to Tasks on the right hand side of the screen and Create New Task
a) Schedule Date field will auto-populate with today’s date, adjust as needed
b) Assigned To field will auto-populate with your username
8. Select appropriate Reason and the Specialist Referral from PCP assessment form
9. Select Start from the Create New Task panel
9
8
7
10.Tag the Specialist (and Attributed PCP if applicable) by adding their name in the Tag Users
section
11.Select Next Section to move on
10
11
165

Ste
ps fo
r C
om
ple
tio
n
www.arcadiasolutions.com Arcadia Healthcare Solutions
Clinically Integrated Network Workflow Guide
Specialist Referral from PCP continued…
12. Complete the appropriate fields in the assessment form
a) Review form tracking metrics to ensure you’ve completed all necessary fields
13. Select Yes to schedule an appointment with patient question
14. Once completed, select Complete at the bottom of the task creation form
15. Confirm that you understand there can be no further edits to this completed assessment
12
14
13
15
166

Ste
ps fo
r C
om
ple
tio
n
www.arcadiasolutions.com Arcadia Healthcare Solutions
Clinically Integrated Network Workflow Guide
Specialist Referral from PCP continued…
15. Once the assessment is complete you will be brought to Care Plan Curation. Select the addition
sign
16. Select Care Coordination interventions to add to the Patient’s Care Plan, and select Save
16
17. Navigate to the patient’s Care Plan and select Schedule on the Schedule Appointment with
Patient intervention
18. Adjust the Assigned To field to the Specialist
19. Mark the appropriate Urgent Flag to indicate whether the task to be completed is Urgent or Not
Urgent
20. Ensure Schedule appointment with patient populates under Description
21. Select Schedule at the bottom of the Task Creation Form
17 18
21
19 20
167

BLUE CROSS BLUE SHIELD OF TEXAS
• Blue Cross Blue Shield Medicare
Advantage (MAPD)
A Physician or Physician Group can elect to participate in the Blue Cross Blue Shield of Texas Health plans offered through Renaissance. A provider must complete an Election to Participate Form and submit the form to their designated Network Operations Representative.
The form can be found on www.myrpo.com under the providers tab.
Blue Cross Blue Shield Medicare Advantage (MAPD)
Providers should be able to easily identify MAPD members by identifying plan type. Renaissance is the sole provider network for Blue Cross Medicare Advantage HMO. Blue Cross Medicare Advantage HMO plans for 2019:
• Blue Cross Medicare Advantage
Basic (HMO)
• Blue Cross Medicare Advantage
Basic Plus (HMO-POS)
• Blue Cross Medicare Advantage
Premier (HMO)
Web: Please visit bcbstx.com/Medicare to view all plan documents. Call: For more information about Blue Cross Medicare Advantage Benefits or formulary, please call 1-877-608-2698 (HMO Plans) BCBSMA 2019 Benefits: Please visit the following link for a detailed summary of 2019 Benefits: https://www.bcbstx.com/medicare/pdf/mapd-sum-hmo-hou-tx-2019.pdf
168

BCBS MA Member ID Card:
169

Claims Submissions: Certain types of services must be submitted to Renaissance Physicians, rather than to BCBSTX claims. When a claim is sent to Blue Cross Medicare Advantage HMO address that should have been sent to Renaissance, the claim will be rejected and you will receive notice to re-file it with the appropriate IPA or Medical Group. Types of services that should be submitted to Renaissance:
• All Physician Services
• Outpatient diagnostic testing
services
BCBS MA Professional Claims Should Be Submitted to RPO:
Certain types of services must be submitted to BCBSTX rather than to Renaissance Physicians. When a claim is sent to Renaissance Physicians that should be sent to BCBSTX, the claim will be rejected and you will receive notice to re-file it with the appropriate IPA or Medical Group. Types of services that should be submitted to BCBS MA:
• Institutional Claims
BCBS MA Institutional Claims Should Be Submitted to BCBS MA HMO:
Electronic Payor ID Availity: RENGQ (HCFA Only) or Emdeon: 76066 (for HCFA and UB-04)
Billing Address RPO Claims PO Box 2888 Houston, TX 77252-2888
Provider Service 877-774-8592
Billing Address: Blue Cross Medicare Advantage HMO c/o Provider Services PO Box 3686 Scranton, PA 18505 -9998
Electronic Payor ID Availity 66006
Customer Service 800-282-4548
170

BCBS MA 2019 Rewards and Incentives program: MAPD members will be eligible to receive rewards for closing certain HEDIS GAP metrics. Healthy Actions that will be awarded in 2019 include:
� Annual Wellness Visit � Annual flu shot � Completion of the Health
Questionnaire
� Colorectal cancer screening � Retinal eye exam � In Home Assessments (for
applicable members)
� Mammograms for women � DA1c and Nephropathy testing for
Diabetics only
� Online logging of fitness activity for an average of 2 days/week for 12
weeks (so 24 times in 84 days) for
non-Diabetics.
� Fall Risk Assessment for all members
� Bone Density Screening for women
2019 Participants: � Who registered in 2018 will not
need to re-register for the program.
� Will be asked to answer a few health related questions during the
onboarding process, as this helps
optimize the content that a
member’s portal will display.
� Care Plans (devised off of a proprietary model) will consist of
relevant Healthy Actions and
educational tools designed to help
a member improve their health.
Registration & General Program Rules: � Registration is required to
participate. Members can sign up
at BlueRewardsTX.com.
� A member will continue to be eligible for a maximum of $100 in
gift card rewards annually. Each
Healthy Action will trigger a $25
award. One reward per healthy
action per year.
� Online members can choose an e-card to be sent to their personal
email accounts and to their
message center within the portal;
while offline members will need to
select a physical gift card to be
mailed to them
Annual Health Assessment Providers will be paid for performing annual health assessments on aligned patients. Payments will be made for one Annual Health Assessment per member per calendar year. Payments will be made on a quarterly basis to provider offices participating in the initiative. Quarterly assessment
171
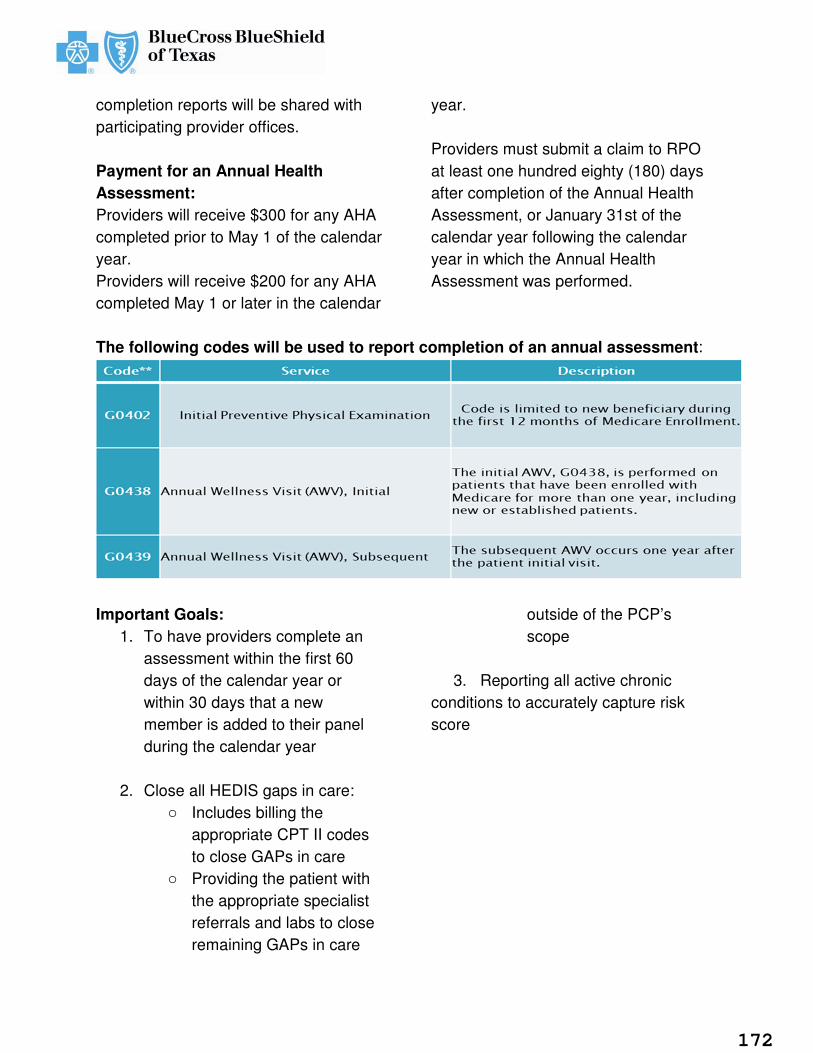
completion reports will be shared with participating provider offices. Payment for an Annual Health Assessment: Providers will receive $300 for any AHA completed prior to May 1 of the calendar year. Providers will receive $200 for any AHA completed May 1 or later in the calendar
year. Providers must submit a claim to RPO at least one hundred eighty (180) days after completion of the Annual Health Assessment, or January 31st of the calendar year following the calendar year in which the Annual Health Assessment was performed.
The following codes will be used to report completion of an annual assessment:
Important Goals:
1. To have providers complete an assessment within the first 60 days of the calendar year or within 30 days that a new member is added to their panel during the calendar year
2. Close all HEDIS gaps in care: o Includes billing the
appropriate CPT II codes to close GAPs in care
o Providing the patient with the appropriate specialist referrals and labs to close remaining GAPs in care
outside of the PCP’s scope
3. Reporting all active chronic conditions to accurately capture risk score
172

Living 365 Program
Living 365 Program offers programs to
help members live healthier lives by
providing educational information and
discounts on health and wellness products
and/or services.
Discounts include:
• Diet and Weight Control Programs
• Elder Care Support Resources
• Laser Vision Correction Services
• Other Weekly Special Deals
-No claims to file, no referrals, and no
additional fees to participate.
PAVE Program
PAVE Program is in partnership with HEB
Pharmacy and Albertson’s (Amigos,
Market Street, Randalls, Sav-On, Tom
Thumb, United) Pharmacies in which local
pharmacists are treated as a clinical
extension of the health plan. The program
drives to improve medication adherence,
decrease utilization of high risk
medications and other clinical
interventions, which include pharmacy
gap in care closures and conversion of
brands to generics. The program is
currently in place for Medicare Advantage
members utilizing Albertson’s and HEB
Pharmacies.
To learn more visit: Blue365 Texas
173

Blue Cross Blue Shield Medicare Advantage Key Contacts
Provider Finder (Professional Services only)
www.myrpo.com
General Provider Service Line (claims, benefits, referrals)
1-844-343-9753
Disease and Case Management Programs
855-390-6567
Mental Health and Chemical Dependency
1-800-327-9251
Durable Medical /Home Health
877-774-8592
Labs
Quest Labs 1-888-277-8772
QuestDiagnostics.com/patient
Dental Networks of America
877-774-8592
Provider Referrals (Professional Services only)
Done via HSC
iExchange (Institutional services only) Web-based application used to submit transaction requests for inpatient admissions and extensions, treatment searches, provider/member searches, referral authorizations and select outpatient services and extensions.
iExchange Web Application: bcbstx.com/provider
iExchange IVR: 877-774-8592
(Mon – Fri, 8am–5pm)
iExchange Help Desk: iexchangehelpdesk@bcbstx,com
eviCore Preauthorization (Certain Institutional Services only) (eviCore will do pre-authorizations for certain professional services; see the link below for services) Pre-Auth CPT Codes/Services Through eviCore
eviCore Healthcare Web Portal https://www.evicore.com (phone)855-252-1117
174

BCBS Commercial Plan Blue Value Base Incentive Plan (VBIP)
Please note that we have two membership populations for Blue Cross Commercial:
• Blue Advantage HMOSM
• Blue Choice PPO SM
Please note there are separate Quick Reference Guides for each population included at the end of this section. Value-Based Care Programs
Value-based care (VBC) programs redefine how BCBSTX and its provider partners collaborate. These models introduce new performance measurements, as well as new compensation processes. The BCBSTX VBC model seeks to partner with providers that deliver sustainable improvements to member care while better managing health care costs. By shifting provider relationships towards VBC models, BCBSTX intends to increase the value of health care services. BCBSTX expects to achieve this through increased collaboration with its provider partners. The VBC programs are supported by:
• Defining financial incentive models that align the interests of all parties around improving patient care and population health, and, • Improving coordination between providers and BCBSTX to reduce cost trends without reducing the level of benefit coverage or the options available to attributed members. Some VBC programs consist of attribution, financial performance targets, quality improvement targets, financial incentive reconciliation, data exchange and reporting. An ACO is a specific type of VBC program.
What is an ACO?
An ACO is a collection of providers that agree to coordinate care across a continuum of health care settings to improve quality outcomes and cost efficiencies. The ACO model is intended to improve members’ health and experience of care while reducing costs by avoiding unnecessary hospital admissions, readmissions, emergency room visits and duplication of services. ACOs center on addressing the health needs of broad member populations while holding providers within the ACO accountable for quality and cost efficiencies delivered for their members – the attributed cohort. BCBSTX supports the ACO by providing information about the attributed cohort that gives providers a more comprehensive profile of the members’ care.
To achieve its goals, the ACO model uses a multidisciplinary approach to better coordinate care, improve quality and reduce costs, which involves provider leadership, primary and specialty care providers, clinical teams, and the member and his or her family.
ACO Attribution Logic and Methodology
BCBSTX identifies members who qualify for inclusion in an ACO during a process called attribution. For purposes of this manual, Health Care Service Corporation (HCSC) includes BCBSTX. HCSC fully insured members, HCSC members from participating self-funded accounts, as well as participating BlueCard members are available for attribution. The BlueCard program enables our members to obtain health care services while traveling or living in another Blue Cross and/or Blue Shield Plan’s service area.
The attribution process runs monthly and includes the following steps: 1. Develop and maintain ACO information used to drive the attribution steps. 2. Identify the provider entity with the strongest relationship to a member. 3. Apply member eligibility requirements. 4. Establish the ACO’s reference population. ACO Financial Performance Measurement and Reports The ACO is measured for financial performance against a BCBSTX-established methodology to compare the actual cost-of-care changes during the performance period against the baseline period in order to determine the earned incentive in accordance with the terms of the Agreement. BCBSTX refers to this methodology as the Adjusted Provider Performance Measurement (APPM). The APPM Model APPM uses statistical regression calculations to create a risk-adjusted performance target for the ACO financial performance. It is designed to measure the cost trends in an ACO attributed cohort over time relative to cost trends that would be expected for the ACO cohort if it were not attributed to the ACO. Establishing an expected cost is critical to setting a benchmark for ACO performance. APPM involves a statistical regression formula that generates an expected medical cost for the ACO attributed cohort based on age, gender and medical conditions. APPM uses the reference population to generate the coefficients for age, gender and medical conditions. These coefficients are then applied to each ACO member based on that member’s specific age, gender and medical condition information to create a cost prediction for each member.
175

The ACO population’s expected cost is the average expected cost of the ACO attributed cohort. This is the same type of predictive modeling technique used to set expected costs in government risk adjustment programs such as Medicare Advantage, the Medicaid Chronic Illness and Disability Payment System model, and the Affordable Care Act risk adjustment model. Expected values are not deemed as reliable as individual person predictions but, rather, they produce reliable population cost predictions as the measured population grows larger. The APPM groups age and gender information into categories and diagnosis information into medical condition categories using AHRQ Clinical Classification System (CCS) diagnosis grouper - level 2. These categories are established in advance by AHRQ and are not subject to manipulation by BCBSTX when calculating performance. The categorization is necessary for the statistical technique to function properly. The benchmark value represents what the ACO attributed cohort would be expected to cost based on age, gender and medical condition information. ACO Inbound Data In order to support the ACO’s success with population health management activities, BCBSTX shares its confidential and proprietary attributed membership information, medical and pharmacy claims, and pre-authorization information with the ACO on a limited-use basis subject to restrictions, terms and conditions set forth in the Confidential Data Release Agreement (CDRA) between the ACO and BCBSTX. A standard CDRA form is provided by BCBSTX. The CDRA must be executed prior to the exchange of any data associated with the attributed population. ACO Outbound Data The ACO is required to electronically submit and share data, including supplemental clinical data as shown below:
• File Type: Supplemental File (Quality Data)
• Description of File: The supplemental file contains clinical data not available in claims data. This data allows BCBSTX to provide quality metric reporting to ACOs on those measures that require clinical-type data.
A complete set of technical specifications, including data dictionaries that define the data elements for each file, is provided to the ACO by BCBSTX.
Supplemental Clinical Data
BCBSTX uses medical claims data, along with supplemental data. If no medical claims data is available, BCBSTX uses only supplemental data provided by the ACO.
BCBSTX requires the ACO to electronically submit supplemental clinical data for the following quality metrics no later than 60 days after the performance period ends:
� Quality Metrics:
o Comprehensive Diabetes Care - HbA1c Control (<8.0%)
o Comprehensive Diabetes Care - Blood Pressure Control (<140/90 mm Hg)
Member Experience Data In most instances BCBSTX selects and pays for a vendor to administer and report results from the CG- CAHPS® member experience survey in the fourth quarter of each calendar year. BCBSTX uses the results for the three quality metrics below:
• Follow-Up on Test Results
• Getting Timely Appointments, Care and Information (composite)
• How Well Providers Communicate with Members (composite)
ACO Quality Performance Measurement and Reports The ACO is measured for quality performance using a maximum of 18 metrics from National Committee for Quality Assurance’s (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS), Agency for Healthcare Research and Quality (AHRQ), and The Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS®) survey. BCBSTX contracts with NCQA-certified vendors to calculate and audit the ACO’s performance results for HEDIS and AHRQ metrics. Note: Results for ACOs with a July 1 effective date cannot be audited because the measurement year is not a calendar year as required by HEDIS and AHRQ. If an agency discontinues any metric, BCBSTX discusses replacement options with the ACO. Also, BCBSTX can take into account extenuating circumstances beyond the ACO’s control that result in a decline in the results for a particular metric, e.g., vaccine shortage. VBIP Quality and Member Experience Metrics Summary See table on following page for quality metrics. Care Management Programs
• Complex & Comprehensive Case Management: For members who have complex medical needs and require a wide variety of resources to manage health and improve quality of life
• Condition Management: Disease specific case management
• Lifestyle management: Weight management and smoking cessation
• Special Beginnings and High Risk Pregnancy: Uncomplicated and high risk pregnancy support
176

