2019 Novel Coronavirus (COVID-19) Inmate Screening/Classification Form Form – J21 ALLAMAKEE COUNTY JAIL Updated – 3/16/2020 CONFIDENTIAL MEDICAL INFORMAION The Allamakee County Jail shall complete the following questionnaire at time of inmate booking to screen inmates for possible exposure to the Coronavirus (COVID-19) to assist with inmate classification if needed. Booking Number:_________________________________________ Inmate Name: ____________________________________________ Time:__________hrs Date: ____________ Screening Questionnaire 1. Does the inmate have a fever (100 or above)? (take inmate temperature with forehead thermometer) Yes No 2. Do you have a cough? a. How long have you had the cough? b. What other health problems do you have? (GERD, smoking, chronic respiratory disease, etc.) If cough is related to a disease process the answer to #2 would be no. Yes No ________________ 3. Do you have new symptoms of shortness of breath? a. When did the symptoms of shortness of breath begin? b. Is there a reason for the shortness of breath? (exercise, anxiety, etc.) If there is a non-medical reason for shortness of breath the answer to #3 would be no. Yes No ________________ ________________ 4. Have you been in direct contact with someone confirmed with COVID-19? If yes, list location: ______________________________ Yes No 5. Have you traveled outside the U.S. in the past two weeks? If yes, list location: ______________________________ Yes No Protocols Initiated: Date: Time: Completed by (staff name):

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
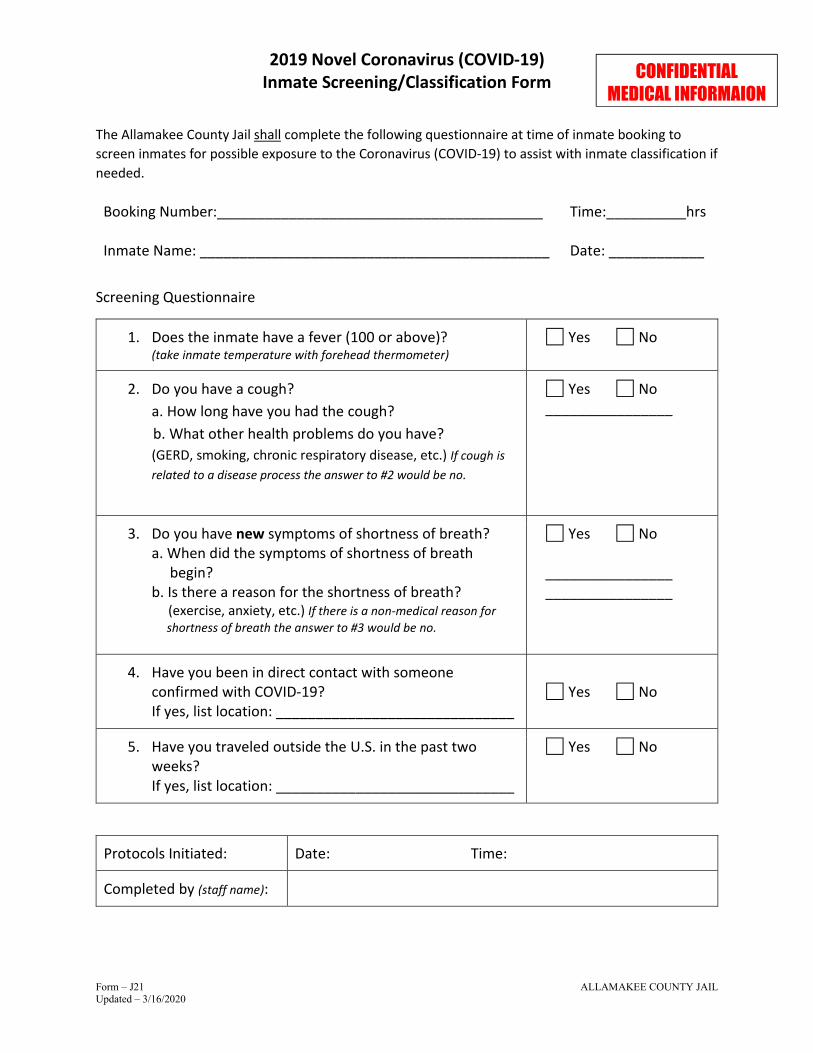
2019 Novel Coronavirus (COVID-19) Inmate Screening/Classification Form
Form – J21 ALLAMAKEE COUNTY JAIL Updated – 3/16/2020
CONFIDENTIAL MEDICAL INFORMAION
The Allamakee County Jail shall complete the following questionnaire at time of inmate booking to
screen inmates for possible exposure to the Coronavirus (COVID-19) to assist with inmate classification if
needed.