� � � � � � � �� � � � � � �� � � � � � � �� � � � � � � � � � � � �� � � � � � � � �� ! � " � #� � � � � � � � �� � � $ � � � � � % � � � & �� � � � � � � � �' � � � � � � � � � � � � � � � � � ( ) � * �� + � � � � � � , � � � � � � � �� � � � � � � � � - ' � � � � � � � % � � . � � � �$ � � � � � � � � � � � � � � � / � � �0 � � 1� � � $ 2 3 2 3 2� � � � � 2 4 � � � � 5 6 � 7 � � 8 9 "� � � � ( ) � * �� � � � � � � �� � � � � � � � $ � �� � � � � �� � � � � � � � �� � � � � � � � � + � � � � � %8 9 " 9 ( : � # �- � � � � � �� � � � � � � �� � � 1 � � � � �� � � � � � �� � � � ; � � � �� � � � � � � � < = > � � � � � � � $ � � � � � � � � � � � ( )? � ( ) � � @ � ) AB B B C 1D E F G H I F J K F GL M N I M O P N O F N K
7 � Q # : R � # � S ) � # 9 " )� ( ) � * � T 7 U � � � � �� � � � � ( ) � * � T 7 U � �� � � V � � � W 1 � � < � � � � � � � � � � �� � � � � � � � V � � � � � � � % � � � � � � � 1# � 9 S � " ! � 6 X � " � � Y Z # � Y� ( ) � * � T 7 U � � � � � � � � � � � � � � � V � 1 1 � � � %� � � � � � � � � � � � � � � � � � � ; � � � $ � � � � $ � � � � � � � � � � � � � � � � � � � � �T 7 U � � � 1 � � � � � $ � � � � � � � � ( ) � * � T 7� � � � � � � � � � � � $ � � � � � � � � � � � � � � � � � � � � � �� � $ � � � � � $ � � � � � � �� � � � � � � � � � $ � � � � � � � �� � � � � � � � � � � � � � � � � � � � [ � � � / � � � � \ � < 2 ] � � � � � � � � < ^ \4 � � � � � � < � % � � � & � � � � % � $ � �" 9 ( : � # � � � � � � � � � 1 � �T 7 U � � � � � % � � � �� � � ( ) � * � T 7 U � � � � � �� � � � � � � � 1 � � � � � � � � � � � < � � � � � � �� � � � � � � � � � � � � � � � � � � � � � � � � � � 1 ' �% � � . � � � � � � � � � � � % � � � 5� � � � � V _ _ _ W ` _ 2� � � � � � � � ( ) � * � T 7 U� � � � � � � $ � � � � � � � � � � � � � � � � � � � � � � � � � � � � ; � a 0 � � � � � � � � $ � �� � � � � � $ � � � 1� ( ) � * � T 7 U � � � � � � � � � � � � � � � � � � � � � � � $ � � � � � � �) � * � T 7 U a 0 � � � � � �A # b Y � ! � # 9 S � � c d dF N e K N J K J e P f K I G K J g P hK M e f i f G e j k i P l m n h P o F J K h
) 9 S " � � ( � Y� ) �� � � � �� � � �� � � � � $ � � � � W � �Y � # # � � ) � � �% & � W �� � 1� � � � � � � � � �7 U� � � � � 1� � p � $ p� � � � � � � � � �\ q� � � � � ��� � �� � � � � � �� � � � � � � � �� 5 6 � 7 � �p r s t _ 1U � � � � � � � � �� � � � � �� $ � � 1 - � �� � ; �� d Z c u d Z
v � < � � � � �� � � � �� � % � �� � � � � � �� � � � � � �c d� � � ,� � � � � < � � �� � � � � %' � � w �� � � � ( ) � *, � � � � xc d d8 � # 9 Y 9 S �� � ! 9 ( 9 " ) #y � � ( " z� � � S � � 9 !� � � S ) # ( 9 Sv � � � � � � �a $ � � � �� � � � � � � � $� � � � $ � � � � � �� 1 q' {� � � � �� � � � $ � �� � � � � �$ � � � � � � � < � � $ � �� � � $ � � � � � � � � � � �� � � � � � � � � � � � �� � � � ( ) � *� � � $ � � � � � � � � � � �� � � � � $� � � � � � � �� � � � 1| } ~ � � � � � �� ~ � � � � � � �� � � ~ � � � � � ~ � �� � � � � � � � � � �� � } ~ � � � � � �� ~ � � � � � � �� � � � � � � �� I F i � h K g K h K N i K M N J l M �h � � � � � � � � � � � � ¡ � ¢ £ ¤
¥ ¦ § ¨ © ª « ¦ ¬ ¦ ¦ « ¦ § ® © ¯ « ° ¦ ± ¨° § ² ¨ ³ ´ µ ¶ ´ ¦ ¥ ¦ · ° § ¦ ³ ¸¹ º » ¼ ½ ¾ ¿ ¼ ¿ À Á ¹ Á ¼ À Â Ã Ä » ¹ Á¾ ¹ » Á ¼ ¿ ½ ¹ Å Ã Â Æ Ç Å » È » Á É Á ¹ ºÈ ¿ ¼ ½  à  À º Â Æ Ã Ê Å Â Á Ê ¿ ° ¸ § ° ¬ ¶ Ë Ì Í Î Ã Â È Á ½ ¿ ÃÃ Ï ¿ Ã È Á Ê ¿ ÐÑ Ñ Ò Ó Ô Õ Ò Ñ Ö × Ø ÙÏ ¹ » ¹ Æ Ú Ä » º ¾ ¿  ¾ ¹ » Á ¼ ¿ ½Å ¿ Û È » Á É Á ¹ º Ü É » Á Ä Ý ¿ Ú ¿ »Þ ¿ ¾ È ¿ ¼ ½  à  À º Â Æ Ã Ê Å ÂÚ ¹ » Ê É » Á Ä ß Ê » É É à « ² ¶¬ ¶ Ë Ì Í Î Ã Â È Á ½ ¿ Ã Ü Æ Ú ¹ ÂÑ Ò Ó Ô Õ Ò Ñ Ö × Ø Ù° § ¦ ³ ¸ á ³ ¶ ¨ ¸ ³ § ° â â « ® §´ ° § ¦ ã ¶ ¨ ¶ ´ ã ¦ · ¶ ¨ ³ ¸ « ® ä å± ¨ ¨ æ ³ ² « á ¶ ¨ ² ± ¦ § §· ° « « ® ç à « ² ¶ å á ã ° ¸ § ° ¬ ¶Ê Î » º  à è é Ð × Ó ê × ÑÅ º Ú Á Ê Á » ¼ ß ë à  À ¿ Ú Ú Á  ¼ » ÉÀ » Ê Á É Á ¹ º  à » ¼ Ê Á É É » à º ë à  Ȼ ë » ë ¿ Ã Ê É » Á Ä ß Ä » Á É Ê É » Áå á ã ° ¸ § ° ¬ ¶ Ë Ì Íì í î  ï ð ð ñ ñ ò ò é » É É » Ú ßó ô õ ö ð ð ÷ ñ ñ ò òÄ Æ Ú ¹ ¾ ¿ Ú Æ ¾ Ä Á ¹ ¹ ¿ ½ Þ Á ¹ Å¿ ½ » ¹ ¿  À Ú ¿ Ã È Á Ê ¿ í Ü É » Á Ä ¹ Ú Æ ¾ Ä Á ¹ ¹ ¿ ½ Þ Á ¹ Å Á ¼ Õ × Ñ½ » ¹ ¿  À Ú ¿ Ã È Á Ê ¿ » à ¿ ¼  ¹Ã à ¿ Á Ä ¾ Æ Ã Ú ¿ Ä ¿ ¼ ¹ í Î Å º Ú¼ » É ë Ã Â È Á ½ ¿ Ã Ú ß À » Ê Á É Á ¹ º  Ãë Ã Â È Á ½ ¿ Ã Ú Ä Æ Ú ¹ Ú Æ ¾ Ä Á ¹ »Ê É » Á Ä À  à » ¼ º Ú ¿ Ã È Á Ê ¿ Ú¹  » Ä ¿ Ä ¾ ¿ à í à « ² ¶¬ ¶ Ë Ì Í ë Å º Ú Á Ê Á » ¼ Ú ß¼ » É ë Ã Â È Á ½ ¿ Ã Ú ß À » Ê Á É Á ¹ º  Ãë Ã Â È Á ½ ¿ Ã Ú Ä » º ¼  ¹ Ú ¿ ¿ øÀ Ã Â Ä ¹ Å ¿ Ä ¿ Ä ¾ ¿ à À Â Ã Ê É» À ¹ ¿ à ¹ Å ¿ Õ × Ñ ½ » º À Á É Á ¼ Çù ú û ü ý ü þ ü û ü ÿ � � � � þ ú � ú � ü ÿ ù� � ú � � û û ù � þ ù � � ü þ ú � ù ü � ú � ù � þ ù � � ü þ ú � ù � ú � � þ ü � ÿ � ú ÿ � �ÿ � � û � ü � � � � � � ù ÿ � � �� � � ÿ � � û � � � þ ú � � � û � ü �� � � � � � � � � � � � � � � � � � � �¤ � £ � ¤ � ! " # " $ " % & % ' ( ) *
+ , - . / 0 1 2¨ ¯ « ° ¦ ±3 ¶ ã ¦ ¶ 4å « «¯ ³ ´ ´ ¶ ¨Â ¼º í Ê Â ÄÂ Ã Ê » É É½ » Ã Ê Å Á Ê ¿ íÂ Ä ¿ ç ³å 5 Í 6§ ¶ á¶ Ë Ì ÍÈ Á ½ ¿ ÃÄ ¹  ÐÅ Á ¼ Õ × ÑÄ ÚÑ ½ » º ÚÚ Á Ê Á » ¼ Ú ßà »Ãø » Á Ä ÚÇ ù � ú �
Ü É » Á Ä Ý ¿ È Á ¿Ü  à à ¿ Ú ë  ¼ ½ ¿ ¼¾ ¿ Ú ¿ ¼ ¹ ¹  Ðà « ² ¶ å á ã ° ¸ § ° ¬Î í ì í î  ï ð ð ñ ñ òé » É É » Ú ß 7 óô õ ö ð ð ÷ ñ ñ ò ò7 Å ¿ Ü É » Á Ä ÝÀ Â Ã Ä Þ Á ¹ Å Á ¼ Ú ¹ ÃÉ Â Ê » ¹ ¿ ½  ¼ ¹ Å ¿Þ ¿ ¾ Ú Á ¹ ¿ о Ê ¾ Ú ¹ ï í Ê Â Ä 8 ë à ÂÊ É Á Ê ø  ¼ ¹ Å ¿ 9 ½» ¼ ½ Ý ¿ À ¿ à ¿ ¼ Ê ¿¹ Å ¿ ¼ Ê É Á Ê ø  ¼ :
� � � � ; ; � < � � � � � < = � � � � � > ? �* @ A B C * D ) E ) D # " F ) C % D G % D
2 H I 2 J . K L M N
O
±4 ¨ ©¨ â ³ ¸ P ´ ¶ ° ² §à ¶ ¸ ¶ ¥ ¦5 ¶ ´¿ Þ Ú » ¼ ½¼ Ê ¿ Ú Å Â Æ É ½¬ ¶ Ë Ì Íò òÝ ¿ È Á ¿ ÞÃ Æ Ê ¹ Á  ¼ Ú Á Ú¿ î Ü î Ï 7 óÂ È Á ½ ¿ ý Æ Ê » ¹ Á  ¼¿ ¹ » ¾ ß: Â Ã Ä ÚÛ Ê Ê ¿ Ú Ú» ë ë É Á Ê » ¹ Á ÂÞ ¿ ¾ Ú Á ¹ ¿ »Å ¹ ¹ ë Ð 8 8 Þ Þ¹ Â Â É Ú 8 Á ¿ ï ʳ ´ Ê » É É ¹ Å ¿Q  Á Ê ¿ Ý ¿ Ú× Ñ Ñ Ò Ó Ô Õ Ò ÑÜ Æ Ã Ã ¿ ¼» ¼ ½ ¹ Å ¿ Á û È » Á É » ¾ É ¿Á 9 ï Ê Å » ¼ ÇÎ Ã Â È Á ½ ¿ à ::  à R ƹ Å ¿ Á 9 ï Ê Å× Ñ Ñ Ò Ø Ó S Ò Ó: Â Ã Ê » ÚÊ Â ¼ ¹ » Ê ¹ ¹ ÅT » ¼ » Ç ¿ ÄÖ Ø Ñ Õ í:  à à ¿ ÀÀ Â Ã Ú ¿ É ¿ Ê ¹ë à ¿ » Æ ¹ Š û ½ Ä Á Ú Ú Á  ¼Þ ¿ ¾ ë » Ç ¿Å ¹ ¹ ë Ð 8 8 Þ Þ ÞÂ É Ú 8 Á ¿ ï Ê Å »� U � ÿ ú V WX � ú � � ÿ �U � ÿ ü � ü � � ÿY ú Z � ü � úû ú � ÿ [ ù ü � úY ú ù � � � �³ ´ à ¿ À ¿ à ¹ Â\ À Â Ã Ä ¿ Ã É ºî É Æ ¿ Û ½ ÈÎ Ã ¿ Ä Á ¿ à ÎÚ ¿ Ê ¹ Á  ¼ Ú:  à ë à ¿Â Æ ¹ ë » ¹Ç ¿ ¼  Äà » ½ Á » ¹ Á¿ È Á Ü Â Ã] \ ^ õ õ _� < ` � � � � � � ` � � � � < = � � � � � aD * A " % & b * c d A d * @ e ) f * @ g )
N h i - j k l m . n . o § æ ¨ © Í ¸ « ¦ ¸ ¶ å â â ´ ³ ã ° «§ ¨ ¥ ³ ´ 5 ¶ « ¶ · § Í ² § â ° § ¦ ¶´ ã ¦ · ¶ ¨ ° ¸ á p ¸ â ° § ¦ ¶ ¸ §å á ± ¦ ¨ ¨ ¦ ³ ¸ ¨Ú ¹ Å ¿ Á 9 ï Ê Å » ¼ Ç ¿ q ¿ ¾Â ¼ ¹ Å Ã Â Æ Ç Å ¹ Å ¿ î Ü î Ï 7 ó» ¹Þ í ¾ Ê ¾ Ú ¹ ï í Ê Â Ä 8 ë Ã Â È Á ½ ¿ ÃÊ Å » ¼ Ç ¿ í Å ¹ Ä É¿ Á 9 ï Ê Å » ¼ Ç ¿ è ¼ ¹ ¿ à » Ê ¹ Á È ¿Ú ë  ¼ Ú ¿ \ è Q Ý _ Ï º Ú ¹ ¿ Ä »Ñ Ö × Ø í¼ ¹ É Á Ú ¹ Á ¼ Ç Ú Â À ë Ã Â È Á ½ ¿ à Úr Î è ¼ Æ Ä ¾ ¿ Ã Ú » à ¿Â ¼ É Á ¼ ¿ ¹ Å Ã Â Æ Ç Å ¹ Å ¿¿ q ¿ ¾ » ë ë É Á Ê » ¹ Á  ¼  Ã: Á ¼ ½ ¿ à s í¿ Ú ¹ Á  ¼ Ú Â Ã ë à  ¾ É ¿ Ä Ú ß Ê »» ¼ Ç ¿ Ï Æ ë ë  à ¹ é ¿ Ú ø » ¹Ó S Õ Ó íÚ ¿ Ä » ¼ » Ç ¿ Ä ¿ ¼ ¹  à ¹ ÂÅ ¿ T ¿ ½ Á Ê » É Ü » à ¿Ä ¿ ¼ ¹ é ¿ ë ¹ í ß Ê » É É × Ô Ô Ò × ê SÀ ¿ à à » É Ú ß » ë ë Ã Â È » É Â À ¾ ¿ ¼Â Æ ¹ ë » ¹ Á ¿ ¼ ¹Ã Á t » ¹ Á  ¼ Ú » ¼ ½ Á ¼ ë » ¹ Á ¿ ¼ ¹¼ Ú ß Ã ¿ À ¿ à ¹  ¹ Å ¿ Á 9 ï Ê Å » ¼» ¹Þ í ¾ Ê ¾ Ú ¹ ï í Ê Â Ä 8 ë Ã Â È Á ½ ¿ à 8» ¼ Ç ¿ í Å ¹ Ä ÉW û ü � u ÿ � ÿ � ú� � ü v � ÿ ü � � wÿ ü � � w Y ú � ú � � � û� ú � ÿ ù x ü ù ÿ ü ù û � � � ÿ ú � ü �� � � ü ý � ÿ ü � � � � � ú � Y ú û �� ú ù y ¹ Å ¿ î É Æ ¿ 9 Ú Ú ¿ ¼ ¹ Á » É Úz T ì î É Æ ¿ 7 ¿ ï » Ú Ï T _ ß» ¼ ¹ » Ç ¿ z T ì » ¼ ½ î É Æ ¿Î Ã Â È Á ½ ¿ à T » ¼ Æ » Éé » ¼ ½ 9 í¿ » Æ ¹ Å Â Ã Á t » ¹ Á  ¼ À  ù Á ¿ ¼ ¹ Ä Â É ¿ Ê Æ É » à » ¼ ½Ä ¿ ¹ ¿ Ú ¹ Á ¼ Ç » ¼ ½ Â Æ ¹ ë » ¹ Á ¿Â ¼ ¹ Å ¿ à » ë º ß Ê Â ¼ ¹ » Ê ¹Ã ¿ » ¹ Þ Þ Þ í ¿ È Á Ê Â Ã ¿ í Ê Â Ä_ ö õ ö ÷ ] ] ] ô í< � � � < � � � � � { | } ~ � � � �) $ ) D # ) C % � G * & � b * & � & �
o . H k . � - j 0 . � � ³ ¥¶ ¸ § � ° ³ ´ ° § ³ ´óà 8¿ » ¹Ê » É ÉS Ò¼ ¿ À Á ¹ Ú¼ Ç ¿8 ¹ Â� ÿ � ú� ÿ ú �ß¿ ¿ ¼ ¹Ä  Ã
� ° ³ ´ ° § ³ ´ ® 5 ¶� Æ ¿ Ú ¹ é Á » Ç ¼ ÂÁ Ú ¹ Å ¿ ¶ � · « ² ¨ ¦ ãà « ² ¶ å á ã ° ¸ § °» É É Â Æ ¹ ë » ¹ Á ¿ ¼ ¹ Êà ¿ À ¿ à ¿ ¼ Ê ¿ É » ¾ ÂÚ ¿ Ã È Á Ê ¿ Ú í: Â Ã É Â Ê » ¹ Á  ¼ Ú ÂR Æ ¿ Ú ¹ Á  ¼ Ú ß Ê Â ¼» ¹ × × × Ò Ö Ø Ø Ò × Ø� Æ ¿ Ú ¹ � Ú Þ ¿ ¾ Ú Á� Æ ¿ Ú ¹ é Á » Ç ¼  ڹ Á ¿ ¼ ¹
� � � � ; � � � � ` ~ � � � � ` � � � � �� ) G ) & � ) & A e " F ) & $ ) ) % ' A B
� � � � + � � � M L L ´ ® 5 ¶ ´ ã ¦ · ¶ ¨ à ¶ä Ì ¶¶ ´ ã ¦ · ¶ ¨Â Ú ¹ Á Ê Ú ß è ¼ Ê íã ¶ É » ¾ À  ð ¬ ¶ Ë Ì Í À  ÃÊ É Á ¼ Á Ê » É à » ¹  à ºÂ ü ¹ » Ê ¹ � Æ ¿ Ú ¹Ø Ø Ö © ³ ´ È Á Ú Á ¹Á ¹ ¿ » ¹ ÐÚ ¹ Á Ê Ú í Ê Â Ä 8 ë »TÎ Ã Â È\ T » Ǿ ¿ Å »Å ¿ » ɽ ¿ ë ¿å á ã7Ê Å ¿ ÊÊ É » Á ÄÈ ¿ à Á À× Ñ Ñ Ò7 ÅÎ Å º ÚÅ ¿ » ÉÊ Â ¼ ¹ë à ¿ »ë » à ¹ ÁÂ Æ ¹ ëÚ ¿ à ÈΠ¾ ¹ »Â À Ê »Ú ¿ à È7 Åë à  À ¿Ã ¿ Ú ëT » Á É ÊT »Î à Â� � � �� þ ÿ �� û � ü �� ú � �
� � � { | } � � � � � � ¡ ¢ £ ¢ £ ¤¥ ¦ § ¨ © ¦ ª « ¬ ® ¯ ° § ¨ © ¦ ±
² ³ ´ µ ¶ · ¸ ² ³ ²¹ º » ¼ ½ ¾ ¿ » À Á ¹ » À  º à ¹ ¿ ¼¹ Ä Â » À Á ¹ » À  º » Ä Å Æ º ¹ ÇÈ ¹ É ¹ Ä Å ¹ Ä Ê Ë ÌÍ Î Ï Ð Ñ Ñ Î Ò Ó Ð Ô Î Õ Ö × Ø Î Ñ Ù ÐÕ Ö Ú Ð Ø Û × Ü Ý Ð Þ Î Û ß à Ò á âÏ Ð Ñ Ñ Î Ò ã á × × Ø Ú Ö Ò Î ä Ð Û Î Ñ ÑÎ Õ Ö × Ø Î Ñ Ô Ð Î Ñ ä Ô å æ Ð Ò ä Î ÑÑ ä Ô Î Ò Ú á Ô Ð æ Ö á Î ÑÐ Ò Ú Ð Ò á ç ã Û Ð Ø Õ Ö á Ð Û Ü × Ø è¼ » Ä Â » é ¹ Á ê ë æ Ð æ ì Ð Ø× × ì ä Î Ö Ò í Ø Ð Î î ä Ô × Ø Ö ï Î ä Öá ð ì Ð Ò Ð Ü Ö ä Û ß Ð Ñ Ö Ï Ö ì Ö Ñ Ö ä ç ßæ Û Û ä Î ä î Û ñ í Ø × ì Ñ Ð æ Û × ØÜ Ö á Î ä Ö × Ò ß á Î Ñ Ñ Í Î Ï Ð Ñ Ñ Î Ò Îò ó ô õ ò ô ö ô ô ÷Ô Ð í Î ä Ö Ð Ò ä ß ø Ø Ö æ Î Ø ç ù ÎÛ Ö á Ö Î Ò å ø ù ø ã × Ø ì Ð Ô Î Õ ÖÑ ä Ô í Ø × Ü Ð Û Û Ö × Ò Î Ñ æ î Û ää Î á ä Í Î Ï Ð Ñ Ñ Î Ò ä ×Î î ä Ô × Ø Ö ï Ð Î Ñ Ñ Ö Ò í Î ä Ö Ð Ò ä ßÖ Î Ñ Ô × Û í Ö ä Î Ñ Ö ï Î ä Ö × Ò Î Ò Úí Î ä Ö Ð Ò ä ì Ð Ô Î Õ Ö × Ø Î Ñ Ô Ð Î Ñ äÕ Ö á Ð Û âØ Ð Î î ä Ô × Ø Ö ï Î ä Ö × Ò æ î Û ä ìÎ Ö Ò Ð Ú ú û ü ý û ä × ä Ô Ð Ú Ð Ñ Ö Õ ÐÎ Ø Ð Ü × Ø ì Ð Ô Î Õ Ö × Ø Î Ñ Ô Ð Î ÑÕ Ö á Ð Û âÔ Ð í Ô ç Û Ö á Ö Î Ò × ØÐ Û Û Ö × Ò Î Ñ í Ø × Õ Ö Ú Ð Ø Ö Ûí × Ò Û Ö ì Ñ Ð Ü × Ø Ü Ö Ñ Ö Ò Ï á Ñ Î Ö æ Ûá Ñ Î Ö æ Û ä × þÎ Ï Ð Ñ Ñ Î Ò Ó Ð Ô Î Õ Ö × Ø Î Ñ Ù Ð Î× Õ Ö Ú Ð Ø Û × Ü Ý Ð Þ Î Û ß à Ò á âÿ ä ä Ò þ ù Ñ Î Ö æ Ûø â � â Ó × Þ � � � � Í Î ØÙ Ð Ö Ï Ô ä Û ß Í � � � � � �� � � � � � � � � � � � � � �� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ! � � � � � � � � � "¤ � # $ % & � � $ £ ¢ ' � # $ ( ¤ & # )± ¥ * ¦ ¨ ° + ¬ , * ® - * ¬ ¯
² . ³ ´ / 0 ¶ 1 2 3 4 56 2 3 7 89 : ; <= 8 > 4? @A B C9 ;D EA D 9 :<EE D F; <? @: ; <D F : 9 B GH I J K LM I NO P Q R S T U V Q
177
W X Y Z [ [ \ ] ] \ ^ _ ` _ a _ ^ _ b
c d e f g h i j k l m n op q r s t u v w x yz t { | } t v w q ~ �� � ~ � ~ } ~ � ~ v | � } x �� v ~ � ~ � x v w x ~ � �� ~ v w ~ � � � w t �� g m � � � � h � � � � � �p � � � � � ~ y q q w t� � t u q � {� � t u q � {� � t u ~ � s t� � { x u � � � ~ y q yp � � � � � ~ y q y � q� � { � ~ � � v x � � � ~� s q x u � ~ � x q � u xq x u � ~ � x � � � v w� w | q ~ � ~ � � p q q ~� � � l � k i � � i � � � kp y ~ � ~ y � y t s� � w | q ~ � � � � �� u t � { { u � � v ~ � ¡ ¢ � u t � ~ � x u£ z £ ¤ ¥ ¦ � ~ � � � t§ x v u t � � v ~ � x � u§ x v u t � � v ~ � x � x� x � � | q ~ � q v � v �� s v w x { u t � ~ � x� t u � u t � ~ � x u §f g h i � m � k ¨ © h o �¥ t � w x � r } x � x� ~ � x � � � v w � v ~ � �� ~ � x � � � t v w x u �� t u q v � v � q t s �f g h i j k l m n o m ª ip � � t � v { � v ~ x � v � � ~¥ w x j « « � � k m � g i �{ u x y ~ � y ¬ � m � i � i � � � k® ¥ w x v w u x® ¥ w x w x �® � � u ~ � � v® � s � y x y® � t u � � � ~¯ � ° ° � g g f � f® � � ~ � ~ } ~ � ~ v |± ² �³ ² � �´ ² �® § x y ~ � � x± ² � µ ¶ · ¸ ¹ º » ¸ » ¼ ½ ¾ ¿ À ¶ Á  à  ¿ ¾ Ä ·
Å Æ Ç È É Ê Ë Ì Í Î Í Ï Ð Ñ Ò Ó Ô ÕÒ Ö × Ò Ø Ù Ú Û Ü Ô Ý Ø Þ Ý ß ß à Ò ßÒ Ú Õ á ß à Ò Ö Ò Ö × Ò Ø Ù Ú Û ÜÓ Ò á â ß Ú Ý Ó Þ ã Õ Ø ä Ò Ø â á â Ô Ý ß â ÕÔ à Ý Ó å Ò æ Ò × Ý ç ç è â Ô Ý ß â Õé Ø Ú Õ á Ý Ó Ò Ö Ò Ø å Ò Ó Ô ê à Õ Úë ì íé è Þ × Ò Ú é × Ö â ß ß Ò Þ Ò è Ò Ô ß Øç ç Õ Ø ß Ø Ò è Ý ß â Ó å ß Õ Ô è Ý â Ö Úç ç Õ Ø ß Ø Ò è Ý ß â Ó å ß Õ Ô è Ý â Ö ÚÕ Ø Ö Ý ß â Õ Ó Õ Ó Ò è Ò Ô ß Ø Õ Ó â ÔÖ é Ú ß × Ò Ú é × Ö â ß ß Ò Þ Õ Ó ßÚ ß × Ò á â è Ò Þ î â ß à ß à Ò â Ó Ú éÖ Ú Ö Ý ê Ó Õ ß × Ò Ú é × Ö â ß ßÒ Ø Ò Ó Þ Ò Ø Ò Þ Þ â Ø Ò Ô ß è ê × ê ß àà Ò Ú Ò Ø ä â Ô Ò â Ú Ø Ò Ó Þ Ò Ø Ò Þ ×â Ú ß Ý Ó ß Ì Ï é Ø å â Ô Ý è ï Ú Ú â Ú ß Ý Óð ñ ò Æ ì ð ó È Å ô ë õ ö ÷ ø ø È ù Åá ú û Þ Ý ê Ú Ý Þ ä Ý Ó Ô Ò Ó Õ ß â ÔÞ Þ Ø Ò Ú Ú ü ç Ø â Ö Ý Ø ê Ì Ú Ò Ô Õ Ó ÞÔ Ò ý Ý Ó Þ ü þ ÿ Í Ý Ô � é ç ã Ô Õ ä ÒØ � Ò Ô Õ Ø Þ Û Ü Ò á á Ò Ô ß â ä Ò Þ Ý ßÕ ß Ý Þ Þ Ì Ô à Ý Ó å Ò Õ Ø Ô Ý Ó Ô ÒØ Õ ä â Þ Ò Ø � Ò Ô Õ Ø Þ Û Ü Ò á á Ò ÔÒ ß î Õ Ø � ç Ý Ø ß â Ô â ç Ý ß â Õ Ó î âé Ú Ô à Ý Ó å Ò Ó Õ ß â á â Ô Ý ß â Õ Ó ÚØ á â è Ò Ú Ô è Ý â Ö Ú Ò è Ò Ô ß Ø Õ Ó â Ô Ý� Ò Ô Õ Ø Þ Û Ü � é Ò Ú ß â Õ Ó Ú Õ Ø ßë ø � Å Æ Å È � � Æ � � � íÒ á â ß Ú Õ Ø Ò è â å â × â è â ß ê Ì Ô Ý è è �Ô è é Þ Ò Ý ú Þ â å â ß Ý è ç à Ý ç ØÔ è Ý â Ö Ú Þ â Ø Ò Ô ß è ê ß Õ ß à Ò � ÕÔ è Ý â Ö Ú á â è Ò Þ ß Õ Í Î Í Ï Ð Ñ Ì ÔÉ Ê Ë Ë � Å � Æ Å � È ì Å � � � ìâ Ó â Ô Ý è Ø Ò á Ò Ø Ò Ó Ô Ò è Ý × Ú Ò Ø ä� Æ õ È � ù Å � � � � â Ó Ô è é Þ Ò ÚË � È õ � � È ô íÒ Ò Ö Õ Ó ß à å Ø Ý Ô Ò ç Ò Ø â Õ Þè ß à ç è Ý Ó â Ú Ø Ò Ú ç Õ Ó Ú â × è Ò áà Ò Ú Ò Ô Õ Ó Þ Ý Ó Þ ß à â Ø Þ Ö ÕÖ × Ò Ø á Ý â è Ú ß Õ ç Ý ê Ý è è Õ é ß Úâ ß â Õ Ó Ý è Þ Ò ß Ý â è Ú Ì å Õ ß Õ î î� � � � Æ ö È � õ ë � � ð È õ � Æ ôê Ý Ó Þ Í Ò Ó Ò á â ß Ú Ü Ò ß Ò Ø Ö â� è Ò Ô ß Ø Õ Ó â Ô Ý Ó Þ ã Õ Ø Ô è Ò Ý Ø â ÓÓ ß Ò Ø Ý Ô ß â ä Ò � Õ â Ô Ò � Ò Ú ç Õ Ó� Ø Õ ä â Þ Ò Ø Î é Ú ß Õ Ö Ò Ø Ï Ò Ø ä âÒ Ø Ú ß Õ Ô à Ò Ô � á Õ Ø å Ø Ý Ô Ò ç� Ø Ò Þ Ò ß Ò Ø Ö â Ó Ý ß â Õ Ó Ú Ì � Ø Ò � » ¼  � � ¿  º ¿ � � ½ º » � �¿ ½ ¸ ¼ Á � à · ¾ ½ Á
Õ é Ø Ý å Ò Ú ß à Ò ç Ø Õ ä â Þ Ò Ø Ù Úß â Ö Ò Õ á Ý ä â Ú â ß ýÔ Ý Ø Þ Ý Ó Þ � Ò Ò ç ß à Ò Ô Õ ç êÓ Ø Ò � é Ò Ú ß Ú Ì Ô Õ Ó ß Ý Ô ß Ý ä ÝÓ Ý ß à ß ß ç � ã ã î î î � × Ô × Ú ß �Ú ç â ß Ý è Ý Þ Ö â Ú Ú â Õ Ó � Õ Ø Ô ÝØ Õ Ó â Ô Ý è è ê � Ð à Ò � è Ò Ô ß Ø Õ Ó â Ôß à Ý ß Ý Ø Ò × Ò â Ó å Ú Ò Ó ß ß Õ ßÝ Ó Þ ã Õ Ø Õ ß à Ò Ø ß Ø Ý Ó Ú Ý Ô ß â Õá â è â Ó å Ì Ý Ô Ô Ò Ú Ú ß à Ò ï ä Ý â è âà Ò Ï ß Ý Ó Þ Ý Ø Þ Î ! Ï " # û ûØ Ò Þ Ù Ú Ô Õ Ö ç è Ò ß Ò é Ó â � é ÒÒ Þ ç Ø â Õ Ø ß Õ ß à Ò Ý ç ç è â Ô Ý ×à Ò ç à ê Ú â Ô â Ý Ó Õ Ø ç Ø Õ á Ò Ú Ú â× ê Ý Ó Õ ß à Ò Ø ç Ø Õ ä â Þ Ò Ø Ì Õ ÓÓ ß Ì ï Þ ä Ý Ó Ô Ò Þ � Ø Ý Ô ß â Ô Ò $Å � � È ò Æ Å È � íÔ Ò â Ú Ø Ò � é â Ø Ò Þ î à Ò Ó Ö Ý �Þ Ý Ø ê Ì ß Ò Ø ß â Ý Ø ê ÿ ý ü % ÿ Í â è è â Ó åÒ Ø â Ó å ç Ø Õ ä â Þ Ò Ø Ú �ß Ò Ú î â è è × Ò Ò Ú ß Ý × è â Ú à Ò Þ ÝÒ è â Ó á Õ Ø Ö Ý ß â Õ Ó Ø Ò è Ý ß Ò Þ ßÔ ß â ä Ò Þ Ý ß Ò Ú î â è è Ó Õ ß × Ò â Úâ è è Ó Õ ß × Ò â Ú Ú é Ò Þ �î â è è Ø Ò Ú é è ß â Ó Ø Ò Þ é Ô Ò Þ ×Ý è è ê Ý Ó Þ ß à Ò â Ø � Ø Õ ä â Þ Ò Ø �ß Õ Õ × ß Ý â Ó Ý � Ø Õ ä â Þ Ò Ø � Ò Ô� � & ' & ( ) * ÷ ü % # + ú ÿ ýÒ á â � Õ Ó ß à Ò Ö Ò Ö × Ò Ø Ù Ú Û ÜÕ Ö Ò � è Ý Ó Ù Ú Ý Þ Þ Ø Ò Ú Ú Ý Ú âÔ Õ Ó ß Ý Ô ß Ý ä Ý â è â ß ê � Ô Õ Ö Õ Øì � ù Æ � , È ø È õ È ì ù È ) Æ - � È õä â Ô Ò Ú Ö é Ú ß × Ò Ø Ò á Ò Ø Ø Ò Þ ßÚ Ý ç Ø Õ ä â Ú â Õ Ó ß à Ý ß å â ä Ò Úâ Ú Õ Ó è ê Ø Ò � é â Ø Ò Þ á Õ Ø Ò Ó Ø Õá Õ Ø Ý Þ . é Þ â Ô Ý ß â Ó å Ô è Ý â Ö Ú ÞÕ Ó ß à Ú Õ á ß à Ò å Ø Ý Ô Ò ç Ò Ø â ÕÚ ß Ý Ó Þ â Ó å ç Ø Ò Ö â é Ö Ú × ê ßî î � � Ò Ý è ß à Ô Ý Ø Ò � å Õ ä �ô Æ õ È /Ó Ý ß â Õ Ó î â è è â Ó Ô è é Þ Ò Ý ç ÝÓ å à Õ é Ú Ò Ô Õ Ö ç è â Ý Ó ß î â ß àÓ Ú Ò ü Û � � ÿ ã Ý é ß Õ Ö Ý ß Ò Þ ßâ Ô ÒÒ Ø â Õ Þ Ú ß Ý ß é Ú î â è è × Ò â Ó Ô èÒ Ý é ß à Õ Ø â 0 Ý ß â Õ Ó Ú Ì � Ò á Ò Ø Ø Ý Á ¸ À ½ 1 » 1 ¿  º ¿ � � ½ º » � �¿ 2 3 À 4 · ¾ ½ »
5 6 7 8 9Õ á á â Ô Ò ß Õ �ê î â ß à ß à Ò ç Ý ß â Ò Ó ß Ù Ú á â è Ò ýâ è â ß ê � Ô Õ Ö Ì Õ Ø Ý î Ò × ä Ò Ó Þ� � Ô Õ Ö ã ç Ø Õ ä â Þ Ò Ø ã ß Õ Õ è Ú ã â ÒÚ Ò Ö Ý Ó Ý å Ò Ö Ò Ó ß Ì Ô Ý è è ß àÔ � Ý ê Õ Ø Û Ü á Õ Ø Í Î Í Ï Ð Ñ â Úß à Ò ï ä Ý â è â ß ê ç è Ý ß á Õ Ø Ö Ì Ú éÕ Ó Ú Ý ä Ý â è Ý × è Ò Õ Ó ß à Ò ï ä Ýß ê î Ò × Ú â ß Ò Ý ß Ý ä Ý â è â ß ê � Ô Õû ü û % ã " % ÿ Õ Ø : Í û ; Ô è Ý â ÖÛ Ü Ó é Ö × Ò Ø â Ó Ô è é Þ â Ó å Ý Ó× è Ò ú û Þ Ý ê ü Ò è Ò Ô ß Ø Õ Ó â Ô ÿ ÕÕ Ó Ý è ç Ø Õ ä â Þ Ò Ø Ì ß à Ò Ú Ò Ø ä âè ê ß à Ò Ø Ò Ó Þ Ò Ø â Ó å ç Ø Õ ä â Þé Ø Ú Ò Ì Î è â Ó â Ô Ý è $ é Ø Ú Ò Ï ç Ò� â Ó å Ô à Ý Ó å Ò Ú Ý á á Ò Ô ß â Ó å ßå Ý Þ Þ Ø Ò Ú Ú ý ü ú ÿ $ � Û Ý Ó Þ �Ý Ú Õ á ß à Ò Þ Ý ß Ò ß à Ò Ô Õ Ö çÕ ß à Ò � Ø Õ ä â Þ Ò Ø � Ò Ô Õ Ø Þ ÛÚ é Ò Þ �× Ò Ó Ò á â ß Ú Õ Ø Ó Õ Ó ç Ý ê Ö Ò Ó� Ò Ô Õ Ø Þ Û Ü Ô à Ý Ó å Ò Ú Ì ß à ÒÔ Õ Ø Þ Û Ü Ý ç ç è â Ô Ý ß â Õ Ó Ì ç è Ò ÝÜ Ô Ý Ø Þ ß Õ Í Î Í Ï Ð Ñ < = > ? @A B C C D B E F G H A I D J B K L GB M D J N D H O G E G P Q G R E KS T U V W XA G Y Z [ W \ ] T ^ _ ` ^ a W b cd D B e A I f H F R E B H K D g B E LG e e D D F M I G I B N D h B O D GO R E i H j A I D P i E F A h G H A I BG O k i F F R D E F I B N D A I D K I GA I D D H O G P A I D A I E D D h Gi O A I E G R j I O B A D B H O J DI A I D d f l m m n o p q n o rA D e D C I G H D F Q F A D hR O D O G H K G E E D F C G H O D HB e F s t u v w u s x y z { | u } ~ s u � � � � � x w
� � � � � � � � � � � � �O G E G P Q G R E K I G i K D G E K BD � K I B H j D � I A h e A G G J A B iI D g D O i K B e � B E D g B H B j D� � � � � �R J h i A A D E F F I G R e O K G H A B KB i e i A Q C G E A B e G E G A I D E m NG h �h P G E h �H Q e D A A D E G E � O i j i A B e C I BG E � � O B Q � C B C D E � K e B i h Fi K D F h B Q J D J i e e D O J Q A ID E K B H J i e e P G E A I G F D F D ED K i B e i F A k � D E A i P i D O � R E F DA I D C E G N i O D E � F � � � � � Fl E G N i O D E ¡ D K G E O f ¢ K I B HC e D A D O B C C e i K B A i G H i F E D K D¢ G H B E D A E G B K A i N D J B F i FH A G P K e B i h F P i e D O R H O D E AC E G N i O D E h R F A K G H A B K A AB F D K G H A B K A A I D l E G N i O D@ £ ¤ ¥ ¦ § ¦ § ¨ ¦ © ª « ¬ ® ¯ ¬ ¦° ± ² ³ ´ µ ´ µ ¶ ´ · ¸ ¹ º » ¼ ½ · ¾¼ ³ ° ¿ ¼ ´ ° · ¼ ½ À À ² ³ ´ ² ° À À ± · ´Á ¸ ¹ ´  ¼ À à ¹ ¿ Ä ´ À ½ ¶ Å · ° Ä ¿ ¾´ ² Å À ½ ¼ ´ µ ´ µ ¶ ´ · ¹ Æ ³ °° Ç ´ ± à À À Å · ´ µ ¿ à µ Å ½ È µ½ ± ² ´ · ½ µ ´ µ ¶ ´ · ´ Ç ² ´ · ¹ ²° ¿ ¼ ´ ° ± ´ ¿ ² ³ ´ · Å ´ Ç ¾ ¿ Ç É ² ³° Ç ² ³ É · ½ ¼ ´ Å ´ · ¿ ° ¾ Ê ² ³ ´ ³Å · ° Ä ¿ ¾ ´ ¾ ¶ È Ë¼ ´ · ´ À ½ ² ´ ¾ ² ° Ë ÌÍ Î Ï Ð Ñ Ò Í Ó Ô Í Õ Ö × Ø Ù Ð Ö Ð Ñ Ò Ú Í Û Ü
Ý Þ ß à á â ã ä ã å ã æ à ã ç Þ½ À À ² ³ ´ ² ° À À ± · ´ ´ è · ° Ä ¿ ¾ ´ ·Ç ½ Å Å · ° Ä ½ À ° ± Ë · ´ ± ´ · · ½ À ¹ Ê´ µ ´ Ç ² » ´ Å ½ · ² µ ´ Ç ² ½ ² é¼ ² ê Ä ½ ¿ À ¿ ² È ë À ¿ ´ Ç ² ì ´ · Ä ¿ ¼ ´Ä ½ ¿ À ¿ ² È Å À ½ ² ± ° · µ ¹ Ê ¹ à ¶ µ ¿ ²½ Å · ´ ± ¿ Â í¹ Å ½ È µ ´ Ç ² Å ´ · ¿ ° ¾ í´ Å ³ È ¹ ¿ ¼ ¿ ½ Ç ° · Å · ° ± ´ ¹ ¹ ¿ °· Ä ¿ ¼ ´ ¹ í î ï ð ñ Ë ò ³ ¿ ¹ ¾ ° ´ ¹ Çó ¿ ¾ Æ ¿ ± ´ ½ Ç ¾ ô ´ É ¿ ¹ ² ´ · ´ ¾² ½ ² à ¹ Ê ´ ¹ Å ´ ¼ ¿ ½ À À È ¿ Ç ² ³ ´Ç É ´ ¹ õ ö ÷ ø ó ° Ä ¿ Ç É ± · ° µ ù´ ¿ Ä ´ ¾ ¿ Ç ² ³ ´ ú ë ú ì ò û ¼ ° ·¹ í² ³ ´ Ç ´ Æ è · ° Ä ¿ ¾ ´ · ô ´ ¼ ° ·² ³ ´ ê Ä ½ ¿ À ¿ ² È ü ´ ½ À ² ³ º Ç ± °´ · ì ´ · Ä ¿ ¼ ´ ¹ ¾ ´ Å ½ · ² µ ´ Ç ²ý þ ¬ § ¨ ¦ © § ÿ � � � � ÿ ® ¾ õ´ ´ è · ° Ä ¿ ¾ ´ · ë à ¹ ² ° µ ´ · ì¾ ´ · � � ñ � ð � � � ï � ð � � �· ´ ¼ ´ ¿ Ä ´ � � � ñ � � ñ �� � � � � � � � � � � � � � � � � � � � �� � � � � � � ! � � � " � # $ � � %� � % � � � & " � � � ' � � � � � � �� � � % � � ! % � � � � & � � � � � � �( ) * + , - . ( / 0 , + / 0 1 + 2 / - . 3 (
4 5 6 7 8 6 6 5 9 5 : ; < = > ; ?� @ � & � " � � � A � � B � � � � �C & � % � � " � � ! � � � � � � & � � B �D E E D F G H I J K #� & � � D J J L M L N O N P Q R H D H� � � � & & � " � % � " � � � � S B �" � � % ! � " B � � � � # T " U � B � �� " � � ! ! % � � " & � � B � � & ! �� V � � & � W � � & � S & & � & � � � � C� " % % " U � � � � � � � & XY � " � ! � " A " % " ! � � � � � Z� ! " � � � � " � � � � # $ � � & � ! !� � [ \ #� � � � � " � V � � U " � ] � � D J J� � F I H F F G F G K J C ^ _ ` a ab c d ^ e c f e c _ c f g ` _ a h e i fA � � B � � � � � � � � � � � � � � �j N k l #m n o m p q r l s t u n p v R L w P x� � � � � � � U � " � � � � � � � B� � � & � � ' � � � � � � � � � � � "� � � � � % � � � & � � � & � � ] � �� � � � � � � � � � � � � y & " B �( 1 z , 2 ) { . / - . 3 ( 1 | } ~
� � � � � � � � � � � � � � � �� � � � � � � � � � � � � � � � � � �� � � � � � � � � � � � � � � � � � � �� � � � � � �� � � � ¡ ¢ � � � � £ � � ¤ � � � � � � ¥� ¦ � § � � � � � ¡ � � � � � � � � � � �� � ¤ � � � � � ¡ � � � � � � ¡ � �¨ � � � � © � � � � � � � � � � � � �ª « ¬ � ¤ � � ® § � � � £ � � � � � � � � � � � � � � � � � � ¦ � � �¯ ° ± ° ² ³ ² ´ µ ¶ � ¥ � � � � � �· ¸ �¹ º » ¼ ½ ¾ ¿ » ¼ ½ À ¾ Á  à ¿ Ä ¹� � � � � � � � � � � � � Å � Æ ÇÈ ¬ � � � É � � ¨ � � � � © � � � � �¤ � � ® � � � ° Ê ´ È �� � � � � � � � § � � � ¤ � � � � � � �� ® � � � § © � � � § � � � � � � �� � � ® � �Ë Ì Í Î Ï Ð Í Ñ Ð Ò Ð Ó Ô Ð Õ Ö Ö × Ö
� � � Ø Ù� � � � � � Å � Æ Ç � � � � �� � � � � � � ¦ � � � � � � � � ¡ � � � � §¥ ¯ ¯ ° ± ° ² ³ ² ´ µ ¶ � ¥ � � � �� § � � � � � � � � � � ¤ � � � � � � � �� � § � � � ¡ � � � � � � � � � � � § �� � © � � � ¤ � � � � � � § � � � � � �� � Ú � � © � � � � � � � � � Û ª Ü ¬ � � ® � � � � � � � � � � � � � � � �� � � � � � � � � � � ¨ Ý Ç Æ Þ ®¹ Á ß ½ à ¾ ß ß ¾ á Á º Ä ¸  à â à Á ¼ ß� � � � �� � � ¦ � � � � � � � � � � � ® � � �� � � � � ¨ � � � � � � � � § � � � � � �� � � � � � � � Å � � � ¡ � � © � � �Ö ã ä å
� � � � � � � � ¦ � � § � � � � � � § � � � �� � � æ� � � � � � � � � � ¡ � � � § � � � �� � � � � � � � � � ¤ � � � � ¦ � � ® �� � ® � � ¡ � � � � � � � � � � � § � � � � ¤ � � ® § � � � Ú � � © � � �� �® � � � � � � � �ß ç º ¼ ç ¿ Ä à à è é ê� � � � � � � � � � � � ¡ � � � � �� � � � � § � � � � ® � � � � � � � � �� � � � � � ® � � � � � © � � � ¡ �
ë ì í îï ðñ ì í î ò ó
í ô õö ð î ë ñ õ
178

÷ ø ù ú û ü ý ø û øþ ÿ � � ü ý� � � � � � � � �� � � � � � � � �� � � � � �� � � � � � � � �� � � � � �� � � � � � � � � � �� � � � �� � � � � � ü ý ú � � � � � �� � � � � � � � � � � � � � �� � � þ ÿ � � ü ý� � � � � � � � � � �� � � � � � � � �� ú û � � û û ø ÿ !û � " � � û � # $� � � � �� � � � � � � � � � � � � � � � � � � � �� � � � � � � � �� � � � � � � �� � � � � � % � � �& � � � � � ' � & � � ( � ) � � $* � � � � � � � � � � +� � � þ ÿ � � ü ý� � � � � � � � � � �� � � � � � � � �� � $ $ � � � � �� � � � , � � � � � � � � � � � � � � � �� � � � � � � - �� � � $. / 0 1 2 3 0 4 5 0 16 7 8 9 5 1 1 0 8 : ; <
ø � = � û � ! = � � ! þý ú � � � � � �� �� � � � � �� � � � � � � � � � �� � � � � > � � � � � � � � �� � � $� � � � � � þ ÿ � �� � � � �� � � � � � ý ú � � �� � � �� � � � � � $! ø û �� � � � � �� � � + � � +� � � � � �� � �� � � � � � � � � ? & > � � � � � �ý ú � � �� � � � � � � � � �� � � � � � , � � > � �� � � � � �þ ü þ @ A� B � B þ úC ø ÿ ÿ ø ! Dþ ÿ � �� � � � � � � � � � � $� � � � � E F� � � G � � � � � � �� � � � � �� � � � �ü ý ú � � �� � � � � � � � �� � E F HI J K L M N O P L QR S R L M T U VW X Y Y R X Z R PQ U M U R X Z R P N0 : [ 5 : 4 5 4 [ 8 \ 5 3 1 56 7 8 ] 0 4 5 7 ^ 6 7 8 ] 0 4 5
� _ � � = ! D ` ÿ � a � b � ÿ � = c D ü ÿ ø@ = ø = � ! ú û d � û � � � ø = � úe f g � � ( � � � � � � � �� � � � � � � � � � � � �� � � � ( � � � � � � � � � $ � � �� � � � � � � � � � � � � h ' h * � i G � � � � ' �* � � � jk l l m n H o m l p k q rs f ' � � � � * � � �� � � � � � � � � � � ( � �t � � � � � � � ' � � � � u � �� � � � � � � � � � �� � � � � $v f � � � � w � � � �� � � � h ' h * � i G � � � � ' � � � � � * � � � jk l l m n H o m l p k q rx f d � û � � � ø = � ú_ ú = ø y y ÿ c = ú ø # z � _ � !! � û { � � � ! ú _ ÿ c | } @ � ~� f } ÿ ÿ � ÿ ø � z !! ý ú � ÿ # b � ! � b z � = = �� ÿ � � = û ú _ � � ø ÿ ÿ c $ h ' h *g � � � � � � G � � � � ) jk n � k l� f � � � � � � � �� � � � � � � � � � � � � � � � � � � � � � � � � � � � �A �ú � F F l l n nD A � q H p F F m l l n n� ü ý ú � � � � � � � � � � � � � � � � � � � E F H � � � � � � � �' � � � � � � � � � � � � � �F H � � � � � � � � � � � � � � � ( � � � � � � � � � � �� � � � � � � � � � � � � � � � � � � � � � � � � � � � � �� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �� � � � � � � ( � � � � � $Q � M � � Q P M � M R � � K R M � J �V � O P P M R R � S � X T X R L � ON Q Z M N � R Q K W � N T O L Q � K �N Q Z M N � R J � � � O L Q M K L � O L M �5 4 9 8 7 � 3 0 � � 7 5 9 5 7 5 :5 7 � ; : 3 ; < 8 : < 0 : 5 ; [
ø � z !ú _ � � {ü ú û� � � � � �� � � � � �� � � � � � � � �� � � � � � � � � � �� � � � � � � �� � � � � � � � � ú _ # ú � !! = û ø = � { �~ y ÿ ø _ ! B! #* � i� � � � � � � � � � � � � � � � � � � j� � � � � � � � � � �� � � � � �� � � � � � � � $ � � � � �� � � � $ þ ÿ � �� � � � � � � � � � � � � � � � � � �O � M� W
' � � � �' � � �� � � � � � �h ' h *G $ � $ h � ,) � � � � �� � � � �� � u � � �� � � � � � �� � � � � �h ' h * � i� � � � � ,� � � � � � g � � � � � � �u � � � � � � �
: � 5 ; : 4 � ; � : 8 [ � 8� � � � ¡ ¢ � £ ¤ ¥ ¦ § £ ¨ © ª « § ¬
® ¯ ° ± ² ³ ´ µ °¶ · ¸ ¹ º» ¹ ¼ ½ ¾ ¿ À · ·Á Á ¼ ¾ Â Ã Ä Å ¼Ä Æ ¼ ÇÀÈ ¼ ·¸ ÄÉ Ê Ë Ì Í Ë Î Ï ÐÑ Ò Ó Ô Ë Ó Õ ËÖ Ë Ï Ë Ó × × Ò ØÙ Ú ÛÜ Ý Ý Þ Þ ß ßÏ à Ú ÛÝ á Þ Þ ß ßâ ã ä Í Éå Ò æ É Î Í × çÒ Ó Ï Í ÏÒ Ó × ç ËÛ Î Ë Ö Ï Í × Ë Øè Õ Ò É Ð Ñ æ Ò Ì Í Ô Ë æ× ç ËÒ Ó ä Ó ÔÓ Õ Ë × ä Ö à × ç Ë Óé Ò æ É Ïê Õ Õä Ñ Ñ ã Í ÕÎ Ë Ö Ï ÍÎ Î Î è Öç ä Ó ë Ëâ ìä Ó Ô ×ä Ì ä Í ã äÍ í Ü Õ çî ï ð ñ òé Ò æÍ í Üó ô õé ÒÕ Ò Ó × ä Õö Ë Ñ × è àé ÒÒ ì × Ñ ä ×ä Ô É Í ÏÍ í Ü Õ ç äç × × Ñ Ø Ð Ð ÎÑ æ Ò Ì Í ÔÊ Ë å Ë÷ Ò × Í å Í Õø Í Ï × ì ÓÖ Õ Ö Ï × Ü× ç Ë Ï ËÑ æ Ë ä ì× ç Ë Í í ÜÊ Ë Ï Ñ Òù ó ó ú óí å å ËÉ ä Ó äÕ Ë æ × ä ÍÏ Ë æ Ì Í Õû æ Ë ä ìÊ Ë å Ë æâ ã Í Ó Í ÕÖ Õ Ö Ï ×Ñ æ Ë ä ìä ì × ç Ò× ç Ë Ë Ìä × ç × × Ñü ý ý á þÿ � � � � � � � � ÿ � � � � � � � � � � � � � � � � � � � � � �
� � � � � � ¯ ´ µ �Ç Á ¼ ¸ � ! à Á ¹ " ¸ ¹ Ã Ä ¿ # Ä · ¹À   Á à » ¸ · à $ % ¼ Ä ¼ $ ¹ ¾ $¼ Æ ¼ Å # �  ¸ ¹ ¼ Ä È ¼ Á »Ä Å & Ä Â ¸ ¹ ¼ Ä À Å º ¹ ¾ ¾ ¹ ÃÕ Ë Ï Ï × ç Ë Í í Ü Õ ç ä Ó ë Ë ' ËÕ ä × Í Ò Ó × ç æ Ò ì ë ç × ç Ë ( â (× Ë ä × ç × × Ñ Ø Ð ÐÖ Õ Ö Ï × Ü è Õ Ò É Ð Ñ æ Ò Ì Í Ô Ë æ Ð × ÒË è ç × É ãì æ æ Ë Ó × ã Í Ï × Í Ó ë Ï Ò å Ñ æ Ò Ì Í Ô Ë× ç Ë Í æ ÷ û ) Ó ì É Ö Ë æ Ï ä æ Ëä Ö ã Ë Ò Ó ã Í Ó Ë × ç æ Ò ì ë ç × ç Ëç ä Ó ë Ë ' Ë Ö ä Ñ Ñ ã Í Õ ä × Í Ò Óò * + ï , ò - * + ï . èæ / ì Ë Ï × Í Ò Ó Ï Ò æ Ñ æ Ò Ö ã Ë É ÏÜ Õ ç ä Ó ë Ë Ù ì Ñ Ñ Ò æ × ö Ë Ï 0õ ú ô õ 1 ô èæ Õ ä Ï Ë É ä Ó ä ë Ë É Ë Ó × Ò æÕ × × ç Ë 2 Ë Ô Í Õ ä ã â ä æ Ë 2 ëÕ ä ã ã ù 3 3 ú ù 4 õ ú 5 ó 6 1 èÒ æ ä Ñ Ñ æ Ò Ì ä ã Ò å Ï Ë ã Ë Õ ×× Í Ë Ó × Ï Ë æ Ì Í Õ Ë Ï ä Ó Ô Í Ó Ñ äÏ Ï Í Ò Ó Ï à æ Ë å Ë æ × Ò × ç Ëä Ó ë Ë Î Ë Ö Ñ ä ë Ë ä ×Î Î Î è Ö Õ Ö Ï × Ü è Õ Ò É ÐÔ Ë æ Ð × Ò Ò ã Ï Ð Í Ë Ü Õ ç ä Ó ë Ë è ç × ÉË æ × Ò × ç Ë û æ Ë ä ì × ç Ò æ Í 7 ä ×Õ ä × Í Ò Ó Ð Ê Ë å Ë æ æ ä ã Ê Ë / ì Í æ ËÓ Ô Ë æ â ã Í Ó Í Õ ä ã Ê Ë Ï Ò ì æ Õ ËÜ è Õ Ò É Ð Ñ æ Ò Ì Í Ô Ë æ × Ò Ô Ë × ËË æ Ì Í Õ Ë Ï × ç ä × æ Ë / ì Í æ Ë× ç Ò æ Í ä × Í Ò Ó Ò æ æ Ë å Ë æ æ ä ã Ï ÒÜ Õ ç ä Ó ë Ë Í Ó × Ë æ ä Õ × Í Ì Ë 8 ÒÒ Ó Ï Ë 9 ) 8 Ê : ä ×ó ô ú ù 3 4 5 èË Õ × Í Ì Ë ü Ð ; Ð ; < ¼ » ¹ ¶ à Á ¼ Îä ë Ë Ñ æ Ë ä ì × ç Ò æ Í 7 ä × Í Ò Ó å ÒÍ Ó Ï Ñ Ë Õ Í ä ã Í 7 Ë Ô Õ ã Í Ó Í Õ ä ãÕ Ë Ï è Ê Ë å Ë æ × Ò × ç Ëì × ç Ò æ Í 7 ä × Í Ò Ó Ð ÷ Ò × Í å Í Õ ä × Í Òæ æ ä ã Ê Ë / ì Í æ Ë É Ë Ó × Ï ø Í Ï ×Õ ä ã Ê Ë Ï Ò ì æ Õ Ë Ï Ò Ó× Ü è Õ Ò É Ð Ñ æ Ò Ì Í Ô Ë æ å Ò æ Ë Ì Í âì × ç Ò æ Í 7 ä × Í Ò Ó æ Ë / ì Í æ Ë É Ë ÓÒ æ Í 7 Ë ¼ » ¹ ¶ à Á ¼ Ï Ë æ Ì Í Õ Ë ÏÌ Í â Ò æ Ë = Ë ä ã × ç Õ ä æ Ë ' Ë ÖÑ Ï Ø Ð Ð Î Î Î è Ë Ì Í Õ Ò æ Ë è Õ Ò Éþ ý þ á ; ; ; < è� � > > � ? @ � � � ÿ ? A � � � ÿ �
� B ° C ° D ° E µ ° F¹ Ä ¼$ à Á» ¹ Æ ¼ ¾Ã Ä ¾ G ¸ H à Á ¸ à Á IË ÖÙ Ú ÛÒ Ò ã Ï Ð Í Ë Ü ÕË æ ÏË Ò æÏ à Õ ä ã ã × ç Ëä × ù 6 6 úæ × Òë É ×ä × Í Ë Ó ×É ãÍ Ò Ó ÐË É Ë Ó × ÏÏ Ò ÓË æ É Í Ó ËÒ æ Õ ä ã ãÒ Í Õ ËÎ Í ã ãæ Ó Ðì Ó Ô Ë æâ Ò æ ËÓ × Ï è Ú ÒÕ Ò Ó × ä Õ ×Ö û Ò æ × ä ãÒ æ Õ ä ã ã
G ¸ H à Á ¸ à Á IJ ì Ë Ï × ö ÍK L M N M L L M OÕ ã Í Ó Í Õ ä ã æ Ë å ËÚ Ò Ï Õ ç Ë Ô ì ã9 û Ù â : ä Ñ Ñ ÒJ ì Ë Ï × ö Í ä ë Óù ù ù ú 5 ó ó ú ù óÚ Ò ã Ò Õ ä × Ë× ç Ë % · � ¼ ¶× ç Ë P Ó ã Í Ó Ë, ò - * + ï Q RS ¸ Å ¹ à · à T IP æ Ô Ë æ Í Ó ëÑ æ Ò Ì Í Ô Ë æ Ï 9 ûÕ Ò Ó × ä Õ × ê ) 2Ò Ö × ä Í Ó ä S ¸9 Ê J ) : å Ò æ × çÑ Ë æ å Ò æ É Ë ÔÑ æ Ò å Ë Ï Ï Í Ò Ó äÔ Ë Ñ ä æ × É Ë Ó ×å æ Ë Ë Ï × ä Ó Ô Í ÓU â Ú Ð âU 2 Ê ) ÐU Ù û íÏ × ì ÔU û í ÚÚ Ò Ò Ö × ä Í Óå Ò ã ã Ò Î Ï Ø¶ ¸ · · ¶ ¼ Ää Í É Ï Ñ Ë Õ Íõ 1 6 ú 6 6 3 6V W X M Y , Z[ ð ï \ ] ^ _ ò\ ï ð ñ ò * + ï _` a ò - ò ` Z a ò -ï + b c + _ d _é Ò æ æ Ò ì × Í ÓÑ ä æ × Ò å × ç Ëâ ç Ò Í Õ Ë û ûû æ Ò Ì Í Ô Ë æ à éû æ Ò Ì Í Ô Ë æ 2� ¬ e ÿ ? f � � � � � � f � � � ÿ
F ¯ ´ g ° h h h h h i j �¸ Ä Å S ¸ Å ¹ à · à T I È ¼ Á » ¹I È ¼ Á » ¹ Æ ¼ ¾Í ä ë Ó Ò Ï × Í Õ Ï à ) Ó Õ è Í Ï × ç Ëk X l X M m n O M Ò ì × Ñ ä × Í Ë Ó ×Ë æ Ë Ó Õ Ë ã ä Ö Ò æ ä × Ò æ o èã Ë ä û ä × Í Ë Ó × Ù Ë æ Ì Í Õ Ë â ËÒ Í Ó × É Ë Ó × à ã Ò ë Ò Ó × ÒÓ Ò Ï × Í Õ Ï è Õ Ò É Ð Ñ ä × Í Ë Ó × Ò æó ó 5 èË Ò × ç Ë æ Ñ ä æ × Í Õ Í Ñ ä × Í Ó ë ã ä Ö! à ¹ Æ ¼ Ç Ç # Ó Ë × Î Ò æ 0 à Ìû æ Ò Ì Í Ô Ë æ ö Í æ Ë Õ × Ò æ o p î ï ðI È ¼ Á » ¹ Æ ¼ ¾ë Ñ ç o Ï Í Õ Í ä Ó Ï ä Ó Ô Ñ æ Ò å Ë Ïû â û Ï ä Ó Ô Ï Ñ Ë Õ Í ä ã Í Ï × Ï :2 Ù Ñ Ë Õ Í ä ã × o = Ë ä ã × ç q r 9 ê¸ Å ¹ à · à T I s � ¸ · ¹ I & Ä ¹ ¹ ¸ç Ë å Ò ã ã Ò Î Í Ó ë Ï Ë æ Ì Í Õ Ë Ï ÎÍ Ó ä Ñ ç o Ï Í Õ Í ä Ó r Ï Ò æä ã Ñ æ Ò Ì Í Ô Ë æ r Ï Ò å å Í Õ Ë à Ò ì ×× Ò å ä ç Ò Ï Ñ Í × ä ã Ò æ äÓ ë Í É ä ë Í Ó ë Õ Ë Ó × Ë æ Øâ Ú ê Ï Õ ä Ó ÏÐ 2 Ê ê Ï Õ ä Ó Ïí â Ú Ð ÷ ì Õ ã Ë ä æ â ä æ Ô Í Ò ã Ò ë oÔ Í Ë ÏÏ Õ ä Ó ÏÓ ä Ê J ) à Õ Ò Ó × ä Õ × ê ) 2 äÄ ¼ Á t ù 6 6 ú ù 3 4 ú 3 5 4 4 & Ä ¼Í ä ã × o ç Ë ä ã × ç è Õ Ò É u ¸ v t ù 66Z w ð \ d ò ð - ò _ Z ñ Z ò a Z x a + ðò ` ò Z - _ ð ï \ ï ð [ + _ _ ò ð - Z a_ y ] ð Z ï + _ c x z ò d d ò - {- [ ð ï z Z d ò ð - [ ð ï + w ò _ d ò - {_ RÓ Ë æ ä Ô Í Ò ã Ò ë o Ï Ë æ Ì Í Õ Ë Ï ÓÊ J ) à æ Ë å Ë æ × Ò × ç Ë ( ã ì Ëû P û ç o Ï Í Õ Í ä Ó Ï à û æ Ò å Ë Ï Ïé ä Õ Í ã Í × o ä Ó Ô ê Ó Õ Í ã ã ä æ o2 ä Ó ì ä ã 9 Ù Ë Õ × Í Ò Ó ( :ÿ ? A � � � ÿ � | ? � � � ? � ÿ � }
~ � � � � � � � � �� � � � � � � � � � �� � � � � � �� �� � � � �� � � �� � � �� � � �� � � ¡ ¢� � � £ � � �¤ ¥ � �¦ § ¨ © � £� � � � �ª � �« � � � � � �¬� �� � � � ®¯ ¯ °± ² ³� £ �� £ � � �
´ µ ¶ � � � � � ®� � � � � � � � �· � ¥ � ¸ � £¹ � º � � » · ¸ ·� � ª � ¼ � £ � � �ª � � � � ª � � ½¾ ¥ � � � � � �� � ¿ ¥ � � � � � À� � ª � ¼ � £ � � �« ª ¬ � � � � � � �� � ¿ ¥ � � � « � �� ª � � ¥ � � � � �¤ � ½ � � � � � ¬ �� � � � ¿ ¥ � � � ½� � « � � � � � � Á «£ ¥ � « � � � � � � �¹ £ £ � � � � � � � ¥ � ªÃ Ä Å Æ Ä � £ � ª �ª � � � � ª � � � ¼Ç � È � � � £Â Â É Â ª ¬ � � � £ ¼ � ½ � � Á Ê � £ ¼ � ½ � � ¨Ë � � � � � � µ� � � � � � � � � � � ¬ £ � § Ì Í Î§ È � ª � « �� � � � ¤ Á ¤ � � �Ê £ � � � � � ¤¬ £ ¥ � � � � � � � £� Ï � Ï ¦ ¼ � � � � � ¬� £ � � � � � � ¼ � � ¬¸ ¥ � � £ ¤ � � ¾Î ¯ ¯ ° Ð Ñ Ò ° ¯ ÓÔ Õ ± Ö ¡ ¢ × Ø Ö � � ¡Ù ³ Ù Ö ¡ Ú Û Ü �Ù Ý Þ Ù Ø ¢ � Þ ¡ ¢ ßÕ à á â × Ö � ¡ ± Ö} ã ä å æ ã ç } è é ê ã ë ë ì
� í � � � î � � ï� � � � � � � � � ð � � � � � � � ñ ò ó ô � � µ � � � � õ � ¶ � ó® ö � � � � � ¶ � � � � � � ÷ ó �� � � � � � � � ø � � ù � � �£ � � � � ½ · � ¥ � ¾ ª � � � ½ £ È· ¾ ¹ ú © ¤ � � � À � � � � �ª � � � � ª � � � ¼ � � � � » ¤ � � � �� ª � ¤ � � � � ½ � « � � ½ � � � ¬ ©� � � � � � � � � � « £ � � � � � � È £ �« � � � ¥ � ª £ � � û � � � £ � Á � � � ª £ª � � � � ª « � £ È � � � � £ � � � � � �£ � � È � ¤ � � ¬ ¤ � ¤ � � � ¤ �� � ¥ � ª £ � � û � � � £ � £ � � � ª �� � � Ï ¦ � � � � � ¼ � � � � ¤ ¥ � � �� � � � � � � � ¬ Ï Â � � � ¥ � ª £ � � û �È � £ ¤ · ¸ · ¾ ¹ ú È £ � � � �« � � � � � � ª £ � « � � � � � û � � � £ � � �� � ª � ¼ � £ � � � ª � � � � ª � � � ¼ � �� « � � � ¥ � ª £ � � û � � � £ � Á � � � �� ô � ð ü ýþ ÿ ÿ � � � þ � � � � �£ � � û � � � £ � ¤ ¥ � � � � £ � � � �� ½ � � � ¼ � � ¬ £ È � � ª � ¼ � £ � � �� � � � Ï£ � ª � £ � � � � � · � ¥ � ¸ ª £ � � �� � � � � Á  � £ È � � � � £ � � �Ê � � � � � � ¬ � � ½ ¦ � � � � � � � ¬� � ¥ � � » ¾ � � � � £ � § ©µ � � � � ÷ � ó ø � � ÷ ø µ � � �� � � � � · ¸ · ¾ ¹ ú � � � � � � £ �Î Ð Î ¯£ ¼ � ½ � � ¤ ¥ � � È � � � � « � « �� � � � ¤ � £ Í· ¸ · ¾ ¹ úÂ Ï É Ï · £ º � � � � Ì � � � � � � � � � � �¤ � � � � � ¥ � � � ¿ ¥ � � � � � Á � £ �£ � � � � £ � � � � � � ¼ � � ¬ ¼ � � ½ £¬ £ � £ � ª � � � � � � � � £ � � �¬ ¼ � � ½ £ � £ � � � � �  � £ ¼ � ½¾ � � ¼ � � � ÍÓ Î � �¡ � � � Ø ¡ � ¡ Ù â � ± Ù ¡ � Õ � �� × Ø Ø ¡ Ù Ù á ³ � Ý Ú Ý Ù Ö � × �ß Ù � ± � � ¢ Ú × Ö � � ± á � Û ¡ Û Ù Ý Þ Ù × Ö ¡ � � Þ � ¢ Ö � á ¡ Ö Ø Û �ì ë } � � é ê é � � � � �
� � !ò � � � �� � � "�� �© Ï�£ ¥ À ª� ½� ¬� È £ È� �� � � £ �� ½� � � ÏÍ� � � ½�� � ó� � �� �� � Á ¹ ú� � � � �£ � Á� �� �� ¡ � Ý ² ²Ù Ø ¢ � Þ ¡ ¢ ß Ù
179

ô � � � µ � ð ÷ ø µ¦ � � � � � � ¤ �# Ê £ � �# Ê £ � �# Ê £ � � � « � � � � � �¦ � � � � � � ¤ �Ì ¥ « � � � � � �§ È � � � ¼ � � � �� ª � � � � ¼ � � �« � £ ¼ � ½ � � Á �« ª ¬ � � � � � �$ � � $ � � � � � ·Ê � � � � � � � � �¦ � � � « � � ª �· � � � � ¥ � � � �% £ � � � � � · ¸% £ � � � � � � � �& � � Ë � � � � ÷ � ô¦ � ' È £ � � ª �¸ £ « ¬ � £ � ª� � � À � � � � � � ¬ Á¸ � � � ¤ ¾ � � �Ê £ � ¸ � � � ¤( � � � � û � � ª �) � � ª � � � * ª$ � � � � ó � � + �¦ ¤ � � � ¤ ¥ ¤» , ©  ª ¬» © ¨ £ ¼- . /  � £ ¼· ¸ · ¾ ¹ ú )Ç � � � £ � � � � ¼Ç � � � £ � � � � ¼Ì � � � ¬ � � � �§ È � ª � « � £ ¼Ê £ �  � £ ¼ � ½� � ÷ � ô � � ó ñ 0¹ £ � ª � � 'Ê � � � � � � � � �Ê � � � � � � £ � ªÊ £ � � � � � ¥ �� � � ½ £ � � �� � ÷ � ô � � � � �¦ § ¨ ¾ « � � �É � ½ � � � � À «½ � « � � � ¤ � �¹ £ £ � � � � �� � ø � Ê � ºÊ £ � � £ ¥ � � � �1 2 3 4 5 6 7 8 4 9 : 5
; < = = < > ? @A B C D E F G H A D G I J K K H F HA D L L C M K M H E N K J O P K C Q E N J IA D L L C M K M H E N K J O P K C Q E N J IO R C M I N K J C O C O H E H Q K M C OI A I D A K G H A D G I J K K H FI D A K G H R J E H F S J K B K B H JQ E N J I A I N T O C K G H A D GA N M H M H O F H M H F F J M H Q K E TH N O F K B H A H M U J Q H J A M H OH V P V W B T A J Q J N O X A A J A K N OC M L M C R H A A J C O N E L M C U J F HY E D H Z M C A A N O F Y E D H [ BN J I A H E H Q K M C O J Q N E E T R C M YH Y Z Y [ \ ] N E E C S N G E H NM J G H M A C O E T R C M F H F D Q K J GZ Y [ \ ] R C M H ^ L H M J I H O K NB H M Y Z Y [ \ ] C M A D G A Q M_ ` > < a b c c d c e > f g a h =H A D G A Q M J G H M i A j k Q N M F NB A J F H A C R K B H A D G A Q M J G HG H O H R J K A l N O F m C M U H M J R J Q NK D A I N T G H C G K N J O H F K BX F n D A K I H O K A l Q N E E Y Z YJ o ^ Q B N O P H p H G N L L E J QB C D M A C R N O H I H M P H O Q Ta > e f q r s ? f t b h u > e vI C R w x F N T A N F U N O Q H OT A J Q N E N F F M H A A y L M J I N M TU J O P R M C I z M C D L K C z M CJ F H M { H Q C M F j k H R R H Q K J U HS J E E O C K N F F l Q B N O P H C MU H W M C U J F H M { H Q C M F j k HU H O H K S C M | L N M K J Q J L N K J C OA K N K D A Q B N O P H O C K J R J Q N KU J F H M R J E H A Q E N J I A H E H Q K M CF H M { H Q C M F j k } D H A K J C Od g h ~ > � ~ � h s h b _ � s < ; = � @G H O H R J K A C M H E J P J G J E J K T l Q NN J I A K B N K J O Q E D F H N w � F J PB H M Q E N J I A F J M H Q K E T K C K B HA C R Q E N J I A R J E H F K C Y Z YA E J A K H F C O K B H L M H U J C D Ab c c d ~ d g h � s h < b ? h � t >J N E K T � H N E K B � i y X j � � S JL B T A J Q J N O A C M L M C U J F H M AO K C R N B C A L J K N E C M N R M H HN { � j l Q C O K N Q K X j � N A^ � � � � ~ � � � ~ � � � � � � � � �H M N F J C E C P T A H M U J Q H A O C� � 9 8 5 � 5 � � � 3 � 5 � 2 � � � � � � 4
E H Q K M C O J Q N E E T V \ B H o E H Q KI A K B N K N M H G H J O P A H O K KI A N O F m C M C K B H M K M N O A N QO J Q R J E J O P l N Q Q H A A K B H X UC O K B H [ K N O F N M F Z � [O A D M H F i A Q C I L E H K H D O J }I J K K H F L M J C M K C K B H N L L EG T K B H L B T A J Q J N O C M L M CO F H M H F G T N O C K B H M L M C UO K l [ D M P J Q N E X A A J A K N O K l XH M VB J H E F C R \ H ^ N A y Y Z Y [ \Y Z Y [ \ ] L N K J H O K A �I C D O K �E H A l Q C A K � A B N M H y Q C J O A DN E l J O U H A K J P N K J U H C M C K B H MM J G H M A R C M Q C U H M H F A H M U J= � Y Z Y [ \ ] H O Q C D M N P H AN K K B H K J I H C R N U J A J K �H M j k Q N M F N O F | H H L K B HN K J C O M H } D H A K A l Q C O K N Q KB M C D P B K B H X U N J E J K T Z E N J IY [ \ ] W M C U J F H M Z D A K C IQ N K J C O N K B K K L � m m S S S V G Q GT B C A L J K N E N F I J A A J C O V � C � � b a h < ¡ b r s h b = @O C K J Q H J A M H } D J M H F S B H OT l A H Q C O F N M T l K H M K J N M T � �C D L L M N Q K J Q H � N O F y ¢ � Y NH F N K H A S J E E G H H A K N G E J AQ N O Q H E J O R C M I N K J C O M H E NH R R H Q K J U H F N K H A S J E E O C KO S J E E O C K G H J A A D H F VJ C O A S J E E M H A D E K J O M H F D QC O J Q N E E T N O F K B H J M W M C U J FA C M K C C G K N J O N W M C U J F HN E E £ x x � ¤ ¢ ¤ � Y ¥ ¦ o y § ¨ £P J K N E L B N L M H R J ^ C O K B H AH � C I H W E N O i A N F F M H A A[ \ ] l Q C O K N Q K T C D M H E H QL N P H A R C M K B H N L L M C L M J> ? ~ ; b e © b ? a ª r < s © ?E E G H M H A L C O A J G E H R C M I NA y W Z W A « A L H Q J N E J A K A � IH A K N O F J O P J I N P J O P Q H O KR C E E C S A � Z N E E Z H O K H M � �� ¬ ® ¯ ° ± ² ³ ° ´ ³ µ ® ¶ ® ³ · ® ¸ ·C K L N M K C R K B H { � j l M H R H M5 ¹ º » � 7 8 8 5 � � ¼ � � ½ ¹ ½ � 4 ¾ 7
¿K M C O J Q W N T C M j k R C M Y Z YK C K B H X U N J E J K T L E N K R C M I lQ K J C O A N U N J E N G E H C O K B H XU N J E J K T S H G A J K H N K N U N J E J K T� À ¨ x x y x § m À § � C M ¦ Y x Á} D H j k O D I G H M J O Q E D F J OJ Q N G E H w x � F N T y H E H Q K M C OC R H A A J C O N E L M C U J F H M l K B HU J F H M l C O E T K B H M H O F H M J OX F U N O Q H F W M N Q K J Q H Â D M\ ] � L N T I H O K L E N O D O F HM N O Q H � N O F I H F J Q N E E T OM S J A H D O L M C U H O C M H ^ Q EQ H A S B J Q B N M H O C K I H FA K B H L M C U J F H M i A C R R J Q H K CH Q C L T S J K B K B H L N K J H O K i AK T C D M N U N J E J K T V Q C I C M NI { H A H N M Q B K C C E C M N SH M [ H M U J Q H N K £ x x � Á ¨ À � xG A K ^ V Q C I m L M C U J F H M m K C C E AC M Q N A H I N O N P H I H O K l QO I N | J O P Q B N O P H A N R R H Qy § � Y J E E J O P N F F M H A A � y w �N Q | D L m Q C U H M J O P L M C U J F HB H F N A C R K B H F N K H K B HN K H F K C K B H W M C U J F H M { HG H J A A D H F VQ H F G H O H R J K A C M O C O � L N TF H M { H Q C M F j k Q B N O P H AH M { H Q C M F j k N L L E J Q N K J Cw � Ã �A D G A Q M J G H M i A j k Q N M F K CA N A J K N L L H N M A C O K B H GQ K M C O J Q Q C O O H Q K J U J K T U H OJ N K H L E N O K T L H V> = h < a q ; s © < ? © � b e ¡ < a bN O N P J O P C D K L N K J H O K l O C OI D A K Q C O K N Q K X j � K C C GK H M � Z \ m Z \ X A Q N O A l � {� � � ~ � � Ä ~ � Å Ä Ä l j O K H M O H K �· Æ ° ´ · Ç È ° É ± Ê Ç µ ³ Ë ³ ® ´ µ °M K C K B H Y E D H Z B C J Q H W W7 : 5 Ì ½ Í Í � ½ Î � 8 6 9 Î 5 6 Ï � 9 3 Ì � 6 ¹
¿ Ð Ñ Ò Ó Ô Õ Ö × Ò ØY [ \ ] J A � Ù Ä � � VA D G I J K K H M A A B C D E F Q C O KX U N J E J K T L C M K N E C M C K B H M XT V Q C I VQ E N J I R C M I VO P N O T E H K K H M C M w � F J P J K NO J Q � C M Á ¨ � F N T y L N L H M � QH A H M U J Q H A I N T G H G J E E H FP L M C U J F H M Q N O G J E E R C M KM A H l Z E J O J Q N E  D M A H [ L HM S B J Q B B H N E K B Q N M H L M CO H Q H A A N M T A H M U J Q H A S B J QD F H F A H M U J Q H A � N O FJ Q N E E T O H Q H A A N M T VC �A R J E H �S H G U H O F C M C R T C D M Q BS H G U H O F C M C R T C D M Q B C Jx § £ ¢ à VA m J H ^ Q B N O P H V B K I E K C C G KQ N E E K B H � H F J Q N E Z N M H �Q K J O P K B H L M C U J F H M i A Y Z Y W j N O F W M C U J F H M { H Q CH M A VQ C I L E H K H F N L L E J Q N K J C OH Q C M F j k C O N M H K M C N Q K J UT I H O K C R Q E N J I A R J E H F D OA l K B H L M C U J F H M I D A K Q C OO l L E H N A H Q C O K N Q K K B H WY Z Y [ \ ] y t > h b � \ B H AG N Q | C R K B H A D G A Q M J G H M i AO F C M l J V H V X U N J E J K T C M C K B Hb = Ú � h s h b u < f b � @Û Ü Ý Þ Ý ß à Ý Û á â ã ä å à Û æ ç è ä áé è å ä Û å ê ë ì í î ï î ð ñ ò ó ëô õ ö ÷ ô ø ç á å Û ç ù ú û ü ý þ öÿ å ä Þ ç � Ý á ä å � è â � Ý å � è � � á æ� � � � � � � � � � � � � � � � �û � û � â ç ä á ä å Û ç ù û ß æ � Ý ç ç ä� � � � � � � � � � � � � � � � � � � � � � ! " � #
$ $ % & ' ( ) ) * + * ,è å á è ø - å ä � ä è â ý � ä Ý Û è ú Ý ß -ø - å ä � ä è â � � å è � æ ß Þ ç ù ç . é Þå � � � å � ß Ý � ä / �á � å ä Þ ç � å â Þ Ý Û è � Ý ß ä æ ã �ã é â è � Ý � � â ç ä á ä å Û æ ß � ßè � æ ç Ý ç Ý ß - ä á Ý ç � 0 î 1 2 ÿ þá ä å � ä ç è ù ý Ý ß è ä � ä Ý ã 3 . ß ç Ýæ � Ý ç ç ä æ Û å � ç å à ß Ý Ý è æ ÿá � å ß Ý � ä Þ ä è Ý ã æ ß Û æ è á ææ ä á Ý æ ß á å � � è � Ý è æ � � Ü � ß Ý Ýä á Ý �è å ä Û ÿ å � � ß æ - å � æ � é Ý Û Ý � ä è÷ å Û å à Ý Þ Ý Û è 4 Ý � å ß è Þ Ý5 ú þ 6 ç è å è . ç ù Ý ç � Ý á ä å � � âæ ß ã õ 4 á � å Û à Ý ç 7 8 9 : ÷ æä ç ß Ý á Ý ä - Ý ã ä Û è � Ý 5 ý 5 úÝ é å ç ä ç �Û ã Ý ß è � Ý Û Ý ; û ß æ - ä ã Ý ß ôÛ è å á è è � Ý ø - å ä � ä è â < Ý å � è �û ß æ - ä ã Ý ß ú Ý ß - ä á Ý ç ã Ý � åç . é ç á ß ä é Ý ß = ç . Û ä > . Ý õ 4ç õ 4 á å ß ã 7Ý ß Ý � Ý á è ß æ Û ä á á æ Û Û Ý á è ä - äá ä Þ å à ä Û à ç Ý ß - ä á Ý ç � æ ßë ï í 1 ñ ? @ í 1 í ë 1 í A 2 8 ô B õ : � æ ßö 3 . á � Ý å ß ý å ß ã ä æ � æ à â ç è .æ Þ� C D � � � � E F G H H � I Jä æ Û å � û ß æ - ä ã Ý ß ç ù K å á ä � ä è âL � � � � � � M � � � � N � � � � O � � � � � P
, Q R S T U V W X Y Z [ \ W] ^ _ ` a b c d e e f g h g i j i k lm ^ c c ` n a a o p q r s _ p t c b _ c un p v ` a a ^ p t b r w n p ] ^ s ` n x yz o ^ a s p ` a t p c b w w r { c p a| ^ s } ^ v ` b t s ~ ` � ^ a c ` n `p ] ` n ` s � ` ^ c o ` n b c c o ` c ^ m` � n p ] ^ s ` n � q a c p m ` n � `c a v p n a ` r ` _ c p q c w b c ^ ` t c` t c b c d � � f d � � f � � e � x{ ^ t c o ` v p r r p } ^ t � b n ` b ap ] ^ t � v n p m � n p q w c p � p� z � _ p n w p n b c ` p v v ^ _ ` x z~ ` _ p n s � � xo � t v p n m b c ^ p t � ` c } p n � bn c m ` t c b c � � � f � � � f � � �t q m � ` n m b { _ p t c b ^ t b^ c { ] ` t s p n p n _ b r r c o ` c p� � � � � � � � � � � � � a q �n c o ` v p r r p } ^ t � a ` n ] ^ _ ` aq s ^ ` a b t s � � z a _ b t a x� � � � � ¡ � � ¢ £ ¤ ¥ ¡ ¦ � £ ¢ £ ¤ §{ b t s u t _ ^ r r b n { � n p ] ^ s `¨ © © ª « ¬ ® ¯ ° ± ¬ ² ³ ¬ ´ µ ¶ · « ¯
W U ¸ Z ¹ ºl » � d � f ¼ � ¼ � ½ xu ] b ^ r ^ c { � r ^ ` t c � ` n ] ^ _ ` ay p } ` ] ` n ¾ ^ v c o ` w o { a ^ _ ^ ba ` n ] ^ _ ` a w n p ] ^ s ` s � { b` s � q n a ` ¿ ^ n a c u a a ^ a c b tm ` p v a ` n ] ^ _ ` p n b v c ` n À �` n ] ^ _ ` t q m � ` n ^ t s ^ _ b c ` sa ` n ] ^ _ ` a b t s ^ t w b c ^ ` t ca Ár p w n b _ c ^ _ ` � Â Ã Ä | p ] ^ t �z o ^ a b w w r ^ ` a c p b r r b s s ^ cb c d e e f g h g i j i k l » � d �e ¾ Å ¤ § Æ Æ Ç xb r w o b _ o b n b _ c ` n a } o ^ _ op r r È v n ` ` � n p ] ^ s ` n � q a c p m� a _ n ^ � ` n a xa } o ` t w ` n v p n m ` s ^ t b§ É � Æ ¦ � Ê ¤ § Ë Ì § Æ ¦ Æ Í Î` n | b t q b r  � ` _ c ^ p t À Ä vµ ¯ ° ± Ï ¬ Ð Ñ ¬ « ² ¯ µ Ñ Ò ± ² «
b c d e e f g h g i j i k l » � d �b t p n w n p v ` a a ^ p t b r w n p ] ^t ` m w r p { ` ` p v b w o { a ^ _t c ¾ } o p ^ a q t s ` n c o ` s ^ n `� À � z � o b a n ` ^ m � q n a ` ss p t c o ` a q � a _ n ^ � ` n Ó a � �b s m ^ a a ^ p t a ¾ m b c ` n t ^ c {v n p m � p r p c p � n p q w w n bc ^ p t a ¾ _ o b t � ` a b t s _ b tf ¼ � ¼ � ½ c p p � c b ^ t b t ` }m b { p n m b { t p c s ^ n ` _ cm ` n � ` n ] ^ _ ` t q m � ` n ^ t sw o { a ^ _ ^ b t Ó a p n w n p v ` a a ^v p n m p n ` s ` c b ^ r a x« Ò ± Ô « ³ Ò ¯ µ Õ Ñ Ô Ö ² ³ ¬ ´ µ Ò ¯ µ
� f ¼ � ¼ � ½ xs ` n s p ` a t p c s ^ n ` _ c r { w_ ^ b t b t s w n p v ` a a ^ p t b r` _ c a q w ` n ] ^ a ^ p t p v c o ` �s c o ` w n p ] ^ s ` n �� _ b n s xt p c ^ v ^ _ b c ^ p t a ¾ p n v p n t p cb _ c ^ _ ` �t _ ` r r b c ^ p t a x} � � � u � n ` ` m ` t c xr { v p r r p } c o ` × È s ^ � ^ c b r ws ^ _ b c ` s p t c o ` a q � a _ n ^ �p t b r w n p ] ^ s ` n Ó a p v v ^ _ ` ¾ pµ Õ Ñ Ô ¨ Ø Ù Ú Û Ü Ý Û Þ ß Ú Û à ß á Ü â
` n v p n m� ^ r r ^ t �c ^ v ^ _ b c ^ p t
o b w n ` v ^ ã Ä �� ` n Ó a � �p q c w b c ^ ` t cä å æ ç
180