Booking Number:_________________________________________
Inmate Name: ____________________________________________
Time:__________hrs
Date: ____________
Screening Questionnaire
1. Does the inmate have a fever (100 or above)? (take inmate temperature with forehead thermometer)
Yes No
2. Do you have a cough?
a. How long have you had the cough?
b. What other health problems do you have?
(GERD, smoking, chronic respiratory disease, etc.) If cough is
related to a disease process the answer to #2 would be no.
Yes No ________________
3. Do you have new symptoms of shortness of breath? a. When did the symptoms of shortness of breath begin? b. Is there a reason for the shortness of breath? (exercise, anxiety, etc.) If there is a non-medical reason for
shortness of breath the answer to #3 would be no.
Yes No ________________ ________________
4. Have you been in direct contact with someone confirmed with COVID-19? If yes, list location: ______________________________
Yes No
5. Have you traveled outside the U.S. in the past two weeks? If yes, list location: ______________________________
Yes No
Protocols Initiated: Date: Time:
Completed by (staff name):

2019 Novel Coronavirus (COVID-19) Inmate Screening/Classification Form
Form – J21 ALLAMAKEE COUNTY JAIL Updated – 3/16/2020
CONFIDENTIAL MEDICAL INFORMAION
JAIL/HEALTH PROVIDER NOTIFICATION PROTOCOLS
If inmate answers yes to two or more of the questions, implement the following protocol;
1. Inmate shall be classified as a possible contagious person.
2. Staff shall implement standard protocols for pathogens / disease.
3. Inmate is to be placed in a special status cell (SS1 or SS2).
4. Staff shall notify Veterans Memorial Hospital at 563-568-3411 and request to speak with
the Charge Nurse for further instructions.
5. Advise arresting officer of possible contamination.
6. Contact Corey Snitker – Allamakee County Emergency Management at 563-568-1911 or
office phone at 563-568-4233.

ALLAMAKEE COUNTY JAIL ADVISORY OF YOUR 804.20 RIGHTS
Inmate Name: Intake Date:
Booking Number: Booking Officer:
804.20 RIGHTS ADVISORY
Any peace officer or other person having custody of any person arrested or restrained of the
person’s liberty for any reason, SHALL allow that person, without unnecessary delay after
arrival at the place of detention to call, consult, and see a member of the person’s family or an
attorney of the person’s choice, or both. Such person shall be permitted to make a reasonable
number of telephone calls as may be required to secure an attorney. If a call is made, it shall be
made in the presence of the person having custody of the one arrested or restrained. If such
person is intoxicated, or a person under 18 years of age, the call may be made by the person
having custody. An attorney shall be permitted to see and consult confidentially with such
person alone, in a private area at the jail or have place of custody with unreasonable delay.
I acknowledge that I have been made aware of 804.20 Rights at this time.
AND
(check one box)
DO / DO NOT want to make any calls to family and/or attorney at this time.
Inmate Signature X______________________________________ Date __________________
Any calls made will be logged into the booking computer at the Allamakee County Jail.

ALLAMAKEE COUNTY JAIL Prison Rape Elimination Act (PREA)
Inmate Name: Intake Date:
Booking Number: Booking Officer:
Handout attached
The Allamakee County Sheriff’s Office is PREA compliant and has a ZERO-TOLERANCE for sexual
misconduct of any kind within its jail facilities of inmates (by inmates and staff). You have been
given a hand out with our agencies policy on sexual misconduct.
The handout contains the following:
OUR AGENCY’S MISSION ON PREVENTING SEXUAL MISCONDUCT
PREVENTERION
DEFINITION OF SEXUAL MISCONDUCT
WHAT TO DO IF YOU ARE A VICTIM
HOW TO REPORT AN ALLEGED INCIDENT
WHO TO REPORT AND ALLEGED INCIDENT TO
RETALIATION
There is additional information regarding this topic in the Inmate Rule Book located in the
section you have been assigned. If you have any questions or concerns, please ask a staff
member.
By signing, I acknowledge that I have received a handout regarding the Allamakee County
Sheriff’s Office policy on Sexual Misconduct within their facilities and that I will read an
familiarize myself with the information I have received.
Inmate Signature X_____________________________________ Date _________________

ALLAMAKEE COUNTY JAIL Inmate Supply Sheet/ Medical Waiver
Inmate Name: Intake Date:
Booking Number: Booking Officer:
SUPPLIES ISSUED AT BOOKING
Qty Item Type Qty Item Type
1 Soap 1 Toilet Paper 1 Blanket 1 Cup 2 Sheet(s) 1 Towel 1 Pillowcase 1 Washcloth 1 PREA handout 1 Comb 1 Uniform 1 Sandals (pr) 1 Toothpaste 1 Toothbrush
PLEASE READ AND SIGN BELOW
I have been informed the Inmate Rule Books are located in the section to which I have been assigned
and I will read and familiarize myself with it. I also understand any violation of rules can result in
disciplinary action. All incoming and outgoing mail that is addressed to me will be censored. The only
exception is mail from my attorney, Judge, Governor of the State of Iowa, Citizen’s Aide Office or a
member of the State or Federal Legislature.
Inmate Signature X______________________________________________
I do not want my mail censored and I understand that because of this, my mail will be placed with my
property until I am released from this facility.
Inmate Signature X_______________________________________________
By signing below, I acknowledge, certify and understand the following:
I answered truthfully the medical questions asked of me. I understand I am financially responsible for all
medical (mental, physical and dental) costs which may incur during my incarceration. I further authorize
the release of this medical information to any doctor or hospital in the event of any medical necessity.
Inmate Signature X_______________________________________________
Upon release from the Allamakee County Jail if personal property is left behind I understand that it is my
responsibility to make arrangements for pickup of that property within 10 days otherwise it will be
destroyed.
Inmate Signature X_______________________________________________
The following inmate has been fingerprinted and a recent picture taken. All property has been moved to
a long term locker and money has been counted, placed on account if requested and secured.