è é ê ë ì í î ï ë ð ñ ì òè è ó ô î õ ö ÷ ø ë îù ú û ü ý þ û ÿ � û ü� � � þ � � � � � û �
� � � � � �� � � � �� � �� � �� �� �� �� � �� � �� � � �� �� � � ! " # $ # % & ' % # ( ) � $* " + * ! , - . / , / % 0 1 * 23 4 5 6 7 5 8 7 8 6 9 : 7 ; 3 7 8 <5 7 = 6 > ? > @ A B C ? D E F G H D I J K L
� M N � O � � � � P Q O RS � � T � U V � � V T � � W� � � � � � � X Y � Z � � [ � \ ] �� � � � \ ^ � � � ^ \ Z _ ` � � ` �� _ ` [ � \ ] � � � � _ � a bc � _ Z [ � � � ` � ] � Z a \ Z a� � Y _ c Y � \ d Y � Z � ` b\ Y � Y e � � � \ _ ^ ` � � � \ d� � \ a a _ � _ � Z \ ^ a � � \ _ ^ ` f [� T N N g O g h i j k � l � m �^ _ [ _ e _ ^ _ � d \ Z a n � Z � � _ � `� � ^ � ] � � � Z _ ] \ Z a o �� � Z � � � \ ] � _ p � q � _ ] �� r � � p _ a � � s c ` � � Y� Y _ Z a � � ` � � ] � � ] t � �� r � � X a � � � � Y _ Z \ � _ �� r � � \ c � � � � _ u \ � _ � Z� � � � � � � \ ^ ` $ v % . % 0 # , w x * " " # % % -2 # * y " / , # ' 0 " ' 0 z 9 { | ; 4 } ~ { 7 < 7 { 7 5 } 7 = 5 8L H �
_ Z ] ^ c a � ` \ � � � p _ ` _ � Z� � � � _ � a _ ` � Z ^ d � � � c _ � �� � Z ` _ e ^ � � � � \ a � c a _ ] \ � _ Z� � _ � a Y � Z � � ` � � � � � [d \ ^ ^ � c � ` � \ Z a _ Z [ � � � Y[ � � � � � � b � � \ ^ � � ] \ � �� � V T � � � � � � � � �� � � � � Y _ Z \ � _ � Z � _ ^ ^ _ Z ]� ] ^ � \ � _ Z [ � � c ` � ] � Y �� � � ` � � Z ` � � � q � � o \ cY � � � � � p _ ] �� [ � \ ] � � � � _ � a ` � \ � c `� Z `Z ` . / , / % 0 1 * 2 # � / + + % /+ ' / , � # z ( " + * ! , ' / , �8 � = � 5 9 6 } 9 5 6 = 4 5 = � � 9 <
� � �� � \ � [ _ p � ` � � \ ^ � � � Z `� a � � � � Z � � ^ ^ � � ` � � � �Z [ ] ^ \ _ Y ` a c � _ Z [ � � � �[ � \ ] � � � � _ � a f _ ` ` c � � ` �Y _ c Y ` e d � � � � Z a � � � �� b [ � p b] ^ c a � \ � \ _ a � � � � c [ � a� ^ _ \ Z � � _ � � � � � � � r � �c � � Y \ � � a � � ^ � � � � Z � `� _ ^ ^ e � _ Z ] ^ c a � a � Z ] � / � % " z ! � # z � % ! ' � z , * 0 ! � # z v w< 6 � 7 5 7 } 7 3 3 = { � 4 5 < 9 { � =
� � � � � � � � � � �c � \ Z ] � � \ � t � � � ^ \ ] � Y[ � \ ] � � � � _ � a �� \ p � Y \ a � � Z � � c ^ ^ � �� _ � ` � Y � Z � � \ � � � � \ Y � Y� \ p � � � � ] � � _ ] � � � � _ � �� � � � � � � X Y � Z � � [ � \ ] �a \ � � \ Z a e � � � � p _ a � a� � � o � � d ` � � Y� � � � ` � � Z a � Z ] � � � ^ \ � � a
¡
' - ! w # w % / � % " z ! � # z � % ) ¢= 6 4 9 5 � £ 9 { 8 7 6 = 4 � 7 8 4 5 < 9
� � � ¤ ¥ ¥ � ¦ � � § ¨Y � Y e � � ` � � � � � ] � _ p �� � � \ d � � � _ � � � � Y _ c Y b� � Y _ c Y � \ d Y � Z � a c � _ ZY e � � � Z � � � ` � � � [ � \ ] �� � � � � Z a _ Z [ � � � ] ^ \ _ Y� � � _ � a f � � � � � \ ^ � � � ^ \e d ©a � � © ¢ - & * 0 ! # ' 0 y * 0 # � � ! z 0 19 { � = 6 4 9 5 ª { 7 < 7 { 6 9 6 � 7 «
¨ � ¬ § � ® ¯ ¨ ¦ � � §� � V � ° � � m � � k T ± kbZ [ � � � e � Z � � _ � d � \ � \ Z� � � � _ � a b � � � ] ^ \ _ Y ` \Y ` � � \ a � c a _ ] \ � _ Z [ � � �\ Z Y c ` � � � � Y _ Z \ � � � � �1 - # 0 " w v« � ; 7 ² � 9 4 } 7 ³ ³ ´ ³ � � 3 4
§ � ¨ µ � ¶ · ¸ ¹ º » ¹ ¼k P � ½ � � � T P � Q S i O �Z a � � � \ � � � � ] � _ p _ Z [ �\ a � c a _ ] \ � � a \ � � � � � a \] ^ \ _ Y ` \ Z a ` � � t _ Z [ \� Y � Y e � � ¾ ` ] � p � � \ [ �} 4 = 5 = 5 8 ³ { 9 < 7 3 3 4 9 5 = �
¼ ¿ À� \ ^ ` � t Z � � Z \ ` ` c e `� � � S i O b\ � � ` � � ` � � p _ ] � � � Z a � �\ � � � c Z a _ � � � � Y � Y e �b� ³ { 9 Á 4 8 7 {  ³ { 9 Á 4 8 7 {
_ a _ � ` f \ � � � � � X Y � Z � �� � a � _ � � _ Z � � � � _ � ` � Y � Z� � a � � ` Z ¾ � � \ d \ ^ ^ � c � ` �Ã Ä Å Æ ÇÄ È Ã É Ê Ã Ë
181

Blue Cross
for billing a
Most mem
alpha prefi
Prefixes ar
There areQ. The firsidentifiesThe accou
accounts;
offices acr
benefits to
the nation
If TDI is pre
August 1, 2
Identifying th
of is now eas
character net
a red font. Th
Medical Iden
benefits may
PPO NetworBCA = Blue C
HMO NetwoHMO = Blue
BAV = Blue A
s and Blue Shield of
and determining ben
mbers with coverage
ix is very important t
re also used to iden
two types of alpha p
st two positions indicthe Texas Plan unt-specific alpha pr
national accounts a
ross multiple states
o their employees an
al account will asso
esent, subject to TDI r
017 Ì Í Î Ï Î Ð Î Ñ Ò Ñ Óe network that a m
sier with the addition
twork value that will
he network value wil
tification cards wher
y apply.
rk Value:
Choice PPO Networ
rk Values:
Essentials
Advantage HMO Ne
f Texas (BCBSTX) o
nefits. When filing a
through a Blue Cros
to the identification n
tify and correctly rou
prefixes: plan-speci
cate the Plan to whic
refixes are assigned
are employer groups
and offer uniform co
nd the alpha prefix a
ciate to the employe
rules & regulations Ó Ô Õ Ö × Ø Ù Ú Ö Û Õ Ü Õ Û Ï Î Ý Õember is a part
n of the three (3)
be displayed in
ll appear on
re network
rk
etwork
Standard Goffers a wide variety
BCBSTX claim, two
ss Blue Shield Plan a
number as the prefix
ute claims to the ap
ific and account-spe
ch the member/subsc
d to national
s that have
overage
assigned to
er’s name.
Ú Ñ Û Þ Ñ Û Ö Ø Î Ñ Ò ß Ö à á Ø á Öâ
Group ID CardVBIP Commof health care prod
o of the most importa
are assigned a three
x acts as a key eleme
propriate Blue Cros
ecific. The plan-spec
criber belongs while
Ö × ã Õ ä Ö × å Õ Ð Õ Û Ï Õ Ú Ñ æ
ç ç è é ê ëâ ì í î ï ð ñ ò ó ô õ ì
ö
d Elements Qmercial Membucts. Each member
ant elements are the
e letter alpha prefixent in confirming the
s Blue Shield Plan f
cific alpha prefixes a
e the third position ide
÷ ø ù ú û ü ù ú ý ú þ ÿ ø ÿ ú þ ÿ
� � � � � � � � � � Quick Referenbership
r’s/subscriber’s ident
e member’s/subscribx that appears at the
e member’s eligibility
for processing.
are assigned to ever
entifies the product
ÿ ú � � � ÿ ú � ÿ ÿ � � � � ÿ � � �
� � �nce Guide
tification (ID) card d
ber’s ID number an
e beginning of their th
y and coverage infor
ry Blue Cross Blue S
in which the membe
� � ÿ � � � � � ù ú þ � � � ÿ � �
displays important in
nd group number.heir unique identifica
rmation.
Shield plan and star
er/subscriber is enro
� ÿ � þ � � � � � ù � � ú
formation required
ation number. The
rt with X, Y, Z or olled. Note: ZG
182

�
� � � ! " # $ % � $ & ' ( ) *+ , ! - . � / 0 0 � . 1 2 3 & 0 / 1 / � . 0" $ , 4 ! 5 � $ 6 7 7 / 0 8 2 $ , 9 / : $ - 7 � � / , . 0- ! ; < = > ? @ A B B ; < = > C D E > < F G H ; I J G ? A K K > @ L E M < N > K O > @ B ? M @ > N M P M Q > K > P RS T U V W X Y Z Z S T U V [ \ ] V T ^ Y _ _ V X Z ` a ` X ] V b c Y _ d ` X V e ` f ` g V e V f b h X Y g X ` e Z _ Y X ] b Z e V e i V X Z j k T V ` Z V Z V Vb \ V T ] Z b ] f g Y _ h X Y g X ` e Z i V T Y l ` f ^ d Y f Z ] ^ V X U b ] T ] m ] f g b \ V e _ Y X c Y U X S W S [ W Y e e V X d ] ` T e V e i V X Zn S T U V W \ Y ] d V k k o ` f ^ S T U V p ^ a ` f b ` g V q r o s jt u v w x y z { t u v w | y } y ~ � � � y t � � y � � ~ � � y v y ~ �� � Y X e V e i V X Z l \ Y \ ` a V d Y e h T V � e V ^ ] d ` T f V V ^ Z ` f ^ X V � U ] X V ` l ] ^ V a ` X ] V b c Y _X V Z Y U X d V Z b Y e ` f ` g V \ V ` T b \ ` f ^ ] e h X Y a V � U ` T ] b c Y _ T ] _ V �� � f d T U ^ ] f g � i U b f Y b T ] e ] b V ^ b Y � e V e i V X ] f a Y T a V ^ ] f r � p � e U T b ] h T V ] f � U X ] V Z �� X ` f Z h T ` f b Z � q ] g \ � ] Z � o S e V e i V X Z � e U T b ] � d \ X Y f ] d d Y f ^ ] b ] Y f Z T V ` ^ ] f g b Y \ ] g \d Y Z b � \ ] g \ U b ] T ] m ` b ] Y ft u ~ � � � � u ~ � � ~ � � y v y ~ �� � ] Z V ` Z V Z h V d ] _ ] d d ` Z V e ` f ` g V e V f b l ] b \ ` _ Y d U Z Y f b \ V � d Y X V d Y f ^ ] b ] Y f Z Y _p Z b \ e ` � � ] ` i V b V Z � W p � � W q � � ` f ^ W o k � i U b e ` c ` T Z Y V f g ` g V l ] b \ e V e i V X Z^ ] ` g f Y Z V ^ l ] b \ d \ X Y f ] d T Y l V X i ` d � h ` ] f� � � y � � � x y v � ~ � � y v y ~ �� � V ] g \ b e ` f ` g V e V f b ` f ^ Z e Y � ] f g d V Z Z ` b ] Y f� w y � � � x � y � � ~ ~ � ~ � � � ~ � � � � } � � ¡ ¢ | y � ~ � ~ � �� £ f d Y e h T ] d ` b V ^ ` f ^ \ ] g \ X ] Z � h X V g f ` f d c Z U h h Y X b� _ c Y U i V T ] V a V Y f V Y _ b \ V Z V e V e i V X Z d Y U T ^ i V f V _ ] b _ X Y e d ` Z V e ` f ` g V e V f b h X Y g X ` e Z � h T V ` Z V X V ` d \Y U b b Y b \ ] Z Z V d U X V V e ` ] T i Y � ` b ¤ t ¥ ¢ | u � � � y | t u x x � ¦ u | � � � u ~ § ¦ � ¦ � � z ¨ � u v j © Y U l ] T T i V d Y f b ` d b V ^i c ` S W S [ d T ] f ] d ] ` f l \ Y l ] T T l Y X � l ] b \ c Y U b Y ` Z Z V Z Z b \ V e V e i V X ` f ^ d Y Y X ^ ] f ` b V d ` X V j� Y a ` T ] ^ ` b V e V e i V X i V f V _ ] b Z � d ` T T ª « ¬ ¬ ¬ « ® ¯ « ¬ ° ¯ ¬ ` f ^ h X Y a ] ^ V b \ V _ Y T T Y l ] f g �± y ~ y | � x v y v ¦ y | � ~ � u | v � � � u ~ ² r V e i V X ³ ` e V � � o S � [ U i Z d X ] i V X � �¢ | y � � | � w � � u ~ � | ´ � � u � y | � � y � ~ � u | v � � � u ~ ² r V e i V X ] f _ Y X e ` b ] Y f ` Z ` i Y a V � ^ X U g f ` e V �³ � W d Y ^ V � p e Y U f b � � ` c Zµ � ¶ ¶ · ´ � w v y ~ � ¦ y ~ y � � � ² r V e i V X ] f _ Y X e ` b ] Y f ` Z ` i Y a V � � r ¸ ^ V Z d X ] h b ] Y f � � ¹ d Y ^ V � W k �W Y ^ V � ` f ^ ³ k � f U e i V X _ Y X h X V Z d X ] i V X ` f ^ � Y X a V f ^ Y Xk T V ` Z V d Y f b ` d b c Y U X k X Y a ] ^ V X � V T ` b ] Y f Z X V h l ] b \ ` f c � U V Z b ] Y f Z jp Z ` T l ` c Z � b \ ` f � c Y U _ Y X c Y U X \ ` X ^ l Y X � ` f ^ ^ V ^ ] d ` b ] Y f b Y � V f ` ] Z Z ` f d V ` f ^ ] b Z e V e i V X Z j183

Updated, as of June 4, 2018 # QUALITY METRICS PREVENTIVE MEDICINE SERVICES (HEDIS) 1 Breast Cancer Screening
2 Cervical Cancer Screening
3 Colorectal Cancer Screening COMPREHENSIVE DIABETES CARE (HEDIS) 4 Comprehensive Diabetes Care - HbA1c Test (Annual) ASTHMA (HEDIS) 5 Medication Management for People with Asthma (75%) INPATIENT UTILIZATION (HEDIS) 6 Plan All-Cause Readmissions (Actual to Expected) OTHER QUALITY METRICS (HEDIS) 7 Appropriate Use of Imaging Studies for Low Back Pain Assessment
8 Avoidance of Antibiotic for Children with Upper Respiratory Infection
9 Appropriate Testing for Children with Pharyngitis MEMBER EXPERIENCE (CG-CAHPS®) 10 Follow-Up on Test Results
11 Getting Timely Appointments, Care and Information (composite)
12 How Well Providers Communicate with Members (composite)
Updated, as of June 4, 2018
7 Appropriate Use of Imaging Studies for Low Back Pain Assessment
8 Avoidance of Antibiotic for Children with Upper Respiratory Infection
7 Appropriate Use of Imaging Studies for Low Back Pain Assessment
8 Avoidance of Antibiotic for Children with Upper Respiratory Infection 8 Avoidance of Antibiotic for Children with Upper Respiratory Infection
9 Appropriate Testing for Children with Pharyngitis 9 Appropriate Testing for Children with Pharyngitis
8 Avoidance of Antibiotic for Children with Upper Respiratory Infection 8 Avoidance of Antibiotic for Children with Upper Respiratory Infection
7 Appropriate Use of Imaging Studies for Low Back Pain Assessment
8 Avoidance of Antibiotic for Children with Upper Respiratory Infection 8 Avoidance of Antibiotic for Children with Upper Respiratory Infection
184

y
A
A
A
Breast Canc
Cervical CanOne or more measuremenyears prior
Colorectal CAnnual FOBTFlex Sig withiColonoscopy
Diabetes CarHbA1C testin
Diabetes Co HbA1c < 8%
Diabetes CarBlood Pressu
AppropriateLow Back Pa
Medication MAsthma
Metricer Screening
ncer Screeninpap tests durt year or the t
ancer ScreenTn 5 yearswithin 10 yea
re:g
ntrol%
re:ure Control < 1
use of Imagiain Assessm
Management
g AgeExcmama
ngring the two
Age
ningars
Age
AgeTwmo
AgeMoyeaval
140/90AgeLasdef
ingent Asseprimhavescanscorat: hplanof-copain
Asseageasthasthremtreathttpplanof-co
Cre 40-69 clude: History
astectomy or tastectomies.
e 21-64
e 50-75
e 18-75 wo lab tests seonths
e 18-75 ost recent lab ar will be the rue.
e 18-75 st BP of yearfined as < 140
esses adults 18 5mary diagnosis of loe an imaging studn) within 28 days ore indicates betterhttp://www.ncqa.orns/state-of-health-contents/low-back-
n#sthash.m1SLJ7v
esses adults and cwho were identifie
hma and were disphma controller medained on for at leatment period. - Se://www.ncqa.org/re
ns/state-of-health-contents/asthma#s º »
riteriay of bilateral wo unilateral
eparated by 3
value during trepresentative
is in control a0/90
50 years of age witow back pain whoy (plain X-ray, MRof the diagnosis (ar performance) - Srg/report-cards/hecare-quality/2016-
vd.dpuf
children 5–85 yeaed as having perspensed appropriatdications that theyast 75 percent of thee more at: eport-cards/healthcare-quality/2016-
sthash.YLiue5I6.dp
CoCPTHCPUB R
CPT88158817
CPTG0345334538
CPTCPT
thee
CPT
asDocCPT
th a o did notRI or CT a higher
See more ealth--table-
ars of sistent teyheir
h--table-puf
odes to IdeT: 77055-7705PCS: G0202, Revenue: 040
T: 88141-881450-88155, 88175
T: G0104-G0128, 82270,8233, 45338, 4585
T:83036, 8303T II:3044F, 304
T II:3044F, 304
umented in cTII: 3044F, 304
entify Scree57G0204, G020
01, 0403
43, 88147-881164-88167, 8
06, G0120- G2274, 45330, 45339, 45378, 4
3745F, 3046F
45F, 3046F
chart45F
enings06
148,8174,
G0122,45331,45380-
185

¼ ¼
All Cause Readmission (Actual to Expected) This measure is used to assess the number of acute inpatient stays during the measurement year that were followed by an unplanned acute readmission for any diagnosis within 30 days and the predicted probability of an acute readmission, for members 18 years of age and older.
Discharge from a hospital is a critical transition point in a patient's care. Poor care coordination at discharge can lead to adverse events for patients and avoidable rehospitalization. Hospitalization readmissions may indicate poor care or missed opportunities to coordinate care better. Research shows that specific hospital-based initiatives to improve communication with beneficiaries and their caregivers, coordinate care after discharge and improve the quality of care during the initial admission can avert many readmissions.
186

½ ¾ ¿ À Á  ¿ Ã Ä Å Ä Ã Å Æ Ä Ã Ç È É Ê Ë Ì Í Î Ï ¿ Â Ì Ð À Ñ Ò À Ó Ô Õ Ö ×Ë À Ø Â Æ Ù
Appendix: Exhibit 2 Ú Û Ü Ý Þ ß à Ü á â ã ä ã å ä æ ä ç è ä æ Þ ä á é ä ã ä ß æ Þ é ê ê Û ã ã Ü æ àë ì í î ï ð ñ ò ó ô õ î ñ ï ö í ÷ ñ ø î ù ú ò ñ û î ü í ü ô õ ô ù ý ó ó ô ò þ ÷ í û í ÷ ÿ � ñ ò ó ñ ò í ü í õ ô î ÷ ù � ú ÷ í ô ù í ò í ð í ò õ ñ� � � � ô ï ü � � � � ù ú í � î ð î � ô õ î ñ ï ù ÿ� ñ ò � � ù ø î õ ì ô ý ÷ þ � í ð ð í � õ î û í ü ô õ í � ô ÷ ÷ ñ ð õ ì í ü ô õ í ù ù ì ñ ø ï ö í ÷ ñ ø ø î ÷ ÷ ö í ô ü � ý ù õ í üð ñ ò ø ô ò ü ö þ ó ñ ï õ ì ù � î ÿ í ÿ � � í � í ó ö í ò � � � ý ï í � � � ÿ� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *+ ) , ! % - . & ) / 0 1 ! ' # 2 ) 3 4 + ) ' 4' , ' , , ) ( # ' , & ) 2 $ # ! ! % * ) # 5 # ! ' 2 &$ ' % $ ! # � 6 � � � � 6 7 � �8 9 : ; <= 3 ' % # ! > ? @ # ! 4 & ) # ! " ) # &A ! > ? ! 2 & ! 4 5 1 ! , " 3 ) 1 ! #( # ) ? " 2� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AG % ! ) # , ) # ! , ' , , ) ( # ' , 2 4 ? # @ % ( & ! H /, ) % & 2 " # @ ) # & ) & ! ! % 4 ) * & ! , ! ' 2 ? # ! , ! % &1 ! ' # I ) , ! % - H & ) / 0 1 ! ' # 2 ) 3 4 ' 2 ) * : ! $ ! , 5 ! # J K ) *& ! , ! ' 2 ? # ! , ! % & 1 ! ' #L � L � � M � � � � 7 7 N � � � � � � � � � � 6G $ & ) 5 ! # K & + ) 1 ! ' # 2 " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & # ) ? ( : ! $ ! , 5 ! # J K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' #+ @ & ' % ' 3 3 ) + ! 4 ( ' " ? " & ) 0 - 4 ' 1 2 " ! # $ ' 3 ! % 4 ' # 1 ! ' #� M � 7 B � � � � �I ) , ! % + ) ' 4 ' 5 @ 3 ' & ! # ' 3 , ' 2 & ! $ & ) , 1 O + ) , ! % + ) ' 4 ' ? % @ 3 ' & ! # ' 3 , ' 2 & ! $ & ) , 1 + @ & ' 5 @ 3 ' & ! # ' 3, ) 4 @ * @ ! # O + ) , ! % + ) ' 4 & + ) ? % @ 3 ' & ! # ' 3 , ' 2 & ! $ & ) , @ ! 2 + @ & 2 ! # P @ $ ! 4 ' & ! 2 K 0 4 ' 1 2 ) # , ) # ! ' " ' # & O, ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
187

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V Z m
� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *+ ) , ! % H K & ) n 0 1 ! ' # 2 ) 3 4 + ) + ! # !2 $ # ! ! % ! 4 * ) # $ ! # P @ $ ' 3 $ ' % $ ! # � 6 � � � � 6 7 � �8 9 : ; <= 3 ' % # ! > ? @ # ! 4 & ) # ! " ) # &A ! > ? ! 2 & ! 4 5 1 ! , " 3 ) 1 ! #( # ) ? " 2� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AI ) , ! % H 0 & ) n 0 1 ! ' # 2 ) 3 4 + ) ' 4 $ ! # P @ $ ' 3$ 1 & ) 3 ) ( 1 " ! # * ) # , ! 4 @ % & ! & # ! ! 1 ! ' # 2 " # @ ) # & ) & !! % 4 ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' #o pI ) , ! % J . & ) n 0 1 ! ' # 2 ) 3 4 + ) ' 4 $ ! # P @ $ ' 3$ 1 & ) 3 ) ( 1 q ? , ' % " ' " @ 3 3 ) , ' P @ # ? 2 r 8 = s t $ ) u & ! 2 & @ % (" ! # * ) # , ! 4 @ % & ! * @ P ! 1 ! ' # 2 " # @ ) # & ) & ! ! % 4 ) * & !, ! ' 2 ? # ! , ! % & 1 ! ' # I ) , ! % H 0 & ) n 0 1 ! ' # 2 ) 3 4 ' 2 ) * : ! $ ! , 5 ! #J K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' #L � L � � M � � � � 7 7 N � � � � � � � � � � 6� ! , ! ' 2 ? # ! , ! % & 1 ! ' # ' % 4 & + ) 1 ! ' # 2 " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # + @ & % ) , ) # ! & ' % ) % ! ( ' " ) *? " & ) 0 - 4 ' 1 2 4 ? # @ % ( ! ' $ 1 ! ' # ) * $ ) % & @ % ? ) ? 2 ! % # ) 3 3 , ! % &� M � 7 B � � � � �I ) , ! % + ) ' 4 ' 1 2 & ! # ! $ & ) , 1 + @ & % ) # ! 2 @ 4 ? ' 3 $ ! # P @ v w $ ! # P @ $ ' 3 ' ( ! % ! 2 @ 2 ) # ' $ > ? @ # ! 4 ' 5 2 ! % $ ! ) *$ ! # P @ v O , ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *, ! , 5 ! # 2 - . & ) / - 1 ! ' # 2 ) 3 4 + ) ' 4' " " # ) " # @ ' & ! 2 $ # ! ! % @ % ( * ) # $ ) 3 ) # ! $ & ' 3$ ' % $ ! # � 6 � � � � 6 7 � �8 9 : ; <= 3 ' % # ! > ? @ # ! 4 & ) # ! " ) # &A ! > ? ! 2 & ! 4 5 1! , " 3 ) 1 ! # ( # ) ? " 2� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AG % ! ) # , ) # ! 2 $ # ! ! % @ % ( 2 * ) # $ ) 3 ) # ! $ & ' 3 $ ' % $ ! # xy ! $ ' 3 ) $ $ ? 3 & 5 3 ) ) 4 & ! 2 & r y G z � t 4 ? # @ % ( & !, ! ' 2 ? # ! , ! % & 1 ! ' # ) # y ; � u : C F & ! 2 &y 3 ! v @ 5 3 ! 2 @ ( , ) @ 4 ) 2 $ ) " 1 ) # { � $ ) 3 ) % ) ( # ' " 14 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' # ) # & ! * ) ? # 1 ! ' # 2" # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' #{ ) 3 ) % ) 2 $ ) " 1 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' # ) #& ! % @ % ! 1 ! ' # 2 " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # E ! , 5 ! # 2 - K & ) / - 1 ! ' # 2 ) 3 4 ' 2 ) * : ! $ ! , 5 ! #J K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' #L � L � � M � � � � 7 7 N � � � � � � � � � � 6� ! , ! ' 2 ? # ! , ! % & 1 ! ' # ' % 4 & ! 1 ! ' # " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # + @ & % ) ( ' " 2 , ) # ! & ' % 0 - 4 ' 1 24 ? # @ % ( ! ' $ 1 ! ' # � M � 7 B � � � � �E ! , 5 ! # 2 + @ & ' 4 @ ' ( % ) 2 @ 2 ) * $ ) 3 ) # ! $ & ' 3 $ ' % $ ! # ) # & ) & ' 3 $ ) 3 ! $ & ) , 1 O , ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ !$ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #188

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V Z [
� � � � � � � � � � � � = ! # $ ! % & ' ( ! ) *, ! , 5 ! # 2 K | & ) / - 1 ! ' # 2 ) 3 4 + @ & 4 @ ' 5 ! & ! 2 , ! 3 3 @ & ? 2 + ) ' 4 ' % 8 5 F K $& ! 2 & � 6 � � � � 6 7 � �8 9 : ; <8 @ ( " # ! P ' 3 ! % $ ! ) * 4 @ ' 5 ! & ! 2 @ %" ) " ? 3 ' & @ ) %� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G A8 5 F K { & ! 2 & 4 ? # @ % ( , ! ' 2 ? # ! , ! % & 1 ! ' # C ? , 5 ! # ) * ! 3 @ ( @ 5 3 ! , ! , 5 ! # 2 K | & ) / - 1 ! ' # 2 ) 3 4' 2 : ! $ ! , 5 ! # J K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # + @ & 4 @ ' ( % ) 2 @ 2 ) * & 1 " ! K ) # & 1 " ! H 4 @ ' 5 ! & ! 2 5 ' 2 ! 4 ) %$ 3 ' @ , 2 ) # " ' # , ' $ 1 4 ' & ' z { z < � } # ! $ ! @ P ! 2 * # ) ,@ & 2 " ' # , ' $ 1 5 ! % ! * @ & , ' % ' ( ! #� � � 7 B � � � � � � � � � � � 6E ! , 5 ! # 2 + ) , ! ! & & ! ' ( ! # ! > ? @ # ! , ! % & @ % & ! , ! ' 2 ? # ! , ! % & 1 ! ' # ' % 4 , ! ! & ' & 3 ! ' 2 & ) % ! ) * & !* ) 3 3 ) + @ % ( 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' # ) # & ! 1 ! ' # " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # xF & 3 ! ' 2 & ) % ! ' , 5 ? 3 ' & ) # 1 " # ! 2 $ # @ " & @ ) % * ) # @ % 2 ? 3 @ % ) # ' % ) # ' 3 1 " ) ( 3 1 $ ! , @ $ q ' % & @ u 1 " ! # ( 3 1 $ ! , @ $ 4 # ? (F & 3 ! ' 2 & & + ) * ' $ ! u & ) u * ' $ ! ! % $ ) ? % & ! # 2 + @ & 4 @ * * ! # ! % & 4 ' & ! 2 ) * 2 ! # P @ $ ! @ % ' % ' , 5 ? 3 ' & ) # 1 2 ! & & @ % ( w! , ! # ( ! % $ 1 # ) ) , w ) 5 2 ! # P ' & @ ) % 2 ! & & @ % ( ) # % ) % u ' $ ? & ! @ % " ' & @ ! % & 2 ! & & @ % ( + @ & ' 4 @ ' ( % ) 2 @ 2 ) * 4 @ ' 5 ! & ! 2F & 3 ! ' 2 & ) % ! * ' $ ! u & ) u * ' $ ! ! % $ ) ? % & ! # @ % ' % @ % " ' & @ ! % & 2 ! & & @ % ( + @ & ' 4 @ ' ( % ) 2 @ 2 ) * 4 @ ' 5 ! & ! 2� M � 7 B � � � � �E ! , 5 ! # 2 + ) 4 ) % ) & ' P ! ' 4 @ ' ( % ) 2 @ 2 ) * 4 @ ' 5 ! & ! 2 @ % ' % 1 2 ! & & @ % ( 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' # ) #1 ! ' # " # @ ) # ~ � � + ) ' 4 ' 4 @ ' ( % ) 2 @ 2 ) * ( ! 2 & ' & @ ) % ' 3 ) # 2 & ! # ) @ 4 u @ % 4 ? $ ! 4 4 @ ' 5 ! & ! 2 @ % ' % 1 2 ! & & @ % ( w 4 ? # @ % (& ! , ! ' 2 ? # ! , ! % & 1 ! ' # w ) # & ! 1 ! ' # " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # O , ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
189

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V � X
� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *, ! , 5 ! # 2 w - & ) | - 1 ! ' # 2 ) 3 4 4 ? # @ % ( & !, ! ' 2 ? # ! , ! % & 1 ! ' # w + ) + ! # ! @ 4 ! % & @ * @ ! 4' 2 ' P @ % ( " ! # 2 @ 2 & ! % & ' 2 & , ' ' % 4 + )+ ! # ! 4 @ 2 " ! % 2 ! 4 ' " " # ) " # @ ' & !, ! 4 @ $ ' & @ ) % 2 & ! 1 # ! , ' @ % ! 4 ) % 4 ? # @ % (& ! & # ! ' & , ! % & " ! # @ ) 4� 6 � � � � 6 7 � �8 9 : ; <y ) # " ! # 2 @ 2 & ! % &' 2 & , ' & @ $ 2 w $ ) % 2 @ 2 & ! % &? 2 ! ) * ' 2 & , ' $ ) % & # ) 3 3 ! #, ! 4 @ $ ' & @ ) % 2 , ' 1@ , " # ) P ! ' 2 & , ' $ ) % & # ) 3� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G A� ! % ? , 5 ! # ) * , ! , 5 ! # 2 + ) * @ 3 3 ! 4 " # ! 2 $ # @ " & @ ) % 2* ) # ' 2 & , ' $ ) % & # ) 3 3 ! # , ! 4 @ $ ' & @ ) % & ' & $ ) P ! # ! 4 ' &3 ! ' 2 & / - " ! # $ ! % & ) * & ! 4 ' 1 2 * # ) , & ! * @ # 2 &$ ) % & # ) 3 3 ! # , ! 4 @ $ ' & @ ) % " # ! 2 $ # @ " & @ ) % 4 ? # @ % ( & !, ! ' 2 ? # ! , ! % & 1 ! ' # & # ) ? ( & ! 3 ' 2 & 4 ' 1 ) * & !, ! ' 2 ? # ! , ! % & 1 ! ' # E ! , 5 ! # 2 + @ & " ! # 2 @ 2 & ! % & ' 2 & , ' + ) ' # ! -& ) | - 1 ! ' # 2 ) 3 4 ' 2 ) * : ! $ ! , 5 ! # J K ) * & !, ! ' 2 ? # ! , ! % & 1 ! ' #L � L � � M � � � � 7 7 N � � � � � � � � � � 6� ! , ! ' 2 ? # ! , ! % & 1 ! ' # ' % 4 & ! 1 ! ' # " # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # + @ & % ) , ) # ! & ' % ) % ! 0 - u 4 ' 1( ' " @ % $ ) P ! # ' ( ! ! ' $ 1 ! ' # O , ? 2 & ' P ! " ' # , ' $ 1 5 ! % ! * @ & 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #� M � 7 B � � � � �E ! , 5 ! # 2 + ) ' 4 ' 4 @ ' ( % ) 2 @ 2 * # ) , ' % 1 ) * & ! * ) 3 3 ) + @ % ( ' & ' % 1 & @ , ! 4 ? # @ % ( & ! , ! , 5 ! # � 2 @ 2 & ) # 1& # ) ? ( : ! $ ! , 5 ! # J K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # x9 , " 1 2 ! , ' w $ # ) % @ $ ) 5 2 & # ? $ & @ P ! " ? 3 , ) % ' # 1 4 @ 2 ! ' 2 ! r { G = : t w ) 5 2 & # ? $ & @ P ! $ # ) % @ $ 5 # ) % $ @ & @ 2{ # ) % @ $ # ! 2 " @ # ' & ) # 1 $ ) % 4 @ & @ ) % 2 4 ? ! & ) * ? , ! 2 q P ' " ) # 2{ 1 2 & @ $ * @ 5 # ) 2 @ 2F $ ? & ! # ! 2 " @ # ' & ) # 1 * ' @ 3 ? # !E ! , 5 ! # 2 + ) ' 4 % ) ' 2 & , ' $ ) % & # ) 3 3 ! # , ! 4 @ $ ' & @ ) % 2 4 @ 2 " ! % 2 ! 4 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #E ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
190

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V � W
� � � � � � � � � � � � y ) # , ! , 5 ! # 2 K | & )n 0 1 ! ' # 2 ) 3 4 w & ! % ? , 5 ! # ) * ' $ ? & !@ % " ' & @ ! % & 2 & ' 1 2 4 ? # @ % ( & !, ! ' 2 ? # ! , ! % & 1 ! ' # & ' & + ! # ! * ) 3 3 ) + ! 45 1 ' % ' $ ? & ! # ! ' 4 , @ 2 2 @ ) % * ) # ' % 14 @ ' ( % ) 2 @ 2 + @ & @ % J . 4 ' 1 2 ) * & !, ! , 5 ! # � 2 4 @ 2 $ ' # ( ! ' % 4 & !" # ! 4 @ $ & ! 4 " # ) 5 ' 5 @ 3 @ & 1 ) * ' % ' $ ? & !# ! ' 4 , @ 2 2 @ ) %� 6 � � � � 6 7 � �A ! ' 4 , @ 2 2 @ ) % 2 ' # ! $ ) 2 & 3 1 ' % 42 ) , ! & @ , ! 2 " # ! P ! % & ' 5 3 !A ! ' 4 , @ 2 2 @ ) % 2 $ ' % @ % 4 @ $ ' & !> ? ' 3 @ & 1 $ ) % $ ! # % 2 ) #) " " ) # & ? % @ & @ ! 2 * ) # @ , " # ) P ! 4$ ) ) # 4 @ % ' & @ ) % ) * " ) 2 & 4 @ 2 $ ' # ( !$ ' # !� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AC ? , 5 ! # ) * 8 9 : ; < u 4 ! * @ % ! 4 ; % 4 ! v 8 ) 2 " @ & ' 3F 4 , @ 2 2 @ ) % 2 + @ & ' # ! ' 4 , @ 2 2 @ ) % + @ & @ % J . 4 ' 1 2 ) *& ! @ % 4 ! v 4 @ 2 $ ' # ( ! 4 ' & ! F 3 3 ' $ ? & ! @ % " ' & @ ! % & 2 & ' 1 2 * ) # , ! , 5 ! # 2 K | & ) n 01 ! ' # 2 ) 3 4 r ' 2 ) * & ! 4 @ 2 $ ' # ( ! 4 ' & ! t + @ & '4 @ 2 $ ' # ( ! 4 ' & ! ) % ) # 5 ! & + ! ! % � ' % ? ' # 1 K ' % 4: ! $ ! , 5 ! # K ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # O @ % $ 3 ? 4 !' $ ? & ! ' 4 , @ 2 2 @ ) % 2 & ) 5 ! ' P @ ) # ' 3 ! ' 3 & $ ' # !* ' $ @ 3 @ & @ ! 2L � L � � M � � � � 7 7 N � � � � � � � � � � 6J n - 4 ' 1 2 " # @ ) # & ) & ! @ % 4 ! v 4 @ 2 $ ' # ( ! 4 ' & ! & # ) ? ( J . 4 ' 1 2 ' * & ! # & ! @ % 4 ! v 4 @ 2 $ ' # ( ! 4 ' & ! + @ & % ), ) # ! & ' % 0 - 4 ' 1 2 ( ' " @ % $ ) P ! # ' ( ! � M � 7 B � � � � �= 3 ' % % ! 4 # ! u ' 4 , @ 2 2 @ ) % 2 + @ & @ % J . 4 ' 1 2 r , ' @ % & ! % ' % $ ! $ ! , ) & ! # ' " 1 w " # @ % $ @ " ' 3 4 @ ' ( % ) 2 @ 2 ) *# ! ' 5 @ 3 @ & ' & @ ) % w ) # ( ' % & # ' % 2 " 3 ' % & w " ) & ! % & @ ' 3 3 1 " 3 ' % % ! 4 " # ) $ ! 4 ? # ! + @ & ) ? & ' % " # @ % $ @ " ' 3 ' $ ? & !4 @ ' ( % ) 2 @ 2 t< & ' 1 2 * ) # & ! * ) 3 3 ) + @ % ( # ! ' 2 ) % 2 x� ; % " ' & @ ! % & 2 & ' 1 2 + @ & 4 @ 2 $ ' # ( ! 2 * ) # 4 ! ' & � F $ ? & ! @ % " ' & @ ! % & 4 @ 2 $ ' # ( ! + @ & ' " # @ % $ @ " ' 3 4 @ ' ( % ) 2 @ 2 * ) # " # ! ( % ' % $ 16 � � � � � � � 6 7 � � � � � N 6 � � � �: ' & ' ' # ! # ! " ) # & ! 4 * ) # & ! * ) 3 3 ) + @ % ( @ % 4 @ $ ' & ) # 2 xK � { ) ? % & ) * @ % 4 ! v ) 2 " @ & ' 3 2 & ' 1 2 r 4 ! % ) , @ % ' & ) # tH � { ) ? % & ) * J . u 4 ' 1 # ! ' 4 , @ 2 2 @ ) % 2 r % ? , ! # ' & ) # tJ � F P ! # ' ( ! ' 4 � ? 2 & ! 4 " # ) 5 ' 5 @ 3 @ & 1 ) * # ! ' 4 , @ 2 2 @ ) %y # ) , & @ 2 4 ' & ' w & ! # ' & @ ) ) * & ! ' $ & ? ' 3 # ! ' 4 , @ 2 2 @ ) % # ' & ! & ) & ! ' P ! # ' ( ! ' 4 � ? 2 & ! 4 " # ) 5 ' 5 @ 3 @ & 1 ) *# ! ' 4 , @ 2 2 @ ) % @ 2 $ ' 3 $ ? 3 ' & ! 4
191