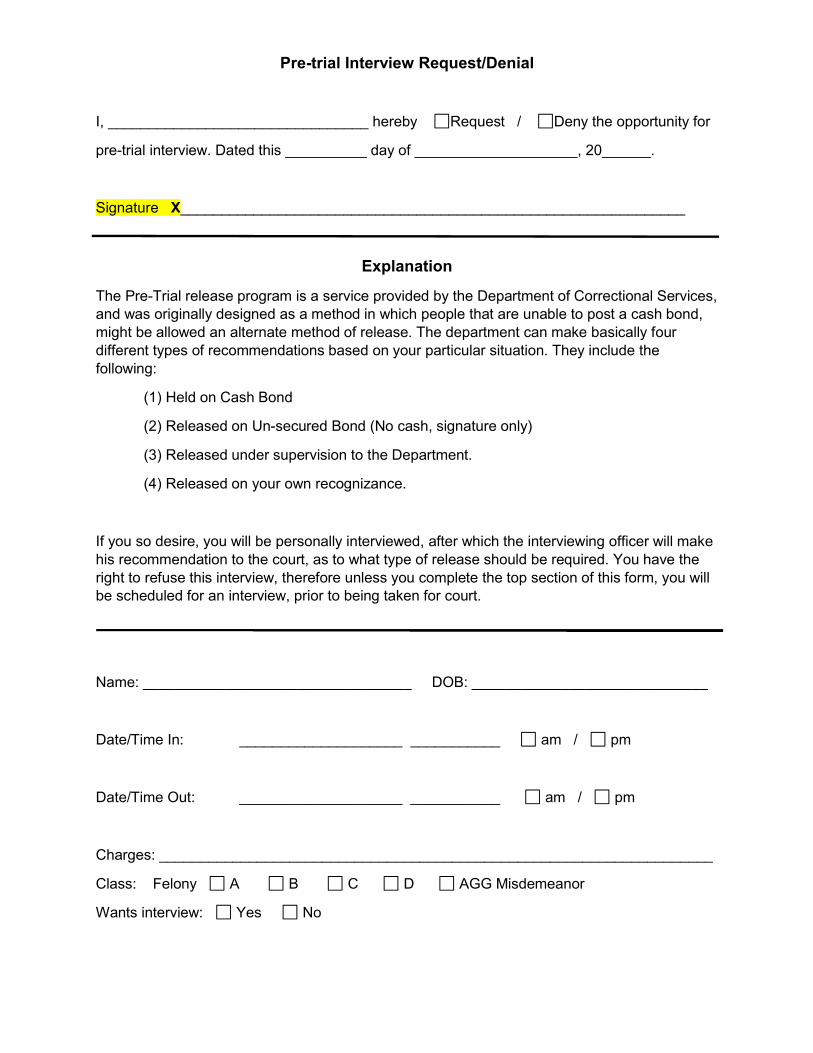
Pre-trial Interview Request/Denial
I, ________________________________ hereby Request / Deny the opportunity for
pre-trial interview. Dated this __________ day of ____________________, 20______.
Signature X______________________________________________________________
Explanation
The Pre-Trial release program is a service provided by the Department of Correctional Services, and was originally designed as a method in which people that are unable to post a cash bond, might be allowed an alternate method of release. The department can make basically four different types of recommendations based on your particular situation. They include the following:
(1) Held on Cash Bond
(2) Released on Un-secured Bond (No cash, signature only)
(3) Released under supervision to the Department.
(4) Released on your own recognizance.
If you so desire, you will be personally interviewed, after which the interviewing officer will make his recommendation to the court, as to what type of release should be required. You have the right to refuse this interview, therefore unless you complete the top section of this form, you will be scheduled for an interview, prior to being taken for court.