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V � �
� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *, ! , 5 ! # 2 + @ & ' " # @ , ' # 1 4 @ ' ( % ) 2 @ 2 ) *3 ) + 5 ' $ � " ' @ % + ) 4 @ 4 % ) & ' P ! ' %@ , ' ( @ % ( 2 & ? 4 1 r " 3 ' @ % } u # ' 1 w E A ; w { �2 $ ' % t + @ & @ % H | 4 ' 1 2 ) * & ! 4 @ ' ( % ) 2 @ 2 � 6 � � � � 6 7 � �8 9 : ; <; , ' ( @ % ( * ) # 3 ) + 5 ' $ � @ 2 @ ( ? & @ 3 @ � ' & @ ) % q @ ( $ ) 2 & * ' $ & ) #D % % ! $ ! 2 2 ' # 1 @ , ' ( @ % ( ! v " ) 2 ! 2 , ! , 5 ! # 2& ) ? % % ! $ ! 2 2 ' # 1 # ' 4 @ ' & @ ) %� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AF % @ , ' ( @ % ( 2 & ? 4 1 + @ & ' 4 @ ' ( % ) 2 @ 2 ) * 3 ) + 5 ' $ �" ' @ % $ ) % 4 ? $ & ! 4 ) % & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! ) #@ % H | 4 ' 1 2 * ) 3 3 ) + @ % ( & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! F 3 3 , ! , 5 ! # 2 w K | 1 ! ' # 2 ) 3 4 ' 2 ) * � ' % ? ' # 1 K ) *& ! , ! ' 2 ? # ! , ! % & " ! # @ ) 4 & ) - . 1 ! ' # 2 ) 3 4 ' 2 ) *: ! $ ! , 5 ! # J K ) * & ! , ! ' 2 ? # ! , ! % & " ! # @ ) 4 w + ) ' 4 ' % ) ? & " ' & @ ! % & ) # ! , ! # ( ! % $ 1 4 ! " ' # & , ! % &! % $ ) ? % & ! # + @ & ' " # @ % $ @ " ' 3 4 @ ' ( % ) 2 @ 2 ) * 3 ) +5 ' $ � " ' @ %L � L � � M � � � � 7 7 N � � � � � � � � � � 6K | . 4 ' 1 2 r 2 @ v , ) % & 2 t " # @ ) # & ) & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! & # ) ? ( H | 4 ' 1 2 ' * & ! # & ! @ % 4 ! v ! " @ 2 ) 4 !2 & ' # & 4 ' & ! + @ & ) ? & ( ' " 2 � � � 7 B � � � � � � � � � � � 6E ! , 5 ! # 2 w K | 1 ! ' # 2 ) 3 4 ' 2 ) * & ! 5 ! ( @ % % @ % ( ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & ) - . 1 ! ' # 2 ' 2 ) * & ! ! % 4 ) *& ! , ! ' 2 ? # ! , ! % & 1 ! ' # w + ) ' 4 xF & 3 ! ' 2 & ) % ! ) ? & " ' & @ ! % & ) # ! , ! # ( ! % $ 1 4 ! " ' # & , ! % & ! % $ ) ? % & ! # + @ & ' " # @ % $ @ " ' 3 4 @ ' ( % ) 2 @ 2 ) * 3 ) +5 ' $ � " ' @ % 4 ? # @ % ( & ! @ % & ' � ! " ! # @ ) 4C ) 3 ) + 5 ' $ � " ' @ % 4 @ ' ( % ) 2 @ 2 4 ? # @ % ( & ! 2 @ v u , ) % & r K | . u 4 ' 1 t " ! # @ ) 4 " # @ ) # & ) & ! * @ # 2 & 3 ) + 5 ' $ �" ' @ % ! % $ ) ? % & ! #8 ' 4 % ) 4 @ ' ( % ) 2 @ 2 * ) # + @ $ ' % @ , ' ( @ % ( 2 & ? 4 1 @ % & ! " # ! 2 ! % $ ! ) * 3 ) + 5 ' $ � " ' @ % @ 2 $ 3 @ % @ $ ' 3 3 1@ % 4 @ $ ' & ! 4� ! @ % & ' � ! " ! # @ ) 4 @ 2 * # ) , & ! 5 ! ( @ % % @ % ( ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & ) H | 4 ' 1 2 " # @ ) # & ) & ! ! % 4 ) * & !, ! ' 2 ? # ! , ! % & 1 ! ' # � M � 7 B � � � � �E ! , 5 ! # 2 + ) ' 4 ' 4 @ ' ( % ) 2 @ 2 ) * $ ' % $ ! # ' & ' % 1 & @ , ! 4 ? # @ % ( & ! , ! , 5 ! # � 2 @ 2 & ) # 1 & # ) ? ( H | 4 ' 1 2' * & ! # & ! ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! O # ! $ ! % & & # ' ? , ' w @ % & # ' P ! % ) ? 2 4 # ? ( ' 5 ? 2 ! ) # % ! ? # ) 3 ) ( @ $ @ , " ' @ # , ! % & O ' % 1& # ' ? , ' 4 ? # @ % ( & ! J , ) % & 2 " # @ ) # & ) & ! ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! & # ) ? ( H | 4 ' 1 2 ' * & ! # & ! ! " @ 2 ) 4 ! 2 & ' # &4 ' & ! O 4 @ ' ( % ) 2 @ 2 ) * 8 ; s w 2 " @ % ' 3 @ % * ! $ & @ ) % w ) # % ! ? # ) 3 ) ( @ $ @ , " ' @ # , ! % & O � @ 4 % ! 1 ) # ) & ! # ) # ( ' % & # ' % 2 " 3 ' % & O, ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
192

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V � �
� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) * $ @ 3 4 # ! % J, ) % & 2 & ) K | 1 ! ' # 2 ) 3 4 + ) + ! # ! ( @ P ! % '4 @ ' ( % ) 2 @ 2 ) * ? " " ! # # ! 2 " @ # ' & ) # 1 @ % * ! $ & @ ) % r D A ; t ' % 4+ ! # ! % ) & 4 @ 2 " ! % 2 ! 4 ' % ' % & @ 5 @ ) & @ $ " # ! 2 $ # @ " & @ ) % � 6 � � � � 6 7 � �8 9 : ; <F $ ? & ! $ ' # ! , ! ' 2 ? # !E ! ' 2 ? # ! * ) # " ! 4 @ ' & # @ $" ) " ? 3 ' & @ ) %F % & @ 5 @ ) & @ $ ) P ! # ? 2 !� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G A: @ 2 " ! % 2 ! 4 ' " # ! 2 $ # @ " & @ ) % * ) # ' % & @ 5 @ ) & @ $ , ! 4 @ $ ' & @ ) % ) % ) # & # ! !4 ' 1 2 ' * & ! # & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! F 3 3 $ @ 3 4 # ! % J , ) % & 2 & ) K | 1 ! ' # 2 ) 3 4' 2 ) * � ? 3 1 K ) * & ! 1 ! ' # " # @ ) # & ) & !, ! ' 2 ? # ! , ! % & 1 ! ' # & ) K | 1 ! ' # 2 ) 3 4 ) *� ? % ! J . ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' #+ @ & ' D A ;L � L � � M � � � � 7 7 N � � � � � � � � � � 6J . 4 ' 1 2 " # @ ) # & ) & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! & # ) ? ( & # ! ! 4 ' 1 2 ' * & ! # & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & !� � � 7 B � � � � � � � � � � � 6{ @ 3 4 # ! % w J , ) % & 2 & ) K | 1 ! ' # 2 ) 3 4 4 ? # @ % ( & ! @ % & ' � ! " ! # @ ) 4 w + ) ' 4 ' D A ; ! % $ ) ? % & ! # + @ & xC ) ) & ! # 4 @ ' ( % ) 2 @ 2 " # ! 2 ! % &C ) ' % & @ 5 @ ) & @ $ , ! 4 @ $ ' & @ ) % " # ! 2 $ # @ 5 ! 4 ) # # ! * @ 3 3 ! 4 + @ & @ % J . 4 ' 1 2 " # @ ) # & ) & ! ! % $ ) ? % & ! # ) # 2 & @ 3 3 ' $ & @ P !) % & ! 4 ' & ! ) * & ! ! % $ ) ? % & ! #C ) 2 " ! $ @ * @ ! 4 $ ) , " ! & @ % ( 4 @ ' ( % ) 2 @ 2 ) % ) # + @ & @ % & # ! ! 4 ' 1 2 * ) 3 3 ) + @ % ( & ! ! % $ ) ? % & ! #� ! @ % & ' � ! " ! # @ ) 4 @ 2 * # ) , 2 @ v , ) % & 2 " # @ ) # & ) & ! 5 ! ( @ % % @ % ( ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & ) 2 @ v , ) % & 2" # @ ) # & ) & ! ! % 4 ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # � � ! ! ' # 3 @ ! 2 & ! " @ 2 ) 4 ! 4 ? # @ % ( & ! @ % & ' � ! " ! # @ ) 4 @ 2 & ! @ % 4 ! v! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! � � M � 7 B � � � � �E ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
193

Q R S T U V S W X Y X W Y Z X W [ \ ] ^ _ ` a b c S V ` d T e f T g h i j k_ T l V � �
� � � � � � � � � � � � � ! " ! # $ ! % & ' ( ! ) *$ @ 3 4 # ! % J & ) K | 1 ! ' # 2 ) 3 4 + ) + ! # !4 @ ' ( % ) 2 ! 4 + @ & " ' # 1 % ( @ & @ 2 w 4 @ 2 " ! % 2 ! 4' % ' % & @ 5 @ ) & @ $ ' % 4 # ! $ ! @ P ! 4 ' ( # ) ? " F2 & # ! " & ) $ ) $ $ ? 2 r 2 & # ! " t & ! 2 & * ) # & !! " @ 2 ) 4 ! � 6 � � � � 6 7 � �8 9 : ; <F $ ? & ! $ ' # ! , ! ' 2 ? # !E ! ' 2 ? # ! * ) # " ! 4 @ ' & # @ $ " ) " ? 3 ' & @ ) %F % & @ 5 @ ) & @ $ ) P ! # ? 2 !� 6 � � � 6 7 � B 7 6 � � � �C D E 9 A F � G A : 9 C G E ; C F � G AF ( # ) ? " F 2 & # ! " & ) $ ) $ $ ? 2 & ! 2 & @ % & ! 2 ! P ! % u 4 ' 1" ! # @ ) 4 * # ) , & # ! ! 4 ' 1 2 " # @ ) # & ) & ! @ % 4 ! v ! " @ 2 ) 4 !2 & ' # & 4 ' & ! & # ) ? ( & # ! ! 4 ' 1 2 ' * & ! # & ! @ % 4 ! v! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! { @ 3 4 # ! % H 1 ! ' # 2 ) 3 4 ' 2 ) * � ? 3 1 K ) * & ! 1 ! ' #" # @ ) # & ) & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & ) K | 1 ! ' # 2 ) 3 4' 2 ) * � ? % ! J . ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # + )+ ! # ! 4 @ ' ( % ) 2 ! 4 + @ & " ' # 1 % ( @ & @ 2 ' % 44 @ 2 " ! % 2 ! 4 ' % ' % & @ 5 @ ) & @ $L � L � � M � � � � 7 7 N � � � � � � � � � � 6J . 4 ' 1 2 " # @ ) # & ) & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! & # ) ? ( J 4 ' 1 2 ' * & ! # & ! @ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & !� � � 7 B � � � �� � � � � � � 6{ @ 3 4 # ! % w H & ) K | 1 ! ' # 2 ) 3 4 4 ? # @ % ( & ! @ % & ' � ! " ! # @ ) 4 w + ) ' 4 ' " ' # 1 % ( @ & @ 2 ! % $ ) ? % & ! # + @ & xC ) ) & ! # 4 @ ' ( % ) 2 @ 2 " # ! 2 ! % &F % ' % & @ 5 @ ) & @ $ " # ! 2 $ # @ 5 ! 4 + @ & @ % & # ! ! 4 ' 1 2 ) * & ! ! % $ ) ? % & ! #C ) ' % & @ 5 @ ) & @ $ , ! 4 @ $ ' & @ ) % " # ! 2 $ # @ 5 ! 4 ) # # ! * @ 3 3 ! 4 + @ & @ % J . 4 ' 1 2 " # @ ) # & ) & ! ! % $ ) ? % & ! # ) # 2 & @ 3 3' $ & @ P ! ) % & ! 4 ' & ! ) * & ! ! % $ ) ? % & ! #� ! @ % & ' � ! " ! # @ ) 4 @ 2 * # ) , 2 @ v , ) % & 2 � � � � � & ) & ! 5 ! ( @ % % @ % ( ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # & ) 2 @ v , ) % & 2� � � � � & ) & ! ! % 4 ) * & ! , ! ' 2 ? # ! , ! % & 1 ! ' # � � ! ! ' # 3 @ ! 2 & ! " @ 2 ) 4 ! 4 ? # @ % ( & ! @ % & ' � ! " ! # @ ) 4 @ 2 & !@ % 4 ! v ! " @ 2 ) 4 ! 2 & ' # & 4 ' & ! � � M � 7 B � � � � �E ! , 5 ! # 2 + @ & ' & 3 ! ' 2 & ) % ! ) 2 " @ $ ! $ 3 ' @ , ) # ! % $ ) ? % & ! # 4 ? # @ % ( & ! , ! ' 2 ? # ! , ! % & 1 ! ' #
194

� � � � � � � � � � � � � � � � � � � � � � � ¡ � � � � ¢ £ ¤ � ¥ � ¦ § ¨ � � � � © ª � � « ¨ � � « ¬ � � ® ¨ � ¢ � � © ¥ « ¯ � ° § ¨ � « � � ¢ «± � ² � � ³ ´ � � � « � ° µ ¨ ¢ � � � ³ � � � �
¶ · ¸ · ¹ º » ¼ ½ · ¾ ¿ À Á ¸ ¾Â à ¼ Ä Å Æ Ç È É Ê Ë Ì Í Î Ï Î Ð Ñ Ò Ó Ô Õ Ò Ö × Í Î Ø Ñ × Î Ù × Ù Ú Û Ï Ð Î Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ô Ú Ï × Í Î Ý Þ ß à Û Ñ Ø Õ × á â Î × Ï Õ Ð Ù ãº Ê Æ ä Å å Ë æ Í Î Ø Ñ × Î Ù × Ù Î × Ú Ô ç è é Ó ê Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ð Ñ Ò ë Î Ô Ú Û Ò Ö Ñ × × Í Î ì Þ í Ý î Î ë Ù Õ × Î ËÍ × × Ü Ë ï ï î î î Ã Ò Ð à Ñ Ã Ú Ï ð ï Í Î Ö Õ Ù ñ à Û Ñ Ø Õ × á ñ â Î Ñ Ù Û Ï Î â Î Ò × ï Í Î Ö Õ Ù ñ â Î Ñ Ù Û Ï Î Ù Ã Ý Ø × Í Ú Û ð Í × Í Î Ý ç ò í Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ö ÚÒ Ú × Ï Î à Û Õ Ï Î Ü Û Ï Ð Í Ñ Ù Î Ù Ú Ô Ø Õ Ð Î Ò Ù Î Ù ó ç Î Ñ Ø × Í Þ Ñ Ï Î ê Î Ï ô Õ Ð Î Þ Ú Ï Ü Ú Ï Ñ × Õ Ú Ò õ ç Þ ê Þ ö Ù × Õ Ø Ø Ï Î Ð Ú â â Î Ò Ö Ù × Í Ñ × Ñ ÒÝ Þ ß Ú ë × Ñ Õ Ò Ù Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ö Õ Ï Î Ð × Ø á Ô Ï Ú â × Í Î Ù Ú Û Ï Ð Î Ã æ Í Î Ý ç ò í î Î ë Ù Õ × Î Ð Ú Ò × Ñ Õ Ò Ù ë Ú × Í Õ Ò Ô Ú Ï â Ñ × Õ Ú Ò Ô Ú ÏÝ ç ò í â Î Ñ Ù Û Ï Î Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Í × × Ü Ë ï ï î î î à à Û Ñ Ø Õ × á Õ Ò Ö Õ Ð Ñ × Ú Ï Ù Ã Ñ Í Ï à à ð Ú ô ï ÷ Ú Ö Û Ø Î Ù ï Ü à Õ ø Ï Î Ù Ú Û Ï Ð Î Ù Ã Ñ Ù Ü ù ö Ñ Ò ÖÞ Ý ç ú ê Ù Û Ï ô Î á Ù õ Í × × Ü Ë ï ï î î î Ã Ñ Í Ï à à ð Ú ô ï Ð Ñ Í Ü Ù ï Õ Ò Ö Î ù Ã Í × â Ø ö Ãû à ¼ Ä Å Æ Ç È É Ê ü Ó Ò × Í Î Ð Ú Ò × Î ù × Ú Ô × Í Î Ý Þ ß í Û Ñ Ø Õ × á ò Î Ü Ú Ï × Ù ó î Í Ñ × Ö Ú Î Ù Ñ ý ç è é Ó ê ñ Ø Õ þ Î ÿ Î Ò ð Õ Ò Î â Î Ñ Ò ãº Ê Æ ä Å å Ë Ý Ð Î Ï × Õ Ô Õ Î Ö ç è é Ó ê Î Ò ð Õ Ò Î Õ Ù Ö Î Ù Õ ð Ò Î Ö × Ú Ï Û Ò × Í Î Ü Ï Õ Ú Ï Ð Ñ Ø Î Ò Ö Ñ Ï á Î Ñ Ï Ú Ô Ð Ø Ñ Õ â Ù Ñ ð Ñ Õ Ò Ù × × Í Î â Ú Ù ×Ð Û Ï Ï Î Ò × á Î Ñ Ï Î Ò ð Õ Ò Î Ñ ô Ñ Õ Ø Ñ ë Ø Î Ã õ è ù Ñ â Ü Ø Î Ë ç è é Ó ê û �  � î Ú Û Ø Ö ë Î Ï Û Ò Û Ù Õ Ò ð û �  � Ð Ø Ñ Õ â Ù Ã ö æ Í Î Î Ò ð Õ Ò ÎÛ Ò Ö Î Ï ð Ú Î Ù ì Þ í Ý Ð Î Ï × Õ Ô Õ Ð Ñ × Õ Ú Ò ó Ñ Ò Ö × Í Î Ï Î Ù Û Ø × Ù Ñ Ï Î Ñ Û Ö Õ × Î Ö Ã � Ú Ï × Í Î â Ú Ò × Í Ø á � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù ó × Í Î Ù ÎÏ Î Ü Ú Ï × Ù Û Ù Î Ð Û Ï Ï Î Ò × á Î Ñ Ï Ð Ø Ñ Õ â Ù â Î Ñ Ù Û Ï Î Ö Ñ ð Ñ Õ Ò Ù × Ñ Ð Ú Ü á Ú Ô × Í Î Ð Û Ï Ï Î Ò × á Î Ñ Ï Ð Î Ï × Õ Ô Õ Î Ö ó Ñ Û Ö Õ × Î Ö ç è é Ó êÎ Ò ð Õ Ò Î Ã æ Í Î Õ Ò × Î Ò × Ú Ô × Í Î Ù Î Ï Î Ü Ú Ï × Ù Õ Ù × Ú ð Õ ô Î Î Ñ Ð Í Ý Þ ß Ñ Ò Î Ñ Ï Ø Õ Î Ï ô Õ Î î Ú Ô à Û Ñ Ø Õ × á Ñ Ð × Õ ô Õ × á Ã Ý ð Ñ Õ Ò ó ë Î Ð Ñ Û Ù ÎÚ Ô × Í Î Ñ Ø × Î Ï Ò Ñ × Î × Õ â Î Ô Ï Ñ â Î Ù Õ Ò ô Ú Ø ô Î Ö ó × Í Õ Ù Õ Ù Ð Ú Ò Ù Õ Ö Î Ï Î Ö Ñ Ò ý Ú Ô Ô ñ Ø Ñ ë Î Ø ÿ Û Ù Î Ú Ô ç è é Ó ê ó Ñ Ò Ö Ù Ú × Í Î Ù Î Ï Î Ü Ú Ï × ÙÑ Ï Î Ð Ú Ò Ù Õ Ö Î Ï Î Ö Ï Û Ò Ñ ð Ñ Õ Ò Ù × Ñ ý ç è é Ó ê ñ Ø Õ þ Î ÿ Î Ò ð Õ Ò Î Ã� ¹ · º ¾ ¿ � º ¸ � · ¹ ¾ � ¹ · · ¸ À ¸ ¶ � � · ¹ � À � º » � º ¸ � · ¹ ¾ � ¹ · · ¸ À ¸ ¶ � � Á » Á ¹ · � ¿ º » � º ¸ � · ¹ ¾ � ¹ · · ¸ À ¸ ¶ à ¼ Ä Å Æ Ç È É Ê Ë ú Ñ × Õ Î Ò × Ù Ñ Ü Ü Î Ñ Ï Õ Ò × Í Î â Ú Ò × Í Ø á � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × î Í Ú Í Ñ ô Î Í Ñ Ö Ñ â Ñ Ù × Î Ð × Ú â á ó Ú ÏÍ á Ù × Î Ï Î Ð × Ú â á ó Ú Ï Ð Ú Ø Î Ð × Ú â á ó Ú Ï Ü Ï Õ Ú Ï Ð Ñ Ò Ð Î Ï Ö Õ Ñ ð Ò Ú Ù Õ Ù Ã ç Ú î Ð Ñ Ò Ñ Ò Ý Þ ß Ü Ï Ú ô Õ Ö Î × Í Î Õ Ò Ô Ú Ï â Ñ × Õ Ú Ò Ò Î Î Ö Î Ö× Ú Î ù Ð Ø Û Ö Î Ñ Ü Ñ × Õ Î Ò × Ô Ï Ú â × Í Î Ö Î Ò Ú â Õ Ò Ñ × Ú Ï ãº Ê Æ ä Å å Ë æ Í Î ç è é Ó ê Î Ò ð Õ Ò Î Ð Ñ Ø Ð Û Ø Ñ × Î Ù × Í Î Ù Î ð Ñ Ü Ù ë Ñ Ù Î Ö Ú Ò Ð Ø Ñ Õ â Ù Ö Ñ × Ñ Ã Ì Í Î Ò Ñ Ü Ñ × Õ Î Ò × Ô Õ Ï Ù × Ù Î Î Ù ÑÜ Ï Ú ô Õ Ö Î Ï î Õ × Í Õ Ò × Í Î Ý Þ ß Ô Ú Ï Ñ Ð Í Î Ð þ Û Ü ó × Í Î Ü Ï Ú ô Õ Ö Î Ï Ù Í Ú Û Ø Ö Õ Ò Ö Õ Ð Ñ × Î × Í Õ Ù Ü Ï Î ô Õ Ú Û Ù â Î Ö Õ Ð Ñ Ø Í Õ Ù × Ú Ï á ë áÑ Ö Ö Õ Ò ð × Í Î Ñ Ü Ü Ï Ú Ü Ï Õ Ñ × Î Ö Õ Ñ ð Ò Ú Ù Õ Ù Ð Ú Ö Î õ Ù ö × Ú × Í Î Ð Ø Ñ Õ â à à ¼ Ä Å Æ Ç È É Ê ü ú Ñ × Õ Î Ò × Ù Ñ Ü Ü Î Ñ Ï Õ Ò × Í Î â Ú Ò × Í Ø á � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × î Í Ú Í Ñ Ö Ñ Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð Ò Ú × Ù Û ë â Õ × × Î Öô Õ Ñ Ñ Ð Ø Ñ Õ â ó Ú Ï î Í Õ Ø Î Ð Ú ô Î Ï Î Ö ë á Ñ Ò Ú × Í Î Ï Í Î Ñ Ø × Í Ü Ø Ñ Ò Ã õ è ù Ñ â Ü Ø Î Ù Ð Ú Û Ø Ö Õ Ò Ð Ø Û Ö Î Ñ Ô Ï Î Î Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð× Í Ï Ú Û ð Í Ñ Ü Û ë Ø Õ Ð Í Î Ñ Ø × Í Ö Î Ü Ñ Ï × â Î Ò × Ú Ï î Ú Ï þ Ü Ø Ñ Ð Î Î ô Î Ò × ó Ú Ï Ñ Ò á Ù Ð Ï Î Î Ò Õ Ò ð î Í Î Ï Î Ñ Ð Ø Ñ Õ â î Ñ Ù Ò Ú ×Ù Û ë â Õ × × Î Ö × Ú ç Þ ê Þ Ô Ú Ï Ñ Ò á Ï Î Ñ Ù Ú Ò Ã ö ç Ú î Ð Ñ Ò Ñ Ò Ý Þ ß Ü Ï Ú ô Õ Ö Î × Í Î Õ Ò Ô Ú Ï â Ñ × Õ Ú Ò Ò Î Î Ö Î Ö × Ú Õ Ò Ð Ø Û Ö Î × Í Ñ ×Ü Ñ × Õ Î Ò × Õ Ò × Í Î Ò Û â Î Ï Ñ × Ú Ï ãº Ê Æ ä Å å Ë æ Í Î ç è é Ó ê Î Ò ð Õ Ò Î Ð Ñ Ø Ð Û Ø Ñ × Î Ù × Í Î Ù Î ð Ñ Ü Ù ë Ñ Ù Î Ö Ú Ò Ð Ø Ñ Õ â Ù Ö Ñ × Ñ Ã ê Õ Ò Ð Î ç Þ ê Þ Õ Ù Ð Ú Ò × Ï Ñ Ð × Û Ñ Ø Ø áÚ ë Ø Õ ð Ñ × Î Ö × Ú Í Ñ ô Î × Í Î à Û Ñ Ø Õ × á â Î Ñ Ù Û Ï Î Ù Ñ Û Ö Õ × Î Ö Ô Ú Ï â Ú Ù × Ý Þ ß Ù ó × Í Î Ö Ñ × Ñ × Õ Î Ö × Ú × Í Î Ù Î â Î Ñ Ù Û Ï Î Ù Ò Î Î Ö Ù × ÚÚ Ï Õ ð Õ Ò Ñ × Î Ô Ï Ú â Ñ Ò Ñ Û Ö Õ × Ñ ë Ø Î Ù Ú Û Ï Ð Î Ã ç Þ ê Þ Õ Ù î Ú Ï þ Õ Ò ð Ú Ò Ñ Ò Î Ò Í Ñ Ò Ð Î â Î Ò × × Ú Ñ Ø Ø Ú î � � � � � � �195

� � � � � � � � � � � � � � � � � � � � � � � ¡ � � � � ¢ £ ¤ � ¥ � ¦ § ¨ � � � � © ª � � « ¨ � � « ¬ � � ® ¨ � ¢ � � © ¥ « ¯ � ° § ¨ � « � � ¢ «± � ² � � ³ ´ � � � « � ° µ ¨ ¢ � � � ³ � � � �
Ù Û Ü Ü Ø Î â Î Ò × Ñ Ø Ö Ñ × Ñ Ô Ú Ï Ý Þ ß Ù Û Ù Õ Ò ð Ù × Ñ Ò Ö Ñ Ï Ö õ Ñ Û × Ú â Ñ × Î Ö ö Î Ø Î Ð × Ï Ú Ò Õ Ð Ô Õ Ø Î Ù ó Ñ Ù Ö Î Ô Õ Ò Î Ö Õ Ò × Í Î ç è é Ó êò Ú Ñ Ö â Ñ Ü Ö Ú Ð Û â Î Ò × Ü Ï Ú ô Õ Ö Î Ö ë á ç Þ ê Þ î Í Õ Ð Í î Ú Û Ø Ö Ü Ï Ú ô Õ Ö Î Ñ â Î Ð Í Ñ Ò Õ Ù â × Ú Î Ò Ñ ë Ø Î Ý Þ ß Ù × Ú Ù Û ë â Õ × × Í Õ ÙÙ Ð Ï Î Î Ò Õ Ò ð Ö Ñ × Ñ î Í Õ Ø Î Ô Û Ø Ô Õ Ø Ø Õ Ò ð Ñ Û Ö Õ × Ï Î à Û Õ Ï Î â Î Ò × Ù ÃÝ Ò Ý Þ ß Ð Ú Û Ø Ö Õ â Ü Ï Ú ô Î × Í Î Õ Ï Ù Ð Ú Ï Î Ù Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ë á Ï Î ô Õ Î î Õ Ò ð × Í Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Î Ñ Ï Ø á Ñ Ò ÖÏ Î Ñ Ð Í Õ Ò ð Ú Û × × Ú Ü Ñ × Õ Î Ò × Ù î Í Ú Ñ Ï Î Î Ø Õ ð Õ ë Ø Î Ô Ú Ï Ù Ð Ï Î Î Ò Õ Ò ð Ã Ý Ò Ú × Í Î Ï Ñ Ð × Õ Ú Ò Ñ Ò Ý Þ ß Ð Ú Û Ø Ö × Ñ þ Î Õ Ù × Ú Ï Î ô Õ Î î × Í Î� Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ñ Ò Ö Õ Ö Î Ò × Õ Ô á Ü Ï Ú ô Õ Ö Î Ï Ù î Í Ú Í Ñ ô Î Ø Ñ Ï ð Î Ï Ø Õ Ù × Ù Ú Ô Ü Ñ × Õ Î Ò × Ù î Õ × Í Ñ ð Ñ Ü ó Ñ Ò Ö Ð Ú Ñ Ð Í × Í ÎÜ Ï Ú ô Õ Ö Î Ï Ù Ñ Ù Ñ Ü Ü Ï Ú Ü Ï Õ Ñ × Î Ã� à ¼ Ä Å Æ Ç È É Ê ü Ì Í á Õ Ù × Í Î Ò Û â Î Ï Ñ × Ú Ï Ù Ú Í Õ ð Í Õ Ò â á ÷ Ñ Ï Ð Í û �  � � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ô Ú Ï â á ë Ï Î Ñ Ù × Ð Ñ Ò Ð Î ÏÙ Ð Ï Î Î Ò Õ Ò ð ó Ð Î Ï ô Õ Ð Ñ Ø Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð Ñ Ò Ö Ð Ú Ø Ú Ï Î Ð × Ñ Ø Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð â Î Ñ Ù Û Ï Î Ù Û Ù Õ Ò ð Ú Ò Ø á Ú Ò Î â Ú Ò × Í Ú ÔÐ Ø Ñ Õ â Ù Ö Ñ × Ñ Ë Ð Ø Ñ Õ â Ù Õ Ò Ð Û Ï Ï Î Ö ï Ü Ñ Õ Ö Ô Ú Ï Â ï  ï û �  � �  ï  ï û �  � ãº Ê Æ ä Å å ü ê Ú â Î â Î Ñ Ù Û Ï Î Ù Ö Î Ô Õ Ò Î × Í Î Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î á Î Ñ Ï Ñ Ù × Í Î Ð Û Ï Ï Î Ò × â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ó î Í Õ Ø Î Ú × Í Î Ïâ Î Ñ Ù Û Ï Î Ù Ù Û Ð Í Ñ Ù × Í Î ë Ï Î Ñ Ù × Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð ó Ð Î Ï ô Õ Ð Ñ Ø Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð Ñ Ò Ö Ð Ú Ø Ú Ï Î Ð × Ñ Ø Ð Ñ Ò Ð Î ÏÙ Ð Ï Î Î Ò Õ Ò ð Ñ Ø Ù Ú Õ Ò Ð Ø Û Ö Î Ð Ø Ñ Õ â Ù Ô Ú Ï × Õ â Î Ü Î Ï Õ Ú Ö Ù Ü Ï Õ Ú Ï × Ú × Í Î Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î Ü Î Ï Õ Ú Ö Ã æ Í Î Ù Î × Õ â Î Ü Î Ï Õ Ú Ö Ù Ñ Ï ÎÚ Û × Ø Õ Ò Î Ö Õ Ò × Í Î ç è é Ó ê Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ã� Ú Ï Î ù Ñ â Ü Ø Î ó Ô Ú Ï × Í Î ë Ï Î Ñ Ù × Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð â Î Ñ Ù Û Ï Î ó û � â Ú Ò × Í Ù Ú Ô Ð Ø Ñ Õ â Ù Ü Ï Õ Ú Ï × Ú × Í Î Î Ò Ö Ú Ô × Í Îâ Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Õ Ù Û Ù Î Ö Ã Ó Ô × Í Î Ü Ñ × Õ Î Ò × Í Ñ Ö Ñ â Ñ â â Ú ð Ï Ñ â Õ Ò é Î Ð Î â ë Î Ï û �  � Ô Ú Ï × Í Î û �  � Ð Ñ Ø Î Ò Ö Ñ Ïá Î Ñ Ï Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î Ü Î Ï Õ Ú Ö ó × Í Î á î Õ Ø Ø Ù × Õ Ø Ø â Î Î × × Í Î Ò Û â Î Ï Ñ × Ú Ï Ð Ï Õ × Î Ï Õ Ñ ÃÝ Ò Î ù Ñ â Ü Ø Î Ú Ô Ñ â Î Ñ Ù Û Ï Î × Í Ñ × Ö Î Ô Õ Ò Î Ù × Í Î Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î á Î Ñ Ï Ñ Ù × Í Î Ð Û Ï Ï Î Ò × â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ñ Ï Î × Í ÎÐ Ú â Ü Ï Î Í Î Ò Ù Õ ô Î Ö Õ Ñ ë Î × Î Ù Ð Ñ Ï Î â Î Ñ Ù Û Ï Î Ù Ã æ Í Î Ð Ú â Ü Ï Î Í Î Ò Ù Õ ô Î Ö Õ Ñ ë Î × Î Ù Ð Ñ Ï Î â Î Ñ Ù Û Ï Î Ù Ï Î à Û Õ Ï Î â Ú Ï ÎÔ Ï Î à Û Î Ò × â Ú Ò Õ × Ú Ï Õ Ò ð Ñ Ò Ö Ù Ð Ï Î Î Ò Õ Ò ð Ù Ú × Í Î ç è é Ó ê × Õ â Î Ø Õ Ò Î Ø Ú Ú þ Ù Ô Ú Ï Ð Ø Ñ Õ â Ù î Õ × Í Õ Ò × Í Î Ð Û Ï Ï Î Ò × Ü Î Ï Ô Ú Ï â Ñ Ò Ð Îá Î Ñ Ï Ú Ò Ø á Ã� Á � � ¹ · � · ¸ ¾ À � · � À º � · ¿ · ¾ � º ¹ · � � � º � � ¿ · ¾ ¿ � º ¸ ¸ ½ º » �¼ Ä Å Æ Ç È É Ê Ë Ì Í á Ö Ú Ü Ñ × Õ Î Ò × Ù Ñ Ü Ü Î Ñ Ï Õ Ò × Í Î â Ú Ò × Í Ø á � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × î Í Ú Ö Ú Ò Ú × Í Ñ ô Î Ö Õ Ñ ë Î × Î Ù ãº Ê Æ ä Å å Ë � Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ó × Í Î ç è é Ó ê Î Ò ð Õ Ò Î Õ Ù × Ï Õ ð ð Î Ï Î Ö ë á Ñ Ð × Õ ô Õ × Õ Î Ù Õ Ò Î Õ × Í Î Ï × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ß ò× Í Î á Î Ñ Ï Ü Ï Õ Ú Ï Ã æ Í Î × Ï Õ ð ð Î Ï Ð Ú Û Ø Ö ë Î Ô Ï Ú â Ñ Ö Õ Ñ ð Ò Ú Ù Õ Ù Ð Ú Ö Î Ú Ò Ð Ø Ñ Õ â Ù ó Ú Ï Ô Ï Ú â Ü Ï Î Ù Ð Ï Õ Ü × Õ Ú Ò Ö Ñ × Ñ Ã Ý ÒÎ ù Ñ â Ü Ø Î Ù Ð Î Ò Ñ Ï Õ Ú î Ú Û Ø Ö ë Î Ñ Ü Ñ × Õ Î Ò × î Í Ú Í Ñ Ö ë Î Î Ò Ö Õ Ñ ð Ò Ú Ù Î Ö î Õ × Í Ö Õ Ñ ë Î × Î Ù Ù Î ô Î Ï Ñ Ø á Î Ñ Ï Ù Ñ ð Ú ó ë Û ×Õ Ò Ù × Î Ñ Ö Ú Ô Ù Î Î Õ Ò ð Ñ Ü Ï Õ â Ñ Ï á Ð Ñ Ï Î Ü Í á Ù Õ Ð Õ Ñ Ò Ô Ú Ï Ñ Ð Í Î Ð þ Û Ü õ î Í Î Ï Î Ü Ï Î Ù Û â Ñ ë Ø á Ñ Ò ç ë Ý Â Ð × Î Ù × î Ú Û Ø Ö ë ÎÐ Ú Ò Ö Û Ð × Î Ö ö ó × Í Î Ü Ñ × Õ Î Ò × Ù Õ â Ü Ø á Ð Ú Ò × Õ Ò Û Î Ö × Ú Í Ñ ô Î Ü Ï Î Ù Ð Ï Õ Ü × Õ Ú Ò Ù Ï Î Ô Õ Ø Ø Î Ö Ã æ Í Î Ï Î Ô Ú Ï Î ó × Í Î Ü Ñ × Õ Î Ò × î Õ Ø Ø Ð Ú Ò × Õ Ò Û Î× Ú ë Î Õ Ò Ð Ø Û Ö Î Ö Õ Ò × Í Î Ö Î Ò Ú â Õ Ò Ñ × Ú Ï Ãé Õ Ñ ë Î × Î Ù â Î â ë Î Ï Õ Ö Î Ò × Õ Ô Õ Ð Ñ × Õ Ú Ò Ð Ï Õ × Î Ï Õ Ñ õ Ñ Ù Ú Ô ç è é Ó ê û �  � ö÷ Î â ë Î Ï Ù Ñ ð Î Â � ñ � � á Î Ñ Ï Ù Ú Ô Ñ ð Î â Î Î × Õ Ò ð Ñ Ò á Ú Ô × Í Î Ô Ú Ø Ø Ú î Õ Ò ð Ð Ï Õ × Î Ï Õ Ñ Ë� × î Ú Ô Ñ Ð Î ñ × Ú ñ Ô Ñ Ð Î Ð Ø Ñ Õ â Ù Ú Ï Î Ò Ð Ú Û Ò × Î Ï Ù Ú Ò Ö Õ Ô Ô Î Ï Î Ò × Ö Ñ × Î Ù Ú Ô Ù Î Ï ô Õ Ð Î Õ Ò Ñ Ò Ú Û × Ü Ñ × Õ Î Ò × Ù Î × × Õ Ò ð ó Î â Î Ï ð Î Ò Ð áÏ Ú Ú â Ù Î × × Õ Ò ð Ú Ï Ò Ú Ò ñ Ñ Ð Û × Î Õ Ò Ü Ñ × Õ Î Ò × Ù Î × × Õ Ò ð î Õ × Í Ñ Ö Õ Ñ ð Ò Ú Ù Õ Ù Ú Ô Ö Õ Ñ ë Î × Î Ù� Ú Ò Î Ô Ñ Ð Î ñ × Ú ñ Ô Ñ Ð Î Ð Ø Ñ Õ â Ú Ï Î Ò Ð Ú Û Ò × Î Ï Õ Ò Ñ Ò Ñ Ð Û × Î Õ Ò Ü Ñ × Õ Î Ò × Ù Î × × Õ Ò ð î Õ × Í Ñ Ö Õ Ñ ð Ò Ú Ù Õ Ù Ú Ô Ö Õ Ñ ë Î × Î Ù� â Î â ë Î Ï Ù î Í Ú î Î Ï Î Ö Õ Ù Ü Î Ò Ù Î Ö Õ Ò Ù Û Ø Õ Ò Ú Ï Ú Ï Ñ Ø Í á Ü Ú ð Ø á Ð Î â Õ Ð Ù Ñ Ò Ö ï Ú Ï Ñ Ò × Õ Í á Ü Î Ï ð Ø á Ð Î â Õ Ð Ù Ú Ò Ñ ÒÑ â ë Û Ø Ñ × Ú Ï á ë Ñ Ù Õ Ù Ã ì Ú × Î Ë � Ø Û Ð Ú Ü Í Ñ ð Î ï â Î × Ô Ú Ï â Õ Ò Õ Ù Ò Ú × Õ Ò Ð Ø Û Ö Î Ö ë Î Ð Ñ Û Ù Î Õ × Õ Ù Û Ù Î Ö × Ú × Ï Î Ñ × Ð Ú Ò Ö Õ × Õ Ú Ò ÙÚ × Í Î Ï × Í Ñ Ò Ö Õ Ñ ë Î × Î Ù � â Î â ë Î Ï Ù î Õ × Í Ö Õ Ñ ë Î × Î Ù Ú Ò × Í Î Ù Î â Î Ö Õ Ð Ñ × Õ Ú Ò Ù Ñ Ï Î Õ Ö Î Ò × Õ Ô Õ Î Ö × Í Ï Ú Û ð Í Ö Õ Ñ ð Ò Ú Ù Õ ÙÐ Ú Ö Õ Ò ð Ú Ò Ø á Ã196

� � � � � � � � � � � � � � � � � � � � � � � ¡ � � � � ¢ £ ¤ � ¥ � ¦ § ¨ � � � � © ª � � « ¨ � � « ¬ � � ® ¨ � ¢ � � © ¥ « ¯ � ° § ¨ � « � � ¢ «± � ² � � ³ ´ � � � « � ° µ ¨ ¢ � � � ³ � � � �
Ý Ò Ý Þ ß Ð Ú Û Ø Ö Õ â Ü Ï Ú ô Î × Í Î Õ Ï Ù Ð Ú Ï Î Ù Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ë á Ï Î ô Õ Î î Õ Ò ð × Í Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Î Ñ Ï Ø á Ñ Ò ÖÏ Î Ñ Ð Í Õ Ò ð Ú Û × × Ú Ü Ñ × Õ Î Ò × Ù î Í Ú Í Ñ ô Î Ò Ú × Í Ñ Ö Ñ Ò ç ë Ý Â Ð × Î Ù × Ã Ý Ò Ú × Í Î Ï Ñ Ð × Õ Ú Ò Ñ Ò Ý Þ ß Ð Ú Û Ø Ö × Ñ þ Î Õ Ù × Ú Ï Î ô Õ Î î× Í Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ñ Ò Ö Õ Ö Î Ò × Õ Ô á Ü Ï Ú ô Õ Ö Î Ï Ù î Í Ú Í Ñ ô Î Ø Ñ Ï ð Î Ï Ø Õ Ù × Ù Ú Ô Ü Ñ × Õ Î Ò × Ù î Õ × Í Ñ ð Ñ Ü ó Ñ Ò Ö Ð Ú Ñ Ð Í × Í ÎÜ Ï Ú ô Õ Ö Î Ï Ù Ñ Ù Ñ Ü Ü Ï Ú Ü Ï Õ Ñ × Î Ã� · � À � º ¿ À Á ¸ � º ¸ º ¶ · � · ¸ ¿ � Á ¹ � · Á � » · � À ¿ � º ¾ ¿ � � º � ! " �# à ¼ Ä Å Æ Ç È É Ê Ë Ì Í á Ñ Ï Î × Í Î Ï Î Ù Ú Ô Î î â Î â ë Î Ï Ù Õ Ò × Í Î Ò Û â Î Ï Ñ × Ú Ï Ñ Ò Ö ï Ú Ï Ö Î Ò Ú â Õ Ò Ñ × Ú Ï ãº Ê Æ ä Å å ü æ Í Õ Ù â Î Ñ Ù Û Ï Î Õ Ù Ö Î Ù Õ ð Ò Î Ö × Ú Ð Ú Û Ò × × Í Î Ò Û â ë Î Ï Ú Ô Ü Ñ × Õ Î Ò × Ù Ö Õ Ñ ð Ò Ú Ù Î Ö î Õ × Í Ñ Ù × Í â Ñ î Í Ú Ô Õ Ø Ø × Í Î Õ ÏÐ Ú Ò × Ï Ú Ø Ø Î Ï â Î Ö Õ Ð Ñ × Õ Ú Ò Ô Ú Ï � � $ Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ã æ Í Î ç è é Ó ê Î Ò ð Õ Ò Î Õ Ù Ö Î Ù Õ ð Ò Î Ö × Ú Ð Ú Û Ò × Ô Ú Ï × Í ÎÔ Û Ø Ø â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ó Ò Ú × Ô Ú Ï � � $ Ú Ô × Í Î á Î Ñ Ï × Ú Ö Ñ × Î Ã æ Í Î Ï Î Ô Ú Ï Î ó × Í Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù î Õ Ø Ø Ò Ú × Í Ñ ô ÎÑ Ò á Ü Ñ × Õ Î Ò × Ù Õ Ò × Í Î Ò Û â Î Ï Ñ × Ú Ï Û Ò × Õ Ø Ñ Ô × Î Ï Ù Õ ù â Ú Ò × Í Ù Õ Ò × Ú × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ó î Í Î Ò Ð Ø Ñ Õ â Ù Ô Ï Ú â Ü Ñ × Õ Î Ò × ÙÔ Õ Ø Ø Õ Ò ð Ü Ï Î Ù Ð Ï Õ Ü × Õ Ú Ò Ù ô Õ Ñ â Ñ Õ Ø Ú Ï Ö Î Ï Ñ Ò Ö Í Ñ ô Î Ú Ï Ö Î Ï Î Ö Ñ × Í Õ Ï Ö # � ñ Ö Ñ á Ù Û Ü Ü Ø á î Õ Ø Ø Ù × Ñ Ï × × Ú Ô Õ Ø × Î Ï × Í Ï Ú Û ð Í × Í Îç è é Ó ê Î Ò ð Õ Ò Î Ã æ Í Î Ò Û â Î Ï Ñ × Ú Ï Ù Í Ú Û Ø Ö × Í Î Ò Õ Ò Ð Ï Î Ñ Ù Î Î ù Ü Ú Ò Î Ò × Õ Ñ Ø Ø á × Í Ï Ú Û ð Í × Í Î Ï Î â Ñ Õ Ò Ö Î Ï Ú Ô × Í Î á Î Ñ Ï ÃÝ Ò Ý Þ ß Ð Ñ Ò Ü Ï Ú Ñ Ð × Õ ô Î Ø á Õ â Ü Ï Ú ô Î Ù Ð Ú Ï Î Ù Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ë á Ï Î Ñ Ð Í Õ Ò ð Ú Û × × Ú Ü Ñ × Õ Î Ò × Ù Ñ Ù Ñ Ï Î â Õ Ò Ö Î Ï × Ú Ï Î Ô Õ Ø ØÐ Ú Ò × Ï Ú Ø Ø Î Ï â Î Ö Õ Ð Ñ × Õ Ú Ò Ù Ã� » º ¸ º » » % � º ½ ¾ · ¹ · º � � À ¾ ¾ À Á ¸ ¾ � º � ¿ ½ º » ¿ Á · & � · � ¿ · � � � à ¼ Ä Å Æ Ç È É Ê Ë ç Ú î Õ Ù × Í Î Î ù Ü Î Ð × Î Ö Ï Ñ × Î Ð Ñ Ø Ð Û Ø Ñ × Î Ö ãº Ê Æ ä Å å ü æ Í Î Î ù Ü Î Ð × Î Ö Ï Ñ × Î Õ Ù Ð Ñ Ø Ð Û Ø Ñ × Î Ö ë á × Í Î ç è é Ó ê Î Ò ð Õ Ò Î ó Û Ù Õ Ò ð Ð Ï Õ × Î Ï Õ Ñ Ù Î × Ô Ú Ï × Í ë á ì Þ í Ý ë Ñ Ù Î Ö Ú Ò× Í Î Ý Þ ß ' Ù Ü Ú Ü Û Ø Ñ × Õ Ú Ò Ö Î â Ú ð Ï Ñ Ü Í Õ Ð Ù Ñ Ò Ö Ï Õ Ù þ ÷ ( ) Å * Ç Å + ¹ Å , + - È Æ Æ È É Ê ¹ , Ç Å . º / Å å , 0 Å º + 1 Ä Æ Ç Å + � å É 2 , 2 È 3 È Ç 4 É 5 ¹ Å , + - È Æ Æ È É Ê ó Ð Ñ Ø Ð Û Ø Ñ × Î Ö Û Ù Õ Ò ð Ï Õ Ù þÑ Ö 6 Û Ù × â Î Ò × ë Ñ Ù Î Ö Ú Ò Ñ ð Î ó ð Î Ò Ö Î Ï ó Ð Ú â Ú Ï ë Õ Ö Õ × Õ Î Ù ó Ü Ï Î Ù Î Ò Ð Î Ú Ô Ù Û Ï ð Î Ï Õ Î Ù Ñ Ò Ö Ö Õ Ù Ð Í Ñ Ï ð Î Ð Ú Ò Ö Õ × Õ Ú Ò Ã ú Ø Î Ñ Ù ÎÏ Î Ô Î Ï × Ú ì Þ í Ý Ô Ú Ï × Í Î Ô Û Ø Ø Ù Ü Î Ð Õ Ô Õ Ð Ñ × Õ Ú Ò Ù Ã  à ¼ Ä Å Æ Ç È É Ê ü ç Ú î Ð Ñ Ò Ñ Ò Ý Þ ß Õ â Ü Ï Ú ô Î × Í Î Ñ Ð × Û Ñ Ø × Ú Î ù Ü Î Ð × Î Ö Ï Ñ × Õ Ú Ú Ô Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ù ãº Ê Æ ä Å å Ë 7 Ò Ø Õ þ Î Ú × Í Î Ï ç è é Ó ê â Î Ñ Ù Û Ï Î Ù ó Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ù Õ Ù Ò Ú × Ï Î Ñ Ø Ø á Ñ ð Ñ Ü × Í Ñ × Ð Ñ Ò ë Î Ð Ø Ú Ù Î Ö Ã Ý Ò Ý Þ ßÐ Ñ Ò Õ â Ü Ï Ú ô Î Õ × Ù Ï Ñ × Õ Ú Ú Ô Ñ Ð × Û Ñ Ø × Ú Î ù Ü Î Ð × Î Ö Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ù ë á Ð Ú Ñ Ð Í Õ Ò ð Õ × Ù Ô Ñ Ð Õ Ø Õ × Õ Î Ù × Ú Ð Ú Ú Ï Ö Õ Ò Ñ × Î Ü Ñ × Õ Î Ò ×Ð Ñ Ï Î Ñ Ò Ö Ö Õ Ù Ð Í Ñ Ï ð Î Ù î Õ × Í Ñ ð Ú Ñ Ø Ú Ô Ï Î Ö Û Ð Õ Ò ð Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ù ÃÌ Î Û Ò Ö Î Ï Ù × Ñ Ò Ö × Í Ñ × Î ô Î Ï á Ñ Ö â Õ Ù Ù Õ Ú Ò Ð Ñ Ò Ò Ú × ë Î Ü Ï Î ô Î Ò × Î Ö ë Û × Î ô Î Ï á Ñ Ö â Õ Ù Ù Õ Ú Ò Ð Ñ Ò ë Î × Ñ Ï ð Î × Î Ö î Õ × ÍÜ Ï Ú Ü Î Ï Ö Õ Ù Ð Í Ñ Ï ð Î Ü Ø Ñ Ò Ò Õ Ò ð ó Ô Ú Ø Ø Ú î Û Ü Ñ Ò Ö Ð Ñ Ï Î Ð Ú Ú Ï Ö Õ Ò Ñ × Õ Ú Ò Î Ô Ô Ú Ï × Ù × Ú Ü Ï Î ô Î Ò × Ñ � ñ Ö Ñ á Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ã æ Í Îâ Î Ñ Ù Û Ï Î Ô Ú Ù × Î Ï Ù 6 Ú Õ Ò × Ñ Ð Ð Ú Û Ò × Ñ ë Õ Ø Õ × á Ñ Ð Ï Ú Ù Ù Î Ò × Õ × Õ Î Ù Ù Û Ð Í Ñ Ù Í Ú Ù Ü Õ × Ñ Ø Ù ó Í Ú â Î Ð Ñ Ï Î ó Ü Ï Õ â Ñ Ï á Ð Ñ Ï Î Ñ Ò ÖÙ Ü Î Ð Õ Ñ Ø Õ Ù × Ù Õ Ò Ú Ï Ö Î Ï × Ú Ü Ï Î ô Î Ò × Ñ ô Ú Õ Ö Ñ ë Ø Î Ï Î Ñ Ö â Õ Ù Ù Õ Ú Ò Ù Ã197

� � � � � � � � � � � � � � � � � � � � � � � ¡ � � � � ¢ £ ¤ � ¥ � ¦ § ¨ � � � � © ª � � « ¨ � � « ¬ � � ® ¨ � ¢ � � © ¥ « ¯ � ° § ¨ � « � � ¢ «± � ² � 8 ³ ´ � � � « � ° µ ¨ ¢ � � � ³ � � � �
½ ¾ · Á � À � º ¶ À ¸ ¶ ¾ ¿ ½ � À · ¾ � Á ¹ » Á � � º � 9 � º À ¸Ý Ò Ý Þ ß Ð Ñ Ò Ü Ï Ú Ñ Ð × Õ ô Î Ø á Õ â Ü Ï Ú ô Î Ô Û × Û Ï Î Ù Ð Ú Ï Î Ù Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ë á Î Ö Û Ð Ñ × Õ Ò ð Ü Ï Ú ô Õ Ö Î Ï Ù Õ Ò Ú Ï Ö Î Ï × Ú Ï Î Ö Û Ð ÎÛ Ò Ò Î Ð Î Ù Ù Ñ Ï á Ü Ñ × Õ Î Ò × Î ù Ü Ú Ù Û Ï Î × Ú Õ â Ñ ð Õ Ò ð Ù × Û Ö Õ Î Ùº � � ¹ Á � ¹ À º ¿ · ¿ ¹ · º ¿ � · ¸ ¿ � Á ¹ � � À » � ¹ · ¸ � À ¿ � ½ � � · ¹ ¹ · ¾ � À ¹ º ¿ Á ¹ : À ¸ � · � ¿ À Á ¸Í Õ Ù â Î Ñ Ù Û Ï Î Õ Ù Ö Î Ù Õ ð Ò Î Ö × Ú Ñ Ù Ù Î Ù Ù Í Ú î â Ñ Ò á Ü Ñ × Õ Î Ò × Ù î Î Ï Î Ò Ú × Ü Ï Î Ù Ð Ï Õ ë Î Ö Ñ Ò × Õ ë Õ Ú × Õ Ð Ù Ï Ñ × Î Õ Ùþ Ò Ú î Ò Ñ Ù Ñ Ò Õ Ò ô Î Ï Ù Î Ï Ñ × Î Ã ; Ú Û Ð Ñ Ò Ð Ñ Ø Ð Û Ø Ñ × Î × Í Õ Ù â Î Ñ Ù Û Ï Î ë á × Ñ þ Õ Ò ð × Í Î Ï Î Ù Û Ø × Ú Ô Ö Õ ô Õ Ö Õ Ò ð × Í Î Ò Û â Î Ï Ñ × Ú Ïë á × Í Î Ö Î Ò Ú â Õ Ò Ñ × Ú Ï ó Ñ Ò Ö Ù Û ë × Ï Ñ Ð × Õ Ò ð × Í Î Ï Î Ù Û Ø × Ô Ï Ú â  Ãè ù Ñ â Ü Ø Î Ë Ñ Ò Ý Þ ß Í Ñ Ö � � Ü Ñ × Õ Î Ò × Ù î Í Ú â Î × × Í Î Ö Î Ò Ú â Õ Ò Ñ × Ú Ï Ð Ï Õ × Î Ï Õ Ñ Ã ß Ò Î Í Û Ò Ö Ï Î Ö Ú Ô × Í Î â ó Ú Ï û � $ óÏ Î Ð Î Õ ô Î Ö Ñ Ò × Õ ë Õ Ú × Õ Ð Ù Ã æ Í Õ Ù â Î Ñ Ò Ù × Í Ñ × � � $ Ú Ô × Í Î Ü Ñ × Õ Î Ò × Ù Ö Õ Ö Ò Ú × Ï Î Ð Î Õ ô Î Ñ Ò × Õ ë Õ Ú × Õ Ð Ù î Í Õ Ð Í î Ú Û Ø Ö ë Î × Í ÎÐ Ñ Ø Ð Û Ø Ñ × Î Ö Ï Ñ × Î Ô Ú Ï × Í Õ Ù Ü Ú Ü Û Ø Ñ × Õ Ú Ò Ã¼ Ä Å Æ Ç È É Ê Ë æ Í Î Õ Ò × Ñ þ Î Ü Î Ï Õ Ú Ö Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î Ú Ð Ð Û Ï Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î ë Î ð Õ Ò Ò Õ Ò ð Ú Ô × Í Îâ Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ó Ñ Ò Ö Î Ò Ö Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î Î Ò Ö Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ã ç Ú î Ð Ñ Ò Ñ Ò Ý Þ ßÐ Ø Ú Ù Î ð Ñ Ü Ù Õ Ô × Í Î Ð Ø Ñ Õ â Ù Í Ñ ô Î Ñ Ø Ï Î Ñ Ö á Ú Ð Ð Û Ï Ï Î Ö ãº Ê Æ ä Å å Ë Ó Ò Ù × Î Ñ Ö Ú Ô â Î Ñ Ù Û Ï Õ Ò ð Ñ Ð Ñ Ø Î Ò Ö Ñ Ï á Î Ñ Ï ó × Í Õ Ù â Î Ñ Ù Û Ï Î Ø Ú Ú þ Ù Ñ × Ð Ø Ñ Õ â Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î Ù × Ñ Ï ×Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï × Í Ï Ú Û ð Í × Í Î Ù Õ ù × Í â Ú Ò × Í Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ã õ è ù Ñ â Ü Ø Î Ë ç è é Ó ê û �  � î Õ Ø ØØ Ú Ú þ Ñ × Ð Ø Ñ Õ â Ù ë Î ð Õ Ò Ò Õ Ò ð � ï  ï û �  < × Í Ï Ú Û ð Í < ï � ï û �  � ó Õ Ò Ù × Î Ñ Ö Ú Ô Â ï  ï û �  � × Í Ï Ú Û ð Í Â û ï  ï û �  � Ñ Ù â Ú Ù ×Ú × Í Î Ï â Î Ñ Ù Û Ï Î Ù Ã öæ Í Õ Ù â Î Ñ Ù Û Ï Î Õ Ù Ö Î Ù Õ ð Ò Î Ö × Ú Í Î Ø Ü Ü Ï Î ô Î Ò × Ú ô Î Ï Û Ù Î Ú Ô Ñ Ò × Õ ë Õ Ú × Õ Ð Ù Ã ß Ò Ð Î Ñ Ü Ï Ú ô Õ Ö Î Ï Í Ñ Ù Ü Ï Î Ù Ð Ï Õ ë Î ÖÑ Ò × Õ ë Õ Ú × Õ Ð Ù Ô Ú Ï Ñ Ð Í Õ Ø Ö î Õ × Í Ñ Ö Õ Ñ ð Ò Ú Ù Õ Ù Ú Ô Ñ Ò Û Ü Ü Î Ï Ï Î Ù Ü Õ Ï Ñ × Ú Ï á Õ Ò Ô Î Ð × Õ Ú Ò ó Õ × Ð Ñ Ò Ò Ú × ë Î Û Ò Ö Ú Ò Î Ã ÷ Ú Ù × Ü Ñ Ï Î Ò × Ù× Ñ þ Õ Ò ð Ñ Ù Õ Ð þ Ð Í Õ Ø Ö × Ú × Í Î Ö Ú Ð × Ú Ï î Õ Ø Ø Ô Õ Ø Ø × Í Î Ü Ï Î Ù Ð Ï Õ Ü × Õ Ú Ò Ñ Ù Ù Ú Ú Ò Ñ Ù Ü Ú Ù Ù Õ ë Ø Î Ã Ý Ò Î ù Ñ â Ü Ø Î Ú Ô Í Ú î Ñ Ò Ý Þ ßÐ Ñ Ò Û Ù Î × Í Î Ù Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ñ Ù Ñ × Ú Ú Ø × Ú Õ â Ü Ï Ú ô Î à Û Ñ Ø Õ × á Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î Õ Ù × Ú Õ Ö Î Ò × Õ Ô á î Í Õ Ð Í Ü Ï Ú ô Õ Ö Î Ï ÙÍ Ñ ô Î Ñ Í Õ ð Í Ò Û â ë Î Ï Ú Ô Ü Ñ × Õ Î Ò × Ù × Í Ñ × â Î Î × × Í Î Ð Ï Õ × Î Ï Õ Ñ Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î Ã æ Í Î Ý Þ ß Ð Ú Û Ø Ö × Í Î Ò î Ú Ï þ î Õ × ÍÑ Ò á Ñ Ü Ü Ø Õ Ð Ñ ë Ø Î Ü Ï Ú ô Õ Ö Î Ï Ù × Ú Ö Î × Î Ï â Õ Ò Î î Í Î × Í Î Ï â Ú Ï Î Î Ö Û Ð Ñ × Õ Ú Ò Ú Ï Ð Ú Ñ Ð Í Õ Ò ð Õ Ù Ò Î Î Ö Î Ö Ãæ Í Õ Ù Õ Ù Ñ Ò Ú Ü × Õ Ú Ò Ñ Ø â Î × Ï Õ Ð Ô Ú Ï ; Î Ñ Ï Â Ã Ý Þ ß Ù Ð Ñ Ò Û Ù Î × Í Î Þ Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ù × Ñ Ï × Õ Ò ð Õ Ò â Ú Ò × Í # Ú Ô ; Î Ñ ÏÂ × Ú Õ Ö Î Ò × Õ Ô á × Í Î Ú Ü Ü Ú Ï × Û Ò Õ × Õ Î Ù Ô Ú Ï ; Î Ñ Ï û Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î Ñ Ò Ö Ù Ú Ô Ú Ï × Í Ô Ú Ï ; Î Ñ Ï Ã
198

� � � � � � � � � � � � � � � � � � � � � � � ¡ � � � � ¢ £ ¤ � ¥ � ¦ § ¨ � � � � © ª � � « ¨ � � « ¬ � � ® ¨ � ¢ � � © ¥ « ¯ � ° § ¨ � « � � ¢ «± � ² � = ³ ´ � � � « � ° µ ¨ ¢ � � � ³ � � � �
º � � ¹ Á � ¹ À º ¿ · ¿ · ¾ ¿ À ¸ ¶ � Á ¹ � � À » � ¹ · ¸ � À ¿ � � � º ¹ : ¸ ¶ À ¿ À ¾Â � à ¼ Ä Å Æ Ç È É Ê Ë æ Í Î Õ Ò × Ñ þ Î Ü Î Ï Õ Ú Ö Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î Ú Ð Ð Û Ï Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î ë Î ð Õ Ò Ò Õ Ò ð Ú Ô × Í Îâ Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï ó Ñ Ò Ö Î Ò Ö Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î Î Ò Ö Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ã ç Ú î Ð Ñ Ò Ñ Ò Ý Þ ßÐ Ø Ú Ù Î ð Ñ Ü Ù Õ Ô × Í Î Ð Ø Ñ Õ â Ù Í Ñ ô Î Ñ Ø Ï Î Ñ Ö á Ú Ð Ð Û Ï Ï Î Ö ãº Ê Æ ä Å å Ë Ó Ò Ù × Î Ñ Ö Ú Ô â Î Ñ Ù Û Ï Õ Ò ð Ñ Ð Ñ Ø Î Ò Ö Ñ Ï á Î Ñ Ï ó × Í Õ Ù â Î Ñ Ù Û Ï Î Ø Ú Ú þ Ù Ñ × Ð Ø Ñ Õ â Ù Ù Õ ù â Ú Ò × Í Ù Ü Ï Õ Ú Ï × Ú × Í Î Ù × Ñ Ï ×Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï × Í Ï Ú Û ð Í × Í Î Ù Õ ù × Í â Ú Ò × Í Ú Ô × Í Î â Î Ñ Ù Û Ï Î â Î Ò × á Î Ñ Ï Ã õ è ù Ñ â Ü Ø Î Ë ç è é Ó ê û �  � î Õ Ø ØØ Ú Ú þ Ñ × Ð Ø Ñ Õ â Ù ë Î ð Õ Ò Ò Õ Ò ð � ï  ï û �  < × Í Ï Ú Û ð Í < ï � ï û �  � ó Õ Ò Ù × Î Ñ Ö Ú Ô Â ï  ï û �  � × Í Ï Ú Û ð Í Â û ï  ï û �  � Ñ Ù â Ú Ù ×Ú × Í Î Ï â Î Ñ Ù Û Ï Î Ù Ã öß Ò Ð Î Ñ Ü Ñ × Õ Î Ò × Í Ñ Ù ë Î Î Ò Ü Ï Î Ù Ð Ï Õ ë Î Ö Ñ Ò × Õ ë Õ Ú × Õ Ð Ù ë á Ñ Ü Í á Ù Õ Ð Õ Ñ Ò ó â Ú Ù × Ü Ñ × Õ Î Ò × Ù î Õ Ø Ø Õ â â Î Ö Õ Ñ × Î Ø á Í Ñ ô Î × Í ÎÜ Ï Î Ù Ð Ï Õ Ü × Õ Ú Ò Ô Õ Ø Ø Î Ö Ã æ Í Î Ï Î Õ Ù Ò Ú × â Û Ð Í × Í Ñ × Ñ Ò Ý Þ ß Ð Ñ Ò Ö Ú × Ú Ð Ú Ï Ï Î Ð × × Í Õ Ù Ú Ò Ð Î Õ × Í Ñ Ù Í Ñ Ü Ü Î Ò Î Ö Ã Ý Ø Ù Ú ó ÑÙ × Ï Î Ü × Î Ù × î Õ Ø Ø Ú Ò Ø á ë Î Ð Ø Õ Ò Õ Ð Ñ Ø Ø á â Î Ñ Ò Õ Ò ð Ô Û Ø Ö Û Ï Õ Ò ð Ñ Ù Í Ú Ï × Ü Î Ï Õ Ú Ö Ú Ô × Õ â Î Ã 7 Ò Ø Õ þ Î Ñ Ð Ñ Ò Ð Î Ï Ù Ð Ï Î Î Ò Õ Ò ð ó × Í Õ Ù Õ ÙÒ Ú × Ñ ð Ñ Ü × Í Ñ × Ð Ñ Ò ë Î Ð Ø Ú Ù Î Ö ë á Ð Ñ Ø Ø Õ Ò ð Ü Ñ × Õ Î Ò × Ù Ø Õ Ù × Î Ö Õ Ò × Í Î Ö Î × Ñ Õ Ø Ï Î Ü Ú Ï × Ñ Ò Ö Í Ñ ô Õ Ò ð × Í Î â × Ñ þ Î Ñ Ù × Ï Î Ü × Î Ù ×Ø Ñ × Î Ï Ã ç Ú î Î ô Î Ï ó Ñ Ò Ý Þ ß Ð Ñ Ò Ü Ï Ú Ñ Ð × Õ ô Î Ø á Õ â Ü Ï Ú ô Î Ù Ð Ú Ï Î Ù Ô Ú Ï × Í Õ Ù â Î Ñ Ù Û Ï Î ë á Î Ö Û Ð Ñ × Õ Ò ð Ü Ï Ú ô Õ Ö Î Ï Ù Ñ Ò ÖÜ Ñ × Õ Î Ò × Ù Ã Ý Ò Ý Þ ß Ð Ú Û Ø Ö Û Ù Î × Í Î Ü Ñ × Õ Î Ò × Ö Î × Ñ Õ Ø Ï Î Ü Ú Ï × Ù × Ú Õ Ö Î Ò × Õ Ô á Ü Ï Ú ô Õ Ö Î Ï Ù î Í Ú â Õ ð Í × Ò Î Î Ö Ð Ú Ñ Ð Í Õ Ò ð × ÚÎ Ò Ù Û Ï Î × Í Î á Ñ Ï Î Ú Ï Ö Î Ï Õ Ò ð Ù × Ï Î Ü × Î Ù × Ù Ô Ú Ï × Í Î Ù Î Ü Ñ × Õ Î Ò × Ù Ñ Ò Ö î Ñ Õ × Õ Ò ð Ô Ú Ï Ü Ú Ù Õ × Õ ô Î Ï Î Ù Û Ø × Ù ë Î Ô Ú Ï Î Ü Ï Î Ù Ð Ï Õ ë Õ Ò ðÑ Ò × Õ ë Õ Ú × Õ Ð Ù Ãæ Í Õ Ù Õ Ù Ñ Ò Ú Ü × Õ Ú Ò Ñ Ø â Î × Ï Õ Ð Ô Ú Ï ; Î Ñ Ï Â Ã Ý Þ ß Ù Ð Ñ Ò Û Ù Î × Í Î � Ñ Ü Ù Õ Ò Þ Ñ Ï Î Ï Î Ü Ú Ï × Ù Ù × Ñ Ï × Õ Ò ð Õ Ò â Ú Ò × Í # Ú Ô ; Î Ñ ÏÂ × Ú Õ Ö Î Ò × Õ Ô á × Í Î Ú Ü Ü Ú Ï × Û Ò Õ × Õ Î Ù Ô Ú Ï ; Î Ñ Ï û Ü Î Ï Ô Ú Ï â Ñ Ò Ð Î Ñ Ò Ö Ù Ú Ô Ú Ï × Í Ô Ú Ï ; Î Ñ Ï Ã
199

APPENDIX
200

PRIOR AUTHORIZATION LIST For dates of service on or after January 1, 2019
Prior Authorization (PA) Requirements
This IPA Prior Authorization list supersedes any lists that have been previously distributed or published–
older lists are to be replaced with the latest version.
Prior Authorization (PA) Policy
PCP’s or referring health care professionals should OBTAIN Prior Authorization BEFORE services
requiring Prior Authorizations are rendered. Prior Authorizations may be obtained via HSConnect
(HSC) or as otherwise indicated in the Health Services section of the 2019 Provider Manual. Please see
the HSConnect section of the provider manual for an overview of the portal capabilities and
instructions for obtaining access.
Rendering providers should VERIFY that a Prior Authorization has been granted BEFORE any service
requiring a Prior Authorization is rendered. Prior Authorizations may be verified via HSConnect or as
otherwise indicated in the Health Services section of the Provider Manual.
IMPORTANT – Prior Authorization and/or Referral Number(s) is/are not a guarantee of benefits or
payment at the time of service. Remember, benefits will vary between plans, so always verify benefits.
Referral Policy
The IPA values the PCP’s role in directing the care of customers to the
appropriate, participating health care professionals. Participating specialists are
contracted to work closely with our referring PCPs to enhance the quality and
continuity of care provided to customers.
Although a Prior Authorization may not be required for certain services, a REFERRAL from a PCP
to a Specialist MUST BE in place. The Referral should indicate PCP approved for a consultation
only or for consultation and treatment, including the number of PCP approved visits.
Refer to the online directory at or contact to locate an in-network health care
professional or facility.
201