Name: _________________________________ DOB: _____________________________
Date/Time In: ____________________ ___________ am / pm
Date/Time Out: ____________________ ___________ am / pm
Charges: ____________________________________________________________________
Class: Felony A B C D AGG Misdemeanor
Wants interview: Yes No
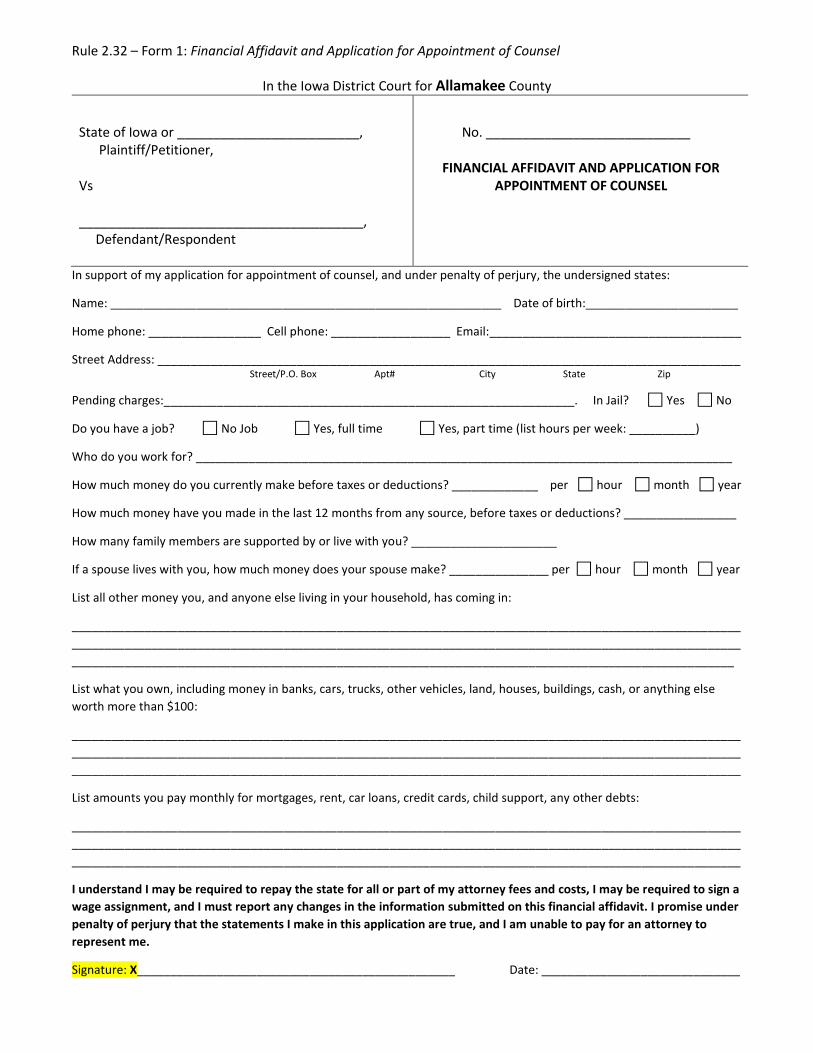
Rule 2.32 – Form 1: Financial Affidavit and Application for Appointment of Counsel
In the Iowa District Court for Allamakee County
State of Iowa or _________________________, Plaintiff/Petitioner, Vs _______________________________________, Defendant/Respondent
No. ____________________________
FINANCIAL AFFIDAVIT AND APPLICATION FOR APPOINTMENT OF COUNSEL
In support of my application for appointment of counsel, and under penalty of perjury, the undersigned states:
Name: ___________________________________________________________ Date of birth:_______________________
Home phone: _________________ Cell phone: __________________ Email:______________________________________
Street Address: ________________________________________________________________________________________ Street/P.O. Box Apt# City State Zip
Pending charges:______________________________________________________________. In Jail? Yes No
Do you have a job? No Job Yes, full time Yes, part time (list hours per week: __________)
Who do you work for? _________________________________________________________________________________
How much money do you currently make before taxes or deductions? _____________ per hour month year
How much money have you made in the last 12 months from any source, before taxes or deductions? _________________
How many family members are supported by or live with you? ______________________
If a spouse lives with you, how much money does your spouse make? _______________ per hour month year
List all other money you, and anyone else living in your household, has coming in:
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
____________________________________________________________________________________________________
List what you own, including money in banks, cars, trucks, other vehicles, land, houses, buildings, cash, or anything else
worth more than $100:
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
List amounts you pay monthly for mortgages, rent, car loans, credit cards, child support, any other debts:
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
I understand I may be required to repay the state for all or part of my attorney fees and costs, I may be required to sign a
wage assignment, and I must report any changes in the information submitted on this financial affidavit. I promise under
penalty of perjury that the statements I make in this application are true, and I am unable to pay for an attorney to
represent me.
Signature: X________________________________________________ Date: ______________________________
Related Documents