Codes marked with an * are designated by CMS for inpatient use only. Admissions *For Blue Cross or Cigna City of Houston/HEB
members, please contact Blue Cross or Cigna directly to obtain authorization*
All inpatient admissions including:
Inpatient Medical and Behavioral Health
Inpatient Observation
Inpatient Rehabilitation
Skilled Nursing Facility
LTAC Ambulance A0430 A0431 A0435 A0999 Cardiology
Echo 93303
93304
93306
93307
93308
93312
93313
93314
93315
93318
93320
93321
93325
C8926
C8927
C8929 EKG 93229 Stress 93350 93351 Other 93260
93261
93582
*93583
93590
93591
93592
93612
93619
93620
93621
93622
93624
93640
93641
93642
93644
93653
93654
93656
93799
0206T
0272T
0273T
0337T
0417T
0418T
0462T
0463T
Diagnostic 91111
91112
91132
91133
91200
91299
92133
92145
92242
92540
92548
93702
93998
94799
95250
95803
95810
95811
95812
95813
95816
95819
95827
95860
95861
95863
95864
95885
95886
95887
95923
95970
95999
96101
96102
96103
0071T
0072T
0198T
0317T
0330T
0358T
0381T
0382T
0383T
0384T
0385T
0386T
0400T
0401T
0422T
0434T
0435T
0436T
0506T
0507T
0508T
Durable Medical Equipment
E0156
E0184
E0188
E0194
E0303
E0466
E0483
E0627
E0628
E0629
E0635
E0651
E0652
E0760
E0766
E0770
E0784
E0986
E1002
E1006
E1007
E1008
E1010
E1220
E1230
E1399
K0005
K0009
K0011
K0554
K0800
K0801
K0802
K0806
K0807
K0808
K0812
K0813
K0814
K0837
K0841
K0848
K0849
K0850
K0851
K0852
K0856
K0858
K0861
K0862
K0898
L2005
202
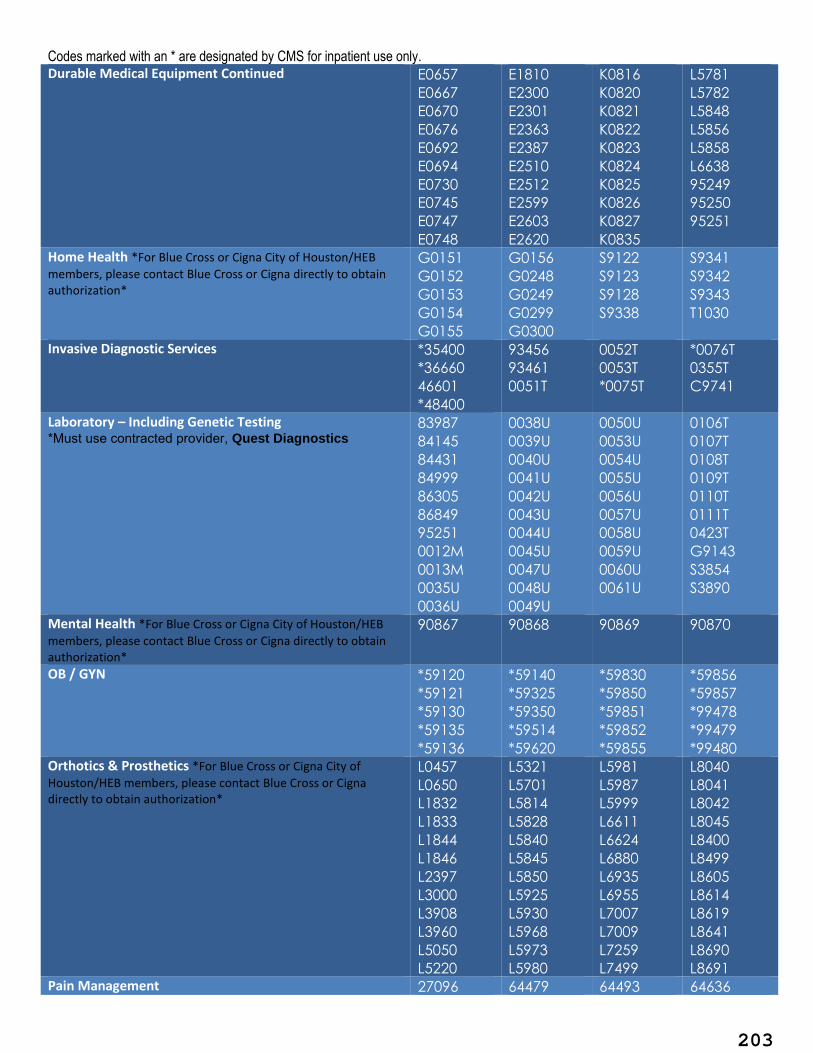
Codes marked with an * are designated by CMS for inpatient use only. Durable Medical Equipment Continued E0657
E0667
E0670
E0676
E0692
E0694
E0730
E0745
E0747
E0748
E1810
E2300
E2301
E2363
E2387
E2510
E2512
E2599
E2603
E2620
K0816
K0820
K0821
K0822
K0823
K0824
K0825
K0826
K0827
K0835
L5781
L5782
L5848
L5856
L5858
L6638
95249
95250
95251
Home Health *For Blue Cross or Cigna City of Houston/HEB
members, please contact Blue Cross or Cigna directly to obtain authorization*
G0151
G0152
G0153
G0154
G0155
G0156
G0248
G0249
G0299
G0300
S9122
S9123
S9128
S9338
S9341
S9342
S9343
T1030
Invasive Diagnostic Services *35400
*36660
46601
*48400
93456
93461
0051T
0052T
0053T
*0075T
*0076T
0355T
C9741
Laboratory – Including Genetic Testing *Must use contracted provider, Quest Diagnostics
83987
84145
84431
84999
86305
86849
95251
0012M
0013M
0035U
0036U
0038U
0039U
0040U
0041U
0042U
0043U
0044U
0045U
0047U
0048U
0049U
0050U
0053U
0054U
0055U
0056U
0057U
0058U
0059U
0060U
0061U
0106T
0107T
0108T
0109T
0110T
0111T
0423T
G9143
S3854
S3890
Mental Health *For Blue Cross or Cigna City of Houston/HEB
members, please contact Blue Cross or Cigna directly to obtain authorization*
90867 90868 90869 90870
OB / GYN *59120
*59121
*59130
*59135
*59136
*59140
*59325
*59350
*59514
*59620
*59830
*59850
*59851
*59852
*59855
*59856
*59857
*99478
*99479
*99480 Orthotics & Prosthetics *For Blue Cross or Cigna City of
Houston/HEB members, please contact Blue Cross or Cigna directly to obtain authorization*
L0457
L0650
L1832
L1833
L1844
L1846
L2397
L3000
L3908
L3960
L5050
L5220
L5321
L5701
L5814
L5828
L5840
L5845
L5850
L5925
L5930
L5968
L5973
L5980
L5981
L5987
L5999
L6611
L6624
L6880
L6935
L6955
L7007
L7009
L7259
L7499
L8040
L8041
L8042
L8045
L8400
L8499
L8605
L8614
L8619
L8641
L8690
L8691 Pain Management 27096 64479 64493 64636
203

Codes marked with an * are designated by CMS for inpatient use only. Pain Management Continued
62263
62360
62361
62362
63650
63685
64480
64483
64484
64490
64491
64492
64494
64495
64633
64634
64635
0232T
0278T
0440T
0441T
0442T
Part B Drugs *For Blue Cross or Cigna City of Houston/HEB
members, please contact Blue Cross or Cigna directly to obtain authorization*
Non-Specialty J0606
J1439
J7312
J7330
J7336
Q0138
Q0139
Q2040
Q2050
Q4102
Q4106
Q4110
Q4117
Q4118
Q4121
Q4124
Q4128
Q4131
Q4132
Q4133
Q4152
Q4159
Specialty C9025
C9026
C9027
C9030
C9031
C9032
C9140
C9399
J0129
J0135
J0178
J0180
J0202
J0220
J0221
J0256
J0257
J0490
J0585
J0586
J0587
J0588
J0597
J0598
J0717
J0725
J0775
J0800
J0881
J0882
J0885
J0886
J0887
J0888
J0897
J1290
J1300
J1438
J1442
J1446
J1458
J1459
J1460
J1556
J1557
J1559
J1561
J1566
J1568
J1569
J1572
J1575
J1595
J1599
J1602
J1743
J1745
J1786
J1931
J2278
J2323
J2354
J2357
J2425
J2503
J2504
J2505
J2507
J2778
J2796
J3060
J3240
J3262
J3357
J3380
J3385
J3490
J3590
J7175
J7179
J7180
J7181
J7182
J7183
J7185
J7186
J7187
J7188
J7189
J7190
J7192
J7193
J7194
J7195
J7197
J7198
J7199
J7200
J7201
J7202
J7205
J7207
J7209
J7316
J7320
J7321
J7322
J7323
J7324
J7325
J7326
J7327
J7328
J7682
J9017
J9035
J9047
J9055
J9214
J9226
J9228
J9271
J9299
J9301
J9303
J9305
J9306
J9308
J9310
J9354
J9355
J9400
J9999
Q2041
Q2043
Q5105
Q5106
Q9991
Q9992
Q9993
Q9995
204

Codes marked with an * are designated by CMS for inpatient use only. Pathology Pathology Continued
81201
81203
81210
81211
81212
81213
81214
81215
81216
81217
81225
81226
81227
81228
81229
81235
81240
81241
81243
81254
81275
81288
81291
81292
81293
81294
81295
81296
81297
81298
81300
81301
81317
81319
81321
81323
81324
81325
81327
81355
81400
81401
81402
81403
81404
81405
81406
81407
81408
81410
81411
81413
81414
81420
81422
81439
81445
81450
81455
81465
81479
81504
81519
81539
0357T
Professional Services 96379
99183
*99184
*99190
*99191
*99192
99199
0341T
0464T
G0277
G0339
G0340 Radiology
CT Scan 70450
70460
70470
70480
70481
70482
70486
70487
70488
70490
70491
70492
70496
70498
71250
71260
71270
71275
72125
72126
72127
72128
72129
72130
72131
72132
72133
72191
72192
72193
72194
73200
73201
73202
73206
73700
73701
73702
73706
74150
74160
74170
74174
74175
74176
74177
74178
74261
74262
74263
75571
75572
75573
75574
75635
76380
76497
77011
77012
77079
0042T
MRI 70336
70540
70542
70543
70544
70545
70546
70547
70548
70549
70551
70552
70553
70554
70559
71550
71551
71552
71555
72141
72142
72146
72147
72148
72149
72156
72157
72158
72197
72198
73218
73219
73220
73221
73222
73223
73225
73718
73719
73720
73721
73722
74182
74183
74185
75557
75559
75561
75563
75565
76390
76498
77021
77058
77059
77084
205

Codes marked with an * are designated by CMS for inpatient use only.
70555
70557
70558
72159
72195
72196
73723
73725
74181
C8907
C8908
S8037 Nuclear Medicine Nuclear Medicine Continued
78399
78451
78452
78453
78454
78459
78466
78469
78472
78473
78481
78483
78491
78492
78494
78496
78499
78608
78609
79101
0331T
0332T
A9606
PET 78811
78812
78813
78814
78815 78816
Radiation Therapy 76965
77014
77261
77262
77263
77280
77285
77290
77293
77295
77299
77300
77301
77306
77307
77316
77317
77318
77321
77331
77332
77333
77334
77336
77338
77370
77371
77372
77373
77385
77386
77387
77399
77401
77402
77407
77412
77417
77423
77424
77425
77427
77431
77432
77435
77469
77470
77499
77520
77522
77523
77525
77750
77761
77762
77763
77767
77768
77770
77771
77772
77778
77789
77790
77799
0394T
0395T
G0458
G6001
G6002
G6003
G6004
G6005
G6006
G6007
G6008
G6009
G6010
G6011
G6012
G6013
G6014
G6015
G6016
G6017
Therapeutic Radiology 00333
*75956
*75957
*75958
*75959
77013
77022
77600
77605
77610
77615
77620
Other 72285
76376
76377
76499
77074
0159T
0348T
0349T
0350T
0351T
0352T
0353T
0354T
C9733
G0210
G0211
G0212
G0214
G0229
S8035 Ultrasound 76873 76882
Rehab & Therapy *For Blue Cross or Cigna City of
Houston/HEB members, please contact Blue Cross or Cigna directly to obtain authorization*
92507
92700
*92971
*92975
96446
97018
97022
97024
97026
97033
97161
97162
97163
97164
97165
97166
97167
97168
97533
97607
97610
97802
G0157
G0158
G0166
Services & Supplies A6196 C1722 C2616 Q4119
206

Codes marked with an * are designated by CMS for inpatient use only. Services & Supplies Continued
A6197
A6212
A6222
A7031
A7032
A7033
A7036
A7046
A7507
A7520
B4150
C1721
C1759
C1764
C1767
C1778
C1783
C1785
C1813
C1874
C1875
C1882
C1889
C2624
K0553
K0606
L6881
L6882
L8679
Q0479
Q0481
Q0495
Q0508
Q4100
Q4135
Q4166
Q4167
Q4168
Q4169
Q4170
Q4171
Q4172
Q4173
Q4174
Q4175
Surgery Anesthesia 0102T Cardio / Thoracic
31626
31643
31651
31660
31661
*31725
*31760
*31766
*31770
*31775
*31780
*31781
*31786
*31800
*31805
31899
*32035
*32036
*32096
*32097
*32098
*32100
*32110
*32120
*32124
*32140
*32141
*32150
*32151
*32160
*32200
*32215
*32220
*32225
*32310
*32320
*32440
*33365
*33366
*33367
*33368
*33369
*33390
*33391
*33404
*33405
*33406
*33410
*33411
*33412
*33413
*33414
*33415
*33416
*33417
*33418
33419
*33420
*33422
*33425
*33426
*33427
*33430
*33460
*33463
*33464
*33465
*33468
*33470
*33471
*33474
*33475
*33476
*33477
*33910
*33915
*33916
*33917
*33920
*33922
*33924
*33925
*33926
*33930
*33933
*33935
*33940
*33944
*33945
*33946
*33947
*33948
*33949
*33951
*33952
*33953
*33954
*33955
*33956
*33957
*33958
*33959
*33962
*33963
*33964
*33965
*33966
*33967
*33968
*33969
*33970
*35539
*35540
*35556
*35558
*35560
*35563
*35565
*35566
*35570
*35571
*35583
*35585
*35587
*35600
*35601
*35606
*35612
*35616
*35621
*35623
*35626
*35631
*35632
*35633
*35634
*35636
*35637
*35638
*35642
*35645
*35646
*35647
*35650
*35654
*35656
*35661
*35663
207

Codes marked with an * are designated by CMS for inpatient use only. Cardio / Thoracic Continued
*32442
*32445
*32480
*32482
*32484
*32486
*32488
*32491
*32501
*32505
*32506
*32507
*32540
32553
*32650
*32651
*32652
*32653
*32654
*32655
*32656
*32658
*32659
*32661
*32662
*32663
*32664
*32665
*32666
*32667
*32668
*32669
*32670
*32671
*32672
*32673
*32674
*32800
*32810
*32815
*32820
*32850
*32851
*32852
*32853
*32854
*32900
*32905
*32906
*32940
*32997
*33478
*33496
*33500
*33501
*33502
*33503
*33504
*33505
*33506
*33510
*33511
*33512
*33513
*33514
*33516
*33517
*33518
*33519
*33521
*33522
*33523
*33530
*33533
*33534
*33535
*33536
*33542
*33545
*33548
*33572
*33600
*33602
*33606
*33608
*33610
*33611
*33612
*33615
*33617
*33619
*33620
*33621
*33622
*33641
*33645
*33647
*33660
*33665
*33670
*33675
*33676
*33971
*33973
*33974
*33975
*33976
*33977
*33978
*33979
*33980
*33981
*33982
*33983
*33984
*33985
*33986
*33987
*33988
*33989
*33990
*33991
*33992
*33993
33999
*34001
*34051
*34151
*34401
*34451
*34502
34803
34806
*34808
*34812
*34813
*34820
34825
34826
*34830
*34831
*34832
*34833
*34834
*34841
*34842
*34843
*34844
*34845
*34846
*34847
*34848
34900
*35665
*35666
*35671
*35681
*35682
*35683
*35691
*35693
*35694
*35695
*35700
*35701
*35721
*35741
*35800
*35820
*35840
*35870
35881
35884
*35901
*35905
*35907
36514
36516
36522
*36823
*37140
*37145
*37160
*37180
*37181
*37182
37183
37205
*37215
*37217
*37218
37221
37225
37226
37227
37228
37229
37230
37231
37236
37238
37239
37241
37242
208

Codes marked with an * are designated by CMS for inpatient use only. Cardio / Thoracic Continued
32998
32999
*33015
*33020
*33025
*33030
*33031
*33050
*33120
*33130
*33140
*33141
*33202
*33203
33206
33207
33208
33211
33212
33213
33214
33216
33221
33224
33227
33228
33229
33230
33231
*33236
*33237
*33238
33240
*33243
33249
*33250
*33251
*33254
*33255
*33256
*33257
*33258
*33259
*33261
33262
33263
33264
*33265
*33266
33270
33271
*33677
*33681
*33684
*33688
*33690
*33692
*33694
*33697
*33702
*33710
*33720
*33722
*33724
*33726
*33730
*33732
*33735
*33736
*33737
*33750
*33755
*33762
*33764
*33766
*33767
*33768
*33770
*33771
*33774
*33775
*33776
*33777
*33778
*33779
*33780
*33781
*33782
*33783
*33786
*33788
*33800
*33802
*33803
*33813
*33814
*33820
*33822
*33824
*33840
*33845
*33851
*35001
*35002
*35005
*35013
*35021
*35022
*35081
*35082
*35091
*35092
*35102
*35103
*35111
*35112
*35121
*35122
*35131
*35132
*35141
*35142
*35151
*35152
*35182
*35189
*35211
*35216
*35221
*35241
*35246
*35251
*35271
*35276
*35281
*35301
*35302
*35303
*35304
*35305
*35306
*35311
*35331
*35341
*35351
*35355
*35361
*35363
*35371
*35372
*35390
*35501
*35506
37243
37244
37246
37248
*37616
*37617
*37618
*37660
37700
37718
37722
37735
37760
37761
37780
*37788
37799
92920
92924
92937
92943
*92970
92986
*92992
*92993
93580
0234T
*0235T
0236T
0237T
0238T
*0254T
*0266T
0267T
0268T
*0345T
0387T
0408T
0409T
0410T
0411T
0412T
0413T
0414T
0415T
0416T
*0451T
*0452T
0453T
0454T
*0455T
209

Codes marked with an * are designated by CMS for inpatient use only. Cardio / Thoracic Continued
33282
*33300
*33305
*33310
*33315
*33320
*33321
*33322
*33330
*33335
*33340
*33361
*33362
*33363
*33364
*33852
*33853
*33860
*33863
*33864
*33870
*33875
*33877
*33880
*33881
*33883
*33884
*33886
*33889
*33891
*35508
*35509
*35511
*35515
*35516
*35518
*35521
*35523
*35526
*35531
*35533
*35535
*35536
*35537
*35538
*0456T
0457T
0458T
*0459T
0460T
*0461T
Dermatology / Plastic 11970
15273
15275
15277
15731
15732
*15756
*15757
*15758
15786
15820
15821
15822
15823
15824
15828
15830
15832
15834
15835
15836
15837
15839
15877
17106
17107
17108
17999
96920
96921
96922
0419T
0420T
C5271
C5272
C5273
C5275
C5276
Ear Nose Throat 30150
30160
30400
30410
30420
30450
30465
30520
30620
30802
30999
31070
*31225
*31230
31240
31254
31256
*31290
*31291
31292
31299
*31360
*31365
*31367
*31368
*31370
*31375
*31380
*31382
*31390
*31395
31400
31540
31580
31591
31599
34805
*35510
*35512
*35522
*35525
*35697
37765
37766
69140
*69155
69502
*69535
69550
69552
*69554
69632
69633
69637
69641
69642
69643
69644
69645
69646
69660
69711
69714
69717
69799
69930
69949
*69950
0406T
0407T
Gastrointestinal *43283
*43327
*43328
*43332
*43333
*43334
*43335
*43336
*43337
*43338
45399
46607
0377T
General Surgery
*11004
*11005
*11006
*11008
*43116
*43117
*43118
*43121
*44156
*44160
44180
*44187
*47480
*47550
47555
47556
210

Codes marked with an * are designated by CMS for inpatient use only. General Surgery Continued
*16036
19105
*19271
*19272
19300
19303
19304
*19305
*19306
19307
19316
19318
19325
19328
19330
19340
19342
19350
19355
19357
*19361
*19364
19366
*19367
*19368
*19369
19370
19371
19380
19499
21743
28124
36468
36470
36471
36473
36474
36475
36476
36478
36479
36482
36483
36825
37785
*38100
*38101
*38102
*38115
38120
38129
*43122
*43123
*43124
43130
*43135
43195
*43279
43280
43281
43282
43284
43285
43289
*43300
*43305
*43310
*43312
*43313
*43314
*43320
*43325
*43330
*43331
*43340
*43341
*43351
*43352
*43360
*43361
*43400
*43401
*43405
*43410
*43415
*43425
*43460
*43496
43499
*43500
*43501
*43502
*43520
*43605
*43610
*43611
*43620
*43621
*43622
*43631
*43632
*43633
*44188
*44202
*44203
*44204
*44205
*44206
*44207
*44208
*44210
*44211
*44212
*44213
*44227
44238
*44300
*44310
*44314
*44316
*44320
*44322
*44345
*44346
*44602
*44603
*44604
*44605
*44615
*44620
*44625
*44626
*44640
*44650
*44660
*44661
*44680
*44700
44799
*44800
*44820
*44850
*44899
*44900
44950
*44960
44979
*45110
*45111
*45112
*45113
*45114
*45116
47564
*47570
*47600
*47605
*47610
*47612
*47620
*47700
*47701
*47711
*47712
*47715
*47720
*47721
*47740
*47741
*47760
*47765
*47780
*47785
*47800
*47801
*47802
*47900
*48000
*48001
*48020
*48100
*48120
*48140
*48145
*48146
*48148
*48150
*48152
*48153
*48154
*48155
*48500
*48510
*48520
*48540
*48545
*48547
*48554
*48556
48999
*49000
*49002
*49010
*49020
211

Codes marked with an * are designated by CMS for inpatient use only. General Surgery Continued
38232
*38380
*38381
*38382
*38562
*38564
38720
*38724
38745
*38746
*38747
*38765
*38770
*38780
38999
*39000
*39010
*39200
*39220
39401
*39499
*39501
*39503
*39540
*39541
*39545
*39560
*39561
*39599
41120
*41130
*41135
*41140
*41145
*41150
*41153
*41155
41530
41820
41874
41899
42140
42145
42160
42410
42420
*42426
42699
42842
*42845
*42894
*43634
*43635
*43640
*43641
43659
43770
*43771
43772
43773
43774
*43775
*43800
*43810
*43820
*43825
*43832
*43840
*43843
*43846
*43847
*43848
*43850
*43855
*43860
*43865
*43880
43886
43888
43999
*44005
*44010
*44015
*44020
*44021
*44025
*44050
*44055
*44110
*44111
*44120
*44121
*44125
*44126
*44127
*44128
*44130
*44132
*44133
*44135
*44136
*44139
*45119
*45120
*45121
*45123
*45126
*45130
*45135
*45136
*45395
*45397
*45400
*45402
*45540
*45550
*45562
*45563
*45800
*45805
*45820
*45825
45999
*46705
46707
*46710
*46712
*46715
*46716
*46730
*46735
*46740
*46742
*46744
*46746
*46748
*46751
46999
*47010
*47015
*47100
*47120
*47122
*47125
*47130
*47133
*47135
47136
*47300
*47350
*47360
*47361
*47362
*49040
*49060
*49062
*49215
*49220
*49255
49322
49329
*49412
*49425
*49428
*49605
*49606
*49610
*49611
49651
49652
49653
49654
49655
49656
49657
49659
*49900
*49904
*49905
*49906
49999
*50250
50592
60200
60210
60212
60225
60240
60252
*60254
*60270
60271
60280
*60505
60520
*60521
*60522
*60540
*60545
*60600
*60605
*60650
60699
*61630
212

Codes marked with an * are designated by CMS for inpatient use only. General Surgery Continued
42950
*42953
*42961
*42971
*43045
*43100
*43101
*43107
*43108
*43112
*43113
*44140
*44141
*44143
*44144
*44145
*44146
*44147
*44150
*44151
*44155
47370
47379
*47380
*47381
47382
47399
*47400
*47420
*47425
*47460
*61635
64575
0263T
0264T
0397T
0446T
0447T
0448T
0505T
S8030
Gynecology 56620
*56630
*56631
*56632
*56633
*56634
*56637
*56640
*57110
*57111
*57112
57156
57260
*57270
*57280
57282
57283
57285
57288
*57305
*57307
*57308
*57311
57410
57426
*57531
*57540
*57545
57700
*58140
*58146
*58150
*58152
*58180
*58200
*58210
*58240
58263
*58267
58270
*58275
*58280
*58285
*58293
58353
*58400
*58410
*58520
*58540
58550
58552
58554
58570
58571
58572
58573
58578
*58605
*58611
58670
58671
58674
*58700
*58720
*58740
*58750
*58752
*58760
*58822
*58825
*58940
*58943
*58950
*58951
*58952
*58956
*58960
Neurosurgery
22867
22868
22869
22870
*61105
*61107
*61108
*61120
*61140
*61150
*61151
*61154
*61156
*61210
*61250
*61253
*61304
*61305
*61312
*61313
*61571
*61575
*61576
*61580
*61581
*61582
*61583
*61584
*61585
*61586
*61590
*61591
*61592
*61595
*61596
*61597
*61598
*61600
*61601
*61605
*62143
*62145
*62146
*62147
*62148
*62161
*62162
*62163
*62164
*62165
*62180
*62190
*62192
*62200
*62201
*62220
*62223
*62256
*62258
62264
*63270
*63271
*63272
*63273
*63275
*63276
*63277
*63278
*63280
*63281
*63282
*63283
*63285
*63286
*63287
*63290
*63295
*63300
*63301
*63302
213

Codes marked with an * are designated by CMS for inpatient use only. Neurosurgery Continued
*61314
*61315
*61320
*61321
*61322
*61323
*61332
*61333
*61340
*61343
*61345
*61450
*61458
*61460
*61480
*61500
*61501
*61510
*61512
*61514
*61516
*61518
*61519
*61520
*61521
*61522
*61524
*61526
*61530
*61531
*61533
*61534
*61535
*61536
*61537
*61538
*61539
*61540
*61541
*61543
*61544
*61545
*61546
*61548
*61550
*61552
*61556
*61557
*61558
*61559
*61563
*61606
*61607
*61608
*61613
*61615
*61616
*61618
*61619
*61624
*61645
*61650
*61680
*61682
*61684
*61686
*61690
*61692
*61697
*61698
*61700
*61702
*61703
*61705
*61708
*61710
*61711
*61735
*61750
*61751
*61760
61796
61798
61799
61800
*61850
*61860
*61863
*61864
*61867
*61868
*61870
61880
61885
61886
61888
*62005
*62010
*62100
*62115
*62117
*62120
62287
62290
62291
62320
62321
62322
62323
62380
63005
63015
63016
63017
63020
63030
63042
63045
63046
*63050
*63051
63056
*63077
*63078
*63081
*63082
*63085
*63086
*63087
*63088
*63090
*63091
*63101
*63102
*63103
*63170
*63172
*63173
*63180
*63182
*63185
*63190
*63191
*63194
*63195
*63196
*63197
*63198
*63199
*63200
*63250
*63251
*63252
*63303
*63304
*63305
*63306
*63307
*63308
63620
63655
63663
63664
*63700
*63702
*63704
*63706
*63707
*63709
*63710
*63740
64555
64561
64566
64568
64569
64570
64590
64595
64611
64612
64615
*64755
*64760
*64809
*64818
*64866
*64868
64895
64999
66711
*0202T
0313T
0316T
0398T
0424T
0425T
0426T
0427T
0428T
0429T
0430T
0431T
0432T
214

Codes marked with an * are designated by CMS for inpatient use only.
*61564
*61566
*61567
*61570
*62121
*62140
*62141
*62142
*63265
*63266
*63267
*63268
0433T
0466T
0467T
0468T Ophthalmology
65091
65093
65101
65103
65105
65140
65155
65175
65205
65210
65222
65235
65265
65270
*65273
65280
65285
65400
65420
65426
65430
65435
65436
65450
65600
65710
65730
65750
65755
65756
65770
65772
65778
65779
65780
65782
65800
65810
65815
65820
65850
65855
65860
65865
65870
65875
65920
66179
66180
66183
66184
66185
66225
66250
66500
66625
66630
66635
66680
66682
66710
66720
66761
66762
66820
66821
66825
66830
66840
66850
66852
66920
66930
66940
66982
66983
66984
66985
66986
66999
67005
67010
67015
67025
67027
67028
67031
67036
67039
67040
67041
67042
67043
67101
67208
67210
67218
67220
67221
67228
67250
67255
67299
67311
67312
67314
67318
67345
67400
67412
67414
67415
67420
67445
67500
67505
67515
67550
67560
67570
67700
67710
67715
67800
67801
67805
67808
67810
67820
67825
67830
67840
67875
67880
67882
67900
67901
67902
67903
67904
67908
67923
67924
67935
67938
67950
67961
67966
67971
67973
67975
67999
68020
68100
68110
68115
68130
68135
68200
68320
68325
68326
68328
68330
68360
68362
68371
68400
68440
68520
68525
68530
68700
68720
68750
68760
68761
68801
68810
68811
68815
68840
0100T
0190T
0191T
0207T
0253T
0356T
215

Codes marked with an * are designated by CMS for inpatient use only. Ophthalmology Continued
65930
66020
66030
66130
66150
66170
66172
66174
66175
67105
67107
67108
67110
67113
67120
67121
67141
67145
67909
67911
67912
67914
67915
67916
67917
67921
0376T
0402T
0444T
0445T
0449T
0450T
0465T
S2202
Orthopedics
20527
*20661
*20664
20696
*20802
*20805
*20808
*20816
*20824
*20827
*20838
20910
20912
*20955
*20956
*20957
*20962
*20969
*20970
20975
20983
20999
21025
21032
21034
*21045
21073
21085
21089
21110
*21141
*21142
*21143
*21145
*21146
*21147
*21151
*21154
*21155
*21159
*21160
*21179
*22328
22510
22511
22513
22514
22515
*22532
*22533
*22534
*22548
22551
*22556
*22558
*22586
*22590
*22595
*22600
*22610
22612
*22630
*22632
*22633
*22634
*22800
*22802
*22804
*22808
*22810
*22812
*22818
*22819
*22830
*22841
*22843
*22844
*22846
*22847
*22848
*22849
*22850
*22852
*22855
25800
25805
25810
*25900
*25905
*25915
*25920
*25924
*25927
26123
26341
26418
*26551
*26553
*26554
*26556
26765
26841
26989
*26992
*27005
*27025
*27030
*27036
*27054
*27070
*27071
*27075
*27076
*27077
*27078
*27090
*27091
*27120
*27122
*27125
*27130
*27132
*27134
*27137
*27138
*27140
*27557
*27558
27570
*27580
*27590
*27591
*27592
*27596
*27598
27599
*27645
*27646
27650
27652
27654
27665
27686
27691
*27702
*27703
27704
27709
*27712
*27715
*27724
*27725
27726
*27727
27756
27784
27792
27814
27827
27828
27860
27870
27871
*27880
*27881
*27882
*27886
*27888
216

Codes marked with an * are designated by CMS for inpatient use only. Orthopedics Continued
*21180
*21182
*21183
*21184
*21188
*21194
21195
*21196
21199
21208
21210
21215
21230
21235
21240
21244
*21247
21248
21249
*21255
*21268
21280
21282
21299
21325
21335
*21343
*21344
*21347
*21348
*21366
21390
21407
*21422
*21423
*21431
*21432
*21433
*21435
*21436
21462
21499
*21510
*21615
*21616
*21620
*21627
*21630
*21632
21685
*21705
22856
*22857
22858
*22861
*22862
*22864
*22865
22899
22999
23078
*23200
*23210
*23220
*23335
23410
23412
23420
23462
23470
*23472
23473
*23474
23485
23491
23515
23615
23616
23670
23680
23700
*23900
*23920
23929
24071
24149
24300
24340
24341
24342
24344
24363
24366
24370
24430
24435
24515
24545
24546
24575
24586
24666
*27146
*27147
*27151
*27156
*27158
*27161
*27165
*27170
*27175
*27176
*27177
*27178
*27181
*27185
*27187
27197
27198
*27222
*27226
*27227
*27228
*27232
*27236
*27240
*27244
*27245
*27248
*27253
*27254
*27258
*27259
*27268
*27269
27275
27279
*27280
*27282
*27284
*27286
*27290
*27295
27299
*27303
27345
*27365
27385
27386
27420
27442
*27445
27446
27899
28062
28102
28108
28118
28119
28289
28291
28295
28296
28297
28298
28299
28300
28302
28309
28322
28406
28415
28446
28465
28485
28705
28715
28725
28730
28735
28737
28740
28750
28755
*28800
28899
29799
29804
29806
29807
29820
29828
29837
29838
29844
29847
29855
29856
29862
29866
29873
29885
29891
29892
217

Codes marked with an * are designated by CMS for inpatient use only. Orthopedics Continued
*21740
*21750
*21825
21899
*22010
*22015
22102
*22110
*22112
*22114
*22116
*22206
*22207
*22208
*22210
*22212
*22214
*22216
*22220
*22222
*22224
*22226
*22318
*22319
*22325
*22326
*22327
24685
*24900
*24920
*24930
*24931
*24940
25020
25215
25259
25263
25320
25332
25337
25350
25390
25400
25405
25415
25440
25447
25526
25575
25606
25607
25608
25609
25628
27447
*27448
*27450
*27454
*27455
*27457
*27465
*27466
*27468
*27470
*27472
*27486
*27487
*27488
*27495
*27506
*27507
27509
*27511
*27513
*27514
*27519
27524
*27535
*27536
*27540
*27556
29893
29895
29899
29915
29916
29999
*0095T
*0098T
*0163T
*0164T
*0165T
*0195T
*0196T
0200T
0201T
*0219T
*0220T
0221T
0265T
0274T
0335T
*0375T
0396T
*G0412
*G0414
*G0415
Other 19296
19297
19298
28890
*32503
*32504
*32855
*32856
*33507
36820
41019
43257
*43644
*43645
43647
*43845
*43881
*43882
*44137
*44157
*44158
*44715
*44720
*44721
*47140
*47141
*47142
*47143
*47144
*47145
*47146
*47147
*48105
*48548
*48551
*49203
*49204
*49205
55875
55876
*57296
58542
*58548
*58957
*58958
64910
97606
0054T
0055T
0101T
0342T
0347T
C9600
C9602
C9604
*G0341
*G0342
*G0343
S2095
S2900 Respiratory 31295 31296 31297 Urology
*48552
49411
*50010
*50040
*50045
*50060
*50065
*50070
*50545
*50546
*50547
*50548
50593
*50600
*50605
*50610
*51550
*51555
*51565
*51570
*51575
*51580
*51585
*51590
*54135
54161
54360
*54390
54400
54401
54405
54408
218

Codes marked with an * are designated by CMS for inpatient use only. Urology Continued
*50075
*50100
*50120
*50125
*50130
*50135
*50205
*50220
*50225
*50230
*50234
*50236
*50240
*50280
*50290
*50300
*50320
*50323
*50325
*50327
*50328
*50329
*50340
*50360
*50365
*50370
*50380
*50400
*50405
*50500
*50520
*50525
*50526
*50540
50542
50543
*50620
*50630
*50650
*50660
*50700
*50715
*50722
*50725
50727
*50728
*50740
*50750
*50760
*50770
*50780
*50782
*50783
*50785
*50800
*50810
*50815
*50820
*50825
*50830
*50840
*50845
*50860
*50900
*50920
*50930
*50940
50947
50949
50961
*51525
*51530
*51595
*51596
*51597
*51800
*51820
*51840
*51841
*51865
*51900
*51920
*51925
*51940
*51960
*51980
52441
52442
52500
52601
52648
52649
53270
53400
53405
*53415
53430
53440
53445
53447
*53448
53850
53852
53860
53899
54112
*54125
*54130
54410
54411
54416
*54430
*54438
54520
54550
54660
55500
*55605
*55650
*55801
*55810
*55812
*55815
*55821
*55831
*55840
*55842
*55845
*55862
*55865
55866
55873
55899
55920
57155
57425
58346
*58953
*58954
0338T
0339T
0421T
C9739
C9740 Vision / Eyewear *For Blue Cross or Cigna City of Houston/HEB
members, please contact Blue Cross or Cigna directly to obtain authorization*
92020
92071
92072
92083
92120
92135
92225
92226
92230
92235
92240
92250
92270
92275
92285
92286
92499
V2020
V2100
V2103
V2200
V2203
V2207
V2300
V2531
V2623
V2624
V2625
V2626
V2627
V2628
V2629
V2632
V2744
V2781
V2784
V2785
V2790
V2799
219

RENAISSANCE PHYSICIANS CASE MANAGEMENT REFERRAL FORM
All programs may not be available in your demographic area. Medical Management will assist in coordinating these members to the most appropriate program available.
220

Advance Directive: Texas
Directive to Physicians and Family or Surrogates Advance Directives Act (see §166.033, Health and Safety Code)
This is an important legal document known as an Advance Directive. It is designed to help you communicate your wishes about medical treatment at some time in the future when you are unable to make your wishes known because of illness or injury. These wishes are usually based on personal values. In particular, you may want to consider what burdens or hardships of treatment you would be willing to accept for a particular amount of benefit obtained if you were seriously ill. You are encouraged to discuss your values and wishes with your family or chosen spokesperson, as well as your physician. Your physician, other health care provider, or medical institution may provide you with various resources to assist you in completing your advance directive. Brief definitions are listed below and may aid you in your discussions and advance planning. Initial the treatment choices that best reflect your personal preferences. Provide a copy of your directive to your physician, usual hospital, and family or spokesperson. Consider a periodic review of the document. By periodic review, you can best assure that the directive reflects your preferences. In addition to this advance directive, Texas law provides for two other types of directives that can be important during a serious illness. These are the Medical Power of Attorney and the Out-of- Hospital Do-Not-Resuscitate Order. You may wish to discuss these with your physician, family, hospital representative, or other advisers. You may also wish to complete a directive related to the donation of organs and tissues.
Directive I , recognize that the best health care is based upon a partnership of trust and communication with my physician. My physician and I will make health care decisions together as long as I am of sound mind and able to make my wishes known. If there comes a time that I am unable to make medical decisions about myself because of illness or injury, I direct that the following treatment preferences be honored: If, in the judgment of my physician, I am suffering with a terminal condition from which I am expected to die within six months, even with available life-sustaining treatment provided in accordance with prevailing standards of medical care: I request that all treatments other than those needed to keep me comfortable be discontinued or withheld and my physician allow me to die as gently as possible; OR I request that I be kept alive in this terminal condition using available life-sustaining treatment. (This selection does not apply to Hospice care.) If, in the judgment of my physician, I am suffering with an irreversible condition so that I cannot care for myself or make decisions for myself and am expected to die without life-sustaining treatment provided in accordance with prevailing standards of medical care: I request that all treatments other than those needed to keep me comfortable be discontinued or withheld and my physician allow me to die as gently as possible; OR I request that I be kept alive in this irreversible condition using available life-sustaining treatment. (This selection does not apply to Hospice care.)
221

Additional Requests: (After discussion with your physician, you may wish to consider listing particular treatments in this space that you do or do not want in specific circumstances, such as artificial nutrition and fluids, intravenous antibiotics, etc. Be sure to state whether you do or do not want the particular treatment.) After signing this directive, if my representative or I elect hospice care, I understand and agree that only those treatments needed to keep me comfortable would be provided and I would not be given available life-sustaining treatments. If I do not have a Medical Power of Attorney, and I am unable to make my wishes known, I designate the following person(s) to make treatment decisions with my physician compatible with my personal values: 1.
2.
(If a Medical Power of Attorney has been executed, then an agent already has been named and you should not list additional names in this document.) If the above persons are not available, or if I have not designated a spokesperson, I understand that a spokesperson will be chosen for me, following standards specified in the laws of Texas. If, in the judgment of my physician, my death is imminent within minutes to hours, even with the use of all available medical treatment provided within the prevailing standard of care, I acknowledge that all treatments may be withheld or removed except those needed to maintain my comfort. I understand that under Texas law this directive has no effect if I have been diagnosed as pregnant. This directive will remain in effect until I revoke it. No other person may do so.
Signed Date
City, County and State of Residence Two witnesses must sign in the spaces below. Two competent adult witnesses must sign below, acknowledging the signature of the declarant. The witness designated as Witness (1) may not be a person designated to make a treatment decision for the patient and may not be related to the declarant by blood or marriage. This witness may not be entitled to any part of the estate and may not have a claim against the estate of the patient. This witness may not be the attending physician or an employee of the attending physician. If this witness is an employee of a health care facility in which the patient is being cared for, this witness may not be involved in providing direct patient care to the patient. This witness may not be an officer, director, partner, or business office employee of a health care facility in which the patient is being cared for or of any parent organization of the health care facility. Witness (1) Witness (2)
222

Definitions: "Artificial nutrition and hydration" means the provision of nutrients or fluids by a tube inserted in a vein, under the skin in the subcutaneous tissues, or in the stomach (gastrointestinal tract). "Irreversible condition" means a condition, injury, or illness: a. that may be treated, but is never cured; b. that leaves a person unable to care for or make decisions for the person's own self; and c. that, without life-sustaining treatment provided in accordance with the prevailing standard of medical care is fatal. Explanation: Many serious illnesses such as cancer, failure of major organs (kidney, heart, liver, or lung), and serious brain disease such as Alzheimer's dementia may be considered irreversible early on. There is no cure, but the patient may be kept alive for prolonged periods of time if the patient receives life-sustaining treatments. Late in the course of the same illness, the disease may be considered terminal when, even with treatment, the patient is expected to die. You may wish to consider which burdens of treatment you would be willing to accept in an effort to achieve a particular outcome. This is a very personal decision that you may wish to discuss with your physician, family, or other important persons in your life. "Life-sustaining treatment" means treatment that, based on reasonable medical judgment, sustains the life of a patient and without which the patient will die. The term includes both life- sustaining medications and artificial life support such as mechanical breathing machines, kidney dialysis treatment, and artificial hydration and nutrition. The term does not include the administration of pain management medication, the performance of a medical procedure necessary to provide comfort care, or any other medical care provided to alleviate a patient's pain. "Terminal condition" means an incurable condition caused by injury, disease, or illness that according to reasonable medical judgment will produce death within six months, even with available life-sustaining treatment provided in accordance with the prevailing standard of medical care Explanation: Many serious illnesses may be considered irreversible early in the course of the illness, but they may not be considered terminal until the disease is fairly advanced. In thinking about terminal illness and its treatment, you again may wish to consider the relative benefits and burdens of treatment and discuss your wishes with your physician, family, or other important persons in your life. Versión 10/26/99
223

Directiva a los médicos y a familiares o substitutos Ley de Directivas Anticipadas (ver §166.033, del Código de Salud y Seguridad)
Éste es un documento legal importante conocido como Directiva Anticipada. Su función es ayudar a comunicar sus deseos relacionados con el tratamiento médico para un momento futuro cuando no esté en capacidad de hacer conocer sus deseos debido a una enfermedad o lesión. Estos deseos se basan generalmente en sus valores personales. En particular, querrá considerar qué nivel o dificultades de tratamiento está dispuesto a soportar a cambio del beneficio que obtendría en caso de estar gravemente enfermo. Se le sugiere que hable sobre sus valores y deseos con su familia y con la persona escogida como su agente, lo mismo que con su doctor. El doctor, otro proveedor médico o una institución médica pueden ofrecerle algunos recursos para ayudarle a completar la directiva anticipada. A continuación se dan unas definiciones breves que le podrán ayudar en sus discusiones y en la planeación. Escriba sus iniciales al lado de las opciones de tratamiento que mejor reflejen sus preferencias personales. Deles una copia de su directiva a su doctor, a su hospital de costumbre, a sus parientes y a su agente. Haga una revisión periódica del documento. Mediante la revisión periódica, puede asegurar que la directiva refleje sus preferencias. Además de esta directiva anticipada, la ley de Texas estipula otros dos tipos de directivas que pueden ser importantes en caso de una enfermedad grave. Estas son: el Poder médico y la Orden de no revivir fuera del hospital. Debe hablar sobre estos con el doctor, su familia, un representante del hospital o con otros consejeros. También es posible que desee llenar una directiva relacionada con la donación de órganos y tejidos.
Directiva Yo, reconozco que la mejor atención médica se basa en una relación de confianza y comunicación con mi doctor. Juntos, mi doctor y yo tomaremos las decisiones médicas mientras yo esté en condiciones mentales de hacer conocer mis deseos. Si en algún momento yo no estoy en capacidad de tomar decisiones médicas respecto a mi salud debido a una enfermedad o lesión, ordeno que se respeten las siguientes preferencias respecto al tratamiento: Si, a juicio de mi doctor, estoy padeciendo de una enfermedad terminal de la que se espera moriré dentro de los seis meses, incluso con tratamientos disponibles para prolongar la vida, suministrado de acuerdo con las normas actuales de atención médica: Yo pido que no me den o que me retiren todo tratamiento salvo aquellos necesarios para mantenerme cómodo, y que mi doctor me deje morir tan dignamente como sea posible; O Yo pido que me mantengan con vida en esta situación terminal usando los tratamientos disponibles para prolongar la vida. (Esta preferencia no se aplica al cuidado de hospicio). Si, a juicio de mi doctor, estoy sufriendo de un padecimiento irreversible, que no permitirá que me atienda yo mismo ni que tome decisiones por mí mismo y se espera que moriré si no me suministran tratamientos para prolongar la vida de acuerdo con las normas actuales de atención médica:
224

Yo pido que no me den o me retiren todo tratamiento salvo aquellos necesarios para mantenerme cómodo, y que mi doctor me deje morir tan dignamente como sea posible; O Yo pido que me mantengan con vida en esta situación irreversible usando tratamientos disponibles para prolongar la vida. (Esta preferencia no se aplica al cuidado de hospicio). Peticiones adicionales: (Después de consultarle al doctor, usted querrá escribir algunos tratamientos en el espacio disponible que usted quiera o no quiera que se le den bajo circunstancias específicas, como la nutrición artificial y los líquidos, los antibióticos por vía intravenosa, etc. Asegúrese de anotar si quiere o no quiere el tratamiento en particular). Después de firmar esta directiva, si mi representante o yo elegimos cuidado de hospicio, entiendo y estoy de acuerdo en que me den solamente aquellos tratamientos para mantenerme cómodo y que no me den los tratamientos disponibles para prolongar la vida. Si no tengo un poder para la atención médica, y no puedo dar a conocer mis deseos, designo a las siguientes personas para que tomen decisiones con mi doctor que sean compatibles con mis valores personales: 1. 2. (Si usted ya ha firmado un poder médico, entonces ya habrá nombrado a un agente y no deberá anotar otros nombres en este documento). Si las personas nombradas antes no están disponibles, o si no hay un vocero designado, comprendo que se escogerá un vocero para mí, siguiendo las pautas especificadas por la ley de Texas. Si, a juicio de mi doctor, mi muerte es inminente dentro de minutos u horas, a pesar de que me den todo tratamiento médico disponible suministrado dentro de las pautas de atención actuales, autorizo que no me den o que me retiren todo tratamiento salvo aquellos necesarios para mantenerme cómodo. Comprendo que bajo la ley de Texas esta directiva no tiene efecto si se ha diagnosticado que estoy embarazada. Esta directiva seguirá en efecto hasta que yo la revoque. Nadie más puede hacerlo.
Firmado Fecha Ciudad, condado y estado de domicilio Dos testigos tienen que firmar en los espacios siguientes. Dos testigos adultos hábiles tienen que firmar a continuación, reconociendo la firma del declarante. El testigo designado Testigo (1) no puede ser una de las personas designadas para tomar decisiones relacionadas con el tratamiento para el paciente y no puede estar relacionado con el declarante por sangre o por matrimonio. Este testigo no puede tener derecho a ninguna parte de la sucesión y no puede tener un reclamo en contra de la sucesión del paciente. Este
225

testigo no puede ser el médico que lo atiende ni un empleado del médico que lo atiende. Si el testigo es empleado del centro de salud en el cual se cuida al paciente, este testigo no puede estar directamente involucrado en el suministro de atención al paciente. Este testigo no puede ser funcionario, director, socio o empleado de la oficina del centro de atención médica donde se atiende al paciente o de ninguna organización matriz del centro de atención médica. Testigo (1) Testigo (2) Definiciones: "Nutrición e hidratación artificial" quiere decir el suministro de nutrientes o líquidos mediante una sonda puesta en una vena, bajo la piel en los tejidos subcutáneos o en el estómago (tracto gastrointestinal). "Padecimiento irreversible” quiere decir un padecimiento, lesión o enfermedad: a. que se puede tratar, pero que nunca sana; b. que deja a la persona incapaz de cuidarse o tomar decisiones por ella misma, y c. que sin el tratamiento para prolongar la vida, suministrado conforme con las normas actuales de atención médica, podría ser fatal. Explicación: muchas enfermedades graves como el cáncer, la insuficiencia de cualquier órgano vital (el riñón, el corazón, el hígado o el pulmón) y una enfermedad del cerebro grave, como la demencia de Alzheimer, se pueden considerar irreversibles desde muy temprano. No hay curación, pero el paciente puede mantenerse con vida por periodos prolongados de tiempo si recibe tratamientos para prolongar la vida. Más tarde durante la misma enfermedad, ésta se puede considerar terminal cuando, incluso con tratamiento, se espera que el paciente muera. Usted deberá considerar qué niveles de tratamiento está dispuesto a soportar para lograr un resultado particular. Ésta es una decisión muy personal que usted deberá discutir con el doctor, la familia u otras personas importantes en su vida. *Tratamiento para prolongar la vida" quiere decir un tratamiento que, a juicio médico, preserva la vida de un paciente y sin el cual el paciente moriría. El término se refiere a medicamentos para preservar la vida y a medios artificiales para mantener la vida como los respiradores mecánicos, el tratamiento de diálisis del riñón, la hidratación y la nutrición artificial. El término no se refiere a la administración de medicamentos para el dolor, la ejecución de un procedimiento quirúrgico necesario para suministrar comodidad ni ningún otro servicio médico ofrecido para aliviar el dolor del paciente. "Padecimiento terminal" quiere decir una enfermedad incurable causada por lesión, enfermedad o dolencia que a juicio médico produciría la muerte dentro de unos seis meses, incluso con el tratamiento disponible para prolongar la vida suministrado de acuerdo con las normas de atención médica actuales. Explicación: muchas enfermedades graves se pueden considerar irreversibles desde muy temprano en la evolución de la enfermedad, pero no se considera terminal hasta que la enfermedad ha avanzado bastante. Al pensar en una enfermedad terminal y su tratamiento, deberá considerar los beneficios y las dificultades relacionados con el tratamiento y discutirlos con el doctor, la familia u otras personas importantes en su vida.
226

Print Form
Figure: 25 TAC §157.25 (h)(2) OUT-OF-HOSPITAL DO-NOT-RESUSCITATE (OOH-DNR) ORDER TEXAS DEPARTMENT OF STATE HEALTH SERVICES
This document becomes effective immediately on the date of execution for health care professionals acting in out-of-hospital settings. It remains in effect until
the person is pronounced dead by authorized medical or legal authority or the document is revoked. Comfort care will be given as needed.
Person's full legal name Date of birth
Male Female
A. Declaration of the adult person: I am competent and at least 18 years of age. I direct that none of the following resuscitation measures be initiated or continued for me: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation. Person's signature
Date Printed name
B. Declaration by legal guardian, agent or proxy on behalf of the adult person who is incompetent or otherwise incapable of communication:
I am the: legal guardian; agent in a Medical Power of Attorney; OR proxy in a directive to physicians of the above-noted person who is incompetent or otherwise mentally or physically incapable of communication. Based upon the known desires of the person, or a determination of the best interest of the person, I direct that none of the following resuscitation measures be initiated or continued for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation.
Signature
Date Printed name
C. Declaration by a qualified relative of the adult person who is incompetent or otherwise incapable of communication: I am the above-noted person's: spouse, adult child, parent, OR nearest living relative, and I am qualified to make this treatment decision under Health and Safety Code §166.088. To my knowledge the adult person is incompetent or otherwise mentally or physically incapable of communication and is without a legal guardian, agent or proxy. Based upon the known desires of the person or a determination of the best interests of the person, I direct that none of the following resuscitation measures be initiated or continued for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation.
Signature Date Printed name
D. Declaration by physician based on directive to physicians by a person now incompetent or nonwritten communication to the physician by a competent person: I am the above-noted person's attending physician and have:
seen evidence of his/her previously issued directive to physicians by the adult, now incompetent; OR observed his/her issuance before two witnesses of an OOH-DNR in a nonwritten manner.
I direct that none of the following resuscitation measures be initiated or continued for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation. Attending physicians signature Date
Printed name Lic#
E. Declaration on behalf of the minor person: I am the minor's: parent; legal guardian; OR managing conservator.
A physician has diagnosed the minor as suffering from a terminal or irreversible condition. I direct that none of the following resuscitation measures be initiated or continued for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation. Signature Date
Printed name
TWO WITNESSES: (See qualifications on backside.) We have witnessed the above-noted competent adult person or authorized declarant making his/her signature above and, if applicable, the above-noted adult person making an OOH-DNR by nonwritten communication to the attending physician.
Witness 1 signature Date Printed name
Witness 2 signature Date Printed name Notary in the State of Texas and County of . The above noted person personally appeared before me and signed the above noted declaration on this date: . Signature & seal: Notary's printed name:
Notary Seal
[ Note: Notary cannot acknowledge the witnessing of the person making an OOH-DNR order in a nonwritten manner ] PHYSICIAN'S STATEMENT: I am the attending physician of the above-noted person and have noted the existence of this order in the person's medical records. I direct health care professionals acting in out-of-hospital settings, including a hospital emergency department, not to initiate or continue for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation. Physician's signature
Printed name
Date
License #
F. Directive by two physicians on behalf of the adult, who is incompetent or unable to communicate and without guardian, agent, proxy or relative: The person's specific wishes are unknown, but resuscitation measures are, in reasonable medical judgment, considered ineffective or are otherwise not in the best interests of the person. I direct health care professionals acting in out-of-hospital settings, including a hospital emergency department, not to initiate or continue for the person: cardiopulmonary resuscitation (CPR), transcutaneous cardiac pacing, defibrillation, advanced airway management, artificial ventilation.
Attending physician's signature
Signature of second physician
Date
Date
Printed name
Printed name
Lic#
Lic#
Physician's electronic or digital signature must meet criteria listed in Health and Safety Code §166.082(c). All persons who have signed above must sign below, acknowledging that this document has been properly completed.
Person's signature Guardian/Agent/Proxy/Relative signature
Attending physician's signature
Second physician's signature
Witness 1 signature Witness 2 signature Notary's signature
This document or a copy thereof must accompany the person during his/her medical transport.
227

INSTRUCTIONS FOR ISSUING AN OOH-DNR ORDER
PURPOSE: The Out-of-Hospital Do-Not-Resuscitate (OOH-DNR) Order on reverse side complies with Health and Safety Code (HSC), Chapter 166 for use by qualified
persons or their authorized representatives to direct health care professionals to forgo resuscitation attempts and to permit the person to have a natural death with peace and
dignity. This Order does NOT affect the provision of other emergency care, including comfort care.
APPLICABILITY: This OOH-DNR Order applies to health care professionals in out-of-hospital settings, including physicians' offices, hospital clinics and
emergency departments. IMPLEMENTATION: A competent adult person, at least 18 years of age, or the person's authorized representative or qualified relative may execute or issue an OOH-
DNR Order. The person's attending physician will document existence of the Order in the person's permanent medical record. The OOH-DNR Order may be executed as
follows:
Section A - If an adult person is competent and at least 18 years of age, he/she will sign and date the Order in Section A.
Section B - If an adult person is incompetent or otherwise mentally or physically incapable of communication and has either a legal guardian, agent in a medical power of attorney, or proxy in a directive to physicians, the guardian, agent, or proxy may execute the OOH-DNR Order by signing and dating it in Section B. Section C - If the
adult person is incompetent or otherwise mentally or physically incapable of communication and does not have a guardian, agent, or proxy, then a qualified relative may
execute the OOH-DNR Order by signing and dating it in Section C. Section D - If the person is incompetent and his/her attending physician has seen evidence of the person's previously issued proper directive to physicians or observed the
person competently issue an OOH-DNR Order in a nonwritten manner, the physician may execute the Order on behalf of the person by signing and dating it in Section D.
Section E - If the person is a minor (less than 18 years of age), who has been diagnosed by a physician as suffering from a terminal or irreversible condition, then
the minor's parents, legal guardian, or managing conservator may execute the OOH-DNR Order by signing and dating it in Section E.
Section F - If an adult person is incompetent or otherwise mentally or physically incapable of communication and does not have a guardian, agent, proxy, or available
qualified relative to act on his/her behalf, then the attending physician may execute the OOH-DNR Order by signing and dating it in Section F with concurrence of a second
physician (signing it in Section F) who is not involved in the treatment of the person or who is not a representative of the ethics or medical committee of the health care facility in which the person is a patient.
In addition, the OOH-DNR Order must be signed and dated by two competent adult witnesses, who have witnessed either the competent adult person making his/her
signature in section A, or authorized declarant making his/her signature in either sections B, C, or E, and if applicable, have witnessed a competent adult person making an
OOH-DNR Order by nonwritten communication to the attending physician, who must sign in Section D and also the physician's statement section. Optionally, a competent
adult person or authorized declarant may sign the OOH-DNR Order in the presence of a notary public. However, a notary cannot acknowledge witnessing the issuance of an
OOH-DNR in a nonwritten manner, which must be observed and only can be acknowledged by two qualified witnesses.
Witness or notary signatures are not required when two physicians execute the OOH-DNR Order in section F. The original or a copy of a fully and properly completed OOH-DNR Order or the presence of an OOH-DNR device on a person is sufficient evidence of the existence of the original OOH-DNR Order and either one shall be
honored by responding health care professionals.
REVOCATION: An OOH-DNR Order may be revoked at ANY time by the person, person's authorized representative, or physician who executed the order. Revocation
can be by verbal communication to responding health care professionals, destruction of the OOH-DNR Order, or removal of all OOH-DNR identification devices from the
person.
AUTOMATIC REVOCATION: An OOH-DNR Order is automatically revoked for a person known to be pregnant or in the case of unnatural or suspicious circumstances.
DEFINITIONS
Attending Physician: A physician, selected by or assigned to a person, with primary responsibility for the person's treatment and care and is licensed by the Texas Medical Board, or is properly credentialed and holds a commission in the uniformed services of the United States and is serving on active duty in this state. [HSC
§166.002(12)].
Health Care Professional: Means physicians, nurses, physician assistants and emergency medical services personnel, and, unless the context requires otherwise,
includes hospital emergency department personnel. [HSC §166.081(5)]
Qualified Relative: A person meeting requirements of HSC §166.088. It states that an adult relative may execute an OOH-DNR Order on behalf of an adult person who has not executed or issued an OOH-DNR Order and is incompetent or otherwise mentally or physically incapable of communication and is without a legal guardian, agent
in a medical power of attorney, or proxy in a directive to physicians, and the relative is available from one of the categories in the following priority:
1) person's spouse; 2) person's reasonably available adult children; 3) the person's parents; or, 4) the person's nearest living relative. Such qualified relative may
execute an OOH-DNR Order on such described person's behalf.
Qualified Witnesses: Both witnesses must be competent adults, who have witnessed the competent adult person making his/her signature in section A, or person's
authorized representatives making his/her signature in either Sections B, C, or E on the OOH-DNR Order, or if applicable, have witnessed the competent adult person
making an OOH-DNR by nonwritten communication to the attending physician, who signs in Section D. Optionally, a competent adult person, guardian, agent, proxy, or qualified relative may sign the OOH-DNR Order in the presence of a notary instead of two qualified witnesses. Witness or notary signatures are not required when
two physicians execute the order by signing Section F. One of the witnesses must meet the qualifications in HSC §166.003(2), which requires that at least one
of the witnesses not: (1) be designated by the person to make a treatment decision; (2) be related to the person by blood or marriage; (3) be entitled to any part of the
person's estate after the person's death either under a will or by law; (4) have a claim at the time of the issuance of the OOH-DNR against any part of the person's estate
after the person's death; or, (5) be the attending physician; (6) be an employee of the attending physician or (7) an employee of a health care facility in which the person is
a patient if the employee is providing direct patient care to the patient or is an officer, director, partner, or business office employee of the health care facility or any parent organization of the health care facility.
Report problems with this form to the Texas Department of State Health Services (DSHS) or order OOH-DNR Order/forms or identification devices at (512)
834-6700.
Declarant's, Witness', Notary's, or Physician's electronic or digital signature must meet criteria outlined in HSC §166.011
Publications No. EF01-11421 - Revised July 1, 2009 by the Texas Department of State Health Services Page 2 of 2
228

Disclosure Statement for Medical Power of Attorney Advance Directives Act (see §166.163, Health and Safety Code)
This is an important legal document. Before signing this document, you should know these important facts:
Except to the extent you state otherwise, this document gives the person you name as your agent the authority to make any and all health care decisions for you in accordance with your wishes, including your religious and moral beliefs, when you are no longer capable of making them yourself. Because "health care" means any treatment, service or procedure to maintain, diagnose, or treat your physical or mental condition, your agent has the power to make a broad range of health care decisions for you. Your agent may consent, refuse to consent, or withdraw consent to medical treatment and may make decisions about withdrawing or withholding life-sustaining treatment. Your agent may not consent to voluntary inpatient mental health services, convulsive treatment, psychosurgery, or abortion. A physician must comply with your agent's instructions or allow you to be transferred to another physician. Your agent's authority begins when your doctor certifies that you lack the competence to make health care decisions. Your agent is obligated to follow your instructions when making decisions on your behalf. Unless you state otherwise, your agent has the same authority to make decisions about your health care as you would have had. It is important that you discuss this document with your physician or other health care provider before you sign it to make sure that you understand the nature and range of decisions that may be made on your behalf. If you do not have a physician, you should talk with someone else who is knowledgeable about these issues and can answer your questions. You do not need a lawyer's assistance to complete this document, but if there is anything in this document that you do not understand, you should ask a lawyer to explain it to you. The person you appoint as agent should be someone you know and trust. The person must be 18 years of age or older or a person under 18 years of age who has had the disabilities of minority removed. If you appoint your health or residential care provider (e.g., your physician or an employee of a home health agency, hospital, nursing home, or residential care home, other than a relative), that person has to choose between acting as your agent or as your health or residential care provider; the law does not permit a person to do both at the same time. You should inform the person you appoint that you want the person to be your health care agent. You should discuss this document with your agent and your physician and give each a signed copy. You should indicate on the document itself the people and institutions who have signed copies. Your agent is not liable for health care decisions made in good faith on your behalf.
229

Even after you have signed this document, you have the right to make health care decisions for yourself as long as you are able to do so and treatment cannot be given to you or stopped over your objection. You have the right to revoke the authority granted to your agent by informing your agent or your health or residential care provider orally or in writing, by your execution of a subsequent medical power of attorney. Unless you state otherwise, your appointment of a spouse dissolves on divorce. This document may not be changed or modified. If you want to make changes in the document, you must make an entirely new one. You may wish to designate an alternate agent in the event that your agent is unwilling, unable, or ineligible to act as your agent. Any alternate agent you designate has the same authority to make health care decisions for you. This Power of Attorney is not valid unless it is signed in the presence of two competent adult witnesses. The following persons may not act as ONE of the witnesses: • the person you have designated as your agent. • a person related to you by blood or marriage; • a person entitled to any part of your estate after your death under a will or codicil
executed by you or by operation of law; • your attending physician; • an employee of your attending physician; • an employee of a health care facility in which you are a patient if the employee is
providing direct patient care to you or is an officer, director, partner, or business office employee of a health care facility or of any parent organization of the health care facility; or
• a person who, at the time this power of attorney is executed, has a claim against any part of your estate after your death.
230

Medical Power Of Attorney Advance Directives Act (see §166.164, Health and Safety Code)
Designation of Health Care Agent: I, (insert your name) appoint:
Name:
Address:
Phone:
as my agent to make any and all health care decisions for me, except to the extent I state otherwise in this document. This medical power of attorney takes effect if I become unable to make my own health care decisions and this fact is certified in writing by my physician. Limitations On The Decision Making Authority Of My Agent Are As Follows: Designation of an Alternate Agent: (You are not required to designate an alternate agent but you may do so. An alternate agent may make the same health care decisions as the designated agent if the designated agent is unable or unwilling to act as your agent. If the agent designated is your spouse, the designation is automatically revoked by law if your marriage is dissolved.) If the person designated as my agent is unable or unwilling to make health care decisions for me, I designate the following person(s), to serve as my agent to make health care decisions for me as authorized by this document, who serve in the following order: First Alternate Agent
Name:
Address:
Phone:
Second Alternate Agent
Name:
Address:
Phone:
The original of the document is kept at The following individuals or institutions have signed copies: Name:
Address: Name:
Address: :
(continued on reverse)
231

Duration
I understand that this power of attorney exists indefinitely from the date I execute this document unless I establish a shorter time or revoke the power of attorney. If I am unable to make health care decisions for myself when this power of attorney expires, the authority I have granted my agent continues to exist until the time I become able to make health care decisions for myself.
(If Applicable) This power of attorney ends on the following date:
Prior Designations Revoked I revoke any prior medical power of attorney. Acknowledgement of Disclosure Statement I have been provided with a disclosure statement explaining the effect of this document. I have read and understand the information contained in this disclosure statement.
(You Must Date and Sign This Power of Attorney) I sign my name to this medical power of attorney on day of (month, year) at
(City and State)
(Signature)
(Print Name) Statement of First Witness I am not the person appointed as agent by this document. I am not related to the principal by blood or marriage. I would not be entitled to any portion of the principal's estate on the principal's death. I am not the attending physician of the principal or an employee of the attending physician. I have no claim against any portion of the principal's estate on the principal's death. Furthermore, if I am an employee of a health care facility in which the principal is a patient, I am not involved in providing direct patient care to the principal and am not an officer, director, partner, or business office employee of the health care facility or of any parent organization of the health care facility. Signature:
Print Name: Date: Address: Signature of Second Witness
Signature:
Print Name: Date:
Address: version 10/25/99
232

Declaración referente al poder médico Ley de Directivas Anticipadas (ver §166.163, del Código de Salud y Seguridad)
Éste es un documento legal importante. Antes de firmar este documento debe saber esta información importante: Salvo los límites que usted imponga, este documento le da a la persona que usted nombre como su agente la autoridad de tomar, en su nombre, y cuando usted ya no esté en capacidad de tomarlas por su propia cuenta, todas y cada una de las decisiones referentes a la atención médica conforme con sus deseos y teniendo en cuenta sus creencias morales y religiosas. Puesto que "atención médica" se refiere a cualquier tratamiento, servicio o procedimiento para controlar, diagnosticar o tratar cualquier padecimiento físico o mental, su agente tiene el poder de tomar, en su nombre, decisiones sobre una amplia gama de opciones médicas. Su agente puede dar consentimiento, negar consentimiento o retirar el consentimiento para recibir tratamiento médico y puede decidir si suspender o no dar tratamiento para prolongar la vida. Su agente no puede autorizar su ingreso voluntario a un hospital para recibir servicios de salud mental, ni que le den tratamiento convulsivo, psicocirugía o un aborto. El doctor deberá seguir las instrucciones de su agente o permitir que se le cambie a usted de doctor. La autoridad de su agente comenzará cuando su doctor certifique que usted no está en capacidad de tomar decisiones de carácter médico. Su agente tiene la obligación de seguir sus instrucciones cuando tome decisiones en su nombre. A menos que usted especifique lo contrario, su agente tiene la misma autoridad que usted tendría para tomar decisiones sobre su atención médica. Antes de firmar este documento, es muy importante que hable sobre éste con el doctor o con cualquier proveedor médico para asegurarse de que entienda la naturaleza y los límites de las decisiones que se tomarán en su nombre. Si no tiene un doctor, debe hablar con alguien más que sepa de estos asuntos y pueda contestar sus preguntas. No necesita la ayuda de un abogado para hacer este documento, pero si hay algo en este documento que usted no entienda, debe pedirle a un abogado que se lo explique. La persona que usted nombre como su agente debe ser alguien conocido y de su confianza. Debe ser mayor de 18 años, o puede ser menor de 18 años si se le ha retirado la incapacidad de minoría de edad. Si usted nombra al proveedor de atención médica o terapeuta (por ejemplo, su doctor o un empleado del centro de salud, hospital, casa para convalecientes o centro de tratamiento terapéutico, que no sea un pariente) esa persona tiene que escoger entre ser su agente o ser su proveedor de atención médica o terapeuta; conforme con la ley, una misma persona no puede desempeñar las dos funciones a la vez. Debe informarle a la persona que usted escoja que quiere que ella sea su agente de atención médica. Usted debe hablar sobre este documento con su agente y con su doctor y darle a cada uno de ellos una copia firmada. Usted debe escribir en el documento el nombre de las personas e instituciones a quienes ha dado copias firmadas. Su agente no puede ser enjuiciado por las decisiones sobre atención médica tomadas de buena fe en su nombre. Aun después de firmar este documento, usted tiene el derecho de tomar decisiones de atención médica mientras esté en capacidad de hacerlo y no se le puede administrar o detener un tratamiento si usted se opone. Tiene derecho de revocar la autoridad otorgada a su agente informándole a su agente o a su proveedor de atención médica o terapeuta, oralmente o por
233

escrito, y firmando un nuevo poder médico. A menos que indique lo contrario, el nombramiento de su cónyuge como su agente se disuelve en el caso de que usted se divorcie. Este documento no se puede modificar o cambiar. Si quiere hacer algún cambio, tiene que hacer un documento nuevo. Es aconsejable que nombre a un tercer agente en caso de que su agente no quiera, no pueda o esté incapacitado para actuar como su agente. Cualquier agente alterno que usted nombre tendrá la misma autoridad de tomar decisiones de atención médica en su nombre.
Este poder no tiene validez a menos que se firme en presencia de dos testigos adultos hábiles. Las
siguientes personas no pueden actuar como UNO de los testigos: • la persona que usted ha nombrado como su agente; • una persona que es su pariente por sangre o matrimonio; • una persona que, después de su muerte, tenga derecho a cualquier porción de su
sucesión de acuerdo con su testamento o con una adición a su testamento firmado por usted o que tenga derecho a ésta por efecto legal;
• el doctor que lo atiende; • un empleado del doctor que lo atiende; • un empleado de un centro de atención médica del cual usted es paciente si el empleado le
está prestando servicios directamente a usted o es un funcionario, director, socio o empleado de las oficinas del centro de atención médica o de cualquier organización matriz del centro de atención médica; o
• una persona que, en el momento de firmar este poder, pueda reclamar cualquier porción de su sucesión después de su muerte.
234

Poder médico Ley de Directivas Anticipadas (ver §166. 164, del Código de Salud y Seguridad)
Nombramiento de un agente de atención médica: Yo, (escriba su nombre) nombro a:
Nombre:
Dirección:
Teléfono: como mi agente para que tome todas y cada una de las decisiones sobre atención médica por mí, a menos que yo diga lo contrario en este documento. Este poder médico entra en vigor si yo no tengo capacidad para tomar mis propias decisiones sobre la atención médica y mi doctor certifica este hecho por escrito. La autoridad de mi agente médico para tomar decisiones tendrá las siguientes limitaciones: Nombramiento de un agente alterno: (Usted no tiene que nombrar a un agente alterno, pero si quiere puede hacerlo. Un agente alterno puede tomar las mismas decisiones médicas que tomaría el agente designado si el agente designado no puede o no quiere hacer las veces de agente. Si el agente designado es su cónyuge, el nombramiento se revoca automáticamente por ley si su matrimonio se disuelve). Si la persona designada como mi agente no es capaz o no está dispuesta a tomar decisiones médicas por mí, nombro a las siguientes personas, para que hagan las veces de agente para tomar decisiones de tipo médico conforme yo las autorice por medio de este documento. Lo harán en el siguiente orden: Primer Agente Alterno
Nombre:
Dirección:
Teléfono:
Segundo Agente Alterno
Nombre:
Dirección:
Teléfono:
235

El original de este documento se mantendrá en: Las siguientes personas o instituciones tienen copias firmadas: Nombre:
Dirección: Nombre:
Dirección: Duración Comprendo que este poder existirá indefinidamente a partir de la fecha en que se firma el documento a menos que yo establezca un término más corto o lo revoque. Si no estoy en capacidad de tomar decisiones médicas por mi propia cuenta cuando este poder se venza, la autoridad que le he dado a mi agente seguirá en vigor hasta que yo pueda volver a tomar decisiones por mí mismo. (Si aplica) Este poder se vencerá en la siguiente fecha: Revocación de nombramientos anteriores Revoco cualquier poder médico anterior. Acuse de recibo de la Declaración Me dieron la declaración en la que se explica las consecuencias de este documento. La leí y la entiendo. (Tiene que escribir la fecha y firmar este poder) Firmo mi nombre en este poder médico el de (mes) de (año) en (Ciudad y Estado) (Firma) (Nombre en letra de molde) Declaración del primer testigo No soy la persona designada como agente por medio de este documento. No soy pariente del poderante ni por sangre ni por matrimonio. No tendré derecho a ninguna parte de la sucesión del poderante después de su fallecimiento. No soy el médico tratante del poderante ni estoy empleado por el médico tratante. No tengo ningún derecho sobre ninguna porción de la sucesión del poderante después de su fallecimiento. Además, si trabajo en el centro de atención médica
donde es paciente el poderante, no tengo que ver con el cuidado directo del poderante y no soy funcionario, director, socio, ni empleado de la oficina del centro de atención médica ni de ninguna organización matriz del centro de atención médica. Firma: Nombre en letra de molde: Fecha: Dirección:
236

Firma del segundo testigo Firma: Nombre en letra de molde: Fecha: Dirección:
versión 10/25/99
237
Related Documents











